Embed Size (px)
DESCRIPTION
Pharma July-August 2011
Citation preview

w w w. p h a r m a - m a g . c o m
The global magazine for the pharmaceutical and biopharmaceutical industry
July/August 2011 ISSN 1746-174X Volume 7 Number 4
Clinical TrialsImproving Patient Retention
BiotechnologyOptimizing Oncolytic Viruses
Freeze DryingControlling Ice Nucleation Temperature
GENERICS & BIOSIMILARS
CORPORATE
PROFILES
Trends, Regulations and Opportunities

STRAP
2 www.pharma-mag.com September/October 2011
The perfecT fiT for Today’s challenges!
Your global Partner
Kirsch Pharma – the leading supplier of raw materials to the food, pharmaceutical, complementary medicine, cosmetic and veterinary industry. backed by a global procurement network serving more than 3000 customers worldwide. Including a range of products specifically catering to your needs. adding value to your final product.
Documentation additional specification parameters, just ask!
Physical Modification the production focused solution.
Blends Ingredients/excipients blended to your own bespoke requirements.
Bespoke Packaging addressing your specific needs, bespoke packaging materials packed to your batch size.
Client Relationships a caring professional attitude towards our client needs.
benefIts wIth KIrsch Pharma
Phone or email us now to start the process that will provide the same benefits for your business.
www.kirschpharma.com
Local contact in UK: mr. Pat reilly phone 0044 (0) 7834 486109 [email protected]

STRAP
2 www.pharma-mag.com July/August 2011
THE PERFECT FIT FOR TODAY’S CHALLENGES!
YOUR GLOBAL PARTNER
Kirsch Pharma – the leading supplier of raw materials to the food, pharmaceutical, complementary medicine, cosmetic and veterinary industry. Backed by a global procurement network serving more than 3000 customers worldwide. Including a range of products specifically catering to your needs. Adding value to your final product.
Documentation Additional specification parameters, just ask!
Physical Modification The production focused solution.
Blends Ingredients/excipients blended to your own bespoke requirements.
Bespoke Packaging Addressing your specific needs, bespoke packaging materials packed to your batch size.
Client Relationships A caring professional attitude towards our client needs.
BENEFITS WITH KIRSCH PHARMA
Phone or email us now to start the process that will provide the same benefits for your business.
www.kirschpharma.com
Local contact in UK: Mr. Pat Reilly phone 0044 (0) 7834 486109 [email protected]

July/August 2011 www.pharma-mag.com 3
Contents
CPhI Preview: More Talking Less Walking
Annemieke Timmers — UBM Live
The Brand Director of CPhI Worldwide talks to Pharma
about the new features of this year’s event in Frankfurt.
Freeze Drying: The Importance of Controlling Ice Nucleation
TemperatureMark Shon and Leslie Mather — SP Scientific
Combining technologies to significantly enhance cycle
optimization and scale-up.
Technology: Rising to the Challenge
R. Arun Kumar — Infosys
How technology is shaping the pharmaceutical industry.
SAEs: Streamlining SAE Reporting
Linda Bowers — IntraLinks
Switching to an online method for SAE reporting and
notification is the way to go.
Biotechnology: The Evolution of a
Novel Form of Cancer TherapeuticsJohn Beadle — PsiOxus
How can oncolytic viruses be optimized given the
emerging complexity of the cancer cell and its environment?
Facility Design: Design for Impact
Javier Ballesteros Cherp — Telstar Life Science
Value Services
Obtaining the best design possible by considering how
every detail will affect the quality of the manufactured final product.
CONTENTS
Marketing & Branding: The Voice of Society
Nicolas Mamier — Appetite
Align the values of your company with those of your
brands to gain support and commitment.
Legislation: How Adequate are your
Anticorruption Procedures?Andrew Legg and Joanne Skoulikas — Mayer Brown
Advice on how to ensure your business does not
unwittingly fall foul of the UK’s Bribery Act.
FOCUS TOPICSGenerics & BiosimilarsContributing Companies: PharmaNet,
Thomson Reuters, Charles River Laboratories,
PA Consulting, Fuld & Company, PMR, ZS Associates
and Bird & Bird.
Industry experts discuss a variety of themes and trends influencing
the sector.
Clinical TrialsContributing Companies: Horizon Discovery,
Wiggin & Dana, ERT, Exco InTouch and Greenphire.
A glimpse of modernizing cancer drug development;
new FDA informed consent regulations; prospective
assessment of suicidality; improving patient retention; and
transforming subject payment.
JULY/AUGUST 2011
For up-to-date news follow us on Twitter (PharmaMag) and join our Pharma group discussions on LinkedIn
08 22
32
34
52
38
54
REGULARSFrom the Editor: Pharming Daffodils
Corrine Lawrence
A commercially viable alternative for Welsh hill
farmers brings hope to individuals suffering from
Alzheimer’s disease.
Stem Cells: A Matter of Definition?
Robert Lundie-Smith — McDermott Will & Emery
Regulatory implications of Advocate General Bot’s
recommendation on the patentability of stem cell
derived inventions.
Nostrapharmus: A Generic Formulation
Nostrapharmus
To successfully take advantage of the impending
patent cliff, generic drug manufacturers need to
combine science and business acumen.
05
06
58
FEATURES
42
46
48
4 www.pharma-mag.com July/August 2011
STAFF
editorCorrine Lawrence+44 (0) 771 517 [email protected]
editorial DirectorKevin Robinson+44 (0) 1392 202 [email protected]
Art Director/Production Paul AndrewsTel. +44 (0) 1372 364 126 [email protected]
Content/Marketing ManagerClaire Day Tel. +44 (0) 1372 364 129 [email protected]
sales ManagerFred Winsor+44 (0) 1372 364 [email protected]
Financial ControllerCatherine Swainson+44 (0) 1372 364 [email protected]
General ManagerMiranda Docherty+44 (0) 1372 364 [email protected]
The Editorial Advisory Board of Pharma comprises a distinguished panel of experts from various
parts of the pharmaceutical industry. They review technical manuscripts, suggest topics for
inclusion, recommend subject matter and potential authors, and act as the quality control
department for the magazine’s editorial content and direction.
Rory Budihandojo
Director, Quality
Systems Audit
Boehringer Ingelheim Shanghai
Pharmaceuticals Co., Ltd
Patrick Crowley
Vice President
Product Line Extensions
GSK (US)
Enric Jo
Plant Director
Reig Jofre Group
Maik W. Jornitz
Senior Vice President
Global Product Management,
Bioprocess
Sartorius North America Inc.
Carlos Lopez
Relationship Director
Healthcare & Pharmaceuticals
Lloyds TSB Corporate Markets
Gino Martini
Director, Strategic Technologies
GSK (UK)
Jim McKiernan
Chief Executive Officer
McKiernan Associates GmbH
Maireadh Pedersen
Head of Business Development
Quay Pharma
Ray Rowe
Chief Scientist/Prof of
Industrial Pharmaceutics
Intelligensys/Uni of Bradford
Harald Stahl
Senior Pharmaceutical
Technologist
GEA Pharma Systems
Kurt Speckhals
Senior Director, Supply Chain
Pfizer Inc.
Geoff Tovey
Visiting Professor
Dept of Pharmacy
King’s College
Wes Wheeler
President,
WPWheeler LLC
Editorial Advisory Board
Registered Office: Via Media UK Ltd, 22 Highacre, Dorking, Surrey RH4 3BF, UK.The publisher endeavours to collect and include complete, correct and current information in Pharma but does not warrant that any or all such information is complete, correct or current. The publisher does not assume, and hereby disclaims, any liability to any person or entity for any loss or damage caused by errors or omissions of any kind, whether resulting from negligence, accident or any other cause. Pharma does not verify any claims or other information appearing in any of the advertisements contained in the publication, and cannot take any responsibility for any losses or other damages incurred by readers in reliance on such content.
Copyright © 2011, Via Media UK Ltd All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording or information storage and retrieval system, without permission in writing from the publisher.
Send permission request in writing to Permissions Department, Pharma, Fax +44 870 487 3469.Authorisation to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted for libraries and other users registered with the Copyright
Licensing Agency, 90 Tottenham Court Road, London W1P 0LP, UK (ISSN: 1742-447X).
To subscribeProfessionals working within the industries we cover may receive Pharma free of charge on completion of a registration card. Individuals in other industries or countries may purchase a year’s subscription by sending a cheque for £100 made payable to : Via Media UK Ltd by post to: Via Media UK Ltd, Wesley House, Bull Hill, Leatherhead, Surrey, KT22 7AH, UK.
Contributors
Innovative Filtration...
The ZetaPlus Encapsulated System
Reduce total filtration costs without compromising quality
3M Purification’s new easy to use, disposable, ergonomically designed system for the bio processing industry has been designed for upstream clarification and downstream applications where impurity removal is essential.
• Reduced machine Downtime• Ease of Use• Minimal product loss• Low cleaning costs• Reduced operator exposure
To find out more about 3M Purification and any of our products, call us or visit us online0845 602 5237www.3M.co.uk/filtration 3

FROM THE EDITOR
Corrine Lawrence
Editor, Pharma
With its unique design, the Glass Oven B-585 opens a wide range of possibilities for the laboratory.Kugelrohr drying ■ , vacuum distillation, sublimation and freeze drying in one instrumentShort heat-up times ■ to a maximum of 300°C and excellent visibility of the drying substancesGentle drying of minimal sample quantities ■ (5 to 40 ml) thanks to vacuum proofed glass designBall tube distillations ■ with rotation function up to 50 rpm
Additional information is available on www.buchi.com>Evaporation Solutions>Glass Oven
BÜCHI Labortechnik AG9230 Flawil / SwitzerlandT +41 71 394 63 63www.buchi.com Quality in your hands
B-585 - the multi-talented in every laboratoryGlass Oven
Issue4_Pharma_GlassOven_halfpage_210x148.indd 1 22/06/2011 10:05:27
A t a time when competition in the generics arena is intensifying and global economics are shaping business strategies, I was heartened to learn of a venture occurring in the
mountains of Wales that is uniting hill farmers and the pharmaceutical industry through the cultivation of daffodils. Whilst relaxing in front of the television recently, I found myself engrossed in a short film concerning a particularly potent characteristic of daffodils. This humble national flower of Wales, I discovered, produces galanthamine — a natural alkaloid that has the potential to significantly slow down the progress of the debilitating Alzheimer’s disease. Galanthamine is found only in the snowdrop and daffodil family; and, although it can be synthesized, the process is, rather unsurprisingly, costly and complex. Professor Trevor Walker and his team at Alzeim have identified galanthamine in commercially viable amounts in certain varieties of Wales-grown daffodil — the API is found only in a few varieties of daffodil and only in significant quantities when it’s
grown at specific altitudes (preferably at a height of 1100 to 1200 feet), which stresses the plant and causes it to produce the chemical.
Some Welsh sheep farmers, who no longer feel that hill farming has a commercial or viable future, have now turned their hand to growing daffodils as an alternative source of the drug as generic manufacturers seek to develop and market an off-patent version of Reminyl. The market is currently worth approximately $8 billion and the occurrence of Alzheimer’s is increasing at an alarming rate. Treating Alzheimer’s with the cheaper alternative of galanthamine, therefore, has the potential to improve the lives of thousands of people. Isn’t it wonderful when the solution to a difficult problem turns out to be relatively simple and is to be found, quite literally, under our very noses? This particular solution not only offers help to those suffering from Alzheimer’s, it also helps to keep pharma fertile and provides hill farmers with a new revenue stream. Now, if someone could just find something equally constructive to do with dandelions, I know where there are plenty!
PhARMING DAffODILS

6 www.pharma-mag.com July/August 2011
COMMENT
STEM CELLSA MATTER Of DEfINITION?
the AG recently delivered a controversial opinion to the Court of Justice of the European Union (CJEU) on the emotive topic of patents in human embryonic stem cell (HeS) research. The AG was
of the opinion that the exclusions from patentability for inventions using human embryos for industrial or commercial purposes (as found in Article 6(2)(c) of Directive 98/44/EC [“the Directive”] meant that an invention could not be patentable where the application of the technical process for which the patent was filed necessitated the prior destruction of human embryos or their use as a base material, even if the description of that process in the patent does not contain any reference to human embryos.
The opinion represents the first time that the CJEU has had to address the meaning of this exclusion, but it is not the first time that this issue has arisen on a pan-European basis. Rule 28(c) of the European Patent Convention provides the same exclusions to patentability and in November 2008 its interpretation was considered by the Enlarged Board of Appeal of the European Patent Office (EPO) in case G_2/06 Wisconsin Alumni Research Foundation (WARF). The AG’s proposed interpretation is closely allied with the interpretation already adopted by the EPO in WARF.
One must therefore ask why the AG’s opinion has been met with such opposition 2.5 years after the decision in WARF; and why this opinion (if followed by the CJEU) would restrict patents for the use of HeS where the decision in WARF did not? The answer lies in a consideration of the different implications of the AG’s opinion and the decision in WARF in relation to a particular class of HeS — pluripotent HeS.1
The Directive does not define ‘embryo’ and interpretation of this term was left for each Member State. The AG, however, considers that harmonization of patent protection for biotechnological inventions cannot be achieved unless a common definition of embryo is employed. In this regard he considers that all stages of development following fertilization that can result in human life should constitute the legal definition of embryo. This includes totipotent cells (which appear after fusion of gametes) and unfertilized ova into which a cell nucleus has been inserted or whose division has
been stimulated by parthenogenesis and the blastocyte. Although the AG (in line with the majority of Member States’ legislation) did not consider that pluripotent HeS fell within this definition of an embryo (as such cells were not capable of developing into a complete human being), he did consider that their use was still excluded from patentability as “it is not possible to ignore the origin of this pluripotent cell.”
The difference between the approach of the AG and that of the Enlarged Board in WARF, is that the latter still left the door open to the Convention States to determine (a) what was a human embryo, and (b) what ‘use’ necessarily results in the destruction of such an embryo (for example, could this include the use of HeS from an already established cell line?); which in turn left the door open to patents for the use of pluripotent HeS.
This open door can be seen from the advice given by the UK Intellectual Property Office following WARF where they commented that “commercial exploitation of inventions concerning [pluripotent HeS] would not be contrary to public policy or morality in the UK.”2 Furthermore, some Member States only legally consider that an embryo comes into existence upon transplantation of a fertilized ovum in the endometrium. In such Member States the in vitro blastocyte would not be an embryo, and the taking of pluripotent HeS from the blastocyte would not, therefore, result in the destruction of an embryo or its use as a base material. The AG’s opinion, if followed, would close these doors.
There is, of course, controversy regarding research using HeS. A lack of patentability for the use of pluripotent HeS will not in itself prevent research in this field and will not even prevent commercialization of such inventions; if research is permitted, some commercialization is bound to occur. What it is likely to do is reduce the funding coming into such research. This is a controversial issue and as the Member States appear to have reserved the definition of an embryo and the specific meaning of what would be contrary to public morality to themselves, this raises the question as to whether the CJEU should be ruling on these specific points at all, or continuing to leave the definition of an embryo up to the Member States.
Regulatory implications of Advocate General Bot’s (the AG) recommendation on the patentability of stem cell derived inventions under European law and the robust response from stem cell scientists.
References1. Cells derived from the
inner cell mass of a human
blastocyst which
in vitro are able to give rise
to all different cell types,
but cannot develop into an
embryo on their own
2. www.ipo.gov.uk/p-pn-
stemcells-20090203.htm
For more informationRobert Lundie-Smith
Associate, Intellectual
Property
McDermott Will & Emery
Tel. +44 207 557 [email protected]
Robert Lundie-Smith

July/August 2011 www.pharma-mag.com 7

8 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
ThE ChANGING BIOSIMILARS MARKETPLACERecent developments and projects, along with new regulations, are set to create new dynamics within the biosimilars market.
B iosimilars comprise one of the fastest growing segments of the pharmaceutical industry, according to US-based market research firm Decision Resources.1 Following the establishment of a
biosimilar approval pathway by the European Medicines Agency (EMA) in 2003 and the recent US legislation, the biosimilars regulatory landscape has changed significantly. In November 2010, FDA held a 2‑day public hearing on the Biologics Price Competition and Innovation Act of 2009 (BPCI Act) and the EMA recently released for consultation a draft guideline on biosimilars containing monoclonal antibodies. Then, in February 2011 it was announced that US regulators plan to unveil rules for reviewing the first copies of biologic medicines very soon, according to FDA Commissioner Margaret Hamburg. 2,3
On 23 March 2010, President Obama signed into law the Patient Protection and Affordable Care Act, a provision of which is the BPCI Act. The BPCI Act amends Section 351 of the Public Health Services Act to create an abbreviated approval pathway for biological products that are demonstrated to be highly similar (biosimilar) to an FDA-approved biological product. It also allows for the possibility of interchangeable biologics. The BPCI Act aligns with FDA’s longstanding policy of permitting appropriate reliance on what is already known about a drug, thereby saving time and resources, and avoiding unnecessary duplication of human or animal testing in clinical trials.
Structural SimilarityAt the core of biosimilarity is the initial need to define and establish structural similarity for therapeutic proteins using appropriate analytical techniques. This becomes particularly challenging as protein complexity increases as a result of increasing molecular weight and potential for post‑translational modifications. The general requirements for the licensing of biosimilars are outlined in the Act, which states that an application for a biosimilar product should contain information demonstrating that the biological product is biosimilar to a reference product based on the following:
• Analytical studies demonstrating that the biological product is highly similar to the reference product.
• Animal studies including an assessment of toxicity.• Clinical studies, including an assessment of
immunogenicity and pharmacokinetics, as well as, where applicable, pharmacodynamics.
It has been left to FDA to establish and evaluate the detailed requirements for specific therapeutic proteins or classes of therapeutic proteins.
Accomplishing Lower Cost BiologicsFDA held a 2-day public hearing in November 2010, to obtain input from interested stakeholders on specific issues and challenges associated with the implementation of the BPCI Act. Members of FDA, consumer advocates and major industry stakeholders including pharmaceutical innovator companies, biosimilar drug development companies, drug distribution entities and clinical research organizations (CROs) attended the hearing. The docket was left open until the end of 2010 to allow for additional comments from stakeholders.
Although all parties generally agreed on the benefits of lower cost biologics, there seemed to be two differing positions on how to accomplish it. The innovator companies and consumer advocate groups focused on the need to obtain sufficient preclinical and robust clinical data to ensure safety and efficacy. They did not favour automatic interchangeablility and were cautious about extrapolation to other indications without appropriate studies. Consumer groups were particularly concerned about safety and efficacy issues associated with aggressive abbreviated development programmes.
The other position, primarily represented by biosimilar and drug distribution companies, put more emphasis on the demonstration of analytical similarity with less focus on conducting what might be unnecessary, preclinical animal and clinical studies. They also favoured interchangeability and extrapolation to other indications.
In addition, particularly with regard to pending monoclonal antibody biosimilar drug development, it became apparent that innovative trial designs would

