Embed Size (px)
Citation preview

Cancer Therapy: Clinical
Phase I Dose-Escalation Study of the Safety, Pharmacokinetics,and Pharmacodynamics of the MEK Inhibitor RO4987655(CH4987655) in Patients with Advanced Solid Tumors
Suzanne Leijen1, Mark R. Middleton3, Patricia Tresca4, Francoise Kraeber-Bod�er�e5, Veronique Dieras4,Max E. Scheulen6, Avinash Gupta3, Vanesa Lopez-Valverde8, Zhi-Xin Xu8, Ruediger Rueger7,Jean J.L. Tessier8, Eliezer Shochat8, Steve Blotner9, Valerie Meresse Naegelen8,Jan H.M. Schellens1,2, and Wilfried Ernst Erich Eberhardt6
AbstractPurpose: This phase I study of the mitogen-activated protein/extracellular signal–regulated kinase
inhibitor RO4987655 (CH4987655) assessed its maximum tolerated dose (MTD), dose-limiting toxi-
cities (DLT), safety, pharmacokinetic/pharmacodynamic profile, and antitumor activity in patients with
advanced solid tumors.
Patients and Methods: An initial dose escalation was conducted using a once-daily dosing schedule,
with oral RO4987655 administered at doses of 1.0 to 2.5 mg once daily over 28 consecutive days in 4-week
cycles. Doses were then escalated from 3.0 to 21.0 mg [total daily dose (TDD)] using a twice-daily dosing
schedule.
Results: Forty-nine patients were enrolled. DLTs were blurred vision (n ¼ 1) and elevated creatine
phosphokinase (n¼ 3). TheMTDwas 8.5mg twice daily (TDD, 17.0mg). Rash-related toxicity (91.8%) and
gastrointestinal disorders (69.4%) were the most frequent adverse events. The pharmacokinetic profile of
RO4987655 showed dose linearity and a half-life of approximately 4 hours. At the MTD, target inhibition,
assessed by suppression of extracellular signal–regulated kinase phosphorylation in peripheral blood
mononuclear cells, was high (mean 75%) and sustained (90% of time >IC50). Of the patients evaluable
for response, clinical benefit was seen in 21.1%, including two partial responses (one confirmed and one
unconfirmed). 79.4% of patients showed a reduction in fluorodeoxyglucose uptake by positron emission
tomography between baseline and day 15.
Conclusion: In this population of heavily pretreated patients, oral RO4987655 showed manageable
toxicity, a favorable pharmacokinetics/pharmacodynamics profile, and promising preliminary antitumor
activity, which has been further investigated in specific populations of patients with RAS and/or RAF
mutation driven tumors. Clin Cancer Res; 18(17); 4794–805. �2012 AACR.
IntroductionConstitutive activation of the Ras-regulated mitogen-
activated protein kinase (MAPK) signaling cascade has beenidentified in various human cancers. The MAPK cascadecomprises 3 enzymes (RAF/MEK/ERK) involved in regula-tion of cell proliferation, differentiation, survival, andmigration (1, 2). Mutations of the Ras proto-oncogenes(KRAS, HRAS, and NRAS) have been found in approxi-mately 30% of cancers (3), whereas BRAF gene mutationshave been identified in up to 66%ofmalignantmelanomas(4).
Mitogen-activated protein kinase kinase (MEK) is theonly known kinase capable of phosphorylating ERK; there-fore, inhibition of MEK can potentially block the activationof multiple downstream pathways. Several small-moleculeinhibitors of MEK are currently being investigated (5–14).RO4987655 is a highly selective adenosine triphosphatenoncompetitive oral MEK inhibitor that has shown
Authors' Affiliations: 1The Netherlands Cancer Institute, Amsterdam;2Department of Pharmaceutical Sciences, Utrecht University, Utrecht, TheNetherlands; 3Oxford NIHR Biomedical Research Centre, Department ofOncology, University of Oxford, Churchill Hospital, Oxford, United King-dom; 4Medical Oncology Department, Institut Curie, Paris; 5Department ofNuclear Medicine/Center for PET/CT, University Hospital and ICO, Ren�eGauducheau Cancer Center, INSERM Unit 892, Nantes, France; 6Depart-ment of Medicine (Cancer Research), West German Cancer Center, Uni-versity Hospital Essen, Essen; 7Roche Diagnostics GmbH, Penzberg,Germany; 8F.Hoffmann-La Roche Ltd., Basel, Switzerland; and 9F.Hoff-mann-La Roche Ltd., Nutley, New Jersey
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
V. Lopez-Valverde, Z.-X. Xu, J.J.L. Tessier, E. Shochat, and M. Naegelenare the members of Roche Pharma Research & Early Development (pRED)Oncology Clinical group.
Corresponding Author: Jan H.M. Schellens, The Netherlands CancerInstitute, Amsterdam, The Netherlands. Phone: 31-0-20-512-24-46; Fax:31-20-512-2572; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-12-0868
�2012 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 18(17) September 1, 20124794
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

promising antitumor activity in a series of human cancerxenograft models [non–small-cell lung cancer (NSCLC),pancreatic cancer, and hepatocellular carcinoma; ref. 15].RO4987655 has a unique ring structure with a high met-abolic stability and slowdissociation fromMEK,whichmayconfer better clinical efficacy compared with other MEKinhibitors (15). In a study of healthy volunteers, once-onlysingle doses of oral RO4987655 (0.5–4 mg) were found tobe safe and well tolerated (16). Toxicity was typically mild/moderate, themost commonadverse events (AE) being skinrelated or gastrointestinal (16). Target effect was assessed bymeasuring the level of phosphorylated ERK (pERK) inperipheral blood mononuclear cells (PBMC), whichshowed pERK inhibition of >80% at higher RO4987655doses (16).The objectives of this study were to determine the max-
imumtolerated dose (MTD), dose-limiting toxicities (DLT),the pharmacokinetics/pharmacodynamic profile, safetyand tolerability, and preliminary antitumor activity ofRO4987655 in a population of patients with advancedcancers (17).
Materials and MethodsPatient selectionPatients selected were aged 18 years or older with
advanced or metastatic solid tumors for which no standardtherapy was available. All patients had an Eastern Cooper-ative Oncology Group performance status (ECOG-PS) of�1, evaluable and/or measurable disease according toResponse Evaluation Criteria In Solid Tumors (RECIST,v1.0; ref. 18), a life expectancy of�12 weeks, and adequateorgan functions (see Supplementary Information for fullinclusion/exclusion criteria). Patients with a history ofocular disorders or other known risk factors were excluded,as were patients who had received recent corticosteroids orhormone therapy (within 2 weeks of first planned
RO4987655 dose) or recent major surgery, chemotherapy,radiotherapy, immunotherapy, or investigational agent(within 4 weeks). Unlimited prior systemic therapy formetastatic disease was permitted.
Study design and dose escalationThis phase I, open-label, dose-escalation study
(NCT00817518) was conducted at 4 European centers, wasapproved by an Independent Ethics Committee, and wasconducted in accordance with the Declaration of Helsinkiand Good Clinical Practice. Written informed consent wasobtained from all patients before carrying out any study-related procedure. RO4987655 was administered as oralcapsules at least 2 hours after a light meal, followed by atleast 1 hour before the next meal.
Initial escalation was conducted using a once-daily do-sing schedule with oral RO4987655 administered over 28consecutive days in 4-week cycles. On the basis of the datafrom a toxicity study in cynomolgus monkeys (15) andclinical data from healthy volunteers (16), a starting doseof 1.0 mg/day was chosen. A regimen of twice-daily dosingwas also investigated, with a starting dose based on interimpharmacokinetics data from the once-daily regimen. Aclassical 3þ3 dose-escalation design was used, with the doseescalated according to the grade/severity of toxicity duringcycle 1. Dose escalation was conducted in 100% incre-ments (according to nearest capsule strength) until theoccurrence of grade II toxicity, after which subsequentescalation took place in increments of 50%. Following theoccurrence of a grade III toxicity that was not a DLT, doseescalation was conducted in increments of 33% untilthe first DLT was observed. This cohort was expanded to 6patients and if further DLTs were not observed in these 6patients, dose escalation continued by 25% increments.Escalationwas stopped if 2 ormorepatients in a given cohortdeveloped a DLT and the preceding dose level expandedto 6 patients to confirm the MTD (defined as the doselevel below the lowest dose at which �2 DLTs were seen).
No dose reductions were permitted during the first28 days of the study (DLT evaluation period). For any givenpatient, amaximumof 1 dose reduction or interruptionwasallowed after day 28 of cycle 1. Reescalation was permittedfor grade �III skin toxicity, which improved to grade �II,and for diarrhea or any other toxicity, which improved tograde �I within 14 days. Patients were treated at theirassigned dose until disease progression, unacceptable tox-icity or patient withdrawal, whichever occurred first.
