Embed Size (px)
DESCRIPTION
kanker vesica urinaria
Citation preview
Bladder Cancer

Epidemiology of Bladder CA• Accts for > 90% of UG tumors
• 4th most common CA in men, 9th in women
• Annual New Cases = 68,810 (51,230 in M & 17,580 in F)– M:F = 3:1, similar w/in all racial groups
• Annual Deaths = 14,100 (7,750 in M & 4,150 in F)
• Caucasians ~ 2x > African Americans > Hispanics & Asians
• Median age at dx = 70. Rarely dx’d before age 40.

Risk Factors for Bladder CA• Age, Gender, Race
• Cigarette smoking (2-4x higher relative risk)
• Exposures– Occupational - Polycyclic aromatic hydrocarbons, benzidine, benzene,
exhaust from combustion gases, arylamines • Al+3 workers; dry cleaners; manufacturers of preservatives,
polychlorinated biphenyls, dye, rubber, & leather; pesticide applicators; painters; truck drivers; hairdressers; printers; machinists
– Cyclophosphamide, Ifosfamide ( 9 fold inc’d risk)– Pelvic radiation txs– Arsenic (eg, in drinking H2O)

Risk Factors for Bladder CA• Infections– Schistosoma haematobium (N Africa) Inc’d risk for
squamous & transitional cell CAR – Chronic UTIs, chronic bladder stones, indwelling Foleys inc’d
risk for squamous cell CAR
• Other– Prior h/o bladder CA– Low fluid intake (inc’d exposure to carcinogens via dec’d bladder
emptying)– Genetics (eg, Retinoblastoma gene)– Bladder birth defects (eg, persistent urachus) inc’d risk for
adenoCAR

Pathology of Bladder CA• Transitional cell CAR (> 95%)
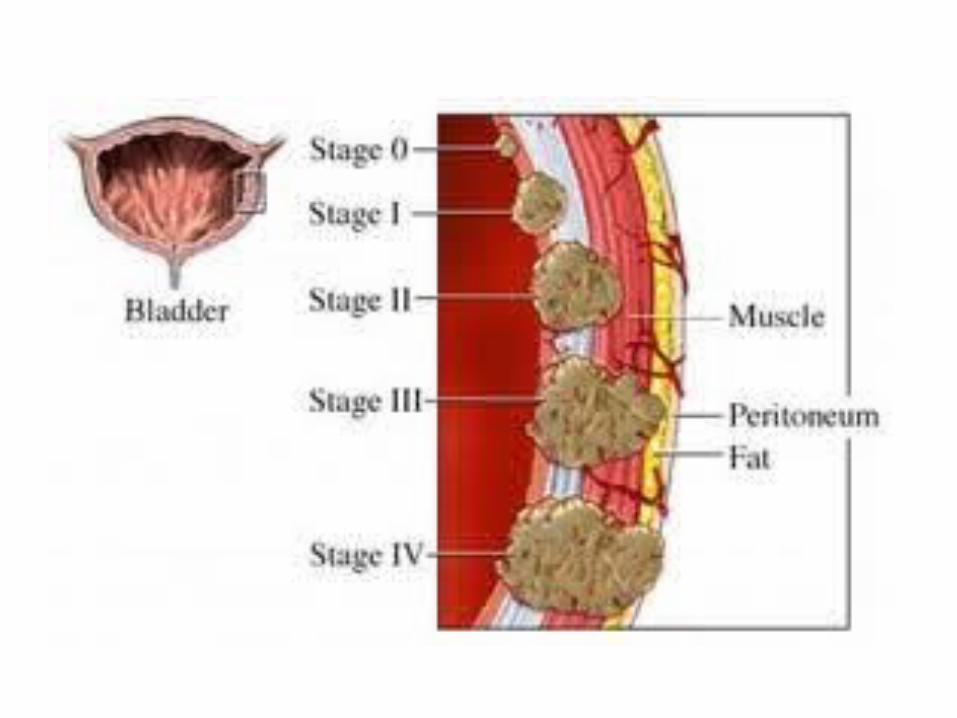
– Papillary (70%) – Grow toward the hollow part of the bladder w/o invading deeper tissues. Often non-invasive.
– Flat – Do not grow toward the hollow part of the bladder. Can be non-invasive or invasive depending on depth of invasion
• Squamous cell (keratinizing) CAR (1-3%) – Generally invasive.
• AdenoCAR (1-2%) – Generally invasive.
• Small cell CAR (< 1%)
• Mixed-histology (predominantly transitional cell w/ areas of other elements) are also common.

