Embed Size (px)
Citation preview

A. Jörres 10-2015
Prof. Achim Jörres, M.D.
Dept. of Nephrology and
Medical Intensive Care
Charité University Hospital
Campus Virchow Klinikum
Berlin, Germany
Septic AKI in ICU patients

A. Jörres 10-2015
Agenda
• Epidemiology
• Pathophysiology
• Initial treatment

A. Jörres 10-2015
• Retrospective analysis of prospectively collected data from the ANZICS
Adult Patient Database, 57 ICUs across Australia, in total 120,123 patients
admitted to ICU for more than 24 hours (1 Jan 2000 to 31 Dec 2005)
• Of 33,375 patients with sepsis-related diagnosis, 14,039 (42.1%) had
concomitant AKI (septic AKI)
• Sepsis accounted for 32.4% of all patients with AKI.
• Septic AKI was associated with greater severity of AKI (RIFLE category
injury or failure) compared with nonseptic AKI.
• Septic AKI was associated with a significantly higher crude and co-variate
adjusted mortality in the ICU (19.8% vs 13.4%; OR 1.60, 95% CI1.5 to 1.7;
P<0.001) and in hospital (29.7% vs 21.6%; OR1.53, 95% CI 1.46 to 1.60;
P<0.001) compared with nonseptic AKI.
Bagshaw SM et al., Crit. Care 2008; 12: R47

A. Jörres 10-2015 Schrier RW & Wang W, NEJM 2004;351:159-69

A. Jörres 10-2015 Bonventre & Yang, J. Clin. Invest. 2011; 121: 4210-21
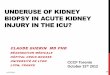
The pars recta of the proximal
tubule and the thick ascending
limb are already normally
hypoxic.
Regional ischemia (especially in
the outer medulla) during AKI is
enhanced by:
• enhanced vasoconstriction
• small vessel occlusion due
to endothelial-leukocyte
interactions
• activation of the coagulation
system
• local edema
Nephron Anatomy and Corticomedullary
Oxygen Gradient
Countercurrent
exchange of oxygen
results in gradient of
decreasing O2
tension in vasa recta

A. Jörres 10-2015
• 423 patients with severe sepsis and electronically recorded continuous hemodynamic
data in the prospective observational FINNAKI study.
• 153 patients (36.2%) had progression of AKI (KDIGO criteria).
• Patients with progression of AKI had significantly lower time-adjusted MAP (74.4
mmHg [68.3-80.8] vs 78.6 mmHg [72.9-85.4], P < 0.001) than those without
progression (cut-off value for prediction 73 mmHg)
Poukkanen M et al, Crit. Care 2013; 17: R295

A. Jörres 10-2015
• 790 patients with AKI I, admitted to the ICU of Guy’s and St. Thomas’ Hospital (July
2007 – June 2009).
• Of 210 patients with haemodynamic monitoring, 85 patients (41.5%) progressed to
AKI III (AKIN criteria) and 91 (43%) died in the hospital.
• AKI progressors had higher SOFA scores, lower indexed systemic oxygen delivery
(DO2I; 325 vs 405 ml/min per m2; P,0.001), higher CVP (16 vs 13; P=0.02), and lower
MAP (71 vs 74 mmHg, P=0.01) in the first 12 h of AKI I
Raimundo M et al, Clin. J. Am. Soc. Nephrol. 2015; 10: 1340-9

A. Jörres 10-2015
• Prospective multicenter, open-label RCT
randomizing 776 patients with septic shock
to undergo resuscitation with a MAP target
of either 80-85 mm Hg (high-target group)
or 65-70 mm Hg (low-target group)
[SEPSIPAM trial].
• No difference in mortality at 28 days (36.6% vs 34.0%) or 90 days
• No overall difference in serious adverse events including renal endpoints or
requirement of acute renal replacement therapy.
• However, among patients with chronic hypertension, those in the high-target group
required less renal replacement therapy than did those in the low-target group.
Asfar P et al, NEJM 2014; 370:1583-93

