Embed Size (px)
Citation preview

PE / DVTPE / DVT
Andrea WilsonAndrea Wilson
May 20/ 2004May 20/ 2004

Virchow’s triadVirchow’s triad
HypercoagulabilityHypercoagulability StasisStasis Venous injuryVenous injury

Risk factors Risk factors (EMR)(EMR)
Hypercoagulability Hypercoagulability Previous DVT/PEPrevious DVT/PE Malignancy Malignancy Inflammatory conditionsInflammatory conditions (SLE, IBD, (SLE, IBD,
PVD)PVD) Nephrotic syndrome Nephrotic syndrome SepsisSepsis HITHIT
Coagulation disordersCoagulation disorders Factor V Leiden mutationFactor V Leiden mutation Resistance to activated Protein C Resistance to activated Protein C Protein S deficiency Protein S deficiency Protein C deficiency Protein C deficiency Antithrombin deficiency Antithrombin deficiency Disorders of fibrinogen or Disorders of fibrinogen or
plasminogen plasminogen Antiphospholipid antibodies (lupus Antiphospholipid antibodies (lupus
anticoagulant and anti-cardiolipin)anticoagulant and anti-cardiolipin)
Increased estrogen Increased estrogen (causes urinary loss of protein S and AT III)(causes urinary loss of protein S and AT III) Pregnancy & Post-partum < 3 monthsPregnancy & Post-partum < 3 months Elective abortion or miscarriage Elective abortion or miscarriage OCP or other estrogensOCP or other estrogens
Intimal damageIntimal damage Intravenous drug abuse Intravenous drug abuse Trauma /Recent surgery Trauma /Recent surgery Central linesCentral lines
MultifactorialMultifactorial Trauma Trauma Recent surgery Recent surgery Immobilization >3 daysImmobilization >3 days Long trips > 4hr in past 4 wksLong trips > 4hr in past 4 wks Age > 60 Age > 60 Cardiac disease: MI, CHF Cardiac disease: MI, CHF Obesity Obesity CVA, neurotraumaCVA, neurotrauma Lower limb arteriopathy Lower limb arteriopathy

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
INCITING EVENT
INTIMAL DEFECT IN VEIN
COAGULATION CASCADE ACTIVATED AND PROMOTES PROXIMAL GROWTH OF THROMBUS
VENOUS HYPERTENSION DEVELOPS
PAIN AND SWELLING
EMBOLIZATION (NOT UNIVERSAL)

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
FIBRINOLYTIC SYSTEM OPPOSES COAGULATION CASCADE
CLOT ORGANIZES/DISSOLVES (PARTIALLY)
RECANALIZATION OVER SEVERAL WEEKS
FIBROBLASTS AND CAPILLARY DEVELOPMENT LEAD TO INTIMAL THCKENING
VENOUS HYPERTENSION AND RESIDUAL CLOT DESTROY VALVES
POSTPHLEBITIC SYNDROME (EDEMA, SCLEROSIS, ULCERATION, ACUTE EPISODES OF PAIN/SWELLING)

Pathophysiology:Pathophysiology:– most start in calf, extend proximally (~90%)most start in calf, extend proximally (~90%)– 70% PE have DVT evidence at autopsy70% PE have DVT evidence at autopsy– Symptomatic DVT in popliteal or prox veins in >80% Symptomatic DVT in popliteal or prox veins in >80%
casescases– Most pts with symptomatic prox DVT but no chest Most pts with symptomatic prox DVT but no chest
sx have PE (40% high probability scans)- Kearonsx have PE (40% high probability scans)- Kearon Anand 1999 says 50%Anand 1999 says 50%
Clive Kearon, CMAJ 2003Tintinalli

HistoryHistory
Many No SxMany No Sx Leg pain in 50% -> nonspecificLeg pain in 50% -> nonspecific Amount pain / tenderness do not correlate to Amount pain / tenderness do not correlate to
severityseverity
What questions would you ask?What questions would you ask?

HistoryHistory
1. Have you or anyone in your family ever had a blood clot 1. Have you or anyone in your family ever had a blood clot in their leg or lung? in their leg or lung?
2. Have you been on a long trip (e.g., car, plane, etc.)? 2. Have you been on a long trip (e.g., car, plane, etc.)? 3. Have you recently been bedridden for more than three 3. Have you recently been bedridden for more than three
days? days? 4. Have you had surgery or trauma in the last 2-3 months? 4. Have you had surgery or trauma in the last 2-3 months?
5. Have you been pregnant in the last three months 5. Have you been pregnant in the last three months (Therapeutic abortion, miscarriage, current pregnancy)? (Therapeutic abortion, miscarriage, current pregnancy)?
6. Are you on birth control pills and do you smoke? 6. Are you on birth control pills and do you smoke? 7. Do you have any medical problems (e.g., malignancy, 7. Do you have any medical problems (e.g., malignancy,
SLE, CHF)? SLE, CHF)? 8.Have you had chest pain or shortness of breath? 8.Have you had chest pain or shortness of breath?
Colucciello SA. Protocols for Deep Venous Thrombosis (DVT): A State-of-the-Art Review Part I: Risk Factor Assessment, Physical Examination, and Current Diagnostic Modalities. www.EMR online

PhysicalPhysical
No ONE reliable history / physical findingNo ONE reliable history / physical finding Sensitivity 60-96%, Specificity 20-72%Sensitivity 60-96%, Specificity 20-72% Need to look @ combination of factorsNeed to look @ combination of factors
– Anand SS, Wells PS, Hunt D, Brill-Edwards P, Cook D, Anand SS, Wells PS, Hunt D, Brill-Edwards P, Cook D, Ginsberg JS. Ginsberg JS. Does this patient have deep vein Does this patient have deep vein thrombosis?thrombosis? JAMA. 1998 Dec 2;280(21):1828-9. JAMA. 1998 Dec 2;280(21):1828-9.

PhysicalPhysical
Edema (unilateral) (> 3cm)Edema (unilateral) (> 3cm) Homan’s (50% sens) = USELESSHoman’s (50% sens) = USELESS Superficial thrombophlebitis (up to 40% can have)Superficial thrombophlebitis (up to 40% can have) Fever (>39.5, something else)Fever (>39.5, something else) Phlegmasia cerulea dolensPhlegmasia cerulea dolens
– Swollen purple leg re venous engorgementSwollen purple leg re venous engorgement– Cyanosis re massive venous obstructionCyanosis re massive venous obstruction
Phlegmasia alba dolensPhlegmasia alba dolens– Whitish inflammation associated with arterial spasm 2nd to Whitish inflammation associated with arterial spasm 2nd to
massive venous obstructionmassive venous obstruction– Worry about arterial occlusionWorry about arterial occlusion

Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? JAMA 1998; 279: 1094-1099.JAMA 1998; 279: 1094-1099.

DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS cellulitiscellulitis • • abscessabscess Baker’s cystBaker’s cyst • • CHFCHF MSK injuryMSK injury •• lymphedema lymphedema postphlebitic syndromepostphlebitic syndrome •• malignancy malignancy superficial phlebitissuperficial phlebitis •• factitious factitious fracturefracture •• AV fistula AV fistula compartment syndromecompartment syndrome •• acute arthritis acute arthritis nerve root irritationnerve root irritation •• myositis myositis
Colucciello SA. Protocols for Deep Venous Thrombosis (DVT): A State-of-the-Art Review Part I: Risk Factor Assessment, Physical Examination, and Current Diagnostic Modalities. www.EMR online

Clinical Presentation:Clinical Presentation:DVTDVT
Calf-poplitealCalf-popliteal– 80-90%, many asymptomatic80-90%, many asymptomatic– pain & swellingpain & swelling– spreads proximallyspreads proximally
IleofemoralIleofemoral– pain in buttock, groinpain in buttock, groin– thigh swellingthigh swelling– 10-20% cases10-20% cases

Case Case 55-year-old woman 55-year-old woman pain, swelling, warmth, and redness R calf. pain, swelling, warmth, and redness R calf. She denies injury to the leg, or previous DVT. She denies injury to the leg, or previous DVT. On IV chemotx for ovarian carcinoma dx 6 mos On IV chemotx for ovarian carcinoma dx 6 mos
ago. Extensive pelvic LN involvement, R>L, was ago. Extensive pelvic LN involvement, R>L, was present at diagnosis, present at diagnosis,
?due to extrinsic compression of the right iliac vein?due to extrinsic compression of the right iliac vein Now… no LNs palpable & recent pelvic U/S Now… no LNs palpable & recent pelvic U/S
showed a reduction in the adenopathy. showed a reduction in the adenopathy. Pitting edema, erythema, increased warmth of R Pitting edema, erythema, increased warmth of R
calf (> 3.5 cm greater than L), & tenderness of the calf (> 3.5 cm greater than L), & tenderness of the popliteal vein. popliteal vein.
Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? JAMA 1998; 279: 1094-1099.JAMA 1998; 279: 1094-1099.

Wells Criteria for Probability of DVTWells Criteria for Probability of DVT
Clinical Hx/Sign Criteria Points
1. Malignancy receiving active treatment for cancerOR have received treatment for cancer in past 6 mo.OR are receiving palliative care for cancer
1.0
2. Limb immobilization
ParalysisOR ParesisOR Recent casting of lower extremity
1.0
3. Patient immobilization
bedrest (except access to BR) > 3 daysOR surgery in previous 4 weeks
1.0
4. Localized tenderness
Along distribution of deep venous system 1.0
5. Entire leg swollen 1.0
6. Calf swelling >3cm when compared with asymptomatic legMeasured 10cm below the tibial tuberosity
1.0
7. Pitting edema Greater in the symptomatic leg 1.0
8. Collateral superficial veins dilated
Non-varicose veins 1.0
9. Alternative Dx as likely or more likely than that of DVT
No specific criteria – use Hx, Physical, CXR, EKG, and labs to decide
-2.0
LOW PROB< 0 points
MOD PROB1 or 2 points
HIGH PROB>3 points

What ifWhat if
60 yo man with calf swelling and active 60 yo man with calf swelling and active cancercancer
?? D-dimer +D-dimer + ?? Duplex U/S negativeDuplex U/S negative ??

