Embed Size (px)
Citation preview

Pathogens of the gastrointestinal tract: Salmonella spp. (salmonellosis and the
enteric fever), Shigella spp.
Dr. Dóra SzabóSemmelweis University
Institute of Medical Microbiology

Enterobacteriaceae
Morphology and General Characteristics
– Gram-negative, non-sporing, rod shaped bacteria
– Oxidase –
– Ferment glucose and may or may not produce gas in the process (aerogenic vs anaerogenic)
Differentiation– biochemical reactions
– differences in antigenic structure
Slideagglutination!

Enterobacteriaceae
– NMember of the normal GI tract
– GI tract of human and animal
– Pathogen species
Enteral pathogens
Extraintestinal pathogens
Osztályozás - több mint -15 különböző törzs:
– Escherichia, Shigella, Edwardsiella, Salmonella, Citrobacter, Klebsiella, Enterobacter, Hafnia, Serratia, Proteus, Providencia, Morganella, Yersinia, Erwinia, Pectinobacterium

Gram-negative facultative anaerobic rods(Positive glucose fermentation)
Oxidase positive Oxidase negative
Vibrionaceae Aeromonadaceae
Vibrio Aeromonas
Enterobacteriaceae
EscherichiaKlebsiella
EnterobacterProteusSerratia
ProvidenciaMorganella
EdwardsiellaCitrobacter
Hafnia
SalmonellaShigellaYersinia
Facultative pathogenic
Obligate pathogenic
Plesiomonas

Escherichia coli
Member of the normal GI tract
Extraintestinal infection urinary tract infections
Neonatal meningitis –strains with the K1 capsular antigen.
Peritonitis, cholecystitis
Nosocomial infections
Intestinal infections - gastroenteritis

E. coli intestinal infections
Gastroenteritis – there are several distinct types of E. coli that are involved in different types of gastroenteritis:
–enterotoxigenic E. coli (ETEC),
–enteroinvasive E. coli (EIEC),
–enteropathogenic E. coli (EPEC) ,
– enteroaggregative E. coli (EAEC), and
– enterohemorrhagic E. coli (EHEC).

E. coli gastroenteritisETEC – enterotoxigenic E. coli
Traveler’s diarrhea and diarrhea in children in developing countries.
Transmission is via contaminated food or water.
The disease is characterized by a watery diarrhea, nausea, abdominal cramps and low-grade fever for 1-5 days.
Pathogenesis
– Colonization factors (CFA)
– Enterotoxins –
LT – is heat labile Increased cAMP alters the activity of sodium and chloride transporters producing an ion imbalance that results in fluid transport into the bowel.
ST – is heat stable, affects the cGMP system.

E. coli gastroenteritisEPEC – enteropathogenic E. coli
In hospitalized infants and in day care centers.
The diarrhea with large amounts of mucous without blood or pus occurs along with vomiting, malaise and low grade fever
Pathogenesis
– Bundle forming pili
– Changes in signal transduction in the cells,
– The exact mode of pathogenesis is unclear, the secretion/absorbtion ratiochanges

E. coli gastroenteritis
enteroinvasive E. coli (EIEC)
Symptoms include fever,severe abdominal cramps, malaise, and watery diarrhea followed by scanty stools containing blood, mucous, and pus.
Virulence genes similar to Shigella.
Pathogenesis: Attachment via and penetration via pili and outer membrane
proteins
invasion in the intestinal cells, mainly in the colon
destruction of the intestinal mucosa
movement of the organism from one cell to adjacent cells

E. coli gastroenteritisenteroaggregative E. coli (EAEC),
Symptoms include watery diarrhea, vomiting, dehydration and occasional abdominal pain.
EAEC – Mucous associated autoagglutinins cause aggregation of the bacteria at the cell surface and result in the formation of a mucous biofilm. – Enteroaggregative ST-like toxin – produced by
enteroaggregative strains of E. coli (EAEC) – causes watery diarrhea.
The organisms attach via pili and liberate a cytotoxin distinct from, but similar to the ST and LT enterotoxins liberated by ETEC.

