Embed Size (px)
Citation preview
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 1/17
Plenary Discussion
Group
15 C
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 2/17
Akhmad Syukri Harahap
Doan
Fajar Tri Decroli
Fathiyyatul Khaira
Hedo Hidayat
Maretha Anthiya Tamimi
Melati Setia Ningsih
Nisha Anggia
Osharinanda Monita
Vini Jamarin
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 3/17
Miss Sinef’s Feet and Stomach Ms. Sinef, 16 years, came to the health center with complaints
of leg swollen and distended abdomen since 2 weeks ago. From the
physical examination found ascites and edema of both legs. From thelaboratory results obtained albuminurine++++. The doctor
explained to Ms. Sinef and his family, may have been a "leak" in the
kidneys and advocate for referral to hospital, for further
examination and treatment. At the same time also encountered
patients present with complaints of pain during urination, and withpolyuria. Laboratory results visible sediment+++ leukocytes. The
patient is anxious that jengkol which he ate yesterday cause
infection.
In the hospital, laboratory examination of the Ms.Sinef, withresults Esbach 4gr/24 hours, total cholesterol 950 mg/dl. The doctor
explained to Ms. Sinef about her illness and asked Ms. Sinef
Approval renal biopsy to more accurate diagnosis and management.
How do you explain what happened in the two patients above?
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 4/17
Terminology
• Ascites : accumulation of serous liquid in
peritoneum cavity
• Edema : accumulation of liquid in interstisium• Poliuria : excretion of urine more than 2L a day
• Albuminuria : presence of albumin in the urine
• Esbach : examination to assess the levels of normal protein
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 5/17
Identification and Analysis
Problems
1. Why are Mrs. Sinef’s feet swollen and distended
abdomen since 2 weeks ago?
Cause of Edema:
Increased hydrostatic pressure. Hydrostatic pressure is the
pressure that drives fluid from the plasma into the interstitial
space (ex: heart failure, cirrhosis hepatis).
Decreased plasma oncotic pressure. Plasma osmotic pressure is the pressure that maintains the fluid in blood
vessels by drawing fluid from the space intersrtitial.
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 6/17
Causes of fall of plasma oncotic pressure:
- Hepatic Cirrhosis impaired protein synthesis
- Nephrotic syndrome albumin out with urine.
- Less intake of protein
Obstruction of lymph channels.
Increased capillary permeability. (Ex: inflammation, allergy)
Cause Ascites:
portal hypertension. The high resistance to blood flow through the
heart vessels switched to mesentrika. High resistance to flow causesincreased vascular mesentrika and increased capillary pressure - fluid
will then leak.
Decrease colloid osmotic pressure
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 7/17
2. How is laboratory interpretation?
Albuminuria ++++: indicates that the protein comes out with urine over 1 gr/100
ml urine. The presence of proteinuria
showed that there was a disease that
affects the kidneys, especially glomerolus.
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 8/17
3. Why does doctor say there may have
been a leak in the kidney Nn. Sinef?
Because of the results of the spending has
occurred with proteinuria, which in a good
state of renal function there is no
expenditure of protein in the urine.
??
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 9/17
4. Why does the second patient complain
with disuria and polyuria
• pain during urination caused by urinary
tract disorders such as trauma, urinary
tract infections, or urinary tract stones.
• Polyuria may occur in patients with DM
and use diuretic.
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 10/17
5. How is interpretation of laboratory of
the second patient?
Leukocytes+++: indicates the presence of
more than 50 leucocytes/LPK. generallyindicate a urinary tract infection.
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 11/17
6. How is jengkol relationship with theillness now?
• not related
• jengkol acid will form crystals that canirritate the kidneys. This crystal will
cause colicky pain in patients
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 12/17
7. How are the interpretation of esbach and
cholesterol examination of Ms. Sinef?
• Esbach 4gr/ 24 hour massive
albuminuria
• Total cholesterol 950 mg/dl means that
hyperlipidemia. Increased lipidemia
associated with hipoalbuminenia
condition.
