Embed Size (px)
Citation preview
Parkinson’s outcomes Project: Report to the Community
Find Answers. Change Lives. Beat Parkinson’s.
The Parkinson’s Outcomes Project
The mission of the Parkinson’s Outcomes Project is to determine
what works best in treatment and care with an aim toward
slowing the impact of the disease. At its heart is an all-inclusive,
international database that will follow patients over time.
Currently tracking more than 5,500 patients in four countries,
the Quality Improvement Initiative (QII) study will grow in the
coming years to follow tens of thousands of patients worldwide.
The Project will:
• Fund comparative research to determine best treatments and
why some people respond better to some therapies than others;
• Create transparency about what strategies produce the best
results and how specific centers measure up;
• Allow individuals to compare their health and treatments to
that of similar people; and
• Inform education and outreach efforts for both families
and professionals.
national Parkinson fou ndation 1
We now have the
deepest pool of
Parkinson’s data
ever collected. If
you have Parkinson’s,
there is almost
certainly someone
like you participating
in the study.
A little over three years ago, the National Parkinson Foundation (NPF) launched an
unprecedented research collaboration: the Quality Improvement Initiative (QII), part of
the Parkinson’s Outcomes Project. It is the largest clinical study of Parkinson’s disease ever
conducted, and the first with the primary goal of identifying and explaining factors that result
in longer, better, and more active lives for people with Parkinson’s.
The result is the deepest pool of Parkinson’s data ever collected, from some 5,500 people in four
countries. If you have Parkinson’s, there is almost certainly someone like you participating in
the study. Some are thriving; others are not doing as well. Our goal is to determine what makes
that difference. We can now consider the interplay of factors that produce different results in
different people, and likely paths toward better outcomes.
Unlike prior studies, this initiative encompasses the entire spectrum of Parkinson’s disease.
No one was too sick or too advanced, or too young or too old, to be included. More than 1,400
participants are now between 55 and 65 years old, the ages when most people are diagnosed. But
participants also include more than 440 with onset before age 40, and more than 100 with onset
after age 80, making it the largest prospective study of both young- and late-onset Parkinson’s
ever conducted.
Our study is equally inclusive in terms of the experience of individuals with Parkinson’s. More
than 650 participants manage at least two other serious illnesses—a group almost always
excluded from other clinical studies. Our data includes an assessment of medications and other
treatment, as well as motor symptoms, cognition, anxiety and depression, and caregiver burden.
To Our Parkinson’s Community:

2 nat ional Parkinson foundation
Mark Guttman, MD
This comprehensive evaluation reflects the complicated nature of Parkinson’s, which over time
can affect nearly every part of a person, as well as their loved ones.
Our study encompasses individuals at 20 leading centers for treating Parkinson’s, all part of
NPF’s Center of Excellence network. By studying the “best of the best,” NPF plans to delve into
the key differences in treatment and outcomes because every person with Parkinson’s deserves
“best practice” care, no matter where they are treated.
When we study how disease affects individuals, we talk about your “health status,” and much of
this report concerns the health status of people in our study. Health status is important because
it encompasses much more than just the disease. Our goal as physicians is to not just help you
function better, but to help you feel better. There is a difference between function and feeling,
and we have found that how people with Parkinson’s feel—their mood and depression—is a
critical factor with a tangible impact on overall health. We have also identified some of the steps
that we as doctors, and you as patients, can take to change this. These opportunities for all of us
to improve health are the highlight of this inaugural report.
We all hope that the next major breakthrough in Parkinson’s disease will be a treatment that
slows down biological progression. When we achieve this, optimizing care will be even more
important: though symptoms may be reduced, they must be addressed over a longer life
expectancy. We will still need to work together to prevent falls, treat depression, and address
John Nutt, MD
national Parkinson fou ndation 3
Eugene Nelson, DSc
John Nutt, MD
Director of the NPF Center of Excellence
Movement Disorders Center at Oregon
Health and Science University, Portland, OR
QII Study Co-Chair
Mark Guttman, MD
Director of the NPF Center of Excellence
Center for Movement Disorders in
Markham Ontario, Toronto, Canada
QII Study Co-Chair
Tanya Simuni, MD
Director of the NPF Center of Excellence
Parkinson’s Disease and Movement Disorders
Center at Northwestern University, Chicago, IL
QII Study Co-Chair
Eugene Nelson, DSc
Director of Quality Administration for the
Dartmouth-Hitchcock Medical Center
Lebanon, NH
QII Study Co-Chair
other factors that can speed the deterioration in your health status. As breakthroughs are
achieved, care will become more personalized, so that the best therapies are applied to your
particular genetic and environmental factors. In short: our goal is not only to optimize today’s
care, but to help guide tomorrow’s.
