Embed Size (px)
DESCRIPTION
just for file
Citation preview

PEDIA CONCEPTS 2:
FROM RESPIRATORY PROBLEMS TO HEMATOLOGIC
MS. ANN EMBRADURA, RN, MN
MS. VALERIE MAE MAGALE, RN
JANUARY TO FEBRAURY 2010

• PROBLEMS RELATED TO DISTURBED RESPIRATORY FUNCTION

APNEA OF PREMATURITY (AOP)
• Etiology: is a common phenomenon in the preterm infant. Characteristically, preterm infants are periodic breathers; they have periods of rapid respiration separated by periods of very slow breathing, and often short periods with no visible or audible respirations.

• Apnea is classified as central, obstructive, or mixed.
• Central: Central apnea is defined as the cessation of both airflow and respiratory effort

• Obstructive apnea is the cessation of airflow in the presence of continued respiratory effort.
• Mixed apnea contains elements of both central and obstructive apnea (see Media file 2), either within the same apneic pause or at different times during a period of respiratory
recording.

• Apnea of infancy• Apnea of infancy (AOI) occurs when
apnea persists in a neonate older than 37 weeks after conception. The physiologic aspects of apnea of prematurity and AOI coincide, though further studies are needed to determine their exact relationship.
• Periodic breathing• Periodic breathing is defined as periods of
regular respiration for as long as 20 seconds followed by apneic periods of 10 seconds or less that occur at least 3 times in succession

• Pathophysiology: the respiratory reflexes are less mature, which may be the contributing factor in the etiology.

• Dx:• Lab studies
• A CBC count and cultures of blood, urine, and spinal fluid are necessary if a serious bacterial or fungal infection is suspected in patients with apnea of prematurity (AOP).Appropriate viral cultures or collection of body fluid for polymerase chain reaction (PCR) analyses are performed if a viral pathogen was suspected.

• Dx:• Imaging:
• Chest radiography and/or a nuclear medicine milk scanning can be helpful if the child has persistent but unexplained lower airway symptoms (eg, wheezing and/or repetitive regurgitation after feeding, rumination)

Treatment and medication
• Goal of medical therapy • The principal goals of treating apnea of
prematurity (AOP) are to address its cause and to provide appropriate medical management. For example, bacterial sepsis that causes apnea is treated with antibiotics and other supportive therapies, whereas seizures require anticonvulsants.

• Medication• Methylxanthine: may help reduce the
incidence of events in a neonate with central apnea, though apnea in 15-20% of infants does not respond to methylxanthines.
• Aminophylline appears to stimulate skeletal and diaphragmatic muscle contraction, increase the sensitivity of the ventilatory center to CO2, and stimulate the central respiratory drive.
• Aminophylline, theophylline, and caffeine act as nonspecific inhibitors of adenosine A1 and adenosine A2a receptors.106 It is this last effect that raises concerns about the safety of
methylxanthine therapy in preterm infants.

Nursing care mgt
• Physical examination should include observation of the infant's breathing patterns while he or she is asleep and awake. The prone or supine sleeping positions and other lying postures may be important during this clinical observation.
• Weight patient, document

• Signs of theophylline or caffeine toxicity are tachycardia (rate greater than 180-190bpm) at rest, irritability, restlessness, diuresis, dysrhytmias, jittiriness and gastritis (hemorrhagic).
• When the alarm in the machine sounds, infants are first assessed for color and for presence of respiration. If they display the usual color and respirations, the nurse should investigate possible causes of a false alarrm, such as faulty lead placement, detached or disconnected leads, improper alarm setting or mechanical failure

RESPIRATORY DISTRESS SYNDROME
• Respiratory distress syndrome (RDS), also known as hyaline membrane disease (HMD), occurs almost exclusively in premature infants. The incidence and severity of respiratory distress syndrome are related inversely to the gestational age of the newborn infant.

• Is a breathing disorder of premature newborns in which the air sacs (alveoli) in a newborn's lungs do not remain open because the production of a substance that coats the alveoli (surfactant) is absent or insufficient. • Little or no surfactant, as occurs in prematurity and in
infants whose mother has diabetes, is a risk factor for respiratory distress syndrome.
• Affected infants have severe difficulty breathing and may appear blue due to a lack of oxygen in the blood.
• The diagnosis is based on symptoms, oxygen levels in the blood, and chest x-ray results.
• Without treatment, the syndrome may cause brain damage or death.