AssessmentsDemographics andmedical history were collected during
screening. Physical examination, vital signs, and safetyassessments [ECOG-PS, 12-lead electrocardiogram (ECG),hematology/biochemistry, echocardiography/multigatedacquisition (MUGA) scan, and ophthalmologic examina-tion (fundoscopy)] were conducted at baseline/screeningand throughout treatment: ECGonday8of cycle 1 (predoseand 2 and 4 hours after drug administration); echocardi-ography/MUGA on day 1 of cycle 3; and all other
Translational RelevanceThe phase I and pharmacologic study has shown
preliminary proof of principle that tumors with selectedmutations are sensitive to mitogen-activated protein/extracellular signal–regulated kinase (MEK) inhibition.Positron emission tomography scan analysis and extra-cellular signal–regulated kinase phosphorylation mea-surement supported concentration-dependent targetengagement. In addition, prolonged patient benefitcould be shown in these patients. This may guide futuredevelopment of the MEK inhibitor RO4987655. Evi-dence of pharmacologic activity, as shown by invasiveand noninvasive biomarkers, combined with documen-ted antitumor activity in this phase I study is an excellentbasis for targeted development in phase II and III studies.Furthermore, despite the reported toxicities, continuoustreatment at adequate levels of drug exposure was fea-sible in the great majority of patients.
Phase I Study of the MEK Inhibitor RO4987655
www.aacrjournals.org Clin Cancer Res; 18(17) September 1, 2012 4795
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

assessments were done predose on days 1, 8, 15, and 22 ofcycle 1, days 1 and15of cycles 2 and3, and thereafter onday1 of each cycle and at final visit. Following observation ofcreatine phosphokinase (CPK) elevation in 1 patient [17.0mg, total daily dose (TDD)], CPK was measured in allsubsequent patients and retrospectively in blood collectedfrom patients receiving lower doses.
SafetyAEs were graded according to the National Cancer Insti-
tute Common Toxicity Criteria (v3.0; ref. 19). DLTs weredefined as: grade �III nonhematologic toxicity; grade �IIInausea/vomiting, skin rash, and/or diarrhea (despite ade-quate supportive care); grade �III skin toxicity not revert-ing to grade �II within 14 days of the scheduled startdate; febrile neutropenia [absolute neutrophil count (ANC)<1.0 � 109/L and fever �38.5�C], and/or documentedinfection (ANC <1.0 � 109/L); grade IV thrombocytopeniaor bleeding requiring a platelet transfusion.
Pharmacokinetics/pharmacodynamicsBlood samples (4 mL in potassium EDTA vacutainers)
were collected before dosing on days 1 and 15 of cycle 1 forpharmacokinetics analysis and at 1, 3, 7, and 12 hoursfollowing drug administration. Trough pharmacokineticssampling was conducted predose on days 8 and 22 of cycle1. The plasma concentration of RO4987655 was deter-mined by a validated liquid chromatography/tandemmassspectrometry (LC/MS/MS)method (16). Pharmacokineticsparameters were calculated via standard noncompartmen-tal methods using WinNonlin V6.1 (Pharsight Corpora-tion) and pharmacokinetics measurements were fitted to apharmacokinetics/pharmacodynamics model of pERKinhibition in PBMCs using NONMEM vVI (ICON).
pERK inhibition. Target inhibition of 4 beta-phorbol12-myristate 13-acetate (PMA)-induced pERK was mea-sured in PBMCs (collected days 1 and 15, cycle 1 from allpatients) using flow cytometry as described previously (16).NONMEM was used to fit pharmacokinetics/pharmacody-namics data to a model of serum and effect compartmentRO4987655 concentration versus pERK inhibition inPBMCs (Supplementary Information). pERK inhibitionwas calculated as the percentage decrease in mean fluores-cent intensity between pre- and postdose samples, withadjustment for non–PMA-stimulated predose values. Theantibody phospho-p44/42 MAPK (ERK1/2; Thr202/Tyr204; clone D13.14.4E, Cell Signaling Technology) wasused to detect endogenous levels of p44 and p42 MAPK(ERK1 and ERK2)when phosphorylated either individuallyor dually at Thr202 and Tyr204 of ERK1 (Thr185 andTyr187 of ERK2).
The effect of RO4987655 on cellular proliferation (Ki67labeling) and target inhibition (pERK expression) wasinvestigated by immunohistochemistry (IHC) in optionalskin and tumor biopsies (collected at baseline/screeningand on day 15 of cycle 1). Apoptosis was analyzed in tumorbiopsies by terminal deoxynucleotidyl transferase–mediat-ed dUTP nick end labeling (TUNEL) assay. A�20% change
in pharmacodynamics biomarkers between baseline andday 15 was considered significant. Mutational analyses forKRAS,NRAS, BRAF (V600),HRAS, PI3KCA, and PTEN losswere conducted if archival tumor samples were available.
Immunohistochemistry. Skin and tumor biopsies wereformalin fixed and paraffin embedded according to stan-dard procedures. IHC for Ki67 was conducted using theultraView detection kit (VentanaMedical Systems Inc.) on aVentana Benchmark XT platform according to the manu-facturer’s instructions. Slides were dewaxed, pretreated withmild Cell Conditioning 1 buffer (CC1; Ventana) and incu-bated for 12 minutes with a primary antibody against Ki67(clone 30.9; Ventana). Slides were then counterstainedwith hematoxylin and bluing reagent, dehydrated, andmounted. For pERK IHC, the iView detection kit (Ventana)was used on a Ventana Benchmark XT platform. Slides weredewaxed and pretreated as before, and incubated for 1 hourwith a phospho-p44/42 MAPK primary antibody (ERK1/2;Thr202/Tyr204; clone D13.14.4E; Cell Signaling Technol-ogy). To reduce nonspecific staining by endogenous biotinpresent in cells and tissues, the Endogenous Biotin BlockingKit (Ventana) was also used. Slides were counterstained andmounted as before.
TUNEL assay. Formalin-fixed tissue sections weredewaxed and washed in PBS. Sections were incubatedin 3% citric acid for 1 hour to decalcify the tissue and,after 3 washes with water, epitope retrieval was con-ducted using proteinase K (Roche). Slides were againwashed in water, and incubated with 100 mL of TUNELreaction mixture (containing FITC-dUTP) at 37�C for 1hour. Following another wash, slides were treated with3% hydrogen peroxide for 15 minutes to block endog-enous peroxidase activity before incubating with a sec-ondary antibody (anti–FITC–HRP; Roche) for 45 min-utes. Finally, slides were washed and 3-amino-9-ethyl-carbazole substrate was added for 10 minutes. Counter-staining was conducted using hematoxylin for 30seconds and slides were mounted using a gelatin–glyc-erin mounting medium.
Mutation analysis. Mutational analysis was conductedcentrally using formalin-fixed tissue. Biopsies were firstassessed to ensure at least 50% tumor cell content andmanually microdissected if required. Real-time PCR withfluorescently labeled, sequence-specific probes was usedto distinguish the wild-type (WT) BRAF (V600) sequence(GTG) from the mutant sequence (GAG). KRAS muta-tions were identified using an investigational assay basedon PCR and melting temperature analysis, with fluores-cently labeled, sequence-specific probes designed to dis-tinguish the WT sequence from mutation bearingsequences in exon 2 (specifically at codons 12 and 13)and in exon 3 (specifically at codon 61). All assays wereconducted on the cobas 4800 system (Roche MolecularSystems, Inc.) according to manufacturer’s instructions.NRAS (in melanoma), HRAS, and PI3K mutations werescreened for by standard sequencing methods and PTENloss was determined by IHC (antibody clone 138G6; CellSignaling Technology).
Leijen et al.
Clin Cancer Res; 18(17) September 1, 2012 Clinical Cancer Research4796
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

FDG-PET. Metabolic activity of tumors was investigat-ed by fluorodeoxyglucose positron emission tomography(FDG-PET; at baseline; day 15, cycle 1; day 1, cycle 3).Baseline and follow-up PET scans were conducted using asingle scanner and under the same conditions (adminis-tered 18F-FDG activity for all scans was maintained within10% of the calculated activity administered at baseline andthe same acquisition time per bed position was used for allscans for each individual patient). Low-dose CT scans wereconducted for all PET scans for attenuation correction.Independent analysis of PET images was conducted cen-trally based on European Organisation for Research andTreatment of Cancer guidelines (20). Lesions with the high-est degree of FDG uptake were selected for quantitativeanalysis (up to 5) and a 10 mm circular/spherical regionof interest drawn. A standardized uptake value (SUV) wasmeasured for each selected lesion and the delta change inSUV between baseline and day 15 of cycle 1 was calculatedfor each patient. FDG-PET scanning took place beforetumor biopsies to avoid interference on FDG uptake.Patients with a recent history of diabetes were excludedfrom FDG-PET analysis.
Tumor responseTumor assessments according to RECIST criteria (ver-
sion 1) were conducted at screening, every 2 cycles and onsuspicion of disease progression.
