Embed Size (px)
Citation preview

“Pediatric radiation oncology”
R. MiralbellHôpitaux Universitaires, Genève

Trends in 5-Year Survival for Pediatric Cancer Patients (<19 yr-old males) in the US (1975-2000)
Tumor site 1975-79 1995-2000
CNS 57% 72%
Soft tiss. sarcoma 62% 73%
Hodgkin 86% 96%
All sites 58% 77%(Annual report to the Nation, Cancer, July 2004)


Author Period #pts Gender Age T-stage M-stage
Hershatter et al 1940-83 127 - - >T2 NE
Tait et al 1975-79 286 female - <T3 NE
Evans et al 1975-81 233 - >4 years - M0
Jenkin et al 1977-87 72 female - <T3 M0-1
Wara et al 1970-95 109 female >3 years - M0
Miralbell et al 1972-91 86 female - - M0
Clinical features favorably influencing survival in pediatric medulloblastoma: univariate analysis

Author Period #pts Gender Age T-stage M-stage
Hershatter et al 1940-83 127 - - >T2 NE
Evans et al 1975-81 233 - >4 years - M0
Jenkin et al 1977-87 72 - - - -
Wara et al 1970-95 109 female - - M0
Miralbell et al 1972-91 86 female - - M0
Clinical features favorably influencing survival in pediatric medulloblastoma: multivariate analysis

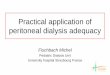
Virtual simulation for cranio-spinal irradiation of medulloblastoma.
Clara Jargy, Philippe Nouet, Raymond Miralbell.Radiation Oncology, Geneva University Hospital

Patient set-up
Lateral markMark on the skin for the spine field

Set-up of the left lateral brain field
with the different structures.

Set-up of the spinal field
Mark on the skin
shifts

Junction (brain-spine) in a sagittal slice

Effect of the table rotation on the field ’s matching
with without

Moving junctions between the brain fields and the spinal field.
We use asymetric fields (one isocenter for the same region).

Moving junction between the two spinal fields.
Fields match on the anterior edge of the spinal cord

Boost on the posterior fossa

Final dosimetry in a sagittal slice passing through the spinal cord.
-Dose at the junction.
-Dose at the spinal cord (depth and SSD vary).

Radiotherapy in pediatric medulloblastoma: quality assessment of
POG Trial 9031
R. Miralbell
QARC & Swiss POGGeneva, CH

Purpose
To evaluate the potential influence of the quality of RT on event-free (EFS) & overall survival (OS) in a group of high-riskpediatric medulloblastoma patients treatedin POG Trial 9031

• Randomize between:- Arm 1: CDDP+VP16 - CSI - vcr+cycloph.- Arm 2: CSI - CDDP+VP16 - vcr+cycloph.
• 224 high-risk stage patients randomized :- Post-op residual tumor: >1.5 cm3
- T3b, T4- M+ (1-3)
POG Trial 9031

Patient material & RT guidelines
• Patients: 197 evaluable
• CSI (dose): M0-1 M2-3 dose/fx
WBI & spine 35.2 Gy 40.0 Gy 1.6 GyPF (boost) 18.0 Gy 14.4 Gy 1.8 GyMetastases 0.0 Gy 4.8 Gy 1.6 Gy

CSI treatment volume boundaries
• WBI: inf border 0.5 cm below base of skull
• Spine: inf border 2 cm below the subdural space
• PF: tentorium+1 cm; C1-C2 interspace; post clinoids; post convexity
• Tumor: 2 cm around the primary tumor

Method of RT quality assessment
• WBI: distance between the inf field limit & both the cribiform plate & floor of the middle cranial fossa
• Spine: distance between the end of the inf field limit & the end of the dural sac (MRI).
• PF: distance between the boost field limits & the tentorium, C1-C2, post clinoids, post convexity
• Tumor: distance between the boost field limits & the tumor borders as seen in the pre-op brain MRI/CT

Treatment deviation guidelines
• WBI: 0-4 mm, minor; <0 mm, major
• Spine: Inf field abutting the sac, minor Inf field transsecting the sac,
major
• PF: < field boundaries, major
• Tumor: 10-18 mm, minor; <10 mm, major

RT deviations: total dose
• Maximum accepted variation: +/- 5%
• Major deviation: 10% or more below dose prescription
• Delays >51 & >58 days were conpensated with 1 or 2 additional fractions to the PF

Endpoints & statistics
• Assessment of 1st site of failure
• 5-year EFS & OS according to treatment correctness
• Kaplan-Meier & log-rank tests

