Embed Size (px)
Citation preview

DOI: 10.5604/01.3001.0009.6004 WWW.PPCH.PL50
case report
Penetrating trauma of the face and facial skeleton – a case series of six patientsAneta Neskoromna-Jędrzejczak1, Katarzyna Bogusiak1, Aleksander Przygoński1, Bogusław Antoszewski2
1Department of Craniomaxillofacial and Oncological Surgery, Medical University of Lodz, Kopcińskiego 22, 90-153 Łódź, Poland; Head: Aneta Neskoromna-Jędrzejczak 2Department of Plastic, Reconstructive and Aesthetic Surgery, Medical University of Lodz, Kopcińskiego 22, 90-153 Łódź, Poland; Head: Bogusław Antoszewski
Article history: Received: 08.03.2016 Accepted: 16.01.2017 Published: 28.02.2017
ABSTRACT: Penetrating traumas of the facial skeleton are relatively rare; however, they can be dangerous and even life-threaten-ing. The epidemiology of facial skeleton trauma is diverse and depends on the affected region, age, and the kind of foreign body that caused the injury. In Poland, the most common cause of penetrating traumas are accidents and as-saults, and only rarely accidents are related to improper use of firecrackers or fireworks.
The aim of this study is to present a literature review and our own experience with penetrating traumas of the face and the facial part of the cranium.
Six cases with severe wounds and fractures of the facial skeleton were treated between the years 2000 and 2012 in our department. The applied treatment methods depended mainly on the general condition of the patients. In all cases, we achieved acceptable functional and aesthetic outcomes.
KEYWORDS: penetrating trauma, maxillofacial trauma
INTRODUCTION
Penetrating traumas of the facial skeleton are not considered to be a frequent condition. The available literature does not pro-vide detailed epidemiological data on penetrating traumas of the face, and it only consists of single case studies or case se-ries. Based on the available literature, craniocerebral injuries that penetrate through the orbital cavity into the neurocrani-um are particularly dangerous in children (1) and adults (2).
Depending on a country, the causes of penetrating traumas are different. In the USA, the majority of penetrating trauma cases are due to gunshots (3), and other causes include suicide attempts, self-mutilation, traffic accidents, and dog bites (3). In Poland, gunshot injuries (including those caused by gunshots and explosions of firecrackers) account for a small percent-age of (0.62% – 1.5%) facial skeleton trauma cases (4), and the most frequent causes of penetrating traumas are due to traffic accidents, accidents at work, or physical assaults (3) with the use of sharp, narrow, and long objects that easily enter the thin bones of the facial skeleton, and especially of the orbital cavity.
Penetrating traumas of the face and facial skeleton can be di-vided into low-energy and high-energy traumas (5, 6). Obvi-ously, the bigger the mass and speed of the offending foreign body, the greater is the kinetic energy and the extent of injury in the bones and soft tissues. Bone injuries are characterised by the presence of small and compound fractures. High-ener-gy traumas may be caused by gunshots (small mass and high speed of the bullet contribute to high kinetic energy) or fire-cracker bursts (associated with high kinetic energy and high temperatures). On the other hand, injuries caused by stabbing with a long, thin, and sharp foreign body are usually low-ener-gy, but they also can cause penetrating wounds, although not as extended as in the case of high-energy traumas.
Based on the available literature, the location of fracture is as-sociated with the type of trauma and the age of patients. For instance, traumas within the orbital cavity are found mostly in children and young people, and sport activity is the most common cause of injuries in this age group, followed by phys-ical assault, traffic accidents, and accidents at work (7). On the other hand, penetrating traumas of the orbital cavity in adults

51POL PRZEGL CHIR, 2017: 89 (1), 50-60
penetrating trauma of the face and facial skeleton – a case series of six patients
are incurred during fights and due to stabbing with a sharp object (2). Suicide attempts with the use of firearms usually lead to traumas in the submandibular area, submental area, and oral cavity (8).
The aim of this study is to present our experience with treat-ment of patients with penetrating traumas of the facial skeleton.
Between the years 2000 and 2012, 2319 people were hospital-ized in our department due to traumas of the facial skeleton, including only 6 patients with penetrating traumas. Facial In-jury Severity Scale (FISS) was used to evaluate the degree of facial injuries. The parameters comprising FISS are present-ed in Table I (9).
