Embed Size (px)
Citation preview

Promoter: dr. Elisa Maina
Co-Promoter: Prof. dr. Eric Cox
Literature review as part of the
Master`s Dissertation
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
Academic year 2014-2015
Pemphigus foliaceus in dogs: the immune pathogenesis and therapies.
Why are some dogs not responsive to the treatment?
By
Marleen PETERMANN
© 2015 Marleen Petermann


Disclaimer
Universiteit Gent, its employees and/or students, give no warranty that the information provided in this
thesis is accurate or exhaustive, nor that the content of this thesis will not constitute or result in any
infringement of third-party rights.
Universiteit Gent, its employees and/or students do not accept any liability or responsibility for any use
which may be made of the content or information given in the thesis, nor for any reliance which may
be placed on any advice or information provided in this thesis.

Promoter: dr. Elisa Maina
Co-Promotor: Prof. dr. Eric Cox
Literature review as part of the
Master`s Dissertation
GHENT UNIVERSITY
FACULTY OF VETERINARY MEDICINE
Academic year 2014-2015
Pemphigus foliaceus in dogs: the immune pathogenesis and therapies.
Why are some dogs not responsive to the treatment?
By
Marleen PETERMANN
© 2015 Marleen Petermann

Preface
This report is the first part of my master thesis, which I could conduct in the fields of immunology and
dermatology. Both have always been of major interest for me so that I felt privileged that I could
deepen my knowledge as part of my study.
The realization of my literature study was enabled by professional assistance and familial support.
In the first place I wish to thank my promoter Dr. Elisa Maina for her time, interest, advice and critical
proof-reading.
I also want to thank my parents for their advice, support and for making my dream, becoming a
veterinarian, possible.

Table of contents:
Abstract .............................................................................................................................................. 1
Samenvatting ...................................................................................................................................... 2
1. Introduction ..................................................................................................................................... 3
1.1.The different forms of the pemphigus complex .................................................................. 3
1.1.1 Pemphigus vulgaris ........................................................................................... 4
1.1.2. Pemphigus vegetans ........................................................................................ 4
1.1.3.Pemphigus erythematosus ................................................................................. 4
1.1.4. Panepidermal pustular pemphigus .................................................................... 5
1.1.5. Paraneoplastic pemphigus ................................................................................ 5
2. Pemphigus foliaceus ....................................................................................................................... 6
2.1.Epidemiology .................................................................................................................... 6
2.2. Clinical signs .................................................................................................................... 6
2.3. Pathogenesis ................................................................................................................... 7
2.3.1. Involved components ........................................................................................ 7
2.3.1.1. Desmosomes: Function, ultrastructure and composition ..................... 7
2.3.1.2. Desmosal cadherins .......................................................................... 8
2.3.1.2.1. Distribution of certain desmosomal and non-desmosomal
adhesion molecules .......................................................................... 8
2.3.1.2.2. Desmoglein as a minor target auto-antigen ......................... 9
2.3.1.2.3. Desmocollin as a major target auto-antigen ..................... 10
2.3.1.2.4. Other auto-antigens ......................................................... 11
2.3.2. The role of neutrophils ................................................................................... 11
2.3.3. Antibodies....................................................................................................... 12
2.3.3.1. Antibody profile ................................................................................ 12
2.3.3.2. IgG subclasses ................................................................................ 13
2.3.3.3. Titer and severity ............................................................................. 13
2.3.3.4. Specificity of the antibodies.............................................................. 13
2.3.4. Pathophysiology ............................................................................................. 14
2.3.4.1. Introduction ..................................................................................... 14
2.3.4.2. Role of the auto-antibodies. ............................................................. 14
2.3.4.3. Proposed mechanisms ................................................................... 14
2.4. Drug-related pemphigus ................................................................................................ 17
2.4.1 Introduction...................................................................................................... 17
2.4.2. Trimethoprim-sulfonamide .............................................................................. 17
2.4.3. Promeris Duo® ............................................................................................... 17
2.4.4. Certifect :®
Fipronil-Amitraz- S-methoprene .................................................... 18

2.4.5. Vectra 3D ....................................................................................................... 18
2.4.6. Others ............................................................................................................ 19
2.5. Therapies....................................................................................................................... 19
2.5.1. Introduction..................................................................................................... 19
2.5.2. Most commonly used drugs in the treatment of cPF ........................................ 19
2.5.2.1. Corticosteroids ................................................................................ 19
2.5.2.2. Azathioprine .................................................................................... 22
2.5.2.3. Chlorambucil ................................................................................... 22
2.5.2.4. Chrysotherapy ................................................................................. 22
2.5.2.5 Tetracycline and niacinamide............................................................ 23
2.5.2.6. Mycophenolate mofetil ..................................................................... 23
2.5.2.7. Cyclosporine and tacrolimus ............................................................ 24
2.5.2.8. Cyclophosphamide .......................................................................... 25
2.5.2.9. Dapsone and sulfasalazine .............................................................. 25
3. Why are some dogs not responsive to the treatment ..................................................................... 26
3.1. Treatment outcome and long-term prognosis ................................................................. 26
3.2. Possible reasons why some dogs are not responding..................................................... 27
3.2.1. Incorrect diagnosis .......................................................................................... 28
3.2.2. Naturally or drug-related pemphigus ............................................................... 28
3.2.3. Drug regime ................................................................................................... 28
3.2.4. Glucocorticoid resistance ............................................................................... 29
3.2.5. Influence of 25-hydroxyvitamin D concentrations ............................................ 29
3.2.6. Tachyphylaxis to topical glucocorticoids, is it proven? ..................................... 29
4. Discussion .................................................................................................................................... 30
5. References ................................................................................................................................... 31

1
Abstract
This literature study reviews up-to-date knowledge on the immunopathogenesis, therapies and
prognosis of pemphigus foliaceus (PF) in dogs. PF is an auto-immune blistering skin disease
described in dogs, humans and other species. The formation of auto-antibodies, primarily IgG4,
against keratinocyte desmosomal adhesion proteins (cadherins) results in acantholysis and
intraepidermal blister formation. Desmocollin-1 was identified as the major auto-antigen and
desmoglein-1 as a minor auto-antigen. PF however appears to be a complex and multifactorial
disease where different auto-antigens, auto-antibodies and pathogenic components are involved. The
exact pathomechanism is not yet fully elucidated but different theories have been suggested. Those
include among others steric hinder by IgG-binding and thereby disabling desmosomal bond-formation;
the initiation of multistep mechanisms of intracellular events triggered by IgG-binding and also
neutrophils seem to play a pathogenic role. It is proposed that predisposing and inducing factors such
as environmental or endogenous factors, e.g. drugs, are necessary for the outbreak of the disease.
Drugs that seem to have a potential to provoke acantholysis similar to PF include trimethoprim-
sulfonamides, Certifect®, Promeris
® and Vectra 3D
®. In most dogs
remission of the lesions is achieved
with an adequate drug regime. The first-line drugs are glucocorticoids. Due to adverse drug reactions
or an insufficient response second-line medication such as azathioprine, cyclosporine or chlorambucil
are used on a regular basis. Some dogs however do not respond to the treatment. The reason
therefore is not yet known.
Key words: Autoimmunity - Blistering - Canine pemphigus foliaceus - Desmosomes - Glucocorticoids

2
Samenvatting
In deze literatuurstudie wordt gepoogd om de huidige kennis omtrent de immunopathogenese en de
verschillende therapeutische benaderingen bij canine pemphigus foliaceus samen te vatten. In het
bijzonder worden mogelijke hypothesen besproken waarom sommige honden niet op de therapie
reageren.
Pemphigus foliaceus is een auto-immune huidaandoening die onder andere bij de mens en de hond is
beschreven. Het lichaam vormt auto-antistoffen, voornamelijk IgG4, die zich tegen adhesie proteïnes
van de keratinocyten in de epidermis richten. Daardoor ontstaat acantholyse en intra-epidermale
blaarvorming. Een aantal jaar geleden kon desmocollin-1 worden aangetoond als het hoofd auto-
antigen en desmoglein-1 als een bijkomend auto-antigen. Pemphigus foliaceus bij honden blijkt een
multifactoriele aandoeningen te zijn met verschillende auto-antigenen, auto-antistoffen en
pathologische componenten. Een reeks aan pathologische mechanismen werden door onderzoekers
voorgesteld. Tot op heden is de exacte immunopathogenese echter nog niet volledig opgehelderd.
Voorgestelde mechanismen verantwoordelijk voor de acantholyse zijn onder andere sterische
hindering door auto-antistoffen die ter hoogte van de desmosomen vasthechten en de intercellulaire
verbinding tussen naburige cellen inhiberen. Ook werd de initiatie van een cascade aan intracellulaire
mechanismen, uitgelokt door IgG-binding, voorgedragen waarbij een reeks aan componenten
betrokken zou zijn. In canine pemphigus foliaceus werd bovendien de betrokkenheid van neutrofielen
aangetoond. In de klassieke humane vorm van pemphigus foliaceus is dit niet het geval.
Onderzoekers vonden daarboven indicaties dat de uitbraak van PF door endogene of exogene
factoren uitgelokt kan worden. Het best beschreven voorbeeld is een uitbraak na toediening van een
beperkt aantal geneesmiddelen. Bij de hond werden uitbraken beschreven na de toediening van
trimethoprim-sulfonamides, Certifect®, Promeris® en Vectra 3D®. Men vermoed dat genetische
factoren eveneens een rol spelen in de pathogenese, omdat sommige rassen gepredisponeerd zijn.
De therapie berust voornamelijk op immunosuppressie. Hierbij zijn glucocorticoide zoals prednisolone
de meest gebruikte farmaceutica. Door ernstige bijwerkingen of een onvoldoende respons kunnen
tweedelijns geneesmiddelen (onder andere azathioprine, cyclosporine of chlorambucil) als vervanger
of in combinatie met glucocorticoiden worden gebruikt. In een beperkt aantal gevallen treedt volledige
remissie op, in de meeste gevallen is levenslange behandeling echter noodzakelijk. Een ander klein
deel van de patiënten reageert niet op de behandeling. De exacte oorzaak hiervoor is niet bekend.
Een aantal hypothesen zijn door de auteur voorgesteld. Hierbij behoren het ontwikkelen van
resistentie tegen glucocortcoide, een foutieve diagnose, het gebruik van een ongeschikt geneesmiddel
protocol of een geïnduceerde vorm van pemphigus in plaats van de spontaan ontstane aandoening.
Sleutelwoorden: Autoimmuniteit – Blaarvorming - Canine pemphigus foliaceus – Desmosoom –
Glucocorticoide

3
Pemphigus foliaceus in dogs: the immune pathogenesis and therapies.
Why are some dogs not responsive to the treatment?
1. INTRODUCTION
This literature study reviews up-to-date knowledge regarding the immunopathogenesis and available
therapies for the canine form of pemphigus foliaceus (PF). PF is a complex disease with many
components involved. The interactions of these components as well as the exact pathologic
mechanisms are not yet identified. It is also not known why some dogs do not respond to a
(glucocorticoid) treatment. This literature study strives to give a better insight in already conducted
research and proposed hypotheses.
Pemphigus foliaceus (PF) is an auto-immune skin disease described in humans,1 cats,
2-4 dogs,
2, 3
horses,3, 5
goats 6 and a Barbary sheep (single case)
7. The word pemphigus originates from the Greek
word for blister 8, which is one of the major characteristics
describing this medical condition.
PF is part of the pemphigus complex, which comprises pemphigus vulgaris, pemphigus vegetans,
pemphigus erythematosus, pemphigus foliaceus, panepidermal pustular pemphigus, paraneoplastic
pemphigus, and drug-related pemphigus.9 The pemphigus diseases have in common that the body
produces auto-antibodies against the adhesion molecules of keratinocytes, resulting in the separation
of the keratinocytes, called acantholysis.10, 11
This becomes clinically visible as pustules, which are
very fragile, transient, and leave crusts and erosions11
.
1.1. THE DIFFERENT FORMS OF THE PEMPHIGUS COMPLEX
Diseases included in the group of pemphigus can be differentiated based on the specific auto
antigens. The various forms of pemphigus recognize different auto antigens, located in different layers
of the skin.12
Thus, depending on where the acantholysis takes place, the clinical signs such as
distribution, severity and location of the lesion changes.13
Figure 1: The figure shows the location of the different pemphigus diseases within the epidermis.