Algorithm for Suspected first DVT:Algorithm for Suspected first DVT:Perrier. Lancet, 1999Perrier. Lancet, 1999
+trea t for D VT
LowD VT excluded
-D VT excluded
+trea t for D VT
Mod/H ighseria l U /S
-consider c linica l proba bility
+U /S
- D VT excluded
D -dim er
suspected D VT

D-Dimer
Neg Positive
STOP CUS legs
Normal DVT
TREAT
LOW PROBABILITY DVT
STOP

D-Dimer
Neg Positive
STOP CUS legs
Normal DVT
TREAT
MODERATE PROBABILITY DVT
CUS legin 1 week
Normal Positive
STOP TREAT

CUS legs
Normal DVT
TREAT
HIGH PROBABILITY DVT
Venography
Normal Positive
STOP TREAT

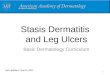
Incidence of DVT by Clinical Incidence of DVT by Clinical ProbabilityProbability
01020304050
60708090
100
Low Mod High Overall
Wells, 1997
Perrier, 1999

D-DimerD-Dimer
Enzyme-linked immunosorbent assays, Enzyme-linked immunosorbent assays, latex agglutination assays, and a whole latex agglutination assays, and a whole blood agglutination test blood agglutination test
PPV poor; NPV excellentPPV poor; NPV excellent NOT to r/o PE in high PTPNOT to r/o PE in high PTP

DIAGNOSIS: BLOOD TESTSDIAGNOSIS: BLOOD TESTS
D-dimerD-dimer– degradation product of cross-linked fibrindegradation product of cross-linked fibrin– measured by whole blood agglutination (SimpliRED), measured by whole blood agglutination (SimpliRED),
latex agglutination, and latex agglutination, and ELISAELISA – advantages: rapid, 93% sensitive for proximal DVTadvantages: rapid, 93% sensitive for proximal DVT– disadvantages: low specificity, false positives in patients disadvantages: low specificity, false positives in patients
with recent surgery/trauma, hemorrhage,recent MI/CVA, with recent surgery/trauma, hemorrhage,recent MI/CVA, acute infection, DIC, pregnancy/recent delivery, active acute infection, DIC, pregnancy/recent delivery, active collagen vascular disease, liver disease, metastatic Ca, collagen vascular disease, liver disease, metastatic Ca, 90% +ve >80 yrs old90% +ve >80 yrs old
– highest NPV in low risk patientshighest NPV in low risk patients

D-dimer AssaysD-dimer AssaysVan der Graaf. Thromb Haemost, 2000.Van der Graaf. Thromb Haemost, 2000.
Assay Ease of use
Sensitivity Specificity
Whole blood agglutination (SimpliRED)
++++ 80-85% 70-90%
Latex agglutination
+++ 90-95% 40-90%
Rapid ELISA ++++ 95-100% 30-60%

Alveolar dead space?Alveolar dead space? AlveolarAlveolar deaddead spacespace should increase after PE as should increase after PE as
a result of arterial vascular occlusion because a result of arterial vascular occlusion because some pulmonary segments are ventilated but not some pulmonary segments are ventilated but not perfused. perfused.
Kline et al (JAMA) evaluated the diagnostic Kline et al (JAMA) evaluated the diagnostic accuracy of alveolar dead space determination + accuracy of alveolar dead space determination + d-dimer assay for dx of PE. d-dimer assay for dx of PE.
combination of tests performs slightly better than combination of tests performs slightly better than either test alone (negative likelihood ratio). either test alone (negative likelihood ratio).
Niemann JT. Diagnostic Accuracy of a Bedside D-Dimer Assay and Alveolar Dead-Space Measurement for Rapid Exclusion of Pulmonary Embolism: A Multicenter Study. Annals of Emergency Medicine. 2001; 38 (6)

UltrasoundUltrasound Duplex doppler ultrasoundDuplex doppler ultrasound
– combines Doppler flow with 2D scanningcombines Doppler flow with 2D scanning– Doppler component evaluates blood flow for Doppler component evaluates blood flow for
proximal obstruction, color flow provides most proximal obstruction, color flow provides most accurate images, and 2D scan provides 2D image accurate images, and 2D scan provides 2D image of vein and surrounding structuresof vein and surrounding structures
– non-invasive, portablenon-invasive, portable– loss of compression = DVTloss of compression = DVT
We don’t look below poplitealWe don’t look below popliteal

Diagnostic Imaging for DVTDiagnostic Imaging for DVT
Duplex / compression U/SDuplex / compression U/S+ve in 30-50% PE; 5% non-dx V/Q scans+ve in 30-50% PE; 5% non-dx V/Q scans– 97% sensitive for acute thrombi above the knee, 97% sensitive for acute thrombi above the knee,
94%specific (Tintinalli)94%specific (Tintinalli)– Only 58% sensitive in asymptomatic DVT Only 58% sensitive in asymptomatic DVT
(Anand)(Anand)– also good for other causes of leg swellingalso good for other causes of leg swelling– limitations: expensive, operator dependent, less limitations: expensive, operator dependent, less
sensitive for: clots below knee (73%), sensitive for: clots below knee (73%), pregnancy, and nonoccluding thrombi, acute vs pregnancy, and nonoccluding thrombi, acute vs chronicchronic

Serial Venous U/SSerial Venous U/S
may avoid angiography in ?PEmay avoid angiography in ?PE In low-risk: an initial N U/S or 2 done 1 In low-risk: an initial N U/S or 2 done 1
wk apart carries a <1% risk of wk apart carries a <1% risk of symptomatic proximal DVT or PE at 3 symptomatic proximal DVT or PE at 3 mos. mos.
You can hold the anticoagulant if initial U/S You can hold the anticoagulant if initial U/S negative (safe)negative (safe)
1-2% +ve in 2 weeks (?PE)1-2% +ve in 2 weeks (?PE)

Anand et al 1999Anand et al 1999 Making the point that if results are Making the point that if results are
discordant then further testing needed.discordant then further testing needed. A lot of venography / different than ours.A lot of venography / different than ours.

Impedance PlethysmographyImpedance Plethysmography
– measures change in lower extremity volume as a function of measures change in lower extremity volume as a function of venous outflow in response to certain stimulivenous outflow in response to certain stimuli
– changes in calf circumference, cutaneous blood flow, or changes in calf circumference, cutaneous blood flow, or electrical resistance occur when there is obstruction of electrical resistance occur when there is obstruction of venous returnvenous return
– Does not allow direct visualization of veinsDoes not allow direct visualization of veins– suggests that DVT is present when significant outflow suggests that DVT is present when significant outflow
obstruction present, (if no extrinsic venous compression or obstruction present, (if no extrinsic venous compression or conditions associated with elevated central venous conditions associated with elevated central venous pressure). pressure).
– operator dependentoperator dependent

Impedance plethysmographyImpedance plethysmography
IPGIPG– false positives occur in the setting of post false positives occur in the setting of post
phlebitic syndrome, abdominal tumors, phlebitic syndrome, abdominal tumors, pregnancy, and CHFpregnancy, and CHF
– sensitivity 73-96% , specificity 83-95%, sensitivity 73-96% , specificity 83-95%, 97%NPV (Tintinalli)97%NPV (Tintinalli)
– sensitivity over a 10d-2 week follow-up period sensitivity over a 10d-2 week follow-up period approaches that of ultrasound, thus used for approaches that of ultrasound, thus used for outpt F/U (Calgary protocol is day 1, 4, 7, and outpt F/U (Calgary protocol is day 1, 4, 7, and 10 after negative U/S at day 0)10 after negative U/S at day 0)
– Not good for calf clots eitherNot good for calf clots either

IPG vs. DopplerIPG vs. Doppler
N=985N=985 PPV U/S=94% (CI 87-98%)PPV U/S=94% (CI 87-98%) PPV IPG =83% (CI 75-90%)PPV IPG =83% (CI 75-90%) P=0.02P=0.02
– Harriet Heijboer, Harry R. Buller, Anthonie Lensing, Harriet Heijboer, Harry R. Buller, Anthonie Lensing, Alexander Turpie, Louisa P. Colly, and Jan Wouter ten Alexander Turpie, Louisa P. Colly, and Jan Wouter ten Cate. Cate. A Comparison of Real-Time Compression A Comparison of Real-Time Compression Ultrasonography with Impedance Plethysmography Ultrasonography with Impedance Plethysmography for the Diagnosis of Deep-Vein Thrombosis in for the Diagnosis of Deep-Vein Thrombosis in Symptomatic Outpatients Symptomatic Outpatients NEJM Volume 329:1365-NEJM Volume 329:1365-1369November 4, 1993Number 19.1369November 4, 1993Number 19.

U/SU/S
What if the U/S or IPG is inconclusive or What if the U/S or IPG is inconclusive or there was a potential for false + or false - there was a potential for false + or false - results? results?
With tx of proximal DVT, residual thrombosis With tx of proximal DVT, residual thrombosis is evident on U/S scans in ~50% of pts after is evident on U/S scans in ~50% of pts after 1 yr1 yr
Contrast venography or MRIContrast venography or MRI

VenographyVenography
““?Gold Standard?”?Gold Standard?” InvasiveInvasive ContrastContrast Need experienced readersNeed experienced readers Non-diagnostic up to 25%Non-diagnostic up to 25% May induce DVT in 3% (Anand) May induce DVT in 3% (Anand)

DIAGNOSIS:IMAGINGDIAGNOSIS:IMAGING
VenographyVenography– gold standard, but:gold standard, but:
radiologists’ interpretations differ 10% of the timeradiologists’ interpretations differ 10% of the time 5-15% are inadequately done5-15% are inadequately done 2-5% of patients develop phlebitis (sup. or deep)2-5% of patients develop phlebitis (sup. or deep) risk of anaphylactoid reactions existsrisk of anaphylactoid reactions exists
+able to distinguish between acute and chronic events as +able to distinguish between acute and chronic events as well as collateral channelswell as collateral channels
+test of choice for the post-surgical patient as U/S not +test of choice for the post-surgical patient as U/S not sensitive enoughsensitive enough
+useful if U/S inconclusive+useful if U/S inconclusive

Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? JAMA 1998; 279: 1094-1099.Thrombosis? JAMA 1998; 279: 1094-1099.

