Embed Size (px)
Citation preview

O
TPI
mmb
(ca
mmc
dhpti
fi
dcirdBsda
soaiit
U
cR
((
sz
td
2205
RIGINAL ARTICLE
ransversus Abdominis and Obliquus Internus Activity Duringilates Exercises: Measurement With Ultrasound Scanning
rit Endleman, MSc, MCSP, Duncan J. Critchley, MSc, MCSP
TaitiaPdi
cMcsnsaam
esmraeittlP
iaaurdpvekdo
m
ABSTRACT. Endleman I, Critchley DJ. Transversus abdo-inis and obliquus internus activity during Pilates exercises:easurement with ultrasound scanning. Arch Phys Med Reha-
il 2008;89:2205-12.
Objective: To assess activity of transversus abdominisTrA) and obliquus internus abdominis (OI) muscles duringlassical Pilates exercises performed correctly and incorrectly,nd with or without equipment.
Design: Repeated-measures descriptive study.Setting: Pilates studio.Participants: A volunteer sample of women (n�18) anden (n�8), mean age � SD (43�14y), with more than 6onths classical Pilates training and no back pain or other
ondition likely to influence abdominal muscle activity.Interventions: Participants performed Pilates imprint, hun-
reds A and B, roll-up, and leg-circle exercises on a mat. Theundreds exercise was also performed on a reformer (slidinglatform). Mat imprint and hundreds exercises were instructedo be performed correctly (with abdominal drawing-in) orncorrectly (without drawing-in).
Main Outcome Measure: Thickness of TrA and OI middlebers measured with ultrasound imaging.Results: TrA thickness increased during the mat imprint, hun-
reds A, hundreds B, leg-circle, and roll-up exercises (all P�.001)ompared with resting. OI thickness increased during the matmprint, hundreds A, hundreds B, leg-circle (all P�.001), andoll-up exercises (P�.002) compared with resting. TrA thicknessuring reformer hundreds B was greater than during mat hundreds
(P�.011); OI thicknesses were not different for this compari-on. During incorrect imprint, neither TrA or OI thicknesses wereifferent to resting. TrA and OI muscle thicknesses were moder-tely correlated (R�.410; P�.001).
Conclusions: This study provides the first evidence that aelection of classic Pilates exercises activates TrA and OI. Usef the reformer exercise machine can result in greater TrActivation in some exercises. TrA and OI did not functionndependently during these exercises. Research into the train-ng effects of Pilates or in patient populations can be under-aken using ultrasonography in submaximal exercises.
Key Words: Abdominal muscles; Exercise; Rehabilitation;ltrasonography.© 2008 by the American Congress of Rehabilitation Medi-
ine and the American Academy of Physical Medicine andehabilitation
From the School of Human Health and Performance, University College LondonEndleman); Academic Department of Physiotherapy, King’s College London,Critchley), London, UK.
No commercial party having a direct financial interest in the results of the researchupporting this article has or will confer a benefit on the authors or on any organi-ation with which the authors are associated.
Reprint requests to Duncan J. Critchley, MSc, MCSP, Academic Dept of Physio-herapy, King’s College London, Guy’s Campus, London, SE1 6RT, UK, e-mail:[email protected].
0003-9993/08/8911-00932$34.00/0doi:10.1016/j.apmr.2008.04.025
HE EXERCISE REGIMEN known as pilates, founded onthe teachings of Joseph Pilates (1880–1967), has become
popular choice for people seeking conditioning and rehabil-tation; devotees in the United States increased 1000-fold be-ween 1990 and 2000.1 Pilates advocates claim the exercisesnvolve activation of the transversus and obliquus internusbdominal muscles thought to stabilize the lumbar spine; henceilates has application in lumbo-pelvic pain rehabilitation andance, sport, or athletic conditioning. This claim has had min-mal formal investigation.2
There has been considerable recent interest in neuromuscularontrol of spinal motion in rehabilitation and conditioning.odels of trunk muscle function developed from Bergmark’s3
lassification of local muscles, such as TrA,4,5 attaching to thepine and global muscles, such as middle fibers of OI,3 span-ing the pelvis to ribs, stress the importance of TrA as a spinaltabilizer, and are influential in contemporary physical therapynd conditioning practice.4,6-10 Others, such as McGill etl,11-13 do not employ this classification, and suggest all trunkuscles have a role in spinal stability.Classic Pilates aims to improve health and well being with
xercises that emphasize abdominal and low back muscletrengthening while maintaining good posture and body align-ent.14 Exercises are mat-based or use equipment, such as the
eformer (fig 1; and see Methods: Materials), as assistivend/or resistive exercise tools.14 It is claimed that Pilates ex-rcises activate TrA and OI muscles15,16; consequently, Pilatess advocated as a progression from spinal stabilization physicalherapy (involving TrA retraining) as maintenance or preven-ative exercises for people with back pain.7 To date, no pub-ished studies have evaluated TrA or OI muscle activity duringilates exercises.All classic Pilates exercises involve the imprint action, pull-
ng the navel toward the spine. Pilates believed pulling in thebdomen in this way protected the spine.14 The imprint actionppears to be similar to the low abdominal drawing-in exercisesed to activate TrA in spinal stabilization training.10 It isecognized that many patients find low abdominal drawing-inifficult to learn even when taught by expert physical thera-ists.10 With the widespread popularity of Pilates, there isariation in teaching standards, and there are differences inmphasis of the importance of the imprint action.14-16 It is notnown whether it is necessary to maintain the imprint actionuring exercises, according to classic Pilates principles, inrder to activate TrA and OI muscles most effectively.Ultrasound imaging has been used as a noninvasive tool foreasuring abdominal muscle thickness change during respira-
List of Abbreviations
ANOVA analysis of varianceEMG electromyographicICC intraclass correlation coefficientsMVC maximum voluntary contractionOI obliquus internus abdominis
TrA transversus abdominisArch Phys Med Rehabil Vol 89, November 2008
tcwtmisa
h(stcdm(gs
fiaf
P
lcc6tsto
M
7tc
pam
P
wrPoAH
U
bsspb
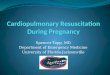
F
A a
2206 ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
A
ion, abdominal muscle exercises, and gait.17-21 Thicknesshange in TrA and OI has been shown to have good correlationith EMG activity up to 30% to 50% MVC,22,23 suggesting
hat thickness change is a valid measure of activity in theseuscles at these levels of effort. Unfortunately, the relationship
n obliquus externus abdominis is much weaker, and ultra-ound-measured thickness change cannot be confidently useds a gauge of activity in this muscle.22,24
The aims of the investigation were to evaluate the followingypotheses with ultrasound measurements of muscle thickness:1) Pilates exercises performed by Pilates-trained healthy per-ons would result in greater activity in TrA and OI muscleshan at rest. (2) Performing the exercises correctly, followinglassic Pilates principles of maintaining the imprint action, orrawn-in abdominal wall, would result in greater TrA and OIuscle activity than performing the same exercises incorrectly.
