Embed Size (px)
Citation preview
The Multiethnic Study of Atherosclerosis (MESA) Cardiovascular Risk in Hispanics
Michael H. Criqui MD, MPH
Distinguished Professor and Chief, Division of Preventive Medicine
Department of Family and Preventive Medicine
Distinguished Professor, Department of Medicine
UCSD School of Medicine
22nd Annual Southwestern Conference on Medicine
Tucson, AZ, April 5, 2013
Financial disclosure - none
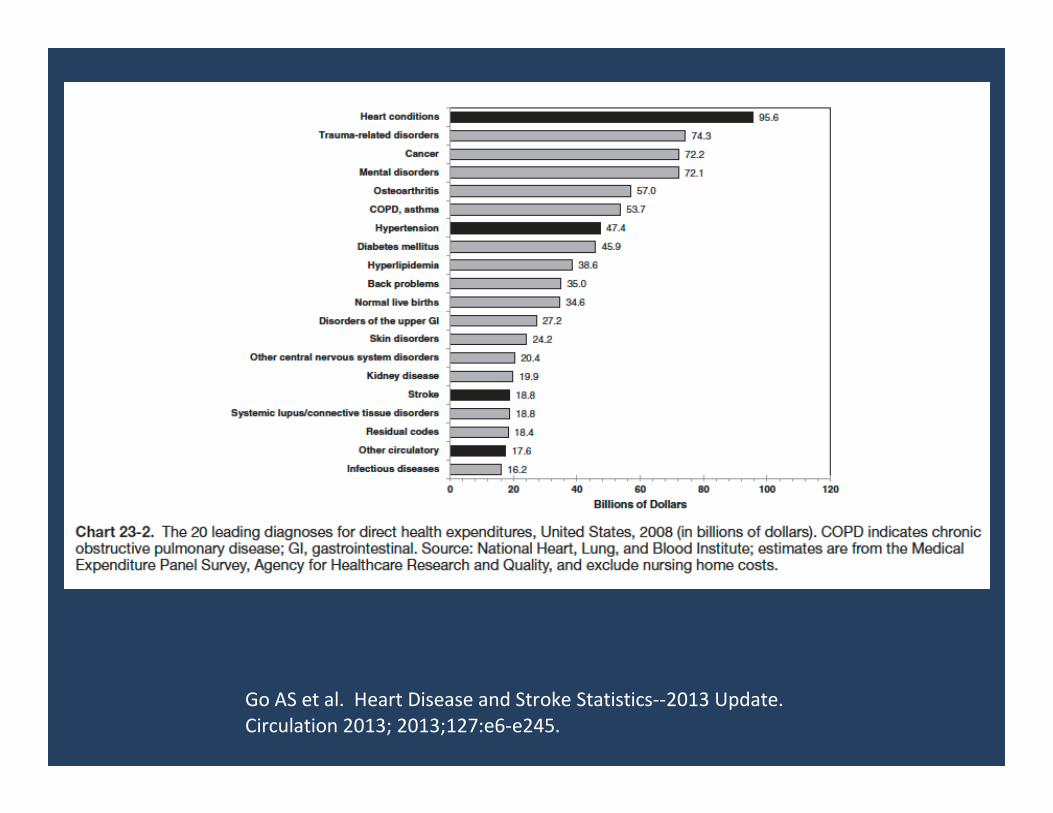
Go AS et al. Heart Disease and Stroke Statistics--2013 Update.
Circulation 2013; 2013;127:e6-e245.
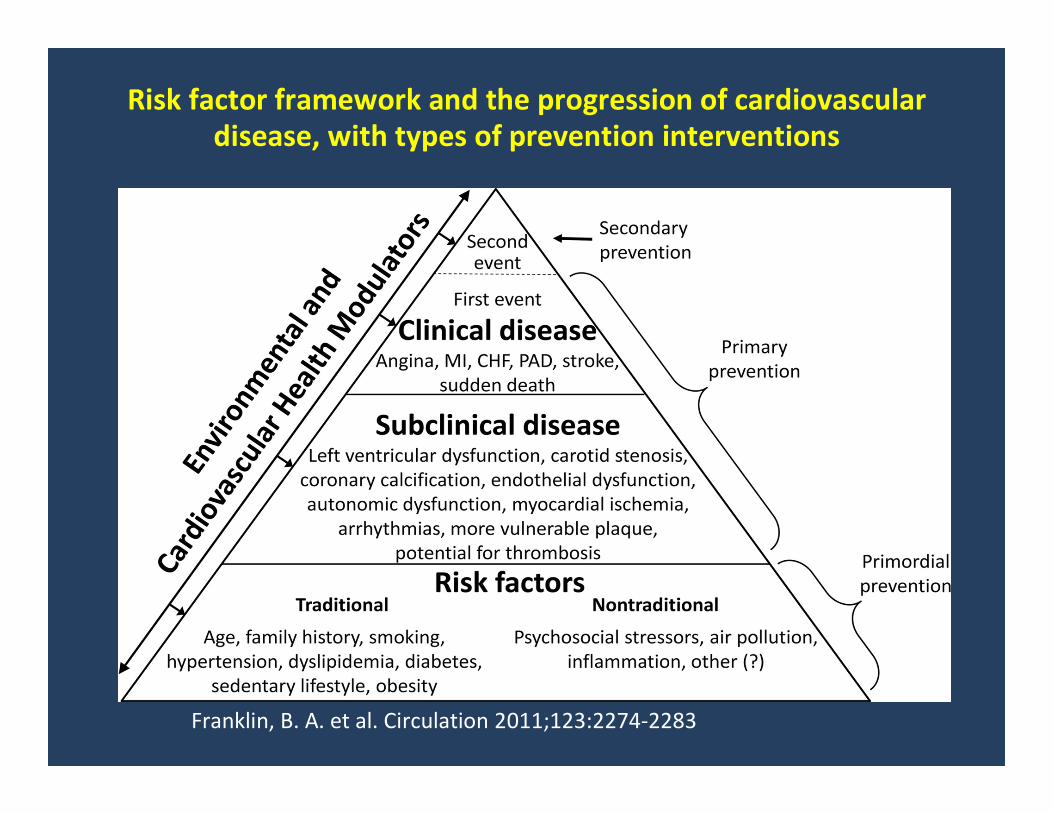
Franklin, B. A. et al. Circulation 2011;123:2274-2283
Risk factor framework and the progression of cardiovascular
disease, with types of prevention interventions
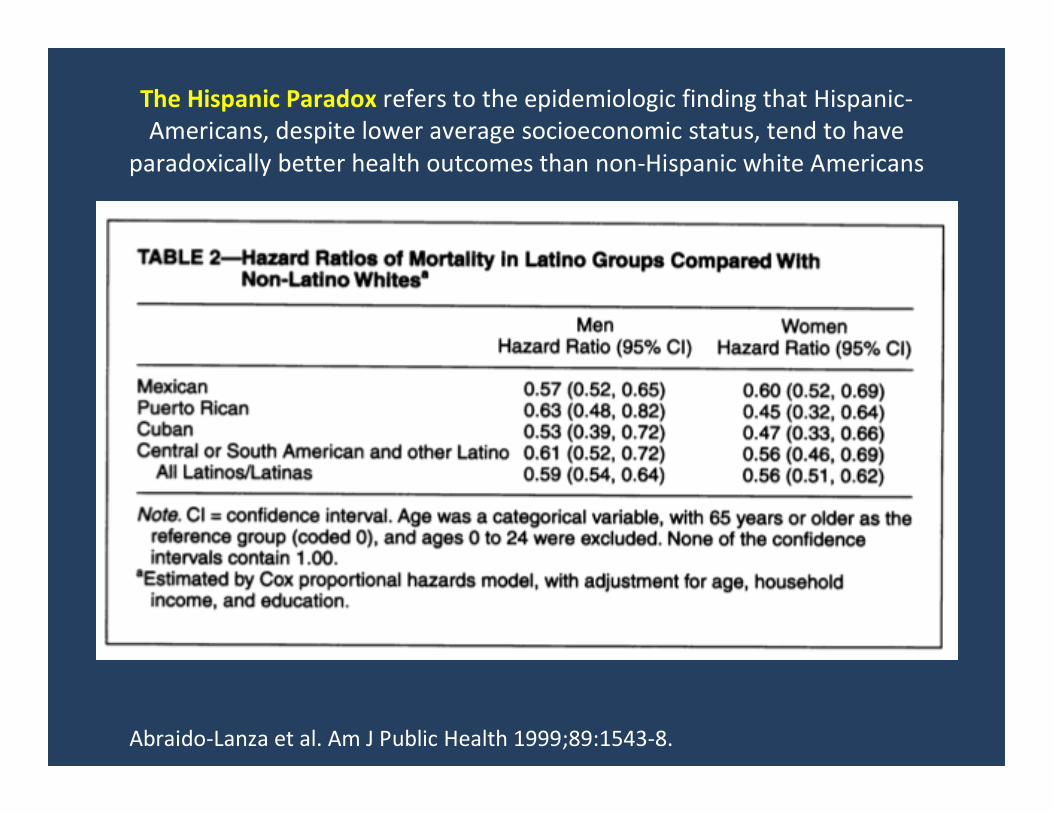
The Hispanic Paradox refers to the epidemiologic finding that Hispanic-
Americans, despite lower average socioeconomic status, tend to have
paradoxically better health outcomes than non-Hispanic white Americans
Abraido-Lanza et al. Am J Public Health 1999;89:1543-8.
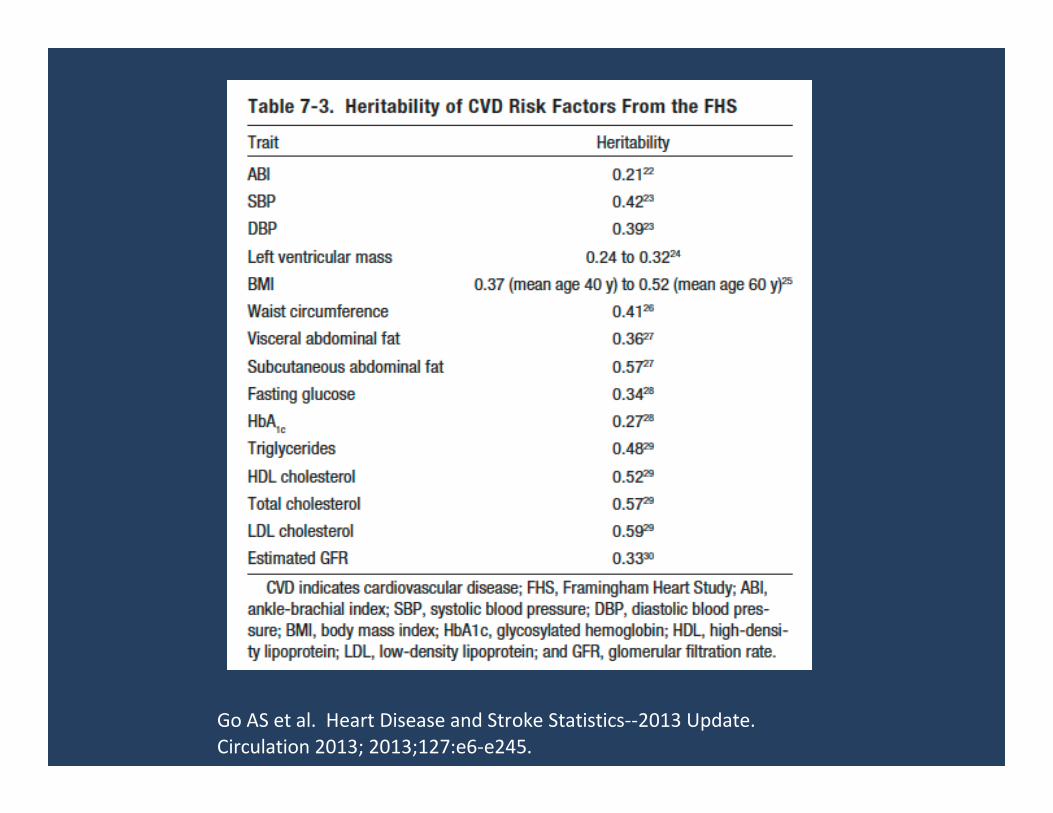
Go AS et al. Heart Disease and Stroke Statistics--2013 Update.
Circulation 2013; 2013;127:e6-e245.