CASE 1
After performing diagnostic imaging and excluding coexist-ing injuries, a 50-year-old patient (D.K) with a pickaxe stab in the subtemporal area, between the zygomatic arch and the right orbital cavity, was transferred in a good condition to the department of craniofacial surgery for further treatment (Fig. 1) On admission, the patient was in a good condition, remained conscious and in good logical and verbal contact (GCS – 15 points), circulatory and respiratorily competent, with pulse equalling 100 bpm (regular and symmetrical) and was well palpable on the circumference, BP was 95/60 mm Hg, and oxygen saturation was 90%. The patient did not have any chronic diseases before the accident. On the physical ex-amination, the patient did not have limb paralysis, meningeal symptoms or other neurological symptoms, rhinorrhea, or bleeding on the wall of the pharynx. There was a pickaxe that was stabbed in the facial skeleton, with the blade stuck in the right subtemporal area, penetrating through the zygomat-ic, buccal, and subnasal area on the right side. The pickaxe reached the left buccal area, causing embossing and tension of buccal soft tissues, tension of the skin in that area, and a small bleeding from the post-traumatic wound. The pickaxe was causing lockjaw and gradual loss of vision in the right eye. On FISS, the injuries were assessed as 6 points. Before surgery, the patient was consulted with ophthalmologists who diagnosed post-traumatic blindness in the right eye, lack of light perception, wide pupil without reaction to light, and im-mobile eyeball due to the presence of a foreign body. CT of the head and facial skeleton, with 3D reconstructions, revealed a large, metal foreign body. Numerous artifacts were seen on the CT scans that were caused by the presence of a massive metallic foreign body, which considerably impaired the eval-uation of the brain and fractures within the facial skeleton. Therefore, only a partial evaluation of the brain was possible,
but intracranial bleeding was excluded (Fig. 2). The patient underwent emergency surgery that was preceded by trache-ostomy under local anaesthesia. Then, under general anaes-thesia, the posttraumatic wound around the stuck blade was surgically widened and the pickaxe was removed. No bleeding from large or medium blood vessels was observed. The blade of the pickaxe in the right subtemporal area passed through the right maxillary sinus, subnasal area, and then penetrat-
Tab. I. Facial Injury Severity Scale – FISS
PARAMETER FINDING POINTS
facial laceration≤ 10 cm 0
>10 cm 1
fracture of the orbital roof or rim present 1
fracture into frontal sinus or bonenon-displaced
1
displaced 5
dento-alveolar injury of the maxilla present 1
Le Fort fracture
Le Fort I 2
Le Fort II 4
Le Fort III 6
naso-orbital-ethmoid (NOE) fractures 3
zygomatico-maxillary complex (ZMC) fracture 1
nasal fracture (alone) 1
dento-alveolar injury of mandible 1
fracture of mandibular body, ramus and/or symphysis
2 × number of fractures
fracture of mandibular subcondyle, condyle or coronoid process
2 × number of fractures
Fig. 1. Patient D.K. with a wound in the subtemporal area between the zygomatic arch and the right orbital cavity.

WWW.PPCH.PL52
case report
ed the lumen of the left maxillary sinus, fracturing its later-al wall and finally reaching the soft tissues of the left cheek. During the procedure, the patient was diagnosed with frac-ture of the lateral wall of the right orbital cavity with a 2-cm intermediate splinter, fracture of the lower wall of the right orbital cavity and zygomatic arch on the right side, defect on the orbital floor (5 mm from the anterior edge to orbital cone), and fracture of the anterior wall of the right maxillary sinus. After clearing all bone splinters from the wound, bone fragments were repositioned and immobilized with plates and screws, enabling reconstruction of the lateral and the lower edge of the right orbital cavity. The orbital wall was recon-structed with a titanium mesh. Hemostasis was achieved af-ter electrocoagulation of small vessels. The post-operative wound was sutured in layers. Due to infection within the post-operative wound related to contamination of the for-eign body, during the procedure, the operating team decided that a 2-stage surgery should be performed, and reconstruc-tion of the zygomatic arch and maxillary bone was delayed. The patient received antibiotics (ceftazidime, 1g once every 8 hours for 6 days) in the intensive care unit (ICU), where he was transferred immediately after surgery. In the ICU, the patient was fed through a naso-gastric tube and was sedat-ed with continuous intravenous infusion of fentanyl (100µg/hour), midazolam (2mg/hour), and thiopental (2mg/hour). Dexamethasone was given at an initial dose of 24mg per day, and then was continued at decreasing doses for 7 days. Post-operative dressing changes were performed every day. Based on wound swab culture results, ceftazidime was changed to oral perfloxacin (400mg every 12 hours) for 9 days. Due to a satisfactory esthetic effect, the patient resigned from the sec-ond stage of management. The patient was hospitalized for 15 days (Fig. 3). The sutures were removed before discharge. We obtained a very good functional outcome with regression
of blindness in the right eye (acuity and field of vision as be-fore the injury, without diplopia) and normal jaw opening.
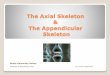
CASE 2
A 59-year-old patient (D.R) incurred an extensive wound of the facial soft tissues and facial skeleton due to a suicide at-tempt with a hunting weapon (the rifle was placed in the left submandibular area) (Fig. 4). On admission, the patient was in a critical condition, unconscious and with hemorrhagic shock (GCS – 8 points). The patient was intubated and sedated with thiopental. In the emergency room (ER), the patient suffered a cardiac arrest, and was successfully resuscitated. The exam-ination of the site of injury revealed a vast, slicing wound with uneven and lacerated edges, considerable loss of soft tissues, rupture of the buccal mucous membrane, facial muscles, and blood vessels that were covering the submandibular area, sub-mental area, and the left cheek (FISS – 6 points). CT of the head and facial skeleton revealed a gunshot fracture in the body of the mandible, next to a complex and small splinter fracture in the ramus of the mandible on the left side, with the loss of the mandibular bone in the area from tooth 35 to the angle of the mandible, zygomatic bone fracture, and fracture of the bot-tom of the left orbital cavity. The patient underwent emergency surgery under general anaesthesia with endotracheal intuba-
Fig. 2. CT scan of a patient stabbed with a pickaxe.
