Embed Size (px)
Citation preview

Gut 1995; 36: 407-410
Pelvic and perineal complications of Crohn'sdisease: assessment using magnetic resonance
imaging
P J Haggett, N R Moore, J D Shearman, S P L Travis, D P Jewell, N J Mortensen
AbstractThis study evaluated the role of magneticresonance imaging (MRI) in the demon-stration ofthe pelvic and perianal compli-cations of Crohn's disease. Twenty fivepatients with active Crohn's disease werestudied (12 male; mean age 41.1 years).MRI examinations were performed usinga 1*5 Tesla system, within 14 days afterclinical assessment. Ti and T2 weightedfast spin echo sequences in two or threeorthogonal planes were performed, withfat suppression in some cases. The MRIresults were correlated with surgical andclinical findings. In 16 patients, cuta-neous, deep perineal or enterovesical fis-tulas or abscesses were diagnosed at MRIwhich showed close correlation with find-ings at examination under anaesthetic. Ineight patients no fistulas or abscesses wereseen at MRI nor was there any evidence ofcomplications on clinical examinationand flexible sigmoidoscopy. There wasone false negative examination in apatient who had a colovesical fistula. Inconclusion, MRI can accurately show thepelvic and perineal complications ofCrohn's disease and may render examina-tion under anaesthetic unnecessary.(Gut 1995; 36: 407-410)
Keywords: Crohn's disease, magnetic resonanceimaging.
Crohn's disease is a chronic granulomatousinflammation, which is prevalent at all agesbut with a high incidence in the youngadult population.' The incidence of perianal
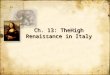
Figure 1: Transverse T2 weighted image (repetition time (TR) =4000 ms, effective echotime (TE) = 102 ms) with suppression of the fat signal, at the level of the external analsphincter. The high signal track (arrow) is a simple trans-sphinctericfistula, passingbetween the internal sphincter (open arrow) and the puborectalis (curved arrow).
inflammation and fistula in ano is particularlycommon in patients with Crohn's disease. Thenature and extent of these complications deter-mine the choice of medical or surgical treat-ment.2 We have performed a prospective studyto determine the value of magnetic resonanceimaging (MRI) in assessing the pelvic andperineal complications of Crohn's disease.
MethodsWe examined 25 patients (mean age 41.4years, 12 male). All patients had symptoms orsigns of active pelvic Crohn's disease; perinealpain, anal discharge, rectal bleeding orpneumaturia. All patients had a clinical exami-nation and flexible sigmoidoscopy carried outby a consultant or senior registrar in gastro-enterology, or examination under anaestheticperformed by a consultant or senior registrar incolorectal surgery. The clinical assessment wasperformed before MRI in seven patients andafter MRI in 18 patients.The MRI examinations were performed on a
high field machine operating at 1.5 Tesla(International General Electric MedicalSystems, Slough) within 14 days of clinicalassessment. All patients had a T1 weighted fastspin echo acquisition performed in the coronalplane (repetition time (TR) =700 ms, effectiveecho time (TE)=17 ms, echotrain=4).Subsequently, axial and sagittal or coronal T2weighted fast spin echo sequences wereacquired (TR=4000 ms, TE= 102 ms, echo-train= 16). The body transmit and receive coilwas used in all examinations. The acquisitionmatrix was either 512 by 256 or 512 by 512,and the field of view was 40-48 cm. The inplane resolution varied from 0.8 mmX0 8 mmto 0.9 mmX1-8 mm. In the early part of thestudy, Ti weighted images were also per-formed in the axial or sagittal plane. Most ofthe T2 weighted sequences were performedwith suppression of the fat signal using thefrequency specific spectral presaturationtechnique.Both the MRI examinations and the clinical
assessment were carried out without priorknowledge of the other worker's findings.The results of the MRI examinations and
the clinical assessments were then compared.