On behalf of NPF and our affiliated centers and institutions, we express our gratitude to those
who have shared our vision and supported our efforts. In particular, we thank the patients,
caregivers, clinicians, and researchers whose participation is steadily filling gaps in our
understanding, and supporting a brighter future in the fight against Parkinson’s. We look
forward to future reports to you, the Parkinson’s community, on our progress.
Tanya Simuni, MD
4 nat ional Parkinson foundation
the Quality imProvement initiative: Who Participates?
NUMBER of paRticipaNts iN thE stUdyNumber of Patients in Study
37%Female 63%
Male
0
2000
4000
6000
8000
10000
7/1/
12
4/1/
12
1/1/
12
10/
1/11
7/1/
11
4/1/
11
1/1/
11
10/
1/10
7/1/
10
4/1/
10
1/1/
10
10/
1/09
7/1/
09
Cumulative Patients
Cumulative Visits
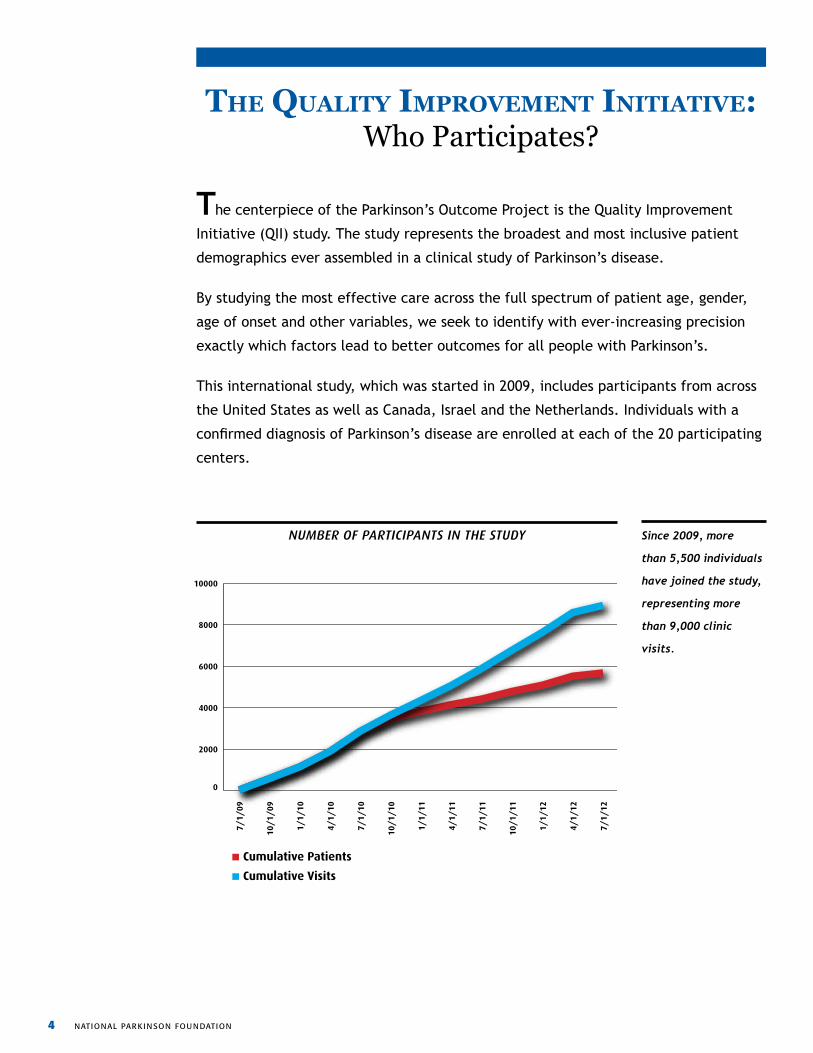
Since 2009, more
than 5,500 individuals
have joined the study,
representing more
than 9,000 clinic
visits.
