Embed Size (px)
Citation preview
Physician and Patient Benefit-Risk Preferences from Two Randomized Long Acting Injectable Antipsychotic Trials
Eva G Katz1*, Brett Hauber2, Srihari Gopal3, Angie Fairchild2, Amy Pugh4, Rachel Weinstein3, Bennett Levitan3
1Janssen Research & Development, LLC, Raritan, NJ, USA; 2RTI Health Solutions, Research Triangle Park, NC, USA; 3Janssen Research & Development, LLC, Titusville, NJ, USA; 4The University of California, San Francisco (UCSF), USA
*Presenting Author
Background: Schizophrenia, a chronic and severe psychiatric disorder, impairs psychosocial functioning, significantly diminishes quality of life, and requires continuous, long-term pharmaceutical treatment. Treatments should balance reducing psychotic symptoms and improving function while minimizing treatment-induced adverse events (AEs). While clinical trials and observational studies provide information on the frequency of symptoms and events, benefit-risk decisions also require judging the clinical impact of these outcomes. These value judgments have traditionally been based on a physician’s perspective, but there is increasing patient group demand and industry and regulatory interest in using patient input for clinical and regulatory decision-making. Purpose: To quantify clinical trial participants’ and investigators’ judgments of the relative importance of benefits and harms of antipsychotic treatments for schizophrenia, and to assess the impact of formulation and adherence on these results. Methods: Discrete-choice experiments were completed by patients with schizophrenia and physician investigators participating in two phase-3 multi-national clinical trials of paliperidone palmitate 3-month long-acting injectable (LAI) antipsychotic. Respondents were asked to choose between hypothetical antipsychotic profiles characterized by efficacy, safety, and mode of administration properties. Data were analyzed using random-parameters logit and probit models. Results: Patients (N=214) and physicians (N=438) preferred complete improvement in positive symptoms to improvement in any other attribute studied. Both preferred 3-month and 1-month injectables to oral formulation (p<0.05), irrespective of prior adherence to oral antipsychotic (OAP) treatment, with greater preference by physicians for a 3-month over a 1-month LAI for nonadherent patients. Physicians were willing to accept LAI treatments with reduced efficacy for patients with prior poor adherence to OAP. The maximum decrease in efficacy (95% confidence interval) physicians would accept for switching a patient from a daily oral to a 3-month injectable were: adherent: 9.8% (7.2–12.4), 20%-nonadherent: 25.4% (21.0–29.9), and 50%-nonadherent: >30%. For patients, up to 10.1% (6.1–14.1) reduction in efficacy would be acceptable for switching an adherent patient to an injectable. For nonadherent patient, no change in efficacy studied was regarded as important. Conclusions: Improvement in positive symptoms is the most important attribute to both patients and physicians. Patients and physicians preferred LAIs over OAPs, with physicians showing greater preference for 3-month over 1-month LAI. Physicians and patients were willing to accept reduced efficacy in exchange for switching a patient from an oral formulation to an LAI.
ABSTRACT
Poster No. P3-10
INTRODUCTION• An understanding of patients’ and physicians’ preferences in choosing an appropriate treatment strategy is
important for effective management of schizophrenia.1,2
• The FDA and EMA have recently recognized the potential value of the patient perspective and the importance of a patient-centric approach to benefit-risk determinations1,3
• This exploratory analysis was performed to identify the key attributes (benefits and harms) of paliperidone palmitate long acting injectable (LAI) and quantify the tradeoffs considered by physicians and patients while balancing these attributes with formulation and adherence.
• The poster presents results of preference surveys administered to trial participants with exacerbated schizophrenia and physician investigators during two phase-3, multinational clinical studies of paliperidone palmitate 3-month (PP3M) formulation.
OBJECTIVE• To quantify clinical trial participants’ and investigators’ judgments of the relative importance of benefits and
harms of antipsychotic treatments for schizophrenia, and to assess the impact of formulation and adherence on these results
METHODSSurvey Respondents• Physicians and patients who participated in one of two phase 3 clinical trials (NCT01515423 or NCT01529515) • Inclusion criteria for physicians: – English speaking physicians who participated as principal investigator or sub-investigator – Had direct contact with patients• Inclusion criteria for patients (all of which must be satisfied): – English speaking patients enrolled at study sites in English-speaking countries (Australia, Canada and USA) – DSM-IV-TR diagnosis of exacerbated schizophrenia for at least 1 year before screening, total Positive and
Negative Syndrome Scale (PANSS) score between 70 to 120 – Symptomatically stable on LAI antipsychotic treatments (including once-monthly PP [PP1M]) other than
PP3M • Exclusion criteria for patients – Active DSM-IV diagnosis other than schizophrenia; suicidal tendency; history of substance dependence
within 6 months before screening; involuntary status in a psychiatric hospital at screening; history of neuroleptic malignant syndrome, tardive dyskinesia, or any malignancy in the previous 5 years except for basal cell carcinoma
– Patients who withdrew or relapsed prior to week 13 of the trial were not issued the surveySurvey Instruments• Two discrete choice experiment (DCE) surveys (one for patients with schizophrenia, and one for psychiatrists)
were incorporated into two pivotal phase-3 trials (NCT01515423 or NCT01529515) as a protocol-prespecified exploratory endpoint requirement.
