Embed Size (px)
Citation preview

Presented by
Revenue Cycle Advancement Center
Eight imperatives for generating efficiencies through
sustainable change
The Path to Revenue Cycle Systemness

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
2
Road mapRoad map
The Case for Systemness1
2 8 Imperatives for generating efficiencies through sustainable change
3 Coda

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
3
1. Moody’s preliminary.
Source: Moody’s Investors Service, “Preliminary Medians – Profitability Holds Steady as Revenues
and Expenses Converge,” April 25, 2019; Moody’s Investors Service, “Revenue Growth and Cash
Flow Margins Hit All-Time Lows in 2013 US Not-for-Profit Hospital Medians,” August 2014.
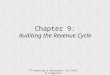
Getting a handle on cost growth, yet margins remain slim
Facing our own affordability issues
Median revenue and cost growth
2009-2018
2018 median operating margins
among not-for-profit hospitals¹
1.7%6.1%
4.6%5.0%
7.1%
5.7%5.1%
0%
1%
2%
3%
4%
5%
6%
7%
8%
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Revenue growth Expense growth
Revenue Cycle Advancement Center research and analysis.
DATA SPOTLIGHT

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
4
Source: Ellison A, “Washington health system files for bankruptcy, cites issues with revenue cycle vendor,” Becker’s Hospital Review,
https://www.beckershospitalreview.com/finance/washington-health-system-files-for-bankruptcy-cites-issues-with-revenue-cycle-vendor.html.
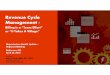
Dire consequences when collections are neglected
Focus on cost at the expense of revenue cycle?
“Washington health system
files for bankruptcy, cites
issues with revenue cycle
vendor”
Becker’s Hospital Review
Although hospital leadership has actively managed the supply chain… this delay
in cash collections has now become severe enough to potentially disrupt the
organization’s ability to pay for crucial items in a timely matter.”
— Astria Health
Revenue Cycle Advancement Center research and analysis.
Ominous Headlines for Astria Health
• 3-hospital health system based in Sunnyside, Washington filed for Chapter 11
bankruptcy protection on May 6, 2019
• System will use bankruptcy process to restructure its finances, enter into a
plan of reorganization with its creditors, and replace its billing company
COMPANY IN BRIEF

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
5
Source: 2017 Hospital Revenue Cycle Benchmark Generator; “The Rise of Self-Pay Accounts,” The Association of Credit and Collection
Professionals, Collector Magazine. http://insurancenewsnet.com/oarticle/2015/02/09/the-rise-of-self-pay-accounts-a-592260.html.
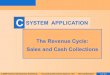
Revenue cycle leaders surrounded by challenging forces
The market is not making it easy
Revenue Cycle Advancement Center research and analysis.
• Significant patient obligations puts ever
greater portion of revenue at risk
• Patient collections no longer just additional
revenue; comprises significant portion of
total patient revenue
Patients becoming payersChallenging payer relationships
90% Increase in denials write-
offs, 2011-2017 30% Of average health care bill now
comes from the patient's pocket
• Automated denials result in difficult to
manage volumes
• Complex criteria, requirements makes
prevention more difficult

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
6
Source: Deloitte Center for Health Solutions and the Healthcare Financial Management Association, “Hospital M&A: When done well, M&A can achieve
valuable outcomes,” https://www2.deloitte.com/content/dam/Deloitte/us/Documents/life-sciences-health-care/us-lshc-hospital-mergers-and-acquisitions.pdf.
Efficiency was never the goal, and was not achieved
Living in the aftermath of the consolidation wave
30% 31%
11%
14% 15%
Don't Know Less than 25% 25-50% 51-75% 76-100%
Percentage of organizations reporting portion of expected
savings actually realized
Anticipated cost savings post-transition
29%Of hospital executives surveyed
sought mergers to improve efficiencies
Bargaining power the main play
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
7
Source: Physician Advocacy Institute, “Updated Physician Practice Acquisition Study: National and Regional Changes in Physician Employment 2012-2016,”
March 2018; Practice Velocity, “Changing ownership trends in urgent care,” February 27, 2017; “Ambulatory Surgery Center Special Report: 2017 Benchmarks,”
Avanza Healthcare Strategies; MedPAC, A Data Book: Health Care Spending and the Medicare Program, June 2017; Tenet Health Q1 Earnings Call 2018.
Revenue cycle no longer confined to a hospital’s four walls
Expanding into an array of ambulatory assets
Revenue Cycle Advancement Center research and analysis.
Physicians
Urgent care
locations
Ambulatory
surgery centers≈31%Of 10,080 urgent care locations
owned or partially owned by
health systems, 2015
≈ 41%Of 5,602 ASCs owned or
partially owned by health
systems, 2017
≈ 47%Of physicians employed
by hospitals, 2018
Increased diversity of health system investments outside the hospital

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
8
Proliferating sites of care mean complications for revenue cycle
Systemness challenges go beyond mergers
Multiple payer contracts
Each with its own rates,
carve-outs and exceptions
Integrated revenue cycle enterprise challenges
Different fee schedules
Requires knowledge of
different coding,
documentation requirements
Variable performance
expectations of staff
Revenue cycle staff across
different settings accustomed
to certain processes, metrics
Disparate IT systems
Multiple EHR, billing systems,
chargemasters add
complexity
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
9
Defining some key terms
Health system
Any health care organization that
provides services at more than one
facility, including acute, outpatient,
and/or ancillary sites
Revenue Cycle Advancement Center research and analysis.
Systemness
The ability to make decisions that are
optimal for the organization as a whole,
rather than for individual service lines,
facilities, or stakeholder groups

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
10
Defining the integrated revenue cycle enterprise
Hallmarks of revenue cycle systemness
Revenue Cycle Advancement Center research and analysis.
• Divisions of authority between various
leadership structures expressly articulated
• Thoughtful balance of powers between
functions, sites, departments
• Incorporates site-level and functional (e.g.
coding, patient access) representation
• Appropriate level of centralization
according to revenue cycle function
• Elimination of redundant departments and
appropriate levels of staffing
• Consistency in process and performance
measurement
Effective governance Operational efficiency
• Clinicians understand the importance of
compliance with revenue cycle requests,
including comprehensive documentation
• Metrics and incentives are designed to
encourage collaboration, joint success
Clinician alignment
• IT systems facilitate exchange of data across
sites, functions, such as integrated billing
systems, EHR
• Culture of knowledge-sharing extends
beyond transparency to curiosity, reflection
Accessible, interoperable data

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
11
Barriers on the road to revenue cycle systemness
Revenue Cycle Advancement Center research and analysis.
Lack of
commitment
Lack of access
to critical dataUnclear roles and
inefficient processes
No bandwidth
for change
Initiative
loses steam
Misaligned
org structure
Siloed
operations
Unsure
where to start

