Embed Size (px)
DESCRIPTION
Pediatric NursingNursing Care of a Newborn I. Care of the Newborn II. Assessment of the NB III. Newborn Screening Test IV. Theories of Growth & developmentNewborn or neonate ± a baby in the neonatal period (the first 28 days of life)Nursing Diagnoses Ineffective airway clearance related to mucus in airway Ineffective thermoregulation related to heat loss from exposure in birthing room Imbalanced nutrition, less than body requirements, related to poor sucking reflex Readiness for enhanced
Citation preview

Pediatric Nursing

Nursing Care of a Newborn
I. Care of the Newborn
II. Assessment of the NB
III. Newborn Screening Test
IV. Theories of Growth & development

PEDIATRIC NURSING MLNGC,MD, RN3
Newborn or neonate – a baby in the neonatal period (the
first 28 days of life)Nursing Diagnoses
Ineffective airway clearance related to mucus in airwayIneffective thermoregulation related to heat loss from exposure in birthing roomImbalanced nutrition, less than body requirements, related to poor sucking reflexReadiness for enhanced family coping related to birth of planned infantHealth-seeking behaviors related to newborn needs

PEDIATRIC NURSING MLNGC,MD, RN4
The Average Newborn

PEDIATRIC NURSING MLNGC,MD, RN5
Profile of a Newborn
X “All newborns look alike.” – Every child is unique. -

PEDIATRIC NURSING MLNGC,MD, RN6
NEWBORN PRIORITIES IN THE FIRST DAYS OF LIFE
1. Initiation & maintenance of respirations2. Establishment of extrauterine circulation
3. Control of body temperature4. Adequate nourishment5. Waste elimination6. Prevention of infection
7. Infant-parent relationship
8. Developmental care

PEDIATRIC NURSING MLNGC,MD, RN7
Immediate Care of the NewbornI. Care of the Newborn at the D.R.
(EXISTING/ OLD PROTOCOL)

PEDIATRIC NURSING MLNGC,MD, RN8

PEDIATRIC NURSING MLNGC,MD, RN9
Establish and Maintain Respiration.
1. Suctioning - Turn head to one side - Suction gently and quickly - Suction the MOUTH first before the nose - Test patency of the airway - Proper position
a. Ensure an open airway.b. Do not hyperextend head - place neonate supine - head slightly extended

PEDIATRIC NURSING MLNGC,MD, RN10
• Suction gently and quickly (5 to 10 seconds). • Prolonged and deep suctioning of the
nasopharynx during the first 5 to 10 minutes of life will stimulate the VAGUS NERVE (located in the esophagus) and cause bradycardia.

PEDIATRIC NURSING MLNGC,MD, RN11
POSITIONING OF THE NEWBORN• The position when suctioning should be one that
promotes drainage of secretions – HEAD LOWER THAN THE REST OF THE BODY BUT C.I. if there are signs of increased ICP:head should be higher than the rest of the body
• Vomiting• Bulging, tense fontanels• Dilated scalp veins• Abnormally large head• Increased BP• Decreased PR and RR• Widening pulse pressure• Shrill, high-pitched cry- late sign

NURSING ALERT1. Always humidify to prevent drying of
mucosa
2. Over dosage of 02 can lead to scarring of retina leading to blindness (RETROLENTAL FIBROFLASIA or RETINOPATHY OF PREMATURITY)
PEDIATRIC NURSING MLNGC,MD, RN13
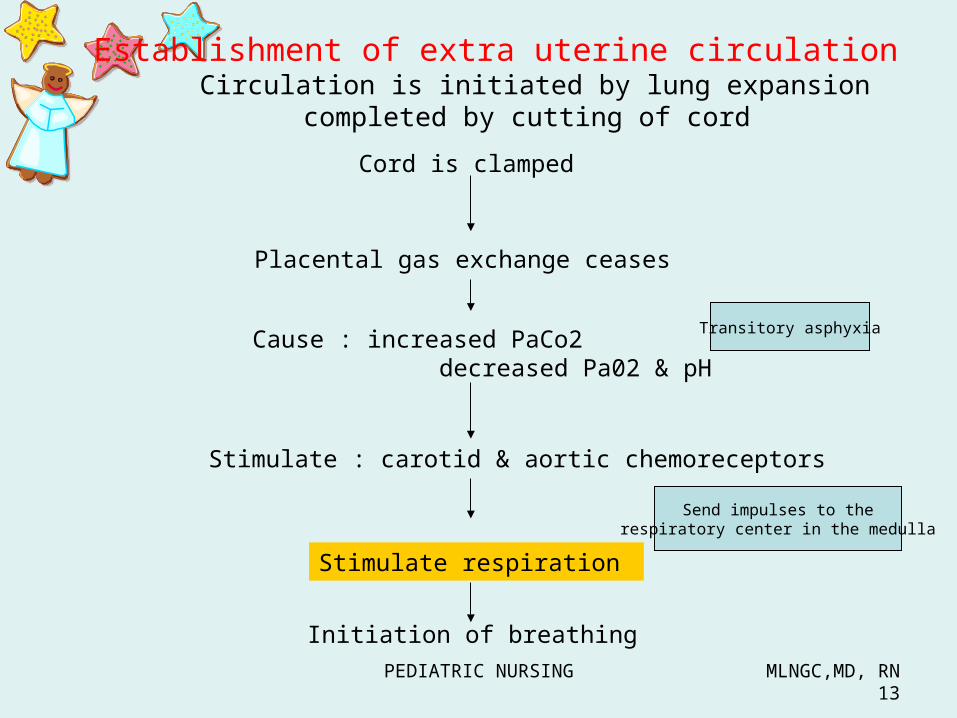
Circulation is initiated by lung expansion completed by cutting of cord
Initiation of breathing
Cord is clamped
Placental gas exchange ceases
Cause : increased PaCo2 decreased Pa02 & pH
Transitory asphyxia
Stimulate : carotid & aortic chemoreceptorsSend impulses to the
respiratory center in the medulla
Stimulate respiration
Establishment of extra uterine circulation

PEDIATRIC NURSING MLNGC,MD, RN14
Establishment of extra uterine circulation
CIRCULATION- several circulatory changes are necessary for successful changes from FETAL circulation to NEONATAL circulation.
A. Pulmonary Blood vessel – dilation, begins at first breath
results : lower pulmonary resistance this allows the blood to freely circulate through the lungs to be oxygenated.

PEDIATRIC NURSING MLNGC,MD, RN15
Establishment of extra uterine circulation
B. Ductus Arteriosus
- reversal blood flow increased pressure in aorta and increase O2 in the blood more blood flowing through the pulmonary arteries for oxygenation.
- closure complete w/in 24H - permanent : 3-4 weeks

PEDIATRIC NURSING MLNGC,MD, RN16
Establishment of extra uterine circulation
C. Foramen Ovale
- closes within minutes after birth because of the higher pressure in the LA than in the RA increase blood flow in the lungs decreases pressure in the RA the return of blood from the lungs increases the pressure in the LA
– Closure : permanent approximately 3 months – Failure to close becomes ASD

PEDIATRIC NURSING MLNGC,MD, RN17
Establishment of extra uterine circulation
D. Ductus Venosus
- cord clamped blood ceases flowing from umbilical vein to ductus venosus and into IVC blood now flows through the LIVER and is filtered as in adult circulation
Obliterates : becomes ligamentum venosum at 2 months

CONTROL OF BODY TEMPERATURE
Goal : to maintain not < 97.7 F (36.5 C)NB prone to cold stress (hypothermia)
NB not capable of shiveringNB born wet

CONTROL OF BODY TEMPERATURE
Effects of Hypothermia Hypoglycemia Metabolic acidosis

PEDIATRIC NURSING MLNGC,MD, RN20
Maintain Appropriate Body Temperature
*Blot dry/ Rub dry the infant.
1. Wrap the newborn immediately2. Wrap him warmly3. Put him under a droplight/ radiant
warmer4. Kangaroo care
PEDIATRIC NURSING MLNGC,MD, RN21
Warmth
• At birth, the newborn must begin thermoregulation (maintenance of body temperature).
3 Factors :• Heat production• Heat retention• Heat loss
PEDIATRIC NURSING MLNGC,MD, RN22
1. Heat Production
The newborn produces heat Thermogenesis – through
• general metabolism• muscular activity• nonshivering thermogenesis (unique to the
newborn)
Newborns rarely shiver as adults do to increase heat production.
Shivering in newborns indicates that the metabolic rate has already doubled.
PEDIATRIC NURSING MLNGC,MD, RN23
Infant in a cool environment requires more heat
metabolic rate increases producing more heat
– Newborn may cry and have muscular activity when cold, but there is no voluntary control of muscular activity.
– if the newborn’s temperature is not adequately raised through increased metabolism, nonshivering thermogenesis : the metabolism of brown fat begins.

PEDIATRIC NURSING MLNGC,MD, RN24
Non Shivering Thermogenesis
- the metabolism of brown fat
Brown fat- special tissue/ fat found only in newborns- appears at about 26-30 wks AOG and increases
until 2-5 wks of age- highly vascularized giving it a brown color- oxidized to produce or conserve heat- located at the back of the neck, intrascapular
region, thorax, around the kidneys and adrenals, in the axillae, around the heart and abdominal aorta and perineal area
• Once the brown fat has been metabolized, the infant no longer has this method of heat production available.
PEDIATRIC NURSING MLNGC,MD, RN25
PEDIATRIC NURSING MLNGC,MD, RN26
2. Heat Retention
Newborns retain heat by staying in a flexed position.
- reduces the area of skin exposed to the environmental temperature, thus decreasing
heat loss- peripheral vasoconstriction retains heat

PEDIATRIC NURSING MLNGC,MD, RN27
Conservation of Heat
1.Brown fat
2. kangaroo care – placing the newborn against themother’s skin and then covering the newborn helps to transfer heat from the mother to the newborn, thus, conserving heat

PEDIATRIC NURSING MLNGC,MD, RN28
REWARMING THE BABY SKIN-SKIN• Before rewarming remove the baby’s cold
clothing• Place the newborn skin-skin on the mother’s
chest dressed in a rewarmed shirt open at the front, a diaper, hat and socks.
• Check the temperature every hour until normal.• Keep the baby with the mother until the baby’s
body temperature is in normal range• If baby is small, encourage the mother to keep
the baby in skin-skin contact for as long as possible, day and night
• Be sure the temperature of the room where rewarming takes place is at least 25C.
• If the baby’s temp is not 36.5C or more after 2 Hrs of rewarming, reassess the baby.
• If referral is needed, keep the baby in skin-skin contact or another person on transport.

PEDIATRIC NURSING MLNGC,MD, RN29
3. Heat Loss
Newborn - thin skin with blood vessels close to the
surface and little subcutaneous fat to prevent heat l oss
Cold Stress - excessive heat loss
PEDIATRIC NURSING MLNGC,MD, RN30
increased metabolism
significant increase in need for oxygen
newborn may experience hypoxia
There may not be enough oxygen for the metabolic rate to increase, and the newborn will not be able to maintain body temperature.
PEDIATRIC NURSING MLNGC,MD, RN31
Effects of Cold Stress (temp<36.5)
1. Metabolic Acidosis- increased BMR, anaerobic glycolysis, increased acid production, metabolic
acidosis
2. Hypoglycemia- increased energy requirement to produce
heat- glucose necessary for increased
metabolism is made available when glycogen stores are converted to glucose
- if the glycogen is depleted, hypoglycemia results

PEDIATRIC NURSING MLNGC,MD, RN32
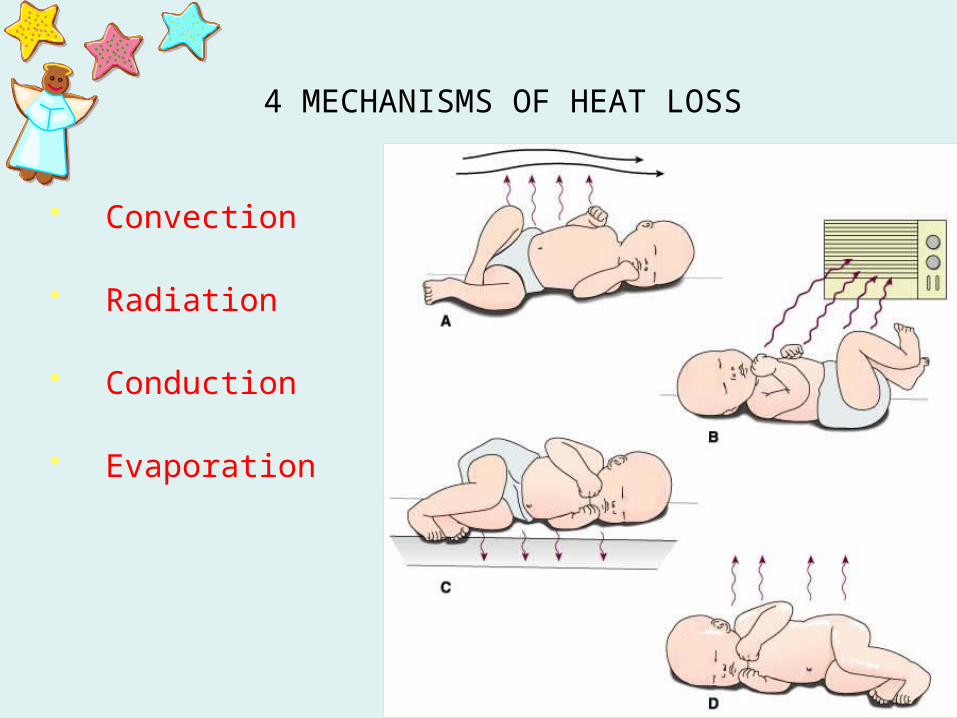
4 MECHANISMS OF HEAT LOSS
1. Convection - flow of heat from the newborn’s body surface to cooler surrounding air
2. Radiation - transfer of body heat to cooler solid object not in contact with the baby
3. Conduction - transfer of body heat to cooler solid object in contact with the baby
4. Evaporation -loss of heat through conversion of liquid to vapor
PEDIATRIC NURSING MLNGC,MD, RN33
4 MECHANISMS OF HEAT LOSS
• Convection
• Radiation
• Conduction
• Evaporation
PEDIATRIC NURSING MLNGC,MD, RN34
ConvectionLoss of heat by the movement of air
EX: air current from the open door or windows, air conditioning or from people moving around increases heat loss

PEDIATRIC NURSING MLNGC,MD, RN35
Radiation Loss of heat by transfer to cooler object nearby, but not through direct contact
EX: an infant placed near a cold window loses heat by radiation to the sides of the crib and the window

PEDIATRIC NURSING MLNGC,MD, RN36
Conduction Loss of heat by direct contact with cooler object:
EX: newborn touched by cold hands or cold stethoscope newborn placed on a cold surface such as Scale
PEDIATRIC NURSING MLNGC,MD, RN37
Evaporation
Loss of heat when water is changed to vapor
EX: When the wet body dries, heat is lost

PEDIATRIC NURSING MLNGC,MD, RN38
Other Causes of Heat Loss
1. insulation in newborn is not effective (little subcutaneous fat )
2. shivering is not present

PEDIATRIC NURSING MLNGC,MD, RN39
Immediate Assessment of the Newborn
PEDIATRIC NURSING MLNGC,MD, RN40
Assessment for Well-being
PEDIATRIC NURSING MLNGC,MD, RN41
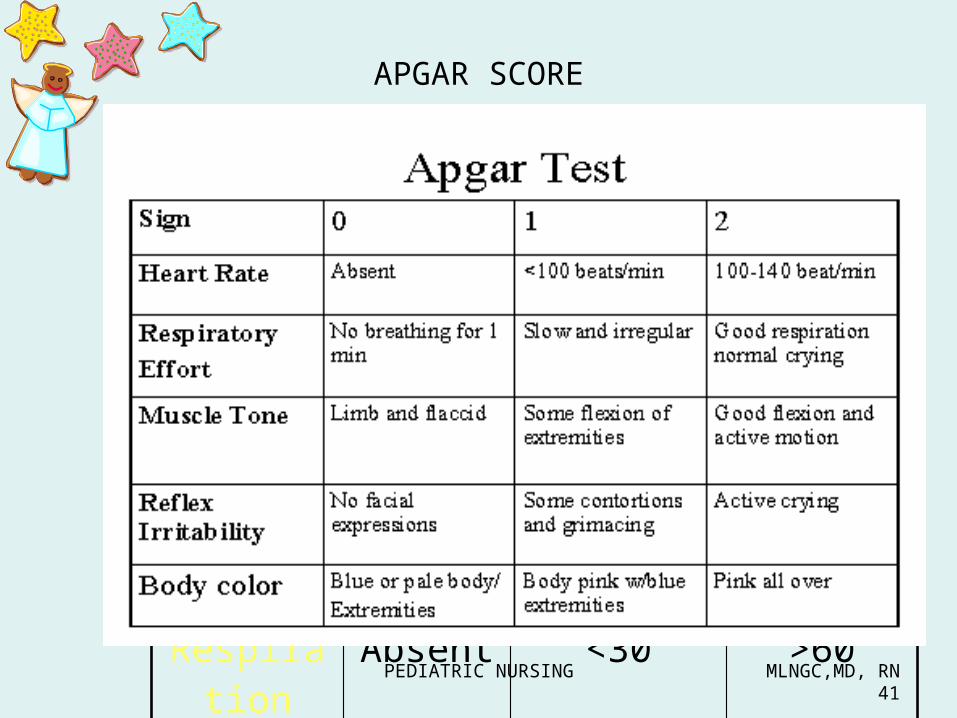
APGAR SCORE
0 1 2Appeara
nceBlue/Pale
Acrocyanosis
Pink; Ruddy
Pulse Absent < 100 > 100
Grimace None Weak cry Good cry
Activity Flaccid Some ext Flex/ext
Respiration
Absent <30 >60
PEDIATRIC NURSING MLNGC,MD, RN42
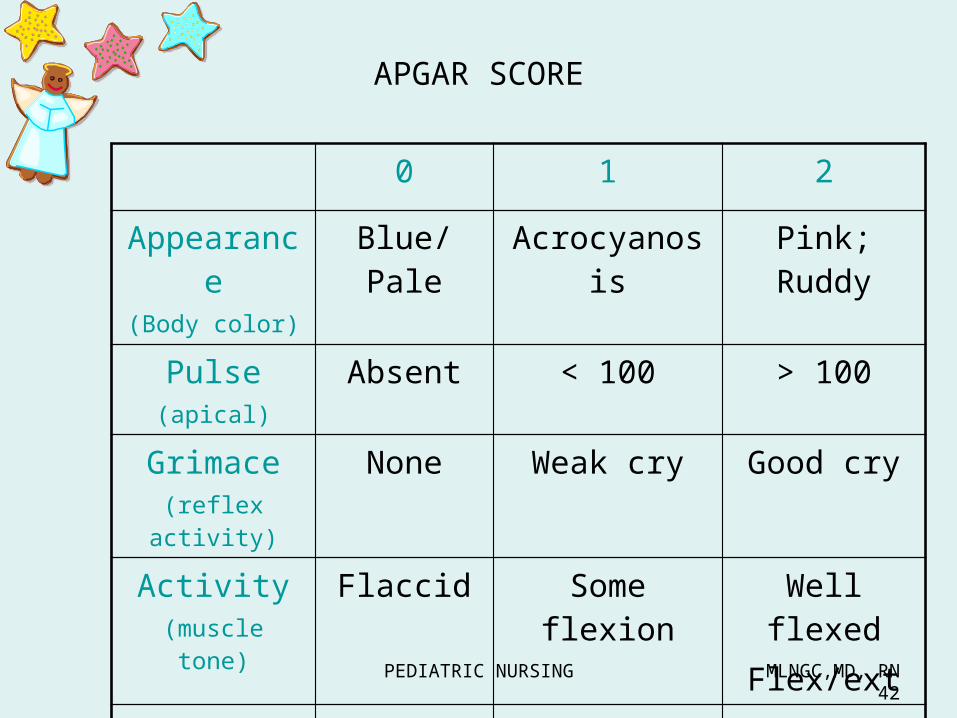
APGAR SCORE
0 1 2Appearanc
e(Body color)
Blue/Pale Acrocyanosis Pink; Ruddy
Pulse(apical)
Absent < 100 > 100
Grimace(reflex activity)
None Weak cry Good cry
Activity(muscle tone)
Flaccid Some flexion Well flexedFlex/ext
Respiration Absent <30 >60

PEDIATRIC NURSING MLNGC,MD, RN43
A ppearance (color) – least important P ulse rate - most important G rimace (reflex activity); irritability A ctivity (muscle tone) R espiration
Per parameter*Lowest individual score is 0.*Highest individual score is 2.

