Embed Size (px)
Citation preview
Defining Results-Based Care Transition
ProcessesMarch 2015
Agenda
• Objectives
• Background
• Root causes of ineffective transitions of care
• Structured approaches to improve Care Transitions
• 8 Care Transition areas to review
• Recommended approach improve Care Transitions
• Question & Answers
Copyright 2015 Digital Collaboration Solutions, LLC 24/10/2015
A consulting and services company that
provides care coordination, collaboration,
and patient/provider engagement solutions.
Care Coordination Collaboration Communications
HEALTHCARE
Process
People
Tech
DCS helps healthcare organizations improve care coordination and care team
engagement through process optimization, better collaboration, digital
communications, and use of innovative technology.
DCS combines in-depth experience
in healthcare, healthcare information
technology and patient/provider
engagement to deliver measurable
results and improved outcomes.
Copyright 2015 Digital Collaboration Solutions, LLC 3
4/10/2015
DCS approach to improving care transitions
1. Quick survey of your existing processes
2. Quantify the risk (impact & cost) today
3. Estimate the revenue impact/costs savings from
implementing the strategy
4. Estimate the costs to implement the process improvement
5. Compute projected return on investment (ROI)
6. Is the return worth it?
Copyright 2015 Digital Collaboration Solutions, LLC 4
4/10/2015
Background
Care transitions processes - increasingly complex as patients receive care
from multiple providers in multiple settings.
• Lower care quality
• waste
• delays
• longer length of stays
• poor transitions of care
• Optimizing care transitions takes the careful integration
of people, process and technology.
Must work for the patient, care teams, and families.
Which are effective and how to get started?
Copyright 2015 Digital Collaboration Solutions, LLC 54/10/2015
Process
People
Tech
Impact Medicare reimbursement through
readmissions penalties, Value Based
Purchasing (VBP) and subjective patient
quality scores (HCHAP)
Objectives
Define care transitions processes that reduce readmissions
and improve overall quality and patient satisfaction
• Real-world processes working for today's hospitals
• Small workflow changes that have big impact
• Technology's role
• How do you get there
Copyright 2015 Digital Collaboration Solutions, LLC 64/10/2015
Benefits of Good Care Transition
• Reduction in readmission rates and penalties
• Reduction in bounce backs
• Reduction in length of stay
• Improved patient satisfaction
• Higher value based purchasing scores
• Improved family satisfaction
• Improved staff satisfaction
Copyright 2015 Digital Collaboration Solutions, LLC 74/10/2015
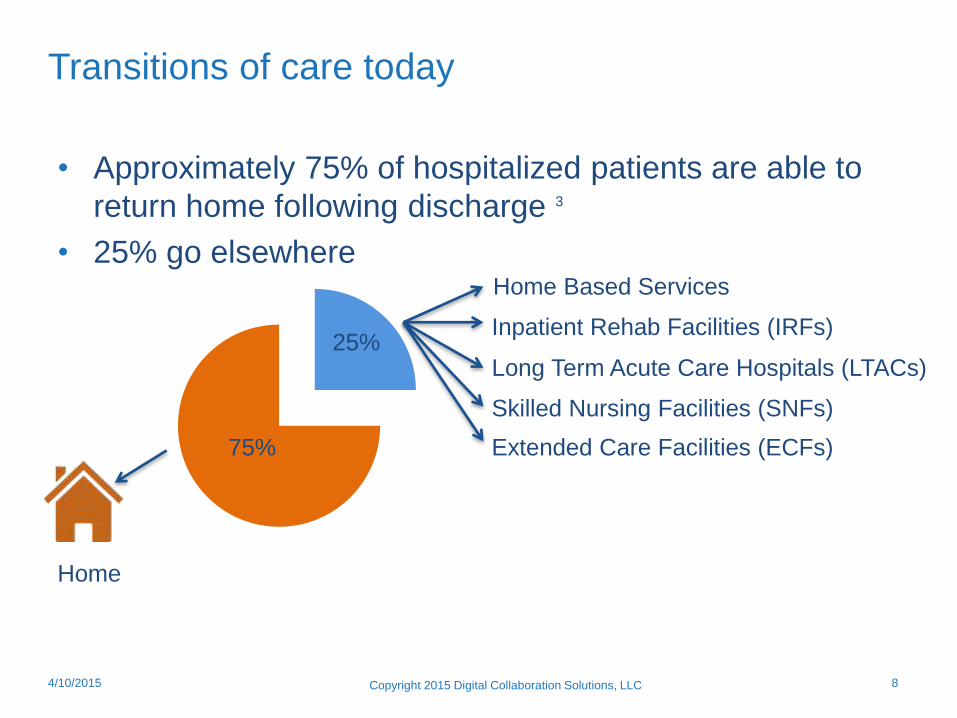
Transitions of care today
• Approximately 75% of hospitalized patients are able to
return home following discharge 3
• 25% go elsewhere
Copyright 2015 Digital Collaboration Solutions, LLC 84/10/2015
Inpatient Rehab Facilities (IRFs)
Long Term Acute Care Hospitals (LTACs)
Skilled Nursing Facilities (SNFs)
Extended Care Facilities (ECFs)
Home Based Services
Home
25%
75%
Transition of Care – Two definitions
The movement of a patient from one setting of care (hospital,
ambulatory primary care facility, long-term care, home health,
rehabilitation facility) to another. 1
The movement of patients between health care practitioners, settings,
and home as their condition and care needs change. 2
Copyright 2015 Digital Collaboration Solutions, LLC 94/10/2015

Root Causes of Ineffective Transitions of Care
Root causes of ineffective transitions of care