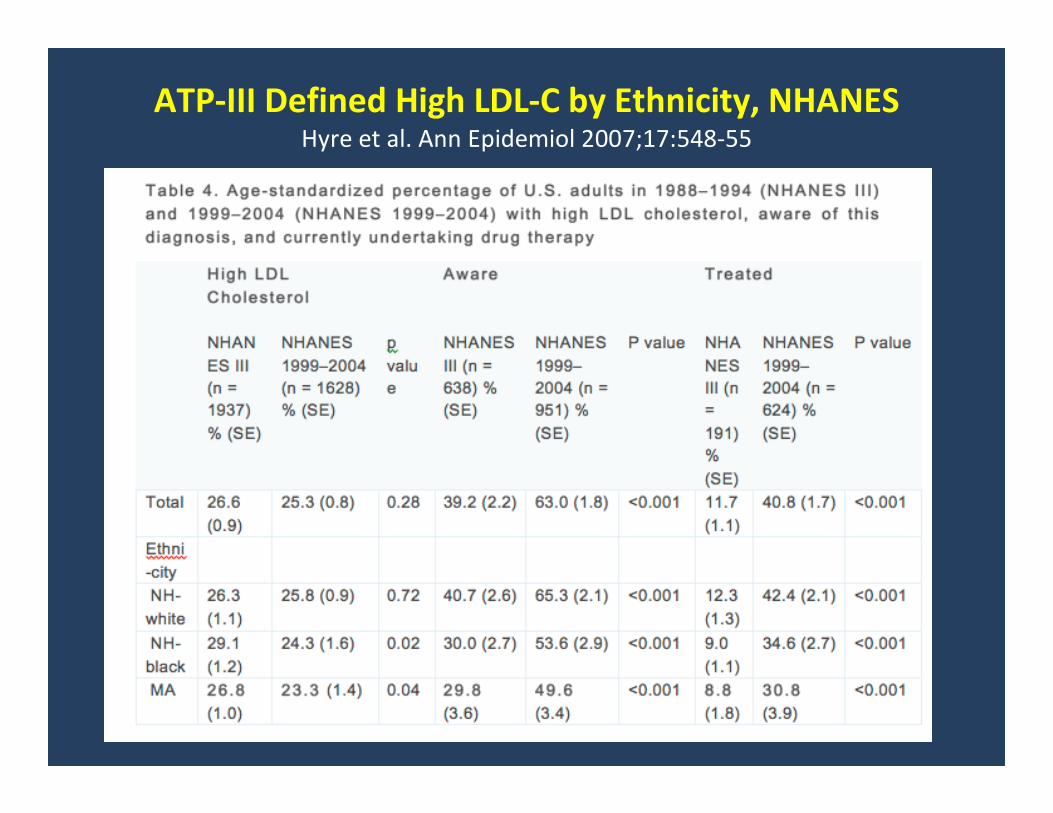
ATP-III Defined High LDL-C by Ethnicity, NHANESHyre et al. Ann Epidemiol 2007;17:548-55
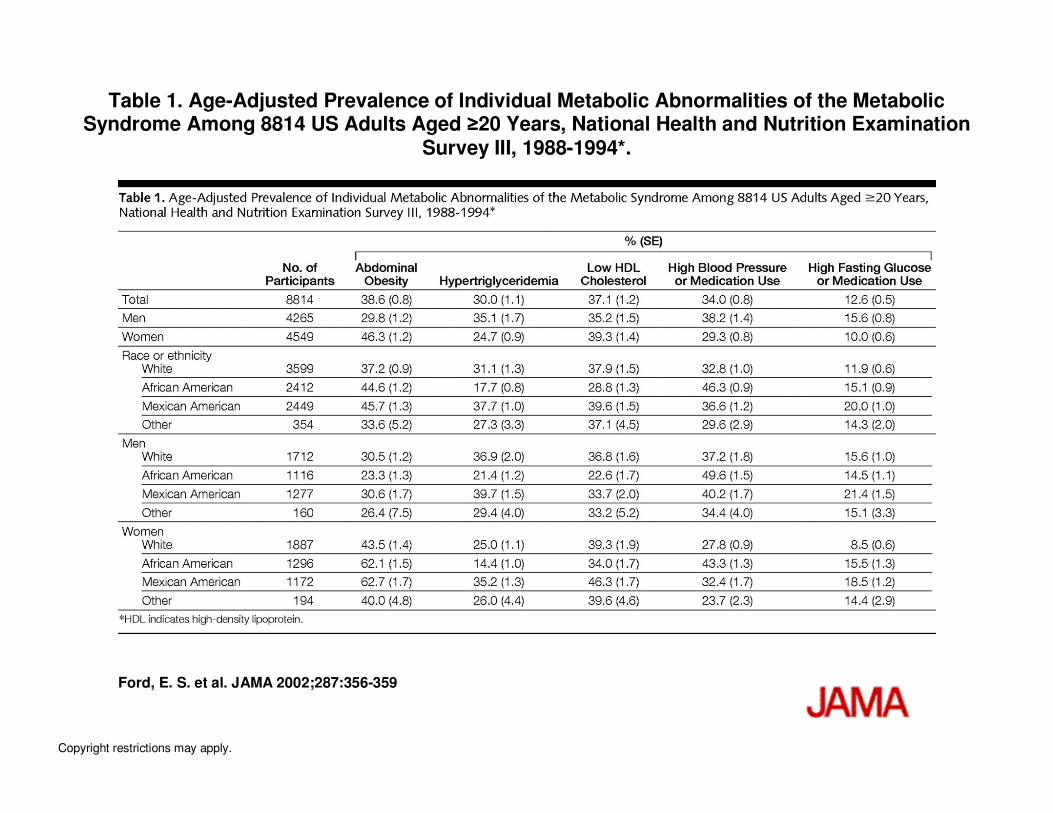
Table 1. Age-Adjusted Prevalence of Individual Metabolic Abnormalities of the Metabolic Syndrome Among 8814 US Adults Aged ≥≥≥≥20 Years, National Health and Nutrition Examination
Survey III, 1988-1994*.
Ford, E. S. et al. JAMA 2002;287:356-359
Copyright restrictions may apply.
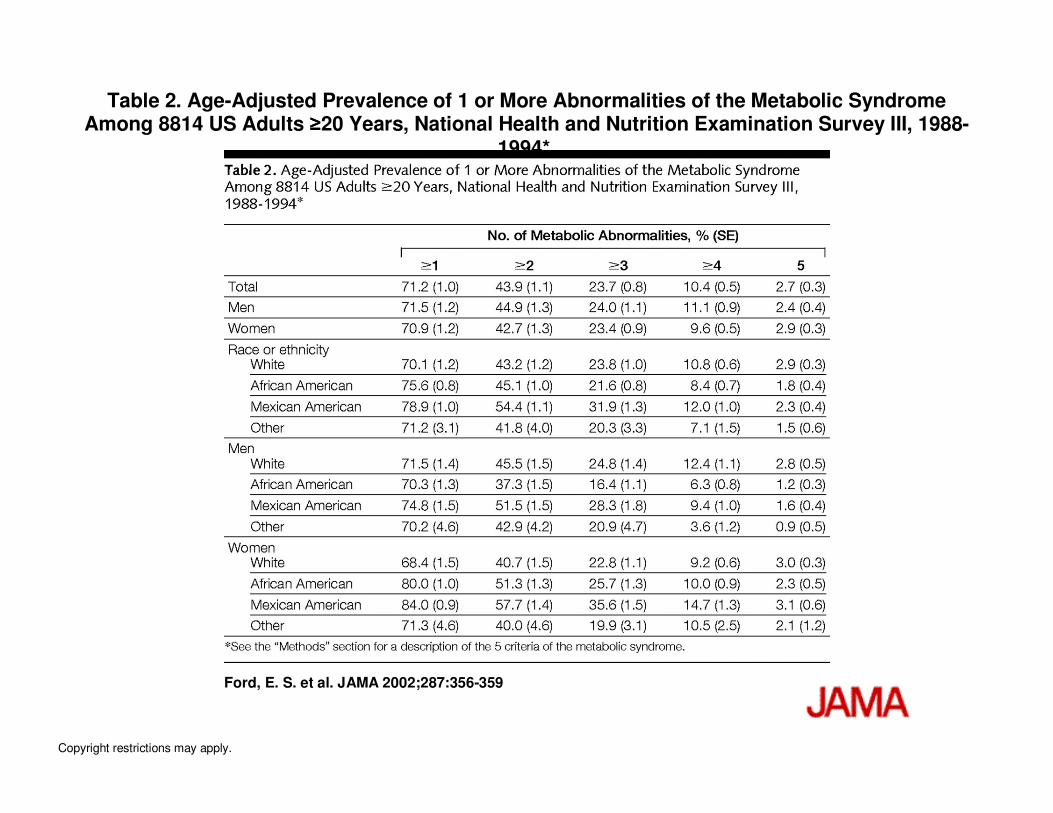
Table 2. Age-Adjusted Prevalence of 1 or More Abnormalities of the Metabolic Syndrome Among 8814 US Adults ≥≥≥≥20 Years, National Health and Nutrition Examination Survey III, 1988-
1994*.
Ford, E. S. et al. JAMA 2002;287:356-359
Copyright restrictions may apply.
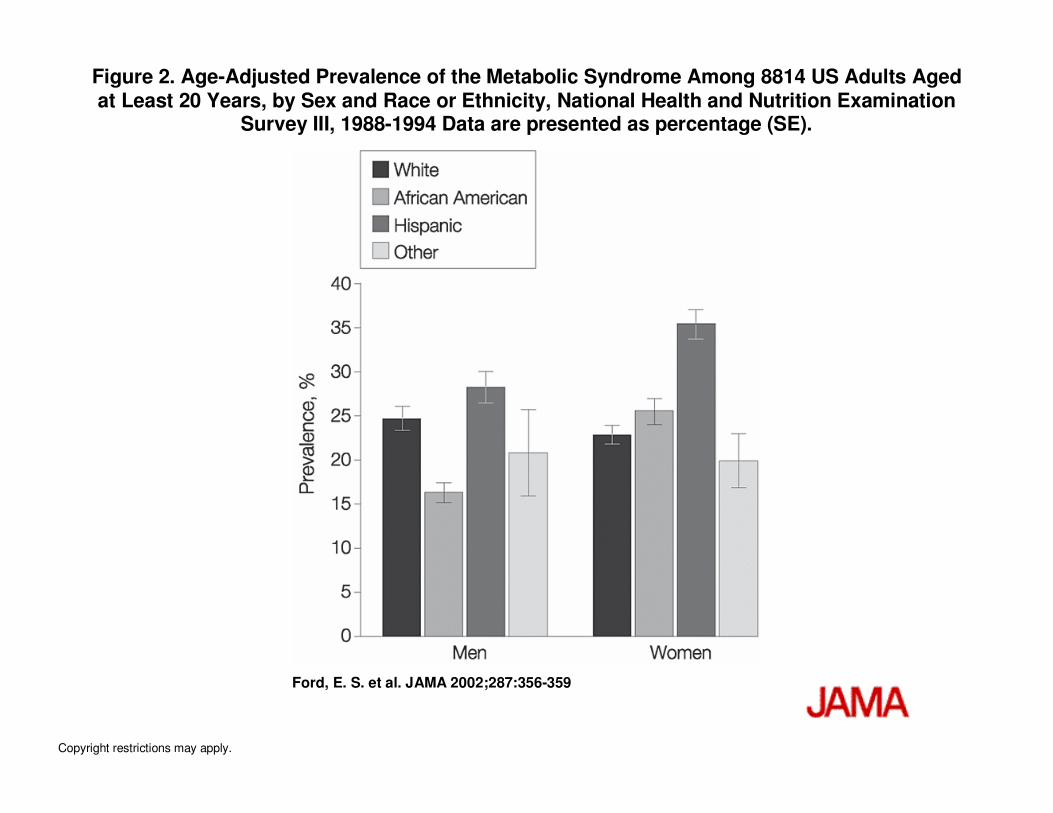
Figure 2. Age-Adjusted Prevalence of the Metabolic Syndrome Among 8814 US Adults Aged at Least 20 Years, by Sex and Race or Ethnicity, National Health and Nutrition Examination
Survey III, 1988-1994 Data are presented as percentage (SE).
Ford, E. S. et al. JAMA 2002;287:356-359
Copyright restrictions may apply.