The centerpiece of the Parkinson’s Outcome Project is the Quality Improvement
Initiative (QII) study. The study represents the broadest and most inclusive patient
demographics ever assembled in a clinical study of Parkinson’s disease.
By studying the most effective care across the full spectrum of patient age, gender,
age of onset and other variables, we seek to identify with ever-increasing precision
exactly which factors lead to better outcomes for all people with Parkinson’s.
This international study, which was started in 2009, includes participants from across
the United States as well as Canada, Israel and the Netherlands. Individuals with a
confirmed diagnosis of Parkinson’s disease are enrolled at each of the 20 participating
centers.
national Parkinson fou ndation 5
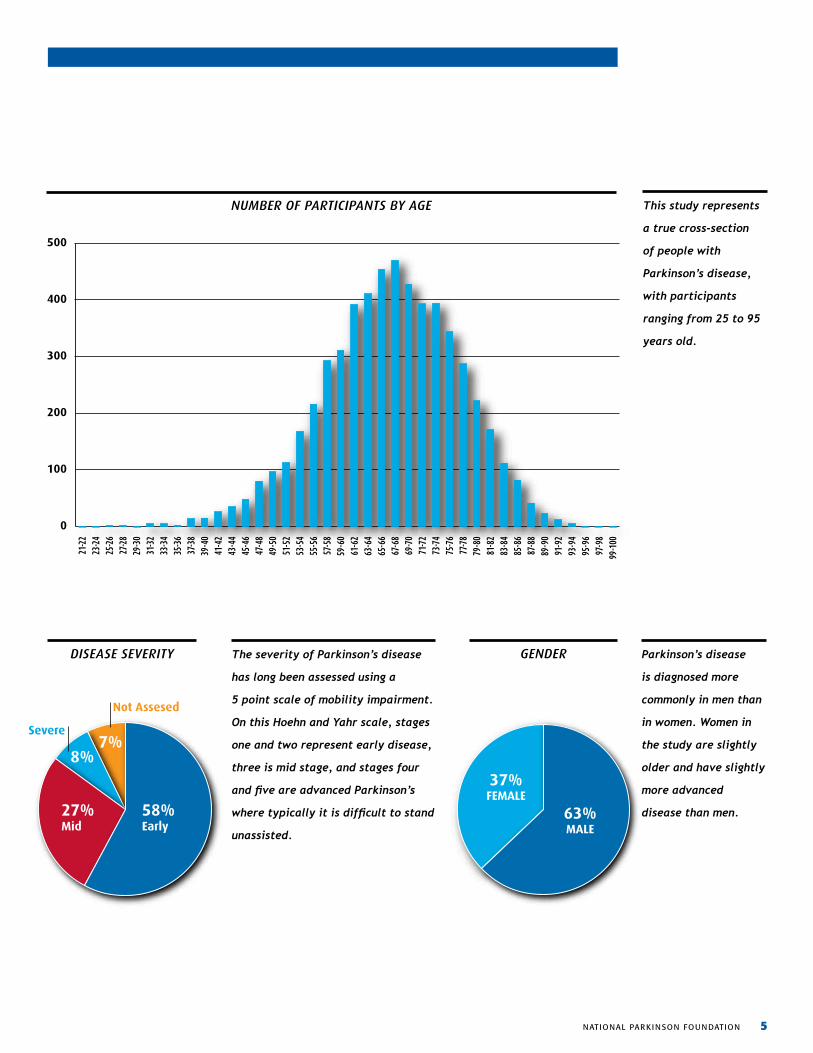
GENdERdisEasE sEvERity The severity of Parkinson’s disease
has long been assessed using a
5 point scale of mobility impairment.
On this Hoehn and Yahr scale, stages
one and two represent early disease,
three is mid stage, and stages four
and five are advanced Parkinson’s
where typically it is difficult to stand
unassisted.
Parkinson’s disease
is diagnosed more
commonly in men than
in women. Women in
the study are slightly
older and have slightly
more advanced
disease than men.
This study represents
a true cross-section
of people with
Parkinson’s disease,
with participants
ranging from 25 to 95
years old.