The Joint Commission defines
three main areas of breakdowns
that are the root causes of
ineffective transitions of care
– Communication breakdowns
– Patient education breakdowns
– Accountability breakdowns
Copyright 2015 Digital Collaboration Solutions, LLC 114/10/2015
Root causes of ineffective transitions of care
• Communication breakdowns
– Handoffs - Care providers do not communicate important information effectively, completely or in a timely fashion:
• Among themselves,
• To the patient, or
• To those taking care of the patient.
– Communication methods – whether verbal, recorded, or written – are ineffective.
– Differing expectations of senders and receivers of handoffs
7
Copyright 2015 Digital Collaboration Solutions, LLC 124/10/2015
Miscommunications
during handoffs is an
important contributing
cause in 80% of
adverse events. 7
The Joint Commission
Discharge Summaries
Reach the primary care
provider by the time of
the first follow-up visit in
only 12 to 34 percent of
such visits, and even
then often lacks key
information 5
Root causes of ineffective transitions of care
• Patient education breakdowns
– Patients or family/friend caregivers sometimes
receive:
• Conflicting recommendations,
• Confusing medication regimens, and
• Unclear instructions about follow-up care.
– Patients and caregivers are sometimes excluded
from the planning related to the transition
process.
– Patients may lack understanding of the medical
condition or care plan. As a result, they do not
buy into the importance of following the care plan
or lack the knowledge or skills to do so.
Copyright 2015 Digital Collaboration Solutions, LLC 134/10/2015
In one interview study of
patient perception and
understanding of
discharge instructions,
among discharged
patients aged >65 years
who felt that they had
good understanding of
their discharge
instructions;
• 40% were unable to
accurately describe
the reason for their
hospitalization
• 54% did not
accurately recall
instructions about
their follow-up
appointment 6
Root causes of ineffective transitions of care
• Accountability breakdowns
– No physician or clinical entity takes responsibility to assure
that care is coordinated across various settings and
providers
– Providers – especially when multiple specialists are involved
– often fail to coordinate care or communicate effectively,
which creates confusion for the patient and those
responsible for transitioning the care of the patient.
– Primary care providers are sometimes not identified by
name, and there is limited discharge planning and risk
assessment.
– Steps are not taken to assure that sufficient knowledge and
resources will be available – either at home or at the next
setting to the patient upon discharge.
Copyright 2015 Digital Collaboration Solutions, LLC 144/10/2015
9% of physicians have
“Turfed” patients.
A survey at 101 Hospitals
revealed that 9% of
physicians have admitted
to “Turfing” patients. The
term refers to refusing to
accept a patient into their
unit by claiming the
patient should be cared
for in another part of the
hospital, transferring a
patient that a physician
was capable of taking
care of, but switching
them to another doctor’s
care to reduce their
patient load. 8

Structured approaches to Care Transition improvement
Current Transition of Care Models
• Care Transitions Intervention (CTI)
• Transitional Care Model (TCM)
• Better Outcomes for Older Adults through Safe
Transitions (BOOST)
• The Bridge Model
• Guided Care
• Geriatric Resources for Assessment and Care of Elders
(GRACE)
• Project RED (Re-Engineered Discharge).
