Embed Size (px)
Citation preview

Kidney International, Vol. 58 (2000), pp. 293–301
Plasma lipids and risk of developing renal dysfunction:The Atherosclerosis Risk in Communities Study
PAUL MUNTNER, JOSEF CORESH, J. CLINTON SMITH, JOHN ECKFELDT, and MICHAEL J. KLAG
Departments of Epidemiology, Biostatistics, Medicine, Health Policy and Management, The Johns Hopkins University Schoolsof Hygiene and Public Health and Medicine, Baltimore, Maryland; Department of Pediatrics, University of Mississippi Schoolof Medicine, Jackson, Mississippi; and Department of Laboratory Medicine and Pathology, University of Minnesota,Minneapolis, Minnesota, USA
Plasma lipids and risk of developing renal dysfunction: The also been demonstrated to have adverse effects on theAtherosclerosis Risk in Communities Study. kidney and is strongly associated with initiation [6] of
Background. Animal and in vitro data suggest that dyslipi- renal disease and accelerated loss of kidney functiondemia plays an important role in the initiation and progression[7–9]. More recently, it has been suggested that dyslipide-of chronic renal disease, but few prospective studies have beenmia may contribute to accelerated development of renalconducted in humans.
Methods. We studied the relationship of plasma lipids to a insufficiency [10–14]. Although there is substantial ani-rise in serum creatinine of 0.4 mg/dL or greater in 12,728 mal evidence supporting a causal relationship betweenAtherosclerosis Risk in Communities (ARIC) participants with lipid levels and the development of glomerular injurybaseline serum creatinine that was less than 2.0 mg/dL in men
leading to glomerulosclerosis [15, 16], human data areand less than 1.8 mg/dL in women.sparse [17–19]. To date, most prospective studies of lipidsResults. During a mean follow-up of 2.9 years, 191 persons
had a rise in creatinine of 0.4 mg/dL or greater, yielding an and renal disease have focused on the progression ofincidence rate of 5.1 per 1000 person years. Individuals with established renal disease rather than renal disease initia-higher triglycerides and lower high-density lipoprotein (HDL) tion [20–23]. There is only one study, to our knowledge,and HDL-2 cholesterol at baseline were at increased risk for
that has focused on lipids predicting renal disease initia-a rise in creatinine after adjustment for race, gender, baselinetion [10]. Therefore, little is known about the prospectiveage, diabetes, serum creatinine, systolic blood pressure, and
antihypertensive medication use (all P trends #0.02). The ad- relationship between lipids and declines in renal functionjusted relative risk for the highest versus lowest quartile of among persons with normal renal function. Such infor-triglycerides was 1.65 (95% CI, 1.1, 2.5, P 5 0.01) and for HDL mation is necessary to identify modifiable risk factorswas 0.47 (95% CI, 0.3, 0.8, P 5 0.003). These associations were
that predict development and progression of renal dis-significant in participants with normal creatinine (defined asease.,1.4 mg/dL for men and ,1.2 mg/dL for women), with diabe-
tes, and without diabetes. The effect of high triglycerides was We sought to determine the association of plasmaindependent of plasma glucose, but was weaker and less consis- lipids with loss of renal function and the clinical onsettent after further adjustment for fasting insulin in nondiabetics. of mild renal insufficiency. To achieve this goal, we pro-Conclusions. High triglycerides and low HDL cholesterol,
spectively assessed 12,728 participants of the Atheroscle-but not low-density lipoprotein cholesterol, predict an in-rosis Risk in Communities (ARIC) study during threecreased risk of renal dysfunction. The treatment of these lipid
abnormalities may decrease the incidence of early renal dis- years of follow-up.ease.
METHODSEpidemiological studies have shown that hypertension The sample population for this study was drawn from
and dyslipidemia are both risk factors for the develop- the ARIC Study cohort, which was comprised of popula-ment of cardiovascular disease [1–5]. Hypertension has tion-based samples from four U.S. communities: Forsyth
County, North Carolina; Jackson, Mississippi; suburbanMinneapolis, Minnesota; and Washington County, Mary-Key words: chronic renal disease, triglycerides, cholesterol, glomerular
injury, progression of renal disease. land. The complete design of ARIC has been publishedpreviously [24]. In brief, 15,792 men and women ages 45Received for publication April 29, 1999to 64 were recruited from 1987 through 1989 throughand in revised form September 15, 1999
Accepted for publication February 1, 2000 the use of probability sampling techniques. Follow-upvisits occurred in three-year intervals, at which time par- 2000 by the International Society of Nephrology
293

Muntner et al: Lipids and renal disease294
ticipants underwent standardized examinations in field was abstracted from questionnaires. Baseline informa-tion on the use of antihypertensive and lipid-loweringcenter clinics. These follow-up visits included measure-
ments of demographic, lifestyle, and physiological char- medications was determined through interview and ex-amination of pill bottles brought to the study interview.acteristics. This report is based on data from the baseline
examination and the first follow-up examination of the The presence of hypertension was defined as a systolicblood pressure $140 mm Hg, a diastolic blood pressurecohort (1987 through 1989 and 1990 through 1993, re-
spectively). The overall ARIC cohort follow-up rate for $90 mm Hg, or the use of antihypertensive medications.Diabetes mellitus was defined as a fasting glucose ofvisit 2 exceeded 93%.$126 mg/dL, nonfasting glucose of $200 mg/dL, or his-
Exclusion criteria tory/treatment of diabetes. Serum glucose was assayedby the hexokinase method. A central laboratory mea-Persons (N 5 53) with severe hypercreatinemia (Cr $
2.0 mg/dL for males, Cr $ 1.8 mg/dL for females) at sured fasting insulin with a nonspecific radioimmuno-assay.baseline were excluded because of the high probability of
substantial renal dysfunction [25]. Participants on lipid-Definition of outcomelowering medications at baseline (N 5 563) were also
excluded because of concerns that their baseline lipid At both the baseline and follow-up visits, serum creati-nine was measured using a modified kinetic Jaffe methodmeasurements may not reflect their true risk profile [26].