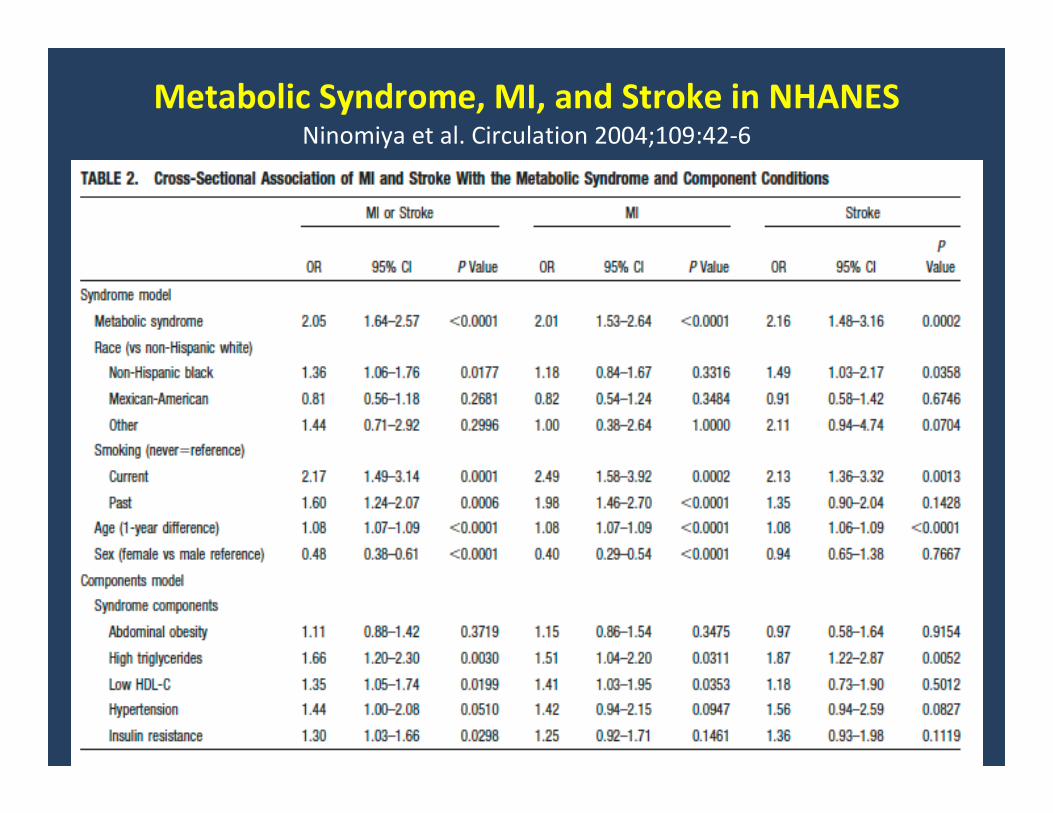
Metabolic Syndrome, MI, and Stroke in NHANES Ninomiya et al. Circulation 2004;109:42-6
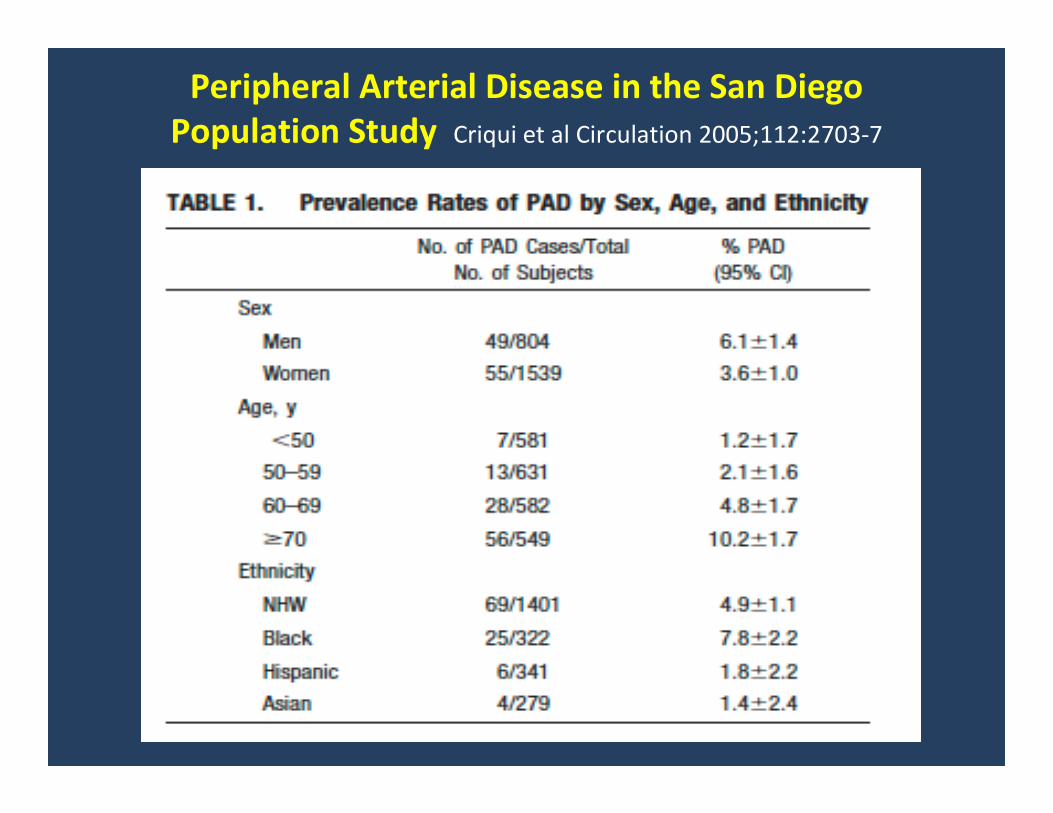
Peripheral Arterial Disease in the San Diego
Population Study Criqui et al Circulation 2005;112:2703-7
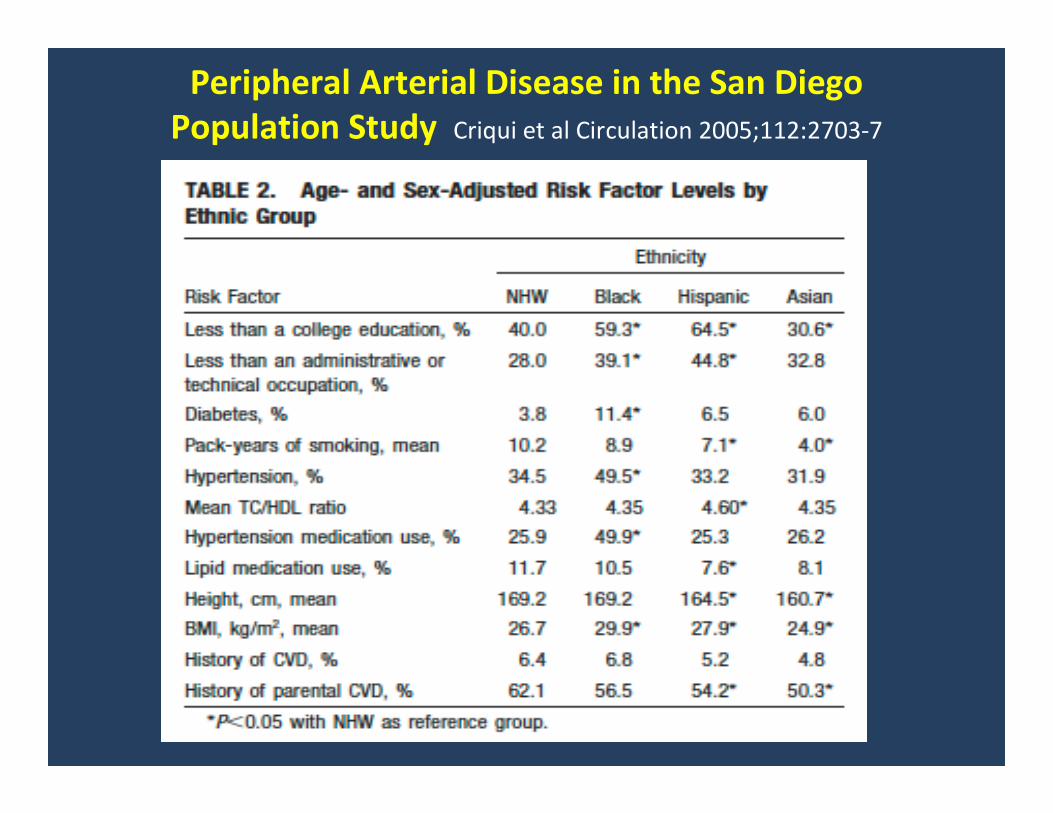
Peripheral Arterial Disease in the San Diego
Population Study Criqui et al Circulation 2005;112:2703-7
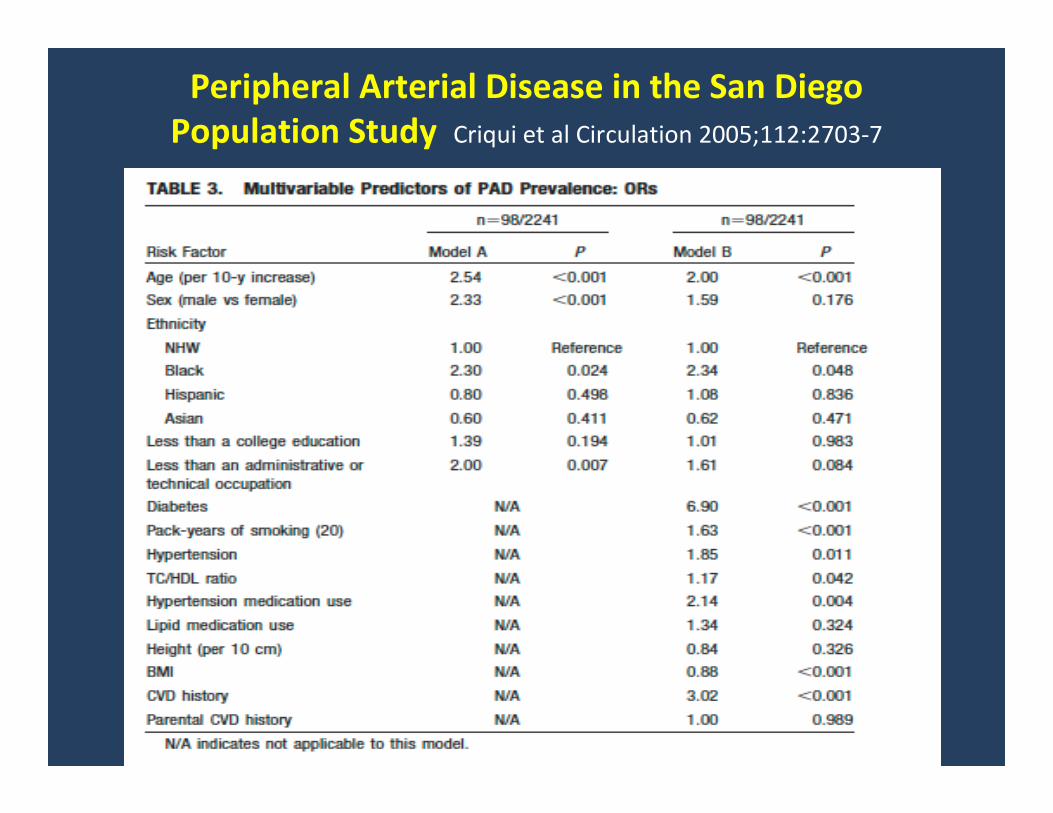
Peripheral Arterial Disease in the San Diego
Population Study Criqui et al Circulation 2005;112:2703-7
Multi-Ethnic Study of Atherosclerosis (MESA)
• 10 year prospective study, 6 Field Centers – NHW, Hispanic, Afr-Amer, Chinese men and women
aged 45-84 at baseline
• Multiple risk factors assessed, including newer
factors (eg. inflammation, infection, genetics)
• Carotid ultrasound for plaque and IMT
• Coronary calcium by CT
• Aortic calcium by CT
• Endothelial function, brachial artery
• Ankle-brachial index (ABI)
• These and other measures are being evaluated in