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
12
Generating efficiencies through sustainable change
Revenue cycle’s system advantage
Revenue Cycle Advancement Center research and analysis.
Creating a unified vision
1. Secure commitment from key
stakeholders
2. Clearly chart the course to
systemness
3. Leverage early wins to bolster
support
4. Create capacity for transformation
1Organizing for efficiency
5. Align organizational structure to
critical metrics
6. Where you can’t own, collaborate
7. Standardize roles and processes
to boost productivity
8. Calibrate degree of centralization
2

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
13
Road mapRoad map
The Case for Systemness1
28 Imperatives for generating efficiencies through
sustainable change
3 Coda

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
14
Source: Ewenstein B, et. Al, “Changing change management,” McKinsey & Company,
https://www.mckinsey.com/featured-insights/leadership/changing-change-management.
Best intentions doomed by lack of unified vision
Revenue Cycle Advancement Center research and analysis.
Consequences of pursing change without a unified vision
Executives do not devote
dedicated resources
Frontline staff fight each
step of the way
Proposal doesn’t solve the
root-cause issue
Proposal is predicated on
unrealistic expectations
Odds not in your favor
70%Percentage of change efforts
that fail, largely due to
employee resistance and lack
of management support

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
15
Stakeholders have different sets of concerns, require different approaches
Customize your approach to your audience
Frontline staffC-Suite leadership
Top-of-mind
questions
• Does this proposal align with our
strategic goals?
• How much will this cost?
• What’s the expected ROI?
Tactics to
gain buy-in
• Does this threaten my job security?
• How does this affect my day-to-day?
• Can I weigh in on proposed changes?
1. Align proposal to organizational
strategic priorities
2. Show how the status quo isn’t working
#1: Secure commitment from key stakeholders
1. Display commitment to right answer,
not your answer
2. Avoid top-down approach
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
16
1. Force ranked from most important to least. Source: 2019 Annual CEO Survey, Health Care Advisory Board, Advisory Board.
All 2019 C-Suite priorities bolstered by revenue cycle systemness
Align your proposal to organizational priorities
Revenue Cycle Advancement Center research and analysis.
2019 C-Suite agenda1 Benefit gained from revenue cycle systemness Overlap
Revenue growth Eliminates revenue leakage through improved operations
Cost containment Identifies redundant and unnecessary costs
Population health and risk strategy Standardizes strategy for risk-based revenue capture
Physician partnership strategy Increases physician engagement with documentation
Consumerism and retail strategy Improves patient financial experience and collections
Enterprise-wide systemness Bolsters revenue cycle coordination across system
Innovation Reveals operational challenges prime for creative solutions
Overlap assessment of current C-Suite agenda and revenue cycle systemness

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
17
Analysis revealed
denials rate for
revenue cycle owned
clinic registration
consistently
outperformed clinic-
owned registration
Chief Revenue Officer at Stanford shows clinic registration denials hurt organizational goal
Using data to highlight current weakness creates urgency
Restructuring patient access at Stanford Health Care
Denials data showed
unacceptable number
of registration denials
Chief Revenue Officer
(CRO) decided clinic
owned patient access
needed to report to
revenue cycle
CRO tied change to
organizational goal of
improving revenue
capture. Demonstrated
expected decrease in
registration denials
System leadership
cleared restructuring
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
18
• Chief Revenue Officer (CRO) decided clinic-owned patient access
registration areas needed to report to revenue cycle to improve clinic
registration denials stemming from system’s clinics.
• In her proposal, the CRO tied the restructuring initiative to Stanford’s
broader organizational goal of improving revenue capture. The CRO also
demonstrated expected decrease in clinic registration denials.
• As a result, the C-Suite allowed the CRO to take over clinic patient
access registration functions in clinics for key areas.
2-hospital health system in Palo Alto, CA
Stanford Health Care
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
19
ED/Registration leadership agreed to the change
VP of Revenue Cycle emphasized the need to try a different
model and communicated flexibility and willingness to
change if unsuccessful after six months
ED/Registration leaders initially pushed back against changing
the historic workflow
1. Frontline staff buy-in
VP demonstrates commitment to right answer, not her answer
Performance before personalities
Emergency department coordinator
manages both registration and
clinical tasks in ED
Registration tasks often incomplete and
overlooked in place of clinical tasks
Flexibility gains frontline buy-in at UW Health
Status quo
Steps toward change
System’s front-end model redesign initiative resulted in
recommendation to split the coordinator role in two: one staff
member for clinical tasks and one for registration
1
2
3
4Early indicators are that ED staff like the new model and
registration metrics are trending in a positive direction.5
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
20
• System’s emergency department registration tasks were often incomplete and
overlooked in place of clinical tasks.
• System’s front-end model redesign initiative resulted in recommendation to split
the coordinator role in two: one staff member for clinical tasks and one for
registration.
• ED/Registration leaders initially pushed back against changing the historic
workflow.
• VP of Revenue Cycle emphasized the need to try a different model and
communicated flexibility and willingness to change if unsuccessful after six
months.
• ED/Registration leadership agreed to the change.
• Early indicators are that the ED staff like the new model and registration
metrics are trending in a positive direction.
3-hospital health system in Madison, WI
UW Health
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
21
CONNECTING THE DOTS
What was the most difficult
function you’ve had to integrate?
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
22
Ultimately realized problem
stemmed from patient access staff
not reporting to revenue cycle team,
which meant staff often pulled into
other clinic duties, leaving little time
for necessary attention to detail
1. Pseudonym.
Understanding current operations and identifying pitfalls saves wasted time and resources
Study where you are, to know where you need to go
Crenshaw1 Health struggles to lift patient access performance in clinicsNext, asked corporate
revenue cycle team to lead
hands-on training for patient
access staff
VP of Revenue Cycle
wants to decrease
eligibility denials in clinics,
assumed issue stemmed
around lack of education
First asked clinics to lead
monthly training sessions for
patient access staff
Then, assigned
eligibility denials to
clinic managers to
encourage
accountability
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
23
Site visits and workflow study enables effective change
AFTERBEFORE
Chief Revenue Officer (CRO) and
Executive Director of Patient Access
& Financial Clearance physically
visited clinics to study
• Patient access workflow
• Patient volumes and workflows
• Patient demographics
1
• Reported up through clinic
managers
• Clinics lacked sufficient training,
revenue cycle support/knowledge
from their respective clinic
manager, and understanding of
the impact of their work
• Exhibited higher rates of
registration denials than their
revenue cycle-owned clinic patient
access counterpart
• Majority of clinic patient access
registration staff report to CRO
across system, with more clinics to
be added over time
• Clinics under the revenue cycle
report decreased registration
denial rate
• Clinic patient access registration
staff now able to seamlessly
transfer to hospital registration,
depending on preference
Restructuring clinic patient access registration at Stanford Health Care
Revenue Cycle Advancement Center research and analysis.
Identified adjustments needed to
mirror revenue cycle-owned clinic
patient access function
2

