Embed Size (px)
Citation preview

REVIEWS
Portal Vein Thrombosis: A Review JONATHAN COHEN, M.D., ROBERT R. EDELMAN, M.D., SANJIV CHOPRA, M.D., Bmton, Massachusetts
Portal vein thrombosis (PVT) is a rare condi- tion that affects both children and adults. This article reviews the existing literature on PVT, with an emphasis on recent developments. A comprehensive description of etiologic factors and clinical aspects is presented. Treatment is- sues that remain unresolved are addressed and a framework for the diagnostic work-up and man- agement of patients with PVT is provided.
From the Department of Medicine, Division of Gastroenterology, and the Department of Radiology, Beth Israel Hospital, Boston, Massachusetts.
Requests for reprints should be addressed to Sanjiv Chopra, M.D., Clinical Hepatology, Beth Israel Hospital, Dana 501, 330 Brookline Ave- nue, Boston, Massachusetts 02215.
Manuscript submitted January 4, 1991, and accepted in revised form June 12, 1991.
Febl wary 1992 The American Journal of Medicine Volume 92 173
P ortal vein thrombosis (PVT), a rare condition affecting both children and adults, occurs in
association with a wide variety of precipitating fac- tors and produces an array of clinical problems. It was first described by Balfour and Stewart [l] in 1868. In autopsy reviews, the overall incidence of portal vein occlusion ranges from 0.05% to 0.5% [2,3]. It is considered the leading cause of extrahe- patic portal hypertension in patients with a normal liver in Western countries [4]. Occlusion of the por- tal vein by a thrombus often produces no acute manifestation. The thrombus becomes organized, and tortuous collateral vessels gradually develop around the blocked portal vein, a process termed cavernous transformation. Patients generally come to medical attention when they develop the sequel- ae of portal hypertension, notably variceal hemorrhage.
In the past decade, there have been significant advances in the understanding of the etiology and clinical consequences of PVT. Increasingly, new ra- diologic techniques have been utilized in the diag- nosis and follow-up of patients with this condition.
In this article, we review the existing literature on PVT, with particular attention to recent develop- ments. A comprehensive description of etiologic factors and clinical aspects is presented. We high- light those treatment issues yet unresolved and of- fer a framework for the diagnostic work-up and management of patients with PVT.
ETIOLOGY Many conditions lead to thrombosis of the portal
vein. These include infectious and inflammatory processes, conditions that lead to decreased portal flow, direct invasion or extrinsic compression of the portal vein by tumor, hypercoagulable states, and mechanical manipulation of the portal vein.
Early series of patients with PVT found no un- derlying etiology in the majority of cases [5-a]. More recently, with increased diagnosis of inherited hypercoagulable states and underlying myeloprolif- erative disorders, several authors have reported a much smaller proportion of patients with idiopath- ic PVT, ranging from 8% to 15% [8,9].
The most common etiologic factor for PVT in children is infection, accounting for 43% to 52% of all cases [lo]. Neonatal umbilical sepsis, the single most frequent infectious cause, is present in 10% to

26% of children with PVT [5,10,11]. However, in- fants with infection of the umbilical vein infre- quently go on to develop PVT. In a prospective study of 86 patients with umbilical vein sepsis, there were no cases of PVT [lo]. Other infectious precipitants of PVT include appendicitis, post-bil- iary tract surgery sepsis, and peritonitis from a vari- ety of other sources [5]. PVT may occur as a conse- quence of the contiguous spread of the inflammatory process. Factors such as dehydration and increased coagulability accompanying sepsis may also contribute [10,12].
Several authors have suggested an association be- tween PVT and certain congenital anomalies such as ventricular septal defect, atria1 septal defect, de- formed inferior vena cava, and biliary tract abnor- malities [5,8,13,14]. Alvarez et al [E] studied 108 children with portal vein obstruction and found 21 patients with congenital malformations, including 11 involving the cardiovascular system. The mecha- nism by which such anomalies might predispose patients to develop PVT is unknown, although the existence of portal vein anomalies remains a possibility.
Cirrhosis has long been considered a major cause of PVT in adults. Cirrhosis has been present in 24% to 32% of patients with PVT [2,12]. The reported incidence of PVT in cirrhotic patients varies widely from 0.6% to 17%. Series that examine autopsy data yield higher incidence rates than do angiographic studies [16-B]. The pathogenesis of PVT in pa- tients with cirrhosis is uncertain, although it has been suggested that decreased portal blood flow and the presence of periportal lymphangitis and fibrosis in these patients promote the formation of thrombus [18].
The other principal cause of PVT in adults is neoplastic disease. In two studies, neoplasms were present in 21% and 24% of patients with PVT [12,19]. Pancreatic cancer and primary hepatocellu- lar carcinoma (PHCC) constitute the majority of cases. Other tumors that have been associated with PVT include carcinoma of the lung, stomach, pros- tate, uterus, and kidney, cholangiocarcinoma, ma- lignant carcinoid, and primary liver lymphoma [3,12,16,20-241. P ancreatic cancer is responsible for 11% to 12% of adult cases of PVT. PHCC accounts for 5% to 6% of the cases of PVT in Western patient populations [12,19]. With the marked preponder- ance of PHCC in other parts of the world, it is likely to have a substantial role in causing PVT world- wide. Angiography performed at the time of diagno- sis of PHCC in 155 patients demonstrated 10 cases of PVT [25].
PVT in patients with neoplastic disease may oc- cur as a consequence of direct invasion of the portal
vein by tumor, extrinsic compression of the portal vein, or periportal fibrosis following surgery or ra- diotherapy [12,16,19,21,26]. A hypercoagulable state secondary to malignancy additionally predis- poses these patients to the development of PVT kG’71.
Infection is also an important cause of PVT in adults, although to a lesser extent than in children. In patients without cirrhosis or malignant disease, approximately 10% to 25% of cases of PVT are asso- ciated with sepsis [5,10,12]. Infectious processes that may lead to portal thrombosis include portal pyemia, biliary tract infections, post-abdominal surgery sepsis, amoebic colitis with hepatic abscess, acute necrotizing pancreatitis, diverticulitis, and generalized septicemia. Portal pyemia appears to be most common and is often secondary to suppura- tive appendicitis [5,10,12,28].
Intra-abdominal inflammatory diseases may pre- cipitate PVT in the absence of infection. This cate- gory represents a small fraction of adult cases of PVT; in fact, Webb and Sherlock [5] make no men- tion of noninfectious inflammatory causes of PVT in their review of 97 patients. However, several cases have been reported of PVT associated with pancreatitis, appendicitis, cholecystitis, and alco- holic hepatits [9,27,29-311. One case of PVT in as- sociation with inflammatory spread from a perfo- rated duodenal ulcer has been reported [32].