July/August 2011 www.pharma-mag.com 9
GENERICS & BIOSIMILARS
likely be needed to complete a reasonably sized clinical programme. It was also acknowledged that the biosimilar drug development/approval process in Europe has been smooth and generally without problems; therefore, a question was raised as to why those approved biosimilars could not enter the US market with minimal additional development effort. This concept, however, is foreign to FDA because it could imply approving a biosimilar drug based on comparative studies to an innovative product unapproved by FDA.
Exclusivity, Approval and User FeesFurther developments in the US include the Obama Administration’s recent proposal that the biologic drug exclusivity period should be reduced from 12 years as currently stated in the legislation to 7 years, to reduce healthcare costs. The Congressional Budget Office estimates that US citizens will save approximately $25 billion during the 2009–2018 period owing to government rules allowing the production and trade of copies of biotechnology drugs.4 Given the current controversies in the Healthcare law, however, it is uncertain if and when this proposal would advance. FDA plans to finalize the US biosimilar approval pathway soon and introduce regulations for reviewing the first copies of biologic medicines. FDA Commissioner Margaret Hamburg, however, has not specified when the first biosimilar products may be approved under the new rules. Companies are already submitting applications to FDA for biosimilar products.
Within the next few months, FDA aims to discuss with the industry how much the agency should charge as a user fee to review applications of biosimilar products under the new legislation. To date, generic drug applications have not been charged user fees, whereas the agency charges approximately $1.5 million in user fees for new brand-name product applications. In return for payment, FDA is willing to provide biosimilar drug manufacturers with feedback during product development, as well as timely consideration of whether their products could be automatically substituted for brand-name medicines.
EMA’s Guideline on Monoclonal AntibodiesWhen FDA sought input regarding the implementation of the BPCI Act, EMA, in an attempt to introduce product‑specific regulations, released (for a 6‑month consultation period) a draft guideline on biosimilar medicines containing monoclonal antibodies. Monoclonal antibodies have been established as a major product class of biotechnology-derived medicinal products. The new EMA guideline lays down the nonclinical and clinical requirements for
monoclonal antibody-containing medicinal products claiming to be similar to another product already marketed. The nonclinical section of the guideline addresses the pharmaco-toxicological requirements, whereas the clinical section refers to the requirements for pharmacokinetic, pharmacodynamic, efficacy and safety studies, as well as pharmacovigilance aspects.5
With regard to nonclinical development, a risk-based approach to evaluate monoclonal antibodies on a case-by-case basis is recommended to decide on the choice and extent of in vitro and in vivo studies. As a general rule, nonclinical studies should be performed prior to initiating clinical development. In vitro studies should be conducted first and a decision should then be made as to the extent of what, if any, in vivo work will be required.
The conduct of large comparative toxicological studies in nonhuman primates is not recommended by the guideline. It does mandate, however, that the approach taken will need to be fully justified. Conversely, considering clinical development, a comparative pharmacokinetic study in a sufficiently sensitive and homogeneous study population normally forms an integral part of biosimilar monoclonal antibodies development, usually in a parallel group design because of the long half-life of monoclonal antibodies and potential interference of immunogenicity. Also, as mentioned earlier, the use of validated biomarkers and surrogate endpoints in clinical trials will be considered/encouraged.
ConclusionAn abbreviated approval pathway for biosimilars presents challenges given the scientific and technical complexities associated with the larger and often more complex structures of these products. As a result, there is much debate and diverse opinions among stakeholders, as demonstrated at the recent 2-day FDA hearing. Patient safety (immunogenicity) will emerge as a key issue and carefully designed clinical trials will be crucial in this process, perhaps with a focus using validated biomarkers and surrogate endpoints to minimize unnecessary clinical trial duration or patient exposure. New legislation will ensure the development of biosimilar drugs with the same efficacy and safety as innovator products, thereby safeguarding public health whilst also generating significant healthcare cost savings. Fortunately, the European experience with biosimilars demonstrates that their safe and effective development is a reality. Industry-leading CROs with experience in clinical development and regulatory issues of branded innovator biologics and generic drugs will play a key role in guiding industry members developing biosimilars, in line with new regulatory developments.
References1. http://decisionresources.com/
2. www.bloomberg.com/
news/2011-02-18/fda-says-
rules-for-copying-amgen-
biotechnology-drugs-to-
arrive-very-soon-.html
3. S.M. Sensabaugh,
“Requirements for
Biosimilars and
Interchangeable Biologic
Drugs in the United States
— in Plain Language,”
Drug Inform. J 45, 155–162
(2011).
4. www.cbo.gov/ftpdocs/94xx/
doc9496/s1695.pdf
5. Guideline on similar
biological medicinal
products containing
monoclonal antibodies
(Draft), 18 November
2010, EMA/CHMP/
BMWP/403543/2010,
European Medicines
Agency, Committee for
Medicinal Products for
Human Use (CHMP).
For more informationJeffrey Freitag
Chief Medical Officer and
Executive VP Consulting
PharmaNet
www.pharmanet.com
Jeffrey Freitag

10 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
During the past 5 years, US companies have dramatically increased their biologics development — nearly 6000 clinical trials with a biological intervention have been reported since
2005. With combined sales totaling $30 billion in 2010, coupled with a recently introduced abbreviated approval pathway for follow-on biologics and an impending patent cliff for blockbuster drugs, the biologics arena looks set to offer a very enticing prospect to pharmaceutical companies and generics alike.1
But not so fast. The abbreviated approval pathway in the US has yet to be tested; as such, it is unclear what we can expect from this nascent market. Questions regarding the regulatory requirements for biosimilar approval still exist and debates on the topic of exclusivity continue a year after the passing of the Affordable Healthcare for America Act. Many forecast models rely on less-than-perfect data, often from outcomes in EU markets that do not reflect the likely dynamics of the US market. Also, it is unclear whether existing models have fully taken into account the potential incentives for follow-on biologic players in the US to file biologics licence applications (BLAs) rather than abbreviated biologics licence applications (aBLAs). If the filing is made through BLAs, the resulting product cannot be considered a biosimilar.
One point of clarity that has emerged is that dynamics of the biosimilar market are unlike those associated with the small molecule generics market. The differences between the policies regulating biosimilars and small molecules generics reflect the dramatic differences between the products themselves. Whereas established business strategies that have shaped the generics industry in the US such as paragraph IV patent challenges will not be part of the biosimilars market, new unique trends, including significant involvement from Big Pharma, are already emerging in US follow-on biologic competition.2
With Big Pharma companies such as Merck investing in follow-on biologics, the companies that will be jockeying for market share may have familiar names, but may not be associated with generic products. Because Big Pharma has unique advantages compared with generic companies regarding the ability to successfully compete in the follow-on biologics arena, namely existing manufacturing capabilities, funding, experience with clinical trials and physician detailing, it makes sense that Big Pharma companies would consider the opportunity.
Multinational generic companies that have already established themselves as biosimilar competitors in other regulated markets, such as Sandoz and Hospira, are also likely to be among the first to compete with follow‑on
biologic products in the US. As a result of their previous experience with biosimilar development and available resources, these major generic companies can capitalize on investments already made in other markets.
Because of provisions in the current US biosimilar regulations, generics may not be incentivized to use the abbreviated pathway but instead file a BLA for follow‑on biologic products, just as Teva did in 2009. Clinical trials may be required for biosimilar candidates to prove the safety and efficacy, similar to the BLA process. Additional studies will be required for biosimilars that are seeking approval for automatic substitution, or “interchangeability”
status. But these studies come at a cost, which some companies may find are not worth the benefits associated with biosimilar approval. Furthermore, under the current legislation, companies receiving approval for a BLA will be granted 12 years of exclusivity, which would limit competition from biosimilar products and thus be yet another motivator to follow the BLA rather than aBLA route. In addition, major generic companies may have improved upon the original biologic product, giving their product a competitive advantage in what may become a market where class competition becomes the norm.
It is possible this strategy employed by major generic companies is not a harbinger of future trends, and eventually the barriers to enter the biosimilars market in the US will diminish. If this proves not to be the case, then the emergence of a follow-on biologic market in the US could be the beginning of new paradigm in industry dynamics, where the line in the sand separating companies in the pharmaceutical industry isn’t based on innovation, but rather the ability to participate in the biologics/biosimilar market.
COMPETITION hEATS UP IN ThE BIOLOGICS MARKET
Notes1. Source: Thomson Reuters
Newport Premium/IMS.
2. ‘Paragraph IV challenge’
is the term for the
process established by
the Hatch-Waxman Act
and provides generic
companies with the
ability to challenge the
patents protecting drugs.
It has become a business
strategy used by major
generic companies to gain
market exclusivity pending
successful challenges.
For more informationAndrew F. Bourgoin
Pharmaceutical
Research Analyst
Thomson Reuters
Andrew F. Bourgoin
DyNAMICS OF ThE BIOSIMILAR MARkET ARE UNLIkE ThOSE ASSOCIATED wITh ThE SMALL MOLECULE GENERICS MARkET.
July/August 2011 www.pharma-mag.com 11

12 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
W orldwide, regulatory authorities have been grappling with the issue of generic competition for biological products. As guidelines have been developed, terms such as “subsequent entry
biologics” (Canada), “biocomparables” (Mexico) and “similar biotherapeutic products” (World Health Organisation) have been used, but the majority of issued international guidelines have settled on “biosimilar” to describe products whose quality, safety and efficacy are designed to be comparable to the originator or reference product.
As regulatory authorities develop approval processes for biosimilars, this type of product is arriving on the market — in Europe, Japan and other countries, companies are licensing biosimilar products. What returns on investment can manufacturers expect in this field? Data from the European experience shows that biosimilars enter at 60–90% of the originator price and can capture up to 30% of the market.1 The market share, however, tends to be split between several manufacturers licensing biosimilar products in a short period of time, with no single product taking significant market share. This situation is likely to be repeated in the US when biosimilars are approved there. In Asia, biosimilars have seen extensive growth with multiple manufacturers supplying local markets. These products will require significant additional testing, frequently with the help of a contract research organization (CRO), to demonstrate comparability with the originator before they are accepted on the more heavily regulated markets where higher prices are achievable.2
If biosimilars will not provide high returns, where should a company capable of developing a biologic, but without
the R&D resources of a major pharmaceutical company, look? Consider taking an existing product with a known target, safety and efficacy profile but with limited stability or dosing options because of the molecule’s characteristics. Add modifications to the molecule to improve the efficacy, dosing regime, safety or some other aspect that enhances the benefit of the product to patients, and you have a new, improved molecule or “bio-better.” Although these products require a full development and testing programme, they will qualify for patent protection and market exclusivity. Compared with a true originator product, the risk in developing a bio-better is significantly reduced and thus the potential for return on investment for a manufacturer is greatly improved.
The industry players for bio-betters cover a wide range, from the originators extending their product portfolio (and thus protecting their share of an indication market), to companies who wish to show their scientific advancement by becoming originators rather than copiers, to the CROs that work side-by-side with biopharmaceutical companies to help perform rigorous and cost-effective testing. The bio-better concept also encourages companies to develop platform technology for the modification of existing proteins and form partnerships with companies capable of producing the original proteins.
The question arises, which is better? Follow the biosimilar pathway with reduced development costs, but low market share at a reduced price, or take the full development cost knowing that the product is more likely to reach the market in a form that will capture a potentially larger share of the indication market at a premium price? The answer will tell us a great deal about the future of the biopharma industry.
SIMILAR OR BETTER?
For more informationNiall Dinwoodie
Head, Product
Characterization
Charles River Laboratories
References1. Federal Trade Commission
report, “Emerging
Healthcare Issues:
Follow-on Biologic Drug
Competition,” June 2009.
2. H. Schellekens,
“Biosimilar Epoetins: How
Similar are They?” Eur. J
Hosp. Pharm. Sci. 10(3),
43–47 (2004).
Drug treatment in the past has typically been an open-loop system. There has been little need for feedback of individual responses to medication beyond that required for clinical trials and market
approval. Closing the loop by means of diagnostics, payment-by-results and measurement of individual responses to treatment is becoming a reality that is being driven by hard economics. Underpinning this, enabling the accurate assessment of patient response, is recording the dosing regimen that the patient has administered.
Of all the stakeholders that have an interest in dosage monitoring it is the pharmaceutical company that is best placed to co-develop the technology with individual drugs, not least because the value of dose monitoring starts with product development. Its use becomes a powerful tool to demonstrate the cost-effectiveness of generic drugs compared with
new drugs, when taken by the right patients in the right way.
Although this incentive may be laid at generic pharma’s door, the specialist disciplines required to develop dose tracking technology range from device design, through software, sensing, communications and electronic technologies to industrial design and regulatory compliance are not those of a pharmaceutical company. Compared with drug development, however, the cost and timescale associated with device development is considerably less. Co-developing dose monitoring technology as part of a delivery or packaging system has never looked more attractive. The challenge to generic pharma is to embrace innovation partnerships laterally to drug development and secure the intellectual property that can prove newer drugs to have limited additional benefit compared with correctly-taken older drugs.
CLOSING ThE LOOP BETwEEN TREATMENT AND PATIENT RESPONSE DOSAGE MONITORING AND RECORDING
For more informationSarah Wren
Drug Delivery Group Leader
PA Consulting Services Ltd

July/August 2011 www.pharma-mag.com 13
2452AB CMO ad 210x280:Layout 1 11/07/2011 15:13 Page 1

14 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
european pharmaceutical firm competitive intelligence analysts polled at the 14th Annual Competitive Intelligence in Pharma Conference in January 2011 in Rome believe the US market will remain strong despite the new healthcare law. Yet,
they believe their companies are most vulnerable to generics and biosimilars eroding their market position in the coming years, according to a recent poll by Fuld & Company.1
The attendees ranked five issues (Figure 1) according to how vulnerable they believed their companies have become:• Shifting investment focus away from the US.• Increased focus on prevention and wellness.• Increased generic and biosimilar competition.• Developing differentiated products.• Lower US drug prices. They were most concerned by the threat of competition from generics and biosimilars. Where marginal differences exist between therapies and assessed by a range of data driven comparative effectiveness criteria — one is generic, the other is branded — generics are likely to win unless proven to be superior in a given population.
The introduction of the Patient-Centered Outcomes Research Institute (PCORI), which replaces the Agency for Healthcare Research and Quality (AHRQ), is likely to have a radical impact on the future of the US drugs market. Similar to the National Institute for Health and Clinical Excellence (NICE), it has the mandate
to undertake clinical comparative effectiveness in any therapy area. With sales and marketing accounting for more than 30% of pharmaceutical sales compared with only 15% for R&D, PCORI will force a radical restructuring of Big Pharma’s spend and how it operates. Manufacturers will need to rethink their R&D strategies perhaps by clearly identifying subpopulations of larger populations that are likely to benefit more from one compound than another with the assistance of genomic or biochemical biomarkers. Yet, given that linking a therapeutic with a diagnostic is still in its infancy, simpler biomarkers such as height, weight or ethnicity can be used to differentiate an individual brand. Where marginal differences exist between therapies and assessed by a range of data driven comparative effectiveness criteria — one is generic, the other is branded — generics are likely to win unless proven to be superior in a given population.
EUROPEAN PhARMA fEELING VULNERABLE
t he share of generic and biological drugs in the Russian pharmaceutical market is approximately 35–40% by value, according to the PMR report “Generic and Innovative Drugs
Market in Russia and Ukraine 2011: Comparative Analysis, Reimbursement Policies and Development Forecasts for 2011–2013.” According to our forecasts, between 2011 and 2013 the generic drug market in Russia is expected to witness a healthy growth of around 20% per annum (compound annual growth rate), assuming a constant euro to local currency rate. All market size forecasts presented in the report were prepared by PMR using statistical models that rely on historical data on the pharmaceutical market, macroeconomic, epidemiological and demographic indicators. There is a general trend in many countries, not only in Russia, toward switching to cheaper generic medicines, accelerated by the expiry of the patents of many blockbusters. In our opinion, branded generics represent the most promising subgroup on the Russian pharmaceutical market. Consumers in Russia are switching to more expensive products, and many
non-branded generics are being withdrawn from the market. The share of branded generics in the Russian pharmaceutical market increased by 0.6 percentage point (p.p.) between 2008 and 2009, whereas at the same time there was a decline of share of non‑branded generics by 0.1 p.p. (in only 2 years). The domestic production will focus mainly on biosimilars, high‑standard generic equivalents of original medicines or the so‑called “me‑too” projects (the manufacture of drugs that have an original patented formula that has a similar structure to the molecule of the class founder). Even now, many Russian manufacturers are developing in this direction; for example, Biocad is developing a biosimilar of Bayer’s Betaferon. As in other CEE countries, domestic drug manufacturers, as a result of limited financial sources for new drugs development, focus on the production of generic pharmaceuticals, whilst innovative medicines are, in most cases, manufactured by large, multinational concerns. There is a much higher share of generic medicines in the hospital segment in Russia than in other CEE countries, which shows the extent of underdevelopment of the healthcare system in the country.
For more informationAgnieszka Stawarska
Pharmaceutical Market
Analyst
PMR
Tel. +48 12 618 90 [email protected]
For more informationTony Nagle
UK & European
Managing Director
Fuld & Company
Tel. +44 207 659 6999www.fuld.com
Reference1. Fuld & Company, “EU
Sentiment Analysis of Obama
Health Reforms,” 2011.
Figure 1: Poll analysis.
TRENDS IN RUSSIA

July/August 2011 www.pharma-mag.com 15
INNOVATIVE PACKAGING SOLUTIONS.SHORT-RUN CAPABILITIES.
For more informati on, contact us at +353 184 183 00,
email us at [email protected], or visit www.millmounthealthcare.com
© Millmount Healthcare Ltd.
Download i-nigma Reader at App Store / Android Market
© 3GVision

July/August 2011 www.pharma-mag.com 59
“
“

July/August 2011 www.pharma-mag.com 15
INNOVATIVE PACKAGING SOLUTIONS.SHORT-RUN CAPABILITIES.
For more informati on, contact us at +353 184 183 00,
email us at [email protected], or visit www.millmounthealthcare.com
© Millmount Healthcare Ltd.
Download i-nigma Reader at App Store / Android Market
© 3GVision

July/August 2011 www.pharma-mag.com 15
INNOVATIVE PACKAGING SOLUTIONS.SHORT-RUN CAPABILITIES.
For more informati on, contact us at +353 184 183 00,
email us at [email protected], or visit www.millmounthealthcare.com
© Millmount Healthcare Ltd.
Download i-nigma Reader at App Store / Android Market
© 3GVision

July/August 2011 www.pharma-mag.com 15
INNOVATIVE PACKAGING SOLUTIONS.SHORT-RUN CAPABILITIES.
For more informati on, contact us at +353 184 183 00,
email us at [email protected], or visit www.millmounthealthcare.com
© Millmount Healthcare Ltd.
Download i-nigma Reader at App Store / Android Market
© 3GVision

16 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
Pharmaceutical companies are anxious to know the degree to which a branded competitor’s patent expiration will affect their own product. Once understood, companies must plan and make decisions
based on this anticipated effect. We advocate several tools to aid in this process. Benchmarking, analogue analysis and understanding customer and influencer insight can help anticipate the effect of generic competition; weighing return with risk and investment can help companies cope with the effects. Before adopting these tools, it is important that companies understand key factors — differentiation, treatment condition and payer focus — that cause and amplify ripples across a market, and the effect that these factors are likely to have.
DifferentiationThe level of product differentiation (or lack thereof) between brands and a competitor coming off patent has a profound effect on the market. Differentiation, in this context, can mean several things, including demonstrable safety or
efficacy advantages, unique benefits for certain patients or a special delivery mechanism.
The level of market disruption is usually in inverse proportion to the amount of differentiation among competitors. This is illustrated vividly in the statin market, when Merck’s Zocor (simvastatin) lost patent protection in the previous decade: doctors wrote 22 million prescriptions for Zocor in 2005; by 2007, after Zocor lost patent protection, the number fell to less than 1 million.1,2
For the statin market, annual growth jumped to 9%, compared with 6% annually prior to the introduction of generic Zocor.1,2 But for Pfizer’s Lipitor, a branded competitor, sales dropped 6% in 2007, compared with growth of 4% in 2006 (Figure 1).2,3 The lack of differentiation (in the eyes of payers) between Zocor and Lipitor played a major role in the decline — about 80% of patients on Lipitor had been using formulations of comparable efficacy to Zocor; thus, there was almost immediate substitution of Lipitor with generic simvastatin.4
Greater differentiation has led to lower market shocks, even to the point where the generic affects one branded product
fACTORS IN ThE GENERIC ‘RIPPLE EffECT’ Approximately 30 branded pharmaceutical products have or will come off patent between 2010 and 2012. These patent losses have implications for the branded drugs, but also for many of their competitors. These implications involve the effect of generic launch on overall market dynamics and what pharmaceutical companies can do to anticipate these effects.
Figure 1: Even while the
statin market grew as a
whole, Lipitor’s market share
and sales dropped with the
introduction of generic Zocor
due to a lack of differentiation
in the eyes of payers. Figure 1