E. coli gastroenteritisenterohemorrhagic E. coli (EHEC).
The symptoms start with a watery diarrhea that progresses to bloody diarrhea without pus and crampy abdominal pain with no fever or a low-grade fever
This may progress to hemolytic-uremic syndromethat is characterized by low platelet count, hemolytic anemia, and kidney failure.
EHEC – The organism attaches via pili to the intestinal mucosa and liberates the shiga-like toxin.
This is most often caused by serotypes O157:H7.

Summary of E.coli strains that cause gastroenteritis.

Gram-negative facultative anaerobic rods(Positive glucose fermentation)
Oxidase positive Oxidase negative
Vibrionaceae Aeromonadaceae
Vibrio Aeromonas
Enterobacteriaceae
EscherichiaKlebsiella
EnterobacterProteusSerratia
ProvidenciaMorganella
EdwardsiellaCitrobacter
Hafnia
SalmonellaShigellaYersinia
Facultative pathogenic
Obligate pathogenic
Plesiomonas

Gram-negative facultative anaerobic rods(Positive glucose fermentation)
Oxidase positive Oxidase negative
Vibrionaceae Aeromonadaceae
Vibrio Aeromonas
Enterobacteriaceae
EscherichiaKlebsiella
EnterobacterProteusSerratia
ProvidenciaMorganella
EdwardsiellaCitrobacter
Hafnia
SalmonellaShigellaYersinia
Facultative pathogenic
Obligate pathogenic
Plesiomonas

SALMONELLA

The genus Salmonella was named
after Daniel Elmer Salmon,
an American veterinary pathologist.
While Theobald Smith was the actual discoverer of the bacteria that causes hog cholera (Salmonella enterica var. Choleraesius)
Salmon was the administrator of the USDA research program and thus the organism was named after him.
DENOMINATION

SALMONELLA SPP.
Gram-negative
motile rods, peritrich flagella
Non-spore forming
Facultative anaerobic
Salmonella grow at an optimum of 37ºC
Optimum pH for growth of Salmonella
is 6.5-7.5; may grow at a pH range of 4.5-9.0
Biochemical properties:
H2S production
Lactose negative, Urease negative, Indol negative

SALMONELLA SEROLOGY
Based on the Kauffman-White scheme of classification: serogroups or serotypes based on O and H (flagella) antigens.
The O antigens– O antigens are vary variable– Mozaic structure– Epitop combination,
special antigens of the isolates
The H (flagella) antigens– H antigens has a mosaic
structure as well– occur in two phases;
1 and 2 and only one phase is expressed at a given time
Salmonella typhi also has a Vi antigen which is a capsular antigen.

SALMONELLA VIRULENCE FACTORS
Endotoxin – may play a role in intracellular survival
Capsule (for S. typhi and some strains of S. paratyphi)
Adhesions – both fimbrial and non-fimbrial
Type III secretion systems and effector molecules
Involved in promoting entry into intestinal epithelial cells
Involved in the ability of Salmonella to survive inside macrophages
Outer membrane proteins - involved in the ability of Salmonella to survive inside macrophages
Flagella – help bacteria to move through intestinal mucous
Enterotoxin - may be involved in gastroenteritis
Iron capturing ability

HOST SPECIFICITY Wide host specificity
– normal flora in the GI of animal
– SALMONELLOSIS-GASTROENTERITIS in human; zoonosis
– S. enteritiditis, S. typhimurium
Adapted to animal– Serious infection in animal
– focal infection in human (mainly kids)
– S. cholerasuis
Adapted to human– only in human: ENTERIC FEVER
– S. typhi, S. paratyphi A, B, and C

SALMONELLA PATHOGENESIS
Disease depends on age of the host
– more severe in newborns, infants, the elderly
Disease also depends on the serovar and type of host
– Host specific serovars: typhi, paratyphi cause disease only in humans
– pullorum/gallinarum in poultry, dublin in cattle;
– choleraesuis serovars in pigs can also infect humans;
– typhimurium and enteritidis are the major serovars that cause disease in humans, cattle, poultry, sheep, pigs, horses, and wild rodents.

Salmonella multiply in the GI tractinducing a strong inflammatory response .
The inflammatory response prevents the spread beyond the GI tract and eventually kills the bacteria.
Salmonella disseminate before they multiply to high enough levels to stimulate a strong inflammatory response.
CLINICAL SIGNIFICANCE
SALMONELLOSIS ENTERIC FEVER

SALMONELLOSIS

SALMONELLOSIS - Pathogenesis I.