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
24
• Clinic patient access registration staff
reported up through their clinic managers.
As a result, staff did not have adequate
training, sufficient support, and clinic
managers were not sufficiently
knowledgeable of revenue cycle practices.
• Clinic registration was often inaccurate and
incomplete, resulting in a higher
percentage of registration denials than
revenue cycle-owned clinic registration
areas.
• Chief Revenue Officer (CRO) decided
patient access in clinics needed to report
through the system’s revenue cycle
department.
• CRO and Executive Director of Patient
Access & Financial Clearance mapped out
the transition by physically visiting each
clinic to understand their patient access
workflow, patient volumes and workflow,
and patient demographics.
• Majority of clinics were transitioned to
revenue cycle leadership, with additional
clinics to be added over time.
• Clinics under revenue cycle now report a
decreased registration denial rate. Clinic
patient access revenue cycle staff are also
able to seamlessly transfer to hospital
registration, depending on preference.
2-hospital health system in Palo Alto. CA
Stanford Health Care
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
25
Impatience risks premature project abandonment
Expect productivity dip after implementation
Revenue Cycle Advancement Center research and analysis.
Productivity curve throughout change initiative
Pro
ductivity New process
implemented
Time
Productivity dip
2
Productivity
breaks even
New benchmark reached
3
4
1
Measurable returns
Consequences of premature
judgement on ROI
• Change leaders discouraged
by lack of results
• Change initiative deemed a
failure and abandoned
• Organization never reaps
benefits of change, despite
investment
CAUTION

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
26
1. Pseudonym.
Hooks Health1 reports unparalleled performance after call center centralization
A year of patience is rewarded
System relocates all
patient billing call centers
to centralized location
Centralizing patient billing call center at Hooks Health
Center metrics exceed
baseline performance
Center reported initial dip in metrics:
• Increased patient wait time
• Increased call abandonment rate
• Increased staff turnover
One year later
Revenue Cycle Advancement Center research and analysis.
Hook’s current metric
performance
57 secondsAverage patient wait time
<20%Abandonment rate
<13% Average staff turnover
DATA SPOTLIGHT

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
27
• System recently centralized all patient billing call centers.
• After the initial change, the center reported a dip in performance metrics,
including increased patient wait-time, increased call abandonment rate,
and increased staff turnover.
• However, the VP of Revenue Cycle stayed patient and allowed an
adjustment period before judging ROI on the centralization.
• One year later, the center’s metrics now exceed baseline performance,
reporting an average wait time of 57 seconds, an abandonment rate less
than 20%, and a staff turnover rate less than 13%.
Medium-size health system in the West
Hooks Health1
1. Pseudonym.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
28
On the journey to systemness, things will
often get worse before they get better.
How long does it take to create lasting change?
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
29
Staff may lose interest as they wait for results
Stakeholder buy-in isn’t static
Tomorrow’s engagement is not guaranteed
Initial stakeholders agree to change
Stakeholders discouraged by delayed
results, no broader buy-in achieved
Early wins are crucial to maintaining
organizational commitment
Early wins:
• Validate the proposal’s vision and strategy
• Give emotional lift to initial supporters
• Attract new supporters through
demonstrated success
• Take power away from cynics
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
30
Systemness initiatives easier when invisible to patients and doctors
Assessing easy wins for systemness
Potential functions to integrate into health system
Clinical Documentation
Improvement
SchedulingFacility coding Prior authorization Patient accessBusiness office
Increasing difficulty
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
31
Partnership will make the first win that much easier
Recognize an opportunity when a volunteer approaches you
Measure your success
Build infrastructure together
Director of Patient Access
worked with clinic leadership
to standardize patient
scheduling templates Additional specialties
continue to volunteer.
System hopes to have
most outpatient clinic
prior authorization
centralized in 3-5
years.
Clinics suggested
prior authorization
be centralized
under revenue
cycle team
Multiple clinics
lacked the time and
expertise to secure
prior authorization
for patient visits
UW Health’s transition to centralized outpatient clinical prior authorization
Director of Patient
Access and VP of
Revenue Cycle
agreedRevenue cycle leadership
tracked decrease in prior
authorization denials
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
32
• Multiple clinics lacked the time and expertise to secure prior authorization
for patient visits.
• Clinics suggested prior authorization be centralized under revenue cycle
team.
• Director of Patient Access and VP of Revenue Cycle recognized
opportunity and agreed.
• Director of Patient Access worked with clinic leadership to standardize
patient scheduling templates.
• Revenue cycle leadership tracked decrease in prior authorization denials.
• Additional specialties continue to volunteer. System hopes to have most
outpatient clinic prior authorization centralized in 3-5 years.
3-hospital health system in Madison, WI
UW Health
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
33
Revenue Cycle Advancement Center research and analysis.
CONNECTING THE DOTS
Creating short-term wins is different from hoping
for short-term wins:
• Where can you create short-term wins?
• How have you leveraged early wins in the past?

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
34
Who’s got time for change?
Overwhelmed is the norm
Revenue Cycle Advancement Center research and analysis.
Number of individual change
initiatives hitting a manager
at any one time5-15 400
Number of annual change
initiatives at one representative
health care organization
Everyone is too busy with day-to-day work…We’ve got to collect $4.1 billion, but we
also have to spend a lot of time thinking about going to a combined system. That’s not a
normal task. It’s a BIG lift. My number one concern right now is the pace, and when that
happens combining becomes just a ‘nice-to-have’.
VP of Revenue Cycle, 3-hospital health system in the West

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
35
Stanford Health Care creates in-house “revenue cycle strategy and analytics” division
Internal teams “keep the knowledge here”
Revenue Cycle Advancement Center research and analysis.
Stanford’s Revenue Cycle Strategy and Analytics
I still use consultants, but not as
much as I did before. I get more
consistency by having it built in.
The knowledge stays here.
Jill Buathier, Chief Revenue Officer
Stanford health care
Composed of one director, several program
managers, and seven FTEs
Oversees revenue cycle strategic planning
efforts, strategy, performance improvement,
analytics/reporting and special projects

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
36
• Stanford recently created a Revenue Cycle Strategy and Analytics team,
which is comprised of a director, several revenue cycle program
managers (who oversee performance improvement), and seven FTEs.
• The team oversees revenue cycle planning efforts, strategy, and special
projects that were previously handled by IT Clinical and Business
Analytics and external consultants.
• The team allows Stanford to improve project efficiency and retention of
critical expertise.
2-hospital health system in Palo Alto, CA
Stanford Health Care
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
37
1. Pseudonym
2. Note: This is an ongoing initiative for Lorde Health and not yet complete.
Lorde Health1 leverages HR and Enterprise team over multiple years
Centralizing pre-authorization requires diverse skills and dedication
Revenue Cycle Advancement Center research and analysis.
Study
• Current workflow
• Volume
• FTE utilization
• Job descriptions
Revenue Cycle
VP utilized enterprise team for revenue cycle
Strategize
• Standardize policies,
workflows
• Calculate required FTEs
• Reconfigure job
descriptions
Train
• Epic training
• Policy and workflow
training
Pilot
• Roll out in one dept.
• Log lessons learned
TASKS
TEAMS
Revenue Cycle HR Health Services Engineering
Repeat