3) Using the Pilates reformera equipment would result inreater TrA and OI muscle activity than when performing theame exercise on mats.
In addition, we evaluated the correlation of TrA and middlebers of OI muscle activity during a range of exercises aimedt promoting trunk stability in order to investigate the degree ofunctional independence of these muscles.
METHODS
articipantsAfter we obtained ethical approval from the University Col-
ege London Research Ethics Committee and written informedonsent, 8 men and 18 women who had attended supervisedlassical Pilates sessions at least once a week for the previousmonths were recruited from a Pilates studio. Potential par-
icipants were excluded if they were under 18 years old, hadpinal or abdominal surgery at any time, had low back pain inhe last 2 years, had visible scoliosis, had neuromuscular dis-rders, or were pregnant.
aterialsA portable ultrasound scannerb was used in B mode with a
.5-MHz linear head. A Pilates reformer, a sliding platform onracks set in a frame, was used for the equipment-based exer-
Fig 1. (A) Reformer hundreds
ise (see fig 1). Participants can lie, sit, or stand on the slidingao
rch Phys Med Rehabil Vol 89, November 2008
latform, which is free to move, thus providing a unidirection-lly unstable base of support. Exercises are performed byoving the platform against spring resistance.
roceduresEach participant’s demographic data, height, and weight
ere recorded. All exercises were initially demonstrated by theesearcher, a physical therapist who is also an experiencedilates instructor. Exercises were conducted in random orderver a 50-minute period to minimize possible fatigue effects.ll testing took place in the studio of Pilates International,ighgate, London, UK.
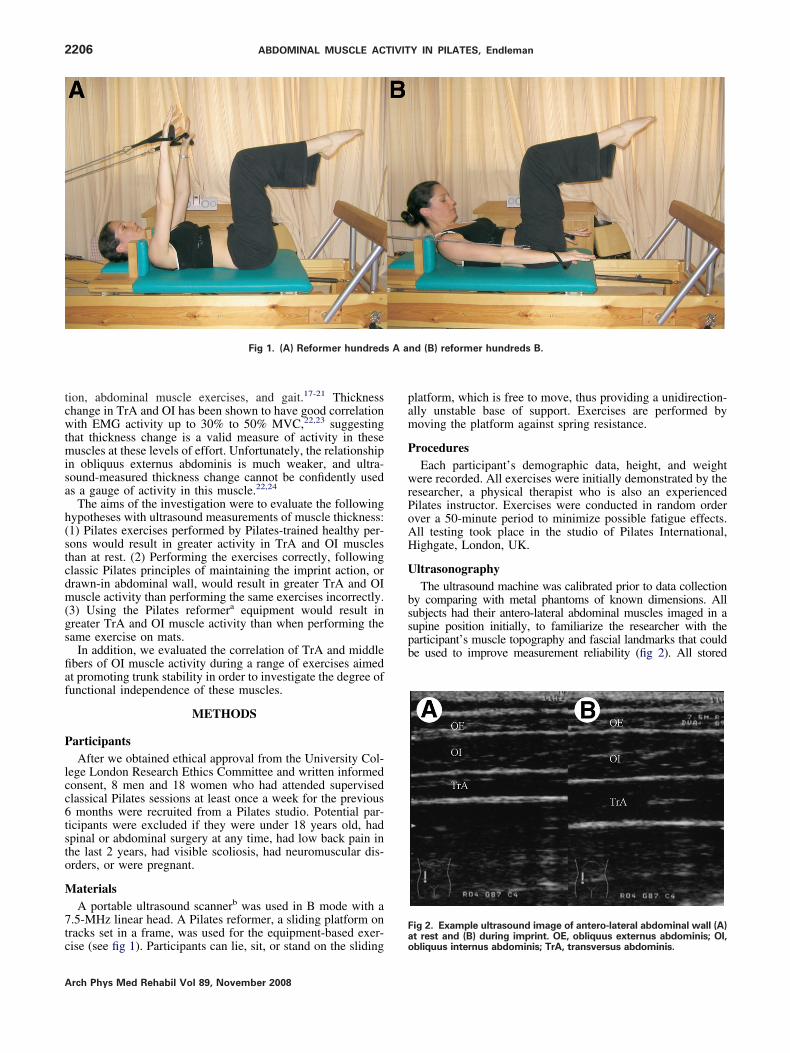
ltrasonographyThe ultrasound machine was calibrated prior to data collection
y comparing with metal phantoms of known dimensions. Allubjects had their antero-lateral abdominal muscles imaged in aupine position initially, to familiarize the researcher with thearticipant’s muscle topography and fascial landmarks that coulde used to improve measurement reliability (fig 2). All stored
ig 2. Example ultrasound image of antero-lateral abdominal wall (A)
nd (B) reformer hundreds B.
t rest and (B) during imprint. OE, obliquus externus abdominis; OI,bliquus internus abdominis; TrA, transversus abdominis.
ioptmmpiwoawlTsr
E
ip
wo4eicpm((haaaip
selcmcdiawirei
D
wB(2enrcr
2207ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
mages for measurement purposes were made with the transducerrientated antero-laterally with the midpoint of the transducerositioned midway between the iliac crest and the lowest rib alonghe anterior axillary line of the left abdomen. At this point, theiddle fibers of TrA can be imaged simultaneously with theiddle fibers of OI.21 Care was taken to position the transducer
erpendicularly to the abdominal wall at all times for optimalmage clarity and increased accuracy of readings. Static viewsere stored using the freeze facility of the scanner timed to the endf exhalation17; the thickness of muscles was measured using theutomatic calipers software of the scanner. All ultrasound scansere taken with the scanner head in the same position, using skin
andmarks or an indelible pen to minimize repositioning error.hicknesses of TrA and OI muscles were measured in restingupine position, during the following exercises, then repeated inesting supine position to assess short-term intratester reliability.