• Patho:• Acute respiratory failure with ↑pulmonary
capillary permeability, pulmonary edema, refractory hypoxemia, and ↓lung compliance. The lungs appear deep purplish red and are liver-like in consistency. Microscopically, extensive atelectasis with engorgement of the interalveolar capillaries and lymphatics can be observed.

• Clinical manifestations:• Tachypnea, respiratory alkalosis are
early signs followed by tachycardia. • The natural course of untreated RDS is
characterized by progressive worsening of cyanosis and dyspnea. If the condition is inadequately treated, blood pressure may fall; fatigue, cyanosis, and pallor increase, and grunting decreases or disappears as the condition worsens

• DX;• Labs
• Blood gases are usually obtained in respiratory distress syndrome (RDS), as clinically indicated, from an indwelling peripheral or central (umbilical) arterial catheter or by means of arterial puncture
• Pulse oximetry is used as a noninvasive tool to monitor oxygen saturation, which should be maintained at 90-95%.

• Dx: • Imaging
• Chest radiographs of a newborn infant with respiratory distress syndrome reveal bilateral, diffuse reticular granular or ground-glass appearances, air bronchograms, and poor lung expansion

Therapeutic MGT:
• Prevention: Administration of betamethasone to women 48 hr before the delivery of fetuses between 24 and 34 wk of gestation significantly reduces the incidence, mortality, and morbidity of RDS
• Corticosteroid treatment at recognition of a risk of preterm delivery is indicated. If the mother does not deliver within 1 week, retreatment may be considered; most perinatologists administer a single, 12-mg dose of betamethasone, rather than 2 doses.

• The mortality rate of respiratory distress syndrome decreased by approximately 50% over the last decade with the advent of surfactant therapy.
• Oxygenation and CPAP• Vapotherm: Vapotherm with heated and
humidified high-flow nasal canula (>2 L/min) has been used for respiratory support of neonates and to facilitate early extubation

• Assisted ventilation• High-frequency ventilation (HFV)

• Nitric oxide (NO)• Supportive therapy:
• Temperature regulation: Hypothermia increases oxygen consumption, further compromising neonates with respiratory distress syndrome who are born prematurely. Therefore, prevent hypothermia in neonates with respiratory distress syndrome during delivery, resuscitation, and transport. Care for these patients in a neutral thermal environment with the use of a double-walled incubator or radiant warmer.

• Circulation and anemia: Assess the baby's circulatory status by monitoring his or her heart rate, peripheral perfusion, and blood pressure
• Antibiotic administration: Start antibiotics in all infants who present with respiratory distress at birth after blood cultures, a CBC count with differential, and C-reactive protein levels are obtained.
• Support the family

Nursing care management
• Observe carefully especially be mindful of the constant threat of hypoxemia and acidosis
• Continuous monitoring and close observation bcause the oxygen saturation changes rapidly.
• Record at least hourly the pulse oximetry readings
• Arterial blood is drawn from the umbilical arterial catheter; assist aseptically when necessary

• Suctioning should be done ONLY when necessary. Should never be carried out as a routine procedure as it may cause bronchospasm, bradycardia because of the vagal stimulation; hypoxia and inc intracranial pressure
• Improper suctioning technique may cause infection, airway damage r even pnuemothorax
• Mouth care, as the infant is taking nothing by mouth.

MECONIUM ASPIRATION SYNDROME
• The first intestinal discharge from newborns is meconium, which is a viscous, dark-green substance composed of intestinal epithelial cells, lanugo, mucus, and intestinal secretions (eg, bile). Intestinal secretions, mucosal cells, and solid elements of swallowed amniotic fluid are the 3 major solid constituents of meconium..

