Embed Size (px)
Citation preview


Injuries in children Unintentional injuries are the leading cause of death in children 0‐19 years
ll MVC #1 cause overall‐MVC Occupants Pedestrians and pedestrian cyclistsp y
Wolters Kluwer‐Lippincott Williams and Wilkens

Leading causes of death by ageLeading causes of death by age group <1 yr‐ suffocation 1‐4 years‐ drowning 5‐19 years‐ vehicle passenger
Wolters Kluwer‐Lippincott Williams and Wilkens

Not all injuries lead to death #1 cause of non‐fatal injuries in children 0‐15 years
falls
Wolters Kluwer‐Lippincott Williams and Wilkens

Differences in Anatomy and Physiology of the Neurologic System of ChildrenSystem of Children First 3 to 4 weeks’ gestation
Infection trauma teratogens and malnutrition can cause physical Infection, trauma, teratogens, and malnutrition can cause physical defects and may affect normal CNS development.
BirthC i l b ll d l d b t t f d i d i k f Cranial bones well developed, but not fused: increased risk for fracture
Brain is highly vascular: increased risk for hemorrhage Child
Spinal cord is mobile: high risk for cervical spine injury
Wolters Kluwer‐Lippincott Williams and Wilkens

Anatomic differencesAnatomic differences Head is large in proportion to body
Increased risk of head injury d/t falls Increased risk of head injury d/t falls Fastest growing body part during infancy until age 5
Wolters Kluwer‐Lippincott Williams and Wilkens


Neurologic development Development is complete but immature at birth
Myelination is incompleted h l d l d h d d k Proceeds in a cephalo‐caudal direction‐ head and neck
control before trunk and extremities
Open sutures allow for brain growthp g
Wolters Kluwer‐Lippincott Williams and Wilkens


Neurologic AssessmentHistory/ Physical Exam
Past Medical History Prenatal exposures – teratogenic exposure, substance abuse,
maternal anemia, maternal illness, maternal malnutrition, lack of , , ,folic acid
Birth history – trauma, hypoxia, low Apgars, prolonged labor Significant past medical history (baby) – birth anomalies, Significant past medical history (baby) birth anomalies,
prematurity, ingestion of toxins, surgeries, infections Developmental milestones – delays? , progression of speech,
language and playg g p y Family history – seizure disorders?, mental retardation?,
hereditary disorders, neural tube defects

Neuro HPI Nausea/vomiting Vision changesHA/ h t h bi HA/photophobia
Neck stiffness Poor feeding Poor feeding Inconsolability Lethargygy Fever Ataxia Trauma history
Wolters Kluwer‐Lippincott Williams and Wilkens

Neuro exam Inspection ,observation, and palpation
Level of consciousnessb l l h l b l Extreme irritability or lethargy/consolability
Pediatric GCS
Head circumferenceHead circumference Important in detecting potential neurologic conditions
Acute changes/changes over timel ( f ll ll l h Fontanels (anterior fontanelle generally open until 18 months
of age) Should be soft and flat
Wolters Kluwer‐Lippincott Williams and Wilkens

Neuro exam Pupil reaction EOM’s Muscle tone
Symmetry, strengthP i (l i ) Posturing (late sign)
Signs of increased ICPE l l t i h t 6 6 i t t Early versus late signs‐ chart 16.1, page 506 in text
Wolters Kluwer‐Lippincott Williams and Wilkens


Wolters Kluwer‐Lippincott Williams and Wilkens

Signs of increased ICPSigns of increased ICPEarly Infancy Increased ICP Assessment Findings *** Change in LOC‐ Irritability, lethargy Bulging fontanels, progressive head enlargementg g , p g g Persistent vomiting, FTT Delay or loss of developmental milestones Sunset eyes Sunset eyes ***Late Signs‐ High, shrill cry Seizures Seizures Change in Vital Signs
Bradycardia, hypertension, respiratory depression‐“Cushing’s triad”
Wolters Kluwer‐Lippincott Williams and Wilkens

Increased ICPIncreased ICPOlder Child Increased ICP Assessment Findings
***Headache nausea/ vomiting Headache, nausea/ vomiting Irritability or change in personality Gait disturbances, vertigo Blurred Vision sunset eyes Blurred Vision, sunset eyes Worsening school performance
S Late Signs ** Significant decrease in LOC Change in Vital Signs‐ Cushings Triad
i d/ dil d il Fixed/ dilated pupils
Wolters Kluwer‐Lippincott Williams and Wilkens