• DCE was used to quantify the relative importance the respondents assign to the treatment attributes which they judge to be more appropriate for a hypothetical patient. The attributes evaluated aspects of treatment-related efficacy, tolerability, and mode of administration considered by patients when choosing a therapy for themselves or when physicians prescribe a therapy to a patient. The patient and physician surveys included analogous sets of attributes and levels, with labels adapted for each group of respondents.
• Preferences for benefits and risks were obtained by asking respondents (physicians and patients) to make eight judgment choices between pairs of constructed treatment outcomes.
• The survey was administered during the maintenance phases of the trials on a tablet-based computer.
Table 1. Attributes and levels included in the survey choice questionnaireAttributes Levels
First series questions
Improvement in positive symptoms
Very much improvedMuch improvedMinimally improvedNo improvement
Improvement in negative symptoms
Very much improvedMuch improvedMinimally improvedNo improvement
Improvement in social functioningMild problemsModerate problemsSevere problems
Weight gainNone7%15%
Improvement in extrapyramidal symptoms No or YesImprovement in hyperprolactinemia No or YesImprovement in hyperglycemia No or Yes
Second series questions Preferred formulation on the basis of past patient adherence
Oral1-month LAI3-month LAI
LAI: long acting injectable. Positive symptoms: having unusual beliefs, hearing voices, and not trusting people; negative symptoms: difficulty speaking with others or showing emotions; social functioning: decreased interest in social activities; weight gain, extrapyramidal symptoms (Parkinsonism, dyskinesia, dystonia, and/or akathisia), hyperprolactinemia, and hyperglycemia within the first year of starting treatment
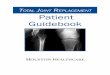
Figure 1. Example Physician Discrete Choice Question (First Set)
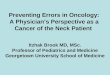
Figure 2. Example Physician/Formulation Choice Question With Follow-Up Adherence Information (Second Set)
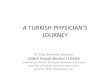
Figure 3. Physician relative importance weights for the main choice questions
Figure 6. Relative importance assigned by patients to second series of choice questions
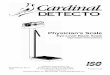
Figure 4. Patient relative importance weights for the main choice questions
A 40-year-old patient with a 20-year history of treated schizophrenia has just been released to your care from a hospital. He was previously stable on his antipsychotic medication but was brought to the hospital when he had an acute exacerbation in symptoms. In this exacerbation, he experienced both severe positive symptoms (e.g., hallucinations, delusions) and severe negative symptoms (e.g., emotional withdrawal, blunted affect). He no longer appears to respond to his current medication, and you need to prescribe a new treatment. The patient has no other comorbidities. The descriptions below show the outcomes the patient will experience after 1 year of treatment. In selecting the better set of outcomes, please do not consider availability or cost of the treatment to your practice or institution or to your patients.
Survey Requirements• Survey requirements were prespecified: respondents were required to complete at least one discrete choice
survey question, and at least one response from each of the two columns (A or B) when all eight questions in the first set of tasks were completed.
• Patient survey duration of at least 7 minutes was pre-specified for a valid attempt.
Statistical Analyses • Random-parameters logit model was used to analyze responses to first series of questions, where the choice
of treatment profile was dependent upon attribute levels, specified as categorical effects-coded variables. This model estimated relative preference weights and importance scores for all attribute levels included in the surveys
• Physicians’ responses to the second series of choice questions were analyzed using a bivariate-probit model that jointly considered respondents’ answers to the primary and follow-up questions and estimated attribute-level weights that maximized the likelihood of both answers by respondents.4
• For patients, preference weights for primary and follow-up questions were computed using separate probit models. The standard errors for both models were standardized to account for correlations between models post-estimation.