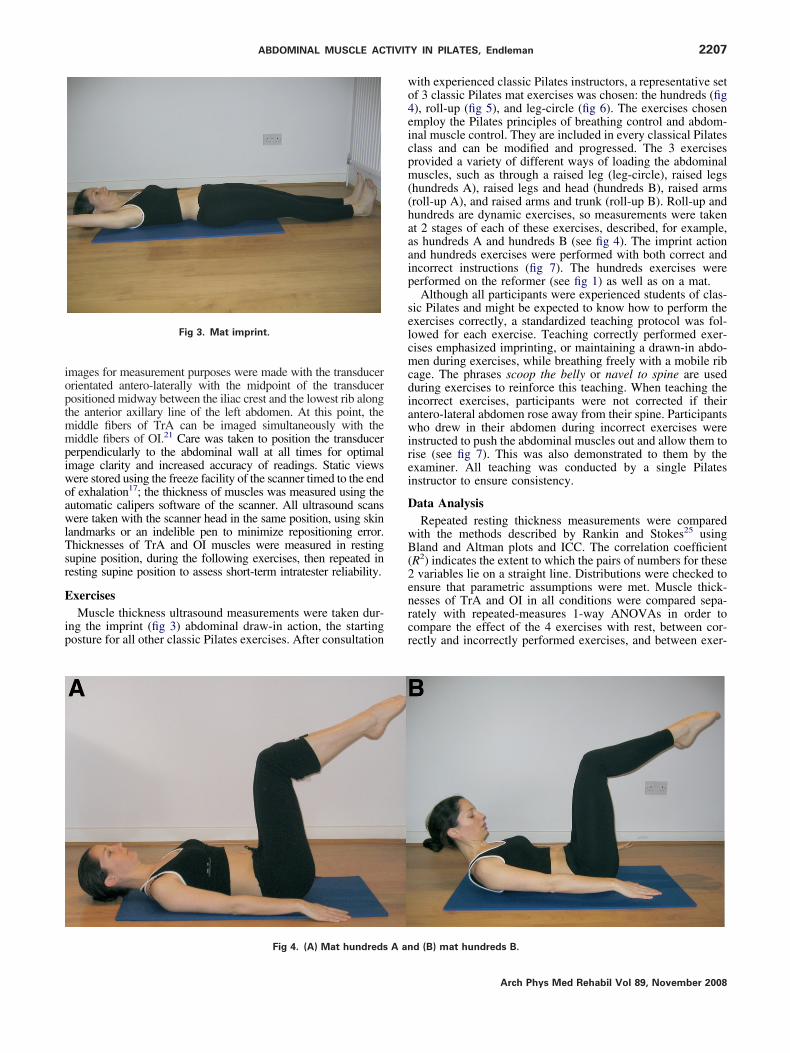
xercisesMuscle thickness ultrasound measurements were taken dur-
ng the imprint (fig 3) abdominal draw-in action, the startingosture for all other classic Pilates exercises. After consultation
Fig 3. Mat imprint.
Fig 4. (A) Mat hundreds A an
ith experienced classic Pilates instructors, a representative setf 3 classic Pilates mat exercises was chosen: the hundreds (fig), roll-up (fig 5), and leg-circle (fig 6). The exercises chosenmploy the Pilates principles of breathing control and abdom-nal muscle control. They are included in every classical Pilateslass and can be modified and progressed. The 3 exercisesrovided a variety of different ways of loading the abdominaluscles, such as through a raised leg (leg-circle), raised legs
hundreds A), raised legs and head (hundreds B), raised armsroll-up A), and raised arms and trunk (roll-up B). Roll-up andundreds are dynamic exercises, so measurements were takent 2 stages of each of these exercises, described, for example,s hundreds A and hundreds B (see fig 4). The imprint actionnd hundreds exercises were performed with both correct andncorrect instructions (fig 7). The hundreds exercises wereerformed on the reformer (see fig 1) as well as on a mat.Although all participants were experienced students of clas-
ic Pilates and might be expected to know how to perform thexercises correctly, a standardized teaching protocol was fol-owed for each exercise. Teaching correctly performed exer-ises emphasized imprinting, or maintaining a drawn-in abdo-en during exercises, while breathing freely with a mobile rib
age. The phrases scoop the belly or navel to spine are useduring exercises to reinforce this teaching. When teaching thencorrect exercises, participants were not corrected if theirntero-lateral abdomen rose away from their spine. Participantsho drew in their abdomen during incorrect exercises were
nstructed to push the abdominal muscles out and allow them toise (see fig 7). This was also demonstrated to them by thexaminer. All teaching was conducted by a single Pilatesnstructor to ensure consistency.
ata AnalysisRepeated resting thickness measurements were compared
ith the methods described by Rankin and Stokes25 usingland and Altman plots and ICC. The correlation coefficient
R2) indicates the extent to which the pairs of numbers for thesevariables lie on a straight line. Distributions were checked to
nsure that parametric assumptions were met. Muscle thick-esses of TrA and OI in all conditions were compared sepa-ately with repeated-measures 1-way ANOVAs in order toompare the effect of the 4 exercises with rest, between cor-ectly and incorrectly performed exercises, and between exer-
d (B) mat hundreds B.
Arch Phys Med Rehabil Vol 89, November 2008

cTbfinSo
D
odm
R
sfO
tn
Ca
pTTm
CP
bigrf(
rdmshbt
A a
2208 ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
A
ise with and without equipment. In order to assess whetherrA and OI thicknesses were related, Pearson’s correlationetween the 2 muscle thicknesses was tested, and lines of bestt for 8 possible relationships were compared. Statistical sig-ificance was accepted at P�.05. Data were analyzed usingPSS 12.0.c All data are presented as means � SDs unlesstherwise stated.
RESULTS
emographic DataParticipants had a mean � SD age of 43�14 year old, weight
f 62.3�9.1kg, 1.70�0.74m tall, 21.7�2.8kg/m2 body mass in-ex and had practiced Pilates for 8.2�7.2 years, ranging from 6onths to 25 years.
epeatabilityVisual inspection of Bland and Altman plots suggested no
ystematic differences between the 2 ultrasound measurementsor either resting muscle. ICCs were .82 and .91 for TrA andI, respectively. These results suggest that there is good short-
Fig 5. (A) Roll-up
Fig 6. Leg-circle.
rch Phys Med Rehabil Vol 89, November 2008
erm intraoperator repeatability for either resting muscle thick-ess measurement using ultrasound imaging.