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 13/17
8. Why need biopsy assessment to Ms.
Sinef
Kidney biopsy is one of the diagnostic
techniques in determining histophatology
of kidney damage.
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 14/17
9. how is the management of these patients in both?
Patient I:
• protein diet, low fat and low salt• Diuretic
• Inhibition of angiotensin-converting (ACE Inhbitor)
Patient II:• Maintain cleanliness around the sex organs and the urinary
tract
• Each urinate, wipe from front to back. This reduces the
possibility of entry of bacteria from the anus to the urethra.
• Do not hold back urine. Discard the urine as needed
• Many consume fluids
• Provide appropriate antibiotic culture results
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 15/17
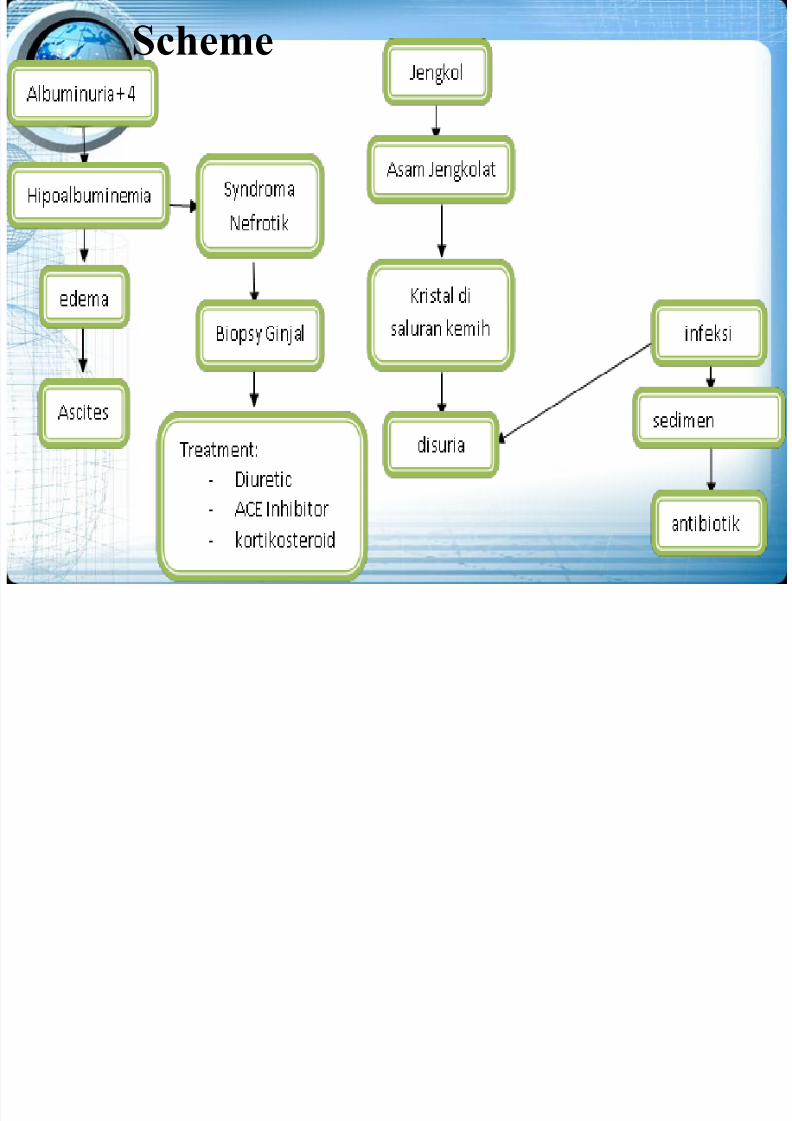
Scheme
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 16/17
LEARNING OBJECTIVES
Student can explain about:
1. Immunology disorder of urinaria
system2. Urine duct Infections
7/29/2019 pleno minggu 3
http://slidepdf.com/reader/full/pleno-minggu-3 17/17
Any Questions??