4
1.1.1. Pemphigus vulgaris
Pemphigus vulgaris (PV) is the most severe and rarest form of the pemphigus complex.10, 12
The auto-
antibodies bind to antigens in the deepest layer of the epidermis, close to the dermal-epidermal
junction. Acantholysis therefore occurs right above the basal cell layer, forming suprabasilar
vesicles.11, 12
PV is divided in both, humans and dogs, in a mucosal-dominant type and a mucocutaneous type. In
the mucosal-dominant type oral lesions dominate with little or no skin involvement, whereas in the
mucocutaneous form oral as well as skin lesions can be seen.14
The clinical signs are primarily bullae, erosions and ulcers of the skin and can be found, depending on
the type, on the mucosae, at the mucocutaneous junctions and on the trunk, especially in areas of
skin-to-skin-contact such as in the groin and axillae. Oral lesions often cause increased salivation,
halithosis and difficulties to eat.9, 10, 11, 12
PV shows varying degrees of pain and pruritus.9
Systemic
symptoms, such as fever, depression or anorexia are frequently seen. 10
Desmoglein-1 was identified as the major-autoantigen in the cutaneous form, thus causing skin-
lesions. Desmoglein-3 on the other side is the target-antigen in the mucosal form, resulting in mucosal
lesions.14
Logically, both auto-antigens (anti-Desmoglein-1 IgG and anti-Desmoglein-3 IgG) are
present in the mucocutaneous form.15
The diagnosis is made by histopathological examination and by immunofluorescence. Histology is
characterized by suprabasilar clefts and vesicles filled with acantholytic cells.12
Acantholytic cells are
round, the cytoplasm is dense and the nucleus hyperchromatic. Depending on the stadium (acute or
chronic), neutrophils and eosinophils can also be found in the vesicles.16
Another diagnostic tool is
immunofluorescence. In affected patients antibody-deposition in the intercellular spaces can be found
on the biopsy after staining with anti-IgG fluorescein.12
1.1.2. Pemphigus vegetans
Pemphigus vegetans is extremely rare in domestic animals. 9, 17
It is seen as a localized and benign
variant of pemphigus vulgaris.18
On histology acantholysis is visible in the middle of the epidermis11
,
causing pustules and erosions.17
The lesions are generalized rather than mucocutaneous.9
In humans two types of pemphigus vegetans are described: The Neumann type and the Hallopeau
type. Both are sought to be a localized form of Pemphigus vulgaris. The Neumann type is more
common. Lesions include large bullae and erosions, which heal by forming granulation tissue. The
Hallopeau type is less aggressive and on clinical examination pustules instead of bullae can be seen.
When they heal, verrucous hyperkeratotic vegetation develops.18
1.1.3. Pemphigus erythematosus
Pemphigus erythematosus (PE) and pemphigus foliaceus are more superficial.11
They affect especially
the stratum corneum, creating intracorneal or subcorneal pustules that rapidly burst, leaving superficial

5
erosions bordered by epidermal collarettes17
, erythema, alopecia, scales and honey-colored to brown
crusts.10,11
Nasal depigmentation is frequently seen.9, 10, 11, 17, 19
The main difference between PE and PF is that pemphigus erythematosus is limited to the face and
ears. It is primarily found on the bridge of the nose, around the eyes and on the ear pinnae.10, 12
The
disease is most common in Collies, German Shepherds and Shetland sheep dogs.9,10,12
Pemphigus erythematous shows clinical, histological and immunological overlap with characteristics of
pemphigus foliaceus as well as characteristics of discoid lupus erythematosus.9, 19
It is thus still
questionable if PE is an own entity, a benign variant of PF restricted to the face or a crossover of PF
and discoid lupus erythematosus. 9,10,19
Pemphigus foliaceus and drug-related pemphigus will be discussed more in detail further on.
1.1.4. Panepidermal pustular pemphigus
Panepidermal pustular pemphigus (PPP) was introduced in 1994 by a research team for a group of
cases that were previously diagnosed as pemphigus vegetans or pemphigus erythematosus.20
An
important criteria for diagnosing PPP is that the pustules can be found throughout all levels of the
epidermis and follicular epithelium.9
This stands in contrast to PF where pustules stay limited to the
granular and upper spinous layers.19
The pustules rupture easily, leaving a thick crust on the skin.9 On
histology
the pustules were found to contain neutrophils, eosinophils and acantholytic cells.20
Desmoglein-1 could be identified as the major auto-antigen,21
just as in PF. Also the distribution of the
lesions is similar to the distribution of PF. It is apparent that features of PPP overlap with features of
PF. It is thus debatable if PPP is an own entity or a variant of PF. 19
1.1.5. Paraneoplastic pemphigus
At last there is paraneoplastic pemphigus (PNP). This form is very rare and shows blistering skin
lesions in association with underlying neoplasms.22, 23
Envoplakin, periplakin, 24, 25
desmoplakin-I and –
II 22
and desmoglein-3 23
were identified as target-antigens in canines.
In humans pemphigus has been associated with a range of neoplasia, such as a lymphoma, chronic
lymphocytic leukemia, spindle cell sarcomas, squamous cell carcinoma of the lung or thymomas. 26
In
dogs only a limited number of cases have been reported to date. A few were linked to a thymic
lymphoma26
, a sertoli cell tumor27
and another to a splenic sarcoma.22
On clinical examination severe
stomatitis and polymorphous ulcerative lesions were seen in the oral cavity, nose, vulva,
mucocutaneous junctions and haired skin.15,22,24,26
On histopathology suprabasal epithelial
acantholysis typical of PV was found as well as apoptotic keratinocytes with satellitosis that showed
similarities with erythema multiforme.22,26

6
2. PEMPHIGUS FOLIACEUS
2.1. EPIDEMIOLOGY
Pemphigus foliaceus was first described in dogs in 1977 by Halliwell and Goldschmidt28
, since then
the disease was mentioned in different species1-6
and further researches were carried out.
However, limited information about the epidemiology in dogs can be found.19
Of the pemphigus
complex, PF is the one most frequently seen. 10,11,12,19,29
A study from 1987 reported an estimated
prevalence of 0,3%. More specific, three out of 1000 presented canine patients with skin diseases in
an animal hospital in New York were diagnosed with pemphigus foliaceus.30
Another study showed
that canine pemphigus foliaceus (cPF) is probably the most common auto-immune skin disease in
dogs19
, accounting for almost one-third of the cases.29
Contrary, in humans pemphigus vulgaris is the
most frequent variant of the pemphigus group.31
Authors of a retrospective study carried out in Brazil
diagnosed 102 dogs with PF over a 25-year period. That is 4.1 cases per year.32
All breeds can be
affected 10
, but some breeds have a higher risk. Different studies describe a higher prevalence in the
Bearded Collie, Akita, Newfoundland, Schipperke, Dachshund, Doberman pinscher, English Springer
Spaniel, English bulldog, Finish Spitz, Labrador retriever, English Cocker Spaniels, Chow Chows,
Shar-Peis and Collies19,33
There appears to be no age or sex predisposition. 10, 33,34
However, most
dogs are middle-aged between four and six years 11, 30
with 4.2years as the mean age of onset.33
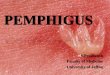
2.2. CLINICAL SIGNS
As mentioned before are PF and PE the more superficial versions of the pemphigus complex,
affecting primarily the stratum corneum.11, 19
The primary lesions are superficial and transient
pustules.10,17
These are yet hard to find, since being very fragile and hidden under the coat.10
The
pustules rupture easily, leaving erythema, yellowish crusts, erosions, alopecia and peripheral
collarettes.9,11,17,33
The lesions most commonly start on the dorsal part of the muzzle, are bilaterally
symmetric and spread gradually.33
PF shows a typical distribution (Fig. 2,3) and most commonly
affects the pinnae, perioral and periocular region, the nasal planum, bridge of the nose and the
footpads. 9,10,11,17,33
The footpad lesions are present in 1/3 of the dogs and are characterized by
hyperkeratosis, cracks, possible erythematous swelling and whitish discoloration.33
Those lesions can
be the only symptom.10
The nailbed can be involved the nails however are usually unaffected. 23
Lesions in the oral cavity and the mucocutaneous junction are rare. 9, 17, 30
In some patients PF can
become generalized, with development of the following symptoms in severe cases: anorexia, fever,
depression, lymphadenomegaly and limb edema. 10, 11, 17
Pruritus can only be found in less than half of
the dogs33
with 17 to 36% showing moderate to severe itching. The disease can be waxing and
waning.10, 11, 17
Figure 2, 3: Typical facial distribution of cPF lesions with scaling, alopecia and pustules.

7
Figure 4: Schematic ultrastructure of a desmosome.
2.3. PATHOGENESIS
2.3.1. Involved components
2.3.1.1. Desmosomes: Function, ultrastructure and composition
Desmosomes or macula adherens are adhesion molecules found in the lateral cell membrane. They
are complex structures that are particularly important in tissues that are subject to mechanical stress,
such as the epidermis or the cardiac muscle. Their main function is cell-cell-adhesion and to assure
tissue integrity. Besides giving strength to epithelia by linkage of the desmosomes to the keratin
intermediate filament of the cytoskeleton, more and more evidence is emerging that desmosomes also
play an important role in intracellular signaling pathways.14,35,36
Desmosomes are classified as glycoproteins and contain an
intra- and an extracellular part that form a complex. They are
spot-like distributed across the lateral cell membrane. 14
Two adjacent cells each possess an outer and an inner dense
plaque. Those plaques are made of proteins of the plakin
(desmoplakin) and armadillo-family (plakoglobin and
plakophilin).14
The inner dense plaque (IDP) consists of
desmoplakin and is linked to intermediate filaments of the
cytoskeleton, to stabilize the cell and keep the desmosomes
on their place. The outer dense plaque (ODP) serves as an
anchor for the cytoplasmic domain of the cadherins. Cadherins
are a third involved protein-family, comprising a cytoplasmic and an extracellular component. Their
name derives from the circumscription “Ca2+
-dependent adhesion” and comprises the glycoproteins
desmocollin (Dsc) and desmoglein (Dsg). Those two are intracellular connected to plakophilin and
plakoglobin and form extracellular heterophilic and homophilic bonds with the adjacent cells.37
Despite their important role in cell-cell adhesion and cell integrity, the desmosomes are not static but
dynamic structures that can change their molecular composition and adhesive properties.38
Recently
two different adhesion states have been described. One is Ca2+
independent, stable and
hyperadhesive, the other is dynamic, weaker and Ca2+
-dependent. Both are reversible through cell
signaling mechanisms which involve protein kinase C and epidermal growth factor receptors.38
It is evident that calcium-ions play an essential role in the induction of desmosome formation. Several
studies revealed that cultured keratinocytes do not form desmosomes in low Ca2+
concentrations
(below 0.1mM). 39-41
When the Ca2+
concentration is however increased desmosomes formed within
two hours.42,43
An increase in extracellular Ca2+
is registered by a Ca2+
sensing receptor (CaR).39-42
CaR activates phospholipase C and triggers the production of inositol 1,4,5-triphosphate (IP3).44
The
increase in IP3 results in an elevated intracellular Ca2+
concentration in keratinocytes.45
Similar
findings were made in cPF research. Seven out of seven human PF sera bound to canine footpad
epithelium under high calcium conditions, but they failed to bind when calcium was chelated (with
EDTA).46
Desmosomes are associated with even more proteins, among others accessory proteins

8
Figure 5: Desmoglein-1 and -3 fluorescence patterns
in canine footpad and buccal mucosa. Intercellular
staining indicates the binding of autoantibodies to
extracellular components. The antibody deposition shows a
typical honey-comb pattern.
such as Perp, corneodesmosin or the armadillo protein p0071.14
The discussion of these goes beyond
the scope of this literature study. Considering the complexity and numerous components of
desmosomes it is intelligible that several of them are plausible candidate autoantigens.47
2.3.1.2. Desmosomal cadherins
2.3.1.2.1. Distribution of desmosomal and non-desmosomal adhesion molecules
In humans there are three isoforms of desmocollin (Dsc 1-3) and four isoforms of desmoglein (Dsg 1-
4). Each cell expresses several isoforms and each desmosome contains more than one type of
desmocollin and desmoglein. 14
The keratinocytes of the epidermis have different degrees of differentiation which are organized in
layers and express a variety of molecular compositions.15
Desmosomal cadherins for example are
expressed in a pattern that is typical for a specific tissue. Except for Dsc-2 and Dsg-2, the expression
of the cadherins is restricted to stratified epithelial tissues. That means that only Dsc-2 and Dsg-2 are
found, for example in the human cardiac muscle, but all seven (Dsc1-3, Dsg1-4) can be found in the
epidermis.14
Bizikova et al. carried out a research in 2011 with the goal to identify possible antigens of PF.
Therefore the research-team immunomapped the major desmosomal (desmoglein-1, desmoglein-3,
desmocollin-1, desmocollin-3, desmoplakin-1/2, plakoglobin and plakophilin-1) and non-desmosomal
adhesion proteins (E-cadherin, claudin-1, zona occludens-1 and occludin). The desmosomal
immunostaining patterns were then compared to the patterns of IF staining with canine PF sera.35
Figure 5 compares the staining patterns of desmoglein 1 and 3 in canine footpad and buccal mucosa.
Of the tested cPF sera 88% showed immunofluorescence-staining laterally of the keratinocytes in the
stratum spinosum and stratum granulosum, 11% showed additional intercellular staining in the stratum
basale, one serum (2%) only bound to the stratum granulosum and 18% also showed intercellular
fluorescence of the buccal mucosae. 80% of the sera thus exhibited a restricted staining pattern to the

9
suprabasal footpad epithelium and very low staining of the buccal mucosa. Several different staining
patterns of the various cPF sera were detected, which implies an immunological heterogeneity of cPF
IgG auto-antibodies.35,48
The figure below (figure 7) shows the distribution of certain desmosomal
components in the canine epidermis. The indirect immunofluorescence (IIF) staining patterns and thus
the distribution of the most relevant molecules for PF are described more in detail below.
Desmoglein-1 and -3
In the canine footpad the fluorescence intensity was highest in the stratum spinosum, with a moderate
decrease towards the stratum granulosum and the stratum basale. Dsg1 is more evenly distributed in
the haired skin with slight decreases towards the basal layer and high fluorescence intensity in the
entire stratum spinosum. Dsg1 is furthermore absent in the stratum distendum of the buccal mucosa.
Dsg1 and 3 show a reciprocal staining pattern in all examined epithelia. Dsg1 is most present in the
superficial layers whereas Dsg3 is highest in the basal layers of the footpad, haired skin and buccal
mucosa.35
Desmocollin
Desmocollin 1 was exclusively found on the margins of suprabasal keratinocytes in the footpads as
well as in the interfollicular epidermis. Interestingly, Dsc1 was not detectable in canine buccal mucosa,
with neither of the anti-Dsc1 antibodies. Dsc3 can well be found in all three tissues, is evenly
distributed in footpad and haired skin and more present in the deeper layers of the buccal mucosa.35
The staining patterns of the human and canine adhesion-molecules showed a more or less identical
distribution.35
In general it can be said that Dsc 2-3 and Dsg 2-3 are primarily expressed in the lower
layers and that Dsc1, Dsg1and Dsg4 are more present in the upper layers of the human epidermis.14
2. 3. 1. 2. 2. Desmoglein as a minor target auto-antigen
The desmosomal cadherin desmoglein-1 is identified as the major auto-antigen in the human form of
pemphigus foliaceus.49
Different tests and studies were carried out to determine the homologous
Figure 6: The diagrams represent the staining patterns and immunofluorescence intensity of desmosomal cadherins
in the different layers of canine footpad, haired skin and buccal mucosa . The column width is in accordance with the
staining intensity.
DSG1: desmoglein-1; DSG3: desmoglein-3; DSC1: desmocollin-1; DSC3: desmocollin-3