PEDIATRIC NURSING MLNGC,MD, RN44
APGAR Scoring System – standard tool to evaluate the condition of the
neonate
Done twice:1st minute: to determine general condition
(NEURO/RESPI/CIRCULATORY CHECK)
5th minute: to determine neonate’s adjustment to extrauterine life

PEDIATRIC NURSING MLNGC,MD, RN45
Apgar Scoring System
Score: 9 – highest score 10 – perfect score
0-3: poor, serious, severely depressed, needs CPR
4-6: fair, guarded, moderately depressed, needs suction
7-10: good, healthy
PEDIATRIC NURSING MLNGC,MD, RN46
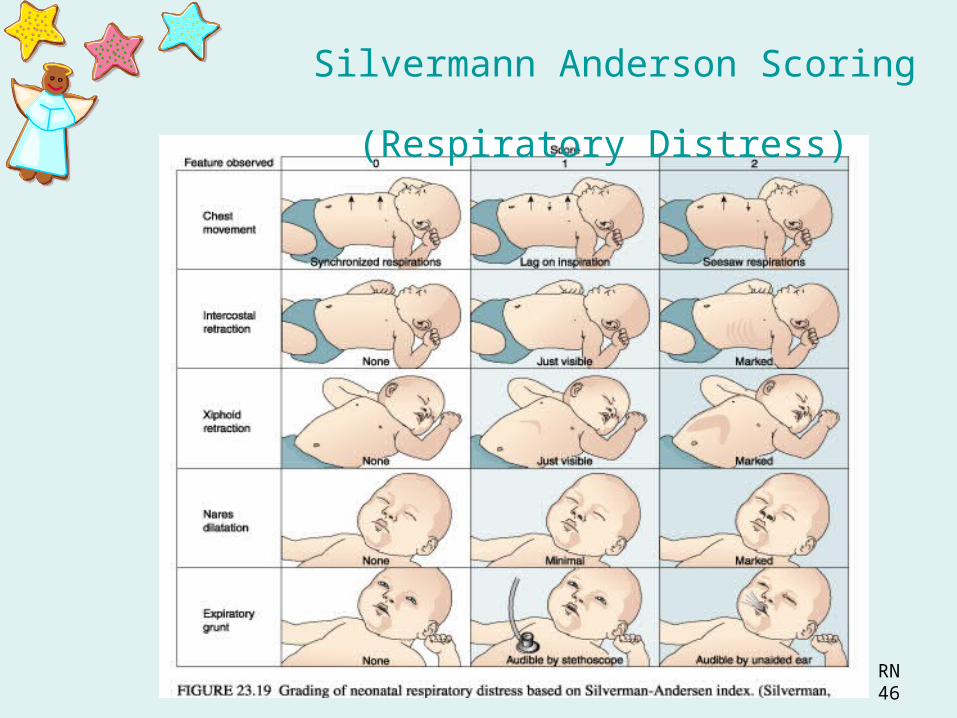
Silvermann Anderson Scoring (Respiratory Distress)

PEDIATRIC NURSING MLNGC,MD, RN47
Silverman Anderson Scoring (Respiratory Distress)
Scoring : 0-3 Normal / slight distress 4-7 moderate RDS 7-10 severe RDS
Assessment tool determines respiration of baby

PEDIATRIC NURSING MLNGC,MD, RN48
Grading of Neonatal Respiratory Distress (Silvermann Anderson)
Feature observed
0 1 2
1.Chest movement
synchronized lag seesaw
2.Intercostal retractions
None just visible marked
3.Xiphoid retraction
none just visible marked
4.Nares dilatation
none minimal marked
5.Expiratory grunt
none audible by stethoscope
audible by Unaided ear

PEDIATRIC NURSING MLNGC,MD, RN49
0: No respiratory distress1 -3: slight distress4-6: moderate distress
7-10: seriously distressed !!!
Grading of Neonatal Respiratory Distress (Silvermann Anderson)
PEDIATRIC NURSING MLNGC,MD, RN50
Congenital Anomalies1. Choanal Atresia - a complete blockage
or severe narrowing of the nasal airway at the posterior nares
2. Tracheobronchial fistula - there is a fistula between the trachea and the distal portion of the esophagus
3. Cleft lip and cleft palate
Substances1. drugs2. smoking3. alcohol

How will you know my age if my mommy doesn’t know
her LMP?

Assessment of GESTATIONAL AGEIt is determined in the first 4 hours after birth so that age related problems can be identified and appropriate care can be initiated.
Second assessment is done within 24 hours.New BALLARD Score is the most commonly used tool
It has 2 elements:External physical characteristicsNeuromuscular maturity

PEDIATRIC NURSING MLNGC,MD, RN53
Dubowitz/ Ballard (Maturity Testing Tool)
• done in the first 24 hours– Pre term – born before the 38th week– Post term – born after 42 weeks– Full term – born at 38 to 42 weeks
– Small Gestational Age (SGA) – BW is < 10th percentile• LBW – BW < 2,500 grams• VLBW – BW 1,500 grams
– Large Gestational Age (LGA) – BW > 90th percentile
– Appropriate Gestational Age (AGA) – BW within 10-90th percentile
IUGR - Rate of growth does not meet expected pattern - growth restriction

PEDIATRIC NURSING MLNGC,MD, RN54

PEDIATRIC NURSING MLNGC,MD, RN55

PEDIATRIC NURSING MLNGC,MD, RN56
Neuromuscular maturity1. Posture: With the infant supine and quiet, score as
follows: Arms and legs extended = 0 Slight or moderate flexion of hips and knees = 1 Moderate to strong flexion of hips and knees = 2 Legs flexed and abducted, arms slightly flexed = 3 Full flexion of arms and legs = 4
2. Square Window: Flex the hand at the wrist. Exert pressure sufficient to get as much flexion as possible. The angle between the hypothenar eminence and the anterior aspect of the forearm is measured and scored:
>90 degrees = -1 90 degrees = 0 60 degrees = 1 45 degrees = 2 30 degrees = 3 0 degrees = 4

PEDIATRIC NURSING MLNGC,MD, RN57
3. Arm Recoil: With the infant supine, fully flex the forearm for 5 seconds, then fully extend by pulling the hands and release. Score the reaction:
Remains extended 180 degrees, or random movements = 0
Minimal flexion, 140-180 degrees = 1 Small amount of flexion, 110-140 degrees = 2 Moderate flexion, 90-100 degrees = 3 Brisk return to full flexion, <90 degrees = 4
4. Popliteal Angle: With the infant supine and the pelvis flat on the examining surface, the leg is flexed on the thigh and the thigh fully flexed with the use of one hand. With the other hand the leg is then extended and the angled scored:
180 degrees = -1 160 degrees = 0 140 degrees = 1 120 degrees = 2 100 degrees = 3 90 degrees = 4 <90 degrees = 5

PEDIATRIC NURSING MLNGC,MD, RN58
5. Scarf Sign: With the infant supine, take the infant's hand and draw it across the neck and as far across the opposite shoulder as possible. Assistance to the elbow is permissible by lifting it across the body. Score according to the location of the elbow:
Elbow reaches or nears level of opposite shoulder = -1 Elbow crosses opposite anterior axillary line = 0 Elbow reaches opposite anterior axillary line = 1 Elbow at midline = 2 Elbow does not reach midline = 3 Elbow does not cross proximate axillary line = 4
6. Heel to Ear: With the infant supine, hold the infant's foot with one hand and move it as near to the head as possible without forcing it. Keep the pelvis flat on the examining surface. Score as shown in the diagram above.
PEDIATRIC NURSING MLNGC,MD, RN59
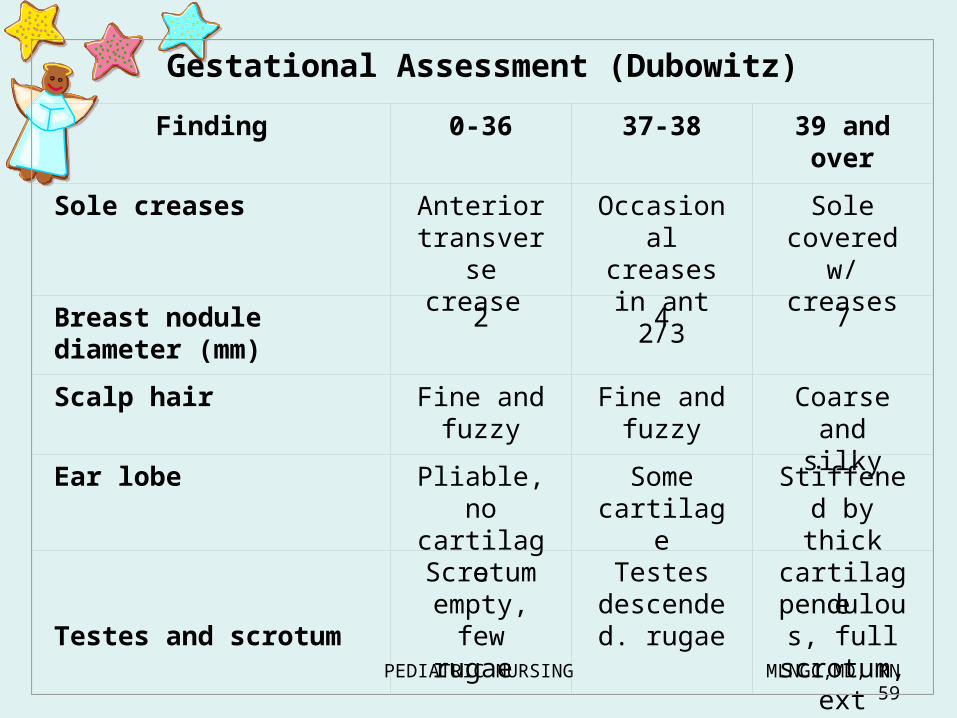
Gestational Assessment (Dubowitz)Finding 0-36 37-38 39 and
overSole creases Anterior
transverse crease
Occasional creases in ant 2/3
Sole covered
w/ creasesBreast nodule
diameter (mm)2 4 7
Scalp hair Fine and fuzzy
Fine and fuzzy
Coarse and silky
Ear lobe Pliable, no cartilage
Some cartilage
Stiffened by thick cartilage
Testes and scrotum
Scrotum empty,
few rugae
Testesdescended. rugae
pendulou
s, full scrotum, ext rugae

PEDIATRIC NURSING MLNGC,MD, RN60

PEDIATRIC NURSING MLNGC,MD, RN61
External physical characteristics

PEDIATRIC NURSING MLNGC,MD, RN62

PEDIATRIC NURSING MLNGC,MD, RN63

PEDIATRIC NURSING MLNGC,MD, RN64

PEDIATRIC NURSING MLNGC,MD, RN65

HIGH-RISK INFANT

PEDIATRIC NURSING MLNGC,MD, RN67
PRETERM newborn
• born before 37 weeks of gestation• Weight usually less than 2500 g ( 5 ½ lbs)
• Primary concern : immaturity of all body systems

PEDIATRIC NURSING MLNGC,MD, RN68
PRETERM newborn• CAUSES:
– Maternal factor: age, smoking , poor nutrition, placental problems, preeclampsia/ eclampsia
– Fetal Factor : multiple pregnancy, intrauterine growth retardation
• SEVERITY : – The earlier the infant is born, the greater the
chance of complication.• COMPLICATIONs:
1. Respiratory distress syndrome2. Thermoregulatory problem3. Conservation of energy4. Susceptibility to Infection5. Hemorrhage

PEDIATRIC NURSING MLNGC,MD, RN69
PE
1. Skin and subcutaneous tissue -thin, transparent2. Increased lanugo3. Decreased plantar creases4. Breast bud scarcely felt5. Pinna flat and shapeless6. Scrotum not pigmented7. Testes not descended8. Labia majora widely separated

PEDIATRIC NURSING MLNGC,MD, RN70
PRETERM newborn• Assessment :
1. Respiratory System:Insufficient surfactantApneic episodesRetraction, nasal flaring, grunting, seesaw
pattern of breathing, cyanosisIncreased respiratory rate
2. Thermoregulation: body temperature fluctuates easily
( less muscle & fat )3.NUTRITIONAL status :
Poor sucking and swallowing reflexPoor gag and cough reflexes
4 mL/kg/dose
PEDIATRIC NURSING MLNGC,MD, RN71
PRETERM newborn• Assessment :
4. Skin : lacks subcutaneous fat ; reddened; translucent
5.Drainage from umbilicus/eye6.Cardiovascular:
Petecchiae caused by fragile capillaries and prolonged prothrombin time
Increased bleeding at injection site7. Neuromuscular:
Poor muscle toneWeak reflexesWeak , feeble cry

PEDIATRIC NURSING MLNGC,MD, RN72
NURSING INTERVENTIONS
1. Maintain respiration at < 60/minute, check q1-2H
2. Administer 02 as ordered : check concentration q 2H to avoid ( retrolental fibroplasia ) while providing oxygenation
3. Auscultate breath sounds to assess lung expansion
4. Encourage breathing with gentle rubbing of back and feet
5. Suction as needed6. Reposition q1-2H for maximum lung expansion
and prevention of exhaustion7. Monitor blood gases and electrolytes
PEDIATRIC NURSING MLNGC,MD, RN73
NURSING INTERVENTIONS8. Maintain thermoneutral body temperature
prevent cold stress9. Maintain appropriate humidity level10. Monitor for signs of infection: little Ab
production and decreased resistance11. Feed according to abilities12. Monitor sucking reflex:
* poor – gavage feeding13. Use “preemie” nipple if bottle feeding14. Monitor I&O, wt gain or loss
* easily dehydrated with poor electrolyte balance
15. Monitor hypoglycemia & hyperbilirubinemia

PEDIATRIC NURSING MLNGC,MD, RN74
NURSING INTERVENTIONS16. Handle with care : organize care to minimize
disturbance17. Provide skin care with special attention to
cleanliness and careful positioning to prevent breakdown
18. Monitor heart rate and pattern q1-2H : listen to apical for 1 full minute
19. Monitor potential bleeding sites: lowered clotting factor
20. Monitor over-all growth and development of infant, check weight, length and HC
21. Provide complete tactile stimulation when caring for or feeding infant
22.Provide complete explanation for parents23.Encourage parental involvement in infant care

PEDIATRIC NURSING MLNGC,MD, RN75
Hypoglycemia
- <40 mg/100 ml- dependent on maternal supply- Birth, continue to produce insulinS/sx: limpness, jitteriness, apnea, twitching
and high pitched cryCX: mental retardationTx: early feeding
D10WNsg: monitor blood glucose level

PEDIATRIC NURSING MLNGC,MD, RN76

PEDIATRIC NURSING MLNGC,MD, RN77
PEDIATRIC NURSING MLNGC,MD, RN78
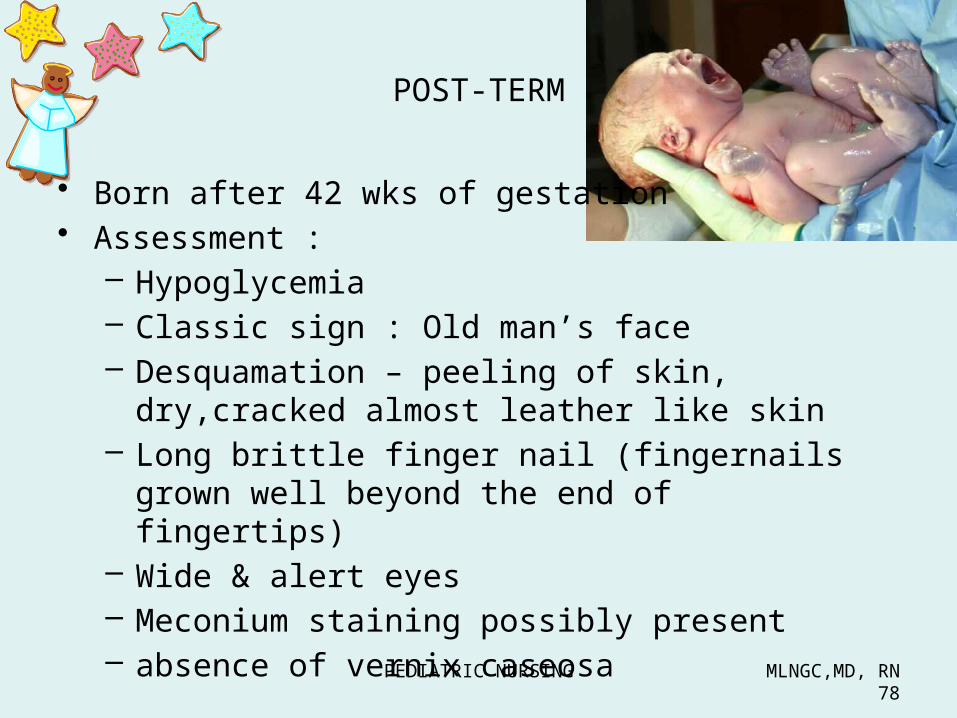
POST-TERM
• Born after 42 wks of gestation• Assessment :
– Hypoglycemia– Classic sign : Old man’s face– Desquamation – peeling of skin, dry,cracked
almost leather like skin– Long brittle finger nail (fingernails grown well
beyond the end of fingertips)– Wide & alert eyes– Meconium staining possibly present – absence of vernix caseosa

PEDIATRIC NURSING MLNGC,MD, RN79
Post-term (>42 weeks)
• INTERVENTIONS:– Provide normal newborn care– Maintain temp– Monitor for meconium aspiration
PEDIATRIC NURSING MLNGC,MD, RN80
• Complications:1. may develop polycythemia (oxygenation)2. hypoglycemia

PEDIATRIC NURSING MLNGC,MD, RN81
IDENTIFICATION(Existing/ Old Protocol)

PEDIATRIC NURSING MLNGC,MD, RN82
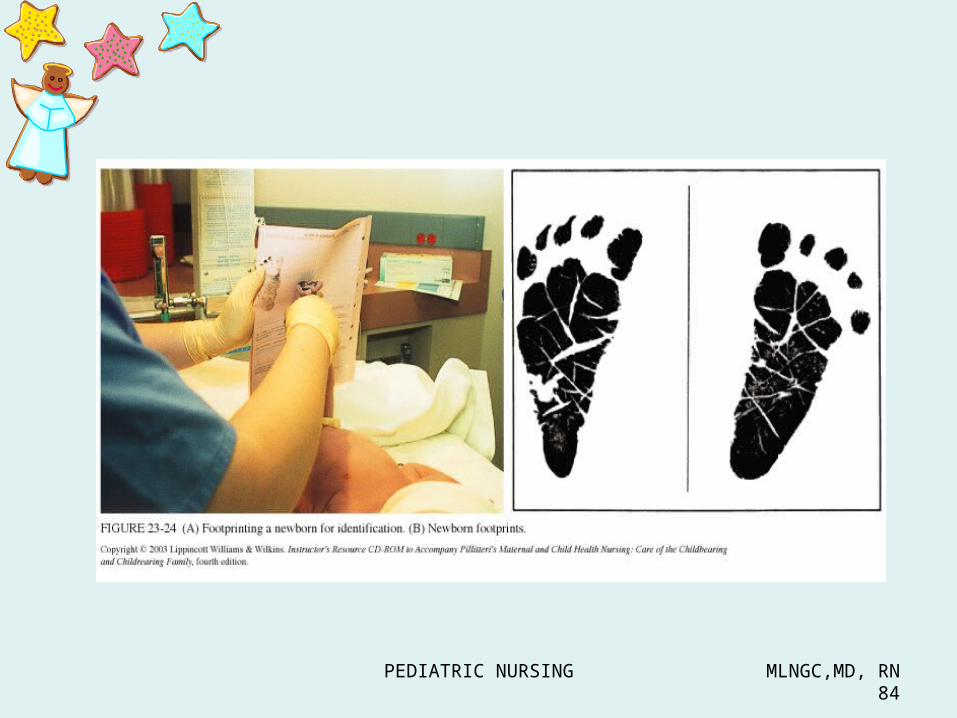
Proper Identification
– done in D.R. before being brought to the Nursery
a. Footprints – most reliable
b. ID bands – ankle, wrist
c. Birthmarks

PEDIATRIC NURSING MLNGC,MD, RN83
PEDIATRIC NURSING MLNGC,MD, RN84
PEDIATRIC NURSING MLNGC,MD, RN85
• Ensure newborn’s proper identification
• Footprint newborn and fingerprint mother on identification sheet per agency policies and procedures
• Place matching identification bracelets on mother and newborn.
• REMEMBER! ID band must be checked and compared to the mother’s band each time the baby is brought into the mother’s room.
PEDIATRIC NURSING MLNGC,MD, RN86
Immediate Care of the Newborn in the Nursery
(Existing/ Old Protocol)

PEDIATRIC NURSING MLNGC,MD, RN87
* Note that ID bands of mother and baby are matched.