NUMBER of paRticipaNts By aGE
Disease Severity
58%Early
27%Mid
8%7%
Severe
Not Assesed GENDER
37%FEMALE
63%MALE
Number of Participants by Age Group
37%Female 63%
Male
0
100
200
300
400
500
99-100
97-98
95-96
93-94
91-92
89-90
87-88
85-86
83-84
81-82
79-80
77-78
75-76
73-74
71-72
69-70
67-68
65-66
63-64
61-62
59-60
57-58
55-56
53-54
51-52
49-50
47-48
45-46
43-44
41-42
39-40
37-38
35-36
33-34
31-32
29-30
27-28
25-26
23-24
21-22
6 nat ional Parkinson foundation
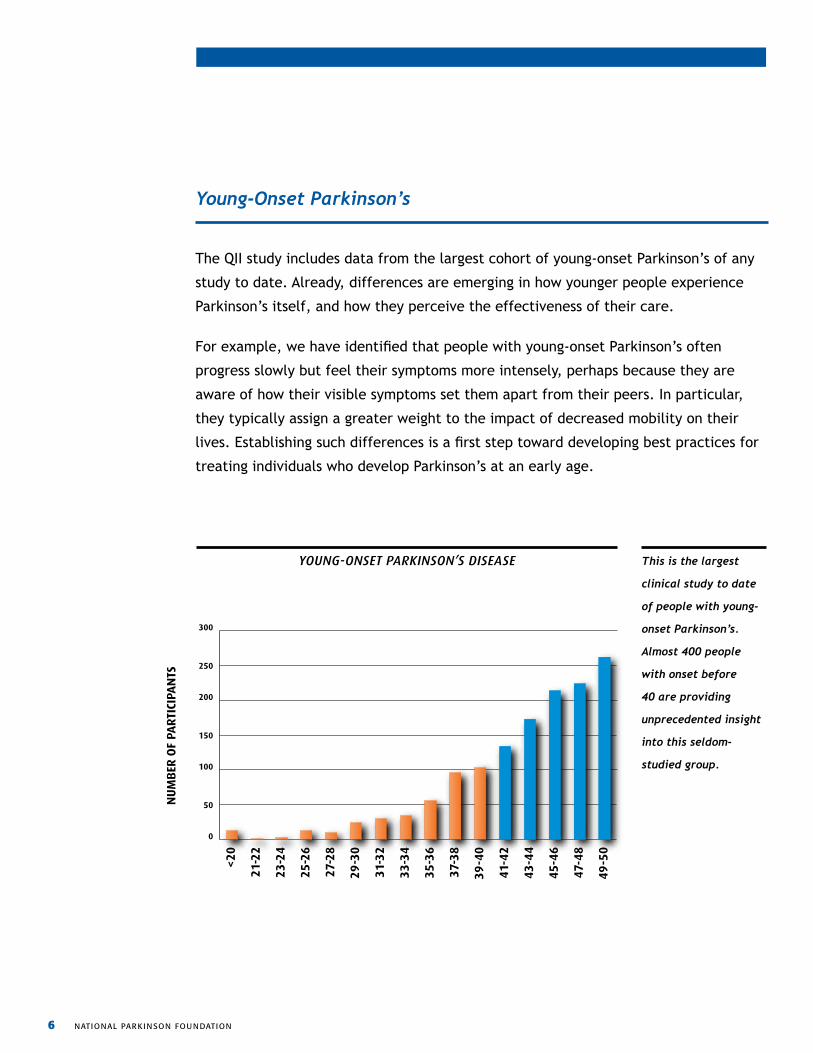
The QII study includes data from the largest cohort of young-onset Parkinson’s of any
study to date. Already, differences are emerging in how younger people experience
Parkinson’s itself, and how they perceive the effectiveness of their care.
For example, we have identified that people with young-onset Parkinson’s often
progress slowly but feel their symptoms more intensely, perhaps because they are
aware of how their visible symptoms set them apart from their peers. In particular,
they typically assign a greater weight to the impact of decreased mobility on their
lives. Establishing such differences is a first step toward developing best practices for
treating individuals who develop Parkinson’s at an early age.
yoUNG-oNsEt paRkiNsoN’s disEasE This is the largest
clinical study to date
of people with young-
onset Parkinson’s.