Results: overall outcome
• EFS (5-y): 69.1% (4.1 SE)
• OS (5-y): 74.4% (3.8 SE)
• Relapsed: 35 patients
• Progressed: 14 patients
• Dead: 57 patients

Results: treatment deviations
• Fully evaluable: 160 patients
# deviations # patients0 691 502 313 094 01

Results: major deviations by site
Site #deviat/total patients
WBI: 54/208 (26%)
Spine: 12/174 (7%)
PF: 82/210 (39%)
Tumor: 33/189 (17%)

Results: EFS & OS by site and deviation status
Target Treatment Number of 5-year EFS p- 5-year OS p-volume deviation patients (SE) value (SE) value
Brain no 154 70.7(4.8) 77.7(4.3)yes 54 67.4(8.4) 0.823 69.5(8.2) 0.454
Spine no 162 70.0(4.8) 75.7(4.4)yes 12 74.1(16.9) 0.684 72.2(17.0) 0.997
Posterior fossa no 128 69.5(5.4) 75.6(4.9)yes 82 69.8(6.5) 0.965 74.8(6.1) 0.497
Primary tumor no 156 68.8(5.0) 74.1(4.6)yes 33 69.1(10.3) 0.854 78.1(9.1) 0.839

Results: outcome & cumulative effect of treatment deviations
5-yearDeviations EFS OS
0-1 72.1% 76.3%
2-4 59.2% (p=0.06) 70.6% (p=0.04)

Summary
• Major treatment deviations were observed in 57% of fully evaluable patients.
• Underdosage or treatment volume misses did not correlate with a worse EFS or OS.
• A «trend» for a better EFS and OS was observed among patients with lesser number of major deviations (i.e., 0-1).
• An involved field to boost the tumor bed may be as effective as, and less toxic than, boosting the whole PF.

RT in children: a unique treatment paradigm

Why?
1. Significant increase in survival in pediatric oncology in the last 25 years
2. Conventional RT frequently associated with severe side effects:
Growth & musculoskeletal
Endocrine & fertility
Neuropsychologic
Secondary cancers

Late sequelae in 306 children treated for orbital rhabdomyosarcomas (1979-92)Type of sequelae Europe USA
Cataract 51% 82%
Reduced vision 54% 70%
Dry eye 28% 23%
Orbital hypoplasia 29% 59%
Maxillary hypoplasia 10% 11%
(Anderson et al, COG news; 2001
)

Bone growth and radiation damage
• Radiation kills dividing chondroblasts
• Arrested chondrogenesis in the epiphysis
• Stop endochondral bone formation: >20 Gy

Changes in skeletal growth: the height
• A consequence of treating the spinal axis:
reduced sitting heights
• Age dependant: <12 years
• Dose dependent: >20 Gy

Endocrine dysfunction and irradiation dose
Dose (Gy) Endocrinopathies
3-10 Gy Spermatogenic failure in male
10-15 Gy Neurosecretory disturbance, adult GH deficiency
15-25 Gy Children GH deficiency, early puberty, ovarian failure in female, Leydig-cell failure
25-30 Gy Primary hypothyroidism
30-55 Gy Evolving pituitary gland dysfunction

Preirradiation endocrinopathies in pediatric brain tumors
Pre-RT endocrinologic dysfunction in 45/68 (66%) patients assessed
Dysfunction %
GH 38
TSH 43
ACTH 22
FSH/LH 13
Merchant et al, IJROBP 54:45-50, 2002

Craniospinal RT for medulloblatoma/PNET

Pituitary gland: 36 Gy

Thyroid: 25-30 Gy
Ovaries: 2-12 Gy

Ways to reduce the risk of radiation induced endocrine dysfunction
1. Total dose and/or field size reduction
2. Total/partial shielding of the gland(s) at risk
3. More than 1 small-fraction a day (hyperfractionation)
4. Free radical scavengers (radioprotectors)
5. Better dose distribution (computer-based optimization of 3-D treatment planning + new highly performant treatment delivery techniques)

Total dose and/or field reduction
1. «Mantle» RT for Hodgkin’s disease: Dose lowered from 44 Gy to 20 Gy and field size reduced. Still excellent survival. Sparing primary hypothyroidism
2. Prophilactic cranial irradiation in pediatric lymphoblastic leukemia or medulloblastoma: Dose lowered to 18 Gy. Sparing GH dysfunction