Acute nursing management of aAcute nursing management of a child with increased ICP Frequent neuro assessment Frequent vital signs Elevate HOB 15‐30 degrees
Facilitates venous return and decreases ICPd l l bl Have emergency equipment readily available
Increased ICP can result in respiratory/cardiac failure
Wolters Kluwer‐Lippincott Williams and Wilkens

Types of Neurologic Disorders inTypes of Neurologic Disorders in Children Structural disorders
Hydrocephalus MyelomeningoceleMyelomeningocele
Seizure disorders Infectious disorders
Meningitis Trauma to the neurologic system
Concussions Chronic disorders
Cerebral palsyBl d fl di i di d Blood flow disruption disorders
Wolters Kluwer‐Lippincott Williams and Wilkens

Hydrocephalus( ) ( ) Derived from the Greek, hydor (water) & kephale (head).
Accumulation of fluid (CSF, blood) in the ventricles of ( , )the brain (impedance of flow, production or absorption).
As CSF increases, the ventricles dilate ‐‐‐> pressure , pincreases within the intracranial vault
INCREASED ICP
CSF‐ secreted by choroid plexus.
Adults/ Children ‐‐> 500cc/day, Infants ‐‐> 25ml/day/ 5 / y, 5 / y
Wolters Kluwer‐Lippincott Williams and Wilkens

Hydrocephalus Etiology
Congenital‐d l fl d Genetic predisposition or environmental influences during
fetal development
Acquiredq Trauma Intraventricular hemorrhage, infection, tumors, etc
Cl ifi i Classification Communicating‐ impaired absorption –too much CSF Non communicating anatomical obstruction Non‐communicating‐ anatomical obstruction
Wolters Kluwer‐Lippincott Williams and Wilkens

Hydrocephalus

Hydrocephalus‐treatment Aqueductal stenosis
Most common type of obstructive hydrocephalusobstructive hydrocephalus
Narrowing of the aqueduct of sylvius( b t rd d (passage between 3rd and 4th ventricles
Endoscopic third ventriculostomy (ETV) Hole made in bottom of 3rd
ventricle Avoids need for a shunt
Wolters Kluwer‐Lippincott Williams and Wilkens

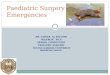
Ventriculoperitoneal shunt
Placement of a VP shunt. Reprinted from 'Principles of Neurosurgery,' 2nd edition, Edited by Setti S. Rengachary, Richard G. Ellenbogen, Copyright (2005)

Shunts Ventriculoperitoneal Ventriculoatrial Ventriculolumbar
Parts of a shunt CatheterP i h b Pumping chamber
One way valve Distal catheter Distal catheter
Wolters Kluwer‐Lippincott Williams and Wilkens

Hydrocephalus What should the nurse monitor for post‐op after
a VPS placement? Vital signs Vital signs S/S increasing ICP I and O Changes in neuro status Changes in neuro status, exam, LOC and GCS Observe shunt surgical sites‐head and abdomen Pain status Keep HOB 30 degreesp 3 g
Wolters Kluwer‐Lippincott Williams and Wilkens

The Neural Tube
l b D f Neural Tube Defect: Example: Myelomeningocele
“Spina Bifida” Spina Bifida

Myelomeningocele Neural tube fails to close at the end of the 4th week of gestationS i l d f d l l f d f Spinal cord often ends at level of defect Absent motor and sensory function beyond that point
L t li ti Long term complications Paralysis Orthopedic deformities Orthopedic deformities Bowel and bladder incontinence
Wolters Kluwer‐Lippincott Williams and Wilkens


Seizures Abnormal electrical discharge of nerve cells in
brain ‐‐‐> loss of consciousness, involuntary movement, behavior &/or sensory alterations.ove e t, be av o &/o se so y a te at o s.
Epilepsy‐ chronic seizure disorder due to an d l i b i b liunderlying brain abnormality
Wolters Kluwer‐Lippincott Williams and Wilkens

Seizures Occur in approximately 10% of children Fever, infection, trauma, hypoxia, toxins, cardiac
arrhythmia’sarrhythmias Familial tendency Unknown cause
Wolters Kluwer‐Lippincott Williams and Wilkens

Seizures Two major categories
Partial‐ large proportion of childhood seizuresl Simple
Complex
GeneralizedGeneralized
Wolters Kluwer‐Lippincott Williams and Wilkens

