Embed Size (px)
Citation preview

PersonalizedFluidResuscitation
MorganSoffler,MD
InstructorinMedicine,HarvardMedicalSchool
Pulmonary,CriticalCare,&SleepMedicine
BethIsraelDeaconessMedicalCenterCOPYRIGHT

Disclosures
• None
COPYRIGHT

Objectives
• Definetheterm“volumeresponsive”
• Describetheinfluenceofvolumestatus,vasculartone,cardiaccontractilityandcardiactransmuralpressureonvenousreturn.
• DescribethelimitationsofCVPonpredictingvolumeresponsiveness
• Identifythestrengthsandlimitationsofdynamicmeasuresofvolumeresponsiveness.
• Evaluatetheresponsetoanempiricfluidchallenge.
COPYRIGHT

ACasetoconsider75yearoldwomanwithHFpEF isadmitted totheICUwithseptic shockfromUTI.
BP75/40à 2LoflactatedringersàBP95/45à BP80/35.
Requiring2LNCtomaintainO2sat>90%
WBC18,lactate4.5,oliguricAKI.
Givenceftriaxone, startedonperipheral norepinephrine andtransferredtothe ICU.
CVO270,CVP12.
USofIVCshowsdiameter>2-cm.
CXRshowspulmonaryedema.
COPYRIGHT

Whichofthefollowingbestdescribesyour
fluidmanagementstrategyandreasoning?
A. Iwouldgivemorefluids– shewasfluidresponsiveprior.
B. Iwouldgivemorefluids– shehaslacticacidosisandhasAKI.
C. IwouldNOTgivemorefluids– sheisnowhypoxemicandhasHFpEF
D. IwouldNOTgivemorefluids– CVPis12andIVCdistended.COPYRIGHT

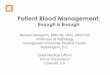
BoydJetal.Crit CareMed 201139(2):259-265
AdjustedSurvivalCurves
FluidBalanceQuartilesDay4
Days**AdjustedforApachescore,ageandpressordose
Survival
Whypredictvolumeresponsiveness?
+
++++
++COPYRIGHT

Whypredictvolumeresponsiveness?
ARDSNet NEngl JMed 2006;354:2564-2575
COPYRIGHT

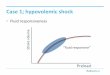
CardiacOutput
Allpossiblecardiacoutputvalues
Predictingfluidresponsiveness
RVEDP=RAP=CVP
COPYRIGHT

CardiacOutput
And
VenousReturn
RVEDP=RAP=CVP
Predictingfluidresponsiveness
VR CO
RAP
COPYRIGHT

GuytonAC.PhysiolRev1955;35:123-129
GuytonAC,etal.Phildelphiaa:W.B.Saunders, 1973
RVEDP=RAP=CVP
CardiacOutput
And
VenousReturn
Predictingfluidresponsiveness
ABILITY
AVAILABILITY
COPYRIGHT

MeanSystemicPressure
Venousreturn= I=V
R
MSP- RAP
RV
GuytonAC.PhysiolRev1955;35:123-129
GuytonAC,etal.Phildelphiaa:W.B.Saunders, 1973
RVEDP=RAP=CVP
CardiacOutput
And
VenousReturn
Predictingfluidresponsiveness
COPYRIGHT

ActualCardiacOutputandVenousReturn
GuytonAC.PhysiolRev1955;35:123-129
GuytonAC,etal.Phildelphiaa:W.B.Saunders, 1973
RVEDP=RAP=CVP
CardiacOutput
And
VenousReturn
Predictingfluidresponsiveness
ActualCVP
COPYRIGHT

Whatdefines“volumeresponsiveness”?
RVEDP=RAP=CVP
CardiacOutput
And
VenousReturnCOPYRIGHT

Anincreaseincardiacoutputinresponseto
increasedmeansystemicpressure– i.e.the
patientisontheascendinglimboftheir
Frank-Starlingcurve
Magder S.Curr Opin Crit Care200616:289–296
Definingfluidresponsiveness
COPYRIGHT

Fluidresuscitation:onesizefits…..
COPYRIGHT

8cmH2O
RVEDP=RAP=CVP
CardiacOutput
And
VenousReturn
Fluidresuscitation:CanweuseCVP?…..
COPYRIGHT

8cmH2O
RVEDP=RAP=CVP
CardiacOutput
And
VenousReturn
Fluidresuscitation:CanweuseCVP?…..
COPYRIGHT

Osman Detal.Crit CareMed 200735:64-68
Falsenegatives
Falsepositives
•150volumechallenges givento
septic ICUpatientsà
“Responders” =15%increase inCI
•CVP<12cmH2Oà PPV47%
•PAOP<12cmH20à PPV54%
CVP
PAOP
R
R
NR
NR
COPYRIGHT

