Embed Size (px)
Citation preview

J Formos Med Assoc 2002 • Vol 101 • No 12
V.C. Wu, S.L. Lin, C.C. Tsai, et al
868
(J Formos Med Assoc2002;101:868–70)
Key words:hemolytic uremic syndromeabruptio placenta
Department of Internal Medicine, En Chu Kong Hospital, Taipei; Departments of 1Internal Medicine and 2Pathology, NationalTaiwan University Hospital and College of Medicine, National Taiwan University, Taipei.Received: 5 June 2002. Revised: 18 July 2002. Accepted: 10 September 2002.Reprint requests and correspondence to: Dr. Hwei-Fang Tien, Department of Internal Medicine, National Taiwan UniversityHospital, 7 Chung-Shan South Road, Taipei, Taiwan.
POSTPARTUM HEMOLYTIC UREMIC SYNDROME
FOLLOWING ABRUPTIO PLACENTA: REPORT OF A CASE
Vin-Cent Wu, Shuei-Liong Lin,1 Chien-Chen Tsai,2 and Hwei-Fang Tien1
The traditional diagnostic criteria for hemolytic uremic syn-drome (HUS) include microangiopathic hemolytic anemia,thrombocytopenia and acute renal failure [1]. The associa-tion between thrombotic microangiopathy and pregnancy israre, with an incidence of one per 25,000 births [2]. It usuallyoccurs in primigravida but has also been reported in multipa-rous women, at a mean age of 27 ± 6 years [3]. HUS typicallymanifests with renal failure and severe thrombocytopeniafollowing a symptom-free interval ranging from a few days toseveral weeks after delivery [4]. However, HUS emergingbefore labor or on the day of delivery has also been reported[5, 6]. When HUS occurs during pregnancy, it may beconfused with preeclampsia, leading to a delay in appropriatetreatment. The distinction between HUS and preeclampsia isimportant because prompt diagnosis and treatment reducethe associated morbidity and mortality by as much as 90%[7]. Here, we report a case of postpartum HUS followingabruptio placenta at 34 weeks’ gestation that was successfullytreated with plasma exchange.
Case Report
A 32-year-old woman (gravida 3, para 1, artificial abortion 1)was admitted because of massive vaginal bleeding at 34
Abstract: Postpartum hemolytic uremic syndrome (HUS) is an unusual complicationthat presents with microangiopathic hemolytic anemia, thrombocytopenia, and acuterenal failure after delivery. In this report, we describe a 32-year-old patient (gravida3, para 1, artificial abortion 1) who developed postpartum HUS following abruptioplacenta. After cesarean delivery due to abruptio placenta, the patient developedacute renal failure, microangiopathic hemolytic anemia, and thrombocytopeniafollowed by hypertension. Plasma exchange led to recovery from thrombocytopeniaand improvement in renal function. This case highlights the importance of obser-vation of peripheral blood smears in patients with abruptio placenta who developthrombocytopenia after delivery.
weeks’ gestation. No hypertension, proteinuria, edema orsudden increase in weight was noted during serial antepar-tum examinations. The patient’s blood pressure was 86/50 mmHg at admission. Clinical findings included externaluterine bleeding, uterine hypertonus and hyperactivity,and fetal death. Laboratory studies disclosed a hemoglobin(Hb) level of 12.4 g/dL and a platelet count of 53,000/µL.The patient underwent cesarean section because of abruptioplacenta with fetal death in utero. The body weight of thefetus was 2.1 kg. Sections of the placenta revealed intensehemorrhage with blood clot formation and hyaline necrosis,which was consistent with abruptio placenta. The patient’sblood pressure returned to 100/76 mmHg 6 hourspostoperatively.
