Embed Size (px)
Citation preview
Physician Ownership of Hospitals & Physician Ownership of Hospitals & Health Facilities: Antitrust & Policy Health Facilities: Antitrust & Policy
IssuesIssues
When Doctors and When Doctors and Hospitals Fight: The Hospitals Fight: The Antitrust Litigation Antitrust Litigation
LandscapeLandscape
Glenn E. DavisGlenn E. DavisJohanna S. LarssonJohanna S. Larsson
Armstrong Teasdale LLPArmstrong Teasdale LLPOctober 25, 2007October 25, 2007
Context of the ContestContext of the Contest
Members of acute care hospital medical staffs invest in, Members of acute care hospital medical staffs invest in, build, and refer patients to a niche facility that competes build, and refer patients to a niche facility that competes directly with the hospitaldirectly with the hospital
Hospitals react with allegedly anticompetitive conduct to Hospitals react with allegedly anticompetitive conduct to interfere with development of the facility and choke off interfere with development of the facility and choke off physician referralsphysician referrals
Common scenarios involve development of:Common scenarios involve development of: single-specialty hospitals (“SSHs”), i.e. inpatient cardiac or single-specialty hospitals (“SSHs”), i.e. inpatient cardiac or
orthopedic services; or orthopedic services; or ambulatory surgery centers (“ASCs”), i.e. outpatient surgical ambulatory surgery centers (“ASCs”), i.e. outpatient surgical
procedures or endoscopy services procedures or endoscopy services Free standing imaging and laboratory facilitiesFree standing imaging and laboratory facilities
Controversial matters of increasing antitrust and health Controversial matters of increasing antitrust and health policy concern and fertile ground for antitrust and related policy concern and fertile ground for antitrust and related forms of litigationforms of litigation
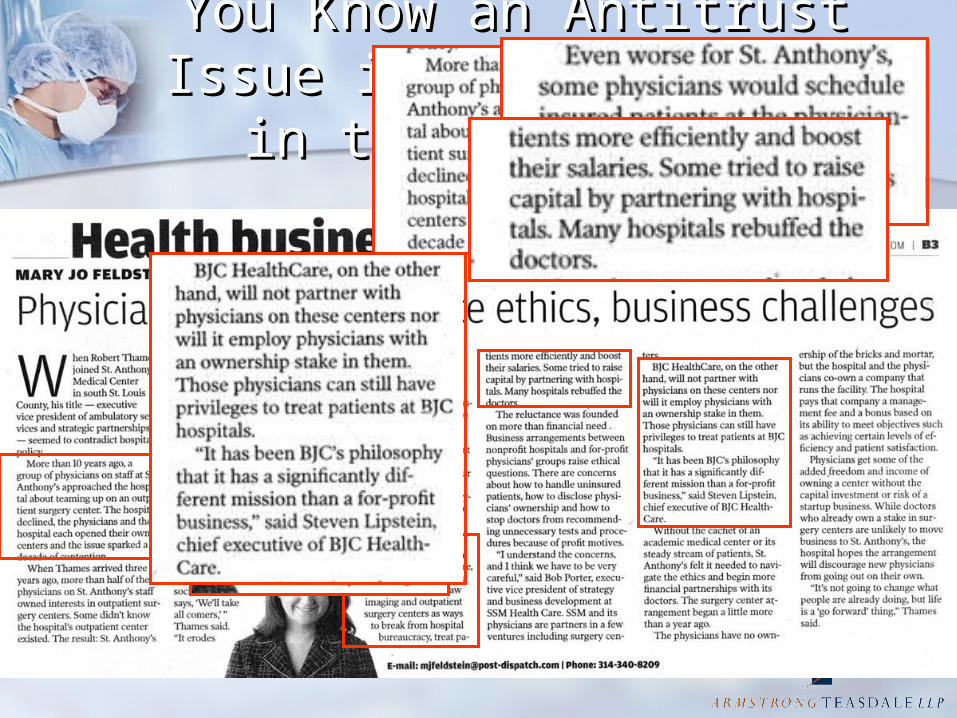
You Know an Antitrust Issue You Know an Antitrust Issue is Hot… When its in the is Hot… When its in the
Newspaper Newspaper
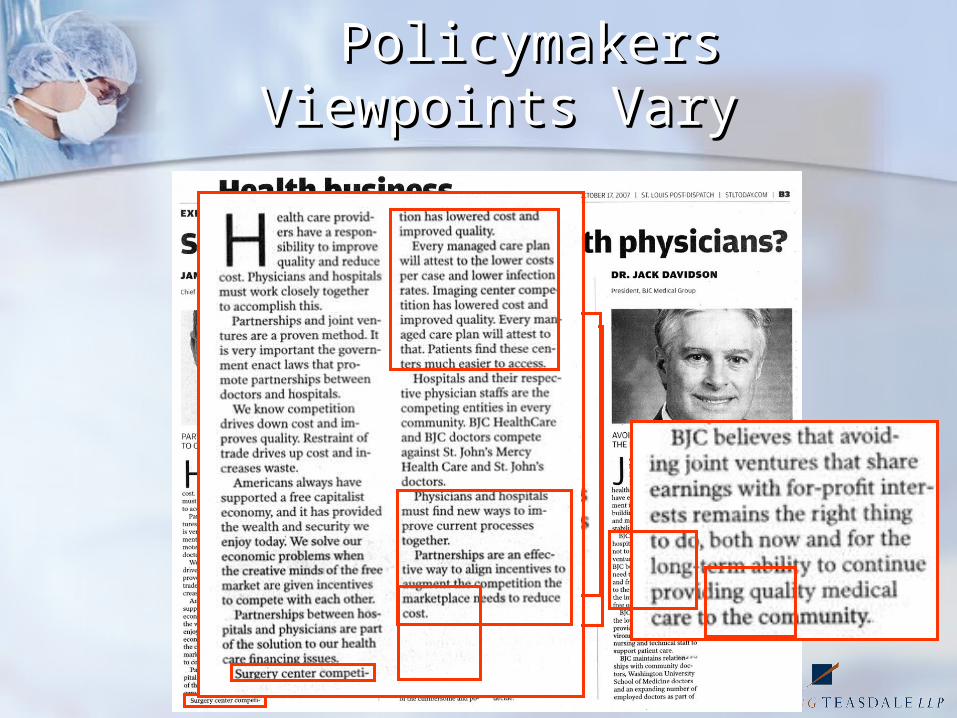
Policymakers Viewpoints Policymakers Viewpoints Vary Vary

Imperfections in Healthcare Imperfections in Healthcare MarketsMarkets
Text book market conditions do not Text book market conditions do not existexist
Hospitals have legal and practical Hospitals have legal and practical obligations to provide careobligations to provide care Regardless of ability to payRegardless of ability to pay Reliance on cost shiftingReliance on cost shifting Cross subsidization of servicesCross subsidization of services
Impact of federal and state Impact of federal and state reimbursement regulationsreimbursement regulations
Managed CareManaged Care Entry and expansion barriersEntry and expansion barriers
Healthcare MarketsHealthcare Markets
Free-riding problemsFree-riding problems Physicians expect support, use of Physicians expect support, use of
facilities & equipment for freefacilities & equipment for free Back up support for exigent Back up support for exigent
circumstancescircumstances Financial survival without access Financial survival without access
even with competing facilityeven with competing facility Yet, physicians bring patients to Yet, physicians bring patients to