44 Gy
Hodgkin’s Lymphoma in 1950’s-1980’s: «mantle» field irradiation

Hodgkin’s Lymphoma in the 1990’s-2000’s: involved field irradiation
20 Gy

Total/partial shielding of the gland(s) at risk
1. Head and neck tumors: Usually high doses to the neck (50-70 Gy) Sparing primary hypothyroidism Sparing pituitary dysfunction
2. Pelvic tumors in boys-men: Shielding of the testicles Dose <3 Gy (sparing fertility)Dose <20 Gy (sparing Leydig-cell function)

Dose-volume relations for thyroid dysfunction in head and neck tumors
• The whole thyroid in the treatment field Risk of thyroid dysfunction: 29%
• Partial shielding of the thyroid Risk of thyroid dysfunction: 5%
Yoden et al, ASTRO proceedings 337, 2001

RT dose-volume effects on GH secretion
Dose to the hypothalamus (HT) vs peak GH value post-RT measured as a function of time and volume
Predictive model for GH peak response after RT:
GH(t) = Exp[ln(bGH) – (0.00058V0-20Gy + 0.00106 V20-40Gy + 0,00156 V40-60Gy) x t]
- bGH : baseline peak GH level (before RT)
- V 0-20Gy: % volume of HT receiving 0-20 Gy
- V 20-40Gy: % volume of HT receiving 20-40 Gy
- V 40-60Gy: % volume of HT receiving 40-60Gy
- t : time after irradiation (in months)
Merchant et al,IJROBP; 52:1264-1270, 2002

Hyperfractionation: 1 Gy/fraction bid
Better tolerance of the thyroid to small fractions (improved repair capacity of radiation induced sublethal lesions).
Reduced risk for primary hypothyroidism
Two studies with craniospinal RT for medulloblastoma/PNET
Author Standard RT Hyperfract RT
Chin et al, 1997 76% 14%
Ricardi et al, 2001 80% 33%

Radioprotectors: amifostine (ethyol)
Organic thiophosphate, dephosphorilated in its active metabolite WR-1065. Acts as free-radical scavenger inside the cell.
Study proposal at Washington Unversity (St Louis, MO) to test the impact of amifostine on subsequent hypothyroidism in irradiated patients with head and neck cancers.
Zoberi et al, Sem Rad Oncol 12:14-17, 2002

3-D conformal RT
• Shapes the prescription dose to the tumor avoiding normal tissues (critical organs).
• The system relies on 3-dimensional imaging to define and target the tumor.

…is further optimization possible?
New treatment technologies such as intensity modulated X-ray beams and proton beams can provide an even superior dose distribution compared to conventional 3-D conformal RT

Intensity Modulated X-ray Beams

Intensity Modulated Radiation Therapy
Beam-letBeam-let
3D Dose DistributionFluence or Intensity Map
IMRT is a highly conformal RT technique whereby many beamlets of varying
radiation intensity within one treatment field can be delivered

Proton Beams


Photon:
No mass, uncharged
Proton:
Large mass, charged « + »

Proton Beams

Four truisms…
1. There is no advantage to any patient for any irradiation of any normal tissue.
2. Radiation complications never ocur in unirradiated tissues
3. That a smaller treatment volume is superior is not a medical research question
4. One may investigate the magnitude of the gain or the cost of achieving that gain
(Suit, IJROBP 53; 2002)

Brainstem (pilocytic) glioma in a 8 y-old girl: 50 Gy (100%).
Pituitary gland
Optic chiasm
Brainstem
Target volume


3-D conformalradiotherapy
Brainstem glioma
Dose to the pituitary gland: 25 Gy (high-risk of GH deficiency)

Brainstem glioma
IMRT
Dose to the pituitary gland: 15 Gy (low-risk of GH deficiency)

Cancer of the nasopharynx in a 16 y-old boy: 70 Gy (100%)

IMRT3-D conformal RT

IMRT3-D conformal RT
Tumor

3-D conformal RT IMRT
Pituitary gland


Standard XRT IMRT (X-rays) Protons
Medulloblastoma in a 3-year old boy. Spinal radiotherapy: 36 GyE (100%)
Thyroid Ovaries

Summary & conclusions
• Dose escalation (against the tumor) as much as dose reduction (to normal tissues) are needed in modern radiation oncology
• Pre-RT endocrinopathies are not uncommon
• Progress in 3-D treatment technology may help to reach the goals of higher local cure with less endocrinologic side effects
• RT induced malignancies may significantly be reduced using proton beams (especially in pediatric oncology)

