Embed Size (px)
Citation preview
IMPROVING CARE TRANSITIONS IN NORTHWEST DENVER
Risa Hayes, CPC
Program Manager, CFMC
Integrating Care for Populations and Communities
ARC Learning Session
February 23, 2012
This material was prepared by CFMC (PM-4010-058 CO 2012), the Medicare Quality Improvement Organization for Colorado under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human
Services. The contents presented do not necessarily reflect CMS policy.
( )
Our Equation
Readmissions
and
Admissions
( ) 2

3
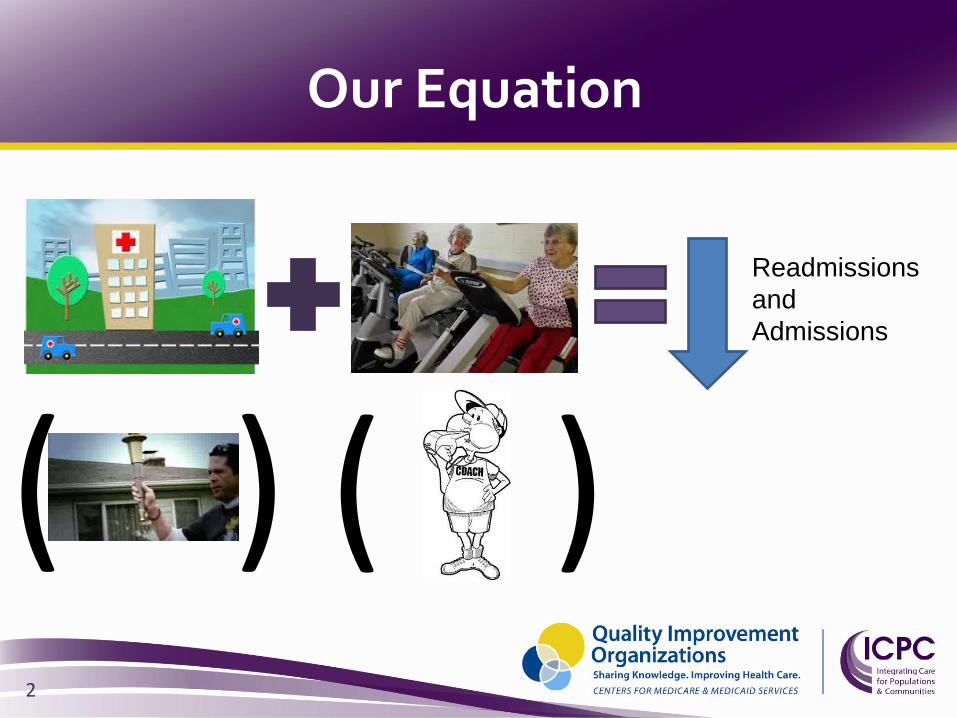
So What is a “Community”?
• The Medicare population that you serve and share with your partners and competitors
• Specified set of zip codes, in which the people you serve live
4

Who is the Community?
• Acute Care Hospitals
• LTACs
• SNFs
• Home Health Agencies
• Non-medical Home Care companies
• Senior Resource Centers
• Physician Offices
• Patient Advocates
• Hospice providers
• Palliative Care providers
• Medical Society
• Mental Health
• AAA
• QIO
• Hospitalists
• Physician management group
5
Why are people readmitted?
