Embed Size (px)
Citation preview

Physician Revenue Cycle and Compliance – Preparing for the OIG
2014 Summer Institute Indiana Chapter, HFMA
Katie Gilfillan
Director HFP, Physician and Clinical Practice
Sandra Wolfskill, FHFMA
Director, HFP, Revenue Cycle MAP

Agenda
• A View of the Physician’s World – 2014
• OIG Reports
• Metrics for the Physician Revenue Cycle
• Q & A
2

Physician World - 2014
• Small groups vs. large groups – challenges:
– Administration and financial
– HIT infrastructure
– Ability to respond to health reform
• Options for the small groups
– Align/join larger groups
– Join a health system/ IDN
– Purchase by a hospital
• COMPLIANCE
3

Group Size - 2013
Group Size Number of Providers
Percent of Total Rank
1 203,970 22.9% 1
2 53,128 6.0% 8
3-4 65,301 7.3% 7
5-9 84,482 9.5% 4
10-24 103,569 11.6% 3
25-49 75,048 8.4% 5
50-99 69,865 7.9% 6
100-999 181,197 20.4% 2
1000+ 52,714 5.9% 9
Total 889,274
4
Source: Physician Compare database of providers registered with Medicare; includes physicians and physician extenders Leavitt Partners, LLC, Physician Groups in the United States: A Look Forward, February, 2014

Integrated Delivery Networks
5
Large Groups: > 25 physicians Affiliation with Integrated Delivery Network
59%
Small Groups: 25 or < physicians Affiliation with Integrated Delivery Network
23%
Implications for: ACOs
Bundled payments Medical homes
VBP Demonstrations

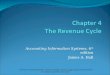
Conceptual View of the Patient-Centered Revenue Cycle
6
Physician or patient identifies need for service; contacts “office” to schedule
Time of service activities- Patient arrival ; $$; Clinical services and documentation; Revenue capture, Coding & Patient discharge
m
Post service – completion of activities required to successfully resolve the financial components for patient and provider
EHR
Visit scheduled and pre-service processing completed

Pre-Service Revenue Cycle
• Need for service identified; patient contacts provider to schedule visit
– Potential compliance issue(s): ____________________________________________________________________________________
• Visit scheduled
– Potential compliance issue(s): ____________________________________________________________________________________
7

Pre-Service Revenue Cycle
• Identification of current and prior balances
– Potential compliance issue(s): ____________________________________________________________________________________
• Discussion and resolution of financial issue(s)
– Potential compliance issue(s): ____________________________________________________________________________________
8

Pre-Service Revenue Cycle
• Collection of payment
– Potential compliance issue(s): ____________________________________________________________________________________
• Automated reminder call(s)
– Potential compliance issue(s): ____________________________________________________________________________________
9

Time of Service Revenue Cycle
• Patient arrival, check-in; collection of co-payment or other balance(s)
– Potential compliance issue(s): ____________________________________________________________________________________
• Clinical documentation
– Potential compliance issue(s): ____________________________________________________________________________________
10

Time of Service Revenue Cycle
• Coding
– Potential compliance issue(s): ____________________________________________________________________________________
• Charging
– Potential compliance issue(s): ____________________________________________________________________________________
11

Time of Service Revenue Cycle
• Additional services/testing ordered
– Potential compliance issue(s): ____________________________________________________________________________________
• Cash posted and bank deposit sent to bank
– Potential compliance issue(s): ____________________________________________________________________________________
12

Post Service Revenue Cycle
• Patient balance billed
– Potential compliance issue(s): ____________________________________________________________________________________
• Unpaid accounts sent to collection agency for processing
– Potential compliance issue(s): ____________________________________________________________________________________
13

OIG - (OMG)
14

15
The OIG alleged that SRMC submitted claims containing CPT codes 99204, 99205, 99214, and 99215, that it submitted for services provided by the physician that were upcoded and that the physician engaged in a pattern or practice of coding at a higher level that he knew or should have known would result in a greater payment than the code applicable to the services he was actually providing.
Physician pays $17,087.58 for allegedly violating the Civil Monetary Penalties Law. The OIG alleged improper billing of Medicare for: (1) new patient E&M office visits for pre-existing patients; (2) upcoded E&M office visits; and (3) services provided by nurse practitioners that were billed under physicians provider number when he was not in the office.
CHICAGO—Mobile Doctors…arrested today on federal health care fraud charges…warrants to seize up to $2.568 million in alleged fraud proceeds from various bank accounts. The charges allege a scheme of fraudulent upcoding.