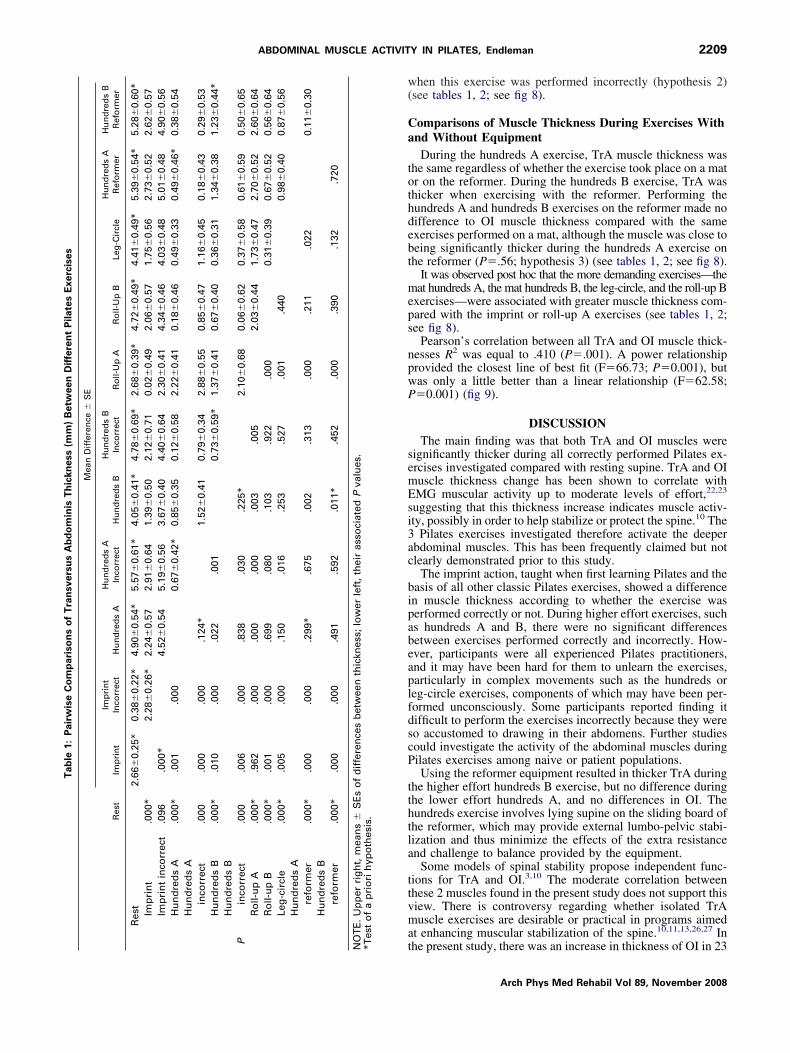
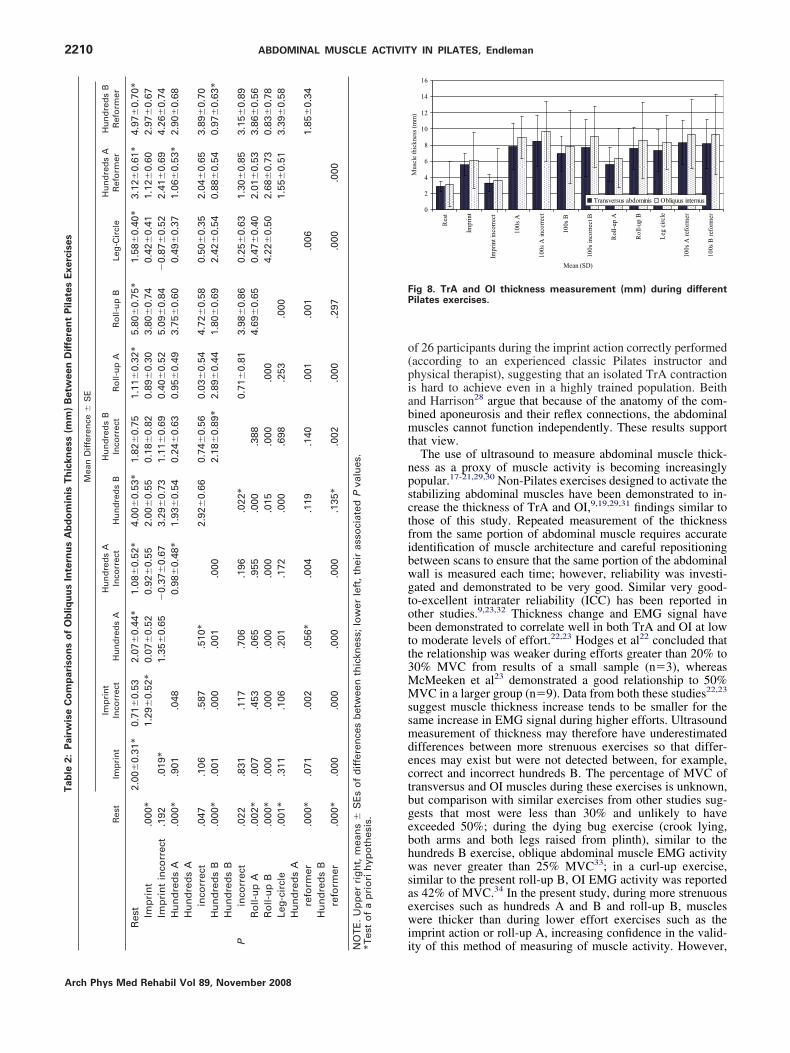
omparisons of Muscle Thickness During Exercisend RestBoth muscles increased in thickness during all correctly
erformed exercises compared with at rest (hypothesis 1).here were significant differences between all exercises in bothrA (P�.001) and OI (P�.001) thickness, assessed witheasures repeated 1-way ANOVAs (tables 1, 2; fig 8).
omparisons of Muscle Thickness During Exerciseserformed Correctly and IncorrectlyThe effects of performing the exercises incorrectly varied
etween the 2 muscles and between different exercises. Themprint exercise performed correctly resulted in significantlyreater thickness than when the exercise was performed incor-ectly in both TrA and OI. During the imprint exercise per-ormed incorrectly, neither TrA nor OI was thicker than at resthypothesis 2) (see tables 1, 2; see fig 8).