Diagnostic Imaging (Tintinalli)Diagnostic Imaging (Tintinalli)Indication Sens
(prox DVT)Pro Con
Duplex DVT 97% Noninvasive, finds alt dx
Poor sens for calf
IPG No duplex >80% Noninvasive Poor sens, false +,
Venography No duplex/ inconclusive
100% Accurate, sees calf DVT
Invasive, painlful, contrast, PPS
Radionuclide study
Inconclusive & contrast C/I
Variable(ok for calf)
None Delayed result, $, high false+
MRI Inconclusive, pelvic DVT, pregnant
>95% Noninv, safe in preg, finds alt dx, acute vs chronic
$, time, magnet

TreatmentTreatment
Goal: prevent PEGoal: prevent PE

TREATMENTTREATMENT Unfractionated heparinUnfractionated heparin
– works on intrinsic pathwayworks on intrinsic pathway
– activates antithrombin III to prevent conversion of fibrinogen to activates antithrombin III to prevent conversion of fibrinogen to fibrinfibrin
– prevents extension of thrombus but does not remove existing prevents extension of thrombus but does not remove existing thrombusthrombus
– narrow therapeutic windownarrow therapeutic window
– significant bleeding in 7-30% of patientssignificant bleeding in 7-30% of patients
– thrombocytopenia in 3%thrombocytopenia in 3%
– use weight based nomogram instead of fixed dosing (more use weight based nomogram instead of fixed dosing (more patients therapeutically anticoagulated within 12 hours)patients therapeutically anticoagulated within 12 hours)
– largely replaced by LMWH for treatment of DVTlargely replaced by LMWH for treatment of DVT

TREATMENTTREATMENT Low molecular weight heparinLow molecular weight heparin
– primarily inhibits factor Xa more so than IIa, therefore, doesn’t primarily inhibits factor Xa more so than IIa, therefore, doesn’t affect PTT and no need for therapeutic monitoringaffect PTT and no need for therapeutic monitoring
– greater bioavailability and more predictable therapeutic greater bioavailability and more predictable therapeutic anticoagulant effectanticoagulant effect
– tinzaparin (Innohep) approved for use in Canada for DVT, tinzaparin (Innohep) approved for use in Canada for DVT, enoxaparin (Lovenox) in the U.S.enoxaparin (Lovenox) in the U.S.
– Can still test for hypercoagulable statesCan still test for hypercoagulable states– reversible with protamine 1 mg/100 U LMWHreversible with protamine 1 mg/100 U LMWH– continue until INR therapeutic for 2 consecutive days, then continue until INR therapeutic for 2 consecutive days, then
stopstop– safety of home administration well-establishedsafety of home administration well-established

Treatment of VTE:Treatment of VTE:AnticoagulationAnticoagulation
LMWH superior to UFH? LMWH superior to UFH? (Gould 1999)(Gould 1999)– More predictable anticoag effect, easier, lower incidence of major More predictable anticoag effect, easier, lower incidence of major
bleeding and HIT, lower mortality, reduction in clot extension, fewer bleeding and HIT, lower mortality, reduction in clot extension, fewer recurrent thromboembolic eventsrecurrent thromboembolic events
– out-pt Rx safe in PE (Kovacs, 2000) out-pt Rx safe in PE (Kovacs, 2000)
Cost-effective (Gould 1999)Cost-effective (Gould 1999) Only measure anti-Xa levels in renal failure pts.Only measure anti-Xa levels in renal failure pts.
– Avoid if CR > 180 umol/LAvoid if CR > 180 umol/L

AnticoagulationAnticoagulation
Enoxaparin 1mg/kg bid or 1.5mg/kg od (max 180 mg)Enoxaparin 1mg/kg bid or 1.5mg/kg od (max 180 mg) Tinzaparin 175 anti-Xa u/kg od (max 18,000 U)Tinzaparin 175 anti-Xa u/kg od (max 18,000 U) Weight-based dosing (actual not ideal weight)Weight-based dosing (actual not ideal weight) start warfarin 5mg on day 1start warfarin 5mg on day 1 d/c LMWH when INR >2.0 x 2 daysd/c LMWH when INR >2.0 x 2 days Rx 3 mos if 1st and reversible causeRx 3 mos if 1st and reversible cause 6 mos if non-reversible6 mos if non-reversible indefinite if recurrent, CA, geneticindefinite if recurrent, CA, genetic Anticoagulation ClinicAnticoagulation Clinic

TREATMENTTREATMENT
WarfarinWarfarin– acts on extrinsic pathway (factor VII) to inhibit vitamin K acts on extrinsic pathway (factor VII) to inhibit vitamin K
dependent factor synthesis (II, VII, IX, X)dependent factor synthesis (II, VII, IX, X)
– started same day as heparinstarted same day as heparin
– theoretical risk of worsening thrombosis if started before theoretical risk of worsening thrombosis if started before heparin in patients with protein C or S deficiency heparin in patients with protein C or S deficiency (procoagulant effect) but studies have demonstrated safety of (procoagulant effect) but studies have demonstrated safety of starting in EDstarting in ED
– INR between 2-3 provides adequate anticoagulation without INR between 2-3 provides adequate anticoagulation without serious increase in bleeding riskserious increase in bleeding risk

TREATMENTTREATMENT
IVC – controversial: no survival benefitIVC – controversial: no survival benefit– If anticoag C/I, major bleed, HIT, persisting DVT or If anticoag C/I, major bleed, HIT, persisting DVT or
embolization after 1-2 wks therapeutic anticoag.embolization after 1-2 wks therapeutic anticoag. ThrombolyticsThrombolytics
– may have decreased risk of post-phlebitic syndrome may have decreased risk of post-phlebitic syndrome over patients treated with heparin? over patients treated with heparin?
– increased risk of hemorrhagic complications over increased risk of hemorrhagic complications over heparin has prevented its widespread useheparin has prevented its widespread use
– should be used for phlegmasia dolens if heparin fails should be used for phlegmasia dolens if heparin fails (also consider thrombectomy)(also consider thrombectomy)
– Consideration for extensive iliofemoral thrombosis and Consideration for extensive iliofemoral thrombosis and UEDVT: SK or tPA + heparinUEDVT: SK or tPA + heparin

Indications for AdmissionIndications for Admission
Unable to ambulateUnable to ambulate Poor social supportPoor social support Unreliable follow upUnreliable follow up Unable to educate re: drug administrationUnable to educate re: drug administration Need for lytic or invasive txNeed for lytic or invasive tx Query arterial ischemia, cellulitis or pelvic Query arterial ischemia, cellulitis or pelvic
mass mass – (Tintinalli)(Tintinalli)

SPECIAL CONSIDERATIONSSPECIAL CONSIDERATIONS
Superficial phlebitisSuperficial phlebitis– while isolated cases are benign and can be treated with while isolated cases are benign and can be treated with
NSAIDs and compression bandages, NSAIDs and compression bandages, Incidence of DVT from extension of a superficial Incidence of DVT from extension of a superficial
thrombus ~3% but incidence of embolization very thrombus ~3% but incidence of embolization very lowlow– recommended that all patients be followed serially with recommended that all patients be followed serially with
U/S or IPG to ensure no propagation to deep venous U/S or IPG to ensure no propagation to deep venous systemsystem
Do F/U U/S in 1 weekDo F/U U/S in 1 week (Tintinalli)(Tintinalli)

SPECIAL CONSIDERATIONSSPECIAL CONSIDERATIONS
Upper extremity DVTUpper extremity DVT– 2-4% of all DVT in axillary or subclavian V 2-4% of all DVT in axillary or subclavian V – can cause PE (originally thought to be benign)can cause PE (originally thought to be benign)– etiology: “effort thrombosis” in physically active etiology: “effort thrombosis” in physically active
people, thoracic outlet syndrome, cervical rib, people, thoracic outlet syndrome, cervical rib, central line, malignancycentral line, malignancy
25% Paget-von Schroetter syndrome25% Paget-von Schroetter syndrome– Exertional DVTExertional DVT– Caused by underlying MSK deformitiesCaused by underlying MSK deformities

Upper Extremity DVTUpper Extremity DVT
N=58 Sx UEDVTN=58 Sx UEDVT IPG, Doppler, venographyIPG, Doppler, venography Test Sens & Spec:Test Sens & Spec:
– compression ultrasonography (96% and 93.5%) compression ultrasonography (96% and 93.5%) – color flow Doppler imaging (100% and 93%)color flow Doppler imaging (100% and 93%)
27 (47%) + UEDVTPE “Objectively” found in 36%27 (47%) + UEDVTPE “Objectively” found in 36% 2 yr F/U: 2 recurrent VTE2 yr F/U: 2 recurrent VTE RF:RF:
– CVCCVC– ThrombophiliaThrombophilia– Previous VTEPrevious VTE
Prandoni P, Polistena P, Bernardi E, et al Upper-extremity deep vein thrombosis. Risk Prandoni P, Polistena P, Bernardi E, et al Upper-extremity deep vein thrombosis. Risk factors, diagnosis, and complications. Arch Intern Med. 1998 Sep 28;158(17):1950-2.factors, diagnosis, and complications. Arch Intern Med. 1998 Sep 28;158(17):1950-2.

U/S Upper Extremity DVTU/S Upper Extremity DVT
The sensitivity of duplex ultrasonography The sensitivity of duplex ultrasonography ranged from 56% to 100%, and the ranged from 56% to 100%, and the specificity ranged from 94% to 100%specificity ranged from 94% to 100%
Unsure if HelpfulUnsure if Helpful Venography or MRI if high clinical suspicion Venography or MRI if high clinical suspicion
but negative U/Sbut negative U/S
Mustafa BO, MD; Rathbun SW, MD; Whitsett TL, MD. Sensitivity and Specificity of Mustafa BO, MD; Rathbun SW, MD; Whitsett TL, MD. Sensitivity and Specificity of Ultrasonography in the Diagnosis of Upper Extremity Deep Vein Thrombosis: A Ultrasonography in the Diagnosis of Upper Extremity Deep Vein Thrombosis: A Systematic Review Arch Int Med 2002 162(4)401Systematic Review Arch Int Med 2002 162(4)401

Upper Extremity DVTUpper Extremity DVT
Thrombus in 35-67% of long term CVC (Randolph)Thrombus in 35-67% of long term CVC (Randolph) 10-30% incidence PE associated10-30% incidence PE associated Meta-analysis by Randolph in Chest 1998 showed Meta-analysis by Randolph in Chest 1998 showed
benefit of prophylactic heparin for CVCbenefit of prophylactic heparin for CVC Therapy:Therapy:
– Anticoagulation alone Anticoagulation alone – Local thrombolytics appears to be Rx of choice with Local thrombolytics appears to be Rx of choice with
literature mainly case studiesliterature mainly case studies– Look for underlying compressive abnormalityLook for underlying compressive abnormality– +/- SVC filter if C/I+/- SVC filter if C/I– Consult your neighbourhood vasc surgeonConsult your neighbourhood vasc surgeon

SPECIAL CONSIDERATIONSSPECIAL CONSIDERATIONS
Calf DVTCalf DVT most DVTs start in calf, extend proximally (~90%)most DVTs start in calf, extend proximally (~90%)
– Isolated calf DVT extend proximally only 20% of timeIsolated calf DVT extend proximally only 20% of time Usually within 1 week Usually within 1 week Nonextending calf DVT rarely cause PENonextending calf DVT rarely cause PE
– it is not universally recommended that isolated calf it is not universally recommended that isolated calf thrombi require anticoagulation, but they at the very thrombi require anticoagulation, but they at the very least require serial studies to ensure no progressionleast require serial studies to ensure no progression
Pelvic Vein ThrombosisPelvic Vein Thrombosis– Postpartum, PID, post pelvic surgery/taumaPostpartum, PID, post pelvic surgery/tauma– Non-spec abdo pain and vomitingNon-spec abdo pain and vomiting– MR or CTMR or CT

PULMONARY EMBOLISMPULMONARY EMBOLISM

MortalityMortality
Approximately 10% of patients who develop PE Approximately 10% of patients who develop PE die within the first hour, die within the first hour,
5-10% of PE have shock at presentation5-10% of PE have shock at presentation USA: 60-80% patients with DVT, >50% Sx free USA: 60-80% patients with DVT, >50% Sx free Autopsy studies: 60% pts who die in hospital had Autopsy studies: 60% pts who die in hospital had
PE, diagnosis missed in >50%PE, diagnosis missed in >50% 30% die from recurrent embolism. Anticoagulant 30% die from recurrent embolism. Anticoagulant
Rx decreases mortality to < 5%Rx decreases mortality to < 5%