Pancreatitis is the most common inflammatory disease that causes PVT. Pancreatitis-associated PVT comprises between 3% to 5% of all cases [6,9,12]. Chronic pancreatitis more commonly leads to splenic vein thrombosis and a unique form of “left-sided” segmental portal hypertension with the development of gastric varices [26,30,33]. PVT may result from pylephlebitis during a single acute bout of pancreatitis, from the repeated inflamma- tion of chronic calcific pancreatitis, or from stasis produced by extrinsic portal compression by a pseudocyst [27,30,31,34].
Myeloproliferative disorders are the focus of an increasing amount of attention as an important cause of PVT. Overt myeloproliferative disorders account for 3% to 12% of adult patients with PVT [5,9,10,12,19]. s ome patients with “idiopathic” PVT have a latent underlying myeloproliferative disorder that becomes evident only years after the diagnosis of PVT is made [9,35]. In order to detect such latent disorders in patients with PVT, Valla et al [9] checked for the spontaneous formation of ery- throid colonies in cultures of bone marrow cells ex- posed to low levels of erythropoietin. They found that 48% of their adult, nonmalignant cases of PVT were associated with either overt or latent myelo- proliferative disorders. In their study of 33 adults
PORTAL VEIN THROMBOSIS / COHEN ET AL
174 February 1992 The American Journal of Medicine Volume 92

with PVT, four patients without overt signs of a myeloproliferative disorder at the time of thrombo- sis had evidence of overt disease within 5 years.
Inherited hypercoagulable states may predispose patients to develop PVT. Familial coagulation dis- orders that have been linked to PVT include defi- ciencies of protein C, protein S, and antithrombin III (AT III). However, the literature to date con- tains only a few case reports of patients with PVT associated with these conditions [9,36-391.
Acquired hypercoagulable states are also consid- ered risk factors for the development of PVT. Pro- tein C, protein S, and AT III levels can be depressed secondary to liver disease [36]. Acquired AT III de- ficiency may be present in patients with nephrotic syndrome, disseminated intravascular coagulation, burns with infection, septicemia, malnutrition, in- flammatory bowel disease, malignancy, after bowel resection, and after oral estrogen administration [39]. PVT has been seen in association with preg- nancy and in conjunction with the oral intake of estrogens [5,10,12,40-421. The incidence of PVT in inflammatory bowel disease may be related to both the hypercoagulable state and the spread of infec- tion to the portal system [43].
One other notable, possible cause of PVT is non- cirrhotic portal fibrosis. A frequent cause of portal hypertension in India, this disease is characterized by variable periportal fibrosis and otherwise nor- mal liver histology. Also known as idiopathic portal hypertension in Japan and hepatoportal sclerosis in the United States, this condition may be associated with PVT in 3% of cases [2,6,44-461.
PVT is seen infrequently in a variety of addition- al settings that entail mechanical damage to the porta hepatis [15]. PVT may occur after blunt trau- ma [6,14,15,47] or after abdominal surgery, in the absence of septic complications [3,8,17,48,49]. Sple- nectomy in patients with underlying myeloprolifer- ative disease or cirrhosis carries a particularly in- creased risk of portal thrombosis. Patients with myeloproliferative disorders have a 13% to 18% inci- dence of PVT following splenectomy, regardless of the degree of thrombocytosis [50,51] (Table I).
CLINICAL ASPECTS PVT presents either in childhood at a mean age
of 6 years or in adulthood at a mean age of 40 years. It occurs with equal frequency in children and adults [5]. There are no significant gender differ- ences in the incidence of PVT, except for the pre- dominantly male subset of patients with PVT with underlying cirrhosis [5,11].
Patients with PVT usually present with hemate- mesis, increased abdominal girth, or abdominal pain [12]. Hematemesis from ruptured varices is the
PORTAL VEIN THROMBOSIS / COHEN ET AL
TABLE I
Etiology of PVT in Adults
Common causes Cirrhosis Neoplasm (primarily pancreatic carcinoma and hepatocellular
carcinoma) Infection Inflammatory (notably pancreatitis) Myeloproliferative disorders Idiopathic
Uncommon causes Hypercoagulable states
Inherited (ATIII, protein C, protein S deficiencies) Acquired (pregnancy, oral estrogen intake, circulating lupus anticoag-
ulant, and diseases such as inflamatoty bowel disease, systemic lupus erythematosus, BehEet’s disease, scleroderma, ldlopathic pulmonary hypertension, and paroxysmal nocturnal hemoglobin- uria 143,52-561)
Miscellaneous Noncirrhotic portal fibrosis/idiopathic portal hypertension/hepatopor-
tal sclerosis Blunt trauma Abdominal surgery Splenectomy in patients with myeloproliferative disorders Distal splenorenal shunt surgery [571 Liver transplantation [58-601 Transhepatic obliteration of varices [81
most frequent reason for seeking medical attention. Melena is also commonljT reported [4-6,15,19, 45,611. Most patients with PVT diagnosed before the first episode of gastrointestinal hemorrhage eventually go on to bleed within a mean of 4 years. However, approximately 10% of patients never bleed [5,61]. Bleeding is often severe enough to re- quire multiple transfusions [ll]. Abdominal pain is commonly reported when the thrombosis also in- volves the superior mesenteric vessels and produces bowel ischemia. Patients with chronic gastrointesti- nal ischemia may also have evidence of gastrointes- tinal bleeding. Measurements of pH in gastrointes- tinal mucosa may provide a useful objective test for evaluating such patients [62]. Other common com- plaints of patients with PVT include nausea, vomit- ing, anorexia, weight loss, diarrhea, and abdominal distention [8,12,15,50].
On physical examination, 75% to 100% of patients have splenomegaly, with the average patient having a spleen extending 8 to 9 cm below the left costal margin. Mild hepatomegaly is commonly present. Patients may also have abdominal tenderness [6,8,15,19,22,45,61]. Ascites is a relatively uncom- mon finding in PVT, and, when present, is usually mild and transient. It may occur immediately after the thrombotic event, before the patient has had time to develop collateral circulation [5,8,15,22,61]. Unless the patient has cirrhosis, stigmata of chronic liver disease and signs of hepatic encephalopathy are rare [6,8]. Patients may also have a low-grade fever [50].