• Factors that promote the passage of meconium in utero include the following:• Placental insufficiency• Maternal hypertension• Preeclampsia• Oligohydramnios• Maternal drug abuse, especially of tobacco and
cocaine• Maternal infection/chorioamnionitis • Fetal gasping secondary to hypoxia• Inadequate removal of meconium from the
airway prior to the first breath• Use of positive pressure ventilation (PPV) prior
to clearing the airway of meconium

• Pathophysiology• n utero meconium passage results from
neural stimulation of a mature GI tract and usually results from fetal hypoxic stress. As the fetus approaches term, the GI tract matures, and vagal stimulation from head or cord compression may cause peristalsis and relaxation of the rectal sphincter leading to meconium passage.

• Clinical manifestations:• Severe respiratory distress may be present.
Symptoms include the following:• Cyanosis• End-expiratory grunting• Alar flaring• Intercostal retractions• Tachypnea• Barrel chest in the presence of air trapping• Auscultated rales and rhonchi (in some
cases)
• Yellow-green staining of fingernails, umbilical cord, and skin may be observed.

• DX:• Labs
• Acid-base status• Serum electrolytes: Obtain sodium,
potassium, and calcium concentrations when the infant with MAS aged 24 hours because the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) and acute renal failure are frequent complications of perinatal stress.
• CBC count

• Imaging:• Chest radiography is essential

Treatment and medication
• Prevention of meconium aspiration syndrome (MAS)Prevention is paramount.
• Respiratory gases• Inhaled nitric oxide (NO) has the direct
effect of pulmonary vasodilatation without the adverse effect of systemic hypotension. It is approved for use, if concomitant hypoxemic respiratory failure occurs.
• Morphine, used for analgesia and sedation• Pediatric0.05-0.2 mg/kg/dose IV over 5
min q2-4h prn

• Fentanyl (Sublimaze)• Potent opioid used for analgesia, sedation, and
anesthesia. Has a shorter duration of action
than morphine.• Phenobarbital (Luminal)
• An anticonvulsant that may be used as a sedative. Suppresses the CNS from the reticular activating system (ie, presynaptic, postsynaptic).
• Pentobarbital (Nembutal)• CNS sedative and hypnotic that acts primarily
on the cerebral cortex and reticular formation through decreased neuronal synaptic activity.

• Neuromuscular blocking agents• These agents are used for skeletal
muscle paralysis to maximize ventilation by improving oxygenation and ventilation. They are also used to reduce barotrauma and minimize oxygen consumption.
• Pancuronium (Pavulon)


Nursing care mgt
• Nursing care in oxygen therapy

AIR LEAK SYNDROMES
• Asymptomatic pneumothorax, usually unilateral, is estimated to occur in 1–2% of all newborn infants; symptomatic pneumothorax and pneumomediastinum are less common
• . Pneumothorax occurs more frequently in males than in females and in term and post-term infants than in premature ones.

• Etiology and pathophysiology• Extraneous air collection
• May occur in normal neonates,• Can result from congenital renal
or pulmonary malformation, and• Often complicates underlying
respiratory disease and its therapy
• PIE

• Tension pneumothorax:• occurs if an accumulation of air within
the pleural space is sufficient to elevate intrapleural pressure above atmospheric pressure.
• Presence of asymetrical chest, altered cardiac sounds-muffled, shifted or diminished, palpable liver, and spleed, and subcutaneous emphysema

• Clinical manifestations• early manifestations of
pneumothorax include tachypnea, restlessness, and irritability, lethargy, grunting, nasal flaring, and retractions.
• Symptomatic pneumothorax is characterized by respiratory distress, which varies from only an increased respiratory rate to severe dyspnea, tachypnea, and cyanosis. Irritability and restlessness or apnea may be the earliest signs.

• Pneumomediastinum occurs in at least 25% of patients with pneumothorax and is usually asymptomatic.
• Pulmonary interstitial emphysema (PIE) may precede the development of a pneumothorax or may occur independently and result in increasing respiratory distress as a result of decreased compliance, hypercapnia, and hypoxia

DX
• The diagnosis of pneumothorax is established by x-ray, with the edge of the collapsed lung standing out in relief against the pneumothorax; pneumomediastinum is diagnosed by hyperlucency around the heart border and between the sternum and the heart border. Transillumination of the thorax is often helpful in the emergency diagnosis of pneumothorax; the affected side transmits excessive light. Associated renal anomalies are identified by ultrasonography.