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
DVT (CALF, ILEOFEMORAL SYSTEM, OR UPPER EXTREMITY)
PORTION OF CLOT BREAKS OFF AND TRAVELS VIA IVC AND RIGHT HEART SYSTEM TO LODGE IN PULMONARY
CIRCULATION
PORTION OF LUNG VENTILATED BUT NOT PERFUSED (PHYSIOLOGIC DEAD SPACE) LEADING TO HYPOXEMIA
AND HYPERCARBIA
COMPENSATORY MECHANISMS (TACHYPNEA, INCREASED DEPTH OF VENTILATION)

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
IF SIGNIFICANT SIZED CLOT (>50% OF VASCULAR TREE INVOLVED), COMPENSATORY MECHANISMS FAIL, WITH
INCREASED PULMONARY VASCULAR RESISTANCE, INCREASED RIGHT-SIDED HEART PRESSURES, AND
INCREASED V/Q MISMATCH
PULMONARY HYPERTENSION, ACUTE COR PULMONALE, DECREASED CARDIAC OUTPUT, AND HEMODYNAMIC
COLLAPSE

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
IF INITIAL EVENT IS SURVIVED, CLOT RECANALIZES OVER SEVERAL WEEKS
CHRONIC PULMONARY HYPERTENSION/COR PULMONALE DEVELOPS

Natural HistoryNatural History
Most pulmonary emboli are multiple, and the lower Most pulmonary emboli are multiple, and the lower lobes are involvedlobes are involved– From deep veins of lower extremities From deep veins of lower extremities – Also pelvic, renal, upper extremity, right heart chambersAlso pelvic, renal, upper extremity, right heart chambers
Large thrombi lodge @ bifurcation of main PA or Large thrombi lodge @ bifurcation of main PA or lobar branches -> hemodynamic compromiselobar branches -> hemodynamic compromise
Smaller thrombi occlude smaller vessels in Smaller thrombi occlude smaller vessels in peripheryperiphery– More likely to cause pleuritic chest pain (inflammatory More likely to cause pleuritic chest pain (inflammatory
response adjacent to parietal pleura)response adjacent to parietal pleura)

Pathophysiology ReviewPathophysiology Review
Normal RV has a narrow range over which it can Normal RV has a narrow range over which it can compensate for acute increases in afterload. The compensate for acute increases in afterload. The pericardium has a limited ability to distend.pericardium has a limited ability to distend.
Increased RV afterload -> elevation in RV wall pressures Increased RV afterload -> elevation in RV wall pressures -> dilation and hypokinesis of the RV wall -> -> dilation and hypokinesis of the RV wall ->
shift of intraventricular septum towards left ventricle shift of intraventricular septum towards left ventricle (tricuspid regurgitation) and decreased LV output.(tricuspid regurgitation) and decreased LV output.

Respiratory ConsequencesRespiratory Consequences
EarlyEarly– Increased alveolar dead space, Pneumoconstriction, hypoxemia, Increased alveolar dead space, Pneumoconstriction, hypoxemia,
hyperventilationhyperventilation Late: Late:
– regional loss surfactant, pulmonary infarctionregional loss surfactant, pulmonary infarction Arterial hypoxemia frequent, not universalArterial hypoxemia frequent, not universal
– V/Q mismatch, shunts, reduced CO, intracardiac shunt via PFO V/Q mismatch, shunts, reduced CO, intracardiac shunt via PFO Infarction uncommon : bronchial arterial collateral Infarction uncommon : bronchial arterial collateral
circulationcirculation

PIOPED SxPIOPED Sx
dyspnea (73%) dyspnea (73%) pleuritic chest pain (66%)pleuritic chest pain (66%) cough (37%) cough (37%) hemoptysis (13%)hemoptysis (13%)

Physical: Size MattersPhysical: Size Matters Acute PE (no infarct)Acute PE (no infarct)
– Non-specificNon-specific– Tachypnea, tachycardia, pleuritic pain, crackles and local wheeze @ embolus Tachypnea, tachycardia, pleuritic pain, crackles and local wheeze @ embolus
sitesite
Multiple PEs Multiple PEs – Non-specificNon-specific– Pulmonary HTN and cor pulmonalePulmonary HTN and cor pulmonale– High JVD, RV heave, palpable impulse 2nd LICS, RV S3 gallop, systolic High JVD, RV heave, palpable impulse 2nd LICS, RV S3 gallop, systolic
murmur over the left sternal border that is louder during inspiration, murmur over the left sternal border that is louder during inspiration, hepatomegaly, ascites, dependent pitting edema.hepatomegaly, ascites, dependent pitting edema.
Massive PEMassive PE– Shock , hypotension, poor perfusion, tachycardia, and tachypneaShock , hypotension, poor perfusion, tachycardia, and tachypnea– Shock index HR/syst BP >1Shock index HR/syst BP >1

Physical examPhysical exam
Signs of pulmonary hypertension Signs of pulmonary hypertension – palpable impulse over 2nd LICS, loud P2, RV S3 gallop, palpable impulse over 2nd LICS, loud P2, RV S3 gallop,
and a systolic murmur louder on inspiration at left and a systolic murmur louder on inspiration at left sternal border (TR)sternal border (TR)
Acute pulmonary infarctionAcute pulmonary infarction– Decreased excursion of involved hemithorax, palpable Decreased excursion of involved hemithorax, palpable
or audible pleural friction rub, localized tendernessor audible pleural friction rub, localized tenderness– Signs of pleural effusion, hemoptysis, feverSigns of pleural effusion, hemoptysis, fever

Physical: PIOPEDPhysical: PIOPED
Tachypnea (70%)Tachypnea (70%) Rales (51%)Rales (51%) Tachycardia (30%)Tachycardia (30%) Fourth heart sound (24%)Fourth heart sound (24%) Accentuated P2 (23%)Accentuated P2 (23%) Fever < 39°C ( 14%) of patients (> 39.5°C not Fever < 39°C ( 14%) of patients (> 39.5°C not
from PE) from PE) Palpable Chest wall tenderness w/o Hx traumaPalpable Chest wall tenderness w/o Hx trauma

CLINICAL FEATURESCLINICAL FEATURES SymptomSymptom Percent Percent
– dyspneadyspnea 73-8473-84– pleuritic chest painpleuritic chest pain 66-7466-74– apprehensionapprehension 5959– coughcough 37-5337-53– leg swellingleg swelling 2828– hemoptysishemoptysis 13-3013-30– diaphoresisdiaphoresis 2727– nonpleuritic chest painnonpleuritic chest pain 4-144-14– syncopesyncope 1313– wheezingwheezing 9 9

CLINICAL FEATURESCLINICAL FEATURES
SignSign Percent with signPercent with sign– tachypnea (RR>20)tachypnea (RR>20) 7070– ralesrales 51-5851-58– accentuated P2accentuated P2 23-5323-53– tachycardia (HR>100)tachycardia (HR>100) 30-4430-44– temp > 37.8temp > 37.8 4343– S3 or S4S3 or S4 3434– thrombophlebitisthrombophlebitis 3232

DIAGNOSIS: ECGDIAGNOSIS: ECG
ECG: most common = non-specific ST T wave ECG: most common = non-specific ST T wave changes. 40% will have tachycardia (EM rap)changes. 40% will have tachycardia (EM rap)
Normal ECG not sensitive enough to R/O PENormal ECG not sensitive enough to R/O PE changes not specific for PE, and reflect signs of right changes not specific for PE, and reflect signs of right
heart strainheart strain– new RBBBnew RBBB– R axis deviationR axis deviation– S1 Q3 T3S1 Q3 T3
others:others:– electrical alternanselectrical alternans– T wave inversionT wave inversion– atrial fibrillationatrial fibrillation– sinus tachycardiasinus tachycardia– normal in 20-30% of casesnormal in 20-30% of cases

DIAGNOSIS: CHEST X-RAYDIAGNOSIS: CHEST X-RAY
abnormal in >80% of cases of PE (up to abnormal in >80% of cases of PE (up to 30% N initially), but nonspecific findings30% N initially), but nonspecific findings– atelectasisatelectasis– pleural effusionpleural effusion– elevated hemidiaphragm (50% of initial CXR’s elevated hemidiaphragm (50% of initial CXR’s
of patients with PE)of patients with PE)– pneumonia-like infiltrates, especially w/i 3 days pneumonia-like infiltrates, especially w/i 3 days
of symptom onset (33-50% of patients with PE)of symptom onset (33-50% of patients with PE)
May mislead you to diagnosing pneumoniaMay mislead you to diagnosing pneumonia

DIAGNOSIS: CHEST X-RAYDIAGNOSIS: CHEST X-RAY other findings:other findings:
– Hampton’s humpHampton’s hump wedge-shaped, pleural based infiltrate with apex toward wedge-shaped, pleural based infiltrate with apex toward
hilum, representing lung infarctionhilum, representing lung infarction
– Westermark’s signWestermark’s sign peripheral oligemia secondary to clot interrupting blood peripheral oligemia secondary to clot interrupting blood
flowflow this is the earliest detectable sign in PE, if presentthis is the earliest detectable sign in PE, if present
– Fleishner’s signFleishner’s sign large sausage-shaped pulmonary artery (some call this large sausage-shaped pulmonary artery (some call this
part of Westermark’s sign)part of Westermark’s sign)

DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
pneumoniapneumonia •• costochondritis costochondritis pneumothoraxpneumothorax •• other emboli other emboli angina/MIangina/MI •• sepsis sepsis pleurisypleurisy •• aortic dissection aortic dissection MSK injuryMSK injury •• pericarditis pericarditis carcinomacarcinoma •• anxiety/panic anxiety/panic asthma/COPDasthma/COPD •• CHF CHF lung abscesslung abscess

What if?What if?
38 yo woman with burning substernal CP 38 yo woman with burning substernal CP radiating to throat. Not pleuritic.radiating to throat. Not pleuritic.
120/80 P-80 RR-18, normal sat, afebrile120/80 P-80 RR-18, normal sat, afebrile Mild mid-epig tendernessMild mid-epig tenderness N ECG and CXRN ECG and CXR ?risk?risk

What if? What if?
Rural EDRural ED 72 yo male72 yo male fever, SOB, pleuritic CP x 2 daysfever, SOB, pleuritic CP x 2 days HR 110, bp 140/90, RR 22, sat 90%HR 110, bp 140/90, RR 22, sat 90% CXR unremarkableCXR unremarkable Pre-test probabilityPre-test probability What test/Rx?What test/Rx?