Almost 400 people
with onset before
40 are providing
unprecedented insight
into this seldom-
studied group.
Young-Onset Parkinson’s
Age at Onset
37%Female 63%
Male
0
50
100
150
200
250
300
49-5
0
47-4
8
45-4
6
43-4
4
41-4
2
39-4
0
37-3
8
35-3
6
33-3
4
31-3
2
29-3
0
27-2
8
25-2
6
23-2
4
21-2
2
<20
NU
MB
ER O
F PA
RTI
CIPA
NTS
national Parkinson fou ndation 7
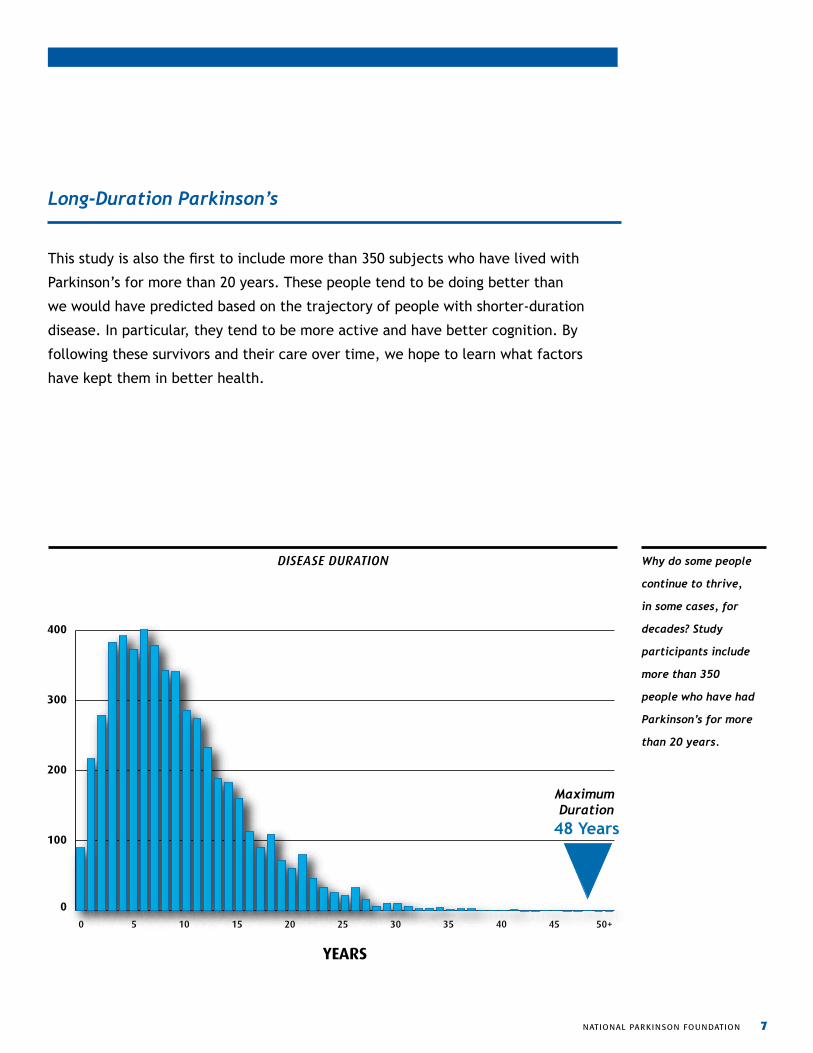
This study is also the first to include more than 350 subjects who have lived with
Parkinson’s for more than 20 years. These people tend to be doing better than
we would have predicted based on the trajectory of people with shorter-duration
disease. In particular, they tend to be more active and have better cognition. By
following these survivors and their care over time, we hope to learn what factors
have kept them in better health.
disEasE dURatioN Why do some people
continue to thrive,
in some cases, for
decades? Study
participants include
more than 350
people who have had
Parkinson’s for more
than 20 years.
Long-Duration Parkinson’s
0
100
200
300
400
50+454035302520151050
DISEASE DURATION
Maximum Duration
48 Years
YEARS
8 nat ional Parkinson foundation
While the participants in our study are unusually diverse, they share one thing in
common: they all have received care at specialty clinics in academic medical centers
designated by NPF as Centers of Excellence. These centers are recognized leaders in
Parkinson’s care and meet rigorous criteria for research, care and outreach, evaluated
in a peer-review site visit.
