Embed Size (px)
Citation preview
Atypical Hemolytic Uremic Syndrome – a new era of treatment?
Dr Stella Chim
Queen Mary Hospital
Hong Kong Paediatric Nephrology Society
2018-09
Case presentation
Background
M/4 years old Gestation 35 weeks Emergency Caesarean section x severe IUGR Birth weight 1.325 kg Medical history: Anaemia treated with iron and folate supplement in
neonatal period (no haemolysis, normal bone marrow response)
History
1st episode of atypical HUS at 17 months old
Initially presented with gastroenteritis, given
symptomatic medication from private doctor
On day 4 of fever, developed 4 episodes of generalised
tonic-clonic seizures
Suspected enterovirus-related encephalitis
CT brain: no focal lesion
CSF biochemistry, cultures not suggestive of meningitis
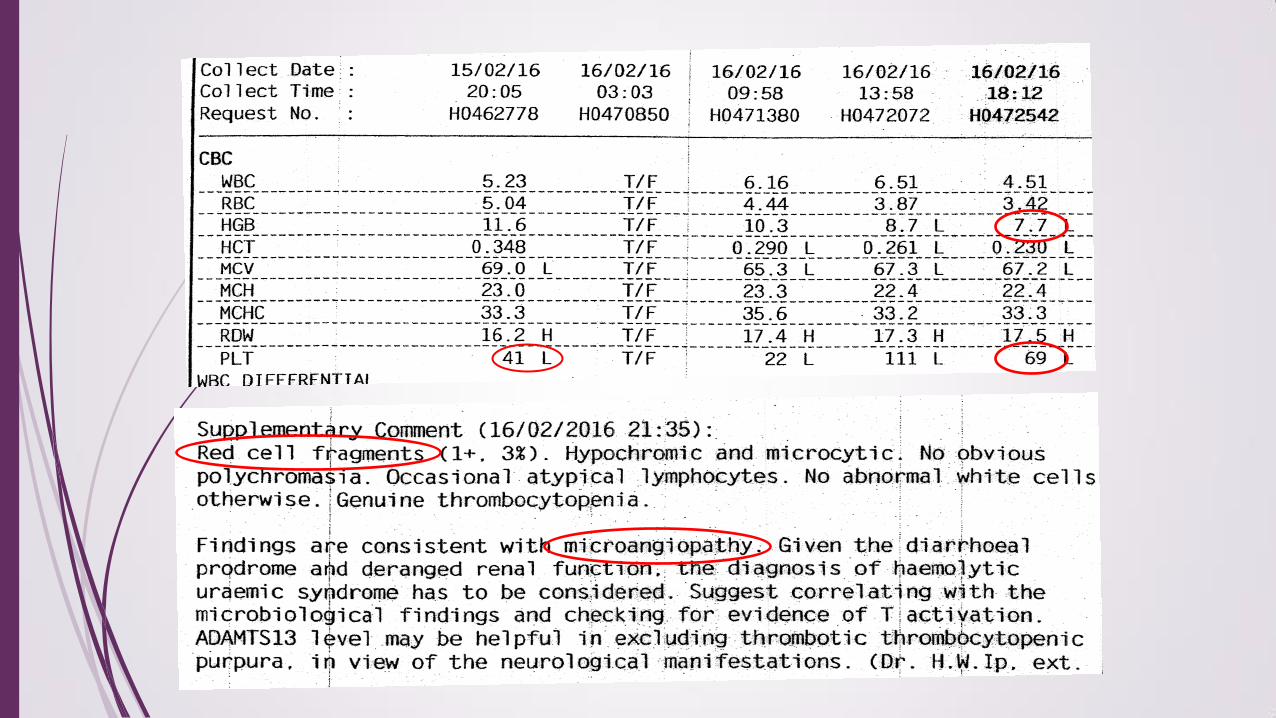
Investigations:
Microangiopathic haemolytic anaemia
Thrombocytopaenia
Acute kidney injury
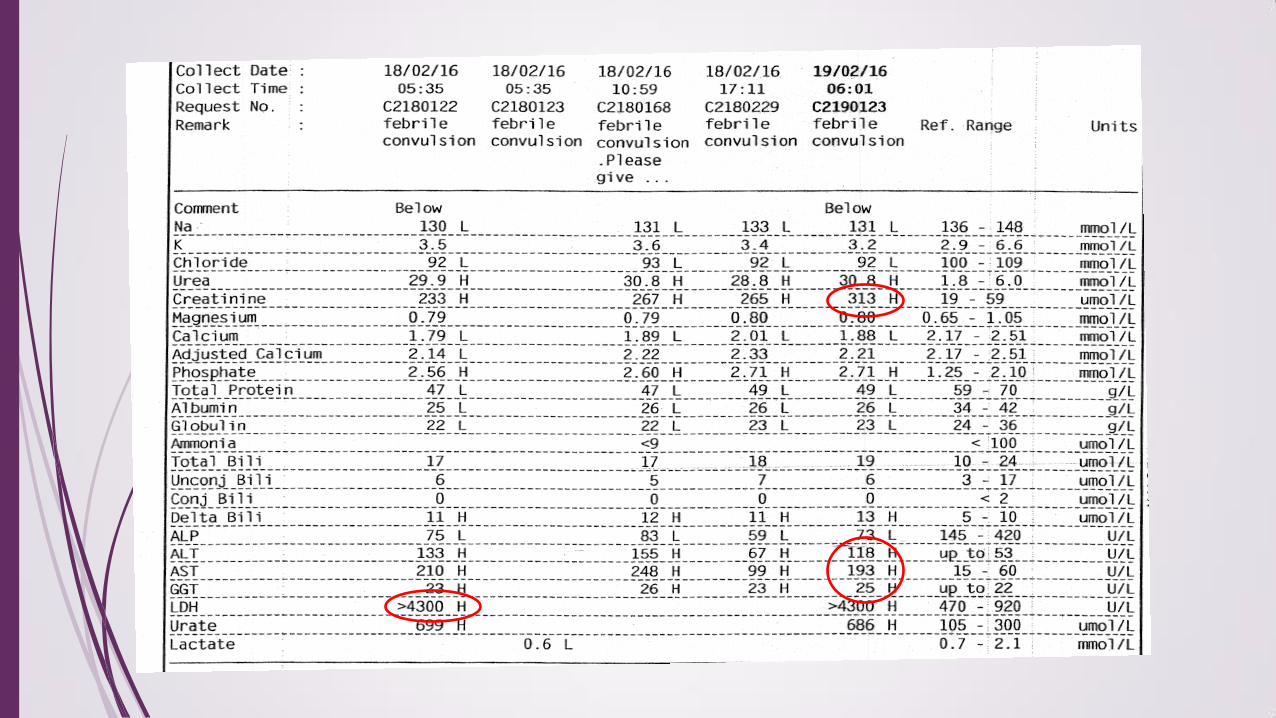
Deranged liver function
Raised LDH, urine haemastix large (RBC < 30/ul)
Clinically suspicious of thrombotic thrombocytopaenic purpura (TTP)
ADAMTS13 activity only marginally low —> not suggestive of TTP
In view of near normal ADAMTS13 activity, absence of autoantibody against
ADAMTS13 and prominent renal impairment, suspected haemolytic uraemia
syndrome