Laboratory tests are for the most part unremark- able. Mild anemia is present in many patients, par-
February 1992 The American Journal of Medicine Volume 92 175

titularly if there has been a recent bleeding episode. A mild decrease in the white blood cell count and the platelet count as a result of hypersplenism may be present. Alternatively, thrombocytosis may be present and should suggest the possibility of an un- derlying myeloproliferative disorder. Liver func- tion tests are usually within normal limits, although mild elevations in transaminases, alkaline phospha- tase, and bilirubin have been reported [8,15,19,22,45,61,63]. Liver biopsy in noncirrhotic patients typically shows normal histology, except for some increased reticulin around the portal tracts, a pattern similar to that seen in patients with noncirrhotic portal fibrosis [6,19,45,61]. Upper gas- trointestinal endoscopy usually demonstrates esophageal varices; gastric varices may also be pre- sent [15].
The clinical course of patients with PVT is punc- tuated by repeated bouts of variceal hemorrhage, with an average of 2.5 to 5 episodes per patient [6,15,49,61]. As many as 24 episodes of hemorrhage in a single patient have been reported [61]. Such episodes increase in severity and frequency around the time of puberty. After puberty, bleeding often abates [5,61]. Approximately 10% to 20% of patients with PVT develop spontaneous splenoadrenorenal or splenogastrorenal shunts. These shunts appear to decrease the frequency of bleeding episodes, but they do not confer total protection [15,63]. Most individuals tolerate repeated bouts of hemorrhage well, without deterioration of liver function [6,7]. The mortality from bleeding secondary to variceal hemorrhage in PVT in patients without cirrhosis is approximately 5% [7,8,49,64].
Although hepatic encephalopathy is rarely pre- sent when the. diagnosis of PVT is made, it may occur later in the course. The patients at greatest risk for encephalopathy are those with coexisting hepatic disease and those who undergo portacaval shunt operations [8,65]. Webb and Sherlock [5] not- ed electroencephalographic (EEG) abnormalities or clinical signs of encephalopathy in 27 of 76 patients with noncirrhotic PVT. Only one of these cases oc- curred after shunt surgery [5]. However, encepha- lopathy in noncirrhotic patients without prior shunt surgery is rare [4,8,11,66-681.
Another major but fortunately rare complication of PVT is small bowel infarction. This occurs when the thrombus extends into the superior mesenteric vein [8,12,29]. It is invariably fatal without prompt surgical intervention [58,69]. Even with expedient bowel resection, mortality approximates 20% [69].
Many clinical aspects of PVT are determined by the underlying etiology. The precipitating condi- tion influences the mode and timing of presentation and the patient’s ultimate prognosis. Four distinct clinical pictures can be observed. First, there is the
classic group of patients without cirrhosis who pre- sent with complications of portal hypertension. PVT in these patients may be related to any of a number of etiologic factors. These patients demon- strate many of the clinical features detailed above.
Cirrhotic patients with PVT have a different pre- sentation and course. While they also tend to expe- rience variceal hemorrhage, abnormal liver func- tion tests and intractable ascites are often present [12]. Variceal hemorrhage is poorly tolerated and may lead to deterioration of liver function, hepatic encephalopathy, and death [4,7,12,59,61].
The third group consists of patients with intra- abdominal malignancy. Patients with malignant disease are less likely than other patients to survive long enough to develop the sequelae of portal hy- pertension and have a relatively low incidence of variceal hemorrhage [12,16,27]. Patients usually have ascites, anorexia, and weight loss at the time of presentation. In these individuals, PVT is often dis- covered serendipitously when ultrasound or com- puted tomography (CT) is performed for the evalu- ation of pain or ascites. Patients with PHCC-related PVT often have mild liver function test abnormalities and an enlarged, nodular liver [=I.
Finally, there is a subset of patients who present with acute symptoms at the time of thrombosis. While uncommon, this clinical picture is most often seen in patients who develop PVT secondary to intra-abdominal sepsis or suppurative pylephlebi- tis 1121. It may also occur in patients with preexist- ing liver disease, often after abdominal surgery [12,59]. While acute PVT is heralded typically by progressive ascites or signs of intestinal ischemia, variceal bleeding may occur if varices already exist. In one study, patients with PVT presenting at the time of acute thrombosis had a mortality of approx- imately 50% [12].
The overall prognosis for patients with nonacute PVT in the absence of cirrhosis or malignancy is good. In Webb and Sherlock’s [5] review of 97 pa- tients, 75% were alive after a mean follow-up of 10 years. The cause of death was hemorrhage in 19 patients and infection in five others [5]. Several other series indicate that overall mortality is 10% or less [7,22,49,59,61,70]. The majority of patients re- viewed in the literature have had some type of pro- cedure to prevent rebleeding. As a result, none of the reported mortality figures reflect the natural course of the disease.
RADIOLOGY A variety of radiologic techniques can be used to
investigate suspected PVT. Definitive diagnosis has long been made using portal venography or su- perior mesenteric arteriography, or at the time of
PORTAL VEIN THROMBOSIS / COHEN ET AL
176 February 1992 The American Journal of Medicine Volume 92

laparotomy. However, recent developments in ul- trasound, CT, and magnetic resonance (MR) imag- ing offer accurate noninvasive alternatives.
Ultrasonography has emerged as a safe and effec- tive screening tool in the evaluation of suspected portal venous occlusion and as a means of following patients diagnosed with this condition. Serial ex- aminations have been used to document the resolu- tion of thrombi after the administration of antico- agulant therapy, the organization of thrombi, the development of cavernous transformation, and the postoperative patency of portasystemic shunts [28,31,59,71,72].
The presence of an echogenic thrombus within the portal vein lumen provides the best ultrasono- graphic evidence of PVT. Additional signs include the dilatation of vessels proximal to the occlusion; the presence of collateral vessels, best seen near the porta hepatis; and the absence of an identifiable portal vein. The lack of variation in portal venous diameter with respiration, coupled with a portal vein diameter greater than 13 to 15 mm, is highly indicative of acute portal occlusion [31,71,73,74]. When the thrombus is long-standing, the portal vein diameter may be small or normal in size [75]. Cavernous transformation may take up to 12 months to occur, although this change has been demonstrated only 5 weeks after the thrombotic event [25,30]. Ultrasound scans often reveal spleno- megaly, and they may also detect an extension of thrombus into the superior mesenteric vein [71].
Ultrasound has the advantage of being a noninva- sive, easily accessible, and relatively inexpensive technique that is highly sensitive in detecting PVT [23,71,74]. Overlying bowel gas, obesity, severe fatty liver, or cirrhosis may hinder adequate penetration of the ultrasound beam [12,31,73]. Ultrasonography is operator dependent, and the diagnosis of PVT may be missed if the examiner is not asked specifi- cally to look for a suspected portal occlusion [76].