The benefits of expert care are well established: those who see an expert neurologist
live longer, better lives than those who don’t. However, even specialized centers have
different approaches to care, and achieve different outcomes.
What, exactly, do various centers do differently? Measuring those differences is our
first goal. Are those differences the real reason for better outcomes? Testing those
explanations is our second goal. And finally, what is the best way to share these
findings with everyone who provides Parkinson’s care?
Ultimately, the Parkinson’s Outcomes Project is a cycle of learning. Physicians and
therapists need to teach what they’ve learned, learn what others have to teach, then
repeat. Together, we can help everyone committed to discovering, understanding
and sharing the most effective ways to treat Parkinson’s.
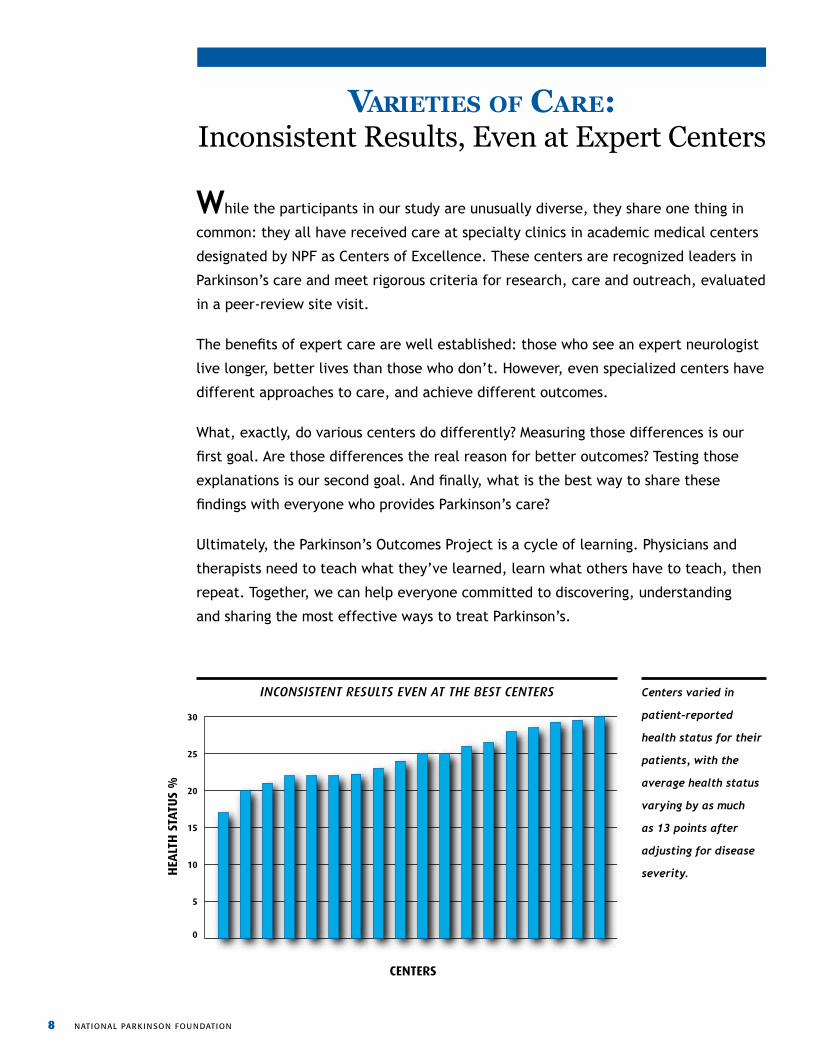
varieties of care: Inconsistent Results, Even at Expert Centers
iNcoNsistENt REsUlts EvEN at thE BEst cENtERs Centers varied in
patient-reported
health status for their
patients, with the
average health status
varying by as much
as 13 points after
adjusting for disease
severity.