Types of Seizures 1. Simple partial seizures‐ Focal ‐ Localized body part ‐ No LOC; No post‐seizure confusion; ; p ; no aura ‐ ~30 secs.
2. Complex partial Seizures‐ Psychomotor ‐ Impaired consciousness‐‐‐>automatisms (may
l d )progress to a generalized seizure) ‐ aura, anxiety/ fear afterwards ‐ ~30secs. ‐ 5 mins.30secs. 5 mins.
Wolters Kluwer‐Lippincott Williams and Wilkens

Partial seizures Simple partial seizures
Sx’s depend on which area of brain affected Tonic/clonic movements of face neck extremities‐localizedTonic/clonic movements of face, neck, extremities localized Child remains conscious‐ no postictal state Last a short time‐ ~30 sec.C l i l Complex partial May have preceding aura Impaired consciousnessp
Repetitive movements (automatisms) picking/pulling Infants‐ lip smackingg
Hard to control
Wolters Kluwer‐Lippincott Williams and Wilkens

Generalized seizures Tonic clonic‐ “grand mal”
Associated with an aura Post‐ictal phasep Loss of sphincter and bladder control is common Entire body contractions http://youtu.be/WsBKg2PtQWcp y g Q
Absence Sudden cessation of motor activity or speech “staring spells”staring spells Very brief‐ 3‐5 seconds http://youtu.be/bC9672CmkZM http://youtu be/9HiKwTm755o http://youtu.be/9HiKwTm755o
Wolters Kluwer‐Lippincott Williams and Wilkens

Febrile seizures Most common type of seizure in childhood Usually in children less than 5 Familial predisposition Associated with a fever‐usually viral illness
Rapid rise in temperature Usually a simple seizure
N CNS h ( f i i i if !) No CNS changes (worry for meningitis if so!) No intervention needed
Look for source of fever Look for source of fever
Wolters Kluwer‐Lippincott Williams and Wilkens

Seizures: Nursing Implications Safety Maintain safe environment during event. Maintain patent airway and adequate oxygenation. Do NOT p y q yg
place anything in child's mouth. Monitor the post‐ictal phase. Administer medications appropriately. Monitor therapeutic
bl d l lblood levels.
Document Date, time and nature of seizure. Note the length of seizure, loss of consciousness, apnea, meds
needed to stop seizure. Precipitating events.
Wolters Kluwer‐Lippincott Williams and Wilkens

Treatment Anticonvulsants Surgery‐ for intractable seizures Ketogenic diet Vagal nerve stimulator
Wolters Kluwer‐Lippincott Williams and Wilkens

Grid Placement Surgery:Identify Locality of Seizure ActivityActivity

Seizures Terms to be familiar with...
Aura‐ sensation that gives warning of an impending sz.
Tonic‐ unconsciousness continuous muscle contraction‐ stiffness Tonic unconsciousness, continuous muscle contraction‐ stiffness
Clonic‐ alternating muscular contraction/ relaxation
Status epilepticus‐ prolonged repetitive sz without regain of p p p g p gconsciousness between attacks or one continuous sz
Post‐ictal Phase‐ Decreased LOC after a seizure; may last hours
Febrile Seizures lf li iti t t t d d Febrile Seizures‐ self‐ limiting; no emergency treatment needed; anti‐pyretics; anticonvulsant may be used for the length of the underlying illness
Intractable Seizures‐ occur despite optimal management
Ketogenic Diet‐ hi fat, low‐carb diet → ketosis → reduces epilepsy
Wolters Kluwer‐Lippincott Williams and Wilkens

Bacterial Meningitis Infection of the meninges, the lining the surrounds the brain and spinal cord
C l d b i d k d f k d Can lead to brain damage, stroke, deafness, stroke and death
Decreased dramatically due to HIB vaccine in USDecreased dramatically due to HIB vaccine in US
Deterioration can be rapidp Need prompt IV antibiotics Lumbar puncture/blood cultures/CBC
Wolters Kluwer‐Lippincott Williams and Wilkens

Signs In older children
Neck stiffness, h d h fheadache, fever
Babies/young children Opisthotonic position Opisthotonic position Bulging fontanelle Inconsolable Rash
Wolters Kluwer‐Lippincott Williams and Wilkens

Cerebral PalsyAb l d l d h f Abnormal development or damage to the motor areas of the brain, resulting in a lesion Causes a disruption in the brain’s ability to control
movementmovement Non‐progressive May be associated with sensory, intellectual, emotional or
seizure disorders. Etiology
Anoxic injury Premature birth or intrapartal asphyxia Congenital or perinatal infections Congenital brain anomalies Many others‐ p 818 in textbook
M h i di i ( di bili ) i Most common chronic condition (permanent disability) in childhood.
Wolters Kluwer‐Lippincott Williams and Wilkens