Workup for haemolytic uraemia syndrome
NPA: H1 influenza A virus detected
Stool x Enterovirus, Norovirus, Rotavirus negative
Stool bacterial C/ST negative
Urine x streptococcal antigen negative
T-antigen activation (pneumococcal associated HUS) negative
—> atypical HUS (aHUS)
Started methylprednisolone, later switched to oral prednisolone
Total 7 sessions of therapeutic plasma exchange done
Acute kidney injury with creatinine up to 313 umol/L and
oliguria, requiring renal replacement therapy (CVVHDF for 6
days, PD for 14 days)
Complete haematological recovery after plasma exchange, liver
function normalised
Renal function returned after 1 month. No need for chronic
dialysis
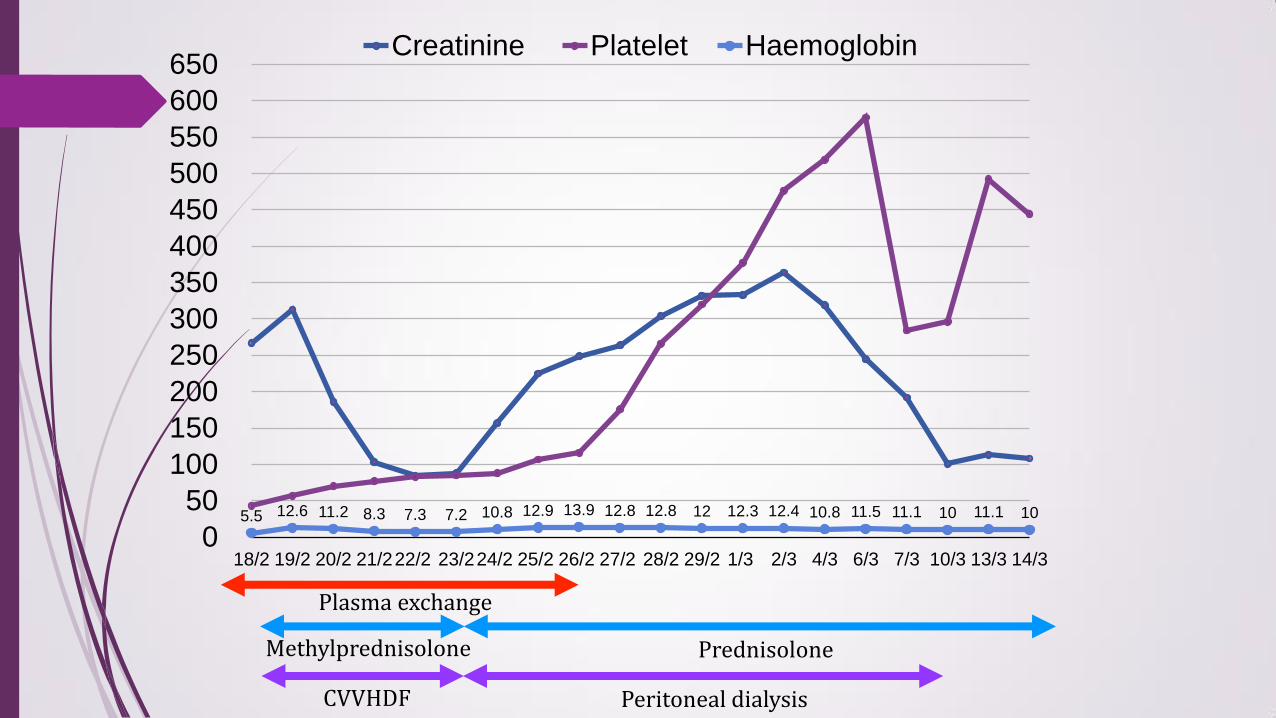
5.5 12.6 11.2 8.3 7.3 7.2 10.8 12.9 13.9 12.8 12.8 12 12.3 12.4 10.8 11.5 11.1 10 11.1 10
0
50
100
150
200
250
300
350
400
450
500
550
600
650
18/2 19/2 20/2 21/222/2 23/224/2 25/2 26/2 27/2 28/2 29/2 1/3 2/3 4/3 6/3 7/3 10/3 13/3 14/3
Creatinine Platelet Haemoglobin
Plasma exchange
Methylprednisolone Prednisolone
Peritoneal dialysis CVVHDF
Overseas genetic testing for aHUS No known pathogenic mutations for CFH, CFI, MCP,
C3, CFB, THBD, DGKE genes Anti-factor H autoantibodies not detected C4 slightly slow, C3 normal, factor H normal Complement factor I 14 mg/L (21-40)
2nd episode of aHUS at 30 months old