Fig. 3. Patient D.K. 15 days after surgery.

53POL PRZEGL CHIR, 2017: 89 (1), 50-60
penetrating trauma of the face and facial skeleton – a case series of six patients
acacia branch with thorns, which revealed a wound within the suborbital area on the right side that penetrated into the lu-men of the maxillary sinus. The wound was sutured in layers. We administered two antibiotics - lincosamide (600mg i.v. every 8 hours) and metronidazole (500mg i.v. every 8 hours). Cleansing of the surgical wound with boric acid and changing of dressing with neomycin-containing ointment was performed every day. The patient was discharged on the 4th day in a good general and local condition.
CASE 4
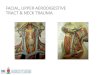
A 53-year-old patient (H.Ż) was hit by a grinder stone, and as a result, he incurred a penetrating trauma within the area of the middle, the upper facial skeleton, and fractures of the frontal sinus bone on the right side, right orbital cavity, maxillary si-nus on the right side, nasal bone, and bone at the basis of the anterior cranial fossa; the right eyeball was damaged (FISS – 11 points). Immediately after the trauma, the condition of the patient was critical. The patient was disorientated and dis-turbed, with tachycardia (120 bpm) but without respiratory distress (GCS – 12 points).
CT revealed a foreign body (fragment of a grinder stone) and complex fractures of the walls in the frontal sinus, maxillary si-nus, right orbital cavity, and nasal bone. The patient underwent emergency surgery on the day of the trauma under endotracheal anesthesia. During surgery, the foreign body was removed from the right orbital cavity, numerous bone splinters were removed from the right frontal sinus, orbital cavity, maxillary sinus, part of the nasal bone, and the eyeball (Fig. 7). Bone loss within the wall of the frontal sinus was reconstructed with TachoComb, and tissue loss in the orbital cavity was filled with muscle tissue
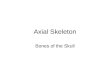
tion. During surgery, the gunshot wound was revised, while the bleeding blood vessels were tied off and underpinned, the ruptured submandibular and sublingual salivary glands were removed, and bone splinters were removed from the wound (Fig. 5). Then, the wound was sutured in layers, and reconstruc-tion of the left cheek was performed. During the procedure, the patient received a transfusion of 2 units of RBCC and 2 units of plasma. In the ICU, the patient was sedated with an continu-ous intravenous infusion of fentanyl (100µg/hour), midazolam (2mg/hour), and thiopental (2mg/hour). The patient received amoxicillin with clavulanic acid (1.2g i.v. every 12 hours) and metronidazole (500mg every 8 hours). Intraoral and extraoral dressings were changed every day. After 7 days, the patient was discharged in a good condition, with local symptoms of facial nerve paresis on the left side (lagophthalmos of the left eye, drooping of the left corner of the mouth, and large facial asymmetry) (Fig. 6).
CASE 3
A 32-year-old patient (K.R.) incurred a penetrating injury in the area of the right orbital cavity after he fell from his bicycle on an acacia branch. The patient reported to the hospital on the 3rd day after the trauma. On admission, the patient was in a good condition, with no disturbances of consciousness (GCS 15 points), and with no neurological symptoms. The patient had oedema of the eyelid in the right eye, and an acacia branch was stuck in the wound. Imaging did not reveal any fracture of the bone in the right orbital cavity, and only fracture of the anterior and lateral walls of the right maxillary sinus was ob-served. The injuries were estimated at 1 point on the FISS scale. Clearance of blood clots from the wound was performed un-der general anaesthesia. We removed a 30-cm fragment of the
Tab. II. Craniofacial injuries in patients 1-6 with the total score of Facial Injury Severity Scale – FISS
PATIENT FRACTURES TOTAL SCORE
LENGTH OF STAY IN HOSPITAL
D.K.Orbital floor and side wall, zygomatic arch with bone loss, multifragmental fracture of the right maxillary sinus walls, left maxillary sinus fracture, multifragmental fracture of the right maxillary sinus walls and left maxillary sinus, walls of lower nasal passages
8 15 days
D.R. Le Fort II, mandible fracture with total bone loss around tooth 35, multifragmental fracture of the left mandibular branch. 6 7 days
K.R. Penetrating wound of the lower eyelid of the left eye to the maxillary sinus. Maxillary sinus fracture 1 4 days
H.Ż.frontal sinus bone on the right side with bone loss and displacement of bone fragments, right orbital walls, maxillary sinus on the right side, nasal bone on the right side, ethmoidal sinuses, bones of the base of the skull
11 38 days
S.J. Fracture of the frontal sinus with bone loss. 6 7 days
W.B.Fracture of the frontal sinus, frontal bone on the right side, Le Fort III, complex fracture of the bone within the upper and medial facial skeleton with interruption in the palatal suture, bones of the base of the skull, double fracture of mandibular body.