ResultsSixteen of 25 patients had perianal fistulas orpelvic abscesses diagnosed at examinationunder anaesthetic. There was accurate correla-tion of the MRI appearances with the findings
Departments ofRadiologyP J HaggettN R Moore
GastroenterologyJ D ShearmanS P L TravisD P Jewell
and SurgeryN J Mortensen
John Radcliffe Hospitaland University ofOxford, Oxford
Correspondence to:Dr P J Haggett, Departmentof Radiology, John RadcliffeHospital, Headington,Oxford OX3 9DU.Accepted for publication9 June 1994
407
on 31 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.36.3.407 on 1 M
arch 1995. Dow
nloaded from

Haggett, Moore, Shearman, Travis, _rewell, Mortensen
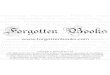
rigure 2: Transverse 1/ weighted image (RK= 4U00 ms, Iti=102 ms) with fatsuppression, showing a complex fistula on both sides of the natal cleft (arrows) withextensive inflammation affecting the right obturator internus muscle (curved arrow).
at examination under anaesthetic. A singlefistula was diagnosed in six patients (Fig 1).Multiple abscesses and fistulas were seen in 10patients (Fig 2). MRI showed additionalfistulas or abscesses in three patients andwithin this group, there were two patients inwhom MRI showed deep and unsuspectedpararectal or ischiorectal abscesses (Figs 3and 4).
Figuri,1e 3: (A) Coruala/ T1Jwzeiglitedl image (JR= 4000
ins, 1 012 nis) it/i fat
suppressiOni %/ioiig
bilateralhloid1 cLollectiions(OnultiloculatedL on the /lt)ii tilL' i.sLchi/o;ectil >ae(Clrrows (Bf) TransverseT2 zwieighzted (TR 4000ns , I J02 min) it/i faltSuppression. 7/os eninns
thehpi lug/i s1ig1nilfluid collectiOns (arrowns).Thic low signeld locuis on theright (curved arron) is
e ithe guLs or anLirLaLi ofcalc/ication). No deepabscesssfionation was
suspected on clin;i'icailexaminldrationi (o at
examinatiiou under
anaesthetic.
In eight of 25 patients, no pelvic abscess orfistula was diagnosed at MRI. Clinical assess-ment in all of these patients did not show anycomplication.
In one patient in whom a pelvic abscess wassuspected, the MRI examination was initiallythought to be normal. On review, however, asmall loculus of gas in the bladder with bladderdome thickening was identified on one axialsection, and an adjacent colonic loop was seen.At subsequent laparotomy, a colovesical fistulawas found.
DiscussionPerianal infection is thought to originate withinthe anal glands. The presence of lymphoidtissue around these glands may account for theincreased incidence of perianal involvement inCrohn's disease.3 The infection may extend asa fistula in the plane between the internal andexternal anal sphincters (intersphincteric), ormay penetrate the external sphincter(transphincteric). More complicated fistulasmay extend around the rectum as a horseshoeabscess, or perforate through the pelvic floor(suprasphincteric). In some patients, particu-larly those with Crohn's disease, the inflamma-tion may extend from the rectum to theperianal region and not affect the sphinctermechanism (extrasphincteric).2
Careful digital examination under anaes-thetic is regarded as the ideal standard for thediagnosis of fistula in ano. Even experiencedsurgeons, however, may fail to detect theinternal opening in up to 13% of cases.4In addition to bidigital palpation, probingof fistula tracks is commonly performed.Considerable care must be taken because in-judicious probing may transform a transphinc-teric fistula into an extrasphincteric fistula,with grave implications to the patient.2Accurate assessment of the anatomy is vitalbecause an incorrect diagnosis may lead toinappropriate surgery. Division of the internaland external sphincters will result in loss ofcontinence.The need for accurate imaging is evident.