Presented with fever and coryzal symptoms
Clinically rhonchi and crepitations bilaterally
Associated with on-off diarrhoea
NPA: metapneumovirus detected —> treated as viral
pneumonitis
After admission, noted 3 episodes of abnormal eye
movement with uncontrolled upward gaze
No seizure or loss of consciousness
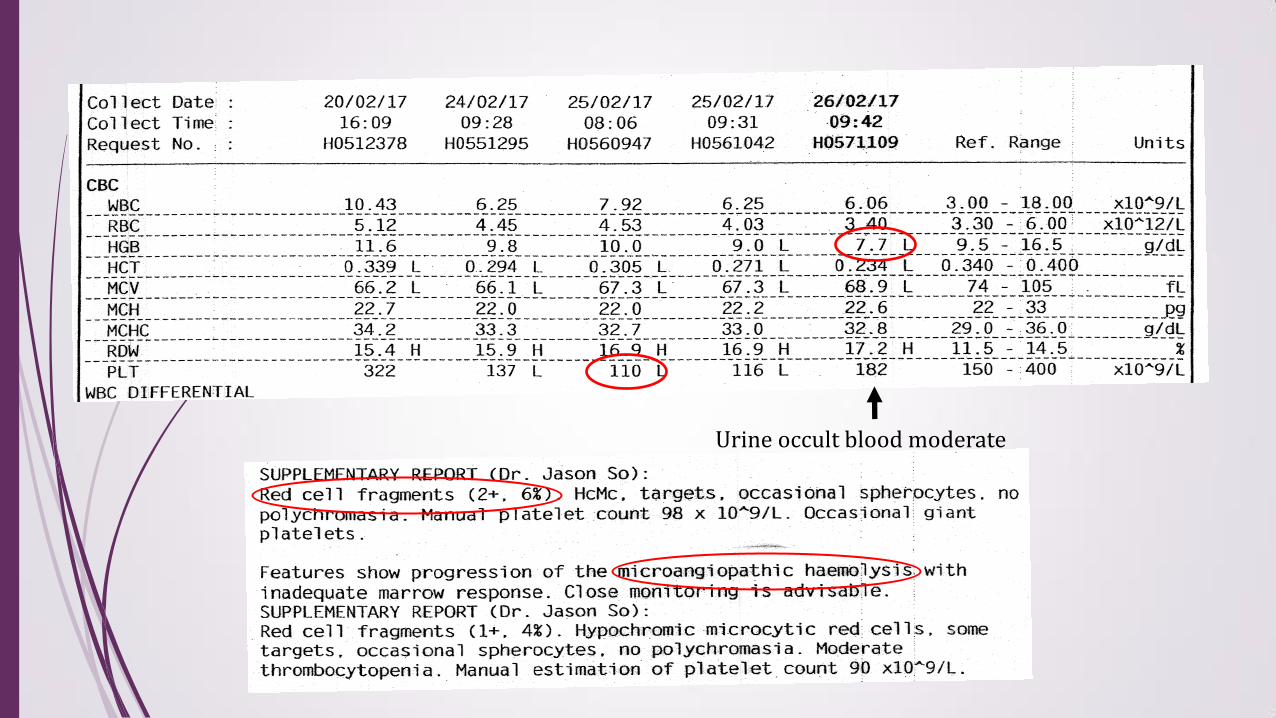
Urine occult blood moderate
Investigations
Microangiopathic haemolytic anaemia
Thrombocytopaenia
Deranged renal function
Raised LDH, urine haemastix moderate (RBC <30/ul)
Stool x Enterovirus, Norovirus, Rotavirus negative
Stool bacterial C/ST negative
Throat swab commensals
T-antigen negative
ADAMTS13 activity normal
Treated as recurrent aHUS
Given 3 doses of Eculizumab on 25/2/2017, 4/3/2017 and
24/3/2017
Already received Haemophilus influenza B and Pneumoccocal
vaccine. Given Penicillin V as meningococcal prophylaxis before
giving Eculizumab
Did not require plasma exchange or RRT
Gradual resolution of anaemia and thrombocytopaenia. Renal
function normalised
Received quadrivalent meningococcal vaccine and
meningococcal B vaccine on follow-up
3rd episode of aHUS at 3.5 years old Presented with fever and coryzal symptoms NPA Influenza B positive, given Tamiflu
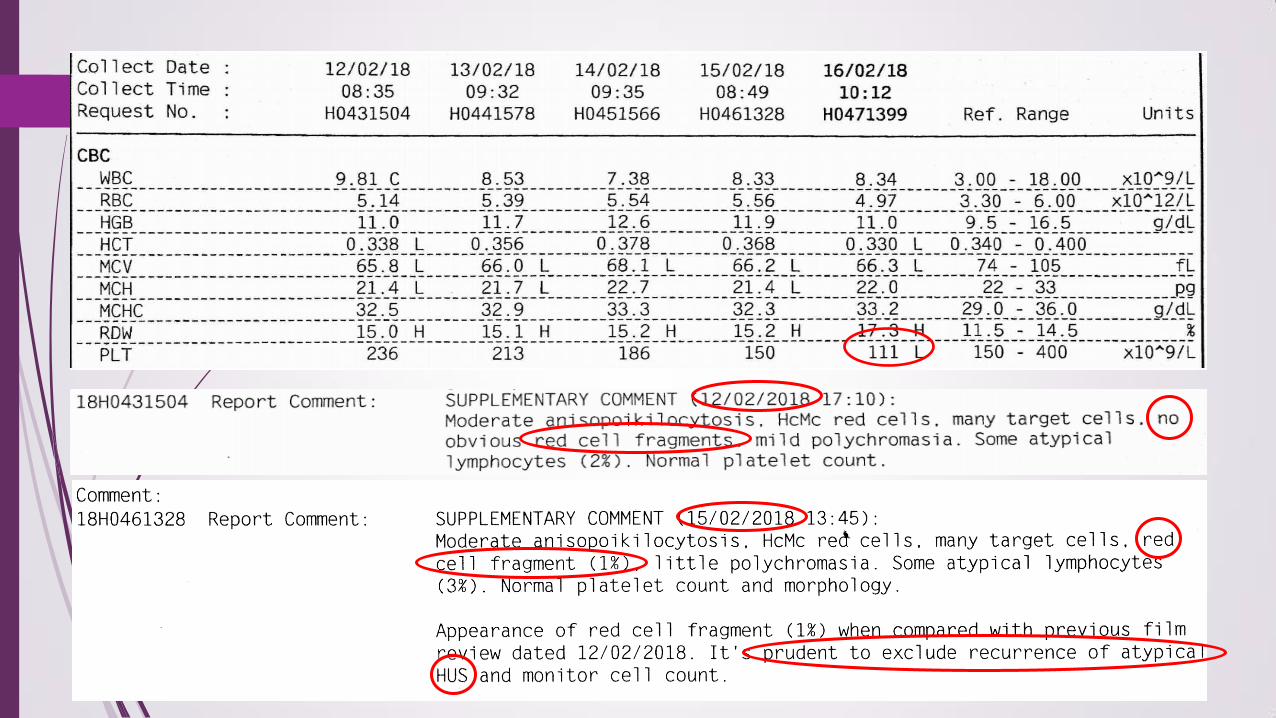
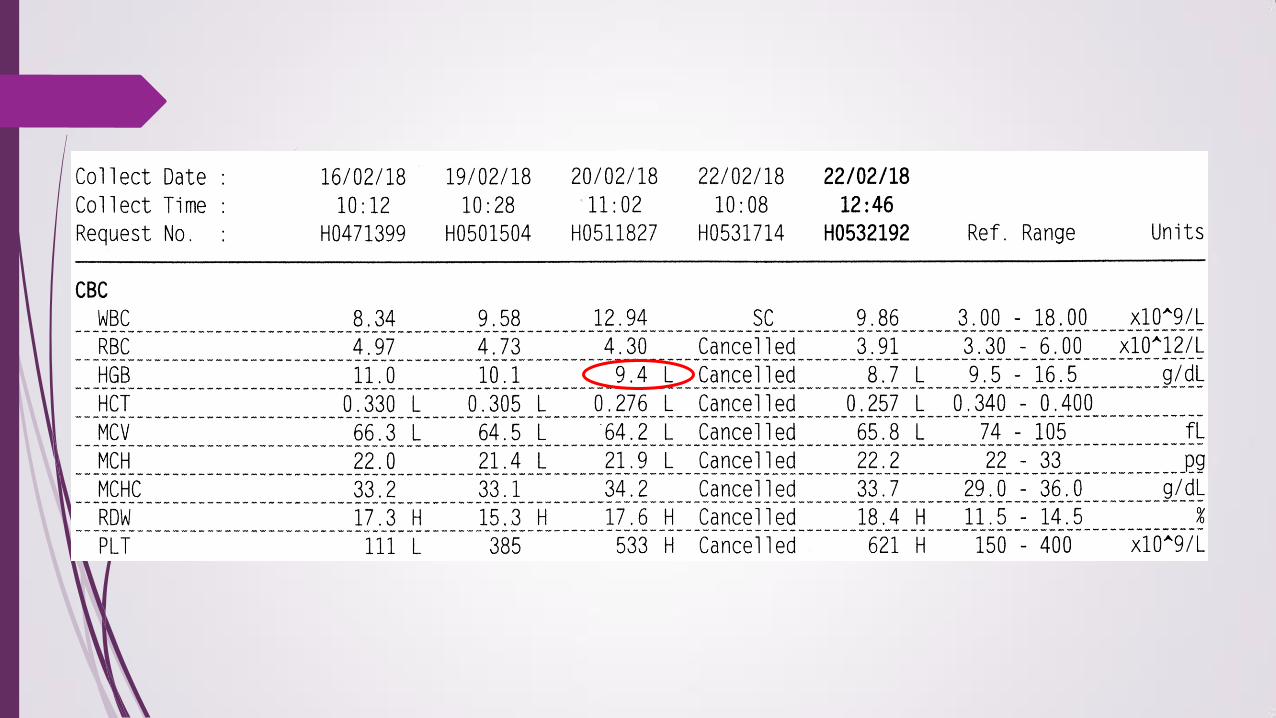