17 45 days

WWW.PPCH.PL54
case report
CASE 6
A 44-year-old patient (W.B.) was transferred to the ER in a crit-ical condition due to multiple injuries of the craniofacial skele-ton that had been caused by a hit with a firecracker in the area of the right eyeball (the patient was leaning over the firecracker when it exploded). In the ER, the patient was confused but able to answer questions, opened eyes to pain, and displayed pur-poseful responses to pain (GCS – 11). Since the patient was in
and fatty tissue harvested from the right abdominal region. Af-ter rejuvenating edges of the wound and performing hemosta-sis, the wound was sutured in layers. Frontal tamponades were applied due to nasal bone fractures. During the procedure, the patient received a transfusion of 3 units of RBCC and 3 units of plasma. Directly after the procedure, the patient was transferred to the ICU, where he was started on antibiotics (ceftazidime, 1g once every 8 for 6 days). In the ICU, the patient was fed through a naso-gastric tube and was sedated with continuous intrave-nous infusion of fentanyl (100µg/hour), midazolam (2mg/hour), and thiopental (2mg/hour).
Postoperative dressing changes were performed every day during hospital stay. The frontal tamponade was removed af-ter 48 hours. After 10 days, the patient was transferred to our department.
The patient was discharged after 38 days of hospitalization in a good condition, with a recommendation of further follow-up on an outpatient basis. He was also recommended to undergo reconstructive procedures in the future.
CASE 5
A 55-year-old patient (S.J.) was admitted after incurring a pen-etrating trauma of the face due to a hit with a chainsaw in the forehead area. Directly after the trauma, the patient was in a critical condition, with tachycardia (over 120 bpm), tachypnea, BP of 80/90 mmHg, and oxygen saturation of 90%. He opened his eyes to pain, used inappropriate verbal responses, and had purposeful movements to painful stimuli (GCS – 10 points). Before the accident, the patient did not have any chronic dis-eases. The local examination revealed a wound in the forehead area, passing slightly obliquely into the nasal area on the right side, with uneven and lacerated edges (FISS – 6 points). The patient underwent surgery under endotracheal anaesthesia on the day of the accident. During the procedure, the wound and the left frontal sinus were revised. The observed bone loss in the anterior part of the frontal sinus was covered with a pol-yurethane sheet. Communication with the frontal sinus was through the left nasal duct, and a drain was introduced through this route. The drain was sutured to the left nasal wing. Hemo-stasis of the vessels was performed. The wound was sutured in layers. The course of treatment was uneventful. The wound was healing and the patient had the drain for 5 days. We adminis-tered two antibiotics, lincosamide (600mg i.v. every 8 hours) and metronidazole (500mg i.v. every 8 hours). On the 7th day after surgery, the patient was discharged with a recommenda-tion for further ambulatory care.
Fig. 4. Patient D.R. with a gunshot injury.
Fig. 5. Patient D.R. - intraoperative view.

55POL PRZEGL CHIR, 2017: 89 (1), 50-60
penetrating trauma of the face and facial skeleton – a case series of six patients
carried out. Additional orthopedic treatment was also imple-mented (laboratory rail and flexible elevator). The post-opera-tive course was uneventful. The patient was discharged on the 45th day after the injury in a good condition with recommen-dations for further ambulatory treatment.
DISCUSSION
Currently, there is a growing number of deaths related to trau-matic injuries. Based on epidemiological data, trauma is the third commonest cause of death. In Poland, nearly 30,000 people die due to trauma each year, whilst this number in the Netherlands is two times smaller. In contrast, in Hungary and in France this figure can be even higher than in Poland (10). Although there are no detailed epidemiological data concerning the frequency of penetrating trauma within the facial skeleton, many authors emphasize that they are extremely rare. In our experience, they comprise only 0.26% of all facial skeleton trauma cases.