By necessity, persons with missing data for lipids or creat- [27]. Assessment of the methodological and day-to-dayvariability within ARIC participants revealed that 0.18inine at baseline (N 5 623), missing covariates (sex, race,
diabetes status, antihypertensive medication use, N 5 mg/dL (methodogical variability, SD 5 0.0494, andwithin-person variability, SD 5 0.043) was the minimal48), or missing creatinine data at follow-up (N 5 1300)
were excluded. Of the 1300 participants with missing change in creatinine at which 95% confidence existedthat a true change had occurred [28]. We defined ancreatinine at follow-up, 307 had died, while 38 were miss-
ing serum measurements, and 955 (6% of visit 1 partici- incident rise in serum creatinine as a change greater thantwice this amount ($0.4 mg/dL) during the approxi-pants) did not attend ARIC visit 2. ARIC participants
who did not fast for eight hours prior to their serum mately three-year follow-up period. A change in esti-mated creatinine clearance during follow-up was useddraw were excluded (N 5 413) from all analyses. In
addition, we limited our analysis to white and African as an additional outcome measure of change in renalfunction. Creatinine clearance was estimated using theAmerican participants because of small numbers of par-
ticipants from other races (N 5 48). These exclusion Cockroft-Gault formula [29] adjusted for body size bydividing by body surface area [30] and multiplying bycriteria left us with a population of 12,728 for our primary
analyses. 1.73. The outcome for this analysis was defined as indi-viduals whose calculated creatinine clearance declined
Measurements by 25% or more.Serum and ethylenediaminetetraacetic acid (EDTA)
Statistical methodsplasma from all participants were drawn at each visit.Participants were asked to fast at least 12 hours before Plasma lipids assessed at baseline were the primary
exposures of interest. These included total cholesterol;the blood draw. Blood was drawn from the antecubitalvein while the participants were seated, and blood chem- HDL cholesterol and its subfractions, HDL-2, and HDL-3
cholesterol; LDL cholesterol; apolipoprotein A-1; apoli-istries were performed at the ARIC central chemistrylaboratory at the University of Minnesota and plasma poprotein-B; Lp(a); and triglycerides. Because of their
skewed distribution, triglycerides were log transformed.lipids at the ARIC central lipid laboratory in Houston,Texas, USA. Plasma cholesterol, plasma triglycerides, Other variables were chosen as covariates, based on a
priori considerations, because they were thought to in-and high-density lipoprotein (HDL) cholesterol were de-termined using enzymatic methods and low-density lipo- fluence change in serum creatinine. These included the
following clinical and demographic characteristics: gen-protein (LDL) cholesterol was calculated using the Frie-dewald equation [27]. Apolipoproteins A-1 and B were der, race, age, diabetes mellitus, systolic blood pressure,
and baseline creatinine. Since some antihypertensivemeasured using radioimmunoassay and Lp(a) using adouble-antibody enzyme-linked immunosorbent assay medications are associated with dyslipidemia [31, 32], we
also adjusted for the type of antihypertensive medication(ELISA) technique [27] for apo(a) detection. ARICtechnicians, trained and certified in the use of a random- being taken. Antihypertensive medications were divided
into four categories: diuretics, ACE inhibitors, thiazides,zero sphygmomanometer, took three blood pressuremeasurements following a standardized procedure; an and any other anti-hypertensive medication.
Length of follow-up between the ARIC baseline visitaverage of the second and third measurements was usedto estimate blood pressure. Gender and age information and the first follow-up visit (ARIC visit 2) was deter-

Muntner et al: Lipids and renal disease 295
Table 1. Baseline characteristics of the study population and casesmined for each participant, and the rise in serum creati-who subsequently developed a rise in creatinine $0.4 mg/dL
nine incidence rate was calculated by quartile of lipids.Characteristic ARIC population CasesTrends in crude incidence rates across lipid quartilesN 12,728 191were determined using Poisson regression [33]. PoissonMale gender 45% 51%regression was also used to determine the adjusted (forBlack race 23% 47%
the a priori chosen clinical and demographic characteris- Diabetes mellitus 10% 29%On antihypertensive medications 23% 43%tics) relative risks and 95% confidence intervals of a riseHypertensive 32% 62%in serum creatinine with the lowest quartile of lipid level
Mean (SD) Mean (SD)as the comparison group. The statistical significance ofthe trends in risk of a rise in serum creatinine across Age years 54 (6) 56 (6)
Creatinine mg/dL 1.09 (0.19) 1.15 (0.29)lipid quartiles was determined for the adjusted modelsSBP mm Hg 121 (18) 133 (26)using the Wald test and quartile number as a continuous DBP mm Hg 74 (11) 78 (14)
variable. Total cholesterol mg/dL 215 (42) 222 (52)Triglycerides mg/dL 128 (79) 160 (121)Analyses with lipid levels as continuous variables wereLoge triglycerides log mg/dL 4.7 (0.5) 4.9 (0.6)used to confirm the associations detected using quartile HDL cholesterol mg/dL 53 (18) 50 (15)
analyses. Relative risks in the continuous analyses are HDL-2 cholesterol mg/dL 15 (9) 13 (8)HDL-3 cholesterol mg/dL 39 (11) 37 (11)quoted for differences that approximate the median dif-LDL cholesterol mg/dL 135 (39) 135 (39)ference between the first and fourth quartiles (threefold Lp(a) 98 (105) 133 (134)
higher triglyceride levels and 40 mg/dL higher HDL cho- Loge Lp(a) 4.0 (1.2) 4.3 (1.2)Apolipoprotein A-I mg/dL 133 (31) 129 (31)lesterol). Analyses with lipids as continuous variablesApolipoprotein B mg/dL 93 (29) 97 (34)were conducted for the overall population and stratified
The study population was limited to persons without severe hypercreatinemiaby creatinine at baseline: normal creatinine (Cr # 1.3 (serum creatinine #2.0 mg/dL for males; #1.8 mg/dL for females) and not onlipid-lowering medications.mg/dL for males, Cr # 1.1 mg/dL for females, N 5
Abbreviations are: SBP, systolic blood pressure; DBP, diastolic blood pres-11,323) and hypercreatinemia (1.4 # Cr # 1.9 mg/dL for sure; ARIC, Atherosclerosis Risk in Communities study.males, 1.2 # Cr # 1.7 mg/dL for females, N 5 1818).Analyses were also conducted stratified by race and dia-betes and hypertension status at baseline.