Wells Criteria for Probability of PEWells Criteria for Probability of PEClinical Hx/Sign Criteria Point
s
1. S/S of DVT leg swelling – objectively measuredAND pain with palpation in the deep vein region
3.0
2. Pulse>100/min 1.5
3. Immobilization bedrest (except access to BR) > 3 daysOR surgery in previous 4 weeks
1.5
4. Previous DVT or PE
Must have been objectively diagnosed 1.5
5. Hemoptysis 1.0
6. Malignancy receiving active treatment for cancerOR have received treatment for cancer in past 6 mo.OR are receiving palliative care for cancer
1.0
7. PE as likely or more likely than an alternative Dx.
No specific criteria – use Hx, Physical, CXR, EKG, and labs to decide
3.0
Total Points Probability LR<2 LOW 0.122-6 MODERATE 1.90>6 HIGH 6.00

PRETEST PROBABILITYPRETEST PROBABILITY
Can docs really assess pretest probability?Can docs really assess pretest probability? while initial PIOPED study divided patients while initial PIOPED study divided patients
into low, moderate, and high probability with into low, moderate, and high probability with no clinical information, now algorithmsno clinical information, now algorithms
<10%, 11-60%, >60%<10%, 11-60%, >60%

Standardized Clinical Standardized Clinical AssessmentAssessment
Geneva score:clinical + ABG + CXRGeneva score:clinical + ABG + CXR Well Criteria: 6 clinical + alternate dxWell Criteria: 6 clinical + alternate dx Pisa-PED: Sx, ECG, CXR Pisa-PED: Sx, ECG, CXR Perrier: 8 clinical, ABG or CXR Perrier: 8 clinical, ABG or CXR
Clive Kearon. Clive Kearon. Diagnosis of pulmonary embolismDiagnosis of pulmonary embolism. . CMAJCMAJ: January 21, 2003; 168 (2): January 21, 2003; 168 (2)


Am J of Am J of Medicine Medicine 20022002

""Excuse Excuse
me. ... I know me. ... I know the game's the game's
almost over; almost over; but just for but just for the record, the record, I don't think I don't think my buzzer my buzzer
was working was working properlyproperly..
by Gary Larsonby Gary Larson

Quiz: Controversies galoreQuiz: Controversies galore
Age does not affect the d-dimerAge does not affect the d-dimer= = wrong: specificity 67% wrong: specificity 67% ≤ 50 yrs, 10% ≥80 yrs≤ 50 yrs, 10% ≥80 yrs
Specificity of D-dimer decreases after surgery Specificity of D-dimer decreases after surgery = = yes 7% inpatients vs 47% outptsyes 7% inpatients vs 47% outpts
Sensitivity of D-dimer decreases after 24 hrs of heparin Sensitivity of D-dimer decreases after 24 hrs of heparin = = yes 96% to 89%yes 96% to 89%
D-dimer is useful in high probability pts D-dimer is useful in high probability pts = = only 28% specificity compared with 54% in low clin prob. High only 28% specificity compared with 54% in low clin prob. High
prevalence of PE means lower NPV - only 77% (comp with 100%)prevalence of PE means lower NPV - only 77% (comp with 100%) Malignancy reduces the specificity of D-dimerMalignancy reduces the specificity of D-dimer
= = yes 48% vs 82%yes 48% vs 82%

All d-dimers are created equalAll d-dimers are created equal=Kovacs 2001: sensitivities SimpliRED, Accuclot and il-=Kovacs 2001: sensitivities SimpliRED, Accuclot and il-
Test were 79, 90 and 87% Test were 79, 90 and 87%
False negative D-dimers are more common in False negative D-dimers are more common in those with sub-segmental PEs those with sub-segmental PEs =true=true
The sensitivity of D-dimer increases if the clot has The sensitivity of D-dimer increases if the clot has been there >72 hrsbeen there >72 hrs=false, circulating T1/2 is 8hrs so if no new clot forming…=false, circulating T1/2 is 8hrs so if no new clot forming…

DIAGNOSIS: D-DIMERDIAGNOSIS: D-DIMER
Degree of elevation proportional to extent of Degree of elevation proportional to extent of PE (Kearon, CMAJ)PE (Kearon, CMAJ)
If high sensitivity then low specificity (40%) If high sensitivity then low specificity (40%) and high false + (53%) and high false + (53%)

Our testOur test
Calgary: Vidas rapid ELISA assayCalgary: Vidas rapid ELISA assay– Perrier Lancet 1999Perrier Lancet 1999– N=918 followed up for 3 months after non-invasive N=918 followed up for 3 months after non-invasive
protocolprotocol– Normal in 31% of consecutive outpts with suspected Normal in 31% of consecutive outpts with suspected
DVT/PE DVT/PE – For DVT: 99.3% NPV (97.5, 99.9%) Supposedly better For DVT: 99.3% NPV (97.5, 99.9%) Supposedly better
for PEfor PE– Negative predictive value of 100% for subsequent Negative predictive value of 100% for subsequent
symptomatic venous thromboembolism.symptomatic venous thromboembolism.

Low clinical prob and negative sensitive D-Low clinical prob and negative sensitive D-dimer = 99% negative predictive value for dimer = 99% negative predictive value for PEPE
Safe method of exclusion: Wells and de Safe method of exclusion: Wells and de GrootGroot
Non-diagnostic V/Q (<high) + neg D-dimer = Non-diagnostic V/Q (<high) + neg D-dimer = negative predictive value of 97% negative predictive value of 97% considered non-diagnostic esp if clinical considered non-diagnostic esp if clinical prob highprob high

DIAGNOSIS: BLOOD TESTSDIAGNOSIS: BLOOD TESTS
A-a gradient (Alveolar-arterial 02 gradient)A-a gradient (Alveolar-arterial 02 gradient)– gradient = PA02 - Pa02gradient = PA02 - Pa02– measure of gas exchangemeasure of gas exchange– [Fi02 (barometric pressure - 47 mm Hg)] - [1.25(PC02) - Pa02][Fi02 (barometric pressure - 47 mm Hg)] - [1.25(PC02) - Pa02]– normal limit = age/4 + 4 (NB: never zero because gas normal limit = age/4 + 4 (NB: never zero because gas
exchange is imperfect)exchange is imperfect)– normal A-a gradient and PC02 > 36 mmHg = 98% NPV for PEnormal A-a gradient and PC02 > 36 mmHg = 98% NPV for PE– very nonspecific (any pulmonary disease process can very nonspecific (any pulmonary disease process can
increase the A-a gradient)increase the A-a gradient)– patients with small PE’s usually have no change in the patients with small PE’s usually have no change in the
gradient other than that expected for agegradient other than that expected for age

Algorithm for suspected PE:Algorithm for suspected PE:Wells. Ann Int Med, 2001Wells. Ann Int Med, 2001
-PE exc luded
+
L owD -dim er
norm a lPE exc luded
L ow
PE exc luded
-
seria l U /S
+
M od D -dim er
seria l U /S
-
angiography
+
HighD -dim er
- D V Tcons ider PT P
+ D V T
non-diagnosticleg U/S
high probabi l i tytrea t for PE
V /Q
M od/HighD -dim er
PT P

Non -Invasive TestingNon -Invasive Testing
NEED TO Dx PE as HIGH MORTALITY IN NEED TO Dx PE as HIGH MORTALITY IN THOSE NOT Dx or MISDIAGNOSED!THOSE NOT Dx or MISDIAGNOSED!
Angiography carries riskAngiography carries risk Mortality 0.5%, invasive, labour intensiveMortality 0.5%, invasive, labour intensive Can make Dx without P. angioCan make Dx without P. angio
Clive Kearon. Clive Kearon. Diagnosis of pulmonary embolismDiagnosis of pulmonary embolism. . CMAJCMAJ: January 21, 2003; 168 (2): January 21, 2003; 168 (2)

DVT in PEDVT in PE
~75% of pts with PE have DVT: 2/3 prox ~75% of pts with PE have DVT: 2/3 prox veinsveins
Up to ¼ of pts with symptomatic PE have Up to ¼ of pts with symptomatic PE have clinical evidence of DVTclinical evidence of DVT
If less extensive PE then less likely to have If less extensive PE then less likely to have prox DVTprox DVT
Clive Kearon. Clive Kearon. Diagnosis of pulmonary embolismDiagnosis of pulmonary embolism. . CMAJCMAJ: January 21, 2003; 168 (2): January 21, 2003; 168 (2)

DIAGNOSIS: ULTRASOUNDDIAGNOSIS: ULTRASOUND
when a patient with known DVT has symptoms of when a patient with known DVT has symptoms of PE, further diagnosis of PE is not necessary as PE, further diagnosis of PE is not necessary as treatment is similartreatment is similar
therefore, lower extremity ultrasound does have a therefore, lower extremity ultrasound does have a role in the workup of patient with PE role in the workup of patient with PE
If it’s negative DON’T STOP: 40% still had PE If it’s negative DON’T STOP: 40% still had PE (Turkstra)(Turkstra)
AAFP: <50% have signs/sx in legs and in AAFP: <50% have signs/sx in legs and in (Turkstra) one study <30% had + doppler(Turkstra) one study <30% had + doppler

U/SU/S
+ venography ~75% sensitivity for PE+ venography ~75% sensitivity for PE + compression U/S ~50% sensitivity for PE+ compression U/S ~50% sensitivity for PE Among pts with nondiagnostic V/Q – U/S is + in Among pts with nondiagnostic V/Q – U/S is + in
5%5% Becomes + in 2% on repeat U/SBecomes + in 2% on repeat U/S Consider venography in pts who are more likely to Consider venography in pts who are more likely to
have a false-positive result have a false-positive result – Indeterminate U/SIndeterminate U/S– Previous DVT with potential for residual abNPrevious DVT with potential for residual abN– Negative D-dimerNegative D-dimer
(Kearon) (Kearon)

Remember…Remember…
50% of symptomatic PE = lobar / main pulm 50% of symptomatic PE = lobar / main pulm arteriesarteries
20 % are in subsegmental arteries (Kearon, 20 % are in subsegmental arteries (Kearon, CMAJ)CMAJ)

Quiz: V/QQuiz: V/Q
Age does not affect the accuracy of a lung scanAge does not affect the accuracy of a lung scan– Wrong: More non-diagnostic (58% Wrong: More non-diagnostic (58% ≥ 80 yrs) vs (32% ≤ ≥ 80 yrs) vs (32% ≤
40 yrs)40 yrs)
The proportion of non-diagnostic scans in COPDThe proportion of non-diagnostic scans in COPD==71%, 81%, 91%71%, 81%, 91%
Previous PE increases PPV of a high prob VQ Previous PE increases PPV of a high prob VQ scanscan= = no, decreases it from 91% to 74%no, decreases it from 91% to 74%

DIAGNOSIS: V/Q SCANDIAGNOSIS: V/Q SCAN perfusion scan:perfusion scan:
– injection of radiolabeled dye (Tc99) injection of radiolabeled dye (Tc99) – most information obtained from perfusion scanmost information obtained from perfusion scan
ventilation scan:ventilation scan:– inhalation of radiolabeled aerosol (Tc99 or Xe inhalation of radiolabeled aerosol (Tc99 or Xe
gas) gas) divided into normal, low, intermediate, and high divided into normal, low, intermediate, and high
probability based upon presence/absence of V/Q probability based upon presence/absence of V/Q mismatchmismatch
Perfusion defects are non-specific (~1/3 of defects Perfusion defects are non-specific (~1/3 of defects = PE) Increased probability of PE with increased = PE) Increased probability of PE with increased size & number, wedge shape, normal vent scan.size & number, wedge shape, normal vent scan.

