Embed Size (px)
Citation preview
Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1006
Bronchial Carcinoids
BY
DAN GRANBERG
ACTA UNIVERSITATIS UPSALIENSISUPPSALA 2001

Dissertation for the Degree of Doctor of Philosopy (Faculty of Medicine) in Medicinepresented at Uppsala University in 2001
ABSTRACT
Granberg, D. Bronchial Carcinoids. Acta Universitatis Upsaliensis. ComprehensiveSummaries of Uppsala Dissertations from the Faculty of Medicine 1006. 75 pp.Uppsala. ISBN 91-554-4957-3.
Bronchial carcinois are subdivided into typical and atypical. Atypical carcinoids are more malig-nant, but typical carcinoids may also influence survival. In the present study immunohistochemistrywas performed to identify prognostic markers in patients with typical bronchial carcinoids. Thediagnostic efficacy of octreoscan was evaluated, in comparison with CT and bone scan, and finallyour experience of treating patients with metastatic bronchial carcinoids is reported.
In an unselected material of 43 patients with typical bronchial carcinoids, metastatic disease wasfound in 12 patients (28%). Five patients (12%) developed distant metastases and died from theirdisease. High Ki-67 index, as well as positive staining for bcl-2 or p53 was associated with de-creased survival time. Positive staining for CD44s, v7-8 and v9, as well as positive nuclear stai-ning for nm23 correlated to decreased mortality. Staining for CD44 and Ki-67 should be performedroutinely for prognostic evaluation in these patients.
Octreoscan positive tumors were found in altogether 20/28 patients (71%). The primary tumorwas detectable in 81% and intrathoracic metastases in 78% of the patients on octreoscan; the corres-ponding figures for CT were 94% and 89% respectively. Liver metastases, as shown by CT, weredemonstable by octreoscan in 64% of patients. Octreoscan showed 70% and bone scan 90%sensitivity for identification of bone metastases.
Plasma chromogranin A was elevated in 28/30 patients (94 %) with metastatic bronchial carcinoidsand was the most sensitive tumor marker. Increased urinary 5’HIAA was found in 68%.
Biotherapy with α-interferon and Octreotide relieved carcinoid syndrome in 7/16 patients.However, only 4/27 patients showed stable disease during median 15 months, while 23 patientsprogressed. Treatment with cisplatinum + etoposide resulted in an objective response or stable dise-ase for 6–8 months in 3/8 patients with widespread tumors. Doxorubicin combined with strepto-zotocin or paclitaxel was associated with stable disease for 9 months in 2/2 patients each. All 7patients treated with streptozotocin+5-FU progressed.
Among the 43 unselected typical bronchial carcinoid patients, 5-year and 10-year survival was95% and 91%, respectively. The prognosis in patients with bronchial carcinoids showing distantmetastases was poor: 5-year survival was 70% from diagnosis and 22% from treatment start.
Key Words: Bronchial carcinoids, immunohistochemistry, prognostic markers, diagnosis,octreoscan, circulating hormones, treatment.
Dan Granberg, Department of Medicical Sciences, Uppsala University, SE-751 85Uppsala, Sweden
© Dan Granberg 2001
ISSN 0282-7476ISBN 91-554-4957-3
Printed in Sweden by Uppsala University, Tryck & Medier, Uppsala 2001
To my mother, who wanted me to make a discovery about cancerand
To my father, who has always wished to witness this momentand
To my beloved children
This thesis is based on the following papers which will be referred to in the text
by their roman numerals.
I. Granberg D, Wilander E, Öberg K, Skogseid B.
Prognostic markers in patients with typical bronchial carcinoid tumors.
Journal of Clinical Endocrinolology and Metabolism 2000;85(9):3425-3430
II. Granberg D, Wilander E, Öberg K, Skogseid B.
Decreased survival in patients with CD44-negative typical bronchial
carcinoid tumors.
International Journal of Cancer 1999;84:484–488.
III. Granberg D, Sundin A, Tiensuu Janson E, Öberg K, Skogseid B, Westlin J-E.
Octreoscan in patients with bronchial carcinoid tumors.
Submitted
IV. Granberg D, Eriksson B, Wilander E, Grimfjärd P, Fjällskog M-L, Öberg
K, Skogseid B.
Experience in treatment of metastatic bronchial carcinoid tumors.
Submitted
CONTENTS
Abbreviations 6
Introduction 7
Aims of the study 21
Patients 22
Methods 24
Results and comments 30
Clinical management 48
General summary 50
Acknowledgements 52
References 55
5
ABBREVIATIONS
ACTH Adrenocorticotropic hormonebax bcl-2-associated X proteinbcl-2 B-cell lymphoma/leukaemia-2 gene proteinCD44s Adhesion molecule CD44, standard (hematopoietic) formCD44v Adhesion molecule CD44, splice variantCEA Carcinoembryonic antigenc-erbB-2 c-erbB-2 = HER-2/neu oncoproteinCRF Corticotropin releasing factorCT Computerized tomography5-FU 5-FluorouracilGRP Gastrin releasing peptidehCGα Human chorionic gonadotropin subunit αhCGβ Human chorionic gonadotropin subunit β5’HIAA 5-hydroxy-indole-acetic acidKi-67 MIB-1 antibody against a nuclear antigen in proliferating cellsLCNC Large Cell Neuroendocrine CarcinomaLOH Loss of heterozygosityMeImAA Tele-methyl-imidazole-acetic acidMEN 1 Multiple endocrine neoplasia type 1MRI Magnetic resonance imagingnm23 Nonmetastatic protein 23/Nucleoside diphosphate kinaseNSE Neuron-specific enolasePP Pancreatic polypeptiderb Retinoblastoma proteinSCLC Small Cell Lung CarcinomaSPECT Single Photon Emission Tomography
6
INTRODUCTION
Neuroendocrine cells are widely distributed in various organs in the body, inclu-
ding the entire gastrointestinal tract and the lungs. The presence of neuro-
endocrine cells in the lungs was first described by Frölich in 1949 (Frölich, 1949)
and confirmed by Feyrter in 1954 (Feyrter, 1954). These cells, which are
argyrophilic (Tateishi, 1973), occur both as solitary cells and as clusters, termed
neuroepithelial bodies (Gould et al., 1983; Lauweryns and Peuskens, 1972).
Positive staining for NSE, serotonin, GRP/bombesin and calcitonin can be
detected both in solitary cells and neuroepithelial bodies, while leucine-
enkephaline is only found in solitary cells (Cutz et al., 1981; Gould et al., 1983;
Tsutsumi et al., 1983; Tsutsumi et al., 1983). In addition, hCGα-positive cells
have been demonstrated in normal bronchial epithelium (Fukayama et al., 1986)
and ACTH-immunoreactive cells in bronchiectasias (Tsutsumi et al., 1983).
Neuroendocrine cells are more frequent in fetal than in adult lungs, and may
proliferate in hypoxia and as response to irritants (Gould et al., 1983). The
number of neuroendocrine cells may increase in the airways of patients with
bronchiectasia (Gould et al., 1983; Memoli et al., 1983).
Neuroendocrine cells in the lungs are thought to be the origin of neuroendocrine
pulmonary neoplasias (Bensch et al., 1968; Bensch et al., 1965; Gould and
Linnoila, 1982; McDowell et al., 1976). Neuroendocrine lung tumors were
earlier subdivided into typical and atypical carcinoids (Arrigoni et al., 1972) and
small cell lung carcinomas, but several other classifications have later been
proposed (Capella et al., 1994; Paladugu et al., 1985; Travis et al., 1991; Warren
7
et al., 1985), and a fourth category, termed Large Cell Neuroendocrine
Carcinomas, has been defined (Travis et al., 1991). Between 81% and 88% of all
bronchial carcinoids are typical, while 12–19% are atypical (Ferguson et al.,
2000; Okike et al., 1976; Soga and Yakuwa, 1999).
Epidemiology
Bronchial carcinoids belong to the foregut neuroendocrine neoplasms (Williams
and Sandler, 1963), constituting 21–25% of all carcinoids (Modlin and Sandor,
1997; Soga and Yakuwa, 1999). They are rare tumors, accounting for 1–2% of
all lung tumors. Age-adjusted incidence is about 0.2:100 000. All ages are affec-
ted, even children, although the peak incidence is around 50 years. The disease is
slightly more common in women than in men (55% vs. 45%), and occurs more
often in whites than in blacks (Godwin, 1975). Although patients with multiple
endocrine neoplasia type 1 (MEN 1) have an increased risk, the etiology of
carcinoid is otherwise unknown. Smoking has not been recognized as a risk
factor.
Gross appearance
Bronchial carcinoids may be located centrally or peripherally. Central tumors are
usually cherry-red, vascular intrabronchial tumors, while peripheral tumors often
lack detectable origin from a bronchus. Both central and peripheral tumors fre-
quently infiltrate the surrounding lung parenchyma (Colby, 1994; Fraser et al.,
1989; Spencer, 1985). Between 5 and 20% of patients with typical carcinoids
develop metastases, while up to 70% of atypical carcinoid tumors metastasize
(Arrigoni et al., 1972; Colby, 1994; Okike et al., 1976). Metastases usually occur
8

to regional lymph nodes, but also distantly to the liver, bones, brain,
subcutaneous tissue or mammary glands. Metastases may be detected late,
several years or even decades after the initial diagnosis (Mokuno et al., 1999).
Microscopy
Bronchial carcinoids are epithelial in origin, reflected by their positivity for
cytokeratin (Bonato et al., 1992). Most tumors are argyrophilic; 100% of typical
and 86% of atypical carcinoids stain positive with Grimelius’ silver stain (Bonato
et al., 1992). Sevier-Munger’s silver stain may also be positive, but Masson’s
argentaffin stain is usually negative.
On light microscopy, bronchial carcinoids consist of small, polyhedral cells with
small, round or oval nuclei. The arrangement of the cells is regular and consists
of ribbons, nests, sheets, or spindling structures, separated by a fibrovascular
stroma. Typical carcinoids may contain amyloid material (Colby, 1994; Fraser et
al., 1989; Spencer, 1985). A spindle-cell variant exists (Ranchod and Levine,
1980). Necroses are only seen in atypical carcinoids (Arrigoni et al., 1972; Travis
et al., 1998). The proliferation rate is low. Staining with Ki-67 (MIB-1), which
recognizes a nuclear antigen in proliferating cells (Gerdes et al., 1983), yields
positive staining of 0.2–1.1% of the nuclei in typical and of 0.3–20.3% of the
nuclei in atypical carcinoids (Böhm et al., 1996). Electron microscopy of typical
carcinoids shows numerous neurosecretory granules varying in size from 90 to
450 nm, while atypical carcinoids contain fewer, diffusely distributed, secretory
granules between 100 and 200 nm in size (Travis et al., 1991; Warren et al.,
1984). Recently, the following criteria for atypical carcinoids (Travis et al., 1998)
9
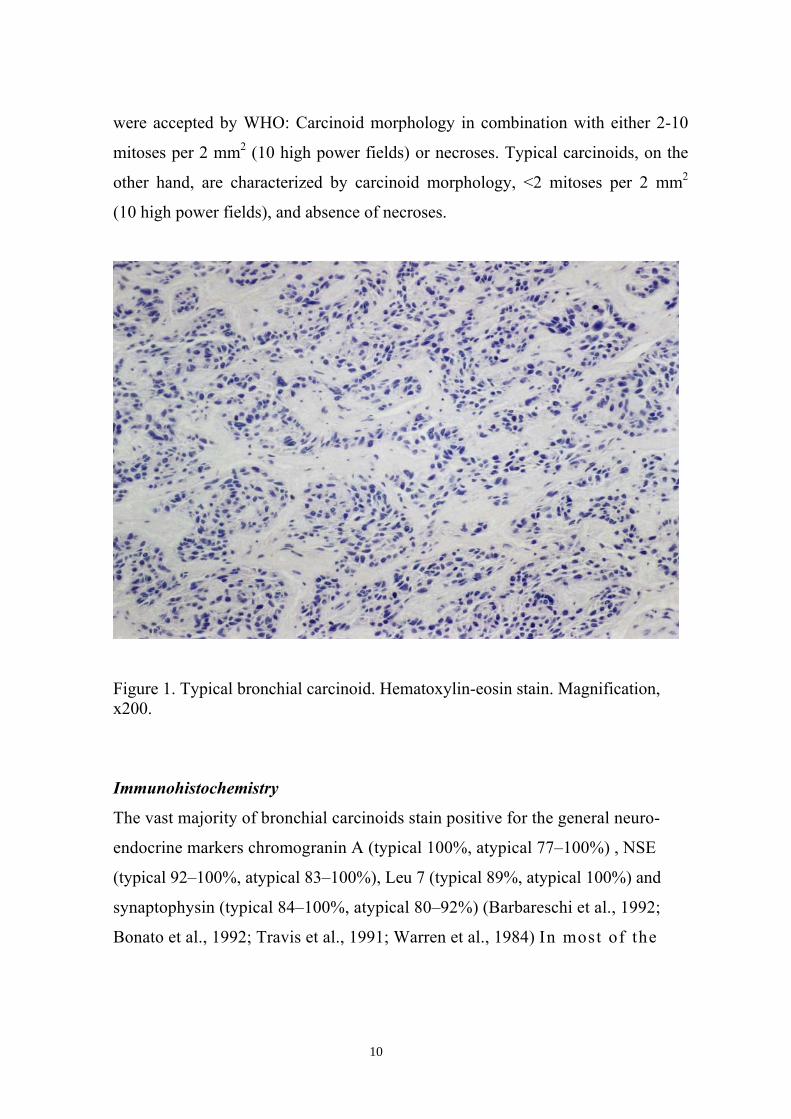
were accepted by WHO: Carcinoid morphology in combination with either 2-10
mitoses per 2 mm2 (10 high power fields) or necroses. Typical carcinoids, on the
other hand, are characterized by carcinoid morphology, <2 mitoses per 2 mm2
(10 high power fields), and absence of necroses.
Figure 1. Typical bronchial carcinoid. Hematoxylin-eosin stain. Magnification,x200.
Immunohistochemistry
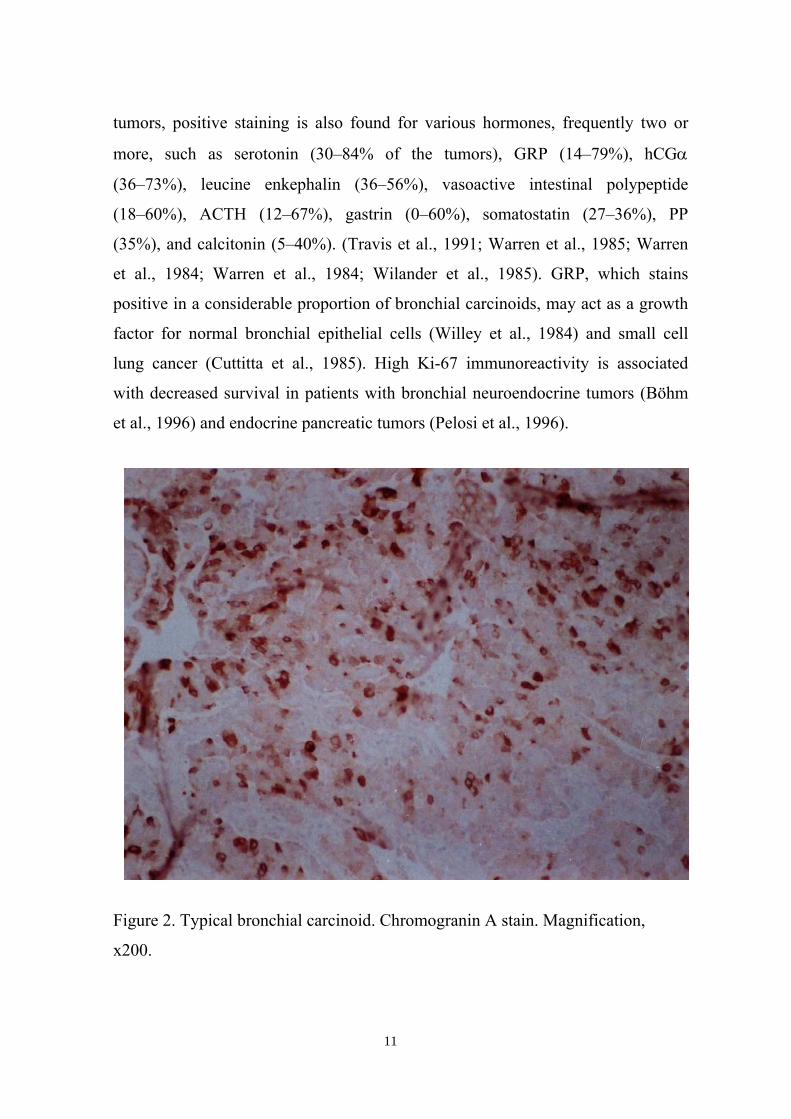
The vast majority of bronchial carcinoids stain positive for the general neuro-
endocrine markers chromogranin A (typical 100%, atypical 77–100%) , NSE
(typical 92–100%, atypical 83–100%), Leu 7 (typical 89%, atypical 100%) and
synaptophysin (typical 84–100%, atypical 80–92%) (Barbareschi et al., 1992;
Bonato et al., 1992; Travis et al., 1991; Warren et al., 1984) In most of the
10
tumors, positive staining is also found for various hormones, frequently two or
more, such as serotonin (30–84% of the tumors), GRP (14–79%), hCGα
(36–73%), leucine enkephalin (36–56%), vasoactive intestinal polypeptide
(18–60%), ACTH (12–67%), gastrin (0–60%), somatostatin (27–36%), PP
(35%), and calcitonin (5–40%). (Travis et al., 1991; Warren et al., 1985; Warren
et al., 1984; Warren et al., 1984; Wilander et al., 1985). GRP, which stains
positive in a considerable proportion of bronchial carcinoids, may act as a growth
factor for normal bronchial epithelial cells (Willey et al., 1984) and small cell
lung cancer (Cuttitta et al., 1985). High Ki-67 immunoreactivity is associated
with decreased survival in patients with bronchial neuroendocrine tumors (Böhm
et al., 1996) and endocrine pancreatic tumors (Pelosi et al., 1996).
Figure 2. Typical bronchial carcinoid. Chromogranin A stain. Magnification,
x200.
11
CD44The adhesion molecule CD44 is a glycoprotein existing in several isoforms. The
gene is localized on chromosome 11p13 close to a region causing suppression of
metastasis in prostatic cancer (Günthert, 1993; Ichikawa et al., 1992) and consists
of 20 exons (Screaton et al., 1993; Screaton et al., 1992). The 5 N-terminal exons
(exons 1-5) plus the 5 C-terminal exons (exons 16-20) encode the standard or
hematopoietic form (CD44s) which is a receptor for hyaluronan (Aruffo et al.,
1990) and is highly expressed on human lymphocytes. Several ”splice variants”
(v1–v10) exist, in which one or more epitopes encoded by the variant exons 6–15
are inserted into the extracellular portion close to the trans-membrane domain
(Günthert, 1993). CD44 is highly expressed in normal bronchial epithelium and
squamous cell lung cancers, as well as in a majority of bronchial carcinoid
tumors, while small cell lung cancers have only weak or absent expression
(Coppola et al., 1996; Givehchian et al., 1996; Mackay et al., 1994). Expression
of the standard or variant isoforms of CD44, especially variant 6 (v6) has been
coupled to more malignant tumor differentiation or worse prognosis in gastric
cancer (Mayer et al., 1993), colorectal cancer (Mulder et al., 1994; Wielenga et
al., 1993), renal cancer (Terpe et al., 1996) and non-Hodgkin lymphomas
(Stauder et al., 1995; Terpe et al., 1994), while CD44s is associated with good
prognosis in patients with neuroblastoma (Christiansen et al., 1995; Combaret et
al., 1995; Terpe et al., 1995). One study reported shorter survival in patients with
breast cancer positive for CD44v3, v 5 or v6 (Kaufmann et al., 1995), while
others have not been able to detect any correlation between CD44 and survival in
breast cancer (Friedrichs et al., 1995; Joensuu et al., 1993).
12
Oncogenes, Tumor Suppressor Genes
Bcl-2, which suppresses apoptosis, is counteracted by bax which hetero-
dimerizes with bcl-2, thereby accelerating programmed cell death (Oltvai et al.,
1993). Expression of bcl-2 correlates to neuroendocrine differentiation in lung
cancer and is found in 90–94% of small cell lung carcinomas (Jiang et al., 1996;
Jiang et al., 1995). Although bcl-2 suppresses apoptosis, non-small-cell lung
cancers positive for bcl-2 have a better prognosis than negative ones (Fontanini
et al., 1995). Positive staining for bcl-2 is rare among typical bronchial carcinoid
tumors, but is more frequent in atypical carcinoids (Coppola et al., 1996;
Lohmann et al., 1993). Decreased survival has been reported in bronchial
carcinoids with overexpression of bcl-2 and downregulation of bax (Brambilla et
al., 1996).
