Embed Size (px)
Citation preview

Investigational New Drugs 4: 171-174, 1986 �9 Martinus Nijhoff Publishers, Boston - Printed in the Netherlands
Phase II trial of 10 deaza-aminopterin in patients with bladder cancer
Tauseef Ahmed ~' *, Alan Yagoda 2, Howard I. Scher ~, Cora Sternberg I & Robin C. Watson 3 I Fe l lowj Medical Oncology, 2Attending Physician, Solid Tumor Service, 3Chief, Department o f Radiology; Memorial Sloan Kettering Cancer Center, 1275 York Avenue, New York, N Y 10021
Summary
Deaza-aminopterin is a folate analog which is transported more rapidly than methotrexate into cells and ap- pears to be more active than methotrexate against human and animal tumor in vitro. Fifteen patients with advanced urothelial tract cancer were given deaza-aminopterin 30-37.5 mg/m ' IV QW. In responding pa- tients drug was given QOW after 4 - 6 consecutive doses. Doses were escalated or de-escalated by 7.5 mg/m 2 depending on toxicity. Twelve patients had received prior chemotherapy which included methotrexate in nine. Three patients achieved a partial remission lasting 1, 3, and 3 months respectively: all responders had previously failed methotrexate after an initial response to a methotrexate containing regimen. None of the six patients who were methotrexate naive responded to deaza-aminopterin; 3 subsequently received metho- trexate without response. Mild mucositis was universal and in 5 was severe. Six patients had an increase in liver transaminases probably secondary to anti-folate hepatotoxicity. Other toxicities included diarrhea, nausea, skin rash and fever. Further studies are needed to define the precise efficacy of deaza-aminopterin in patients with urothelial tract cancers.
Introduction
Transitional cell carcinoma of the urothelial tract is a chemotherapeutically responsive tumor. Metho- trexate is one of the single most active agents against this tumor demonstrating a complete and partial remission rate in 29~ of patients (1). Although response duration to low dose methotrex- ate, 30 -40 mg/m 2 IV QW is generally short-lived, a clear-cut dose-response relationship for metho- trexate in patients with bladder cancer has not been established (2). Sirotnak, et al. have demonstrated that at least part of the anti-tumor effects of anti- folate drugs are regulated at the level of the cell membrane (3).
10-deaza-aminopterin is an aminopterin deri-
vative with an azo group at position 10 (4). Alkyla- tion at the N 1~ position increases the differential up- take relative to methotrexate in murine and human tumor cells in vitro (5). Compared to methotrexate, deaza-aminopterin demonstrates a two to three fold greater anti-tumor effect in certain tumors especial- ly Sarcoma 180, Ehrlich carcinoma, and the Taper liver tumor (3). A recent Phase I trial which sug- gested a dose of 37.5 mg/m 2 as the ideal starting dose for Phase II trials described mucositis, and drug-induced hepatitis as frequent toxicities (6). A Phase II disease-oriented drug trial of deaza- aminopterin was undertaken at Memorial Sloan- Kettering Cancer Center in patients with advanced bidimensionally measurable transitional cell car- cinoma of the urothelial tract.
Address f o r offprints: Dr Alan Yagoda, Memorial Sloan Kettering Cancer Center, 1275 York Ave., New York, NY 10021. * Present address: Director of Bone Marrow Transplantation Services, Division of Neoplastic Diseases, New York Medical College, Valhalla, NY 10595.
172
Materials and methods
Patients with advanced, pathologically confirmed transitional cell carcinoma were eligible to receive deaza-aminopterin provided they had adequate blood counts: WBC > 4,000 cells/ram 3, platelets > 150,000 cel ls /mm 3, Karnofsky performance
status (KPS) > 50%, bilirubin < 1.0 mg%, BUN < 30 mg%, creatinine < 1.5 mg% and bidimen- sionally measurable parameters for indicator le- sions. All patients had a complete history and physical examination with measurement of the two longest perpendicular diameters, o f all palpable lesions by two independent investigators. Prior to each dose a CBC, and a platelet count was obtain- ed, 12 channel biochemical screening profile and serum creatinine were obtained every 2 - 4 weeks. Chest roentgenograms, were performed every three
to six weeks. In selected cases computerized trans- axial tomograms (CT scans) were performed initial- ly and repeated every six weeks to evaluate disease activity. All x-rays and scans were evaluated in- dependently (RCW).