Inconsistent Results Even at the Best the Centers
0
5
10
15
20
25
30
HEA
LTH
STA
TUS
%
CENTERS
national Parkinson fou ndation 9
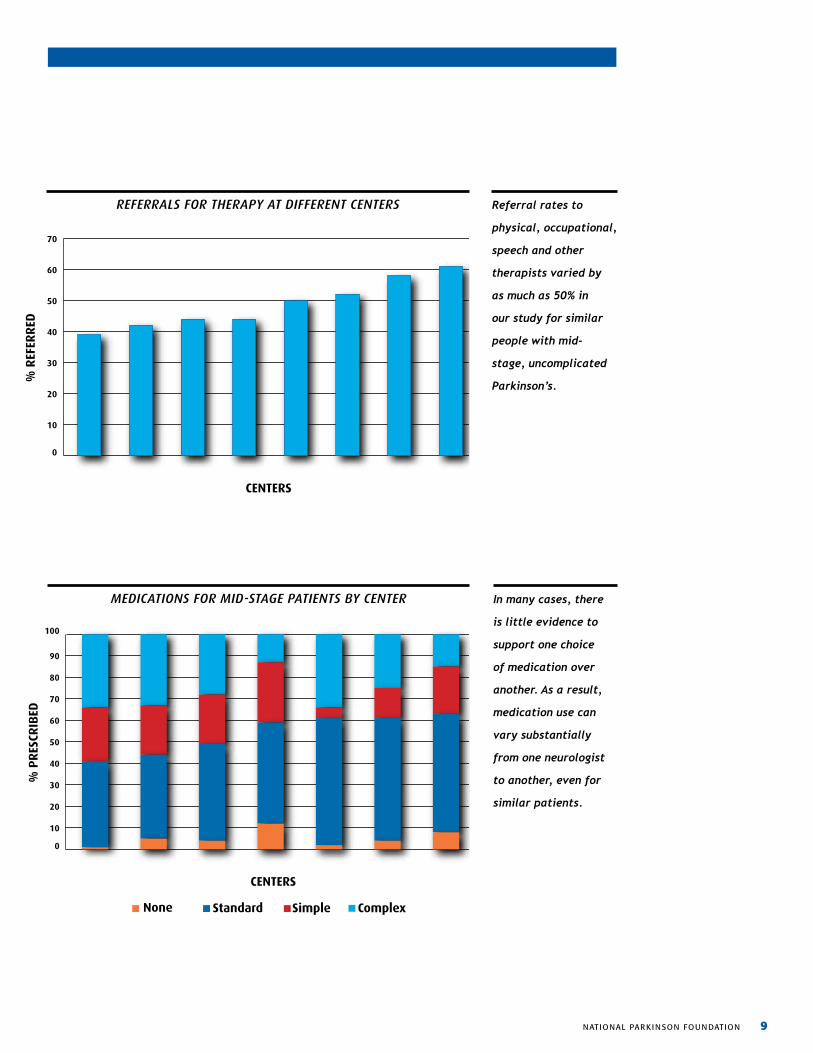
Referrals for therapy at different centers
0
10
20
30
40
50
60
70
CENTERS
% R
EFER
RED
Referral rates to
physical, occupational,
speech and other
therapists varied by
as much as 50% in
our study for similar
people with mid-
stage, uncomplicated
Parkinson’s.
REfERRals foR thERapy at diffERENt cENtERs
MEdicatioNs foR Mid-staGE patiENts By cENtER In many cases, there
is little evidence to
support one choice
of medication over
another. As a result,
medication use can
vary substantially
from one neurologist
to another, even for
similar patients.
MEDICATIONS FOR MID-STAGE PATIENTS BY CENTER
0
10
20
30
40
50
60
70
80
90
100
%
PR
ESCR
IBED
CENTERS
None Standard Simple Complex
10 nat ional Parkinson foundation
managing mood: The Importance of Addressing
Depression and AnxietyA clear finding of the study is that, taken together, depression and anxiety have
the greatest impact of health status. In fact, in a study of QII data presented at
a Parkinsons conference in 2012, scientists showed that the impact of depression
on health status is almost twice that of the motor impairments universally
associated with Parkinson’s.
At least 50 percent of people with Parkinson’s experience depression, and anxiety
is also frequently reported. Depression can be disabling, resulting in difficulty with
work or engaging in activities like exercise that can help manage symptoms. Yet
physicians often have trouble recognizing anxiety and depression, or their roles in
hampering efforts to treat Parkinson’s.