A. Jörres 10-2015
• Mechanically ventilated pigs with faecal peritonitis and sepsis and Noradrenaline
infusion to maintain mean MAP 65 mmHg
• All pigs developed hyperdynamic shock and AKI but renal blood flow and renal
vascular resistance remained unchanged.
• Renal perfusion pressure and renal
cortex microvascular perfusion
significantly decreased as a result of
increased renal venous pressure.
• Renal histology with only subtle changes
without signs of ATN.
Chvojka J et al, Crit. Care 2008; 12: R164
• Data challenge the concept of renal vasoconstriction and tubular necrosis as substrate
of early septic AKI and point at renal venous congestion as a hidden and clinically
unrecognised mechanism.
Tubular epithelial
cell vacuolisation
with damage of
brush border

A. Jörres 10-2015
• 137 patients diagnosed with severe sepsis or septic shock in surgical ICU of
Lariboisière Hospital, Paris (2006 – 2010).
• 69 patients had new or persistent AKI.
• AKI patients higher SOFA scores, and higher mortality, but no difference in MAP,
ScvO2 and CO than patients without AKI.
• AKI patients had lower diastolic artery
pressure and higher CVP (P=0.0003).
• CVP level was associated with the risk of
developing new or persistent AKI even
after adjustment for fluid balance and
PEEP (OR = 1.22 [1.08-1.39], P = 0.002)
• There was a linear relationship between
CVP and the risk of new or persistent AKI
Legrand M et al, Crit. Care 2013; 17: R278

A. Jörres 10-2015
• Animal models and human studies have shown that the occurrence of
sepsis-induced AKI is not exclusive of decreased renal blood flow states,
and that, on the contrary, can develop in the setting of increased RBF
• A consistent observation in septic humans and animals, regardless of
disease stage, severity, or organ examined, appears to be the presence of
three main alterations:
– diffuse microcirculatory flow abnormalities
– inflammation
– cell bioenergetic adaptive responses to injury
Gomez H et al, Shock 2014; 41: 3-11

A. Jörres 10-2015 Prowle JR & Bellomo R, Semin. Nephrol. 2015; 35: 64-74
Normal Sustained AKI

A. Jörres 10-2015 Prowle JR & Bellomo R, Semin. Nephrol. 2015; 35: 64-74

A. Jörres 10-2015
Ischemia/reperfusion AKI with disruptions of the
glycocalyx and endothelial monolayer
Bonventre & Yang, J. Clin. Invest. 2011; 121: 4210-21
• Ischemia/reperfusion causes
– swelling of endothelial cells
– disruptions of glycocalyx and
endothelial monolayer
– upregulation of adhesion molecules
(ICAMs; VCAMs; selectins) resulting
in enhanced leukocyte-endothelium
interactions.
• There is formation of microthrombi, and
some leukocytes migrate through the
endothelial cells into the interstitial
compartment.
• The interstitial compartment is expanded
with enhanced numbers of inflammatory
cells and interstitial edema forms.
Immune response in ischemic AKI

A. Jörres 10-2015 Bonventre & Yang, J. Clin. Invest. 2011; 121: 4210-21
Immune response in ischemic AKI
• The injured tubular epithelium
releases proinflammatory
cytokines and chemokines,
which aid in recruiting immune
cells, and express adhesion
molecules, TLRs, and T cell
costimulatory molecules.
• Neutrophils, macrophages, and
natural killer T cells cause direct
injury to tubular epithelial cells.
• Dendritic cells are involved in
both the innate and adaptive
immune responses through
secretion of inflammatory
cytokines and presentation of
antigens to T lymphocytes.