Patients with penetrating trauma of the face are at risk of incur-ring injury of important anatomical structures of the nervous system, respiratory system, peripheral nervous system, or visual
post-traumatic shock, anti-shock treatment was implemented. On the local examination, there was a vast wound of the face that involved soft tissues of the cheek, zygomatic area on the right side, eyelids of the right eye, right eyeball, upper lip, skin of the lateral nasal surface on the right side, mucous membrane of the hard palate in the medial line, and the upper gingiva in the area between tooth 11 and tooth 21. It was also revealed that the patient had fracture of the right frontal bone, complex fracture of the bone within the upper and medial facial skeleton with interruption in the palatal suture, and double fracture of the mandibular body. The patient also experienced an injury of the cornea, sclera, and had detached retina in the left eye. The patient had complete blindness of the left eye. Addition-ally, the patient was also diagnosed with I˚ skin burn (<5% of the body surface). The overall FISS score was 12 points. The patient underwent emergency surgery under general anaes-thesia. The facial wounds were surgically managed, small bone splinters and foreign bodies were removed, and fractures of the maxilla and the mandible were temporarily managed with the figure-of-8-ligature (ligatures). Drains were inserted in the right maxillary sinus and in both frontal sinuses, and anterior and posterior tamponades were performed. Subsequently, we removed the ruptured right eyeball. Due to exacerbation of symptoms of hemorrhagic shock and worsening of the overall condition, the previously scheduled surgical osteosynthsis of the fractures within the facial skeleton was delayed, and 3 units of RBCC were transfused. Directly after the procedure, the pa-tient was transferred to the ICU, where the patient underwent tracheostomy and was started on mechanical ventilation. The patient was sedated with continuous intravenous infusion of fentanyl (100µg/hour), midazolam (2mg/hour), and thiopen-tal (2mg/hour). The patient was treated with ceftazidime (1g every 8 hours for 6 days). During subsequent hospitalization, the overall condition of the patient improved. Then, the patient was transferred to a department of neurosurgery in order to undergo plastic surgery of the anterior cranial fossa because of leakage of cerebrospinal fluid. The procedure was done un-der general anaesthesia, through bifrontal craniotomy and an intradural approach with cranialization of the frontal sinuses. Reconstruction of the anterior cranial fossa was performed with the use of alloplastic material (codubix). The lacerations of the dura matter were surgically closed and supplied with Tachocomb. The soft tissues above that area were sutured in layers. In the neurosurgical ward, the patient was started on oral pefloxacin (400mg every 12 hours). Only on the 17th day of hospitalization, the overall condition of the patient was sta-ble enough to perform the maxillofacial surgery. During this procedure, osteosynthesis of fractures within the mandibular body was performed, fractures of the lateral and lower rims of the orbital cavities were managed with titanium plates, and reconstruction of the orbital walls with titanium sheet was
Fig. 6.Patient D.R. 7 days after surgery.

WWW.PPCH.PL56
case report
the least frequent trauma cases, since they were observed only in 2 cases. As regards the discussed cases of penetrating trauma, 3 patients were diagnosed with fractures of the the frontal sinus, and according to the FISS scale, these were qualified as fractures of the upper facial skeleton. These fractures were associated with other injuries within the facial skeleton – fractures of the maxilla (Le Fort II or Le Fort III) and fractures of the walls of the orbital cavity, naso–orbito–ethmoidal complex, anterior cranial fossa, and the body of the mandible. These resulted from high-ener-gy penetrating trauma caused by a grinder stone, chainsaw, or a firecracker. Therefore, the scope of the penetrating injuries within the facial skeleton observed in our patients differs from the typ-ical location of facial traumas that is described in the literature. It is well known that the most frequent location of trauma in the facial skeleton is the nose and the mandible (i.e., areas within the massive middle and lower facial skeleton (13)).
Penetrating traumas are associated with a significant risk of in-fection due to the mode of injury and the presence of foreign bodies in the wound. Moreover, many authors emphasize that injuries within the frontal sinuses are associated with a particu-larly high risk of inflammatory complications, and they are fre-quently associated with other fractures of the facial skeleton (1). In that respect, penetrating trauma within the upper facial skel-eton may lead to a situation when an inflammatory condition can expand towards the central nervous system (meningitis and brain abscesses), not to mention cranial cerebral penetrating in-juries, when the risk of inflammation is extremely high (14). Due to presence of a foreign body, all injuries of soft tissues are classi-fied as infected wounds (15). Other factors that increase the risk of infection are injuries of the mucous membrane, long surgery times (more than 2 hours), and delayed treatment (when surgery starts after 4 hours since injury) (15). All of the above-presented patients received antibiotics. In those who were not hospital-ized in the ICU, we routinely used lincosamide with metronida-
and circulatory systems. This can lead to long-term disability or even death due to hemorrhagic shock, damage of cerebral structures, or inflammatory complications. The consequences of penetrating trauma depend on the affected anatomical struc-tures, the scope of penetration, impact and direction of the of-fending foreign body, and resistance of tissues affected by the trauma. In our experience, trauma with the highest FISS score was caused by a firecracker explosion (12 points), followed by a grinder stone injury (11 points). Apart from extensive facial wounds, these injuries also led to serious damage within more than one anatomic structure in the bones of the frontal sinus-es, maxilla, naso–orbito–ethmoidal complex, and mandible.
In the case of head trauma, penetrating foreign bodies lose their energy due to absorption by internal anatomical struc-tures. Trauma within the scope of the facial skeleton may cause dreadfully appearing external injuries; however, because the energy is absorbed by bone structures, post-traumatic injuries cover a much smaller extent than when the traumatic force im-pacts on the cranial vault.
As regards facial injuries caused by sharp objects, they may lead to massive bleeding from damaged blood vessels. It is worth remembering that a foreign body constitutes a certain tampon for the damaged blood vessel, and quite often, the removal of the foreign body leads to a massive bleeding. Penetrating trau-mas within the facial skeleton may cause physical injuries of the brain, calvarial fracture, fractures within the anterior cranial fossa, and rupture of the dura matter with subsequent rhinor-rhea. The complex anatomical structure of the facial skeleton and of the neck, together with the surrounding blood vessels and the nervous system, requires precise, individually planned, and multi-specialist management.