There were no differences in TrA thickness between cor-ectly and incorrectly performed mat hundreds A or mat hun-reds B exercises, and both correctly and incorrectly performedat hundreds A and mat hundreds B exercises resulted in
ignificantly greater TrA thickness than at rest. During the matundreds A exercise, there was no difference in OI thicknessetween correctly and incorrectly performed exercises; duringhe mat hundreds B exercise, OI muscle thickness was greater
nd (B) roll-up B.
Fig 7. (A) Correct imprint and (B) incorrect imprint.
w(
Ca
tothdebt
meps
npwP
semEsi3ac
bipabeaplfdscP
tthtla
ttvma
Tab
le1:
Pair
wis
eC
om
pa
riso
ns
of
Tra
nsv
ers
us
Ab
do
min
isT
hic
kn
ess
(mm
)B
etw
een
Dif
fere
nt
Pil
ate
sE
xerc
ises
Mea
nD
iffe
ren
ce�
SE
Res
tIm
pri
nt
Imp
rin
tIn
corr
ect
Hu
nd
red
sA
Hu
nd
red
sA
Inco
rrec
tH
un
dre
ds
BH
un
dre
ds
BIn
corr
ect
Ro
ll-U
pA
Ro
ll-U
pB
Leg
-Cir
cle
Hu
nd
red
sA
Ref
orm
erH
un
dre
ds
BR
efo
rmer
Res
t2.
66�
0.25
*0.
38�
0.22
*4.
90�
0.54
*5.
57�
0.61
*4.
05�
0.41
*4.
78�
0.69
*2.
68�
0.39
*4.
72�
0.49
*4.
41�
0.49
*5.
39�
0.54
*5.
28�
0.60
*Im
pri
nt
.000
*2.
28�
0.26
*2.
24�
0.57
2.91
�0.
641.
39�
0.50
2.12
�0.
710.
02�
0.49
2.06
�0.
571.
75�
0.56
2.73
�0.
522.
62�
0.57
Imp
rin
tin
corr
ect
.096
.000
*4.
52�
0.54
5.19
�0.
563.
67�
0.40
4.40
�0.
642.
30�
0.41
4.34
�0.
464.
03�
0.48
5.01
�0.
484.
90�
0.56
Hu
nd
red
sA
.000
*.0
01.0
000.
67�
0.42
*0.
85�
0.35
0.12
�0.
582.
22�
0.41
0.18
�0.
460.
49�
0.33
0.49
�0.
46*
0.38
�0.
54H
un
dre
ds
Ain
corr
ect
.000
.000
.000
.124
*1.
52�
0.41
0.79
�0.
342.
88�
0.55
0.85
�0.
471.
16�
0.45
0.18
�0.
430.
29�
0.53
Hu
nd
red
sB
.000
*.0
10.0
00.0
22.0
010.
73�
0.59
*1.
37�
0.41
0.67
�0.
400.
36�
0.31
1.34
�0.
381.
23�
0.44
*H
un
dre
ds
Bin
corr
ect
.000
.006
.000
.838
.030
.225
*2.
10�
0.68
0.06
�0.
620.
37�
0.58
0.61
�0.
590.
50�
0.65
Ro
ll-u
pA
.000
*.9
62.0
00.0
00.0
00.0
03.0
052.
03�
0.44
1.73
�0.
472.
70�
0.52
2.60
�0.
64R
oll-
up
B.0
00*
.001
.000
.699
.080
.103
.922
.000
0.31
�0.
390.
67�
0.52
0.56
�0.
64Le
g-c
ircl
e.0
00*
.005
.000
.150
.016
.253
.527
.001
.440
0.98
�0.
400.
87�
0.56
Hu
nd
red
sA
refo
rmer
.000
*.0
00.0
00.2
99*
.675
.002
.313
.000
.211
.022
0.11
�0.
30H
un
dre
ds
Bre
form
er.0
00*
.000
.000
.491
.592
.011
*.4
52.0
00.3
90.1
32.7
20
TE
.U
pp
erri
gh
t,m
ean
s�
SE
so
fd
iffe
ren
ces
bet
wee
nth
ickn
ess;
low
erle
ft,
thei
ras
soci
ated
Pva
lues
.es
to
fa
pri
ori
hyp
oth
esis
.
2209ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
hen this exercise was performed incorrectly (hypothesis 2)see tables 1, 2; see fig 8).
omparisons of Muscle Thickness During Exercises Withnd Without EquipmentDuring the hundreds A exercise, TrA muscle thickness was
he same regardless of whether the exercise took place on a matr on the reformer. During the hundreds B exercise, TrA washicker when exercising with the reformer. Performing theundreds A and hundreds B exercises on the reformer made noifference to OI muscle thickness compared with the samexercises performed on a mat, although the muscle was close toeing significantly thicker during the hundreds A exercise onhe reformer (P�.56; hypothesis 3) (see tables 1, 2; see fig 8).
It was observed post hoc that the more demanding exercises—theat hundreds A, the mat hundreds B, the leg-circle, and the roll-up B
xercises—were associated with greater muscle thickness com-ared with the imprint or roll-up A exercises (see tables 1, 2;ee fig 8).
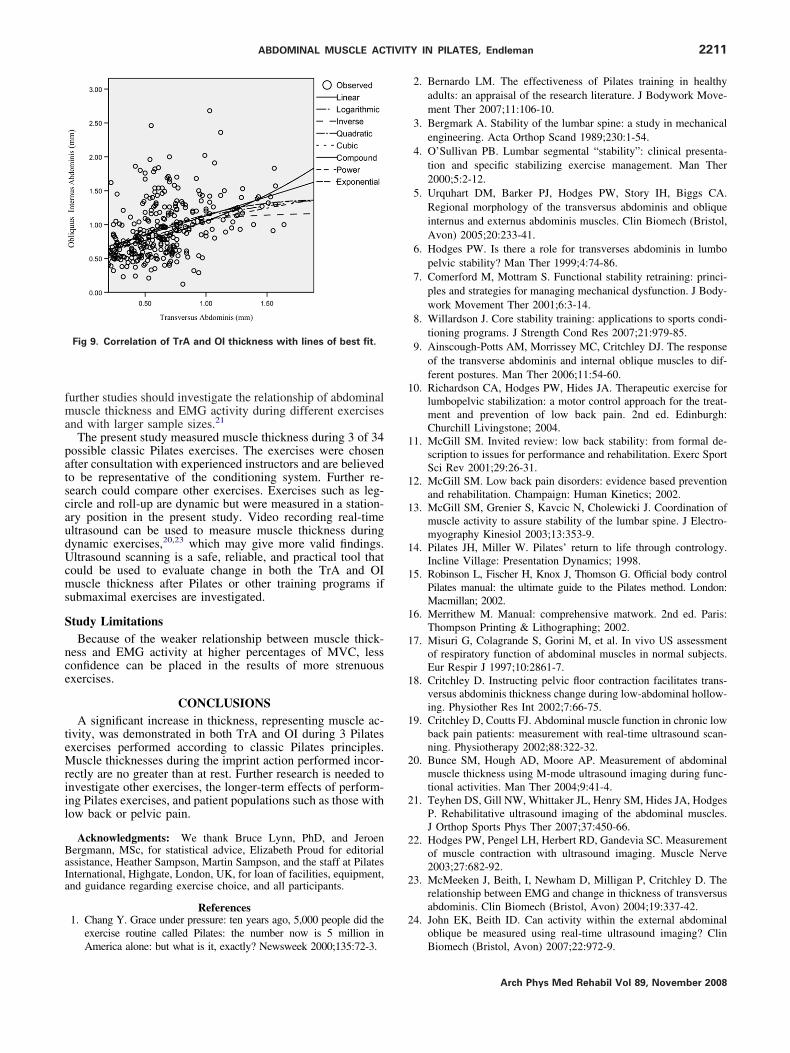
Pearson’s correlation between all TrA and OI muscle thick-esses R2 was equal to .410 (P�.001). A power relationshiprovided the closest line of best fit (F�66.73; P�0.001), butas only a little better than a linear relationship (F�62.58;�0.001) (fig 9).