July/August 2011 www.pharma-mag.com 17
GENERICS & BIOSIMILARS
only. Risperdal, a Johnson & Johnson atypical antipsychotic, lost 80% of its sales almost immediately after generic introduction (the first generic of an atypical antipsychotic).5 Yet other antipsychotics, such as market leader Seroquel, were barely affected. Why? One reason is that atypical antipsychotics have vastly different safety and side-effect profiles that differentiate them, and lead to prescribing decisions based on individual patient conditions.
And in the case of GlaxoSmithKline’s antibacterial Augmentin (amoxicillin-clavulanate), at least one competitor’s sales continued to rise after Augmentin lost patent in 2002. Whereas Augmentin sales fell 52% in the 12 months after it lost patent protection, sales of Pfizer’s Zithromax antibiotic rose 17%.6 There was a good reason for this — Augmentin required two tablets per day, Zithromax only required one.
Treatment ConditionWhen generic Ambien (zolpidem) went off patent, within a fortnight its market share of nonbarbiturate sleep aids fell from 42.4% to 12.5%.7 Unlike Lipitor, however, even as branded Ambien’s market share fell dramatically, the market share fell moderately for Rozerem (to 0.9% of the market) and Lunesta (6.7%), and only within several years (Figure 2).8
Compared with atypical antipsychotics, the difference is large — insomnia is usually a far less urgent condition than psychosis, and physicians are much more likely to allow for generic substitution for a sleep aid than an antipsychotic. Markets such as oncology, which treat serious conditions and demand specific treatment protocols, also are much more likely to resist generic effects. Payers are unlikely to demand physicians change their product preferences for treating a serious illness.
Payer FocusIn 2008 — even after generics were introduced — statins represented nearly 13% of all Medicare drug spending, making it the largest single drug class for Medicare.9 Prior to Zocor going off patent, statins were considered the largest driver of increases in total prescription spending nationwide. Because they were one of the largest payer burdens prior to patent expiration, statins were a clear candidate for generic product substitution.
Compared with statins, generic entry for nonbarbiturate sleep aids had a moderate effect only on the market. Sleep aids were moderately expensive products and so, payers were less focused on keeping costs down in this market as they were for statins. Because Ambien had a huge market share, payers immediately substituted its generic on formularies. It took them several years, however, before they became savvy as a group to the potential savings regarding generics.
Tools to Anticipate and Cope with DisruptionBenchmarking and Analogue AnalysisBenchmarking and analogue analysis supplement brand manager analysis of differentiation, treatment condition and payer focus. By comparing their market to similar ones in which generics have recently been introduced, companies can get an idea of their future in which a branded competitor loses patent protection.
Take the expiring patent of Cozaar-Hyzaar, and its effect on the angiotensin receptor blocker (ARB) class of products. When evaluating this market, brand managers could have looked to the statin market for clues to help predict what would happen next. Both statins and ARBs have relatively limited differentiation and heavy payer control.
References1. www.drugs.com/top200_
units_2005.html
2. www.drugs.com/top200_
units_2007.html
3. www.drugs.com/
top200_2006.html
4. www.fuld.com/News/
Ratcliffe_pharma_
alert_0608.pdf
5. http://decisionresources.
com/Products-and-
Services/Report.
aspx?r=algocg0609
6. MIDAS Sales Data, IMS
Health (2003).
7. http://blogs.wsj.com/
health/2007/05/16/
pharma-box-office-
ambien-falls-out-of-bed/
8. http://analystreports.
som.yale.edu/internal/
F2009/prof_ind/
IndustryPharmaJuly2009.pdf
9. http://medco.
mediaroom.com/
download/2009+DRUG+
TREND+REPORT.pdf
10. IMS National Prescription
Audit (March 2011).
11. Novartis International AG,
Second Quarter 2010 Financial
Report (15 July 2010).
Figure 2: Generic competition
caused branded Ambien to
see an immediate drop in
prescriptions; other brands’
market share experienced only
a small drop that happened
over several years.
Figure 2

18 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
Most of the branded ARBs lost market share to generic Cozaar-Hyzaar. Novartis’s Diovan, for example, went from 41.5% of the market in April 2010 to 34.2% a year later.10 But that only told part of the story — Diovan actually saw total sales increase 1% from the second quarter of 2009 to the second quarter of 2010.11 A possible reason is that Diovan is the only ARB approved for three cardiovascular indications. It’s important to stress that brand managers and prognosticators should not simply assume parallel results: dynamics change rapidly, and companies must be careful to avoid stale analogues and validate analysis with additional research.Examining Customer and Influencer InsightIn the US, payers generally favour generics to branded products; the former often replaces the latter in the first tier whereas brands are demoted to second- or third-tier status. This demonstrates that marketers need to consider the power of treatment influencers, such as payers and customers (physicians and patients).
The brand’s value proposition weighs heavily when considering how customers and influencers determine the effect of generic entry, as the value proposition often has a direct correlation to differentiation. When a brand has a
unique benefit that makes it irreplaceable, customers and even payers will hesitate before substituting a generic. Weighing Return With Risk and InvestmentIn markets with little differentiation, high payer focus and a non-life-threatening treatment condition, a market leader may not want to take any action when a competitor goes off patent. That might seem counterintuitive to some marketers, but taking such a viewpoint is consistent with taking into account a life cycle evaluation of alternatives.
There may be some situations in which a company is unable to stop a generic of a competing brand from wreaking havoc on the market, and it may make sense to shift sales and marketing resources elsewhere. Being able to anticipate this possibility enables executives to make optimal managerial decisions.
Patent expirations are leading to what could be a tumultuous time for branded competitors, but the market reaction to any given generic introduction is as varied as the pharmaceutical market itself. Likewise, when evaluating the effect of patent expiration on the market as a whole, disruption cannot be predicted by a single factor, nor can companies rely upon a single tool (Figure 3). Using all three tools in combination, however, can help give them insight into how the market will react — and provide guidance on what to do next.
For more informationJudith Kulich
Principal
ZS Associates
www.zsassociates.com
Figure 3: Balancing all three
tools against the three factors
market effects can help
pharmaceutical companies
both anticipate and react to the
introduction of a generic for
branded competition.
Figure 3

Just to make sure!
SCHMIDT® Flow Sensors surpass the reliable detection of pre-defi ned fl ow velocities and precisely measure the energy effi ciencies from clean room to clean room environments.
This is of high importance for individual safety and quality management.
Perfectly suitable for users and manufacturers of cleanrooms and phar-maceutical equipment with high quality demands.
SCHMIDT Technology GmbH78112 St. Georgen/Germany
Phone +49(0) 77 24 / 89 [email protected]
SCHMIDT® Flow Sensors
Simply a question ofbetter measurement
The high requirements of modern control technology in ventilation systems require an accurate measurement of volumetric flows in air or gases. Its documentation is essential in areas in which people or products are subject to safety requirements or the air conditions must meet certain hygienic requirements.
A perfect method of measuring volumetric flows is offered by thermal flow sensors from SCHMIDT Technology. The particular advantage of this technology is its wide measurement range, completely covering all relevant air and gas flows in air-conditioning technology for cleanrooms. This includes minimum air velocities, such as the ones observed during idle periods, and maximum flows at full load. The striking feature of the so-called thermal anemometry is that it allows easy, accurate and direct measurement and ultimately simple evaluation of the detected data.
Selectively designed for demanding applicationsThe newly developed thermal flow sensors SS 20.250 from SCHMIDT Technology
present a minimum resistance in the air flow and are easy to mount, due to the little space required. The patented dumbbell technology can be positioned safely and quickly in the gas flow. In addition to that, the completely seamless design of the sensor head inhibits the adhesion of dirt particles, thus making it easy to clean. If required, the sensors can be delivered with a protective coating that makes them resistant to aggressive media and to reagents present in disinfectants.
The sensors are an adequate solution for applications such as the continuous monitoring of filter units, the control of volumetric flow in extractors or the monitoring of laminar flows in cleanrooms.
SCHMIDT Technology GmbHFeldbergstr. 1D-78112 St. GeorgenPhone +49 (0) 7724/899-0Fax +49 (0) 7724/899-101E-mail: [email protected] Internet: www.schmidttechnology.de
Direct measurement of air or gas volumes PErFEct Flow mEasurEmEnt For clEanrooms and sImIlar dEmandIng ProcEssEs

20 www.pharma-mag.com July/August 2011
GENERICS & BIOSIMILARS
During the next few years, the fundamental patents protecting many of the best-selling biological medicinal products — such as the blockbuster monoclonal antibodies (mAbs),
Herceptin, Avastin, Enbrel and Humira — are due to expire, potentially opening the market to copy products. The revisions to European medicine regulation introduced in 2005 make obtaining approval for the marketing of such copies more feasible than it would have been previously, and considerably more so than under the regulatory regime applied in the US. The scene is therefore set for a wave of litigation, as biosimilar companies attempt to clear a way through the palisades of secondary patents (formulations, dosage regimes and the like) erected to protect these key products.
Gaining approval for marketing a biosimilar will never be straightforward. Where traditional small molecule drugs are concerned, an active ingredient can be replicated exactly by well-known synthesis techniques. Consequently, once the regulator is satisfied that the first version of the drug works and is safe, all that remains to be verified is that the generic versions are the same and manufactured to a suitable quality. It would be unnecessary and, therefore, unethical to repeat trials on animals and human patients.
The same does not necessarily apply where the product is an artificially produced version of a natural protein — a hormone, enzyme or antibody. The biochemical activity of these much larger molecules results not only from the chemical formula that describes their component atoms, but also from the three-dimensional shape the molecule twists into once it has been made. Furthermore, they can only be synthesized in a living cell — a process far more variable than any small molecule synthesis. The choice of host cell type, the growth conditions, the extraction mechanism can all lead to variations in the final product, which may be impossible to measure precisely. Incompletely synthesized molecules may end up in the final extract along with traces of the culture medium and random proteins leached from the host cells. Because the precise mechanisms by which these molecules act in the body are almost never fully understood, any change in the way the product is made could significantly change the way the molecule behaves pharmaceutically, including the additional risk that the variation may provoke an immune reaction from the body.
In the EU, the European Medicines Agency was first established with a remit to take over the regulation of any biotechnology derived product. It has taken the lead internationally in promulgating standards for the approval of a biosimilar based in part upon the originator’s clinical data. There are general guidelines regarding quality, and nonclinical and clinical issues, and detailed annexes relating to particular molecules including, insulin, EPO, G-CSF and the human growth hormone somatropin. A draft on mAbs was circulated for comment late in 2010 and should be finalized shortly. Applicants, therefore, have a relatively clear path to follow to obtain marketing authorization for a biosimilar.
Given the high value of these therapies, collectively generating billions of euro in sales for their manufacturers, it is unsurprising that a number of companies are lining up to launch biosimilars at the earliest possible opportunity. Secondary patents around Herceptin, for example, are already being opposed at the European Patent Office (EPO) by at least seven would-be competitors, and more are preparing to join the fray. But whatever cracks may be made in the defences through the EPO route, the originators will certainly have patents to assert when the first biosimilars are launched during the next few years. With no centralized patents court, now delayed further by the Court of Justice’s rejection in December 2010 of its proposed jurisdiction, numerous cases will have to be fought out in the national courts of the EU countries with, no doubt, the usual variation of outcomes that has plagued European patent litigation for decades.
By contrast, until last year the US legislation has treated most biological products apart from hormones completely separately from small molecule pharmaceuticals, so that there was a real issue as to whom within FDA was most appropriate to handle applications for approval. The new legislation — the Patient Protection and Affordable Care Act of 2010 — resolves that question, but in its place sets up a complex and burdensome system for managing patent litigation for biosimilars, which may deter manufacturers from using the procedure at all. The alternative, of simply applying for authorization as if the biosimilar product were a completely new drug and then dealing with patent issues on a level playing field, may in practice be more acceptable. But biosimilar launches, and litigation, may well be delayed compared with the EU, as companies work their way through the full set of clinical trials and regulatory issues for each one.
ThE BIOSIMILAR ‘BATTLEGROUND’ Of EUROPE
For more informationLorna Brazell
Partner
Bird & Bird
Tel. +44 207 415 6000www.twobirds.com
Lorna Brazell

July/August 2011 www.pharma-mag.com 21
22 www.pharma-mag.com July/August 2011
CLINICAL TRIALS
W hen it comes to addressing complex diseases such as cancer, we find ourselves in a time of great opportunity, where rapid advances in whole genome
analysis will soon translate into knowing all the ‘ground zero’ genetic events that drive cancer, and by extension, provide an extensive array of rational drug targets for future interrogation. Novel therapies that target the root causes of cancer (such as B-Raf, Bcr-Abl, EGFR and HER2), when given to the ‘right’ patients harboring those defects, clearly demonstrate substantial benefits compared with older chemo and radiation treatments — so much so, that biotech and pharma companies are now fully bought into this concept, even if it means smaller patient populations. There are, however, still many bumps and even road-blocks that challenge this paradigm of ‘stratified’ or ‘personalized’ medicine moving forward.
The following paragraphs will briefly highlight these issues and suggest where new tools, practices or even incentives can be applied to help accelerate an affordable and diverse toolbox of new ‘targeted’ therapies. The ethical driver being, that when tailored to the right patients using companion diagnostics and combined with early detection methods to catch tumours before they metastasize and become almost impossibly genetically complex, effective long-term management of cancer could be within our grasp.
key Bottlenecks and New TechnologiesThe first issue that needs to be solved is to ‘de‑orphan’ and validate the next generation of conventional drug targets. Unless biologic-based drugs — such as antibodies or RNAi — can be consistently designed to access intracellular targets (where most existing and new cancer genes reside), we will continue to develop small molecule synthetic chemicals as drugs.
In this sphere, most candidate cancer genes (of which there are hundreds now) are still challenging for small molecule drug discovery. Gain‑of‑function ‘oncogenes’ are rarely simple ‘drugable’ enzymes with large active sites (such as kinases) and loss‑of‑function ‘tumour suppressors’ are almost impossible to compensate for with a small molecule. To make matters worse, most new cancer genes are rare in isolation and little information exists on how they might stack up into pathways (Figure 1).
Much basic research is therefore required to define how ‘orphan’ cancer genes interact with one another (so they collectively become more economically attractive) and find new targets downstream of undrugable cancer genes. Functional ‘synthetic lethality’ screens using RNAi libraries is an increasingly common way to de-orphan undrugable cancer genes and uncover unexpected nodes of selective toxicity to tumour cells harboring specific genetic backgrounds.
Such pursuits and the faster definition of on‑target compounds in early drug discovery phases would be
MODERNIZING CANCER DRUG DISCOVERYModern cancer therapy is moving towards developing an expanding class of novel ‘targeted’ agents that will need to be precisely tailored to match the underlying genetics of each and every patient. To make the diversity of agents required to achieve such ‘personalized’ therapies — and to do so with favourable economics — many new technologies and practices will be required to speed up the process of drug discovery.
ThE MOST IMPORTANT PROCEDUraL ChANGE ThAT NEEDS TO OCCUR IS REVISING ThE CLINICAL TRIALS PROCESS.

July/August 2011 www.pharma-mag.com 23
CLINICAL TRIALS
greatly aided by having a consistent source of genetically defined, or ‘isogenic’ human disease models (where they differ only with respect to a presence or absence of a specific mutant or normal version of a gene) that accurately reflect and predict the responses of specific target patient populations in the laboratory. This goal would require the ability to precisely edit the genome of human cells, just as we have been able to do in mice for many years and is now achievable using a technique called GENESIS, which uses the power of recombinant Adeno-Associated Viruses (rAAV) to perform targeted homologous recombination in mammalian cells.
It is now routinely possible to delete or modify (at single nucleotide resolution) any endogenous genomic loci, in any mammalian cell line growing in tissue culture, which is set to transform the study of gene function, the modeling of patient genetics and the development of physiologically relevant pathway reporter screens (particularly as many new target classes emerge that can only be screened in a live cell format). One can even imagine using gene editing in combination with stem cells to directly correct certain genetic diseases. Yet, the most dramatic impact will likely be to predict responsive patients prior to entering clinical trials, and thus streamline the most expensive late stages of drug development. If drugs fail in these patients, one can either decide to cancel a programme early to focus on a more promising alternative, or move more quickly into combination therapy.
Indeed, there may be only be a minority of cancers that respond fully or in a sustained way to single agents, and so finding rational combinations will be the next big challenge for drug developers. Here, panels of in vitro models harboring defined pairs or matrices of mutational defects will allow the empirical testing of pre-existing gene combinations in patients that may be imparting ‘de novo’ resistance to targeted therapies; and provide tools to rationally screen for
resistance-reversing drug combinations once validated. Moreover, cDNA and/or RNAi libraries can be used with proven models of ‘sensitive’ patient populations to predict genes that impart ‘acquired’ drug resistance and define new targets for combination therapy downstream of undrugable resistance genes.
Equally important to developing new targeted therapies is a range of diagnostics that can detect cancers early, define their driving mutational events and ideally, assess tumour load and its response to therapy in a serial and minimally invasive way. This is a vigorous area of R&D and CRO establishment right now, currently focussed on ‘single‑shot’ mutation tests capable of profiling tumour biopsies, but with multiplexed tests and next-generation DNA-sequencers likely to supersede these relatively quickly. Expression signatures and drug-activity markers will also become more commonplace to confirm whether pathways are still active in tumours and to define optimal drug dosing regimens. Here, isogenic disease models will not only help identify such markers and signatures, but also provide ideal reference materials for performance testing diagnostic platforms and services being provided to, or within, healthcare systems.
Assaying mutations in rare circulating tumour cells or DNA in blood using, for example, ‘BEAMing,’ is another rapidly advancing and important area. ‘Personalized’ tumour‑load markers have recently been discovered in the form of unique translocation events present in most patients’ cancers and these can be sensitively detected using ‘paired‑end’ PCR tests. Further behind, however, is the development of imaging techniques that can diagnose and localize tumours early, which will be essential to maximize therapy options using surgery and future adjunct targeted therapy. Here, finding new imaging compatible, tumour selective, biomarkers are greatly needed, which may come in the form of defining and detecting key metabolic switches in cancers harboring specific genetic alterations.
Figure 1: Representation of
mutational frequencies of
known cancer genes in colon
and breast tumours, showing
a) that the majority are low in
their incidence and b) even
the common genes are not
always able to be ‘drugged’ (for
example, K-Ras, APC and p53).
Figure 1