Mutations in the tumor suppressor gene p53 are found in many different cancer
types. Accumulation of mutated p53 protein, which can be detected by positive
immunostaining, is frequently found in highly malignant neuroendocrine lung
tumors and in atypical carcinoids, but is rare among typical bronchial carcinoids
(Coppola et al., 1996; Lohmann et al., 1993). Altered structure and expression of
the retinoblastoma gene (rb), another tumor suppressor gene, is common in small
cell lung cancer, and inactivation of rb may have pathogenetic implications for
the malignant phenotype and neuroendocrine differentiation in lung tumors
(Barbareschi et al., 1992; Gouyer et al., 1994; Hensel et al., 1990). Rb is usually
expressed in typical carcinoids, but only occasionally in atypical ones
(Barbareschi et al., 1992; Dosaka-Akita et al., 2000; Gouyer et al., 1998).
Amplification of the oncogene c-erbB-2 has been coupled to relapse and poor
13
survival in breast cancer (Wright et al., 1989), whereas c-erbB-2 has been
reported to stain negative in bronchial carcinoids (Roncalli et al., 1991).
nm23 was first identified in 1988 as a candidate metastasis suppressor gene
(Steeg et al., 1988). The protein product of nm23 is a heterodimeric enzyme
which acts as a nucleoside diphosphate kinase (Biggs et al., 1990; Gilles et al.,
1991). Two nm23 genes exist, nm23-H1 and nm23-H2 (Stahl et al., 1991), each
coding for one of the enzyme’s two chains (Gilles et al., 1991). Higher expres-
sion of nm23 has been associated with decreased risk of metastases in breast
cancer (Tokunaga et al., 1993), colorectal cancer (Ayhan et al., 1993; Yamaguchi
et al., 1993) and hepatocellular cancer (Yamaguchi et al., 1994). This antimetas-
tatic effect is usually coupled to the H1 form. In contrast, no correlation has been
found between nm23 expression and metastases in neuroendocrine lung tumors
(Gazzeri et al., 1996) or pulmonary adenocarcinoma (Higashiyama et al., 1992).
Genetics
Aneuploidy is found in 5–32% of typical carcinoids and in 17–79% of atypical
carcinoids (El-Naggar et al., 1991; Jones et al., 1988; Thunnissen et al., 1988;
Travis et al., 1991). Both typical and atypical carcinoids frequently show
deletions of 11q, including the MEN 1 locus. One study found homozygous
somatic inactivation of the MEN 1 gene in 36% of sporadic bronchial carcinoids
(Debelenko et al., 1997) and in a recent study 36% of bronchial carcinoids
showed deletions in 11q, but none had loss of 18p or 18q (Zhao et al., 2000). In
addition, atypical carcinoids frequently have deletions on 10q and 13q (Walch et
al., 1998). Other authors reported LOH at the rb locus to be infrequent in
14
carcinoids (around 20%) compared to LCNC (62%) and SCLC (71%). There was
also an increasing incidence of LOH at 5q21 from typical carcinoids (0%) to
atypical carcinoids (25%), LCNC (46%) and SCLC (86%). LOH at 5q21
correlated to shorter survival among carcinoid patients (Onuki et al., 1999).
Symptoms
A substantial proportion (13–51%) of patients with bronchial carcinoids are
asymptomatic, and the tumor is detected on routine chest X-ray. Presenting
symptoms include cough, hemoptysis, dyspnea, wheezing, chest pain and
recurrent pulmonary infections (Bertelsen et al., 1985; Harpole et al., 1992;
McCaughan et al., 1985; Mendonça et al., 1997; Mårtensson et al., 1987; Okike
et al., 1976). The carcinoid syndrome with flushing, diarrhea, wheezing and
elevated urinary 5’HIAA is infrequent, occuring in 2–12% of the patients
(Dusmet and McKneally, 1996; Harpole et al., 1992; Soga and Yakuwa, 1999).
Liver metastases are detected in most patients displaying the carcinoid synd-
rome (Davila et al., 1993; Dusmet and McKneally, 1996; Ricci et al., 1973). An
atypical carcinoid syndrome depending on histamine secretion may occasionally
be detected in patients with bronchial carcinoids. These patients suffer from
severe generalized flushing, swelling, lacrimation, asthma and diarrhea. Ectopic
Cushing’s syndrome, due to secretion of ACTH or CRF, is seen in 2–6% of
bronchial carcinoid patients (Dusmet and McKneally, 1996; Soga and Yakuwa,
1999). Acromegaly, caused by tumor production of growth hormone releasing
hormone, is exceedingly rare in patients with bronchial carcinoids (Ezzat et al.,
1994; Huber et al., 1991).
15

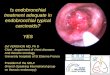
Figure 3. Bronchoscopy of a typical carcinoid in the right main bronchus
Diagnosis
More than 60% of the primary tumors are detectable on chest X-ray (Soga and
Yakuwa, 1999; Stefani et al., 1999). Peripheral tumors are visble as nodules,
while central tumors may be disclosed by a peripheral atelectasis or obstructive
pneumonia (Fraser et al., 1989). Computerized tomography or magnetic reso-
nance imaging is more sensitive, especially in detecting lymph node metatastases
(Ginsberg, 1994; Magid et al., 1989; Soga and Yakuwa, 1999). Up to 75% of the
central tumors are detectable by bronchoscopy (Ginsberg, 1994), Figure 3.
Despite a small risk for bleeding, it is usually safe to take biopsies (Chughtai et
al., 1997; Hurt and Bates, 1984). Plasma chromogranin A is a valuable tumor
marker in both midgut (O’Connor and Deftos, 1986) and gastric carcinoids
16

(Granberg et al., 1998), but its value in bronchial carcinoids has not been investi-
gated. Elevation of urinary 5HIAA or serotonin has been described in up to 25%
of patients with bronchial carcinoids (Harpole et al., 1992).
Treatment
The main treatment of bronchial carcinoids is surgery with removal of the
primary tumor and affected lymph nodes. Surgical procedures include pneumon-
ectomy, bilobectomy, lobectomy, segmentectomy, sleeve resection and wedge
resection. The aim is to remove the primary tumor and affected lymph nodes
radically, sparing as much lung parenchyma as possible (Chughtai et al., 1997;
Stamatis et al., 1990). Because of the risk of recurrence, extirpation by YAG
laser via bronchoscopy is not recommended except for patients with obstructive
symptoms unable to undergo radical surgery. Thoracic radiotherapy is some-
times administered when mediastinal lymph node metastaes are present; in
addition, radiotherapy is used to relieve pain in patients with bone metastases.
Chemotherapy with streptozotocin combined with cyclophosphamide or 5-FU
(Moertel and Hanley, 1979) or cisplatinum + etoposide (Moertel et al., 1991) has
been tried in patients with metastatic bronchial carcinoids, but the results are
poor. Octreotide may be of value for symptomatic relief of patients with the
carcinoid syndrome (Kvols, 1989). In case of carcinoid crisis, somatostatin
analogue treatment is life-saving .
17
Prognosis
The mortality rate varies between 0 and 8% for patients with typical carcinoids
(Padberg et al., 1996; Travis et al., 1991; Vadasz et al., 1993; Warren and Gould,
1990) and between 20 and 55% in patients with atypical carcinoids (Arrigoni et
al., 1972; Padberg et al., 1996; Valli et al., 1994). Patients with typical carcinoids
have 90-100% 5-year and 87-96% 10-year survival, while the 5- and 10-year
survival in patients with atypical carcinoids is only 40-72% and 35-60%� respec-
tively (Beasley et al., 2000; Chughtai et al., 1997; Ferguson et al., 2000; Garcia-
Yuste et al., 2000; Harpole et al., 1992; McCaughan et al., 1985; Rea et al., 1989;
Stamatis et al., 1990). Known adverse prognostic factors are atypical histology
(Arrigoni et al., 1972; McCaughan et al., 1985; Padberg et al., 1996; Travis et al.,
1998), lymph node metastases at diagnosis (El-Naggar et al., 1991; Jones et al.,
1988; McCaughan et al., 1985; Torre et al., 1989), presence of satellite lesions
(Chughtai et al., 1997), high proliferative activity assessed by staining with Ki-67
(Böhm et al., 1996), high mitotic rate (Beasley et al., 2000), high apoptotic index
(Laitinen et al., 2000) and elevation of urinary 5’HIAA or serum serotonin
(Harpole et al., 1992). The results of DNA aneuploidy and tumor size as
prognostic markers have been inconsistent (El-Naggar et al., 1991; Jones et al.,
1988; McCaughan et al., 1985; Padberg et al., 1996; Torre et al., 1989; Vadasz et
al., 1993). Positive immunostaining for CEA was a strong negative prognostic
factor in one study (Bishopric and Ordóñez, 1986).
18
111Indium labelled Octreotide
Somatostatin producing cells are widely distributed in the body. The peptide is
present in the central nervous system, in the pituitary gland, thyroid, adrenal
medulla, prostate, placenta, kidneys, in neuroendocrine cells in the gastro-
intestinal tract and in D-cells in the pancreas. Somatostatin has inhibitory effects
on the secretion of insulin and glucagon in the pancreatic islets (Koerker et al.,
1973), and on growth hormone secretion in the pituitary gland (Brazeau et al.,
1973). Somatostatin acts by specific G-protein coupled receptors, five of which
have so far been identified (Yamada et al., 1993; Yamada et al., 1992; Yamada et
al., 1992). For clinical use, more long-acting synthetic somatostatin analogues
are now available, such as octreotide and lanreotide.
Scintigraphy with 111Indium-labelled octreotide (octreoscan) is valuable for
diagnosis of neuroendocrine tumors. Octreoscan positive lesions can be found in
more than 90% of patients with midgut carcinoids (Kwekkeboom et al., 1993;
Kälkner et al., 1995; Shi et al., 1998), paragangliomas (Kwekkeboom et al.,
1993), and gastrinomas as well as 86% of pheochromocytomas are detectable on
octreoscan (Kwekkeboom and Krenning, 1997). Insulinomas are more rarely
(<50%) demonstrable by this method. Kälkner et.al. reported that 4/12 foregut
carcinoids could not be visualized on octreoscan (Kälkner et al., 1995) but in
another study 8/8 primary lung carcinoids were demonstrable (Musi et al., 1998).
The sensitivity for detection of liver metastases in neuroendocrine gastro-entero-
pancreatic tumors is about 90–100% (Chiti et al., 1998; Krausz et al., 1998;
Scherübl et al., 1993). In several case reports, octreoscan identified the primary
tumor in patients with occult ectopic Cushing’s syndrome (Carretta et al., 1997;
19
Mansi et al., 1997; Phlipponneau et al., 1994; Weiss et al., 1994). The value of
octreoscan in localizing small ACTH-producing bronchial carcinoids was
however questioned in two recent studies (Tabarin et al., 1999; Torpy et al.,
1999). In small cell lung cancer patients, octreoscan detects nearly all primary
tumors, but distant metastases are seen less frequently (Berenger et al., 1996;
O’Byrne et al., 1994; Reisinger et al., 1998). Other diseases that may be positive
on octreoscan include non-small-cell lung cancer (Lau et al., 2000), sarcoidosis
(Kwekkeboom et al., 1998), pneumonia (Castellani et al., 1999), malignant
lymphomas (Reubi et al., 1992) and Graves’ disease (Postema et al., 1994).
Octreoscan can be used to predict the response to treatment with somatostatin
analogues in patients with malignant midgut carcinoids (Tiensuu Janson et al.,
1994).
20
AIMS OF THE STUDY
The aims of the present study were to
• Find prognostic markers for patients with typical bronchial carcinoids
• Identify tumor markers in plasma or urine suitable for treatment monitoring
and early detection of recurrence
• Evaluate the effectiveness of octreotide scintigraphy for the diagnosis of
bronchial carcinoids and for identifying metastases
• Survey the treatment of patients with metastatic bronchial carcinoids at the
Department of Endocrine Oncology, University Hospital, Uppsala
21
PATIENTS
Paper I and II
All 43 patients admitted to our hospital between 1985 and 1995 whose pathology
specimens (paraffin blocks containing tumor tissue) fulfilled the criteria for
typical bronchial carcinoid (Figure 1) (Travis et al., 1998), were included. All
specimens showed less than 2 mitoses per 10 high power fields. Sixteen of the
patients were men and 27 were women. Their median age was 56 years (range
18-75). Median follow-up was 74 months (14–330) in paper I and 65 months
(14-325) in Paper II. The primary tumor was studied in 41 patients, while in one
patient only a brain metastasis and in another patient an intrathoracic lymph node
metastasis was available.
The carcinoid tumor diagnosis was made because of respiratory symptoms in 32
patients. Nine cases were found on routine chest X-ray and one patient was
operated on for a brain metastasis, that turned out to be derived from a typical
bronchial carcinoid. The last patient presented with ectopic Cushing’s syndrome.
Two patients had carcinoid syndrome at diagnosis, and two more patients
developed this syndrome when liver metastases were detectable 12 and 20 years
after primary surgery.
Altogether 12/43 patients (28%) displayed metastatic disease. Ten patients (23%)
had lymph node involvement at diagnosis (including one patient who recurred
locally 26 years after bronchoscopic extirpation of an intrabronchial carinoid),
and distant metastases have occurred in 5 patients (12%).
22
Surgical removal of the primary tumor and lymph node dissection was performed
in 42 patients, one of whom had undergone bronchoscopic extirpation of an
intrabronchial carcinoid 26 years earlier. In one patient surgery was denied
because of extensive intrathoracic tumor growth.
Paper III
All 28 patients referred for octreoscan at our hospital between 1992 and May
2000 who suffered from histologically verified bronchial carcinoids were
studied. One patient was subjected to octreoscan on 3 different occasions, while
the remaining 27 patients were examined once. Four patients had atypical and 24
patients had typical carcinoids (Travis et al., 1998). There were 13 men and 15
women. Their median age was 57 years (range 16–83). Carcinoid syndrome was
present in 9 patients and ectopic Cushings syndrome in 5; one of these patients
had both syndromes. The primary tumor had been surgically removed prior to the
octreoscan investigation in 12 patients. Altogether 22 patients harbored
metastatic disease: Intrathoracic recurrence or metastases (n=9), liver (n=14),
bones (n=10), breast, brain and abdominal lymph nodes (1 patient each). Five
patients were receiving treatment with octreotide.
Paper IV
All 31 patients (14 men and 17 women) treated at the Department of Endocrine
Oncology, University Hospital, Uppsala who harbored bronchial carcinoids with
distant metastases were included in this study. Four patients had atypical while
the remaining 27 had typical carcinoids (Travis et al., 1998). Their median age
23
was 60 years (15–84). Carcinoid syndrome was present in 16 patients, while 2
patients had ectopic Cushing’s syndrome. Metastases were present at the start of
treatment in 29 of the patients, while the remaining 2 developed metastases
during the observation period. Median follow-up from the start of treatment was
25 months (4–106). Surgery for the primary tumor had been performed in 22 of
the patients. In addition, 7 patients had been subjected to surgery of metastases in
the brain, ovaries, mammary glands or subcutaneous tissue.
METHODS
Immunohistochemistry
All specimens were stained with hematoxylin and eosin. Immunohistochemistry
was performed on all tumors in Papers I and II with the antibodies shown in
Table 1. In addition, 17 tumors of patients (15 with typical and 2 with atypical
carcinoids) in Paper IV were stained with bcl-2, CD44s, GRP, hCGα, Ki-67,
nm23, p53 and serotonin. The following procedure was used: Formalin-fixed and
paraffin-embedded blocks were cut in 4 µm sections. After deparaffinization and
rehydration of the sections, endogenous peroxidase was blocked with 0.3%
hydrogen peroxide for 30 min. For some of the antibodies, antigen unmasking
was performed by pretreatment according to Table 1. The slides were repeatedly
washed in phosphate saline buffer solution, pH 7.4 (PBS), whereafter horse or
goat serum diluted 1:5 in PBS was applied in order to avoid non-specific
secondary antibody binding. Primary antibody diluted in PBS was employed for
1.5 hours in room temperature or overnight at 4°C. Biotinylated horse anti-mouse
24
or goat anti-rabbit Ig, diluted 1:200, was used as secondary antibody and was
applied for 45 min. The reaction was visualized with an ’Elite’ kit (Vector
Laboratories, Burlingame, CA) with 0.006% hydrogen peroxide as substrate and
3-amino-9-ethyl-carbazole (Sigma Chemical Co., St Louis, MO) in dimethyl-
sulfoxide as chromogen. Finally, counterstaining of the slides was performed
with hematoxylin. A positive control was always included. All slides were
assessed by an experienced pathologist (E. Wilander) without knowledge about
the clinical data. The stainings of CD44 (standard form and splice variants) and
bax were graded as positive or negative. For Ki-67, the percentage of positive
cells was calculated. The remaining stainings were graded as follows: -, negative;
+, <10% positive cells; ++, 10-50% positive cells; +++, >50% positive cells. For
c-erbB-2 membranous staining, which correlates to gene amplification
(Gusterson et al., 1988) was re�quired for positivity.
Hormones
Plasma chromogranin A, plasma chromogranin B, serum PP, serum calcitonin,
serum hCGα and hCGβ were analyzed according to methods described earlier
(Almqvist et al., 1974; Hällgren et al., 1977; Stridsberg et al., 1993; Stridsberg et
al., 1995; Öberg and Wide, 1981). Urinary 5’HIAA was sampled on two conse-
cutive days and the mean value was calculated. Urinary MeImAA, the principal
metabolite of histamine, was collected for 24 hours and analyzed as described
earlier (Granerus et al., 1966).
25
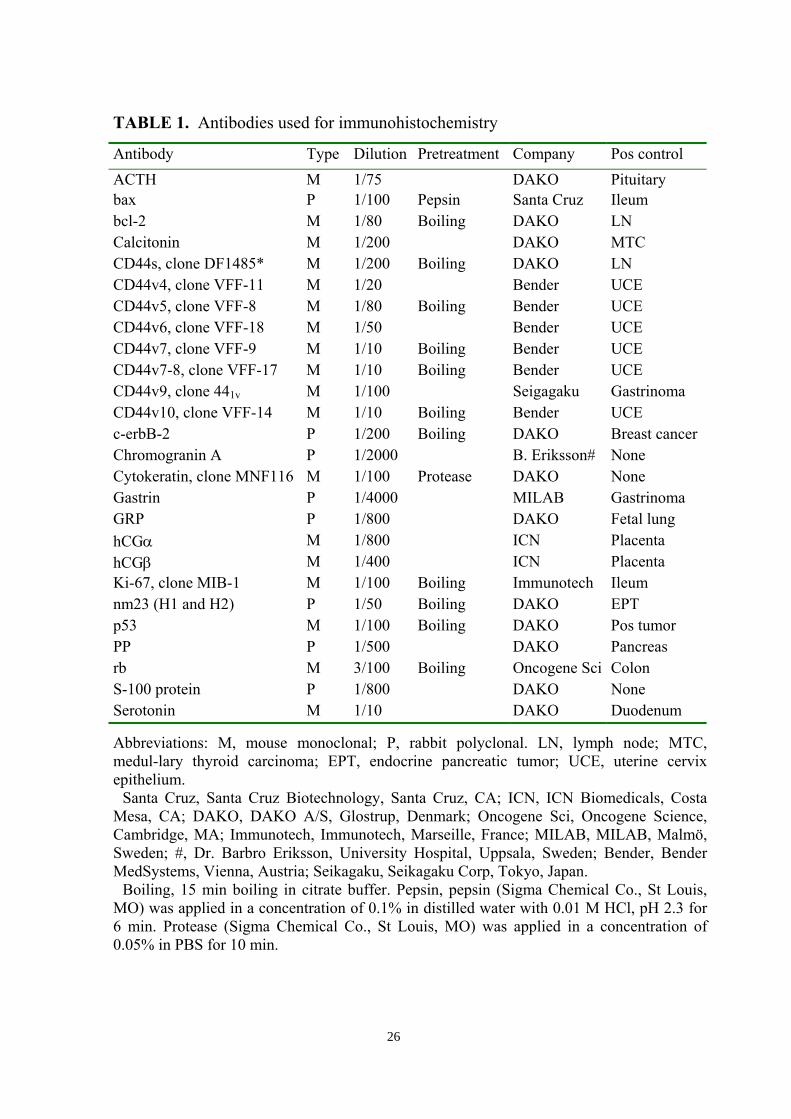
TABLE 1. Antibodies used for immunohistochemistry
Antibody Type Dilution Pretreatment Company Pos controlACTH M 1/75 DAKO Pituitarybax P 1/100 Pepsin Santa Cruz Ileumbcl-2 M 1/80 Boiling DAKO LNCalcitonin M 1/200 DAKO MTCCD44s, clone DF1485* M 1/200 Boiling DAKO LNCD44v4, clone VFF-11 M 1/20 Bender UCECD44v5, clone VFF-8 M 1/80 Boiling Bender UCECD44v6, clone VFF-18 M 1/50 Bender UCECD44v7, clone VFF-9 M 1/10 Boiling Bender UCECD44v7-8, clone VFF-17 M 1/10 Boiling Bender UCECD44v9, clone 441v M 1/100 Seigagaku GastrinomaCD44v10, clone VFF-14 M 1/10 Boiling Bender UCEc-erbB-2 P 1/200 Boiling DAKO Breast cancerChromogranin A P 1/2000 B. Eriksson# NoneCytokeratin, clone MNF116 M 1/100 Protease DAKO NoneGastrin P 1/4000 MILAB GastrinomaGRP P 1/800 DAKO Fetal lunghCGα M 1/800 ICN PlacentahCGβ M 1/400 ICN PlacentaKi-67, clone MIB-1 M 1/100 Boiling Immunotech Ileumnm23 (H1 and H2) P 1/50 Boiling DAKO EPTp53 M 1/100 Boiling DAKO Pos tumorPP P 1/500 DAKO Pancreasrb M 3/100 Boiling Oncogene Sci ColonS-100 protein P 1/800 DAKO NoneSerotonin M 1/10 DAKO Duodenum
Abbreviations: M, mouse monoclonal; P, rabbit polyclonal. LN, lymph node; MTC,medul-lary thyroid carcinoma; EPT, endocrine pancreatic tumor; UCE, uterine cervixepithelium.