DISCUSSIONThe main finding was that both TrA and OI muscles were
ignificantly thicker during all correctly performed Pilates ex-rcises investigated compared with resting supine. TrA and OIuscle thickness change has been shown to correlate withMG muscular activity up to moderate levels of effort,22,23
uggesting that this thickness increase indicates muscle activ-ty, possibly in order to help stabilize or protect the spine.10 The
Pilates exercises investigated therefore activate the deeperbdominal muscles. This has been frequently claimed but notlearly demonstrated prior to this study.
The imprint action, taught when first learning Pilates and theasis of all other classic Pilates exercises, showed a differencen muscle thickness according to whether the exercise waserformed correctly or not. During higher effort exercises, suchs hundreds A and B, there were no significant differencesetween exercises performed correctly and incorrectly. How-ver, participants were all experienced Pilates practitioners,nd it may have been hard for them to unlearn the exercises,articularly in complex movements such as the hundreds oreg-circle exercises, components of which may have been per-ormed unconsciously. Some participants reported finding itifficult to perform the exercises incorrectly because they wereo accustomed to drawing in their abdomens. Further studiesould investigate the activity of the abdominal muscles duringilates exercises among naive or patient populations.Using the reformer equipment resulted in thicker TrA during
he higher effort hundreds B exercise, but no difference duringhe lower effort hundreds A, and no differences in OI. Theundreds exercise involves lying supine on the sliding board ofhe reformer, which may provide external lumbo-pelvic stabi-ization and thus minimize the effects of the extra resistancend challenge to balance provided by the equipment.
Some models of spinal stability propose independent func-ions for TrA and OI.3,10 The moderate correlation betweenhese 2 muscles found in the present study does not support thisiew. There is controversy regarding whether isolated TrAuscle exercises are desirable or practical in programs aimed
t enhancing muscular stabilization of the spine.10,11,13,26,27 In
the present study, there was an increase in thickness of OI in 23P NO*T
Arch Phys Med Rehabil Vol 89, November 2008
o(piabmt
npsctfibwgtobtt3MMssmdectbgebhwsaewi
FP
Tab
le2:
Pair
wis
eC
om
pa
riso
ns
of
Ob
liq
uu
sIn
tern
us
Ab
do
min
isT
hic
kn
ess
(mm
)B
etw
een
Dif
fere
nt
Pil
ate
sE
xerc
ises
Mea
nD
iffe
ren
ce�
SE
Res
tIm
pri
nt
Imp
rin
tIn
corr
ect
Hu
nd
red
sA
Hu
nd
red
sA
Inco
rrec
tH
un
dre
ds
BH
un
dre
ds
BIn
corr
ect
Ro
ll-u
pA
Ro
ll-u
pB
Leg
-Cir
cle
Hu
nd
red
sA
Ref
orm
erH
un
dre
ds
BR
efo
rmer
Res
t2.
00�
0.31
*0.
71�
0.53
2.07
�0.
44*
1.08
�0.
52*
4.00
�0.
53*
1.82
�0.
751.
11�
0.32
*5.
80�
0.75
*1.
58�
0.40
*3.
12�
0.61
*4.
97�
0.70
*Im
pri
nt
.000
*1.
29�
0.52
*0.
07�
0.52
0.92
�0.
552.
00�
0.55
0.18
�0.
820.
89�
0.30
3.80
�0.
740.
42�
0.41
1.12
�0.
602.
97�
0.67
Imp
rin
tin
corr
ect
.192
.019
*1.
35�
0.65
�0.
37�
0.67
3.29
�0.
731.
11�
0.69
0.40
�0.
525.
09�
0.84
�0.
87�
0.52
2.41
�0.
694.
26�
0.74
Hu
nd
red
sA
.000
*.9
01.0
480.
98�
0.48
*1.
93�
0.54
0.24
�0.
630.
95�
0.49
3.75
�0.
600.
49�
0.37
1.06
�0.
53*
2.90
�0.
68H
un
dre
ds
Ain
corr
ect
.047
.106
.587
.510
*2.
92�
0.66
0.74
�0.
560.
03�
0.54
4.72
�0.
580.
50�
0.35
2.04
�0.
653.
89�
0.70
Hu
nd
red
sB
.000
*.0
01.0
00.0
01.0
002.
18�
0.89
*2.
89�
0.44
1.80
�0.
692.
42�
0.54
0.88
�0.
540.
97�
0.63
*H
un
dre
ds
Bin
corr
ect
.022
.831
.117
.706
.196
.022
*0.
71�
0.81
3.98
�0.
860.
25�
0.63
1.30
�0.
853.
15�
0.89
Ro
ll-u
pA
.002
*.0
07.4
53.0
65.9
55.0
00.3
884.
69�
0.65
0.47
�0.
402.
01�
0.53
3.86
�0.
56R
oll-
up
B.0
00*
.000
.000
.000
.000
.015
.000
.000
4.22
�0.
502.
68�
0.73
0.83
�0.