• Treatment: • Without a continued air leak,
asymptomatic and mildly symptomatic small pneumothoraces require only close observation.
• Frequent small feedings may prevent gastric dilatation and minimize crying, which can further compromise ventilation and worsen the pneumothorax.



Nursing care mgt
• Most effective function is EARLY DETECTION
• And close vigilance for possible susceptible infants.
• For infants at risk, needle aspiration equipment (30ml syringe, three-way stopcock, and a 23-,to 25-gauge needles) should be at the bedside for emergency use.
• Assess breath sounds freq, monitor the efficacy of gas exchange, and regulating oxygen therapy.

Bronchopulmonary Dysplasia
• Is sometimes referred to as chronic lung dysplasia or syndrome, it is a pathologiic process that may develop in primarily ELBW, and VLBW infants with RDS.
• This may also develop in infants with MAS, persistent pulmonary hypertension, pneumonia, and cyanotic heart disease.

• Pathophysiology• The pathogenesis of bronchopulmonary
dysplasia remains complex and poorly understood
• The pulmonary changes are characterized by interstitial edema and epithelial swelling followed by thickening and fibrotic proliferation of the alveolar walls and squamous mettaplasia of the bronchiolar epithelium

• Clinical:• Physical examination may reveal
tachypnea, tachycardia, increased work of breathing (with retractions, nasal flaring, and grunting), and significant weight loss during the first 10 days of life.
• Infants with severe bronchopulmonary dysplasia are often extremely immature and had a very low birth weight. Their requirements for oxygen and ventilatory support often increase in the first 2 weeks of life.

• Diagnosis• ABG assessment in patients with
bronchopulmonary dysplasia (BPD) may reveal acidosis, hypercarbia, and hypoxia (with increased oxygen requirements).
• Continuously monitor oxygenation by using pulse oximeter because of frequent desaturations.
• Chest radiography is helpful in determining the severity of bronchopulmonary dysplasia and in differentiating bronchopulmonary dysplasia from atelectasis, pneumonia, and air leak syndrome

• Treatment• Nutrition supplementation• Fluid restriction• Diuretics• Inhaled bronchodilators• O2 supplementation as needed
• Respiratory syncytial virus (RSV) monoclonal antibody

Nursing Care Mgt
• Provide adequate hydration...care not to overhydrate as it might affect his heart status.
• Infants with BPD may become difficult or maladaptive feeders if they are aware of hunger yet compromise by not easting fast enough
• One may decrease oxygenation requirements during feedings, decreasing environmental stimuli, fortifying feedings, and provide more contact with primary caregiver.


Problems related to infectious processes

SEPSIS/SEPTICEMIA
• Refers to a generalized bacterial infection in the bloodstream. Infections are a frequent and important cause of neonatal and infant morbidity and mortality.
• Neonatal sepsis occurs in 0.5 to 8.0/1000 births. The highest rates occur in low-birth-weight (LBW) infants, those with depressed respiratory function at birth, and those with maternal perinatal risk factors.
• A neonate may be predisposed to sepsis by obstetric complications, eg, premature rupture of membranes (PROM) occurring ≥ 18 h before birth or maternal bleeding (placenta previa, abruptio placentae), toxemia, precipitous delivery, or maternal infection (particularly of the urinary tract or endometrium, most commonly manifested as maternal fever shortly before or during parturition).

• Etiology• Early-onset sepsis (ie, within 7 days of
birth) usually results from organisms acquired intrapartum. In > 50% of cases, early-onset sepsis appears within 6 h of birth, and most cases occur within 72 h. Late-onset sepsis (after 7 days) is often acquired from the environment

Patho
• The physical and chemical barriers to infection in the human body are present in the newborn but are functionally deficient. Skin and mucus membranes are broken down easily in the premature infant. Neonates who are ill and/or premature are additionally at risk because of the invasive procedures that breach their physical barriers to infection.
• Defense mechanisms of neonates are further hampered by a low level of complement, diminished opsonization ability, monocyte dysfunction and a reduced number and inefficient functionsof leucocytes.