“ThemostusefulwaytouseCVPistoobservetheclinicalresponsetoachangeinCVP…”
• Aretherewaystodothiswithoutgivingvolume?
Magder S.Curr Opin Crit Care200511:264-270
HowtouseCVP
COPYRIGHT

WhatISadynamicmeasureoffluid
responsiveness?
OurgoalistoshiftthevenousreturncurvetotheRIGHT….
Increasemeansystemic
fillingpressurewith
venousvolume
Changeinintrapleural
pressureà inRAP
(respiration)
• Passivelegraisetest
• Empiricboluschallenge
• Pulsepressurevariation
• IVCcollapsibility
• IVCdistensibility
COPYRIGHT

A65yearoldwomanwithchronickidneydiseaseisadmittedtotheICUwithfever,diarrhea,andhypotensionafterarecenthospitalizationforpneumonia.Afterreceiving3Lofintravenousfluidsherbloodpressureimprovesto85/50mmHgbutsheisnowrequiring3L/minuteofsupplementaloxygentomaintainanoxygenationsaturation>90%.
Whichofthefollowingisthemostappropriatemaneuvertoassesswhetherhercardiacoutputwillimprovewithfluidadministration?
COPYRIGHT

Question 8 – Dr. Hibbert
AnswerChoices
A. Passivelegraisetest
B. Pulsepressurevariation
C. IVCdistensibility
D. Centralvenousoxygensaturation
COPYRIGHT

Question 8 – Dr. Hibbert
AnswerChoices
A. Passivelegraisetest
B. Pulsepressurevariation
C. IVCdistensibility
D. Centralvenousoxygensaturation
COPYRIGHT

Boulain etal.Chest.2002;121(4):1245-1252
Dynamicmeasures:PassiveLegRaise
Non-InvasiveCardiacOutputMonitor(NICOM)
BloodPressure
Urineoutput
COPYRIGHT

Boulain etal.Chest.2002;121(4):1245-1252
Pros
•Easybedsidemaneuver
Cons
•Maybeinsufficient volumeto
increase CVP
•Elevated intra-thoracicorintra-
abdominal pressuresmayblunt
increase invenousreturn
•Maybecontraindicated in
traumaandneuroICUpatients
Dynamicmeasures:PassiveLegRaise
COPYRIGHT

•Measuredin40paralyzed,mechanicallyventilatedpatientswithsepsis.
• Volumechallengeprovidedwith500-mLofstarch,“responder”hadatleast15%increaseincardiacindex.
• Δ PPvalueof13%discriminatedbetweenrespondersandnon-responders(sens=94%,spec=96%)
Michard F,etal.AJRCCM2000162:134–138
Dynamicmeasures:Pulsepressurevariation
COPYRIGHT

Michard F,etal.AJRCCM2000162:134–138
Increasedintra-thoracicpressure
à decreasedvenousreturn
Decreasedvenousreturnà decreased
RVoutput
DecreasedRVoutputà decreased
LVoutput
**ΔPPwillbegreaterinpatientswhoareonthe
steeppartoftheirFrank-Starlingcurve
Dynamicmeasures:Pulsepressurevariation
COPYRIGHT

Michard F,etal.AJRCCM2000162:134–138
Pros
•Observational, nointervention
required
Cons
•NotvalidatedwithlowerVT
•Unclearapplicability topatients
withverylowlungcompliance
•Mustbeinsinusrhythm
Dynamicmeasures:Pulsepressurevariation
COPYRIGHT

Question 9 – Dr. Hibbert
A58year oldmandevelopssevereARDSduringanadmissiontothetraumaICUforpelvicandfemurfracturesfollowingaMVA. Heisputonlowtidalvolumeventilationwith 6cc/kg andaPEEPof12cmH20andstartedonparalytic.Onthethirddayofhisadmission,hedevelopshypotensionanddespitereceivingoneliterofnormalsalinehasabloodpressureof75/40mmHgandlactate 4. AnultrasoundofhisIVCisperformedanditisnotedthatduringinspirationhisIVCdiameterisgreaterthanIVC
diameterduringexhalation(percentdifference30%).
Whichofthefollowingisthemostaccuratestatementregardingassessmentofvolumeresponsivenessinthispatient?
COPYRIGHT

Question 9 – Dr. Hibbert
AnswerChoices
A. IncreasedIVCdiameterduringinhalationisduetoincreasedvenousreturnfromincreasedintrathoracicpressure.
B. AchangeinIVCdiameterof30%indicatesthatthispatientislikelytobevolumeresponsive
C. Pulsepressurevariationwillbemoresensitiveinthesettingoflowtidalvolumeventilation
D. Passivelegraisewouldbeabetterpredictorofvolumeresponsiveness inthispatientCOPYRIGHT