Office of the Inspector General Report
• Review of Medicare Part B claims for E/M services
• Found $6.7 billion on improper payments in 2010
• Represents 21.4 % of all E/M payments
16

Previous Report:
• 2006: OIG reports 75% of E/M consultations did not meet Medicare coverage requirements leading to $1.1 B in improper Medicare payments.
17 17

Previous report: OIG reports increased billing of higher level E/M codes
18

Previous Reports
• 2012 Survey: 57% of physicians who provide E/M Services used an EHR system
– 75% use EHR system to document E/M services
– 88% of Medicare physicians assign codes manually
– 12% have codes assigned by staff or professional coders
19

Current Report: Methodology
• Requested medical records from a sample of physicians from each strata.
• Reviewers determined whether the E/M service documented in the medical record for each sampled claim was correctly coded/sufficiently documented.
20
High Coding Physicians
• Top 1 %
• Two highest codes
Other Physicians
• Not high coding

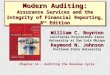
Findings
• 42 % of claims were incorrectly coded
• 19 % of claims lacked documentation
21
0 10 20 30 40 50
Upcoded
Downcoded
Other
0 20 40
Insufficient Documenation
Undocumented

High coding physicians more likely to incorrectly code
0
10
20
30
40
50
60
70
-4 -3 -2 -1 1 2 3 4
High Coding Physicians
Other Physicians
22

Recommendations from Report and CMS response
• Educate physicians on coding and documentation requirements for E/M services.
• Continue to encourage contractors to review E/M services billed for by high-coding physicians.
• Follow up on claims for E/M services that were paid for in error.
23

Other Areas of Focus • Upcoming Report: Documentation
vulnerabilities of E/M services using EHR systems.
• Outpatient E/M services billed at the “new” patient rate
• Place of Service Coding Errors
• Ophthalmologists and Anesthesiologists
• Diagnostic Radiology and Electrodiagnostic Testing
• Schedule II controlled substance prescribing
• Meaningful Use Audits by CMS
24

Strategies for Physician Offices
• Develop and Implement a Compliance Program
– Now required under PPACA
– Include 7 Steps recommended by OIG
25

1. Conducting internal monitoring and auditing through periodic audits.
2. Implementing compliance and practice standards through the development of written standards and procedures.
3. Designating a Compliance Officer or contact(s)
4. Conducting appropriate training and education on practice standards and procedures.
7 Steps to OIG Compliance Plan
26

5. Responding to detected violations through investigations of allegations
6. Developing open lines of communication among staff regarding fraudulent conduct
7. Enforcing disciplinary standards through publicized guidelines
7 Steps to OIG Compliance Plan
27

Strategies for Physician Offices
• E/M audits should be part of your overall compliance program
• Consult Evaluation and Management Services Guide
• Consult OIG and CMS Resources for Physicians
28

Metrics – Physician Revenue Cycle
29

Physician Practice KPIs
• Common metrics that provide strategic-level month over month data
• Ability to select and report on a variety of peer comparisons
• Developed by HFMA and industry experts
• Monitored and updated to meet emerging needs
30

Benefits of Benchmarking
• Provides performance context
• Aids discovery of improvement opportunity
• Helps identify the right performance targets
• Supports the identification of practices with proven positive outcomes
31

Just How Above “Good” Do You Need to Be?
• To optimize improvement efforts, you need to first understand what a change in performance will mean
32
You need targets
that are:
Industry accepted
Measurable and quantifiable;
timely
Defined by true “peer groups”

Example: Days in A/R
• Consider a practice where Days in A/R improved to 38.7, and performance has been sustained most months for the past year:
33
IMPROVED & SUSTAINED
Days in
A/R
38.7
JAN
FEB
MAR
APR
MAY
JUN
JUL
AUG
SEPT
OCT