78Le
g-c
ircl
e.0
01*
.311
.106
.201
.172
.000
.698
.253
.000
1.55
�0.
513.
39�
0.58
Hu
nd
red
sA
refo
rmer
.000
*.0
71.0
02.0
56*
.004
.119
.140
.001
.001
.006
1.85
�0.
34H
un
dre
ds
Bre
form
er.0
00*
.000
.000
.000
.000
.135
*.0
02.0
00.2
97.0
00.0
00
TE
.U
pp
erri
gh
t,m
ean
s�
SE
so
fd
iffe
ren
ces
bet
wee
nth
ickn
ess;
low
erle
ft,
thei
ras
soci
ated
Pva
lues
.es
to
fa
pri
ori
hyp
oth
esis
.
2210 ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
A
f 26 participants during the imprint action correctly performedaccording to an experienced classic Pilates instructor andhysical therapist), suggesting that an isolated TrA contractions hard to achieve even in a highly trained population. Beithnd Harrison28 argue that because of the anatomy of the com-ined aponeurosis and their reflex connections, the abdominaluscles cannot function independently. These results support
hat view.The use of ultrasound to measure abdominal muscle thick-
ess as a proxy of muscle activity is becoming increasinglyopular.17-21,29,30 Non-Pilates exercises designed to activate thetabilizing abdominal muscles have been demonstrated to in-rease the thickness of TrA and OI,9,19,29,31 findings similar tohose of this study. Repeated measurement of the thicknessrom the same portion of abdominal muscle requires accuratedentification of muscle architecture and careful repositioningetween scans to ensure that the same portion of the abdominalall is measured each time; however, reliability was investi-ated and demonstrated to be very good. Similar very good-o-excellent intrarater reliability (ICC) has been reported inther studies.9,23,32 Thickness change and EMG signal haveeen demonstrated to correlate well in both TrA and OI at lowo moderate levels of effort.22,23 Hodges et al22 concluded thathe relationship was weaker during efforts greater than 20% to0% MVC from results of a small sample (n�3), whereascMeeken et al23 demonstrated a good relationship to 50%VC in a larger group (n�9). Data from both these studies22,23
uggest muscle thickness increase tends to be smaller for theame increase in EMG signal during higher efforts. Ultrasoundeasurement of thickness may therefore have underestimated
ifferences between more strenuous exercises so that differ-nces may exist but were not detected between, for example,orrect and incorrect hundreds B. The percentage of MVC ofransversus and OI muscles during these exercises is unknown,ut comparison with similar exercises from other studies sug-ests that most were less than 30% and unlikely to havexceeded 50%; during the dying bug exercise (crook lying,oth arms and both legs raised from plinth), similar to theundreds B exercise, oblique abdominal muscle EMG activityas never greater than 25% MVC33; in a curl-up exercise,
imilar to the present roll-up B, OI EMG activity was reporteds 42% of MVC.34 In the present study, during more strenuousxercises such as hundreds A and B and roll-up B, musclesere thicker than during lower effort exercises such as the
mprint action or roll-up A, increasing confidence in the valid-
0
2
4
6
8
10
12
14
16
Res
t
Impr
int
Impr
int i
ncor
rect
100s
A
100s
A in
corre
ct
100s
B
100s
inco
rrect
B
Rol
l-up
A
Rol
l-up
B
Leg
circ
le
100s
A re
form
er
100s
B re
form
er
Mean (SD)
Mus
cle
thic
knes
s (m
m)
Transversus abdominis Obliquus internus
ig 8. TrA and OI thickness measurement (mm) during differentilates exercises.
ity of this method of measuring of muscle activity. However,P NO
*T
rch Phys Med Rehabil Vol 89, November 2008
fma
patscaudUcms
S
nce
teMriil
BaIa
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2211ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
urther studies should investigate the relationship of abdominaluscle thickness and EMG activity during different exercises
nd with larger sample sizes.21
The present study measured muscle thickness during 3 of 34ossible classic Pilates exercises. The exercises were chosenfter consultation with experienced instructors and are believedo be representative of the conditioning system. Further re-earch could compare other exercises. Exercises such as leg-ircle and roll-up are dynamic but were measured in a station-ry position in the present study. Video recording real-timeltrasound can be used to measure muscle thickness duringynamic exercises,20,23 which may give more valid findings.ltrasound scanning is a safe, reliable, and practical tool that
ould be used to evaluate change in both the TrA and OIuscle thickness after Pilates or other training programs if
ubmaximal exercises are investigated.
tudy LimitationsBecause of the weaker relationship between muscle thick-
ess and EMG activity at higher percentages of MVC, lessonfidence can be placed in the results of more strenuousxercises.
CONCLUSIONSA significant increase in thickness, representing muscle ac-
ivity, was demonstrated in both TrA and OI during 3 Pilatesxercises performed according to classic Pilates principles.uscle thicknesses during the imprint action performed incor-
ectly are no greater than at rest. Further research is needed tonvestigate other exercises, the longer-term effects of perform-ng Pilates exercises, and patient populations such as those withow back or pelvic pain.
Acknowledgments: We thank Bruce Lynn, PhD, and Jeroenergmann, MSc, for statistical advice, Elizabeth Proud for editorialssistance, Heather Sampson, Martin Sampson, and the staff at Pilatesnternational, Highgate, London, UK, for loan of facilities, equipment,nd guidance regarding exercise choice, and all participants.
References1. Chang Y. Grace under pressure: ten years ago, 5,000 people did the
exercise routine called Pilates: the number now is 5 million in
Fig 9. Correlation of TrA and OI thickness with lines of best fit.
America alone: but what is it, exactly? Newsweek 2000;135:72-3.
2. Bernardo LM. The effectiveness of Pilates training in healthyadults: an appraisal of the research literature. J Bodywork Move-ment Ther 2007;11:106-10.
3. Bergmark A. Stability of the lumbar spine: a study in mechanicalengineering. Acta Orthop Scand 1989;230:1-54.
4. O’Sullivan PB. Lumbar segmental “stability”: clinical presenta-tion and specific stabilizing exercise management. Man Ther2000;5:2-12.
5. Urquhart DM, Barker PJ, Hodges PW, Story IH, Biggs CA.Regional morphology of the transversus abdominis and obliqueinternus and externus abdominis muscles. Clin Biomech (Bristol,Avon) 2005;20:233-41.