Fistulography will delineate a fistula track ifthe external orifice can be cannulated, but itgives little information about immediateanatomical relations.5 Fistulography may alsofail to show the complete extent of complexfistulas and deep abscesses. Computed tomo-graphy is successful in showing most perianalfistulas and abscesses but requires the use oforal, rectal, and intravenous contrast media.Some fistulas escape detection, or may be diag-nosed as inflammatory streaking only, if air orbarium do not enter the track.6 The substantialradiation dose to the pelvis in this group ofyoung patients is undesirable.7
Anal endosonography has many advantageswhen used by experienced operators and maydetect simple fistulas with an accuracy equalto that of examination under anaesthetic.4Endosonography is not reliable, however, inthe detection of extrasphincteric and supra-sphincteric fistulas. The short focal length pro-hibits the detection of ischiorectal abscesses.4
408
on 31 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.36.3.407 on 1 M
arch 1995. Dow
nloaded from

Pelvic and perineal complications ofCrohn 's disease: assessment using magnetic resonance imaging
Endosonography can be painful and difficultiesoccur with previous sepsis or surgery becauseendosonography cannot distinguish the lowreflectivity track of a fistula from that of scartissue.MRI has many advantages in the assessment
of the pelvis. It offers excellent soft tissue dis-crimination, multiplanar image acquisition, awide field of view, and it does not use ionisingradiation. The coronal acquisition plane is par-ticularly valuable in the assessment of perianaldisease because the relation of a fistula in anoto the levator ani and puborectalis muscles(Fig 4) is crucial for surgical planning.
In this study, MRI correctly identified surgi-cally verified perianal fistulas in all patients.MRI correctly classified six of six simple fis-tulas and showed multiple fistulas in 10 of 10.Furthermore, MRI showed additional compli-cations in three patients, and in two patientsMRI showed deep and unsuspected abscesses(Figs 3 and 4). Rounded areas ofhigh signal onT2 images were diagnosed as abscesses. Linearhigh signal may represent fluid or inflamma-tion in fistula tracks. Enhancement of signal onT1 images after gadolinium diethylenetriaminepentacetic acid (Gd DTPA) injection mayserve to distinguish fluid from inflammation.We did not use Gd DTPA because the treat-ment of the patient would not have been in-fluenced in the presence of a dischargingfistula. Furthermore, Gd DTPA is expensiveand an additional TI sequence would prolongexamination time.
J:iguire 4: (A) A coronal
Ti weighted imnage(TR= 700 tins, TE-= 17ms)
show-ing a siupra.sphziucteniCjistula (arrow%'. The
extern^al anal sphincter(cucrTved ar1row)Z is nornnal.(B) A transverse T2weighted image (JR= 4000nis, Ti> 102 ins) withsuppression of'theflatsignall, s/wws a rounded
area of high signal (arrow)in the levator anii muscleindicating abscessform;1atio(1n.
MRI was also successful in excluding fistulain ano. In no case was a fistula shown eitherclinically or at examination under anaestheticwhen MRI was negative. MRI prospectivelyfailed to detect one vesicoenteric fistula,although this was visible in retrospect.The results of this study may be taken in
context with previous studies.8-10 Lunnisset al8 used spin echo Ti and short Tau inver-sion recovery images at 0.5 T in the transverseand coronal planes. The short Tau inversionrecovery sequence provides good suppressionof fat and inflammatory tissue and gives a highsignal because of long TI and T2 relaxationtimes. Although successful in detecting activeinflammation, the short Tau inversionrecovery sequence entails long acquisitiontimes and the images tend to be of poorerspatial resolution than equivalent spin echosequences. This may have contributed to thedifficulty in distinguishing the internalsphincter from the anal mucosa.8 Skalej et al 9also showed the value of MRI in the detectionof perianal complications. They showed simplefistulas in 13 of 16 and complex fistulas in 18of 18 patients who had Crohn's disease andsuspected perianal disease. The sensitivity ofMRI is equivalent to the results that we report,however, their group is not fully representativeand the outcome may be biased in that thespecificity ofMRI was not assessed.Our examinations were obtained using the
