Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 64 ■ July 201676
Pernicious Anaemia with Gastric CarcinoidsShaik Jani Basha1, NR Shetty2, Harshad Devarbhavi3
AbstractWe report the case of a 42 year male with history of chronic anaemia who was found to have pernicious anaemia with beta thalassemia trait and had on esophago-gastric-duodenoscopy, gastric carcinoids with gastric atrophy. Pernicious anaemia and gastric carcinoids occurring simultaneously in a single individual is rare. Our case emphasises the need for esophago-gastric-duodenoscopy in cases of pernicious anaemia.
Introduction
Bo t h p e r n i c i o u s a n a e m i a a n d g a s t r i c c a r c i n o i d s o c c u r r i n g
simultaneously in a single individual is rare. Our case is probably the first one from India.
Case Report
A 42 year male presented with progress ive symptoms of fa t igue of 6 months duration. He gave no history of any other symptom including hematemesis or malena. His past history was signif icant for severe anaemia (Hb-2.9) 5 yrs ago for which he had received blood transfusions. In the intervening period he was apparently well. Six months before admission he was operated for deep vein thrombosis (details were not available). Physical examination and systemic examination was unremarkable except for pallor.
Laboratory investigations showed the following: haemoglobin – 4.6 gm/dl (13-16 gm/dl), white blood cells– 6,500/µL (4000-11000/µL), platelet count – 172,000/µL (150,000-400,000/ µL), serum ferritin- 234.67 ng/ml (12-300 ng/mL), iron– 136.6 ug/dl (65 to 176 µg/dL), total iron binding capacity– 250.3 ug/dl (240–450 µg/dL), unsaturated iron binding capacity– 113.7 ug/dl (150-375 ug/dl), vitamin B12- 63.27pg/dl (200-900 pg/dl), serum folate - 15.49 ng/dl (3.6-20 ng/dl).
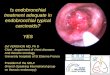
Peripheral smear (Figure 1) showed marked anisopoik i locytos i s wi th admixture of microcytic hypochromic r e d c e l l s , m a c r o c y t e s i n c l u d i n g macroovalocytes and hypersegmented polymorphs. He underwent esophago-gastric-duodenoscopy for cause of anaemia which showed multiple tiny
the incidence of pernicious anaemia in Indian population although it is 354 per 1,00,000 population in South-western Amer ican Indians . 3 I t i s known that patients with pernicious anaemia have a higher risk to develop gastrointestinal malignancies such as gastric adenocarcinoma, carcinoid tumours, or oesophageal squamous cell carcinoma.4 Our case was one such, with concomitant pernicious anemia and gastric carcinoids.
As the gastric nodules were small (~5mm) endoscopic resect ion was not recommended. Instead regular surveillance was planned. Our patient also appeared to have type I gastric carcinoid which is characterized by the triad of hypergastrinemia, the presence of anti-parietal cell antibodies and macrocytic anaemia. The other two types are as follows: type II develops in patients with combined Multiple Endocrine Neoplasia type 1 and the Zollinger–Ellison syndrome, and type I I I i s sporadic . 5 The incidence of metastases is less than 5%.6 Another c o n c e r n i s t h e d e v e l o p m e n t o f concomitant gastric adenocarcinoma, which was reported to occur in up to 6% of patients with type 1 gastric carcinoid tumours.7 Therefore regular annual endoscopic examination was recommended to our patient . The American Society for Gastrointestinal Endoscopy recommends a s ing le endoscopic evaluation at the diagnosis of pernicious anaemia.8 This is largely to conf irm gastr i t i s and rule out gastric carcinoid and other gastric cancers, since patients with pernicious anaemia are at increased risk for such cancers and to ensure that no single lesion is enlarging. Gastric resection is recommended for any large lesions >1.5 to 2 cm or lesions that have deeply penetrated the stomach wall into the submucosa or muscularis.9 Antrectomy which leads to the disappearance of hyperplastic G-cells, is sufficient to reduce circulating gastrin to a level
1Resident, 2Consultant, Dept of General Medicine, 3Consultant, Dept of Gastroenterology, Kokilaben Dhirubhai Ambani Hospital and Research Centre, Mumbai, MaharashtraReceived: 30.09.2014; Accepted: 10.06.2015
nodules (~5 mm) with summit erosions suggestive of gastric carcinoids (Figure 2). Gastric mucosa was also remarkable for prominent sub-epithelial vessels suggestive of gastric atrophy (Figure 3). Endoscopic gastric nodule biopsies obtained showed enterochromaffin-like cell hyperplasia which was positive for chromogranin and synaptophysin (Figures 4 and 5) thereby confirming gastric carcinoids or neuroendocrine tumour.