PEDIATRIC NURSING MLNGC,MD, RN88
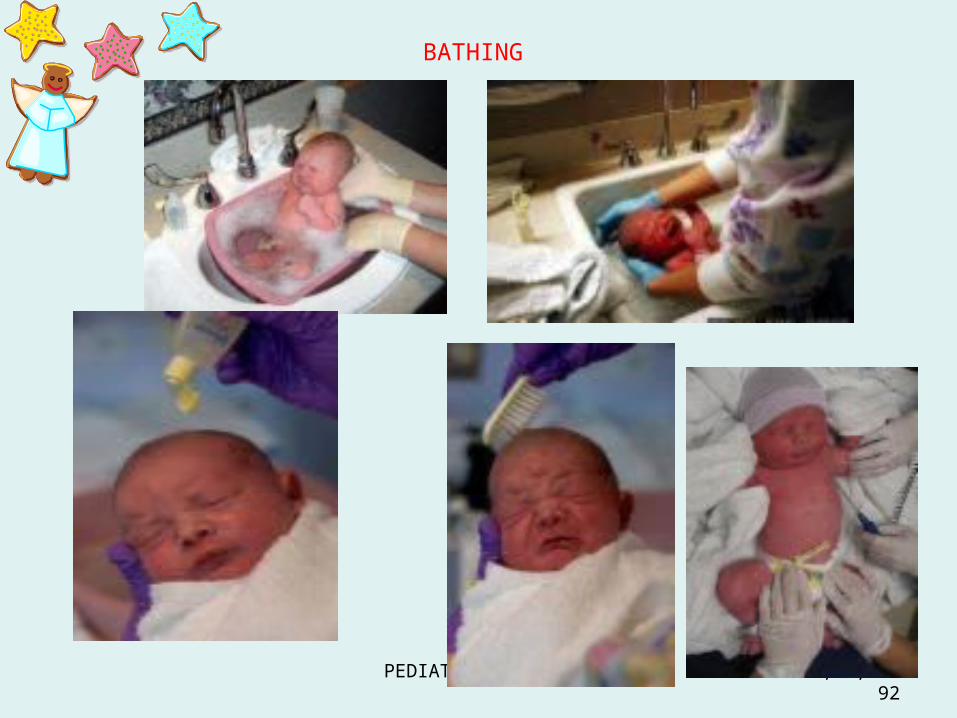
Special Initial Care1. Initial bath – best done with temp of NB is
stable or at least 37oC– Water bath – 98-100 F or 37-38 C– Water with non-alkaline soap
– Oil – for vernix caseosa– Antimicrobial solution – most preferred in NB if
mother has infection in the vaginal canal.a. Trichomoniasisb. Candidiasisc. Chlamydiad. Gonorrhea

PEDIATRIC NURSING MLNGC,MD, RN89
First bath
• Complete bath within an hour after birth to remove vernix caseosa
• For the next 10 days to 2 weeks – sponge bath.• NB are not generally given tub bath until the cord
has fallen off and healing is complete• Nurse giving the first bath to NB must wear
gloves to comply with standard precautions regarding contact with blood or body fluids

PEDIATRIC NURSING MLNGC,MD, RN90
2.Taking the Temperature
* Maintain temperature to prevent cold stress
* Use Rectal route
* Meconium - 24-48 hrs

PEDIATRIC NURSING MLNGC,MD, RN91
PEDIATRIC NURSING MLNGC,MD, RN92
BATHING
PEDIATRIC NURSING MLNGC,MD, RN93
3. Initial Cord dressing
• Inspect for A .V. A.• Done with strict aseptic technique practice• Apply cord clamp to prevent bleeding• Application of antiseptic solution
– Povidone iodine– 70% alcohol
to prevent Tetanus Neonatorum and Omphalitis
(streptococcal and staphylococcal infections)

PEDIATRIC NURSING MLNGC,MD, RN94
Initial Cord Dressing
CORD: 2 A + 1 V*Practice aseptic technique
Signs of Omphalitis:
*Reddening of the area*Fever*Discharge and foul smell
Application of sterile cord clamp to prevent bleeding within the 1st 24 hours ** The cord will fall off after – 7-10 days

PEDIATRIC NURSING MLNGC,MD, RN95

PEDIATRIC NURSING MLNGC,MD, RN96
7-10 days Will fall-off

PEDIATRIC NURSING MLNGC,MD, RN97
4. Crede’s prophylaxis• Preventive or prophylactic treatment against
OPHTHALMIA NEONATORUM - acquired during passage to the birth canal
• Gonorrheal Conjunctivitis (Neisseria gonorrhea) causes blindness if not treated. Infection can be acquired during delivery from a mother with untreated gonorrhea.
• Medications such as :– Eye ointment : Terramycin , Gentamycin ,
Erythromycin , Chloramphenicol .– Eye drop : Silver Nitrate 1% but this
causes CHEMICAL CONJUNCTIVITIS

PEDIATRIC NURSING MLNGC,MD, RN98

PEDIATRIC NURSING MLNGC,MD, RN99
CREDE’S PROPHYLAXIS
Ophthalmic drops – BEFORE: Silver Nitrate or AgNO3 1% 1-2 drops
1-2 gtts into the lower conjunctival sac
AT PRESENT:Ointment – inner to outer canthus
TerramycinGentamycinChloramphenicolErythromycin – drug of choice of
Chlamydial TrachomatisChemical Conjunctivitis- usually develops in 3-4 days after application of either ointment or drops

PEDIATRIC NURSING MLNGC,MD, RN100
Eye / Crede’s prophylaxis

PEDIATRIC NURSING MLNGC,MD, RN101
Erythromycin
- Pull eyelids downward- 0.5-1 cm- Inner to outer canthus- Wipe excess away

PEDIATRIC NURSING MLNGC,MD, RN102
5. Vitamin K Injection
• To prevent bleeding because of decreased Vit K synthesis due to sterile GIT
• Facilitates production of clotting factor
• Medications: – Phytonadione – Aquamephyton– Phytomenadione – Konakion
– DOSE : Fullterm : 1 mg = 0.1 ml Preterm : 0.5 mg = 0.05 ml
• ROUTE : IM lateral anterior thigh (Vastus lateralis)

PEDIATRIC NURSING MLNGC,MD, RN103

PEDIATRIC NURSING MLNGC,MD, RN104
6. Take anthropometric measurements7. Initial feeding8. Physical assessment

INTAKE OF ADEQUATE NOURISHMENT

PEDIATRIC NURSING MLNGC,MD, RN106
Nutrition
Recommended Daily Allowances:Calories – 120 cal/kg body weight (KBW)/day
= 50-55 cal/lb body weight/day = more or less 380 cal/day
Proteins – 2.2 grams/KBW/dayFluids – 160-200 cc/KBW/day = 2.5-3 oz/lb body
weight/day = more or less 20 oz/day
Vitamins – Vitamins A, C and D are recommended for both bottlefed and breastfed babies during entire first year of life.

PEDIATRIC NURSING MLNGC,MD, RN107
• NB stomach Capacity is only 20 ml (30ml= 1 0z)
• 7 days old – 60-90 ml ( can consume 2-3 0z )
• Gastric capacity = age in months + 2

PEDIATRIC NURSING MLNGC,MD, RN108
CRITERIA FOR INITIATING FEEDING 1. no history of excessive oral secretion 2. non-distended, soft abdomen 3. clinically stable 4. RR < 60 CPM

PEDIATRIC NURSING MLNGC,MD, RN109
Initial Feeding
1-6 hours after birth
CS : BF after 4 HNSD : ASAP
1 oz of sterile water
Subsequent feeding – by demand

PEDIATRIC NURSING MLNGC,MD, RN110
• May breastfeed immediately after birth– Philippine Milk Code EO 51 : Promote
breastfeeding– Rooming-in Act of 1992 RA 7600 : promotes
breastfeeding and requires immediate rooming-in of the newborn
PEDIATRIC NURSING MLNGC,MD, RN111
Breastfeeding1. bonding2. uterine contraction3. colostrum 4. Contraceptive5. Cheap6. Right temperature7. Antibacterial – Lactoferrin, Lactobacillus bifidus,
lysozyme, macrophage, T lymphocytes, lactoperoxidase
8. Breastfeed baby has a higher IQ9. Antibodies to E. coli10. Anti-staphylococcus factor11. decreased incidence of dental caries

PEDIATRIC NURSING MLNGC,MD, RN112
BREASTFEEDING• Emphasize the importance of
exclusive breastfeeding on demand for the first 6 months of life.
• EXPRESSED MILK SHELF LIFE
Expressed milk Consume w/in 6HFresh frozen expressed milk
Not consumed within the next 24 H ( lasts 48H)
Refrigerated Consumed within 24H
PEDIATRIC NURSING MLNGC,MD, RN113
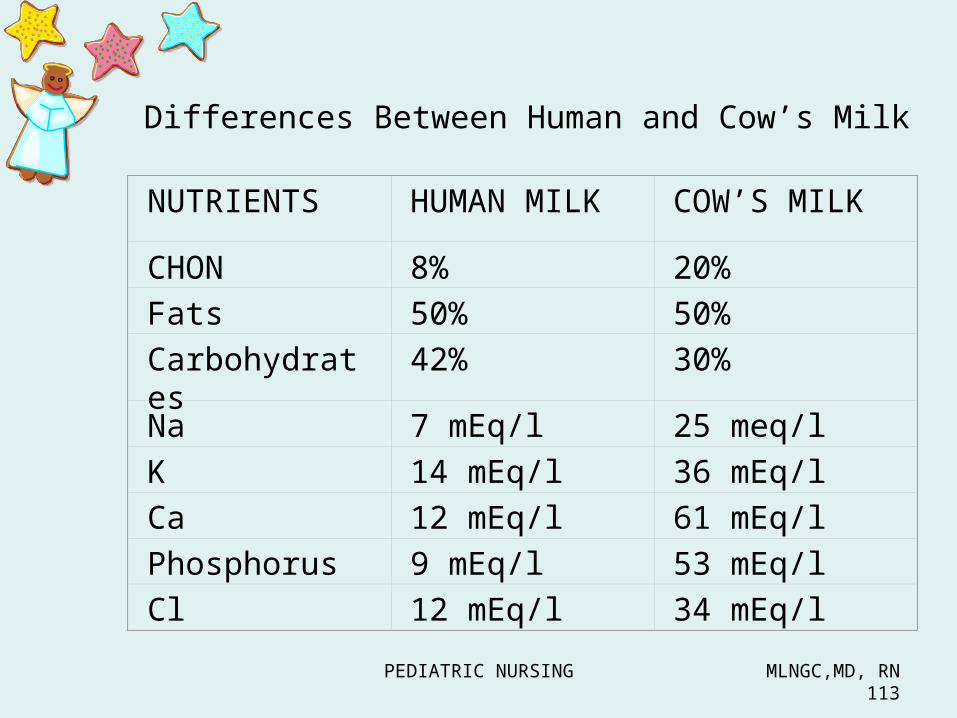
Differences Between Human and Cow’s Milk
NUTRIENTS HUMAN MILK COW’S MILKCHON 8% 20%Fats 50% 50%Carbohydrates
42% 30%Na 7 mEq/l 25 meq/lK 14 mEq/l 36 mEq/lCa 12 mEq/l 61 mEq/lPhosphorus 9 mEq/l 53 mEq/lCl 12 mEq/l 34 mEq/l
PEDIATRIC NURSING MLNGC,MD, RN114
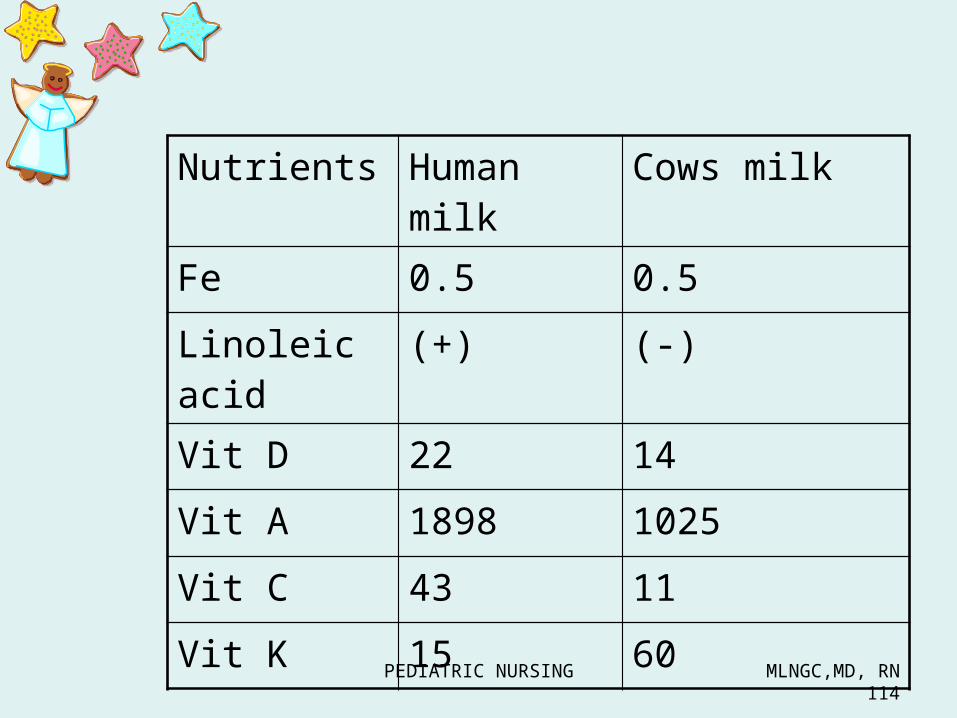
Nutrients Human milk
Cows milk
Fe 0.5 0.5Linoleic acid
(+) (-)
Vit D 22 14 Vit A 1898 1025Vit C 43 11Vit K 15 60
PEDIATRIC NURSING MLNGC,MD, RN115
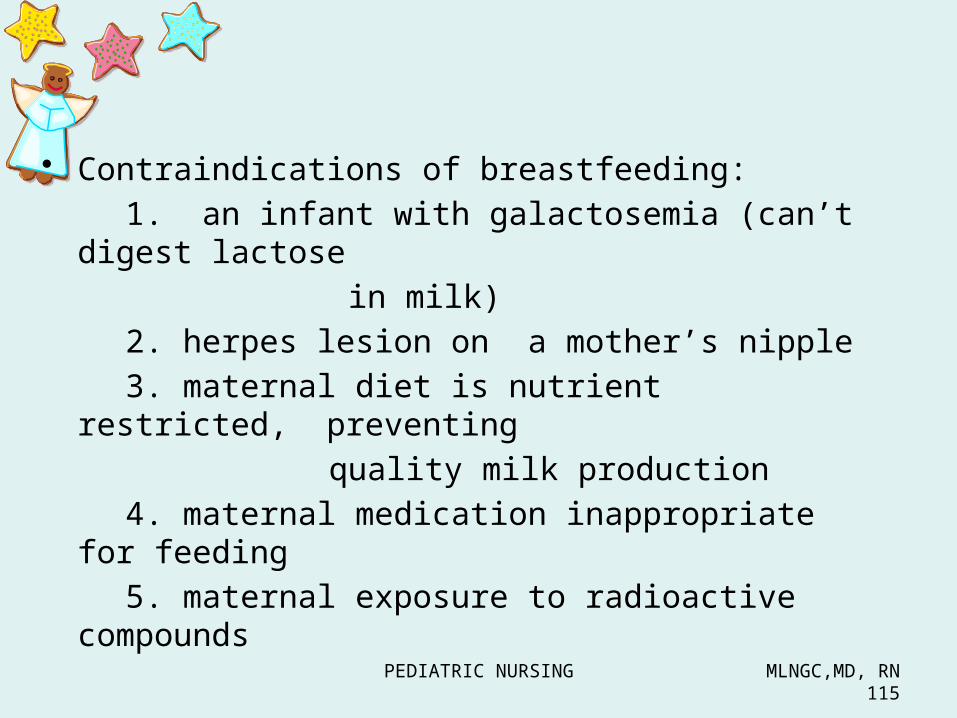
• Contraindications of breastfeeding:1. an infant with galactosemia (can’t
digest lactose in milk)
2. herpes lesion on a mother’s nipple3. maternal diet is nutrient restricted,
preventing quality milk production
4. maternal medication inappropriate for feeding
5. maternal exposure to radioactive compounds