Patients with intracranial pneumatocele and rhinorrhea con-firmed on CT require a thorough observation in order to ex-clude symptoms of increased intracranial pressure. Intracranial hemorrhage poses a direct threat to life and often requires emer-gency neurosurgery. What is more, the presence of post-trau-matic fistula may be associated with infections, which is why patients require wide-spectrum antibiotics.
Some authors emphasize that even in patients admitted in a good condition, who were not diagnosed with post-traumat-ic changes in the CNS on initial CT, a follow-up CT scan may reveal such changes in 44% of patients. This confirms the need to perform repeated imaging in order to monitor the dynam-ics of changes (11, 12).
The majority of our patients had fractures within the upper facial skeleton (4/6 cases) (Table II). Massive lower facial injuries were
Fig. 7. Patient H.Ż. who was hit by a grinder stone - intraoperative view.

57POL PRZEGL CHIR, 2017: 89 (1), 50-60
penetrating trauma of the face and facial skeleton – a case series of six patients
age of the dura matter and may result in omission of the orig-inal rhinorrhea source. One disadvantage of this approach is a limited view into the anterior cranial base. Indications for the epidural access are limited and include rhinorrhea from a known location and postoperative rhinorrhea in the sell-ar area (34). Otherwise, intradural approach (preferred op-tion) provides full view of the anterior cranial fossa, i.e., both wings of the sphenoid bone are visible to the anterior clinoid processes, upper orbital floor, and ethmoid wall. Usually, bi-frontal craniotomy and cranialization of the frontal sinuses is performed in order to prevent the formation of cyst lining and subsequent infections. In the intradural approach, intraopera-tive administration of mannitol and gravitational effect of the frontal lobes reduce the need for retraction of the frontal lobes and minimize the risk of complications such as hematoma or impaired sense of smell.
There are various methods of surgical closure of lacerations in the dura matter. The simplest method is to sew up the dura matter. As regards reconstruction, different materials can be used, like adipose tissue, muscle, fascia lata, cartilage of the nasal septum, vascularized portion of a epicranial aponeuro-sis or artificial dura (35). Dura matter lacerations can also be fixed by sewing or fibrin glue. Spongostan and TachoSil can be applied as additional sealing materials. The final choice of material depends on the severity of the defect and the type of trauma. In patients with otorrhea, the choice of surgical ap-proach depends on the source of liquorrhea - the middle or posterior cranial cavity. If the fistula is located in the posteri-or cranial cavity, surgical treatment with an approach through or behind the mastoid process can be performed. If the lac-eration of dura matter is located in the middle cranial fossa, an approach above the ear at the level of the middle temporal gyrus is performed, which allows to view the base of the skull.
If dura matter lacerations necessitate surgical treatment, it is preferred to manage that during a single-stage operation to-gether with repositioning of the facial bone fractures and soft tissue wound closure.
CONCLUSIONS:
Diagnostic and therapeutic work-up in patients with penetrat-ing trauma within the facial skeleton should include coopera-tion between specialists in the fields of maxillofacial surgery, ophthalmology, laryngology, neurology, neurosurgery, plastic surgery, and anaesthesiology.
The patient is usually in critical condition and requires immediate implementation of proper diagnostic work-up and management.
zole. For patients transferred to the intensive medical care unit, antibiotics were implemented in accordance with the policy of the committee for infections in our hospital that is based on the profile of drug resistance and epidemiological data regarding the ICU (ceftazidime or amoxicillin with clavulanic acid, and metronidazole). In the presented group of patients, we did not observe any intracranial inflammatory complications. Except for local and systemic infectious complications (e.g., meningi-tis, wound infections, intracranial abscesses), other common complications include fluid fistulas, hydrocephalus, epilepsy, and intracranial hematomas (16).
Patients with penetrating injuries may be in various general con-ditions. Nevertheless, the ‘ABC’ (Airway, Breathing, Circulation) scheme should be performed before transporting the patient and on admission. This procedure should be followed by further di-agnostic work-up, including CT and, if necessary, angiography (in the case of penetrating injuries reaching the central nervous system in order to exclude possible vascular abnormalities and injuries). Preoperative angiography is recommended only for pa-tients in a stable general and neurological condition (16). It was observed that around 30% of patients with penetrating head and brain trauma have complications due to injuries of veins and arter-ies of the CNS (16). Unfortunately, a short period of preparation often does not allow to perform angiography (17). Full diagnos-tic work-up can be carried out only when the patient’s condition is stable. In most cases, there is not enough time to perform all diagnostic tests. Also, detailed history can be difficult to obtain. Sometimes, penetrating traumas are caused by small objects that can be neglected by the injured person. Such cases of trauma can be asymptomatic and cause phlegmon after many years (16).