He underwent further investigations including anti parietal cell antibody and anti- intrinsic factor antibody which were both posi t ive . Serum chromogranin A levels were 227.5 mg/ml (36.4 µg/L). Serum gastrin level was 1597 pg/ml (0-200 pg/ml). Intrinsic Factor Blocking Ant ibody ( IFBA) was 15.3 (equivocal). Haemoglobin electrophoresis was suggestive of beta thalassemia Trait and HbA2 was 5.6% (1.5-3.1%).
A diagnosis of severe vitamin B12 deficiency secondary to pernicious a n a e m i a w i t h a t r o p h i c g a s t r i t i s and gastric carcinoid was made. he was treated with daily injection of methylcobalamin 1 mg intramuscular for a week followed by weekly injection for a month and then monthly injection.
Discussion
Pe r n i c i o u s a n a e m i a 1 i s a r a r e autoimmune disorder which is common in African or European population2 but rare in the Indian population. There is no clear data available regarding

Journal of The Association of Physicians of India ■ Vol. 64 ■ July 2016 77
Fig. 1: Peripheral smear H and E stain: hypersegmented polymorphs
Fig. 3: OGD scopy shows thin sub-epithelial blood vessels suggestive of atrophic gastritis
Fig. 4: Synaptophysin positive enterochromaffin-like cell hyperplasia
Fig. 5: Chromogranin A positive enterochromaffin-like cell hyperplasia
Fig. 2: Gastric nodule of 6 mm size with erosions at its summit suggestive of gastric carcinoid
that does not promote signif icant ECL cell hyperplasia, thus leading to carcinoid regression and inhibiting additional carcinoid formation.10,11 If carcinoid tumours do not regress after an antrectomy, additional monitoring is necessary and a total gastrectomy should be considered. Co-incidentally our patient had thalassemia trait along with pernicious anaemia.
In our case response to administered vitamin B12 was sat isfactory and
without further blood transfusion his haemoglobin rose to 12.3 gm/dl. Given the discrete nature of the gastric nodules, an endoscopic submucosal resection may be considered if the sizes increase to >1.5 or 2 cm.Conclusion
We emphasise the need for screening upper GI endoscopy in all patients of pernicious anaemia to rule out underlying gastric pathology.
References1. Stabler SP, Allen RH. Vitamin B12 deficiency as a worldwide
problem. Annu Rev Nutr 2004; 24:299-326.
2. Wun Chan JC, Yu Liu HS, Sang Kho BC et al. Pernicious anaemia in Chinese: a study of 181 patients in a Hong Kong hospital. Medicine (Baltimore) 2006; 85:129-38.
3. Sievers ML, Metzger AL, Goldberg LS, Fudenberg HH. Pernicious anemia in southwestern American Indians. Blood 1973; 41:309–17.
4. Toh BH, Chan J, Kyaw T, Alderuccio F. Cutting edge issues in autoimmune gastritis. Clin Rev Allergy Immunol 2012; 42:269-78.
5. Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E. Three subtypes of gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma: a clinicopathologic study. Gastroenterology 1993; 104:994-1006 Web of Science.
6. Dakin GF, Warner RR, Pomp A, et al. Presentation, treatment, and outcome of type 1 gastric carcinoid tumours. J Surg Oncol 2006; 93:368–372.
7. Gladdy RA, Strong VE, Coit D et al. Defining surgical indications for type I gastric carcinoid tumour. Ann Surg Oncol 2009; 16:3154–3160.
8. Hirota WK, Zuckerman MJ, Adler DG et al. ASGE guideline: the role of endoscopy in the surveillance of premalignant conditions of the upper GI tract. Gastrointest Endosc 2006; 63:570-80.
9. Olivia Y. Hung and Shishir K. Maithel. Hypergastrinemia, Type 1 Gastric Carcinoid Tumors: Diagnosis and Management. Journal of Clinical Oncology 2011; 29:e713-e715.
10. Ozao-Choy J, Buch K, Strauchen JA, et al. Laparoscopic antrectomy for the treatment of type I gastric carcinoid tumours. J Surg Res 2010; 162:22–25.