PEDIATRIC NURSING MLNGC,MD, RN116
• Advantages of breastfeeding : to the baby1. contains secretory immunoglobulins A2.contain lactoferrin ( iron-binding chon in breast milk that interferes with growth of pathogenic bacteria3. contains antibodies4. reduces incidence of diarrhrea( presence of L.Bifidus interferes with colonization of pathogenic bacteria in the GIT)5.contains high amount of mineral and electrolytes6. contains more linoleic acid ( essential fatty acid for skin integrity and less Na,K,Ca and phosporous)
PEDIATRIC NURSING MLNGC,MD, RN117
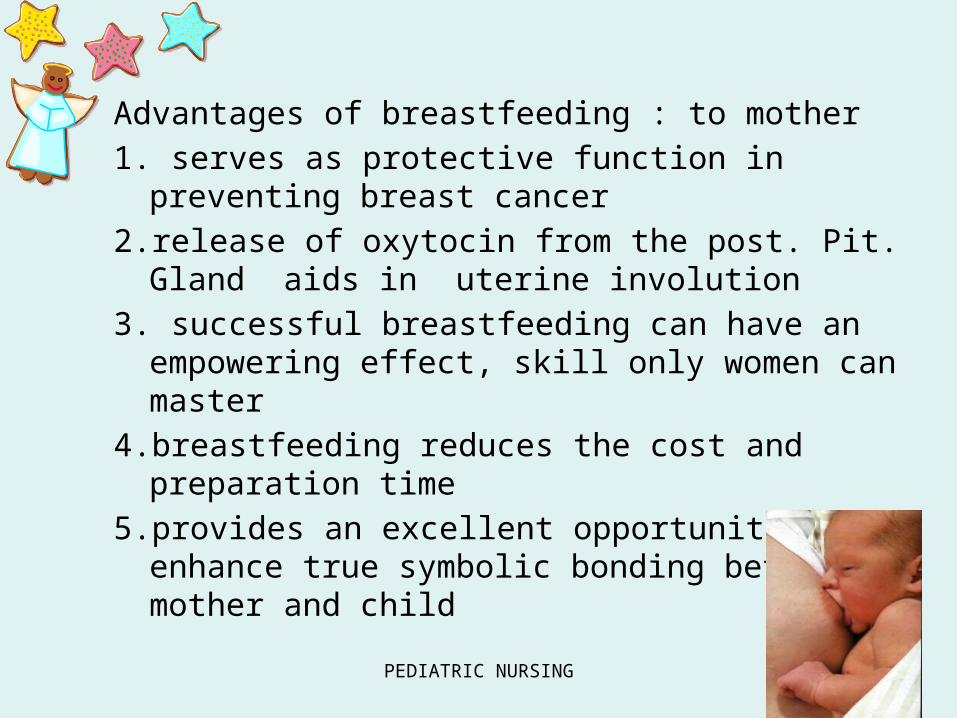
Advantages of breastfeeding : to mother1. serves as protective function in preventing
breast cancer2.release of oxytocin from the post. Pit. Gland aids
in uterine involution3. successful breastfeeding can have an
empowering effect, skill only women can master4.breastfeeding reduces the cost and preparation
time5.provides an excellent opportunity to enhance
true symbolic bonding between mother and child

PEDIATRIC NURSING MLNGC,MD, RN118
BREASTFEEDING BOTTLEFEEDING•Non-allergenic•Meet infant ‘s specific nutritional needs•Immunologic properties help prevent infection•Easily digested•Constipation unlikely•Overfeeding less likely•No formula or bottles to buy•No formula and bottle to prepare•Oxytocin release help involution•Mother more likely to eat well balance diet•May help with mother’s weight loss•Enhances mother/infant attachment through skin to skin contact•Frozen -20c (6 mos)•Refrigerated 4c ( 24 H)
•Father or others may feed infant day or night•Feed less frequently (3-4H)•Amount of milk taken at each feeding known
ADVANTAGES
PEDIATRIC NURSING MLNGC,MD, RN119
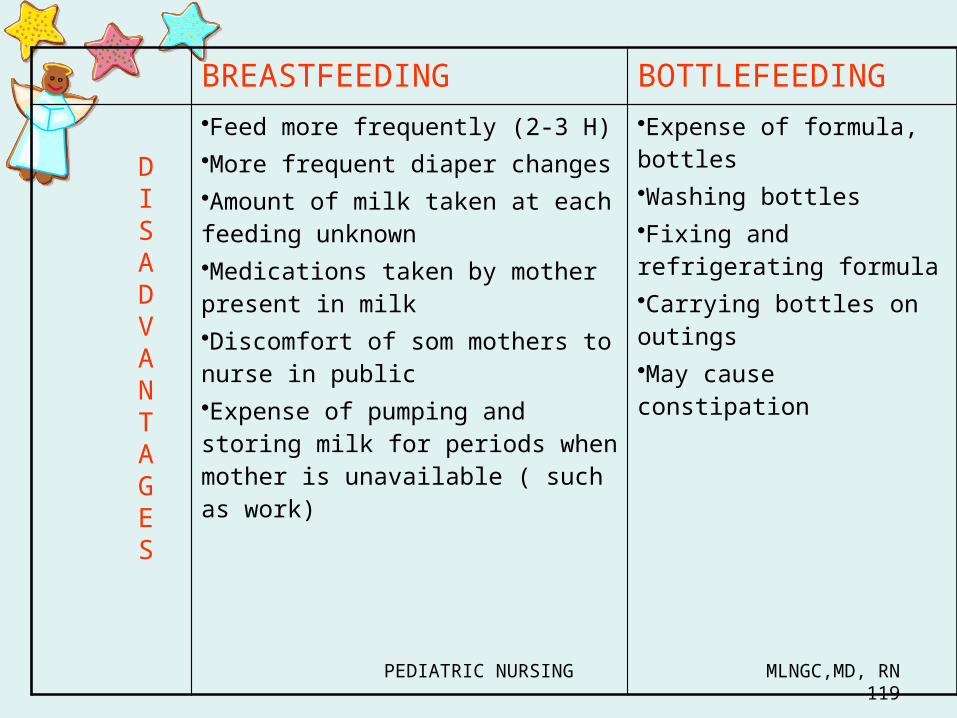
BREASTFEEDING BOTTLEFEEDING•Feed more frequently (2-3 H)•More frequent diaper changes•Amount of milk taken at each feeding unknown•Medications taken by mother present in milk•Discomfort of som mothers to nurse in public•Expense of pumping and storing milk for periods when mother is unavailable ( such as work)
•Expense of formula, bottles•Washing bottles•Fixing and refrigerating formula•Carrying bottles on outings•May cause constipation
DISADVANTAGES

BREASTFEEDINGHealth teaching:1. Proper hygiene2. Best position - upright sitting3. Stimulate & evaluate feeding reflexes
1. Rooting2. Sucking3. ExtrusionCriteria for effective sucking4. baby’s mouth is hiked up to areola5. Mom experiences after pain6. Other nipple is flowing with milk

PEDIATRIC NURSING MLNGC,MD, RN121
Breastfeeding• Position for feeding: Teach the mother
to -Make sure the baby’s head and body are in straight line– Make sure the baby is facing the
breast, with the nose opposite the mothers nipple
– Hold the baby ‘s body close to her body
– Cradle hold with infant’s head in the bend of the mother’s elbow and arm supporting the infant’s body
– OTHERS:• Football hold• Side lying position• Across lap
Cradling

PEDIATRIC NURSING MLNGC,MD, RN122
BreastfeedingHELP THE BABY TO ATTACH
– Latching on• TEACH THE MOTHER TO
– Touch the baby’s lips with her nipple– Wait until the baby’s mouth is opened
wide, then position the baby’s mouth onto her breast so that the baby’s mouth is well around the areola.
• SIGN OF GOOD ATTACHMENT:– Slow , deep sucks with occasional pauses– Unsatisfactory: try again then reassess– Breast engorged : express small amount of
BM before starting to breastfeed to soften the nipple area and facilitate easier attachment
Cradling

PEDIATRIC NURSING MLNGC,MD, RN123
Breastfeeding
• Length of feeding– Varies with each mother /infant unit
• BURPING- – ALL INFANTS REQUIRE BURPING– TO EXPEL THE AIR SWALLOWED
WHEN THE INFANT SUCKS– SOME INFANT SWALLOW MORE
AIR THAN OTHERS AND REQUIRE MORE FREQUENT BURPING
Cradling

PEDIATRIC NURSING MLNGC,MD, RN124
BURPING TECHNIQUE
1. OVER THE SHOULDER
2. FACE DOWN ON YOUR LAP
3. SITTING UP

PEDIATRIC NURSING MLNGC,MD, RN125
Waste Elimination3 types of stools passed by NB:
1. Meconium – greenish-blackish, viscous - amniotic fluid, intestinal secretions and cells shed from mucosa- take note of time when meconium first passed ( Normally : 24-36H)
Failure to Pass : THINK OF HIM
1. Hirschsprung disease2. Imperforate Anus
3. Meconium Ileus

PEDIATRIC NURSING MLNGC,MD, RN126
2. Transitional – passed from 3rd to 10th day3. Milk stool
a. Breast fed infant stool – loose golden yellow in color with sweet odor; 2-3 times a day
b. Bottle fed infant stool – formed, pale yellow with a typical odor; usually passed 1-2 times a day

PEDIATRIC NURSING MLNGC,MD, RN127
DIFFERENT STOOLSJaundiced baby Light stoolUnder phototherapy Bright greenMucus mixed with stool Milk allergyObstruction to bile duct Clay colored
After Barium enema Chalk clay coloredGIT bleeding Black stoolAnal fissure Blood flecked stoolIntussusceptions Currant jelly stoolHirschsprung Ribbon like stoolMalabasorption syndrome ( celiac, cystic fibrosis)
Steatorrhea ( fatty foul smelling stool)

PEDIATRIC NURSING MLNGC,MD, RN128
Parent/Infant Bonding
• interaction between parents and infant should be promoted as soon as the infant is stable
• The nurse may assist the parents in holding their baby or give them permission to examine the infant

PEDIATRIC NURSING MLNGC,MD, RN129
Behavioral Characteristic
During the first 6-10 hours after birth infant has a fairly predictable pattern of behavior called
PERIOD OF REACTIVITY
PEDIATRIC NURSING MLNGC,MD, RN130
Period of reactivity
• 2 periods of reactivity occur during the first few hours of life
• Separated by a period of sleep
– FIRST PERIOD OF RACTIVITY• The first 30 minutes after birth• Newborn is awake, alert and active• Primetime for parents/infant interaction• Newborn acts hungry, with strong
sucking reflex• Ideal time to begin breastfeeding• HR , RR are rapid & bowel sounds
seldom heard

PEDIATRIC NURSING MLNGC,MD, RN131
Period of reactivity
– FIRST PERIOD OF REACTIVITY– Sleep period
• The newborn enters a sleep period that usually lasts from 2-4 hours.
• Time of deep sleep• Difficult to awaken NB• HR , RR return to baseline and bowel
sounds become audible

PEDIATRIC NURSING MLNGC,MD, RN132
Period of reactivity– FIRST PERIOD OF RACTIVITY– SECOND PERIOD OF REACTIVITY
• Lasts from 4 to 6 hours• NB is once again awake and alert• HR , RR with period of apnea w/c causes HR
to decrease• NB may gag, spit up or choke or gastric and
respiratory mucus increases• CLOSE OBSERVATION is a must – maintain
clear airway• First meconium stool is often passed• First voiding may occur

PEDIATRIC NURSING MLNGC,MD, RN133
Physical Assessment

PEDIATRIC NURSING MLNGC,MD, RN134
Senses
1. hearing- becomes acute after birth, recognizes mothers voice
immediatelyfunctional at birth as soon as the external ear canal is cleaned
2. vision- focuses best on black and white at a distance of 9 to 12 inches. not well developed at birth
4 months of age – clear vision
7 y/o = 20/20 vision
PEDIATRIC NURSING MLNGC,MD, RN135
Senses
3. Tactile ( touch) starts in early prenatal life from face, then spreads to limbs and finally to the trunks in cephalocaudal succession.
Pain sensation – not well developed in NB lasts a weekResponse to pain – generalized
movement & crying7-9 months – can localize the site of
pain and withdraw from it.12-16 months – shoves painful away
and bring hand to irritated area

PEDIATRIC NURSING MLNGC,MD, RN136
Senses
4. Taste – can taste but unable to distinguish flavor.
3 months old – acute taste discrimination is achieved.
5. Olfactory – observed at birth more acute at later age

PHYSICAL CHARACTERISTICS OF THE NEWBORN
Vital Signs
Anthropometric measurement
General Appearance
PEDIATRIC NURSING MLNGC,MD, RN138
Immediate Assessment of the Newborn
• The newborn infant should undergo a complete P.E within 24 hours of birth.– NOTE :
• It is easier to listen to the heart and lungs first when the infant is quiet
• Warm the stethoscope before using to decrease the likehood of making the infant cry

PEDIATRIC NURSING MLNGC,MD, RN139
Assessment of The Newborn
• Initial Physical Examination :A. General Guidelines:
• Keep the NB warm during the examination.• Begin with general observations and then
perform assessment that are least disturbing to the NB first.
• Initiate nursing interventions for abnormal findings.
• Document all abnormal findings.
PEDIATRIC NURSING MLNGC,MD, RN140
1. Vital Signs• using apical pulse = PMI: Point of Maximum Impulse
(located at MCL 4th- 5th ICS or below the left nipple line)• 1 full minute
– This is done using a stethoscope.– Radial pulse is normally not prominent. – If it is, it may be a sign of congenital heart anomaly
(i.e., PDA).– Femoral or brachial pulses – if absent, indicates,
coarctation of the aorta and hip dislocation.
– Pulse is IRREGULAR, RAPID>160-180 beats/min. at birth
120-140 (stable)
Assessment of The Newborn

PEDIATRIC NURSING MLNGC,MD, RN141
During sleep - 90-110 bpmIf crying, up to 180 bpm
Pulse : heart rate in utero- 120 t0 160 bpm after 1 hr newborn settles, heart rate stabilizes to an average of 120 to 140 bpm- remains irregular because of immaturity of cardiac regulatory center in the medulla- when crying, rate might increase to 180 bpm- may decrease to 90 to 110 bpm during sleep- femoral pulses are more appreciated than radial and temporal pulses ( always palpate for the femoral pulses; their absence suggests coarctation of aorta)

PEDIATRIC NURSING MLNGC,MD, RN142
B. Respirations - 1 full minute
- irregular, shallow, rapid w/ brief apneic spells < 15s
60-80 breaths/min at birth
NORMAL: 30–60/minute

PEDIATRIC NURSING MLNGC,MD, RN143
Respiration : average is 30 to 60 breaths per minute- respiratory rate, rhythm, depth are likely to be irregular and short periods of apnea ( periodic respiration) are normal- coughing and sneezing are present at birth to clear the airway- newborns are obligate nose-breathers

PEDIATRIC NURSING MLNGC,MD, RN144
C. Blood Pressure - not usually measured
*not routinely obtained except for suspicion of Coarctation of the Aorta.
80–60/45–40 mm Hg at birth 100/50 mm Hg at day 10
PEDIATRIC NURSING MLNGC,MD, RN145
D. Temperature
Normal range: 36.5C–37.5C (axilla)
Axillary: 36.4C–37.2C Skin: 36.0 C–36.5C Rectal: 36.6C–37.2C
* Temperature 37.2 at birth

PEDIATRIC NURSING MLNGC,MD, RN146
Crying - increases body temperature slightly
Radiant warmer - falsely increases axillary temperature

PEDIATRIC NURSING MLNGC,MD, RN147
Anthropometric Measurements (Vital Statistics)
BW: 2.5 – 3.4 kgs(5.5 – 7.5 lbs)
* 1 K = 2.2 lbs
BL: 47.5 – 53.75 cm (19 – 21 ½ in)
Average: 50.8 cm/20 in
* 1 inch = 2.54 cm

PEDIATRIC NURSING MLNGC,MD, RN148

PEDIATRIC NURSING MLNGC,MD, RN149
Physiologic weight loss
- 5-10 % in 10 days
Causes1. no longer under influence of maternal
hormones2. voids and passes out stools3. relatively low nutritional intake4. beginning difficulty establishing sucking

PEDIATRIC NURSING MLNGC,MD, RN150
Breastfed infant recaptures birth weight within 10 days
Formula fed infant recaptures weight gain with in 7 days
Then continues to gain weight of 2lb/month( 6-8oz/ wk) for the 1st 6 months of life

PEDIATRIC NURSING MLNGC,MD, RN151
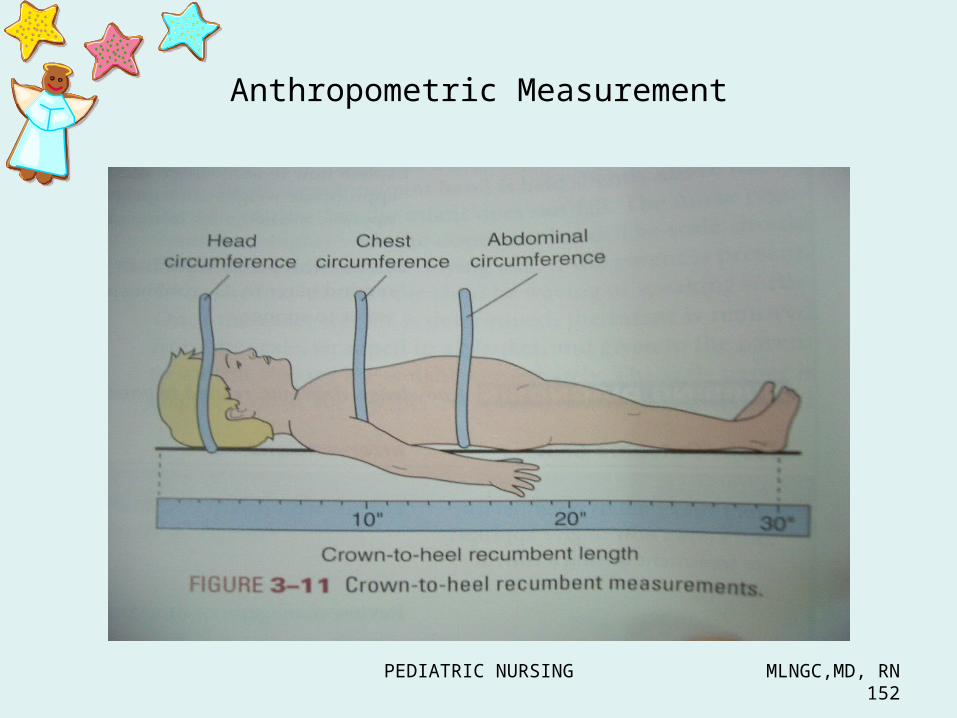
HC: 33 – 35 cmCC: 31 – 33 cmAC: 31 – 33 cm
Chest circumference :Should be equal to or 2-3 cm Less than the HC
PEDIATRIC NURSING MLNGC,MD, RN152
Anthropometric Measurement

PEDIATRIC NURSING MLNGC,MD, RN153
• Length : mature female neonate - 53 cm (20.9 in) mature male - 54 cm (21.3in)
• Head circumference: mature newborn - 34-35 cm (13.5 to 14 in)
Measure with the tape measure drawn across the center of the forehead and around the most prominent portion of the posterior head.
• Chest circumference: term newborn – 2 cm less than head circumference, measured at the level of the nipples
PEDIATRIC NURSING MLNGC,MD, RN154
Immediate Assessment of the Newborn
General appearance
- Skin- Head- Eyes- Ears- Neck- Chest- Abdomen- Genitalia- Back- Extremities
PEDIATRIC NURSING MLNGC,MD, RN155
General Appearance
• Full term newborns have a flexed posture• The head is flexed• Arms are flexed on the chest• Legs are flexed on the abdomen
PEDIATRIC NURSING MLNGC,MD, RN156
Skin
• Plethora ( deep, rosy red color) more common in infants with polycythemia vera but can be seen in an overoxygenated or overheated infant.
• Vernix caseosa – a white creamy substance may thinly cover the skin.
• Lanugo – fine downy hair , may still be seen on the forehead and shoulders or it may all disappear.
PEDIATRIC NURSING MLNGC,MD, RN157
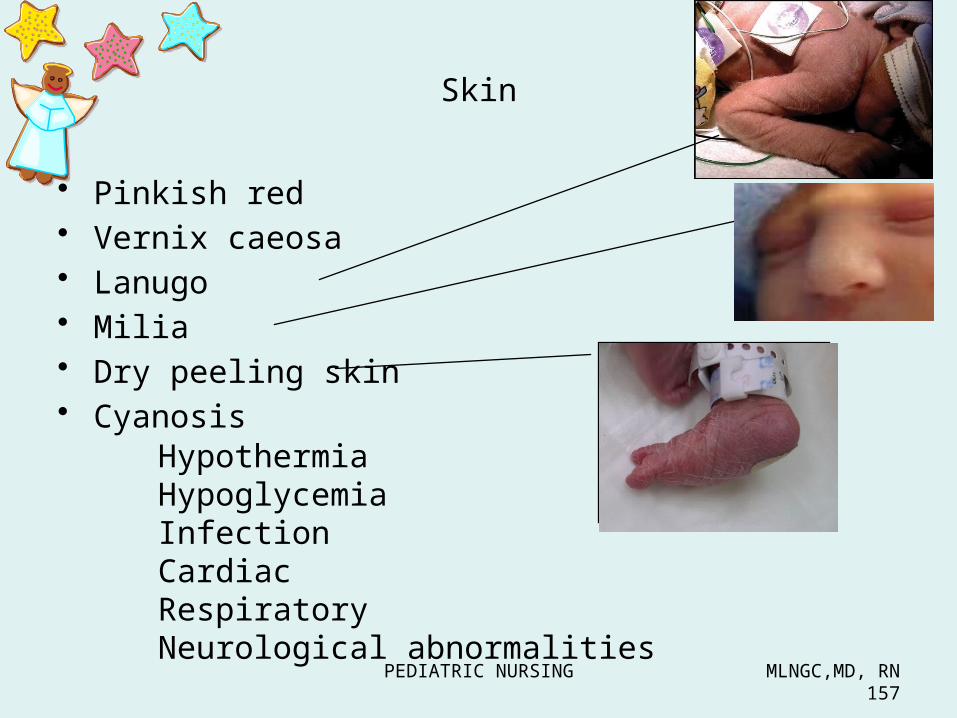
Skin
• Pinkish red• Vernix caeosa• Lanugo• Milia• Dry peeling skin• Cyanosis
HypothermiaHypoglycemiaInfectionCardiacRespiratoryNeurological abnormalities

PEDIATRIC NURSING MLNGC,MD, RN158
SKIN Cyanosisa. central ( bluish skin, including the tongue and lips- associated with low oxygen saturation in the
blood and it may be associated with congenital Heart disease ( CHD)
b. Peripheral cyanosis – bluish skin with pink lips and tongue
c. Acrocyanosis - bluish hands and feet only - may be normal for an infant who has just been
born.