10
canine target molecule. A study carried out by Iwasaki and his team in 1997 used
immunofluorescence and western blotting to detect candidate antigens extracted from canine
keratinocytes. By western blotting sera of canine PF patients recognized a 160kDa protein (50% of the
sera), a 85kDA protein (25%) and a 120kDa protein (31, 25%). There were indications that the 160kda
protein corresponds with the human desmoglein-1. The same study also showed that binding between
antibody and antigen could only be seen at the sites of the cell-cell adhesions and not on the entire
surface of the cells.50
Further researches were conducted about the hypothesis of desmoglein-1 being the major auto-
antigen using a novel screening strategy to detect conformational epitopes. In this study from 2006
only 6% of the sera from dogs with pemphigus foliaceus contained antibodies that recognized canine
desmoglein-1.15
Another study by Yabuzoe et al. from 2008 showed similar results. All sera (n=3)
bound to the extracellular part of the desmosomes where adjacent cells made contact. However, only
a limited number of cPF sera bound to Dsg1 specifically. These findings suggest that the target auto-
antigen is a desmosomal protein.51
They furthermore denunciate desmoglein-1 as a minor autoantigen
in cPF.46
What is more, it illustrates that pemphigus foliaceus is a heterogenous disease, with more
than one antigen being involved.
In a study that aimed at detecting the main autoantigen in cPF researchers found that calcium
depletion and glycosylation have an influence on the recognition of dsg1 in epithelial cells. The role of
calcium in expressing epitopes is described more in detail in section 2.3.1.1. To test their hypothesis,
the researchers incubated canine footpad epithelium as a substrate in 1mM calcium buffer or 5mM
ethylenediamine tetracetic acid (EDTA) for thirty minutes. Ensuing they tested the binding of human
PF sera to the substrate with calcium being respectively present or absent. All seven human PF sera
bound to canine footpad epithelium under high calcium conditions, but the IgG in the sera did not bind
when calcium was chelated. Based on those results they concluded that membrane-bound canine
dsg1 was expressed in a calcium-dependent conformation. Another interesting finding is, that the
binding of the few canine and human PF sera that contained Dsg1-antibodies, depended on
glycosylation. This was investigated by inhibiting protein glycosylation with tunicamycin.46
2.3.1.2.3 Desmocollin as a major target auto-antigen
Desmocollin is an important molecule of the cell-cell adhesion of adjacent keratinocytes. The
importance of Dsc1 in cell-to-cell adhesion was demonstrated with the aid of genetically modified
mice. Those mice were lacking Dsc1 and showed epidermal fragility and spontaneous blister
formation in superficial epidermal layers as aresult.52
After localizing the major desmosomal adhesion molecules those profiles were compared to the
staining profiles of cPF serum IgG. 80% of the tested cPF sera showed a similar staining profile to that
of desmocollin-1 (Dsc1). This suggests Dsc1 being a relevant candidate antigen. Desmocollin-1 is
additionally not detectable in canine buccal mucosae,35
which matches the clinical signs of PF, since
the pustules typically form in the superficial layers and the oral cavity rarely being involved.9, 17, 30

11
Further researches demonstrated that the sera of most PF affected dogs contain specific IgG
antibodies against Dsc1 that are not present in normal dogs. Those findings define Dsc1 (variant “b”)
as a major auto-antigen in canine pemphigus foliaceus. The Dsc-variants “a” and “b” differ in the
splicing pattern of the mRNA transcript that codes for the Dsc1-protein. In variant “a” an exon
containing a stop-codon is removed. The resulting coding sequence is thus translated into the longer
Dsc1a protein.14
Similarly to human PF, serum of dogs may contain antibodies against more than one auto-antigen.
Sera were found in dogs that contained antibodies against Dsg1 and Dsc1 at the same time.47
Interestingly, although Dsg1 is the major auto-antigen in human PF, desmocollins (Dsc1-3) are
identified as auto-antigens in some human PF patients with aberrant forms of superficial pemphigus,
especially in those with neutrophil-rich skin lesions.35,54
2.3.1.2.4. Other auto-antigens
So far desmoglein-1 and desmocollin-1 have been specified as auto-antigens in cPF. In humans they
also identified the non-desmosomal adhesion protein E-cadherin as a target. The relevance of anti E-
cadherin antibodies is not yet clear.36
In a study that involved double-sided immunogold labeling of canine PF sera the researchers detected
that more antibodies were bound to the intracellular part of the desmosomes than to the extracellular
part. The location of the detected antibodies was similar to that of desmoplakin, an intracellular
component of desmosomes. By immunoblot analysis the IgG recognized a 250kDa epidermal protein,
which is also conform with desmoplakin.51
In canine pemphigus vulgaris envoplakin and periplakin
(besides Dsg1 and -3) are well known as target antigens.55
Another study found two separate auto-antibody staining patterns in PF-dogs as well as in normal
dogs. They detected with indirect immunofluorescence one group of antibodies that bound to the
superficial layer of the epidermis (predominantly in the stratum granulosum) to peripheral cellular
antigens and another group that bound intracellular in the deep layers of the epidermis, especially the
stratum basale. Both patterns often co-existed. Most normal and PF dogs contained the superficial
antibodies, while only few sera were detected that contained the antibodies that bound to the stratum
basale. It is suspected that the cytoplasmic target antigen, just like in humans25
, is a plaque protein of
the plakin family. The author thinks that the antibodies that bind to the deeper skin layers do not play a
pathogenic role, since PF is a superficial skin disease.48
The (possible) pathogenic role of the
desmoplakin antibodies is not yet clear. The authors suggest that anti-desmoplakin antibodies can
intrude the cell after cell-membrane damage by other factors and that it might act as an accelerator of
the disease. They describe this phenomenon as epitope spreading. 51
2.3.2. The role of neutrophils
In contrast to the human form of PF, the formed pustules of the canine PF patients contain intense
neutrophilic infiltrations.15,56,57
Electron microscopy showed neutrophils next to acantholytic

12
keratinocytes, as well as in the epidermis next to the pustules. They could be found in the
intraepidermal pustules as well as in the superficial ones. 58
Neutrophil chemotaxis might be the result
of chemokine secretion by keratinocytes after IgG-binding48
which can be seen in some human PF-
patients that also show neutrophil-rich lesions.59
Eosinophils were present without pathologic findings.
Interestingly, all half-desmosomes were seen at the contact points between the granulocytes and
keratinocytes. None were observed on cell surfaces where no neutrophils made contact. The
neutrophils featured invaginations that enclosed half-desmosomes of the acantholytic keratinocytes.
Remarkably, the half-desmosomes in the invaginations had intact attachment plaques and attached
tonofilaments that did not show any retraction. (Retraction of tonofilaments and internalization of
desmosomes was described in humans with PV and PF).58
In the early stages of acantholysis, neutrophils developed pseudopodia that were brought in between
the half-desmosomes of two adjacent keratinocytes. In a later phase, the same study showed that the
granules of the neutrophils were secreted to the surface of the acantholytic keratinocytes, resulting in
disassembly of the half-desmosomes. Those findings suggest a supplementary pathogenic role of the
neutrophils regarding the degeneration of cell- adhesion and separation of adjacent keratinocytes.56
2.3.3. Antibodies
2.3.3.1. Antibody profile
In different studies IgG was found as the main immunoglobulin deposited in a net-like manner around
the keratinocytes of canine PF patients.35,48,56
Also, in the immunomapping study from Bizikova et al,
all cPF sera (n=66) contained anti-keratinocyte IgG in the serum and IgG-depositions primarily
suprabasal and membrane-associated.35
Yabuzoe et al found IgG deposition on the keratinocytes
perilesionally and in the serum, but not that of IgA, IgM or C3.56
Bizikova and her team conducted a study in 2014 to investigate the serum antibody profiles (IgG, IgA
and IgM) of anti-keratinocyte, anti-Dsc1 and anti-Dsg1 immunoglobulines in cPF patients. They
detected the auto-antibodies by indirect immunofluorescence (IIF). More sensitive methods might
however result in higher positive numbers. Conversely, they found that 18% (n=6) of the sera
contained auto-reactive IgA, around 3% (n=1) contained (anti-desmocollin1) IgE and none of the sera
contained IgM. An IgA pemphigus without IgG-antibodies, similar to certain human PF forms, was not
discovered. Those findings suggest that canine PF is a predominantly IgG-mediated disease and that
IgE and IgA can only be detected in rare cases.60
In humans two forms of pemphigus are described that feature anti-Dsc1 IgA in a higher extent than in
the classical form.61,62
These are called atypic pemphigus and IgA pemphigus.63
In the latter IgA is the
dominant antibody isotype.63
Remarkably both of them, contrarily to the classic human PF form and
similarly to canine PF, also feature neutrophilic pustules.19, 63

13
2.3.3.2. IgG subclasses
Four IgG subclasses (IgG1-4) are described in the dog. IgG are composed of four peptide chains; two
identical light chains and two identical heavy chains. The subclasses are defined primarily by the
amino acid composition and the structure of the hinge region. Furthermore, they differ in abundance in
the canine serum.64
The predominant subclasses of antikeratinocyte antibodies present in canine PF
sera are IgG1 and IgG4. In normal healthy dogs those two autoantibodies are present in relatively
lower titers, with IgG1 being the most prominent one of the IgG subclasses. In normal and cPF dogs
no significant differences in the titers and seroprevalence of IgG1, IgG2 and IgG3 could be detected.
IgG4 however was almost exclusively found in dogs with PF (80%) and in only 7% of normal dogs.
The same author described furthermore decreasing or stable IgG4 titers when the skin lesions
resolved, whereas such development could not be seen in IgG1. IgG4 might thus be used as a marker
for disease activity since it is higher in severe cases and decreases when the skin lesions diminish.
Based on those findings the author suggests that IgG4 antibodies is most likely the pathogenic isotype
in cPF.48
2.3.3.3. Titer and severity
Different studies suggest that the serum titers are positively correlated with the severity of the clinical
signs.46, 47, 48, 131
When skin lesions improved antikeratinocyte IgG4 titers stayed constant or
decreased. The maximum reduction was seen when the disease improved or reached remission. The
titer of IgG1 was not significantly affected by the degree of severity. 48
Bizikova and colleagues
conducted a study in 2012 to investigate the relationship between anti Dsc1 IgG titers and disease
severity. They selected ten dogs with PF, applied a scoring system to score the severity of the disease
and took serum samples before and during treatment. In all dogs a noticeable clinical improvement
could be seen. The antibody titre decreased in 70% of the dogs (n=7) together with the decrease in
severity.48
2.3.3.4. Specificity of the antibodies
As mentioned earlier, more than one auto-antigen and antibody are involved in the pathogenesis of
PF. So far anti- Dsg1 and anti-Dsc1 antibodies have been identified. The detection of auto-antibodies
is, however, apparently strongly depending on the substrate. In normal bovine esophagus antibodies
were detected in 65% of the cPF-patients65
, indirect IF on cultured canine keratinocytes was positive
for all tested cPF sera66
, when however other substrates were used the frequency of the antibody
detection decreased significantly.65

14
2.3.4. Pathophysiology
2.3.4.1 Introduction
The underlying mechanisms and factors that induce the production of pathogenic antibodies are not
fully understood yet. Nevertheless several theories and involved components are proposed. Besides a
genetic predisposition, different exogenous factors are proposed to play an important role in the
pathogenesis. Drugs are the best-recognized triggers.67-69
Other hypotheses include a suppressor T-
cell dysfunction or bypass; a modification of self-antigen; a cross-reaction with exogenous antigens;
abnormalities of the major histocompatibility complex II and access of T-cells to previously hidden self-
antigens.11
2.3.4.2 Role of the auto-antibodies
Intradermal injections of PF IgG in neonatal mice resulted in the formation of pustules that were
histologically similar to those of human and canine PF patients. The location of the lesions in the skin
were similar to those of PF as well. Passive transfer of the serum of normal dogs to the mice did not
lead to blister formation. This proves the pathogenic role of the antikeratinocyte antibodies.48
An
important difference between the induced PF-lesions in the mice and natural ones is however that the
induced pustules lack eosinophil and neutrophil granulocytes that predominate in natural cPF.48,56
2.3.4.3. Proposed mechanisms
The mechanism between the auto-antibodies and the induction of acantholysis is not satisfyingly
explained yet. A logic and simple explanation would be, that the auto-antibodies interfere with the
extracellular adhesion by steric hinder. By this means the bond between the extracellular cadherins
would be disabled, resulting in the separation of the keratinocytes.14
A research conducted by
Waschke et al in 2005, however, has revealed that pemphigus foliaceus IgG from patients was not
able to break a homophilic Dsg1-Dsg1 bond. 70
Conversely, evidence is increasing that PF is a more complex disease with several pathogenic
components involved. Several papers suggest that serum IgG can trigger a multistep mechanism of
intracellular events.31
Research in humans proposes numerous mechanisms of acantholysis after the
antibody bound to desmosomal antigens. These include the internalization of the antibody-antigen
complex and fusion with intracellular lysosomes; an increased amount of urokinase-type plasminogen
activator in the affected epithelium, resulting in high concentrations of extracellular plasmin and thus
destruction of the adhesion molecules.71-73
Another possible (supplementary) pathologic mechanism
includes the activation and fixation of complement.74
It is proven in humans that the binding of IgG-antibodies induces the following changes in the
keratinocytes. IgG binding activates the Fas/Fas ligand cell death pathway and the mitogen activated
protein (MAP)-kinase pathway. It also induces phospholipase-C activation, inositol 1, 4, 5-triphosphate