No community infrastructure for achieving common goals
Provider-Patient interface Unmanaged condition worsening
Use of suboptimal medication regimens Return to an emergency department
Unreliable system support Lack of standard and known processes Unreliable information transfer Unsupported patient activation during transfers
6
The Project
Goal:
• Improve care transitions for Medicare beneficiaries in 44 zip codes in NW Denver
• As evidenced by:
– 2% reduction in 30 day all-cause readmission rate
What we did:
Community Action Teams
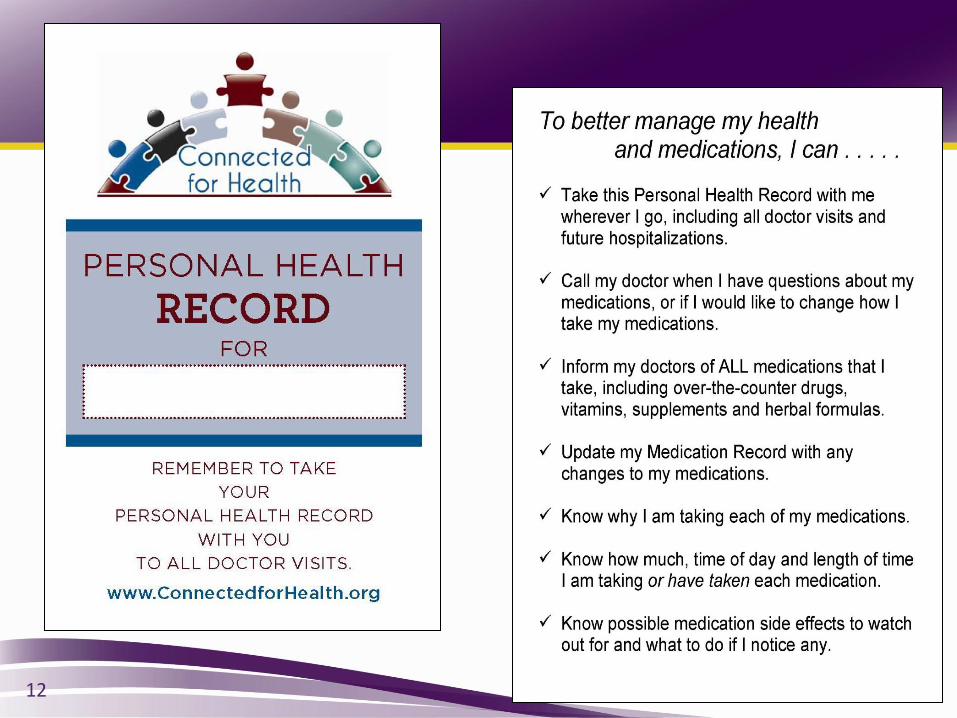
• Standardized Community PHR
• Post-acute Care Options Tool
Coaching
• PAM®-tailored CTISM
• Volunteer Advocates
7
Community-Specific Root Cause Analysis
• Data Analysis • Readmissions by admit source
• Rates by diagnosis
• Process Mapping • Clip board & stop watch
• Process flow – is it standardized or “it depends”
• Chart Reviews
• Patient/Stakeholder feedback • 10 interviews – open ended questions
8
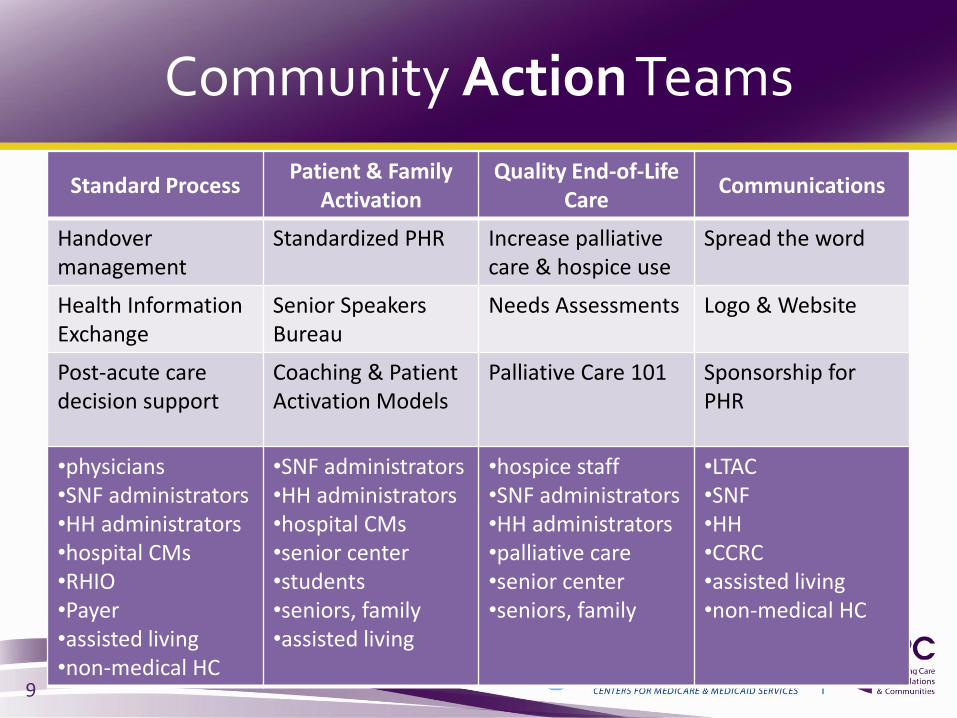
Community Action Teams