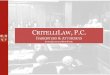
POSTTEST PROBABILITY OF PE WITH POSTTEST PROBABILITY OF PE WITH COMBINATION OF CLINICAL SUSPICION COMBINATION OF CLINICAL SUSPICION
AND V/Q SCANNING (PIOPED)AND V/Q SCANNING (PIOPED)
SCAN
NORMAL LOW INT. HIGH
HIGH ~ 40 66 96
MOD. 6 16 28 88
LOW 2 4 16 56
CLINICAL
PROB.

VQ scan (from EM rap)VQ scan (from EM rap)
MustMust be used with pre-test probability be used with pre-test probability Low pre-test + low prob VQ = low prob (1-2%)Low pre-test + low prob VQ = low prob (1-2%) High and high = (96%)High and high = (96%) Very useful if concordantVery useful if concordant Relatively low radiation and no dye loadRelatively low radiation and no dye load Poor accessability at night, sending them awayPoor accessability at night, sending them away Near useless in COPD/ CHF: indeterminateNear useless in COPD/ CHF: indeterminate More useful if normal CXR (otherwise consider More useful if normal CXR (otherwise consider
spiral CT)spiral CT)

If indeterminateIf indeterminate
High prob scans in ~50% of pts with PE and 10% of pts High prob scans in ~50% of pts with PE and 10% of pts tested for PE tested for PE
1/3 of pts tested for PE = N scans1/3 of pts tested for PE = N scans– therefore 65% of pts with suspected PE have intermediate or low therefore 65% of pts with suspected PE have intermediate or low
prob scansprob scans Continue on to pulmonary angiogram or another testContinue on to pulmonary angiogram or another test More likely that PE is in subsegmental pulmonary artery More likely that PE is in subsegmental pulmonary artery
(~20% of symptomatic PE)(~20% of symptomatic PE)
Consider the label of PE and further workups every time Consider the label of PE and further workups every time the pt is SOB, insurance problemsthe pt is SOB, insurance problems
6 mos 1% risk of signif bleeding over 1 yr6 mos 1% risk of signif bleeding over 1 yr

When the testing is indeterminateWhen the testing is indeterminate
Prevalence of PE of 20%Prevalence of PE of 20% Too high to ignore and too low to treat Too high to ignore and too low to treat
(although some would)(although some would) Can do pulm angiography OR U/SCan do pulm angiography OR U/S

Spiral CTSpiral CT

DIAGNOSIS: SPIRAL CTDIAGNOSIS: SPIRAL CT
more sensitive for large central than small more sensitive for large central than small peripheral/subsegmental (> 4th generation peripheral/subsegmental (> 4th generation vessels) emboli (86% vs. 63%)vessels) emboli (86% vs. 63%)
role in establishing diagnosis unclear at role in establishing diagnosis unclear at presentpresent– ? after V/Q scan and negative doppler ? after V/Q scan and negative doppler
U/SU/S– ? after V/Q scan? after V/Q scan– ? instead of V/Q scan? instead of V/Q scan

Diagnostic Imaging for PE:Diagnostic Imaging for PE:Spiral CTSpiral CT
Plain CT (without dye bolus and look at pulm Plain CT (without dye bolus and look at pulm vasculature) not sensitive at allvasculature) not sensitive at all
IV contrast, direct visualizationIV contrast, direct visualization subsegmental PE not well seensubsegmental PE not well seen more specific, underlying lung dxmore specific, underlying lung dx sens depends on CT, experiencesens depends on CT, experience wide variation in studieswide variation in studies
– De Monye Sens 69% spec 86%De Monye Sens 69% spec 86% Only 21% for subsegmental PEOnly 21% for subsegmental PE
– Rathbun. Ann Intern Med, 2000 (review)Rathbun. Ann Intern Med, 2000 (review) sens 53-100%, spec 81-100%sens 53-100%, spec 81-100%

Spiral CTSpiral CT
Perrier. Ann Intern Med, 2001Perrier. Ann Intern Med, 2001– sens 70%, spec 91% , 4% inconclusivesens 70%, spec 91% , 4% inconclusive– PE rate on F/U is <5% after N CT angio with + PE rate on F/U is <5% after N CT angio with +
D-dimerD-dimer– good interobserver agreementgood interobserver agreement
Combined results: Combined results: – sensitivity for subsegmental PE is ~30% sensitivity for subsegmental PE is ~30% – accounts for 20% of symptomatic PE accounts for 20% of symptomatic PE – = substantial risk of recurrence = substantial risk of recurrence – normal CT alone does not exclude PEnormal CT alone does not exclude PE– (Kearon)(Kearon)

Algorithms that incorporate helical CT Algorithms that incorporate helical CT require further validation.require further validation.
role? role? – no evidence to withhold Rx if CT negativeno evidence to withhold Rx if CT negative– Ability to reveal alternative pulmonary dxAbility to reveal alternative pulmonary dx– CT/ MRI may replace angiography CT/ MRI may replace angiography
CT venography:CT venography:– benefit over U/S not determined benefit over U/S not determined

EchoEcho
~50% of pts diagnosed with PE have echo ~50% of pts diagnosed with PE have echo evidence of right ventricular dysfunction at evidence of right ventricular dysfunction at presentation, presentation,
Marker of occult hemodynamic instabilityMarker of occult hemodynamic instability = associated with an elevated short-term = associated with an elevated short-term
mortality (Kearon, CMAJ)mortality (Kearon, CMAJ)

Diagnostic Imaging in PE:Diagnostic Imaging in PE:EchocardiographyEchocardiography
useful for patients in shock/arrest useful for patients in shock/arrest – r/o DDx: tamponade, Ao dissection, AMIr/o DDx: tamponade, Ao dissection, AMI
May see embolized thrombi in R heart or central May see embolized thrombi in R heart or central pulm arteriespulm arteries
indirect evidence of PE:indirect evidence of PE:– RV overload, septal shift to L, TR, RV overload, septal shift to L, TR, PA pressure, RV PA pressure, RV
wall motion abn wall motion abn – Sensitivity ~50% and specificity ~90% for PESensitivity ~50% and specificity ~90% for PE
Because of low sensitivity = not suitable as routine Because of low sensitivity = not suitable as routine diagnostic testdiagnostic test

Diagnostic Imaging in PE:Diagnostic Imaging in PE:EchocardiographyEchocardiography
useful for patients in shock/arrest useful for patients in shock/arrest – r/o DDx: tamponade, Ao dissection, AMIr/o DDx: tamponade, Ao dissection, AMI
indirect evidence of PE:indirect evidence of PE:– RV overload, septal shift to L, TR, RV overload, septal shift to L, TR, PA PA
pressure, RV wall motion abn pressure, RV wall motion abn
‘‘sub-massive’ PE: independent predictor of sub-massive’ PE: independent predictor of mortality (?significance)mortality (?significance)


Diagnostic Imaging for PE:Diagnostic Imaging for PE:Pulmonary AngiographyPulmonary Angiography
Gold standard (imperfect)Gold standard (imperfect)– sens 98%, spec 95-98%sens 98%, spec 95-98%
pigtail catheter inserted into the R and L pigtail catheter inserted into the R and L pulmonary arteries (as well as their pulmonary arteries (as well as their branches) with injection of contrast dyebranches) with injection of contrast dye
Can be prelude to catheter fragmentation to Can be prelude to catheter fragmentation to reduce clot burden.reduce clot burden.

DIAGNOSIS: PULMONARY ANGIOGRAMDIAGNOSIS: PULMONARY ANGIOGRAM
Angiography preferred when:Angiography preferred when:– Segmental intraluminal filling defect on helical Segmental intraluminal filling defect on helical
CTCT– Subsegmental intraluminal filling defect on Subsegmental intraluminal filling defect on
helical CT and high clinical prob of PEhelical CT and high clinical prob of PE– High prob V/Q scan and low clinical suspicionHigh prob V/Q scan and low clinical suspicion– Serial testing not feasible (eg, pts scheduled for Serial testing not feasible (eg, pts scheduled for
surgery or geographic inaccessibility)surgery or geographic inaccessibility) Otherwise consider serial U/SOtherwise consider serial U/S

DIAGNOSIS: PULMONARY ANGIOGRAMDIAGNOSIS: PULMONARY ANGIOGRAM
ED physicians reluctant to use:ED physicians reluctant to use:– invasive, risks (0.5% mortality), requires expertise, not invasive, risks (0.5% mortality), requires expertise, not
readily available, time consuming, $, contra-indicated in readily available, time consuming, $, contra-indicated in renal impairment (1% renal failure)renal impairment (1% renal failure)
Limitations:Limitations:– difficult to diagnose emboli in 3rd order (lobular) or difficult to diagnose emboli in 3rd order (lobular) or
smaller arteries smaller arteries smaller emboli are the precursors to massive PEsmaller emboli are the precursors to massive PE
– false positives with intraluminal tumors or extrinsic false positives with intraluminal tumors or extrinsic massesmasses
– 0.5-1% mortality (anaphylactoid reactions, 0.5-1% mortality (anaphylactoid reactions, dysrhythmias, cardiac arrest, endocardial dysrhythmias, cardiac arrest, endocardial injury/perforation)injury/perforation)
~1% with N angiogram have PE w/i a few mos ~1% with N angiogram have PE w/i a few mos (Tintinalli)(Tintinalli)

LOW PROBABILITY PE:
D-Dimer
Neg Positive
STOP VQ Scan
Normal
STOP
Non-high High
CUS legs
Normal DVT
Pulm Angio
NormalPositive
CUSIn 1 week
TREAT STOP TREAT

MODERATE PROBABILITY PE:
D-Dimer
Neg Positive
STOP VQ Scan
Normal Non-high High
CUS legs
Normal DVT
CUSIn 1 week
TREAT
TREAT
Pulm AngioOR

HIGH PROBABILITY PE:
VQ Scan
Normal Non-high High
CUS legs
Normal DVT
CUSIn 1 week
TREAT
TREAT
Pulm Angio OR
Pulm Angio OR OR Pulm Angio

Clive Kearon. Clive Kearon. Diagnosis of Diagnosis of pulmonary pulmonary embolismembolism. . CMAJCMAJ: : January 21, 2003; January 21, 2003; 168 (2)168 (2)

Some numbersSome numbers Low PTP + neg D-dimer = NPV of 99-100%Low PTP + neg D-dimer = NPV of 99-100%
Non-diagnostic scan + negative D-dimer + normal U/S = NPV 98%Non-diagnostic scan + negative D-dimer + normal U/S = NPV 98%
Non-diagnositic lung scan + negative D-dimer = NPV of 97 % (keep Non-diagnositic lung scan + negative D-dimer = NPV of 97 % (keep going)going)
Non-diagnostic scan + normal U/S = NPV 95%Non-diagnostic scan + normal U/S = NPV 95% There is evidence that pts with these results have a low (<2% risk of There is evidence that pts with these results have a low (<2% risk of
presenting with symptomatic venous thromboembolism during follow presenting with symptomatic venous thromboembolism during follow up)up)
Some will still choose to do serial testing anywaySome will still choose to do serial testing anyway