Question 9 – Dr. Hibbert
AnswerChoices
A. IncreasedIVCdiameterduringinhalationisduetoincreasedvenousreturnfromincreasedintrathoracicpressure.
B. AchangeinIVCdiameterof30%indicatesthatthispatientislikelytobevolumeresponsive
C. Pulsepressurevariationwillbemoresensitiveinthesettingoflowtidalvolumeventilation
D. Passivelegraisewouldbeabetterpredictorofvolumeresponsiveness inthispatientCOPYRIGHT

• 23mechanically ventilated patientsà nobaseline difference in
hemodynamics, respirophasic IVCchangesmeasured
• IVCdistention wasdefined as:
• Maximumdiameterwasobservedduring inhalationandminimumdiameter
wasobservedduringexhalation
• Volumeexpansion 7ml/kgwasgivenand“responders” hadanincrease inCIat
least15%
DMAX - DMIN
DMIN
Barbier C,etal.IntensiveCareMed200430:1740–1746
Dynamicmeasures:IVCDistensibility
COPYRIGHT

Barbier C,etal.IntensiveCareMed200430:1740–1746
Pros
• Observational
• Ultrasounds readilyavailable
• Highersensitivity (90%v40%)andspecificity (90%v80%)thanCVPcutoffof
7cmH20
Cons
• Requires experienced operator
• Sometimes difficulttogetadequate images
• HighPEEPorlowrespiratorysystemcompliancemaydecrease sensitivity
Dynamicmeasures:IVCDistensibility
COPYRIGHT

Question 7 – Dr. Hibbert
A 75-year-old woman with heart failure presents to the ED with alteredmental status and fever. Her temperature is 101° F, HR 115 bpm, BP 85/40mmHg, RR 16 breaths/minute, O2 saturation 94%. Her lab results are notablefor a WBC 17, creatinine 1.2, and lactate of 4.
Antibiotics are started and a central line is placed. She is given 2 liters ofintravenous crystalloid without significant improvement in blood pressure.The central venous pressure (CVP) is measured at 11 cm H2O and centralvenous saturation is 60%. Upon arrival to the ICU, another 500cc of IV fluidsare administered; her CVP increases from 11 to 13 cm H20 withoutimprovement in blood pressure.COPYRIGHT

Question 7 – Dr. Hibbert
AnswerChoices
A. ACVPof11cmH2Oindicatessheisfluidreplete
B. Thelackofimprovementinbloodpressurefollowingtheinitial2LofIVFindicatessheisnotvolumeresponsive.
C. TheincreaseinCVPof2cmH2Oaftervolumeadministrationindicatesthefluidchallengewasadequate.
D. Thecentralvenoussaturationindicatesshehascardiogenicshockandwillnotbenefitfromfurtherfluidadministration.
COPYRIGHT

Question 7 – Dr. Hibbert
AnswerChoices
A. ACVPof11cmH2Oindicatessheisfluidreplete
B. Thelackofimprovementinbloodpressurefollowingtheinitial2LofIVFindicatessheisnotvolumeresponsive.
C. TheincreaseinCVPof2cmH2Oaftervolumeadministrationindicatesthefluidchallengewasadequate.
D. Thecentralvenoussaturationindicatesshehascardiogenicshockandwillnotbenefitfromfurtherfluidadministration.
COPYRIGHT

CardiacOutput
and
VenousReturn
RVEDP=RAP=CVP
Chooseaparameter
tomonitor
•Thermodilution
(CO/CI)
•Pulsepressure
•SBP
•MAP
•Urineoutput
Assessingefficacyofempiricfluidchallenge
COPYRIGHT

Youmustgivesufficientintravascularvolumetoachieveanincreaseinmeansystemicpressure– thiswillbereflectedbyanincreaseinCVP(at
least2-3cmH2O).
Magder S.Curr Opin Crit Care2005;11:264-270
Wasadequatevolumegiven?
COPYRIGHT

• Definingfluidresponsiveness requiresunderstandingoftheintegratedeffectsofcardiacfunction,vasculartone,andintravascularvolume
• Predictingfluidresponsiveness isacoreskillincriticalcareandcanprotectpatientsfromnon-beneficialfluids.
• Dynamicmeasuresarebetterpredictorsoffluidresponsiveness thanstaticmeasures.
• Ifempiricfluidsaregiven,endpointstoassesschangeincardiacoutputandadequacyoffluidchallengearecrucial.
TakeHomePoints
COPYRIGHT