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
38
• System currently working to centralize prior authorization across the revenue cycle.
• Initiative utilizes a range of Lorde’s teams, including Human Resources and
Lorde’s enterprise team, the “Health Services Engineering” team.
• HR, the Health Services Engineering team, and Lorde’s existing revenue cycle
staff are beginning the initiative by studying current operations to understand
workflows, patient volumes, and FTE utilization.
• Change leaders will then standardize policies and workflows, calculate the required
FTEs, and reconfigure job descriptions. They will also train staff on new Epic and
workflow changes.
• Finally, the system’s revenue cycle team will pick a department to pilot
centralization, logging lessons learned before expanding scope to all departments.
Medium-size health system in Mid-Atlantic
Lorde Health1
1. Pseudonym.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
39
“We couldn’t do it on our own…Operational staff alone
does not have the knowledge, skills, and abilities to
lead a transformation. You need expertise you don’t
have. You need bandwidth. You need political cover.”
VP of Revenue Cycle, large health system in the West
• Source: Revenue Cycle Advancement Center research and
analysis.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
40
Weigh your options for building capacity
Revenue Cycle Advancement Center research and analysis.
Comparison Benefits Drawbacks What it sounds like
Consultants
RISK
QUALITY
COST
• Immediate increase in
capacity
• Objectivity
• Deep expertise
• Agility
• Lack of continuity
• High short-term expense
“I know what happens when
consultants come and go…we
need a really strong discipline
in the organization to keep the
momentum going.”
Revenue cycle
strategy staff
RISK
QUALITY
COST
• Easily accessible
• Maintains knowledge and
discipline close to revenue
cycle team
• Must keep a continuous
pipeline of work
• Hiring difficult
“One of the things I would
have done differently is I
would have hired a dedicated
project director for
consolidation efforts.”
Enterprise
team
RISK
QUALITY
COST
• Specialized expertise
• Objectivity and institutional
knowledge
• Lower cost than external
consultants
• Must wait in queue
“They help drive a lot of
successful initiatives…they’re
unbiased in the process.”
Operational
staff
RISK
QUALITY
COST
• Requires no additional
resources
• Project likely to fall behind
other priorities
• May overload operational staff
“We did it all internally and I
think I almost burnt out all of
my staff.”

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
41
YOURSELF
ASK
WHO’S MOST LIKELY TO DO THE JOB WELL?
WHO’S LEAST LIKELY?
&
a b c d e
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
42
Generating efficiencies by achieving economies of scale
Revenue cycle’s system advantage
Revenue Cycle Advancement Center research and analysis.
Creating a unified vision
1. Secure commitment from key
stakeholders
2. Clearly chart the course to
systemness
3. Leverage early wins to bolster
support
4. Create capacity for transformation
1Organizing for efficiency
5. Align organizational structure to
critical metrics
6. Where you can’t own, collaborate
7. Standardize roles and processes
to boost productivity
8. Calibrate degree of centralization
2

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
43
Division is a slippery slope
Signs of an inefficient revenue cycle
Poor accountability
Missed opportunities for synergy, cost reduction
Limited professional growth
Staff are not measured by the metrics they impact
Revenue Cycle Advancement Center research and analysis.
Disengaged staff
Functional siloes

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
44
No standard definition for how we organize
The puzzle of revenue cycle governance
Clinic patient access
Health Information Management (HIM)
Physician credentialing and enrollment
Revenue Cycle Advancement Center research and analysis.
?
?
It’s all very confusing as to who is
responsible. It’s almost like a
Rubik’s cube…I’m not at all proud
of how we structure ourselves.
VP of Revenue Cycle
3-hospital health system in the West

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
45
Some things ARE black and whiteFront office staff reporting to revenue cycle improves performance
“When it comes to denial rate for
registration, we outperform clinic
staff each and every time.”
Source: Becker’s Hospital Review, “Breaking Down Silos to Improve Patient
Flow, Hospital Efficiency,” https://www.beckershospitalreview.com/patient-
flow/breaking-down-silos-to-improve-patient-flow-hospital-efficiency.html;.
Revenue Cycle Advancement Center research and analysis.
“Our pre-admitting call center does not
report up through the revenue cycle
leadership, and as a result, 40%-50%
of our denials are based on eligibility.”
© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 07/25

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
46
UW Health aligned HIM to revenue cycle organization
Govern what impacts you
1
The path to systemness in action:
2
HIM reports to CIO
HIM reports to Revenue Cycle
BEFORE: Functional alignment
AFTER: Strategic alignment
External consultants recommended HIM be re-aligned
to report to revenue cycle; System executive
leadership directed VP to implement recommendation
Through integration and with HIM at the table with
other areas of the revenue cycle, it is now easier to
work towards common goals in the following areas:
• Identity management
• Missing/incomplete documentation
• Releasing information
• Denial management
• Overall EHR information governance
HIM previously reported up through Chief
Information Officer (CIO)
3
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
47
• HIM previously reported up through the Chief Information Officer (CIO).
• External consultants recommended HIM be re-aligned to report to revenue
cycle; System executive leadership directed VP to implement recommendation.
• Through integration and with HIM at the table with other areas of the revenue
cycle, it is now easier to work towards common goals in the following areas:
– Identity management
– Missing/incomplete documentation
– Releasing information
– Denial management
– Overall EHR information governance
• The restructuring’s full impact on revenue cycle metrics is still pending.
3-hospital health system in Madison, WI
UW Health
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
48
Delays impact entire system’s metrics
New physician onboarding not just a clinic issue
Onboarding hurdle Consequence of delay
Credentialing
System obtains and validates
physician’s qualification and
experience
1
50-90 daysAverage turnaround time
Physician can neither see nor bill
patients but may still receive salary
Cost of a one month’s
credentialing delay for
primary care physician
$30,000
Revenue Cycle Advancement Center research and analysis.
Payer enrollment
System submits physician’s
credentials to payer’s internal
credentialing review department
2
60-120 daysAverage turnaround time
Physician can see patients but cannot
bill payers for reimbursement
Disrupts cash flow and may
ultimately result in an untimely claim
denial from commercial payers