Ultrasonographic examination using the pulsed duplex Doppler technique is helpful in confirming the diagnosis of PVT and the existence of cavernous transformation [74]. When a thrombus completely occludes the portal vein, Doppler examination yields no signal. Blood flow through collateral ves- sels in the porta hepatis produces a characteristic waveform signal on Doppler [72]. A study of 20 pa- tients correlating Doppler scans with angiographic findings showed Doppler to have an 83% sensitivity in detecting hepatofugal blood flow. However, Doppler failed to demonstrate the only case of par- tial PVT in this study and had difficulty assessing the patency of the splenic and superior mesenteric veins [77]. The recent implementation of color Doppler techniques, which display flowing blood in color depending on the direction of flow, has greatly
improved the ease of identifying the portal vein and will likely result in further improvements in the diagnostic accuracy for PVT.
CT can be used both to confirm the diagnosis of PVT and to follow the course of patients with this condition [28,78]. Generally, intravenous contrast material is required for the CT demonstration of PVT. However, several cases of high attenuation thrombi of recent onset have been seen on plain CT scans [78,79]. The typical findings of contrast-en- hanced CT include a focus of decreased intralumin- al density, sharp collateral vessels, and peripheral ring-like enhancement on transverse sections. This enhancement is associated with proliferation of the vasa vasorum; it is observed less frequently than the hypodense thrombus and occurs more often when the thrombus is old [23,78,79]. Dynamic CT pro- duces even clearer images by taking multiple scans in rapid succession after an intravenous injection of contrast [78].
Contrast CT demonstration of PVT is highly spe- cific. In one study, angiography or autopsy con- firmed the CT diagnosis of PVT in all 111 patients examined [79]. CT is less operator dependent than ultrasound and circumvents the obstacle presented by bowel gas. However, a comparison of CT, ultra- sound, and angiography data in 17 patients with PVT found contrast-enhanced CT to be less sensi- tive than ultrasound in detecting thrombus (76% versus 94%) 1231. CT is limited by its inability to provide images in the axis of the portal vein and its difficulty in demonstrating intrahepatic portal ves- sels [23,31]. Clearly, the radiation, the high cost, and the need for contrast make CT a less than ideal test.
MR imaging has recently been introduced into the evaluation of patients with suspected PVT. PVT often produces a bright signal on Tl- and T2- weighted images when the thrombus is subacute (less than or equal to 5 weeks old). Older thrombi may have variable intensity on Tl-weighted im- ages, but generally appear hyperintense on T2- weighted scans. Zirinsky et al [80] compared MR with CT and ultrasound in imaging patients with PVT. MR images demonstrated more portal vein branches, more extensive thrombosis in these por- tal branches, and more collateral vessels than did either CT or ultrasound. However, neither dynamic CT nor Doppler techniques were routinely employed.
With the new technique of MR angiography, im- ages can be produced that display only flowing blood, without significant contamination from sta- tionary tissues. This makes it possible to uniquely distinguish slowly flowing blood from actual throm- bus in the portal vein. Images are postprocessed to create a projection portal venogram. Moreover, it is
PORTAL VEIN THROMBOSIS ,’ COHEN ET AL
February 1992 The American Journal of Medicine Volume 92 177

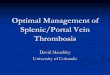
Figure 1. CT and MR images of a 35-year-old woman with polycythemia Vera, portal vein thrombosis (PVT), and splenic infarction. Top left, contrast-enhanced CT shows a hypo- dense thrombus (arrow) in the right portal vein. Top right, the Tl-weighted axial MR image using the standard spin-echo technique fails to demonstrate PVT; it shows only an irregular high-signal region (arrow) in the spleen, consistent with hem- orrhagic infarction. Bottom right, the MR angiogram shows occlusion of both the intrahepatic portal branches and the proximal splenic vein. Associated varices are well delineated (arrow). The hepatic veins and inferior vena cava (V) appear normal.
possible to tag flowing blood with a radiofrequency pulse to determine flow direction and velocity [81,82]. The results of MR angiography in the portal venous system are preliminary but nonetheless quite exciting. Recently, a study compared MR an- giography to surgical findings and ultrasound in a series of 21 patients undergoing liver transplanta- tion. MR angiography correctly determined portal vein patency in 18 of 19 patients and the distribu- tion of varices in all subjects. MR angiography was not impeded by bowel gas, as ultrasound sometimes was, and was superior to ultrasound in assessing varices (Finn P, personal communication) (Figures 1 and 2).
What is the appropriate radiologic approach to the work-up of PVT? The key to the diagnostic work-up is clinical suspicion. This should lead the physician to order a real-time ultrasound examina- tion, preferably with color Doppler capability, with attention to the portal vein. If the study is of good quality and if all of the portal venous structures of interest are seen, then the work-up is finished. If the ultrasound study is of suboptimal quality, if it is nondiagnostic and the clinical suspicion is high, or if more information is required (such as the distri- bution of varices), then MR is the procedure of choice, particularly if expertise in flow imaging techniques is available at the MR site. If MR is not available, dynamic contrast CT may be performed. If noninvasive tests are unsatisfactory, angiography
PORTAL VEIN THROMBOSIS / COHEN ET AL
should be performed, especially if shunt surgery is being considered [15,64].
MANAGEMENT The treatment of patients with PVT has tradi-
tionally focused on the control of acute bleeding episodes and attempts to prevent recurrent variceal hemorrhage.
Most instances of gastrointestinal bleeding in pa- tients with PVT are easily controlled with conser- vative measures. These include hospitalization, cor- rection of coagulation defects, and transfusions [11,22,59,61]. Additional measures such as Sangsta- ken-Blakemore balloon tamponade or intravenous vasopressin are occasionally required. Endoscopic variceal sclerotherapy (EVS) is often performed for the control of acute bleeding episodes [70,83]. Emergency surgery is rarely needed [11,19,61]. In
178 February 1992 The American Journal of Medicine Volume 92

PORTAL VEIN THROMBOSIS/COHEN ET AL
the management of acute hemorrhage in PVT, EVS is clearly preferable to emergency esophageal tran- sections or shunt operations, which have an opera- tive mortality of more than 30% [83].
Once the acute bleeding episode has ended, ef- forts must begin to determine the etiology of the thrombosis. In some instances, an underlying con- dition is discovered that is potentially treatable. For example, busulfan might be used to manage a patient with an underlying essential thrombocythe- mia [35].