cholesterol, and apolipoprotein A-1 demonstrated lowerBecause higher triglyceride levels and lower HDL cho-incidence rates (all P # 0.05). A greater than twofoldlesterol levels are markers of the insulin-resistance syn-difference in incidence rates across lipid quartiles oc-drome [34–36], additional analyses were performed usingcurred with HDL cholesterol. The incidence of a creati-continuous lipid levels and adjusting for baseline glucosenine rise was not associated with total cholesterol, LDLand insulin levels. Insulin levels in diabetics are consid-cholesterol, or apolipoprotein B levels (P 5 0.31, 0.66,ered not reliable; therefore, the effect of lipid levels wasand 0.33, respectively).assessed applying insulin levels in nondiabetics and a
As shown in Table 1, individuals who later developeddummy variable for insulin levels for ARIC participantsa rise in creatinine were substantially more likely to bewith diabetes mellitus. Finally, Poisson regression mod-black, have diabetes, and use antihypertensive medica-els were fit using a decline in creatinine clearance, ap-tions at baseline. In addition, cases had a higher meanproximated by the Cockroft-Gault formula, 25% or moreage, baseline serum creatinine, and blood pressure. Theas the outcome. All analyses were also conducted with-bottom row of each lipid listing in Table 2 shows theout adjustment for baseline serum creatinine and yieldedrelative risk of a rise in creatinine after adjustment forsimilar results.all of these, and other, characteristics. Quartiles of tri-glycerides, HDL cholesterol, and HDL-2 cholesterol
RESULTS maintained strong dose response associations with anBaseline characteristics of the ARIC participants are incident rise in creatinine (P # 0.05) after adjusting for
displayed in Table 1. The mean length of follow-up be- race, gender, age, and baseline systolic blood pressure,tween the ARIC baseline visit and the first follow-up visit type of antihypertensive medication use, diabetes melli-was 2.9 years. During follow-up, 1.7% of the participants tus status, and creatinine. Additionally, the relative risk(N 5 191) experienced a creatinine rise of $0.4 mg/dL comparing the highest with the lowest quartile of HDL(characteristics are displayed in Table 1), yielding an and HDL-2 cholesterol, and triglycerides were all sig-overall incidence rate of 5.1 per 1000 person years of nificantly different from 1.0. The risk of a rise in creati-follow-up. In contrast, only 0.2% had a fall of #0.4 mg/dL. nine in the highest quartile of triglycerides was 1.65 times
Higher quartiles of triglycerides and Lp(a) were asso- that for the lowest quartile (P 5 0.01). Persons in theciated with a higher incidence of creatinine rise (Table 2). highest quartiles of HDL cholesterol and HDL-2 choles-
terol were 0.47 and 0.57, respectively, times as likely toIn contrast, higher quartiles of HDL, HDL-2, and HDL-3

Muntner et al: Lipids and renal disease296
Table 2. Incidence, adjusteda relative risks and 95% confidence intervals of a rise in creatinine $0.4 mg/dL from baseline to the 3-yearfollow-up by lipid quartiles at baseline in 13,141 participants
Quartile
Lipid 1 2 3 4 P trend
Total cholesterol mg/dLRange #186 187–212 213–239 $240N events 45 47 45 54Rate per 1000 patient-years 4.8 4.9 4.9 5.9 0.31Adjusted relative riska 1.0 1.02 (0.7,1.5) 0.96 (0.7,1.5) 1.06 (0.7,1.6) 0.85
TriglyceridesRange #78 79–109 110–155 $156N events 38 36 50 67Rate per 1000 patient-years 4.0 3.9 5.4 7.2 0.0009Adjusted relative riska 1.0 0.99 (0.6,1.6) 1.31 (0.9,2.0) 1.65 (1.1,2.5) 0.008
HDL cholesterol mg/dLRange #41 42–51 52–63 $64N events 62 48 55 26Rate per 1000 patient-years 6.8 5.1 5.8 2.8 0.0009Adjusted relative riska 1.0 0.73 (0.5,1.1) 0.86 (0.6,1.3) 0.47 (0.3,0.8) 0.01
HDL-2 cholesterol mg/dLRange #9 10–13 14–19 $20N events 72 41 49 29Rate per 1000 patient-years 6.6 4.4 5.6 3.5 0.01Adjusted relative riska 1.0 0.65 (0.4,1.0) 0.84 (0.6,1.2) 0.57 (0.4,0.9) 0.05
HDL-3 cholesterol mg/dLRange #31 32–38 39–46 $47N events 56 53 51 31Rate per 1000 patient-years 6.3 5.2 5.5 3.5 0.02Adjusted relative riska 1.0 0.89 (0.6,1.3) 0.99 (0.7,1.5) 0.67 (0.4,1.1) 0.17
LDL cholesterol mg/dLRange #109 110–132 133–159 $160N events 48 44 50 49Rate per 1000 patient-years 5.0 4.9 5.2 5.4 0.66Adjusted relative riska 1.0 0.97 (0.6,1.5) 0.97 (0.7,1.4) 0.90 (0.6,1.3) 0.62
Lp(a)Range #3.14 3.15–4.09 4.10–4.97 $4.98N events 40 42 44 65Rate per 1000 patient-years 4.3 4.4 4.7 7.0 0.01Adjusted relative riska 1.0 0.96 (0.6,1.5) 0.83 (0.5,1.3) 1.10 (0.7,1.7) 0.70
Apolipoprotein A mg/dLRange #111 112–130 131–151 $152N events 62 45 47 37Rate per 1000 patient-years 6.6 4.8 5.1 4.1 0.03Adjusted relative riska 1.0 0.73 (0.5,1.1) 0.79 (0.5,1.2) 0.66 (0.4,1.0) 0.08
Apolipoprotein B mg/dLRange #73 74–89 90–110 $111N events 46 41 55 49Rate per 1000 patient-years 4.8 4.5 5.7 5.5 0.33Adjusted relative riska 1.0 0.87 (0.6,1.3) 1.03 (0.7,1.5) 0.88 (0.6,1.3) 0.73
Adjusted relative risks compare quartile of plasma lipids to the lowest quartile (quartile 1) of lipid level.aAdjusted for age, race, gender, and baseline systolic blood pressure, diabetes mellitus, antihypertensive medication use and serum creatinine
experience a rise in creatinine compared with those in cal characteristics, log triglycerides remained predictiveof an incident rise in creatinine, while HDL cholesterolthe lowest quartile (P , 0.02 for each).