Table 2. Demographic characteristics of physicians and patientsPhysicians
Question Survey Physicians (N=438)n (%)
SexMen 255 (58.5)Missing 2 (0.5)
Years in practice<1-3 23 (5.3)4-9 95 (21.8)10-20 162 (37.2)>21 156 (35.8)Missing 2 (0.50)
Average number of schizophrenia patients treated/month<5 9 (2.1)5-20 140 (32.1)21-50 150 (34.4)51-100 94 (21.6)>100 43 (9.9)Missing 2 (0.5)
% of doses of oral antipsychotics patients actually took as prescribed in the past month, as assessed by physiciansMean (SD) 68.5 (15.5)Missing 18 (4.1)
RegionUkraine 71 (16.2)China 50 (11.4)USA 46 (10.5)Russia 45 (10.3)Othera 226 (51.6)
PatientsQuestion Survey Patients (N=214) Trial Patients (N=1935)
n (%) N (%)Age (years), Mean (SD) 40.5 (12.2) 38.4 (11.7)Sex Men 166 (77.6) 1161 (60.0)Race White 79 (36.9) 1077 (55.7) Black or AA 123 (57.5) 223 (11.5) Asian 3 (1.4) 554 (28.6) Other 7 (3.3) 77 (4.0) Multiple 2 (0.9) 4 (4.0)BMI (kg/m2), Mean (SD) 29.1 (5.8) 26.5 (5.1)Age at 1st Schizophrenia diagnosis (years) Mean (SD) 26.6 (10.1) 27.2 (9.0)Total PANSS Score, Mean (SD) 80.1 (14.0) 82.6 (13.2)Preferences on frequency of medicationb
Every day 23 (10.7) 62 (3.2)Every month 96 (44.9) 686 (35.5)Every 3 month 73 (34.1) 1018 (52.6)No preference 15 (7.0) 161 (8.3)Missing 7 (3.3) 8 (0.4)
Preference between pills and injectionsb
Pills 128 (59.8) 433 (22.4)Injection 83 (38.8) 1497 (77.4)Missing 3 (1.4) 5 (0.3)
Civil statusSingle 37 (17.3) n/aMarried/in a long-term partnership 48 (22.4) n/aWidowed 7 (3.3) n/aDivorced 17 (7.9) n/aMissing 105 (49.1) n/a
Taking a depot antipsychotic within 8 weeks prior to entering this studyYes 11 (5.1) 98 (5.1)No 94 (43.9) 295 (15.2)Missing 109 (50.9) 1542 (79.7)
RegionUS 199 (93.0) 325 (16.8)Canada 8 (3.7) 11 (0.6)Australia 7 (3.3) 7 (0.4)Other 0 (0) 1592 (82.3)
BMI, body mass index; n, number of respondents who answered question; n/a, not applicable; PANSS, positive and negative syndrome scale, SD, standard deviation. aIncludes Argentina, Australia, Belgium, Brazil, Bulgaria, Canada, Czech Republic, France, Germany, Greece, Hungary, Japan, Korea, Mexico, Po-land, Portugal, Romania, Slovakia, Spain and Taiwan. Each country represents <5% of physician respondents. b”Preference” in these questions is meant in the convention sense and not as a formal measure of patient preference.
• Second-series preference weights were used to compute the mean maximum acceptable reduction in benefit that would offset increases in utility associated with changes in treatment formulation for hypothetical patients with different levels of past adherence. Both analyses were conducted using NLOGIT 4.0 (Econometric Software, Inc., Plainview, NY, USA).
RESULTSPhysicians Sample• Total 452 physicians from 27 countries completed the survey by answering at least one choice question; 14
physicians were excluded due to selection of same response for all 8 questions from first series.
• Majority of participating physicians were men (255/438, 58.5%); and 73% (318/438) had been practicing medicine for over 10 years.
Patient Sample• A total of 219 patients completed the survey and answered at least one choice question; 5 patients were excluded (selection of same response to 8 questions from first series). • The majority of patients who participated in the survey were men (166/214, 77.6%); African-American
(123/214, 57.5%) with mean age of 40.5 years.Relative Importance Weights for Main Choice Question • For both patients and physicians, improvement in positive symptoms was the most preferred outcome over
the range of levels assessed and was assigned a mean relative importance score of 10.Benefit and risk tradeoffs
EPS: extrapyramidal symptoms. N: number of respondents who answered the question. Note: Each bar represents the improvement in utility associated with switching from the least preferred to the most preferred level of each attribute. The vertical bars surrounding each mean preference weight denote the 95% confidence interval about the point estimate.
N: number of respondents who answered the question; Note: Line plot is used here rather than bar plot, since the preference changes are not monotonic and cannot be represented by single bars. The vertical bars surrounding each mean preference weight denote the 95% confidence interval about the point estimate.
EPS: extrapyramidal symptoms. N: number of respondents who answered the question. Note: Each bar represents the improvement in utility associated with switching from the least preferred to the most preferred level of each attribute. The vertical bars surrounding each mean preference weight denote the 95% confidence interval about the point estimate.
• Physicians considered complete improvement in positive symptoms as the major attribute with the relative importance score of 10 followed by improved social functioning (score: 7.38) and improved negative symptoms (score: 5.19).
• Total negative symptoms improvement was considered half as important as the total improvement in positive symptoms.
• Patients considered complete improvement in positive symptoms (relative importance score: 10) as approximately four times or more as important as the rest of the attributes examined in the survey.