Copyright 2015 Digital Collaboration Solutions, LLC 164/10/2015
3 basic types of common transition of care interventions
Copyright 2015 Digital Collaboration Solutions, LLC
1. Pre discharge interventions
Patient education, discharge planning, medication
reconciliation, scheduling a follow-up appointment
2. Post discharge interventions
Follow-up phone call, communication with ambulatory provider,
home visits
3. Bridging interventions
Transition coaches, patient-centered discharge instructions,
physician continuity between inpatient and outpatient settings
174/10/2015
The Joint Commission - seven foundations of safe and
effective transitions of care to home
Leadership support
Multidisciplinary collaboration
Early identification of patients/clients at risk
Transitional planning
Medication management
Patient and family action/engagement
Transfer of information
Multi-Component Intervention
Comprehensive Care Coordination Program
4/10/2015 Copyright 2015 Digital Collaboration Solutions, LLC 18
8 Care Transition Processes Areas to Review
1. Multidisciplinary communication, collaboration and
coordination - from admission through transition.
– Care team – including physician, nurse, pharmacist,
social worker, and others – communicates,
collaborates and coordinates effectively.
– Team starts at admission and throughout patient’s
hospital stay to assure a successful transition.
– In addition to daily rounding/meetings, actively teach
• patient and family/friend caregivers to learn and
practice self-care and
• to follow the care plan, including how to self-
manage medications.
Copyright 2015 Digital Collaboration Solutions, LLC 204/10/2015
2. Clinician involvement and clear accountability during all
points of transition.
• Both sending and receiving clinicians are involved in and
accountable for a successful transition.
• They are identified by name and exchange information
electronically or by fax or telephone during the time of
transition.
• At every point during the transition, the responsible
coordinating clinician (such as a primary care physician
or nurse practitioner) is identified for the patient.
Copyright 2015 Digital Collaboration Solutions, LLC 214/10/2015
3. Comprehensive planning and risk assessment
throughout hospital stay.
• Each patient and family/friend caregiver has a discharge risk assessment completed during the hospital stay, usually within the first 24-48 hours of admission.
• Discharge planning begins immediately after admission.
• During the hospital stay, patients are assessed for risk factors that may limit their ability to perform necessary aspects of self-care.– Low literacy, recent hospital admissions, multiple chronic conditions or
medications, and poor self-health ratings.
• Clinicians begin to assess risks that may be present at the receiving setting. – For example, the clinician should confirm that the patient will have access to
medications he or she needs at the next setting, as the pharmacy formulary there may not have the medications, or the ability to compound medications as ordered.
Copyright 2015 Digital Collaboration Solutions, LLC 224/10/2015
4. Standardized transition plans, procedures and
forms.
• Written transition plan or discharge summary includes:
– Active issues,
– Diagnosis,
– Medications,
– Required services,
– Warning signs of a worsening condition, and
– Whom to contact 24/7 in case of emergency.
• Plans are provided in the patient’s preferred language
and use pictures for patients having low literacy.
Copyright 2015 Digital Collaboration Solutions, LLC 234/10/2015
5. Standardized training
• Begin by defining what constitutes a successful transition.
• Staff are taught the necessary steps to complete a successful
transition and are engaged in real-time performance
feedback.
• Successful transitions are an organizational priority and
performance expectation.
• Medical schools - incorporate risk assessment, collaboration,
care planning, and medication management relating to
transitions of patient care into curricula.
• Nursing schools - include training on transitions elements and
risks and how they can contribute to safe care transition.
Copyright 2015 Digital Collaboration Solutions, LLC 244/10/2015
6. Timely follow-up, support and coordination after the
patient leaves a care setting.
• Develop processes that provide for timely post-discharge follow-up
and successful recoveries
– Telephone or in-person follow-up, support, and coordination
– By a case manager, social worker, nurse, or another health care
provider
– 24-48 hours after discharge
• A 24/7 call center provides a recently transitioned patient or family
member with information or reassurance
• Have a transitional care nurse accompany the patient to the first
follow-up outpatient visit
• Schedule home care visits for the patient.
Copyright 2015 Digital Collaboration Solutions, LLC 254/10/2015
7. If a patient is readmitted within 30 days, gain an
understanding of why.
• 30 day readmissions can often be prevented by providing a
safe and effective transition of care.