Statistical analysesPharmacokinetics/pharmacodynamics, safety, and tumor
response data were analyzed by descriptive statistics. Corre-lations between specific AEs and antitumor activity or phar-macokinetics were assessed by logistic regression andANOVA.
ResultsForty-nine patients were enrolled between January 2009
and June 2010 (Table 1), all received at least 1 dose ofRO4987655. The most common tumor types were mela-noma (n¼ 27, 55.1%; including choroidal melanoma, n¼9) and colorectal cancer (CRC, n¼ 11, 22.4%). None of thepatients had previously received treatment with a MEKinhibitor. Thirteen patients received RO4987655 once daily(1.0–2.5mg) and 36 received RO4987655 twice daily (3.0–21.0 mg TDD; Supplementary Fig. S1). Patients received amedian of 2 treatment cycles (range, 0–12; 93.8% ofpatients completed at least 1 cycle), with amedian durationof treatment of 57 days (range, 2–337).Four DLTs were observed during the first 28 days of
treatment, all with twice-daily dosing (Table 2). At 8.5 mgtwice daily (TDD, 17 mg), 1 patient experienced grade IIIelevated CPK. No further DLTs were observed when thiscohort was expanded to 9 patients in total. After escalationto 10.5mg twice daily (TDD, 21mg), 3 patients experiencedDLTs (grade III blurred vision, grade III elevated CPK, andgrade IV elevated CPK). Accordingly, 8.5 mg twice daily(TDD 17.0 mg) was defined as the MTD. All DLTs werereversible.
SafetyPatients experienced 189 treatment-related AEs, includ-
ing 20 grade III AEs (in 17 patients) and 2 grade IV AEs(in 2 patients). The most common AEs (�10% ofpatients; Table 2) were skin toxicity [rash related, n ¼ 45(92%of patients); dry skin, n¼ 7 (14%); skin fissures, n¼ 6(12%)] and gastrointestinal [diarrhea, n ¼ 16 (33%); nau-sea, n ¼ 7 (14%); vomiting, n ¼ 6 (12%); stomatitis, n ¼ 5(10%)]. Grade III/IV AEs were primarily limited to twice-daily dosing of �5.0 mg. Among the rare (<10% patients)grade �III toxicities, isolated and reversible grade III neu-tropenia occurred in 2 patients in the 1.5 and 10 mg dosecohorts and 1 case of reversible grade III anemia occurred inthe 13mgdose cohort treatedby transfusiononday 63.Onepatient was reported with a grade III left ventricle ejection
Table 1. Patient demographics and clinicalcharacteristics
Totalpatients
N ¼ 49
SexMale 30 (61%)Female 19 (39%)Age, yMedian 53Range 22–79RaceWhite 48 (98%)Asian 1 (2%)Baseline ECOG-PS0 23 (47%)1 25 (51%)Unknown 1 (2%)Prior anticancer therapies, median (range) 3 (1–9)Primary cancer site and mutational statusMelanoma 27BRAF (V600) 2No mutation 7Unknown 18
Colon/large intestine and rectum 11KRAS 6a
PI3KCA 1a
No mutation 1Unknown 4
Lung 3b
Ovarian 2b
Pancreas 1b
Synovial sarcoma 1b
Thymoma 1b
Unknown 1b
Cervix 1b
Clear-cell sarcoma 1b
aOne tumor contained both a KRAS and PI3KCA mutation.bMutational status unknown.
Phase I Study of the MEK Inhibitor RO4987655
www.aacrjournals.org Clin Cancer Res; 18(17) September 1, 2012 4797
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

Tab
le2.
Trea
tmen
t-relatedtoxicity
Totald
aily
dose
(mg)
Num
ber
of
patients
Onc
e-daily
dosing
a
Twice-daily
dosing
b
(n)
1.5(n
¼4)
3 (n¼
3)4 (n
¼3)
5.5
(n¼
4)7.5
(n¼
4)10 (n
¼4)
13 (n¼
4)17 (n
¼9)
21 (n¼
4)
DLT
sGradeIII
blurred
vision
(n¼
1)1
GradeIII
elev
ated
CPK(n
¼2)
1c1
GradeIV
elev
ated
CPK(n
¼1)
1Treatmen
t-relatedAEs
AEs(allgrades
)AEs(gradeIII–IV
only)
n%
Ras
hrelatedd
4591
.81
12
2Diarrhe
a16
32.7
Eye
relatede
1326
.51
1Eleva
tedCPK
918
.41
32
Fatig
ue8
16.3
Dry
skin
714
.3Nau
sea
714
.3Skinfiss
ures
612
.2Vom
iting
612
.2Stomatitis
510
.2Pruritus
36.1
1Asthe
nia
36.1
1Neu
trop
enia
36.1
11
Ane
mia
24.1
1Dec
reas
edap
petite
24.1
1Dep
ress
ion
12.0
1Dec
reas
edEjectionFrac
tion
12.0
1Treatmen
t-relatedSAEs(allgrades
)n
%SAEs(allgrades
)Dep
ress
ion
12.0
1Ane
mia
f1
2.0
1Retinal
vein
occlus
ion
12.0
1Asthe
nia
12.0
1Dec
reas
edap
petite
12.0
1Cho
rioretin
opathy
12.0
1Eleva
tedCPK
12.0
1Blurred
vision
12.0
1
NOTE
:Datacu
toff:J
anua
ry28
th20
11.O
nlythemos
tsev
ereintens
itywas
coun
tedform
ultip
leoc
curren
cesof
thesa
meAEin
oneindividua
l.Adve
rseev
ents
occu
rringin
>10%
ofpa
tientsaresh
ownab
ovethedottedline.
aOnlyon
egrad
eIII
toxicity
(neu
trop
enia)w
asreportedin
only
onedo
sing
-coh
ortin
theon
ce-daily
regimen
(1.5
mgon
cedaily).
bTh
emos
tcom
mon
AEswerereportedat
grad
eIIIor
IVse
verityinthetw
ice-dailydos
ingco
horts.Tw
ograd
eIV
AEsoc
curred
,bothelev
ated
CPK(8.5
and10
.5mg,
twiceda
ily).No
grad
eVAEsoc
curred
.Nau
sea/vo
miting
,skinrash
,and
/ord
iarrhe
awereon
lyco
nsidered
aDLT
ifthey
reac
hedgrad
e�I
IIse
veritydes
pite
adeq
uate
supportiv
eca
remea
sures.SAEs
weredefi
nedas
anyAE,w
hich
was
fatal;life-threaten
ing;
requiredin-patient
hosp
italizationor
prolong
ationof
existin
gho
spita
lization;
resu
ltedin
persistent
orsign
ifica
ntdisab
ility/
inca
pac
ity;w
asaco
ngen
italano
maly/birthdefec
t;was
med
icallysign
ifica
ntor
requiredinterven
tionto
preve
nton
eor
othe
rofthe
outcom
eslistedab
ove.NoSAEsoc
curred
inon
ce-
daily
dos
ingco
horts.
cNofurthe
rDLT
swereob
served
whe
nthe17
.0mg(tw
icedaily)c
ohortwas
expan
ded
to9patients.
dInclud
esdermatitisac
neifo
rm,ras
h,de
rmatitis,
pap
ular
rash
,folliculitis,
andge
nitalras
h.eInclud
esblurred
vision
,pho
topsia,
cornea
lerosion
,dry
eyes
,periorbita
ledem
a,ch
orioretin
opathy
,pun
ctateke
ratitis,a
ndretin
alve
inoc
clus
ion.
f Nosign
sof
chronicor
acutega
strointestinal
bleed
ingwereob
served
andno
hemog
lobinuria
was
reco
rded
.
Leijen et al.