All chemotherapy was stopped at least three weeks prior to the start of protocol. The initial starting dose was 37.5 m g / m 2 IV weekly. Patients with ileal conduits or borderline renal function (i.e. creatinine > 1.3 mg%) received 30 m g / m 2 q week. Depending on whether the patient experienced
mucositis or severe myelosuppression, dose escala- tion or de-escalation by 7.5 m g / m 2. Patients re- ceiving more than two doses of the drug with toxi- city were deemed to have undergone an adequate trial.
Response criteria included: complete remission (CR), complete disappearance of clinical radio- graphic and biochemical evidence of tumor for at least one month; partial remission (PR), predicted > 50~ decrease in the summed products of per- pendicular diameters of all measurable lesions for one month; minor response (MR), denoted a 25 to 49070 decrease in measurable lesions for one month; stabilization (STAB), < 2507o change in tumor size for 3 months; and progresssion (PROG), a > 250/o increase in tumor size.
Mucositis was graded according to the following scale: 1 + = mild ulcerations, normal diet: 2 + =
food intact impaired, IV fluids not required; 3 + = Intravenous fluids required; 4 + = life-threatening hospitalization imperative.
Results
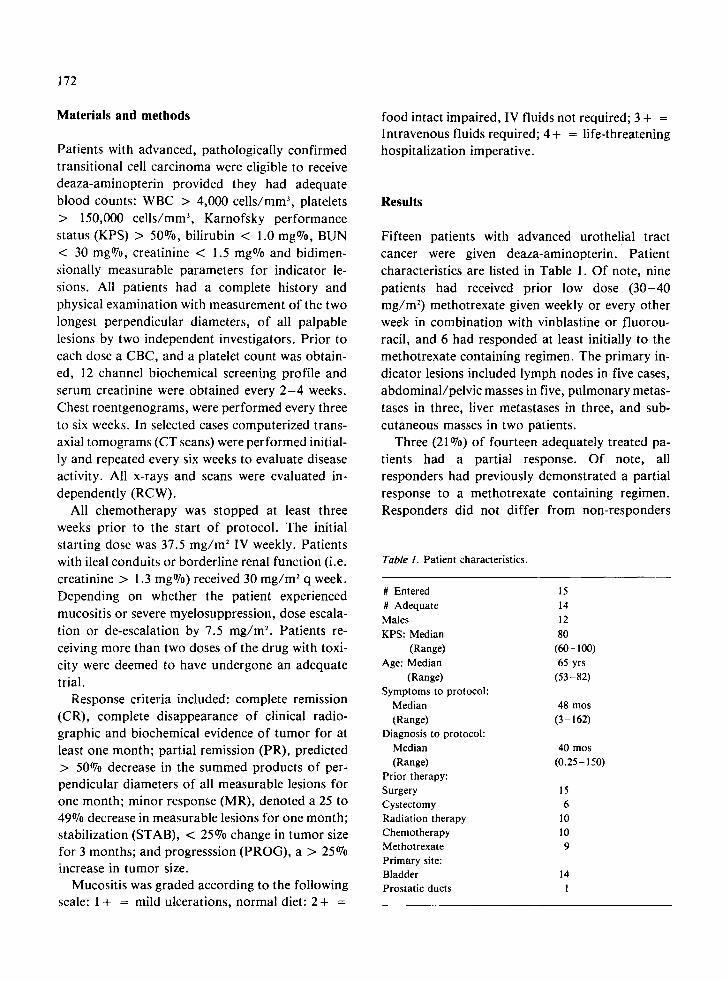
Fifteen patients with advanced urothelial tract cancer were given deaza-aminopterin. Patient characteristics are listed in Table 1. Of note, nine patients had received prior low dose (30-40 m g / m 2) methotrexate given weekly or every other week in combination with vinblastine or fluorou- racil, and 6 had responded at least initially to the methotrexate containing regimen. The primary in- dicator lesions included lymph nodes in five cases, abdominal /pelvic masses in five, pulmonary metas-
tases in three, liver metastases in three, and sub- cutaneous masses in two patients.