hospitals without remunerationhospitals without remuneration
Healthcare MarketsHealthcare Markets
Agency problems in the Agency problems in the physician-hospital relationshipphysician-hospital relationship Information aysmmetry between Information aysmmetry between
physicians and patientsphysicians and patients Selection bias and incentivesSelection bias and incentives
Professional service feesProfessional service fees Profit sharing from facility usageProfit sharing from facility usage
Conflict of interestConflict of interest
Healthcare MarketsHealthcare Markets
Potential for physician actions Potential for physician actions adverse to hospital financial interestsadverse to hospital financial interests Referral of patients requiring higher Referral of patients requiring higher
treatment costs to hospitalstreatment costs to hospitals Referral of less acutely ill patients, less Referral of less acutely ill patients, less
cost intensive procedures to physician cost intensive procedures to physician facilityfacility
Physicians’ supplier induced demandPhysicians’ supplier induced demand Incentives for over-utilizationIncentives for over-utilization
The Policy Battle between The Policy Battle between Physicians and HospitalsPhysicians and Hospitals
Physician/Investors:Physician/Investors: Enhanced consumer choice for lower cost Enhanced consumer choice for lower cost
alternative to hospitalsalternative to hospitals Higher quality, better convenience and Higher quality, better convenience and
amenitiesamenities More efficient delivery of servicesMore efficient delivery of services Permit physicians to control delivery of Permit physicians to control delivery of
servicesservices Permit physicians to supplement Permit physicians to supplement
diminished revenue streams from diminished revenue streams from government and commercial payorsgovernment and commercial payors
The Policy Battle (cont’d)The Policy Battle (cont’d)
Hospitals:Hospitals: Physician cherry picking takes highest Physician cherry picking takes highest
margin business from hospitalsmargin business from hospitals Physicians have unfair advantage in Physicians have unfair advantage in
incentive and ability to control referralsincentive and ability to control referrals Proliferation of facilities results in excess Proliferation of facilities results in excess
capacity, over-utilization, and higher capacity, over-utilization, and higher health care costshealth care costs
Physicians can free ride on hospital Physicians can free ride on hospital capital investment while competingcapital investment while competing
Revenue siphoning threatens ability of Revenue siphoning threatens ability of hospitals to care for uninsured, hospitals to care for uninsured, underinsured, and provide unprofitable underinsured, and provide unprofitable servicesservices
Common Hospital Common Hospital ResponsesResponses
Joint Ventures with physiciansJoint Ventures with physicians Lobbying and CON opposition Lobbying and CON opposition Economic CredentialingEconomic Credentialing
Referral % requirementsReferral % requirements Conflict of Interest policies/ triggered reviewsConflict of Interest policies/ triggered reviews