24 www.pharma-mag.com July/August 2011
CLINICAL TRIALS
With the above advances, one can perhaps imagine a time when GPs/clinicians become the ultimate arbiters of truly personalized cancer medicine; that is, in relative real-time, a bespoke combination and/or sequence of therapies are tailored directly to each patient. The technology required to achieve this may arrive sooner than the regulatory framework to deal with it, where currently every combination must still be tested in a dedicated, population-based, clinical trial. Although this tide may turn, it does further highlight the need to maximize the chances of seeing single-agent benefit in clinical trials.
Here we come to the most important procedural change that needs to occur: revising the clinical trials process. Although stratified trials are becoming more common, they are not mandatory. Moreover, novel targeted agents with marked efficacy in Phase I, still need to go through much larger Phase-II and III trials to be approved (which were historically there to assess the marginal efficacy and overt toxicity of older chemotherapies). If efficacy can be seen without the need for statistics in small Phase-I trials, particularly for agents that directly target mutant oncogenes and if they had clear therapeutic windows in prior disease models (for example, B-Raf inhibitors in B-Raf mutant melanomas), perhaps any secondary testing is now only required to ascertain specific side-effects. In the meantime, conditional approval could be granted, which would be far more ethical to patients who are currently left waiting for such new and promising therapies. Mandatory biomarker
driven trials would also help healthcare and insurance agencies to ultimately prescribe an increasing array of expensive new treatments once approved.
IncentivesGiven the issues highlighted above, what realistic ideas and incentives can we now apply to help progress targeted therapies as fast as possible into the clinic, plus bring healthcare stakeholders more cohesively together to ultimately deliver personalized medicine? A five‑point plan is presented below for open discussion and comment by scientists, biotech/pharma executives, regulators, funding agencies, healthcare professionals and politicians alike:• Foster early‑stage translational projects in academia
— the primary site for risky research — by removing the publication shackles. Collaborative grants such as the EU FP7‑framework; for example, ‘COLTHERES,’ ‘Predict’ and ‘4D‑cell fate’ in the cancer and stem cells fields, are a good example of bringing together multidisciplinary teams and translate new data directly into applications. ‘Big science’ calls should also now consider adding a ‘human functional genome’ project to decipher all the new genetic variations being found in humans.
• Support innovative start‑ups, but not by trying to pick winners. Tax breaks on the first 25 employees and government-matched research or business grants could be a way to reward early success, plus get small companies to the stage where they can negotiate private institutional funding on more equal terms.
• Provide pharma with incentives to progress riskier targets by extending the patent lifetime on any ‘first‑in‑class’ drug. This proposal is not only simple and ethically progressive, but exploits market forces and comes at no cost to society.
• Set up a panel of independent scientists and oncologists to modernize drug trials and approvals. Areas to debate are mandatory focused (genotype selected patients), biomarker-driven (for drug action) clinical trials, with rapid pre-approval of drug candidates with positive outcome data in such trials. This panel could also make recommendations to politicians, particularly in the UK with its opportunity via the NHS, on how to roll out personalized medicine.
• Accelerate biotech and pharma working in a more open‑innovation way to find rational drug combination therapies. A panel of independent scientists and clinicians could also have the power to initiate publicly funded combination trials using drugs from two different companies, to precipitate these interactions and best progress effective next-generation treatments into patients. This will also help maximize the sector’s resources and reduce their historical redundancy in developing new targeted agents to combine in the future.
For more informationDr Chris Torrance
CEO
Horizon Discovery
Tel. +44 1223 655 580Fax +44 1223 862 240
Dr Chris Torrance

July/August 2011 www.pharma-mag.com 25
Tyvek® labo
Trust the new Tyvek® Labo coverall from DuPont!
www.dpp-europe.com
OutsideProtecting
the processes
InsideProtecting the people
12/2010 - TM and ® are registered trademarks or trademarks of E.I. du Pont de Nemours and Company or its affiliates. © Copyright, 2010 E.I. du Pont de Nemours and Company. All rights reserved.
Especially designed for laboratories and the pharmaceutical industry.
Suitable for classes ISO-7/ISO-8/ISO-9 (C/D)
Chemical Protective Coverall, Category III
• Double protection: Protecting people Protecting the products
& processes
Tyvek® is made of continuous strong high density polyethylene fibres that do not break off.
• New innovative ‘feel good effect’ fit

26 www.pharma-mag.com July/August 2011
CLINICAL TRIALS
there is increasing concern regarding suicidal ideation and behaviours in patients taking medication as part of clinical trials. Significant evidence has indicated that medicines that were
previously thought to have minimal effects on the central nervous system, actually pose a risk of increased suicidal ideation or behaviour, including compounds for dermatology, pain, multiple sclerosis and respiratory indications. As a result, FDA recently released a guidance document on Suicidality Monitoring, which highlights the importance of proactively monitoring and identifying patients who exhibit these symptoms.1 The guidance identifies the Columbia‑Suicide Severity Rating Scale (C-SSRS), a semistructured clinician administered interview, as an acceptable prospective assessment instrument. Procedural variability in the way clinical staff administer clinical assessments are administered, however, has been a shortcoming and can negatively affect the reliability of the scale results. Electronic patient reported outcomes (ePRO) solutions effectively address this limitation. This approach was used to develop a fully structured, electronic self-report C-SSRS
script — the eC-SSRS. Using interactive voice response technology the eC-SSRS has demonstrated clinical validity and reliability in more than 30,000 suicidality monitoring applications. Designed in collaboration with scale authors and in anticipation of the FDA guidance, the eC-SSRS is a fully structured C-SSRS interview comprising standardized questions, appropriate branching to follow-up questions and error-handling routines. Similar to the C-SSRS, it assesses lifetime suicidality during an initial baseline evaluation and then monitors ideations and behaviours at subsequent study visits. The industry can benefit from using this new approach: first, the C‑SSRS algorithm ensures that all questions are asked in a consistent manner, reducing clinical variability; second, suicidality risks are identified with timely feedback to study sites for prompt follow-up; and third, the investigator site burden is reduced whilst costing no more for the total cost of clinician support, data collection, reconciliation and reporting. Co-ordinating the eC-SSRS self-rated interviews and standardized reports of the patient’s responses with the investigator’s judgement can facilitate accurate, efficient and thorough assessment of suicidal risk.
USING ePRO SOLUTIONS TO COMPLY wITh ThE fDA GUIDANCE ON PROSPECTIVE ASSESSMENT Of SUICIDALITY
Reference1. www.fda.gov/downloads/
Drugs/GuidanceCompliance
RegulatoryInformation/
Guidances/UCM225130.pdf
For more informationMichael Federico
Vice President
ePRO Solutions
ERT
[email protected]/suicidality-monitoring-ec-ssrs
Patient retention and compliance are critical to the success of clinical studies. Depending on the therapeutic area, patient discontinuation rates can be as high as 40%, impacting significantly
on the timeline of studies, as well as decreasing data quality; common practice is for sponsors to manage the risk of anticipated high discontinuation rates by setting high enrolment targets, hence introducing further costs. Motivating patients through timely engagement and simple communication channels can considerably increase the rate of patient retention, and the use of accessible every-day technology such as mobile phones, offers a familiar mechanism for that communication.Mobile communication solutions can be used to send automated, scheduled, action-driven messages directly to the participant. Such communication strategies provide immediate access to patients, ensure enhanced engagement and can be used to guide them through (often complicated) clinical trial processes. These discrete and personalized messages improve both site-patient relationship management and compliance in line with
the study requirements. Messages can include reminders such as visit schedule, dosage and dosing frequency, advice on taking the medication safely, correct storage, or words of motivation or appreciation (for example, congratulations on reaching a milestone, ‘Thank You’ for participating).
Mobile technology can also be leveraged to facilitate electronic patient reported outcomes (ePRO) data capture. Mobile phone ePRO solutions offer the pharmaceutical/healthcare industries a real-time, user-friendly modality, which can be customized to suit the specific trial requirements. This ubiquitous mobile platform provides patients with a tool that integrates unobtrusively into their lives, regardless of location, and ensures high quality (that is, timely, complete and accurate) data. For clinical trials requiring extremely complex or extensive patient data collection, downloadable cell phone applications containing eDiaries can be deployed. This modern approach has proven to be an effective patient communication channel, rewarding sponsors with higher levels of compliance and retention.
IMPROVING PATIENT RETENTION USING MOBILE TECHNOLOGy
For more informationJudith Teall
Director of Patient
Recruitment
Exco InTouch
Tel. +44 1279 709 040 +1 877 327 5777www.excointouch.com

July/August 2011 www.pharma-mag.com 27
C
M
Y
CM
MY
CY
CMY
K
Pharma.pdf 1 17/06/2011 11:04:17

28 www.pharma-mag.com July/August 2011
CLINICAL TRIALS
NEw fDA INfORMED CONSENT REGULATIONS EffECTIVE MARCh 2011
F DA has amended its regulations to require the inclusion in informed consent forms for certain clinical trials a statement that information about the trial will be posted on www.clinicaltrials.gov, the
US National Institutes of Health/National Library of Medicine (NIH/NLM) registry. The new requirement applies to clinical trials that meet the definition of “applicable clinical trial” under the FDA Amendments Act of 2007 (FDAAA).
Since 2007, the FDAAA has required all Phase II–IV clinical trials involving drugs, devices or biological products subject to regulation by FDA (applicable clinical trials) to be registered on www.clinicaltrials.gov. The statute establishes deadlines for registration and specifies the information that must be included in the registry.
The FDAAA additionally requires FDA to update its informed consent regulations to require inclusion in the informed consent documents and processes for applicable clinical trials a statement that information about the trial will be posted on www.clinicaltrials.gov. In accordance with this legislative mandate, on 4 January 2011 FDA issued a final rule amending its informed consent regulations at 21 CFR Part 50 (76 Fed. Reg. 256). The final rule is effective 7 March 2011, but applies only to informed consent documents for applicable clinical trials initiated on or after 7 March 2012. Such informed consent documents must include the following statement: “A description of this clinical trial will be available on http://www.ClinicalTrials.gov, as required by U.S. Law. This Web site will not include information that can identify you. At most, the Web site will include a summary of the results. You can search the Web site at any time.”1
Sponsors, institutional review boards (IRBs) and investigators must use this exact language and do not have flexibility to craft their own language or modify the required statement in any way (although they may include additional information about www.clinicaltrials.gov, if desired). The final rule does not dictate where in the informed consent document the statement must appear. The statement must, however, be included ‘in’ the informed consent form and may not be set forth in a separate document or in an attachment.
As noted above, the final rule applies to applicable clinical trials initiated on or after 7 March 2012. For purposes of this requirement only, a clinical trial has been “initiated” if any informed consent documents have been cleared or approved by an IRB, a regulatory body or other human subjects review entity. The final rule provides the following additional guidance:• An applicable clinical trial initiated prior to 7 March
2012 is not subject to the new requirement, even if the informed consent document for the trial is amended for other reasons ‘after’ 7 March 2012.
• Reconsenting of subjects based solely on the new requirement is not required for clinical trials initiated before 7 March 2012.
• In the case of a multisite clinical trial, if the informed consent documents have been approved for one or more sites, but not for all sites, before 7 March 2012, the trial will be considered to have initiated before 7 March 2012; the new requirement accordingly will not apply, and the informed consent documents for the remaining sites do not have to include the required statement.
• There is no exemption for clinical trials conducted outside of the US. Informed consent documents for ‘all’ applicable clinical trials initiated on or after 7 March 2012 — whether conducted within or outside of the US — must contain the required statement.
• The wording of the FDAAA led some to believe that the updated regulations would only apply to applicable clinical trials involving drugs. The final rule puts this question to rest and clarifies that the statement is required in informed consent documents for applicable clinical trials involving drugs, biological products or medical devices, or a combination thereof.
Sponsors of clinical trials, and institutions and investigators, as applicable, should take time now before the 7 March 2012 compliance date to review and refine procedures for determining whether a clinical trial is an “applicable clinical trial” within the meaning of the FDAAA, and update model forms and related documents to include the required statement for applicable clinical trials.
Reference1. 21 CFR § 51.25(c).
For more informationAlyssa Cunningham
Associate
Wiggin and Dana LLP
Tel. +1 860 297 [email protected]
Alyssa Cunningham

July/August 2011 www.pharma-mag.com 29
CLINICAL TRIALS
210x140_Pharma_C5.indd 1 15.06.11 15:16
A pproximately 60 million adult Americans currently have no bank account. As a result, the only method of payment available to such subjects participating in clinical trials has been cheques, which not only require
time-consuming paperwork administration, but can also drive fees of 5–20% of the face value of each cheque when cashed. The lack of an accessible and cost-effective method of payment can significantly hamper subject retention and as a result affect the overall success of a clinical trial.
Recent innovations in electronic debit card systems have revolutionized subject payment and communications within clinical trials by automating site-level and sponsor-level processes associated with paying and communicating with subjects. Fully compliant with the Institutional Review Board or Ethics committee approved guidelines, the new electronic systems function as Web-based payment and communication platforms, which eliminate the need for paper cheques and provide significant administrative time savings.
The systems can be configured to automatically pay participants based on a study‑specific schedule, make
one time ad-hoc payments, or add funds remotely to instantly cover travel-related costs for a subject who would not otherwise make an appointment. Consequently, the systems provide rapid access to funds for subjects, ensuring immediate gratification and reinforcing positive study behavior and increased overall subject retention. The electronic nature of the systems, removes cheque-handling fees and patients’ funds are secured against loss or theft. Electronic debit card systems can also easily integrate with any clinical trial management software platform to automatically trigger payments and further reduce administrative burden at the site.
The downstream benefits and savings of these systems provide sponsors and sites with an increased return on investment, both by decreasing site level operating costs and increasing subject retention. The new systems have already been adopted by leading pharmaceutical, biotechnology and medical device companies in Europe and North America in addition to numerous universities and research hospitals, including an Ivy League institution.
TRANSfORMING SUBJECT PAYMENT IN CLINICAL TRIALS wITh ELECTRONIC PREPAID DEBIT CARD SYSTEMS
For more informationSamuel Whitaker
CEO
Greenphire
Tel. +1 215 609 [email protected]
Samuel Whitaker

www.roquettepharma.com
efficient
Are allsuperdisintegrants
versatilein all your formulations?
equallyReliable superdisintegrant efficiencycomes with Roquette’s long-standing experience in the field. GLYCOLYS® has been developed and produced exclusively byROQUETTE for more than 20 years.
Offering GLYCOLYS®, GLYCOLYS® LVand GLYCOLYS® Low pH, it is a complete range of sodium starch glycolate products designed for yourspecific formulation needs.
We deliver!
GLYCOLYS®
and
- Cré
dits
phot
os :
Digi
tal V
ision
, Im
agew
erks
.
11296_AP_Glycolis_GB_REVUE: PHARMA UK_FRT: 210x280mm x211296_AP_Glycolis_GB 12/07/11 10:53 Page 1

www.roquettepharma.com
efficient
Are allsuperdisintegrants
versatilein all your formulations?
equallyReliable superdisintegrant efficiencycomes with Roquette’s long-standing experience in the field. GLYCOLYS® has been developed and produced exclusively byROQUETTE for more than 20 years.
Offering GLYCOLYS®, GLYCOLYS® LVand GLYCOLYS® Low pH, it is a complete range of sodium starch glycolate products designed for yourspecific formulation needs.
We deliver!
GLYCOLYS®
and
- Cré
dits
phot
os :
Digi
tal V
ision
, Im
agew
erks
.
11296_AP_Glycolis_GB_REVUE: PHARMA UK_FRT: 210x280mm x211296_AP_Glycolis_GB 12/07/11 10:53 Page 1

32 www.pharma-mag.com July/August 2011
CPhI WORLDWIDE PREVIEW
MORE TALKING, LESS wALKINGAnnemieke Timmers, Brand Director CPhI, UBM Live talks to Pharma about the various initiatives they’ve implemented to promote effective networking and easy navigation at this year’s CPhI worldwide event in Frankfurt, 25–27 October.Every year, exhibitors and visitors can expect something new at CPhI. This year, CPhI has two new zones — Generic APIs and Finished Dosage. Why have these two zones been added and why now?We instituted the zones at last year’s events in Paris as a result of exhibitor and visitor feedback to facilitate navigation of the event. The response to these initial zones was overwhelmingly positive and as a result of their success, and our post-show research, we have introduced the Generic APIs and Finished Dosage zones, to further facilitate the ‘more talking, less walking’ ethos. Our decision to launch these new zones has been vindicated by the response, with early registration patterns indicating that the Finished Dosage Zone is the second most popular area of interest to our visitors after the API Zone.
How has the global economic climate affected the number of exhibitors and/or their stand designs this year?Last year’s events in Paris saw an overall attendance in excess of 28,500 — an increase of more than 14% compared with the 2009 show. Exhibitor numbers
also grew during the previous year, from 1808 to 1934, with a total of 109 new exhibitors. This record attendance and the positive expressions from exhibitors and visitors were strong indicators of the market’s recovery and we see this continuing to enhance our 2011 events. Exhibitor numbers are up again for the events in Frankfurt, with a 7% increase in space taken compared with last year’s final square footage, with 3 months to go until the events open their doors

July/August 2011 www.pharma-mag.com 33
CPhI WORLDWIDE PREVIEW
What are you looking forward to most at this year’s CPhI Worldwide event?We are particularly excited to be holding the first ever CPhI Pre-connect event, our new virtual event, which is scheduled for 8 September. CPhI Pre-connect will create a whole new range of pre-show networking opportunities. It will be promoted to the entire CPhI Worldwide database of pharma professionals, making it a fantastic opportunity for our exhibitors to engage visitors, highlight their business and start generating leads prior to the actual face-to-face meetings in Frankfurt. Details are currently being finalized, but the event will feature a content-rich seminar area, networking lounges featuring cutting-edge pharma industry topics, private chats, and a social media suite.
What can you tell us about CPhI visitors?Primarily, visitors (many of whom are CEOs and department managers) attend CPhI Worldwide to make new business contacts and to meet face-to-face with their existing contacts, under one roof, during the course of just 3 days. By colocating CPhI Worldwide alongside complementary events such as P-MEC for equipment, machinery and technology; ICSE for contract services, clinical trials and packaging; and the new InnoPack event, focused on innovative packaging concepts in the pharmaceutical packaging market, we
offer a global meeting point covering every aspect of the pharma industry.
More than 28,500 attendees from 140 countries attended the 2010 events. Our post-event visitor surveys indicated that in excess of 83% found the products or services that they were looking for, and more than 90% of attendees said they made new business contacts. One feature that we have typically observed when we have previously staged the events in Frankfurt is that despite the fact that Germany is one of Europe’s pharma powerhouses, we continue to attract a high proportion of international visitors, with approxiamtely 90% nondomestic attendees.
What trends have you seen since last year’s event in Paris?We are currently well up on pre-registrations across the board compared with this time last year and are optimistic of beating the attendance record that was set at the Paris events. As mentioned above, the CPhI Pre-connect virtual event (www.cphi.com/pre-connect) has been introduced this year as our exhibitors and visitors identified a desire to create a networking opportunity in advance of the physical event. We see virtual events as having an increasingly important role for our customers in the future, as inevitably, some are unable to attend the physical events and even those who do can’t visit every stand.
For more informationAnnemieke Timmers
Brand Director CPhI
UBM Live
www.cphi.com
CPhI Zones• APIs
• Generic APIs
• Custom Manufacturing
• Fine Chemicals
• Intermediates
• Finished Dosage
• Excipients/Formulation
• General
Speakers’ Corner Companies• DSM
• Bachem AG
• Technology Catalysts
• Chemetall GmbH
• Lambiotte & Cie S.A./N.V.
• Novozymes
• Heraeus Precious Metals
• Registrar Corporation
• Thomson Reuters
• Elan Drug Technologies
• Horphag AG
• Siegfried
• Grace Davison
Discovery Sciences
• LGC Standards GmbH
• Evocatal GmbH
• American Peptide
Company Inc.
• Avantor Performance
Materials B.V. formerly
Mallinckrodt Baker
• Winclove Bio Industrie
• Thermo Fisher Scientific
Annemieke Timmers

34 www.pharma-mag.com July/August 2011
FREEZE DRYING
t he importance of nucleation temperature in freeze drying has been known for some time. A number of earlier techniques to control nucleation, whilst demonstrating the
potential for process improvement, were not easily transferrable to development or production freeze dryers, from a commercial standpoint. These include the “Ice Fog” technique and ultrasound.1,2 A novel technology for controlling nucleation, ControLyo Nucleation On-Demand Technology, has been shown to significantly improve both product and process in many experimental systems.3 ControLyo technology is now commercially available on the new FTS/SP Scientific, Lyostar 3 development freeze dryer. This technology has been fully integrated and can be easily practised even by relatively inexperienced users. In addition, existing commercial freeze dryers can be modified or upgraded to accommodate the technology if they have ASME-rated pressure chambers (for example, SIP systems) and sufficiently sized orifices for depressurization. This paper reviews ice nucleation, describes the ControLyo technology and shows data for controlled nucleation on the Lyostar 3. In addition, application of the technology in a number of freeze drying environments is presented.
Review of Nucleation“Control and characterization of the degree of super-cooling can provide a solution to what is perhaps the biggest freeze drying scale-up problem.”4
This quote from a paper by Pikal et al. sets the stage for the discussion below. A primary goal of cycle development and scale-up is to establish optimum cycle parameters whilst maintaining product quality. A well-optimized process can reduce the cycle time (and
therefore cost) in freeze drying. In our experience, focusing on reducing the time of primary drying achieves this, as this is usually the longest part of the cycle. Optimization of the freezing step is rarely a focus. To a large extent, however, the temperature at which freezing occurs, and the degree of super-cooling that occurs determine how much optimization can be done to reduce the length of primary drying. The freezing step has been largely ignored partly because development scientists have not had access to tools and technology to affect this step (the technology was not available until the advent of the Praxair ControLyo technology). Other than annealing, the freezing step has been an unexploited opportunity to improve the freeze drying process.5
To better understand the benefits of ControLyo technology in the context of optimizing the freezing step, it is helpful to understand the basics of nucleation and super-cooling. These physical behaviours are summarized below:• Nucleation temperature is the temperature at which
freezing or ice crystal formation begins to happen.• Nucleation rarely occurs at the equilibrium or
thermodynamic freezing point of the solution. In a lab or development freeze dryer, it is common for nucleation to occur 10–20 °C below the
ThE IMPORTANCE Of CONTROLLING ICE NUCLEATION TEMPERATUREThe recent capability to reliably control nucleation during the freezing step in freeze drying has allowed researchers to demonstrate numerous process and product improvements. The SP Scientific FTS Lyostar 3 is the first commercially available freeze dryer that incorporates this ControLyo Nucleation On-Demand Technology.
Figure 1: Typical freezing curve. Figure 1
A PRIMARy GOAL OF CyCLE DEVELOPMENT AND SCALE‑UP IS TO ESTABLISh OPTIMUM CyCLE PAraMETERS whILST MAINTAINING PRODUCT qUALITy.