Algorithm for suspected PE:Algorithm for suspected PE:Wells. Ann Int Med, 2001Wells. Ann Int Med, 2001
-PE exc luded
+
L owD -dim er
norm a lPE exc luded
L ow
PE exc luded
-
seria l U /S
+
M od D -dim er
seria l U /S
-
angiography
+
HighD -dim er
- D V Tcons ider PT P
+ D V T
non-diagnosticleg U/S
high probabi l i tytrea t for PE
V /Q
M od/HighD -dim er
PT P

Wells’ Algorithm:Wells’ Algorithm:CriticismCriticism
Uses SimpliRED assay: lower sens.Uses SimpliRED assay: lower sens.– NPV for clinical prob + D-dimer = 99.5% NPV for clinical prob + D-dimer = 99.5%
(99.1%-100%)(99.1%-100%)
spiral CT not includedspiral CT not included– could replace angiography?could replace angiography?
Low prevalence of PE (9%)Low prevalence of PE (9%) not validated by other RCTsnot validated by other RCTs

Angio or CT if low prob
Venography/CT if high susp, severe sx or
poor cardiopulm reserve
+/- venography
If CT instead, stop if large Pulm A
or segmental


Treatment GoalsTreatment Goals
reduce mortalityreduce mortality prevent extension/recurrenceprevent extension/recurrence restore pulmonary vascular resistancerestore pulmonary vascular resistance prevent pulmonary hypertensionprevent pulmonary hypertension

TreatmentTreatment
Without tx, ~50% of symptomatic prox DVT or PE Without tx, ~50% of symptomatic prox DVT or PE are expected to have recurrent venous are expected to have recurrent venous thromboembolism within 3 mos.thromboembolism within 3 mos.
With tx of PE, ~50% resolution of perfusion With tx of PE, ~50% resolution of perfusion defects is expected after 2-4 wks. defects is expected after 2-4 wks.
Eventually , complete resolution of PE expected in Eventually , complete resolution of PE expected in ~2/3 of pts. (Kearon , CMAJ)~2/3 of pts. (Kearon , CMAJ)
Significant long-term nonresolution of emboli Significant long-term nonresolution of emboli causing pulmonary HTN or cardiopulmonary causing pulmonary HTN or cardiopulmonary symptoms uncommonsymptoms uncommon

Treatment (from EMrap)Treatment (from EMrap)
IV heparin – use weight-based protocolIV heparin – use weight-based protocol 5000 U bolus (80 U/kg) and then 1280 U/hr 5000 U bolus (80 U/kg) and then 1280 U/hr
(18 U/kg/hr) drip for average 70 kg man (18 U/kg/hr) drip for average 70 kg man MaxMax = 40,000 /day and 15,000 bolus = 40,000 /day and 15,000 bolus
(EMrap)(EMrap) Start coumadin on day 1 if VTE confirmedStart coumadin on day 1 if VTE confirmed

TREATMENTTREATMENT
heparin (UFH or LMWH) X 4-5 daysheparin (UFH or LMWH) X 4-5 days– currently IV UFH is still used locally for initial currently IV UFH is still used locally for initial
treatmenttreatment

Treatment of VTE:Treatment of VTE:AnticoagulationAnticoagulation
Out-patient LMWHOut-patient LMWH LMWH superior to UFH? LMWH superior to UFH? (Gould 1999)(Gould 1999)
out-pt Rx safe in PE (out-pt Rx safe in PE (Kovacs, 2000)Kovacs, 2000)
DVT: start Rx, definitive test in 24hr DVT: start Rx, definitive test in 24hr baseline B/Wbaseline B/W

LMWH (EM rap)LMWH (EM rap)
No lab monitoring, decreased hospitalization and No lab monitoring, decreased hospitalization and complication for DVTcomplication for DVT
Approved for documented DVT + PEApproved for documented DVT + PE 1 mg/kg BID Enoxaparin1 mg/kg BID Enoxaparin Dalteparin and TinzaparinDalteparin and Tinzaparin Arch of Int Med 2000 PE txArch of Int Med 2000 PE tx Lower recurrence risk of PE and lower rates of Lower recurrence risk of PE and lower rates of
major bleedingmajor bleeding With LMWH as initial tx and oral anticoagulation With LMWH as initial tx and oral anticoagulation
for INR of 2-3, rate of major bleeding at 3 mos is for INR of 2-3, rate of major bleeding at 3 mos is ≤3% and mortality is ≤0.5% (BTS)≤3% and mortality is ≤0.5% (BTS)

1) Can LMWH alone be given from the start 1) Can LMWH alone be given from the start or do you need a bolus of UFH (most or do you need a bolus of UFH (most studies)studies)
2) Are the various LMWHs equivalent?2) Are the various LMWHs equivalent?

AnticoagulationAnticoagulation
Enoxaparin 1mg/kg bid or 1.5 odEnoxaparin 1mg/kg bid or 1.5 od Tinzaparin 175 anti-Xa u/kg odTinzaparin 175 anti-Xa u/kg od start warfarin 5mg on day 1start warfarin 5mg on day 1 d/c LMWH when INR >2.0 x 2 daysd/c LMWH when INR >2.0 x 2 days Rx 3 mos if 1st and reversible causeRx 3 mos if 1st and reversible cause 6 mos if non-reversbile6 mos if non-reversbile indefinite if recurrent, CA, geneticindefinite if recurrent, CA, genetic

SPECIAL CONSIDERATIONSSPECIAL CONSIDERATIONS
““One shot heparin and imaging in the One shot heparin and imaging in the morning”morning”– after hours DI difficult to obtainafter hours DI difficult to obtain– safety of single dose LMWH with U/S the next safety of single dose LMWH with U/S the next
day established and now common practice day established and now common practice (Bauld et al. Am J Emerg Med 1999: 17: 11-15)(Bauld et al. Am J Emerg Med 1999: 17: 11-15) the above study looked at 128 patients, 44 + test, 84 the above study looked at 128 patients, 44 + test, 84
neg neg Followed for 3 months after dalteparinFollowed for 3 months after dalteparin No serious adverse effectsNo serious adverse effects
Bauld DL, Kovacs MJ. Dalteparin in Emergency Patients to Prevent Bauld DL, Kovacs MJ. Dalteparin in Emergency Patients to Prevent Admission Prior to Investigation for Venous Thromboembolism. American Admission Prior to Investigation for Venous Thromboembolism. American Journal of Emergency Medicine. 1999; 17 (1): 11-14Journal of Emergency Medicine. 1999; 17 (1): 11-14

Treatment of PE:Treatment of PE:Criteria for admissionCriteria for admission
Hemodynamic instabilityHemodynamic instability O2 requirementO2 requirement surgery < 48hrsurgery < 48hr risk of active bleedingrisk of active bleeding history of HIThistory of HIT IV pain controlIV pain control

THROMBOLYTICSTHROMBOLYTICS
indications:indications:– shock/hemodynamic instabilityshock/hemodynamic instability– exhausted cardiopulmonary reserveexhausted cardiopulmonary reserve
hypoxemia or hypotensionhypoxemia or hypotension severe comorbid illnesses (prev. lobectomy, severe comorbid illnesses (prev. lobectomy,
cardiomyopathy, other cardiopulm. disease)cardiomyopathy, other cardiopulm. disease)
– high likelihood of recurrence high likelihood of recurrence helps prevent chronic cor pulmonale from recurrent helps prevent chronic cor pulmonale from recurrent
emboli with incomplete recanalizationemboli with incomplete recanalization

ThrombolyticsThrombolytics
no evidence of mortality benefitno evidence of mortality benefit– including in cardiac arrest (case series)including in cardiac arrest (case series)
No benefit of intrapulm infusionNo benefit of intrapulm infusion protocols:protocols:
– t-PA: 100mg over 2 hrt-PA: 100mg over 2 hr– SK: 250,000U over 30min; 100,000 x 24hSK: 250,000U over 30min; 100,000 x 24h– (UK: 4400U/kg over 10min; rpt x 12-24hr)(UK: 4400U/kg over 10min; rpt x 12-24hr)– arrest: t-PA 10mg/kg bolus x 2 q 30 minarrest: t-PA 10mg/kg bolus x 2 q 30 min

Treatment of massive PE:Treatment of massive PE:ThrombolyticsThrombolytics
no benefit in hemodynamically stableno benefit in hemodynamically stable– Including those with RV dysfunction on echo Including those with RV dysfunction on echo
(evidence not there yet)(evidence not there yet)
5-10% major bleed, 1-2% ICH5-10% major bleed, 1-2% ICH

EmbolectomyEmbolectomy
Indicated in acute, massive PE if:Indicated in acute, massive PE if:– contraindication to thrombolyticscontraindication to thrombolytics– unresponsive to medical mgt – sustained unresponsive to medical mgt – sustained
hypotensionhypotension
moribund pt moribund pt poor results poor results no evidence cf. with thrombolyticsno evidence cf. with thrombolytics percutaneous vs. surgicalpercutaneous vs. surgical
– ?role?role

IVC FiltersIVC Filters
Indications:Indications:– contraindication to anticoagulationcontraindication to anticoagulation– recurrent VTE despite anticoagulationrecurrent VTE despite anticoagulation– after surgical embolectomyafter surgical embolectomy
no long term adv vs. anticoagulationno long term adv vs. anticoagulation anticoagulate if no contraindicationsanticoagulate if no contraindications Decousus 1998: RCT for prox DVT Decousus 1998: RCT for prox DVT
– Not good:Not good:– Effective for the first 12 days but no improvement in Effective for the first 12 days but no improvement in
short or long term mortalityshort or long term mortality– At 2 yrs, the recurrence of DVT greater in the IVC groupAt 2 yrs, the recurrence of DVT greater in the IVC group

What if?What if?
50 yo pt diagnosed 2 weeks ago with 50 yo pt diagnosed 2 weeks ago with DVT/PE and has been on warfarinDVT/PE and has been on warfarin
Returns today with palpitationsReturns today with palpitations ?? Check INR, HR, sat, leg-swelling, Check INR, HR, sat, leg-swelling, Ask re: dyspnea, hemoptysisAsk re: dyspnea, hemoptysis In general, do the test that proved the VTE In general, do the test that proved the VTE
the first time (U/S and IPG may be false +)the first time (U/S and IPG may be false +)

What if?What if?
450 lb male with pleuritic chest pain and 450 lb male with pleuritic chest pain and dyspneadyspnea
?? May be too large for CT/ VQ/ MRIMay be too large for CT/ VQ/ MRI D-dimer, U/S, look for alternate dxD-dimer, U/S, look for alternate dx Consider empiric anticoagulationConsider empiric anticoagulation No good evidence for thisNo good evidence for this Difficult to dose LMWH, some docs exceed Difficult to dose LMWH, some docs exceed
recommended limit.recommended limit.