Exclusive or selective contracting practicesExclusive or selective contracting practices Closure of departmentsClosure of departments
Exclusionary contracts with third-party Exclusionary contracts with third-party payerspayers Network configuration clausesNetwork configuration clauses Bundled service discountsBundled service discounts
Hospital and Medical Staff boycottsHospital and Medical Staff boycotts
Core Antitrust TheoriesCore Antitrust Theories
§1 of the Sherman Act§1 of the Sherman Act Contracts, combinations and conspiracies Contracts, combinations and conspiracies
in restraint of tradein restraint of trade §2 of the Sherman Act§2 of the Sherman Act
Monopolization, attempts to monopolize, Monopolization, attempts to monopolize, and conspiracies to monopolizeand conspiracies to monopolize
§3 of the Clayton Act§3 of the Clayton Act Exclusive dealing and tying arrangementsExclusive dealing and tying arrangements
§5 of the FTC Act§5 of the FTC Act Unfair trade practicesUnfair trade practices
Key IssuesKey Issues
Unilateral conduct versus collusive Unilateral conduct versus collusive conduct in response to market conduct in response to market developmentsdevelopments
Product and geographic market definitionProduct and geographic market definition Assessment of market power (monopoly Assessment of market power (monopoly
and monopsony) facing healthcare and monopsony) facing healthcare professionals, hospitals and health professionals, hospitals and health insurersinsurers
Injury to competition versus competitors Injury to competition versus competitors and consumer welfareand consumer welfare
Impact of recent Supreme Court cases on Impact of recent Supreme Court cases on pleading and proving conspiracies and pleading and proving conspiracies and the scope of antitrust immunities and the scope of antitrust immunities and exemptions exemptions

State Law TheoriesState Law Theories
State antitrust actionsState antitrust actions State unfair competition statutesState unfair competition statutes Tortious interference with Tortious interference with
contracts and/or prospective contracts and/or prospective relationshipsrelationships
Civil conspiracyCivil conspiracy Non-Compete AgreementsNon-Compete Agreements Breach of contractBreach of contract
Regional Antitrust CasesRegional Antitrust Cases
Heartland Surgical Specialty Hospital, Heartland Surgical Specialty Hospital, LLC v. Midwest Division, Inc. d/b/a HCA LLC v. Midwest Division, Inc. d/b/a HCA Midwest Division, et al., Midwest Division, et al., No. 05-2164-No. 05-2164-MLB (D. Kan. 10/1/07)(summary MLB (D. Kan. 10/1/07)(summary judgment)judgment) Plaintiff sued eighteen defendants consisting of
MCO’s and Hospital Defendants Alleged broad conspiracy to boycott plaintiff from
contracting with MCO’s in violation of §1 of the Sherman Act
District Court framed the issues: “[T]his case ultimately involves the proper place of physician-owned healthcare ventures in the broad landscape of United States healthcare Both sides insist they solely possess the moral high ground….Neither side can make a colorable argument that the parties’ profits is not a central factor in their dispute”.