the MESA
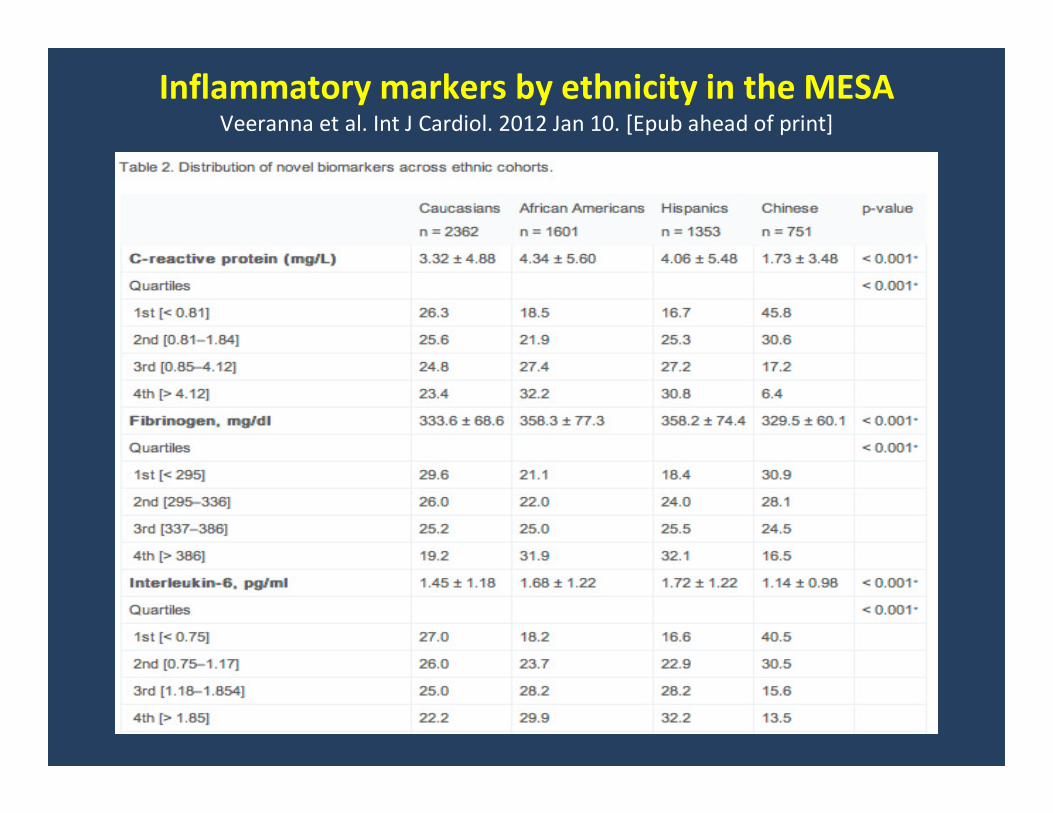
Inflammatory markers by ethnicity in the MESAVeeranna et al. Int J Cardiol. 2012 Jan 10. [Epub ahead of print]
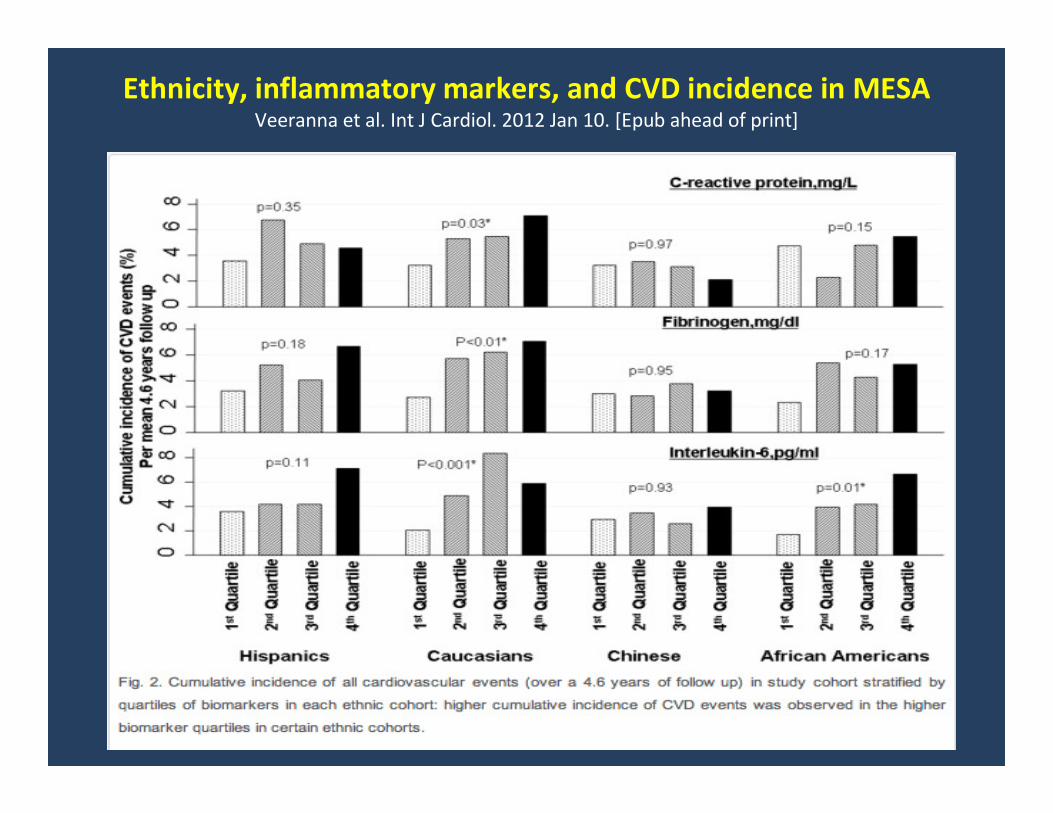
Ethnicity, inflammatory markers, and CVD incidence in MESA Veeranna et al. Int J Cardiol. 2012 Jan 10. [Epub ahead of print]
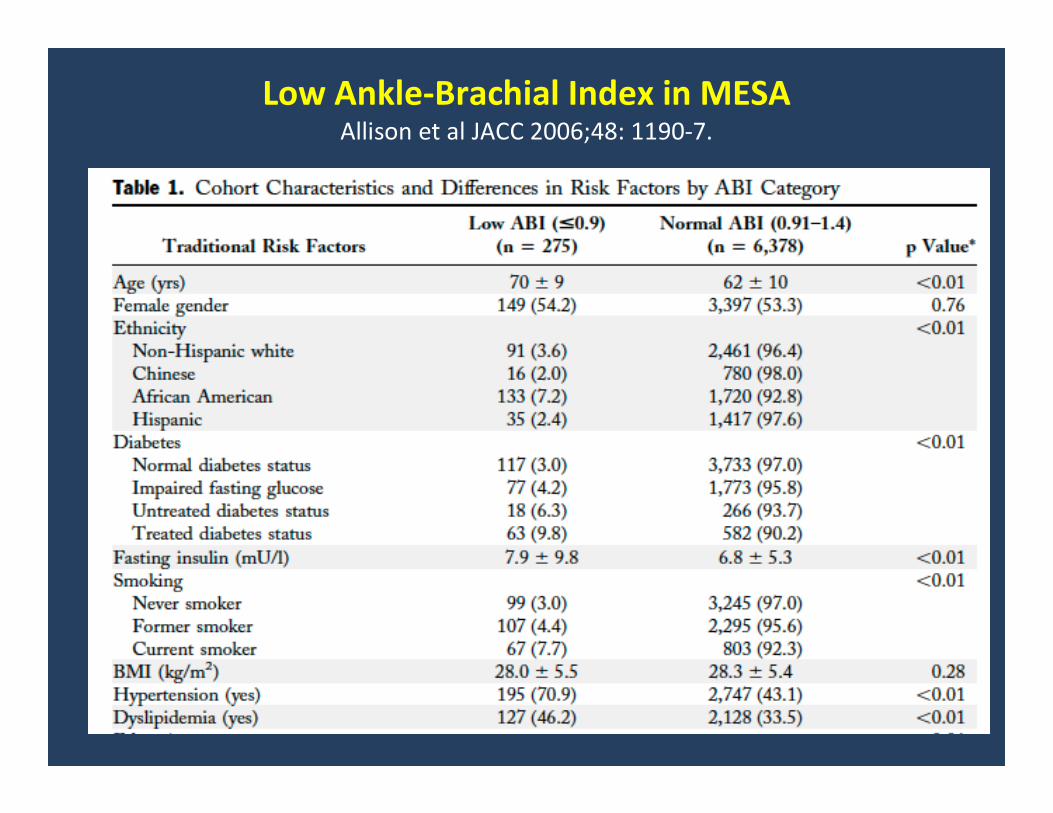
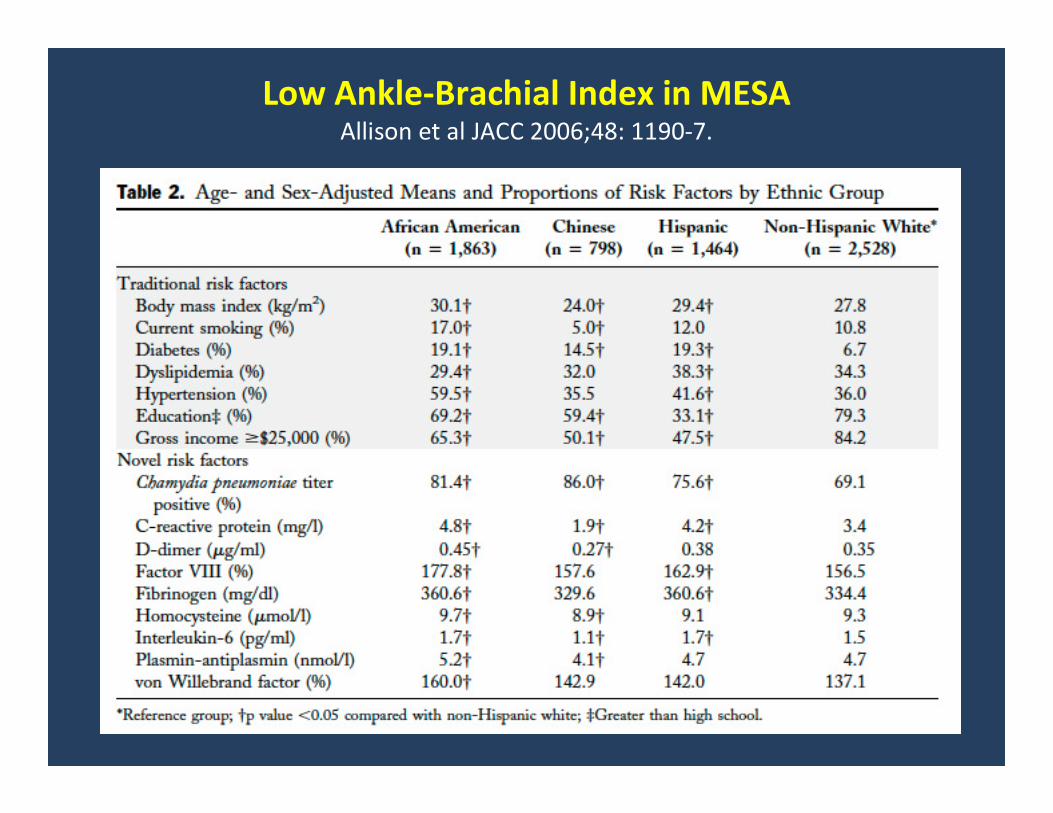
Low Ankle-Brachial Index in MESA Allison et al JACC 2006;48: 1190-7.
Low Ankle-Brachial Index in MESA Allison et al JACC 2006;48: 1190-7.
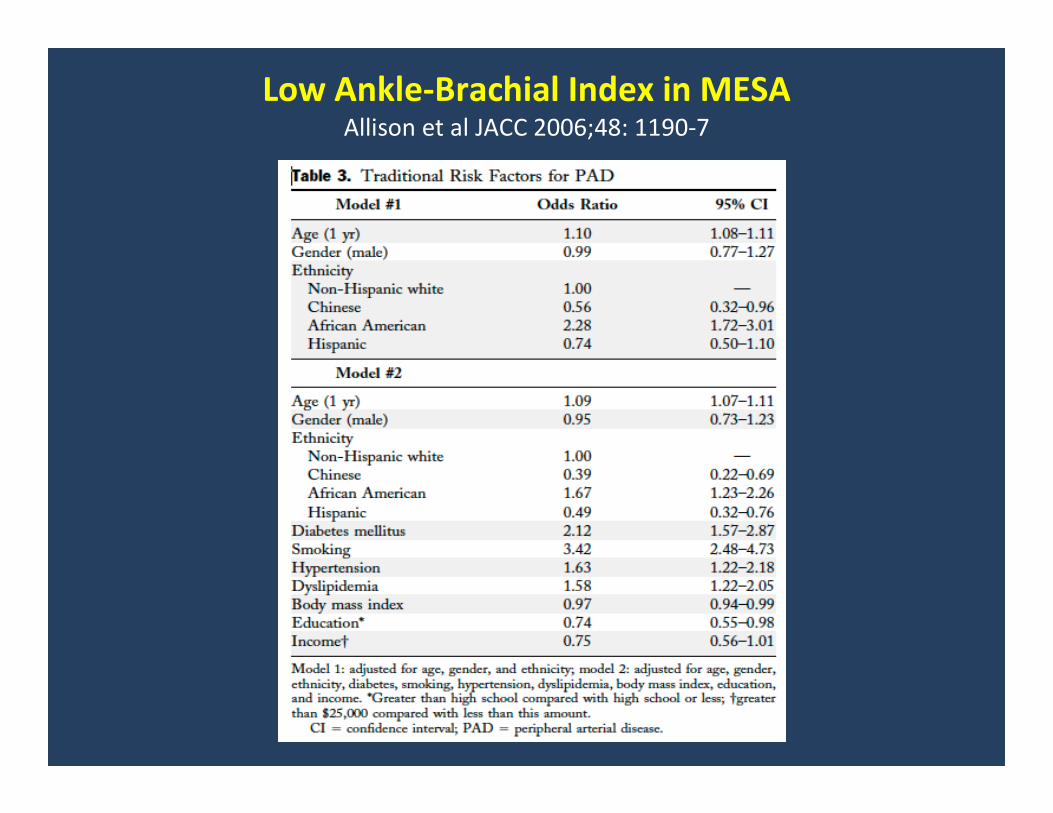
Low Ankle-Brachial Index in MESA Allison et al JACC 2006;48: 1190-7
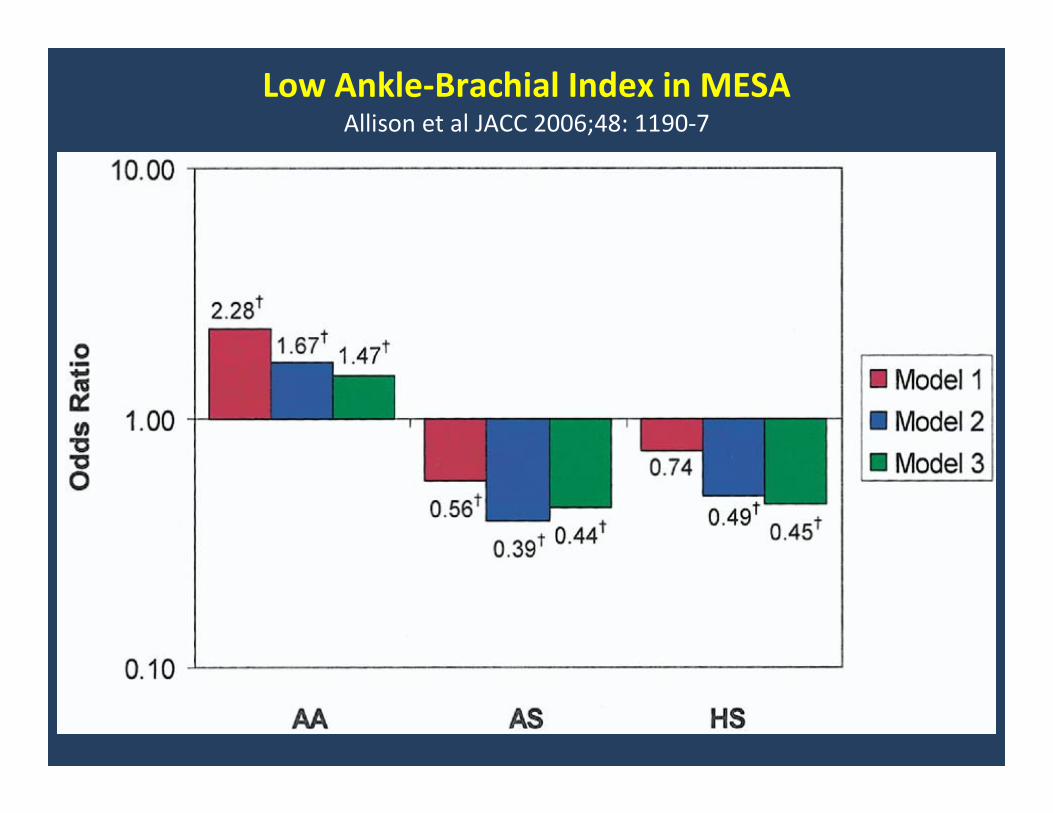
Low Ankle-Brachial Index in MESA Allison et al JACC 2006;48: 1190-7
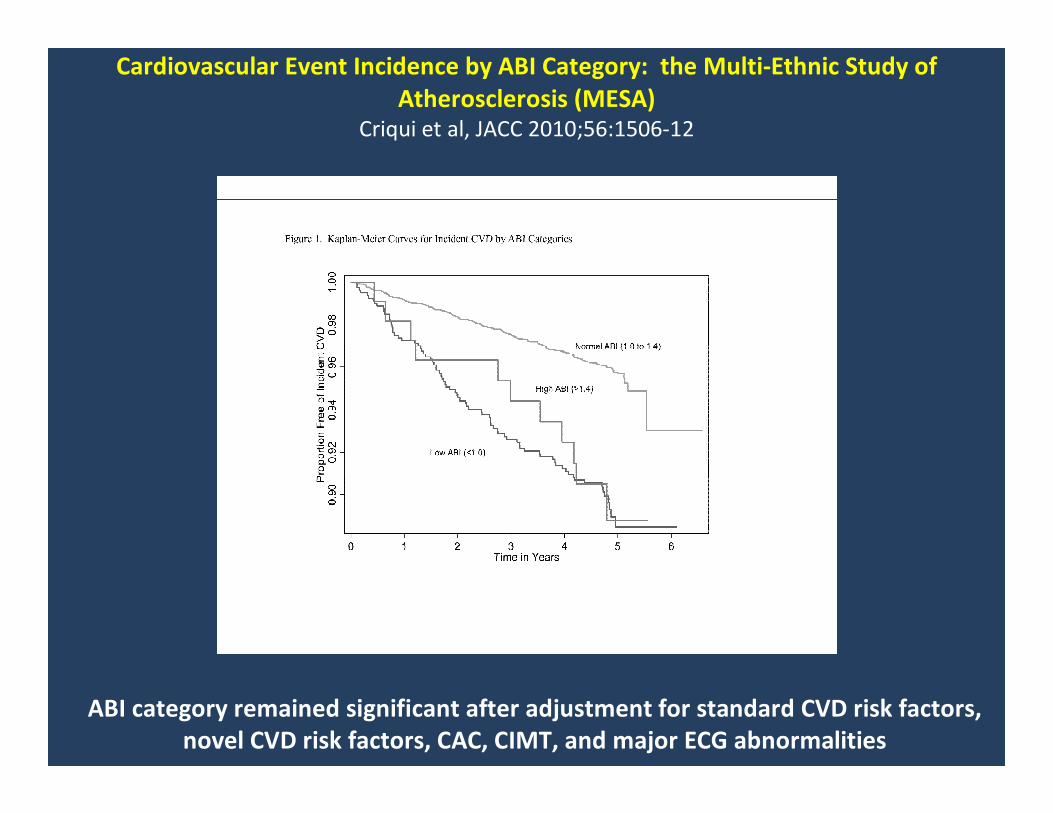
Cardiovascular Event Incidence by ABI Category: the Multi-Ethnic Study of
Atherosclerosis (MESA)Criqui et al, JACC 2010;56:1506-12
ABI category remained significant after adjustment for standard CVD risk factors,