A. Jörres 10-2015 Bonventre & Yang, J. Clin. Invest. 2011; 121: 4210-21
Damage and Repair Cycle of Tubular
Epithelial Cells

A. Jörres 10-2015
Agenda
• Epidemiology
• Pathophysiology
• Initial treatment

A. Jörres 10-2015
• Prospective RCT in 263 patients
with severe sepsis / septic shock
upon hospital admission, six
hours of early goal-directed
therapy vs. standard therapy
before admission to ICU
• In-hospital mortality was 30.5%
in the group with early goal-
directed therapy, vs. 46.5% with
standard therapy (P=0.009).
Rivers E et al, NEJM 2001; 345:1368-77

A. Jörres 10-2015
• Total fluid administered over 72
h was not different between the
groups, however:
• During the first 6 hours patients
with early goal-directed therapy
received significantly more fluid
infusion
“Early golden hours”
Rivers E et al, NEJM 2001; 345:1368-77

A. Jörres 10-2015
Protocol-based hemodynamice management
New studies after Rivers et al. (2001)
N=1.600
NEJM 2014; 370: 1683-1693
N=1.341
NEJM 2014; 371: 1496-506
NEJM 2014; 371: 1496-506
N=1.260

A. Jörres 10-2015
Updated Bundles in Response
to New Evidence (April 2015)
With publication of 3 trials that do not demonstrate superiority of required use of a central
venous catheter to monitor central venous pressure (CVP) and central venous oxygen
saturation (ScvO2) in all patients with septic shock who have received timely antibiotics
and fluid resuscitation compared with controls or in all patients with lactate >4 mmol/L, the
SSC Executive Committee has revised the improvement bundles as follows:
TO BE COMPLETED WITHIN 3 HOURS OF TIME OF PRESENTATION:
1. Measure lactate level
2. Obtain blood cultures prior to administration of antibiotics
3. Administer broad spectrum antibiotics
4. Administer 30 ml/kg crystalloid for hypotension or lactate ≥4mmol/L
http://www.survivingsepsis.org/

A. Jörres 10-2015
Updated Bundles in Response
to New Evidence (April 2015)
TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION:
5. Apply vasopressors (for hypotension that does not respond to initial fluid
resuscitation) to maintain a mean arterial pressure (MAP) ≥65mmHg
6. In the event of persistent hypotension after initial fluid administration
(MAP < 65 mm Hg) or if initial lactate was ≥4 mmol/L, re-assess volume
status and tissue perfusion and document findings.
7. Re-measure lactate if initial lactate elevated.
http://www.survivingsepsis.org/

A. Jörres 10-2015
Updated Bundles in Response
to New Evidence (April 2015)
DOCUMENT REASSESSMENT OF VOLUME STATUS AND TISSUE
PERFUSION WITH EITHER
• Repeat focused exam (after initial fluid resuscitation) by licensed
independent practitioner including vital signs, cardiopulmonary, capillary
refill, pulse, and skin findings.
OR TWO OF THE FOLLOWING:
• Measure CVP
• Measure ScvO2
• Bedside cardiovascular ultrasound
• Dynamic assessment of fluid responsiveness with passive leg raise or fluid
challenge
http://www.survivingsepsis.org/

A. Jörres 10-2015
Excessive Fluid Resuscitation Clinical consequences
• Impaired pulmonary function
• Impaired mental status
• Bowel dysfunction
• Intra-abdominal compartment syndrome
• Myocardial dysfunction
• Increased risk of decubital ulcers
• Delayed wound healing
• Muscle weakness / impaired mobilisation

A. Jörres 10-2015
• Prospective observational
study; 618 critically ill
patients with AKI (5 US-
centres)
• Fluid overload (>10% over
baseline) independently
associated with mortality…
• …but kidney function and
renal recovery not improved
Bouchard et al., Kidney Int. 2009; 76: 422-7
With RRT
Without RRT

A. Jörres 10-2015
Fluid Resuscitation
• Early interventions to achieve
hemodynamic stability in
patients with septic shock may
reduce mortality
• Rapid fluid resuscitation of
central importance
• Excessive fluid resuscitation
and overhydration may lead to
increased mortality and worse
renal recovery