Regional Cases- Regional Cases- HeartlandHeartland
The MCO defendants account for 90% of The MCO defendants account for 90% of managed care enrollment in the Kansas City managed care enrollment in the Kansas City Metro AreaMetro Area
The Hospital Defendants net patient The Hospital Defendants net patient revenue share is 74%revenue share is 74%
Heartland directly competes for hospital Heartland directly competes for hospital based inpatient and outpatient acute care based inpatient and outpatient acute care services in the KC metro areaservices in the KC metro area Owned by orthopedic, neurological, plastic, pain Owned by orthopedic, neurological, plastic, pain
management, and general surgery specialistsmanagement, and general surgery specialists 48 licensed inpatient beds48 licensed inpatient beds Advertised higher standard of care, lower costs, Advertised higher standard of care, lower costs,
lower infection rates, and higher patient lower infection rates, and higher patient satisfaction ratessatisfaction rates
Regional Cases-Regional Cases-HeartlandHeartland
Heartland’s Conspiracy EvidenceHeartland’s Conspiracy Evidence DirectDirect
Unwritten but understood agreement among MCO’s not to extend managed care contracts to SSHs
“Gentlemen’s agreement” among MCO’s to include facilities majority owned by Hospital Defendants in managed care plans
Network configuration agreements excluding SSHs but allowing competing hospitals to include new facilities
Cooperation among hospitals and MCO’s on common network configuration agreement terms
Statements to plaintiff by MCO’s that their contracts prevented them from granting plan access to physician-owned facilities
Regional Cases-Regional Cases-HeartlandHeartland
Heartland’s conspiracy evidence: Circumstantial or indirect:
Initial positive feedback from MCO’s Hospitals shared concerns with threat of freestanding
facilities with each other and MCO’s communicated with each other on strategies
Hospitals recognition of Heartland as a competitor and discussions about threats from specialty hospitals
Hospital statements to MCO’s in public forums that way to protect profit margins was for MCO’s to deny contracts with freestanding facilities
Individual complaints by hospitals to MCO’s to keep freestanding facilities out of MCO networks
MCO’s denied Heartland access without need analysis MCO’s permitted access to new hospital facilities Hospitals agreed to lower reimbursement rates in
exchange for exclusionary provider agreements with network clauses
Regional Cases: Regional Cases: HeartlandHeartland
Court denied summary judgment Court denied summary judgment motions of all but one defendantmotions of all but one defendant Direct evidence weak, but sufficient to Direct evidence weak, but sufficient to
avoid need to produce evidence to exclude avoid need to produce evidence to exclude the possibility of independent actionthe possibility of independent action
Circumstantial evidence given more weight Circumstantial evidence given more weight due to economic plausibility of claimsdue to economic plausibility of claims
Parallel business behavior insufficient to Parallel business behavior insufficient to support claims absent demonstration of support claims absent demonstration of “plus factors”“plus factors”
Interplay of Interplay of Matsushita Matsushita and and Twombly Twombly evidentevident
Regional Antitrust CasesRegional Antitrust Cases
Ferguson Medical Group, L.P. v. Missouri Ferguson Medical Group, L.P. v. Missouri Delta Medical Center, 2006 WL 2225454 Delta Medical Center, 2006 WL 2225454 (E.D.Mo. 2006)(motion to dismiss)(E.D.Mo. 2006)(motion to dismiss) FMG was a long standing physician group located
adjacent to Mo Delta, a regional acute care hospital in Sikeston, MO
FMG expanded into ancillary medical and outpatient diagnostic and surgical services
FMG maintained non-compete agreements with employed physicians
Mo Delta responded with recruitment of FMG physicians, elimination of coverage, limitations on access, and aggressive peer review and credentialing actions alleged to be an attack on FMG
Regional Cases- FMGRegional Cases- FMG
FMG filed a state court action for interference FMG filed a state court action for interference with physician contracts and raiding with physician contracts and raiding
FMG filed a separate federal action for FMG filed a separate federal action for attempted monopolization and conspiracy to attempted monopolization and conspiracy to monopolize against Mo Delta and members of monopolize against Mo Delta and members of its medical staff committees and administration its medical staff committees and administration under under §2 of the Sherman Act and Missouri’s §2 of the Sherman Act and Missouri’s antitrust statuteantitrust statute Complaint alleged defendants attempting to Complaint alleged defendants attempting to
monopolize the market for ancillary medical, monopolize the market for ancillary medical, outpatient diagnostic, and surgical servicesoutpatient diagnostic, and surgical services