Santa Cruz, Santa Cruz Biotechnology, Santa Cruz, CA; ICN, ICN Biomedicals, CostaMesa, CA; DAKO, DAKO A/S, Glostrup, Denmark; Oncogene Sci, Oncogene Science,Cambridge, MA; Immunotech, Immunotech, Marseille, France; MILAB, MILAB, Malmö,Sweden; #, Dr. Barbro Eriksson, University Hospital, Uppsala, Sweden; Bender, BenderMedSystems, Vienna, Austria; Seikagaku, Seikagaku Corp, Tokyo, Japan.
Boiling, 15 min boiling in citrate buffer. Pepsin, pepsin (Sigma Chemical Co., St Louis,MO) was applied in a concentration of 0.1% in distilled water with 0.01 M HCl, pH 2.3 for6 min. Protease (Sigma Chemical Co., St Louis, MO) was applied in a concentration of0.05% in PBS for 10 min.
26
OctreoscanScintigraphy was performed with 111In-DTPA-D-Phe1-octreotide delivered by
Mallinckrodt Medical, Petten, the Netherlands. The labelling procedure (Bakker
et al., 1991) was briefly as follows: 244 MBq of 111In-chloride was added to 20
µg lyophilized (DTPA-D-Phe1)-octreotide and incubated for 30 min at room
temperature. The labelling yield, which was checked by chromatography using
SEP-PAK (Bakker et al., 1990), always exceeded 97%. Each patient received an
intravenous bolus injection of 220 MBq of the 111In-pentetreotide solution. Planar
antero-posterior and lateral images covering the whole body with the exception
of the extremities were obtained after 24 hours. In addition, a single photon
emission tomography (SPECT) study was performed over the abdomen after 24
hours, using a gamma scintillation SPECT-camera delivered by Nuclear
Diagnostics, Hägersten, Sweden. To collect the original SPECT data, a 64 step
rotation of 360° in a 64x64 word matrix was used. For the reconstruction of
SPECT images, a Wiener filter was applied (Westlin et al., 1992). The results
were compared to intravenously contrast enhanced computerized tomography
(CT) for detection of primary tumors and soft tissue metastases, and to
conventional bone scan and plain X-ray or magnetic resonance imaging (MRI)
using the standard protocl for bone metastases. Octreoscan and CT were assesed
by different observers without knowledge of the results of the other examination.
Treatment schedules
Our first line treatment in patients with metastatic bronchial carcinoids has been
α-interferon in a dose of 9–42 (median 15) million units/week administered in 3
or 5 subcutaneous injections. The dose had been adjusted according to leukocyte
27
count and side effects. In cases of disabling carcinoid syndrome, α-interferon has
been combined with octreotide. When this treatment has failed, we have changed
to a combination of streptozotocin + 5-FU. If the tumor has continued to grow,
we have used cisplatinum + etoposide as third line therapy. Other regimens used
as third or fourth line treatment are streptozotocin + doxorubicin, α-interferon +
5-FU, paclitaxel and paclitaxel + doxorubicin. The chemotherapy schedules are
shown in Table 2. Liver embolization with gel-foam has been used as second or
third line therapy when the liver contained the majority of the tumor burden. A
few patients with advanced disease have received targeted radiotherapy with111In-Octreotide or 131I-MIBG. An objective response was defined as a ≥50%
decrease in radiological size (product of two perpendicular measures), and a
biochemical response was defined as a ≥50% decrease of at least one hormone
marker. A ≥25% increase in tumor size or the occurrence of new metastases was
regarded as progression, and a ≥25% increase of at least one hormone marker
was considered as biochemical progression. Time to progression was defined as
the time from start of the treatment to the first occasion when progression was
observed. Duration of response was defined as time from start of treatment to the
last occasion when disease was considered stable. Our intention was to monitor
the patients every third month.
28

TABLE 2. Chemotherapy regimens used
Drugs, doses Interval
cisplatinum 45 mg/m2 day 2–3 + etoposide 100 mg/m2 day 1–3 4 weeks
streptozotocin 2000 mg day 1 + 5-FU 400 mg/m2 day 1 3 weeks
streptozotocin 2000 mg day 1 + doxorubicin 40 mg/m2 day 1 3 weeks
paclitaxel 150 mg/m2 day 1 + doxorubicin 40 mg/m2 day 1 3 weeks
paclitaxel 175 mg/m2 day 1 3 weeks
α-interferon 9–25 million units/week+ 5-FU 500 mg/m2 day 1–3 4 weeks
Statistics
The median and range were used as measures of central tendency and variation,
respectively. When calculating the statistics, comparison was made only between
positive and negative staining, except for Ki-67. Correlation between antibody
expression and metastasis or mortality was analyzed by the χ2 test or (for Ki-67)
the Mann-Whitney U test. Survival time was calculated by Kaplan-Meier
cumulative survival plot and Mantel-Cox logrank test except for Ki-67, where
Cox proportional Hazards was applied. p<0.05 was considered significant. A
patient who died from an unrelated cause (paper I and II) was omitted from the
survival calculations.
29
RESULTS AND COMMENTS
Proliferation
Figure 3. The results for Ki-67 are shown in tables 3, 4 and 5. Among the 43
patients in Paper I and II, Ki-67 did not correlate to the incidence of distant
metastases (p=0.2), or to metatstatic disease (p=0.4), although higher Ki-67 index
was associated with decreased survival time (p<0.01). If, however, the 15
additional immunostained typical carcinoids from Paper IV were included in the
analysis, Ki-67 correlated both to distant metastases (p<0.001), metastatic
disease (p<0.01), mortality and shorter survival time (p<0.01). This more
comprehensive patient material encompasses a higher number of metastatic
typical carcinoid tumors. Similar results were reported by Böhm et.al.: No
correlation was found between Ki-67 and survival for typical carcinoids, but
when patients with atypical carcinoids (well differentiated neuroendocrine
carcinomas) and SCLC were included, the difference was significant (Böhm et
al., 1996). Analysis of Ki-67 expression adds prognostic information in patients
with neuoendocrine lung tumors and should be performed routinely.
Immunohistochemistry
The results of the immunohistochemical stainings for the individual patients are
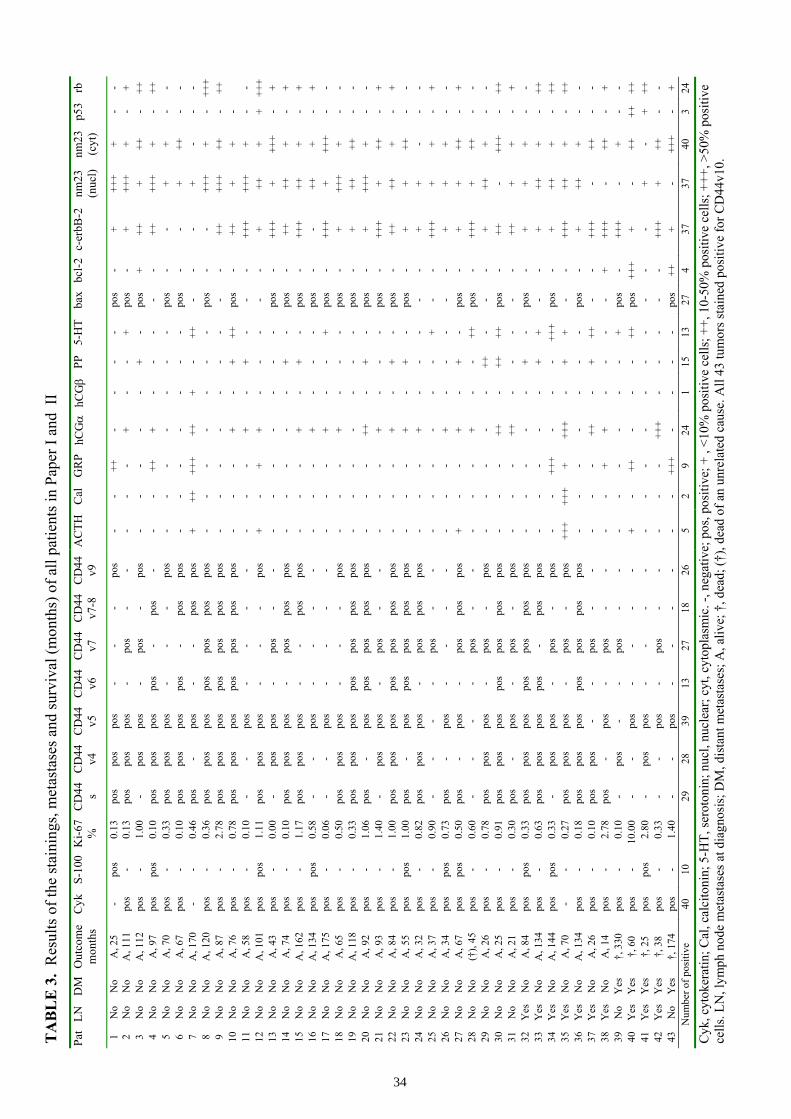
summarized in Tables 3 and 4 and the correlations are shown in Table 5. All 43
tumors in Paper I and II stained positive for chromogranin A (Figure 2). Cyto-
keratin was positive in 40 tumors, confirming their epithelial origin, and S-100
protein in 10. S-100 showed no correlation to metastases or survival. Positive
staining for mutiple hormones was common, although only a few patients
30
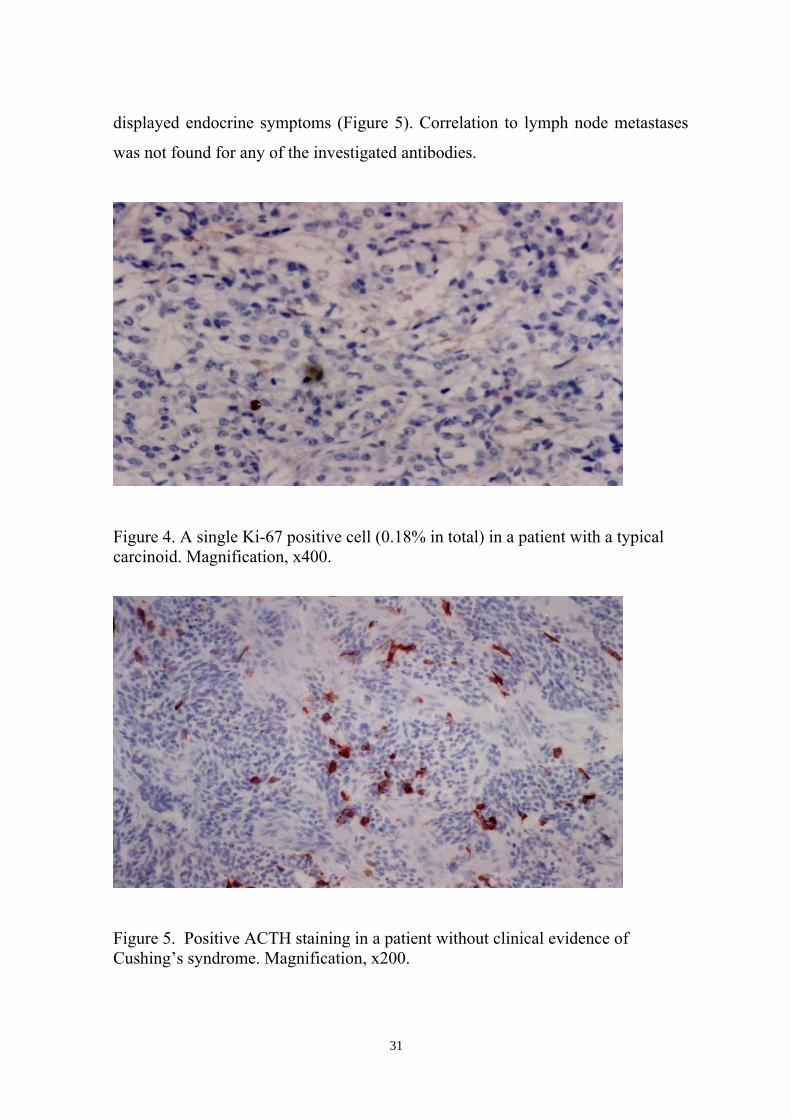
displayed endocrine symptoms (Figure 5). Correlation to lymph node metastases
was not found for any of the investigated antibodies.
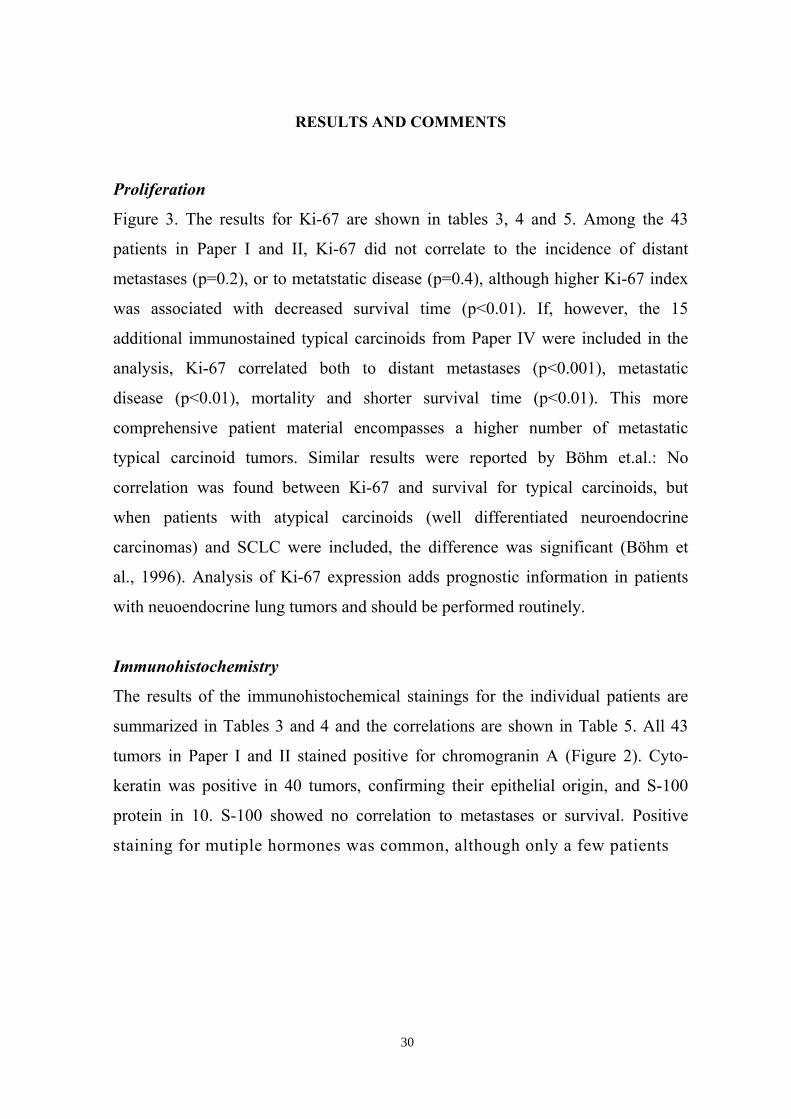
Figure 4. A single Ki-67 positive cell (0.18% in total) in a patient with a typicalcarcinoid. Magnification, x400.
Figure 5. Positive ACTH staining in a patient without clinical evidence ofCushing’s syndrome. Magnification, x200.
31
Positive staining for the CD44 isoforms CD44s (Figure 6), v9 and v7-8 (Paper I
and II) correlated to decreased incidence of distant metastases and mortality
(p<0.001, p<0.01 and p=0.04 for the respective CD44 isoforms). This is consis-
tent with earlier observations that normal bronchial epithelium shows high
expression of CD44s and v5, v6, v9 while SCLC tumors have weaker or no
expression (Givehchian et al., 1996), and that CD44s and v6 are correlated to
more aggressive variants of neuroendocrine lung tumors (Coppola et al., 1996).
If the 15 immunostained typical carcinoids from Paper IV were included,
positive staining for CD44s still correlated to decreased risk for distant
metastases and death (p<0.0001). In addition, correlation was now reached to
metastatic disease (p<0.001). Thus, by increasing the number of observations
and the proportion of patients harboring distant metastases, the findings from
paper I and II were strengthened. CD44 expression did not correlate to lymph
node metastases, which is the predilective metastatic site. We conclude that
immunostaining with CD44s may give useful prognostic information in patients
with bronchial carcinoids and should be performed routinely. It is unclear if the
absence of CD44 expression has a causative role in the metastatic process or
merely accompanies poor differentiation. Several theories exist as to how CD44
can inhibit metastasis. One posiible mechanism is to promote adhesion between
tumor cells or between tumor cells and the basement membrane (Fujita et al.,
1994). Another theory is that CD44 mediates adhesion of tumor cells to hyalu-
ronic acid molecules in the intercellular matrix (Penno et al., 1994).
32
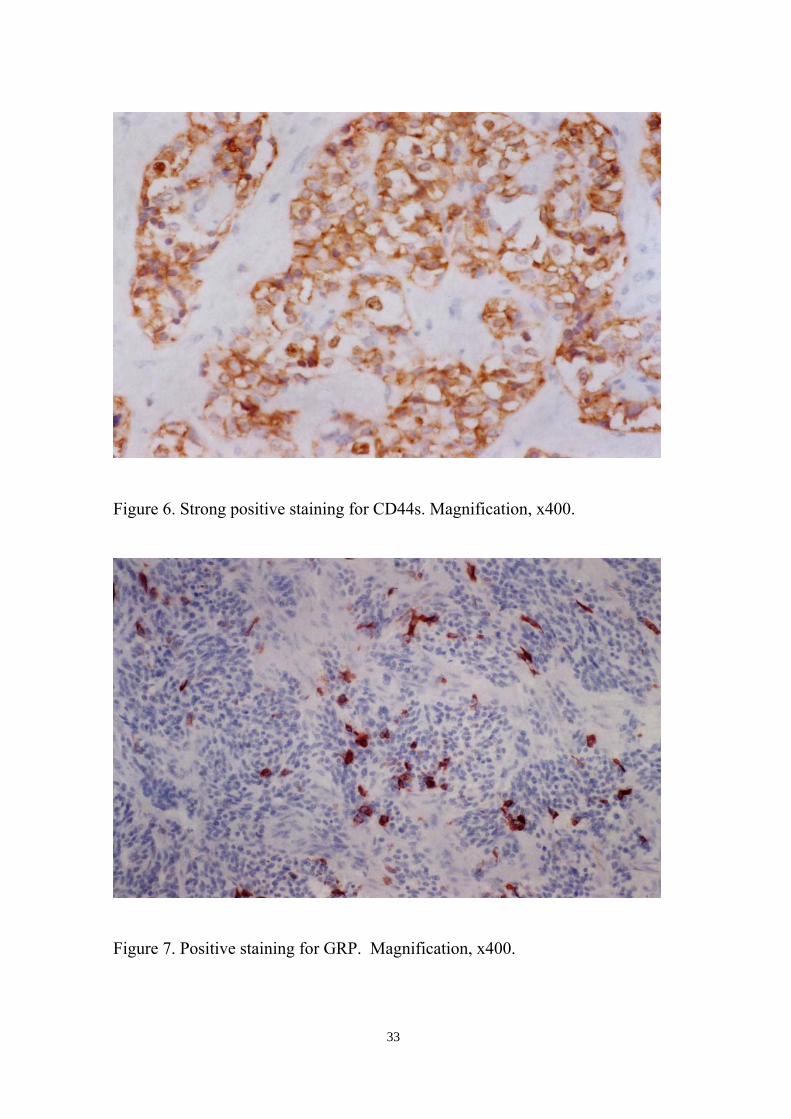
Figure 6. Strong positive staining for CD44s. Magnification, x400.