PATHOGENESIS OF ASCENDING BACTERIAL INFECTION
• In most cases, the fetus or neonate is not exposed to potentially pathogenic bacteria until the membranes rupture and the infant passes through the birth canal and/or enters the extrauterine environment.
• Chorioamnionitis results from microbial invasion of amniotic fluid, often as a result of prolonged rupture of the chorioamniotic membrane

• Clinical• A few neonatal infections are easily recognized:
pyoderma, conjuctivitis, ompahlitis.• Cardiac signs: In overwhelming sepsis, an initial
early phase characterized by pulmonary hypertension, decreased cardiac output, and hypoxemia may occur
• Metabolic signs: Hypoglycemia, hyperglycemia, metabolic acidosis, and jaundice all are metabolic signs that commonly accompany neonatal sepsis syndrome
• Neurologic signs: Meningitis is the common manifestation of infection of the CNS

• Hematologic signs: The platelet count in the healthy newborn is rarely less than 100,000/µL in the first 10 days of life.
• GI signs: The intestinal tract can be colonized by organisms in utero or at delivery by swallowing infected amniotic fluid

• Dx• Labs
• Blood, cerebrospinal fluid (CSF), and urine culturesAerobic and anaerobic cultures are appropriate for most of the bacterial etiologies associated with neonatal sepsis.
• A Gram stain provides early identification of the gram-negative or gram-positive status of the organism for preliminary identification.
• Urine cultures are most appropriate when investigating late-onset sepsis.

• Imaging studies• Chest radiography may reveal segmental or
lobar infiltrate but more commonly reveals a diffuse, fine, reticulogranular pattern, much like what is observed in respiratory distress syndrome (RDS). Pleural effusions may also be observed.
• MRI

• Treatment and medication:• Antibiotics
• Vancomycin has been favored for this coverage; however, concern exists that overuse of this drug may lead to vancomycin-resistant organisms, Oxacillin therapy is preferred by some clinicians because of this.
• Additional therapies include granulocyte transfusion, intravenous immune globulin (IVIG) replacement, exchange transfusion, and the use of recombinant cytokines.

• Granulocyte transfusion has been shown to be suitable for infants with significant depletion of the storage neutrophil pool
• IVIG infusion • Recombinant human cytokine
administration to stimulate granulocyte progenitor cells has been studied as an adjunct to antibiotic therapy

• Diet• The neonate may need to be given nothing by
mouth (NPO)• Feeding may be restarted via a nasogastric
tube for the infant with serious compromise.
• Activity• The infant with temperature instability needs
thermoregulatory support with a radiant warmer or incubator.
• Once the infant is stable from a cardiopulmonary standpoint, parental contact is important.

• Medications:• Antibiotics
• Ampicillin• Gentamicin• Cefotaxime (Claforan)• Vancomycin (Vancocin)• Metronidazole (Flagyl)• Oxacillin (Bactocill)• Piperacillin• Erythromycin (Erythrocin)

• Meds• Antivirals
• Acyclovir (Zovirax)• Zidovudine (Retrovir, ZDV, AZT)
• Antifungals• Fluconazole (Diflucan)• Amphotericin B (Fungizone)• Amphotericin B, liposomal (AmBisome)


• Prognosis• With early diagnosis and treatment, term
infants are not likely to experience long-term health problems associated with neonatal sepsis; however, if early signs and/or risk factors are missed, the mortality rate increases. Residual neurologic damage occurs in 15-30% of neonates with septic meningitis.

Nursing care mgt
• Prompt recognition of the warning signs• Knowledge of the side effects of the specific
antibiotics and proper regulation and administration of the drug are vital.
• In addition, antibiotics predispose the infant to growth of resistant organisms and superinfection from fungal or mycotic agents, (C. Albicans)
• Provide an optimum thermoregulated environment. Anticipate dehydration and hypoxia
• Proper handwashing and disposal of excretions.

NECROTIZING ENTEROCOLITIS• is the most common life-threatening emergency of
the gastrointestinal tract in the newborn period• The disease is characterized by various degrees
of mucosal or transmural necrosis of the intestine.• The incidence of NEC is 1–5% of infants in
neonatal intensive care units. • Symptoms and signs include feeding intolerance,
lethargy, temperature instability, ileus, bloating, bilious emesis, hematochezia, reducing substances in the stool, apnea, and sometimes signs of sepsis.
• Etiology : In infants who develop NEC, 3 intestinal factors are usually present: a preceding ischemic insult, bacterial colonization, and intraluminal substrate (ie, enteral feedings).