Clin Cancer Res; 18(17) September 1, 2012 Clinical Cancer Research4798
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

fraction decrease in the 13 mg dose cohort which occurredon day 56 when drug was stopped because of the progres-sion of the disease. The other grade III toxicities includedgeneral disorders (asthenia, depression, decreased appetite)and skin disorders (Table 2). Most rash-related toxicitieswere grade I/II, with 6 patients experiencing grade III eventsand no grade IV events reported. Median time to develop-ment of grade III rash was 49.5 days (range, 9–146). Skintoxicity developed primarily in the face, upper trunk, andback; comprising red papulopustules and crusts, occasion-ally accompanied by swelling (mainly the nose). Severepsychologic impacts were reported in patients experiencingsubstantial alterations in appearance.Sixteen eye-related AEs occurred in 13 [27%] patients
[including blurred vision, photopsia, corneal erosion, dryeyes, periorbital edema, chorioretinopathy, punctate kera-titis, and retinal vein occlusion (RVO)]. Blurred vision wasassociated with fluid accumulation in the subretinal space,identified by optical coherence tomography (OCT), result-ing in serous retinal detachment (SRD) in one patient. Twopatients experienced grade III ocular toxicity [RVO (8.5 mgtwice daily) and blurred vision (10.5 mg twice daily)].Median time-to-onset of ocular toxicity was 12 days (range,1–175 days), and median duration of toxicity was 14 days(range, 2–104 days). Ocular toxicity resolved either spon-taneously or with drug interruption (2 grade II and 2 gradeIII) except for 1 patient with grade III visual disturbancesassociated with RVO who improved to grade I at studycompletion, and 1 with grade I blurred vision whose con-dition remained unresolved at study completion.Nine (18%) patients experienced elevated CPK includ-
ing 4 grade III (1 at 2.0 mg twice daily, 2 at 8.5 mg twicedaily, and 1 at 10.5 mg twice daily) and 2 grade IV events(at 8.5 mg twice daily and 10.5 mg twice daily). CPKelevation was reversible with drug interruption and wasasymptomatic in most patients and not associated witheither clear rhabdomyolysis symptoms or cardiac dys-function. Three cases of grade I myalgia (in 3 patients),1 grade I joint swelling, 1 grade II joint stiffness, 1 grade IIneck pain, 1 grade I pain in an extremity, and 1 grade IImuscular weakness were reported in association with CPKelevation.Eight patients experienced dose reductions due to
treatment-related AEs (1 patient at 1.5 mg once daily and4.0/3.5 mg twice daily, and 3 patients at 8.5 mg twice dailyand 10.5 mg twice daily), including 5 patients who expe-rienced more than one AE-related dose interruption (1patient at 1.5 mg once daily and 2 patients each at 8.5 mgtwice daily and 10.5 mg twice daily). Of the 9 patientsreceiving RO4987655 at the RP2D (8.5mg twice daily), themedian duration of dosing was 87.5 days (range, 50–194)in the 6 patients who did not undergo dose modification.Median time to dose modification in the remaining 3patients was 37 days (range, 14–51).Eleven patients experienced temporary drug interrup-
tions due to AEs (1 each at 1.5 mg once daily, 2.0 mg oncedaily, 4.0/3.5 twice daily, and 5.0mg twice daily; 2 at 6.5mgtwice daily and 10.5mg twice daily; and 3 patients at 8.5mg
twice daily). The median duration of interruption was 7days (range, 1–21; Supplementary Table S1).
Seven patients experienced 8 treatment-related seriousAEs (SAEs; all grade II/III; Table 2). Five of the SAEs wereresolved, 2 with dose modifications, 2 without dose mod-ifications, and 1 with treatment discontinuation. Theremaining 3 SAEs were unresolved. Two deaths followingdisease progression were not considered to be treatmentrelated.
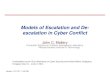
Antitumor activityClinical benefit [defined as partial response (PR) or stable
disease (SD) lasting �16 weeks] was seen in 8 of the 38evaluable patients (21.1%; Fig. 1), including one confirmedand one unconfirmed PR in patients with skin melanomas(mutational status unknown). These patients received treat-ment with RO4987655 for 113 and 224 days (mean 168.5days) and responses lasted for 48 and 168 days (mean 108days). Six other patients achieved SD lasting >16 weeks: 3patients with melanoma, 2 patients with choroidal mela-noma, and 1 patient with a rectal adenocarcinoma. Themedian percentage change in tumor size at maximumreduction from baseline in evaluable patients was 9.8%(range �66.9% to 101.4%).
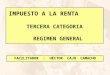
PharmacokineticsPK was assessed in 43 patients (87.8%). Plasma concen-
trations of RO4987655 increased rapidly following oraladministration. For the majority of patients, maximumplasma drug concentration (Cmax) was reached approxi-mately 30 to 60 minutes after dosing (Fig. 2A, Table 3).Mean terminal half-life was approximately 4 hours. Plasmaexposure increased approximately dose proportionally onday 1 (Fig. 2B) and increased linearly with dose at steadystate (Fig. 2C). Intrapatient variability in plasma exposurewas limited (Table 3). At the MTD, Cmax and area under theplasma concentration–time curve (AUC0–12h) were 425 ng/mL and 1,660 ng�h/mL, respectively, at day 1 and 530 ng/mL and 2,577 ng�h/mL, respectively, at steady state. Themean accumulation index (AUCday 15/AUCday 1) was 1.53(range, 1.15–1.96). Increased steady-state plasma exposurewas significantly associated with occurrence of grade II/IIIrash (logistic regression, P ¼ 0.01) and showed a trendtoward association with CPK elevation (ANOVA; P¼ 0.07).
PharmacodynamicspERK inhibition in peripheral blood lymphocytes. Assess-
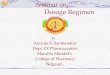
ment of target suppression was evaluated by measuring theextent of pERK inhibition in a surrogate tissue, PBMC. Therelationship between exposure (RO4987655 plasma con-centration) and pharmacodynamics effect (pERK inhibi-tion in PBMCs) was characterized by a direct link pharma-cokinetics/pharmacodynamics (effect compartment) mod-el, which revealed 70% to 80% pERK inhibition at plasmaconcentrations of >200 ng/mL (Fig. 3A).
Tumor/skin biopsies. Between baseline and day 15,pERK expression in tumor biopsies decreased by �20% in6 of 11 evaluable patients and increased by �20% in the
Phase I Study of the MEK Inhibitor RO4987655
www.aacrjournals.org Clin Cancer Res; 18(17) September 1, 2012 4799
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

other (Fig. 3B, Supplementary Table S2). One tumorshowed >90% reduction in pERK expression. Paired pre-treatment and posttreatment normal skin biopsies wereavailable from 20 patients; 5 showed a decrease in pERKexpression of �20% by day 15, 14 showed no change, andIHC failed in 1 patient (Fig. 3B, Supplementary Table S2).One skin biopsy showed >90% pERK reduction. Mosttumor and skin biopsies showed no change in cell prolif-eration (Ki67 labeling) between baseline and day 15 (Sup-plementary Table S2). Three of 5 paired tumor biopsiesshowedno change in apoptotic signal betweenbaseline andday 15 (TUNEL assay; Supplementary Table S2). No corre-lations were observed between changes in biomarker levelsand tumor response, mutational status, or exposure.
Mutational analysis. Mutational analyses were con-ducted for tumor samples from a total of 30 patients; 22samples were suitable for assessment of BRAF V600 andKRAS mutations, 21 were suitable for NRAS, 18 for HRASand PI3K, and 10 samples were suitable for assessment ofPTEN loss. Of the 30 tumor samples assessed, 8 revealedmutations (Table 1) including 2 melanomas with BRAF(V600) mutation, 5 CRC with KRAS mutation and 1 CRCwith both KRAS and PI3K mutations. Figure 1 shows themutational status of tumors that were evaluable for tumorresponse.
FDG-PET. FDG-PET was conducted in 34 patients.Between baseline and day 15, 27 patients (79.4%, oncedaily, n¼ 1; twice daily, n¼ 26) showed a reduction in FDGuptake (Fig. 3C). In most cases, reductions in FDG uptakewere maintained until at least Week 8 in patients notprogressing between assessments. Excluding one outlier,
there was a positive relationship between dose/exposureand change in FDG uptake between baseline and day 15 inthe overall population. This relationship was more pro-nounced in patients with melanoma, where larger changesin FDG uptake were observed as dose increased. Change inFDG-PET uptake was weakly correlated with tumorresponse (RECIST). All patients achieving a PR or SD(>16 weeks) showed a reduction in FDG uptake by day15 (see Supplementary Fig. S2). Larger reductions in FDGuptake between baseline and day 15 were observed withincreased pERK inhibition in PBMCs.
DiscussionIn patients with advanced solid tumors, oral RO4987655
was moderately tolerated with manageable toxicity andshowed a favorable pharmacokinetics/pharmacodynamicprofile and encouraging antitumor activity. The safety pro-file of RO4987655 in this study was consistent with datafrom healthy volunteers with no new safety signals beingidentified. The management and treatment of safety eventswas facilitated by the short half-life of RO4987655. TheMTDof RO4987655was 8.5mg twice daily (17.0mgTDD).DLTs were grade III blurred vision (n ¼ 1) and grade III/IVelevated CPK (n ¼ 3); all of which were reversible withouttreatment.
The most frequent RO4987655-related AEs were skintoxicity and gastrointestinal disorders. MEK inhibitor classeffects included rash (91.8%) and eye-related toxicity(26.5%). Previous studies with MEK inhibitors havereported rash, diarrhea, nausea, fatigue, and visual distur-bances as the most common treatment-related AEs
100
80
60
40
20
0
–20
–40
–60
–80
–100
Pe
rce
nta
ge
ch
an
ge
fro
m b
ase
line
(su
m o
f th
e lo
ng
est
dia
me
ter)
Other
Melanoma
CRC
(RECIST cutoff
for PR, 30%)
Mutation not known
BRAF V600
KRAS
WT
PI3K
3.0
/2.5
mg b
.i.d
.
8.5
mg b
.i.d
.
5.0
mg b
.i.d
.
4.0
/3.5
mg b
.i.d
.
2.0
mg q
.d.
8.5
mg b
.i.d
.
8.5
mg b
.i.d
.