body coil and not a phased array multicoilsystem. Phased array multicoils would have theadvantage of an improved signal to noise ratio,but would not influence spatial resolution for afixed field ofview. An endorectal coil combinesthe advantages of an increased signal to noiseratio and a small field of view; we do not havean endorectal coil. Although endorectal coilsare used to stage prostatic carcinoma,'1 thereare no reported studies of perianal diseaseusing an endorectal coil. The smaller field ofview may be a disadvantage in the assessmentof pelvic sidewall extension, and the distensionof the 100 ml balloon would be very painful inthis group of patients.The high sensitivity and specificity achieved
in this study may be attributed to the use ofmultiplanar high resolution T2 images. This isonly possible in a clinically manageableappointment time with the use of fast spin echosequences. Fat suppression is a valuableadjunct because fat has a higher signal intensityon fast spin echo sequences than a comparableconventional spin echo sequence.'2 Small fociof high signal in fistula tracks are appreciatedmore readily when fat suppression is used. Fatsuppression by selective radiofrequency pre-saturation is easier to perform at 1. 5 T becausethe resonant frequency of fat is 220 Hz higherthan water. The efficiency of suppression maynot be uniform, however, and care must betaken to place the patient close to the centre ofthe magnet to maximise homogeneity of fatsuppression.We conclude that MRI is a valuable tech-
nique in the assessment of patients with activeperianal Crohn's disease. MRI offers a non-ionising painless alternative to examination
409
on 31 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.36.3.407 on 1 M
arch 1995. Dow
nloaded from

410 Haggett, Moore, Shearman, Travis, Jewell, Mortensen
under anaesthetic and provides valuable infor-mation for preoperative planning in cases ofcomplex fistulas and abscess formation.
1 The National Cooperative Crohn's Disease study.Gastroenterology 1979; 77: 829.
2 Parks AG, Gordon PH, Hardcastle JD. A classification offistula-in-ano. BrJ Surg 1976; 63: 1-12.
3 Parks AG, Morson BC. Proc Roy Soc Med 1962; 55: 751-4.4 Choen S, Burnett S, Bartram CI, Nicholls RJ. Comparison
between anal endosonography and digital examination inthe evaluation of anal fistulae. BrJ Surg 1991; 78: 445-7.
5 Kuijpers HC, Schulpen T. Fistulography for fistula-in-ano.Dis Colon Rectum 1985; 28: 103-4.
6 Yousem DM, Fishman EK, Jones B. Crohn's disease;perirectal and perianal findings at CT. Radiology 1988;167: 331-4.
7 Dosimetry Working Party of the Institute of PhysicalSciences in Medicine. National Protocol for Patient Dose
Measurements in Diagnostic Radiology. 1992: NationalRadiological Protection Board.
8 Lunniss PJ, Armstrong P, Barker PG, Reznek RH, PhillipsRKS. Magnetic resonance imaging of anal fistulae. Lancet1992; 340: 394-6.
9 Skalej M, Bongers H, Aicher H, Weinlich M, Starlinger M,Jenss H. Value of MR tomography in perianal Crohn'sdisease; a prospective study. Gastroenterology 1992; 102(suppl); A697.
10 Koelbel G, Schmiedl U, Majer MC, Weber P, Jenss H,Kueper K, et al. Diagnosis of fistulae and sinus tracts inpatients with Crohn's disease: value ofMR imaging. AJR1989; 152: 999-1003.
11 Mirowitz AS, Brown JJ, Heiken JP. Evaluation of theprostate and prostatic carcinoma with gadoliniumenhanced endorectal coil magnetic resonance imaging.Radiology 1993; 186: 153-7.
12 Hinks RS, Martin D. Bright fat, fast spin echo and CPMG.Proceedings of the 11th Annual Scientific Meeting of theSociety of Magnetic Resonance in Medicine. Berkeley, CA:Society of Magnetic Resonance in Medicine, 1992: 4503.
on 31 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.36.3.407 on 1 M
arch 1995. Dow
nloaded from