Three (21 ~ of fourteen adequately treated pa- tients had a partial response. Of note, all responders had previously demonstrated a partial response to a methotrexate containing regimen. Responders did not differ from non-responders
Table 1. Patient characteristics.
# Entered 15 # Adequate 14 Males 12 KPS: Median 80
(Range) (60-100) Age: Median 65 yrs
(Range) (53-82) Symptoms to protocol:
Median 48 mos (Range) (3-162)
Diagnosis to protocol: Median 40 mos (Range) (0.25-150)
Prior therapy: Surgery 15 Cystectomy 6 Radiation therapy 10 Chemotherapy 10 Methotrexate 9 Primary site: Bladder 14 Prostatic ducts 1
with regard to age or performance status. Remis- sion duration was short with deaza-aminopterin lasting 1, 3 and 3 months respectively. Responding sites included skin nodules in one patient, palpable lymph nodes in another, and pulmonary masses measured by chest x-ray in the third. One patient had a partial response in a lymph node involved with metastatic transitional cell carcinoma. He developed brain metastases more than one month after having a partial remission and while still responding to deaza-aminopterin systemically. Of the six patients who had not received prior metho- trexate and three patients who had not responded to methotrexate, none responded to deaza-amino- pterin. Three patients were subsequently treated with low dose methotrexate on a weekly schedule without evidence of tumor regression, although one did have a partial response to a combination of cis- platin and doxorubicin.
One patient received two doses of deaza-amino- pterin, developed severe 4+ mucositis and was taken off protocol. The other fourteen patients received a median of 5 doses (range 3-12) . Eight patients were started at 37.5 mg/m 2 and seven at 30 mg/m 2. Only one patient was able to tolerate deaza- aminopterin well enough at 37.5 mg/m 2 to be escalated to 45 mg/m-'. Of the six patients treated at the 30 mg/m ~ dose level, only one could be escalated to 37.5 mg/m 2. Two of the three respond- ing patients were treated with deaza-aminopterin at the 30 mg/m 2 dose level. Dose attenuation was re- quired in six patients on account of mucositis.
The toxicity of deaza-aminopterin appeared similar to that of methotrexate. Mucositis was the most frequent side effect and was noted in 14 (95%) cases, generally occurring after a median of two doses (range 1 to 5). Severe (Grade 3 -4 ) mucositis was observed in five patients. Abnormalities of liver function tests defined as doubling the SGOT or serum bilirubin higher than 1.5 mg% were noted in six (40%) cases. The median number of doses given prior to the detection of abnormalities of liver function tests was four (range 2 to 6). A liver biopsy disclosed changes compatible with antifolate in- duced hepatotoxicity in one patient. This patient progressed to hepatic failure and died. Significant myelosuppression was not a major problem: the
173
median nadir WBC count was 5.2 x 103 cells/mm ~ (range 0.6 to 6.8) and the median nadir platelet count was 200 x 103 cells/mm 3 (range 44 to 284). Diarrhea was noted in two patients, while nausea, skin rash, and fever were noted in one instance each. Significant nephrotoxicity was not seen.
Discussion
Antifolate drugs have demonstrated activity against a variety of human tumors. The therapeutic efficacy of folate analogs can be increased by en- hancing the transport of the drug into neoplastic tissue. Sirotnak and co-workers have demonstrated that the cell membrane is crucial in regulating drug transport into the cell (7). Whether deaza-amino- pterin is superior to high dose methotrexate with citrovorum factor rescue is unclear. In bladder cancers moderately high dose methotrexate, i.e., 250 to 1500 mg/m 2 with citrovorum factor rescue did not appear to be superior to conventional dose methotrexate i.e. 30 to 40 mg/m 2 (2). High dose methotrexate did in fact, in these trials, appear to be more toxic.