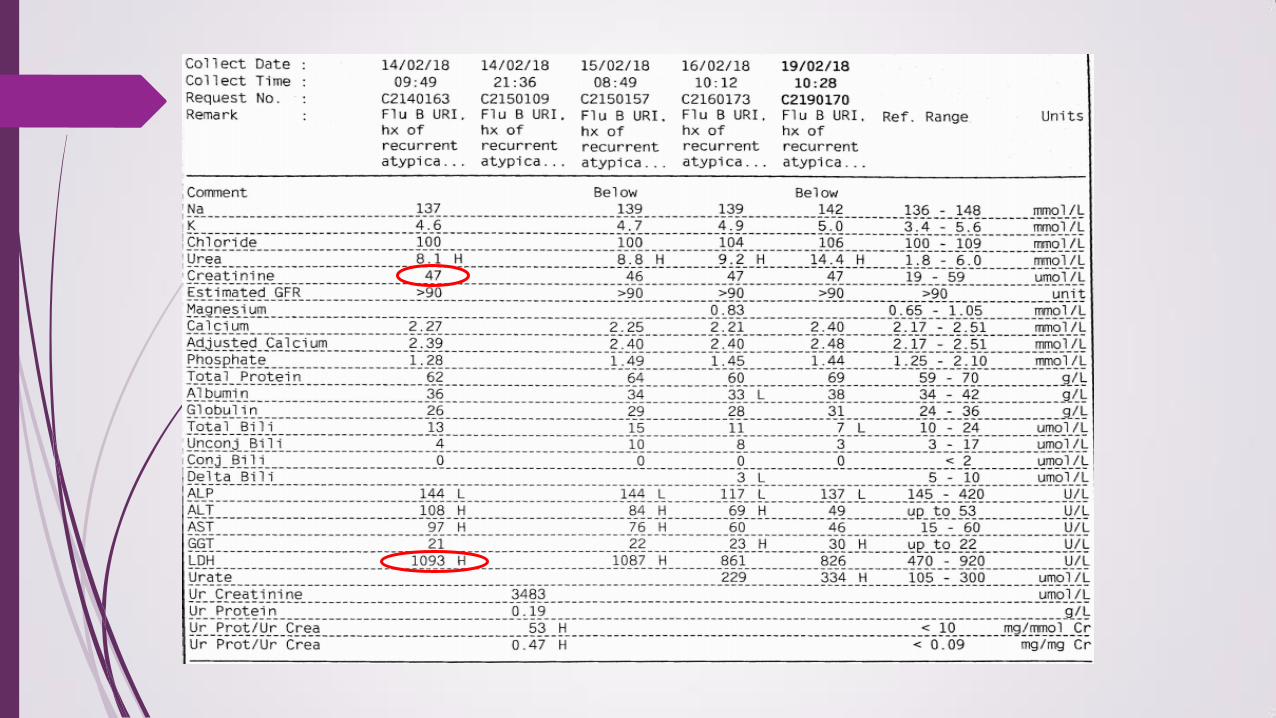
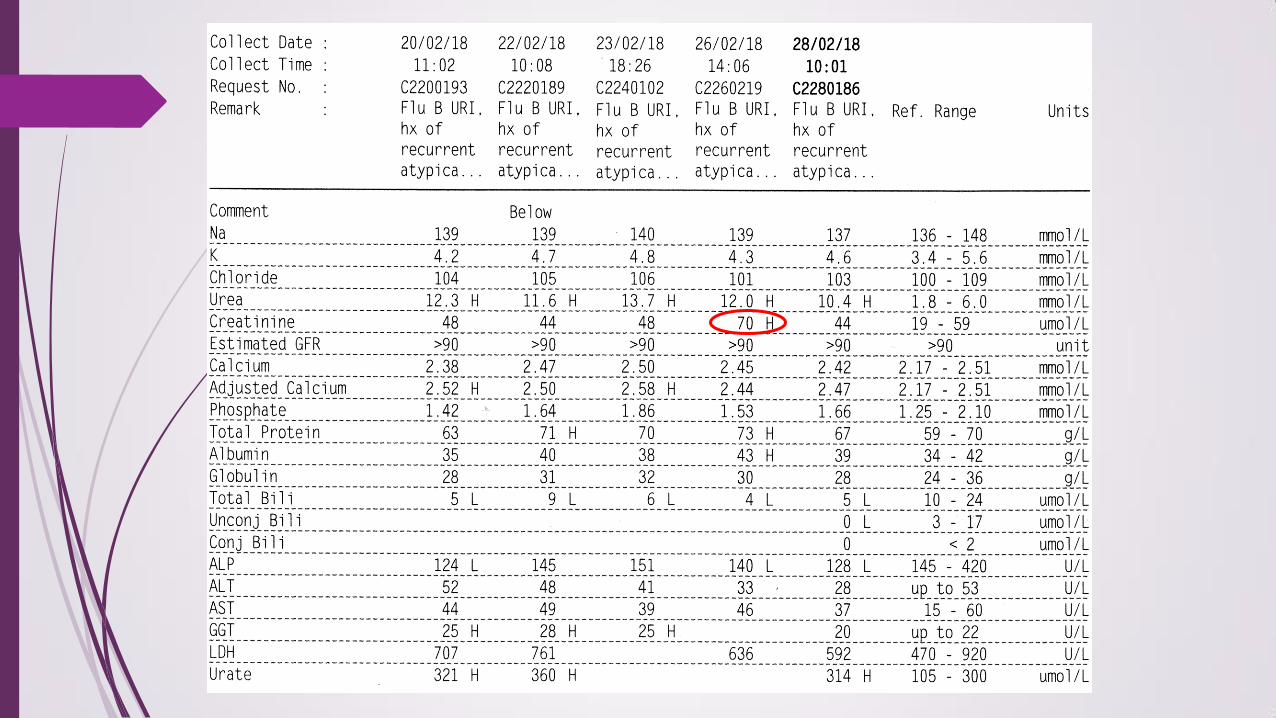
Red cells fragments, raised LDH, urine haemastix trace/neg, Cr normal (14-15 Feb 2018) dropped in platelet dropped in Hb raised creatinine
Noted 1 episode of abnormal eye movement with vertical movement of eyes
No seizure or loss of consciousness Proceeded to Eculizumab infusion in view of
haemolysis, given on 15/2/2018, 22/2/2018 and 8/3/2018
Haemolytic picture resolved, platelet count normalised
Diagnosis of Hemolytic Uremic Syndrome (HUS)
Diagnosis of HUS
Microangiopathic hemolytic anemia
Thrombocytopenia
Acute kidney injury
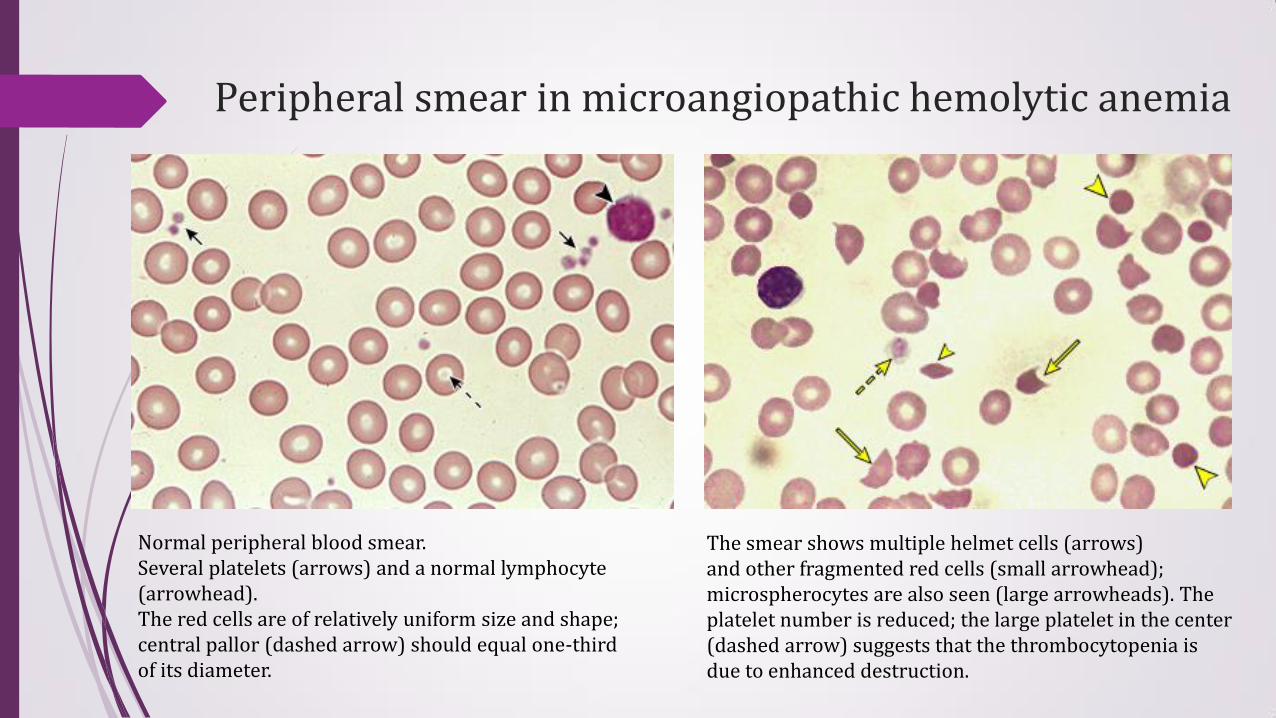
Peripheral smear in microangiopathic hemolytic anemia
The smear shows multiple helmet cells (arrows) and other fragmented red cells (small arrowhead); microspherocytes are also seen (large arrowheads). The platelet number is reduced; the large platelet in the center (dashed arrow) suggests that the thrombocytopenia is due to enhanced destruction.
Normal peripheral blood smear. Several platelets (arrows) and a normal lymphocyte (arrowhead). The red cells are of relatively uniform size and shape; central pallor (dashed arrow) should equal one-third of its diameter.
Management of atypical HUS
Atypical hemolytic uremic syndrome (aHUS) in the last decade