PEDIATRIC NURSING MLNGC,MD, RN159
2. Skin
Dark red – prematurityAcrocyanosis – up to 48 hoursCentral cyanosis – indicates decreased O2Generalized mottling Gray color - infection Pale color - anemiaYellow color –jaundiceHarlequin sign – pale and pink

PEDIATRIC NURSING MLNGC,MD, RN160
Pallor
* Excessive blood loss when cord is cut
* Untimely cutting of the cord
* Inadequate iron stores because of poor maternal nutrition
* Blood incompatibility
PEDIATRIC NURSING MLNGC,MD, RN161
MILIA• Newborn sebaceous glands are
immature. At least one pin-point white papule (a plugged or unopened sebaceous gland) can be found in the cheek or across the bridge of the nose of every newborn.
• Disappears by 2-4 wks of age as the sebaceous glands mature and drain.
• Parents should be instructed to avoid scratching or squeezing the papules to prevent secondary infection.

PEDIATRIC NURSING MLNGC,MD, RN162
Milia
Benign cystsDisappear Within few weeksAfter birth

PEDIATRIC NURSING MLNGC,MD, RN163
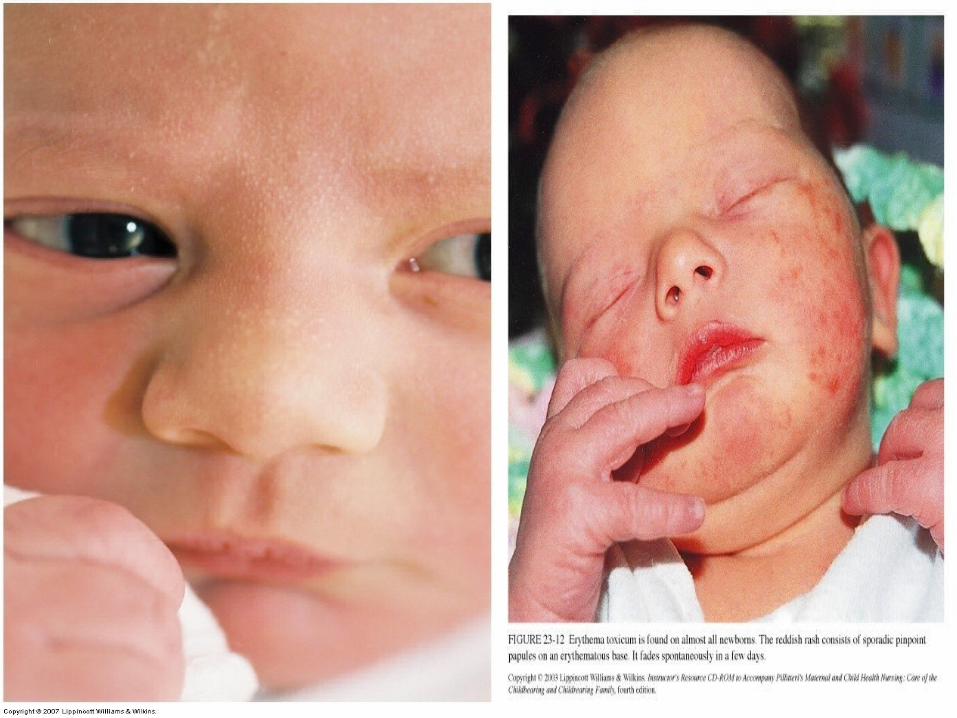
ERYTHEMA TOXICUM
• in most normal mature infants - newborn rash• usually appears on the 1st to 4th days of life, but
may appear up to 2 wks of age• Also called Flea bite rash• One of the chief characteristics of the rash is the
lack of pattern.

PEDIATRIC NURSING MLNGC,MD, RN164
Lesions are most noticeable 48HAfter birth but may appear as late as
7-10 daysBENIGN RASH resolves spontaneously
PEDIATRIC NURSING MLNGC,MD, RN165

PEDIATRIC NURSING MLNGC,MD, RN166
Mottling lacy pattern May be seen in the
healthyinfant or infant with 1. Cold stress2. Hypovolemia3. Sepsis
Persistent mottling-referred to as cutis marmorata

PEDIATRIC NURSING MLNGC,MD, RN167
Candida albican rashAppears as erythematous plaquewith sharply demarcated edgesskin folds are involved
Treatment :
Nystatin ointment or cream Applied to the rash 4x daily for 7-10 days

PEDIATRIC NURSING MLNGC,MD, RN168
Acne Neonatorum
• Lesion typically seen over the check, chin and forehead
• Benign and requires no therapy• Severe cases may require treatment with mild
keratolytic agent such as 3% sulfur salicylic acid

PEDIATRIC NURSING MLNGC,MD, RN169
ACNE
PEDIATRIC NURSING MLNGC,MD, RN170
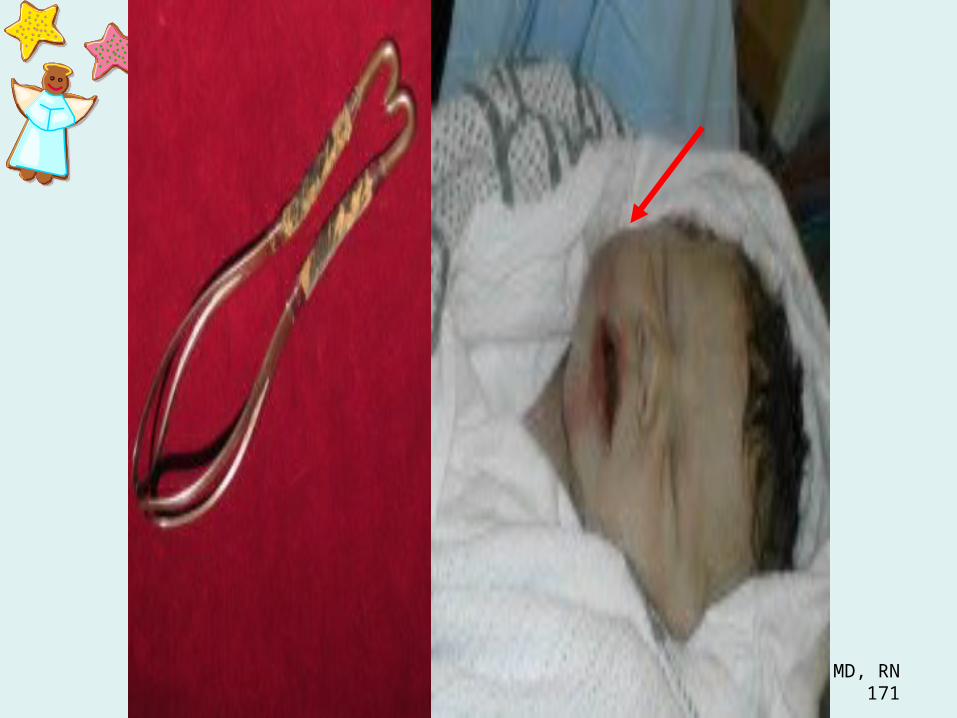
FORCEPS MARK
• There may be a circular or linear contusion matching the rim of the blade of the forcep on the infant’s cheek.
• The mark disappears in 1-2 days along with the edema that accompanies it.
PEDIATRIC NURSING MLNGC,MD, RN171

PEDIATRIC NURSING MLNGC,MD, RN172
Jaundice Types: 1. Physiologic Jaundice / Icterus Neonatorum 2nd day– 7th day – TERM (12mg/dl- indirect bilirubin) 2nd day – 10th day - PRE-TERM 2. Pathologic Jaundice- before the first 24 hours of life
– Causes: Infection Hemolytic disorders Inability of the newborn to conjugate bilirubin
Decreased conversion of bilirubin to urobilirubin
Decreased uptake of free bilirubin by hepatic cells

PEDIATRIC NURSING MLNGC,MD, RN173
Normal total serum bilirubin = 15%
Direct bilirubin = 1.7 Indirect bilirubin = 13.2
Breastfed babies have longer physiologic jaundice because human milk has PREGNANEDIOL depresses the action of glucoronyl transferase (enzyme responsible for converting indirect bilirubin to direct bilirubin)

PEDIATRIC NURSING MLNGC,MD, RN174
Breastmilk jaundice
Pregnanediol
Decrease glucoronyl transferase
Decrease conversion of indirect to direct bilirubin
jaundice

PEDIATRIC NURSING MLNGC,MD, RN175
Goal of treatment: to decrease the bilirubin levels
Management: Bililight (Phototherapy)
Nursing Care:1. Cover eyes with an opaque
mask to prevent blindness.2. Maintain a distance of about 18-
20 inches from source of light.3. Monitor V/S especially temp.4. Cover the genitalia to prevent
PRIAPISM (continuous erection).5. Turning the baby q2hours.6. Hydration.

PEDIATRIC NURSING MLNGC,MD, RN176
KERNICTERUS
Accumulation of bilirubin in the brain tissues• SEIZURES• MENTAL RETARDATION• EXCHANGE TRANSFUSION

PEDIATRIC NURSING MLNGC,MD, RN177

PEDIATRIC NURSING MLNGC,MD, RN178

NURSE ALERT!!!
Most accurate method of assessing the presence of jaundice: Use natural light and blanch skin on the chest or
tip of the nose.
PEDIATRIC NURSING MLNGC,MD, RN181
Skin
• Acrocyanosis- hand and feet ; peripheral circulation is sluggish within 24H
• Harlequin sign– Deep pink or red color develop over one side
while the other side remains PALE or normal color
– Indicative of shunting of blood with cardiac problem or sepsis
• Birthmarks

PEDIATRIC NURSING MLNGC,MD, RN182
Birth marks• Telangiectatic Nevi ( stork bites) – disappear at
2yrs – pale pink or red, flat , dilated capillaries
• Nevus Flammeus ( port- wine stain)– No fading with time – Require surgery in the future– Common on face– Non-elevated, sharply demarcated red to
purple dense area of capillaries• Nevus Vasculosus ( strawberry mark)
– Disappear at 7-9 yrs old– Common in head– Dark red
• Mongolian Spot – fades at 1-2 years old – Bluish black pigmentation– Lumbar dorsal area or buttocks

PEDIATRIC NURSING MLNGC,MD, RN183
Common Marks
1. Harlequin Sign - BECAUSE OF IMMATURITY OF CIRCULATION, AN INFANT WHO HAS BEEN LYING ON HIS SIDE WILL APPEAR RED ON THE DEPENDENT SIDE & PALE ON THE UPPER SIDE.
2. Mongolian spots – bluish gray or dark nonelevated pigmentation area over the lower back and buttocks present at birth; primarily nonwhite, disappears at SCHOOL AGE

PEDIATRIC NURSING MLNGC,MD, RN184
3. Milia – unopened sebaceous glands; tip of nose and chin of the baby.
• Newborn sebaceous gland is immature. At least one pin-point white papule (a plugged or unopened sebaceous gland) can be found in the cheek or across the bridge of the nose of every newborn.
• Disappears by 2-4 wks of age as the sebaceous glands mature and drain.
• Parents should be instructed to avoid scratching or squeezing the papules to prevent secondary infection.
4. Lanugo - fine downy, hair that covers a newborn’s shoulder, back and upper arms
• Found also in the forehead and ears.• The newborn of 37-39 wks has more lanugo than
the 40th wks old infant.• Post-mature infants have rarely have lanugo• By age of 2 wks, it disappears

PEDIATRIC NURSING MLNGC,MD, RN185
Common Marks
5. Desquamation- peeling; at birth, postmaturity• Within 24 hrs. of birth, the skin of most newborns
has become extremely dry• The dryness is particularly evident on the palms
of the hands and soles of the feet.• this is normal and needs no treatment.
6. Vernix Caseosa• White, cream-cheese-like substance that serves
as a skin lubricant, usually noticeable on a newborn skin, prominently seen in the skin folds, at birth in a term neonate.

PEDIATRIC NURSING MLNGC,MD, RN186
7. Portwine Stain or Nevus Flammeus – birth; red to purple color, usually flat discoloration commonly on the face or neck; does not grow and does not fade; does not blanch on pressure nor disappear
8. Strawberry Mark or Nevus Vascularis – 2nd most common type of capillary hemangioma. elevated, sharply demarcated or bright or dark red, rough surface swelling. (+) school age or even longer.
PEDIATRIC NURSING MLNGC,MD, RN187
9. Erythema Toxicum or Erythema Neonatorum – Newborn rash or fleabite rash/ dermatitis; transient; papules with vesicles at nape, back and buttocks.
• It usually appears in the 1st to 4th day (2nd day) of life, but may appear up to 2 wks of age
• One of the chief characteristic of the rash is the lack of pattern; disappears without treatment.
10. Nevi – stork bites or Telangiectasia Nevi; pink or red flat areas of capillary dilatation at upper eyelids, nose, upper lip, lower occiput bone, nape and neck. can be blanched by the pressure of the finger; usually fade during infancy- 1st and 2nd year.
PEDIATRIC NURSING MLNGC,MD, RN188
11. Cutis Marmorata – transitory mottling when exposed to cold
12. FORCEPS MARK• There may be a circular or linear contusion
matching the rim of the blade of the forcep on the infants cheek.
• The mark disappears in 1-2 days along with the edema that accompanies it.

PEDIATRIC NURSING MLNGC,MD, RN189
Nevus flammeus/Portwine Stain

PEDIATRIC NURSING MLNGC,MD, RN190
Stork’s beak mark

PEDIATRIC NURSING MLNGC,MD, RN191
Strawberry Hemangioma

PEDIATRIC NURSING MLNGC,MD, RN192
Cavernous Hemangioma

PEDIATRIC NURSING MLNGC,MD, RN193
Mongolian Spot
PEDIATRIC NURSING MLNGC,MD, RN194
Milia

PEDIATRIC NURSING MLNGC,MD, RN195
Erythema toxicum
PEDIATRIC NURSING MLNGC,MD, RN196
Head
- largest part of the human body (1/4 of his total body length)
- forehead is large and prominent- chin is receding when startled or crying

PEDIATRIC NURSING MLNGC,MD, RN197
Head • 25% of the body length ( cephalocaudal development).
Larger Part• Sutures are palpable • Fontanels are unossified membranous tissue at the junction
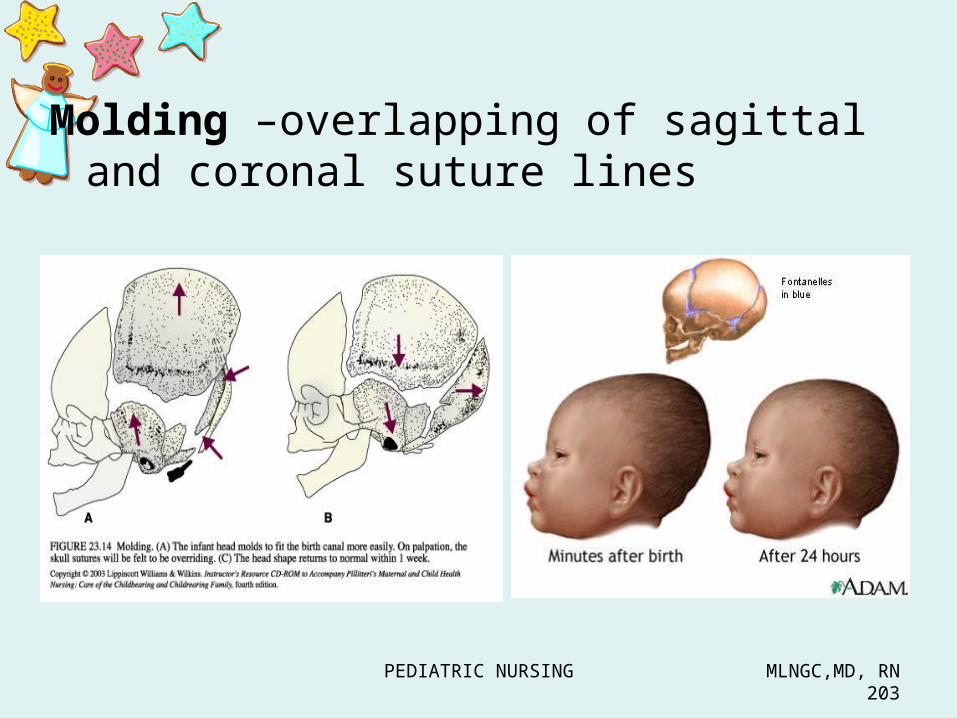
of the sutures• Molding is asymmetry of the head resulting from the
pressure in the birth canal, overlapping of sagittal and coronal suture line
Assessment of The Newborn
SUTURES:Lambdoid (2) Coronal (2) Frontal (1) Sagittal (1)

PEDIATRIC NURSING MLNGC,MD, RN198
Fontanels1. Anterior – diamond shape
- closes at 12-18 months - 3-4 cm long/2-3 cm wide - junction of 2 parietal bones and 2 fused
frontal bones- not indented/not depressed- suture lines - never appear widely separated
2. Posterior – triangular in shape- junction of the parietal bones and the occipital bones. - 1 cm wide- closes at 2-3 months of age