What if?What if?
30 yo 330 yo 3rdrd trimester woman with pleuritic CP trimester woman with pleuritic CP What considerations?What considerations?

PregnancyPregnancy
Modifications:Modifications: D-dimer D-dimer in pregnancy in pregnancy Start with U/S: if + then tx Start with U/S: if + then tx
– gravid uterus compresses the IVC, thereby gravid uterus compresses the IVC, thereby changing Doppler flow in the lower extremities. changing Doppler flow in the lower extremities.
V/Q safe, no breastfeed x 15hr postV/Q safe, no breastfeed x 15hr post If angiography use brachial approach with If angiography use brachial approach with
abd screenabd screen No safety data for spiral CT – try to avoidNo safety data for spiral CT – try to avoid

DIAGNOSIS: V/Q SCANDIAGNOSIS: V/Q SCAN
radiation from complete scan = 50 mrad (5 chest X-rays) most radiation from complete scan = 50 mrad (5 chest X-rays) most of which comes from ventilation scanof which comes from ventilation scan
toxic dose of radiation for a fetus ~ 5 radtoxic dose of radiation for a fetus ~ 5 rad in pregnancy, modifications include: in pregnancy, modifications include:
– full V/Q scan with different radiolabeling agent (sulfur colloid) full V/Q scan with different radiolabeling agent (sulfur colloid) for ventilation scan to decrease fetal absorption (preferred for ventilation scan to decrease fetal absorption (preferred regimen in Calgary)regimen in Calgary)
– full dose perfusion scan with ventilation scan as needed the full dose perfusion scan with ventilation scan as needed the following day (if normal perfusion scan, no need to persist following day (if normal perfusion scan, no need to persist with ventilation scan)with ventilation scan)
– 1/2 dose perfusion scan followed by same day 1/2 dose 1/2 dose perfusion scan followed by same day 1/2 dose ventilation scan (results in grainy images)ventilation scan (results in grainy images)

PregnancyPregnancy
MRI helpfulMRI helpful Risk of inaccurate dx of PE in pregnancy exceeds Risk of inaccurate dx of PE in pregnancy exceeds
the risk of radiation exposure with dx testing.the risk of radiation exposure with dx testing. LMWH in DVT, not studied in PELMWH in DVT, not studied in PE PE: UFH IV x 4-5 days, then s/cPE: UFH IV x 4-5 days, then s/c treat x 3 months or 6 weeks postpartum treat x 3 months or 6 weeks postpartum
(whichever is longer)(whichever is longer) switch to oral postpartum (OK for breastfeeding)switch to oral postpartum (OK for breastfeeding)

The end – Questions?The end – Questions?

Thanks to…Thanks to…
Rhonda NessRhonda Ness Rob Hall for interesting Rob Hall for interesting
questionsquestions Slides from Denise Slides from Denise
Watt, Mark Yarema, Watt, Mark Yarema, Tony ChadTony Chad

ReferencesReferences Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? JAMA 1998; 279: 1094-Anand SS, Wells PS, Hunt D et al. Does This Patient Have Deep Vein Thrombosis? JAMA 1998; 279: 1094-
1099.1099. Ault M. Ault M. Upper Extremity DVT: What Is the Risk?Upper Extremity DVT: What Is the Risk? Arch Intern Med. 1998 Sep 28;158(17):1950-2.Arch Intern Med. 1998 Sep 28;158(17):1950-2. Bauld DL, Kovacs MJ. Dalteparin in Emergency Patients to Prevent Admission Prior to Investigation for Bauld DL, Kovacs MJ. Dalteparin in Emergency Patients to Prevent Admission Prior to Investigation for
Venous Thromboembolism. American Journal of Emergency Medicine. 1999; 17 (1): 11-14Venous Thromboembolism. American Journal of Emergency Medicine. 1999; 17 (1): 11-14 British Thoracic Society Standards of Care Committee Pulmonary Embolism Guideline Development Group. British Thoracic Society Standards of Care Committee Pulmonary Embolism Guideline Development Group.
British Thoracic Society guidelines for the management of suspected acute pulmonary embolism. Thorax British Thoracic Society guidelines for the management of suspected acute pulmonary embolism. Thorax 2003; 58: 470-484.2003; 58: 470-484.
Chagnon I, Bounameaux H, Aujesky D, et al. Comparison of Two Clinical Prediction Rules and implicit Chagnon I, Bounameaux H, Aujesky D, et al. Comparison of Two Clinical Prediction Rules and implicit Assessment among Patients with Suspected Pulmonary Embolism. Am J of Med.2002 113: 269-275.Assessment among Patients with Suspected Pulmonary Embolism. Am J of Med.2002 113: 269-275.
Colucciello SA. Protocols for Deep Venous Thrombosis (DVT): A State-of-the-Art Review Part I: Risk Factor Assessment, Physical Examination, and Current Diagnostic Modalities. www.EMR online
Davidson BL. Davidson BL. Controversies in Pulmonary Embolism and Deep Venous ThrombosisControversies in Pulmonary Embolism and Deep Venous Thrombosis . . AAFP Nov 1999 AAFP Nov 1999 Virginia Mason Medical Center, Seattle, Washington Virginia Mason Medical Center, Seattle, Washington
Decousus H, Leizorovicz A, Parent F et al. A clinical trial of vena caval filters in the prevention of pulmonary Decousus H, Leizorovicz A, Parent F et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. N Engl J med 1998; 338:409-15.embolism in patients with proximal deep-vein thrombosis. N Engl J med 1998; 338:409-15.
Gould MK, Dembitzer AD, Anders GD et al. Low-Molecular-Weight Heparins Compared with Unfractionated Gould MK, Dembitzer AD, Anders GD et al. Low-Molecular-Weight Heparins Compared with Unfractionated Heparin for Treatment of Acute Deep Venous Thrombosis: A Cost-Effectiveness Analysis. Annals of Internal Heparin for Treatment of Acute Deep Venous Thrombosis: A Cost-Effectiveness Analysis. Annals of Internal Medicine 1999; 130 (10): 789-799Medicine 1999; 130 (10): 789-799
Gould MK, Dembitzer AD, Doyle RL et al. Low-Molecular-Weight Heparins Compared with Unfractionated Gould MK, Dembitzer AD, Doyle RL et al. Low-Molecular-Weight Heparins Compared with Unfractionated Heparin for Treatment of Acute Deep Venous Thrombosis: A Meta-Analysis of Randomized, Controlled Heparin for Treatment of Acute Deep Venous Thrombosis: A Meta-Analysis of Randomized, Controlled Trials. Ann Intern Med. 1999; 130:800-809.Trials. Ann Intern Med. 1999; 130:800-809.

More referencesMore references Kearon C. Diagnosis of pulmonary embolism. Kearon C. Diagnosis of pulmonary embolism. CMAJCMAJ: January 21, 2003; 168: January 21, 2003; 168 Kovacs MJ, MacKinnon KM, Anderson D, et al. A comparison of three rapid D-dimer methods for the Kovacs MJ, MacKinnon KM, Anderson D, et al. A comparison of three rapid D-dimer methods for the
diagnosis of venous thromboembolism. British Journal of Haemoatology 2001. 115: 140-144. diagnosis of venous thromboembolism. British Journal of Haemoatology 2001. 115: 140-144. Mustafa BO, MD; Rathbun SW, MD; Whitsett TL, MD. Sensitivity and Specificity of Ultrasonography Mustafa BO, MD; Rathbun SW, MD; Whitsett TL, MD. Sensitivity and Specificity of Ultrasonography
in the Diagnosis of Upper Extremity Deep Vein Thrombosis: A Systematic Review Arch Int Med 2002 in the Diagnosis of Upper Extremity Deep Vein Thrombosis: A Systematic Review Arch Int Med 2002 162(4)401162(4)401
Niemann JT. Diagnostic Accuracy of a Bedside D-Dimer Assay and Alveolar Dead-Space Measurement for Rapid Exclusion of Pulmonary Embolism: A Multicenter Study. Annals of Emergency Medicine. 2001; 38 (6)
Perrier A, Desmarais S, Miron M-J et al. Non-invasive diagnosis of venous thromboembolism in Perrier A, Desmarais S, Miron M-J et al. Non-invasive diagnosis of venous thromboembolism in outpatients. Lancet 1999. 353: 190-195.outpatients. Lancet 1999. 353: 190-195.
PIOPED investigators. Value of the Ventilation/Perfusion Scan in Acute Pulmonary Embolism: PIOPED investigators. Value of the Ventilation/Perfusion Scan in Acute Pulmonary Embolism: Results of the Prospective Investigation of Pulmonary Embolism Diagnosis. JAMA 1990; 263(20): Results of the Prospective Investigation of Pulmonary Embolism Diagnosis. JAMA 1990; 263(20): 2753-2759.2753-2759.
Prandoni P, Polistena P, Bernardi E, et al Upper-extremity deep vein thrombosis. Risk factors, Prandoni P, Polistena P, Bernardi E, et al Upper-extremity deep vein thrombosis. Risk factors, diagnosis, and complications. Arch Intern Med. 1998 Sep 28;158(17):1950-2.diagnosis, and complications. Arch Intern Med. 1998 Sep 28;158(17):1950-2.
Prandoni P, Polistena P, Bernardi E, et al. Upper-extremity deep vein thrombosis. Prandoni P, Polistena P, Bernardi E, et al. Upper-extremity deep vein thrombosis. Arch Intern Med.Arch Intern Med. 1997;157:57-62. 1997;157:57-62.
Randolph AG, Cook DJ, Gonzales CA. Benefit of Heparin in Central Venous and Pulmonary Artery Randolph AG, Cook DJ, Gonzales CA. Benefit of Heparin in Central Venous and Pulmonary Artery Catheters. Chest 1998;113:165-171.Catheters. Chest 1998;113:165-171.
Tintinalli JE, Kelen GD, Stapczynski JS. Emergency Medicine: A comprehensive Study Guide. Tintinalli JE, Kelen GD, Stapczynski JS. Emergency Medicine: A comprehensive Study Guide. 2004. 410-415, 386-3932004. 410-415, 386-393
Wells PS, Anderson DR, Rodger M et al. Excluding Pulmonary Embolism at the Bedside without Wells PS, Anderson DR, Rodger M et al. Excluding Pulmonary Embolism at the Bedside without Diagnostic Imaging: Management of Patients with Suspected Pulmonary Embolism Presenting to the Diagnostic Imaging: Management of Patients with Suspected Pulmonary Embolism Presenting to the Emergency Department by Using a Simple Clinical Model and D-Dimer. Annals of Int Med. 2001. Emergency Department by Using a Simple Clinical Model and D-Dimer. Annals of Int Med. 2001. 135 (2): 87-107135 (2): 87-107
http://images.google.ca/imgres?imgurl=www.physweekly.com/pictshttp://images.google.ca/imgres?imgurl=www.physweekly.com/picts