In under a decade, complement alternative pathway (AP) dysregulation has emerged as the major cause of aHUS
Facilitated development of novel, rational treatment options targeting terminal complement activation
E.g. using an anti-C5 antibody Eculizumab
Propose a diagnostic and therapeutic approach for aHUS in children
Introduction
Complement alternative pathway (AP) dysregulation is responsible for 60-70% of cases of aHUS
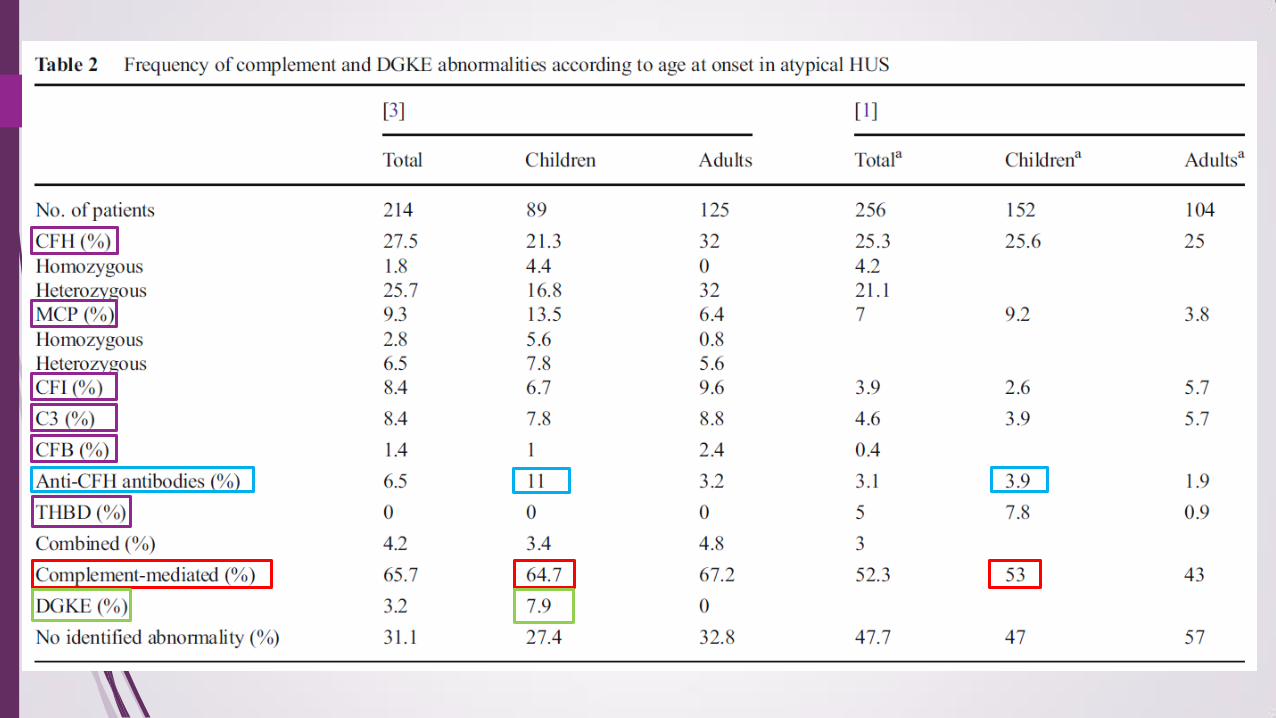
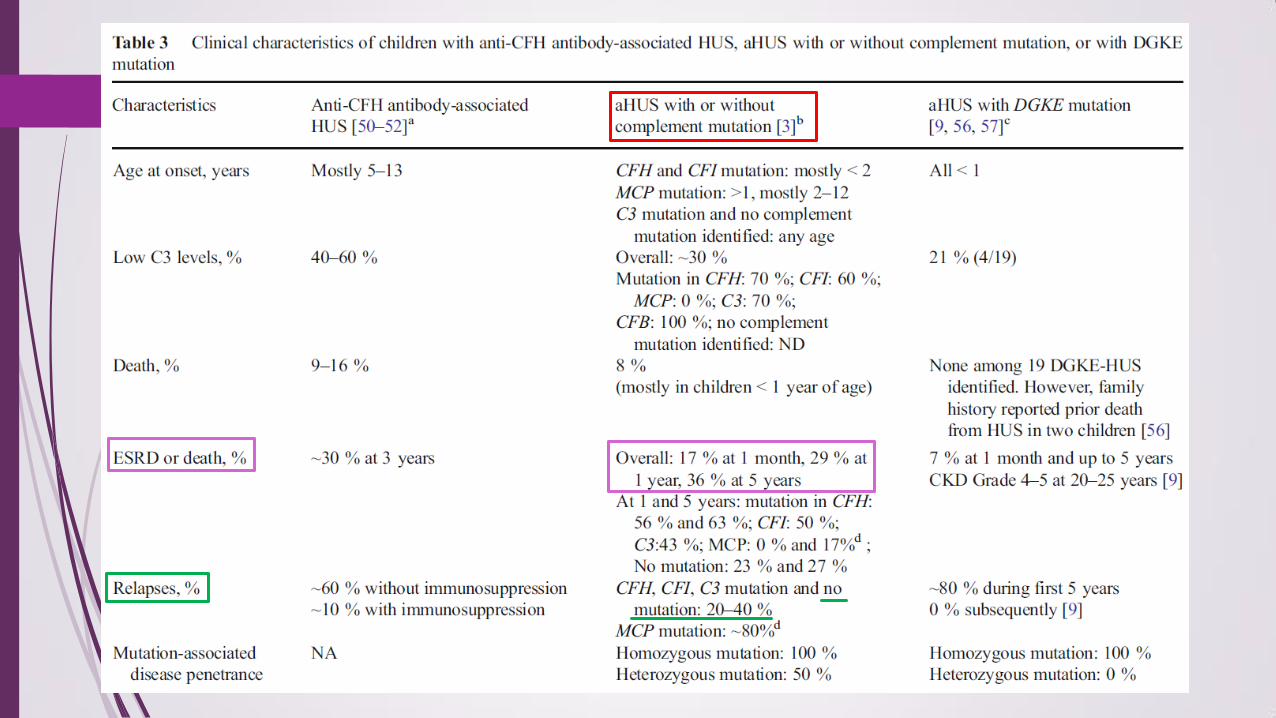
Genotype-phenotype correlations
More precise definition of aHUS HUS without coexisting disease
Identified mutations in gene encoding diacylglycerol kinase (DGKE) suggest complement-independent forms of aHUS
Introduction
Plasma therapy was mainstay of treatment for aHUS until 2009
Since 2009, 4 prospective trials and over 80 case reports on the effective terminal complement blockage with eculizumab
Rescue native kidney function or allow successful kidney transplantation after renal loss due to aHUS
Definition of atypical HUS
Etiology and pathophysiology-based classification of various forms of thrombotic microangiopathies (TMA)
Emerging agreement among haematologists and nephrologists that aHUS should be reserved for HUS without coexisting disease
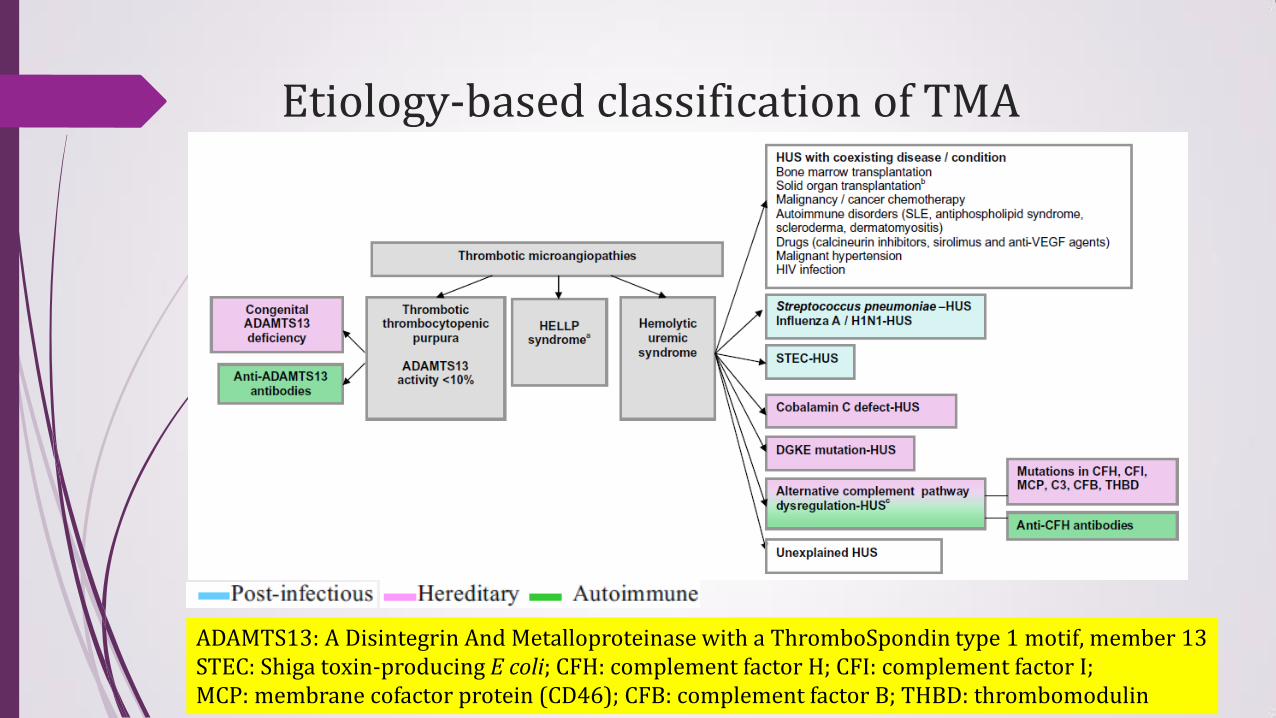