PEDIATRIC NURSING MLNGC,MD, RN199
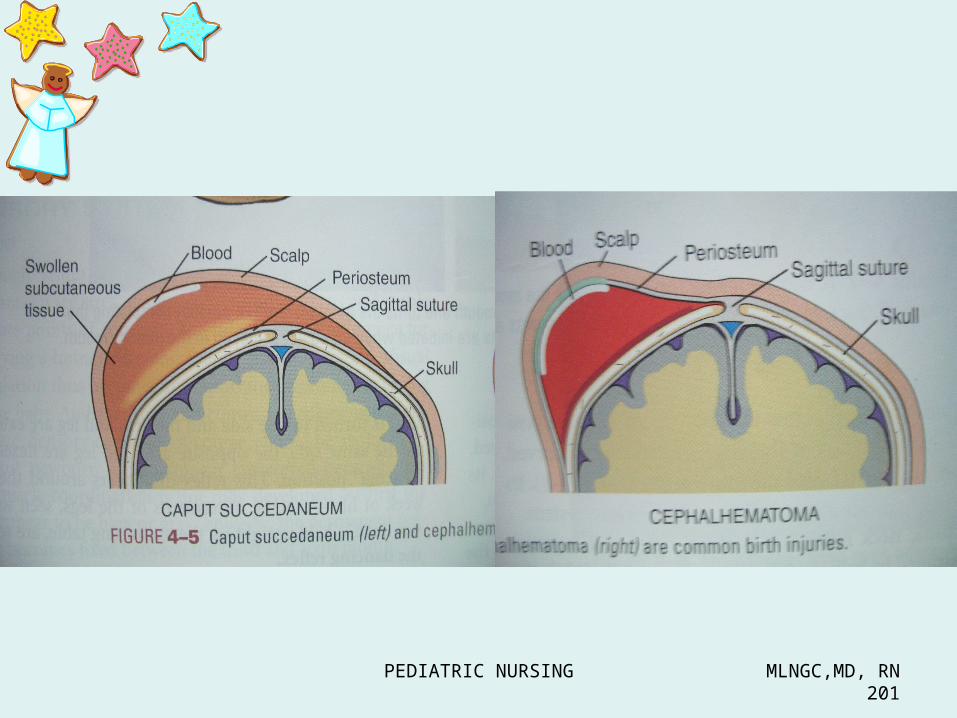
Masses from birth trauma• Caput succedaneum – edema of
the soft tissue over bone ( crosses over suture line)– No treatment; subsides in few
days• Cephalhematoma – swelling
caused by bleeding into an area between the bone and its periosteum ( does not cross over suture line )– Absorbed within 6 weeks – No treatment
PEDIATRIC NURSING MLNGC,MD, RN200
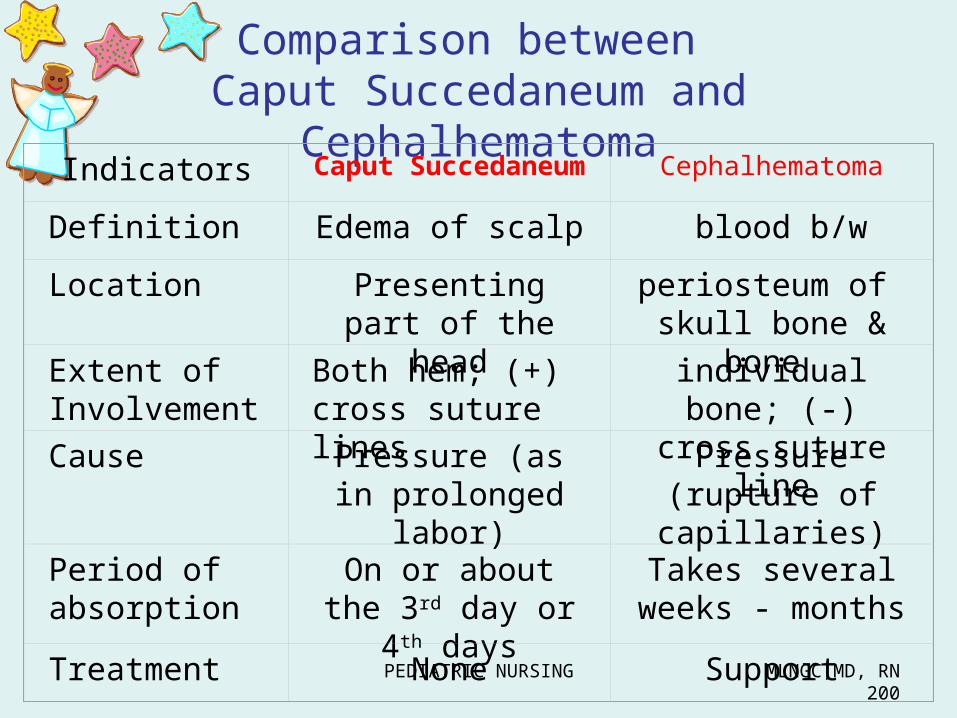
Comparison between Caput Succedaneum and
CephalhematomaIndicators Caput Succedaneum
Cephalhematoma
Definition Edema of scalp blood b/wLocation Presenting part
of the headperiosteum of skull bone &
bone Extent of Involvement
Both hem; (+) cross suture lines
individual bone; (-) cross suture
lineCause Pressure (as in prolonged labor)
Pressure (rupture of capillaries)
Period of absorption
On or about the 3rd day or 4th
days
Takes several weeks - months
Treatment None Support
PEDIATRIC NURSING MLNGC,MD, RN201

PEDIATRIC NURSING MLNGC,MD, RN202
CRANIOSYNOSTOSIS - suture lines separated or fontanels prematurely closed; leads to mental retardation.
Craniotabes – localized softening of cranial bones - indented by pressure of a finger – Corrects w/o treatment in weeks or
months.– Common to firstborn because of early
lightening
Hydrocephalus – anterior fontanel open after 18 months
Microcephaly – small growing brain
Anencephaly – absence of cerebral hemisphereFRAGILE
PEDIATRIC NURSING MLNGC,MD, RN203
Molding –overlapping of sagittal and coronal suture lines

PEDIATRIC NURSING MLNGC,MD, RN204
• Seborrheic dermatitis – “ Cradle cap”– Scaling greasy-appearing salmon colored
patches, seen on the scalp behind ears and umbilicus
– CAUSE :• Improper hygiene
– Mgt:• Proper hygiene• Oil before shampoo

PEDIATRIC NURSING MLNGC,MD, RN205
Signs of ALARM
• fused sutures• bulging or depressed fontanels when quiet• widened sutures and fontanels• craniotabes
PEDIATRIC NURSING MLNGC,MD, RN206
Eyes • Symmetrical and clear• Pupil equal, round , react to light by
accommodation• Blink reflex present• Strabismus common – weak EOM• Ability to track and fixate momentarily• Red reflex present • Eyelid often edematous• Absence of tears• Corneal reflex (+)• Visual acuity = 20/200; 20/800
PEDIATRIC NURSING MLNGC,MD, RN207
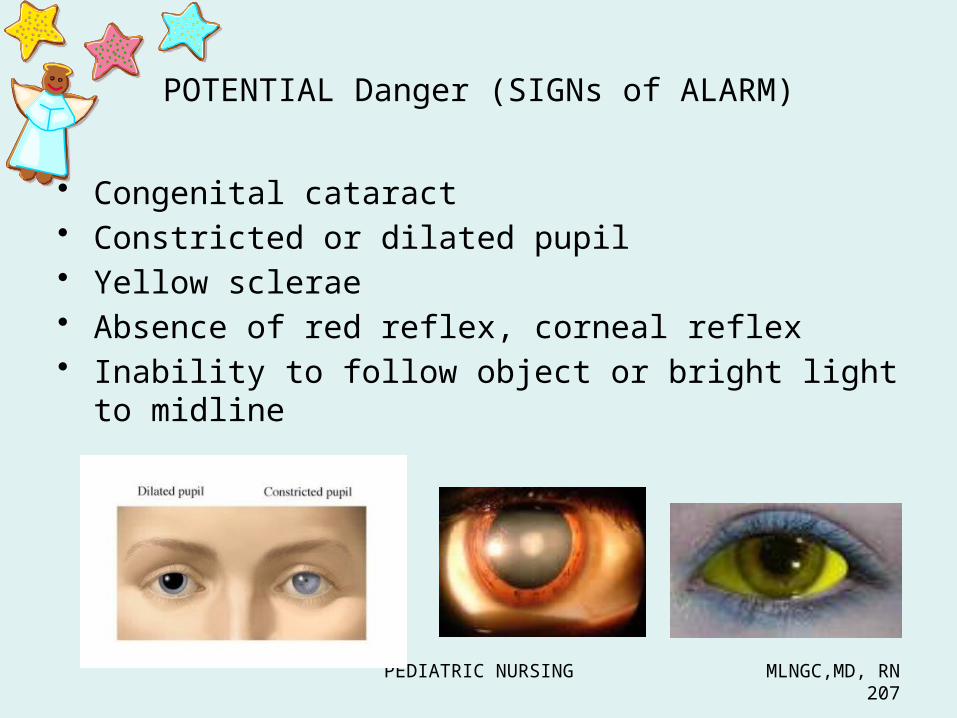
POTENTIAL Danger (SIGNs of ALARM)
• Congenital cataract• Constricted or dilated pupil• Yellow sclerae• Absence of red reflex, corneal reflex• Inability to follow object or bright light to midline
PEDIATRIC NURSING MLNGC,MD, RN208
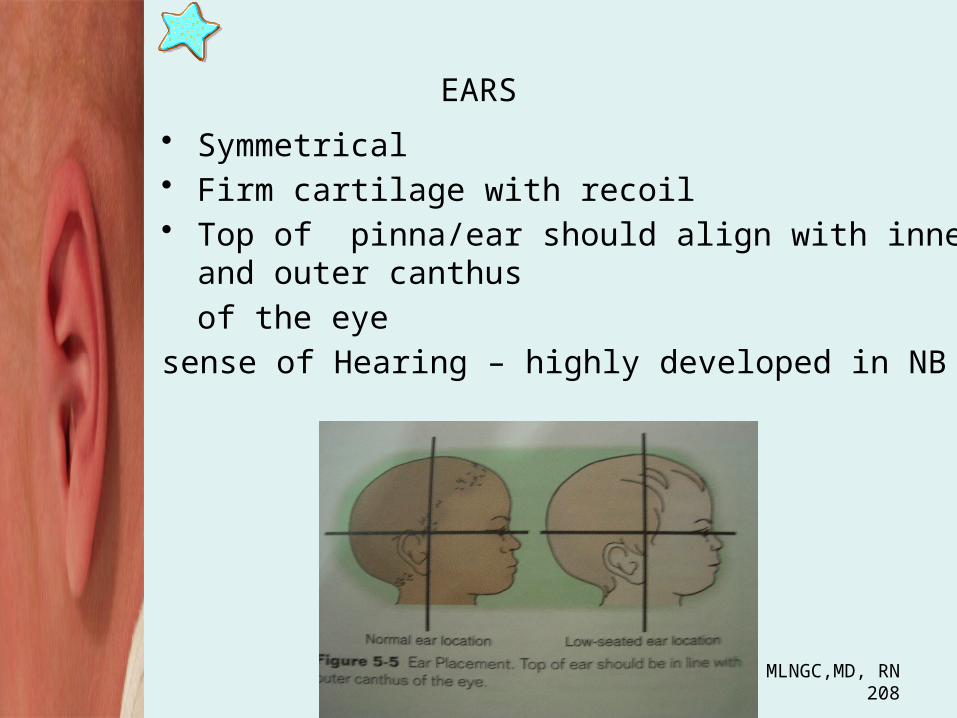
EARS• Symmetrical• Firm cartilage with recoil• Top of pinna/ear should align with inner and
outer canthus of the eye
sense of Hearing – highly developed in NB

PEDIATRIC NURSING MLNGC,MD, RN209
Potential Danger: ALARM
• Low set ears & minor abnormalities (chromosomal defect & kidney anomalies)
• Absence of startle reflex in response to loud noise

PEDIATRIC NURSING MLNGC,MD, RN210
Nose
• Nasal obligates• Note for marked flaring of alae nasi.
– indicative of airway obstruction
Causes of obstruction:1. secretions2. septal deviation
• Sense of smell – least developed
PEDIATRIC NURSING MLNGC,MD, RN211
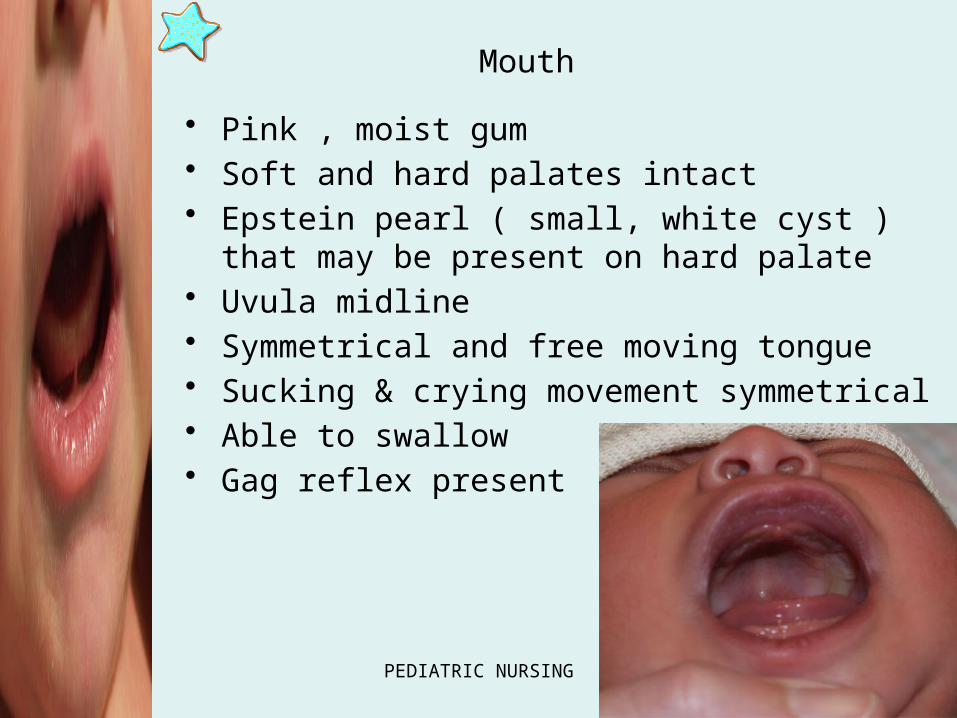
Mouth• Pink , moist gum• Soft and hard palates intact• Epstein pearl ( small, white cyst ) that may
be present on hard palate • Uvula midline • Symmetrical and free moving tongue• Sucking & crying movement symmetrical• Able to swallow• Gag reflex present

PEDIATRIC NURSING MLNGC,MD, RN212
• Common– Natal teeth
• Potential Danger:– Cleft lip– Cleft palate– Large protruding tongue– Profuse salivation or drooling– Candidiasis ( thrush)
PEDIATRIC NURSING MLNGC,MD, RN213
NECK
• Thyroid gland not palpable
• Soft, palpable and creased with skin folds
• Head - rotates freely on the neck and flexes forward and back
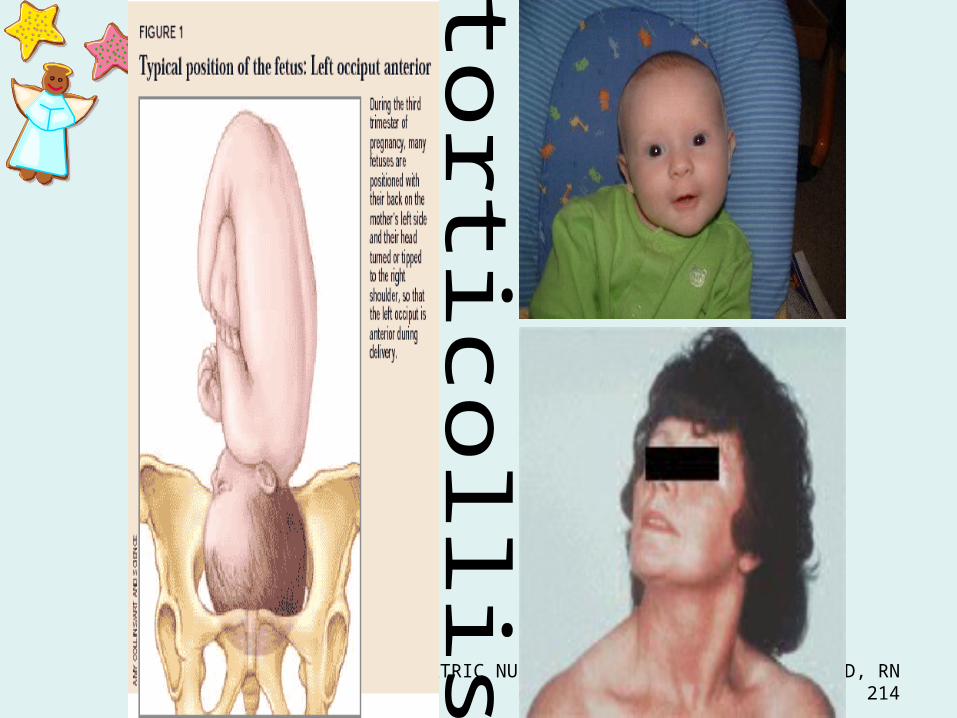
• (+) rigidity of the neck- CONGENITAL TORTICOLLIS (injury to SCM sternocleidomastoid)
• NB whose membranes ruptured 24 hours before birth-nuchal rigidity meningitis
PEDIATRIC NURSING MLNGC,MD, RN214

PEDIATRIC NURSING MLNGC,MD, RN215
CYSTIC HYGROMA
BLOCKAGE OF LYMPHATIC SYSTEM

PEDIATRIC NURSING MLNGC,MD, RN216
CHEST
• Circular appearance – AP and Lateral diameter are about EQUAL.
• Diaphragmatic respiration• Bronchial sounds heard on auscultation• Nipples prominent & edematous• Milky secretion common ( witch milk)• Breast tissue present• Clavicles need to be palpated to assess for
fracture• Symmetrically expands (retraction indicates
respiratory distress)
- Breasts may be engorged (due to maternal hormones) There could be passage of thin, transparent watery fluid known as WITCH’S MILK.
PEDIATRIC NURSING MLNGC,MD, RN217
• Commonly seen :– Pectus excavatum ( funnel shaped)– Pectus carinatum ( Pigeon chest)– Supernumerary nipples
• SIGN of Potential Danger– Depressed sternum– Marked retraction of chest and ICS ( during
respiration)– Redness & firmness around nipple– Wide spaced nipple
PEDIATRIC NURSING MLNGC,MD, RN218
LUNGS
• Abdominal respiration• Cough reflex is absent at birth
– (+) by 1-2 days– Bilateral equal bronchial breath sound
• RESPIRATION: Irregular rate & depth • (+) crackles - after birth

PEDIATRIC NURSING MLNGC,MD, RN219
POTENTIAL DANGER
• Inspiratory stridor• Expiratory grunt and retraction• Persistent irregular breathing• Periodic breathing with repeated apneic spells• Seesaw respiration ( paradoxical)• Unequal and diminished breath sound• Persistent fine crackles• Peristaltic bowel sounds on one side with
diminished breath sounds on the same side

PEDIATRIC NURSING MLNGC,MD, RN220
HEART
• Located : Apex 4th-5th ICS, lateral to left sternal border
• Heart rate increases with inspiration and decreases with expiration
• Transient cyanosis when crying or straining