novel CVD risk factors, CAC, CIMT, and major ECG abnormalities
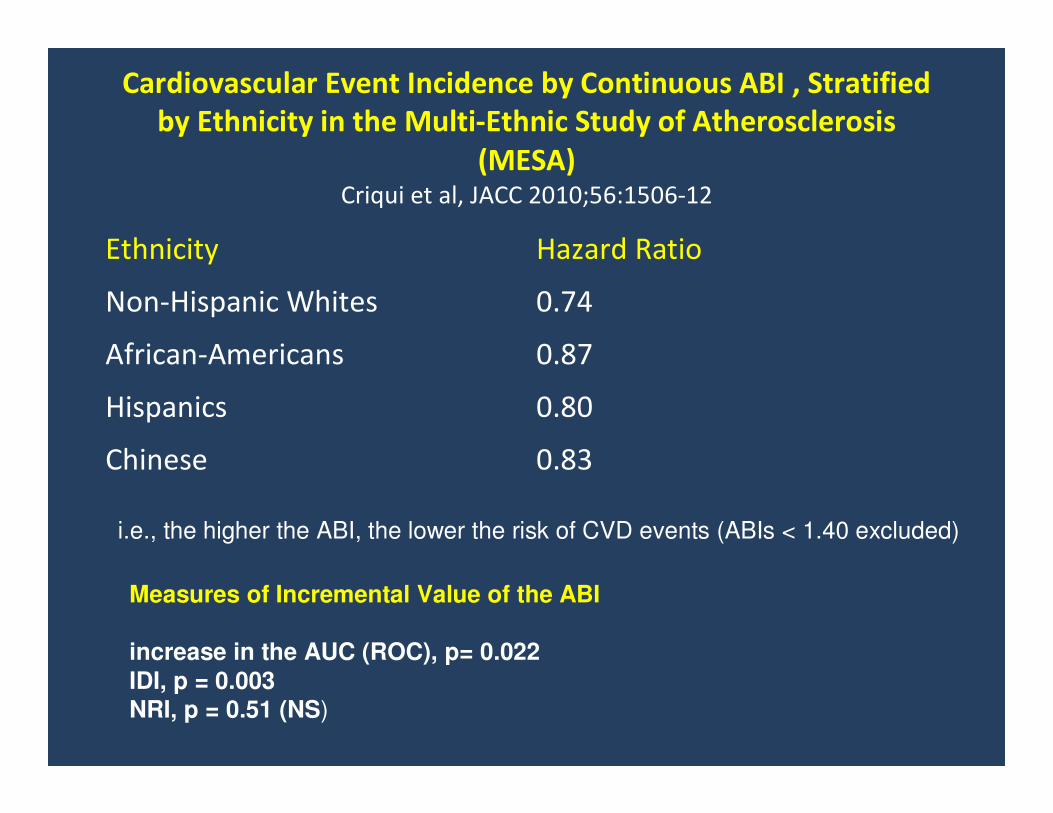
Cardiovascular Event Incidence by Continuous ABI , Stratified
by Ethnicity in the Multi-Ethnic Study of Atherosclerosis
(MESA)Criqui et al, JACC 2010;56:1506-12
Ethnicity Hazard Ratio
Non-Hispanic Whites 0.74
African-Americans 0.87
Hispanics 0.80
Chinese 0.83
i.e., the higher the ABI, the lower the risk of CVD events (ABIs < 1.40 excluded)
Measures of Incremental Value of the ABI
increase in the AUC (ROC), p= 0.022
IDI, p = 0.003NRI, p = 0.51 (NS)
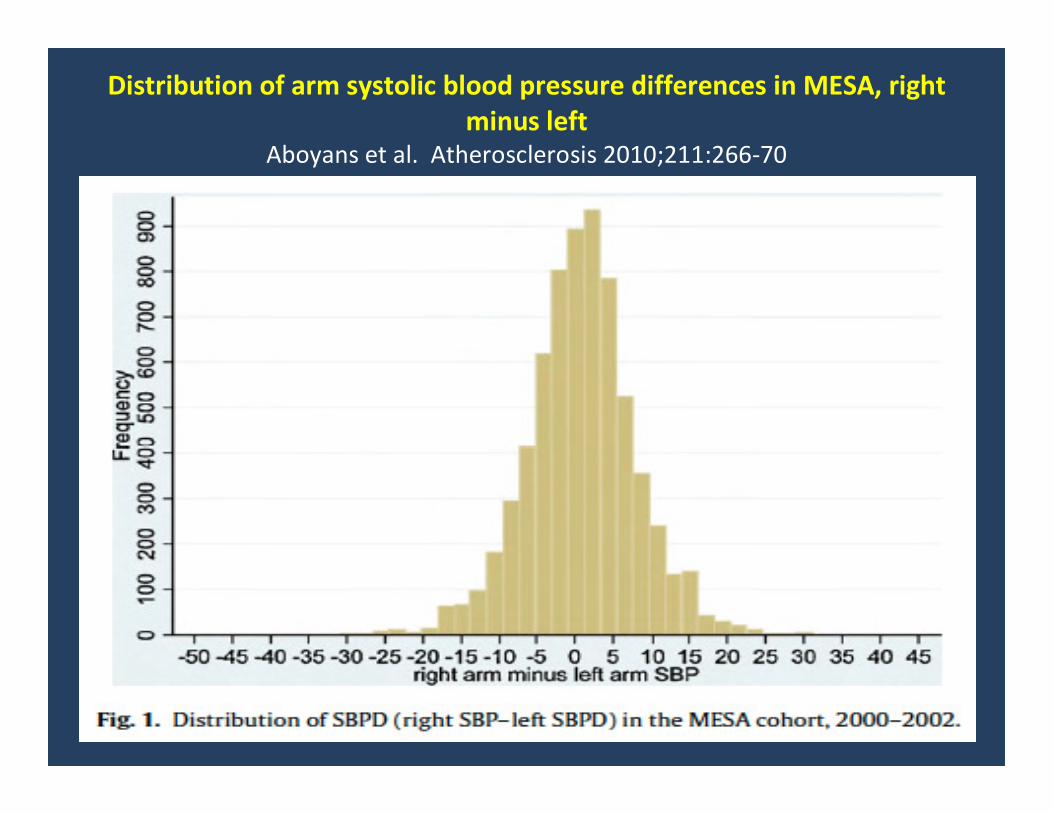
Distribution of arm systolic blood pressure differences in MESA, right
minus leftAboyans et al. Atherosclerosis 2010;211:266-70
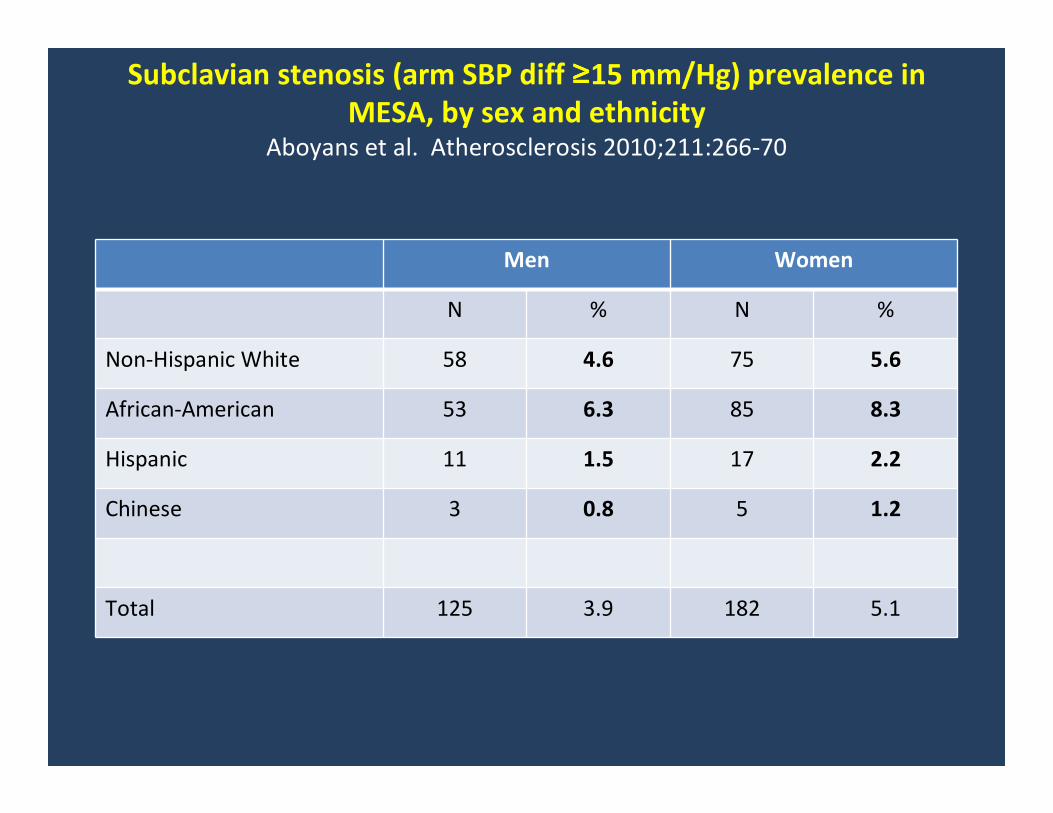
Subclavian stenosis (arm SBP diff ≥≥≥≥15 mm/Hg) prevalence in
MESA, by sex and ethnicityAboyans et al. Atherosclerosis 2010;211:266-70
Men Women
N % N %
Non-Hispanic White 58 4.6 75 5.6
African-American 53 6.3 85 8.3
Hispanic 11 1.5 17 2.2
