-
7/31/2019 Cycle of Revenue
1/32
-
7/31/2019 Cycle of Revenue
2/32
Purpose of this Case Study
An assessment was performed to identify opportunitiesfor
improvement in the Revenue Cycle, focusing oncase management.
Findings and recommendations address areas ofimprovement that
could impact revenue capture,compliance, and reduce RAC
denials.
-
7/31/2019 Cycle of Revenue
3/32
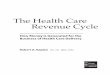
What is Revenue Cycle?
FINANCIALCOUNSELING
INSURANCEVERIFICATION
PRE-REG &PRE-CERT
SCHEDULING
REGISTRATION& POS CASH
COLLECTIONS
CHARGECAPTURE& ENTRY
MEDICAL
MANAGEMENT
MEDICALRECORD &
CODINGCLAIMS
SUBMISSION
THIRD PARTYFOLLOW-UP
PAYMENTPOSTING
REJECTIONPROCESSING
DENIAL &APPEAL
MANAGEMENTCONTRACTMANAGEMENT
EDI-capability
FOCUS AREA
RegulatoryCompliance
Metrics & KPIsCDM
-
7/31/2019 Cycle of Revenue
4/32
Assessment
Conducted over 4 to 6 days, consisting of:
Interviews
What have you inherited that may not belong in your
department? Observations
Chart review
Data Analysis
-
7/31/2019 Cycle of Revenue
5/32
-
7/31/2019 Cycle of Revenue
6/32
RegistrationFindings
Staff require orders prior to procedures
Staff do not always ask to see insurance cards and
identification
Inefficient communication between patient access and
utilization
Recommendations Implement a quality audit for registration and
insurance verification
Involve patient access in the weekly case management meetings
toaddress authorization issues
Patient access and utilization review staff need to consistently
utilizework lists provided by the system to ensure information is
sharedbetween departments
-
7/31/2019 Cycle of Revenue
7/32
Denial Management
Findings Medicaid denials are appealed by an LPN in case
management
All other denials are reviewed in the business office by
non-clinical staff
Recommendations
All denials reviewed by same area, reporting to patient
access
All clinical denials reviewed by a nurse
Enhance denial tracking by using a common work list with
alldenials in process and capturing denial reasons to uncover
trends
-
7/31/2019 Cycle of Revenue
8/32
Utilization Review
Findings UR staff each have their own daily work flow; however,
the
process is similar enough to allow staff to cover for each
other
Process is paper driven and requires a number of manual
steps
UR staff do not use the provided system for work lists
Recommendations
Define work flow and processes
Evaluate staffing plan to promote teamwork with CM
Provide feedback on denial trends to UR staff
-
7/31/2019 Cycle of Revenue
9/32
Case Management
Findings Documentation process is inconsistent for case
management, and
forms are ineffective
Documentation does not always stay with the patients chart
There is no defined or consistent work flow process
Staff lack tools required for their jobs: text pagers/cell
phones,printers, fax machines
The Important Message from Medicare and Choice letters are
not
provided to patients on a consistent basis
-
7/31/2019 Cycle of Revenue
10/32
Case Management
Findings (continued) No formal discharge rounds or long-stay
patient meetings
currently being conducted
Tasks are assigned by discipline (SW versus RN), which
creates
confusion for patients, hospital staff, and amongst themselves
No physician advisor/champion to support the department in
difficult physician situations or to appeal denials
Nursing home referral process is disjointed, involving
various
departments
-
7/31/2019 Cycle of Revenue
11/32
Case Managers
Findings Case Managers lack a consistent daily work flow
Most try to see Observation patients first
Reactive versus proactive
Case Manager carrying 30-50 patients a day
Limited direct communication with physicians
Limited insight into financial impact of case management
-
7/31/2019 Cycle of Revenue
12/32
Social Workers
Findings Social workers receive unnecessary referrals as a
result of limited
patient screening performed by nursing staff
Confusion regarding which tasks require a social worker and
which belong to case managers Social workers spend a significant
amount of their time on
nursing home placements
-
7/31/2019 Cycle of Revenue
13/32
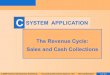
Case Management ModelsRoles: People