• Dx• CBC count• Platelet count• Blood culture• Serum sodium: Hyponatremia is a worrisome
sign that is consistent with capillary leak and "third spacing" of fluid within the bowel and peritoneal space.
• Arterial blood gasses

Treatment and medication
• Stoppage of feedings: if NEC is suspected• Double lumen, NGT for decompression• Fluid resuscitation• Broad-spectrum antibiotics• TPN• Possibly surgery

• medication• Gentamicin• Vancomycin (Vancocin, Vancoled)• Metronidazole (Flagyl)
• Vasopressors• Dopamine (Intropin)• Dobutamine (Dobutrex)• Epinephrine (Adrenaline)• Naloxone (Narcan)
• Volume expanders• Albumin (5% and 25%)• Sodium chloride 0.9% (Normal saline, NS,
Isotonic saline)• Fresh frozen plasma

• Glucocorticosteroids• Hydrocortisone sodium succinate (Solu-Cortef)
• Opioid analgesics• Morphine sulfate (Duramorph, Astramorph)• Fentanyl (Sublimaze)
• Antifungal • Probiotics
• Lactobacillus acidophilus/Bifidobacterium infantis (Infloran)

Nursing care mgt
• Prompt recognition• Observe for early development of NEC
by checking the abdomen frequently for distention (measuring abdominal girth, measuring residual gastric contents before feedings, and listening for the presence of bowel sounds), and performing all routine assessments for high risk neonates
• Conscientious attention to nutrition a d hydration
• STRICT HANDWASHING


CARDIO- VASCULAR
AND HEMATOLOGIC COMPLICATIONS

PATENT DUCTUS ARTERIOSUS
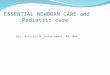
• During fetal life, most of the pulmonary arterial blood is shunted through the ductus arteriosus into the aorta


In patent ductus arteriosus, pulmonary blood flow, LA and LV volumes, and ascending AO volume are increased.
AO = aorta; LA = left atrium; LV = left ventricle; PA = pulmonary artery.

• Clinical manifestation:• When the defect is large, CHF with
dyspnea and poor weight gain or failure to thrive are the main presentations.
• Tachypnea • Tachycardia • Diaphoresis • Cyanosis• Bounding peripheral pulses and wide pulse
pressure• Hyperactive precordium: Systolic thrill• Clubbing

• Dx • Laboratory Studies
• Pulse oximetry/arterial blood gas analysis
• Imaging Studies• Chest radiography• Echocardiography/Doppler imaging -
Procedure of choice to confirm a diagnosis of PDA
• Contrast echocardiography• Cardiac catheterization• Computed tomography• Magnetic resonance imaging (MRI)


Treatment and medication
• General measures• Pulmonary support• Oxygen to correct hypoxemia• Sodium and fluid restriction• Correction of anemia
• Medical management consists of amelioration of CHF symptoms.
• No exercise restriction is required in the absence of pulmonary hypertension.
• Prophylaxis against infective endocarditis is recommended.

• Medication• Indomethacin is currently the drug of
choice for closure of the ductus in premature infants.
• When surgical ligation is not indicated, prostaglandin inhibitors (eg, NSAIDs) are used to close the ductus arteriosus.

• A few com;lications• Left heart failureP• ulmonary hypertension• Right heart hypertrophy and failure• Eisenmenger physiology (Pulmonary
hypertension usually develops in patients with a large PDA who do not undergo surgical
treatment)• Bacterial endocarditis• Myocardial ischemia• Necrotizing enterocolitis

Nursing care mgt
• Responsibilities:• Assisting in early detection• Careful assessing of cardiovascular
status• Monitoring for complications after
implementation of therapy• Assess renal function (BUN, Creatinine
levels)• Post op: monitor for pneumothorax,
bleeding, s/s of infections, supportive respi care, pan mgt

Persistent Pulmonary Hypertension of the Newborn
• Persistent pulmonary hypertension of the newborn is the persistence of or reversion to pulmonary arteriolar constriction, causing a severe reduction in pulmonary blood flow and right-to-left shunts through both the foramen ovale and the ductus arteriosus.
• Persistent pulmonary hypertension of the newborn is a disorder of pulmonary vasculature that affects term or postterm infants.