Chinese 3 0.8 5 1.2
Total 125 3.9 182 5.1
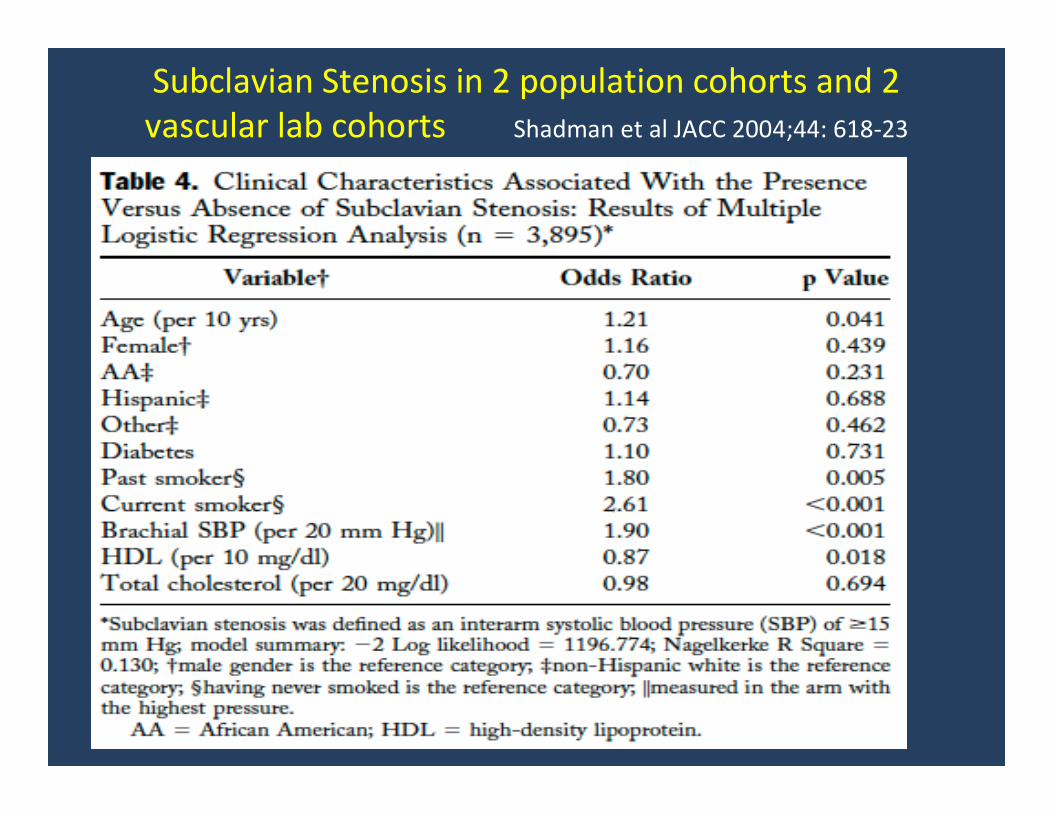
Subclavian Stenosis in 2 population cohorts and 2
vascular lab cohorts Shadman et al JACC 2004;44: 618-23
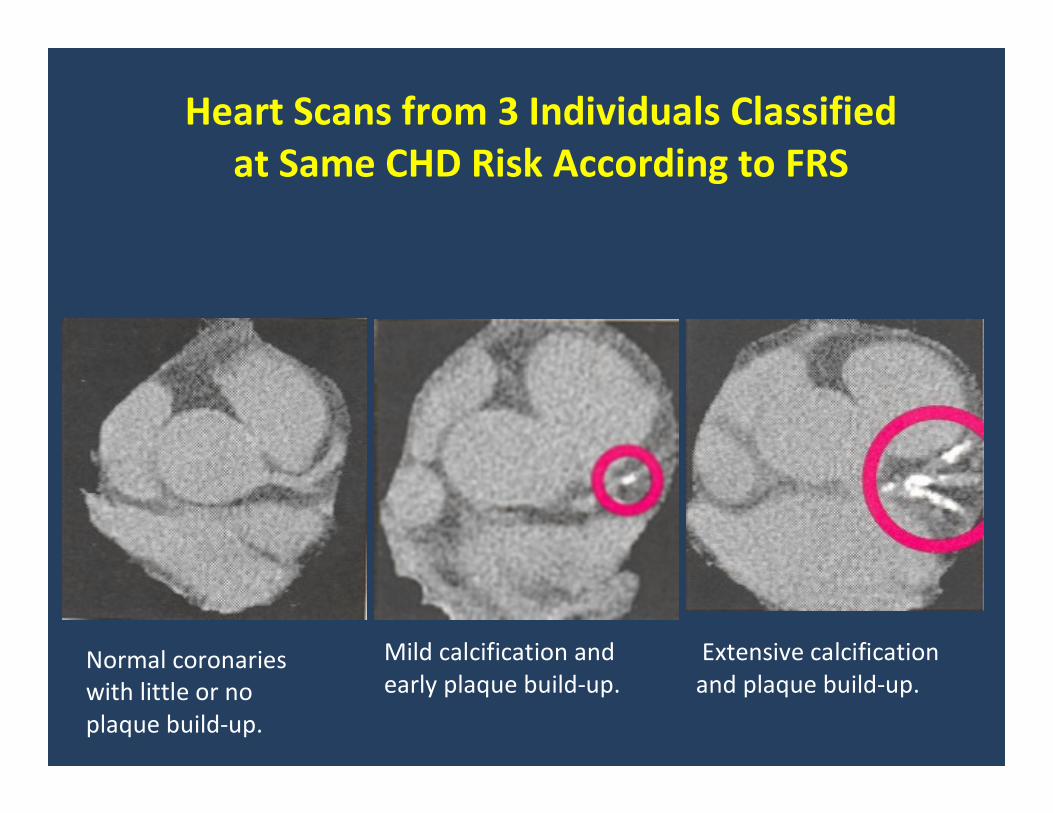
Normal coronaries
with little or no
plaque build-up.
Mild calcification and
early plaque build-up.
Extensive calcification
and plaque build-up.
Heart Scans from 3 Individuals Classified
at Same CHD Risk According to FRS
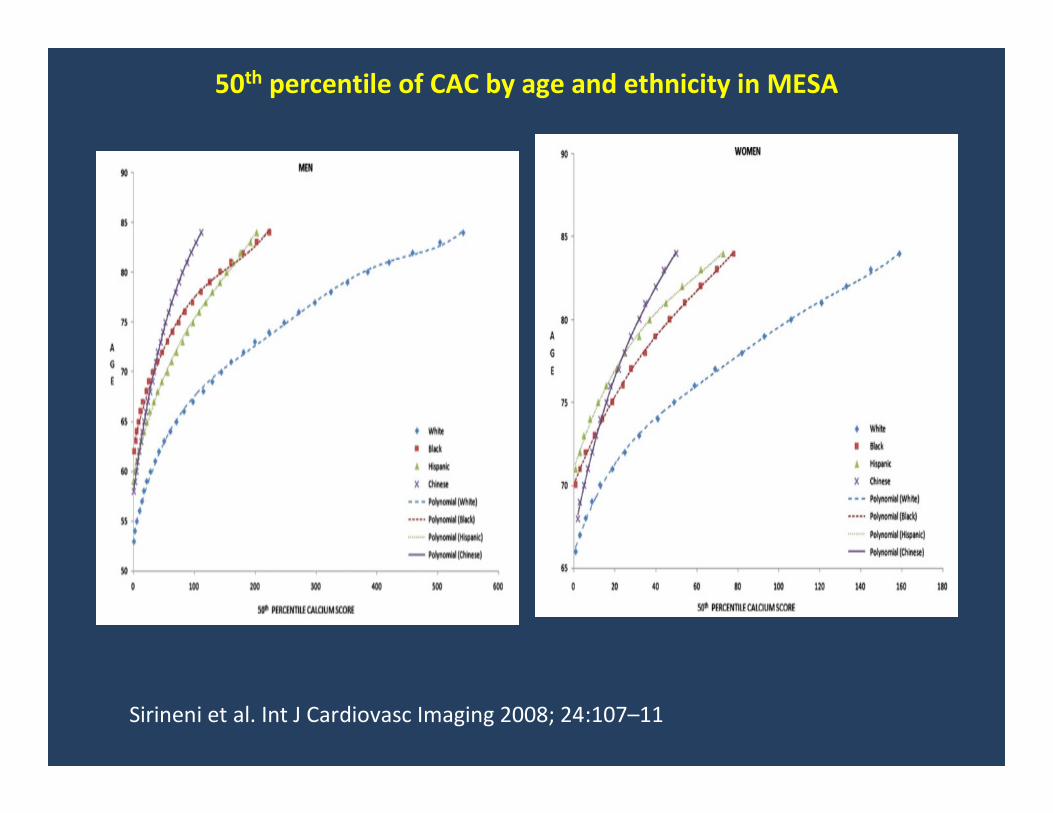
50th percentile of CAC by age and ethnicity in MESA
Sirineni et al. Int J Cardiovasc Imaging 2008; 24:107–11
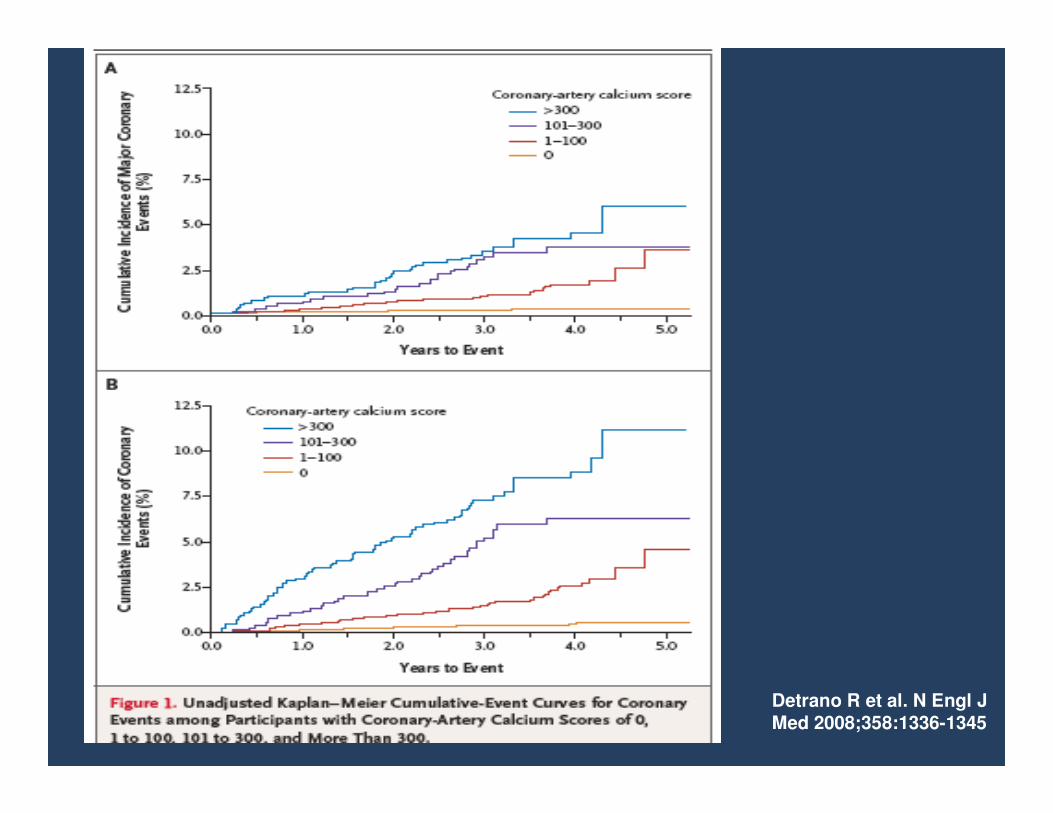
Detrano R et al. N Engl J
Med 2008;358:1336-1345
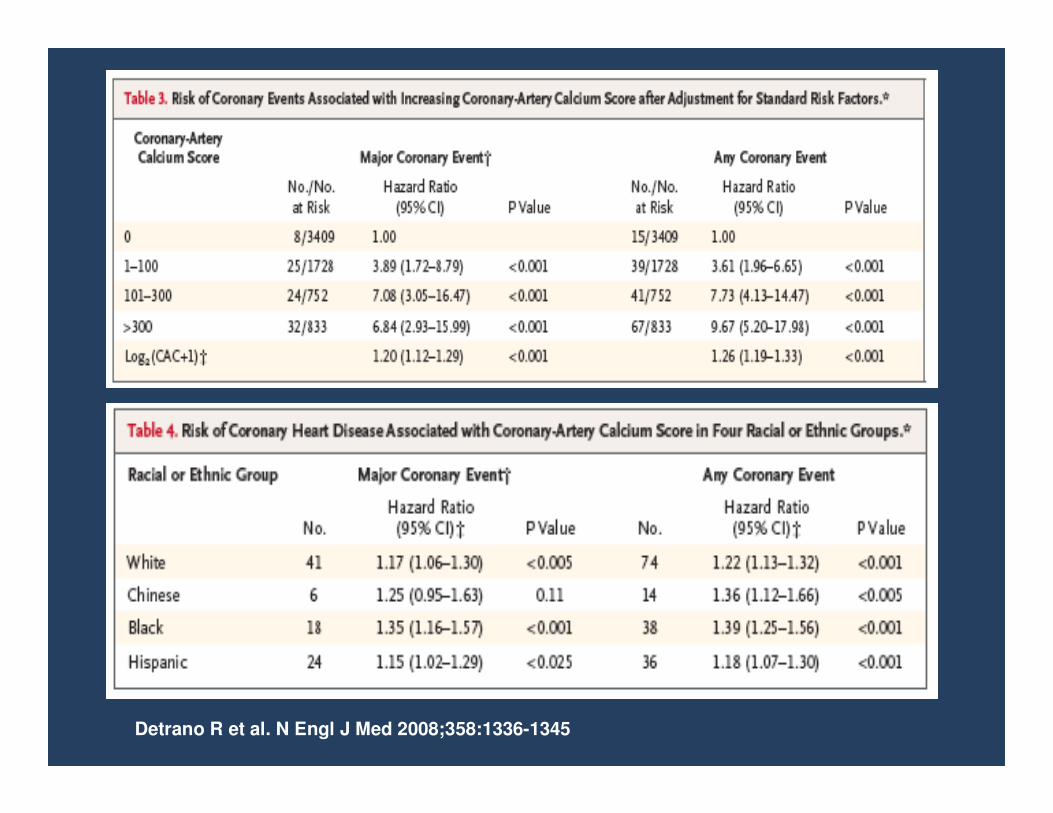
Detrano R et al. N Engl J Med 2008;358:1336-1345
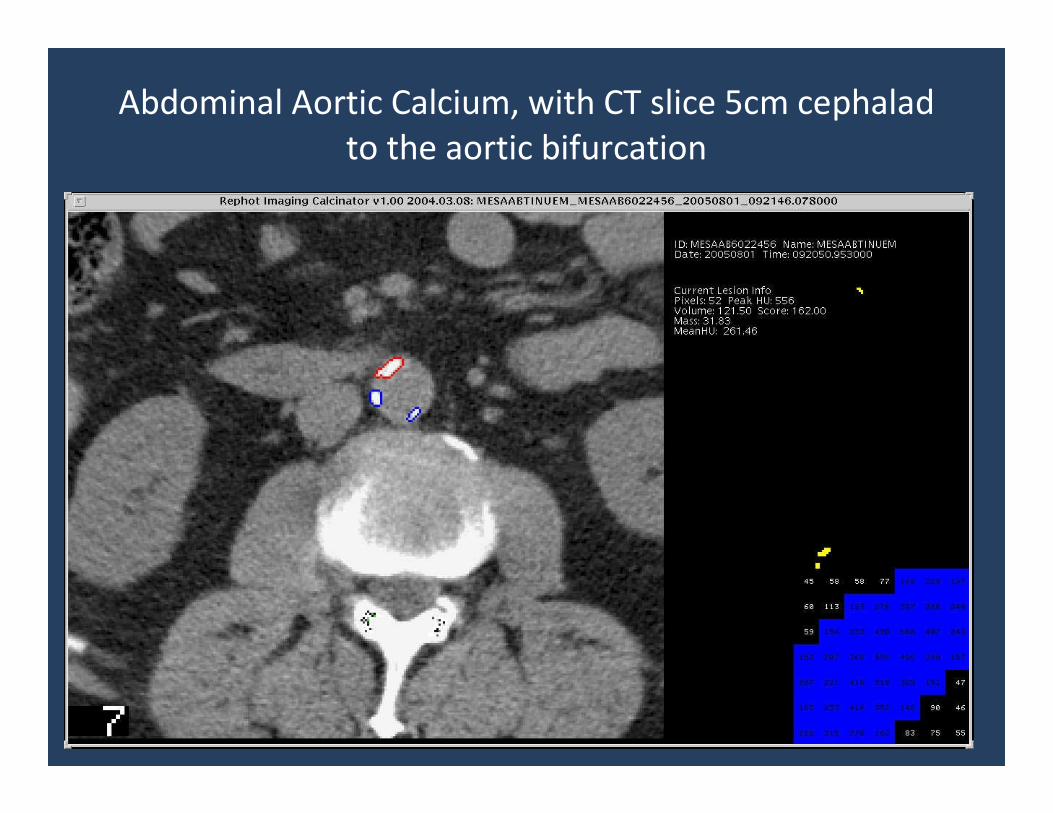
Abdominal Aortic Calcium, with CT slice 5cm cephalad
to the aortic bifurcation
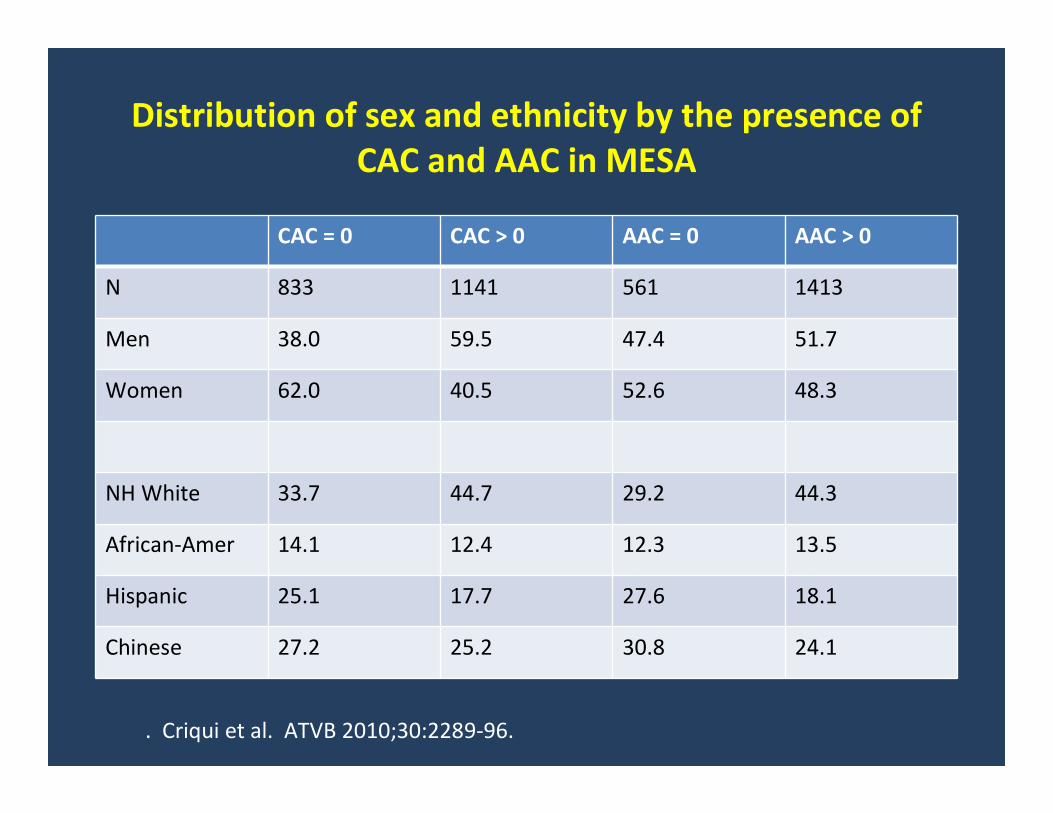
Distribution of sex and ethnicity by the presence of
CAC and AAC in MESA