Levels of plasma triglycerides and HDL cholesterol did not. The risk of a rise in creatinine was 1.45 (95%CI, 1.0, 2.1, P 5 0.04) times greater for threefold higherwere inversely associated with each other (correlation
of 20.5). To discern whether the effects of these lipids (1.09 loge units) triglycerides; HDL cholesterol was notassociated with loss of renal function after adjustmentwere independent, a Poisson regression model with
plasma triglycerides and HDL cholesterol as well as clini- for triglycerides (RR 5 0.72 for an 40 mg/dL increasein HDL cholesterol; 95% CI, 0.5, 1.1, P 5 0.15). Becausecal and demographic variables was fit. To enhance the
power of the analysis, lipids were modeled as continuous of the high correlation between HDL and HDL-2 choles-terol (r 5 0.81), HDL-2 was not included in this model.variables with triglycerides log transformed because of
their skewed distribution. In a model containing HDL Using HDL-2 cholesterol rather than HDL cholesterolyielded similar results.cholesterol, log triglycerides, and demographic and clini-

Muntner et al: Lipids and renal disease 297
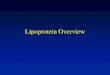
Fig. 1. Adjusted relative risk of an incidentrise in creatinine between ARIC visit 1 andvisit 2 for a threefold higher baseline plasmatriglyceride level (1.10 loge units) overall andin selected subgroups. Relative risks were ad-justed for sex, race, and baseline age, diabetesmellitus status, systolic blood pressure, typeof hypertension medication use, and creati-nine in a Poisson regression model.
To determine the consistency of the relationship be- in addition to the a priori chosen clinical and demo-graphic characteristics only slightly attenuated the asso-tween increased triglyceride levels and a rise in creati-
nine, analyses were conducted stratified by race, creati- ciations between triglycerides and HDL and a rise increatinine (model 3 compared with model 2; Table 3).nine level, diabetes mellitus, and hypertension status at
baseline (Fig. 1). For each threefold higher triglycerides, Further adjustment for insulin levels in nondiabetics sub-stantially attenuated the associations between HDL cho-the adjusted relative risk of a rise in creatinine was 2.39
(P 5 0.001) among African Americans and 1.31 (P 5 lesterol, triglycerides, and a rise in creatinine (model 4;Table 3). Among nondiabetics, adjustment for insulin0.20) among whites, a difference in effect of triglycerides
that was not statistically significant (P interaction 5 negated the associations between both triglycerides andHDL cholesterol and a rise in creatinine (both P . 0.20).0.08). The adjusted relative risk among persons with
normal creatinine at baseline was 1.68 (P 5 0.005). Next, the data were analyzed using change in creati-nine clearance as the outcome, defined as a $25% de-Among persons with borderline or definite hypercreati-
nemia, the relative risk was 1.35 (P 5 0.35). This disparity crease in creatinine clearance. There were 407 incidentcases during follow-up. Over 93% of cases defined by awas consistent with random variation (P interaction 5
0.78). The adjusted relative risk of a rise in creatinine rise in creatinine met this alternate outcome definition,but only 48% of persons having a $25% decrease inamong nondiabetics at baseline was 1.48 (P 5 0.04) for
each threefold higher triglycerides and 2.44 (P 5 0.007) calculated creatinine clearance had a creatinine increase$0.4 mg/dL. After adjusting for age, sex, race, diabetes,among diabetics (P interaction 5 0.19). Additionally, for
each threefold higher triglycerides, the adjusted relative systolic blood pressure, type of antihypertensive medica-tion, and baseline creatinine clearance, the relative riskrisk of a rise in creatinine was 1.65 (P 5 0.05) and 1.57
(P 5 0.03) for normotensives and hypertensives, respec- of developing a $25% decrease in creatinine clearancewas 1.54 (95% CI 1.2, 1.9, P 5 0.001) for each threefoldtively. Body mass index was not associated with declining
renal function, and further adjustment for it yielded no higher triglycerides. Redefining the outcome as a largerdecline ($30%, $40%) in creatinine clearance resultedmeaningful changes in the association between lipids and
renal dysfunction. in progressively larger relative risks. For each threefoldhigher triglycerides, the relative risks of developing aAdjustment for serum glucose as a continuous variable

Muntner et al: Lipids and renal disease298
Table 3. Relative risks and 95% confidence intervals for a rise in creatinine for threefold higher plasma triglycerides and 30 mg/dLhigher HDL cholesterol
Overall No Diabetes Mellitus Diabetes Mellitus
Lipid Model RR (95% CI) P value RR (95% CI) P value RR (95% CI) P value
Plasma 1. Crude 1.77 (1.3,2.4) 0.0001 1.44 (1.0,2.0) 0.04 1.77 (1.0,3.2) 0.05triglycerides 2. Adjusteda 1.64 (1.2,2.2) 0.002 1.48 (1.0,2.1) 0.04 2.44 (1.3,4.7) 0.007
3. Glucoseb 1.49 (1.1,2.1) 0.02 1.42 (1.0,2.1) 0.07 1.88 (1.0,3.7) 0.074. Fullc 1.37 (1.0,1.9) 0.07 1.25 (0.8,1.9) 0.28 — —
HDL 1. Crude 0.53 (0.4,0.8) 0.0008 0.66 (0.4,1.0) 0.03 0.38 (0.1,1.1) 0.06cholesterol 2. Adjusteda 0.58 (0.4,0.9) 0.01 0.62 (0.4,1.0) 0.03 0.31 (0.1,1.0) 0.05
3. Glucoseb 0.63 (0.4,0.9) 0.03 0.65 (0.4,1.0) 0.05 0.39 (0.1,1.2) 0.114. Fullc 0.70 (0.5,1.1) 0.10 0.75 (0.5,1.2) 0.22 — —
aAdjusted for sex, race, and baseline age, antihypertensive medications, serum creatinine, and systolic blood pressurebAdjusts for baseline glucose in addition to the factors in model 2cAdjusts for baseline glucose, insulin in nondiabetics, and the factors in model 2