Standard Process Patient & Family
Activation Quality End-of-Life
Care Communications
Handover management
Standardized PHR Increase palliative care & hospice use
Spread the word
Health Information Exchange
Senior Speakers Bureau
Needs Assessments Logo & Website
Post-acute care decision support
Coaching & Patient Activation Models
Palliative Care 101
Sponsorship for PHR
•physicians •SNF administrators •HH administrators •hospital CMs •RHIO •Payer •assisted living •non-medical HC
•SNF administrators •HH administrators •hospital CMs •senior center •students •seniors, family •assisted living
•hospice staff •SNF administrators •HH administrators •palliative care •senior center •seniors, family
•LTAC •SNF •HH •CCRC •assisted living •non-medical HC
9

10
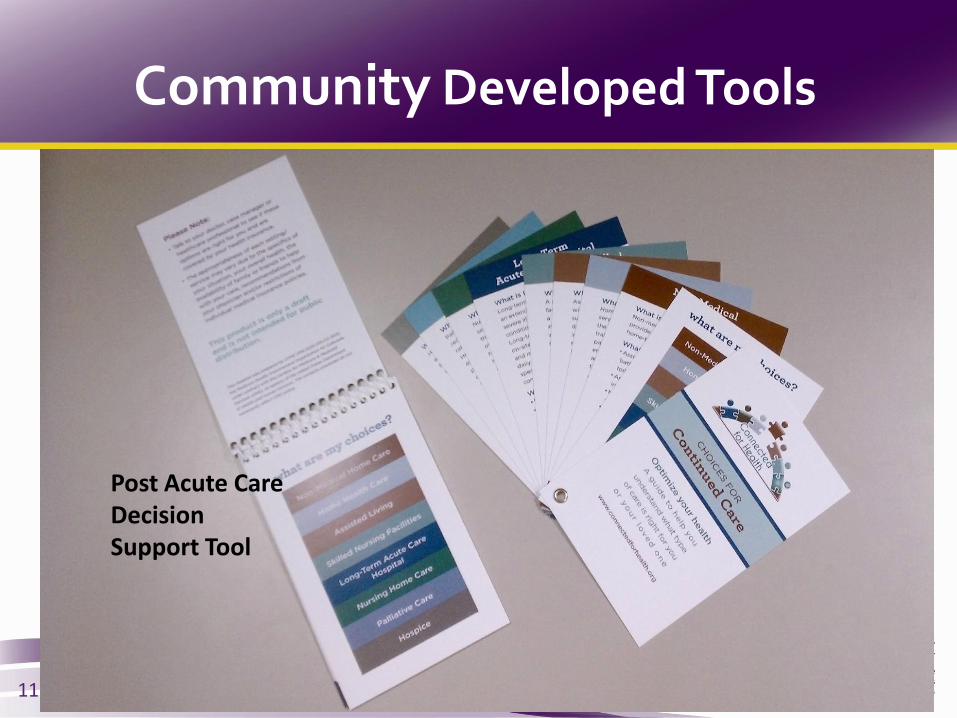
Community Developed Tools
Post Acute Care Decision Support Tool
11
12

Community Unity
• A true NW
Denver Partnership
• Involved a large group of community providers
• 21,000 printed copies
• Available online for future use
13
POWER OVER
14