CAC = 0 CAC > 0 AAC = 0 AAC > 0
N 833 1141 561 1413
Men 38.0 59.5 47.4 51.7
Women 62.0 40.5 52.6 48.3
NH White 33.7 44.7 29.2 44.3
African-Amer 14.1 12.4 12.3 13.5
Hispanic 25.1 17.7 27.6 18.1
Chinese 27.2 25.2 30.8 24.1
. Criqui et al. ATVB 2010;30:2289-96.
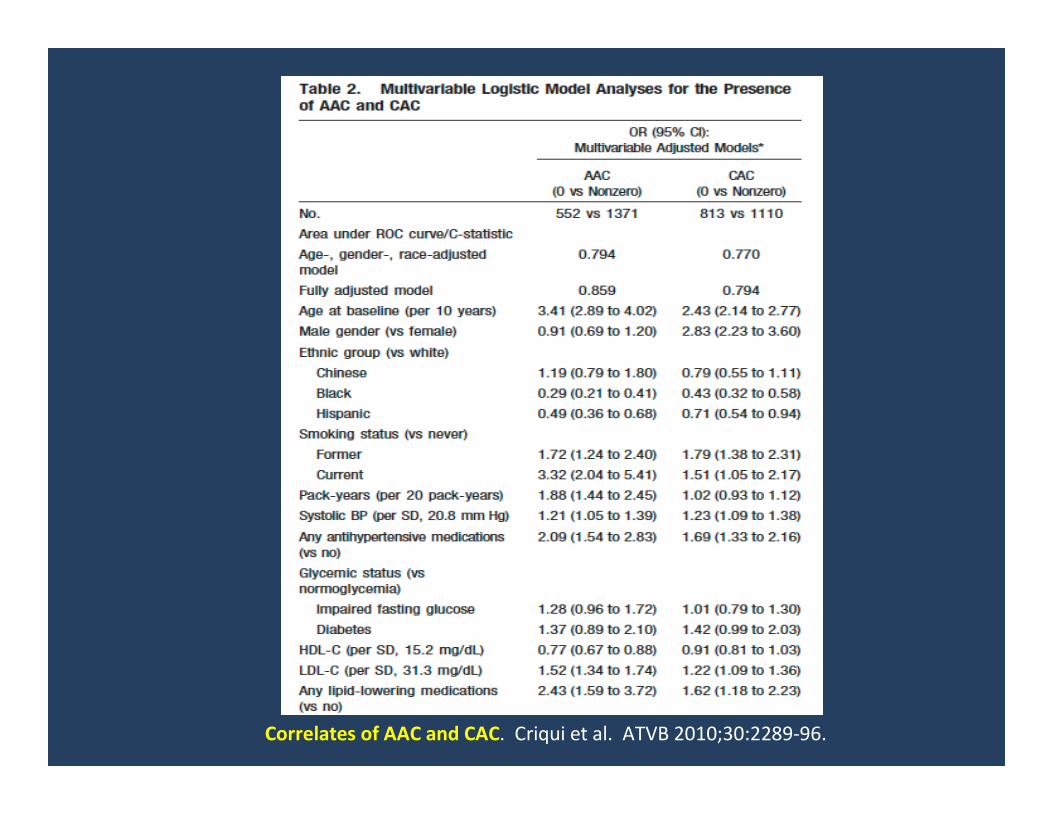
Correlates of AAC and CAC. Criqui et al. ATVB 2010;30:2289-96.
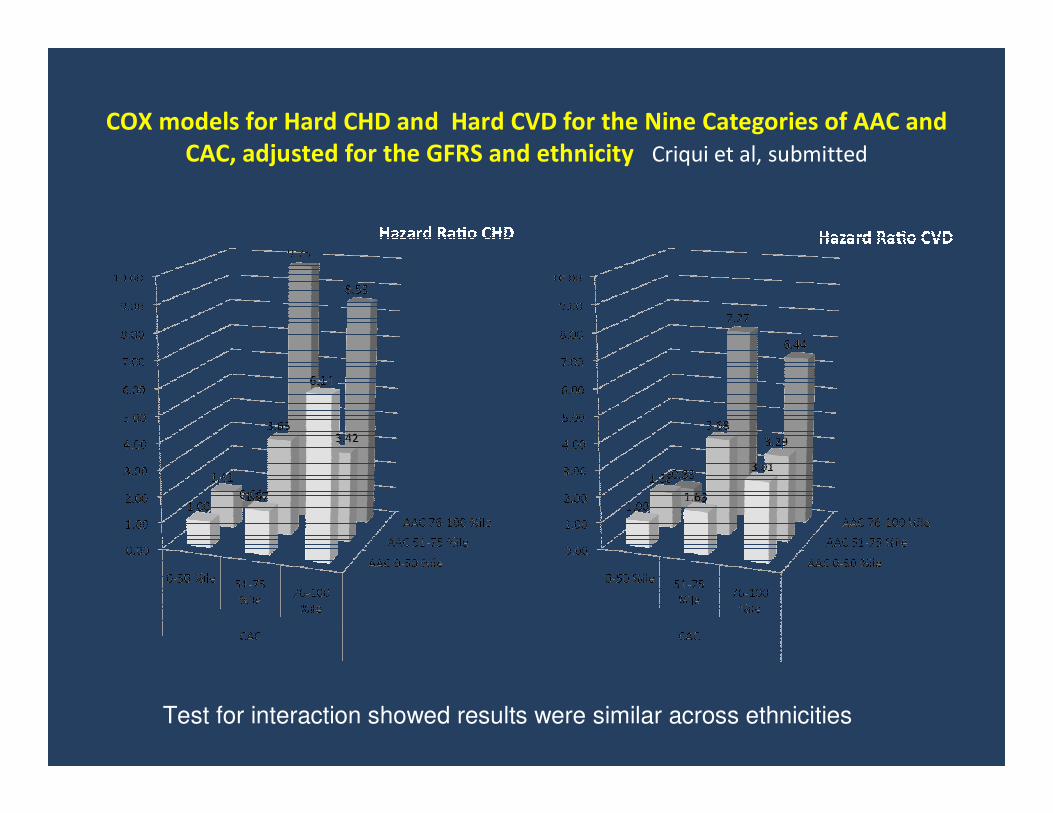
COX models for Hard CHD and Hard CVD for the Nine Categories of AAC and
CAC, adjusted for the GFRS and ethnicity Criqui et al, submitted
Test for interaction showed results were similar across ethnicities
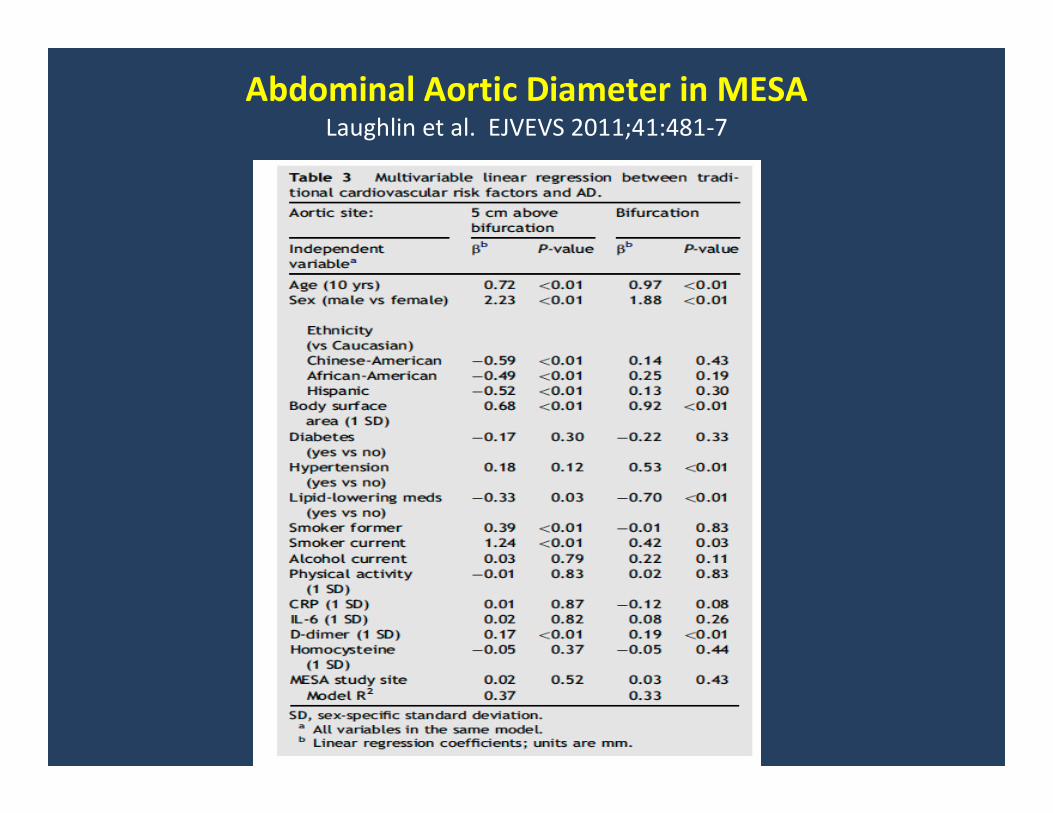
Abdominal Aortic Diameter in MESA Laughlin et al. EJVEVS 2011;41:481-7
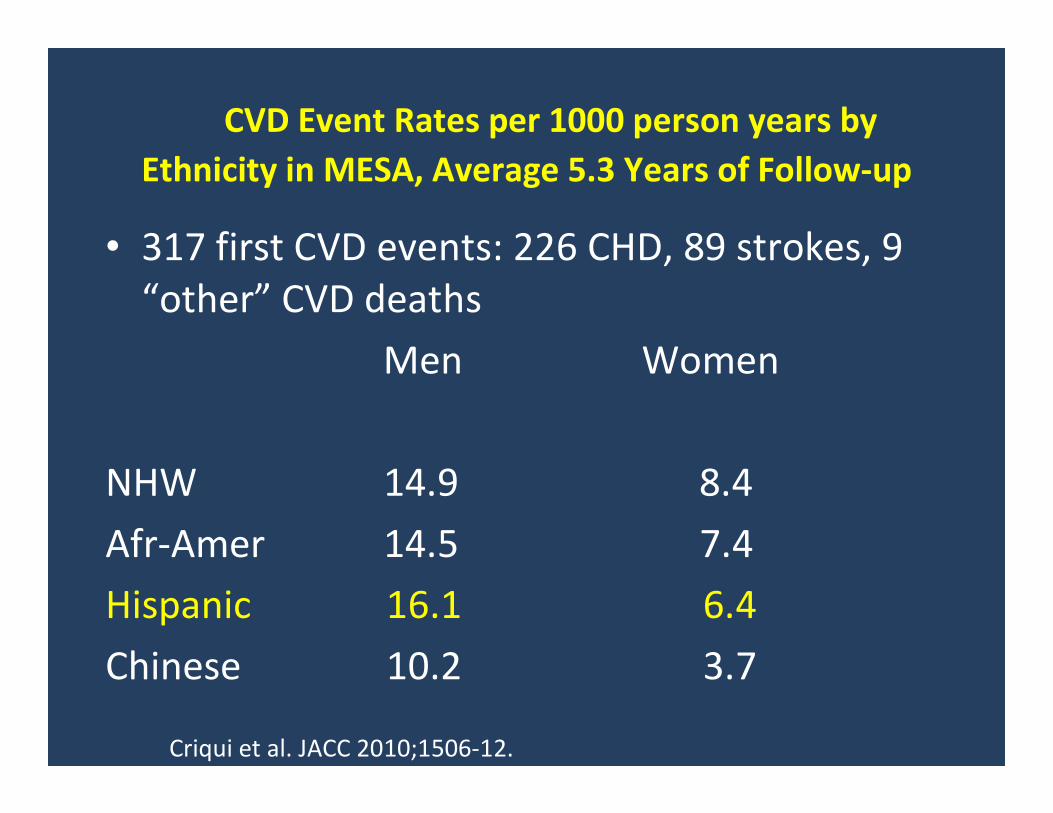
CVD Event Rates per 1000 person years by
Ethnicity in MESA, Average 5.3 Years of Follow-up
• 317 first CVD events: 226 CHD, 89 strokes, 9
“other” CVD deaths
Men Women
NHW 14.9 8.4
Afr-Amer 14.5 7.4
Hispanic 16.1 6.4
Chinese 10.2 3.7
Criqui et al. JACC 2010;1506-12.