Complaint alleged geographic market based on Complaint alleged geographic market based on patient migration data under the patient migration data under the Elzinga-Hogarty Elzinga-Hogarty test, test, consisting of the areas surrounding Sikeston from consisting of the areas surrounding Sikeston from which 80-90% of Mo Delta’s patients actually go to for which 80-90% of Mo Delta’s patients actually go to for services services
Regional Cases- FMGRegional Cases- FMG
Mo Delta moved to dismiss, principally attacking the Mo Delta moved to dismiss, principally attacking the market definition as gerrymanderedmarket definition as gerrymandered
The District Court agreed and dismissed the complaintThe District Court agreed and dismissed the complaint Emphasized critical issue is not where consumers of relevant Emphasized critical issue is not where consumers of relevant
services actually go, but rather where they could practically services actually go, but rather where they could practically turn for alternative careturn for alternative care
FMG failed to adequately plead a viable relevant geographic FMG failed to adequately plead a viable relevant geographic marketmarket
Court influenced by prior experience with defining a relevant Court influenced by prior experience with defining a relevant market in the region in market in the region in FTC v. Tenet Health Care Corp., FTC v. Tenet Health Care Corp., 186 186 F.3d 1045 (8F.3d 1045 (8thth Cir. 1999)(FTC market too narrow in merger Cir. 1999)(FTC market too narrow in merger enforcement action)enforcement action)
Note: this result may or may not be consistent with the FTC’s Note: this result may or may not be consistent with the FTC’s new rejection of patient origin data as a useful tool in defining new rejection of patient origin data as a useful tool in defining geographic markets, and focus on services sold to payors geographic markets, and focus on services sold to payors versus patients in defining product markets in hospital merger versus patients in defining product markets in hospital merger cases. cases. In the Matter of Evanston Northwestern Healthcare In the Matter of Evanston Northwestern Healthcare Corporation Corporation (FTC Opinion)(FTC Opinion)..
FMG, however, vigorously pressed the State Court claims FMG, however, vigorously pressed the State Court claims and the parties entered into a confidential settlementand the parties entered into a confidential settlement
Regional Antitrust CasesRegional Antitrust Cases
Branson Heart Center, P.C. v. The Skaggs Community Branson Heart Center, P.C. v. The Skaggs Community Hospital Association, et. al., Circuit Court, Stone Hospital Association, et. al., Circuit Court, Stone County, MissouriCounty, Missouri Physicians who formed a center for cardiology and interventional Physicians who formed a center for cardiology and interventional
cardiology services sued an acute care hospital in Branson, MO, cardiology services sued an acute care hospital in Branson, MO, alleging attempt to monopolize under Missouri law and various alleging attempt to monopolize under Missouri law and various state tort and breach of contract claimsstate tort and breach of contract claims
Allegations of a campaign to destroy plaintiffs’ financial viability Allegations of a campaign to destroy plaintiffs’ financial viability included:included:
Unreasonable, arbitrary and capricious credentialing and peer review Unreasonable, arbitrary and capricious credentialing and peer review actionsactions
Verbal threatsVerbal threats Creation of adversarial work environmentCreation of adversarial work environment Disseminating false information to hospital employees, other Disseminating false information to hospital employees, other
physicians and the publicphysicians and the public Selective application of hospital policies to interfere with plaintiffs Selective application of hospital policies to interfere with plaintiffs
activitiesactivities Discriminatory and unreasonable false allegations of violations of Discriminatory and unreasonable false allegations of violations of
hospital policies and abuse of disciplinary and review processeshospital policies and abuse of disciplinary and review processes Establishing onerous requirements for interventional procedures to Establishing onerous requirements for interventional procedures to
prevent plaintiffs physicians from obtaining privilegesprevent plaintiffs physicians from obtaining privileges After extensive and contentious discovery and denials of After extensive and contentious discovery and denials of
motions to dismiss, parties entered into a confidential motions to dismiss, parties entered into a confidential settlement settlement
Potential Litigation Game Potential Litigation Game ChangersChangers
Bell Atlantic v. Twombly, Bell Atlantic v. Twombly, __ U.S.__, 127 __ U.S.__, 127 S. Ct. 1955 (2007)S. Ct. 1955 (2007) Class plaintiffs allegations of exclusively parallel Class plaintiffs allegations of exclusively parallel