Figure 7. Positive staining for GRP. Magnification, x400.
33
TA
BL
E 3
. R
esul
ts o
f the
stai
ning
s, m
etas
tase
s and
surv
ival
(mon
ths)
of a
ll pa
tient
s in
Pape
r I a
nd I
IPa
t LN
D
MO
utco
me
mon
ths
Cyk
S-10
0K
i-67
%C
D44 s
CD
44v4
CD
44v5
CD
44v6
CD
44v7
CD
44v7
-8C
D44
v9A
CTH
Cal
GR
PhC
Gα
hCGβ
PP5-
HT
bax
bcl-2
c-er
bB-2
nm23
(nuc
l)nm
23(c
yt)
p53
rb
1N
oN
oA
, 25
-po
s0.
13po
spo
spo
s-
--
pos
--
++-
--
-po
s-
+++
++
--
2N
oN
oA
, 111
pos
-0.
13po
spo
spo
s-
pos
--
--
-+
--
+po
s-
+++
++
-+
3N
oN
oA
, 112
pos
-1.
00-
pos
pos
-po
s-
pos
--
--
-+
-po
s+
+++
++-
++4
No
No
A, 9
7po
spo
s0.
10po
spo
spo
spo
s-
pos
--
-++
+-
--
--
++++
++
-++
5N
oN
oA
, 70
pos
-0.
33po
spo
spo
s-
--
pos
--
--
--
-po
s-
-+
+-
-6
No
No
A, 6
7po
s-
0.10
pos
pos
pos
pos
-po
spo
s-
--
--
--
pos
--
+++
--
7N
oN
oA
, 170
--
0.46
pos
-po
s-
-po
spo
s+
++++
+++
+-
++-
--
+-
--
8N
oN
oA
, 120
pos
-0.
36po
spo
spo
spo
spo
spo
spo
s-
--
--
--
pos
--
+++
+-
+++
9N
oN
oA
, 87
pos
-2.
78po
spo
spo
spo
spo
spo
spo
s-
--
--
--
--
++++
+++
-++
10N
oN
oA
, 76
pos
-0.
78po
spo
spo
spo
spo
spo
spo
s-
--
+-
+++
pos
-++
++
-11
No
No
A, 5
8po
s-
0.10
--
pos
--
--
--
-+
-+
--
-++
+++
++
--
12N
oN
oA
, 101
pos
pos
1.11
pos
pos
pos
--
-po
s+
-+
+-
--
--
+++
++
+++
13N
oN
oA
, 43
pos
-0.
00-
pos
pos
-po
s-
--
--
--
--
pos
-++
++
+++
-+
14N
oN
oA
, 74
pos
-0.
10po
spo
spo
s-
pos
pos
pos
--
--
-+
-po
s-
++++
+-
+15
No
No
A, 1
62po
s-
1.17
pos
pos
pos
--
pos
pos
--
-+
-+
-po
s-
+++
+++
-+
16N
oN
oA
, 134
pos
pos
0.58
--
pos
--
--
--
-+
--
-po
s-
-++
+-
+17
No
No
A, 1
75po
s-
0.06
--
pos
--
--
--
-+
--
+po
s-
+++
+++
+-
-18
No
No
A, 6
5po
s-
0.50
pos
pos
pos
--
-po
s-
--
+-
--
pos
-+
+++
+-
-19
No
No
A, 1
18po
s-
0.33
pos
pos
pos
pos
pos
pos
pos
--
--
--
-po
s-
+++
++-
-20
No
No
A, 9
2po
s-
1.06
pos
-po
spo
spo
spo
spo
s-
--
++-
+-
pos
-+
+++
+-
-21
No
No
A, 9
3po
s-
1.40
-po
spo
s-
pos
--
--
-+
--
-po
s-
+++
+++
-+
22N
oN
oA
, 84
pos
-1.
00po
spo
spo
spo
spo
spo
spo
s-
--
+-
+-
pos
-++
+++
-+
23N
oN
oA
, 55
pos
pos
1.00
pos
-po
spo
spo
spo
spo
s-
--
+-
+-
pos
-+
+++
--
24N
oN
oA
, 32
pos
-0.
82po
spo
spo
s-
pos
pos
pos
--
-+
--
--
-+
+-
--
25N
oN
oA
, 37
pos
-0.
90-
--
-po
s-
--
--
--
-+
--
+++
++
-+
26N
oN
oA
, 34
pos
pos
0.73
pos
-po
s-
--
--
--
+-
--
--
++
+-
-27
No
No
A, 6
7po
spo
s0.
50po
s-
pos
-po
spo
spo
s+
--
+-
+-
pos
-+
+++
-+
28N
oN
o(†
), 45
pos
-0.
60-
--
-po
s-
--
--
+-
-++
pos
-++
++
++-
-29
No
No
A, 2
6po
s-
0.78
pos
pos
pos
-po
s-
pos
--
--
-++
--
-+
+++
--
30N
oN
oA
, 25
pos
-0.
91po
spo
spo
spo
spo
spo
spo
s-
--
++-
++++
pos
-++
-++
+-
++31
No
No
A, 2
1po
s-
0.30
pos
-po
s-
pos
-po
s-
--
++-
--
--
+++
+-
+32
Yes
No
A, 8
4po
spo
s0.
33po
spo
spo
spo
spo
spo
spo
s-
--
--
+-
pos
-+
++
--
33Y
esN
oA
, 134
pos
-0.
63po
spo
spo
spo
s-
pos
pos
--
--
-+
+-
-+
+++
-++
34Y
esN
oA
, 144
pos
pos
0.33
-po
spo
s-
pos
-po
s-
-++
+-
--
+++
pos
-+
+++
-++
35Y
esN
oA
, 70
--
0.27
pos
pos
pos
-po
s-
pos
+++
+++
+++
+-
++
--
+++
+++
-++
36Y
esN
oA
, 134
pos
-0.
18po
spo
spo
spo
spo
spo
spo
s-
--
--
--
pos
-+
+++
--
37Y
esN
oA
, 26
pos
-0.
10po
spo
s-
-po
s-
--
--
++-
+++
--
+++
-++
--
38Y
esN
oA
, 14
pos
-2.
78po
s-
pos
-po
s-
--
-+
+-
--
-+
+++
-++
-+
39N
oY
es†,
330
pos
-0.
10-
pos
--
pos
--
--
--
--
+po
s-
+++
-+
--
40Y
esY
es†,
60
pos
-10
.00
--
pos
--
--
+-
++-
--
++po
s++
++
-++
++++
41Y
esY
es†,
25
pos
pos
2.80
-po
spo
s-
--
--
--
--
--
--
-+
-+
++42
Yes
Yes
†, 3
8po
s-
0.33
--
pos
-po
s-
--
--
+++
--
--
-++
++
++-
-43
No
Yes
†, 1
74po
s-
1.40
--
pos
--
--
--
+++
--
--
pos
+++
-++
+-
+N
umbe
r of p
ositi
ve40
1029
2839
1327
1826
52
924
115
1327
437
3740
324
Cyk
, cyt
oker
atin
; Cal
, cal
cito
nin;
5-H
T, se
roto
nin;
nuc
l, nu
clea
r; cy
t, cy
topl
asm
ic. -
, neg
ativ
e; p
os, p
ositi
ve; +
, <1
0% p
ositi
ve c
ells
; ++,
10-
50%
pos
itive
cel
ls; +
++, >
50%
pos
itive
cells
. LN
, lym
ph n
ode
met
asta
ses a
t dia
gnos
is; D
M, d
ista
nt m
etas
tase
s; A
, aliv
e; †
, dea
d; (†
), de
ad o
f an
unre
late
d ca
use.
All
43 tu
mor
s sta
ined
pos
itive
for C
D44
v10.
34
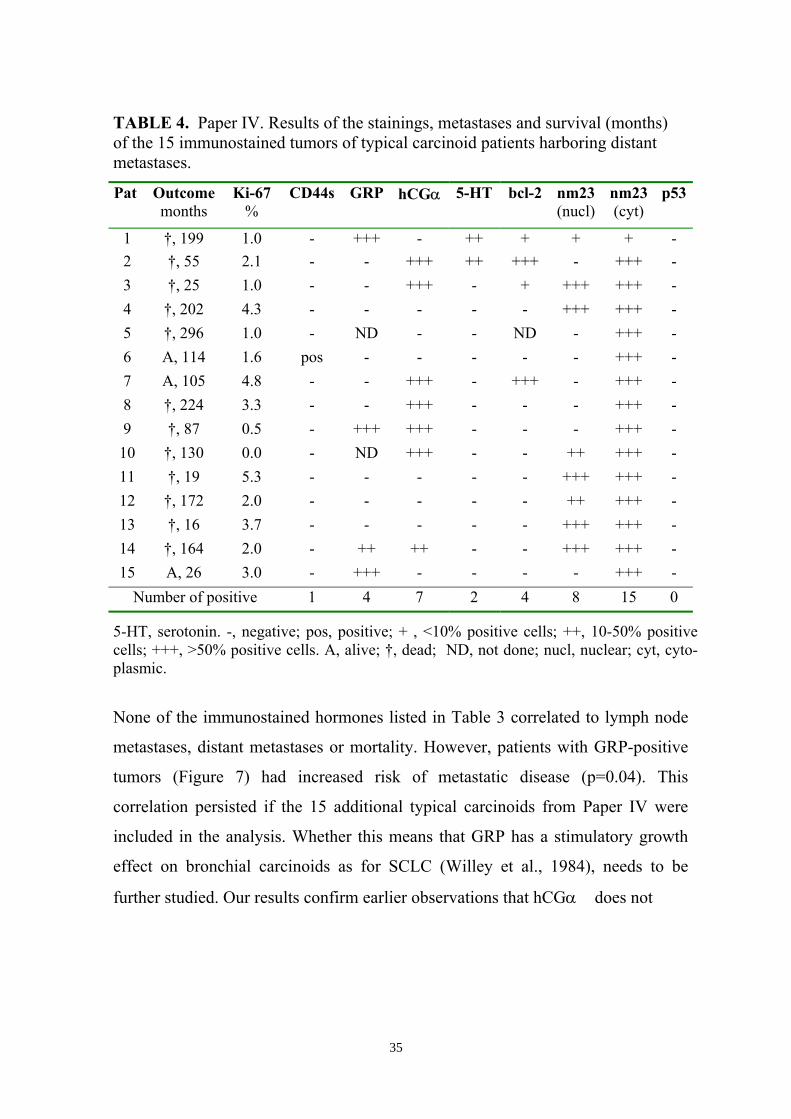
TABLE 4. Paper IV. Results of the stainings, metastases and survival (months)of the 15 immunostained tumors of typical carcinoid patients harboring distantmetastases.
Pat Outcomemonths
Ki-67%
CD44s GRP hCGα 5-HT bcl-2 nm23(nucl)
nm23(cyt)
p53
1 †, 199 1.0 - +++ - ++ + + + -2 †, 55 2.1 - - +++ ++ +++ - +++ -3 †, 25 1.0 - - +++ - + +++ +++ -4 †, 202 4.3 - - - - - +++ +++ -5 †, 296 1.0 - ND - - ND - +++ -6 A, 114 1.6 pos - - - - - +++ -7 A, 105 4.8 - - +++ - +++ - +++ -8 †, 224 3.3 - - +++ - - - +++ -9 †, 87 0.5 - +++ +++ - - - +++ -10 †, 130 0.0 - ND +++ - - ++ +++ -11 †, 19 5.3 - - - - - +++ +++ -12 †, 172 2.0 - - - - - ++ +++ -13 †, 16 3.7 - - - - - +++ +++ -14 †, 164 2.0 - ++ ++ - - +++ +++ -15 A, 26 3.0 - +++ - - - - +++ -
Number of positive 1 4 7 2 4 8 15 0
5-HT, serotonin. -, negative; pos, positive; + , <10% positive cells; ++, 10-50% positivecells; +++, >50% positive cells. A, alive; †, dead; ND, not done; nucl, nuclear; cyt, cyto-plasmic.
None of the immunostained hormones listed in Table 3 correlated to lymph node
metastases, distant metastases or mortality. However, patients with GRP-positive
tumors (Figure 7) had increased risk of metastatic disease (p=0.04). This
correlation persisted if the 15 additional typical carcinoids from Paper IV were
included in the analysis. Whether this means that GRP has a stimulatory growth
effect on bronchial carcinoids as for SCLC (Willey et al., 1984), needs to be
further studied. Our results confirm earlier observations that hCGα� does not
35
correlate to malignancy in neuroendocrine lung tumors (Heitz et al., 1987;
Tsutsumi, 1989).
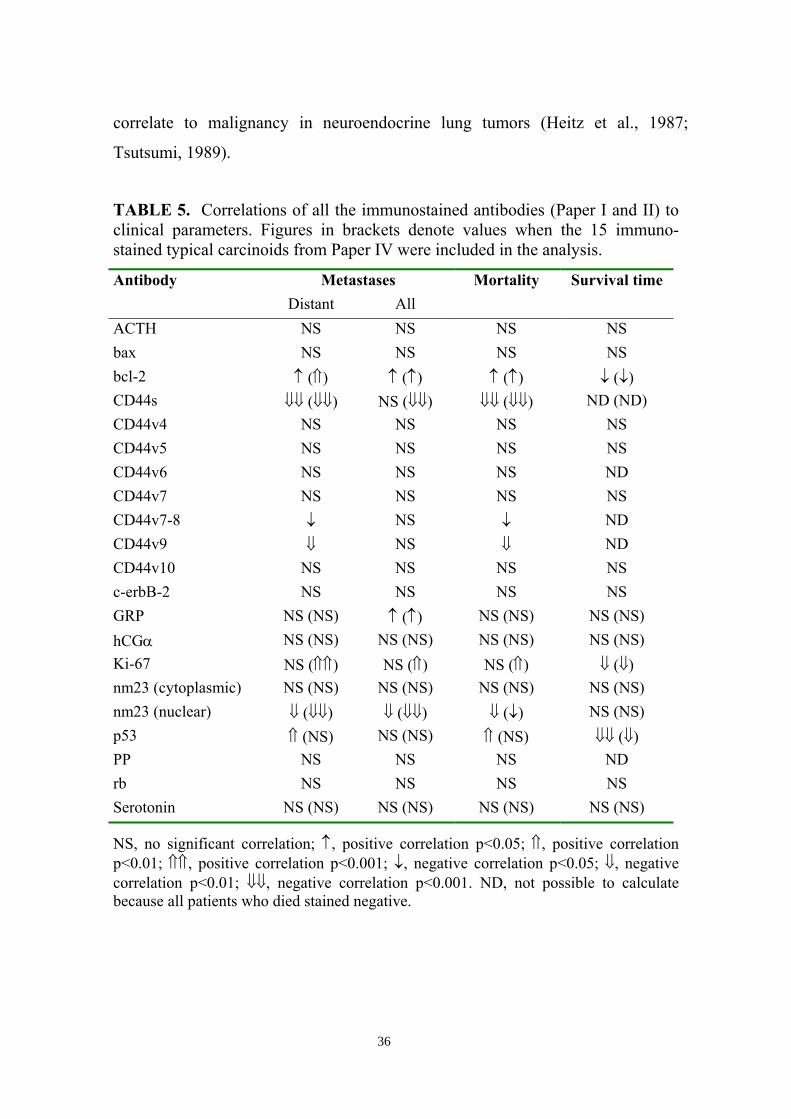
TABLE 5. Correlations of all the immunostained antibodies (Paper I and II) toclinical parameters. Figures in brackets denote values when the 15 immuno-stained typical carcinoids from Paper IV were included in the analysis.
Antibody Metastases Mortality Survival timeDistant All
ACTH NS NS NS NSbax NS NS NS NSbcl-2 ↑ (⇑) ↑ (↑) ↑ (↑) ↓ (↓)CD44s ⇓⇓ (⇓⇓) NS (⇓⇓) ⇓⇓ (⇓⇓) ND (ND)CD44v4 NS NS NS NSCD44v5 NS NS NS NSCD44v6 NS NS NS NDCD44v7 NS NS NS NSCD44v7-8 ↓ NS ↓ NDCD44v9 ⇓ NS ⇓ NDCD44v10 NS NS NS NSc-erbB-2 NS NS NS NSGRP NS (NS) ↑ (↑) NS (NS) NS (NS)hCGα NS (NS) NS (NS) NS (NS) NS (NS)Ki-67 NS (⇑⇑) NS (⇑) NS (⇑) ⇓ (⇓)nm23 (cytoplasmic) NS (NS) NS (NS) NS (NS) NS (NS)nm23 (nuclear) ⇓ (⇓⇓) ⇓ (⇓⇓) ⇓ (↓) NS (NS)p53 ⇑ (NS) NS (NS) ⇑ (NS) ⇓⇓ (⇓)PP NS NS NS NDrb NS NS NS NSSerotonin NS (NS) NS (NS) NS (NS) NS (NS)
NS, no significant correlation; ↑, positive correlation p<0.05; ⇑, positive correlationp<0.01; ⇑⇑, positive correlation p<0.001; ↓, negative correlation p<0.05; ⇓, negativecorrelation p<0.01; ⇓⇓, negative correlation p<0.001. ND, not possible to calculatebecause all patients who died stained negative.
36
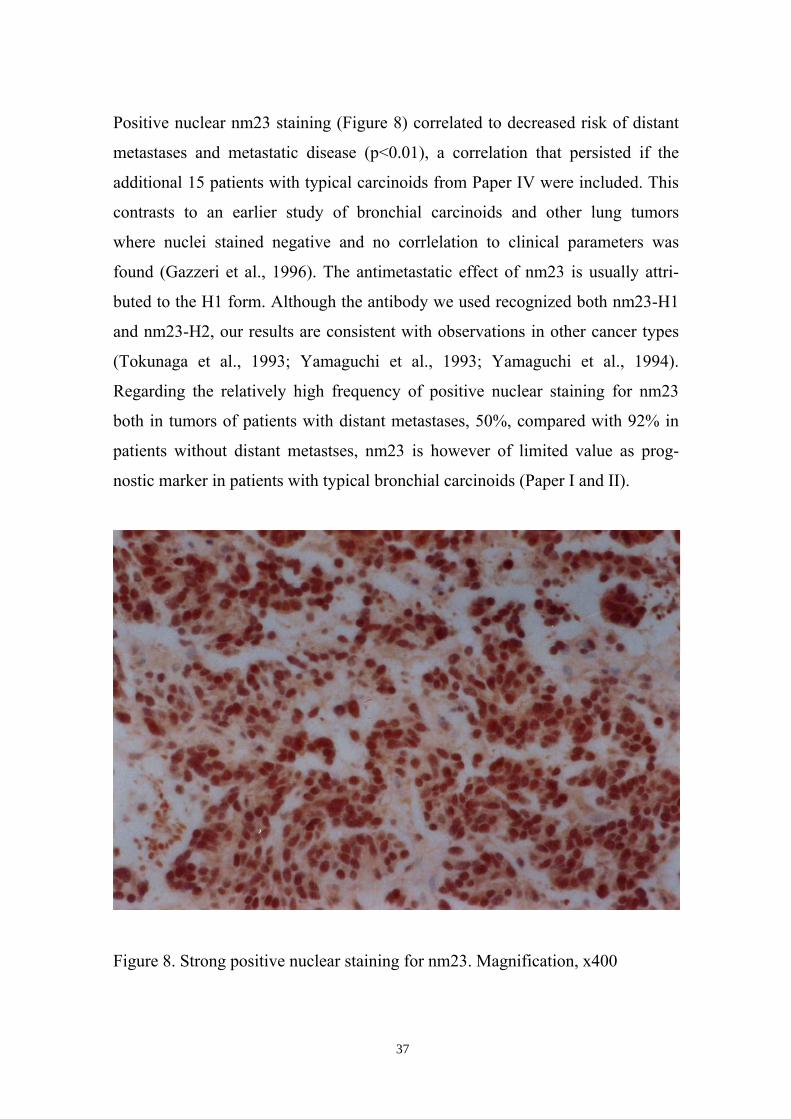
Positive nuclear nm23 staining (Figure 8) correlated to decreased risk of distant
metastases and metastatic disease (p<0.01), a correlation that persisted if the
additional 15 patients with typical carcinoids from Paper IV were included. This
contrasts to an earlier study of bronchial carcinoids and other lung tumors
where nuclei stained negative and no corrlelation to clinical parameters was
found (Gazzeri et al., 1996). The antimetastatic effect of nm23 is usually attri-
buted to the H1 form. Although the antibody we used recognized both nm23-H1
and nm23-H2, our results are consistent with observations in other cancer types
(Tokunaga et al., 1993; Yamaguchi et al., 1993; Yamaguchi et al., 1994).