SALMONELLOSIS - Pathogenesis II.

SALMONELLOSIS - Clinical picture I.
Symptoms generally appear 18 to 36 hours after exposure, but they can occur as quickly as 12 hours or as long as 72 hours after exposure.
GASTROENTERITIS, but can be: – dizziness– vomiting– Abdominal pain
The symptoms can be similar to dysentery
The symptoms moderate in a few days – spontan recovery in a week
After recovery carrier status can occur– That patient can a source of infection later

SALMONELLOSIS - Clinical picture II.
Transient bacteraemia can occur
Permanent bacteraemia, sepsis, meningitis: – Very old patient
– Very young patient
– Immunsuppressed and AIDS patient
Focal infections can occur – lung
– brain
– in atherosclerotic plaque of aorta
– prothesis

SALMONELLOSIS - Epidemiology
One of the most common cause of foodpoisoning– More than 15 000 known cases per year in Hungary
– 1-10% of the real cases
– Increasing incidence
Reservoirs: – Chicken –and duck eggs
– Chicken and swine
– The feces of some pets,
especially those with diarrhea
– Reptiles: turtles, lizards, snakes
Insufficient heat treatment is necessary!!

SALMONELLOSISMicrobiological diagnosis I.
Clinical specimen: faeces: positive from first week, and may remain positive for several weeksblood for blood-culture: just in 2-4 % (+); liquorfood leftover
Microscopic examination:Direct smear has no value in the diagnosis.
Culture:Samples are inoculated onto brilliant green and/or bismuth sulphite selective, differentiating media.

Brillant-green culture media
brillant green – for selection
lactose, dextrose, saccharose
Andrade indicator
(acidic pH -
Salmonella lactose neg.– no colour
- E. coli lactose+ - red)
Bismuth-sulphite media
brillant green – for selection
bismuth salt + sodium sulphite
Salmonella H2S production
Bismuth sulphide (black)

SALMONELLOSISMicrobiological diagnosis II.
Biochemical identification:o Lactose (-)o dextrose fermentationo gas formationo H2S (+)
Serological identification:Slide agglutination with specific antibodies to detect presence the O and H antigens on the bacteria culture

Bacteriophage typing
o the surface of the plate is inoculated with a broth culture of the investigated strain
o a number of phages are spotted on the plate
o after incubation the phage type is determined by the pattern of lyses
SALMONELLOSISEpidemiological investigations I.

SALMONELLOSISEpidemiological investigations II.
Molecular methods– PCR-s (arbritary primed (AP)-PCR, ERIC-PCR)
– Pulsed-field gel-electrophoresis (PFGE)
– rRNS sequencing

SALMONELLOSIS - Therapy
1. Water and electrolytes replacement
2. The vast majority of enterocolitis cases do not require an antibiotic treatment. After antibiotic treatment carrier status occurs more frequently.
Antimicrobial treatment of Salmonella infection of neonates, as well as invasive salmonella infections is important.– ampicillin – sulfomethoxazole + trimethoprim– fluoroquinolones – 3rd generation cephalosporinsAntibiotic susceptibility tests are important

1984 Rajneeshee bioterror attack
750 individuals
The Dalles, Oregon, US
Ten local restaurants
Contaminated salad bar with Salmonella
To incapacitate the voting population of the city
The first bioterrorist attack
Salmonella as biological weapon

ENTERIC FEVER

ENTERIC FEVER
THYPHOID FEVER
caused by S. typhi ,
PARATHYPHOID FEVER
caused by S. paratyphi A, B and C milder disease
The source is always human!!

ENTERIC FEVER - Pathogenesis I. First period is the PRIMER BACTERAEMIA
– After oral infection the incubation period is two weeks – Bacteria get through mucosa via the M cells of Peyer plaques– Infect the local macrophages– Macrophages deliver the bacteria to the mesentarial lymph nodes – Through the ductus
thoracicuson and blood stream the bacteria get to spleen, liver, kidney, lung The CFU is low
– The patient is asymptomatic or subfebrile

ENTERIC FEVER - Pathogenesis II.
SECUNDER BACTERAEMIABacteria multiply in RES
Mainly in Kupffer-cells – Getting out the bactera there is a bacteraemia with high CFU
PERFORATION the terminal ileum and proximal colon: Through bile back to the intestine multiplication in the Peyer’s patches ulceration bleeding perforation
Permanent carrier stage– From bile