15
generation, increases intracellular calcium concentration and a redistribution of protein kinase C (PKC)
inside the cell. Additionally, it interferes with RhoA signaling.75-78
Rhoa stands for RAS homolog family
member A and plays a role in the regulation of cytoskeletal dynamics, transcription, cell cycle
progression and cell transformation.79
Another study regarding human PF suggests as well that IgG binding to desmoglein or other surface-
molecules activates a variety of mechanisms resulting in the disassembly of the desmosomes,
tonofilament retraction and internalization of desmosomal structures in cultured keratinocytes.14,58
A
part of this mechanism could be due to the phosphorylation of desmoglein and thus its dissociation
from plakoglobin.36
Additionally, desmoglein could disappear from the surface by
endocytosis.58,65
However, those findings are not totally in accordance with the findings in cPF. In cPF
a study examined more than twenty half-desmosomes of keratinocytes from canine PF patients. All of
them had intact intracytoplasmic dense plaques and no remarkable tonofilament retraction. That might
suggest that in cPF IgG does not trigger an alteration of the intercellular pathways and interference
with the cell-cell adhesion.56
As described previously, it is also likely that neutrophils play a pathogenic role by forming
pseudopodia and release enzymes to break adhesion bonds.54, 56
A different article describes that the onset and course of PV is based on predisposing and inducing
factors. The inducing factors can be environmental or endogenous factors. That also implies that a
predisposed genetic background alone is not sufficient for the diseases to break out but also requires
a trigger.31
Endogenous factors might be hormone disorders, emotional stress, immune suppression
etc. Environmental factors starting the disease could be drug intake (see “Drug related pemphigus”
below), viral infections, diet, contact allergens etc. The same principle might apply to cPF. A genetic
background that predisposes certain breeds to cPF has already been mentioned.19
The disease was
furthermore found in two Shetland sheepdog littermates.80
In humans there is an endemic form of PF described in Brazil, called “fogo selvagem”.81
Different
authors suggest a genetic predisposition together with an environmental trigger to develop clinical
signs. 15, 31
Additionally, in specific pathogen free (SPF) dogs lower frequencies and titres of
antikeratinocyte antibodies were detected, compared to normal outbred client-owned dogs. It is not
known if those findings are relevant, but it might indicate that environmental factors might play a role in
the pathogenesis.48
Pilot studies were conducted in dogs with PF. Flea infestation was one of the
exogenous factors associated with the disease82
, whereas UV-rays might induce new skin lesions.83
All the mechanisms mentioned above do not exclude each other. It might be possible that several
mechanisms occur simultaneously or even trigger or enhance each other. Waschke et al describe in
their article that the binding of IgG to the extracellular part of the desmosomes causes steric
hindrance, impaired signal transduction, keratin retraction, cytoskeleton collapse and of course
acantholysis. The study was based on human research and not on dogs.37
Kitajima et al proposes in his review article from 2013 the term “Desmosome–remodeling impairment
disease”, which shows similarities with some of the mechanisms proposed above. This theory includes

16
a mechanism of Dsg3 non-assembly and depletion from desmosomes when in the “weak adhesion
state”. In human PV the binding of autoantibodies to Dsg3 results in the activation of intracellular
events, more specific in the activation of protein kinase C (PKC). PKC induces subsequently a switch
from the Ca2+-
independent hyperadhesive state to the weak-adhesion state. This seems to be the
more susceptible state, creating keratinocytes that are more sensitive to blistering processes.38,42
Then endocytosis of Dsg3 and thus a depletion of Dsg3 from the cell surface takes place. 38
An article by Ruocco et al from 2013 states that there must be additional auto-antigens in human
pemphigus vulgaris (hPV), besides Dsg1 and Dsg3. Otherwise, when both, anti-Dsg1 and anti-Dsg3
antibodies, would be present the epidermis would completely disintegrate. They suggest the
keratinocyte acetylcholine receptors as a non-desmoglein pemphigus antigen. The receptors play an
important role in the mediation of intercellular adhesion and in particular the expression of desmoglein.
Again, similar to the findings of the varying immunostaining-patterns of affected the dogs, it is likely
that different subsets of auto-antibodies are involved, which would explain the variety of clinical and
biological symptoms.31
As described earlier pemphigus vulgaris in humans has a mucosal-dominant type, caused by anti-
Dsg3 autoantibodies and a mucocutaneous form with anti- Dsg1 and -3 autoantibodies. The mucosal-
dominant type can evolve into the mucocutaneous form when autoantibodies against Dsg1 develop
aswell.14
Based on those findings the “desmoglein compensation theory” emerged. This theory states
that one isoform of desmoglein can compensate the loss of another.84
This theory, or hypothesis,
would explain why there is no blister formation in the epidermis in the mucosal-dominant PV form. The
auto-antibodies attack Dsg3, but Dsg1 expression in the basal layers can compensate for this loss of
function and keeps the epidermis intact. Blistering would, according to this theory, only occur when
both, Dsg1 and Dsg3 get attacked.14
Thus there are only superficial lesions in PF, since adhesion in
the basal epidermal layer, is maintained by Dsg3.38
This hypothesis is however not completely
conclusive. In November 2014 a case was reported of a human patient with suprabasilar acantholysis,
but was at the same time found positive for Dsg-3 and negative for Dsg-1 antibodies. 85
According to
this hypothesis also Dsg4 should be able to compensate for the loss of the other isoforms, which is
apparently not the case. 14
It is evident that the responsible immunopathogenesis is not yet clearly elucidated. Many
investigations offer however valuable clues. The current research shows a huge variety of cell biologic
processes that might be involved. Some of them are primarily pathogenic; others only trigger a
cascade of mechanisms leading finally to acantholysis. Some components are essential, others add
up to the clinical signs.38

17
2.4 DRUG-RELATED PEMPHIGUS
2.4.1. Introduction
There seems to be a condition of cPF which occurs as a response to drug therapy. Drug related
pemphigus may be further divided in drug-induced and drug-triggered PF.9,86
The first one is a
transient form of pemphigus in which clinical signs disappear after discontinuing the drug. Conversely,
the latter is permanent.19,86
Several drugs have been associated with a PF outbreak in dogs so far.
The majority of the reported patients developed localized lesions, whereas only a small percentage
showed generalized lesions. More than half of the dogs also developed systemic signs (lethargy,
fever, anorexia, pain and lameness). Interestingly, most of the dogs were of large breeds.87
Drug-
related PF is clinically, histologically and immunologically similar to the naturally occurring form of
canine pemphigus foliaceus. The history helps to differentiate naturally occurring PF from drug-related
PF.67
In the drug-related form the dog must have received the inducing drug, there is an unusually fast
onset of clinical signs, an unusually early onset and unusual clinical characteristics (e.g. oral
lesions).86
Most of the drugs related to cPF outbreaks were insecticides. In humans different pathomechanisms
are suggested on how pesticides (including insecticides) induce PF. The proposed pathomechanisms
include an alteration of the keratinocyte membrane biochemistry and/or an interaction with the
immune-system.67
Many of the described drugs contain a thiol-group, which might be an indication.31
One theory describes the blocking of keratinocyte nicotinic acetylcholine receptors and thus inhibiting
signaling which is important for cell-cell adhesion in the epidermis.69
Another possibility could be a
modification of the skin by the drug and thus creating neoantigens and secondary auto-antigens.88,89
Other theories include an increased cytokine production or an alteration in enzyme activity that are
involved in cell-adhesion. 90
2.4.2. Trimethoprim-sulfonamide
Trimethoprim together with sulfamethoxazole, sulfadiazine or sulfamethoxypyridazine may induce
pemphigus foliaceus9, 27, 87, 91, 92
as well as other skin diseases, such as erythema multiforme or
perforating folliculitis. 93
Once the administration stopped the lesions resolved within a few weeks.27
2.4.4. Promeris Duo®
Promeris Duo® (Zoetis Animal Health) is an insecticide, containing metaflumizone
94 and amitraz. It is
associated with currently 22 cases 132
of drug-triggered as well as drug-induced PF.86-88
Promeris is no
longer on the market. The lesions strongly resemble those triggered by Certifect®. Systemic signs
were reported in both entities, however, it was more frequently described in Promeris-triggered PF
(PTPF; 64%) than in Certifect-triggered PF (CTPF; 43%). 91% of the dogs were large breeds and
bitches were affected more frequently (68%). Also here the majority of the patients (86%) reached

18
complete remission. Just as in natural PF ( 82%), most sera of CTPF (71%) as well as PTPF ( 75%)
dogs contained anti- Dsc1 IgG`s.67
No distinct differences between the histopathology of the skin lesions of CTPF, PTPF and natural PF
were identified. The exact trigger or component of the drug (amitraz, metaflumizone, fipronil, the
vehicles or a combination) causing the eruptions is not yet known but the clinical, histological and
immunological similarities imply a common pathogenesis with natural PF.67
Promeris and Certifect both comprise amitraz 67
, but amitraz has been widely used against other
ectoparasites such as Demodex or Sarcoptes mites without inducing PF.87
Given the large number of
amitraz treated dogs and the relatively low number of PF-outbreaks, it is likely that also other factors
influence the disease outbreak, such as the genetic background, environment, immunological or
hormonal status.67
Another interesting finding is that lesions developed in 67% of the affected dogs
within two weeks. The production of auto-antibodies however takes a minimum of three to four weeks
after primary sensitization.95
Moreover, recent articles describe contact-triggered PF also after the
application of another antiparasitic drug that does not contain amitraz but even other components
(Vectra 3D®).
86,87
2.4.3. Certifect:®
Fipronil-Amitraz- S-methoprene
Certifect®
(Merial) was released in 2011 as an ectoparasiticide which contains fipronil, amitraz and S-
methoprene. It has been found to provoke acantholytic pustular dermatitis in some patients. 67
21
cases were reported to date.87
It shows a close clinically, histologically and immunologically similarity
to the naturally occurring form of canine pemphigus foliaceus. 67
Most of the affected dogs were larger
breeds and middle-aged or older.67
There were more females affected (71%) than male dogs.
Systemic signs were exhibited in 43% (n=9) of the dogs. In 29% (n=9) the lesions were limited to the
application site, while the rest of the affected canines also showed distant lesions. In 33% of the dogs
one application of the drug was sufficient for clinical symptoms and 29% developed symptoms after
the second application. IgG autoantibodies were found in the sera with Desmocollin-1 being the main
target antigen (79% of the cases, n=11). Canine desmoglein-1 was found not to be targeted at all.
Those findings suggest that this new ectoparasiticide is capable of triggering PF. Complete remission
was reported in most of the dogs (81%). Due to its complex composition it is not possible to identify
the actual pathogenic agent. 67
In humans pesticides are also suggested as PF-triggering factors.68
2.4.5. Vectra 3D
Vectra 3D is used as a flea preventative and contains dinotefuran, pyriproxyfen and permethrin.67,86, 96
The insecticide has been reported to trigger PF-like lesions in three dogs to date.87, 96
Cytology and
skin biopsy revealed the same histopathological lesions as in naturally occurring PF.86, 96

19
2.4.6. Others
Other drugs that are associated with a drug-related PF outbreak include cephalexin, oxacillin92
and
polymixin B.97
Additionally, a puppy with juvenile cellulitis was treated with amoxicillin-clavulanic acid
and topical oxytetracycline and developed ensuing signs of PF. Those symptoms resolved after drug
withdrawal.98
2.5 THERAPIES
2.5.1. Introduction
Pemphigus foliaceus is based on auto-reactive processes. Consequently most treatments contain a
component that suppresses or modulates the immune system. The most popular and first-line choice
of drugs are glucocorticoids. 27
Considering the side-effects of corticosteroids, a general consideration
should always be to keep the patient on an as low as possible dose, even though that could mean a
few remaining lesions.19
Besides glucocorticoids, azathioprine, cyclosporine, chlorambucil, tetracycline
and niacinamide are most commonly used for the treatment, according to Rosenkrantz.27
There are
further drugs that can be used additionally to glucocorticoids or as a substitute. Possible reasons to
use second or third-line drugs are unacceptable side- effects, sparing of glucocorticoids or an
insufficient response with glucocortcicoids.27
2.5.2. Most commonly used drugs in the treatment of cPF
2.5.2.1. Corticosteroids
Historically the standard treatment for cPF was an immunosuppressive therapy with oral
glucocorticoids at daily dosages from 2 to 6.6mg kg-1.
34, 33, 27, 99 When the lesions diminish the dose
and/or administration frequency is reduced, preferably to an alternate day intake.27, 33
In some patients
however, immunosuppression alone did not lead to the desired remission.33
In those cases
corticosteroids are combined with cytotoxic or other alternative drugs. Frequently used cytotoxic drugs
are azathioprine, cyclophosphamide or chlorambucil. 27, 33, 34
Topical glucocorticoids can be used in localized lesions and if necessary in combination with systemic
therapies. Glucocorticoids with different potencies are available. It is advised to initially use an
immunosuppressive dosage, for example 2.2-4.4mg kg-1
of prednisone or prednisolone daily. If
adequate response is achieved after two weeks it is possible to switch to a less potent glucocorticoid
and/or gradually reduce this dosage over a period of 30 to 40days. If no significant improvement or
unacceptable adverse reactions appear after ten to 14 days it is possible to add another
immunosuppressive drug to the treatment regime.11
The final goal is to reach a dosage of 1mg kg-1
on
an alternate day basis or less.