PEDIATRIC NURSING MLNGC,MD, RN221
POTENTIAL DANGER
• DEXTROCARDIA – heart at right side• Cardiomegaly• Displacement of apex, muffled• (+) murmur or thrills• Persistent cyanosis• Hyperactive precordium

PEDIATRIC NURSING MLNGC,MD, RN222
Abdomen• Umbilical cord
– Monitor cord for meconium staining– Assess for umbilical hernia– Note for abdominal depression– Assess for abdominal distention– Monitor bowel sounds – audible 1-2H after birth
• Liver palpable 2-3 cm below right costal margin• Spleen: tip palpable at the end of first week of age• Kidney : palpable 1-2 cm above umbilicus• Umbilical cord : bluish white at birth, 2 arteries and 1
vein• Femoral pulses : equal and bilateral

PEDIATRIC NURSING MLNGC,MD, RN223
omphalocele
Gastrochisis

PEDIATRIC NURSING MLNGC,MD, RN224
GI SYSTEM• Newborn’s stomach holds about 60-90 ml• Has limited ability to digest fat and starch
because the pancreatic enzymes, lipase and amylase, are deficient for the 1st few months of life
• Because milk, the infant’s main diet for the 1st year is low in Vit. K, intestinal synthesis is necessary for blood coagulation

PEDIATRIC NURSING MLNGC,MD, RN225
Abdomen
• Umbilical cord
• ANUS– Ensure anal opening is patent– First stool meconium should pass within first 24H
PEDIATRIC NURSING MLNGC,MD, RN226
Potential Danger
• Abdominal distention• Distended veins• Absent bowel sound• Enlarged spleen and liver• Ascites• Visible peristaltic waves• Scaphoid or concave abdomen• Green umbilical cord• Presence of only 1 artery in cord

PEDIATRIC NURSING MLNGC,MD, RN227
Genitals• Female :
– Labia edematous , clitoris enlarged– Pseudomenstruation (+)– First voiding occurs within 24H
• Male– Prepuce covers glans skin– Scrotum is edematous– Verify meatus at tip of penis– Testes descended, retracts at cold
tempearture– Assess for hernia or hydrocoele– First voiding occurs w/in 24H

PEDIATRIC NURSING MLNGC,MD, RN228
Male Genitalia
– Scrotum may be edematous due to maternal hormones.
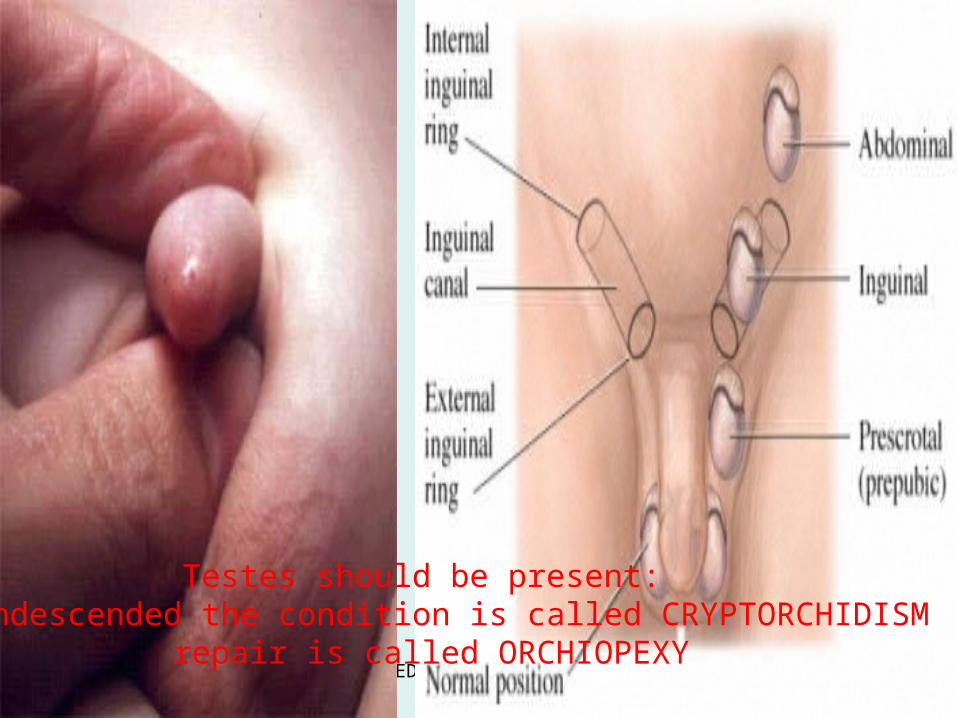
- Testes should be present; if undescended - CRYPTORCHIDISM
PEDIATRIC NURSING MLNGC,MD, RN229
Conditions for Cryptorchidism
1. Agenesis – absence of an organ2. Ectopic testes – Testes cannot enter the scrotum because opening of the scrotal sac is closed.3. Vas deferens or artery is too short to allow the testes to descend.
PEDIATRIC NURSING MLNGC,MD, RN230
– Care of the penis• Uncircumcised –
– do not force retraction of foreskin (complete separation of foreskin and glans penis takes 3-5 y)
– parents should be told to gently test for retraction occasionally during bath
– and when it has occurred, gently clean glans with soap and water
PEDIATRIC NURSING MLNGC,MD, RN231
Circumcision – prior to discharge from nursery, preferably end of 1st week
Procedure:1. Vitamin K injected IM2. Infant is restrained; penis is cleansed with soap and water
3. clamp is used4. Petroleum gauze dressing is applied to prevent adherence of circumcised site to the diaper while applying pressure to prevent bleeding

PEDIATRIC NURSING MLNGC,MD, RN232
PEDIATRIC NURSING MLNGC,MD, RN233
Nursing Care
- Check hourly for bleeding.- Do not attempt to remove exudates which persist for 2-3 days; just wash with warm water. - Diaper must be pinned loosely during the 1st 2-3 days when the base of the penis is tender.
PEDIATRIC NURSING MLNGC,MD, RN234
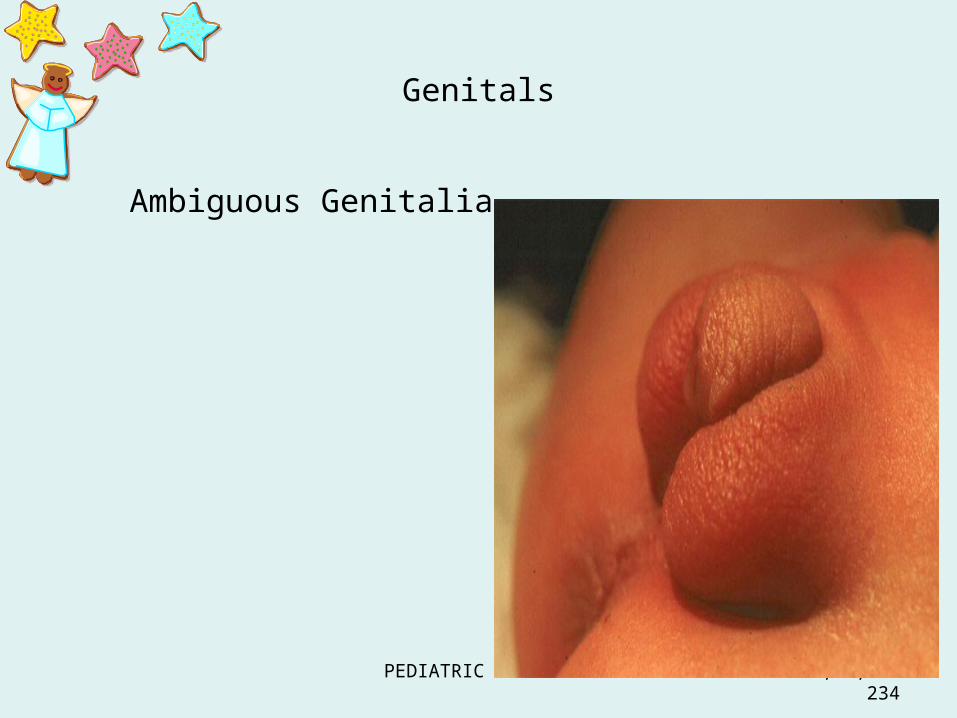
Genitals
Ambiguous Genitalia

PEDIATRIC NURSING MLNGC,MD, RN235
URINARY SYSTEM
• The average newborn voids within 24 hrs after birth– Newborns who do not void within this time
should be examined for the possibility of ureteral stenosis or absent kidneys or ureter
• A single voiding in a newborn is only about 15 ml• The daily urinary output for the 1st 1-2 days is
about 30-60 ml total.• The 1st voiding may be pink or dusky because of
uric acid crystals that were formed in the bladder in utero
PEDIATRIC NURSING MLNGC,MD, RN236
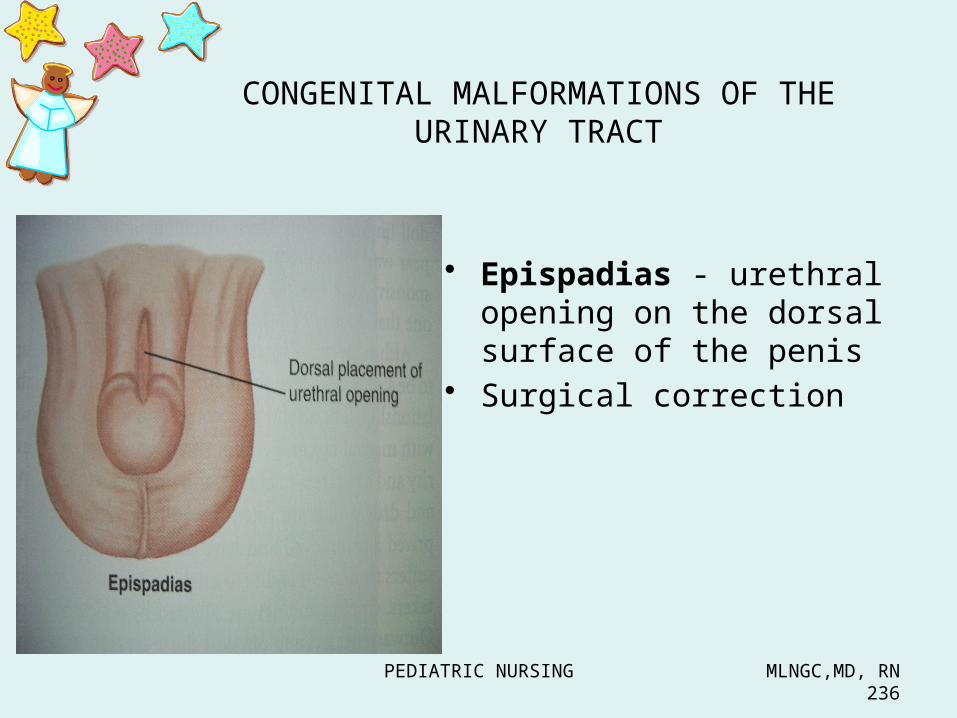
CONGENITAL MALFORMATIONS OF THE URINARY TRACT
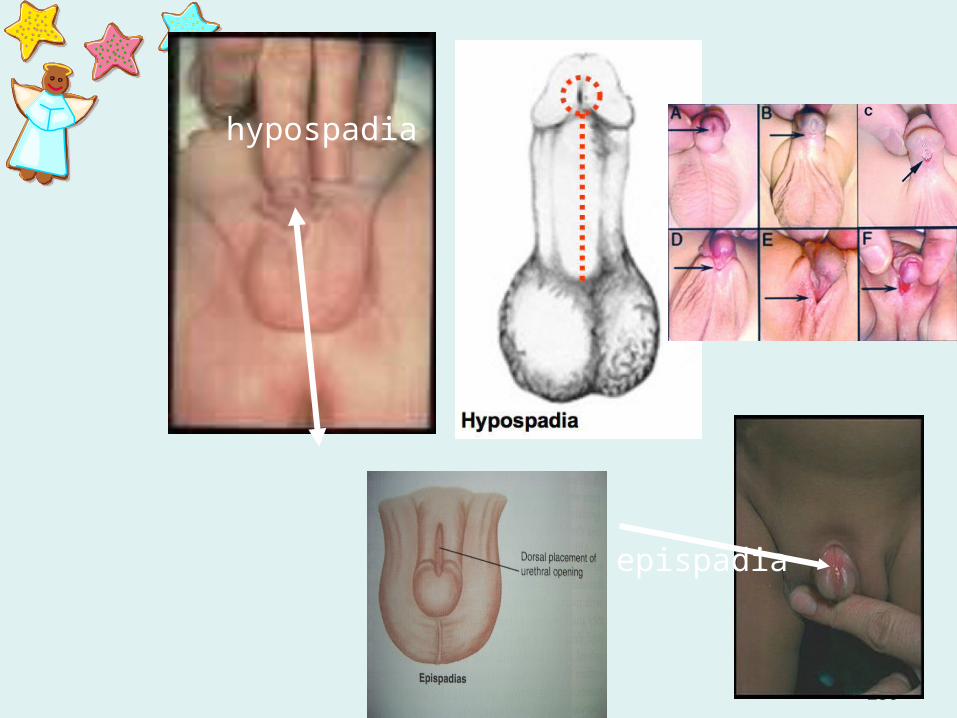
• Epispadias - urethral opening on the dorsal surface of the penis
• Surgical correction

PEDIATRIC NURSING MLNGC,MD, RN237
• HYPOSPADIA• Male urethral opening
on the ventral surface of penis, or female urethral opening in vagina
• Surgical reconstruction

PEDIATRIC NURSING MLNGC,MD, RN238
HYPOSPADIA
PEDIATRIC NURSING MLNGC,MD, RN239
hypospadia
epispadia
PEDIATRIC NURSING MLNGC,MD, RN240
Testes should be present: if undescended the condition is called CRYPTORCHIDISM
repair is called ORCHIOPEXY

PEDIATRIC NURSING MLNGC,MD, RN241
HYDROCOELE INGUINAL HERNIA

PEDIATRIC NURSING MLNGC,MD, RN242
SPINE
• Straight• Posture flexed• Supportive of head momentarily when prone• Arms and legs flexed• Chin flexed on upper chest• Well-coordinated, sporadic movement• Hypotonic or hypertonic indicates CNS
damage
PEDIATRIC NURSING MLNGC,MD, RN243
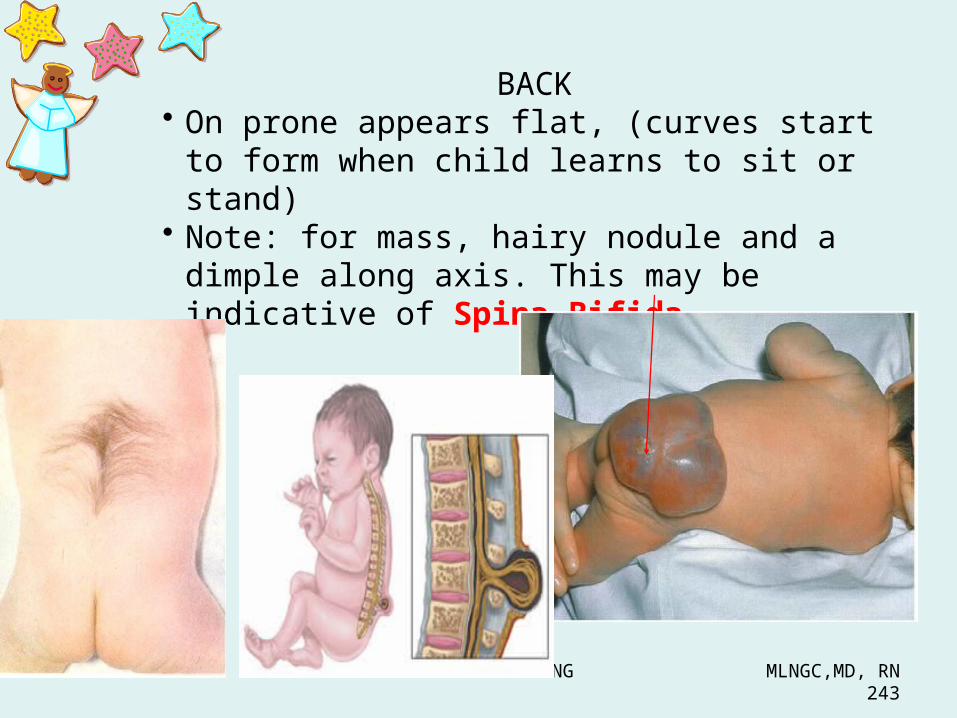
BACK• On prone appears flat, (curves start to form
when child learns to sit or stand)• Note: for mass, hairy nodule and a dimple
along axis. This may be indicative of Spina Bifida.

PEDIATRIC NURSING MLNGC,MD, RN244
Extremities
• Flexed• Symmetrical movement• Fists clenched• Ten finger , 10 toes• Legs - bowed• Creases on soles of feet• Pulses palpable• Slight tremor common but could be sign of
hypoglycemia• Assess for hip dysplasia- no click should be heard
PEDIATRIC NURSING MLNGC,MD, RN245
Supernumerary = polydactyly; Fused or webbed = syndactyly
Simean line - Asymmetrical movement of upper and lower
extremities - ERB – DUCHENE PARALYSIS - Observe for clubfoot deformities

PEDIATRIC NURSING MLNGC,MD, RN246
SYNDACTYLY
POLYDACTYLY
POLYDACTYLY & SYNDACTYLY

PEDIATRIC NURSING MLNGC,MD, RN247
Simian crease

PEDIATRIC NURSING MLNGC,MD, RN248
Congenital hip dysplasia/dislocation
• 0.1% of infants• with a predilection for females to males of 5:1• infants with a family history (first-degree relative
affected) of CHD, the incidence is 10 times higher• also higher in infants born in the breech position
and infants with certain other congenital abnormalities, including torticollis, clubfoot, metatarsus adductus, and hyperextension of the knee

PEDIATRIC NURSING MLNGC,MD, RN249
PEDIATRIC NURSING MLNGC,MD, RN250
A. Ortolani’s test
• In this maneuver, the infant is examined in the supine position.
• Place the infant in frog-leg position. Abduct the hip by using the middle finger to apply gentle INWARD and UPWARD pressure over the greater trochanter.
• In the infant with an unstable hip, the examiner will feel a sudden shifting sensation and may hear or feel a "clIck" simultaneously as the hip reduces anteriorly.

PEDIATRIC NURSING MLNGC,MD, RN251
Ortolani’s test
PEDIATRIC NURSING MLNGC,MD, RN252
B. Barlow’s test
• In this maneuver, the infant is examined in the supine position.
• The examiner holds the infant's pelvis with one hand to stabilize it during manipulation.
• Adduct the hip by using the thumb to apply OUTWARD and BACKWARD pressure over the inner thigh
• In the infant with an unstable hip, a similar "click" may be felt as the hip subluxes posteriorly.