ENTERIC FEVER - Clinical picture
First week: The disease classically presents with step-ladder fashion rise in temperature (40 - 41°C) over 4 to 5 days, accompanied by headache, vague abdominal pain, and constipation.
Second week: Between the 7 th -10 th day of illness, mild hepato-splenomegally occurs in majority of patients. Relative bradycardia may occur and rose-spots may be seen.
Third week: The patient will appear in the "typhoid state" which is a state of prolonged apathy, toxaemia, delirium, disorientation and/or coma. Diarrhoea will then become apparent. If left untreated by this time, there is a high risk (5-10%) of intestinal hemorrhage and perforation.
Rare complications:typhoid hepatitis, empyema, osteomyelitis, cystitis and psychosis.
2-5% patients may become gall-bladder carriers

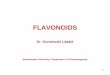
Rose spots on the chest and abdomen of patients with typhoid fever due to Salmonella typhi.
ENTERIC FEVER – Clinical symptoms

Skin symptoms
Ileum necrosisPerforation of Peyer-plaques
ENTERIC FEVER – Clinical symptoms
Ulceration of Peyer-plaques
Skin symtoms

ENTERIC FEVER Microbiological diagnosis I.
Clinical specimen: faeces: positive from the second or third weeks (45-75% positive)urine : positive from the second week (45-75% positive)bile, bone marrow aspirate (85-95% positive)blood for blood-culture : often positive (70-80%) in the first week
Microscopical examination:Direct smear has no value in the diagnosis.
Polymerase chain reaction (PCR) on peripheral mononuclear cells. More sensitive than blood culture alone (92% )
Culture: Samples are inoculated onto brilliant green and/or bismuth sulphiteselective media.
Biochemical identification: Lactose (-), dextrose fermentation gas formation, H2S (+)

Serological identification:
Slide agglutination with specific antibodies to show presence of S. typhi cells in the bacteria culture.
Blood serology => Gruber-Widal reaction (Widal`s type tube agglutination): (Ag = 'H' as well as 'O' antigens of the laboratory strain of S. typhi) to show presence and establish titre of specific antibodies in the patient’s serum. High titre of antibody to O antigen > 1:640 is
suggestive but not specific.
ENTERIC FEVER Microbiological diagnosis II.

TreatmentAntibiotics according to susceptibility tests: S. typhi strains are usually susceptible to– ampicillin,
– sulfomethoxazole + trimethoprim,
– 3rd generation cephalosporins.
Prevention– Specific sanitary measures and control of chronic carriers.
– VaccinationInjectable Typhoid vaccine (TYPHIM –Vi,TYPHIVAX)The live oral vaccine (TYPHORAL)TAB vaccine
“Carriers”3 % of survivors of typhoid become permanent carriers, harbouring the organisms in the gall-bladder, biliary tract or urinary tract.
ENTERIC FEVER Treatment and prevention

In 1906, Irish immigrant
Mary Mallon worked as a
cook in the Oyster Bay summer
home of New York banker
Charles Henry Warren and
his family. By the end of the
summer, six members of the
household had contracted typhoid fever. Mallon, while immune herself to the disease, was its carrier. For three years, she was isolated on North
Brother Island earning the nickname "Typhoid Mary." Instructed
not to cook for others upon her release, she nevertheless changed her name and became a cook at a maternity hospital in Manhattan. At least 25 staff members contracted typhoid. "Typhoid Mary" returned to North Brother Island, where she lived alone for 23 years, until her death in 1938. She died of a stroke after 23 years in quarantine.
Mary Mallon
(wearing glasses)
photographed
with
bacteriologist
Emma Sherman
on North Brother
Island in 1931 or
1932, over 15
years after she
had been
quarantined there
permanently.