The prognosis in patients with penetrating facial trauma depends on the clinical condition of the patient. The mortality rate in pa-tients with GCS 3- 8 ranges between 60 and 90%. For patients with higher GCS (between 9 and 15), the risk of fatal complications is below 10% (18). The prognosis is worse in patients with rhinor-rhea who require craniotomy. The use of transcranial approach is correlated with the mortality risk 0 to 6% (19, 20, 21). The risk of rhinorrhea recurrence varies between 5 to 32% (22, 23, 24). Re-construction of the anterior cranial fossa can be also done with the use of endoscopic approach (25). Endoscopic techniques, in comparison to classical external approaches to cranial fossa, give a better field of view with enhanced illumination and magnifica-tion. The positioning of the underlay or overlay grafts is also more accurate (26-31). There are different endoscopic approaches ded-icated to access different areas – transfrontal, transcribriform, transplanum, transsellar, transclival, and transpterygoid (32, 33).
As regards craniotomy, both intra- and epidural approach is used. Epidural access often leads to further iatrogenic dam-

WWW.PPCH.PL58
case report
In special circumstances, when there is a strong suspicion that the contaminated foreign body may infect wounds, it is rec-ommended to implement a 2-stage management.
Depending on the overall condition of the injured patient, the management may slightly differ. Lifesaving procedures, such as anti-shock therapy and closure of wounds, are most important.
REFERENCES1. Nowosławska E, Polis L, Mikołajczyk W, et al.: Urazy drążące twarzo- i
mózgoczaszki u dzieci w oparciu o doświadczenia własne Kliniki Neuro-chirurgii ICZMP. Rocznik Dziecięcej Chirurgii Urazowej 2002: 6: 74-80.
2. Abraszko R, Zub L, Wroński J, et al.: Transorbital penetrating brain in-juries in the clinical material of the Department of Neurosurgery, Uni-versity of Medicine, Wrocław, Poland. Pol Przegl Chir 1997: 266-271
3. Czyżewski P, Blok T, Błaszczyk M, et al.: Penetrating injuries – rare ca-ses of head and brain trauma. Neuroskop 2006; 8: 53-60.
4. Lewandowski B, Kulig T: Gunshot Injuries of Face and Facial Cranium – Personal Cases. Dent Med Probl 2005; 42(2): 371-377.
5. Bartlett CS, Helfet DL, Hausman MR, et al.: Ballistics and gunshot wounds: effects on musculoskeletal tissues. J Am Acad Orthop Surg 2000; 8: 21-36.
6. Chen AY, Stewart MG, Raup G: Penetrating injuries of the face. Oto-laryngol Head Neck Surg 1996; 115: 464-470.
7. Samolczyk - Wanyura D: Epidemiological, clinical and radiological eva-luation of patients treated for isolated fractures of the floor of the orbit – the authors’ own observations. Czas Stomatol 2005; 58(5): 343-349.
8. Lewandowski B, Kulig T: Postrzałowe obrażenia twarzy i czaszki twa-rzowej - przypadki własne. Dent Med Probl 2005; 42(2): 371-377.
9. Bagheri SC, Dierks EJ, Kademani D, et al.: Application of a facial in-jury severity scale in craniomaxillofacial trauma. J Oral Maxillofac Surg 2006; 64: 408-414.
10. Centers for Disease Control and Prevention, National Center for In-jury Prevention and Control. Web–based Injury Statistics Query and Reporting System (WISQARS) http://www.cdc.gov/injury/wisqars. June 9, 2014.
11. Aremu SK, Makusid MM, Ibe IC: Oro-cranial penetrating pencil inju-ry. Ann Saudi Med 2012; 32(5): 534-536
12. Bell RB, Osborn T, Potter BE, et al.: Management of penetrating inju-res: a new paradigm for civilian trauma. J Oral Maxillofac Surg 2007; 65(4): 691-705.
13. Hwang K, You SH: Analysis of facial bone fractures: An 11-year study of 2,094 patients. Indian J Plast Surg 2010; 43(1): 42-48.
14. Seider N, Gilboa M, Lautman E, Miller B: Delayed presentation of or-bito-cerebral abscess caused by pencil-tip injury. Ophthal Plst Reconstr Surg 2006; 4: 316-317.
15. Rekomendacje diagnostyki, terapii i profilaktyki antybiotykowej za-każeń w szpitalu. Edit. Hryniewicz W, Ozorowskiego T. Ministry of Health, Warsaw, 2015.
16. Trask T, Narajan RK: Management of penetrating head injuries. W: The Practice of Neurosurgcry. Red. G.T. Tindall, Williams&Wilkins Electronic, Baltimore, 1998
17. Greenberg MS: Non-missle penetrating trauma. Handbook of Neuro-surgery. Fifth Edition. New York 2001, 676-677.
18. Zafonte RD, Wood DL, Harrison-Felix CL, Millis SR, Valena NV: Se-vere Penetrating Head Injury: A Study of Outcomes. Arch Phys Med Rehabil. 2001; 82: 306-310.