Regarding the relatively high frequency of positive nuclear staining for nm23
both in tumors of patients with distant metastases, 50%, compared with 92% in
patients without distant metastses, nm23 is however of limited value as prog-
nostic marker in patients with typical bronchial carcinoids (Paper I and II).
Figure 8. Strong positive nuclear staining for nm23. Magnification, x400
37
Positive staining for bcl-2 correlated to increased risk of distant metastases
(p=0.01) and metastatic disease (p<0.05) as well as decreased survival time
(p<0.05), indicating that apoptosis may have prognostic importance in these
tumors. This is consistent with earlier observations in patients with neuro-
endocrine lung tumors (Brambilla et al., 1996). Weak positive staining for p53
has earlier been found in bronchial carcinoids (Coppola et al., 1996). In our
material, 3 tumors were positive for p53, which correlated to increased risk of
distant metastases (p<0.01) as well as decreased survival time (p<0.001). If all 58
immunostained typical carcinoids from Papers I+II and IV were included, p53
still correlated to decreased survival time (p<0.01) but not to metastases or
mortality. Since positive staining is rare for both bcl-2 and p53 in typical
bronchial carcinoids (14% and 5% respectively in our material), they are not
suitable for routine use as prognostic markers (Paper I and II).
Octreoscan
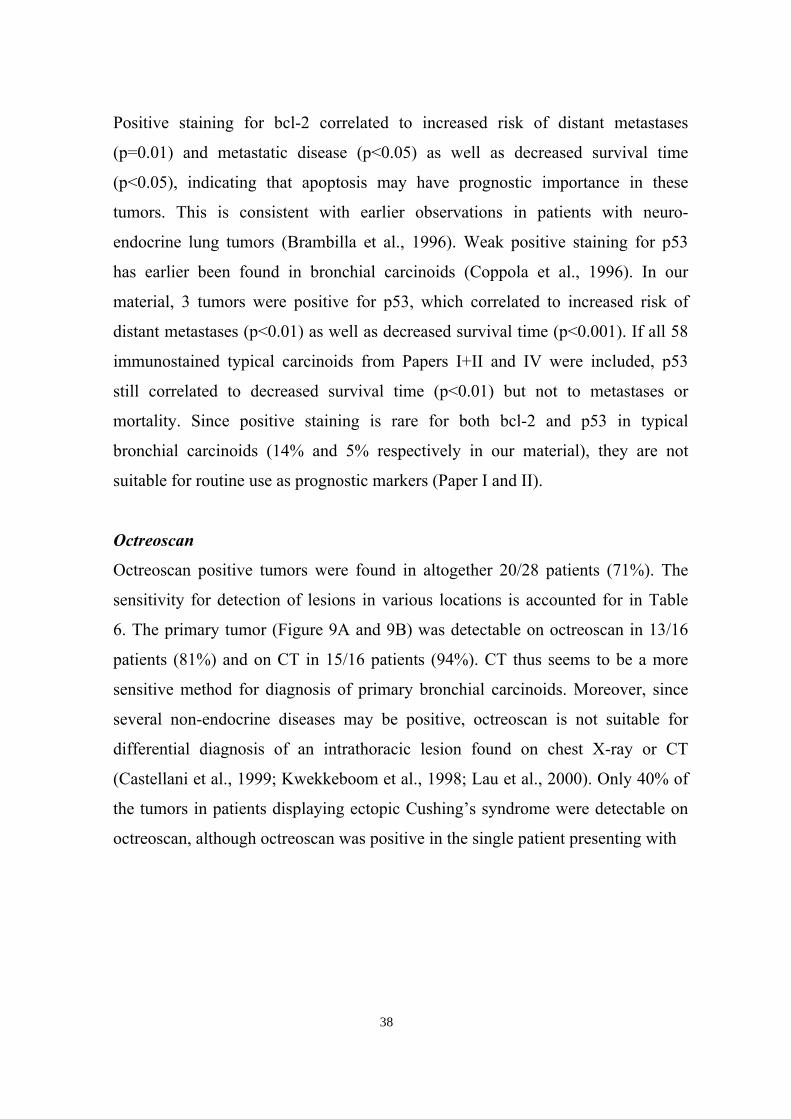
Octreoscan positive tumors were found in altogether 20/28 patients (71%). The
sensitivity for detection of lesions in various locations is accounted for in Table
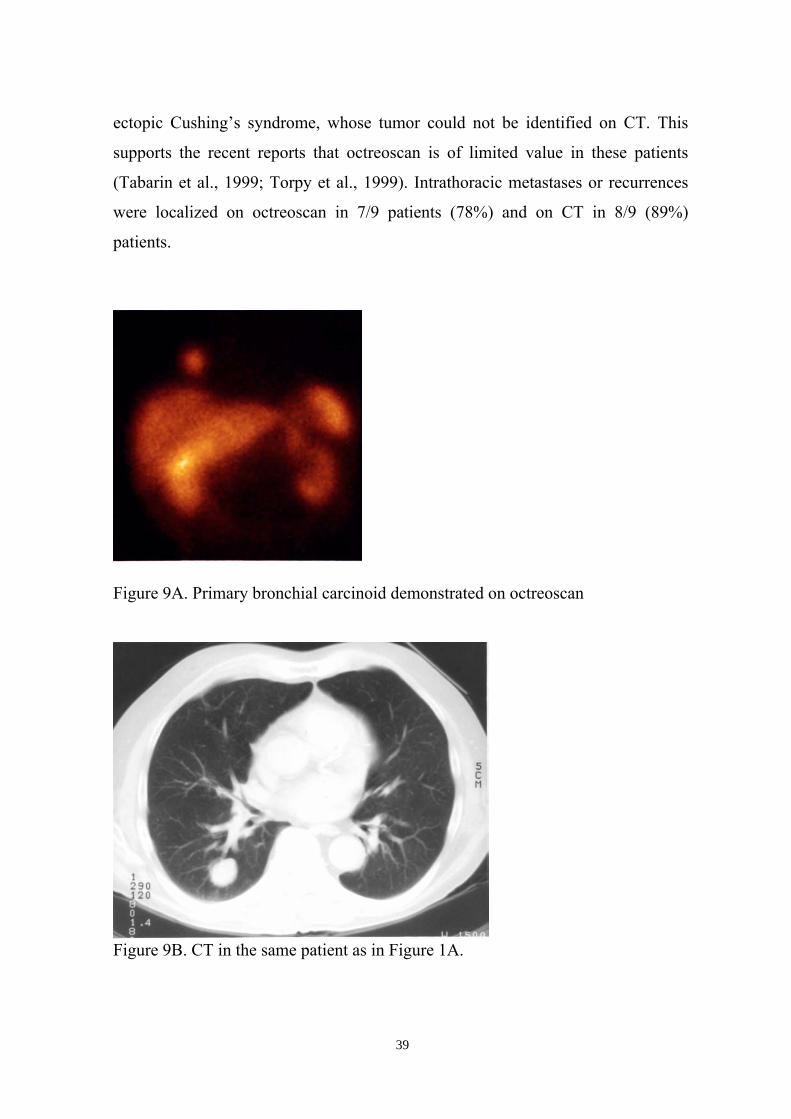
6. The primary tumor (Figure 9A and 9B) was detectable on octreoscan in 13/16
patients (81%) and on CT in 15/16 patients (94%). CT thus seems to be a more
sensitive method for diagnosis of primary bronchial carcinoids. Moreover, since
several non-endocrine diseases may be positive, octreoscan is not suitable for
differential diagnosis of an intrathoracic lesion found on chest X-ray or CT
(Castellani et al., 1999; Kwekkeboom et al., 1998; Lau et al., 2000). Only 40% of
the tumors in patients displaying ectopic Cushing’s syndrome were detectable on
octreoscan, although octreoscan was positive in the single patient presenting with
38
ectopic Cushing’s syndrome, whose tumor could not be identified on CT. This
supports the recent reports that octreoscan is of limited value in these patients
(Tabarin et al., 1999; Torpy et al., 1999). Intrathoracic metastases or recurrences
were localized on octreoscan in 7/9 patients (78%) and on CT in 8/9 (89%)
patients.
Figure 9A. Primary bronchial carcinoid demonstrated on octreoscan
Figure 9B. CT in the same patient as in Figure 1A.
39
Octreoscan managed to demonstrate liver metastases in 9/14 (64%) of the pati-
ents with liver metastases seen on CT, yielding 64% sensitivity for recognition of
liver involvement. This is slightly lower than earlier reported figures (89–93%)
in patients with neuroendocrine gastro-entero-pancreatic tumors (Chiti et al.,
1998; Krausz et al., 1998; Scherübl et al., 1993).
Bone metastases were visualized on octreoscan in 7/10 patients (70%) and on
conventional bone scan in 9/10 patients with bone metastases confirmed by plain
X-ray or MRI. Conventional bone scan or plain X-ray revealed a higher number
of metastases than octreoscan in 5 of the 7 patients with bone metastases seen on
octreoscan. Bone scan has thus a higher sensitivity for detection of bone
metastases than octreoscan. Octreoscan is nevertheless suitable for follow-up and
screening of relapse in patients with octreoscan positive bronchial carcinoids. In
order to select the appropriate patients to follow with octreoscan, it is crucial to
perform an examination before curative surgery. If this is not done, an alternative
is to immunostain the primary tumor for somatostatin receptor expression
(Tiensuu Janson et al., 1998) (Paper III).
The number of patients in this study is somewhat limited, and the recorded
differences of sensitivity for octreoscan and CT may reflect this circumstance. If
the sensitivity for octreoscan to detect lesions in various locations is calculated in
only those patients whose tumors are known to be octreoscan positive, the
figures will of course be slightly higher than in Table 6. The superiority of CT,
however, remains (Paper III).
40
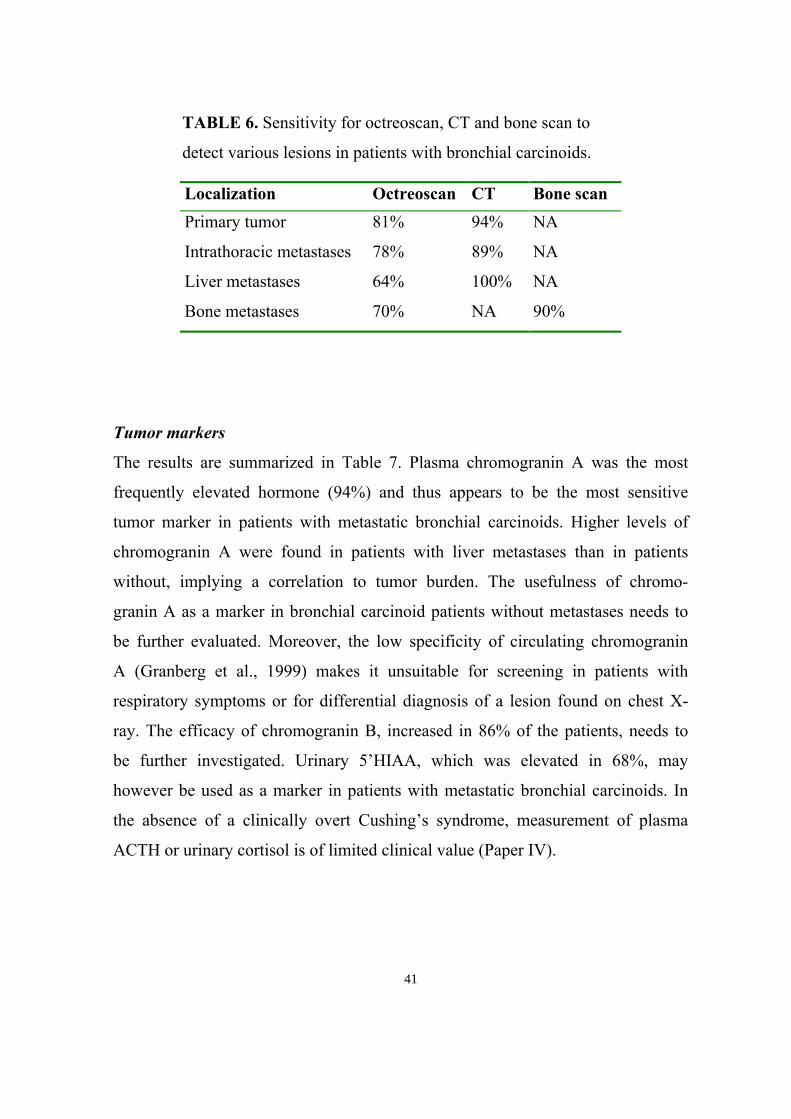
TABLE 6. Sensitivity for octreoscan, CT and bone scan to
detect various lesions in patients with bronchial carcinoids.
Localization Octreoscan CT Bone scanPrimary tumor 81% 94% NA
Intrathoracic metastases 78% 89% NA
Liver metastases 64% 100% NA
Bone metastases 70% NA 90%
Tumor markers
The results are summarized in Table 7. Plasma chromogranin A was the most
frequently elevated hormone (94%) and thus appears to be the most sensitive
tumor marker in patients with metastatic bronchial carcinoids. Higher levels of
chromogranin A were found in patients with liver metastases than in patients
without, implying a correlation to tumor burden. The usefulness of chromo-
granin A as a marker in bronchial carcinoid patients without metastases needs to
be further evaluated. Moreover, the low specificity of circulating chromogranin
A (Granberg et al., 1999) makes it unsuitable for screening in patients with
respiratory symptoms or for differential diagnosis of a lesion found on chest X-
ray. The efficacy of chromogranin B, increased in 86% of the patients, needs to
be further investigated. Urinary 5’HIAA, which was elevated in 68%, may
however be used as a marker in patients with metastatic bronchial carcinoids. In
the absence of a clinically overt Cushing’s syndrome, measurement of plasma
ACTH or urinary cortisol is of limited clinical value (Paper IV).
41
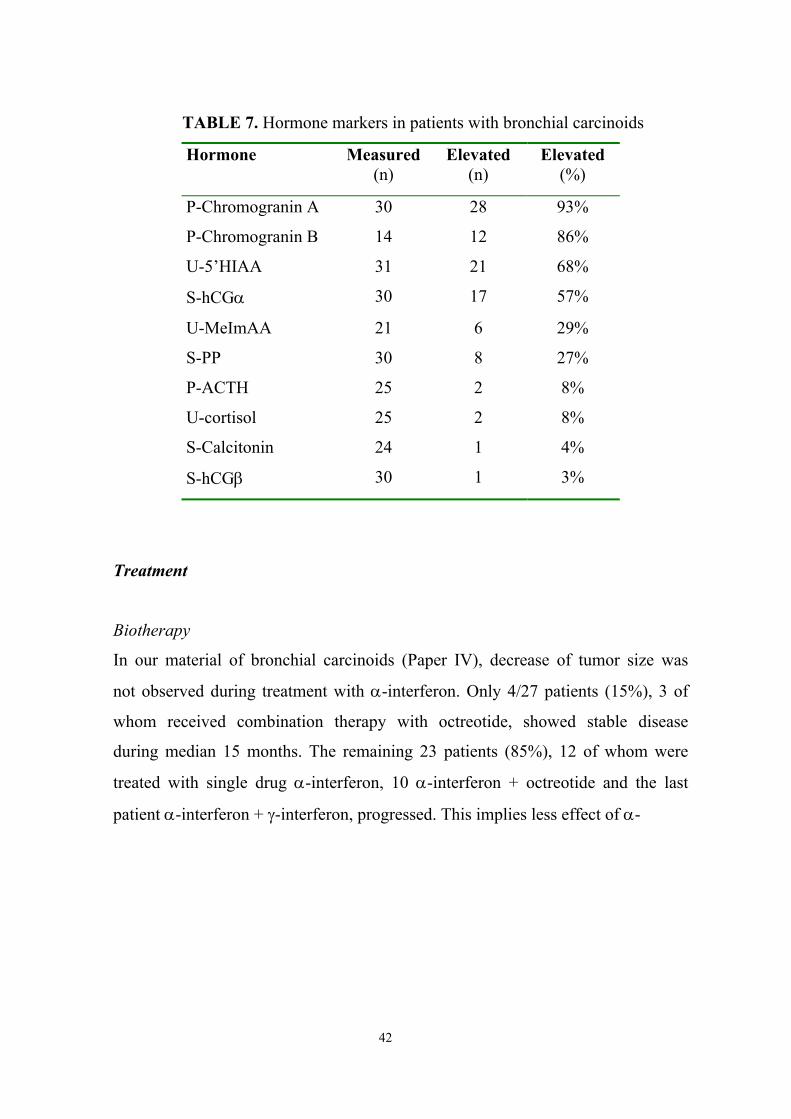
TABLE 7. Hormone markers in patients with bronchial carcinoids
Hormone Measured(n)
Elevated(n)
Elevated(%)
P-Chromogranin A 30 28 93%
P-Chromogranin B 14 12 86%
U-5’HIAA 31 21 68%
S-hCGα 30 17 57%
U-MeImAA 21 6 29%
S-PP 30 8 27%
P-ACTH 25 2 8%
U-cortisol 25 2 8%
S-Calcitonin 24 1 4%
S-hCGβ 30 1 3%
Treatment
Biotherapy
In our material of bronchial carcinoids (Paper IV), decrease of tumor size was
not observed during treatment with α-interferon. Only 4/27 patients (15%), 3 of
whom received combination therapy with octreotide, showed stable disease
during median 15 months. The remaining 23 patients (85%), 12 of whom were
treated with single drug α-interferon, 10 α-interferon + octreotide and the last
patient α-interferon + γ-interferon, progressed. This implies less effect of α-
42
interferon on tumor growth in bronchial than in midgut carcinoids (Frank et al.,
1999). Symptomatic relief of carcinoid syndrome, which was achieved in 7/16 of
our patients, seems to be the principal effect of biotherapy with α-interferon and
octreotide in bronchial carcinoids.
Treatment with γ-interferon was used in altogether 14 patients without being
apparently beneficial. Intolerable side-effects necessitated withdrawal within 2
months in 4 patients (3 of whom received concomitant α-interferon). In another 7
patients (5 of these 7 were treated with α-interferon in combination with γ-
interferon) progressive disease was observed within 6 months. Only 3 patients (1
treated with α-interferon + γ-interferon and 2 receiving γ-interferon + octreo-
tide) showed stable disease during 10– 29 months. Progressive disease was
however later recorded in these cases as well. None of the patients treated with
octreotide (n=3) or lanreotide (n=1) as single drug therapy experienced an
objective response. This therapy is only indicated in patients with disabling
carcinoid syndrome. In addition, we have seen symptomatic improvement and
decrease of hormone levels during treatment with octreotide in bronchial carci-
noid patients displaying ectopic Cushing’s syndrome.
Chemotherapy
The response rates are summarized in Table 8. The combination of streptozoto-
cin + 5-FU, for which reponse rates of 45–63% have been reported in patients
with endocrine pancreatic tumors (Eriksson and Öberg, 1993; Moertel et al.,
1980; Moertel et al., 1992), was not effective in our patients (Paper IV). Six
patients progressed continously, while one patient, showing stable disease for 8
43
months, progressed after 12 months. Streptozotocin + 5-FU is thus not indicated
in bronchial carcinoid patients. On the other hand, doxorubicin combined with
either streptozotocin or paclitaxel resulted in stable disease for about 9 months in
2/2 patients each. Doxorubicin-containing regimens may be of value for patients
with bronchial carcinoids and should be further evaluated in controlled studies.
The combination of cisplatinum + etoposide, which is effective in small cell lung
cancer, was used in 8 of our patients (Paper IV), receiving 3–8 (median 6) cour-
ses. Two patients showed decrease in tumor size lasting 6 and 8 months respec-
tively and one had stablilization of the disease for 7 months. The remaining five
patients progressed after 3–4 months, although the hormones decreased and
symptomatic relief was obtained in a patient with ectopic Cushing’s syndrome
who received concomitant α-interferon. There was no correlation of response to
Ki-67 expression; both patients with objective responses had typical carcinoids
with 1% and 3% Ki-67-positive cells respectively. Our encouraging results
contrast to another study of patients with neuroendocrine tumors, where neither
of 2 patients harboring well differentiated lung carcinoids showed decreased
tumor size or reduction of urinary 5’HIAA during treatment with cisplatinum +
etoposide (Moertel et al., 1991). Although renal and neurologic side-effects limit
the number of tolerated courses, further studies of Cisplatinum + Etoposide are
justified in bronchial carcinoid patients.