• Etiology• The most common causes involve:
Perinatal asphyxia or hypoxia• Premature ductus arteriosus or foramen
ovale closure,• Polycythemia• Congenital diaphragmatic hernia• Neonatal sepsis

• Because a patent foramen ovale and patent ductus arteriosus are normally present early in life, elevated pulmonary vascular resistance in the newborn produces extrapulmonary shunting of blood, leading to severe and potentially unresponsive hypoxemia. With inadequate pulmonary perfusion, neonates are at risk for developing refractory hypoxemia, respiratory distress, and acidosis.

• Clinical• Upon initial examination, the primary
finding is cyanosis, which is usually associated with tachypnea and respiratory distress. Cardiac examination may reveal a loud, single S2 sound or a harsh systolic murmur secondary to tricuspid regurgitation.
• The patient may have evidence of poor cardiac function and perfusion.
• Cynosis

• Diagnosis• Labs
• ABG: (Cyanosis unresponsive to O2 therapy)
• CBC count• Serum electrolytes (serum calcium)
• Imaging • Echocardiogram• X-ray to identify underlying disorders

• Imaging • Echocardiogram• X-ray to identify underlying disorders

Treatment and medication
• The care of newborns with persistent pulmonary hypertension of the newborn (PPHN) requires meticulous attention to detail.
• Use a minimal stimulation protocol to minimize the need to handle the patient and to perform invasive procedures, such as suctioning.
• Mechanical ventilation• Treatment with inhaled nitric oxide (iNO)

• Medication• Opioid analgesics (Fentanyl (Sublimaze))• Neuromuscular-blocking agents
(Pancuronium (Pavulon), Vecuronium (Norcuron))
• Vasopressors (Dopamine (Intropin), Dobutamine (Dobutrex), Milrinone (Primacor).
• surfactants:

Nursing care mgt
• Normal fluid, electrolyte, glucose, and Ca levels must be maintained. Infants should be kept in a neutral thermal environment and treated with antibiotics for possible sepsis until culture results are known. Inotropes and pressors may be required as part of circulatory support.
• Continuous monitoring for oxygenation, temperature, CVP, V/S, BP. And acid base-balance

ANEMIA
• Anemia is a disorder in which there are too few red blood cells in the blood.
• Anemia can occur when red blood cells are broken down too rapidly, too much blood is lost, or the bone marrow does not produce enough red blood cells.
• If a large amount of blood is lost very rapidly, the newborn may be in shock, appear pale, have a rapid heart rate, and have low blood pressure along with rapid, shallow breathing.

• Normally, the bone marrow does not produce new red blood cells between birth and 3 or 4 weeks of age, causing a slow drop in the red blood cell count (called physiologic anemia)
• Blood loss is another cause of anemia.

• Symptoms and Diagnosis• Moderate anemia may result in
sluggishness (lethargy), poor feeding, or no symptoms.
• Diagnosis is based on symptoms and is confirmed with blood tests.

• Treatment• Newborns who have rapidly lost large
amounts of blood, often during labor and delivery, are treated with intravenous fluids followed by a blood transfusion
• Recombinant human erythropoietin (r-HuEPO) has been used to prevent or treat chronic anemia associated with prematurity, bronchopulmonary dysplasia, and the hyporegenerative anemia of erythroblastosis fetalis.

Nursing care mgt
• Careful monitoring• Sign of anemia in the preterm infant are
poor feeding, decreased oxygen saturation, systolic murmur, dyspnea, tachycardia, tachypnea, diminished activity, and pallor

POLYCYTHEMIA
• Polycythemia is an abnormally high concentration of red blood cells.
• Plethora, a ruddy, deep red-purple appearance associated with a high Hct, is often due to polycythemia, defined as a central Hct of 65% or higher
• This disorder may result from postmaturity, diabetes in the mother, or a low oxygen level in the fetal blood.