A. Jörres 10-2015
• Prospective, randomised study; 6,997 ICU patients in Australia and New Zealand
• Comparison of fluid resuscitation with 4% albumin vs. saline (28 days)
• 726 deaths in the albumin group, 729 deaths in the saline group
(RR 0.99; 95 % CI, 0.91-1.09; P=0.87).
• No difference regarding:
– ICU days (6.5 ± 6.6 with albumin vs. 6.2 ± 6.2 with saline, P=0.44)
– Hospital days (15.3 ± 9.6 vs. 15.6+/-9.6, P=0.30)
– Days on mechanical ventilation (4.5 ± 6.1 and 4.3 ± 5.7, P=0.74)
– Days on RRT (0.5 ± 2.3 and 0.4 ± 2.0, P=0.41).
Finfer et al, NEJM 2004; 350: 2247-56

A. Jörres 10-2015
• Meta-analysis of 38 randomized controlled trials
• Hydroxyethyl starch was found to be associated with
– increased mortality among 10,290 patients (RR 1.09; 95% CI 1.02 -1.17)
– increased renal failure among 8,725 patients (RR, 1.27; 95% CI 1.09-1.47) and
– increased use of renal replacement therapy among 9,258 patients (RR, 1.32;
95% CI, 1.15 to 1.50)
Zarychanski R et al, JAMA 2013; 309 (7):678-688
FDA & EMEA:
Do not use HES solutions in critically ill adult patients,
including those with sepsis!

A. Jörres 10-2015
Hemodynamic monitoring and support
for prevention and management of AKI
1. In the absence of hemorrhagic shock, we recommend using isotonic
crystalloids rather than colloids (albumin or starches) as initial management
for expansion of intravascular volume in patients at risk for AKI or with AKI.
(1B)
2. We recommend the use of vasopressors to maintain perfusion pressure in
volume-resuscitated patients with vasomotor shock with, or at risk for, AKI.
(1C)
3. We suggest using protocol-based management of hemodynamic and
oxygenation parameters to prevent development or worsening of AKI in
high-risk patients. (2C)
The ad-hoc working group of ERBP, NDT 2012; 27: 4263-4272

A. Jörres 10-2015
Vasoctive Agents
• If hypotension is severe or if it persists despite adequate fluid resuscitation,
use of vasopressors is indicated:
– Vasopressor of first choice: Norepinephrin (0.1-2.0 µg/kg/min)
– Dopamin not better than Norepinephrin but may induce more arrhythmias,
increased mortality in cardiogenic shock*
– Epinephrin not better than Norepinephrin**
• Inotropic agent of first choice: Dobutamine
• PDE-III inhibitors (Milrinone, Enoximone) combine inotropic and vasodilatory effects
and may reinforce the effects of dobutamine
*De Backer D et al., NEJM 2010; 362: 779-89
**Annane D et al., Lancet 2007; 370: 676-84

A. Jörres 10-2015
Summary for the Clinician
• Sepsis can initiate a deleterious cascade of:
– impaired microcirculation,
– activation of inflammatory pathways,
– tubular cell injury or death,
resulting in impaired kidney function and the initiation of a repair response.
• The assumption that renal perfusion pressure essentially equals MAP is
probably not valid in the clinical scenario of sepsis with severe capillary
leak and aggressive fluid resuscitation.
• Both venous congestion due to elevated right atrial/central venous pressure
and sepsis-induced capillary leak with consecutive tissue oedema may lead
to increased renal venous pressure and associated reduction in the
glomerular filtration gradient.

A. Jörres 10-2015
Summary for the Clinician
• Initial treatment must aim at rapid restoration of (systemic and renal)
circulation
– fluid resuscitation (cristalloids)
– vasopressor therapy (+ inotropes if required)
• Conservative treatment must then aim at
– optimising fluid status; avoid fluid overload (monitor fluid intake and
output; assess daily body weight if feasible)
– correcting metabolic/electrolyte abnormalities
– avoiding nephrotoxins
• There is currently no established specific pharmacotherapy for
prevention/treatment of septic AKI