large decline in creatinine clearance ($30%, $40%) for other lipid levels, demographic, and clinical charac-were 1.68 (P 5 0.004) and 4.67 (P 5 0.001), both of teristics, higher triglycerides at baseline were associatedwhich were statistically significant. Adjustment for fast- with a significantly higher risk of creatinine rise duringing insulin and glucose had only a minimal effect on the follow-up. When insulin levels among nondiabetics weremagnitude of these associations, and triglycerides, but considered in the analysis, however, the effect of triglyc-not HDL cholesterol, were a statistically significant pre- erides was reduced and no longer significant. In contrast,dictor of a decline in creatinine clearance. After adjust- when a 25% or greater decline in creatinine clearancement for insulin, glucose, and the other covariates, a was used as the outcome, higher plasma triglyceridesthreefold higher amount of triglycerides was associated predicted a loss of renal function independent of insulinwith a relative risk of 1.51 (95% CI, 1.2 to 2.0; P 5 0.003) levels. These results raise the possibility that the insulin-for a 25% decline in creatinine clearance. resistance syndrome may underlie or mediate the ob-
As mentioned previously, ARIC participants on lipid- served associations between lipids and a loss of renallowering medications were excluded from these analyses. function. Although BMI is frequently associated withWhen the 563 participants on lipid-lowering medications both renal disease and the insulin-resistance syndrome,were included, the results remained virtually identical in further adjustment for BMI yielded no changes in theboth magnitude and significance. Re-analyzing the data association between lipids and renal dysfunction.excluding persons who were placed on lipid-lowering Possible mechanisms whereby dyslipidemia causes re-medications during follow-up (N 5 605, 22 cases of renal nal injury have been reviewed [8, 37, 38]. While thedysfunction) did not substantially change the results of pathophysiology by which hypercholesterolemia mayany of our analyses. cause damage to the kidney is uncertain, experimental
data support the hypothesis that glomerulosclerosis andatherosclerosis share common mechanisms [38]. Similar-DISCUSSIONities in anatomical origin and functional properties ofThis study is the first to our knowledge to assess pro-glomerular mesangial cells to those of vascular smoothspectively the association between a large number ofmuscle cells provide clues to analogous cellular re-lipids and the subsequent decline in renal function insponses common to both atherosclerosis and glomerulo-the general population. In this study, HDL, HDL-2 cho-sclerosis [37, 38]. Many of the studies reviewed havelesterol, and triglycerides were all significant predictorsshown that glomerular lipid deposits and the appearanceof a rise in serum creatinine, a measure of renal function.of foam cells accompany renal injury in models of hyper-These associations persisted after adjustment for demo-lipidemia. Experimental data also suggest that dyslipide-graphic and clinical information, including sex, race, age,mia influences renal injury. In several animal models,systolic blood pressure, diabetes mellitus status, and typefeeding high cholesterol diets were associated with theof antihypertensive medication use. Among the lipidsinitiation of renal dysfunction [38], and pharmacologicwe investigated, triglycerides had the strongest and mostlowering of lipids with either clofibrate or lovastatin re-statistically significant association with a future declinesulted in a reduction of renal injury [39–41].in renal function. After adjustment for clinical and demo-
Several prospective studies in humans have shown angraphic factors, the highest quartile of log triglyceridesassociation between dyslipidemia and renal disease pro-imparted a 65% higher risk of developing a rise in creati-gression among patients with proven renal diseasenine $0.4 mg/dL within three years compared with the
lowest quartile of triglycerides. Even after adjustment [18–21]. In the Modification of Diet in Renal Disease

Muntner et al: Lipids and renal disease 299
(MDRD) study, low HDL cholesterol independently the length of follow-up is sufficiently long. In the pilotpredicted the rate of renal decline among 840 partici- phase of the MDRD study [45], this correlation was 0.70pants, but triglycerides were not examined [20]. In for 15 months of follow-up. The correlation in this studysmaller studies, total cholesterol [21, 22] and LDL choles- with three years of follow-up is likely to be even greater.terol [22], or apo(B) [22, 23] predicted renal disease Third, our results remained very similar when severalprogression. A detailed lipoprotein analysis in 44 pa- different definitions of substantial renal functional de-tients [18] showed a strong correlation of the rate of cline were applied. While examination of proteinuriaglomerular filtration rate decline with the plasma concen- would have been helpful as an additional confirmationtration of triglyceride-rich apoB containing lipoproteins of renal dysfunction, urine was not collected in the ARICbut no significant association with cholesterol-rich apoB- study.containing lipoproteins. Only one prospective study has We use the term early renal disease progression toexamined dyslipidemia and the risk of renal function reflect the fact that the majority of the individuals aredecline among persons without known renal disease. In making the transition from a “normal” serum creatininea subset of 2700 males from the Helsinki Heart Study to an “abnormal” serum creatinine. Although the results(HHS), a randomized clinical trial originally designed to of this study hold for patients with a normal serum creati-investigate the ability of gemfibrozil to prevent coronary nine at baseline, we cannot determine that these patientsheart disease, low HDL predicted a rise in creatinine, had no renal pathology at baseline. Thus, we cannotwhile no association was seen with triglycerides [10]. conclude that lipids affect renal disease initiation ratherThe association between HDL cholesterol and a rise in than early progression.creatinine was present in both the gemfibrozil treatment A possible concern with our analysis is the phenome-and placebo groups of the HHS, while no association non