1.5
mg b
.i.d
.
2.5
mg q
.d.
1.5
mg q
.d.
1.5
mg b
.i.d
.
1.5
mg q
.d.
6.5
mg b
.i.d
.
1.5
mg b
.i.d
.
2.0
mg q
.d.
1.0
mg q
.d.
2.5
mg q
.d.
8.5
mg b
.i.d
.
1.0
mg q
.d.
6.5
mg b
.i.d
.
1.5
mg q
.d.
8.5
mg b
.i.d
.
6.5
mg b
.i.d
.
3.0
/2.5
mg b
.i.d
.
4.0
/3.5
mg b
.i.d
.
5.0
mg b
.i.d
.
3.0
/2.5
mg b
.i.d
.
2.0
mg b
.i.d
.
8.5
mg b
.i.d
.
8.5
mg b
.i.d
.
2.0
mg b
.i.d
.
1.5
mg q
.d.
4.0
/3.5
mg b
.i.d
.
8.5
mg b
.i.d
.
8.5
mg b
.i.d
.
2.0
mg q
.d.
8.5
mg b
.i.d
.
8.5
mg b
.i.d
.
*
*
{
Figure 1. Relative change (%) in sum of lesion size from baseline at best overall response. Thirty-eight patients were evaluable for tumor response. Targetlesionswere notmeasured in 7patients, 3 patientswere not evaluable at day1of cycle 3, and tumor assessmentwas not completed for 1 patient. By the endofthe study, 44patients hadprogressed.All patientswere eventuallywithdrawn from treatment: 43due todisease progression, 5 due toAEs, and1due to refusalof treatment. Tumor response assessments were conducted according to RECIST criteria (version 1). Dotted line indicates the RECIST cutoff for partialresponse (�30%). The figure alsodepictsmutation status for patientswith responsedata: BRAF (�), KRAS (~),WT (*), PI3K (&); 1 patientwithmelanomawithBRAF mutation and 2 CRC patients with KRAS mutation were not evaluable for response and are not shown. b.i.d., twice daily; q.d., once daily.
Leijen et al.
Clin Cancer Res; 18(17) September 1, 2012 Clinical Cancer Research4800
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

(5, 8, 13, 21, 22). An indirect comparison betweenRO4987655 and the phase I published data from otherMEK inhibitors suggests that RO4987655 has a compar-able safety profile with a higher frequency of rash-relatedtoxicity (92% vs. 38%–79%), but a generally lower inci-dence of diarrhea (32% vs. 32%–55%), nausea (14% vs.29%–54%), and eye-related toxicity (27% vs. 33%–50%;refs. 5, 8, 13, 21, 22), while CPK elevation which wasobserved regularly in this study, has so far not been observ-ed with other MEK inhibitors (5, 13, 21, 23).
Ocular toxicity is a known class effect of MEK inhibitorsandwas also observed in this study. Two episodes of blurredvision evenoccurred very early in treatment, after 1 or 2 daysof dosing. Themajority of visual symptoms reported in thisstudy were due to SRD, but OCT was not systematicallyconducted, preventing accurate evaluation of the incidenceof associated SRD. Although ocular toxicities can be alarm-ing for both patients and physicians, all cases of SRDreported in this study were reversible without any specifictreatment and without long-term damage. This is in linewith blurred vision reported in other studies (5, 8, 13).Other class-related ocular complications in this studyoccurred less frequently than SRD and include ocularhypertension, which can be detected by regular measure ofintraocular pressure, and RVO, that can be detected early byregular fundus photographs. Because the pathogenesis ofMEK-related eye disorders remains unknown and experi-ence with chronic administration of MEK inhibitors islimited, careful monitoring of ocular disorders should beimplemented in further clinical trials with MEK inhibitorsto ensure adequate management of patients.
CPK elevation was reported in this study and consideredrelated to RO4987655. Systematic measurement of CPK inthis studymay have generated a higher incidence of reports.Most elevated CPK episodes were asymptomatic and noRO4987655-related cardiovascular disorders or rhabdomy-olysis were observed. The mechanism behind the observedCPK elevation remains unknown at present. A direct roleof MEK inhibition cannot be excluded as the MAPK path-way plays a key role in regulation of muscle cell signaling(24–27).
RO4987655 monotherapy showed encouraging antitu-mor activity as measured by RECIST. Like other MEK inhi-bitors, RO4987655 showed clinical activity against mela-noma (13, 21–23). Seven of the 8 patients who achievedclinical benefit with RO4987655 had melanoma tumors,including 2 PRs (1 confirmed, 1 unconfirmed; both at8.5 mg twice daily). No clear correlation existed betweenresponse and mutational status; however, the number ofpatients withmutation data was limited. On the basis of thesafety and pharmacokinetics/pharmacodynamics profiledata presented here, a dose regimen of 8.5 mg twice daily(17.0 mg TDD) RO4987655 is recommended for phase IIstudies.
PK analyses showed that RO4987655 was absorbedrapidly, reaching Cmax 0.5 to 1 hour after dosing, andthat plasma concentration and exposure increased approx-imately dose proportionally. The pharmacokinetics of
600
400
200
00 3 6 9 12
Pla
sm
a c
oncentr
ation o
f R
O4987655 (
ng/m
L)
Time (h)
10.5 mg
8.5 mg
6.5 mg
5 mg
4 mg
3 mg
2 mg
1.5 mg
4,000
3,000
2,000
1,000
00 3 6 9 12
AU
C0
–1
2 h (
ng
•h/m
L)
Dose (mg)
4,000
3,000
2,000
1,000
00 3 6 9 12
AU
C0
–1
2 h (
ng
•h/m
L)
Dose (mg)
A
B
C
Figure 2. Mean plasma concentration (A) and plasma exposure (B) on day1 and plasma exposure on day 15 (C) of RO4987655 following oraladministration. Blood was collected for pharmacokinetics assessmentfrom 43 patients on day 1: predose (0 hours) and 1, 3, 7, and 12 hourspostdose. For patients on twice-daily dosing cohorts, pharmacokineticsparameters were measured after the first daily dose. A, mean plasmaconcentration: data points represent themean plasma concentrations onday 1. Cmax was reached approximately 0.5 to 1 hour after dosing. Meanterminal half-life was approximately 4 hours. The figure legend showsadministered dose, rather than total daily dose. B, plasma exposure onday 1, and C, plasma exposure on day 15: steady-state conditions werereached by day 15 anddrug accumulationswere assessed by the plasmaexposure (AUC0–12h). Data points represent mean plasma exposure anderror bars represent standard deviation.
Phase I Study of the MEK Inhibitor RO4987655
www.aacrjournals.org Clin Cancer Res; 18(17) September 1, 2012 4801
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

RO4987655 was linear, time independent, and consistentwith an earlier study in healthy volunteers, with the excep-tion of terminal half-life, which was much shorter thanpreviously reported (4 hours vs. 25 hours, respectively;ref. 16). Although the reason for this remains unclear, itmayindicate that the longer sampling period used previouslyallowed for a more accurate assessment of the terminalphase half-life: RO4987655 was monitored for 72 hourspostdosing in healthy volunteers but only 12 hours inthis study because of the inclusion of twice-daily dosing.The influence of food on the absorption of RO4987655remains to be determined. Data from recent studies withother MEK inhibitors are conflicting; although administra-tion with a high-fat meal was shown to increase exposureto the oral inhibitor CI-1040, exposure to selumetinibwas reduced when administered with food (28, 29).Patients in this study were lightly fasted before dosingwith RO4987655; the effect of food on the exposure toRO4987655 will be investigated during further develop-ment of this compound.
Although higher plasma concentrations of RO4987655were associated with greater pERK inhibition in PBMCs andalmost all tumor samples showed a significant decrease inpERK expression by day 15 (cycle 1), target suppression inskin biopsies was observed in only a quarter of cases.Overall, skin and tumor biopsies showed no change ineither tumor cell proliferation or apoptosis between base-line and day 15, possibly reflecting the RO4987655’s cyto-static nature. Data on inhibition of tumor cell proliferationand induction of apoptosis in response to MEK inhibitionare limited; decreased tumor Ki67 has been showed inresponse to treatment with AZD6244 and PD-0325901(5, 13). The exactmechanismbywhich apoptosis is inducedby MEK inhibition has not been identified and betterunderstanding will be important in the development ofstrategies to overcome treatment resistance (30, 31).
Evidence of biologic activity was shown by FDG-PET,particularly in melanoma where decrease in FDG uptakeappeared to be associated with dose and drug exposure.In addition, a weak relationship was observed betweenchange in FDG uptake (between baseline and day 15) andRECIST tumor assessment. All patients achieving a PRor SD lasting >16 weeks showed a reduction in FDGuptake by day 15, suggesting that an FDG decrease wasnecessary, but not sufficient, for later tumor response.Furthermore, FDG-PET data correlated with PBMC pERKinhibition; larger changes from baseline were associatedwith increased inhibition of pERK. Clinical studies inves-tigating other signal transduction inhibitors, like imatinib(in gastrointestinal stromal tumors and soft-tissue sarco-mas; refs. 32, 33) and erlotinib (in NSCLC; refs. 34, 35)and the chemotherapy agent irinotecan (in CRC; ref. 36),have supported the role of FDG-PET as a predictivemarker of clinical activity, although this needs large-studyconfirmation.