Therapeutic modalities available to prevent re- current bleeding include EVS and portal-systemic shunt surgery. Expectant management of bleeding in PVT results in an overall mortality of approxi- mately 10% [7,68]. Because of selection bias in de- termining which patients have been managed with- out intervention, this figure is only an estimate [4,5,67]. There are no randomized, controlled stud- ies comparing EVS, shunt surgery, and expectant management of bleeding in patients with PVT. The utility of rubber band ligation of varices in the man- agement of variceal bleeding in PVT remains to be defined.
Endoscopic obliteration of varices can signifi- cantly reduce recurrent bleeding in PVT. Although longer follow-up of patients treated with EVS is needed, it appears that this technique is as effective as shunt surgery in preventing hemorrhage in chronic PVT. Belli et a2 [4] used sclerotherapy as a first-line treatment and were able to eradicate var- ices in all 15 of the patients in whom it was attempt- ed. None of these patients bled after eradication of varices, during a mean follow-up of 4 years. Other authors have reported similar results, with a low incidence of rebleeding and few deaths [11,84-881.
Complications of EVS include pain, esophageal mucosal injury, esophageal stenosis, bacteremia, and pleural effusions. However, these complica- tions are generally mild and can be managed easily [85,89]. Extremely rare reported complications of EVS include brain abscess, adult respiratory dis- tress syndrome, and paralysis from sclerosant entry into the vertebral venous plexus [67,70,89]. A major theoretic concern with EVS is the risk of sclerosant- induced retrograde thrombosis. Any further portal thrombosis might preclude the use of a portacaval shunt or precipitate intestinal infarction [89-911. A few cases have been reported of patients who devel- oped portal and mesenteric venous thrombosis af- ter EVS [90,91].
Given the high success, low mortality, and tolera- ble morbidity associated with EVS, and given the risks in shunt surgery of operative death or hepatic encephalopathy, sclerotherapy should be attempt- ed in patients as the first-line of treatment to pre-
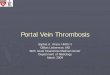
Figure 2. MR coronal projection venogram of a 42-year-old man with cirrhosis and portal hypertension. The image dem- onstrates a patent portal vein (straight arrow) with extensive splenic and paraesophageal varices (curved arrow). Note that the arterial signal is eliminated, and only the veins are shown.
vent bleeding. Patients may require several sessions (average four to eight) in order to eradicate the varices. Shunt surgery is indicated in patients who continue to bleed despite EVS and if access to health care services is a significant problem. When a patient lives far away from medical facilities, non- operative management of PVT may be too risky and the multiple repeated visits required for vari- teal eradication by sclerotherapy may be unfeasible k351.
Shunt surgery is also indicated in the rare patient who has PVT and is bleeding from varices at a site not accessible to the endoscopist. One of our pa- tients with documented PVT and a past history of a hepaticojejunostomy experienced repeated bouts of gastrointestinal bleeding from jejunal varices. EVS sclerotherapy was not feasible, and a splenorenal shunt operation was performed.
Candidacy for shunt surgery requires the pres- ence of vessels of sufficient caliber that are free of thrombus [18,64]. The location of suitable vessels dictates the type of anastomosis that can be con- structed. Thrombectomy or removal of fibrotic inti- ma1 thickening from organized thrombi may be re- quired in order to make a vessel suitable for the creation of a shunt [18]. Successful shunts can be constructed using vessels as narrow as 4 mm in di- ameter [49,64]. Selective, distal splenorenal shunts may be preferred in an effort to preserve portal perfusion and thereby decrease the risk of post- shunt encephalopathy [67].
Shunt surgery can greatly reduce the incidence of rebleeding in PVT. Several authors report success rates in excess of 80% with shunt procedures [11,49,59,64,67,92]. A rebleeding rate as low as 4%
February 1992 The American Journal of Medicine Volume 92 179

has been achieved [64]. Shunt surgery in the non- cirrhotic patient is generally accompanied by a low operative mortality rate and a good long-term sur- vival. Several authors report a combined operative and late mortality rate for patients undergoing shunt surgery that is less than the 10% figure esti- mated to result from expectant management [5,7,11,61,64,67]. Boles et a2 [ll] reported an 83% success rate with no deaths in 23 patients receiving either splenorenal or mesocaval shunts in 9 to 28 years of follow-up.
A major complication of shunt surgery is throm- bosis of the shunt itself, which often manifests as recurrent hemorrhage. The ‘reported incidence of shunt thrombosis is 8% to 24% [64,67]. Other report- ed complications of shunt surgery include the de- velopment of deep venous thromboses, varicosities, phlebitis, transfusion hepatitis, and pulmonary hy- pertension [ll]. Postoperative infection is also a concern.
One other complication of shunt surgery has been a matter of controversy. Voorhees et al [7,65] re- ported a high rate of portal-systemic encephalopa- thy manifested by emotional disturbances in pa- tients who had normal livers. Other authors have found no clinical or EEG evidence of this condition in up to 10 years of follow-up [11,49,61,67,93], and some have questioned whether the emotional dis- turbances noted by Voorhees et al [7,65] might be explained by the impact of repeated morbidity and hospitalizations [41,61].
In cirrhotic patients with PVT, the operative mortality rate for shunt surgery is between 4% and 8%. There is an approximately 50% 5-year survival rate in these patients [18]. Despite this poor out- come and the high incidence of portal-systemic en- cephalopathy in cirrhotic patients, this is better than the prognosis of untreated cirrhotics with PVT [12,18].
Direct operations such as portoazygous discon- nection and transesophageal variceal ligation have been employed in patients with PVT who are un- suitable candidates for shunt surgery. These direct procedures have operative mortality rates as high as 20%.and fail to prevent rebleeding in the majority of patients [5,7,11,61,64,67,68]. Such procedures are only indicated as a last resort for acute bleeding uncontrollable by any other means.
Another operation previously performed in pa- tients with PVT is splenectomy. There is a consen- sus in the literature that splenectomy alone is of minimal value in preventing bleeding and that it is rarely indicated for the treatment of hypersplenism in PVT [5,11,19,61,67,68]. Splenectomy, which is the treatment of choice for gastrointestinal bleed-
ing secondary to splenic vein thrombosis, is con- traindicated in patients with PVT because it may preclude the option of a splenorenal shunt opera- tion at a later date [26,33].
The role of anticoagulation in the management of patients with PVT has not been resolved. Several authors recommend the use of anticoagulation in certain patients to prevent recurrent thrombosis, but there is little evidence in the literature that it is of any benefit [8,18,29,36,50,69]. Given the lack of clinical data, the physician must weigh the estimat- ed chances of rebleeding against the risks of reth- rombosis, both in the portal vein and elsewhere. The best candidates for chronic anticoagulation are patients who have undergone shunt surgery, the success of which depends heavily on the prevention of shunt thrombosis, and patients with an underly- ing hypercoagulable state [36,50,52]. It also would be prudent to administer an anticoagulant to pa- tients with acute PVT who have undergone surgery to remove infarcted bowel, in order to avoid further thrombosis [29,69].