19. Cairns H: Injuries of the frontal and ethmoidal sinuses with special reference to cerebrospinal fluid rhinorrhea and aeroceles. J Laryngol Otol. 1937; 52: 589-623.
20. Friedman JA, Ebersold MJ, Quast LM: Post-traumatic cerebrospinal fluid leakage. World J Surg. 2001; 25: 1062-1066.
21. Rocchi G, Caroli E, Belli E, Salvati M, Cimatti M, Delfini R: Severe craniofacial fractures with frontobasal involvement and cerebrospi-nal fluid fistula: indications for surgical repair. Surg Neurol. 2005; 63: 559-564.
22. Bell RB, Dierks EJ, Homer L, Potter BE: Management of cerebrospinal fluid leak associated with craniomaxillofacial trauma. J Oral Maxillo-fac Surg. 2004; 62: 676-684.
23. Laun A: Traumatic cerebrospinal fl uid fi stulas in the anterior and middle cranial fossae. Acta Neurochir. 1982; 60: 215-222.
24. Lewin W: Cerebrospinal fluid rhinorrhoea in closed head injuries. Br J Surg. 1954; 42: 1-18.
25. Scholsem M, Scholtes F, Collignon F, Robe P, Dubuisson A, Kaschten B. et al.: Surgical management of anterior cranial base fractures with cerebrospinal fluid fistulae: a single-institution experience. Neurosur-gery 2008; 62: 463-471.
26. Dodson EE, Gross CW, Swerdloff JL, Gustafson LM: Transnasal endo-scopic repair of cerebrospinal fluid rhinorrhea and skull base defects: a review of twenty-nine cases. Otolaryngol Head Neck Surg 1994; 111: 600-605.
27. Hegazy HM, Carrau RL, Snyderman CH, Kassam A, Zweig J: Transnasal endoscopic repair of cerebrospinal fluid rhinorrhea: a meta-analysis. Laryngoscope 2000; 110: 1166-1172.
28. Lee TJ, Huang CC, Chuang CC, Huang SF: Transnasal endoscopic re-pair of cerebrospinal fluid rhinorrhea and skull base defect: ten-year experience. Laryngoscope 2004; 114(8):1475-1481.
29. Lopatin AS, Kapitanov DN, Potapov AA: Endonasal endoscopic repair of spontaneous cerebrospinal fluid leaks. Arch Otolaryngol Head Neck Surg 2003; 129: 859-863.
30. Marshall AH, Jones NS, Robertson IJ: CSF rhinorrhoea: the place of endoscopic sinus surgery. Br J Neurosurg 2001; 15: 8-12.
31. Ryall RG, Peacock MK, Simpson DA: Usefulness of beta 2-transferrin assay in the detection of cerebrospinal fluid leaks following head in-jury. J Neurosurg 1992; 77:737-739.
32. Cappabianca P, Cavallo LM, Esposito F, Valente V, De Divitiis E: Sell-ar repair in endoscopic endonasal transsphenoidal surgery: results of 170 cases. Neurosurgery 2002; 51: 1365-1371.
33. Fraser JF, Nyquist GG, Moore N, Anand VK, Schwartz TH: Endoscopic endonasal minimal access approach to the clivus: case series and tech-nical nuances. Neurosurgery 2010; 67: 150-158.
34. Schmidek & Sweet: Operative Neurosurgical Techniques Indications, Methods and Results. Elsavier 2006; Vol. 1 Section II, T. Forcht Dagi, 134-135.
35. Wieloch M, Żukiel R, Nowak S, Jankowski R: Large tumors of anterior cranial base. Cranial analysis of 45 cases. Neuroskop 2003; 5: 107-111.

59POL PRZEGL CHIR, 2017: 89 (1), 50-60
penetrating trauma of the face and facial skeleton – a case series of six patients
DOI:
Table of content:
Copyright:
Competing interests:
Corresponding author:
Cite this article as:
Word count: 5000 Page count: 11 Tables: 2 Figures: 7 References: 35
10.5604/01.3001.0009.6004
http://ppch.pl/resources/html/articlesList?issueId=9609
Copyright © 2017 Fundacja Polski Przegląd Chirurgiczny. Published by Index Copernicus Sp. z o. o. All rights reserved.
The authors declare that they have no competing interests.
The content of the journal „Polish Journal of Surgery” is circulated on the basis of the Open Access which means free and limitless access to scientific data.
This material is available under the Creative Commons - Attribution 4.0 GB. The full terms of this license are available on: http://creativecommons.org/licenses/by-nc-sa/4.0/legalcode
Katarzyna Bogusiak, Department of Craniomaxillofacial and Oncological Surgery, Medical University of Lodz, Kopcińskiego 22, 90-153 Łódź, Poland; Phone: +48 42 677 67 88, Email: [email protected]
Neskoromna-Jędrzejczak A., Bogusiak K., Przygoński A., Antoszewski B.; Penetrating trauma of the face and facial skeleton – a case series of six patients; Pol Przegl Chir 2017: 89 (1): 50-60x