20
A systemic glucocorticoid therapy is however the most used approach for cPF.27
Frequently used
glucocorticoids are prednisone, methylprednisolone or prednisolone.19
Rosenkrantz describes in his
article that he prefers to use methylprednisolone due to less mineralocorticoid effects and thus less
polyuria and polydipsia. Furthermore, some patients respond better to the latter.27
Much more potent
glucocorticoids (six to ten times stronger) are triamcinolone and dexamethasone. Both are
administered orally. Those can be used in more persevering cases, in dogs with extensive polyuria
and polydipsie or changed behavioral patterns. The starting immunosuppressive dosage for
triamcinolone is 0.2-0.6mg kg -1
daily and 0.2-0.4 mg kg -1 for dexamethasone. For maintenance it is
sufficient to give the drugs every third day, since they suppress the hypothalamic-pituitary-adrenal axis
for 24 to 48hours. The maintenance dosage for triamcinolone lies between 0.1-0.2 mg kg
-1 every
second or third day, whereas for dexamethasone only 0.05-0.1mg kg-1
is advised every second or
third day as well.27
Glucocorticoids affect many cells and tissues of the body, thus initiate a wide range of changes that
involve different cell types simultaneously. Their main effect is anti-inflammatory as well as
immunosuppressive. Long-term administration can influence the blood count. More specifically it
results in neutrophilic leukocytosis together with eosinopenia, monocytopenia, and lymphocytopenia.
One of the main anti-inflammatory mechanisms is the hindrance of the neutrophils and monocytes to
migrate to the inflammation site. Granulocyte function is relatively less impeded in comparison to the
monocyte-macrophage function which seems to be particularly sensitive to corticosteroids.100
Another
article also describes the inhibition of inflammatory mediators and suppression of autoantibody
levels.101
Another observed side-effect is a transient lymphocytopenia of all detectable lymphocyte
subpopulations.102
That is explained by a redistribution of the circulating lymphocytes.100
In some
species (mouse, rat, rabbit) the lymphocytopenia was also caused by induced cell-death. In humans
that phenomenon was only seen in immature or activated T-cells, but not in resting T-cells.103,104
Glucocorticoids are steroid hormones that can easily diffuse through the cell membranes when in their
free form. In the cytoplasm they bind, with high affinity, to cytoplasmic glucocorticoid receptors. The
formed ligand-receptor complexes migrate into the nucleus where it can modify the transcription of
specific genes that encode proteins responsible for the action of the glucocorticoids. In normal T-cells,
when antigens bind to the T-cell receptor, a phosphate group is added to the tyrosine amino acid of
several intracellular proteins. As a result protein kinase C (PKC) is activated and also the intracellular
calcium concentration rises. These two events (PKC and calcium increase) are necessary for the
transcription factors to bind to the IL-2 gene promotors and initiate the transcription. The messenger
RNA (mRNA) then translocates to the cytoplasm where it is either translated by ribosomes to the IL-2
protein or degraded by RNAases. Glucocorticoids are capable of intervening with several of these
steps of the T-cell cycle. They inhibit the tyrosine phosphorylation; they inhibit calmodulin kinase II, an
enzyme of the calcium pathway and they inhibit the binding of transcription factors to transcript and
later translate IL-2 mRNA to effective proteins. Furthermore there is an increase in mRNA
degradation.100

21
Cytokines are essential for the proper functioning of T-cells. IL-2 in particular promotes T-cell
proliferation and generation of effector, suppressor, and cytotoxic functions. Consequently, the
generation, proliferation, and function of helper and suppressor T cells are depressed by these
drugs.105
Cytotoxic T-cell responses are also impeded by moderate-to-high doses of glucocorticoids
because of the blockade of cytokine expression and to a lesser extent because of the lysis of reactive
T-cell clones.106
Generally speaking the cellular immunity is more susceptible than the humoral immunity, which means
that the B-cells are relatively resistant to the immunosuppressive effects of glucocorticoids. These
drugs inhibit the proliferation of B-cells but have a minimal effect on the transformation of B-cells into
active immunoglobulin-secreting plasma cells. Their major effect on B-cells is on the antibody titre.
Low doses of glucocorticoids have no significant effect on the titre, however, daily high-doses result in
decreasing immunoglobulin levels with the greatest suppression after two to four weeks.107
The
suppression is the result of an initial elevated catabolism followed by reduced production. Another
reason is the impeded production of cytokines and the decreased activity of helper T-cells that play an
essential role in the activation of B-cells.100
Side-effects are commonly seen in long-term treatments with corticosteroids (daily for >14days) and
more frequently with the more potent derivatives. Described side-effects of topical treatment include
atrophy, alopecia and localized pyoderma. By licking or dermal absorption systemic effects are also
possible.
In systemic therapies with strong glucocorticoids iatrogenic hyperadrenocorticism is
described 27
with cushingoid and diabetic effects. Due to those hormonal alterations, polyphagia,
muscle atrophy, a poor hair coat, weight gain, calcinosis cutis, hepatomegaly, and panting can be
seen regularly. 102
The glucocorticoids have varying mineralocorticoid effects resulting in polyuria and
polydipsia. Since being an immunosuppressive drug, patients are also more prone to infections, such
as secondary bacterial skin infections, cystitis or demodicosis and experience delayed healing.102
Reported are also gastrointestinal side-effects, such as ulcerations, pancreatitis, vomiting and/or
diarrhea.27
Besides the physical side-effects, also behavioral changes are observed. Some dogs are
described to be lethargic, others become more aggressive or restless. 108
Due to the side-effects especially on the blood count, monitoring including complete blood counts,
chemistry profiles, urinalysis and urine cultures should be performed every six months.27
The prognosis after a glucocorticoid therapy alone is moderate. Several studies have been conducted
to analyze the treatment outcome and gained similar results. Ihrke et al registered a positive outcome
with corticosteroids alone in 39% of the examined PF patients33,
Rosenkrantz and colleagues
documented 35% of the PF cases to be adequately controlled with only glucocorticoid therapy27
and
Mueller and his team reported complete remission with only glucocorticoids in 38% of the patients
within 1.5-12months after treatment-begin (average 7months).99

22
2.5.2.2. Azathioprine
Azathioprine is an immunosuppressive drug and can be administered solely, in combination with
glucocorticoids or with other immunosuppressive drugs.27
It is the first choice to be added to the
glucocorticoid treatment regimen as a glucocorticoid-sparing agent.11
Azathioprine is a prodrug that
inhibits DNA and RNA-synthesis by blocking purine-biosynthesis. Especially fast growing cells such as
B- and T-cells are affected because of their lack of a salvage pathway which is necessary for purine
biosynthesis. As a result the drug decreases lymphocyte proliferation, lymphocyte numbers and T-cell
dependent antibody synthesis.109
The main side effects are myelosuppression110
and gastrointestinal
symptoms such as vomiting, diarrhea and hepatotoxicity.111
Bone marrow suppression occurs after
one to two weeks after therapy onset and is reversible. Rare side-effects comprise hepatic necrosis
and pancreatitis. 110
The advised doses are 1.5-2.5mg kg-1
every 24 to 48hours. It shows a delayed
onset and takes normally one or two months until clinical effects become visible. 27
It is thus important
to not stop or reduce the therapy too fast.
11 Complete blood counts are recommended every two to
three weeks for the first three months after therapy onset, subsequent monitoring should be carried
out semi-annually.27
The success rate of the treatment with prednisolone and azathioprine together was reported in 55% of
the cPF patients99
. Five dogs in this study did not react on prednisolone alone but underwent complete
remission when both drugs were administered. Nevertheless, more adverse drug effects were
described with this combination. The benefit is thus controversial.99
2.5.2.3. Chlorambucil
Chlorambucil is an alkylating agent that interferes with the DNA-synthesis and is thus cytotoxic. It acts
primarily in on B-cells and is considered a slow-acting immunosuppressive drug that takes two (to
six)11
weeks before therapeutic effects can be seen.109
Reported side-effects include bone marrow
suppression, hepatoxicity and gastrointestinal distress which shows through vomiting, diarrhea and
anorexia. Myelosuppression is nevertheless rather mild and occurs one or two weeks after the
therapy onset.109
Chlorambucil is used as an alternative to azathioprine, solely when other therapies
are not tolerated or in combination with corticosteroids and azathioprine in difficult cases.27
It is the
first choice for cats together with glucocorticoids.11
2.5.2.4. Chrysotherapy
To prevent extensive side-effects by the long-time administration of corticosteroids an alternative
approach is described by administering goldsalts, such as aurothiomalate and aurothioglucose. 27,33,34
Aurothioglucose is however no longer commercially available. Rosenkrantz found it effective for feline
pemphigus, but not for canine pemphigus.27
The exact mechanism of action is not fully elucidated, but
it works immune-modulating and anti-inflammatory10, 27
A disadvantage is a long lag phase of ten to 16
weeks.27
It can be used solely or adjunctive with glucocorticoids, and orally as well as in form of an

23
injection. Adverse reactions to the therapy include bone marrow suppression, oral ulceration and
glomerulonephropathy. Furthermore are the injections very painful and deep. One case is reported
where two dogs died from a toxic epidermal necrolysis after a sudden change from azathioprine to
aurothioglucose.112
Regular monitoring is advised. The monitoring should contain a complete blood
count every two to three weeks, and biochemistry and urinalysis every four to six weeks for the first
few months after start of the therapy and then repeated every three to six months.10
2.5.2.5. Tetracycline and niacinamide
A few cases are also described where PF patients responded to tetracycline and niacinamide
treatment.99, 113
Tetracycline is a broad-spectrum antibiotic with anti-inflammatory properties.
Niacinamide is part of the vitamin B-group, inhibits mast-cell degranulation and also
phosphodiesterase. A common side-effect is an upset gastrointestinal tract that might result in
diarrhea, increased liver enzymes, vomiting and anorexia. In those cases decreasing or discontinuing
niacinamide can relief the symptoms. The drugs have a delayed effect. Clinical benefits are thus not
visible before one or two months after therapy onset. The dosage or the frequency of administration
may then be reduced. The advised dosage for both are 250mg three times a day for dogs under 10kg
and 500mg every 8hours for dogs above 10kg.27
2.5.2.6. Mycophenolate mofetil
Mycophenolate mofetil is the prodrug of mycophenolic acid and interferes with the synthesis of de
novo purine.27
T- and B- lymphocytes are especially sensitive since they cannot use the salvage
synthesis pathway. This feature enables the drug to selectively inhibit lymphocyte proliferation and
the production of antibodies.27,109
Further mechanisms include a suppression of dendritic cell
maturation and decreased monocyte recruitment to the inflammation site.109
Adverse drug reactions
include bone marrow suppression, being more prone to infections and gastrointestinal problems. 27, 109
Most studies on drugs are executed retrospectively and the drugs were originally developed for
humans.19
A prospective clinical trial was, however carried out in a 16-week pilot study with
mycophenolate mofetil (20-40mg kg-1
, 3 times daily). Of the eight examined dogs only three improved.
Dosages between 22-39mg kg-1
per day were used spread over three applications per day. Adverse
drug reactions were minimal. Most commonly were pyoderma, Malassezia infestations, diarrhea and
leukocytosis.27
Due to high costs and a lack of proven efficiency, this drug is not recommended as a
treatment by the researchers.114

24
2.5.2.7. Cyclosporine and Tacrolimus
Cyclosporine and tacrolimus are immunosuppressive drugs115
that are extensively used in human
medicine, especially in patients that received organ transplants.27
Both drugs have the same proposed
mechanism of action and immunomodulating properties.116
Tacrolimus is however more potent and
more toxic for dogs.27
Both drugs bind to intracellular receptors called immunophilins. More specifically, cyclosporine binds
to cyclophilin, while tacrolimus binds to FK506-binding proteins. Thereby, they inhibit calcium-
dependent pathways including that of calcineurin. Calcineurin is a calmodulin-dependent protein
phosphatase. This enzyme activates nuclear factor of activated T-cells (NF-AT) by dephosphorylation.
NF-AT is a transcription factor of T-cells that is responsible for the initiation of interleukin synthesis.
The activated NF-AT is translocated into the nucleus and upregulates interleukin-2 synthesis.
IL-2 is important for the proliferation and differentiation of T-cells.100
As a consequence cyclosporine
causes a decrease in canine lymphocytes and immunosuppression.117, 118
It also affects different
cytokines, such as IL-2, IL-3, IL-4 and tissue necrosis factor alpha (TNF). IL-2 is also responsible for
lymphocyte proliferation.10, 115
It furthermore modifies the function of granulocytes, macrophages,
natural killer cells, eosinophils and mast cells.109
In a study from 2004 good results were achieved in
two dogs within four to six weeks with 25mg kg -1
per day. Another patient received 15mg kg -1
whereupon the clinical signs subsided. When the severity however got worse the patient did not
respond to higher doses.27, 119
A pilot study on cyclosporine carried out by Olivry investigated whether cyclosporine A (CsA)
monotherapy (microemulsified CsA) would be effective for the induction of treatment in cPF. Of the
five tested dogs only one showed mild side-effects (intermittent diarrhea). The used induction doses
was 5-10mg kg -1 administered daily. None of the dogs showed complete remission of the lesions.
Four of the five dogs were even withdrawn due to worsening of the score based on the Pemphigus
foliaceus extent and severity index (PEFESI). Based on those results cyclosporine is not
recommended as a sole therapy in the proposed doses. It might nevertheless be effective in higher
doses or in combination with oral glucocorticoids. 115
Cyclosporine can be administered orally in combination with ketoconazole or oral
glucocorticoids.Ketoconazole inhibits the hepatic microsomal isoenzyme P450 system, resulting in
increased blood cyclosporine levels, allowing lower dosages and thus reduced costs.27
The reported side-effects of cyclosporine include anorexia, emesis and diarrhea, especially during the
first days of treatment.27, 116
More severe side-effects are rare and appear to be dose-dependent.
Weight loss, nephrotoxicity, gingival hyperplasia, papillomatosis, hirsutism, hepatotoxicity,
opportunistic infections, lymphoproliferative disorders and involuntary shaking are reported.119, 116, 120
Tacrolimus shows more extensive side effects than CsA when administered orally alone or in
combination. Those adverse reactions include anorexia, vomiting, diarrhea, weight loss, impaired
glucose metabolism, marked hepatotoxicity and infections.121
Nevertheless no side-effects and good

25
results have been achieved in discoid lupus erythematosus and pemphigus erythematosus when
tacrolimus was administered topically (0.1%). 27,122
2.5.2.8. Cyclophosphamide
Cyclophosphamide is also an alkylating agent. It interferes with DNA replication by adding an alkyl-
group to DNA. It is used, among others, as a cancer therapy agent and against auto-immune
disorders. It can be used solely or in combination with other drugs. The drug is very potent and shows
thus severe side-effects such as hemorrhagic cystitis,27
anorexia, vomiting, diarrhea and weight
loss.123
Because of those undesired reactions and sufficient alternative therapies it is not used by
default. The recommended dosage is 1.5mg kg -1
every alternate day. 27
2.5.2.9. Dapsone and sulfasalazine
Dapsone is an antibiotic with anti-inflammatory features. It inhibits neutrophil chemotaxis, reduces
complement activation, antibody production and lysosomal enzyme synthesis. As described earlier are
the lesions in dogs, contrary to the human form, infiltrated with neutrophils and is dapsone thus more
effective in dogs. Dapsone should be given 1mg kg -1 every eight hours. The drug shows a delayed
effect after one to two months. The following adverse reactions are described in dogs: anemia,
neutropenia, thrombocytopenia, hepatotoxicity, gastrointestinal signs, neuropathies and cutaneous
drug eruptions. Therefore close and regular monitoring of the thrombocytes, chemistry profiles and
urinalyses are recommended.27
Sulfasalazine metabolites have anti-inflammatory features as well. It is dosed at 10-40mg kg -1
spread
over the day, thus one dose every eight hours. A big disadvantage is the risk on developing
keratoconjunctivitis sicca. Therefore it is recommended to monitor tear production as well as blood
counts and chemistry profiles regularly. Tear production is best monitored every two to four weeks,
blood counts and chemistry profile initially (first 1.5 months) every two weeks and then reduced to
every two to four months.27