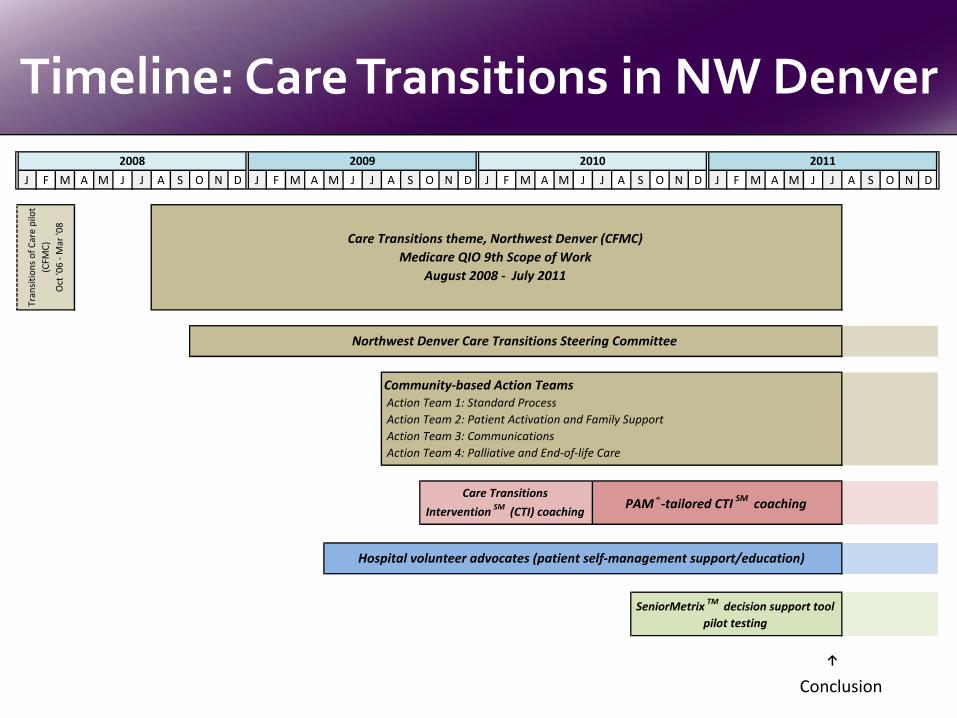
Timeline: Care Transitions in NW Denver
15
J F M A M J J A S O N D J F M A M J J A S O N D J F M A M J J A S O N D J F M A M J J A S O N D
↑
now
SeniorMetrix TM decision support tool
pilot testing
Tran
siti
on
s o
f C
are
pilo
t
(CFM
C)
Oct
'06
- M
ar '0
8
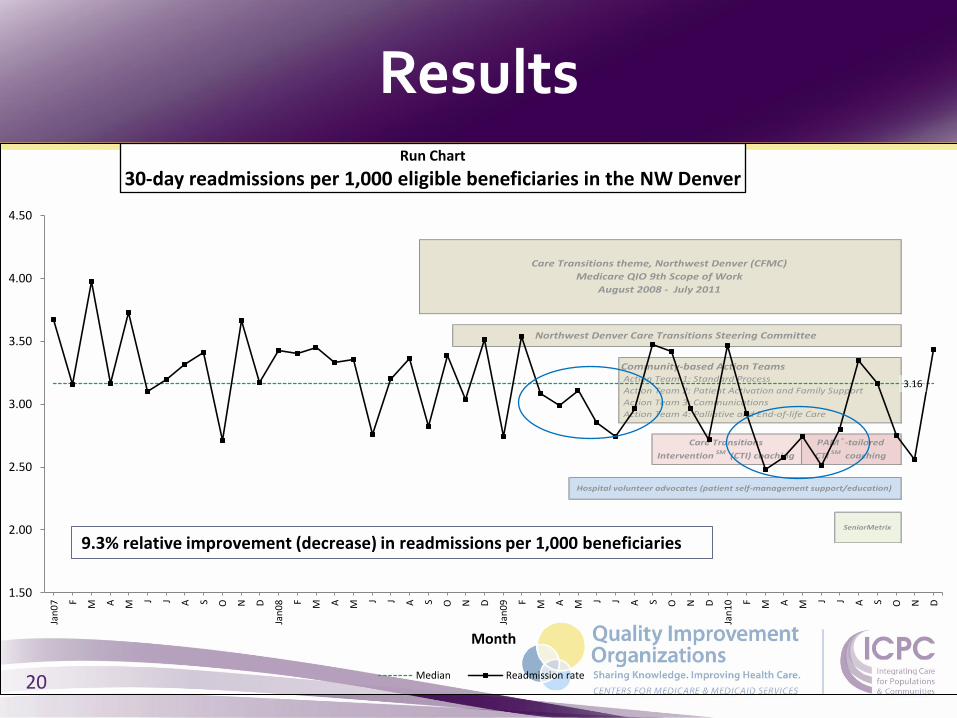
Northwest Denver Care Transitions Steering Committee
PAM®-tailored CTI SM coachingCare Transitions
Intervention SM (CTI) coaching
Hospital volunteer advocates (patient self-management support/education)
Community-based Action Teams Action Team 1: Standard Process
Action Team 2: Patient Activation and Family Support
Action Team 3: Communications
Action Team 4: Palliative and End-of-life Care
2008 2009 2010 2011
Care Transitions theme, Northwest Denver (CFMC)
Medicare QIO 9th Scope of Work
August 2008 - July 2011
Conclusion
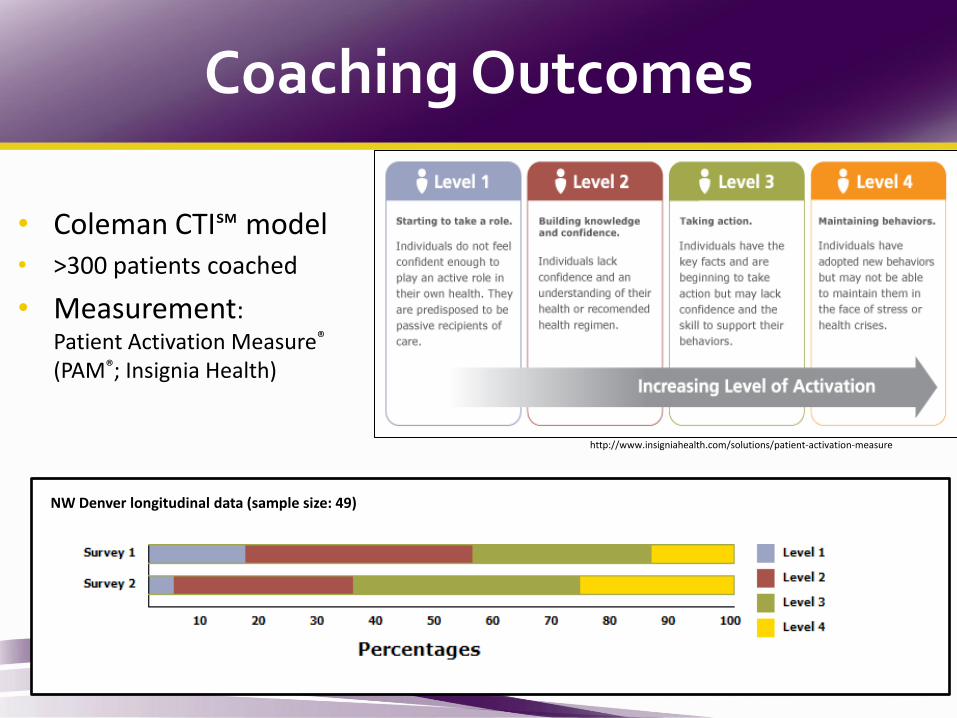
Coaching Outcomes
16
• Coleman CTI℠ model
• >300 patients coached
• Measurement: Patient Activation Measure® (PAM®; Insignia Health)