• The incidence of neonatal polycythemia is increased at high altitudes; in postmature vs term infants; in small for gestational age vs large for gestational
• during the 1st day of life (peak, 2–3 hr); in the recipient infant of a twin-twin transfusion;
• after delayed clamping of the umbilical cord; in infants of diabetic mothers;
• in trisomy 13, 18, or 21; • in adrenogenital syndrome; in neonatal
Graves disease, etc....• which stimulates erythropoietin
production and increases RBC production.

• Clinical manifestations • include irritability, lethargy, tachypnea,
respiratory distress, cyanosis, feeding disturbances, hyperbilirubinemia, hypoglycemia, and thrombocytopenia.
• Severe complications include seizures, stroke, pulmonary hypertension, necrotizing enterocolitis, renal vein thrombosis, and renal failure.

• Treatment • of symptomatic polycythemic newborns
is partial exchange transfusion (with normal saline)
• Most asymptomatic infants develop normally.
• Appropriate therapy for correcting metabolic disturbances....hypoxia, hypoglycemia, hyperbilirubinemia

Nursing care mgt
• Watch out for these signs: plethora, peripheral cyanosis, respiratory distress, lethargy, jitteriness/ seizure activity, hypoglycemia, hyperbilirubinemia.

RETINOPATHY OF PREMATURITY
• Retinopathy of prematurity is a disorder in which the small blood vessels in the back of the eye (retina) grow abnormally.
• It can be mild with no visual defects, or it may become aggressive with new blood vessel formation (neovascularization) and progress to retinal detachment and blindness.

• As smaller and younger babies are surviving, the incidence of ROP has increased.

• Patho • ROP is characterized by severe vascular
restriction in the immature retinal vasculature, followed by hypoxia in those areas.
• Stimulation of vascular proliferation of retinal capillaries in to the hypoxic areas, where veins become numerous and dilate.
• As new vessels proliferate toward the lens, the aqueous humor ad vitreous humor become turbid.
• Retina becomes edematous, and haemorrhages separate the retina from its attachment

Dx • Stages of ROP
• Stage 0: This is the mildest form of ROP. It is immature retinal vasculature. No clear demarcation of vascularized and nonvascularized retina is present
• Stage 1: A fine, thin demarcation line between the vascular and avascular region is present. This line has no height and no thickness.
• Stage 2: A broad, thick ridge clearly separates the vascular from the avascular retina.
• Stage 3: The extraretinal fibrovascular proliferation (neovascularization) may be present on the ridge, on the posterior surface of the ridge or anteriorly toward the vitreous cavity.
• Stage 4: This stage is a subtotal retinal detachment beginning at the ridge. The retina is pulled anteriorly into the vitreous by the fibrovascular ridge.
• Stage 5: This stage is a total retinal detachment in the shape of a funnel.
• Plus disease is defined as arteriolar tortuosity and venous engorgement of the posterior pole, iris vascular engorgement, pupillary rigidity, and vitreous haze, which are part of the subclassification given to the above stages

• Other terms mentioned with ROP include the following• Popcorn: Regressed neovascularization
seen anterior to the internal limiting membrane. This is a cicatricial change and usually regresses completely over several weeks.
• Hot dog: A "red hot" active ridge, probably the site of increasing vascular channels

• Imaging Studies• a telemedicine study showed that single-
image and multiple-image telemedicine examinations perform comparably in the determination of a recommended follow-up interval and in the detection of plus disease• The instruments used are a Sauer
speculum (to keep the eyes gently open), a Flynn scleral depressor (to rotate and depress small eyes), and a 28-diopter lens (for proper identification of zones).

Treatment and medication
• Surgical Care• Cryotherapy was the original mode of
treatment• Laser surgery (eg, xenon, argon, diode)
has been shown to be as effective as cryotherapy for ROP
• Scleral buckling surgery and/or vitrectomy is usually performed for stages 4 and 5

Nursing care mgt
• Focus on decreasing the constant bright environment light and stimuli
• Decrease or avoid events known to cause fluctuations ion systemic blood pressure and oxygenation
• Intraop: stabilize and monitor v/s, adm of meds
• Post op: signs of pain and pain mgt• PARENTS need a considerable amount of
support and assistance in meeting his or her special development needs.

Any questions ??????
Thank you for you attention.
THE END!