of regression to the mean. Because of variabilitybetween triglyceride levels and a rise in creatinine was or measurement error, participants with a low serumpresent in either group. The difference between our creatinine measurement at baseline may have a higherstudy and the HHS in the relative importance of HDL measurement at follow-up because their baseline mea-and triglycerides may be due to restriction of the Helsinki surement was lower than their long-term average (orstudy to persons with elevated non-HDL cholesterol. In “true”) value [46]. These participants’ serum creatinineaddition, the analysis in the HHS focused on the mean may have merely regressed back to its long-term meanprogression rate in all individuals, not the development level. We identified 32 ARIC participants whose creati-of hypercreatinemia as in our study. The mean progres- nine was 0.2 mg/dL or greater below the mean at baselinesion rate was not related to age, a well-demonstrated and whose creatinine measurement at the follow-up visitrisk factor for loss of renal function, and surprisingly was
was 0.4 mg/dL higher. Removing these 32 cases andmore strongly related to HDL cholesterol than blood
repeating our analyses yielded nearly identical results.pressure. Results from the present study provide addi-Alternatively, defining cases as individuals who had ational evidence that an excess of triglyceride-rich lipo-normal serum creatinine at baseline and a rise in creati-proteins and associated low HDL cholesterol plays anine of $0.4 mg/dL to at least 0.2 mg/dL greater thanlarger role in the decline of renal function than totalthe upper limit of normal yielded similar results as well.cholesterol or LDL cholesterol. Our results extend the
Even though the consistent prospective associationHHS findings to a different population with a broaderbetween lipids and a rise in creatinine was statisticallyrange of lipid measurements.significant and independent of other risk factors, theAlthough serum creatinine is quite commonly used aspotential for reverse causality is of concern. Lipoproteina measure of renal function, it has been criticized forabnormalities are very common in end-stage renal dis-being unreliable [42, 43]. Some people with low serumease patients [47–49]. The most common abnormalitiescreatinine may suffer from renal dysfunction, while someare elevated triglycerides and low HDL cholesterol. Inpeople with high serum creatinine do not always havethis analysis of ARIC data, lipids were measured onlyrenal impairment [44]. Nevertheless, we feel it appro-three years prior to the follow-up determination of creat-priate to use the change in serum creatinine betweeninine at visit 2. Dyslipidemia may have been presentbaseline and follow-up as a measure of renal impairmentbecause of subclinical renal disease at baseline. It is possi-for three reasons. First, most large prospective cohortble that like hypertension, dyslipidemia accelerates renalstudies investigating the risk of renal disease progressiondisease progression and renal disease increases dyslipi-use serum creatinine as a measure of renal functiondemia. An appropriate approach to reduce the effect of[9, 10] since direct measurement of the glomerular filtra-subclinical disease is to perform a study with longer fol-tion rate is substantially more expensive and time con-low-up. Serum creatinine measurements will soon besuming. Second, there is a strong correlation betweenavailable from the nine-year follow-up of the ARIC co-declines in the glomerular filtration rate assessed using
125I-iothalamate and changes in serum creatinine when hort. These data will provide an excellent opportunity

Muntner et al: Lipids and renal disease300
4. MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neatonto more fully determine the effect that dyslipidemia hasJ, Abbott R, Godwin J, Dyer A, Stamler J: Blood pressure,
on the incidence of declining renal function. stroke, and coronary heart disease. I. Prolonged differences inblood pressure: Prospective observational studies corrected forIn conclusion, this study implicates hypertriglyceride-regression dilution bias. Lancet 335:765–774, 1990mia in the initiation of mild renal insufficiency. Specifi-
5. Stamler J, Stamler R, Neaton JD: Blood pressure, systolic andcally, our study shows that persons with low HDL choles- diastolic and cardiovascular risks: US population data. Arch Intern
Med 153:598–615, 1993terol and hypertriglyceridemia at baseline have a higher6. Perneger T, Nieto F, Whelton P, Klag MJ, Comstock GW,risk of having a loss of renal function. While several
Szklo M: A prospective study of blood pressure and serum creati-clinical trials have shown that the use of lipid-lowering nine: Results from the “CLUE” study and ARIC study. JAMA
269:488–493, 1993medications and low cholesterol diets are effective in7. Ma KW, Greene EL, Raij L: Cardiovascular risk factors in chronicraising HDL cholesterol and lowering triglycerides in
renal failure and hemodialysis populations. Am J Kidney Dispersons with renal insufficiency [50–53], it is not known 19:505–513, 1992
8. Diamond J, Karnovsky M: Focal and segmental glomerulosclero-whether lipid-lowering therapy reduces renal diseasesis: Analogies to atherosclerosis. Kidney Int 33:917–924, 1988progression. Additional studies, of the long-term effects
9. Klag M, Whelton P, Randall B, Randall BL, Neaton JD,of dyslipidemia on mild renal insufficiency, the benefits Brancati FL, Ford CE, Shulman NB, Stamler J: Blood pressure
and end-stage renal disease in men. N Engl J Med 334:13–18, 1996of lipid-lowering therapy in preventing renal insuffi-10. Manttari M, Tiula E, Alikoski T, Manninen V: Effects of hyper-ciency, and the role of the insulin resistance syndrome tension and dylipidemia on the decline in renal function. Hyperten-
on the development of early renal dysfunction need to sion 26:670–676, 199511. Kamanna VS, Roh DD, Kirschenbaum MA: Atherogenic lipopro-be performed.