The management of symptomatic acute PVT is primarily surgical. Signs of intestinal infarction ne- cessitate laparotomy with excision of any necrotic bowel. Thrombectomy is sometimes helpful [48,58,69]. Antibiotics should be given if sepsis is pre- sent. When a patient presents with what appears to be an acute thrombotic event without any evidence of intestinal ischemia and radiologic tests demonstrate a thrombus that does not involve mesenteric veins, thrombolytic therapy and anticoagulation with care- ful clinical and radiologic follow-up may be indicated. In two instances of patients with PVT treated with heparin and/or bicoumarols, the thrombus was shown to dissolve on serial imaging studies [71,94]. There is also some evidence that thrombolytic therapy is help- ful [95,96]. B lb i ao et al [96] describe a patient diag- nosed with acute PVT in whom prompt percutaneous transhepatic infusion of urokinase led to recanaliza- tion of the portal vein. Regardless of whetherthrom- bolysis or laparotomy is undertaken, the management of acute PVT requires accurate and expedient diag- nosis and meticulous follow-up.
REFERENCES 1. Balfour GW, Stewart TG. Case of enlarged spleen complicated with ascites, both depending upon varicose dilatation and thrombosis of the portal vein. Edinburgh Med J 1869; 14: 589-98. 2. Okuda K. Ohnishi K, Kimura K, et a/. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology 1985; 89: 279-86. 3. Tscholl-Ducommun J. Thrombose veineuse du systeme Porte et cirrhose hepatique. Syndrome paraneoplastique? Arch Anat Cytol Pathol 1980; 28: 163-8. 4. Belli L, Romani F. Riolo F, et al. Thrombosis of portal vein in absence of hepatic disease. Surg Gynecol Obstet 1989: 169: 46-9.
PORTAL VEIN THROMBOSIS / COHEN ET AL
180 February 1992 The American Journal of Medicine Volume 92

PORTAL VEIN THROMBOSIS / COHEN ET AL
5. Webb LJ, Sherlock S. The aetiology. presentation and natural history of extra- hepatic portal venous obstruction. Q J Med 1979; 192: 627-39.
6. Maddrey WC, Malik KCB, lber FL, Basu AK. Extrahepatic obstruction of the portal venous system. Surg Gynecol Obstet 1968; 127: 989-98. 7. Voorhees AB, Price JB. Extrahepatic portal hypertension. A retrospective
analysis of 127 cases and associated clinical implications. Arch Surg 1974; 108: 338-41. 8. Brown KM, Kaplan MM, Donowitz M. Extrahepatic portal venous thrombosis: frequent recognition of associated diseases. J Clin Gastroenterol 1985; 7: 153-9. 9. Valla D, Casadevall N, Huisse MG, et a/. Etiology of portal vein thrombosis in adults. A prospective evaluation of primary myeloproliferative disorders. Gastro- enterology 1988; 94: 1063-g. 10. Thompson EN, Sherlock S. The aetiology of portal vein thrombosis with particular reference to the role of infection and exchange transfusion. Q J Med 1964; 132: 465-79. 11. Boles ET Jr, Wise WE Jr, Birken G. Extrahepatic portal hypertension in children, Long-term evaluation. Am J Surg 1986; 151: 734-9. 12. Witte CL, Brewer ML, Witte MH, Pond GB. Protean manifestations of pyleth- rombosis. A review of thirty-four patients. Ann Surg 1985; 202: 191-202. 13. Odievre M, Pige G, Alagille D. Congenital abnormalities associated with ex- trahepatic portal hypertension. Arch Dis Child 1977; 52: 383-5. 14. Triger DR. Leading article. Extra hepatic portal venous obstruction. Gut 1987; 28: 1193-7. 15. Alvarez F. Bernard 0, Brunelle F. Hadchouel P, Odievre M, Alagille D. Portal obstruction in children. I. Clinical investigation and hemorrhage risk. J Pediatr 1983; 103: 696-702. 16. Albacete RA, Matthews MJ, Saini N. Portal vein thromboses in malignant hepatoma. Ann Intern Med 1967; 67: 337-48. 17. Monarca A, Natangelo R, Tavani E, Azzolini V. Cirrhosis and portal vein thrombosis [letter]. Gastroenterology 1986; 90: 509. 18. Belli L, Sansalone CV, Aseni P, Romani F, Rondinara G. Portal thrombosis in cirrhotics. A retrospective analysis. Ann Surg 1986; 203: 286-91. 19. Macpherson AIS. Portal hypertension due to extrahepatic portal venous obstruction, A review of 40 cases, J R Coil Surg Edinb 1984; 29: 4-10. 20. Legmann P. Oilier P. Barge J, eta/. Primary lymphoma of liver: an exception- ally rare tumor. Ultrasonography and computed tomography imaging in one case and review of the literature. J Radio1 1985; 66: 599-602. 21. Gold JA, Sostman HD, Burrell Ml. Cholangiocarcinoma with portal vein ob- struction. Radiology 1979; 130: 15-20. 22. Penek J, Webber BL. Kirsch RE. Portal vein thrombosis with ascites. A case report, S Afr Med J 1976; 50: 173-6. 23. Subramanyam BR, Balthazar EJ. Lefleur RS, Horii SC, Hulnick DH. Portal venous thrombosis: correlative analysis of sonography, CT, and angiography. Am J Gastroenterol 1984; 79: 773-6. 24. Araki T, Suda K, Sekikawa T, lsjii Y. Hihara T, Kachi K. Portal venous tumor thrombosis associated with gatric adenocarcinoma. Radiology 1990; 174: 811-4. 25. Ohnishi K. Okuda K, Ohtsuki T, eta/. Formation of hilar collaterals or cavern- ous transformation after portal vein obstruction by hepatocellular carcinoma. Observation in ten patients. Gastroenterology 1984; 87: 1150-3. 26. Harnar T. Johansen K, Haskey R. Barker E. Left-sided portal hypertension from pancreatic pseudotumor. Am J Gastroenterol 1982; 77: 639-41. 27.Terada T, Hoso M. Nakanuma Y. Ohta T, Makino H. Extrahepatic portal venous obstruction of different pathogenesis in pancreatic diseases: reports of 4 autopsy cases with chronic pancreatitis and pancreatic carcinoma. Gastroen- terol Jpn 1989; 24: 414-20. 