44

TABLE 8. Response rates to medical treatment in patients with metastatic
bronchial carcinoids
Treatment Total Stable disease Duration* n n % months
α-interferon 27 4 15% 15
streptozotocin + 5-FU 7 1 14% 8
streptozotocin + doxorubicin 2 2 100% 9
cisplatinum + etoposide 8 3# 38% 7
paclitaxel + doxorubicin 2 2 100% 9
* Median duration in patients who showed stable disease or objective response.# Two of these patients displayed objective response.
Other treatments
Five patients underwent liver embolization with gel-foam (Paper IV). The proce-
dure was performed on one occasion in 1 patient, on two occasions in 2 patients
and on three occasions in 2 patients. Clinical improvement was achieved in 3
patients. Biochemical stabilization was observed in 2 patients, while 3 patients
experienced reduction of hormones. One patient showed decreased size of the
liver metastases lasting 11 months, while the remaing 4 patients showed radiolo-
gically stable disease for 8–23 months. As could be expeted from earlier data
regarding midgut carcinoids (Eriksson et al., 1998), liver embolization may as
well be of value for debulking of liver metastases in patients with bronchial
carcinoids, and may produce symptomatic relief and reduction of hormones. The
effect is, however, short-lived and most pronounced after the first embolization
in each lobe.
45

None of the 3 patients receiving targeted radiotherapy (111In-Octreotide, n=2; 131I-
MIBG, n=1) responded, but the limited number of cases and the fact that all
patients harbored advanced disease makes it difficult to settle the role for targe-
ted radiotherapy in patients with metastatic bronchial carcinoids.
Prognosis
All 5 patients with distant metastases in Paper I and II have died from their tumor
disease during the observation period; one of them, however, died after Paper II
was published. Moreover, one patient died from an unrelated cause, free of car-
cinoid recurrence. The relatively high mortality rate, 12%, contrasts to several
other reports (Padberg et al., 1996; Travis et al., 1991; Warren and Gould, 1990).
This may be due to differences in the patient populations. It is possible that, in
other studies reporting surgical materials, patients with widespread disease were
not referred to surgery and therefore not included. On the other hand, our inten-
tion was to identify all patients with typical carcinoids in the referral area of the
hospital. Confirming the results in previous studies (El-Naggar et al., 1991; Jones
et al., 1988; McCaughan et al., 1985; Torre et al., 1989), lymph node metastases
at diagnosis were associated with increased risk of distant metastases (p=0.04)
and shorter survival time (p<0.001). The 5- and 10-year survival in our unselec-
ted patient material of 43 typical bronchial carcinoids (Paper I and II) was 95%
and 91%, respectively, which is consistent with other reports (Chughtai et al.,
1997; Garcia-Yuste et al., 2000; Harpole et al., 1992; Okike et al., 1976). The
46
discrepancy between the relatively high mortality rate and the long survival time
reflects the slow growth of these tumors.
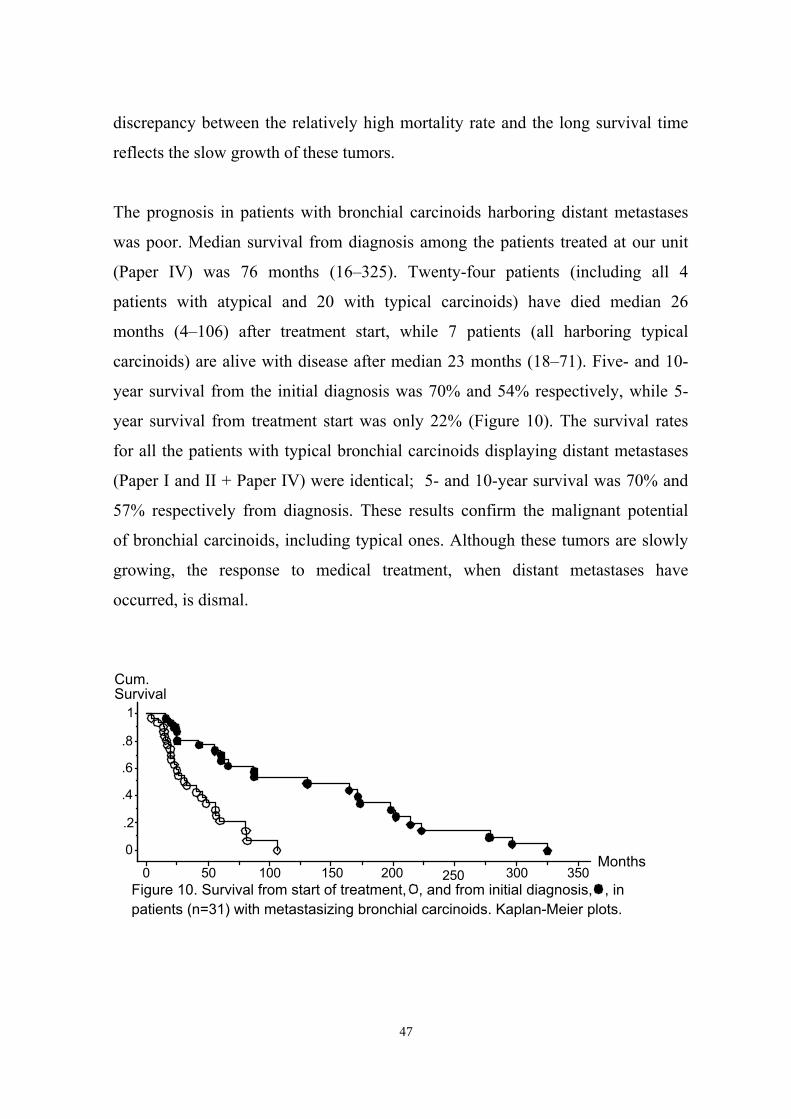
The prognosis in patients with bronchial carcinoids harboring distant metastases
was poor. Median survival from diagnosis among the patients treated at our unit
(Paper IV) was 76 months (16–325). Twenty-four patients (including all 4
patients with atypical and 20 with typical carcinoids) have died median 26
months (4–106) after treatment start, while 7 patients (all harboring typical
carcinoids) are alive with disease after median 23 months (18–71). Five- and 10-
year survival from the initial diagnosis was 70% and 54% respectively, while 5-
year survival from treatment start was only 22% (Figure 10). The survival rates
for all the patients with typical bronchial carcinoids displaying distant metastases
(Paper I and II + Paper IV) were identical; 5- and 10-year survival was 70% and
57% respectively from diagnosis. These results confirm the malignant potential
of bronchial carcinoids, including typical ones. Although these tumors are slowly
growing, the response to medical treatment, when distant metastases have
occurred, is dismal.
0 50 100 150 200 250 300 350
0
.2
.4
.6
.8
1
Cum.Survival
Months
Figure 10. Survival from start of treatment, , and from initial diagnosis, , inpatients (n=31) with metastasizing bronchial carcinoids. Kaplan-Meier plots.
47
CLINICAL MANAGEMENT
Figure 11. When a patient is found to have a lesion suspected to be a bronchial
carcinoid, either on chest X-ray or at bronchoscopy, histological diagnosis is
mandatory. If the tumor is not accessible by bronchoscopy, transthoracic needle
biopsy guided by CT should be considered. A CT scan of the thorax is warran-
ted for identification of intrathoracic lymph nodes, and CT or ultrasonography of
the abdomen is indicated to screen for liver metastases. An octreoscan ought to
be performed as well. Plasma chromogranin A should be analyzed; if the patient
presents with carcinoid syndrome, measurement of U-5’HIAA and U-MeImAA
is also indicated. Sampling of P-ACTH and U-cortisol is not necessary unless
Cushing’s syndrome is clinically overt. After these diagnostic measures, the
patient should be referred to surgery with curative intent. The aim of the surgical
procedure is to remove the tumor and all affected lymph nodes, sparing as much
lung parenchyma as possible. It is necessary to take intraoperative biopsies with
frozen section. For assessment of prognosis, the tumor should be classified as
typical or atypical and immunostained with CD44s and Ki-67. When radical
surgery of the primary tumor is not possible or distant metastases are present,
chemotherapy with doxorubicin combined with streptozotocin or paclitaxel may
be considered; another alternative is cisplatinum + etoposide. Thoracic
radiotherapy may be given to control local tumor growth. All patients with
bronchial carcinoids ought to be followed for more than a decade, since
metastases may occur late. The follow-up should include measurement of plasma
chromogranin A and regular screening for local recurrence and distant (liver and
bone) metastases.
48
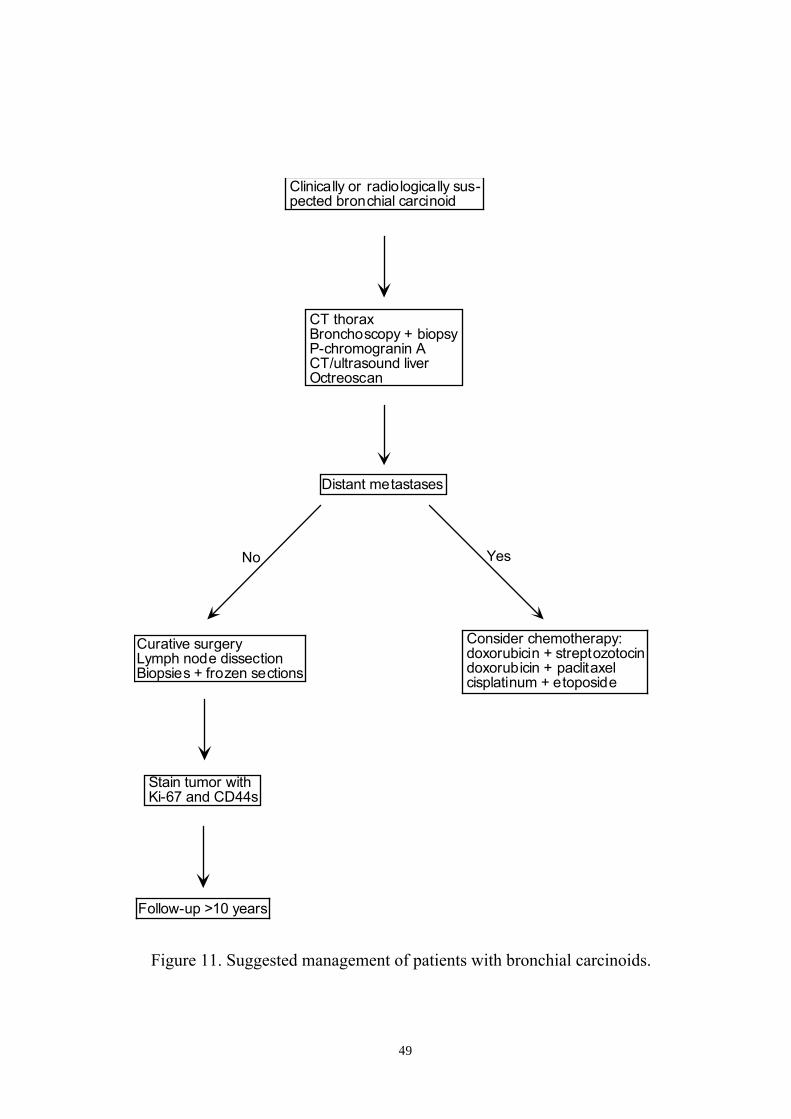
Figure 11. Suggested management of patients with bronchial carcinoids.
Curative surgery Lymph node dissection Biopsies + frozen sections
CT thorax Bronchoscopy + biopsy P-chromogranin A CT/ultrasound liver Octreoscan
Clinically or radiologically sus-pected bronchial carcinoid
Distant metastases
No Yes
Stain tumor withKi-67 and CD44s
Consider chemotherapy: doxorubicin + streptozotocindoxorubicin + paclitaxel cisplatinum + etoposide
Follow-up >10 years
49
GENERAL SUMMARY
Typical bronchial carcinoids are potentially malignant tumors. In our unselected
material of 43 patients, altogehter 12 (28%) displayed metastatic disease. Distant
metastases were found in 5 patients (12%), who all died of their tumors. Lymph
node metastasis at diagnosis is associated with increased risk of distant
metastases and death. A high Ki-67 index correlates to increased risk of distant
metastases and mortality and to decreased survival time. Positive staining for
CD44s, v9 and v7-8, as well as positive nuclear nm23 staining is associated with
decreased risk of distant metastases and mortality. On the other hand, positive
staining for bcl-2 correlates to increased risk of distant metastases and death as
well as decreased survival time, while p53 only correlates to decreased survival
time. GRP merely shows correlation to metastatic disease. Immunostaining for
CD44s, CD44v7-8, CD44v9, nm23, Ki-67, bcl-2 and p53 might provide
additional information on the individual tumor biology and prognosis in patients
with typical bronchial carcinoids. For routine use as prognostic markers in these
patients, CD44s and Ki-67 are most suitable.
In patients with bronchial carcinoids, octreoscan is less sensitive for detection of
the primary tumor and liver metastases than CT. Conventional bone scan is more
effective than octreoscan for identification of bone metastases. Octreoscan may
nevertheless be useful in the follow-up of patients with somatostatin-receptor-
positive bronchial carcinoid tumors. An octreoscan should be performed in all
these patients prior to surgery with curative intent.
50
Plasma chromogranin A is the most sensitive tumor marker; in addition urinary
5’HIAA may be used as a marker in patients with metastatic bronchial carci-
noids. In the absence of clinically overt Cushing’s syndrome, measurement of
plasma ACTH or urinary cortisol seems to be of limited value.
Biotherapy with α-interferon and/or octreotide has mainly symptomatic effects in
patients with bronchial carcinoids, although a limited number of subjects may
experience stable disease. The combination of streptozotocin + 5-FU is not indi-
cated in these patients. On the other hand, doxorubicin combined with strepto-
zotocin or paclitaxel may result in stable disease and should be further studied.
Cisplatinum + etoposide resulted in tumor reduction or stable disease in 38% of
the patients. Although renal and neurologic side effects limit the number of
courses that can be administered, this combination seems to be useful in a subset
of patients with bronchial carcinoids. Liver embolization with gel-foam may for
limited periods result in symptomatic improvement in addition to reduction of
hormone markers and stabilization of tumor size.
The prognosis in bronchial carcinoid patients harboring distant metastases is
poor. Median survival was 76 months (16–325) from diagnosis, while 5- and 10-
year survival was 70% and 54% respectively. Five-year survival from treatment
start was only 22%. Although these tumors are slowly growing, the response to
medical treatment is discouraging. Radical surgery still offers the best hope for
cure. Since metastases may occur decades after the initial diagnosis, these
patients have to be followed for a long period of time.
51
ACKNOWLEDGEMENTS
This study was carried out at the Department of Endocrine Oncology, Division of
Medicine, University Hospital, Uppsala, Sweden. Financial support was received
from the Swedish Cancer Society, Lions Foundation for Cancer Research, the
Swedish Medical Council, the Swedish Society for Medical Research, the
Uppsala County Association against Heart and Lung Diseases and from Torsten
and Ragnar Söderbergs Foundation.