conduct by major telecommunications providers conduct by major telecommunications providers failed to state a conspiracy claim under failed to state a conspiracy claim under §1 of the §1 of the Sherman ActSherman Act
Complaint failed to plead sufficient facts to Complaint failed to plead sufficient facts to support inference of conspiracy rather than support inference of conspiracy rather than identical but independent actionidentical but independent action
Not a hard core price fixing caseNot a hard core price fixing case What will be required to sustain complaints for What will be required to sustain complaints for
alleged conspiracies in healthcare antitrust cases?alleged conspiracies in healthcare antitrust cases? Clear direction to move beyond notice pleading Clear direction to move beyond notice pleading
under Fed.R.Civ.P. 8 for conspiracy allegations under Fed.R.Civ.P. 8 for conspiracy allegations
Game ChangersGame Changers
Billing v. Credit Suisse First BostonBilling v. Credit Suisse First Boston Underwriters immune from antitrust Underwriters immune from antitrust
liability for actions in connection with liability for actions in connection with underwriting public offeringsunderwriting public offerings
IPO activities “squarely within the IPO activities “squarely within the heartland of securities regulation”; SEC heartland of securities regulation”; SEC regulatory authority and antitrust principles regulatory authority and antitrust principles incompatibleincompatible
What about implied immunity for hospitals What about implied immunity for hospitals in the healthcare arena?in the healthcare arena?
CON requirementsCON requirements HCQIAHCQIA Accreditation Accreditation
The FutureThe Future
Litigated cases are fact intensive and cases will continue to be filedLitigated cases are fact intensive and cases will continue to be filed Twombly Twombly may make it harder to sustain a conspiracy complaintmay make it harder to sustain a conspiracy complaint Characterization and proof of conduct in response to freestanding Characterization and proof of conduct in response to freestanding
facilities as exclusionary and meeting the injury to competition facilities as exclusionary and meeting the injury to competition requirementrequirement
Rural hospitals with more alleged market power may be more Rural hospitals with more alleged market power may be more vulnerablevulnerable
Increase in state court cases to avoid federal treatmentIncrease in state court cases to avoid federal treatment Hospital systems will continue to expand with their own free-standing Hospital systems will continue to expand with their own free-standing
facilitiesfacilities Hospitals should carefully maintain appearance of unilateral action in Hospitals should carefully maintain appearance of unilateral action in
dealing with competitive threats and avoid intertwining conduct with dealing with competitive threats and avoid intertwining conduct with physicians or specialty groups or MCO’sphysicians or specialty groups or MCO’s
Hospitals should carefully consider medical staff development plans, Hospitals should carefully consider medical staff development plans, credentialing criteria, and medical staff and board policies to avoid credentialing criteria, and medical staff and board policies to avoid language that could be misinterpreted as anticompetitivelanguage that could be misinterpreted as anticompetitive
Structure medical staff peer review and credentialing criteria to take Structure medical staff peer review and credentialing criteria to take full advantage of immunity provided in the HCQIAfull advantage of immunity provided in the HCQIA
Both hospital systems and physician groups should consider the public Both hospital systems and physician groups should consider the public interest and their mutual dependence in fashioning relationships with interest and their mutual dependence in fashioning relationships with one another and dealing with perceived threatsone another and dealing with perceived threats
Overcoming the moral high groundOvercoming the moral high ground Board leadership and physician character in litigation mattersBoard leadership and physician character in litigation matters
Helpful SourcesHelpful Sources
CaselawCaselaw Cascade Health Solutions v. PeaceHealth, Cascade Health Solutions v. PeaceHealth, ___ F. 3d ___, 2007 ___ F. 3d ___, 2007
WL 2473229 (9WL 2473229 (9thth Cir. 2007) Cir. 2007) Flegel v. Christian Hospital Northeast-Northwest, Flegel v. Christian Hospital Northeast-Northwest, 4 F.3d 682 4 F.3d 682
(8(8thth Cir. 1993) Cir. 1993) Miller v. Indiana Hospital, Miller v. Indiana Hospital, 843 F.2d (3d Cir. 1988)843 F.2d (3d Cir. 1988) Gordon v. Lewistown Hosp., Gordon v. Lewistown Hosp., 272 F.Supp.2d 393 (M.D. Pa. 2003)272 F.Supp.2d 393 (M.D. Pa. 2003) Williamson v. Sacred Heart Hospital of Pensacola, Williamson v. Sacred Heart Hospital of Pensacola, 1993 WL 1993 WL
543002 (N.D. Fla. 1993)543002 (N.D. Fla. 1993) Surgical Care Center of Hammond. L.C. v. Hospital Service Dist. Surgical Care Center of Hammond. L.C. v. Hospital Service Dist.