Clinical Manifestations of Bladder CA
• Hematuria (80-90%) – Generally painless and gross hematuria– However, 20% can have only microscopic hematuria
• Other urinary Sxs – Frequency, urgency, nocturia – d/t irritative Sxs or dec’d bladder
capacity
• Pain (less common & often reflects tumor location)– Lower abdominal pain – Bladder mass– Rectal discomfort & perineal pain – Invasion of prostate or
pelvis. – Flank pain - Obstruction of ureters

Dx of Bladder CA
• Screening of aSx’c pts not recommended
• Pts w/ hematuria, especially if > 40 yoa – Urinary Cytology – Cystoscopy, regardless of cytology results
(mainstay of dx)– Transurethral resection of all visible tumors to
determine histology & depth of invasion– Biopsies of erythematous (& possibly normal)
areas to assess for CIS


Dx of Bladder CA
• Pts w/ (+) cytology but no apparent bladder tumors and/or (-) biopsies – Intravenous peylogram or CT urogram to evaluate for upper
urinary tract dz
• Imaging – Generally only if (+) cystoscopy– U/S, CT, or MRI - Can help determine extent of tumor spread
(eg, into perivsesical fat, prostate or vagina, LNs)– CT chest / abdomen, MRI, radionuclide imaging of skeleton to
assess for distant mets

Tx & Prognosis of Bladder CA – Superficial Dz
• ~ 50% have recurrences, w/ 5-30% of these progressing to a more advanced stage
• Requires at least complete endoscopic resection +/- intravesical therapy
• Surveillance via cystoscopy & urine cytology – Q3 mos x 1 yr, Q4 mos x 1yr, Q6 mos x 1 yr
• Periodic surveillance of upper GU tracts
• Tx for persistent dz = repeat BCG or cystectomy

Tx & Prognosis of Bladder CA – Intravesical Therapy
• Indications– Adjuvant tx w/ resection to prevent recurrence– Eliminate dz that cannot be controlled by endoscopic resection alone
(less common)– Recurrent dz, > 40% involvement of bladder surface, diffuse CIS, T1 dz – Generally not needed for solitary papillary lesions
• Agents– Std agent -- BCG
• Generally 6 weekly txs then monthly maintenance x 1-3 yrs• Toxicities = Bladder irritability / spasm, hematuria, dysuria, & rarely
systemic TB– Other agents – Mitomycin-C, Interferon, Gemcitabine
Tx & Prognosis of Bladder CA – Muscle-Invasive Dz
• Generally radical cystectomy & pelvic lymphadenectomy unless significant metastatic dz– Removal of bladder & pelvic LNs w/ creation of a conduit or
reservoir for urinary flow.– + Removal of prostate, seminal vesicles, & proximal urethra in
males. Generally impotence.– + Removal of urethra, uterus, fallopian tubes, ovaries, anterior
vaginal wall, & surrounding fascia in females.– 5-yr dz-free survival in 75-80% w/ organ-confined dz; ~ 50%
w/ tumors extending into the perivesical tissues, & in ~ 33% w/ mets to regional LNs.

Tx & Prognosis of Bladder CA – Muscle-Invasive Dz
• Neo-adjuvant chemo x 12 wks prior to cystectomy– Inc’d 5-yr dz-free survival– MVAC (Methotrexate, Vinblastine, Doxorubicin, Cisplatin) – 3
cycles q 28 days
• Concomitant Chemo & Radiation– For those w/ a solitary early-stage lesion and no hydronephrosis– Generally Cisplatin– 5-yr dz-free survival rate of 50%,

Tx & Prognosis of Bladder CA – Muscle-Invasive Dz
• Sometimes bladder sparing approach is used (~ 5-10% are candidates) – Complete endoscopic resection; partial
cystectomy; or combination of resection, chemo, and radiation
– Considered when dz is limited to the bladder dome, 2 cm can be achieved, no CIS in other sites, & bladder capacity adequate after tumor removal.

Tx & Prognosis of Bladder CA – Muscle-Invasive Dz – Mgmt of Urine
Flow• Conduit Diversion – Urine is drained from the ureters to a loop of small bowel anastomosed to the
abdominal skin surface. It is then collected in an external appliance. Currently uncommonly used.
• Continent Cutaneous Reservoir – Created from a detubularized segment of bowel attached to the abdominal wall w/
a continent stoma that can be regularly self-cath’d. – Continence in 65–85% of men at night and 85–90% of men during the day.
• Orthotopic Neobladder– Low-pressure reservoirs anastomosed to the urethra more natural drainage, as
pts can void via the urethra. – CI’s = Renal insuff, inability to self-catheterize, or an exophytic tumor or CIS in the
urethra.

Tx & Prognosis of Bladder CA – Metastatic Dz
• 2 Main Regimens (Gemcitabine + Cisplatin OR MVAC)– 6 cycles over 6 mos– GC is often better tolerated.– Both 5 yr survival rate of ~ 15% (20-33% if good
performance status and mets confined to LNs), w/ median survival of ~ 14 mos.

References• Harrison’s Internal Medicine• Cecil Textbook of Medicine• Cancer: Principles & Practice of Oncology• National Cancer Institute website• American Cancer Society website

























![Women and Bladder Cancer - Oncoscan yellow 8-20_.pdf · bladder cancer [18,170] than cervical cancer [11,270] > 500,000 people in the U.S. have/had bladder cancer – highest recurrent](https://img.pdfslide.us/doc/110x75/5f694c18ea002e289e4b0db0/women-and-bladder-cancer-yellow-8-20pdf-bladder-cancer-18170-than-cervical.jpg)