Twenty-four hours after cesarean section, the patientdeveloped anemia (Hb, 6.8 g/dL) and thrombocytopenia(platelet count, 22,000/µL). Packed red blood cells 4 U andplatelets 18 U were given, after which the patient’s bloodpressure rose to 150/72 mmHg. She was then transferred toNational Taiwan University Hospital for further evaluationand treatment on the third postpartum day. There was nomore vaginal bleeding after arrival. No purpura was found onphysical examination. Repeated blood examination revealedanemia (Hb, 6.0 g/dL) with normal reticulocytes (2.44%),thrombocytopenia (platelet count, 16,000/µL), normal pro-thrombin time (13.7 sec) and activated partial thromboplastintime (44.9 sec), negative plasma, protamine, paracoagulation
BRIEF COMMUNICATIONS

J Formos Med Assoc 2002 • Vol 101 • No 12 869
Hemolytic Uremic Syndrome Following Abruptio Placenta
(3p) test, mild elevation of fibrin-degradation products (10–20 µg/mL), and negative direct and indirect Coombs’ tests.Blood chemistry revealed marked elevation of serum lactatedehydrogenase (LDH) level (5,830 U/L), mild elevation ofserum glutamate-oxaloacetate transaminase (73 IU/L), butnormal serum glutamate-pyruvate transaminase level (GPT; 2IU/L). The blood urea nitrogen level was elevated to 68.3 mg/dL and serum creatinine level was 6.0 mg/dL, with daily urineoutput of 3,850 mL. Serum bilirubin was mildly elevated(total bilirubin, 1.35 mg/dL).
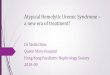
Fragmented red blood cells (schistocytes and helmetforms) and poikilocytosis were found in the blood smears (Fig.1). Urinalysis showed microscopic hematuria and proteinuria.Marked hypertension of up to 209/103 mmHg was noted, andwas controlled with labetalol from the third to the sixthpostpartum days. Hb and platelet levels remained low, eventhough no abnormal vaginal bleeding was noted afteradmission, and packed red blood cells were repeatedlytransfused.
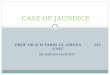
Because HUS was highly suspected, the patient receivedsix courses of plasma exchange starting on the fifth postpar-tum day. Hemodialysis was also performed once on thefifth postpartum day. Dramatic improvements in renal func-tion and the hemogram were noted after plasma exchange(Fig. 2). On the 10th postoperative day, creatinine level was4.33 mg/dL, platelet count was 427,000/µL, Hb was 10.6 g/dL, and LDH was 1,188 U/L. The creatinine level droppedfurther to 2.32 mg/dL 4 days later. Renal biopsy on the 12thpostpartum day showed focal increase in mesangial cellular-ity and matrix, with swollen endothelium and focal oblitera-tion of capillary lumina. Periodic acid-Schiff stain revealedfocal, double-contour appearance of glomerular basementmembrane. Electron microscopy showed endothelial changewith sub-endothelial loosening and an appearance compat-ible with thrombotic microangiopathy (Fig. 3). No neurologicsymptoms or signs were noted during the hospitalization. Thepatient was discharged in a stable condition on the 19thpostpartum day. Serum creatinine level was 0.67 mg/dL 1
●
●
●
●
●
●●
● ●
●
■
■
■ ■■■
■
■
■
▲
◆
◆
▲
▲
▲
▲
▲
▲
▲▲
▲
▲
▲
◆
LD
H (
U/L
)
8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0
0 5 10 15
Seru
m c
reat
inin
e (m
g/dL
)
10
9
8
7
6
5
4
3
2
1
0
Plat
elet
s (x
100/
uL)
Days postpartum
Days of plasma exchangeDay of hemodialysis
Fig. 1. Peripheral blood smear showing fragmented red blood cells(arrow) and poikilocytosis.
Fig. 2. Association of plasma exchange with improvement in lactatedehydrogenase (LDH), platelets and serum creatinine levels.
Fig. 3. Electron microscopy of a segment of the glomerular capillaryshowing endothelial change and electron-lucent fluffy material (arrow)deposited in the sub-endothelium (original magnification x 3,000).
month after discharge and on follow-up 6 months later. Thepatient remained normotensive with no signs of impairedrenal function.
Discussion
HUS seems to occur under certain stresses, includinginfections, autoimmune diseases, intake of certain medicines,

J Formos Med Assoc 2002 • Vol 101 • No 12
V.C. Wu, S.L. Lin, C.C. Tsai, et al
870
pregnancy, or even idiopathically. In pregnant women withthrombocytopenia, it is not easy to distinguish HUS fromthrombotic thrombocytopenic purpura (TTP) andpreeclampsia, specifically the variant called HELLP syn-drome (hemolysis, elevated liver enzymes and low plateletcount). HUS and TTP have similar clinical pictures ofhypertension, hemolysis, elevated liver enzymes, low plate-let counts, and renal failure [3]. However, TTP usually occursin the first trimester, while HUS is typically seen in theperipartum or postpartum period [8]. Unlike TTP, HUS hasfew neurologic deficits but usually shows severe renalinvolvement. The absence of impaired consciousness and thepresence of acute renal failure in our patient favored thediagnosis of HUS rather than TTP.