• Convene care team meeting including attending physician,
other staff, patient and family members.
• Ask patient questions about what happened after discharge.
• Find out if there were financial or transportation barriers,
and whether or not home caregivers were unavailable.
– This important information can be used by organizations to improve
care transitions for patients and family/friend caregivers
Copyright 2015 Digital Collaboration Solutions, LLC 264/10/2015
8. Clear measurements throughout transitions of care
• Monitor compliance with standardized forms, tools, and
methods for transitions of care.
• Use surveys and data collection
– Find root causes of ineffective transitions and
– Identify patient and caregiver satisfaction with transitions and
their understanding of the care plan.
• Measure important results
– Readmission rates
– Time between discharge order creation and discharge
– Bed wait time
– Intervals between blank electronic discharge summaries
Copyright 2015 Digital Collaboration Solutions, LLC 274/10/2015

Recommended Approach to Improve Care Transitions
Copyright 2015 Digital Collaboration Solutions, LLC 294/10/2015
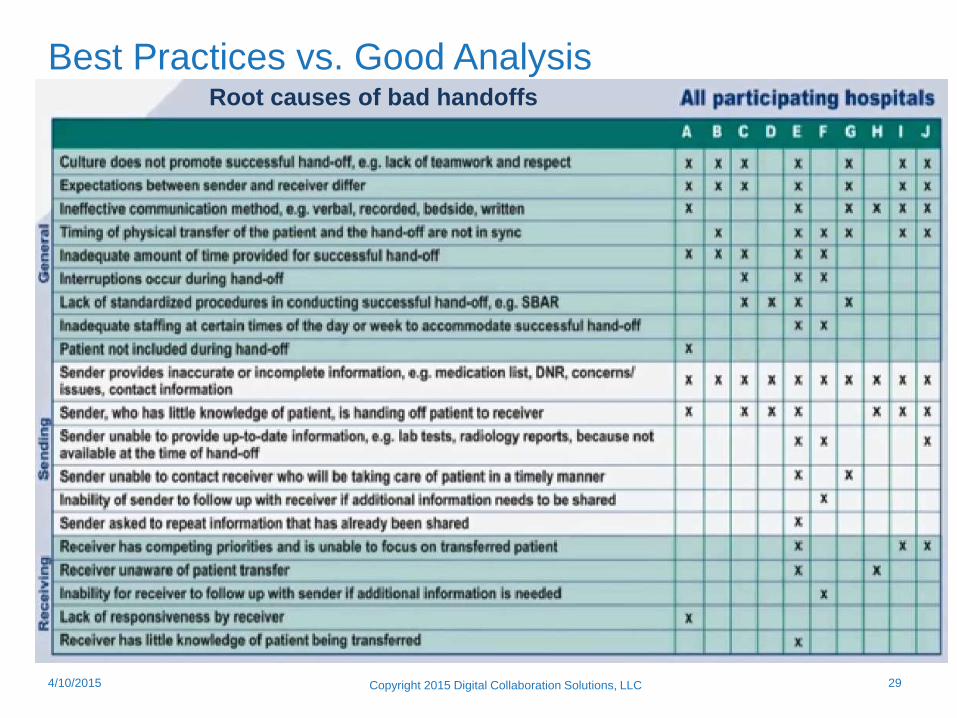
Best Practices vs. Good AnalysisRoot causes of bad handoffs
Copyright 2015 Digital Collaboration Solutions, LLC 304/10/2015
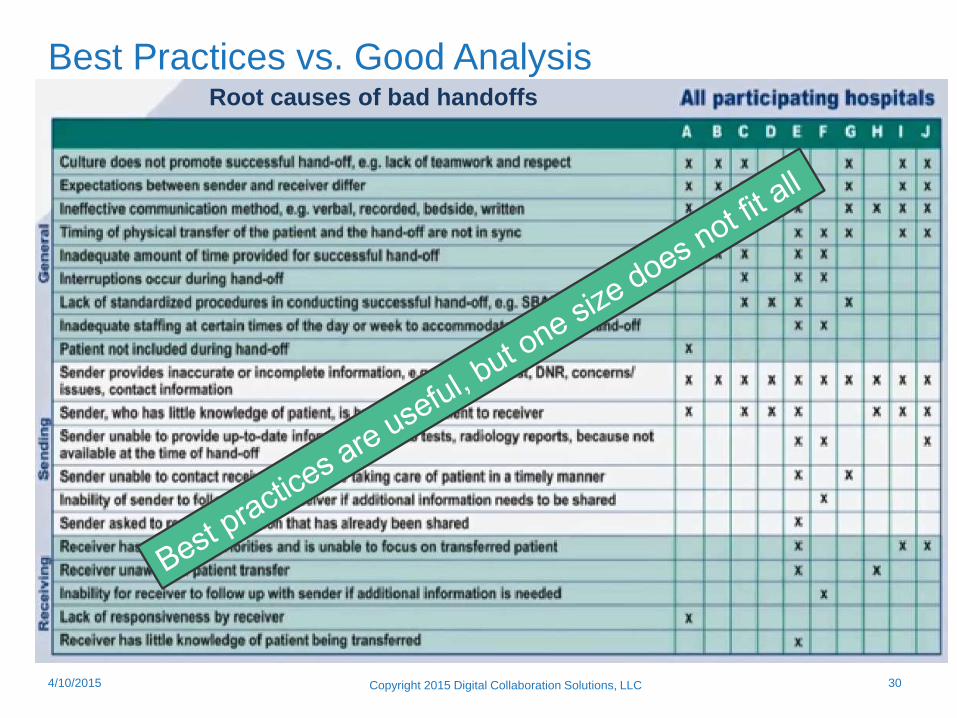
Best Practices vs. Good AnalysisRoot causes of bad handoffs
Recommendations and take a ways
Copyright 2015 Digital Collaboration Solutions, LLC 314/10/2015
• To improve Transitions of Care, you have to confront and improve:
– Communication breakdowns
• Align the expectations of the senders and receivers of handoffs!
– Patient Education breakdowns
– Accountability breakdowns
• 8 Care Transition processes areas to review
• Best practices alone may not be best for you
• Define and measure your existing processes
– Understand where your issues are and their impact
• Financial
• Care delivery success
• Care team effectiveness
• Each transition of care is complex and will fight you.
• Be deliberate, incorporate the stakeholders and show results