Etiology-based classification of TMA
ADAMTS13: A Disintegrin And Metalloproteinase with a ThromboSpondin type 1 motif, member 13 STEC: Shiga toxin-producing E coli; CFH: complement factor H; CFI: complement factor I; MCP: membrane cofactor protein (CD46); CFB: complement factor B; THBD: thrombomodulin
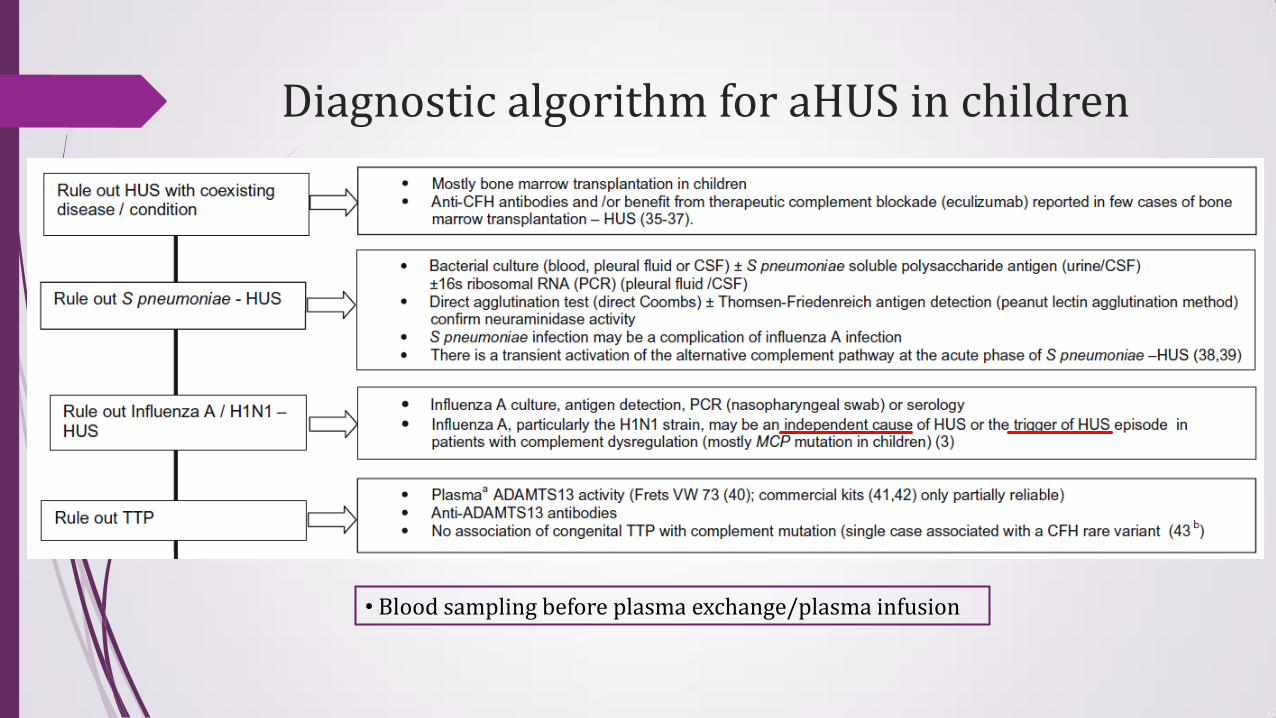
Diagnostic algorithm for aHUS in children
• Blood sampling before plasma exchange/plasma infusion
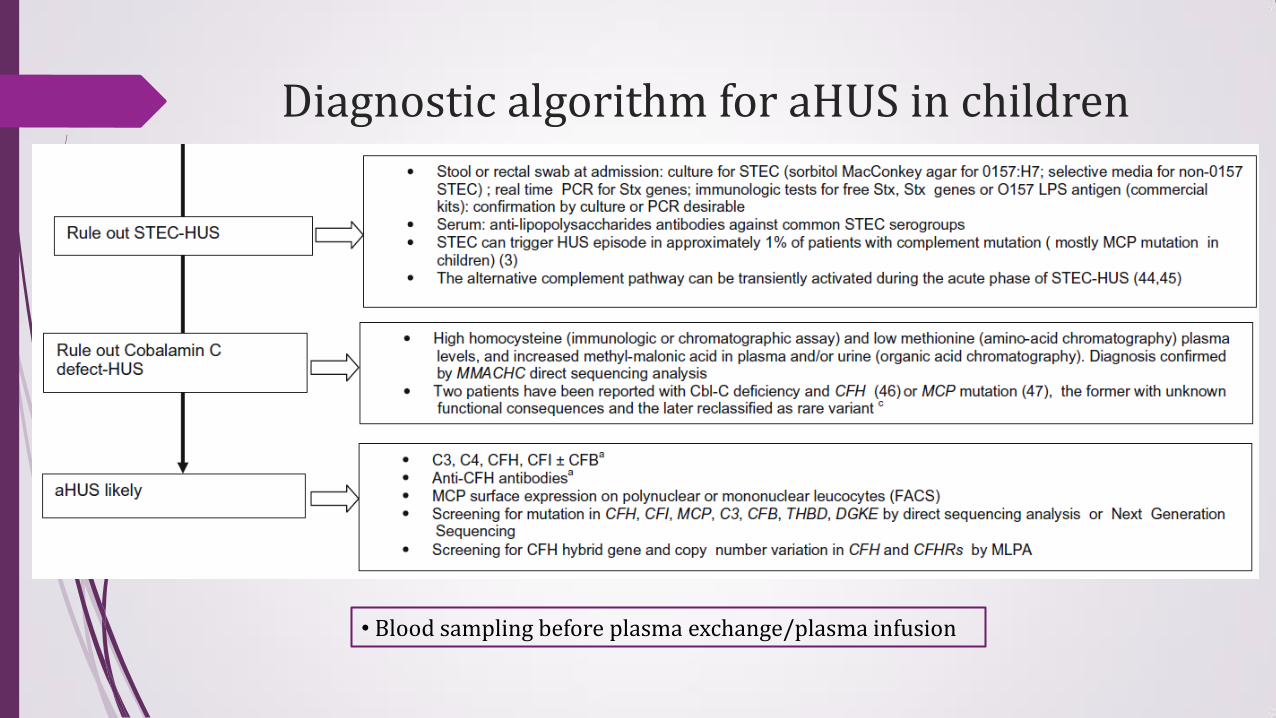
Diagnostic algorithm for aHUS in children
• Blood sampling before plasma exchange/plasma infusion
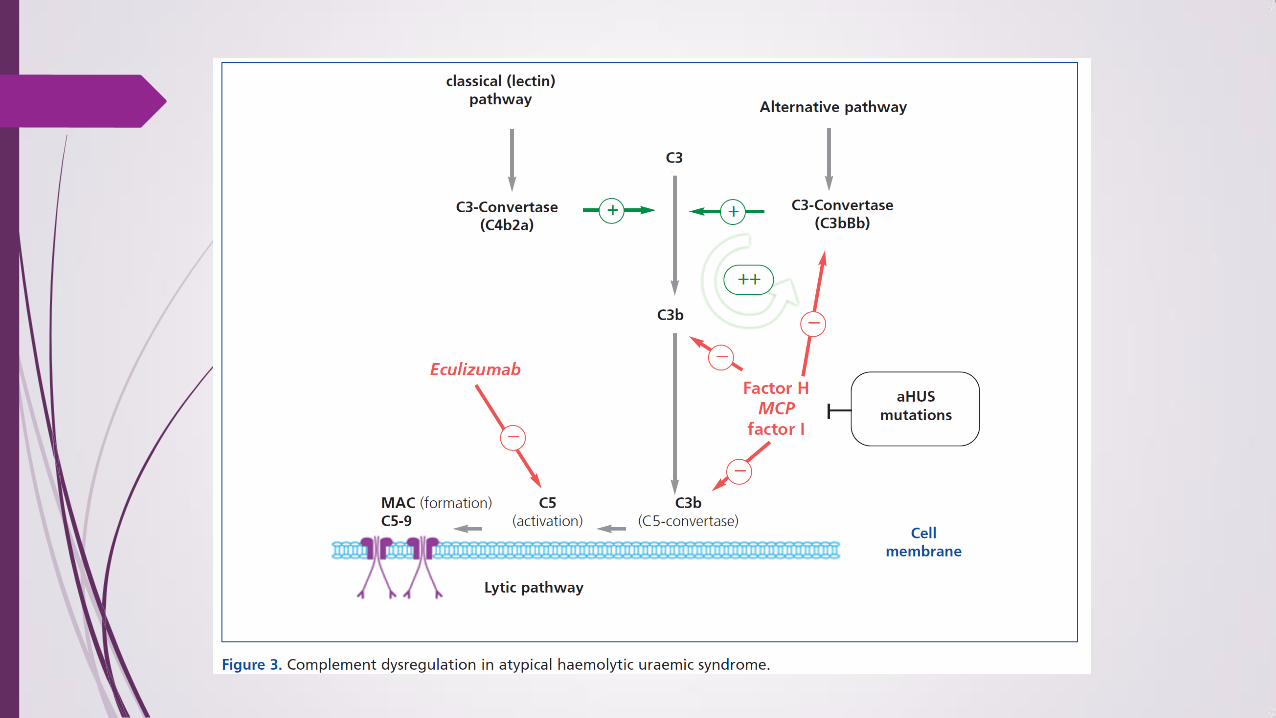
Complement investigations in aHUS
60-70% of aHUS patients carry currently identifiable mutations in complement genes or anti-CFH antibodies (2 large series)
Resulted in loss of protection of endothelial cells and platelets from complement attack TMA lesions
Normal C3, C4, CFH and CFI plasma levels do not exclude the diagnosis of complement dependent – HUS
Decreased C3 level observed in acute phase of STEC-HUS & Streptococcal Pneumoniae-HUS
Decreased C3 observed in 30-40% of aHUS
Levels of C5a and soluble C5b-9 (sC5b-9) are elevated in acute phase of aHUS, may be biological markers to differentiate aHUS from TTP
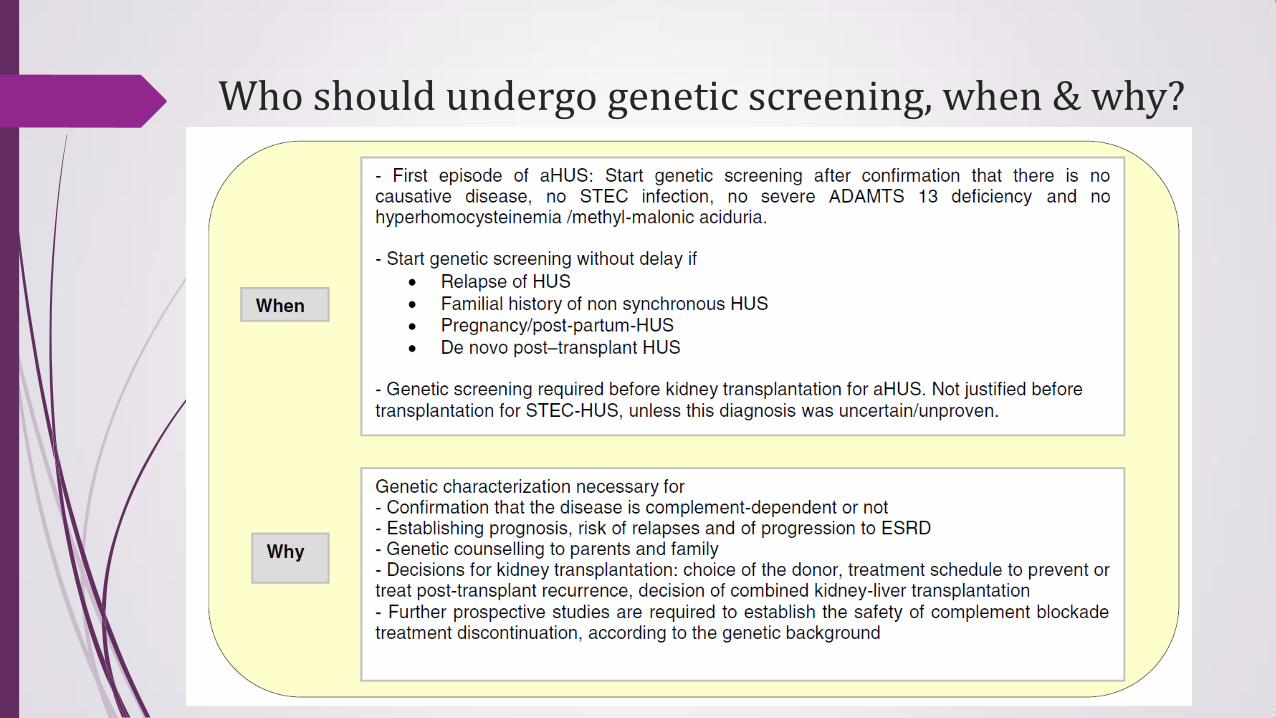
Who should undergo genetic screening, when & why?