26
3. WHY ARE SOME DOGS NOT RESPONSIVE TO THE TREATMENT
3.1 TREATMENT OUTCOME AND LONG-TERM PROGNOSIS
Even after a verified diagnosis of cPF there seems to be quite some variation regarding the treatment
outcome and the long-term prognosis.27
Different studies reported different outcomes. It is assumed
that this might be due to different treatment approaches as well as due to a variation of clinical signs
and disease severity.19
In a study from 1985, 37 dogs with PF were examined and followed-up for one to seven years. The
dogs were treated with different drug regimens with the following outcome: 39% responded to
corticosteroids solely, 50% responded to prednisone and cytotoxic drugs and 55% reacted to
prednisone in combination with aurothioglucose. 47% of the dogs died in less than one year.33
A more recent study that was carried out between 1994 and 2000 with 43 cPF patients aimed at
identifying the factors that can influence the outcome of cPF. The researchers recorded a case fatality
rate of 60.5%. The majority (60%) of the dogs that passed away died within the first year of treatment.
Interestingly, the survival rate increased when antibiotics were administered in the beginning of the
immunosuppressive therapy and also lowered the number of patients with adverse drug effects. That
could be explained by the patients being less susceptible to secondary bacterial infections. What is
more, the researchers detected a positive correlation between the duration of the treatment and the
survival rate. 92% of the dogs from the non-survival group had died within one year after treatment
initiation, but only two died after twelve months. That proposes a better prognosis for survival after a
certain period of time. The median of death in the non-survival group was ten months. Also the
number of complications shows a significant association with the survival rate.
The following factors were not significantly associated with prolonged survival: the sex, age at
diagnosis, previous or additional atopic or thyroidal diseases, extent of the skin involvement, time
period between clinical signs and PF-diagnosis or the administration of gastric protectants when
glucocorticoids were used. There was also no link between the survival time and whether a veterinary
dermatologist or primary care veterinarian managed the long-term treatment.
Of the dogs that died 69% (n=18) were euthanized, four dogs for causes unrelated to PF. Most of the
euthanized patients underwent two to four changes in treatment protocol, due to unsatisfying results or
unacceptable adverse drug effects, before deciding to euthanize the patient.
Remarkably, four of the treated dogs stayed in prolonged remission with no further clinical signs of PF
after discontinuation of the treatment. Also, there was no significant link between initial treatment
protocol and survival time or rate. The used initial treatment protocols comprised prednisone (n=16),
prednisone together with azathioprine (n=23), mycophenolate mofetil (n=2), tetracycline and
niacinamide (n=1) and prednisone in combination with chlorambucil (n=1). However, due to the high-
incidence of corticosteroid-related side-effects and the great amount of deaths within the first year the
authors (124)
advice to choose a combination treatment to minimalize the required corticosteroid
maintenance doses.124
However, Mueller et al described contradictory that the combination of

27
glucocorticoids and azathioprine causes more side-effects in cPF patients.99
The benefit of a
combination therapy is thus controversial.
Three other studies, one by Rosenkrantz27
and colleagues, one by Mueller99
and colleagues and one
by Kummel11
reported a more positive outcome. Rosenkrantz reported 71% of the patients still being
alive after one year of treatment.27
Mueller and colleagues examined 91 dogs, whereof only 13%
(n=11) were euthanized.99
And Kummel documented a 75% survival rate after treatment with no or few
side-effects.125
Rosenkrantz stated, similar to the findings by Gomez, (124)
that there was no significant
difference in rate or degree of remission between dogs that were treated with prednisolone alone or
together with azathioprine. However, contrary to Gomez Rosenkrantz also reported that there is no
association between the survival rate and the use of antibiotics in combination with
immunosuppressive drugs.99
Prolonged remission is described in a small number of cases after discontinuation of the
immunosuppressive therapy. In a study by Olivry et al 51 were either treated with immunosuppressive
doses of oral glucocorticoids or with glucocorticoids together with azathioprine. Clinical remission
occurred after 1.5 to 5months after initiation of the therapy. The doses was progressively reduced and
finally withdrawn. The total period of administering immunosuppressive therapy ranged between three
and 22 months. In six dogs clinical symptoms did not reappear for the duration of the trial (1.5 to
6years).103
This study suggests that a relapse of the lesions does not necessarily occur after withdrawal of the
drug and that in some dogs immunosuppressive therapy can lead to a long-term remission of the
lesions. 51 dogs met the criteria for the research and six of those went into complete and long-term
remission (12%). In a study investigating long-term outcome of treatment in humans with PV it was
found that patients with mild to moderate PV were twice as likely to undergo complete remission
compared to those with severe lesions.126
A similar research by Mueller and colleagues found that the
distribution of the lesions, localized versus generalized, had no effect on resolving of the lesions or
death and that 7-22% of the affected dogs stayed in remission after ending the immunosuppressive
therapy. 99
Another finding by Olivry et al was that patients with a rapid response to the
immunosuppressive therapy were more likely to benefit from prolonged remission.127
In contrast, in
dogs the severity of the disease appears to play no major role in long term remission. The average
time to undergo complete remission after initiating the therapy was two months.126
3.2 POSSIBLE REASONS WHY SOME DOGS ARE NOT RESPONDING
To the best of our knowledge, there are no studies investigating why a conspicuous number of dogs
are unresponsive to the treatment. Nevertheless, research is giving some hints why some cPF
patients might not be responsive.

28
3.2.1. Incorrect diagnosis
A possible cause could be an incorrect diagnosis. As described earlier, pemphigus foliaceus is an
heterogenous disease with a wide variety of clinical features. It is thus important to rule out other
differential diagnostics for pustular dermatitis , such as pustular dermatophytosis.126
3.2.2. Naturally or drug-related pemphigus
In those cases where the history is unknown, it is impossible to determine with certainty if PF is
naturally occurring or if it is induced or triggered by drugs.To verify the diagnosis a drug provocation
test should be done. This provocative test is carried out rarely due to the potential risk for the patient.
The diagnosis of drug related PF is thus based on history, clinical signs, histopathology and the
response to drug withdrawal.126
Rosenkrantz states in a report that many cases that are actually drug
induced, have been misleadingly accredited to chronic diseases and have often been treated with
long-term drugs.128
3.2.3. Drug regime
In the study from Olivry et al investigating the long-term remission, it becomes obvious that there is no
static therapy regime and dosage. Each of the patients received a different drug therapy and dosage
depending on the individual response. In the six studied cases patient one did not react to initial
prednisone therapy, therefore azathioprine was added and the lesions resolved. Case number two
showed marked improvement on prednisone alone. The third and fourth case required prednisone as
well as azathioprine before clinical remission occurred. Case five and six were initially treated with
only prednisolone and due to unacceptable adverse side-effects prednisolone dosage was reduced
and azathioprine added with a positive outcome. Also, each dog received a different dosage of
glucorticoids (and azathioprine) which was adapted if necessary. For a satisfying outcome it is thus
important to find the right dosage, frequency of administration and the right combination of drugs
(antibiotics, corticosteroids, chrysotherapy, azathioprine etc or combination of those?) for each patient
individually.126
Especially for the chrysotherapy, dapsone, azathioprine and, tetracycline and niacinamide a lag-phase
is described. Depending on the used agent it is important to not stop the therapy after a lack of
response too early.27, 109
3.2.4. Glucocorticoid resistance
Glucocorticoids are the first-line therapy for the treatment of pemphigus diseases yet some patients do
not respond. That might be due to the development of resistance. To investigate glucocorticoid
resistance in PF patients a study evaluated the glucocorticoid sensitivity. The sensitivity was analyzed
on the basis of the number of binding sites, the affinity of glucocorticoid receptors to dexamethasone
and the cytokine pattern. The number of binding sites, as well as the affinity of the receptors were

29
found to be significantly higher in pemphigus patients compared to a control group. Furthermore the
study showed a higher production of pro-inflammatory cytokines in human PF patients, especially of
IL-6 and TNFα. In summary, the study showed a pro-inflammatory cytokine profile and altered
glucocorticoid sensitivity in PF patients. That might be an indication that pro-inflammatory cytokines
play a role in developing glucocorticoid resistance in human pemphigus patients. 129
Another proposed explanation for the insufficient response could be an increased expression and/or
function of P- glycoprotein in lymphoid cells. The protein is located in the cell membrane and by being
able to pump foreign substances out of cells it can influence the bioavailability of the drugs. These
proteins might thus be capable of reducing the intracellular concentration of glucocorticoids, thereby
weakening its therapeutic effects. Research however found neither increased p-glycoprotein levels in
pemphigus patients that responded poor to steroids, nor differences in p-glycoprotein activity.
Consequently, p-glycoprotein does not seem to be involved in the poor response to steroid treatment
seen in some pemphigus patients. 130
3.2.5 Influence of 25-hydroxyvitamin D concentrations
The active form of vitamin D is well known for its properties of regulating calcium levels in the blood
and assuring bone health. As described earlier, calcium is also essential for the functioning of
glucocorticoids and has an impact on the expression of cell surface molecules. Recent research
revealed further effects of vitamin D on the immune system,132
especially on T-cells. It has been
proven in animal models that 1,25-dihydroxyvitamin D3 can prevent or suppress certain autoimmune
diseases. A proposed mechanism therefore is an influence on the cytokine profile which might
consequently suppress inflammatory T-cell activity.133 Another study investigated the relationship
between 25hydroxy-vitamin-D serum concentrations and the response to a subsequent
glucocorticoid-therapy in dogs with atopic dermatitis. Interestingly, dogs that showed a a good
response to the glucocorticoid treatment also had significantly higher pretreatment serum 25(OH)D
concentrations compared to dogs with a poor response. That might be an indication that vitamin D has
a synergistic therapeutic effect with glucocorticoids and that low vitamin D-serum concentrations might
attenuate the response. Further research to confirm or refute this hypothesis is necessary.134
3.2.6. Tachyphylaxis to topical glucocorticoids, is it proven?
Tachyphylaxis( the fast onset of tolerance) to topical glucocorticoids has been reported in literature
and is an widely accepted belief. A study was conducted reviewing relevant published articles on the
internet, to look for evidence to support this concept. Although they found 52 relevant articles they
could not find proof that glucocorticoid treatments are susceptible to tachyphylaxis. Although some of
the described effects indeed resembled tolerance effects, the clinical significance however is not
known nor proven. The authors assume that the described phenomenon of tolerance is due to other
factors such as poor adherence of the therapy over time or that the drugs have a maximum effect in
the first weeks resulting in remission but only to a certain degree.135

30
4. Discussion
In the last decades much research regarding canine pemphigus foliaceus has been conducted and
much knowledge was gained. Nevertheless, compared with the human form of PF little is known about
the pathogenesis and even less is proven. Many pathogenic factors have been associated with the
disease and many possible pathological mechanisms proposed. However the exact pathogenic role
and importance of most of them are still unclear or questionable. Some of the studies mentioned
above even described contradictory results.
Not all the findings from human research can furthermore be extrapolated to dogs. For example cPF
involves a strong neutrophilic infiltration of the pustules, which can only be found in seldom cases of
human PF. The same applies to the therapies. Veterinary immunosuppressive therapeutics were
initially adopted from human medication and research, and thus knowledge of their therapeutic
efficacy and potential for adverse effects in dogs remains limited. Most of the studies are also
retrospective, a blinded prospective study especially regarding treatment protocols could bring more
clarity.
The majority of the canine patients reacts well to the treatment protocols and receives remission. A
few of the patients however, initially or after a relapse, do not respond to glucocorticoids (anymore).
Different reasons have been proposed but little research was conducted to investigate this issue and
no satisfactory explanation can be given yet. Thus also here, more research is needed.
In summary, this literature study shows that cPF is a very interesting and complex disease. It has
been getting an increasing degree of awareness among scientists and veterinarians in the last
decades and much progress has been made. There are however, still many open questions that
require further attention. Answers to the remaining questions about especially the
immunopathogenesis could help to develop a more specific treatment with minimal side-effects.

5. References
1. Korman N. (1988). Continuing medical education: Pemphigus. Journal of the American
academy of dermatology. 18 (6):1219-1238
2. Day M.J., Hanlon L. and Powell L.M. (1993) Immune-mediated skin diseases in the dog and
cat. Journal of comparative pathology. 109 (4): 395-407
3. Manning T.O., Scott D.W., Smith C.A. et al. (1983) Pemphigus and Pemphigoid in dogs,
cats and horses. Annals of the New York Academy of sciences.420:353-360
4. Preziosi D.E., Goldschmidt M.H., Greek J.S. et. al (2003) Feline pemphigus foliaceus : a
retrospective analysis of 57 cases. Veterinary Dermatology. 14 (6):313-321
5. Vandenabeele S.I., White S.D., Affolter V.K. et al. (2004) Pemphigus foliaceus in the horse:
a retrospective study of 20 cases. Veterinary dermatology. 15(6):381-388
6. Pappalardo E., Abramo F. and Noli C. (2002) Pemphigus foliaceus in a goat. Veterinary
Dermatology.13(6):331-336.
7. Brenner D.J., Stokking L. Donovan T.A. et al (2009) Pemphigus foliaceus in a Barbary
sheep (Ammotragus lervia). The Veterinary record. 165(17): 509-510
8. Noli C. and Scarampella F. (2005) 2nd
edition. Praktische Dermatologie bei Hund und Katze.
Schlütersche Verlagsgesellschaft mbH &Co KG. p.271-277
9. Birchard J.E. and Robert Sherding. (2006) 3rd edition. Saunders Manual of small animal
practice. Saunders Elsevier. St. Louis. p.492-499.
10. Hnilica K.A. (2010) 3rd
edition. Dermatology: a color atlas and therapeutic guide. Saunders
Elsevier. Knoxville, Tennessee. Chapter: Autoimmune and Immune-mediated skin
disorders.p. 227
11. Campbell C.L. (2004) 1st edition. Small animal dermatology secrets: 32. Immune mediated
skin diseases. Hanley& Belfus. Philadelphia.p.231-243
12. Gershwin L.J. (2010) Autoimmune diseases in small animals. Veterinary clinics of North
America: Small animal practice. 40(3): 439-457
13. Scarff D. (2009) Pemphigus in the dog and cat. Part 1: Aetiology, pathogenesis and clinical
signs. UK Vet Companion animal. 14(9):1-4
14. Garrod D. and Chidgey M. (2008) Desmosome structure, composition and function.
Biochimica et Biophysica Acta- Biomembranes. 118 (3): 572-587
15. Olivry T. and Linder K.E. (2009) Dermatoses affecting desmosomes in animals: a
mechanistic review of acantholytic blistering skin diseases. Veterinary Dermatology. 20 (5)
313-326
16. Amagai M. et al. (1996) Pemphigus Vulgaris Antigen (Desmoglein-3) Is Localized in the
Lower Epidermis, the Site of Blister Formation in Patients. Journal of Investigative
Dermatology .106:351-355
17. Scott D.W. (1983) Pemphigus in Domestic Animals. Clinics of dermatology. 1(2):141-152
18. Goldsmith L.A., Katz S.I., Gilchrest B.A. et al. (2012) 8th edition. Mcgraw-Hill Publ.Comp.
New York. Chapter 54: Pemphigus.