28. Knockaert DC, Robaeys GK, Cox EJ. Marchal GJ. Suppurative pyle-thrombo- sis: a changing clinical picture. Gastroenterology 1989: 97: 1028-30. 29. Harch JM, Radin RD, Yellin AE. Donovan AJ. Pylethrombosis. Serendipitous radioiogic diagnosis. Arch Surg 1987; 122: 1116-9. 30. Zalcman M. Van Gansbeke D, Matos C, Engelholm L, Struyven J. Sonogra- phic demonstration of portal venous system thromboses secondary to inflam- matory diseases of the pancreas. Gastrointest Radio1 1987; 12: 114-6. 31. Van Gansbeke D, Avni EF, Delcour 6, Engelholm L, Struyven J. Sonographic features of portal vein thrombosis. AJR Am J Roentgen01 1985; 144: 749-52. 32. Ballantyne B. Portal vein thrombosis and portal hypertension as a possible complication of duodenal ulceration. Am J Dig Dis 1969; 14: 748-52. 33. Simpson WG, Schwartz RW. Strode1 WE. Splenic vein thrombosis. South Med
J 1990; 83: 417-21. 34. Varriale P, Bonanno CA, Grace WJ. Portal hypertension secondary to pan- creatic pseudocysts. Arch Intern Med 1963; 112: 191-8. 35. Lang R. lnbal A, Jutrin I, Ravid M. Recurrent venous thrombosis: the sole manifestation of an occult myeloproliferative disease. Isr J Med Sci 1982; 18: 705-7. 36. Valla D, Denninger M-H, Delvigne J-M, Rueff B, Benhamou J-P. Portal vein thrombosis with ruptured oesophageal varices as presenting manifestation of hereditary protein C deficiency. Gut 1988; 29: 856-9. 37. Sas G. Blask6 G. Petr I, Griffin JH. A protein S deficient family with portal vein thrombosis [letter]. Thromb Haemost 1985; 54: 724. 38. Prat F, Ouzan D, Treuiak N, Trepo C. Portal and mesenteric thrombosis revealing constitutional protein C deficiency [letter]. Gut 1989; 30: 416. 39.Thaler E. Lechner K. Antithrombin Ill deficiency and thromboembolism. Baillieres Clin Haematol 1981; 10: 369-90. 40. Donaldson LB, Plant RK. Pregnancy complicated by extrahepatic portal hypertension: review of literature and report of 2 cases, Am J Obstet Gynecol 1971; 110: 255-64. 41. Nesbit RR Jr, Deweese JA. Mesenteric venous thrombosis and oral contra- ceptives. South Med J 1977; 70: 360-2. 42. Capron J-P, Lemay J-L, Muir J-F, Dupas J-L, Lebrec D, Gineston J-L. Portal vein thrombosis and fatal pulmonary thromboembolism associated with oral contraceptive treatment. J Clin Gastroenterol 1981; 3: 295-8. 43. Reh TE, Srivisal S. Schmidt EH Ill. Portal venous thrombosis in ulcerative colitis: CT diagnosis with angiographic correlation. J Comput Assist Tomogr 1980; 4: 545-7. 44. Ohnishi K, Saito M, Terabayashi H, Nomura F, Okuda K. Development of portal vein thrombosis complicating idiopathic portal hypertension. A case re- port. Gastroenterology 1985; 88: 1034-40. 45. Boyer JL, Sen Gupta KP, Biswas SK, et al. Idiopathic portal hypertension. Comparison with the portal hypertension of cirrhosis and extrahepatic portal vein obstruction. Ann Intern Med 1967; 66: 4167. 46. Maksoud JG. Mies S, Gayotto LC da C. Hepatoportal sclerosis in childhood. Am J Surg 1986; 151: 484-8. 47. Taylor TV, Torrance B. Portal vein thrombosis following a seat-belt injury. J R Coll Surg Edinb 1978; 23: 88-9. 48. Mergenthaler FW, Harris MN. Superior mesenteric vein thrombosis compli- cating pancreatoduodenectomy: successful treatment by thrombectomy. Ann Surg 1968; 167: 106-11. 49. Grauer SE, Schwartz SI. Extrahepatic portal hypertension: a retrospective analysis. Ann Surg 1979; 189: 566-72. 50. Broe PJ. Conley L, Cameron JL. Thrombosis of the portal vein following splenectomyfor myeloid metaplasia. Surg Gynencol Obstet 1981; 152: 488-92. 51. Rossi P. Passariello R, Simonetti G. Portal thrombosis: high incidencefollow- rng splenectomy for portal hypertension. Gastrointest Radio1 1976; 1: 225-7. 52. Pertuiset E, Tribout B, Wechsler B, et al. Systemic lupus erythematosus presenting with portal venous thrombosis. Am J Med 1989; 86: 501-2. 53. Ordi J, Vargas V, Vilardell M, Barquinero J, Guardia J. Lupus anticoagulant and portal hypertension. Am J Med 1988; 84: 566-8. 54. Bayraktar Y, Balkanci F, Kansu E. Dundar S. Telatar H. Portal hypertension in Behcet syndrome [letter]. AJR Am J Roentgen01 1989; 152: 1342. 55. Bower JS, Dantzker DR. Naylor B. Idiopathic pulmonary hypertension asso- ciated with nodular pulmonary infiltrates and portal venous thrombosis. Chest 1980; 78: 111-3. 56. Zimmerman D, Bell WR. Venous thrombosis and splenic rupture in paroxys- mal nocturnal hemoglobinuria. Am J Med 1980; 68: 275-9. 57. Henderson JM, Millikan WJ Jr, Chipponi J. et a/. The incidence and natural history of thrombus in the portal vein following distal splenorenal shunt. Ann Surg 1982; 196: 1-7. 58. Jaffe Y. Lygidakis NJ, Blumgart LH. Acute portal vein thrombosis after right hepatic lobectomy: successful treatment by thrombectomy. Br J Surg 1982; 69: 211. 59. Rouch DA, Emond JC, Ferrari M, Yousefzadeh D. Whiington P, Broelsch CE. The successful management of portal vein thrombosis after hepatic transplanta- tion with a splenorenal shunt. Surg Gynecol Obstet 1988: 166: 311-6. 60. Marino IR, Esquivel CO, Zajko AB. et a/. Distal splenorenal shunt for portal vein thrombosis after liver transplantation. Am J Gastroenterol 1989; 84: 67-70. 61. Fonkalsrud EW, Myers NA. Robinson MJ. Management of extrahepaticportal
February 1992 The American Journal of Medicine Volume 92 181

PORTAL VEIN THROMBOSIS / COHEN ET AL