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
49
Elevate new physician onboarding to the system-level
Two tactics to systematize physician credentialing and enrollment
Assign new physicians a
credentialing coordinator
Coordinator acts as the physician’s advocate
Secure delegated status with
major commercial payers
Perform all credentialing and enrollment in
exchange for annual audit from payer
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
50
• System secured delegated credentialing
status with all 36 major payers.
• New physicians are assigned a
credentialing coordinator, who assists the
physician in the credentialing and
enrollment process.
• Physicians only fill out one batch of
paperwork for both credentialing and
enrollment.
• The physician’s paperwork is reviewed by
Medical Director. Director approves “clean
files,” or files without malpractice history,
within 24 hours. If additional time is
needed, the paperwork is reviewed by the
entire credentialing team, comprised of
Medical Director and five physicians.
• After approval, new physician is added to
system’s roster, which is sent to every
payer on a weekly basis.
• Between these two tactics, a new physician
with a “clean file” is credentialed and
enrolled within 20-30 days from date of
hire, compared to the industry average of
60-120 days.
51-hospital health system based in Renton, WA
Providence St. Joseph Health
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
51
Delegated status eliminates delays from payer non-responsiveness
Leverage system strength to decrease payer reliance
Revenue Cycle Advancement Center research and analysis.
Providence St.
Joseph’s Health
New physician
joins system
Physician
completes
paperwork
System’s Medical
Director approves
“clean files”
New physician
joins system
Physician
completes
paperwork
Delegated credentialing at Providence St. Joseph Health
System’s credentialing
department approves file
Non-delegated
system
Physician added
to system’s
enrollment roster
Physician’s file
individually sent
to each payer
Physician’s
file signed off
by each payer
Physician cleared
to bill patients
10-12 days
60-120 days
Physician cleared
to bill patients

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
52
Providence St. Joseph Health assigns new physicians coordinators to streamline onboarding
Offer system assistance from the get-go
Credentialing coordinators at Providence
St. Joseph Health
• Each coordinator assigned 200 new physicians
in regional area
• Coordinators serve as the physician’s advocate
during the credentialing and enrollment process
• Assists the physician in filing out one dual
application for credentialing and enrollment
• Enrolls the physician in Medicare and Medicaid
• High school degree or GED required, Associate
or Bachelor’s degree preferred
Providence’s credentialing and enrollment
timeframe from hire date, compared to
industry average of 60-120 days
20-30 days
Physician only fills out one batch of paperwork,
decreasing delays in paperwork completion
System stays informed of the exact status of
the onboarding process
Physician’s early impression of system is
that of support and personalized attention
Benefits of a credentialing coordinator
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
53
Revenue Cycle Advancement Center research and analysis.
CONNECTING THE DOTS
• Which functions do you own now?
• How hard would it be to get what you need?

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
54
Critical of top-down mandates to conform
operations to system-wide standard
Concern that clinic claims will be overlooked
for high-dollar hospital accounts
Reluctant to relocate staff to system level
Clinic operations prior to acquisition
Family mentality with unclear division of labor
Revenue cycle functions are wholly-owned
and often on-site
Assumption that acquisition will change little
in day-to-day operations
VPs not likely to receive clinic blessing for full revenue cycle ownership
Clinic integration easier said than done
Revenue Cycle Advancement Center research and analysis.
Clinic objections post-acquisition
“It’s been a challenging and painful process. The doctors scream, ‘I used to have 25 staff and now I have
10.’ But that was because they weren’t making money in their practice. That’s why they sold it to us.”
VP of Revenue Cycle, large Midwest health system

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
55
Stakeholders monitor new strategies to
ensure changes corrected root issue
Staff specialized by denial type:
1. Pseudonym.
Steinman Health1 clinics own denials management, but denials mitigation is collaborative
Compromise with collaboration
Subgroups meet weekly to discuss how
adjustments impact their specific setting
Monthly meetings to root-cause denials
and brainstorm workflow adjustments
Denials management
Denials management owned and operated by clinics
Denials mitigation
$200K Recovered revenue from denials
coordinators in one month’s time
One system-wide workgroup with both professional
and hospital stakeholders
6% Steinman’s system-wide
initial denial rate
Revenue Cycle Advancement Center research and analysis.
Denials coordinators work denials that require
clinical coding (e.g. medical necessity)
Clinic billers work mundane denials
(e.g. eligibility, registration errors)

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
56
• Denials function within clinics split between management and mitigation.
• Denials management owned and operated by clinics, with staff specializing by
denial type. Denials coordinators work denials that require clinical coding (e.g.
medical necessity) and clinic billers work mundane denials (e.g. eligibility,
registration errors).
• Steinman’s denials coordinators recovered $200,000 in one month.
• Clinic denials mitigation is operated via one, system-wide workgroup of
professional and hospital stakeholders.
• The workgroup holds monthly meetings to root-cause denials and brainstorm
workflow adjustments. Subgroups meet weekly to discuss how adjustments
impact their specific setting.
• Steinman reports a 6% initial denials rate across the system.
Large health system in Mid-Atlantic
Steinman Health1
1. Pseudonym.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
57
System strength increases denial leverage over payers
Clinics own denials, with option to call in reinforcements
1Attempt appeal
• If denial trend remains
unresolved in the JOC
log, the issue is escalated
to the System CFO
Flag leadership
42Elevate to system
• PB Follow Up and Denials
staff first attempt to appeal
denial through typical
processes
• If denial trend remains
unresolved, the trend is
escalated to the system’s
payer representative
• Representative tracks the
denial trend and brings
issue to routine
conversation with payer
• Most denial trends are
resolved at this stage
• If needed, denial trend is
elevated to the monthly
joint operating committee
(JOC) meetings with the
payer and the system’s
managed care team
3Loop in JOC
Ochsner Health System’s appeal escalation strategy
2%-3%Ochsner’s PB initial
controllable denial rate
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
58
• System’s professional revenue cycle owns denials management with option to elevate
denial to the system level if needed.
• PB Follow Up and Denials staff first attempt to appeal the denial through typical
processes.
• If denial trend remains unresolved, the trend is escalated to the system’s payer
representative, who brings up the issue in routine conversations with payer.
• If needed, the denial trend is elevated to the monthly joint operating committee (JOC)
meetings with the payer and the system’s managed care team.
• If denial remains unresolved in the JOC log, the denial is escalated to the System CFO.
• Ochsner Health System reports a initial controllable PB denial rate initial of 2%-3%.
30-hospital health system in southeastern Louisiana
Ochsner Health System
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
59
• Source: Revenue Cycle Advancement Center research and
analysis.
Revenue Cycle Advancement Center research and analysis.
“Everybody wore all the hats, and everyone pitched
in…but we didn’t collect the money, we had high
denials, and the patients weren’t satisfied.”
VP of Revenue Cycle, large health system in Midwest