THYPHOID FEVER Geographical distribution

SHIGELLA

DENOMINATION
1888 Chantamesse and Widal isolated the first member of Shigella
1891 Grigorjev
1898 Shiga isolated a bacteria causing dysenteriae, agglutinated by the serum of the patient
1900 same result by Flexner

SHIGELLA SPP.
Gram-negative
Short rods
Non-motile
Non –encapsulated
Non-spore-forming
Facultative anaerobic
pH 6.4 to 7.8
Temperature 10-40 (optimal temperature 37ºC)

SHIGELLA GENUS
Contains four species that differ antigenically based on antigen and to a lesser extent, biochemically.
Serogroup A: S. dysenteriae (12 serotypes)
Serogroup B: S. flexneri (6 serotypes)
Serogroup C: S. boydii (23 serotypes)
Serogroup D: S. sonnei (1 serotype)
OBLIGATE HUMAN PATHOGEN

VIRULENCE FACTORS OF SHIGELLA
Shiga toxin – chromosomally encoded
– role in the ulceration of the intestinal mucosa and in the cell death
– produced by S. dysenteriae and in smaller amounts by S. flexneriand S. sonnei.
– Effect the capillar endothel cells
– B-subunit binds to Gb3 glycolipid receptor
– A-subunit inhibit the protein synthesis binding by inactivating the
60S ribosomal subunit of aminoacyl-transfer RNA
Iron capturing ability
Other toxins: neurotoxic, cytotoxic and enterotoxic

SHIGELLOSIS - Pathomechanism I.

SHIGELLOSIS - Pathomechanism II.
Shigella penetrate the mucosa and the epithelial cells of
colon, but most commonly in the rectum and ampulla.
No before terminal ileum.
Lead to inflammation of the colon, and necrosis of the
colonic epithelium.
The underlying physiological insult that initiates this
inflammatory cascade is the invasion of Shigella into the
colonic epithelium and the lamina propria, and cell death
due to shiga toxin.
It is rare for the organism to disseminate.

SHIGELLOSIS– Clinical picture
There is an incubation of 1-7 days
Fever, cramping, abdominal pain, and diarrhea (due to the toxin) for 1-3 days.
This may be followed by frequent, scant stools with blood, mucous, and pus (due to invasion of intestinal mucosa).
Complications:
– HUS
– reactive arthritis
– Reiter-syndrome
The severity of the disease depends upon the species one is infected with:
– S. dysenteria is the most pathogenic followed by S. flexneri, S. sonnei and S. boydii.

Ulcers in the colon
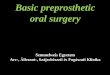
SHIGELLOSIS – Clinical symptoms

Sigmoidiscopic view of colonic mucosa in a mild case of infection due to S. flexneri. The thin whitish exsudate is made up of fibrin and polymorphonuclear leucocytes.
Sigmoidiscopic view of colonic mucosa in a fatal case of infection with S. dysenteriae type 1 showing extensive pseudomembranous colitis.
SHIGELLOSIS – Clinical symptoms

SHIGELLOSIS – Epidemiology
Transmission is via the fecal-oral route, but by food and by water as well.
The infective dose required to cause infection is very low (10-200 organisms).„Dirty hand disease”
Shigella dysenteriae 1: Asia, Africa, Middle-America
Shigella sonnei: US, Europe

SHIGELLOSISMicrobiological diagnosis I.
Clinical specimen: faeces, food leftover
Microscopic examination:Direct smear has no value in the diagnosis.
Culture: Samples are inoculated on selective-differentiating medias.

Desoxycholate-citrate agar containing desoxycholic acid, sodium citrate, lead acetate, ferrous ammonium sulfate, lactose, and neutral red indicatorShigellae: small, round-shaped, colourless colonies (lactose -, H2S-).
Eosine-methylenblue agar small, round-shaped, colourless colonies (lactose -)

Other commonly
used selective –
differentiating
culture medias
Culture

SHIGELLOSISMicrobiological diagnosis II.
o Biochemical identification:o Lactose (-), o dextrose fermentation w/o o gas formation, o H2S (-)o Shigella dysenteriae mannit negativeo Catalase negative, indole negative, ONPG positive
o Serological identification:Slide agglutination with specific antibodies to detect presence the O antigens on the bacteria
o Positive Serény test:Keratoconjunctivitis in the rabbit
produced by the instillation of shigella microorganism.

SHIGELLOSIS-Treatment and prevention
Treatment– Water and electrolytes replacement
– Antimicrobial therapy– Sulfonamides are commonly used as are streptomycin,
tetracycline, ampicillin, and chloramphenicol.
– Resistant strains are becoming increasingly common, so sensitivity testing is required.
Prevention– Vaccination
Live attenuated vaccine
Subunit vaccines

Thank you for the attention!