PEDIATRIC NURSING MLNGC,MD, RN253
Barlow test
PEDIATRIC NURSING MLNGC,MD, RN254
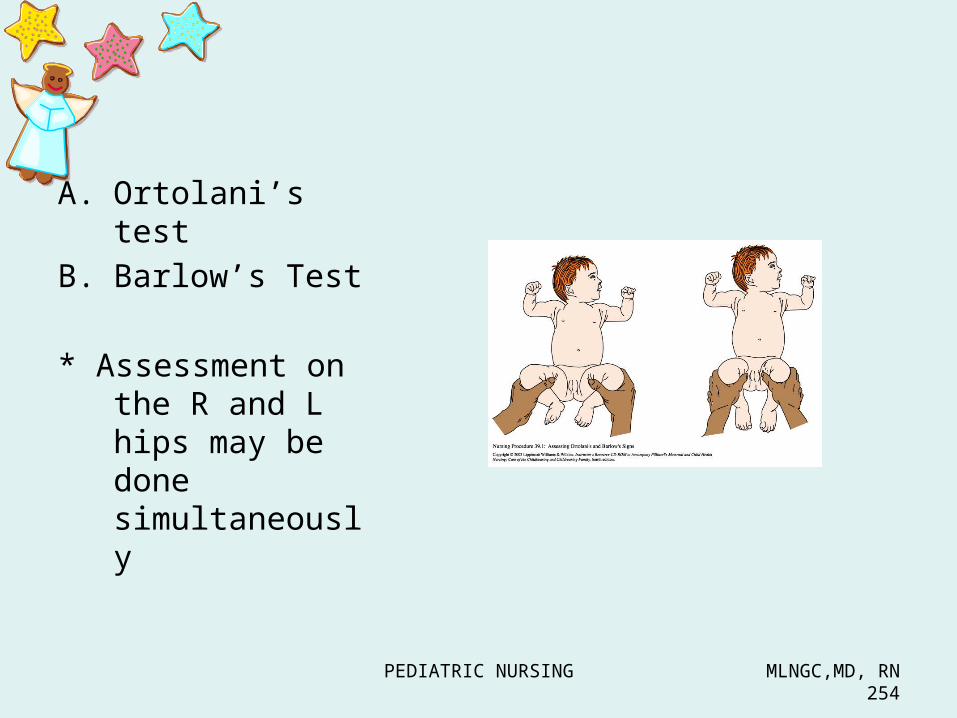
A. Ortolani’s testB. Barlow’s Test
* Assessment on the R and L hips may be done simultaneously

PEDIATRIC NURSING MLNGC,MD, RN255
Clubfoot
• A birth deformity in which the front portion of the foot is deformed and turned inward. It can be benefited greatly by surgery.

PEDIATRIC NURSING MLNGC,MD, RN256

PEDIATRIC NURSING MLNGC,MD, RN257
• IMMUNE SYSTEM– NB receives passive immunity via placenta (IgG)– NB receives passive immunity from colostrum
(IgA)– Infection – IgM– Use aseptic technique when handling NB– Observe standard precaution when handling NB– handwashing– Infection-free staff cares for the NB– Monitor NB temp.
• The newborn is prone to infection– Due to difficulty forming antibodies against
invading antigen until they are about 2 mos. of age.
– This inability to form antibodies early also is the reason that most immunization against childhood diseases are not given to infants younger than 2 mos.

PEDIATRIC NURSING MLNGC,MD, RN258
• METABOLIC SYSTEM/GI SYSTEM– NB can digest simple CHO, unable to digest FAT
because lack of lipase– CHON broken down only partially– NB small stomach capacity ( 60-90ml)– Rapid intestinal emptying time 2-3 H– Observe feeding reflexes– Observe for normal stool– Perform NB screening test

PEDIATRIC NURSING MLNGC,MD, RN259
• Blood Values– 80-110 ml/kg of body weight or about
300 ml– High WBC at birth about 15,000 to
30,000 cells/mm3
• Increased WBC count should not be taken as evidence of infection
• Blood Coagulation– Most newborns are born with a
prolonged coagulation or Prothrombin time, because their blood levels of Vitamin K are lower than normal.
– It takes 24 hrs. for flora to accumulate and vitamin K to be synthesized

NEUROMUSCULAR
PEDIATRIC NURSING MLNGC,MD, RN261
REFLEXES• B – blink reflex– Babinski
• S– Sucking– Swallowing– Startle/ moro reflex – Stepping or walking
• T– Tonic Neck or fencing
• L– Landau reflex
• E– Extrusion reflex
• P– Palmar- Plantar reflex– Placing reflex– Paracheute
• Rooting reflex
• TrunK Incurvation Reflex
BaSTa LEP RoT

PEDIATRIC NURSING MLNGC,MD, RN262
– Reflexes
• Blink Reflex - to protect the eye from any object coming near it by rapid eyelid closure

PEDIATRIC NURSING MLNGC,MD, RN263
• Babinski’s sign – stroking the sole of the foot from heel upward like an inverter “J” across ball of foot will cause all toes to fan (reverts to usual adult response by 12 mos)

PEDIATRIC NURSING MLNGC,MD, RN264
• Sucking Reflex- when newborn’s lips are touched, the baby makes a sucking motion. It diminishes at about 6 months of age.
• if it disappears immediately / if never stimulated - tracheoesophageal fistula
• Swallowing Reflex- food that reaches the posterior portion of the tongue is automatically swallowed

PEDIATRIC NURSING MLNGC,MD, RN265
• Moro or Startle Reflex – elicited by sudden disturbance in the infant’s immediate environment, body will stiffen, arms in tense extension followed by embrace gesture with thumb and index finger a “c” formation (disappears by 6 mos)
• can be stimulated by startling the newborn with loud noise or by jarring the bassinet, fades on 4th or 5th month of life
• aka Startle Reflex
If the reflex persists, it is a sign of brain damage, neurological impairment, or motor reflex difficulties.
PEDIATRIC NURSING MLNGC,MD, RN266
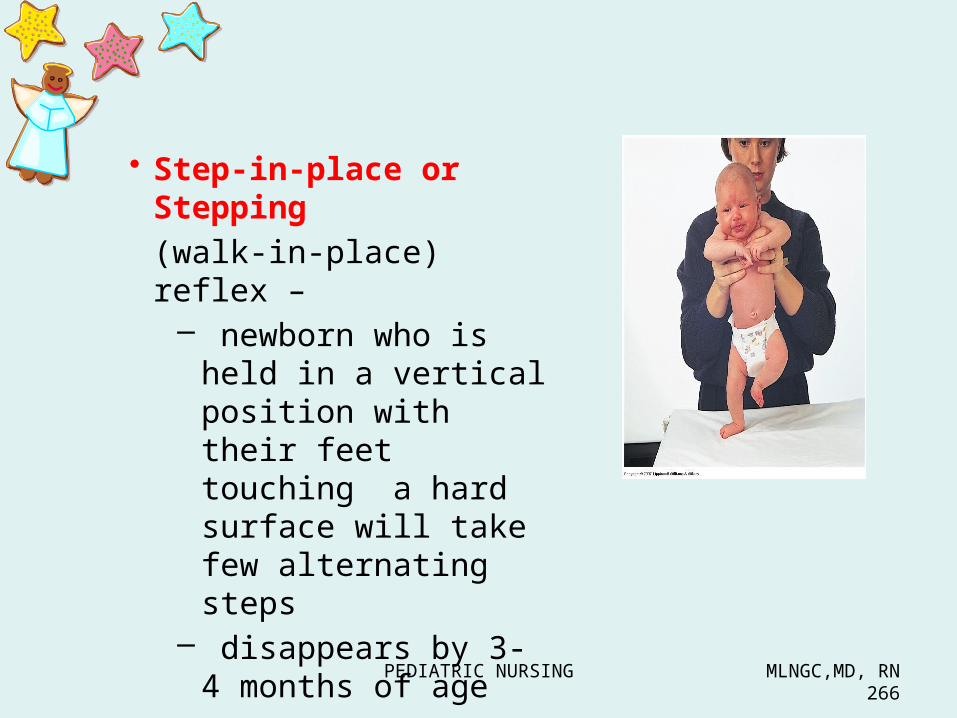
• Step-in-place or Stepping (walk-in-place) reflex –
– newborn who is held in a vertical position with their feet touching a hard surface will take few alternating steps
– disappears by 3- 4 months of age

PEDIATRIC NURSING MLNGC,MD, RN267
Tonic Neck (Fencing) Reflex
-If the Babies' head is rotated to the left,-The left arm (face side) stretches into extension -The right arm flexes up above head Opposite reaction if head is rotated rightward
if it persists after infancy, it may indicate abnormal development of the central nervous system.

PEDIATRIC NURSING MLNGC,MD, RN268
• Landau reflex-Displayed at about three months of age. When NB is placed on its stomach faced
down, NB will raise her head and arch its back.
This reflex will persist until 1 year old Absence of this reflex suggests problems in
motor development.

PEDIATRIC NURSING MLNGC,MD, RN269
EXTRUSION REFLEX-
• a newborn will extrude any substance that is placed in the anterior portion of the tongue.– Protective reflex prevents the swallowing of
inedible substance– Disappears at 6 wks to 3 mos.

PEDIATRIC NURSING MLNGC,MD, RN270
• Palmar grasp – pressure on palm elicits grasp (fades by 3-4 mos)

PEDIATRIC NURSING MLNGC,MD, RN271
• Placing Reflex- – similar to step-in-place Reflex, except it is
elicited by touching the anterior surface of a newborns leg against the edge of a bassinet or table
– A newborn will make a few quick lifting motions as if to step onto the table
it is obtainable in the normal infant up to the age of six weeks

PEDIATRIC NURSING MLNGC,MD, RN272

PEDIATRIC NURSING MLNGC,MD, RN273
• PARACHUTE
occurs in the slightly older infant, and is elicited by holding the child upright then rotating the body quickly face forward (as if falling). The arms are reflexively extended as if to break a fall.

PEDIATRIC NURSING MLNGC,MD, RN274
Rooting Reflex• Turns toward any object
touching/stroking cheek/mouth, opens mouth, and sucks rhythmically when finger/nipple is inserted into mouth (usually disappears by 6 wks.)

PEDIATRIC NURSING MLNGC,MD, RN275
TrunK Incurvation Reflex( Gallant reflex)
Trunk incurvation reflex - newborn lies on prone position and is touched along the paravertebral area by probing finger, NB
flexes its trunk and swings pelvis toward the touch

PEDIATRIC NURSING MLNGC,MD, RN276
• FEEDING REFLEXES1. Rooting2. Sucking3. Extrusion
• Protective REFLEXES1. Blinking2. Sneezing & coughing3. Yawning4. gagging

PEDIATRIC NURSING MLNGC,MD, RN277
Common Health Problems
1.Constipation 2.Loose stools 3.Colic 4.Spitting up5.Diaper rash/Skin irritation6.Miliaria (prickly heat/bungang araw)7.Seborrheic dermatitis/cradle cap 8.Occasional “crossed eyes”
Sleep pattern – babies sleep 16-20 hours a day

PEDIATRIC NURSING MLNGC,MD, RN278
Common Health Problems 1. Constipation – more common among bottle-fed infants
Add more fluids or carbohydrates/sugar2. Loose stools – careful history should be taken; management depends on cause
3. Colic – paroxysmal abdominal pain common in infants below three months of ageCauses:
Overfeeding , gas distention Too much carbohydratesTense and unsure mother
Management :Feed by demand. It is the best schedule because it meets the individual needs of the newborn.
PEDIATRIC NURSING MLNGC,MD, RN279
4. Spitting up – due to poorly developed cardiac sphincter; more common among bottle-fed infants. Will disappear when coordination with swallowing is achieved and digestion improves.Feed in upright position because gravity will aid in gastric emptying.
Position on right side after feedingBubble/burp more frequently
5. Diaper rash/Skin irritation – maybe due to either poor hygiene or irritation from urine, feces and some laundry products
PEDIATRIC NURSING MLNGC,MD, RN280
6. Miliaria (prickly heat/bungang araw) – starch bath or Johnson’s starch powder
7. Seborrheic dermatitis/cradle cap – involves the sebaceous glands; due to poor hygiene. Management: apply mineral oil or Vaseline on the scalp at night before giving shampoo in the morning.
8. Occasional “crossed eyes” – normal in many babies because the eye muscles of coordination have not yet fully developed; will disappear spontaneously

PEDIATRIC NURSING MLNGC,MD, RN281
Expanded Program on Immunization
Vaccine Age at 1st dose
Dose Number of Doses
Min Interval
Possible Reaction
BCG At birth
0.05 ml ID
1 Keloid, suppurative adenitis
DPT 6 wks 0.5 ml IM
3 4 wks Fever, restlessness, irritability
OPV 6 wks 2 drops
3 4 wks Paralytic polio rare
Hepa B 6 wksAT BIRTH
0.5 ml IM
3 4 wks ArthralgiaNeuro reactions rare
Measles
9 mos 0.5 ml SC
1 Fever and rash 5-10 days after dose
MMR 12-15 mos
0.5 ml SC
1 Fever, rash,arthralgia, lymphadenopathy,rare – febrile seizures, nerve deafness, encephalitis

PEDIATRIC NURSING MLNGC,MD, RN283
Newborn Screening Act of 2004
REPUBLIC ACT NO. 9288
“…ensure that every baby born in the Philippines is offered the opportunity to undergo newborn screening and thus be spared from heritable conditions that can lead to mental retardation and death if undetected and untreated.”

PEDIATRIC NURSING MLNGC,MD, RN284
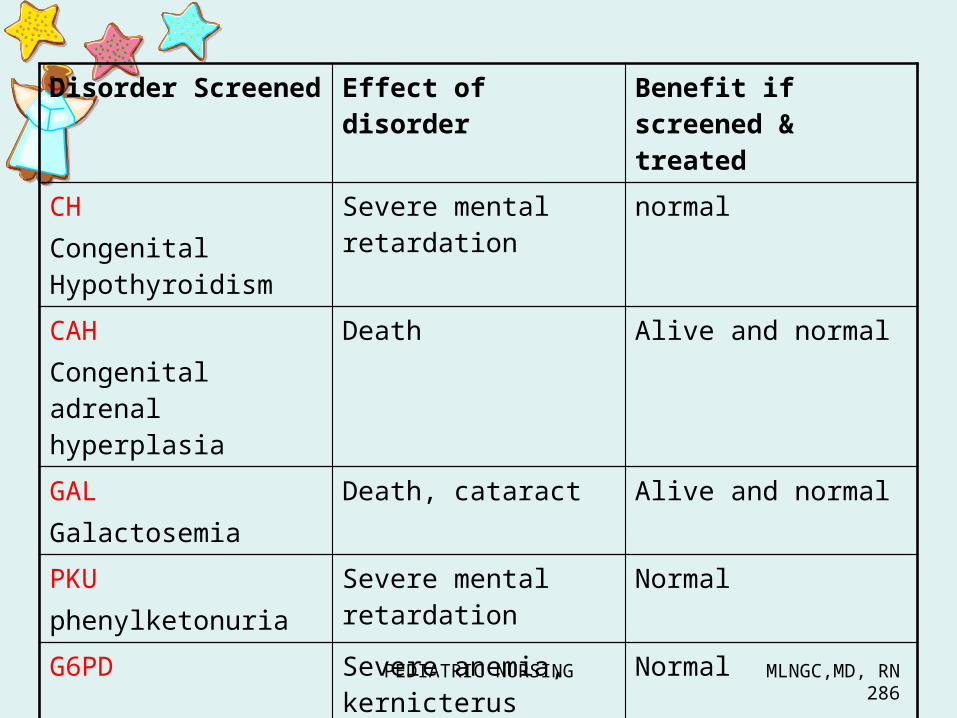
NEWBORN SCREENING
C 1. Congenital Hypothyroidism ( CH ) 2. Congenital Adrenal Hyperplasia (CAH)
P 3. PHENYLKETONURIA (PKU)
G 4. G6PD DEFICIENCY 5. Galactosemia
PEDIATRIC NURSING MLNGC,MD, RN285
NB screen
• Should be done after 24-48 hours of life• After the infant is fed• done through extraction of blood in the heel of
the foot
PEDIATRIC NURSING MLNGC,MD, RN286
Disorder Screened
Effect of disorder Benefit if screened & treated
CHCongenital Hypothyroidism
Severe mental retardation
normal
CAHCongenital adrenal hyperplasia
Death Alive and normal
GALGalactosemia
Death, cataract Alive and normal
PKUphenylketonuria
Severe mental retardation
Normal
G6PD Severe anemia, kernicterus
Normal

PEDIATRIC NURSING MLNGC,MD, RN287
1. CONGENITAL HYPOTHYROIDISM
• Thyroid hypofunction or enzyme defect • reduced T3, T4• Females
S/sx: excessive sleeping, enlarged tongue, noisy respiration, poor suck, cold extremities, slow pulse and respiratory rate, lethargy and fatigue, short and thick neck, dull expression, open mouthed, slow DTR, obesity, brittle hair, delayed dentition, dry, scaly skin

PEDIATRIC NURSING MLNGC,MD, RN288
1. CONGENITAL HYPOTHYROIDISM
Dx: low T3 T4, inc TSH
Mx: synthetic thyroid hormone
Nsg Care: Assist parents administer drugs

PEDIATRIC NURSING MLNGC,MD, RN289
After 2-3 mos of treatment
Congenital hypothyroidism
PEDIATRIC NURSING MLNGC,MD, RN290
2. CONGENITAL ADRENAL HYPERPLASIA
-inability to synthesize cortisol >>> inc ACTH >>> stimulate adrenal glands to enlarge >>> inc androgen
S/sx: masculinization, sexual precocity
Mx: Steroids to decrease stimulation of ACTH

PEDIATRIC NURSING MLNGC,MD, RN291
3. G6PD DEFICIENCY Glucose 6 phospate dehydrogenase
deficiency- reduction in the levels of the enzyme G6PD in RBC
leads to hemolysis of the cell upon exposure to oxidative stress
Dx: blood smear – heinz bodies rapid enzyme screening test, electrophoresis
Mx: avoid drugs ie ASA, sulfonamides, antimalarials, fava beans
PEDIATRIC NURSING MLNGC,MD, RN292
4. GALACTOSEMIA(-) enzyme that converts galactose to glucoseGalactose 1 phosphate uridyltransefrase
S/sx: wt loss, vomiting, hepatosplenomegaly, jaundice and cataract
Dx: Beutler test
Tx: decrease lactose – soy based formula regulate diet

PEDIATRIC NURSING MLNGC,MD, RN293
5. PHENYLKETONURIA (PKU)- Deficient or absent phenylalanine
hydroxylase w/c converts phenylalanine to tyrosine
S/sx: mental retardation, musty odor of urine, blond hair, blue eyes
Dx: Guthrie bld test
Tx: decrease phenylalanine (Lofenalac) regulate diet

PEDIATRIC NURSING MLNGC,MD, RN294
PEDIATRIC NURSING MLNGC,MD, RN295
Discharge instructions
a. Bathingb. Cord Carec. Nutrition
Calories 120 kcal/kg body weight/dayCHON 2.2 gms /KBW/dayFluids 160-120 cc/KBW/dayVitamins A,C, D for formula and breastfed
babies

PEDIATRIC NURSING MLNGC,MD, RN296
Common Health Problems
1. Constipation 2. Loose stools 3. Colic Causes: Overfeeding Gas distention Too much carbohydrates

PEDIATRIC NURSING MLNGC,MD, RN297
Management Feed by demand
Burp infant Feed in upright position
May need to change formula
PEDIATRIC NURSING MLNGC,MD, RN298
Diaper RashMiliariaSeborrheic DermatitisOccasional “Crossed Eyes”ClothingSleep Pattern

PEDIATRIC NURSING MLNGC,MD, RN299
DANGER SIGNS TO WATCH OUT FOR:
1. Deepening jaundice up to palms and soles or persistent jaundice beyond 2 weeks of life
2. Decreased sucking reflex or refusal to feed3. Unusual sleepiness4. No urine output for >48H5. Temperature instability6. Unusual movement7. Fast breathing with or without cyanosis or pallor

PEDIATRIC NURSING MLNGC,MD, RN334