6. Hodges PW. Is there a role for transverses abdominis in lumbopelvic stability? Man Ther 1999;4:74-86.
7. Comerford M, Mottram S. Functional stability retraining: princi-ples and strategies for managing mechanical dysfunction. J Body-work Movement Ther 2001;6:3-14.
8. Willardson J. Core stability training: applications to sports condi-tioning programs. J Strength Cond Res 2007;21:979-85.
9. Ainscough-Potts AM, Morrissey MC, Critchley DJ. The responseof the transverse abdominis and internal oblique muscles to dif-ferent postures. Man Ther 2006;11:54-60.
0. Richardson CA, Hodges PW, Hides JA. Therapeutic exercise forlumbopelvic stabilization: a motor control approach for the treat-ment and prevention of low back pain. 2nd ed. Edinburgh:Churchill Livingstone; 2004.
1. McGill SM. Invited review: low back stability: from formal de-scription to issues for performance and rehabilitation. Exerc SportSci Rev 2001;29:26-31.
2. McGill SM. Low back pain disorders: evidence based preventionand rehabilitation. Champaign: Human Kinetics; 2002.
3. McGill SM, Grenier S, Kavcic N, Cholewicki J. Coordination ofmuscle activity to assure stability of the lumbar spine. J Electro-myography Kinesiol 2003;13:353-9.
4. Pilates JH, Miller W. Pilates’ return to life through contrology.Incline Village: Presentation Dynamics; 1998.
5. Robinson L, Fischer H, Knox J, Thomson G. Official body controlPilates manual: the ultimate guide to the Pilates method. London:Macmillan; 2002.
6. Merrithew M. Manual: comprehensive matwork. 2nd ed. Paris:Thompson Printing & Lithographing; 2002.
7. Misuri G, Colagrande S, Gorini M, et al. In vivo US assessmentof respiratory function of abdominal muscles in normal subjects.Eur Respir J 1997;10:2861-7.
8. Critchley D. Instructing pelvic floor contraction facilitates trans-versus abdominis thickness change during low-abdominal hollow-ing. Physiother Res Int 2002;7:66-75.
9. Critchley D, Coutts FJ. Abdominal muscle function in chronic lowback pain patients: measurement with real-time ultrasound scan-ning. Physiotherapy 2002;88:322-32.
0. Bunce SM, Hough AD, Moore AP. Measurement of abdominalmuscle thickness using M-mode ultrasound imaging during func-tional activities. Man Ther 2004;9:41-4.
1. Teyhen DS, Gill NW, Whittaker JL, Henry SM, Hides JA, HodgesP. Rehabilitative ultrasound imaging of the abdominal muscles.J Orthop Sports Phys Ther 2007;37:450-66.
2. Hodges PW, Pengel LH, Herbert RD, Gandevia SC. Measurementof muscle contraction with ultrasound imaging. Muscle Nerve2003;27:682-92.
3. McMeeken J, Beith, I, Newham D, Milligan P, Critchley D. Therelationship between EMG and change in thickness of transversusabdominis. Clin Biomech (Bristol, Avon) 2004;19:337-42.
4. John EK, Beith ID. Can activity within the external abdominaloblique be measured using real-time ultrasound imaging? Clin
Biomech (Bristol, Avon) 2007;22:972-9.Arch Phys Med Rehabil Vol 89, November 2008

2
2
2
2
2
3
3
3
3
3
a
b
2212 ABDOMINAL MUSCLE ACTIVITY IN PILATES, Endleman
A
5. Rankin G, Stokes M. Reliability of assessment tools in rehabili-tation: an illustration of appropriate statistical analysis. Clin Re-habil 1998;12:187-99.
6. Grenier SG, McGill SM. Quantification of lumbar stability byusing 2 different abdominal activation strategies. Arch Phys MedRehabil 2007;88:54-62.
7. Beith ID, Synnott RE, Newman SA. Abdominal muscle activityduring the abdominal hollowing manoeuvre in the four pointkneeling and prone positions. Man Ther 2001;6:82-7.
8. Beith ID, Harrison PJ. Stretch reflexes in human abdominal mus-cles. Exp Brain Res 2004;59:206-13.
9. Stuge B, Mørkved S, Haug Dahl H, Vøllestad N. Abdominal andpelvic floor muscle function in women with and without longlasting pelvic girdle pain. Man Ther 2006;11:287-96.
0. Raney NH, Teyhen DS, Childs JD. Observed changes in lateralabdominal muscle thickness after spinal manipulation: a caseseries using rehabilitative ultrasound imaging. J Orthop SportsPhys Ther 2007;37:472-9.
1. Hides JA, Wilson S, Stanton W, et al. An MRI investigation
into the function of the transversus abdominis muscle during crch Phys Med Rehabil Vol 89, November 2008
“drawing-in” of the abdominal wall. Spine 2006;31:E175-E178.
2. Hides JA, Miokovic T, Belavý DL, Stanton WR, Richardson CA.Ultrasound imaging assessment of abdominal muscle functionduring drawing-in of the abdominal wall: an intrarater reliabilitystudy. J Orthop Sports Phys Ther 2007;37:480-6.
3. Souza GM, Baker LL, Powers CM. Electromyographic activity ofselected trunk muscles during dynamic spine stabilization exer-cises. Arch Phys Med Rehabil 2001;82:1551-7.
4. Escamilla RF, Babb E, DeWitt R, et al. Electromyographicanalysis of traditional and nontraditional abdominal exercises:implications for rehabilitation and training. Phys Ther 2006;86:656-71.
Suppliers. Pilates International, Unit 1, Broadbent Close, 20/22 Highgate High
St, London, N6 5JG UK.. Aloka 55D-900; Aloka Co Ltd, 6-22-1, Mure, Mitaka-shi, Tokyo,
181-8622 Japan.
. SPSS Inc, 233 S Wacker Dr, 11th Fl, Chicago, IL 60606.








![Second Slide%20 %20 Slide%20 Sharing%20 Made%20 Easy%20with%20the%20 Innovation%20 Second Slide%20 Service[1]](https://img.pdfslide.us/doc/110x75/55a267641a28abca6b8b47e1/second-slide20-20-slide20-sharing20-made20-easy20with20the20-innovation20-second-slide20-service1.jpg)













![Investigating%20 earthquakes%20with%20arcexplorer%20gis[1]](https://img.pdfslide.us/doc/110x75/55bac8ddbb61ebfc108b47c1/investigating20-earthquakes20with20arcexplorer20gis1.jpg)