This patient lacked clinical and laboratory evidence ofcoagulopathy during progressive anemia and thrombocy-topenia after delivery. Furthermore, the findings of normalGPT level and the development of progressive renal dysfunc-tion and thrombocytopenia, as well as hemolysis after cesar-ean section, made the diagnosis of HELLP unlikely. On theother hand, persistent renal failure, thrombocytopenia,microangiopathic hemolytic anemia with fragmented redblood cells in peripheral blood smear after delivery, and thehistopathologic findings of the renal biopsy, supported thediagnosis of HUS. Also, an accurate diagnosis to differentiateHUS from preeclampsia is required because early, intensivetreatment can reduce the associated morbidity and mortalityof HUS by as much as 90% [7].
Remuzzi et al first demonstrated how plasma exchangecould successfully correct thrombocytopenia in adult pa-tients with HUS [9]. The patient in our report also showeddramatic improvement after plasma exchange. Pajor et alreported a similar case of postpartum HUS following abruptioplacenta and proposed that placental substances releasedinto the maternal circulation during and after separation ofthe placenta may be a factor in triggering HUS; this patientalso responded well to plasma exchange, with rapid improve-ment of clinical and laboratory profile [10]. Dashe et alreported the long-term consequences in patients with throm-botic microangiopathy in pregnancy [2]. In their review of 13cases of TTP or HUS associated with pregnancy, at least onerecurrence of thrombotic microangiopathy appeared in halfof the patients. Three women suffered from multiple relapses,and one died. In our patient, there was no residual renalinsufficiency or hypertension. Sibai et al reported that theprognosis was most favorable in patients with reversible
acute tubular necrosis without preexisting chronic hyperten-sion [11].
In summary, a high index of suspicion is needed torecognize thrombotic microangiopathy in pregnancy, as manywomen with this disorder present initially with symptoms thatare non-specific or may be confused with preeclampsia. Ifdelivery does not ameliorate the condition after 72 hours, thediagnosis of TTP or HUS must be considered. Once thediagnosis is made, prompt and aggressive therapy with plasmaexchange is indicated.
References
1. Thompson CE , Damon LE , R ies CA: Thrombot icmicroangiopathies in the 1980s: clinical features, response totreatment, and the impact of the human immunodeficiency virusepidemic. Blood 1992;80:1890–5.
2. Dashe JS, Ramin SM, Cunningham FG: The long-term subse-quence of thrombotic microangiopathy in pregnancy. ObstetGynecol 1998;91:662–8.
3. Weiner CP: Thrombotic microangiopathy in pregnancy and thepostpartum period. Semin Hematol 1987;24:119–29.
4. Churg J, Kottler D, Paronetto F, et al: Hemolytic uremic syn-drome as a cause of postpartum renal failure. Am J ObstetGynecol 1970;108:253–61.
5. Ponticelli C, Imbasciati E, Tarantino A, et al: Postpartum renalfailure with microangiopathic hemolytic anemia. Nephron 1972;9:27–41.
6. Jacobs P. Hemolytic-uremic syndrome during the first trimester ofpregnancy. Case report. Br J Obstet Gynaecol 1983;90:578–80.
7. Bell WR, Braine HG, Ness PM, et al: Improvement in survival inthrombotic thrombocytopenic purpura-hemolytic uremicsyndrome. Clinical experience in 108 patients. N Engl J Med1991;325:398–403.
8. Esplin MS, Branch DW: Diagnosis and management of throm-botic microangiopathies during pregnancy. Clin Obstet Gynecol1999;42:360–7.
9. Remuzzi G, Misiani R, Marchesi D, et al: Treatment of thehemolytic uremic syndrome with plasma exchange. Clin Nephrol1979;12:279–84.
10. Pajor A, Hintalan A, Bakos L, et al: Postpartum hemolytic uremicsyndrome following placental abruption. Eur J Obstet GynecolReprod Biol 1993;49:201–4.
11. Sibai BM, Ramadan MK: Acute renal failure in pregnanciescomplicated by hemolysis, elevated liver enzymes, and lowplatelets. Am J Obstet Gynecol 1993;168:1682–90.