Treatment options in pre-complement blockade treatment era
Plasma exchange/plasma infusion
Uncertain benefit
Technique-related complications in children
Sensitized to plasma components
Kidney transplantation
Terminal complement blockade treatment: Eculizumab
A monoclonal humanized anti-C5 antibody
Prevents C5 cleavage and the formation of C5a and C5b-9
Blocking the C5a pro-inflammatory and C5b-9 pro-thrombotic consequences of complement activation
100 patients treated within 4 prospective, open-label, single-arm trial
80 more case reports
Drawback
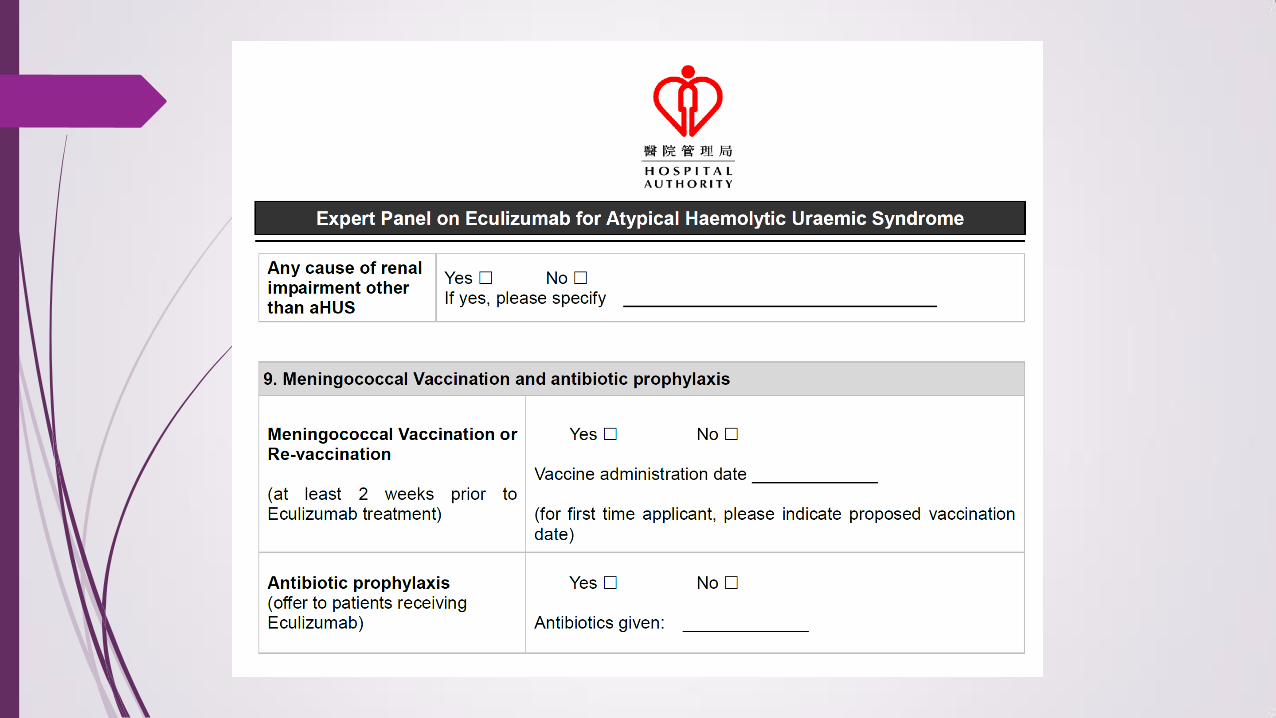
Risk of meningococcal infection
Immunity against Neisseria meningitis depends on the lytic terminal complement complex C5b-9
Meningococcal vaccines are recommended
Antibiotic prophylaxis is recommended before completion of vaccines
Very expensive self finance item
Life long treatment and possible development of neutralizing antibodies
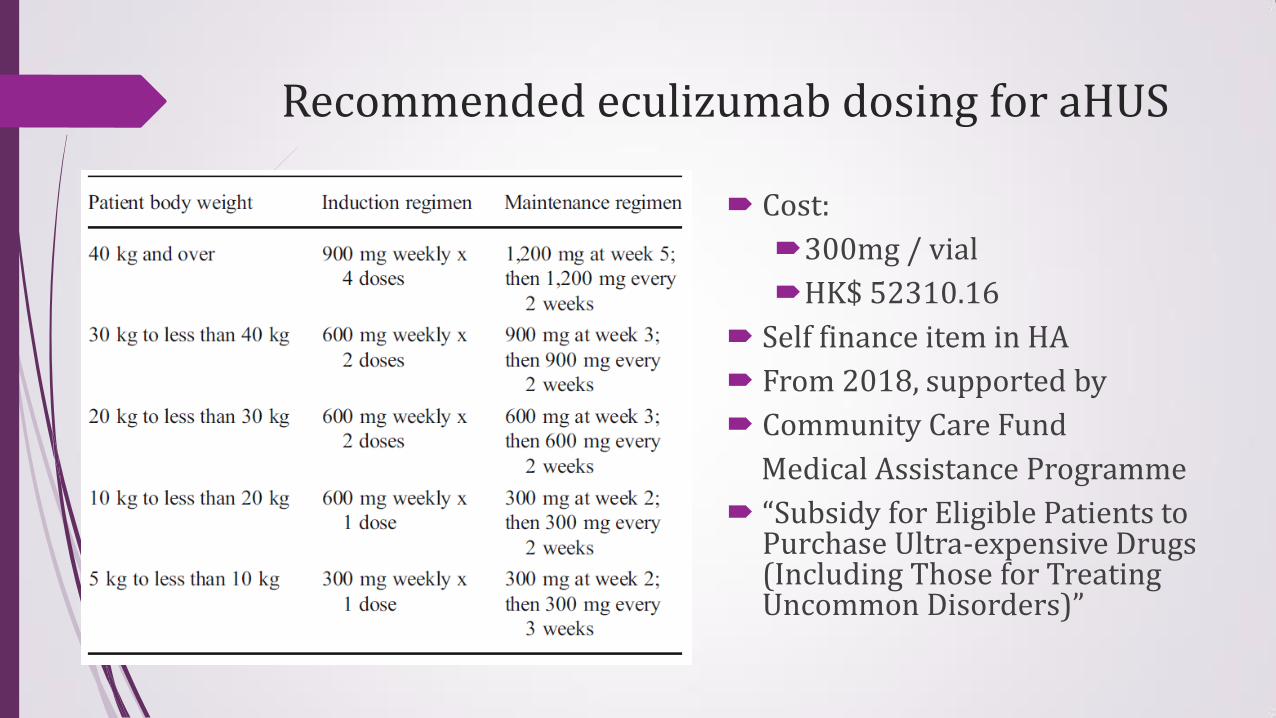
Recommended eculizumab dosing for aHUS
Cost:
300mg / vial
HK$ 52310.16
Self finance item in HA
From 2018, supported by
Community Care Fund
Medical Assistance Programme
“Subsidy for Eligible Patients to Purchase Ultra-expensive Drugs (Including Those for Treating Uncommon Disorders)”
Efficacy of eculizumab in aHUS
Systematic review of 1st two trials in UK
Indicated eculizumab was highly effective in aHUS
Despite study design limitations
Possibility of biased selection
Lack of control group
Lack of use of surrogate markers
In trial 3 (children; early initiation)
The “best of all” recovery of renal function observed in children with early treatment initiation
Efficacy of eculizumab in aHUS
Eculizumab effective in both groups of patients with or without complement mutation, but more % of patients with complement mutation responded
Eculizumab effective to treat or prevent post-transplant recurrence of aHUS
Risk of meningococcal infection under eculizumab
Immunity against Neisseria meningitis depends on the lytic terminal complement complex C5b-9
Prevention of meningococcal infection crucial
Vaccination / antibiotic prophylaxis
Clinical practice recommendations for patients with aHUS in 2014 Children with clinical diagnosis of aHUS propose eculizumab
as first-line treatment
To avoid plasma exchange and complications of central venous catheters
Confirmation of a complement mutation is not required prior to treatment initiation
Undue treatment delay may affect ultimate renal recovery & increase risk of early progression to ESRD
Should be initiated within 24-48 hrs of onset or admission
If eculizumab not available, plasma exchange should be started as in 2009
Clinical practice recommendations for patients with aHUS in 2014
Genetic screening is required for longer-term management of patients
Anti-CFH antibody – only complement investigation urgently needed during acute phase, as positive additional treatment options
Consider combining plasma exchange (PE) with eculizumab + steroid + immunosuppressive agent
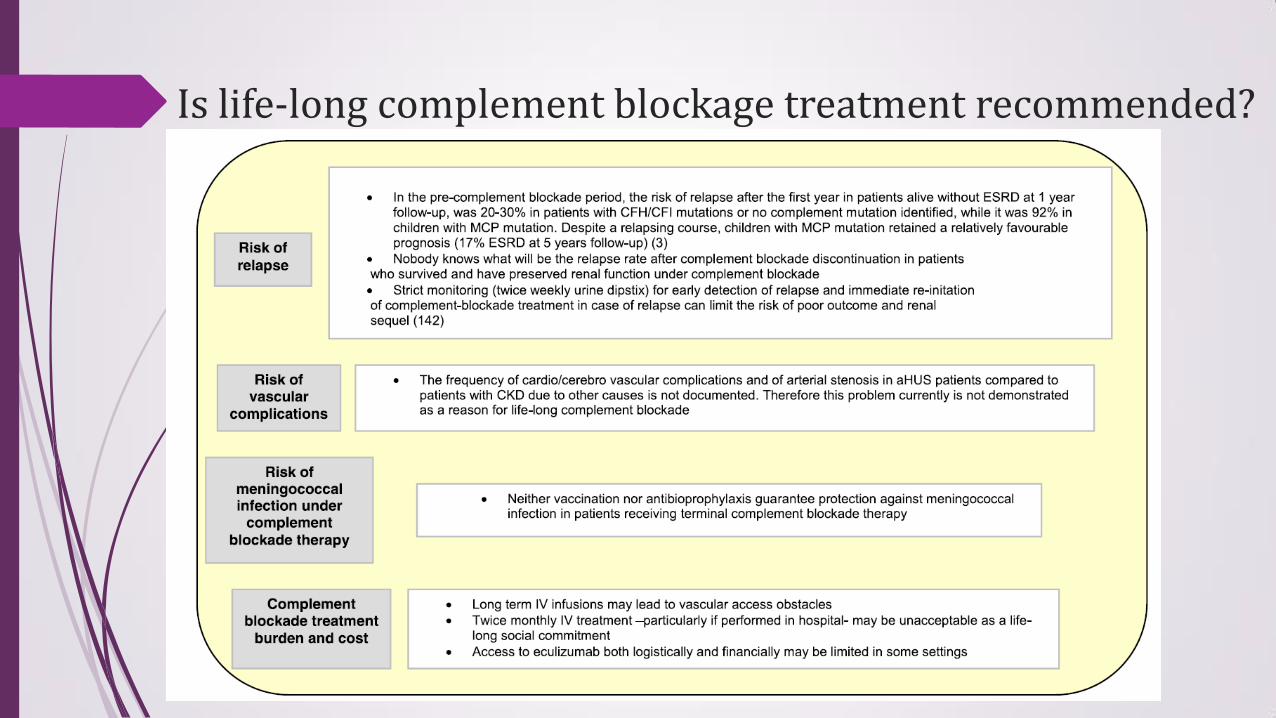
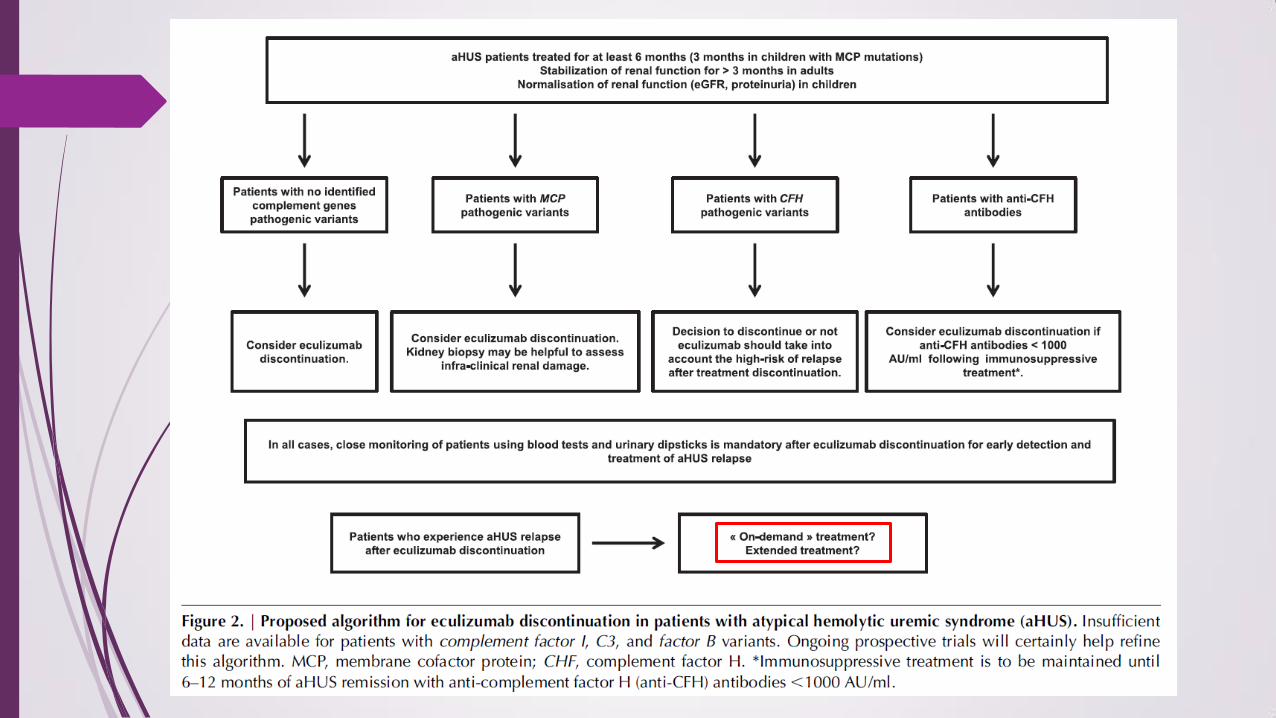
Is life-long complement blockage treatment recommended?