3:3 Model 2:1 Model 3:1 Model
1. Social Workers (SW) Discharge Planners Psychosocial Needs
2. Utilization Management (UM) RN
Insurance Management Other
3. Case Managers (CM) Nurses
Models within
CM assignment varies Unit Physician Payer
Disease Management
Two versions1. UM/CM (2) with SW on own2. CM/SW (2) with UM on
own
CM assignment varied as in 3:3
Unit Physician
Payer
Disease Management
CM/UM/SW roles in oneperson
Assignments
Unit Physician
Payer
Disease Management
-
7/31/2019 Cycle of Revenue
14/32
Model ComparisonModel Advantages Disadvantages
3:3 Individual Expertise
Easiest to implement
3 people in chart
Poor productivity
Confusing to customers
Confusing to patientsDifficult case sharing
Hand-off mishaps
More staff to manage
2:1 Works well in certain hospitals
Expertise driven
Promotes teamwork
Good transition to 3:1
2 people in chart
Confusing to customers
Difficult case sharing
Hand-off mishaps
3:1 1 person in chart
Clear assignment for customersComplete start to finish care
Fewer staff to manage
Comprehensive understanding of all aspects has
positive revenue implications
Only for high-functioning hospitals
Requires more training than others
-
7/31/2019 Cycle of Revenue
15/32
Choosing the Right Model
FTEs will depend on hospital services
Denial resolution falls with front or back end regardless
ofmodel utilized
Caseloads
3:3 40-50s
3:1 22-25
Hospital culture
Compliant and revenue-conscience
-
7/31/2019 Cycle of Revenue
16/32
Recommendations
New staffing model
Caseloads 22-25 based on floor assignment
2-in-1 model
Nursing home placement coordinator
Gatekeeper 24/7
Cross training is key to success
New orientation plan
-
7/31/2019 Cycle of Revenue
17/32
Case Manager/Social WorkRecommendations
Move entire Case Management department to the CFO
Weekly revenue cycle meetings
Registration/Patient Access Supervisor
Registration/BO Director
CM Director
HIM Director
Coding Supervisor
Charge Master leader
Director Revenue Cycle
Representative negotiating managed care contracts
CFO
-
7/31/2019 Cycle of Revenue
18/32
Recommendations
Implement weekly long stay/high dollar meeting Goal: review
patients with LOS>5 days; charges higher than $50,000; and
all self-pay patients
Attendees
Case Managers/Social Workers/Utilization Review staff Patient
Access
HIM/ coding
Physicianhospitalist group
Physician advisor or CMO
Nursing
Financial counselor
-
7/31/2019 Cycle of Revenue
19/32
Meeting Process
Distribute list 24 hours ahead of meeting
Schedule for each Case Manager (e.g., 3-3:10 Mary)
Script expectations
Basic clinical, Days authorized, Days left for Medicare,
Discharge plan, Problems Physician issues
Compliments to be shared
Follow-up on compliments
-
7/31/2019 Cycle of Revenue
20/32
Sample Patient Report
Patient Jon Doe admitted 7 days ago for sudden onset
confusion
My discharge plan is
I faxed clinicals yesterday and have 3 more days authorized
Report for tracking: Supervisor works it that AM and knows whois
behind
Dr. Smith seems to be dragging out the stay
No family support
Id like to thank the PT that saw him yesterday, she was very
patient (specifics)
-
7/31/2019 Cycle of Revenue
21/32
Tools Implemented
Defined work flow and updated policies and procedures
Improved documentation with customized forms to assess riskand
plan for placement
Defined which case management documents become apermanent part
of the chart and are scanned promptly
Provided tools like cell phones and laptops with wireless
access
Trained staff to use Interqual criteria to document medical
necessity
-
7/31/2019 Cycle of Revenue
22/32
InterQual
InterQual (IQ) criteria is a trademarked tool provided
byMcKesson Health Solutions
IQ is the preferred tool used by the Centers for Medicare
andMedicaid Services and most RAC audits
CMS requires hospitals to monitor and document medicalnecessity
to assure compliance
Methods
IQ books
Software purchased from McKesson Case Management software that
includes IQ within its product
-
7/31/2019 Cycle of Revenue
23/32
Level of Care DefinitionsCategory or setting based on the
clinical picture when patient is admitted to the
hospital and/or when patient reaches clinical stability at one
level.