teins: Mediators of glomerular injury. Am J Nephrology 13:1–5,1993
ACKNOWLEDGMENTS 12. Wheeler DC, Bernard DB: Lipid abnormalities in the nephroticsyndrome: Causes, consequences, and treatment. Am J Kidney Dis
The ARIC study is carried out as a collaborative study supported 23:331–346, 1994by Contracts N01-HC-55015, N01-HC-55016, N01-HC-55018, N01-HC- 13. Appel G: Lipid abnormalities in renal disease. Kidney Int 39:169–55019, N01-HC-55020, N01-HC-55021, and N01-HC-55022 from the 183, 1991National Heart, Lung, and Blood Institute. Dr. Muntner was supported 14. Cramp DG: Plasma lipid alterations in patients with chronic renalby National Institutes of Health training grant T32HL07024-23. Dr. disease. CRC Crit Rev Clin Lab Sci 17:77–101, 1982Coresh was supported by grants from the National Institute of Diabetes 15. Kasiske B, O’Donnell M, Garvis W: Pharmacologic treatmentDigestive and Kidney Disease (DK48362) and the National Center of hyperlipidemia reduces glomerular injury in rat 5/6 nephrectomyfor Research Resources (GCRC grant RR00722). We wish to thank model of chronic renal failure. Circ Res 62:367–375, 1988the staff at the ARIC field centers and the coordinating center. In 16. Kasiske B, O’Donnell M, Schmitz P, Kim Y, Keane WF: Renalparticular, the following persons are acknowledged: Phyllis Johnson, injury in diet induced hypercholesterolemia in rats. Kidney IntMarilyn Knowles, and Melisa LaVergne from the University of North 37:880–891, 1990Carolina at Chapel Hill; Amy Haire, Delilah Posey, and Leslie Angel- 17. Sammuelsson O, Attman P, Knight-Gibson C, Larsson R, MulecPotter from the University of North Carolina at Winston Salem; Mary- H, Wedel H, Weiss L, Alaupovic P: Plasma levels of lipoproteinLouise Lauffer, Suzanne Pillsbury, and Anne Safrit from Wake Forest (a) do not predict progression of human chronic renal failure.University, Winston Salem; Cora L.K. Peoples, Cecile Snell, and Betty Nephrol Dial Transplant 11:2237–2243, 1996S. Warren from University of Mississippi Medical Center at Jackson; 18. Sammuelsson O, Attman P, Knight-Gibson C, Larsson R, MulecMolly Harrington, Darlene Heath, and Eli Justiniano from University H, Weiss L, Alaupovic P: Complex apolipoprotein B-containingof Minnesota, Minneapolis Center; Sunny Harrell, Patricia Hawbeaker, lipoprotein particles are associated with a higher rate of progressionand Joan Nelling from The Johns Hopkins University, Baltimore; Susan of human chronic renal insufficiency. J Am Soc Nephrol 9:1482–Mitterling, Ashley Ewing, and R. Christy Moore from the University 1488, 1998of Texas Medical School at Houston; Doris J. Harper, Charles E. 19. Diamond J: Effects of dietary interventions on glomerular patho-Rhodes, and Julita Samoro from Methodist Hospital Atherosclerosis physiology. Am J Physiol 258:F1–F8, 1990Clinical Laboratory, Houston; and Debbie Rubin Williams, Patsy 20. Hunsicker LG, Adler S, Gaggiula A, England BK, Greene T,Tacker, and Lily Wang from the ARIC Coordinating Center at the Kusek JW, Rogers NL, Teschan PE: Predictors of the progressionUniversity of North Carolina at Chapel Hill. of renal disease in the Modification of Diet in Renal Disease Study.