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
60
• Clear accountability
• Reduced duplication of effort
• Streamlined workforce
• Improved quality
Standardizing roles and processes avoids overwhelm, lost productivity
From chaos to clarity
Ill-defined roles and
processesStandardized roles
and processes
• Endless requests
• Countless trade-offs
• Rampant juggling
• Lost productivity
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
61
1. Pseudonym.
Standardizing patient access at Morrison Health1
• Report to clinic manager
• Provide clinical administration support,
operational support, and revenue cycle support
• Report to revenue cycle
• Scheduling
• Insurance verification
• Registration
Clinical staff Non-clinical staff
Before: Generalist role After: Roles delineated by focus
• Report to clinic manager
• Patient medication questions
• General office support
Non-clinical staff able to switch patient access
settings, if desired
Improved performance on revenue cycle metrics
Staff collectively ignores unpleasant tasks
Unclear accountability
Shifting priorities
Constant interruptions
Patient Access staff
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
62
• Clinic patient access staff did not report up through revenue cycle. As a result,
staff rarely prioritized revenue cycle functions.
• VP of Revenue Cycle wanted to take over staff reporting and standardize role
across system’s settings.
• VP split the clinic’s patient access staff in two: clinical staff now report to the
clinic manager and do not execute revenue cycle functions. Non-clinical staff
report to revenue cycle and handle scheduling, insurance verification, and
registration.
• As a result, the system’s clinics report improved revenue cycle performance
and increased staff engagement in the clinic’s patient access, as non-clinical
staff are able to switch to the hospital’s patient access setting, if desired.
Large health system in Midwest
Morrison Health1
1. Pseudonym.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
63
Source: Davidson, N, “The Funniest Video Game News Headlines Ever,” Ranker, https://www.ranker.com/list/funny-
video-game-news-headlines/nathandavidson/2017/01/31/how-video-games-can-save-the-world#1109cea9dddb.
Actually, a lot…
Games, what are they good for?
Rescuing the
revenue cycle?!?
AND…Getting a job
21-year-old gamer landed a job as
a football manager, after playing
the game “Football Manager”
Many companies consider good
guild-masters in the World of Warcraft
video game to be effective leaders.
Leadership development
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
64
Vendor agreed to
work with Sharp to
create platform.
Seven months from
commitment to pilot
group implementation
Source: Lopukhina, D. “How Gamification in the Workplace Impacts Employee Productivity,” Medium,
https://medium.com/swlh/how-gamification-in-the-workplace-impacts-employee-productivity-a4e8add048e.
Frustration – the other mother of invention
Gamifying pre-billing
Revenue Cycle Advancement Center research and analysis.
I was talking to my daughter and she kept looking down at her phone. I was
starting to get annoyed and realized she was playing a game. She said she
was almost to the next level and it hit me that my employees are doing
something similar (working accounts) but they don’t know if they are almost
to the next level.
Gerilynn Sevenikar, VP of Revenue Cycle
Sharp Healthcare
90%Percentage of employees that are
more productive when they use
gamification
70% Percentage of business
transformation efforts that fail due
to lack of engagement
48%Average gamification boost to
engagement
Why gamify?
VP pitched the
idea to vendor

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
65
Effective gamification requires a definition of excellence
Building the game
Workgroup articulates the
gold standard workflow
Gamification layered on top of
trigger events in workflow
Gamification platform creates extreme clarity about expectations
Staff earns coins based upon
level of adherence to gold
standard workflow
1 2 3
Badges Real time feedbackLeaderboards
Staff sees performance against peers and gets recognition in real time
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
66
Level up!
10% Reduction in FTEs
10%–35%Increased productivity
18 months into three year
pilot with pre-billing
Revenue Cycle Advancement Center research and analysis.
Previously, I would never know if employees had their
most productive day. The employee wouldn’t even know.
Now throughout the day, we both know if they are tracking
to have their ‘best day ever’ and we can celebrate it!
Gerilynn Sevenikar, VP of Revenue Cycle
Sharp Healthcare
Staff proactively taking on
greater workloads

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
67
• VP of Revenue Cycle recently electronically “gamified” pre-billing functions of the
revenue cycle.
• VP pitched the idea to their existing vendor, the vendor agreed to develop the game
over a seven-month timeline.
• To develop the game, a system workgroup studied the pre-billing function and decided
on a gold standard workflow. The vendor then laid an analytics platform on top, so
when an employee executes the complete gold standard workflow, their avatar is
rewarded with electronic coins.
• Through this game, pre-billing staff see their performance against peers and get
recognition in real time.
• As a result, Sharp has measured a 10%-35% increase in productivity for all pre-billing
employees. This increase has allowed them to reduce staff by 10% while maintaining
best practice DNFB and clean claim rates.
7-hospital fully integrated health care system based in San
Diego, CA
Sharp HealthCare
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
68
Centralize according to your needs
Revenue Cycle Advancement Center research and analysis.
One
location
Unified
workflow
Common
information Benefits Applicable to
Virtual
Centralization □• Reduce cost by saving space
• Avoid getting employees pulled
into non-essential tasks
• Coding
Centralization
• Minimize duplicative services
• Reduce FTEs
• Leverage scale
• Business office
• Prior authorization
• Patient call centers
Co-location □ □• Facilitate collaboration
between staff
• Billers
• Cash posters
Decentralization □ □• In-person communication
with physicians• CDI
Collaboration
Responsiveness
of physicians
Focus
Use when you
want to increase

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
69
1. Centralization Source: 2017 Hospital Revenue Cycle Benchmark Generator.
Central business office ubiquitous for a reason
No shortage of reasons to integrate the business office
Patient access0.7%
Mid-cycle0.8%
1.2% Business office
2017 Advisory Board Hospital Revenue Cycle Survey
Median cost to collect by area (% NPR) Benefits of a centralized business office
Biggest cost center within revenue cycle
Under control of finance
Farthest from physician involvement
Revenue Cycle Advancement Center research and analysis.
“Any fully integrated health care delivery system will have at
least some version of a central business office.”
Gerilynn Sevenikar, VP of Revenue Cycle
SHARP Healthcare

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
70
Unity Point chooses top-performing region as location for financial clearance center
Centralization not just for billing functions
Centralizing patient financial clearance
Before
• Unity Point’s financial clearance functions performed by patient
access staff in each site of care
• Each region reported differing performance on key metrics,
such as authorization denials and point-of-service collections
Executive Director of Patient Access proposed centralizing
financial clearance functions across the system
After
Director identified Quad Cities region as best location for patient
financial clearance center due to region’s
• Existing leadership structure
• Top-notch metric performance
Quad cities region
1
2
Benefits of centralized financial clearance
Improved performance of authorization
denials and POS collections
Reduced number of FTEs
Standardized patient experience
across system
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
71
Centralization provides consistent pre-access performance, patient experience across system
Two work streams cover six of the system’s regions
50%Measured reduction
in front-end denials
for one region,
within 6 months of
centralization
Patient schedules care
Must provide minimum data set
schedule non-emergent care
• Full demographics
• Full insurance information
Pre-access work stream
• 15 pre-access specialists
• Mail patient price estimates
• Attempt to collect portion of
obligation via phone
Pre-authorization work stream
• 12 authorization specialists
• Secure pre-authorization for
outpatient and inpatient
services
Financial clearance center
Financial clearance at Unity Point
Patient arrives for care
If patient obligation could not
be collected via phone, patient
access staff will request
payment at check-in
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
72
• Recently transitioned six of the system’s regions under a centralized financial
clearance center
• System’s Executive Director of Patient Access identified the top-performing
region as the location for the center
• Centralized financial clearance center has two work streams
– Prior authorization team oversees inpatient and outpatient authorizations
– Pre-access team generates patient price estimates and attempts to collect
portion of patient obligation before care
• Since the initiative, Unity has measured a decline in front-end authorization
denials for all regions under the centralized model, reducing one region’s denials
by 50% within 6 months. In addition, the system has measured a system-wide
increase in point-of-service collections
• Unity is currently working to bring all regions under the financial clearance center
20-hospital health system based in West Des Moines, IA
Unity Point
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
73
1. Pseudonym.
Morrison Health1 professional and facility billers address underpayments together
Boosting synergies and normalizing workloads
Revenue Cycle Advancement Center research and analysis.
• Professional fee and facility billers
were physically siloed
• Each biller could only address
underpayments for their particular
payment type
Billers have increased payer
leverage and resolve underpayments
in a shorter timeframe
Co-located billers at Morrison Health
• VP of Revenue Cycle co-located billers
• If billers are struggling with a specific
underpayment, they will contact the
payer together, pulling up the entire
episode of care