hypertension in children. Ann Surg 1974; 180: 487-91. 62. Fiddian-Green RG, Stanley JC, Nostrant T, Phillips D. Chronic gastric isch- emia. A cau$e of abdominal pain or bleeding identified from the presence of gastric mucosal acidosis. J Cardiovasc Surg 1989; 30: 852-9. 63. Dilawari JE, Chawla YK. Spontaneous (natural) splenoadrenorenal shunts In extrahepatic portal venous obstruction: a series of 20 cases. Gut 1987; 28: 1198-200. 64. Bismuth H, Franc0 D. Portal diversion for portal hypertension in early child- hood. Ann Surg 1976; 183: 439-47. 65. Vorrhees AB, Chaitman E, Schneider S, Nicholson JF, Kornfeld DS. Price JB. Portal-systemic encephalopathy in the noncirrhotic patient. Effect of portal- systemic shunting. Arch Surg 1973; 107: 659-62. 66. Yik KY, Sullivan SN. Troster M. Neuropsychiatric disturbance due to occult occlusion of the portal vein. Can Med Assoc J 1982; 126: 50-2. 67. Warren WD, Henderson JM, Millikan WJ. Galambos JT, Bryan FC. Manage- ment of variceal bleeding in patients with noncirrhotic portal vein thrombosis. Ann Surg 1988; 207: 623-32. 68. Fonkalsrud EW. Surgical management of portal hypertension in childhood. Long-term results. Arch Surg 1980; 115: 1042-5. 69. Harrison TA. Portal phlebothrombosis: the role of thrombectomy. Ann R Coll Surg Engl 1978; 60: 320-3. 70. Lilly JR, Van Stiegmann G, Stellin G. Esophageal endosclerosis in children with portal vein thrombosis. J Pediatr Surg 1982; 17: 571-5. 71. Schwerk WB. Portal vein thrombosis: real-time sonographic demonstration and follow-up. Gastrointest Radio1 1986; 11: 312-8. 72. Koslin DB. Berland LL. Duplex Doppler examination of the liver and portal venous system. JCU 1987; 15: 675-86. 73. Walker DW, Tonkin AK, Joly D. Portal vein thrombosis shown by ultrasonog- raphy. South Med J 1983; 76: 925-6. 74. Johansen K, Paun M. Duplex ultrasonography of the portal vein. Surg Clin North Am 1990; 70: 181-90. 75. Miller VE, Berland LL. Pulsed Doppler duplex sonography and CT of portal vein thrombosis. AJR Am J Roentgen01 1985; 145: 73-6. 76. Black M, Friedman AC. Ultrasound examination in the patient with ascites. Ann Intern Med 1989; 110: 253-5. 77. Alpern MB, Rubin JM, Williams DM, Capek P. Porta hepatis: duplex Doppler US with angiographic correlation, Radiology 1987; 162: 53-6. 78. Mathieu D, Vasile N, Grenier P. Portal thrombosis: dynamic CTfeatures and course. Radiology 1985; 154: 737-41. 79. Mori H, Hayashi K, Uetani M, Matsuoka Y, lwao M, Maeda H. High-attenua- tion recent thrombus of the portal vein: CT demonstration and clinical signifi- cance. Radiology 1987; 163: 353-6.
80. Zirinsky K, Markisz JA, Rubenstein WA, et a/. MR imaging of portal venous thrombosis: correlation with CT and sonography. AJR Am J Roentgen01 1988; 150: 283-8. 81. Edelman RR, Mattle HP, Atkinson DJ, Hoogewoud HM. MR angiography. AJR Am J Roentgen01 1990; 154: 937-46. 82. Edelman RR, Zhao B, Liu C, et al. MR angiography and dynamic flow evalua- tion of the portal venous system. AJR Am J Roentgen01 1989; 153: 755-60. 83. Johnston GW. Six years’ experience of oesophageal transection for oeso- phageal varices, using a circular stapling gun. Gut 1982; 23: 770-3. 84. Howard ER, Stamatakis JD. Mowat AP. Management of esophageal varices in children by injection sclerotherapy. J Pediatr Surg 1984; 19: 2-5. 85. Kahn D, Terblanche J. Kitano S, Bornman P. Injection sclerotherapy in adult patients with extrahepatic portal venous obstruction. Br J Surg 1987; 74:
600-2. 86. Bhargava DK, Dwivedi M, Dasarathy S, Arora A. Endoscopic sclerotherapy for portal hypertension due to extrahepatic obstruction: long-term follow-up. Gastrointest Endosc 1989; 35: 309-11. 87. Paquet KJ. Ten years experience with paravariceal injection sclerotherapy of esophageal varices in children. J Pediatr Surg 1985; 20: 109-12. 88. Vane DW, Boles ET, Clatworthy HW. Esophageal sclerotherapy: an effective modality in children. J Pediatr Surg 1985; 20: 703-7.
89. Schuman BM. The systemic complications of sclerotherapy of esophageal varices. Gastrointest Endosc 1985; 31: 348-9. 90. Deboever G, Elegeert I, Defloor E. Portal and mesenteric venous thrombosis as a complication of endoscopic sclerotherapy. Am J Gastroenterol 1989; 84: 1336-7. 91. Leach SD, Meter GH. Gusberg RJ. Endoscopicsclerotherapy: a riskfactorfor splanchnic venous thrombosis. J Vast Surg 1989; 10: 9-12. 92. Henderson JM, Millikan WJ. Galambos JT. Warren WD. Selective variceal decompression in portal vein thrombosis, Br J Surg 1984; 71: 745-9. 93. Alagille D, Carlier JC, Chiva M, Ziade R. Ziade M, Moy F. Long-term neuropsy- chological outcome in children undergoing portal-systemic shunts for portal vein obstruction without liver disease. J Pediatr Gastroenterol Nutr 1986: 5: 861-6.
94.Verbanck JJ, Rutgeerts LJ. Haerens MH, et a/. Partial splenoportal and superior mesenteric venous thrombosis. Early sonographic diagnosis and suc- cessful conservative management. Gastroenterology 1984; 86: 949-52. 95. Fidler H, Booth A, Hodgson HJ. Calam J, Luzatto L. Hughes JM. Portal vein thrombosis in myeloproliferative disease. Uses of thrombolytic and antiplatelet treatment. BMJ 1990; 300: 590-2. 96. Bilbao JI, Rodriguez-Cabello J, Longo J, Zornoza G, Paramo J, Lecumberri FJ. Portal thrombosis: percutaneous transhepatic treatment with urokinase-a case report. Gastrointest Radio1 1989; 14: 326-8.
182 February 1992 The American Journal of Medicine Volume 92