Kidney Int 51:1908–1919, 1997Reprint requests to Josef Coresh, M.D., Ph.D., Welch Center for 21. Washio M, Okuda S, Ikeda M, Hirakata H, Nanishi F, Onoyama
Prevention, Epidemiology, and Clinical Research, The Johns Hopkins K, Yoshimura T, Fujishima M: Hypercholesterolemia and theMedical Institutions, 2024 East Monument Street, Suite 2-600, Baltimore, progression of the renal dysfunction in chronic renal failure pa-Maryland 21205-2223, USA. tients. J Epidemiol 6:172–177, 1996E-mail: [email protected] 22. Samuelsson O, Mulec H, Knight-Gibson C, Attman PO, Kron
B, Larsson R, Weiss L, Wedel H, Alaupovic P: Lipoproteinabnormalities are associated with increased rate of progression ofREFERENCEShuman chronic renal insufficiency. Nephrol Dial Transplant 12:1908–1915, 19971. Neaton J, Wentworth D: Serum cholesterol, blood pressure, ciga-
rette smoking, and death from coronary heart disease: Overall 23. Samuelsson O, Aurell M, Knight-Gibson C, Alaupovic P, Att-man PO: Apolipoprotein-B containing lipoproteins and the pro-findings and differences by age for 316,099 white men: Multiple
Risk Factor Intervention Trial Research Group. Arch Intern Med gression of renal insufficiency. Nephron 63:279–285, 199324. The ARIC Investigators: The Atherosclerosis Risk in Communi-152:55–64, 1992
2. Castelli WP: Epidemiology of coronary heart disease: The Fra- ties (ARIC) Study: Design and objectives. Am J Epidemiol129:687–702, 1989mingham study. Am J Med 76:4–12, 1984
3. Stamler J, Dyer AR, Shekelle RB, Neaton J, Stamler R: Rela- 25. Perrone R, Madias N, Levey A: Serum creatinine as an index ofrenal function: New insights into old concepts. Clin Chem 38:1933–tionship of baseline major risk factors to coronary and all-cause
mortality, and to longevity: Findings from long-term follow-up of 1953, 199226. Benfante R, Hwang LJ, Masaki K, Curb JD: To what extent doChicago cohorts. Cardiology 82:191–222, 1993

Muntner et al: Lipids and renal disease 301
cardiovascular risk factor values measured in elderly men represent nephrectomy model of chronic renal failure. Circ Res 62:367–374,1988their midlife values measured 25 years earlier? A preliminary re-
41. Kasiske B, O’Donnell M, Cleary M, Keane WF: Treatment ofport and commentary from the Honolulu Heart Program. Am Jhyperlipidemia reduces glomerular injury in obese Zucker rats.Epidemiol 140:206–216, 1994Kidney Int 33:667–672, 198827. National Heart Lung and Blood Institute Atherosclerosis
42. Shemesh O, Golbertz H, Kriss J, Myers BD: Limitations ofRisk in Communities (ARIC) Study: Operations Manual No. 7:creatinine as a filtration marker in glomerulopathic patients. Kid-Blood Collection and Processing. Bethesda, National Heart, Lungney Int 28:830–838, 1985and Blood Institute, 1987
43. Walser M, Drew HH, LaFrance ND: Reciprocal creatinine slopes28. Eckfeldt JH, Chambless LE, Shen YL: Short-term within personoften give erroneous estimates of progression of chronic renalvariability in clinical chemistry results: Experience from the Ath-failure. Kidney Int 36(Suppl 27):S81–S85, 1989erosclerosis Risk in Communities Study. Arch Pathol Lab Med
44. Walser M, Drew HH, LaFrance ND: Creatinine measurements118:496–500, 1994 often yielded false estimates of progression in chronic renal failure.29. Cockroft DW, Gault MH: Prediction of creatinine clearance from Kidney Int 34:412–418, 1988
serum creatinine. Nephron 16:31–41, 1976 45. Modification of Diet in Renal Disease (MDRD) Study Group:30. du Bois D, du Bois EF: A formula to estimate the approximate Assessing the progression of renal disease in clinical studies: Effect
surface area if height and weight be known. Arch Intern Med of duration of follow-up and regression to the mean. J Am Soc17:863–871, 1916 Nephrol 1:1087–1094, 1991
31. Kasiske BL, Ma JZ, Kalil RSN, Louis TA: Effects of antihyper- 46. Yudkin PL, Stratton IM: How to deal with regression to thetensive therapy on serum lipids. Ann Intern Med 122:133–141, 1995 mean in intervention studies. Lancet 347:241–243, 1996
32. Weidmann P, Uehlinger DE, Gerber A: Antihypertensive treat- 47. Cameron J: The nephrotic syndrome and its complications. Am Jment and serum lipoproteins. J Hypertens 3:297–306, 1985 Kidney Dis 10:157–171, 1987
33. STATA: Version 5.0. College Station, TX 48. Cutler R: Lipid disorders in renal disease: Prevalence, pathogene-sis and diagnosis. Dial Transplant 17:533–536, 198834. Dengel DR, Goldberg AP, Mayuga RS, Kairis GM, Weir MR:
49. Chan M, Varghese Z, Moorhead J: Lipid abnormailities in ure-Insulin resistance, elevated glomerular filtration fraction, and renalmia, dialysis, and transplantation. Kidney Int 19:625–637, 1981injury. Hypertension 28:127–132, 1996
50. Goldberg A, Applebaum-Bowden D, Bierman EL, Hazzard35. Reaven GM: The kidney: An unwilling accomplice in syndromeWR, Haas LB, Sherrard DJ, Brunzell JD, Huttunen JK, Ehn-X. Am J Kidney Dis 30:928–931, 1997holm C, Nikkila EA: Increase in lipoprotein lipase during clofi-36. Dzurik R, Spustova V, Janekova K: The prevalence of insulinbrate treatment of hypertriglyceridemia in patients on hemodialy-resistance in kidney disease patients before the development ofsis. N Engl J Med 301:1073–1076, 1979renal failure. Nephron 69:281–285, 1995
51. Sherrard D, Goldberg A, Hass L, Brunzell JD: Chronic clofi-37. Klahr S, Schreiner G, Ichikawa I: The progression of renal brate therapy in maintenance hemodialysis patients. Nephrondisease. N Engl J Med 318:1657–1670, 1988 25:219–221, 1980
38. Diamond JR, Karnovsky MJ: Focal and segmental glomeruloscle- 52. Sanfelippo M, Swenson R, Reaven G: Response of plasma triglyc-rosis: Analogies to atherosclerosis. Kidney Int 33:917–924, 1988 erides to dietary changes in patients on hemodialysis. Kidney Int
39. Kasiske B, O’Donnell M, Cowardin W, Keane WF: Lipids and 14:180–186, 1978the kidney. Hypertension 15:443–450, 1990 53. Cattran D, Steiner G, Fenton S, Ampil M: Dialysis hyperlipid-
40. Kasiske B, O’Donnell M, Garvis W, Keane WF: Pharmacologic emia: Response to dietary manipulation. Clin Nephrol 13:177–182,1980treatment of hyperlipidemia reduces glomerular injury in rat 5/6