Cerebral Palsyd Assessment Findings
*** Delayed gross motor development
Usually identified at well baby check‐up‐‐ Not usually identified at birth
Abnormal posturing‐‐most evident with spastic CP
Persistence of primitive infantile reflexes and/or reflex Persistence of primitive infantile reflexes and/or reflex hypersensitivity
M t h t l t d ti May or may not have mental retardation
Wolters Kluwer‐Lippincott Williams and Wilkens

Cerebral Palsy Classification
Spastic‐ (75%) increased tone (hypertonicity), rigid, poor control of posture, balance and coordination, contracturesp , ,
Athetoid/Dyskinetic‐ (10‐15%) abnormal involuntary movements‐ disappear during sleep, increase with stress
Ataxic‐ (5‐10%) wide‐based gait rapid repetitive movements Ataxic‐ (5‐10%) wide‐based gait, rapid repetitive movements performed poorly
Mixed Types

Cerebral Palsyh l h bl Accompanying health problems
Contractures Pain Feeding problems/ swallowing/ reflux/ nutrition Respiratory problems Dental disease
H i i i Hearing impairment Delayed Speech Mental Retardation S i Seizures Visual impairment (i.e. Strabismus) Functional abilities to perform ADL's Immobility Immobility
Wolters Kluwer‐Lippincott Williams and Wilkens

Cerebral Palsy Management
** Early recognition is important so that optimum development can be promoted‐mobility it criticalp p y
Physical/ Occupational Therapy Mobility Devices, AFO's (ankle foot orthotics) Promote self‐care activities to maximize ability Promote self‐care activities to maximize ability Pharmacologic‐ Anti‐spasmodics (Baclofen, Botulinum
toxin, diazepam) Surgery Tendon release Achilles tendon lengthening Surgery‐ Tendon release, Achilles tendon lengthening,
Hamstring release
Wolters Kluwer‐Lippincott Williams and Wilkens

Cerebral Palsy: Tendon Releases
Achilles Tendon Release: Achilles Tendon Release: After this surgery heals, the child may be able to stand flat‐footed.
Femoral Osteotomy

Cerebral Palsy: Splints, AFO's

Head trauma‐Concussions Most common head injury Lots of attention in recent years
Why? Greater understanding of its role as a form of traumatic brain injury injury
Often from a blow or jolt to the head Sports injuriesp j
Kids are more susceptible to injuries than adults
Motor vehicle injuriesll Falls
Wolters Kluwer‐Lippincott Williams and Wilkens

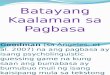
Concussion signsConcussion signs
Thinking/Remembering
Physical Emotional/Mood
Sleep
Difficulty thinking Headache Irritability Sleeping more than Difficulty thinking clearly
Headache
Fuzzy or blurry vision
Irritability Sleeping more than usual
Feeling slowed down
Nausea or vomiting(early on)
Sadness Sleep less than usualdown (early on)
Dizziness
usual
Difficulty concentrating
Sensitivity to noise or light
More emotional Trouble falling asleepconcentrating or light
Balance problems
asleep
Difficulty remembering new
Feeling tired, having no energy
Nervousness or anxietyg
informationg gy y
Wolters Kluwer‐Lippincott Williams and Wilkens

Concussion symptoms May or may not have loss of consciousness CT scan and MRI are normal, as it does not result in
l d h b istructural damage to the brain
Wolters Kluwer‐Lippincott Williams and Wilkens

Return to play A child with a concussion MUST NOT return to play the same day
Sh ld b i hil d i h i Should be asymptomatic while at rest and with exertion before return to play is considered
Closer monitoring during 1st 24‐48 hours after injuryCloser monitoring during 1 24 48 hours after injury Potential for more severe injury needing evaluation
Wolters Kluwer‐Lippincott Williams and Wilkens

Red Flags! Need to be evaluated Looks very drowsy or cannot be awakened. Unequal pupilsS i Seizures.
Cannot recognize people or places. Are getting more and more confused restless or agitated Are getting more and more confused, restless, or agitated. Have unusual behavior. Loss of consciousness Loss of consciousness Infants/young children
Will not stop crying and cannot be consoled. Will not nurse or eat.
www.cdc.ogv

Prevention of head injuries inPrevention of head injuries in children Proper use of car seats Helmets for sport activities Safety gates and window guards for young children Safe, absorbent playground surfaces
www.cdc.ogv

Thank you
Wolters Kluwer‐Lippincott Williams and Wilkens