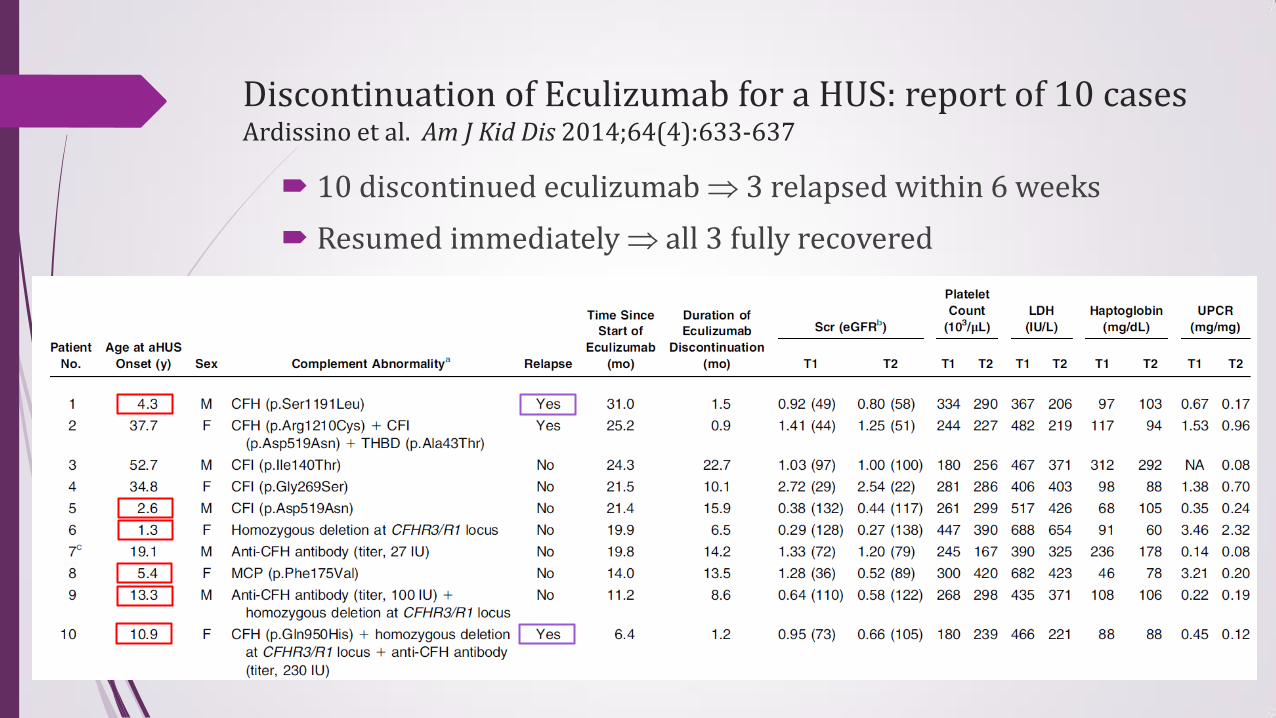
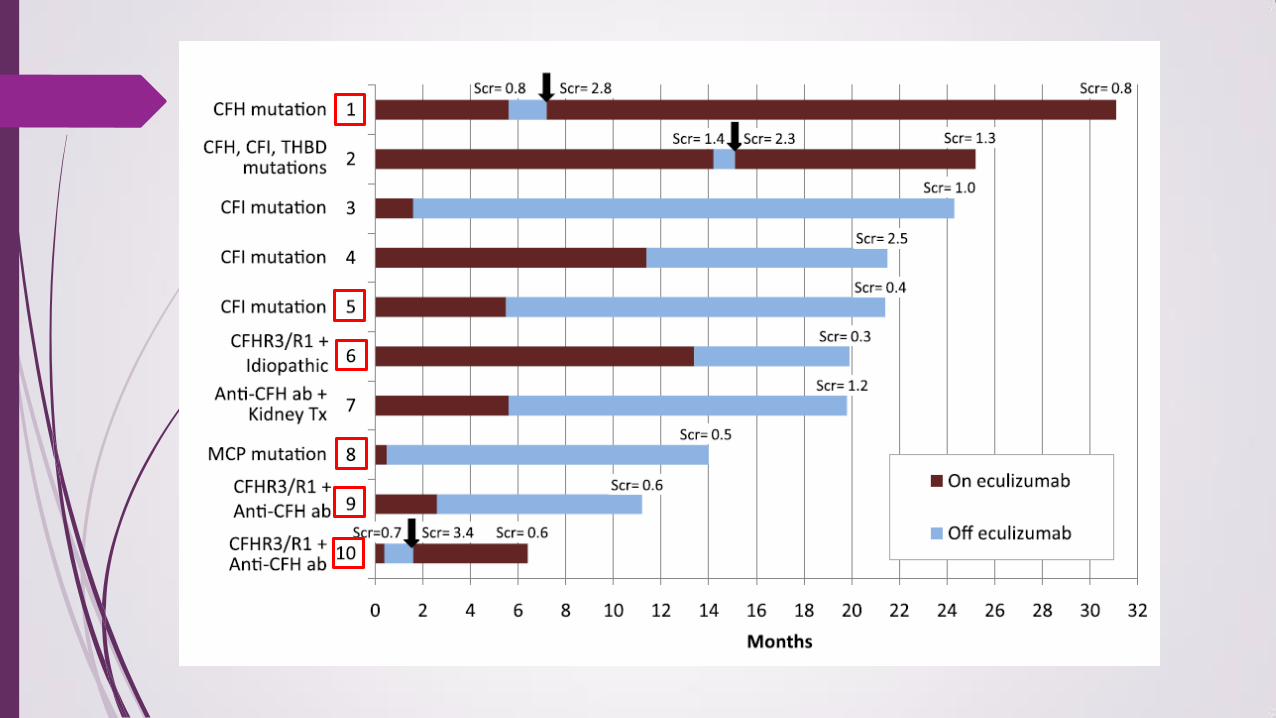
Discontinuation of Eculizumab for a HUS: report of 10 cases Ardissino et al. Am J Kid Dis 2014;64(4):633-637
10 discontinued eculizumab 3 relapsed within 6 weeks
Resumed immediately all 3 fully recovered
Risk of aHUS relapse after eculizumab discontinuation Fakhouri et al. Clin J Am Soc Nephrol 2017;12:50-59
Eculizumab discontinued in 38 (9 children 29 adults) of 108 patients (median treatment duration 17.5 months)
55% carried novel or rare complement genes variants
Renal recovery under eculizumab equally good with or without complement gene variants
Median FU 22 months 12 relapse, higher risk with pathogenic variants in complement genes
Early reintroduction of eculizumab (within 48 hrs) rapid hematologic remission & creatinine return to baseline
Progress of our patient
Febrile illness in Apr & June 2018
Given Eculizumab infusion early at illness, without progression to hemolysis, no further doses as no hemolysis developed
Further review on overseas experience, decided on future episodic “on-demand” treatment at the early phase of “documented” aHUS recurrence
Regular monitoring of CBP, RFT, LDH, urine haemastix
Thank you