I wish to express my sincere gratitude to the following persons:
Britt Skogseid, my supervisor, for introducing me into the mysteries of research
Kjell Öberg, the former head of our department, for including me into his team
and providing me with the possibilities to perform research in the field of cancer,
and for his support, listening and interest
Erik Wilander, my co-supervisor, for fruitful collaboration and help with
interpretation of the immunohistochemistry
Barbro Eriksson, the head of our department, for her human attitude to
everybody
52
Anders Sundin and Jan-Erik Westlin, my co-authors in Paper IV, for their
interest, help and support and Ola Hessman for valuable comments about the
manuscript
Rajni Dyal, for teaching me the laboratory work, and Margareta Halin-
Lejonklou, for help with the immunohistochemical stainings
Lena Hultström, for excellent secretarial assistance and generous help with
practical problems of all kinds
Marie-Louise Fjällskog, Jarl Hellman, Eva Tiensuu Janson, Staffan Welin,
Håkan Örlefors and all other colleagues at our department for good cooperation
and interesting discussions
Peter Stålberg and Shu Wang for fruitful research cooperation
Gertrud Fredriksson, for generous help in finding patient records
Anita, Doris, Gunnel, Gunvi, Helena, Maj, Maud, Monica, Ragnvi and all
other staff at 30 B2 for their enthusiasm and warm care of the patients and
making our ward a nice place to work
Yesuf Taha, my friend, for interesting discussions and being a pleasant room-
mate
53
Gösta Tjernberg, my friend, for plenty of help in solving computer problems
Riselda, for love and tenderness
Kjell, my father, for his never-ending love, help with everything and support
Caroline and Niklas, my beloved children
54
REFERENCES
Almqvist, S., Telenius-Berg, M. and Wästhed, B. Serum calcitonin in medullarythyroid carcinoma. Acta Med Scand 1974;196:177-180
Arrigoni, M.G., Woolner, L.B. and Bernatz, P.E. Atypical carcinoid tumors of thelung. J Thorac Cardiovasc Surg 1972;64:413-421
Aruffo, A., Stamenkovic, I., Melnick, M., Underhill, C.B. and Seed, B. CD44 isthe Principal Cell Surface Receptor for Hyaluronate. Cell 1990;61:1303-1313
Ayhan, A., Yasui, W., Yokozaki, H., Kitadai, Y. and Tahara, E. Reducedexpression of nm23 protein is associated with advanced tumor stage and distantmetastases in human colorectal carcinomas. Virchovs Arch B Cell Pathol1993;63:213-218
Bakker, W.H., Albert, R., Bruns, C., Breeman, W.A.P., Hofland, L.J., Marbach,P., Pless, J., Pralet, D., Stolz, B., Koper, J.W., Lamberts, S.W.J., Visser, T.J. andKrenning, E.P. [111In-DTPA-D-Phe1]-octreotide, a potentialradiopharmaceutical for imaging of somatostatin receptor-positive tumors:synthesis, radiolabeling and in vitro validation. Life Sci 1991;49:1583-1591
Bakker, W.H., Krenning, E.P., Breeman, W.A., Koper, J.W., Kooij, P.P., Reubi,J.-C., Klijn, J.G., Visser, T.J., Docter, R. and Lamberts, S.W.J. ReceptorScintigraphy with a Radioiodinated Somatostatin Analogue: Radiolabeling,Purification, Biologic Activity, and In Vivo Application in Animals. J Nucl Med1990;31:1501-1509
Barbareschi, M., Girlando, S., Mauri, F.A., Arrigoni, G., Laurino, L., DallaPalma, P. and Doglioni, C. Tumour suppressor gene products, proliferation, anddifferentiation markers in lung neuroendocrine neoplasms. J Pathol1992;166:343-350
55
Beasley, M.B., Thunnissen, F.B.J.M., Brambilla, E., Hasleton, P., Steele, R.,Hammar, S.P., Colby, T.V., Sheppard, M., Shimosato, Y., Koss, M.N., Falk, R.and Travis, W.D. Pulmonary atypical carcinoid: predictors of survival in 106cases. Hum Pathol 2000;31:1255-1265
Bensch, K.G., Corrin, B., Pariente, R. and Spencer, H. Oat-Cell Carcinoma of theLung. Its Origin and Relationship to Bronchial Carcinoid. Cancer 1968;22:1163-1172
Bensch, K.G., Gordon, G.B. and Miller, L.R. Electron Microscopic andBiochemical Studies on the Bronchial Carcinoid Tumor. Cancer 1965;18:592-602
Berenger, N., Moretti, J.L., Boaziz, C., Vigneron, N., Morere, J.F. and Breau,J.L. Somatostatin Receptor Imaging in Small Cell Lung Cancer. Eur J Cancer1996;32A:1429-1431
Bertelsen, S., Aasted, A., Lund, C., Badsberg, E., Christoffersen, I., Jacobsen,M., Skov Jensen, B., Ludwigsen, E., Paulsen, P., Paulsen, S.M. and Vejlsted, H.Bronchial Carcinoid Tumors—A Clinicopathologic Study of 82 Cases. Scand JThor Cardiovasc Surg 1985;19:105-111
Biggs, J., Hersperger, E., Steeg, P.S., Liotta, L.A. and Shearn, A. A DrosophilaGene That Is Homologous to a Mammalian Gene Associated with TumorMetastasis Codes for a Nucleoside Diphosphate Kinase. Cell 1990;63:933-940
Bishopric, G.A., Jr. and Ordóñez, N.G. Carcinoembryonic Antigen in PrimaryCarcinoid Tumors of the Lung. Cancer 1986;58:1316-1320
Bonato, M., Cerati, M., Pagani, A., Papotti, M., Bosi, F., Bussolati, G. andCapella, C. Differential diagnostic patterns of lung neuroendocrine tumours—Aclinico-pathological and immunohistochemical study of 122 cases. VirchowsArch A 1992;420:201-211
Brambilla, E., Negoescu, A., Gazzeri, S., Lantuejoul, S., Moro, D., Brambilla, C.and Coll, J.-L. Apoptosis-Related Factors p53, Bcl2, and Bax in NeuroendocrineLung Tumors. Am J Pathol 1996;149:1941-1952
56
Brazeau, P., Vale, W., Burgus, R., Ling, N., Butcher, M., Rivier, J. andGuillemin, R. Hypothalamic Polypeptide That Inhibits the Secretion ofImmunoreactive Pituitary Growth Hormone. Science 1973;179:77-79
Böhm, J., Koch, S., Gais, P., Jütting, U., Präuer, H.W. and Höfler, H. PrognosticValue of Mib-1 in Neuroendocrine Tumours of the Lung. J Pathol 1996;178:402-409
Capella, C., Heitz, P.U., Höfler, H., Solcia, E. and Klöppel, G. RevisedClassification of Neuroendocrine Tumors of the Lung, Pancreas and Gut.Digestion 1994;55(suppl 3):11-23
Carretta, A., Chiesa, G., Magnani, P., Songini, C., Melloni, G., Zannini, P. andGrossi, A. Imaging of bronchial carcinoid tumors associated to Cushingsyndrome with 111In-Octreoscan scintigraphy and immunoscintigraphy withchromogranin monoclonal antibodies. Report of two cases. J Cardiovasc Surg1997;38:191-194
Castellani, M., Reschini, E., Gasparini, M. and Gerundini, P. Indium-111Pentetreotide Lung Uptake in Infectious Lung Disease. Clin Nucl Med1999;24:343-345
Chiti, A., Fanti, S., Savelli, G., Romeo, A., Bellanova, B., Rodari, M., vanGraafeiland, B.J., Monetti, N. and Bombardieri, E. Comparison of somatostatinreceptor imaging, computed tomography and ultrasound in the clinicalmanagement of neuroendocrine gastro-entero-pancreatic tumours. Eur J NuclMed 1998;25:1396-1403
Christiansen, H., Sahin, K., Berthold, F., Hero, B., Terpe, H.-J. and Lampert, F.Comparison of DNA Aneuploidy, Chromosome 1 Abnormalities, MYCNAmplification and CD44 Expression as Prognostic Factors in Neuroblastoma.Eur J Cancer 1995;31A:541-544
Chughtai, T.S., Morin, J.E., Sheiner, N.M., Wilson, J.A. and Mulder, D.S.Bronchial carcinoid—Twenty years’ experience defines a selective surgicalapproach. Surgery 1997;122:801-808
57
Colby, T.V. Carcinoid and Other Neuroendocrine Tumors. , Tumors of theLower Respiratory Tract, Atlas of Tumor Pathology. 1994; Vol. 3rd: pp. 287-317, Armed Forces Instute of Pathology, Bethesda
Combaret, V., Lasset, C., Frappaz, D., Bouvier, R., Thiesse, P., Rebillard, A.-C.,Philip, T. and Favrot, M.C. Evaluation of CD44 Prognostic Value inNeuroblastoma: Comparison With the Other Prognostic Factors. Eur J Cancer1995;31A:545-549
Coppola, D., Clarke, M., Landreneau, R., Weyant, R.J., Cooper, D. and Yousem,S.A. Bcl-2, p53, CD44, and CD44v6 isoform expression in neuroendocrinetumors of the lung. Mod Pathol 1996;9:484-490
Cuttitta, F., Carney, D.N., Mulshine, J., Moody, T.W., Fedorko, J., Fischler, A.and Minna, J.D. Bombesin-like peptides can function as autocrine growth factorsin human small-cell lung cancer. Nature 1985;316:823-826
Cutz, E., Chan, W. and Track, N.S. Bombesin, calcitonin and leu-enkephalinimmunoreactivity in endocrine cells of human lung. Experientia 1981;37:765-767
Davila, D.G., Dunn, W.F., Tazelaar, H.D. and Pairolero, P.C. BronchialCarcinoid Tumors. Mayo Clin Proc 1993;68:795-803
Debelenko, L.V., Brambilla, E., Agarwal, S.K., Swalwell, J.I., Kester, M.B.,Lubensky, I.A., Zhuang, Z., Guru, S.C., Manickam, P., Olufemi, S.-E.,Chandrasekharappa, S.C., Crabtree, J.S., Kim, Y.S., Heppner, C., Burns, A.L.,Spiegel, A.M., Marx, S.J., Liotta, L.A., Collins, F.S., Travis, W.D. and Emmert-Buck, M.R. Identification of MEN1 gene mutations in sporadic carcinoid tumorsof the lung. Hum Mol Genet 1997;6:2285-2290
Dosaka-Akita, H., Cagle, P.T., Hiroumi, H., Fujita, M., Yamashita, M., Sharma,A., Kawakami, Y. and Benedict, W.F. Differential Retinoblastoma andp16(INK4A) Protein Expression in Neuroendocrine Tumors of the Lung. Cancer2000;88:550-556
58
Dusmet, M.E. and McKneally, M.F. Pulmonary and Thymic Carcinoid Tumors.World J Surg 1996;20:189-195
El-Naggar, A.K., Ballance, W., Abdul Karim, F.W., Ordõñez, N.G., McLemore,D., Giacco, G.G. and Batsakis, J.G. Typical and Atypical BronchopulmonaryCarcinoids—A Clinicopathologic and Flow Cytometric Study. Am J Clin Pathol1991;95:828-834
Eriksson, B. and Öberg, K. An update of the medical treatment of malignantendocrine pancreatic tumors. 1993;32:203-208
Eriksson, B.K., Larsson, E.G., Skogseid, B.M., Löfberg, A.-M., Lörelius, L.-E.and Öberg, K.E. Liver Embolizations of Patients with Malignant NeuroendocrineGastrointestinal Tumors. Cancer 1998;83:2293-2301
Ezzat, S., Asa, S.L., Stefaneanu, L., Whittom, R., Smyth, H.S., Horvath, E.,Kovacs, K. and Frohman, L.A. Somatotroph Hyperplasia without PituitaryAdenoma Associated with a Long Standing Growth Hormone-ReleasingHormone-Producing Bronchial Carcinoid. J Clin Endocrinol Metab 1994;78:555-560
Ferguson, M.K., Landreneau, R.J., Hazelrigg, S.R., Altorki, N.K., Naunheim,K.S., Zwischenberger, J.B., Kent, M. and Yim, A.P.C. Long-term outcome afterresection for bronchial carcinoid tumors. Eur J Cardiothorac Surg 2000;18:156-161
Feyrter, F. Über die Argyrophilie des Helle-Zelle-Systems in Bronchialbaum desMenschen. Z Mikrosk Anat Forsch 1954;61
Fontanini, G., Vignati, S., Bigini, D., Mussi, A., Lucchi, M., Angeletti, C.A.,Basolo, F. and Bevilacqua, G. Bcl-2 protein: a prognostic factor inverselycorrelated to p53 in non-small-cell lung cancer. Br J Cancer 1995;71:1003-1007
Frank, M., Klose, K.J., Wied, M., Ishaque, N., Schade-Brittinger, C. and Arnold,R. Combination Therapy With Octreotide and α-interferon: Effect on TumorGrowth in Metastatic Endocrine Gastroenteropancreatic Tumors. Am JGastroenterol 1999;94:1381-1387
59
Fraser, R.G., Paré, J.A.P., Paré, P.D., Fraser, R.S. and Genereux, G.P. NeoplasticDisease of the Lung (neoplasms of pulmonary neuroendocrine cells). , Diagnosisof Diseases of the Chest. 1989; : pp. 1476-1494, Saunders, Philadelphia
Friedrichs, K., Franke, F., Lisboa, B.-W., Kügler, G., Gille, I., Terpe, H.-J.,Hölzel, F., Maass, H. and Günthert, U. CD44 Isoforms Correlate with CellularDifferentiation but not with Prognosis in Human Breast Cancer. Cancer Res1995;55:5424-5433
Frölich, F. Die "Helle Zelle" der Bronchialschleimhaut und ihre Beziehungenzum Problem der Chemoreceptoren. Frankfurter Z Pathol 1949;60:517-559
Fujita, N., Yaegashi, N., Ide, Y., Sato, S., Nakamura, M., Ishiwata, I. andYajima, A. Expression of CD44 in Normal Human versus Tumor EndometrialTissues: Possible Implication of Reduced Expression of CD44 in Lymph-Vascular Space Involvement of Cancer Cells. Cancer Res 1994;54:3922-3928
Fukayama, M., Hayashi, Y., Koike, M., Hajikano, H., Endo, S. and Okumura, H.Human Chorionic Gonadotropin in Lung and Lung Tumors.Immunohistochemical Study on Unbalanced Distribution of Subunits. Lab Invest1986;55:433-443
Garcia-Yuste, M., Matilla, J.M., Alvarez-Gago, T., Duque, J.L., Heras, F.,Cerezal, L.J., Ramos, G. Prognostic Factors in Neuroendocrine Lung Tumors: ASpanish Multicenter Study. Ann Thorac Surg 2000;70:258-263
Gazzeri, S., Brambilla, E., Negoescu, A., Thoraval, D., Veron, M., Moro, D. andBrambilla, C. Overexpression of nucleoside diphosphate/kinase A/nm23-H1protein in human lung tumors: association with tumor progression in squamouscarcinoma. Lab Invest 1996;74:158-167
Gerdes, J., Schwab, U., Lemke, H. and Stein, H. Production of a MouseMonoclonal Antibody Reactive With a Human Nuclear Antigen Associated WithCell Proliferation. Int J Cancer 1983;31:13-20
60
Gilles, A.-M., Presecan, E., Vonica, A. and Lascu, I. Nucleoside DiphosphateKinase from Human Erythrocytes. Structural characterization of the twopolypeptide chains responsible for heterogeneity of the hexameric enzyme. J BiolChem 1991;266:8784-8789
Ginsberg, R.J. Carcinoid Tumors. In: T.W. Shields (ed.), General ThoracicSurgery. 1994; : pp. 1287-1297, Williams&Wilkins, Baltimore
Givehchian, M., Woerner, S.M., Lacroix, J., Zöller, M., Drings, P., Becker, H.,Kayser, K., Ridder, R. and von Knebel Doeberitz, M. Expression of CD44 splicevariants in normal respiratory epithelium and bronchial carcinomas: no evidencefor altered CD44 splicing in metastasis. Oncogene 1996;12:1137-1144
Godwin, J.D., II. Carcinoid Tumors. An Analysis of 2837 Cases. Cancer1975;36:560-569
Gould, V.E. and Linnoila, R.I. Pulmonary neuroepithelial bodies, neuroendocrinecells, and pulmonary tumors. Hum Pathol 1982;13:1064-1066
Gould, V.E., Linnoila, R.I., Memoli, V.A. and Warren, W.H. NeuroendocrineComponents of the Bronchopulmonary Tract: Hyperplasias, Dysplasias, andNeoplasms. Lab Invest 1983;49:519-537
Gouyer, V., Gazzeri, S., Bolon, I., Drevet, C., Brambilla, C. and Brambilla, E.Mechanism of Retinoblastoma Gene Inactivation in the Spectrum ofNeuroendocrine Lung Tumors. Am J Respir Cell Mol Biol 1998;18:188-196
Gouyer, V., Gazzeri, S., Brambilla, E., Boulon, I., Moro, D., Perron, P., Benabid,A.L. and Brambilla, C. Loss of Heterozygosity at the Rb Locus Correlates withLoss of Rb Protein in Primary Malignant Neuro-Endocrine Lung Carcinomas. IntJ Cancer 1994;58:818-824
Granberg, D., Stridsberg, M., Seensalu, R., Eriksson, B., Lundqvist, G., Öberg,K. and Skogseid, B. Plasma Chromogranin A in Patients with MultipleEndocrine Neoplasia Type 1. J Clin Endocrinol Metab 1999;84:2712-2717
61
Granberg, D., Wilander, E., Stridsberg, M., Granerus, G., Skogseid, B. andÖberg, K. Clinical symptoms, hormone profiles, treatment and prognosis inpatients with gastric carcinoids. Gut 1998;43:223-228
Granerus, G., Lindell, S.E., Waldenström, J., Westling, H. and White, T.Histamine metabolism in carcinoidosis. Lancet 1966;:1267-1268
Gusterson, B.A., Gullick, W.J., Venter, D.J., Powles, T.J., Elliott, C., Ashley, S.,Tidy, A. and Harrison, S. Immunohistochemical localization of c-erbB-2 inhuman breast carcinoma. Mol Cell Probes 1988;2:383-391
Günthert, U. CD44: A Multitude of Isoforms with Diverse Functions. CurrTopics Microbiol Immunol 1993;184:47-63
Harpole, D.H., Jr., Feldman, J.M., Buchanan, S., Young, W.G. and Wolfe, W.G.Bronchial Carcinoid Tumors: A Retrospective Analysis of 126 Patients. AnnThorac Surg 1992;54:50-55
Heitz, P.U., von Herbay, G., Klöppel, G., Komminoth, P., Kasper, M., Höfler,H., Müller, K.-M. and Oberholzer, M. The Expression of Human ChorionicGonadotropin (hCG) by Nontrophoblastic, Nonendocrine, and EndocrineTumors. Am J Clin Pathol 1987;88:467-472
Hensel, C.H., Hsieh, C.-L., Gazdar, A.F., Johnson, B.E., Sakaguchi, A.Y.,Naylor, S.L., Lee, W.-H. and Lee, E.Y.-H.P. Altered Structure And Expressionof the Human Retinoblastoma Susceptibility Gene in Small Cell Lung Cancer.Cancer Res 1990;50:3067-3072
Higashiyama, M., Doi, O., Yokouchi, H., Kodama, K., Nakamori, S., Tateishi, R.and Kimura, N. Immunohistochemical analysis of nm23 gene product/NDPkinase expression in pulmonary adenocarcinoma: lack of prognostic value. Br JCancer 1992;66:533-536
Huber, R.M., Schopohl, J., Losa, M., Wolfram, G., Thetter, O., Permanetter, W.and v. Werder, K. Growth-Hormone Releasing Hormone in a BronchialCarcinoid. Cancer 1991;67:2538-2542
62
Hurt, R. and Bates, M. Carcinoid tumours of the bronchus: a 33 year experience.Thorax 1984;39:617-623
Hällgren, R., Lundqvist, G. and Chance, R.E. Serum levels of human pancreaticpolypeptide in renal disease. Scand J Gastroenterol 1977;12:923-927
Ichikawa, T., Ichikawa, Y., Dong, J., Hawkins, A.L., Griffin, C.A., Isaacs, W.B.,Oshimura, M., Barrett, J.C. and Isaacs, J.T. Localization of metastasis suppressorgene(s) for prostatic cancer to the short arm of human chromosome 11. CancerRes 1992;52:3486-3490
Jiang, S.-X., Kameya, T., Sato, Y., Yanase, N., Yoshimura, H. and Kodama, T.Bcl-2 Protein Expression in Lung Cancer and Close Correlation withNeuroendocrine Differentiation. Am J Pathol 1996;148:837-846
Jiang, S.-X., Sato, Y., Kuwao, S. and Kameya, T. Expression of bcl-2 OncogeneProtein is Prevalent in Small Cell Lung Carcinomas. J Pathol 1995;177:135-138
Joensuu, H., Klemi, P.J., Toikkanen, S. and Jalkanen, S. Glycoprotein CD44Expression and Its Association with Survival in Breast Cancer. Am J Pathol1993;143:867-874
Jones, D.J., Hasleton, P.S. and Moore, N. DNA ploidy in bronchopulmonarycarcinoid tumours. Thorax 1988;43:195-199
Kaufmann, M., Heider, K.-H., Sinn, H.-P., von Minckwitz, G., Ponta, H. andHerrlich, P. CD44 variant exon epitopes in primary breast cancer and length ofsurvival. Lancet 1995;345:615-619
Koerker, D.J., Ruch, W., Chideckel, E., Palmer, J., Goodner, C.J., Ensinck, J. andGale, C.C. Somatostatin: Hypothalamic Inhibitor of the Endocrine Pancreas.Science 1973;184:482-484
Krausz, Y., Bar-Ziv, J., de Jong, R.B.J., Ish-Shalom, S., Chisin, R., Shibley, N.and Glaser, B. Somatostatin-Receptor Scintigraphy in the Management ofGastroenteropancreatic Tumors. Am J Gastroenterol 1998;93:66-70
63
Kvols, L.K. Therapy of the Malignant Carcinoid Syndrome. Endocrinol MetabClin North Am 1989;18:557-568
Kwekkeboom, D.J. and Krenning, E.P. Radiolabeled somatostatin analogscintigraphy in oncology and immune diseases: an overview. Eur Radiol1997;7:1103-1109
Kwekkeboom, D.J., Krenning, E.P., Bakker, W.H., Oei, H.Y., Kooij, P.P.M. andLamberts, S.W.J. Somatostatin analogue scintigraphy in carcinoid tumours. Eur JNucl Med 1993;20:283-292
Kwekkeboom, D.J., Krenning, E.P., Kho, G.S., Breeman, W.A. and Van Hagen,P.M. Somatostatin receptor imaging in patients with sarcoidosis. Eur J Nucl Med1998;25:1284-1292
Kwekkeboom, D.J., van Urk, H., Pauw, B.K.H., Lamberts, S.W., Kooij, P.P.M.,Hoogma, R.P.L.M. and Krenning, E.P. Octreotide Scintigraphy for the Detectionof Paragangliomas. J Nucl Med 1993;34:873-878
Kälkner, K.-M., Tiensuu Janson, E., Nilsson, S., Carlsson, S., Öberg, K. andWestlin, J.-E. Somatostatin Receptor Scintigraphy in Patients with CarcinoidTumors: Comparison between Radioligand Uptake and Tumor Markers. CancerRes 1995;55:5801s-5804s