1. Observation: onset last 24 hours, reasonable expectation that
duration ofassessment is 6-24 hours, assessment/medications
unresponsive for at least 4 hoursER treatment, psychiatric crisis
intervention
2. Acute: onset within one week, medications requiring
monitoring q4-8 hours, IVmedications, post critical care, post vent
wean
3. Intermediate: onset within last 24 hours, medications
requiring monitoring at least2-4 hours, hemodynamically stable,
telemetry, neuro assessment, post-op trauma
4. Critical: reasonable expectation for patient to stabilize
with high-tech critical care,hemodynamically unstable, medication
monitoring q1-2 hours, acute intubation, etc
5. Levels continue with LTAC, Acute rehab, sub-acute rehab, SNF,
Home Care, home
-
7/31/2019 Cycle of Revenue
24/32
Definitions Severity of Illness (SI) criteria consists of
objective, clinical
indicators of illness including chronic illness or
co-morbidities,which focus on an individual patients clinical
presentation rather
than the diagnosis
Intensity of Service (IS) criteria consists of monitoring
and
therapeutic services, singularly or in combination, that can
only beadministered at a specific level of care
Discharge Screens (DS) are organized by the levels of care
subsetsand provide objective, clinical indicators to determine if
the
patient has reached the level of clinical stability appropriate
for asafe transfer to a different level of care
-
7/31/2019 Cycle of Revenue
25/32
Review Process
1. Pre-admission review (Acute)
2. Admission review (Acute or Observation)
3. Continued stay review (Acute or Observation)
Cannot go backwards (e.g., acute back to observation)4.
Discharge review
Gatekeeper or case manager to perform IQ reviews
Always start with acute care section to see if criteria is met
Observation status should be used if case does not meet acute
criteria
-
7/31/2019 Cycle of Revenue
26/32
-
7/31/2019 Cycle of Revenue
27/32
Observation Process
Findings Observation versus Inpatient status determined by
physician
recommendation upon admissionUM review for clinical support
oftheir decision
Presence of the order is checked after discharge unless CM
happens to
be reviewing the chart
If the order is unclear or missing, CM calls the physician for
aclarification order
Continued stay reviews are completed but not retained in the
patient
record
Poorly understood process by all involved
-
7/31/2019 Cycle of Revenue
28/32
Observation Process
Recommendations
Implement 24/7 gatekeeper role to recommend status on
allpatients entering the hospital at all access points
Order present Charges entered
Case managed
Change billing to hourly
-
7/31/2019 Cycle of Revenue
29/32
Gatekeeper Role: Overview
Responsible for patients needing a bed: inpatient,
observation,ED, L&D, etc.
Ensures that a status order is in all records
First to know of requests for beds to allow for immediate
assessment of status, then calls House Supervisor Logistics
Two or more FTEs to cover at least 12 hours a day, 7 days a
week
RNs preferred, with previous Utilization Review Experience
Laptop needed for mobility around hospital
-
7/31/2019 Cycle of Revenue
30/32
Observation Responsibilities
Entering OBS hours with appropriate start and stop times
Run OBS list twice a day
Visit floor to assess OBS patient progress toward
discharge Perform usual CM tasks to manage these patients,
including discharge planning
Upon discharge or conversion to inpatient, enter order
and enter exact observation hours into system
-
7/31/2019 Cycle of Revenue
31/32
Results
Improved compliance, with an appropriate level of careassigned
within 24 hours of admission and with acorresponding order present
in the chart
Improved revenue capture due to proper procedures in
place at beginning of patient stay Reduced LOS with proactive
planning for discharge and
interdepartmental meetings on long stay/high dollar cases
Reduced RAC denials
-
7/31/2019 Cycle of Revenue
32/32
Impact on RAC Audit
Using InterQual criteria to determined the correct level of
carewill establish medical necessity and ensure that an
appropriateorder is in the chart within 24 hours of admission.
Assigning an appropriate patient status prevents one day
inpatient stays, which have been targeted for RAC. Continued
stay reviews ensure that a patient meets the Intensity
of Service requirement and are performed every three days
toprevent an unnecessarily extended length of stay.
If there is no documentation in the chart to support the level
ofcare chosen by the physician, these continued stay reviews
mayprompt improved clinical documentation.