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
74
• System struggled with payer underpayments across inpatient and
outpatient settings.
• VP of Revenue Cycle decided to co-locate professional and facility billers.
• As a result, billers enjoy increased leverage over their payers. When a
payer underpays a claim, the billers can pull up the entire payer record
and start talking about both facility and professional underpayments.
Large health system in Midwest
Morrison Health1
1. Pseudonym.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
75
1. Virtual Centralization
Taking functions remote is the ultimate overhead reduction opportunity
Coding highly amenable to virtual centralization
Partners moves hospital coding offsite…
Hospital coding
100% remote
coding FTEs
84Encounters processed
per day
2,124
Estimated savings compared
to non-remote centralized
coding, per FTE
$10KEstimated savings for
offshore staff, per FTE
$55K
Removed physicians from charge capture,
reducing administrative burden
Improved accuracy and efficiency of coding;
expect to eliminate need for 10 coding FTEs
Professional fee coding
Staff manually inputs codes based on
documentation
In-house IT tool translates EHR-based
documentation into billing codes
Remote work strategy
Takes advantage of coding talent shortage in local
market by tapping national labor pool; offshore strategy
takes advantage of labor cost savings
Benefits
…and automates professional fee coding
Legacy process
Automated process
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
76
• System struggled with coding talent shortage in local market and wanted
to reduce costs across the revenue cycle.
• VP of Revenue Cycle moved all hospital coders to virtual centralization,
saving an estimated $55,000 per off-shored FTE.
• VP also automated professional coding to through an in-house IT tool that
translates EHR-based documentation into billing codes.
• Automation of professional codes has improved accuracy and efficiency
of coding; system expects to eliminate need for 10 coding FTEs.
11-hospital health system based in Boston, MA
Partners Health
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
77
CDI programs must maintain facility-level presence
CDI benefits from in-person interactions
Revenue Cycle Advancement Center research and analysis.
CDI functions that require local support
Physician rounding
Provides an opportunity for specialists
to teach clinicians what details should
be included in the patient chart; helps
specialist understand patient status
Physician queries
While most programs use an electronic
or automated query process, in-person
physician follow-up, or escalation to the
CMO, may be necessary
Physician education
CDI specialists must provide multi-
specialty, specialty-specific, and
sometimes individual education that
shows link between documentation,
quality outcomes, and reimbursement
In-person education critical for program success
“80% of our educational events are held face-to-face. We tried using webinars, but
physicians were not engaged, and we saw no improvements in documentation.”
Manager, Coding and Clinical Documentation Improvement Department

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
78
Source: Prosci Inc., “Best Practices in Change Management,” 2014,
https://www.prosci.com/resources/articles/reinforce-and-sustain-change; .
Systemness must be sustained
Don’t let complacency kick-in
Revenue Cycle Advancement Center research and analysis.
61%Percentage of successful
change projects that
implemented
sustainment efforts
Common causes of unsustained change
Premature judgement on project outcomes
Poor communication with key stakeholders
throughout the change process

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
79
Source: Sirkin, H et al., “The Hard Side of Change Management,” Harvard
Business Review, https://hbr.org/2005/10/the-hard-side-of-change-management.
Success is not just a roll of the dice
Four factors predict success in any transformation initiativeP
robabili
ty o
f success
DICE score
Duration
Integrity
Effort
The project team’s
performance
integrity; that is, its
ability to complete
the initiative on timeDuration of time until the
change program is complete
or amount of time between
reviews of milestones
The commitment
to change that
top management
and employees
affected by the
change display
Harvard study found that project
success was positively
correlated with the strength of
four metrics.
The sum of these metrics is
called a DICE score:
DICE = Duration + Integrity +
Commitment + Effort
Commitment
Revenue Cycle Advancement Center research and analysis.
The effort over
and above the
usual work that
the change
initiative
demands of
employees

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
80
Road mapRoad map
The Case for Systemness1
2 8 Imperatives for generating efficiencies through sustainable change
3 Coda