It was interesting that only patients who had previously demonstrated an initial response to methotrexate responded to deaza-aminopterin. Methotrexate enters cells by energy dependent, temperature sensitive, and concentrative process that probably depends on a specific intramembrane protein (8). There appears to be a positive corre- lation between drug response and transport (9). Defective transport has been reported as a mechanism of drug resistance in experimental systems (10, 11). Compared to methotrexate, deaza-aminopterin is transported more rapidly into tumor cells, and appears to be more active in vitro (5).
Further trials are necessary to define the role of deaza-aminopterin in the treatment of patients with advanced urothelial tract cancer. However, based on these preliminary data it appears that patients with advanced bladder cancer may respond to deaza-aminopterin after becoming refractory to methotrexate containing regimens.

174
Acknowledgements
Dr. Scher is a recipient of the Untermeyer Fellow- ship.
This study was supported in part by CA-05826.
References
1. Ahmed T, and Yagoda A: Chemotherapy of advanced uroo thelial tract cancer. In A comprehensive guide to the therapeutic use of methotrexate in bladder cancer: Hall RR (ed): Pharmalibri, Chicago, 1983 pp. 27-50
2. Natale RB, Yagoda A, Watson RC, Whitmore WF, Jr., Blumenreich M, Braun DW, Jr: Methotrexate: an active drug in bladder cancer. Cancer 47:1246-1250, 1981
3. Sirotnak F, DeGraw J, Chello P, Moccio D, Dorick D: Biochemical and pharmacological properties of a new folate analog, 10-deaza-aminopterin, in mice. Cancer Treat Rep 66:351-358, 1983
4. Sirotnak F, DeGraw J, Moccio D, Dorick D: Antitumor properties of a new folate analog 10-deaza-aminopterin in mice. Cancer Treat Rep 62:1047-1052, 1978
5. Moccio D, Sirotnak F, Samuels L, Ahmed T, Yagoda A, DeGraw J, Piper J: Similar specificity of membrane transport for folate analogues and their metabolites by murine and human tumor cells: a clinically directed laboratory study. Cancer Res 44:352-257, 1984
6. Currie V, Warrell RP, Arlin Z, Tan C, Sirotnak F, Greene G, Young C: Phase I trial of 10-deaza-aminopterin in pa- tients with advanced cancer. Cancer Treat Rep 67:149-154, 1983
7. Sirotnak F, Chello P, Brockman R: Potential for exploita- tion of transport systems in anticancer drug design. Methods Cancer Res 16:382, 1979
8. Goldman ID, Lichetenstein NS, Olivero VT: Carrier- mediated transport of the folic acid analog, methotrexate, in the Ll210 leukemia cell. J Biol Chem 243:5007-5617, 1968
9. Kessel D, Hall TC, Roberst D: Uptake as a determinant of methotrexate in mouse leukemias. Science 150:752-754, 1965
10. Hill BT, Bailey BD, White JC et al.: Characteristics of transport of 4-amino antifolates and folate compounds by two lines of LSI87Y lymphoblasts, one with impaired transport of methotrexate. Cancer Res 39:2440-2446, 1979
I I. Sirotnak FM: Correlates of folate analog transport, phar- macokinetics and selective anti-tumor action. Pharmacol Ther 8:71-103, 1980







![Intestinal metaplasia of the bladder in 89 patients: a ...Oct 10, 2015 · bladder extrophy, long-term catheterization, bladder calculi and neurogenic bladder [1]. The presence of](https://img.pdfslide.us/doc/110x75/60b92038f4dd374d6469d737/intestinal-metaplasia-of-the-bladder-in-89-patients-a-oct-10-2015-bladder.jpg)