19. Olivry T. (2006) A review of autoimmune skin diseases in domestic animals: I- Superficial
pemphigus. European society of veterinary dermatology. 17(5):291-305
20. Wurm S., Mattise A.W., Dunstan R.W. (1994) Comparative pathology of pemphigus in dogs
and humans. Clinics in dermatology.12(4):515-524
21. Scarff D., (2009) Pemphigus in the dog and cat. Part 1:Aetiology, pathogenesis and clinical
signs. UK Vet Companion animal. 14(9):1-4
22. Elmore S. A., Basseches J., T. Olivry et al (2005) Paraneoplastic Pemphigus in a Dog with
Splenic Sarcoma. Veterinary Pathology. 42(1): 88-91
23. Nishifuji K., Olivry T., Ishii K. et al (2007) IgG autoantibodies directed against desmoglein 3
cause dissociation of keratinocytes in canine pemphigus vulgaris and paraneoplastic
pemphigus. Veterinary Immunology and Immunopathology.117 (3-4): 209-221
24. De Bruin A., Müller E., Wyder M. et al (1999) Periplakin and envoplakin are target antigens
in canine and human paraneoplastic pemphigus. Journal of the American Academy of
Dermatology. 40(5):682-685
25. Kazerounian S., Mahoney M.G., Uitto J. et al (2000) Envoplakin and periplakin, the
paraneoplastic pemphigus antigens, are also recognized by pemphigus foliaceus
autoantibodies. Journal of Investigative Dermatology. 115: 505-507
26. Lemmens P., De Bruin A., De Meulemeester J. et al. (1998) Paraneoplastic pemphigus in a
dog. Veterinary Dermatology. 9(2):127-134
27. Rosenkrantz W.S. (2004) Pemphigus: current therapy. Veterinary Dermatology. 15(2): 90-
98
28. Halliwell, R.E.W. and Goldschmidt, M.H. (1977) Pemphigus foliaceus in the canine: A case
report and discussion. Journal of the American Animal Hospital Association. 13: 431-436
29. Werner L.L., Brown K.A., Halliwell R.E.W. (1983) Diagnosis of autoimmune skin disease in
the dog: correlation between histopathologic, direct immunofluorescent and clinical findings.
Veterinary immunology and Immunopathology. 5(1): 47-65
30. Day M.J., Hanlon L. and Powell L.M. (1993). Immune-mediated skin disease in the dog and
cat. Journal of comparative pathology.109 (4): 395-407
31. Ruocco V., Ruocco E., Schiavo A.L. et al (2013) Pemphigus: Etiology, pathogenesis, and
inducing or triggering factors: Facts and controversies. Clinics in Dermatology. 31(4): 374-
381
32. Odaguiri J., Lucarts L., Mchalany N et al (2012) Canine pemphigus foliaceus: a
retrospective study of 102 cases (1986-2011) in Sao Paulo, Brazil. Veterinary Dermatology.
23 (Suppl.1): 2-104
33. Ihrke PJ, Stannard AA. Ardans AA et al. (1985) Pemphigus foliaceus in dogs: a review of 37
cases. Journal of the American Veterinary Medical Association. 186(1): 59-66 (abstract)
34. Scott DW, Walton DK, Slater MR et al.(1987) Immune-mediated dermatoses in domestic
animals: ten years after-Part I. Compendium on continuing education for the practicing
Veterinarian. 9: 424-35.

35. Bizikova P., Linder K.E. and olivry T. (2011) Immunomapping of desmosomal and
nondesmosomal adhesion molecules in healthy canine footpad, haired skin and buccal
mucosal epithelia: comparison with canine pemphigus foliaceus serum immunoglobulin G
staining patterns. Veterinary Dermatology.22(2)132-142
36. Evangelista F., Dasher D.A., Diaz L.A. et al. (2008) E-cadherin is an additional
immunological target for pemphigus autoantibodies. Journal of Investigative
Dermatology.128:1710-1718
37. Waschke J. (2008) The desmosome and pemphigus. Histochemistry and cell biology
130(1):21–54
38. Kitajima Y. (2013) New insights into desmosome regulation and pemphigus blistering as a
desmosome-remodeling disease. Kaohsiung Journal of Medical Science. 29(1): 1-13
39. Tu C.L., Oda Y. and Bikle D.D.(2000) Effects of a calcium receptor activator on the cellular
response to calcium in human keratinocytes. Journal of investigative Dermatology.113(3):
340-345
40. Oda y., Tu C.L., Chang W. et al ( 2000) The calcium sensing receptor and its alternatively
spliced form in murine epidermal differentiation. Journal of biological Chemistry. 275(2):
1183-1190
41. Tu C.L., Chang W., Bikle D.D. (2001) The extracellular calcium sensing receptor is required
for calcium-induced differentiation in human keratinocytes. Journal of biological Chemistry.
276(44): 41079-41085.
42. Sheu H.M., Kitayama Y. and Yaoita H. (1989) Involvement of protein kinase C in
translocation of desmoplakins from cytosol to plasma membrane during desmosome
formation in human squamous cell carcinoma cells grown in low and normal calcium
concentration. Experimental cell research journal. 185(1): 176-190
43. Kitajima Y., Aoyama Y. and Seishima M. (1999) Transmembrane signaling for adhesive
regulation of desmosomes and hemidesmosomes, and for cell-cell detachment induced by
pemphigus Igg in cultured keratinocytes: involvement of protein kinase C. Journal of
investigative dermatology symposium proceedings. 4(2): 137-144
44. Xie Z., Bikle D.D. (2007) The recruitment of phosphatidylinositol 3-kinase to the E-cadherin-
catenin complex at the plasma membrane is required for calcium-induced phospholipase C-
gamma1 activation and human keratinocyte differentiation. Journal of biological
Chemistry.282(2): 8695-8703
45. Berridge M.J. and Irvine R.F. (1982) Inositol triphosphate, a novel second messenger in
cellular signal transduction. Nature. 312: 315-321
46. Olivry T., LaVoy A., Dunston SM et al ( 2006). Desmoglein-1 is a minor autoantigen in dogs
with pemphigus foliaceus. Veterinary immunology and immunopathology. 110(3-4): 245-255

47. Bizikova P., Dean G.A., hashimoto T and olivry T. (2012) Cloning and establishment of
canine desmocollin-1 as a major autoantigen in canine pemphigus foliaceus. Veterinary
Immunology and Immunopathology. 149(3-4): 197-207
48. Olivry T., Dunston S.M., Walker R.H. et al (2008) Investigations on the nature and
pathogenicity of circulating antikeratinocyte antibodies in dogs with pemphigus foliaceus.
Veterinary dermatology. 20(1): 42-50
49. Emery D.J., Diaz L.K., Fairley J.A. et al (1995). Pemphigus Foliaceus and Pemphigus
Vulgaris Autoantibodies React with the Extracellular Domain of Desmoglein-1. Journal of
Investigative Dermatology. 104(3): 323–328
50. Iwasaki T, shimizu M, Obata H. et al ( 1997). Detection on pemphigus foliaceus autoantigen
by immunoblotting. Veterinary immunology and immunopathology. 59(1-2): 1-10
51. Yabuzoe A., Shimizu A., Nishifuji K. et al (2009) Canine pemphigus foliaceus antigen is
localized within desmosomes of keratinocyte. Veterinary Immunology and
immunopathology. 127(1-2): 57-64
52. Chidgey, M., Brakebusch, C., Gustafsson, E., et al. (2001)Mice lacking desmocollin 1 show
epidermal fragility accompanied by barrier defects and abnormal differentiation. Journal of
cellular biology. 155(5): 821–832
53. Starr T.K., Jameson S.C. and Hogquist K.A.(2003) Positive and negative selection of T-
cells. Annual review of immunology. 21:139-176
54. Heng A., Nwaneshiudi A., Hashimoto T. et al ( 2006) Intraepidermal neutrophilic IgA/ IgG
antidesmocollin 1 pemphigus. British journal of dermatology. 154(5): 1018- 1020
55. Olivry T., Alhaidari Z., Gohestani R.F. et al (2000) Anti-plakin and desmoglein
autoantibodies in a dog with pemphigus vulgaris. Veterinary pathology. 37(5): 496-499
56. Yabuzoe A., Iwasaki T., Nishifuji K. et al (2008) Neutrophils contact to plasma membrane of
keratinocytes including desmosomal structures in canine pemphigus foliaceus.70(8): 807-
812
57. Scott D.W. and Lewis R.M. (1981) Pemphigus and pemphigoid in dog and man:
comparative aspects. Journal of the American Academy of Dermatology. 5(2): 148-167
58. Calkins C.C., Setzer S.V., Jennings J.M. et al (2006) Desmoglein endocytosis and
desmosome disassembly are coordinated responses to pemphigus autoantibodies. Journal
of Biological chemistry.281(11): 7623-7634
59. O`Toole E.A., Mak L.L., Guitart J. et al (2000) Induction of keratinocyte IL-8 expression and
secretion by IgGautoantibodies as a novel mechanism of epidermal neutrophil recruitment
in a pemphigus variant. Clinical and experimental immunology. 119(1): 217-224
60. Bizikova P., Olivry T., Mamo L.B. and Dunston S.M. (2014) Serum autoantibody profiles of
IgA, IgE and IgM in canine pemphigus foliaceus. Veterinary Dermatology. 25(5): 471-475

61. Hisamtasu Y., Amagai M., Garrod D.R., et al (2004) The detection of IgG and IgA
autoantibodies to desmocollins 1-3 by enzyme-linked immunosorbent assays using
baculovirus-expressed proteins, in atypical pemphigus but not in typical pemphigus. British
Journal of Dermatology. 151(1): 73-83
62. Heng A., Nwaneshiudu A., Hashimoto et al (2006) Intraepidermal neutrophilic IgA/IgG
antidesmocollin 1 pemphigus.British Journal of Dermatology. 154(5): 1018-1020
63. Tsuruta D., Ishii N., Hamada T. et al (2011) IgA pemphigus. Clinics of Dermatology. 29(4):
437-442
64. Mazza G., Whiting A.H., Day M.J. et al (1994) Preparation of monoclonal antibodies specific
for the subclasses of IgG.Research in Veterinary science. 57: 133-139
65. Iwasaki T. , Shimizu M. Obata H. et al (1996) Effect of substrate on indirect
immunofluorescence test for canine pemphigus foliaceus. Veterinary Pathology.33(3):332-
336
66. Iwasaki T., Shimizu M., Obata H. et al (1997)Detection of canine pemphigus foliaceus
autoantigen by immunoblotting. Veterinary pathology and immunopathology.59(1-2):1-10
67. Bizikova P., Linder K.E. and Olivry T. (2014) Fipronil- amitraz-S-methoprene-triggered
pemphigus foliaceus in 21 dogs: clinical, histological and immunological characteristics.
Veterinary Dermatology. 25(2):103 -111
68. Brenner S., Mashiah J., Tamir E. et al (2003) Pemphigus: an acronym for a disease with
multiple etiologies. Skinmed. 2(2): 163-167
69. Grando S.A. (2006) Cholinergic control of epidermal cohesion. Experimental dermatology.
15(4): 265- 282
70. Waschke J., Bruggeman P., Baumgartner W. et al (2005) Pemphigus foliaceus IgG causes
dissociation of desmoglein 1-containing junctions without blocking desmoglein 1
transinteraction. The Journal of clinical investigation. 115(11): 3157-3165
71. Hanakawa Y., Amagai M., Shirakata Y. et al (2002) Differential effect of Dsg1 and Dsg3 on
desmosome formation. Journal of Investigative Dermatology. 119: 1231- 1236
72. Suter et al. (1993) Identification of canine pemphigus antigens. In: Ihrke PJ, Mason IS,
Whitse SD eds. Advances in Veterinary dermatology. Vol1 Oxford, UK: Pergamon Press, p.
376-380
73. Suter M.M., de Bruin A, Wyder M et al (1996) Autoimmune diseases of domestic animals:
an update. In: Kwochka K, Willemse T, von Tscharner C eds Advances in veterinary
dermatology. Vol.3. oxford, UK: Butterworth- Heinemann.p. 321-337
74. Nishikawa T., Kurihara S., Harada T. et al ( 1977) Capability of complement fixation of
pemphigus antibodies in vitro. Archives for dermatological research. 260: 1-6