GE HealthcareLife Science
imagination at work
Confidence comes with the right interactions.Join leading scientists from academia and industry at Developments in Protein Interaction Analysis (DiPIA), November 12-15, Boston, Massachusetts, USA.
This scientific conference offers opportunities to meet and discuss the latest developments in label-free interaction and stability analysis using Biacore™ Surface Plasmon Resonance (SPR) and MicroCal™ microcalorimetry systems.
Register at www.gelifesciences.com/dipia
© 2011 General Electric Company – All rights reserved.GE Healthcare Bio-Sciences AB, Björkgatan 30,751 84 Uppsala, SwedenK11074. First published May 2011.
k11074 - DIPIA Ad v3.indd 1 5/10/2011 10:29:14 AM

36 www.pharma-mag.com July/August 2011
FREEZE DRYING
thermodynamic freezing point. In a commercial freeze dryer (Class 100 Clean Environment), nucleation tends to occur 20–30 °C below the thermodynamic freezing point, and may even exceed that level. In this clean environment, there are fewer particulates that can serve as nucleation points during the freezing step.
• The degree of super‑cooling can have a dramatic impact on the drying behaviour.
• High degree of super‑cooling = smaller ice crystals = smaller pores during sublimation. This increases resistance to mass transfer and increases primary drying times.
• Low degree of super‑cooling = larger ice crystals = larger pores during drying. This reduces resistance to mass transfer and decreases primary drying times.
Previous studies have demonstrated that for every 1 °C increase in the nucleation temperature, primary drying time can be reduced by as much as 3–4%.6
Figure 1 shows the temperature of a vial filled with water during freezing. As the vial is cooled, it passes through the thermodynamic freezing point (Tf), which for water is 0 °C, and below which nucleation occurs. Nucleation is an exothermic event, and this is observed in by the rapid temperature spike that approaches the thermodynamic freezing point. The nucleated contents of the vial then cool, following a temperature history dictated by the cooling ramp of the shelf. The point at which nucleation begins is called the temperature of the onset of nucleation (Tn). The difference between Tf and Tn is the degree of super-cooling of the sample.
Uncontrolled Nucleation ResultsFigure 2 shows the results of uncontrolled nucleation during the freezing step in a cycle run on a LyoStar 3 (Figure 3). This is typical behaviour in a lab freeze dryer. A tray was loaded with 10‑mL vials of 3% sucrose with a fill volume of 2.0 mL. Self‑adhesive thermocouples were adhered to the outside of 16 vials, including edge and interior vials. The outside placement prevents unintended nucleation resulting from the thermocouple itself.
The graph shows the thermocouple data from eight vials. During a 0.5-°C/min ramp from –4 °C to –45 °C, the first nucleation event occurs at –12.9 °C. Random nucleation of other vials occurs during an approximately 15‑min period, with the final nucleation event occurring at –18.5 °C, approximately 18 °C below the thermodynamic freezing point of the sucrose solution. Using the data supplied by Searles, Carpenter & Randolph, the drying time of the last vial to nucleate could be almost 20% longer than the first vial, and 45% longer than a vial made to freeze close to its thermodynamic freezing point by controlled nucleation!6
Longer cycle times are not the only consequence of uncontrolled nucleation during freeze drying. Other adverse effects have been observed or are known industry concerns.
Controlled Nucleation Results Using ControLyo TechnologyThe ControLyo technology is simple and easy to use on the Lyostar 3. A typical controlled nucleation run is described below:• Load vials onto shelves precooled to 4 °C.• After loading, reduce the temperature to –4 °C (or
whatever your desired nucleation temperature is) using a 0.5-°C/min shelf ramp rate.
• After reaching –4 °C, pressurize the system with an inert gas (nitrogen or argon) to approximately 25 psig (1.7 bar).
• Equilibrate at –4 °C for as long as necessary to achieve vial-to-vial temperature homogeneity (for example, 30–45 min).
Figure 2: Graph of
uncontrolled nucleation.
Figure 3: LyoStar 3 with
ControLyo Nucleation
On-Demand Technology.
Figure 4: Graph of controlled
nucleation.
Table I: Benefits of ControLyo
Nucleation On-Demand
Technology.7
Figure 2
Figure 3
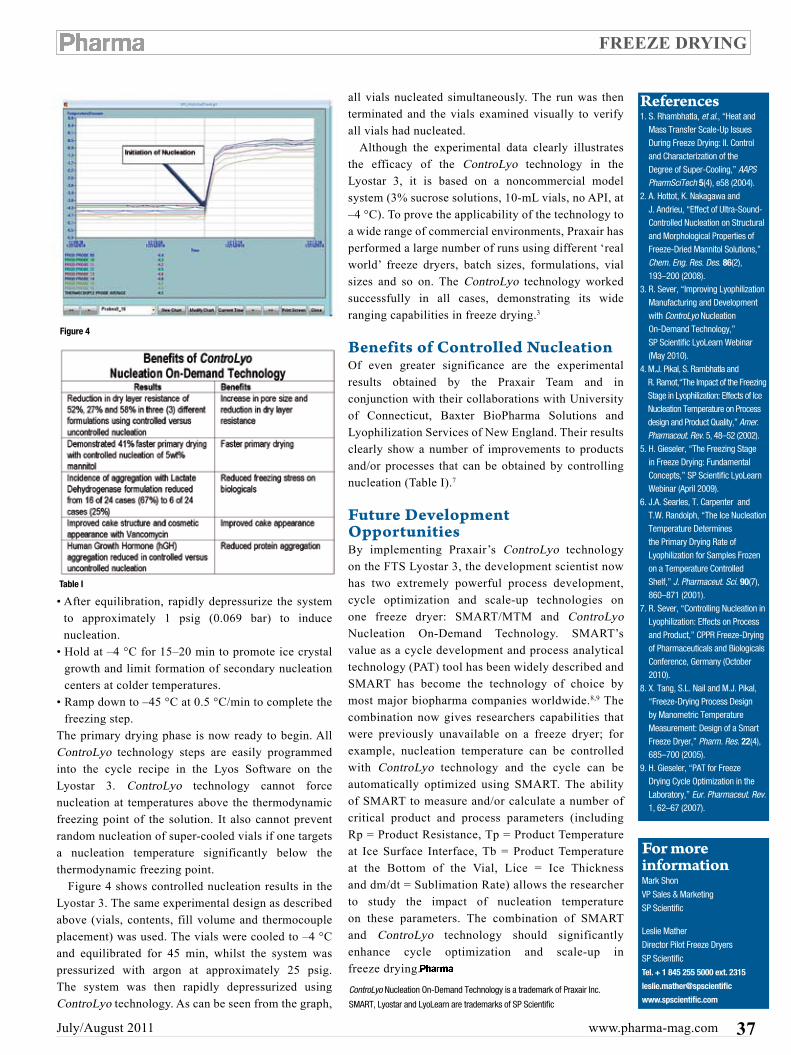
July/August 2011 www.pharma-mag.com 37
FREEZE DRYING
• After equilibration, rapidly depressurize the system to approximately 1 psig (0.069 bar) to induce nucleation.
• Hold at –4 °C for 15–20 min to promote ice crystal growth and limit formation of secondary nucleation centers at colder temperatures.
• Ramp down to –45 °C at 0.5 °C/min to complete the freezing step.
The primary drying phase is now ready to begin. All ControLyo technology steps are easily programmed into the cycle recipe in the Lyos Software on the Lyostar 3. ControLyo technology cannot force nucleation at temperatures above the thermodynamic freezing point of the solution. It also cannot prevent random nucleation of super-cooled vials if one targets a nucleation temperature significantly below the thermodynamic freezing point.
Figure 4 shows controlled nucleation results in the Lyostar 3. The same experimental design as described above (vials, contents, fill volume and thermocouple placement) was used. The vials were cooled to –4 °C and equilibrated for 45 min, whilst the system was pressurized with argon at approximately 25 psig. The system was then rapidly depressurized using ControLyo technology. As can be seen from the graph,
all vials nucleated simultaneously. The run was then terminated and the vials examined visually to verify all vials had nucleated.
Although the experimental data clearly illustrates the efficacy of the ControLyo technology in the Lyostar 3, it is based on a noncommercial model system (3% sucrose solutions, 10‑mL vials, no API, at –4 °C). To prove the applicability of the technology to a wide range of commercial environments, Praxair has performed a large number of runs using different ‘real world’ freeze dryers, batch sizes, formulations, vial sizes and so on. The ControLyo technology worked successfully in all cases, demonstrating its wide ranging capabilities in freeze drying.3
Benefits of Controlled NucleationOf even greater significance are the experimental results obtained by the Praxair Team and in conjunction with their collaborations with University of Connecticut, Baxter BioPharma Solutions and Lyophilization Services of New England. Their results clearly show a number of improvements to products and/or processes that can be obtained by controlling nucleation (Table I).7
Future Development OpportunitiesBy implementing Praxair’s ControLyo technology on the FTS Lyostar 3, the development scientist now has two extremely powerful process development, cycle optimization and scale-up technologies on one freeze dryer: SMART/MTM and ControLyo
Nucleation On-Demand Technology. SMART’s value as a cycle development and process analytical technology (PAT) tool has been widely described and SMART has become the technology of choice by most major biopharma companies worldwide.8,9 The combination now gives researchers capabilities that were previously unavailable on a freeze dryer; for example, nucleation temperature can be controlled with ControLyo technology and the cycle can be automatically optimized using SMART. The ability of SMART to measure and/or calculate a number of critical product and process parameters (including Rp = Product Resistance, Tp = Product Temperature at Ice Surface Interface, Tb = Product Temperature at the Bottom of the Vial, Lice = Ice Thickness and dm/dt = Sublimation Rate) allows the researcher to study the impact of nucleation temperature on these parameters. The combination of SMART and ControLyo technology should significantly enhance cycle optimization and scale-up in freeze drying.
References1. S. Rhambhatla, et al., “Heat and
Mass Transfer Scale-Up Issues During Freeze Drying: II. Control and Characterization of the Degree of Super-Cooling,” AAPS PharmSciTech 5(4), e58 (2004).
2. A. Hottot, K. Nakagawa and J. Andrieu, “Effect of Ultra-Sound-Controlled Nucleation on Structural and Morphological Properties of Freeze-Dried Mannitol Solutions,” Chem. Eng. Res. Des. 86(2), 193–200 (2008).
3. R. Sever, “Improving Lyophilization Manufacturing and Development with ControLyo Nucleation On-Demand Technology,” SP Scientific LyoLearn Webinar (May 2010).
4. M.J. Pikal, S. Rambhatla and R. Ramot,“The Impact of the Freezing Stage in Lyophilization: Effects of Ice Nucleation Temperature on Process design and Product Quality,” Amer. Pharmaceut. Rev. 5, 48–52 (2002).
5. H. Gieseler, “The Freezing Stage in Freeze Drying: Fundamental Concepts,” SP Scientific LyoLearn Webinar (April 2009).
6. J.A. Searles, T. Carpenter and T.W. Randolph, “The Ice Nucleation Temperature Determines the Primary Drying Rate of Lyophilization for Samples Frozen on a Temperature Controlled Shelf,” J. Pharmaceut. Sci. 90(7), 860–871 (2001).
7. R. Sever, “Controlling Nucleation in Lyophilization: Effects on Process and Product,” CPPR Freeze-Drying of Pharmaceuticals and Biologicals Conference, Germany (October 2010).
8. X. Tang, S.L. Nail and M.J. Pikal, “Freeze-Drying Process Design by Manometric Temperature Measurement: Design of a Smart Freeze Dryer,” Pharm. Res. 22(4), 685–700 (2005).
9. H. Gieseler, “PAT for Freeze Drying Cycle Optimization in the Laboratory,” Eur. Pharmaceut. Rev. 1, 62–67 (2007).
For more informationMark Shon
VP Sales & Marketing
SP Scientific
Leslie Mather
Director Pilot Freeze Dryers
SP Scientific
Tel. + 1 845 255 5000 ext. 2315
leslie.mather@spscientific
www.spscientific.comControLyo Nucleation On-Demand Technology is a trademark of Praxair Inc.
SMART, Lyostar and LyoLearn are trademarks of SP Scientific
Figure 4
Table I
38 www.pharma-mag.com July/August 2011
TECHNOLOGY
RISING TO ThE ChALLENGETechnology is helping pharma to tackle some of the big issues affecting the sector, including the increasing consolidation of pharmaceutical companies, the changing sales and marketing landscape, and the growing pressure on R&D projects. Furthermore, it will help pharmaceuticals and shape the industry’s future.
t he pharmaceutical industry came away relatively less harmed than the financial or manufacturing sector during the worst recession in modern time. The sector has, however, been experiencing
difficulties for a variety of other macro factors and is about to become more acute as the industry approaches a massive revenue cliff as a result of expiring patents.
The spending on IT and technology did slow down considerably in the last couple of years because of pressures on the cost structure and the fundamental business model changes affecting the industry. The pharmaceutical sector has been a late adopter of outsourcing, particularly regarding IT and software, which is a surprise considering the extent of outsourcing they already do in clinical trials and manufacturing. But companies are now realizing that more mature and accelerated technology outsourcing using the global delivery model and a managed shared services approach can help them to rise to the challenge of a changing industry. Technology is also driving some fundamental changes in their business models and defining key trends.
Current ChallengesMore Mergers and AcquisitionsInnovation has always been key to pharmaceutical success and for the first time this is happening beyond the biggest pharmaceutical vendors with more than 50% of new drugs and molecular entities being approved from smaller biotechs. This has led to an increase in merger and acquisition (M&A) activity as the larger pharmaceutical companies try to plug the innovation gap, bulk up their portfolios and enter new markets by using their financial muscle to buy smaller innovators. Yet, it has not just been larger companies buying smaller ones, the industry has also seen more large M&A deals, such as Pfizer–Wyeth, Roche–Genentech, and Merck–Schering Plough.
To be successful, however, M&As require technology to consummate them. Bringing two
companies together, regardless of their size, creates numerous challenges across all aspects of the business, including the integration of front-end and back-end systems, duplication of research and manufacturing sites and systems, overlap in sales and marketing teams and product portfolios. Technology is key to helping pharmaceutical companies align the various systems, rationalize the applications, create consolidated master databases and remove duplications. Shifting Sales and Marketing LandscapeAnother prevalent challenge facing the industry is how to adapt sales and marketing techniques to an evolving customer demographic. The increased use of social media is transforming how pharmaceutical companies conduct their marketing operations, patient adherence, key opinion leader management and sales analytics.
In the past, ‘in person’ detailing and sampling were the primary modes of interaction between the medical sales staff and the physicians. Increasingly more physicians, however, are now using the Web, other key opinion leaders and their own efforts to keep abreast of the changes and advancements in medicines, and bypassing the traditional sales and marketing channels.
At the same time, patients are becoming more empowered and behaving akin to demanding consumers. They do their own research via the Web, use their social networks to discuss their problems and find alternative solutions, and are unafraid to confront their doctors with suggestions or even demands for specific treatments or drugs.
Technology in the form of Web 2.0, social media sites, collaboration tools and digital content is playing a huge role in amplifying these changes. The dependence on a regular sales force is reducing, but the need for collaboration between the brand teams and the clinical development teams to get real-time feedback from the market, analyse the data and take corrective actions is increasing.