There is currently anunmet need for effective treatment ofpatients with tumors containing KRAS mutations andpatients with WT BRAF melanoma (37–41). Althoughthe mutational analysis in this study was limited, MEKinhibition may offer a therapeutic option independent ofKRAS and BRAFmutation state, most likely in combinationwith chemotherapy and/or another targeted agent. Recentpreclinical data show that combined RAF/MEK inhibitorscan block ERK activation in resistant cells and may delayemergence of resistance (42, 43). Studies with other MEKinhibitors are investigating combinations with AKT inhibi-tors, PI3K inhibitors, and chemotherapy agents such aspaclitaxel and docetaxel (44–48). The optimum partnersfor RO4987655 remain to be determined; however, in vitroand in vivo data show that combination withPI3-kinasepathway inhibitors (mTOR, PI3K inhibitors; ref. 15),other targeted agents, or chemotherapy agents (cisplatin,
Table 3. Summary of pharmacokinetics of RO4987655 in patients following oral administration
Day 1 Day 15
Regimen N
AUC0–12h
ng�h/mL(% CV)
Cmax
ng/mL(% CV)
t1/2 h(% CV) N
AUC0–12h
ng�h/mL(% CV)
Cmax
ng/mL(% CV) t1/2 h (% CV)
Accumu-lationindexa
1.5 mg (twice daily) 4 278 (27%) 88.0 (30%) 4.7 (12%) 4 460 (18%) 105 (30%) 6.0 (19%) 1.652.0 mg (twice daily) 3 321 (7%) 72.9 (64%) 3.7 (50%) 3 629 (12%) 129 (25%) 7.6 (47%) 1.963.0 mg (twice daily) 4 596 (44%) 171 (39%) 3.4 (20%) 4 861 (47%) 176 (58%) 4.0 (20%) 1.154.0 mg (twice daily) 4 608 (38%) 142 (51%) 4.2 (11%) 4 1053 (13%) 183 (61%) 6.1 (16%) 1.905.0 mg (twice daily) 4 797 (64%) 209 (89%) 3.3 (20%) 4 1157 (60%) 201 (66%) 3.8 (8%) 1.456.5 mg (twice daily) 3 1005 (35%) 207 (51%) 3.3 (12%) 4 1458 (21%) 282 (36%) 3.9 (28%) 1.458.5 mg (twice daily)b 9 1660 (39%) 425 (50%) 3.4 (25%) 9 2577 (48%) 530 (53%) 8.0 (157%) 1.5010.5 mg (twice daily) 4 2282 (43%) 601 (66%) 3.7 (66%) 2 2638 (12%) 399 (45%) 8.1 (87%) 1.16
Abbreviations: CV, coefficient of variation; t1/2, plasma half-life.aAccumulation index represents AUCday 15/AUCday 1.bMTD.
Leijen et al.
Clin Cancer Res; 18(17) September 1, 2012 Clinical Cancer Research4802
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

paclitaxel, and gemcitabine) may potentiate RO4987655’santitumor activity.Single-agent RO4987655 is currently under investigation
in an expansion of this study in 4 parallel patient cohortsincluding patients with: (i) melanoma tumors carrying theBRAF (V600)mutation, (ii) melanoma tumors not carryingthe BRAF (V600) mutation, (iii) NSCLC carrying KRASmutations, and (iv) CRC carrying KRAS and/or BRAF
(V600) mutations. The primary endpoint of this expansioncohort studywill be to investigate the efficacyof single-agentRO4987655 in these specific tumor genotypes, usingapproximately 20 patients per cohort. Further developmentof RO4987655 will involve combination with chemother-apy or other signal transduction inhibitors.
In summary, oral RO4987655 was reasonably well tol-erated in patients with advanced ormetastatic solid tumors,
Figure 3. A, RO4987655 plasmaand effect concentrations versusPBMC pERK inhibition (all doses); B,case study: pERK expression inpaired tumor (i and ii) and normal skin(iii and iv) biopsies obtained beforetreatment with RO4987655(baseline) and onday 15 of cycle 1;C,relative change (%) in FDG-PET frombaseline to day 15 of cycle 1. A,measurements were fitted to aneffect compartmentpharmacokinetics/pharmacodynamics model of pERKinhibition in PBMCs (SupplementaryInformation). Seventy percent toeightypercent inhibitionof pERKwasobserved at RO45987655 plasmaconcentrations of >200 ng/mL. Halfmaximal inhibitory concentration(IC50), 53 ng/mL; 90% inhibitoryconcentration (IC90), 480 ng/mL.Average regression is representedbythe blue line, and 90% confidenceintervals of the mean regression areshown aspurple lines. A timedelay ofapproximately 3 hours was observedbetween Cmax and the maximumeffect generated by thepharmacokinetics/pharmacodynamics model. B,representative images depicting IHCfor pERK in paired tumor biopsiestaken from a patient with melanoma.This patient received RO4987655 ata dose of 8.5 mg twice daily (17.0 mgTDD) and the patient achieved stabledisease lasting for 28 weeks. In thiscase study, reductions in nuclearpERK expression of 65% and 97%were observed in the tumor and skinbiopsies, respectively, betweenbaseline and day 15. C, �, þ320%change from baseline (PET%change) was trimmed at þ125% foraesthetic purposes; ��, patients whoachieved partial responses [thepatient initially treated at 10.5 mgtwice daily underwent a dosereduction to 8.5mg twice daily due toa DLT (CPK elevation)]. FDG-PETwas conducted at baseline and onday 15 of cycle 1 in 34 patients(69.4%; 3 patients receivedRO4987655 once daily and 31received RO4987655 twice daily).b.i.d., twice daily.
80
60
40
20
00 100 200 300 400 500
pE
RK
inhib
itio
n (
%)
RO4987655 plasma concentration (ng/mL)
80
60
40
20
00 100 200 300 400 500
pE
RK
inhib
itio
n (
%)
RO4987655 effect concentration (ng/mL)
A
B
C100
50
0
–50
–100
Perc
enta
ge c
hange in
FD
G-P
ET
fro
m b
aselin
e
Other
Melanoma
CRC
10
.5 m
g b
.i.d
.
8.5
mg
b.i.d
.
2.0
mg
q.d
.
3.0
/2.5
mg
b.i.d
.
3.0
/2.5
mg
b.i.d
.
4.0
/3.5
mg
b.i.d
.
1.5
mg
q.d
.
1.5
mg
b.i.d
.
2.0
mg
b.i.d
.
4.0
/3.5
mg
b.i.d
.
4.0
/3.5
mg
b.i.d
.
2.0
mg
b.i.d
.
6.5
mg
b.i.d
.
4.0
/3.5
mg
b.i.d
.
10
.5 m
g b
.i.d
.
5.0
mg
b.i.d
.
5.0
mg
b.i.d
.
2.5
mg
q.d
.
3.0
/2.5
mg
b.i.d
.
6.5
mg
b.i.d
.
6.5
mg
b.i.d
.
8.5
mg
b.i.d
.
8.5
mg
b.i.d
.
1.5
mg
b.i.d
.
2.0
mg
b.i.d
.
6.5
mg
b.i.d
.
8.5
mg
b.i.d
.
8.5
mg
b.i.d
.
8.5
mg
b.i.d
.
1.5
mg
b.i.d
.
8.5
mg
b.i.d
.
5.0
mg
b.i.d
.
10
.5 m
g b
.i.d
.
8.5
mg
b.i.d
.
*
** **
Baseline Day 15
Phase I Study of the MEK Inhibitor RO4987655
www.aacrjournals.org Clin Cancer Res; 18(17) September 1, 2012 4803
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

but often resulted in skin toxicity (91.8%; primarily facial,and with psychosocial impact reported). RO4987655revealed a safety profile comparable with other MEK inhi-bitors. The main DLTs were reversible blurred vision andelevated CPK. At the RP2D, high (70%) and sustained(>IC50 for >90% of time) pERK inhibition was observed inPBMCs, and plasma drug concentrations were in the rangepredicted to be efficacious in preclinical models. Metabolicand anatomic responses were observed in all tumor types,but particularly in patients with melanoma tumors.
Disclosure of Potential Conflicts of InterestEmployment: V. Lopez-Valverde, Z.-X. Xu, R. Rueger, J.L.T. Tessier, E.