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
81
Few systems boast unified IT
…leaving the patient lost in the middle
Hospital B
Patient Account
System
Hospital A EHR
Clinic C EHR
Clinic D Billing System
Many systems rely on multiple platforms…
Consequences of disparate IT systems:
Patient asked demographic data multiple times
Patient receives multiple bills
Staff unable to answer patient account
questions across settings
“When I think about the patient who sees Kettering Health
Network on the billboards and chooses us for their care—
they are trusting one brand. The more we look, act, and
perform alike, the better for our patient.”
JoAnn Yohn, VP of Revenue Cycle
Kettering Health
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
82
Overheard in a fragmented system
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
83
1. Survey data only: Includes all operational and depreciation revenue cycle costs, including staff salaries and
benefits, technology solutions, outsourcing costs, and overhead costs (space, office materials, etc.).
2. Low, median, and high performance categories correspond to 25th, 50th, and 75th percentiles
3. As a percentage of Net Patient Revenue, for an average 350-bed hospital with $350M in Net Patient Revenue Source: 2011-2017 Hospital Revenue Cycle Benchmarking Survey.
Cost-to-Collect stagnation: No more gains available, or lack of systemness?
Efficiency achieved?
Full cost to collect1,2
Percentage of net patient revenue
n=51 (2011); n=31 (2013); n=59 (2015); n=48 (2017)
2.8%
2.3%1.9%
4.2%
3.0%2.6%
4.0%
3.0%
2.0%
3.7%
3.0%
2.2%
Low performance Median High performance
2011 2013 2015 2017
2019 Revenue Cycle benchmarking coming soon
We are currently accepting submissions. Please email
[email protected] for more information.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
84
1. Electronic Data Inquires
Source: Konda S, “Artificial intelligence can alleviate revenue cycle management
challenges“ Medical Economics, http://www.medicaleconomics.com/technology/artificial-
intelligence-can-alleviate-revenue-cycle-management-challenges.
Wide variety of capabilities on display
Opportunities across the revenue cycle spectrum
Envisioning a revenue cycle powered by AI
Machine learning
optimizes EDI1
queries
Documentation
Patient Access Mid-Cycle Business Office
Machine learning improves
patient price estimates
Natural language
processing generates
claims with computer-
assisted coding
Scheduling and
Pre-Registration
Registration BillingArrival CollectionsCoding Discharge
Natural language
processing automates prior
authorization questions
Machine learning
optimizes edits by payer
Machine learning
scores denials to
inform high
potential appeals
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
85
If insurance is discovered, technology updates the patient
accounting system and sends new coverage information to billing
Technology logs onto payer portals and checks all self-pay
patients eligibility within 25 minutes
System struggled with keep pace with
self-pay patients needing to be screened
for eligibility after registration
Legacy process was entirely manual and
required 2-3 hours of work each day
MedStar Health’s automated eligibility verification
Source: Becker’s Hospital Review, “Employing a Digital Workforce to Transform the Revenue Cycle,”
https://go.beckershospitalreview.com/employing-a-digital-workforce-to-transform-the-revenue-cycle.
MedStar uses RPA to automate eligibility verification for self-pay patients
The first step towards automation
Status quo Steps to change
System partnered with Olive, an AI vendor, to automate self-pay
eligibility verification with robotic process automation (RPA)1
2
3
4
Technology automatically assigned to examine self-pay
patients registered the prior day
Number of eligibility
transactions in first 9 months
of implementation
198,000
25 minutes Time required to check each
day’s batch compared to 2-3
hours under legacy process
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Case in brief
86
• Recently partnered with Olive, an AI vendor, to automate self-pay eligibility
verification with robotic process automation (RPA).
• Technology was built and deployed within 22 days.
• Technology automatically assigned to examine patients registered the prior
day. It logs onto each payer’s portal and checks each day’s batch of self-pay
patients for eligibility.
• If insurance is discovered, technology updates the patient accounting system
and sends new coverage information to billing department.
• Technology can check each day’s batch within 25 minutes, compared to
previous timeline of 2-3 hours under manual verification.
• Within 9 months, technology has competed 198,000 eligibility transactions.
10-hospital health system in Columbia, MD
MedStar Health
Source: Becker’s Hospital Review, “Employing a Digital Workforce to Transform the Revenue Cycle,”
https://go.beckershospitalreview.com/employing-a-digital-workforce-to-transform-the-revenue-cycle.
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
87
1. **Requires complex data infrastructure
Revenue Cycle AI held back by our underwhelming data infrastructure
Are we standing in our own way?
Four degrees of AI technology
Robotic process automation (RPA)
Natural language processing (NLP)**
Machine learning (ML)**
Deep learning (DL)**
Incre
asin
g c
om
ple
xity
“AI isn’t just a black box that you plug in to
perfect operations. This technology is
actually predicated on your ability to
feed in comprehensive data. That’s why
vendors with giant clearinghouses of claims
are the only players we see right now in
revenue cycle automation.”
Senior Advisory Board Researcher
Overheard in the research
Revenue Cycle Advancement Center research and analysis.

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
88
Look for additional research on AI in the revenue cycle in late 20191. Coming soon
Revenue Cycle Advancement Center research and analysis.
CONNECTING THE DOTS
Have you explored using AI in the
revenue cycle?

© 2019 Advisory Board • All rights reserved • advisory.com • WF953632-b 09/11
Credits
89
Stefanie Kuchta
Design Consultant
Eric Fontana
Program Leadership
Anita Mago
Rachel Matthews
Research Team
Robin Brand
Project Director
Revenue Cycle Advancement Center

LEGAL CAVEAT
Advisory Board has made efforts to verify the accuracy of the information it provides to members. This report relies on data obtained from many sources, however, and
Advisory Board cannot guarantee the accuracy of the information provided or any analysis based thereon. In addition, Advisory Board is not in the business of giving legal,
medical, accounting, or other professional advice, and its reports should not be construed as professional advice. In particular, members should not rely on any legal
commentary in this report as a basis for action, or assume that any tactics described herein would be permitted by applicable law or appropriate for a given member’s situation.
Members are advised to consult with appropriate professionals concerning legal, medical, tax, or accounting issues, before implementing any of these tactics. Neither Advisory
Board nor its officers, directors, trustees, employees, and agents shall be liable for any claims, liabilities, or expenses relating to (a) any errors or omissions in this report,
whether caused by Advisory Board or any of its employees or agents, or sources or other third parties, (b) any recommendation or graded ranking by Advisory Board, or (c)
failure of member and its employees and agents to abide by the terms set forth herein.
Advisory Board and the “A” logo are registered trademarks of The Advisory Board Company in the United States and other countries. Members are not permitted to use these
trademarks, or any other trademark, product name, service name, trade name, and logo of Advisory Board without prior written consent of Advisory Board. All other
trademarks, product names, service names, trade names, and logos used within these pages are the property of their respective holders. Use of other company trademarks,
product names, service names, trade names, and logos or images of the same does not necessarily constitute (a) an endorsement by such company of Advisory Board and its
products and services, or (b) an endorsement of the company or its products or services by Advisory Board. Advisory Board is not affiliated with any such company.
IMPORTANT: Please read the following.
Advisory Board has prepared this report for the exclusive use of its members. Each member acknowledges and agrees that this report and the information contained herein
(collectively, the “Report”) are confidential and proprietary to Advisory Board. By accepting delivery of this Report, each member agrees to abide by the terms as stated herein,
including the following:
1. Advisory Board owns all right, title, and interest in and to this Report. Except as stated herein, no right, license, permission, or interest of any kind in this Report is intended
to be given, transferred to, or acquired by a member. Each member is authorized to use this Report only to the extent expressly authorized herein.
2. Each member shall not sell, license, republish, or post online or otherwise this Report, in part or in whole. Each member shall not disseminate or permit the use of, and shall
take reasonable precautions to prevent such dissemination or use of, this Report by (a) any of its employees and agents (except as stated below), or (b) any third party.
3. Each member may make this Report available solely to those of its employees and agents who (a) are registered for the workshop or membership program of which this
Report is a part, (b) require access to this Report in order to learn from the information described herein, and (c) agree not to disclose this Report to other employees or
agents or any third party. Each member shall use, and shall ensure that its employees and agents use, this Report for its internal use only. Each member may make a
limited number of copies, solely as adequate for use by its employees and agents in accordance with the terms herein.
4. Each member shall not remove from this Report any confidential markings, copyright notices, and/or other similar indicia herein.
5. Each member is responsible for any breach of its obligations as stated herein by any of its employees or agents.
6. If a member is unwilling to abide by any of the foregoing obligations, then such member shall promptly return this Report and all copies thereof to Advisory Board.
90© 2019 Advisory Board • All rights reserved • advisory.com