STRAP
July/August 2011 www.pharma-mag.com 39
For more information or to book your place and take advantage of our great group rates and early bird discounts:
CALL registration hotline: +44 (0)20 7202 7690
EMAIL: [email protected]
VISIT: www.wtg-training.com/pharma
Quoting booking ref: pharmamkt
• Scienceofscaleapproaches• Resourceconservation• Designspace• Riskmanagement
• Designforsixsigma• Leansixsigma• Scaleupandtechnologytransfer
Course highlights:
Stephen R. Wicks, PhD.FRPharmSProfessorinPharmaceuticalSciences,The School Science, University of Greenwich. FormerVicePresidentofPharmaceuticalScience&Technology,Pfizer Global Research and Development and Director of Pfizer UK
Jeff Duke,C.Chem,C.Sci,FRSCIndependentConsultantandManagingDirector,Grove Lodge Consulting. FormerHeadofMaterialsScienceandOralProductR&D;Head of Strategy and Coordination in the Asia Business Development Group
Course leaders:
Inassociationwith:
WTG Training in conjunction with The University of Greenwichispleasedtointroduceaseriesofcuttingedgeshortcoursesandadvancedworkshops:
Quality by Design:RegulatoryChemistryManufacturingandControlinthePharmaceuticalIndustryLondon,12th–14thSeptember2011&17th–19thOctober2011
The Late Stage Development and Commercialisation of Medicinal Products:ManagingRiskandQualityinthePharmaceuticalIndustryLondon,26th–28thSeptember2011&14th–16thNovember2011
Integrated Commercialisation of Medicinal Products:ManagingQuality,Speed,Scale&CostintheModernPharmaceuticalEnvironmentLondon,10th–12thOctober2011&5th–7thDecember2011
www.wtg-training.com/pharma

40 www.pharma-mag.com July/August 2011
TECHNOLOGY
Increased Pressure for Improved R&D OutcomesThe industry is suffering from a major innovation deficit, just when demand and alternatives are opening up the market. And though it might provide some breathing room, the innovation deficit is not going to be solved through heightened M&A activity. The era of blockbuster drugs is over and the industry will not see another multibillion drug coming out their labs in a hurry. The drug industry size is going to shrink as a result of the revenue cliff, but a few players will grow in size through M&As. The cost structure of the business is going to fundamentally change, as companies fight to maintain their bottom lines, whilst the top lines shrink (according to an estimate, more than $150 billion of annual drug sales will disappear down the revenue cliff in the next 2–3 years).1
To tackle this challenge, companies are renewing their focus on improving R&D productivity by investing in better collaboration and analytical tools. Research departments are using next generation sequencing technologies to fail fast and fail cheaper, in their quest to determine and then identify the right target drug candidate. They are using technology to increase their externalization efforts and collaborate with external partners when in-house research is not delivering results. In addition, pharmaceuticals companies are working to standardize analytical tools for better reuse of existing digital assets and information, whilst their sales and marketing are beginning to embrace the Web, particularly the Web 2.0 models of social networks and media, with regard to physician–patient interactions.
Looking to the FutureSoftware and IT are helping to tackle the pharmaceutical industry’s current problems; they are also helping to shape the future of the pharmaceutical economy. During the next 3–5 years, the industry is going to be driven by three big imperatives — affordability, prevention and patient-centricity — because healthcare costs are ballooning out of control in several developed countries: in the US, healthcare accounts for now in excess of 16% of the entire GDP. Even in several European countries, the figure is 10–12% and is going up.
Healthcare has become a crucial part of the world economic engine, driven by an ageing population and an increased prevalence of chronic diseases. Subsequently, pharmaceutical vendors are investing increasingly in technology; according to Gartner, the IT spending on healthcare is expected to reach approximately $44 billion by the end of 2011.2
There is increased awareness of health issues and shift in demand from treatment to prevention. Literate
and knowledgeable consumers are demanding better outcomes. Each of these areas offers the drug industry the opportunity — with the help of software and technology — to adapt and prosper. Specifically, mobility, interoperability, cloud computing and predictive analytics will see increased investment as pharmaceutical companies seek to exploit the changing industry.
MobilityThe use of mobile technologies will drive the adoption of remote health monitoring, telehealth, patient compliance apps, and physician and patient interactions. Companies are waking up to the potential for cost reduction, better customer service and differentiation, which is inherent in a well-thought-out and executed mobility strategy. Usage of telemedicine and remote health monitoring for areas such as diabetes, cardiac and sleep disorders will increase because of popularity and obvious cost advantages for various stakeholders. In addition, mobile devices such as iPads, Tablets, Smartphones, and Mobile Apps are streamlining the information flow and making the right information available to the right person at the right time.
The impact of mobility will be felt across the whole enterprise; for internal employees, in terms of the enterprise apps and info that needs to be consumed by the sales and product teams, and in interactions with customers such as physicians, prescribers and patients. Mobility in a broader sense is also gaining in importance, both within the enterprise, and with providers and patients.
ThE INDUSTRy IS SUFFERING FROM A MAjOR INNOVATION DEFICIT, jUST whEN DEMAND AND ALTERNATIVES ARE OPENING UP ThE MARkET.

July/August 2011 www.pharma-mag.com 41
TECHNOLOGY
InteroperabilityInteroperability of data across the various parts of the healthcare value chain is something of a holy grail in this industry. There is a huge amount of data that is being generated during research, trials, marketing and usage. There is an equally, if not more, amount of data on patients that is with providers, hospitals and payers. As the degree of digitization of health records increases, driven by the massive investment funding by governments, the ability to interconnect disparate data sets across the functional and organizational boundaries will fuel innovation and lower transaction costs.
In addition, there is need for more integrated data sharing across research, development, manufacturing and sales functions to improve trials, increase time-to-market for drugs, and utilize feedback faster. The data collection, analysis and reporting requirements will have to evolve to make comparative effectiveness research an integral part of business decisions and investments for pharmaceutical companies.
Cloud ComputingThe impact of cloud computing is just beginning to be felt in research, development and healthcare information exchange. The explosion of data as a result of next generation sequencing, growing importance of biologics in the research process and the importance of public–private partnerships (PPPs) to come up with new discoveries, is making cloud-based computing an increasingly important aspect of R&D.
We are already seeing complex genetic sequences and biomarker data being hosted on the cloud by a few open source bodies, which are then accessed securely by individual companies for their research needs. Pharmaceutical companies are exploring the use of both public and private clouds for data storage, hosting and access needs. Companies such as
Amazon, Google and Microsoft have already launched cloud-based healthcare information offerings (for example, Google Health and MS HealthVault) to leverage the power of the cloud in harnessing electronic patient health records and ultimately try to create a data continuum between pharma companies, patients, providers and payers. Software as a service (SaaS) -based offerings also depend on the cloud and are being offered in multiple ways.
Predictive AnalyticsAs the healthcare value chain becomes digitized and integrated, business intelligence, modelling and analysis of the data will get the maximum focus regarding technology and investments. The ability to analyse in real-time — and sometimes ahead of time — using predictive analytics, will allow more effective research, more successful trials and approvals, and better sales and marketing decisions around launches, pricing, promotions and customer interactions. Technologies such as Signal Detection are allowing for more adaptive trials by using signals to make changes in test protocols much earlier than previously possible. Predictive modelling is helping scientists fail faster and fail cheaper in their quest to identify the target drug molecule by helping them know, for example, who has worked previously on those compounds or sequences, what kind of results are likely and which genetic pathway is more promising.
Looking AheadThe main immediate financial impact of these changing software/IT trends on pharmaceutical companies is to reduce dependence on their own IT infrastructure and move away from capital expenditure-intensive deployments to more operational expenditure, pay-as-you-go business models. There will also be more focus on aspects related to security, privacy, data protection and IP management. Software and IT advancements offer a way for pharmaceutical companies to move with the changing market, and adapt to meet new industry and customer demands. The key advantages are more standardized and streamlined operations, higher reusability, better integration, and stronger collaboration with external entities and the healthcare ecosystem.
The pharmaceutical industry is changing rapidly. Technology is playing a key role in driving some of these changes and in capitalizing on them to the industry’s benefit. With the recent trends and advances in mobility, cloud computing and predictive analytics, technology is poised to shape the future of the pharmaceutical industry and help it rise to the challenges ahead.
References1. IMAP, “Pharmaceuticals
& Biotech Industry Global
Report” (2011).
2. www.rncos.com/Report/
IM321_fig.htm
For more informationR. Arun Kumar
Vice President and Head of
Global Life Sciences
Infosys
R. Arun Kumar

42 www.pharma-mag.com July/August 2011
SAEs
U ntil recently, the public often assumed that drugs approved as safe and effective by regulatory agencies were, in fact, safe and effective; but a series of highly publicized
product withdrawals and black box warnings placed on marketed drugs during the past few years has alerted the public that regulators must focus more closely on safety signals that arise during drug development. As a result, the accurate and timely reporting of serious adverse events (SAEs) during clinical trials is under intense scrutiny.
The traditional paper-based process for SAE reporting is notoriously cumbersome and potentially error-prone because of multiple exchanges of documents among team members, often on different continents, in different time zones, using different languages. The inability of an investigative site to communicate the narrative to the sponsor, or the failure of a sponsor to report the event to all the other study investigators in accordance with specified timeframes, can increase the risk to other study volunteers and
possibly result in sponsor liability. And yet, in this increasingly complex and regulated environment, companies continue to use unsecure manual methods for SAE reporting and notification, such as fax, email and overnight mail.
There is, however, an online alternative — a hosted Web-based platform that is simple to use, secure and much cheaper than paper. Many large pharmaceutical companies using this method can save millions of dollars annually in overnight mail costs, whilst making the process far less labour-intensive. In addition, this virtual method centralizes all documents in a single, online location for 24/7/365 availability, thereby shortening the timeframe for notification from days to minutes, which reduces the risk for both study subjects and sponsors. With these benefits, the cost of maintaining the status quo exceeds the cost of implementing new technology designed to streamline SAE procedures.
Better SAE ReportingThe growing interest in broad-based safety data is leading to larger and more global clinical trials. As part of this effort, investigative products are being studied in a wider array of subjects to improve the detection of adverse events. And when those events are deemed serious (Figure 1), the clinical community — investigative sites, sponsors, contract research organizations (CROs), institutional review boards/ethics committees (IRBs/ECs), regulatory agencies — need to know fast.
Evidence that better SAE reporting is a hot button issue comes from FDA, which issued final regulations in September 2010 for safety reporting requirements for investigational new drug applications (INDs), and for bioavailability and bioequivalence studies. The intent of the new rule, which went into effect in March 2011, is to implement internationally harmonized definitions and reporting standards so that critical safety information about investigational drugs is accurately and rapidly reported to the agency. Importantly, certain safety information that previously
Regulatory mandates are putting pharma companies under the spotlight to find quicker ways to report on serious adverse events (SAEs) during clinical trials. Moving away from manual methods for SAE reporting and notification to an online alternative that is far more secure, efficient and cost effective is the way to go.
STREAMLINING SAE REPORTING
Figure 1: Definition of a
Serious Adverse Event. Figure 1

July/August 2011 www.pharma-mag.com 43
The definitive showcase for processing & packaging machinery
Jointly owned by: Co-located with:
Gain a competitive edge in our brand new Manufacturing Forum; a comprehensive seminar programme where you can draw inspiration from the latest case studies and success stories and join in the lively debate
Discover how to improve productivity and reduce waste with the latest technology and services being showcased by over 300 suppliers
LIVE machinery demonstrations – see equipment on select stands put through its paces to help you make all the right sourcing decisions
Find out who are the industries shining stars in the Ones to Watch awards, where we will be highlighting some of the young talent who are innovating the processing & packaging world
Register NOW for your FREE entry badge via: www.ppmashow.co.uk/pharma
Have a smartphone? Then scan this QR barcode and be taken directly to register for free entry.
RegisterFREENow!
4358 PPMA Pharma advert 210x280v2.indd 1 07/07/2011 14:12

44 www.pharma-mag.com July/August 2011
SAEs
had not been required to be reported to FDA must now be reported within 7–15 days of becoming aware of an occurrence (Figure 2).
In Europe, sponsors with at least one active investigative site are to report on an expedited basis to the Central Authority of the involved member states and to the ECs all relevant information about suspected unexpected serious adverse reactions (SUSARs). Timelines for reporting are 7 days for fatal and life-threatening SUSARs, with an additional 8 days for relevant follow-up. All other SUSARS are to be reported within 7–15 days.
Sharing all of this critical information is often inefficient because of the redundant and manual elements of this paper-based approach. The process of printing, collating, labelling, mailing, faxing or e-mailing SAE information to an ever-expanding global site community is quite intensive, and does not generate a reliable audit trail for the sponsor. Moreover, research suggests that managing adverse events and SAEs can consume 10–20% of a study co-ordinator’s time at the investigative site, and the documents they handle are unsecured, could go to the wrong recipient or get lost. This awkward scenario is destined to improve with the introduction of secure online solutions and the growing emphasis on earlier and more accurate safety signal detection.
Reporting SAEs By web-Based PlatformForward-thinking companies are considering proactive methods for better collection, evaluation and distribution of SAE-related information. With tight deadlines for reporting and disseminating information to thousands of sites and other parties in response to an SAE, it is no longer practical for sponsors to rely on manual, paper-based methods of communication.
Transitioning to proactive mode is happening through the use of secure Web-based platforms. When properly designed, these online solutions can
facilitate end-to-end safety communication capable of integrating with existing clinical applications. From collecting SAE information from sites to automatically alerting parties who need to review it, to ensuring the secure, auditable distribution of safety letters to all affected parties, these online platforms speed and simplify the entire process. By centralizing and standardizing the management and communication of safety events on a single platform, sponsors are able to easily organize, track and search important safety information. This approach streamlines the SAE process, cuts time and costs, and allows sponsors and CROs to adhere more readily to regulatory timelines and demonstrate compliance.
To reap these benefits, a company must decide between building Web-based capability internally or partnering with an information technology (IT) provider. The prospect of building, implementing and maintaining an internally supported safety document exchange solution from the ground up can be a daunting task for a company whose core competency is developing new biopharmaceutical products. Although some sponsors and CROs, particularly larger ones, may have extensive in-house IT capability, maintaining a Web-based system for thousands of end-users worldwide and keeping the requisite software in compliance with evolving security standards may be beyond the capacity (and interest!) of internal departments. Further challenges for in-house systems include the ongoing need for constant updating, training and 24/7/365 support in multiple time zones and languages.
A Software-as-a-Service (SaaS) solution from a trusted IT partner — whereby the provider hosts the platform, and assumes all responsibility for software
Figure 2: Safety information
to be reported within 15 days
to FDA.
Figure 2
By CENTraLIZING AND
STANDARDIZING ThE
MANAGEMENT AND
COMMUNICATION OF
SAFETy EVENTS ON A
SINGLE PLATFORM,
SPONSORS ARE ABLE TO
EASILy ORGANIZE, TraCk
AND SEARCh IMPORTANT
SAFETy INFORMATION.

July/August 2011 www.pharma-mag.com 45
SAEs
For more informationLinda Bowers
Vice President of Life
Sciences Product Marketing
IntraLinks
management and updates, maintenance and end-user support provider — is a practical choice for companies of all sizes. Furthermore, neither the sponsor nor CRO needs upfront capital investment and, significantly, this model frees up internal IT resources to focus on other activities.
Because the provider generally owns the SaaS infrastructure and maintains state-of-the-art online security features, clients don’t have to worry about the security of the environment. The client is, however, given the power to grant access to users inside and outside the firewall, and assign them varying levels of capability permission, allowing the client to maintain strict access control. In addition to controlling access, clients can also tightly control the content. Document rights management and version control ensure content is controlled and everyone is working off the same information. In the case of safety reporting, an online platform serves as a single, central repository for safety documents in which the safety team can manage, track and store all documents related to safety in clinical trials, as well as standardize the collection, distribution and communication of such documents with investigative sites, IRBs, CROs and others.
Making the ChangeAs stakeholders worldwide adapt to an ever more vigilant atmosphere toward SAE reporting, they must be ready to gather and disseminate safety information in accordance with specific regulatory timeframes. Continuing with manual processes for preparing safety packages and generating SUSAR letters is giving way to Web-based solutions that can expedite these activities and reduce the risk to subjects participating in studies. Moving from a paper-based method to an online platform provides the scalability and flexibility to stay in compliance with continually changing regulatory timeframes for global safety reporting.
In making the transition to an online safety reporting solution, companies are faced with the classic “build versus buy” question. The scope and breadth of the global safety reporting process, and the system requirements to support it, must be carefully considered. Companies must evaluate their ability to develop and manage all aspects of an in-house system versus partnering with a trusted provider. The fact that the provider can host the platform for global team members and provide the necessary maintenance, upgrades and support makes outsourcing an attractive choice for improving safety-related document exchange.
Linda Bowers
ShOwCASEIt’s In Our Nature The design team at Measom Freer
have again added more shapes to
their stock bottle ranges. There is the
tall elegant tapered ‘Nature’ range
which launches with both 100 and 200ml options, manufactured in house in
clear PVC, with colours and PETG available to order and the ‘Pageant’ bottle
which is designed with a flowing triangular shape and a good on-shelf presence
with large front and back panels for product graphics and details. The Pageant
is currently available as a 100ml in clear PVC with other sizes to follow. Both
shapes stand out on the shelves from other bottles and will give your products
the ‘presence’ they deserve.
The neck sizes on both shapes are standard European R4 (USA 415) which
suit Measom Freer’s stock range of caps, dispensers, neck plugs and pumps
giving you flexibility on how you want your product delivered. Screen printing
in one or several colours is also available to complete the desired look. These
bottles are ideal for liquids, gels, pharmaceutical and medical products.
Measom Freer also manufacture and stock an extensive plastic packaging
range, from jars and boxes to measuring scoops and fasteners with all their
products designed and manufactured in-house. Speak to their Sales team now
to find out more about how these new and interesting bottles can enhance
your brand image and shelf presence. In addition, their stock packaging has a
minimum order quantity of just a single box which means minimal lead-times,
optimising your cash flow and stock management.
Their Sales team look forward to discussing your requirements
soon: Telephone +44 (0)116 2881588, Fax +44 (0)116 2813000,
[email protected] or online at www.measomfreer.co.uk
96-Channel handheld Electronic PipetteThe INTEGRA VIAFLO
96 is a 96-channel
electronic pipette that
enables the fast, precise
and easy simultaneous
transfer of 96 samples.
No special skills or
training are required
to operate the VIAFLO
96, which features the
company’s popular
Touch Wheel pipette
user interface, enabling
the simple and fast programming of a wide range of pipetting modes
(repeat dispense, serial dilute and sample dilute). Fast replication or
reformatting of 96 and 384 well plates and high precision transferring
of reagents, compounds and solutions to or from microplates is now
as easy as pipetting with a standard electronic pipette into a single
tube. Four heads with pipetting volumes up to 12.5, 125, 300 or
1250 µL are available for the VIAFLO 96. These pipetting heads are
interchangeable within seconds, enabling optimal matching of the
available volume range to the application performed. The VIAFLO
96 uses VIAFLO GripTips that provide a perfect seal every time and
won’t fall off during use. The unique combination of features provided
by the VIAFLO 96 will not only increase your productivity but also
facilitate the accurate delivery of liquids to target vessels, reduce
cross-contamination, lower operating fatigue and provide consistent
results (www.integra-biosciences.com).
46 www.pharma-mag.com July/August 2011
BIOTECHNOLOGY
Cancer is a complex disease and the more we understand about it the more complex it seems to become. Within any given tumour there are multiple underlying genetic factors, multiple mutations, overlapping
signalling pathways and the ability to adapt and to develop resistance to various forms of treatment, so that even within a single patient we are not seeing a single disease during the course of time.
Most scientists working on anticancer therapeutics are directing their expertise on ever more well‑defined and detailed elements of this increasing complexity, seeking to discover small molecules, antibodies or other biological agents to induce cancer cell death. These approaches are focused upon single receptors or single molecular pathways to become more selective, with the current buzzwords in the field of oncology being ‘targeted therapies’ and their associated ‘biomarkers.’ A much smaller group of scientists have been working (much more quietly) on a more novel approach to cancer therapeutics called oncolytic viruses. The recent news of Amgen’s billion dollar deal for BioVex and their oncolytic herpes virus OncoVEX, which is in Phase III clinical development for melanoma, has thrust this novel approach much more into the spotlight, but for now it remains a less well-known discipline.
Oncolytic viruses are live viruses that selectively infect and kill tumour cells. This is a unique drug class and currently the only class of agent for any disease able to replicate itself at the site of action. This selective replication and the resultant tumour cell lysis serves to both eradicate the target tumour cells whilst further amplifying the therapeutic, thus providing progeny viruses to kill surrounding cancer cells in a spreading wave of infection. Although this approach may at first sound somewhat worrying, it has transpired in clinical trials (now with more than 3000 patients treated) that this is also a relatively safe form of cancer therapy. As these viruses are by definition selective for cancer cells, they spare the surrounding normal cells; if there is no tumour then the virus will not replicate and the spread simply stops at the tumour margins.
Unfortunately, as for many other approaches to cancer therapeutics (think antibodies and vaccines), the early promise of oncolytic viruses has not yet been fully realized. BioVex appears to have developed a potential winner, but
will there be others who follow? It is of course a complex problem and there are a number of significant issues to address. A replicating virus has considerable complexity when compared with a small molecule or even to most complex biologics. Viruses have evolved during millions of years to replicate within normal cells, so how can we now rapidly and reliably design one that has the optimized characteristics of tumour selectivity, potency and stability?
Genetic engineering of viruses has now become commonplace, and wild type or attenuated viruses can be modified with a virtually limitless variety of gene modifications, insertions, deletions and substitutions in almost any molecular laboratory in the world. The Amgen OncoVEX virus, for example, is a wild type herpes simplex virus modified with the addition of the gene for Granulocyte-macrophage colony-stimulating factor (GMCSF) and the deletion of certain immune suppressor genes. Jennerex has developed an attenuated pox virus with a GMCSF insert and the thymidine kinase (TK) gene deleted. Oncos may have taken this concept of ‘intelligent design’ the furthest, modifying their adenovirus with the addition of GMCSF, replacing the capsid receptor gene and modifying other genes to drive tumour selectivity.
Despite what appears to be increasing success with some of these agents in the clinic, some scientists are now worried that the genetic manipulation of viruses in an attempt to increase selectivity and potency may be significantly hampered by our limited knowledge of cancer cells. The complexity and plasticity of tumour cells and their interaction with viruses may thus hinder the rational or intelligent design of new oncolytic viruses. It is currently impossible to predict the optimal changes to be made to any given virus to optimize it, as even a single base pair change could result in significant changes in function and activity. Although the list of new oncolytic viruses developed using virus types including measles, reovirus and Newcastle disease virus each with varied modifications for potency and selectivity is growing monthly, the potential for new ones is endless and we are still a very long way from enjoying the diversity of viral agents required to run a high throughput screening process.
One novel approach is to go back to the original process of viral ‘design,’ which was not by an ‘intelligent designer’ at all, but by the process of evolution and natural selection.
As science continues to find the limitations of current therapeutic approaches, it is clear that totally new modalities are urgently required for the treatment of cancer. The field of oncolytic viruses is a novel form of cancer therapy that is just beginning to see success in the clinic, but how can this form of therapy be optimized given the emerging complexity of the cancer cell and its environment?
ThE EVOLUTION Of A NOVEL fORM Of CANCER ThERAPEUTICS