Schochat, S. Blotner, V. Meresse Naegelen; Commercial research grant: W.Eberhardt (Eli Lilly); Other commercial research support: M.R. Middleton(Roche); Honoraria from speaker’s bureau: M.R. Middleton (Roche), V.Dieras (GSK, Roche, EISAI), W. Eberhardt (Roche, Astra Zeneca, GSK,Novartis, MSD, Eli Lilly); Consultant/Advisory Board: M.R. Middleton(Roche), V. Dieras (Roche, Genetech, Novartis, GSK, Sanofi Aventis, Amgen,Pfizer), F. Kraeber-Bod�er�e (Roche), W. Eberhardt (Roche, Astra Zeneca, GSK,Novartis, MSD, Eli Lilly). No potential conflicts of interest were disclosed bythe other authors.
Authors' ContributionsConception and design: M.R. Middleton, Z.-X. Xu, R. Rueger, V. MeresseNaegelen, J.H.M. Schellens, W.E.E. EberhardtDevelopment of methodology: R. Rueger, J.J.L. Tessier, V. Meresse Nae-gelen, J.H.M. Schellens, W.E.E. EberhardtAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): S. Leijen, M.R. Middleton, P. Tresca, V. Dieras, M.
E. Scheulen, A. Gupta, V. Lopez-Valverde, Z.-X. Xu, R. Rueger, J.H.M.Schellens, W.E.E. EberhardtAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): S. Leijen, F. Kraeber-Bod�er�e, V. Dieras, M.E. Scheulen, A. Gupta, V. Lopez-Valverde, Z.-X. Xu, R. Rueger, J.J.L. Tessier, E.Shochat, S. Blotner, V. Meresse Naegelen, J.H.M. Schellens, W.E.E. EberhardtWriting, review, and/or revision of the manuscript: S. Leijen, M.R.Middleton, P. Tresca, F. Kraeber-Bod�er�e, V. Dieras, M.E. Scheulen, A. Gupta,V. Lopez-Valverde, Z.-X. Xu, R. Rueger, J.J.L. Tessier, E. Shochat, S. Blotner, V.Meresse Naegelen, J.H.M. Schellens, W.E.E. EberhardtAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): R. Rueger, S. BlotnerStudy supervision: J.J.L. Tessier, V. Meresse Naegelen, J.H.M. Schellens, W.E.E. Eberhardt
AcknowledgmentsThe authors thank patients and staff at the study sites, and Stefanie
DeSchepper (HistoGeneX), Astrid Heller and Miro Venturi (Roche Transla-tional Research Science), Lucy Lee (ex-Hoffman La Roche), and YoshitakaOgita (Chugai Pharmaceutical Co., Ltd.).
Third-party writing assistance was provided by Laura McDonagh, PhD,and Jamie Ashman, PhD (Prism Ideas).
Grant SupportThis study and editorial support for the preparation of the manuscript
were funded by F. Hoffmann-La Roche Ltd.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received March 26, 2012; revised May 22, 2012; accepted June 21, 2012;published OnlineFirst July 5, 2012.
References1. Dhillon AS, Hagan S, Rath O, Kolch W. MAP kinase signalling path-
ways in cancer. Oncogene 2007;26:3279–90.2. Pearson G, Robinson F, Beers GT, Xu BE, Karandikar M, Berman K,
et al. Mitogen-activated protein (MAP) kinase pathways: regulationand physiological functions. Endocr Rev 2001;22:153–83.
3. Bos JL. Ras oncogenes in human cancer: a review. Cancer Res1989;49:4682–9.
4. Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, et al.Mutations of the BRAF gene in human cancer. Nature 2002;417:949–54.
5. Adjei AA, Cohen RB, Franklin W, Morris C, Wilson D, Molina JR, et al.Phase I pharmacokinetic and pharmacodynamic study of the oral,small-molecule mitogen-activated protein kinase kinase 1/2 inhibitorAZD6244 (ARRY-142886) in patients with advanced cancers. J ClinOncol 2008;26:2139–46.
6. Davies BR, Logie A, McKay JS, Martin P, Steele S, Jenkins R, et al.AZD6244 (ARRY-142886), a potent inhibitor of mitogen-activatedprotein kinase/extracellular signal-regulated kinase kinase 1/2kinases: mechanism of action in vivo, pharmacokinetic/pharmacody-namic relationship, andpotential for combination in preclinicalmodels.Mol Cancer Ther 2007;6:2209–19.
7. Lang I, Adenis A, Boer K, Escudero P, Kim T, Valladares M, et al.AZD6244 (ARRY-142886) versus capecitabine (CAP) in patients (pts)with metastatic colorectal cancer (mCRC) who have failed prior che-motherapy. J Clin Oncol 26;20s, 2008 (suppl; abstr 4114).
8. Banerji U, Camidge DR, Verheul HM, Agarwal R, Sarker D, Kaye SB,et al. The first-in-human study of the hydrogen sulfate (Hyd-sulfate)capsule of the MEK1/2 inhibitor AZD6244 (ARRY-142886): a phase Iopen-label multicenter trial in patients with advanced cancer. ClinCancer Res 2010;16:1613–23.
9. Bekaii-Saab T, Phelps MA, Li X, Saji M, Goff L, Kauh JS, et al. Multi-institutional phase II study of selumetinib in patients with metastaticbiliary cancers. J Clin Oncol 2011;29:2357–63.
10. O'Neil BH, Goff LW, Kauh JS, Strosberg JR, Bekaii-Saab TS, Lee RM,et al. Phase II study of the mitogen-activated protein kinase 1/2
inhibitor selumetinib in patients with advanced hepatocellular carci-noma. J Clin Oncol 2011;29:2350–6.
11. Gilmartin AG, BleamMR, Groy A, Moss KG,Minthorn EA, Kulkarni SG,et al. GSK1120212 (JTP-74057) is an inhibitor of MEK activity andactivation with favorable pharmacokinetic properties for sustained invivo pathway inhibition. Clin Cancer Res 2011;17:989–1000.
12. Hoeflich KP, Merchant M, Orr C, Chan J, Den OD, Berry L, et al.Intermittent administration of MEK inhibitor GDC-0973 plus PI3Kinhibitor GDC-0941 triggers robust apoptosis and tumor growth inhi-bition. Cancer Res 2012;72:210–9.
13. Lorusso PM, Krishnamurthi SS, Rinehart JJ, Nabell LM, Malburg L,Chapman PB, et al. Phase I pharmacokinetic and pharmacodynamicstudy of the oral MAPK/ERK kinase inhibitor PD-0325901 in patientswith advanced cancers. Clin Cancer Res 2010;16:1924–37.
14. Iverson C, Larson G, Lai C, Yeh LT, Dadson C, Weingarten P, et al.RDEA119/BAY 869766: a potent, selective, allosteric inhibitor ofMEK1/2 for the treatment of cancer. Cancer Res 2009;69:6839–47.
15. Isshiki Y, Kohchi Y, Iikura H, Matsubara Y, Asoh K, Murata T, et al.Design and synthesis of novel allosteric MEK inhibitor CH4987655 asan orally available anticancer agent. Bioorg Med Chem Lett 2011;21:1795–801.
16. Lee L, Niu H, Rueger R, Igawa Y, Deutsch J, Ishii N, et al. The safety,tolerability, pharmacokinetics, and pharmacodynamics of single oraldoses of CH4987655 in healthy volunteers: target suppression using abiomarker. Clin Cancer Res 2009;15:7368–74.
17. LeijenS,MiddletonM, TrescaP, Kraeber-Bodere F, Dieras V, ScheulenME, et al. Phase I (Ph) safety, pharmacodynamic (PD), and pharma-cokinetic (PK) trial of a pure MEK inhibitor (i), RO4987655, in patientswith advanced/metastatic solid tumor. J Clin Oncol 29, 2011 (suppl;abstr 3017).
18. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS,Rubinstein L, et al. New guidelines to evaluate the response to treat-ment in solid tumors. European Organization for Research and Treat-ment ofCancer,NationalCancer Instituteof theUnitedStates,NationalCancer Institute of Canada. J Natl Cancer Inst 2000;92:205–16.
Leijen et al.
Clin Cancer Res; 18(17) September 1, 2012 Clinical Cancer Research4804
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

19. National Cancer Institute Cancer Therapy Evaluation Program Com-mon Terminology Criteria for Adverse Events, version 3.0. [cited 2006Aug 9]. Available from: http://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcaev3.pdf.
20. Young H, Baum R, Cremerius U, Herholz K, Hoekstra O, LammertsmaAA, et al. Measurement of clinical and subclinical tumour responseusing [18F]-fluorodeoxyglucose and positron emission tomography:review and 1999 EORTC recommendations. European Organizationfor Research and Treatment of Cancer (EORTC) PET Study Group. EurJ Cancer 1999;35:1773–82.
21. Delord J, Houede N, Awada A, Taamma A, Faivre SJ, Besse-HammerT, et al. First-in-human phase I safety, pharmacokinetic (PK), andpharmacodynamic (PD) analysis of the oral MEK-inhibitor AS703026(two regimens [R]) in patients (pts) with advanced solid tumors. J ClinOncol 28:15s, 2010 (suppl; abstr 2504).