75. Seishima M., Esaki C., Osada K et al (1995) Pemphigus IgG, but not bullous pemphigoid
IgG, causes a transient increase in intracellular calcium and inositol 1,4,5-triphosphate in
DJM-1 cells, a squamous cell carcinoma line. Journal of investigative dermatology.
104(1):33–37
76. Esaki C.,Seishima M., Yamada T. et al (1995) Pharmacologic evidence for involvement of
phospholipase C in pemphigus IgG-induced inositol 1,4,5-trisphosphate generation,
intracellular calcium increase, and plasminogen activator secretion in DJM-1 cells, a
squamous cell carcinoma line. Journal of investigative dermatology. 105(3):329–333
77. Osada K., Seishima M., Kitajima Y. (1997) Pemphigus IgG activates and translocates
protein kinase C from the cytosol to the particulate/cytoskeleton fractions in human
keratinocytes. Journal of investigative dermatology 108(4):482–487
78. Waschke J., Spindler V.,Bruggeman P. et al. (2006) Inhibition of Rho A activity causes
pemphigus skin blistering. Journal of cell biology. 175(5):721–727
79. McBeath R, Pirone D.M., Nelson C.M., et al (2004). Cell shape, cytoskeletal tension, and
RhoA regulate stem cell lineage commitment. Developmental cell 6 (4): 483–495
80. Noxon J.O. and Myers R.K. (1989) Pemphigus foliaceus in two Shetland sheepdog
littermates. Journal of the American veterinary medical association. 194(4): 545-546
81. Moraes J.R., Moraes M.E.,Fernandez-Vina M, et al (1991) HLA antigens and risk for
development of pemphigus foliaceus (fogo selvagem) in endemic areas of Brazil.
Immunogenetics. 33: 388-391
82. Pascal A., Shiebert J. Ihrke P. (1995) Seasonality and environmental risk factors for
pemphigus foliaceus in animals: a retrospective study of 83 cases presented to the
veterinary medical teaching hospital, University of California Davis from 1976 and 1994
(abstract). In: Proceedings of the 11th AAVD/ACVD Meeting, Santa Fe, p.24-25
83. Iwasaki T., Maeda Y. (1997) The effect of ultraviolet (UV) on the severity of canine
pemphigus erythematosus (abstract). In: American academy of veterinary Dermatology and
American College of Veterinary Dermatology Annual Meeting, Nashville, TN 1997;86
84. Hanakawa, Y.,Matsuyoshi N., Stanley J.R. et al (2002) Expression of desmoglein 1
compensates for genetic loss of desmoglein 3 in keratinocyte adhesion. Journal of
Investigative Dermatology (2002). 119(1): 27–31
85. Carew B.J. and Wagner G. (2014). Cutaneous pemphigus vulgaris with absence of
desmoglein 1 autoantibodies. An example of the extended desmoglein compensation
theory. Australasian Journal of Dermatology. 55(4): 292-295
86. Moriello K.A., Behr M. (2012) Pemphigus-like drug reaction in a dog after a single
application of Vectra 3D. Veterinary Dermatology. 23(Suppl.1): 77 (abstract)

87. Bizikova P. (2015) Pemphigus foliaceus- recent update on the pathogenesis, diagnosis and
treatment. In: the webinar vet- veterinary education made easy. Published 16 February
2015. http://www.thewebinarvet.com/2015/02/pemphigus-foliaceus-recent-update-on-the-
pathogenesis-diagnosis-and-treatment/ (Consulted: 14.03.2015)
88. Brenner S., Wolf R, Ruocco V.(1994) Contact pemphigus: a subgroup of induced
pemphigus. International journal of dermatology. 33(12): 843-845
89. Wohl Y., Goldberg I. and Brenner S. (2004) Chlorpyrifos as a possible pemphigus-inducing
pesticide- an in vitro study. Journal of the American Academy of dermatology. 50 (Suppl):94
(abstract)
90. Brenner S., Goldberg I. (2011) Drug-induced pemphigus. Clinics in Dermatology. 29: 455-
457
91. C. Noli , J.P. Koeman and T. Willemse (1995) A retrospective evaluation of adverse
reactions to trimethoprim‐sulphonamide combinations in dogs and cats. Veterinary
Quarterly. 17(4):123-128
92. White S.D., Carlotti D.N., Pin D. et al (2002) Putative drug-related pemphigus foliaceus in
four dogs. Veterinary Dermatology. 13(4): 195-202
93. Medleau L., Shanley K.J, Rakich, P.M. (1990) Trimethoprim-sulfonamide-associated drug
eruptions in dogs. Journal of the American Animal Hospital Association. 26(3): 305-311
94. Rust M.K., Rugg D. and Rock D. (2007) Metaflumizone- a new ectoparasiticide for dogs and
cats. Veterinary Parasitology. 150(3):175-176
95. Tizard I.R. (2012) Veterinary immunology: An introduction. 9th edition. St Louis, M.O.:
Elsevier Saunders.p 551
96. Bizikova P, Moriello K.A., Linder K.E. et al (2015) Pyriproxyfen/permethrin pemphigus-like
drug reaction in three dogs. Veterinary dermatology march 2015 (early preview) . Wiley
online library. Published 10 march 2015. (Consulted: 09.04.2015)
97. Rybnicek J. and Hill P.B. (2007) Suspected polymyxin B-induced pemphigus vulgaris in a
dog. Veterinary Dermatology. 18(3): 165-170
98. Horvath C., Neuber A. and Litschauer B. (2007) Pemphigus foliaceus-like drug reaction in a
3-month-old crossbred dog treated for juvenile cellulitis. Veterinary Dermatology. 18(5):
353-359
99. Mueller R.S., Krebs I., Power H.T. et al (2006) Pemphigus foliaceus in 91 dogs. Journal of
the American Animal Hospital Association. 42(3): 189-196
100. Boumpas D.T., Chrousos G.P., Wilder R.L. et al (1993) Glucocorticoid therapy for
immune-mediated diseases: Basic and clinical correlates. Annals of internal medicine.
119(12): 1198-1208

101. Werth V.P., Lazarus G.S. (1999) Systemic glucocorticoids. In: Freedberg I.M., Eisen
A.Z., Wolff K. et al., eds. Fitzpatrick`s Dermatology in general medicine V. New York: Mc
Graw-Hill. p.2783-2789
102. Fauci A.S., Dale D.C. and Balow J.E.. (1976) Glucocorticosteroid therapy:
mechanisms of action and clinical considerations. Annals of internal medicine. American
college of physicians. 84 (3): 304-315(abstract)
103. Galili N., Galili U., et al (1980) Human T lymphocytes become glucocorticoid-sensitive
upon immune activation. Cellular Immunology. 50(2):440-444
104. Nieto M.A., Gonzalez A., Gambon F. et al (1992) Apoptosis in human thymocytes after
treatment with glucocorticoids. Clinical and Experimental Immunology. 88(2):341-4.
105. Boumpas D.T., Paliogianni F., Anastassiou E.D. et al (1991) Glucocorticosteroid
action on the immune system: molecular and cellular aspects. Clinical and Experimental
Rheumatology. 9(4):413-23
106. Almawi W.Y., Lipman M.L., Stevens A.C. et al (1991) Abrogation of glucocorticoid-
mediated inhibition of T cell proliferation by the synergistic action of IL-1, IL-6, and IFN.
Journal of immunology. 146(10):3523-3527
107. Butler W.T. and Rossen R.D. (1973) Effects of corticosteroids on immunity in man:
decreased serum IgG concentration caused by 3 or 5 days of high doses of
methylprednisoloneJournal of clinical investigation. 52 (10):2629-2640
108. Notari L. and Mills D. (2011) Possible behavioral effects of exogenous corticosteroids
on dog behavior: a preliminary investigation. Journal of Veterinary behavior. 6(6): 321-327
109. Viviano K.R. (2013) Update on Immunosuppressive Therapies for dogs and cats.
Veterinary Clinics of North American Small Animal Practices. 43(5):1149-1170
110. Houston D.M., Taylor J.A. (1991) Acute pancreatitis and bone marrow suppression in
a dog given azathioprine. Canadian Veterinary Journal. 32(8): 496-497
111. Schwab M., Schaffeler E., Marx C. et al (2002) Azathioprine therapy and adverse drug
reactions in patients with inflammatory bowel disease: impact of thiopurine S-
methyltransferase polymorphism. Pharmacogenetics. 12 (6): 429-436
112. Kummel B.A. (1995) Medical treatment of canine pemphigus-pemphigoid. In:
Bonagura, J.D., ed Kirk`s current Veterinary Therapy XII. Philadelphia: W.B. Saunders.
P.636-638
113. White S.D., Rosychuk R.A.W., Reinke S.I. et al (1992) Use of tetracycline and
niacinamide for treatment of autoimmune skin disease in 31 dogs. Journal of the American
Veterinary Medical association. 200(10): 1497-1500

114. Byrne K.P. and Morris K.O. (2001) Study to determine the usefulness of
mycophenolate mofetil for the treatment of pemphigus foliaceus in dogs. Veterinary
Dermatology. 12:226
115. Olivry T., Rivierre C. and Murphy K.M. (2003) Efficacy of cyclosporine for treatment
induction of canine pemphigus foliaceus. Veterinary record. 152: 53-54
116. Guaguère E., Steffan J. and Olivry T. (2004) Cyclosporin A: a new drug in the field of
canine dermatology. Veterinary Dermatology. 15(2): 61-74
117. Archer T.M., Fellman C.L., and Stokes J.V. et al (2011) Pharmacodynamic monitoring
of canine T-cell cytokine responses to oral cyclosporine. Journal of Veterinary Internal
medicine. 25(6): 1391-1397
118. Fellman C.L., stokes J.V., Archer T.M. et al (2011) Cyclosporine A affects the in vitro
expression of T-cell activation-related molecules and cytokines in dogs. Veterinary
immunology and immunopathology. 140(3-4): 175-180
119. Rosenkrantz W.S, Griffin C.E. and Barr R.J. (1989) Clinical evaluation of cyclosporine
in animal models with cutaneous immune-mediated disease and epitheliotrophic lymphoma.
Journal of the American Animal Hospital Association. 25: 377-384
120. Robson D. (2003) Review of the pharmacokinetics, interactions and adverse reactions
of cyclosporine in people, dogs and cats. Veterinary record. 152(24): 739-748
121. Kelly P.A., Burckart G.J., Venkataramanan R. (1995) Tacrolimus: a new
immunosuppressive agent. American Journal of Health- Systematic Pharmacology. 52(14):
1521-1535
122. Griffies J.D., Mendelsohn C.L., Rosenkrantz W.S. et al (2004) Topical 0.1% tacrolimus
for the treatment of discoid lupus erythematosus and pemphigus erythematosus Journal of
the American Animal Hospital association. 40(1): 29-41
123. Amber E.I., Henderson R.A., Adeyanju J.B. et al (1990) Single-drug chemotherapy of
canine transmissible Veneral tumor with cyclophosphamide, methotrexate, or Vincristine.
Journal of Veterinayr Internal Medicine. 4(3): 144-147
124. Gomez S.M., Morris D.O., Rosenbaum M.R. et al (2004) Outcome and complications
associated with treatment of pemphigus foliaceus in dogs: 43 cases (1994-2000). Journal of
the American Veterinary medical association. 224(8): 1312-1316
125. Kummel B.A. (1995) Medical treatment of canine pemphigus and pemphigoid: In:
Bonagura J., ed. Kirk`s current veterinary therapy XII. Philadelphia: WB Saunders Co. p.
636-638
126. Olivry T., Bergvall K.E. and Atlee B.A. (2004) Prolonged remission after
immunosuppressive therapy in six dogs with pemphigus foliaceus. 15(4): 245-252,

127. Herbst A. and Bystryn J.C. (2000) Patterns of remission in pemphigus vulgaris.
Journal of the American Academy of Dermatology. 42(3): 422-427
128. Rosenkrantz W.S. (1993) Pemphigus foliaceus. In: Griffin C.E., Kwochka K.W.,
MacDonald J.M. eds. Current Veterinary Dermatology. St Louis, MO: Mosby.p. 141-148
129. Chriguer R.S., Roselino A.M., De Castro M. (2012) Glucocorticoid sensitivity and
proinflammatory cytokines pattern in pemphigus. Journal of Clinical Immunology. 32 (4):
786-793
130. Nishifuji K., Yoshida- Yamakita K. and Iwasaki T. (2005) A canine pemphigus
foliaceus case showing parallel relationship of disease activity and titer of serum anti-
keratinocyte cell surface antibodies. Journal of Veterinary medical science. 67(9): 943-945
131. Oberkirchner U., Olivry T., Bizikova P. et al (2011) Metaflumizone-amitraz (Promeris)-
associated pustular acatholytic dermatitis in 22 dogs: evidence suggests contact drug-
triggered pemphigus foliaceus. Veterinary Dermatology. 22(5): 217-225
132. Miller J. and Gallo R.L. (2010) Vitamin D and innate immunity. Dermatologic therapy.
23(1): 13-22
133. Deluca H.F. and Cantorna M.T. (2001) Vitamin D: its role and uses in immunology.
The FASEB Journal. 15 (4): 2579-2585
134. Kovalik M., Thoday K.L., Berry J. et al (2012) Prednisolone therapy for atopic
dermatitis is less effective in dogs with lower pretreatment serum 25-hydroxyvitamin D
concentrations. Veterinary Dermatology 23(2): 125-130
135. Taheri A., Cantrell J. and Feldman S.R. (2013) Tachyphylaxis to topical
glucocorticoids; what is the evidence? Dermatology online journal.19(7):1
Figures
o Figure 1: Campbell C.L. (2004) 1st edition. Small animal dermatology secrets: 32. Immune
mediated skin diseases. Hanley& Belfus. p.231-243
o Figure 2,3. : Dr. Elisa Maina. Private archive
o Figure 4: Waschke J. (2008) The desmosome and pemphigus. Histochemistry and cell biology
130:21–54
o Figure 5,6,: Bizikova et al (2010) Immunomapping of desmosomal and nondesmosomal
adhesion molecules in healthy canine footpad, haired skin and buccal mucosal epithelia:
comparison with canine pemphigus foliaceus serum immunoglobulin G staining patterns.
Veterinary Dermatology. 22(2):132-142




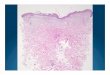




![Oral Manifestations of Pemphigus Vulgaris: Clinical ... · bullous pemphigus, and paraneoplastic pemphigus [4]. The differential diagnosis includes other dermatological diseases with](https://img.pdfslide.us/doc/110x75/5cbb138688c9930c5f8bb27d/oral-manifestations-of-pemphigus-vulgaris-clinical-bullous-pemphigus-and.jpg)