Laitinen, K.L.J., Soini, Y., Mattila, J. and Paakko, P. AtypicalBronchopulmonary Carcinoids Show a Tendency Toward Increased Apoptoticand Proliferative Activity. Cancer 2000;88:1590-1598
Lau, S.K., Johnson, D.S. and Coel, M.N. Imaging of Non-Small-Cell LungCancer With Indium-111 Pentetreotide. Clin Nucl Med 2000;25:24-28
Lauweryns, J.M. and Peuskens, J.C. Neuro-epithelial Bodies (Neuroreceptor orSecretory Organs?) in Human Infant Bronchial and Bronchiolar Epithelium. AnatRec 1972;172:471-481
64
Lohmann, D., Fesseler, B., Pütz, B., Reich, U., Böhm, J., Präuer, H., Wünsch,P.H. and Höfler, H. Infrequent Mutations of the p53 Gene in PulmonaryCarcinoid Tumors. Cancer Res 1993;53:5797-5801
Mackay, C.R., Terpe, H.-J., Stauder, R., Marston, W.L., Stark, H. and Günthert,U. Expression and Modulation of CD44 Variant Isoforms in Humans. J Cell Biol1994;124:71-82
Magid, D., Siegelman, S.S., Eggleston, J.C., Fishman, E.K. and Zerhouni, E.A.Pulmonary Carcinoid Tumors: CT Assessment. J Comput Assist Tomogr1989;13:244-247
Mansi, L., Rambaldi, P.F., Panza, N., Esposito, D., Esposito, V. and Pastore, V.Diagnosis and radioguided surgery with 111In-pentetreotide in a patient withparaneoplastic Cushing's syndrome due to a bronchial carcinoid. Eur JEndocrinol 1997;137:688-690
Mayer, B., Jauch, K.W., Günthert, U., Figdor, C.G., Schildberg, F.W., Funke, I.and Johnson, J.P. De-novo expression of CD44 and survival in gastric cancer.Lancet 1993;342:1019-1022
McCaughan, B.C., Martini, N. and Bains, M.S. Bronchial carcinoids—Review of124 cases. J Thorac Cardiovasc Surg 1985;89:8-17
McDowell, E.M., Barrett, L.A. and Trump, B.F. Observations on Small GranuleCells in Adult Human Bronchial Epithelium and in Carcinoid and Oat CellTumors. Lab Invest 1976;34:202-206
Memoli, V.A., Linnoila, I., Warren, W.H., Rios-Dalenz, J. and Gould, V.E.Hyperplasia of Pulmonary Neuroendorine Cells and Neuroepithelial Bodies(abstr). Lab Invest 1983;48:57A
Mendonça, C., Baptista, C., Ramos, M. and Yglesias de Oliveira, J.Ã. Typicaland Atypical Lung Caarcinoids: Clinical and Morphological Diagnosis. MicroscRes Tech 1997;38:468-472
65
Modlin, I.M. and Sandor, A. An Analysis of 8305 Cases of Carcinoid Tumors.Cancer 1997;79:813-829
Moertel, C.G. and Hanley, J.A. Combination chemotherapy trials in metastaticcarcinoid tumor and the malignant carcinoid syndrome. Cancer Clin Trials1979;2:327-334
Moertel, C.G., Hanley, J.A. and Johnson, L.A. Streptozocin Alone ComparedWith Streptozocin Plus Fluorouracil in the Treatment of Advanced Islet-CellCarcinoma. N Engl J Med 1980;303:1189-1194
Moertel, C.G., Kvols, L.K., O´Connell, M.J. and Rubin, J. Treatment ofNeuroendocrine Carcinomas With Combined Etoposide and Cisplatin. Evidenceof Major Therapeutic Activity in the Anaplastic Variants of These Neoplasms.Cancer 1991;68:227-232
Moertel, C.G., Lefkopoulo, M., Lipsitz, S., Hahn, R.G. and Klaassen, D.Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in thetreatment of advanced islet-cell carcinoma. N Engl J Med 1992;326:519-523
Mokuno, Y., Katoh, T., Yoshida, K., Kamiya, S., Chigira, H. and Maeda, M.Liver Metastasis Nineteen Years After Surgery for Typical Bronchial Carcinoid.Hepatogastroenterology 1999;46:2961-2964
Mulder, J.-W.R., Kruyt, P.M., Sewnath, M., Oosting, J., Seldenrijk, C.A.,Weidema, W.F., Offerhaus, G.J.A. and Pals, S.T. Colorectal cancer prognosisand expression of exon-v6-containing CD44 proteins. Lancet 1994;344:1470-1472
Musi, M., Carbone, R.G., Bertocchi, C., Cantalupi, D.P., Michetti, G., Pugliese,C. and Virotta, G. Bronchial carcinoid tumours: a study on clinicopathologicalfeatures and role of octreotide scintigraphy. Lung Cancer 1998;22:97-102
Mårtensson, H., Böttcher, G., Hambraeus, G., Sundler, F., Willen, H. and Nobin,A. Bronchial Carcinoids: An Analysis of 91 Cases. World J Surg 1987;11:356-364
66
O’Byrne, K.J., Ennis, J.T., Freyne, P.J., Clancy, L.J., Prichard, J.S. and Carney,D.N. Scintigraphic imaging of small-cell lung cancer with [111In]pentetreotide, aradiolabelled somatostatin analogue. Br J Cancer 1994;69:762-766
O’Connor, D.T. and Deftos, L.J. Secretion of chromogranin A by peptide-producing endocrine neoplasms. N Engl J Med 1986;314:1145-1151
Okike, N., Bernatz, P.E. and Woolner, L.B. Carcinoid Tumors of the Lung. AnnThorac Surg 1976;22:270-277
Oltvai, Z.N., Milliman, C.L. and Korsmeyer, S.J. Bcl-2 Heterodimerizes In Vivowith a Conserved Homolog, Bax, That Accelerates Programmed Cell Death. Cell1993;74:609-619
Onuki, N., Wistuba, I.I., Travis, W.D., Virmani, A.K., Yashima, K., Brambilla,E., Hasleton, P. and Gazdar, A.F. Genetic Changes in the Spectrum ofNeuroendocrine Lung Tumors. Cancer 1999;85:600-607
Padberg, B.-C., Woenckhaus, J., Hilger, G., Beccu, L., Jochum, W., Range, U.,Kastendieck, H. and Schröder, S. DNA Cytophotometry and Prognosis inTypical and Atypical Bronchopulmonary Carcinoids. Am J Surg Pathol1996;20:815-822
Paladugu, R.R., Benfield, J.R., Pak, H.Y., Ross, R.K. and Teplitz, R.L.Bronchopulmonary Kulchitzky Cell Carcinomas. Cancer 1985;55:1303-1311
Pelosi, G., Bresaola, E., Bogina, G., Pasini, F., Rodella, S., Castelli, P., Iacono,C., Serio, G. and Zamboni, G. Endocrine Tumors of the Pancreas: Ki-67Immunoreactivity on Paraffin Sections is an Independent Predictor forMalignancy: A Comparative Study With Proliferating-Cell Nuclear Antigen andProgesterone Receptor Protein Immunostaining, Mitotic Index, and OtherClinicopathologic Variables. Hum Pathol 1996;27:1124-1134
Penno, M.B., August, J.T., Baylin, S.B., Mabry, M., Linnoila, R.I., Lee, V.S.,Croteau, D., Yang, X.L. and Rosada, C. Expression of CD44 in Human LungTumors. Cancer Res 1994;54:1381-1387
67
Phlipponneau, M., Nocaudie, M., Epelbaum, J., de Keyzer, Y., Lalau, J.D.,Marchandise, X. and Bertagna, X. Somatostatin Analogs for the Localization andPreoperative Treatment of an Adrenocorticotropin-Secreting Bronchial CarcinoidTumor. J Clin Endocrinol Metab 1994;78:20-24
Postema, P.T.E., Krenning, E.P., Wijngaarde, R., Kooy, P.P.M., Oei, H.Y., vanden Bosch, W.A., Reubi, J.-C., Wiersinga, W.M., Hooijkaas, H., van der Loos,T., Poublon, R.M.L., Lamberts, S.W.J. and Henneman, G. [111In-DTPA-D-Phe1] octreotide scintigraphy in thyroidal and orbital Graves' disease: Aparameter for disease activity? J Clin Endocrinol Metab 1994;79:1845-1851
Ranchod, M. and Levine, G.D. Spindle-cell carcinoid tumors of the lung—aclinicopathologic study of 35 cases. Am J Surg Pathol 1980;4:315-331
Rea, F., Binda, R., Spreafico, G., Calabrò, F., Bonavina, L., Cipriani, A., DiVittorio, G., Fassina, A. and Sartori, F. Bronchial Carcinoids: A Review of 60Patients. Ann Thorac Surg 1989;47:412-414
Reisinger, I., Bohuslavitzki, K.H., Brenner, W., Braune, S., Dittrich, I., Geide,A., Kettner, B., Otto, H.-J., Schmidt, S. and Munz, D.L. Somatostatin ReceptorScintigraphy in Small-Cell Lung Cancer: Results of a Multicenter Study. J NuclMed 1998;39:224-227
Reubi, J.-C., Waser, B., van Hagen, M., Lamberts, S.W., Krenning, E.P.,Gebbers, J.-O. and Laissue, J.A. In vitro and in vivo detection of somatostatinreceptors in human malignant lymphomas. Int J Cancer 1992;50:895-900
Ricci, C., Patrassi, N., Massa, R., Mineo, C. and Benedetti-Valentino, F., Jr.Carcinoid Syndrome in Bronchial Adenoma. Am J Surg 1973;126:671-677
Roncalli, M., Springall, D.R., Varndell, I.M., Gaitonde, V.V., Hamid, Q.,Ibrahim, N.B.N., Grimelius, L., Wilander, E., Polak, J.M. and Coggi, G.Oncoprotein immunoreactivity in human endocrine tumours. J Pathol1991;163:117-127
68
Scherübl, H., Bäder, M., Fett, U., Hamm, B., Schmidt-Gayk, H., Koppenhagen,K., Dop, F.-J., Riecken, E.-O. and Wiedenmann, B. Somatostatin-ReceptorImaging of Neuroendocrine Gastroenteropancreatic Tumors. Gastroenterology1993;105:1705-1709
Screaton, G.R., Bell, M.V., Bell, J.I. and Jackson, D.G. The Identification of aNew Alternative Exon with Highly Restricted Tissue Expression in TranscriptsEncoding the Mouse Pgp-1 (CD44) Homing Receptor. J Biol Chem1993;268:12235-12238
Screaton, G.R., Bell, M.V., Jackson, D.G., Cornelis, F.B., Gerth, U. and Bell, J.I.Genomic structure of DNA encoding the lymphocyte homing receptor CD44reveals at least 12 alternatively spliced exons. Proc Natl Acad Sci USA1992;89:12160-12164
Shi, W., Johnston, C.F., Buchanan, K.D., Ferguson, W.R., Laird, J.D., Crothers,J.G. and McIlrath, E.M. Localization of neuroendocrine tumours with [111In]DTPA-octreotide scintigraphy (Octreoscan): a comparative study with CT andMR imaging. QJM 1998;91:295-301
Soga, J. and Yakuwa, Y. Bronchopulmonary Carcinoids: An Analysis of 1,875Reported Cases with Special Reference to a Comparison between TypicalCarcinoids and Atypical Varieties. Ann Thorac Cardiovasc Surg 1999;5:211-219
Spencer, H. Rare Pulmonary Tumours. , Pathology of the Lung. 1985; Vol. 2: pp.934-946, Pergamon Press, Oxford
Stahl, J.A., Leone, A., Rosengard, A.M., Porter, L., King, C.R. and Steeg, P.S.Identification of a Second Human nm23 gene, nm23-H2. Cancer Res1991;51:445-449
Stamatis, G., Freitag, L. and Greschuchna, D. Limited and radical resection fortracheal and bronchopulmonary carcinoid tumour. Report on 227 cases. Eur JCardiothorac Surg 1990;4:527-532
69
Stauder, R., Eisterer, W., Thaler, J. and Günthert, U. CD44 Variant Isoforms inNon-Hodgkin´s Lymphoma: A New Independent Prognostic Factor. Blood1995;85:2885-2899
Steeg, P.S., Bevilacqua, G., Kopper, L., Thorgeirsson, U.P., Talmadge, J.E.,Liotta, L.A. and Sobel, M.E. Evidence for a Novel Gene Associated With LowTumor Metastatic Potential. J Natl Cancer Inst 1988;80:200-204
Stefani, A., Morandi, U., Urgese, A.L., Rivasi, F. and Lodi, R. Carcinoid tumorsof the lung. An analysis of 65 operated cases. J Cardiovasc Surg (Torino)1999;40:607-612
Stridsberg, M., Hellman, U., Wilander, E., Lundqvist, G., Hellsing, K. andÖberg, K. Fragments of chromogranin A are present in the urine of patients withcarcinoid tumors: development of a specific radioimmunoassay for chromograninA and its fragments. J Endocrinol 1993;139:329-337
Stridsberg, M., Öberg, K., Li, Q., Engström, U. and Lundqvist, G. Measurementof chromogranin A, chromogranin B (secretogranin I), chromogranin C(secretogranin II) and pancreastatin in plasma and urine from patients withcarcinoid tumours and endocrine pancreatic tumours. J Endocrinol 1995;144:49-59
Tabarin, A., Valli, N., Chanson, P., Bachelot, Y., Rohmer, V., Bex-Bachellerie,V., Catargi, B., Roger, P. and Laurent, F. Usefulness of Somatostatin ReceptorScintigraphy in Patients with Occult Ectopic Adrenocorticotropin Syndrome. JClin Endocrinol Metab 1999;84:1193-1202
Tateishi, R. Distribution of Argyrophil Cells in Adult Human Lungs. Arch Pathol1973;96:198-202
Terpe, H.-J., Christiansen, H., Gonzalez, M., Berthold, F. and Lampert, F.Differentiation and Prognosis of Neuroblastoma in Correlation to the Expressionof CD44s. Eur J Cancer 1995;31A:549-552
70
Terpe, H.-J., Koopman, R., Imhof, B.A. and Günthert, U. Expression of IntegrinsAnd CD44 Isoforms in Non-Hodgin´s Lymphomas: CD44 Variant Isoforms ArePreferentially Expressed in High-Grade Malignant Lymphomas. J Pathol1994;174:89-100
Terpe, H.-J., Störkel, S., Zimmer, U., Anquez, V., Fischer, C., Pantel, K. andGünthert, U. Expression of CD44 Isoforms in Renal Cell Tumors. PositiveCorrelation to Tumor Differentiation. Am J Pathol 1996;148:453-463
Thunnissen, F.B.J.M., van Eijk, J., Baak, J.P.A., Schipper, N.W., Uyterlinde,A.M., Breederveld, R.S. and Meijer, S. Bronchopulmonary Carcinoids andRegional Lymph Node Metastases—A Quantitative Pathologic Investigation.Am J Pathol 1988;132:119-122
Tiensuu Janson, E., Stridsberg, M., Gobl, A., Westlin, J.-E. and Öberg, K.Determination of Somatostatin Receptor Subtype 2 in Carcinoid Tumors byImmunohistochemical Investigation with Somatostatin Receptor Subtype 2Antibodies. Cancer Res 1998;58:2375-2378
Tiensuu Janson, E., Westlin, J.-E., Eriksson, B., Ahlström, H., Nilsson, S. andÖberg, K. [111In-DTPA-D-Phe1]octreotide scintigraphy in patients withcarcinoid tumours: the predictive value for somatostatin analogue treatment. EurJ Endocrinol 1994;131:577-581
Tokunaga, Y., Urano, T., Furukawa, K., Kondo, H., Kanematsu, T. and Shiku, H.Reduced Expression of nm23-H1, But Not of nm23-H2, is Concordant With theFrequency of Lymph-Node Metastasis of Human Breast Cancer. Int J Cancer1993;55:66-71
Torpy, D.J., Chen, C.C., Mullen, N., Doppman, J.L., Carrasquillo, J.A.,Chrousos, G.P. and Nieman, L.K. Lack of Utility of (111)In-PentetreotideScintigraphy in Localizing Ectopic ACTH Producing Tumors: Follow-Up of 18Patients. J Clin Endocrinol Metab 1999;84:1186-1192
Torre, M., Barberis, M., Barbieri, B., Bonacina, E. and Belloni, P. Typical andatypical bronchial carcinoids. Respir Med 1989;83:305-308
71
Travis, W.D., Linnoila, R.I., Tsokos, M.G., Hitchcock, C.L., Cutler, G.B., Jr.,Niemann, L., Chrousos, G., Pass, H. and Doppman, J. Neuroendocrine Tumors ofthe Lung With Proposed Criteria for Large-Cell Neuroendocrine Carcinoma. AnUltrastructural, Immunohistochemical, and Flow Cytometric Study of 35 Cases.Am J Surg Patol 1991;15:529-553
Travis, W.D., Rush, W., Flieder, D.B., Falk, R., Fleming, M.V., Gal, A.A. andKoss, M.N. Survival Analysis of 200 Pulmonary Neuroendocrine Tumors WithClarification of Criteria for Atypical Carcinoid and Its Separation From TypicalCarcinoid. Am J Surg Pathol 1998;22:934-944
Tsutsumi, Y. Expression of the Alpha Subunit of Human ChorionicGonadotropin in Normal and Neoplastic Neuroendocrine Cells. AnImmunohistochemical Study. Acta Pathol Jpn 1989;39:413-419
Tsutsumi, Y., Osamura, R.Y., Watanabe, K. and Yanihara, N. Simultaneousimmunohistochemical localization of gastrin-releasing peptide (GRP) andcalcitonin (CT) in human bronchial endocrine-type cells. Virchows Arch A1983;400:163-171
Tsutsumi, Y., Osamura, Y., Watanabe, K. and Yanihara, N.Immunohistochemical Studies on Gastrin-Releasing Peptide- andAdrenocorticotropic Hormone-Containing Cells in the Human Lung. Lab Invest1983;48:623-632
Vadasz, P., Palffy, G., Egervary, M. and Schaff, Z. Diagnosis and treatment ofbronchial carcinoid tumors: clinical and pathological review of 120 operatedpatients. Eur J Cardio-thorac Surg 1993;7:8-11
Valli, M., Fabris, G.A., Dewar, A., Hornall, D. and Sheppard, M.N. Atypicalcarcinoid tumour of the lung: a study of 33 cases with prognostic features.Histopathology 1994;24:366-369
Walch, A.K., Zitzelsberger, H.F., Aubele, M.M., Mattis, A.E., Bauchinger, M.,Candidus, S., Prauer, H.W., Werner, M. and Höfler, H. Typical and AtypicalCarcinoid Tumors of the Lung Are Characterized by 11q Deletions as Detectedby Comparative Genomic Hybridization. Am J Pathol 1998;153:1089-1098
72
Warren, W.H. and Gould, V.E. Long-Term Follow-up of Classical BronchialCarcinoid Tumors. Clinicopathologic Observations. Scand J Thorac CardiovascSurg 1990;24:125-130
Warren, W.H., Gould, V.E., Faber, L.P., Kittle, C.F. and Memoli, V.A.Neuroendocrine neoplasms of the bronchopulmonary tract. A classification of thespectrum of carcinoid to small cell carcinoma and intervening variants. J ThoracCardiovasc Surg 1985;89:819-825
Warren, W.H., Memoli, V.A. and Gould, V.E. Immunohistochemical andUltrastructural Analysis of Bronchopulmonary Neuroendocrine Neoplasms. I.Carcinoids. Ultrastruct Pathol 1984;6:15-27
Warren, W.H., Memoli, V.A. and Gould, V.E. Immunohistochemical andUltrastructural Analysis of Bronchopulmonary Neuroendocrine Neoplasms. II.Well-Differentiated Neuroendocrine Carcinomas. Ultrastruct Pathol 1984;7:185-199
Weiss, M., Yellin, A., Huza’r, M., Eisenstein, Z., Bar-Ziv, J. and Krausz, Y.Localization of Adrenocorticotropic Hormone-secreting Bronchial CarcinoidTumor by Somatostatin-Receptor Scintigraphy. Ann Int Med 1994;121:198-199
Westlin, J.-E., Tiensuu Janson, E., Ahlström, H., Nilsson, S., Öhrvall, U. andÖberg, K. Scintigraphy Using a 111Indium-labeled Somatostatin Analogue forLocalization of Neuroendoccrine Tumors. Antibody, Immunoconj. Radiopharm.1992;5:367-384
Wielenga, V.J.M., Heider, K.-H., Offerhaus, G.J.A., Adolf, G.R., van den Berg,F.M., Ponta, H., Herrlich, P. and Pals, S.T. Expression of CD44 Variant Proteinsin Human Colorectal Cancer Is Related to Tumor Progression. Cancer Res1993;53:4754-4756
Wilander, E., Lundqvist, M. and El-Salhy, M. Serotonin in Fore-Gut Carcinoids.A Survey of 60 Cases With Regard to Silver Stains, Formalin-InducedFluorescence and Serotonin Immunocytochemistry. J Pathol 1985;145:251-258
73
Willey, J.C., Lechner, J.F. and Harris, C.C. Bombesin and the C-TerminalTetradecapeptide of Gastrin-releasing Peptide are Growth Factors for NormalHuman Bronchial Epithelial Cells. Exp Cell Res 1984;153:245-248
Williams, E.D. and Sandler, M. The classification of carcinoid tumors. Lancet1963;1:238-239
Wright, C., Angus, B., Nicholson, S., Sainsbury, J.R.C., Cairns, J., Gullick, W.J.,Kelly, P., Harris, A.L. and Horne, C.H.W. Expression of c-erbB-2 Oncoprotein:A Prognostic Indicator in Human Breast Cancer. Cancer Res 1989;49:2087-2090
Yamada, Y., Kagimoto, S., Kubota, A., Yasuda, K., Masuda, K., Someya, Y.,Ihara, Y., Li, Q., Imura, H., Seino, S. and Seino, Y. Cloning, functionalexpression and pharmacological characterization of a fourth (hSSTR4) and a fifth(hSSTR5) human somatostatin receptor subtype. Biochem Biophys Res Commun1993;195:844-852
Yamada, Y., Post, S.R., Wang, K., Tager, H.S., Bell, G.I. and Seino, S. Cloningand functional characterization of a family of human and mouse somatostatinreceptor expressed in brain, gastrointestinal tract and kidney. Proc Natl Acad SciUSA 1992;89:251-255
Yamada, Y., Reisine, T., Law, S.F., Ihara, Y., Kubota, A., Kagimoto, S., Seino,M., Seino, Y., Bell, G.I. and Seino, S. Somatostatin receptors, an expanding genefamily; cloning and functional characterization of human SSTR3, a proteincoupled to adenylyl cyclase. Mol Endocrinol 1992;6:2136-2142
Yamaguchi, A., Urano, T., Fushida, S., Furukawa, K., Nishimura, G., Yonemura,Y., Miyazaki, I., Nakagawara, G. and Shiku, H. Inverse association of nm23-H1expression by colorectal cancer with liver metastasis. Br J Cancer 1993;68:1020-1024
Yamaguchi, A., Urano, T., Goi, T., Takeuchi, K., Niimoto, S., Nakagawara, G.,Furukawa, K. and Shiku, H. Expression of Human nm23-H1 and nm23-H2Proteins in Hepatocellular Carcinoma. Cancer 1994;73:2280-2284
74

Zhao, J., de Krijger, R.R., Meier, D., Speel, E.-J.M., Saremaslani, P., Muletta-Feurer, S., Matter, C., Roth, J., Heitz, P.U. and Komminoth, P. GenomicAlterations in Well-Differentiated Gastrointestinal and BronchialNeuroendocrine Tumors (Carcinoids) : Marked Differences Indicating Diversityin Molecular Pathogenesis. Am J Pathol 2000;157:1431-1438
Öberg, K. and Wide, L. HCG and HCG-subunits as tumour markers in patientswith endocrine pancreatic tumours and carcinoids. Acta Endocrinol (Copenh)1981;98:256-260
75