22. Infante JR, Fecher LA, Nallapareddy S, Gordon MS, Flaherty KT, CoxDS, et al. Safety and efficacy results from the first-in-human study ofthe oral MEK 1/2 inhibitor GSK1120212. J Clin Oncol 28:15s, 2010(suppl; abstr 2503).
23. Thompson DS, Flaherty K, MessersmithW, Harlacker K, NallapareddyS, Vincent C, et al. A three-part, phase I, dose-escalation study ofGSK1120212, a potent MEK inhibitor, administered orally to subjectswith solid tumors or lymphoma. J Clin Oncol 27, 2009 (suppl; abstre14584).
24. Ciuffini L, Castellani L, Salvati E, Galletti S, Falcone G, Alema S.Delineating v-Src downstream effector pathways in transformedmyo-blasts. Oncogene 2008;27:528–39.
25. KolchW.Meaningful relationships: the regulation of the Ras/Raf/MEK/ERK pathway by protein interactions. Biochem J 2000;351 Pt 2:289–305.
26. Garcia R, Grindlay J, Rath O, Fee F, Kolch W. Regulation of humanmyoblast differentiation by PEBP4. EMBO Rep 2009;10:278–84.
27. Lawlor MA, Feng X, Everding DR, Sieger K, Stewart CE, Rotwein P.Dual control of muscle cell survival by distinct growth factor-regulatedsignaling pathways. Mol Cell Biol 2000;20:3256–65.
28. Leijen S, Soetekouw PM, Jeffry Evans TR, Nicolson M, Schellens JH,LearoydM, et al. A phase I, open-label, randomized crossover study toassess the effect of dosing of the MEK 1/2 inhibitor Selumetinib(AZD6244; ARRY-142866) in the presence and absence of food inpatients with advanced solid tumors. Cancer Chemother Pharmacol2011;68:1619–28.
29. Lorusso PM, Adjei AA, Varterasian M, Gadgeel S, Reid J, Mitchell DY,et al. Phase I and pharmacodynamic study of the oralMEK inhibitor CI-1040 in patients with advanced malignancies. J Clin Oncol2005;23:5281–93.
30. Meng J, Fang B, Liao Y, Chresta CM, Smith PD, Roth JA. Apoptosisinduction by MEK inhibition in human lung cancer cells is mediated byBim. PLoS One 2010;5:e13026.
31. Wang YF, Jiang CC, Kiejda KA, Gillespie S, Zhang XD, Hersey P.Apoptosis induction in human melanoma cells by inhibition of MEK iscaspase-independent and mediated by the Bcl-2 family membersPUMA, Bim, and Mcl-1. Clin Cancer Res 2007;13:4934–42.
32. Van den Abbeele AD, Badawi RD. Use of positron emission tomog-raphy in oncology and its potential role to assess response to imatinibmesylate therapy in gastrointestinal stromal tumors (GISTs). EurJ Cancer 2002;38 Suppl 5:S60–5.
33. Stroobants S, Goeminne J, SeegersM, Dimitrijevic S, Dupont P, NuytsJ, et al. 18FDG-Positron emission tomography for the early predictionof response in advanced soft tissue sarcoma treated with imatinibmesylate (Glivec). Eur J Cancer 2003;39:2012–20.
34. Zander T, SchefflerM,Nogova L, KobeC, Engel-RiedelW,HellmichM,et al. Early prediction of nonprogression in advanced non–small-celllung cancer treated with erlotinib by using [(18)F]fluorodeoxyglucose
and [(18)F]fluorothymidinepositronemission tomography. JClinOncol2011;29:1701–8.
35. Aukema TS, Kappers I, Olmos RA, Codrington HE, van TH, van PR,et al. Is 18F-FDG PET/CT useful for the early prediction of histopath-ologic response to neoadjuvant erlotinib in patientswith non–small celllung cancer? J Nucl Med 2010;51:1344–8.
36. Bystrom P, Berglund A, Garske U, Jacobsson H, Sundin A, Nygren P,et al. Early prediction of response to first-line chemotherapy bysequential [18F]-2-fluoro-2-deoxy-D-glucose positron emissiontomography in patients with advanced colorectal cancer. Ann Oncol2009;20:1057–61.
37. Bonanno L, SchiavonM, Nardo G, Bertorelle R, Bonaldi L, Galligioni A,et al. Prognostic and predictive implications of EGFRmutations, EGFRcopy number and KRAS mutations in advanced stage lung adenocar-cinoma. Anticancer Res 2010;30:5121–8.
38. Douillard JY, Shepherd FA, Hirsh V, Mok T, Socinski MA, Gervais R,et al. Molecular predictors of outcome with gefitinib and docetaxel inpreviously treated non–small-cell lung cancer: data from the random-ized phase III INTEREST trial. J Clin Oncol 2010;28:744–52.
39. Massarelli E, Varella-Garcia M, Tang X, Xavier AC, Ozburn NC, Liu DD,et al. KRASmutation is an important predictor of resistance to therapywith epidermal growth factor receptor tyrosine kinase inhibitors in non–small-cell lung cancer. Clin Cancer Res 2007;13:2890–6.
40. Flaherty KT, Puzanov I, Kim KB, Ribas A, McArthur GA, Sosman JA,et al. Inhibition of mutated, activated BRAF in metastatic melanoma. NEngl J Med 2010;363:809–19.
41. Bollag G, Hirth P, Tsai J, Zhang J, Ibrahim PN, Cho H, et al. Clinicalefficacy of a RAF inhibitor needs broad target blockade in BRAF-mutant melanoma. Nature 2010;467:596–9.
42. Su F, Yang H, Higgins B, Kolinsky K, Packman K, Kim M, et al.Molecular mechanisms underlying disease relapse on treatment withselective BRAF inhibitor vemurafenib (PLX4032). J Clin Oncol 29, 2011(suppl; abstr 8517).
43. Infante J, FalchookG, LawrenceD,Weber J, Kefford R, Bendell J, et al.Phase I/II study to assess safety, pharmacokinetics, and efficacy of theoral MEK 1/2 inhibitor GSK1120212 (GSK212) dosed in combinationwith the oral BRAF inhibitor GSK2118436 (GSK436). J Clin Oncol 29,2011 (suppl; abstr CRA8503).
44. Kurzrock R, Patnaik A, Rosenstein L, Fu S, Papadopoulos K, Smith D,et al. Phase I dose-escalation of the oral MEK1/2 inhibitorGSK1120212 (GSK212) dosed in combination with the oral AKTinhibitor GSK2141795 (GSK795). J Clin Oncol 29, 2011 (suppl; abstr3085).
45. Shapiro G, LoRusso P, Kwak E, Cleary J, Musib L, Jones C, et al.Clinical combination of the MEK inhibitor GDC-0973 and the PI3Kinhibitor GDC-0941: a first-in-human phase Ib study testing daily andintermittent dosing schedules in patients with advanced solid tumors.J Clin Oncol 29, 2011 (suppl; abstr 3005).
46. Tolcher A, Baird R, Patnaik A, Moreno Garcia V, Papadopoulos K,Garrett C, et al. A phase I dose-escalation study of oral MK-2206(allostericAKT inhibitor) with oral selumetinib (AZD6244;MEK inhibitor)in patients with advanced or metastatic solid tumors. J Clin Oncol 29,2011 (suppl; abstr 3004).
47. McDaid HM, Lopez-Barcons L, Grossman A, Lia M, Keller S, Perez-Soler R, et al. Enhancement of the therapeutic efficacy of taxol bythe mitogen-activated protein kinase kinase inhibitor CI-1040 innude mice bearing human heterotransplants. Cancer Res 2005;65:2854–60.
48. Haass NK, Sproesser K, Nguyen TK, Contractor R, Medina CA,Nathanson KL, et al. The mitogen-activated protein/extracellular sig-nal-regulated kinase kinase inhibitor AZD6244 (ARRY-142886)induces growth arrest in melanoma cells and tumor regression whencombined with docetaxel. Clin Cancer Res 2008;14:230–9.
Phase I Study of the MEK Inhibitor RO4987655
www.aacrjournals.org Clin Cancer Res; 18(17) September 1, 2012 4805
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868

2012;18:4794-4805. Published OnlineFirst July 5, 2012.Clin Cancer Res Suzanne Leijen, Mark R. Middleton, Patricia Tresca, et al. (CH4987655) in Patients with Advanced Solid Tumorsand Pharmacodynamics of the MEK Inhibitor RO4987655 Phase I Dose-Escalation Study of the Safety, Pharmacokinetics,
Updated version
10.1158/1078-0432.CCR-12-0868doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2012/07/05/1078-0432.CCR-12-0868.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/18/17/4794.full#ref-list-1
This article cites 40 articles, 22 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/18/17/4794.full#related-urls
This article has been cited by 7 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/18/17/4794To request permission to re-use all or part of this article, use this link
on February 23, 2021. © 2012 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 5, 2012; DOI: 10.1158/1078-0432.CCR-12-0868