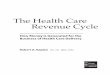
Example: Days in A/R
• Meanwhile, Days in A/R for the organizations peers have dropped even more …
Source: Analysis of HFMA's MAP AppSM ,
DAYS IN A/R AMONG PEER GROUPS OF SIMILAR REVENUE, PAYER MIX
33.0 34.0 35.0 36.0 37.0 38.0 39.0
35.5 Peer 3
38.1 Peer 2
38.7 Case Example Practice
38.0 Peer 1
34

State
Two letter abbreviation of state in which practice is located
(MAP App utilizes A/B Mac Jurisdiction to group states)
Number of Sites
Total number of sites/locations physicians are practicing by physical address (#)
Number of Practices Total number of MAP App Practices being reporting
Academic Affiliation Practice’s affiliation with major teaching hospital (yes/no)
Net Patient Revenue
(monthly average) Net Revenue of practice (= annual net patient revenue / 12 months). Use last fiscal.
“Buckets” “Options”
Custom Peer Group Options
35

Total Number of
FTE Physicians
* Primary Count: number of FTE physicians that are Family Practice, Internal Medicine
and Pediatrics, OB/GYN, and hospitalists
* Specialty Count: number of FTE physicians that are all other
* Specialty Percent - will be calculated for you
* Physician Extender Count: number of FTE physician extenders; includes CRNA, PA,
NP, and Midwife.
* Physician Extender Percent - will be calculated for you
* Total Physicians - will be calculated for you
Note: FTE is defined as greater than 32 patient care hours
“Buckets” “Options”
Custom Peer Group Options
36

• Clearly defined
• Measurable
• Discerning
• Comparable
37
HFMA MAP Keys

Sample of an HFMA MAP Key
38
See the list at www.hfma.org/map
Indicator
Purpose
Value
Calculation
Net days in A/R
Trending indicator of overall A/R performance
Indicates revenue cycle efficiency
Net A/R
Net patient service revenue

Physician Practice Management Keys
• 14 Individual Keys
• 4 Categories
– Patient Access – 2 keys
– Revenue Integrity – 1 keys
– Claims Adjudication – 2 keys
– Management – 9 keys
• Similar concept to hospital side with other keys unique to physician practice management
39

14 Physician Practice Management MAP Keys℠
• 1a. Primary Physician Practice Operating Margin Ratio
• 1b. Specialty Physician Practice Operating Margin Ratio
• 1c.Net Income/Loss per Primary FTE§ Physician
• 1d.Net Income/Loss per Specialty FTE§ Physician
• 2. Practice Net Days in Accounts Receivable (A/R)
• 3. Practice Cash Collection Percentage
• 4a.Total Primary Physician Compensation as a Percentage of Net Revenue
40

14 Physician Practice Management MAP Keys℠
• 4b. Total Specialty Physician Compensation as a
Percentage of Net Revenue
• 5. Percent of Patient Schedule Occupied
• 6. Professional Services Denial Percentage
• 7. Point-of Service (POS) Collection Rate
• 8. Total Charge Lag Days
• 9.Aged Accounts Receivable (A/R) by Payer Group as a Percentage of Outstanding Total A/R
• 10.Aged Accounts Receivable (A/R) as a Percentage of Outstanding Accounts Receivable
41

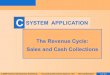
% Patient Schedule Occupied
0.78
0.8
0.82
0.84
0.86
0.88
0.9
0.92
0.94
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
42

POS Collection Rate
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
43

Charge Lag Days
0
1
2
3
4
5
6
7
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
44

Practice Cash Collection Percentage
Peer Group: Nationwide
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
140.0%
160.0%
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile Specific Region
45

Practice Net Days in A/R
0
10
20
30
40
50
60
70
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
46

Aged A/R 90+
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
47

A/R: Medicare Traditional 90+
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
48

Payment Denial Rate
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
A/B MAC 5 & 6 Median Performance 90th Decile 75th Percentile
Peer Group: Nationwide
Specific Region
49

Key Indicator of a Revenue Cycle in Need of Help!
Welcome to a meeting of the practice managers…
50
CFO
CMO

Thank You!
51

Contact Information
• Katie Gilfillan
Director, HFP – Physician and Clinical Practice
[email protected]; 800-252-4362
• Sandra J Wolfskill, FHFMA
Director, HFP – Revenue Cycle MAP
[email protected]; 800-252-4362
52