July/August 2011 www.pharma-mag.com 51
“
“

July/August 2011 www.pharma-mag.com 47
BIOTECHNOLOGY
Directed evolution or bio-selection provides an ideal process to explore and resolve the combined complexity of cancer cells and viruses. In some respects this is a high-throughput screening platform for the discovery of novel oncolytic viruses (Figure 1). Directed evolution is not a new concept in the field of virology and has been utilized as a way to modulate viral vectors and to enhance gene delivery with a focus primarily upon enhancing infectivity or modulating tropism by changes to the viral coat. For oncolytic viruses the process seeks to drive a pool of viruses that have naturally evolved to replicate in normal cells so that they become adapted to replicating in and killing cancer cells.
Although the biological alterations needed to reach this goal are still highly complex (the same as those facing the intelligent designer), the scientist running a directed evolution experiment does not need to think at all about the individual gene alterations that are required. As for natural evolution, the directed evolution approach is dependent upon two main factors, namely diversity and selection. By creating a large diversity in the starting pool and establishing the correct selection pressure the scientist is able to drive the evolutionary process towards a desired goal without ever knowing what the end product may be. The process allows literally millions of experiments to run in parallel with each individual virus ‘tested’ for its ability to survive in the cancer cells. The more the variability in the starting pool, the more ‘experiments’ are conducted. Only those viruses that replicate well and thus kill the cancer cells release their progeny fast enough for selection in the next round. At each round in the selection process the ‘fittest’ viruses are thus those with increased potency and selectivity in their new environment. Ultimately, an entirely new viral ‘species’ can
be selected from the pool. The ‘survival of the fittest’ in this case will be the virus best adapted to kill cancer cells, but no longer able to replicate in normal cells.
ColoAd1 is the first oncolytic virus developed by directed evolution. It happens to be an Ad11/Ad3 chimeric adenovirus with a number of genetic modifications, including a new chimeric E2B region and the loss of E3 and E4orf4 genes; but, the point is that it is a virus that does not occur in nature and yet has a much higher potency and selectivity in cancer cells than any of the original parent viruses in the starting pool. Recent work conducted by Professor Len Seymour’s group at the University of Oxford suggests that these genetic changes may have had profound effects upon the way that the virus kills cancer cells: “Most viruses kill cells using the same terminal apoptotic pathways that are used by other traditional chemotherapeutic drugs. This process might be seen as a form of ‘assisted suicide’ for the cancer cell. ColoAd1 on the other hand appears to have evolved a more direct necrotic killing mechanism, which we might regard as tumour cell ‘murder’,” explained Professor Seymour at the 6th International Conference on Oncolytic Viruses as Cancer Therapeutics in las Vegas earlier this year. Professor Seymour admits that it remains unclear which of the many genetic modifications within ColoAd1 are specifically responsible for this changed activity, a fact that underlies the power of the directed evolution approach. ColoAd1 will be taken into a Phase I/II clinical study in metastatic colorectal cancer by PsiOxus Therapeutics next year, where the value of this novel approach will be put to the ultimate test; if positive, then directed evolution could form an important platform for the development of further novel oncolytic viruses.
For more informationJohn Beadle
CEO
PsiOxus Therapeutics Ltd
www.psioxus.com
Figure 1: Directed evolution
schematic.
Figure 1

48 www.pharma-mag.com July/August 2011
FACILITY DESIGN
e very facility’s main objective must be to ensure that manufactured medicinal products will be fit for their intended use, will comply with the requirements of the marketing authorization and will
not place patients at risk because of inadequate safety, quality or efficacy. Having a proper facility design will facilitate obtaining appropriate quality products and will allow work to be done in an easier and proper manner in accordance with the existing machines, products, materials, flows and company policies. To undertake the design of a new or renovated plant, facility or system, the starting point is to detail the requirements with which to comply.
Basis Of Design: Multidisciplinary EvaluationThere are many factors to consider other than GMP requirements, which are mandatory, when designing a new or renovated plant or facility — logistics, economics and cultural aspects are just as important and sometimes have a greater impact on the design. Today, issues such as social responsibility, environmental sustainability and minimized energy consumption are becoming more important and, therefore, a responsible and well-prepared design must address them.
Designs can of course include innovation and improvements; improvisation, however, should be omitted. The complete design process must be consistent, rationally justified and constantly under control by following appropriate written procedures to avoid missing relevant design inputs. Issues that have not been fully considered during the design stage are likely to result in difficulties and higher costs further down the line.
All factors must be analysed as a whole rather than independently to make the appropriate decisions. Furthermore, they have to be analysed as combined variables and the analysis must address different points of view, which requires the involvement of multidisciplinary teams.
Design decisions must be oriented to find the best solution with regard to quality, reliability,
efficiency and lowest costs of investment, operation and maintenance. The best design is not the one with the most technically sophisticated or expensive solution; the real added value of a design is to have the best solution possible for each specific situation. Evaluating all parameters and possible solutions will help to avoid over-engineering and excessive costs.
New Plant Design: Main ConditioningsMany issues can affect and will condition the design of a new pharmaceutical plant; but generally, the main ones are location, products and manufacturing processes.LocationThe plot of ground where the building is to be allocated is a particularly important decision to make because of the following: • Physical limitations of the building or the different
location areas. In addition to the available area, special attention should be paid to vertical limitations that may occur because of the building height. There must be enough space between floor levels to include appropriate technical floors and areas where utilities piping, HVAC ducting and luminaries will be fitted, to facilitate organized distribution, good identification and easy access for maintenance. Check local regulations about civil works and estimate whether the area and height of the building will permit the desired floors and space.
• Availability of the required quantity and quality of utilities. Check the external supply of main services (electricity, water): the normal and maximum supply capacities, and its quality all year round — insufficient quantity can limit production capacity and inadequate quality will require higher costs to take its quality parameters into required ranges. It is also important to consider where the supplied external utilities will enter in the building plot. In the conceptual design of the plant, allocate utility technical areas depending on the supply points to the building plot and the utility point, whilst trying to minimize the distances from outside to
DESIGN fOR IMPACT
The design of a facility is instrumental to a plant’s future success. The author shares some tops tips to consider during the planning stage of the design.

July/August 2011 www.pharma-mag.com 49
FACILITY DESIGN
the equipment utilities and from there to the points of use.
• Logistics. To facilitate the logistics for distribution is not critical for the design itself, but having optimum communications for distribution is important for the manufacturers. The entrance and exit of materials and products should be as easy and smooth as possible. The frequency and the amounts of received or dispatched products, together with the required materials and products warehousing stocks, should be estimated to assign adequate dimensions for the estimated storage capacities for each warehouse.
• Climatic conditions. Depending on the required conditions of temperature and humidity for production and the warehouses, the location of the plant may become cost-critical — it may greatly affect utilities design, particularly for the HVAC system, energy consumption and maintenance to keep variables inside range limits.
Products and Manufacturing Process• Pharmaceutical forms, batch sizes, facility production
capacity and manufacturing processes are the main criteria for machinery selection and main area sizing and distribution.
• Production capacities, manufacturing and finished products outputs. Once the machines are chosen, simulate the different production scenarios to check the plant output capacity against the considered design. A good design must consider future increase production capacities through increasing the effective production time, shift numbers, batch
sizes; alternatively, design the facility in advance to include future extensions with new machines or lines as predicted.
• To ensure final product quality and protection, the HVAC must be well designed. The clean room architecture must permit the required environmental cleanliness levels to be achieved and maintained according to regulations and guidelines. Cleanliness levels depend on many issues analysed individually and together as they affect each other: finished product quality requirements, pharmaceutical forms, manufacturing processes, product risk of contamination as a result of its condition and exposure to the environment (open versus closed system), and the possibility of removing contaminants in later manufacturing steps (final sterilization versus aseptic manufacturing).
• Depending on the product toxicity/potency specific containment requirements have to be met for each product and process: primary containment for immediate environment, personnel safety and cross-contamination prevention; and secondary containment for environmental safety.
• Contamination risks — particularly cross‑contamination in multiproduct facilities.
Others• Areas included in the plant to be sized adequately
in relation to the production capacities, stocks and number of workers: warehouses, production, quality control (QC), ancillary areas (dress rooms, offices, technical areas).

July/August 2011 www.pharma-mag.com 53
Major pharmaceutical and food companies are increasingly turning to T-Tubes, a new form of advanced insulation for stainless steel process lines in clean environments. Developed jointly by Zotefoams and UFP Technologies, and inherently flame retardant, T-Tubes is an FM 4910/4924-approved, advanced insulation system. Comprising a clamshell design, straight components for a wide range of pipe sizes and custom-moulded components to insulate elbows and tees, the T-Tubes system delivers savings in both installation time and long-term ownership costs.
Easy and Cost-Effective to InstallEach component in the T-Tubes system is thermoformed from closed cell, cross-linked ZOTEK F PVDF foam — which inhibits moisture and vapour ingress — while thermoforming provides a durable, cleanable, puncture-resistant skin. As such, the expensive to install stainless steel or PVC jacketing that many competing open-cell or fibrous insulating materials need are not required. Individual T-Tubes components are fitted quickly and secured and sealed with an overlapping, PVDF, pressure-sensitive adhesive tape or the fast curing T-Tubes adhesive, making them far more economical to install than conventional, jacketed insulation. The dust-free, nature of the ZOTEK F foam means that T-Tubes can be cut to size without the use of bags or hoods and without compromising clean environments.
Low Maintenance RequirementBecause T-Tubes are resilient and the foam has a ‘memory,’ the system is less susceptible to damage during installation and subsequent use. Even if a T-Tubes system component becomes punctured, the
closed cell nature of the ZOTEK foam itself will not allow moisture to enter and the insulation remains effective. As T-Tubes do not wick moisture, allow mould growth or deteriorate with use, they can be reused after equipment replacements or inspections, making them a truly economical proposition with a low overall lifetime cost.
Good thermal insulation propertiesOnly 6.35 mm in thickness, the T-Tubes insulation system is highly efficient with tests indicating a thermal conductivity (K) of 0.0317 W/mK @ 22 °C (72 °F) according to the ASTM C-518 test method. Being so thin means that it can be installed in practically any situation. T-Tubes have a working temperature range of –80 °C (-112°F) to +160 °C (320 °F) making them ideal for both low and high temperature insulation (from refrigerated fluids to superheated steam).
Notoriously, refrigerated steel pipe work induces condensation, even in clean environments. Condensate often provides a breeding ground for micro-organisms; but, more importantly, it adversely affects the temperature gradient along the length of the line and makes it more susceptible to ambient humidity and temperature conditions. Using T-Tubes allows companies to better control their energy costs while maintaining constant process conditions.
Excellent Chemical ResistanceZotefoams claims that T-Tubes are as robust and chemically sound as PVDF base resin. In addition, they are reported to be generally resistant to chemicals with a pH up to 12 and, when tested against widely used sanitization chemicals such as hydrogen peroxide, they exhibit neither visual damage nor chemical absorption.
When Time is ImportantTime is critical during installation, so the speed with which the T-Tubes system can be installed has a beneficial effect on a project’s critical path. However, minimizing the cost of maintaining and repairing the insulation when the plant is up and running is also a significant consideration. T-Tubes is a durable system but offers a rapid, easy repair facility that will reduce production downtime and help to maximize plant availability. Plant operators interested in minimizing lifetime costs would be well advised to consider T-Tubes for process pipe insulation in clean areas.
ADVERTORIAL
July/August 2011 www.pharma-mag.com 53
T-TUBES: ADVANCED INSUlATIONSpace efficient, coSt Saving, chemical reSiStant clean room pipe inSulation
For more informationNorth America: UFP Technologies Inc.Tel. +1 800 372 [email protected]
Europe, Asia, Middle East: Zotefoam plcTel. +44 208 664 [email protected]

50 www.pharma-mag.com July/August 2011
FACILITY DESIGN
• Personnel, materials, products and waste flows. The different areas (warehouses, production, QC) should be laid out according to cleanliness levels and flow of personnel, materials, products and waste.
• Hygienic and cleanliness requirements. Regulations stipulate the minimum levels to comply with; occasionally, manufacturers may have internal policies that specify higher requirements.
• Machinery and their main characteristics, for example, the size, the utilities supply requirements and consumptions, the level of containment/protection provided by the machine.
• Other regulations; for example, local regulations, safety regulations, specific requirements for explosion proof areas.
Traceability and Project qA: Commissioning and qualification The design will be the first phase of a complete project to build and start up a new facility. A well-planned and consistent commissioning and qualification (C&Q) programme must be implemented to strictly control all these steps from design to facility turnover. The C&Q approach is intended to be consistent with the requirements of the factory commissioning and qualification policies and procedures. All facilities, systems and equipment will be commissioned according to Good Engineering Practices (GEP); those affecting the quality of the product should also be qualified following Good Manufacturing Practices (GMP).
Once determined, the boundaries of all facilities, systems and equipment should be classified according to its pharmaceutical importance and adhering to GMP guidelines. Depending on how they may affect manufactured product quality, all can be classified as
• Direct impact system (DIS): a system that is expected to have a direct impact on product quality. These systems will be considered GMP systems, designed and commissioned in accordance to GEP and qualified for GMP compliance. For these, a global approach should be developed to perform the risk analysis for the complete equipment functions. The qualification approach will be based on this risk analysis.
• Indirect impact system (IIS): a system that is not expected to have a direct impact on product quality, but typically will support a direct impact system.
• No impact system (NIS): a system that will not have any impact either directly or indirectly on product quality.
C&Q milestones have to be scheduled for the complete project. The design of all systems must be reviewed at an appropriate stage for conformance to all operational and regulatory expectations. This documented review — enhanced design review (EDR) — should be mandatory as requisite for design approval. EDR does not need to be documented as a GMP compliance document unless the reported data will be used as referenced results for qualification purposes.
An integrated C&Q plan is well planned and meets specific conditions; some commissioning test reports can be referenced as qualification valid tests without the need to repeat the tests — thereby saving time, efforts and money — only when• referenced documents, protocols and reports are
documented in compliance with GMP documentation requirements
• the qualified person responsible must supervise or witness the commissioning test execution to accept the result as valid for qualification
Conclusions The best design possible is obtained through conscious design that considers how every detail will affect the quality of the manufactured final product. This is known as ‘design for impact’ and should be performed by an appropriate team of qualified professionals who specialize in the different aspects that must be considered: QC, quality assurance, engineering, maintenance and production.
Although the design is perhaps the most important phase of a project to ensure the best facility at the minimum cost, it is extremely important to have the complete project development and execution under control until the facility hand over, to ensure compliance and documented traceability with the initial requirements. This can be achieved by implementing a well-planned and consistent C&Q programme for all project steps: design, procurement, construction, installation and start up.
For more informationJavier Ballesteros Cherp
Conceptual Design Project
Manager & Senior Project
Manager
Telstar Life Science Value
Services
Consultancy Division
Pharma & Biotech Processes
Telstar
ThE COMPLETE DESIGN PROCESS MUST BE CONSISTENT, raTIONALLy jUSTIFIED AND CONSTANTLy UNDER CONTROL By FOLLOwING APPROPRIATE wRIttEN PROCEDURES TO AVOID MISSING RELEVANT DESIGN INPUTS.

July/August 2011 www.pharma-mag.com 51
Key Account Management USA 2011
Use KAM to revolutionize your pharma sales strategies and maximize profitabilityImplement KAM to achieve:
Two-day pharmaceutical conference - September 13th-14th, Philadelphia
First ever KAM specific pharma conference in North America
Benchmark your KAM strategies against our expert speakers:
Visit www.eyeforpharma.com/kamusa/ for the latest speaker line up,
agenda, free podcasts and easy registeration!
Increased market share and access: Exploit the multiple benefits of KAM to escalate your market share and access while providing a better customer experience
A positive return on investments and objectives: Learn from experts how to set your company’s key account goals and execute them effectively
Improved stakeholder management: Find out how you can effectively enhance stakeholder relationships and increase customer retention through best practices
Higher retention of top sales talent: Examine ways to retain your best talent by training them to be effective KAM enforcers
Dramatic sales growth: Boost your sales figures like never before with a dynamic KAM model
PLUS
KAM in action: Hear successful case studies from companies leading the field in KAM and how it has positively affected sales
Developed by:
Edward DepazDirector, Corporate AccountsShire
Bernard QuancardCEOSAMA
Lee GittingsDirector, Customer AlliancePfizer
Joe CoffeyVP SalesBaxter
Juan OrriolsRegional Director, SFEJohnson & Johnson
Mary StuttsVP, Global Corporate CommunicationsBMS
36OPMTHE FULL SPECTRUM OF PRODUCT MANAGEMENT
36O
Media Partners:
“eyeforpharma always deliver cutting-edge, concise conferences on a global scale. I am proud to be associated with them and see them as a key player in delivering up-to-date intelligence to the industry”
Len Strarnes, Bayer - Schering