NW Denver longitudinal data (sample size: 49)
http://www.insigniahealth.com/solutions/patient-activation-measure
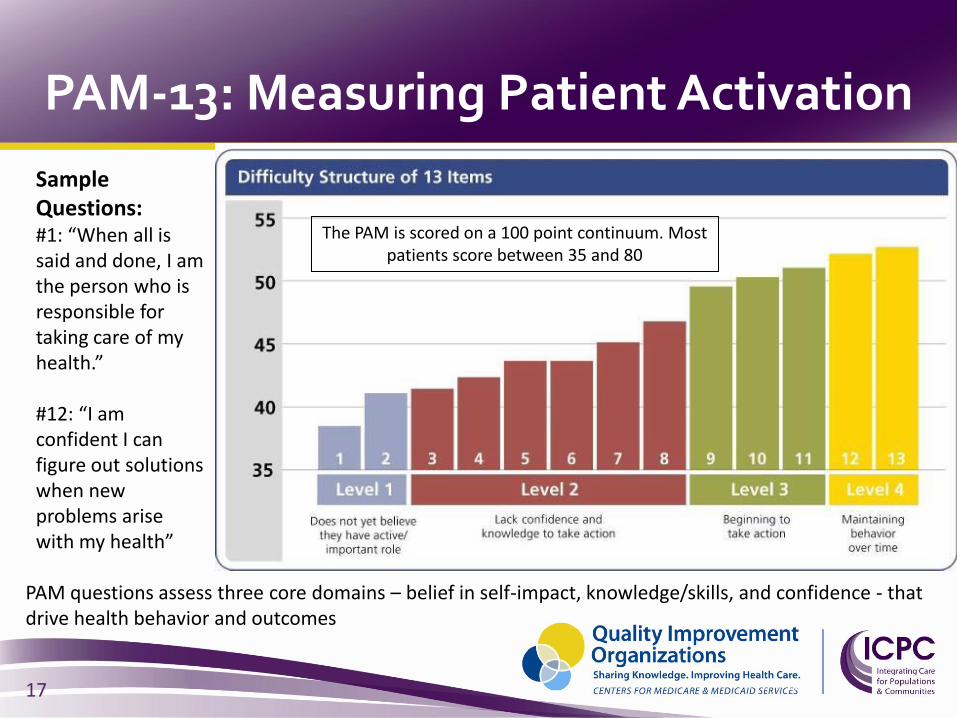
PAM questions assess three core domains – belief in self-impact, knowledge/skills, and confidence - that drive health behavior and outcomes
17
Sample Questions: #1: “When all is said and done, I am the person who is responsible for taking care of my health.” #12: “I am confident I can figure out solutions when new problems arise with my health”
The PAM is scored on a 100 point continuum. Most patients score between 35 and 80
PAM-13: Measuring Patient Activation
17
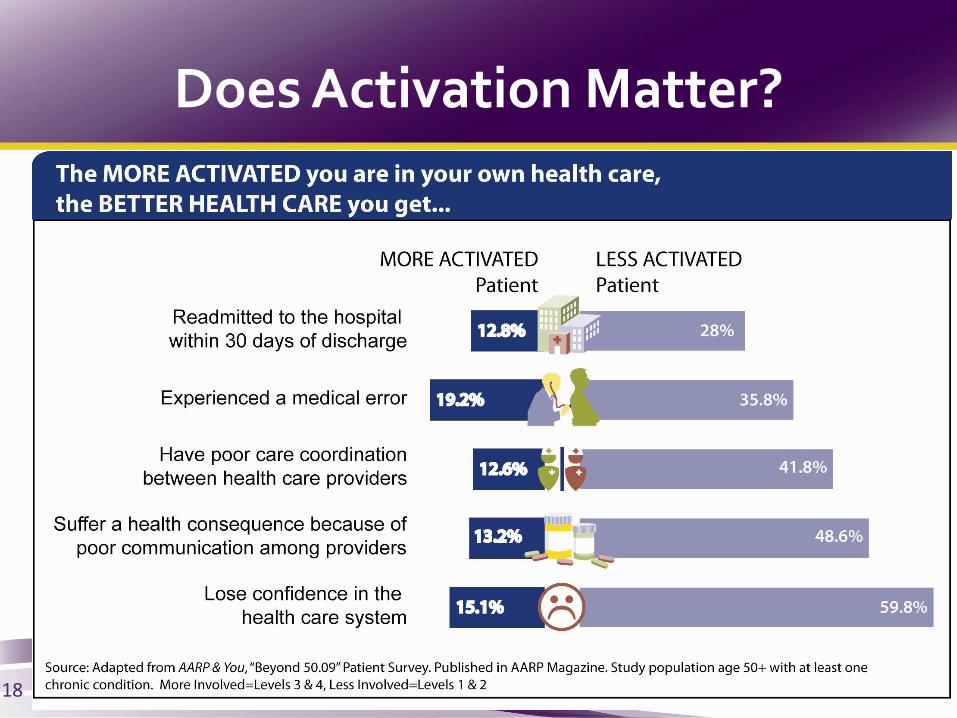
Does Activation Matter?
18
Inspiration
“I feel that I must tell someone about
how greatly I benefited from and
appreciate the services of the nurse
who follows up on patients
discharged from your hospital.
She comforted me and helped make
several forceful phone calls, and
soon all was well. What a great help!
What a relief! Thanks.”
Mr. H: A Patient Story
19
SeniorMetrix