Quality of life in CNS tumor survivors:XRT vs no-XRT
Measure % Survivors odds ratio
Never employedXRT 21 16.0no-XRT 8 4.5
Emotional problems XRT 16 3.0no-XRT 8 1.6
Fair or poor healthXRT 30 13.1no-XRT 10 1.0
(Mostow et al, JCO; 1991)

Risk of G-3/G-4 ototoxicity versus dose after RT to the posterior fossa in children
RT technique Dose to the cochlea Risk (%)
3-D CRT 54.2 Gy (mean) 64%
IMRT 36.7 Gy (mean) 13%
( Huang et al, IJROBP, 52;2002)

Brainstem glioma
3-D conformalradiotherapy
(CRT)

Brainstem glioma
3-D conformal with dynamic
mMLC & IMRT

Comparative planning
3-D mMLC (CRT) 3-D mMLC (dynamic IMRT)

Medulloblastoma, post. fossa boost
3-D conformal radiotherapy
(CRT)

Medulloblastoma, post. fossa boost
3-D conformal with dynamic mMLC &
IMRT

Axial view:cochlear level
3-D CRTIMRT

Comparative planning
3-D mMLC (CRT) 3-D mMLC (dynamic IMRT)
PTVPTV
Rt cochleaRt cochlea
Lt cochleaLt cochlea
O. chiasmO. chiasm

Nonperoperative strokes in children with CNS tumors
• Incidence: 13/807 patients (1.6%)
• Ocurrence: 2.3 years from diagnosis
• Increased risk:
- treatment with RT
- optic pathway gliomas
(Bowers et al, Cancer 94;2002)

Oligo-astrocytoma G-II of the mesencephalus in a 12-year old girl

PTV
Brainstem
O. chiasm
Rt & Lt Cochleae
O. nerves

Protons
Pylocitic astrocytoma of the right optic pathway in a 8 year old girl (type-I NF):

Secondary cancers
• Observed/expected ratios (95% CI):
- Hodgkin disease: 9.7 (8.0-11.6)
- Soft-tissue sarcoma: 7.0 (4.9-9.7)
- Neuroblastoma: 6.6 (3.3-11.8)
- CNS tumors: 4.4 (1.8-5.4)
• Increased risk: female & young age.(JNCI, 93;2001)


Purpose
To assess the potential influence of improved dose distribution with proton beams compared to conventional or IM X-ray beams on the incidence of treatment-induced 2nd cancers in pediatric oncology.

Material
• A 7-y old boy with a rhabdomyosarcoma (RMS)
of the left paranasal sinus: 50.4 Gy (28 x 1.8 Gy,
qd) to the tumor bed.
(IJROBP, 47;2000)
• A 3-y old boy with a medulloblastoma
(MDB): 36 Gy (20 x 1.8 Gy, qd) to the spine.
(IJROBP, 38;1997)

Conformal XRT IMXT
Protons IMPT

Standard XRT IMRT (X-rays) Protons

Estimation of 2nd cancer incidence
Based on ICRP #60 guidelines
M = St Mt Ht/Lt
M; probability in % of 2nd cancer incidence (Sv-1) (total)
Mt; probability in % of fatal 2nd cancer (Sv-1) (organ-specific)
Ht; average dose (Sv) in the outlined organs
Lt; organ-specific cancer lethality

ICRP #60: organ-specific probability of fatal 2nd cancer (%) per Sv-1 & lethality
Organ Mt Lt
Oesophagus 0.55 0.95
Stomach 2.18 0.90
Colon 1.65 0.55
Breast 0.39 0.50
Lung 1.60 0.95
Bone 0.03 0.70
Thyroid 0.07 0.10

RMS: Estimated absolute yearly rate (%) of 2nd cancer
X-rays IMXT Protons IMPT
Yearly rate 0.06 0.05 0.04 0.02
RR compared
to X-rays 1 0.8 0.7 0.4

MDB: Estimated absolute yearly rate (%) of 2nd cancer
Tumor site X-rays IMXT ProtonsOesoph. & stomach 0.15 0.11 0.00Colon 0.15 0.07 0.00Breast 0.00 0.00 0.00Lung 0.07 0.07 0.01Thyroid 0.18 0.06 0.00Bone & soft tissue 0.03 0.02 0.01Leukemia 0.07 0.05 0.03All 0.75 0.43 0.05
RR (compared to X-rays) 1 0.6 0.07

Conclusions
• Proton beams may reduce the expected
incidence of radiation-induced 2nd cancers by a
factor of >2 (RMS) or >8 (MDB)
• With a lower risk of 2nd cancers the cost per life
saved may be significantly reduced