52 www.pharma-mag.com July/August 2011
MARKETING & BRANDING
the relationship between a company’s values and the same values it attaches to its brands has always been important, but often overlooked. With the rapid development of social media and the proliferation of
peer-to-peer reviews, forums and bulletin boards, the way people make choices and how they exchange information has changed and is no longer under the control of companies or traditional influencers such as the medical professional.
The new voice of social influence lies in the World Wide Web. This mutation reviews company reputations, scrutinizes claims and broadcasts hypocrisies. The importance of having corresponding internal and external values with strong synergy between corporate message, brand claims and product delivery is critical.
Many companies have strong, ethical and unique corporate values. Pharmaceutical companies in particular generally benefit from well‑articulated credos and visions and missions because of their position as championing worldwide health care and wellbeing. Yet, and this is particularly true in the pharmaceutical sector where the drug is being marketed around a condition ‘need,’ these values can often feel remote from the specific drugs or product categories marketed. In truth, the closer one gets to the product, the less voice these values tend to have. This is now an issue worth considering. As consumers increasingly self-medicate or self-diagnose online, the distance between corporate reputation and product positioning and performance is only a click away.
The impact and corporate damage that a lack of product performance, unrecognized side-effects or even worse, a recall, can have is well documented. But what if a company’s corporate message or actions do not correlate to its products’ marketing? Not only will this affect the performance of the drug/product, but the reputation of the corporate brand can be equally at risk, with potential impact on sister brands and parent share price. This lack of synergy has a special impact on the over-the-counter (OTC) market as information on these products are now freely available online — and thereby beyond the control of the company.
People are now able to research drugs online, reading both product details and public responses in blogs, and make their choices based upon this information. It is in this online space where the reputation of a company can be built or lost. It is said that nature abhors a vacuum. Similarly, consumers on the Web seem to have an insatiable desire for peer approval in their search for any given cure to any given condition. Anonymous requests and answers for product
information or shared experiences now fill a real anxiety gap left by the silence of the corporate voice. Would it be trusted if it was more outwardly present? I believe so, as long as it is not the corporation talking but people from it. Herein lies the dilemma between the anonymous corporate voice, the voice of society and the voice of the individual.
Could it be that the pharmaceutical sector has grown too accustomed to the shroud of secrecy that the medical profession still embraces? What would be the price to pay if it was to engage in a direct, honest and personal dialogue with its customers and end-users? In reality, the battle for secrecy has already been fought and lost online. As Scott McNealy, past CEO of Sun Microsystem, once famously said: “Privacy is dead, get over it.”
Add a certain cynicism about the sector and customer concern about global trading integrity, and you have a real need for change in the way pharmaceutical companies talk about themselves and their brands to their customers. Filling this void of ‘personal voice’ messaging and addressing the new voice of society is the challenge for pharmaceutical companies. Alignment of internal and external marketing methods is a first step. Alignment of corporate messaging with product or portfolio marketing is another. Ensuring that the voice of society, our new Web-savvy society, is addressed to achieve an effective transfer of values from both the corporate and the very individual external spheres is a further key developmental step.
Creation of shared value platforms across internal and external frameworks and communications is essential for employees and employers. For example, investment in employee wellness programmes at Johnson and Johnson (a key tenet of the company’s values) saved $250 million on healthcare costs and ongoing help in stopping smoking complements Nicorette (a key J&J brand) and demonstrates a strong connection between the company values and the product brand.
This is the challenge: pharmaceutical companies must align the product portfolio and marketing mission closely to corporate values. And they must come out from behind the wall of corporate missives and speak frankly and directly to their stakeholders. From business, R&D and marketing strategies and tactics to sales practices, all need to be firmly guided by the ethical values of the corporation. The voice (and conscience) of society is never far away and is ever-ready to uncover any dissonance. This new voice of society is here to stay. So now is a good time to align the values of your company with those of your brands to gain support and commitment.
For more informationNicolas Mamier
Managing Director
Appetite
www.appetiteuk.com
As the freedom of information has grown so too has the need for pharmaceutical companies to align their corporate values to their product portfolio and marketing mission. The voice of society is never far and nor is the need to be acknowledged, which forms an important incentive for companies to manage their brand reputation and act with morals and ethics.
ThE VOICE Of SOCIETY
Nicolas Mamier
Nicolas Mamier
July/August 2011 www.pharma-mag.com 53
• Complete solutions - with full print & camera verification
control for pharmaceutical industry
• Anti-counterfeiting - Datamatrix barcodes,
UV & Infrared printing
• Compliance with GAMP and other regulations
• Touch or key based interface - for fast, easy message
creation at exceptional value
• Prints up to 600x600 dpi
• Print speeds up to 300 meters/min
• Product identification, 1D & 2D barcodes, expiry codes,
graphics, date & time, batch numbers
• Clean/Maintenance free - Easy to change cartridges in
same way as your desktop printer
• Bulk ink system - for all surface types
• Compact - with flexible print head mounting for down
and side printing
• Multiple cartridge mounting - for increased print height,
up to 50mm print height
• Database integration - and custom software solutions
www.xactpack.co.ukt: 0800 112 3620 e: [email protected]
NEW HP Thermal Inkjet Printers from Xact
Xact’s range of HSA thermal inkjet printers operate using the reliable HP TIJ 2.5 technology, delivering high resolution, cost effective print to the pharmaceutical industry and increase security of pharmaceutical products.
PHARMA MAG ADVERT.indd 1 10/05/2011 14:42

July/August 2011 www.pharma-mag.com 53
ZOTE FARMADVERTORIAL

LEGISLATION
M ost importantly for businesses, the Act introduces a new offence (section 7 [s7]) committed by an organization that fails to prevent bribery by associated persons; a
term that the Act defines as including those who provide services on the organization’s behalf. There is a rebuttable presumption that this will include employees, but it may also include agents, consultants and other intermediaries.
On the surface, this new offence has particularly wide extra-territorial reach. All that is required to establish jurisdiction is that the organization should “carry on a business, or part of a business, in the UK.” Each case will be determined on its own facts, but it is possible that an overseas company, which carries on business in the UK through a local subsidiary or a representative office, is exposed to the risk of prosecution in the UK for a contravention of the s7 offence even where the bribery occurs outside the UK and by an associated person who has no connection with the UK.
This new offence is often described as one of strict liability, but there is one statutory defence — if an organization can show that it had “adequate procedures” in place to prevent
such bribery from occurring. Although the issue of whether or not an organization had “adequate procedures” is ultimately a question for the courts, the Government has now (on 30 March 2011) provided guidance on how to determine whether procedures are adequate (the “Guidance”), which is designed to be of general application and is formulated around six principles:• Proportionate procedures: a commercial organization’s
procedures to prevent bribery by persons associated with it should be proportionate to the bribery risks it faces and to the nature, scale and complexity of the commercial organization’s activities. They should also be clear, practical, accessible, effectively implemented and enforced.
• Top‑level commitment: the top-level management of a commercial organization (be it a board of directors, the owners or any other equivalent body or person) should be committed to preventing bribery by persons associated with it. They must foster a culture within the organization in which bribery is never acceptable.
• Risk assessment: the commercial organization should assess the nature and extent of its exposure to potential external and internal risks of bribery on its behalf by persons associated with it. The assessment should be periodic, informed and documented.
• Due diligence: the commercial organization should apply due diligence procedures, taking a proportionate and risk-based approach, in respect of persons who perform or will perform services for or on behalf of the organization, to mitigate identified bribery risks.
• Communication (including training): the commercial organization must seek to ensure that its bribery prevention policies and procedures are embedded and understood throughout the organization through internal and external communication, including training, that is proportionate to the risks it faces.
• Monitoring and review: the commercial organization should monitor and review procedures designed to prevent bribery by persons associated with it and make improvements where necessary.
In essence, these principles boil down to embedding a culture of anti-bribery into a commercial organization with the emphasis falling on the need for a risk-based approach and for procedures that are put in place to be proportionate to the corruption risk faced by an organization. Indeed, the Government deferred the date for final publication, reviewed
On 1 july this year, the Uk’s Bribery Act came in to force. Unprepared businesses may find themselves unwittingly falling foul of its provisions.
hOw ‘ADEQUATE’ ARE YOUR ANTICORRUPTION PROCEDURES?
54 www.pharma-mag.com July/August 2011
July/August 2011 www.pharma-mag.com 55
Organised by
Register now at www.vitafoodsais.com/pharma
Nutraceuticals Functional foods Functional drinks Dietary supplements
Discover the world of ingredients for
FREE
TO ATTEND
REGISTER N
OW
More than a trade show...•Meet over 100 international ingredients and
raw materials suppliers•Attendover25freeseminars•Hearfreekeynotepresentations•DiscovertheNewProductsZone
•DebatewithyourpeersattheDiscussionForum•Networkingopportunities•FreeAdvisorySessions•Marketandtrendforecasts
And much more...
Supportedby
Portfolioincludes
Media & Association Supporters:
VF Asia11 visprom ad 210x280_pharma.indd 1 01/07/2011 21:13

56 www.pharma-mag.com July/August 2011
LEGISLATION
the guidance carefully and has now introduced the need for proportionate procedures as a new first principle.
Senior management should be aware that the emphasis on risk assessment and proportionality cuts both ways. It will be for management to review carefully the potential risks to which their business is exposed (for example, risk profile of their industry sector, location of operations, use of agents and other intermediaries, operational requirements or import/export licences, contracts with overseas Governments) and introduce appropriate measures to counter such risks. In addition, the Government has provided specific guidance on certain other aspects of the Act, which had been of concern to businesses.
Facilitation PaymentsThese are small bribes paid to facilitate routine Government action and could trigger either the offence under the Act of bribing a foreign public official or, where there is an intention to induce improper conduct, including where the acceptance of such payments is itself improper, the offence of bribing another person and (unlike the US Foreign Corrupt Practices Act), therefore, potential liability under s7. As was the case under the old law, the Bribery Act does not provide any exemption for such payments.
The Guidance though reveals a slightly softer approach, with the Government recognizing the problems that commercial organizations face in some parts of the world and in certain sectors, but maintains the eradication of facilitation payments as a long-term objective. The Serious Fraud Office and Director of Public Prosecutions joint guidance for prosecutors (published on the same date as the Guidance) sets out factors that might favour prosecution, including large or repeated payments, facilitation payments that are planned for or accepted as part of a standard way of conducting business, indications of an element of active corruption of the official and if internal procedures concerning the avoidance of facilitation payments have been followed incorrectly.1
Conversely, the guidance for prosecutors indicates it may not be in the public interest to prosecute a single small payment, which might result in only a nominal penalty. The guidance for prosecutors also states that other factors, such as whether the payer was in a vulnerable position arising from the circumstances in which the payment was demanded, will be taken into account.
Corporate hospitality and Promotional ActivityAnother concern raised by commercial organizations was the extent to which corporate hospitality and promotional activity would fall foul of the Act. The Guidance has since made it clear that “…bona fide hospitality and promotional, or other business expenditure which seeks to improve the image of a commercial organization, better to present products and services, or establish cordial relations, is recognized as an
established and important part of doing business and it is not the intention of the Act to criminalize such behaviour.”
Nevertheless, the Guidance acknowledges that hospitality and other promotional activities can be a bribe. The Guidance envisages that organizations may wish to review policies on corporate hospitality and promotional activities to ensure that they are seen to be acting both “competitively” and “fairly.” The Guidance recognizes that different business sectors may apply different standards and leaves it for individual businesses or representative bodies to determine what those standards might be. The point, however, is made that even if the corporate hospitality/promotional activity was in accordance with industry standards, that in itself would be insufficient evidence on its own that bribery had not occurred, particularly if those standards were “extravagant.”
Associated PersonsThe finalized Guidance indicates that due diligence should be conducted on all those business counterparties who provide, or might provide, services on behalf of an organization; that is, if they are capable of falling within the statutory definition of an “associated person.” This is potentially a highly relevant issue for pharma and life science businesses, but once again, the approach should be tempered by the need to take a risk-based and proportionate approach. In relation to existing relationships, the Guidance recognizes that it may not be possible to take any particular steps, but it does expect all that is practicable, within the framework of proportionality, to be done.
jurisdictionIn terms of jurisdictional reach, the UK Government had previously been resistant to providing any clarification on what it would mean to “carry on a business or part of a business in the UK.” The Guidance still leaves this as a matter for the UK courts to determine on the facts of each
Andrew Legg
Joanne Skoulikas
DUE DILIGENCE ShOULD BE CONDUCTED ON ALL ThOSE BUSINESS COUNTERPARTIES whO PROVIDE, OR MIGhT PROVIDE, SERVICES ON BEhALF OF AN ORGANIZATION.

LEGISLATION
particular case; but, it advocates a common sense approach emphasizing that only those organizations that have a “demonstrable business presence in the UK” would be subject to the s7 offence. It has highlighted that the listing/trading of a company’s securities on a UK Exchange or merely having a UK subsidiary would be unlikely on its own to satisfy the business presence test; for example, it is said that the UK subsidiary may conduct business independently of its parent, but whether it does or not is a question of fact.
ConclusionUltimately, the Guidance makes clear that though there is no safe harbour, in relation to corporate liability for failing to prevent bribery on its behalf, a link is made between the adoption of bribery prevention procedures and the self-reporting to the appropriate authorities of any bribery concerns that come to light. It seems clear that a commercial organization that has done its best to address its exposure to bribery risk should expect to be dealt with leniently.
Pharma and life science businesses will inevitably have to factor in the accompanying risks of working in countries and markets with significant exposures, given potentially looser monitoring mechanisms and anticorruption legislation. The very nature of these
industries and their frequent direct interaction with public officials and agencies will also be a significant exposure factor. Questions will additionally have to be considered regarding the method and extent to which ‘encouraging’ intermediaries, such as doctors, to use particular products is appropriate. It is elements such as these that will play a role in considering whether the procedures that are in place can be described as “adequate.”
Through the mechanism of a criminal law statute, the Government is seeking to ensure that appropriate standards of good corporate governance are adopted and rigorously applied to combat corruption worldwide. The Serious Fraud Office (the leading UK law enforcement agency with primary responsibility for the investigation and prosecution of cases involving overseas bribery) has indicated that whilst they wish to work with businesses to eradicate corruption, they intend to come down very heavily indeed on those organizations that use corrupt practices to obtain a business advantage. The new s7 offence is likely to make those businesses that have a business presence in the UK a potentially easy target; those businesses that do not have adequate procedures in place to prevent the bribery that has occurred will find that they have no defence to such a prosecution, which could prove to have very costly consequences for the organization concerned.
Reference1. Bribery Act 2010: Joint
Prosecution Guidance of the
Director of the Serious Fraud
Office and the Director of
Public Prosecutions,”
30 March 2011.
For more informationAndrew Legg
Partner
Mayer Brown
Joanne Skoulikas
Associate
Mayer Brown

58 www.pharma-mag.com July/August 2011
NOSTRAPHARMUS
the generic pharmaceutical industry currently has more opportunity than it can handle! Nostrapharmus notes that much of that opportunity will be more concentrated in emerging markets such as India. With
$100 billion worth of drugs coming off patent in the next 2 years, the result will be an increase in the US from 77% of prescriptions in the first half of 2010 to as much as 85% by 2014.1 Indian drug firms, which account for a third of US abbreviated new drug applications (ANDA), could add $2.5 billion in US sales in the next 5 years.1
The threats to acquiring this market share, however, are also increasing on a number of fronts. Competition among generic manufacturers is fierce, and lawsuits are common and increasing in volume. Also, regulators — particularly in the US — are much stricter with many generic companies currently facing compliance issues. The rigour of regulators and the fierce competition is reflected by the current time taken for ANDA approvals, which has increased from an average of 25–30 months a year ago, to 30 months.2
The challenge for generic companies is to combine science and business acumen. This is partly forced by the regulations as an important section of the Hatch-Waxman Act, which actually encourages generic companies to challenge patents. If a generic company is the first to file its ANDA with a Paragraph IV certification (a patent challenge) and prevails in the subsequent lawsuit, that generic company is granted a period of market exclusivity of 180 days. Most, if not all, generic companies, in both emerging and mature markets, have made the Paragraph IV certification a routine part of doing business. In an industry where profit margins are tight, 6 months of exclusivity for a product can increase a generic’s cash flow exponentially.
So, Nostrapharmus comments, the question that the industry as a whole must solve is: How can you combine the need for speed, whilst remaining compliant? The generic industry business model places significant strain on the operational infrastructure to develop a reliable, robust product in a short span of time. We can take two examples to illustrate this: one pre- and the other -post ANDA submission.
Pre-ANDA ApprovalMuch of the business focus pre-ANDA approval is on R&D and product development with the initial characterization
of the product, and the assessing functionality, impurities and stability to prove bioequivalence. Yet, how much rigour is the purchasing group applying at this same time to evaluate all suppliers and ensure that all product ingredients and components will meet quality standards? Many will ask ‘why should we apply time and resources to evaluating the supply chain for this potential new product when the ANDA has not been approved yet?’ This is a valid ‘business’ argument; but, with increasingly globalized supply chains, FDA requires more, and better, information about product supply chains and will monitor this information throughout the product lifecycle. The data from the FDA Strategic Priorities further highlight this trend and the challenges faced.
Post-ANDA ApprovalPost-ANDA approval, the business priorities shift to the final optimization of product and technology transfer, for scale up to commercial production. Once the product hits the commercial shop floor, just how well has the ‘knowledge transfer’ for the new product taken place? Were manufacturing supervisors involved in the technology transfer process so they can address production issues? Can they assess production excursions (for example, a short temperature spike in a fluid bed) to determine whether it is product impacting? Finally, with the number of ANDA submissions, what happens if a company gets two approvals simultaneously; does it have the bandwidth for scale-up without compromising quality?
Nostrapharmus predicts the principles of Quality by Design will need to be embraced within the generic industry to decrease many of the compliance issues that companies currently face. Quality will not just be about satisfying regulatory requirements, but meeting the requirements of all stakeholders, including customers and shareholders. This will also involve incorporating quality into areas where compliance is not a regulatory necessity including budgeting, purchasing and recruitment. This will be a greater challenge in emerging markets where governance many not be sufficiently mature. To achieve this effective, innovative quality management system, it is important that it encompasses corporate-wide methodology. With increasingly globalized supply chains where the risks are greater, regulators may need to curb the incentives for speed to promote these principles and ensure patient safety.
ThE GENERIC fORMULATIONCan the generic pharmaceutical industry embrace the principles of quality by Design to keep risks low and patients safe?
References1. http://in.reuters.com/
article/2011/04/12/
idINIndia-56277020110412
?pageNumber=1
2. www.pincmoney.com/
Upload/Pharma%20
Results%20Preview%20
Q4FY11.pdf
3. www.fda.gov/downloads/
AboutFDA/Reports
ManualsForms/Reports/
UCM252092.pdf
For more [email protected]
July/August 2011 www.pharma-mag.com 59
www.icsexpo.com
Contract Manufacturing
Clinical Trails
Logistics & Supply Chain
“It is a great way to find new suppliers, to have reunions with actual suppliers from around the world and find new product.”
“Going to ICSE always brings money back to my company.”
“ The best way to meet the right people.”
“ A major professional event which gives the opportunity to meet new customers and potential partners.”
“ All you need to know, under one roof “
Visitor survey
About ICSE:ICSE is the only dedicated Pharma International Contract Services Event to be part of the world’s largest pharmaceutical exhibition; CPhI Worldwide. ICSE connects the pharmaceutical community with global outsourcing solution providers, showcasing the latest innovations and developments within the Pharma Outsourcing industry.
What more could you need?4 shows in 1: ICSE is collocated with 3 specialist Pharma events focused on ingredients, machinery, technology, equipment and packaging. ICSE also includes a diverse conference program, free learning sessions and renowned ‘Innovation Awards’.
Held over three days and attended by key professionals from the global pharmaceutical community, this truly is the annual event not to miss.
Benefits of visiting ICSE 2011:• The combined event attracts over 1,900 exhibitors and
more than 28,500 industry professionals• 90% of 2010 visitors found the products/services they were
looking for• 94% of the 2010 visitors made new business contacts
Register online for FREE
ICSE is the best networking event
for the Pharma Outsourcing industry
ICSE connects the pharmaceutical community with outsourcingsolution providers, offering a forum for business development, networking and education
ContractResearch
AnalyticalServices
C
M
Y
CM
MY
CY
CMY
K
ICSE visitor 210x280 244.pdf 18/5/11 09:38:41

STRAP
60 www.pharma-mag.com July/August 2011
For Europe, Middle East and AsiaZOTEFOAMS PLC, 675 Mitcham Road, Croydon, Surrey, CR9 3AL, UKTel: +44 (0) 20 8664 1600 Fax: +44 (0) 20 8664 1616email: [email protected]
For North AmericaUFP Technologies, Inc.172 East Main Street. Georgetown, MA 01833, USATel: 978.352.2200Fax: 978.352.5616email: [email protected]
EASy TO INSTALLNO jACKETING REqUIREdPVdF hIGh PERFORMANCE FOAMINhERENTLy FLAME RETARdANTdURAbLE ANd RESISTANTNON ShEddINGSPACE SAVING WAShAbLEREUSAbLE
The 21sT CenTury InsulaTIon sysTem for proCess pIpIng In ConTrolled envIronmenTs
advanCed Clean room InsulaTIon





