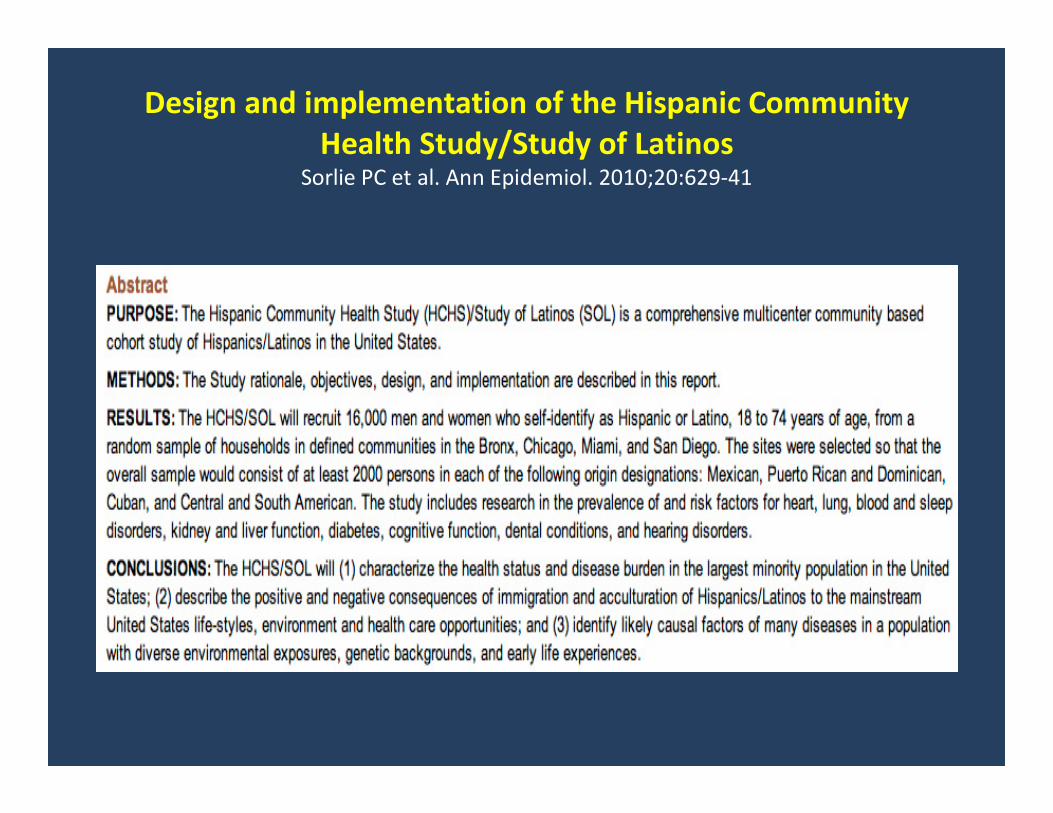
Design and implementation of the Hispanic Community
Health Study/Study of Latinos Sorlie PC et al. Ann Epidemiol. 2010;20:629-41
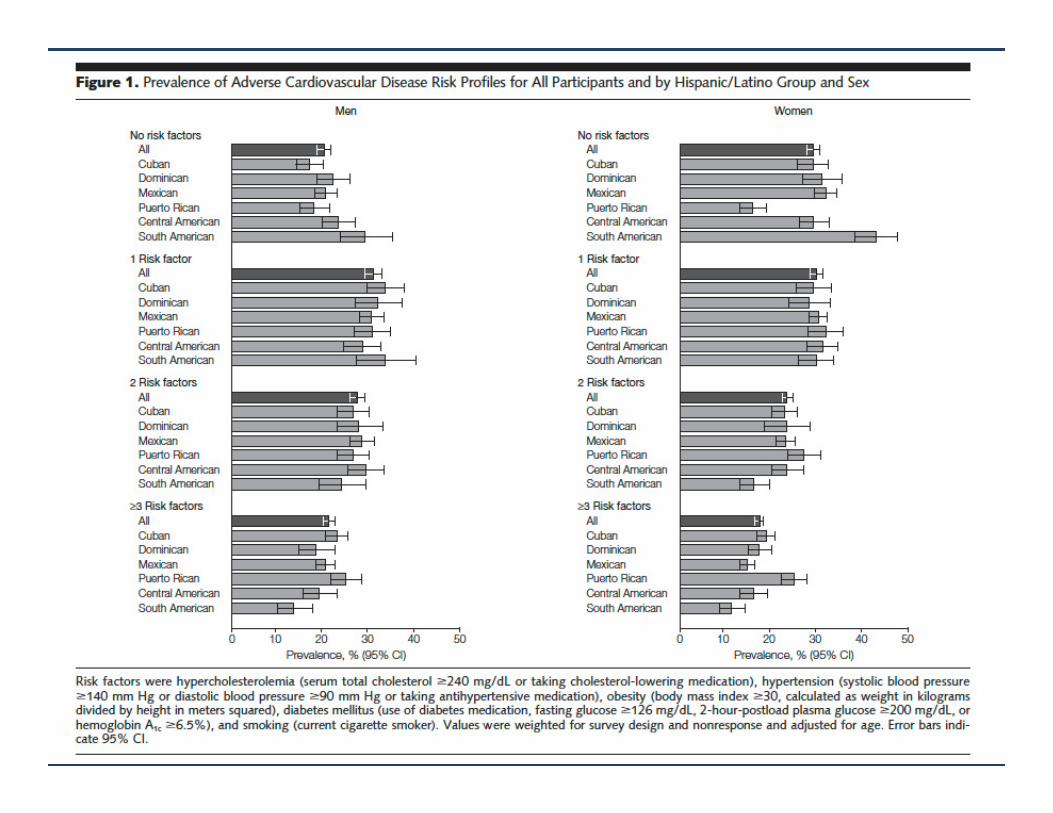
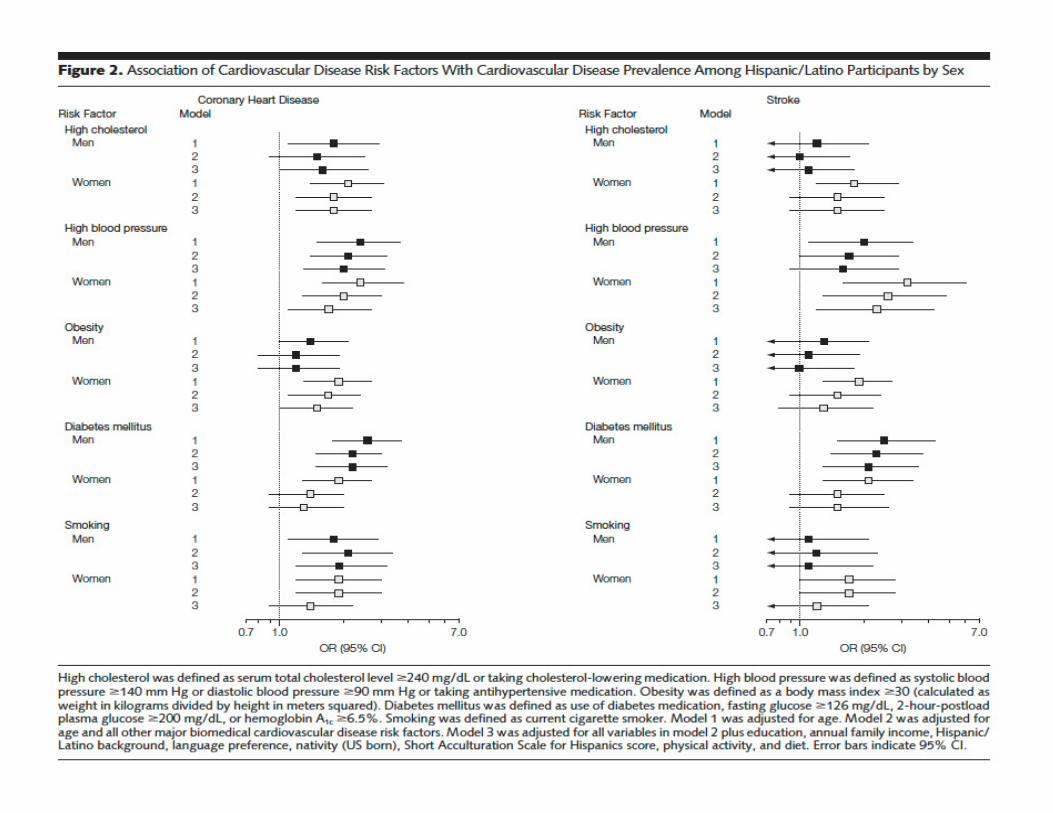
Prevalence of major cardiovascular risk factors and
cardiovascular diseases among Hispanic/Latino individuals
of diverse backgrounds in the United States
JAMA 2012;308:1775-84
Daviglus ML, Talavera GA, Avilés-Santa ML, Allison M, Cai J,
Criqui MH, Gellman M, Giachello AL, Gouskova N,
Kaplan RC, LaVange L, Penedo F, Perreira K, Pirzada A,
Schneiderman N, Wassertheil-Smoller S, Sorlie PD,
Stamler J.
Conclusions
• Compared to non-Hispanic whites, Hispanics have higher levels of obesity,
diabetes, hypertension, dyslipidemia (but not elevated LDL), and the
metabolic syndrome.
• Subclinical atherosclerosis is paradoxically less severe in Hispanics vs. non-
Hispanic whites
• Hispanics in general have paradoxically better CVD outcomes than non-
Hispanic whites
• For clinical and public health purposes, the univariate rate for CVD in
Hispanics is the relevant metric. The multivariate rate is much lower since
it adjusts away the risk associated with higher levels of risk factors in
Hispanics
• Increasing obesity in the US and differential access to health care may
narrow the gap between Hispanic and non-Hispanic white CVD outcomes