Care Transitions theme, Northwest Denver (CFMC)
Medicare QIO 9th Scope of Work
August 2008 - July 2011
Northwest Denver Care Transitions Steering Committee
Community-based Action Teams Action Team 1: Standard Process
Action Team 2: Patient Activation and Family Support
Action Team 3: Communications
Action Team 4: Palliative and End-of-life Care
PAM®-tailored
CTI SM coaching
Hospital volunteer advocates (patient self-management support/education)
Care Transitions
Intervention SM (CTI) coaching
3.16
1.50
2.00
2.50
3.00
3.50
4.00
4.50
Jan
07
F M
A
M J J A S O
N
D
Jan
08
F M
A
M J J A S O
N
D
Jan
09
F M
A
M J J A S O
N
D
Jan
10
F M
A
M J J A S O
N
D
Month
Run Chart
30-day readmissions per 1,000 eligible beneficiaries in the NW Denver
Median Readmission rate
9.3% relative improvement (decrease) in readmissions per 1,000 beneficiaries
Results
20

Peak: Celebration meeting – June 21st
Evaluation & Next Steps: Apply for CCTP funding AND…
Peak: Create PHR, PAC tool, Palliative/Hospice curriculum and community talks
Peak: Form Action teams
Kick off: Community meeting
Foundation: Determine community
Northwest Denver: Campaign
Outcome Peak: Reduce hospital readmissions and improve patient activation
21
22

Energy Boost
23
Questions?
• Terrey Currie [email protected]
• Hilarea Amthauer, MPH, BSN, RN [email protected]
• Risa Hayes, CPC [email protected]
• Access the Care Transitions Toolkit:
http://www.cfmc.org/caretransitions/
24
How to Access Resources
• Contact your QIO http://www.cfmc.org/integratingcare/files/ICPC_contacts.pdf
• Join (and listen to archived) Care Transitions Learning Sessions
http://www.cfmc.org/integratingcare/learning_sessions.htm
• Browse our Toolkit http://www.cfmc.org/integratingcare/toolkit.htm
25

Additional Resources
• Medicaring – an independent website for improving care transitions www.medicaring.org
• Partnership for Patients
www.healthcare.gov/compare/partnership-for-patients/
• Community-based Care Transitions Program http://go.cms.gov/caretransitions
• The AoA Toolkit www.aoa.gov/AoARoot/AoA_Programs/HCLTC/ADRC_caretransitions/Toolkit/index.aspx
26