No. 1 of Tangipahoa Parish, No. 1 of Tangipahoa Parish, 2001-1 Trade Cas. (CCH) 2001-1 Trade Cas. (CCH) ¶73,215 ¶73,215 (E.D. La. 2001) (E.D. La. 2001) aff’d aff’d 309 F.3d 836 (5309 F.3d 836 (5thth Cir. 2002) Cir. 2002)
Rome Ambulatory Surgery Center, LLC v. Rome Memorial Rome Ambulatory Surgery Center, LLC v. Rome Memorial Hospital, Hospital, 339 F. Supp. 2d 389 (N.D.N.Y. 2004)339 F. Supp. 2d 389 (N.D.N.Y. 2004)
Woman’s Clinic, Inc. v. St. John’s Health System, Woman’s Clinic, Inc. v. St. John’s Health System, 252 F. Supp. 252 F. Supp. 2d 857 (E.D. Mo. 2002)2d 857 (E.D. Mo. 2002)
Little Rock Cardiology Clinic, P.A. v. Baptist Health, Little Rock Cardiology Clinic, P.A. v. Baptist Health, 4-06-cv-4-06-cv-1594-JLH (E.D.Ark. Nov. 2006)1594-JLH (E.D.Ark. Nov. 2006)
Mahan v. Ahera St. Luke’s, Mahan v. Ahera St. Luke’s, 621 N.W. 2d 150 (S.D. 2000) 621 N.W. 2d 150 (S.D. 2000)
Helpful SourcesHelpful Sources
Secondary MaterialsSecondary Materials Robert W. McCann, “Another Dose of Competition,” Robert W. McCann, “Another Dose of Competition,”
Health Law Handbook Health Law Handbook (A. Gosfield ed. 2005)(A. Gosfield ed. 2005) David A. Argue, David A. Argue, An Economic Model of Competition An Economic Model of Competition
Between General Hospitals and Physician-Owned Between General Hospitals and Physician-Owned Specialty Hospitals, Specialty Hospitals, ABA Antitrust Law Section Health ABA Antitrust Law Section Health Care Chronicle, Jul. 2006Care Chronicle, Jul. 2006
John K. Iglehart, John K. Iglehart, The Emergence of Physician-Owned The Emergence of Physician-Owned Specialty Hospitals, Specialty Hospitals, N. Engl. J. Med., Jan. 6, 2005N. Engl. J. Med., Jan. 6, 2005
Elizabeth A. Weeks, Elizabeth A. Weeks, The New Economic The New Economic Credentialing: Protecting Hospitals from Competition Credentialing: Protecting Hospitals from Competition by Medical Staff Members, by Medical Staff Members, 36 J. Health L. (2003)36 J. Health L. (2003)
FTC and U.S. Department of Justice, FTC and U.S. Department of Justice, Improving Improving Health Care: A Dose of Competition, Health Care: A Dose of Competition, Exec. Summ. & Exec. Summ. & Chs. 1 & 3 (2003)(Joint Report)Chs. 1 & 3 (2003)(Joint Report)
Daniel Rubenfeld, Daniel Rubenfeld, 3M’s Bundled Rebates: An 3M’s Bundled Rebates: An Economic Perspective, Economic Perspective, 72 U. Chi. L. Rev. 243 (2005)72 U. Chi. L. Rev. 243 (2005)