continuously.

Michael Levinger
President & CEO
Digital Collaboration Solutions
V: 781.307.7898
Skype: mlevinger
Twitter: @mlevinger
Questions & Answers
Timothy Perkins
Vice President
Digital Collaboration Solutions
V: 781.424.3698
Skype: timperkins80
Twitter: @timperkins
References
1. Eligible Professional Meaningful Use Menu Set Measures 7 of 9 Stage 1 (2014 Definition) Last Updated: May 2014
http://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/downloads/8_Transition_of_Care_Summary.pdf (accessed March
2015)
2. Hot topics in Healthcare - Transitions of Care: The need for a more effective approach to continuing patient Care,
The Joint Commission, 06/2012
3. Hospital Discharge and Readmission, UptoDatehttp://www.uptodate.com/contents/hospital-discharge-and-
readmission (accessed March 2015)
4. Discharge planning: issues and challenges for gerontological nursing. A critique of the literature, Journal of
Advanced Nursing, 1994;Mar;19(3):492-502
5. Deficits in communication and information transfer between hospital-based and primary care physicians:
implications for patient safety and continuity of care.
Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW, JAMA. JAMA 2007;297(8):831
6. Quality of discharge practices and patient understanding at an academic medical center.
Horwitz LI, Moriarty JP, Chen C, Fogerty RL, Brewster UC, Kanade S, Ziaeian B, Jenq GY, Krumholz HM
JAMA Intern Med. 2013;173(18):1715.
7. Targeted Solutions Tool Webinar, http://www.centerfortransforminghealthcare.org/multimedia/tst-for-hand-off-
communications-webinar-playback_july-26-2012/ (accessed March 2015)
8. Participation in unprofessional behaviors among hospitalists: A multicenter study, Shalini T. Reddy MD1, James A.
Iwaz BS2,Aashish K. Didwania MD3, Kevin J. O'Leary MD, MS3, R. Andy Anderson MD4, Holly J. Humphrey
MD1, Jeanne M. Farnan MD, MHPE1, Diane B. Wayne MD3 andVineet M. Arora MD, MAPP, Journal of Hospital
Medicine, 543-550, September 2012
Copyright 2015 Digital Collaboration Solutions, LLC 334/10/2015





