Effect of formulation and adherence
Figure 5. Relative importance assigned by physicians in second series of choice questions
N, number of respondents who answered the question. Note: The vertical bars surrounding each mean preference weight denote the 95% confidence interval about the point estimate.
• Physicians preferred LAI over daily pill (p<0.05) for both adherent and non-adherent patients. • Physicians had greater preference for 3-month LAI over 1-month LAI for patients with a history of skipping
20% (p=0.02) and 50% (p=0.003) doses. • According to physicians, while switching from daily oral pill to 1-month LAI, maximum acceptable reduction in
efficacy for adherent patients was up to 8.9% (95% confidence interval [CI]: 6.4-11.5) with at least minimally improved positive symptoms; for non-adherent patients with 20% and 50% missing doses, decrease in efficacy up to 21.2% (95% CI: 17.3-25.0) and 35.6% (95% CI: 27.8-43.4) was acceptable, respectively.
• Switching from daily oral pill to 3-month LAI, physicians would accept a decrease in efficacy of 9.8% (95% CI: 7.2-12.4), 25.4% (95% CI: 21.0-29.9), and >30% for adherent, 20% nonadherent, and 50% nonadherent patients, respectively.
• Both LAIs (1-month and 3-month) were equally preferred by adherent and non-adherent patients over oral daily pills (p<0.05), with no difference between the two levels of non-adherence levels (20% and 50% missing doses).
• Patients valued increasing efficacy for hypothetical adherent patients (i.e. increasing the percentage of patients with mild versus severe positive symptoms), whereas for non-adherents, the differences in preference weights were very small and not statistically significant, suggesting respondents perceived little value for improvement in efficacy of non-adherent patients.
• The maximum acceptable decrease in efficacy for patients switching form daily oral pill to 3-month LAI was 10.1% (95% CI: 6.1–14.1) for adherent patients.
LIMITATIONS• Stated preferences may differ from observed preferences, or real world decisions. • Both patients and physicians chose to participate in a clinical trial and had to satisfy specific criteria. For these
reasons, our sample may have preferences that differ from the underlying populations.
CONCLUSIONS• Physician investigators and patients preferred treatments mainly on the basis of improvement in positive
symptoms.• Both patients and physicians judged LAIs to be better than the oral formulation regardless of patient’s
adherence, with physicians preferring 3-month over 1-month LAI. • These results provide insight into patients’ and physicians’ preferences to support decision-making.
REFERENCES: 1. Food and Drug Administration (FDA). Enhancing benefit-risk assessment in regulatory decision-making, 2014. Available at: http:// www.fda.gov/ForIndustry/UserFees/PrescriptionDrugUserFee/ ucm326192.htm. Accessed on 4 Sep 2015; 2. Mullard A. Patient-focused drug development programme takes first steps. Nat Rev Drug Discov. 2013;12(9):651-652; 3. European Medicines Agency, “The patient’s voice in the evaluation of medicines. How patients can contribute to assessment of benefit and risk,” October 2013, EMA/607864/2013, available at: http://www.ema.europa.eu/docs/en_GB/document_library/Report/2013/10/WC500153276.pdf. Accessed on 4 September 2016; 4. Hanemann M, Loomis J, Kanninen B. Statistical efficiency of double-bounded dichotomous choice contingent valuation. American Journal of Agricultural Economics. 1991;73(4):1255-1263.
ACKNOWLEDGMENTS: We acknowledge Ashwini Patil, ISMPP CMPPTM (SIRO Clinpharm Pvt. Ltd.) for medical writing support, and Ellen Baum, PhD (Janssen Research & Development, LLC) for additional editorial support for the development of this poster.
AUTHOR CONTRIBUTIONS: Drs. Katz, Levitan, Gopal, Fairchild, Hauber, Pugh and Weinstein contributed to the design of this study, data analysis, interpretation and authorship. All authors met ICMJE criteria and all those who fulfilled those criteria are listed as authors. All authors had access to the study data, provided direction and comments on the poster, had final approval of the document and made the final decision about where to present these data.
DISCLOSURES: Drs. Katz, Gopal, Levitan, and Weinstein are employees of Janssen, and hold company stocks. Dr. Levitan is also a stockholder in Baxter International, Inc., Pharmaceutical Holdrs Trust, and Zimmer Holdings, Inc. Dr. Levitan also owns stock in a variety of companies that at times include pharmaceutical and health care-related companies. Dr. Hauber is an employee of RTI Health Solutions. Drs. Pugh and Fairchild were employees of RTI Health Solutions at the time this study was conducted.
Funded by Janssen Research & Development, LLC Presented at American Psychiatric Association IPS: Mental Health Services Conference, October 6-9, 2016, Washington D.C., USA