As previous studies have found, addressing depression can positively impact levels
of disability, relapse and quality of life. Indeed, participants in clinics with the most
active approach to counseling reported the lowest rates of depression. For many
people with Parkinson’s, acknowledging depression is a critical step toward more
effective treatment, and better health status overall.
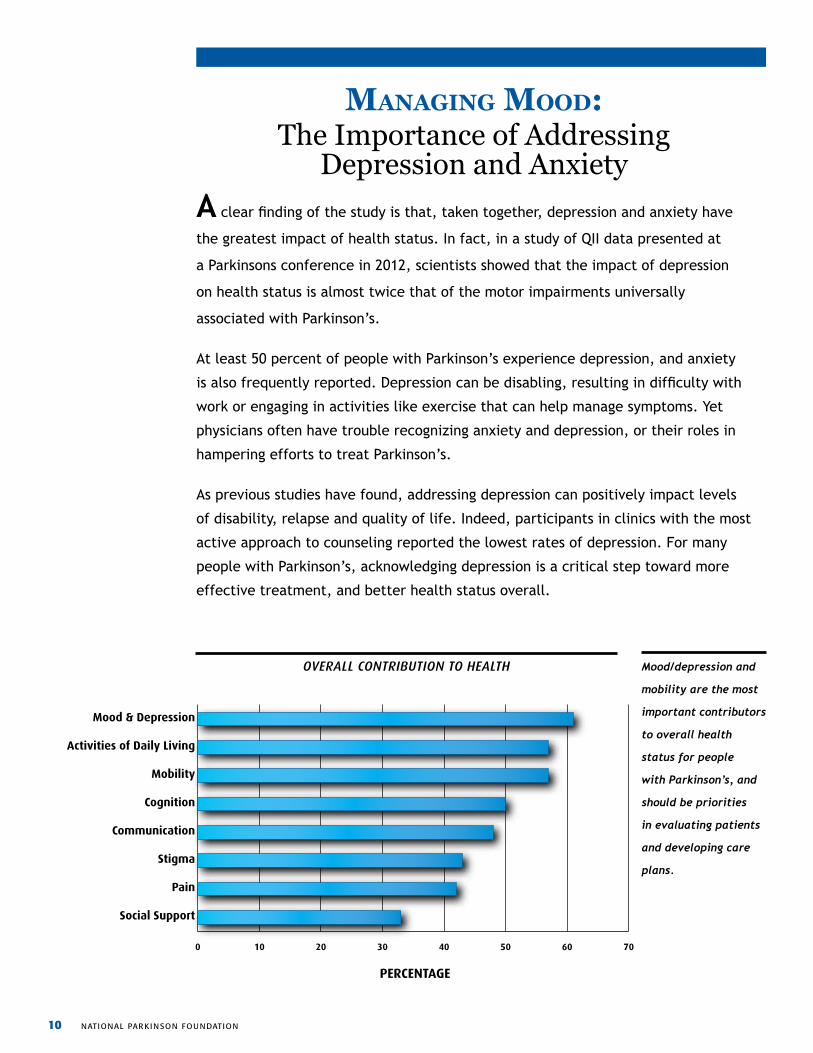
ovERall coNtRiBUtioN to hEalth Mood/depression and
mobility are the most
important contributors
to overall health
status for people
with Parkinson’s, and
should be priorities
in evaluating patients
and developing care
plans.
Overall Contribution to Health
0 10 20 30 40 50 60 70
Social Support
Pain
Stigma
Communication
Cognition
Mobility
Activities of Daily Living
Mood & Depression
PERCENTAGE
national Parkinson fou ndation 11
Depression in Parkinson’s disease is mainly caused by a chemical imbalance in
the brain; however, it can also arise from the simple sadness associated with the
diagnosis of the disease.
Antidepressants are often effective in reducing symptoms, but they should seldom
be used in isolation. A mix of medication, exercise and counseling is typically most
helpful in addressing depression, and may help further engage patients and families in
other critical aspects of managing care for Parkinson’s.
Depression in Parkinson’s Disease
NPF Recommends: • Physicians should screen you for depression at least once a year.
• You should discuss any change in your mood with a healthcare professional, and make sure that your Parkinson’s doctor is aware.
• You should bring a family member with you to your doctor’s office and he or she should be encouraged to discuss any changes in your mood.
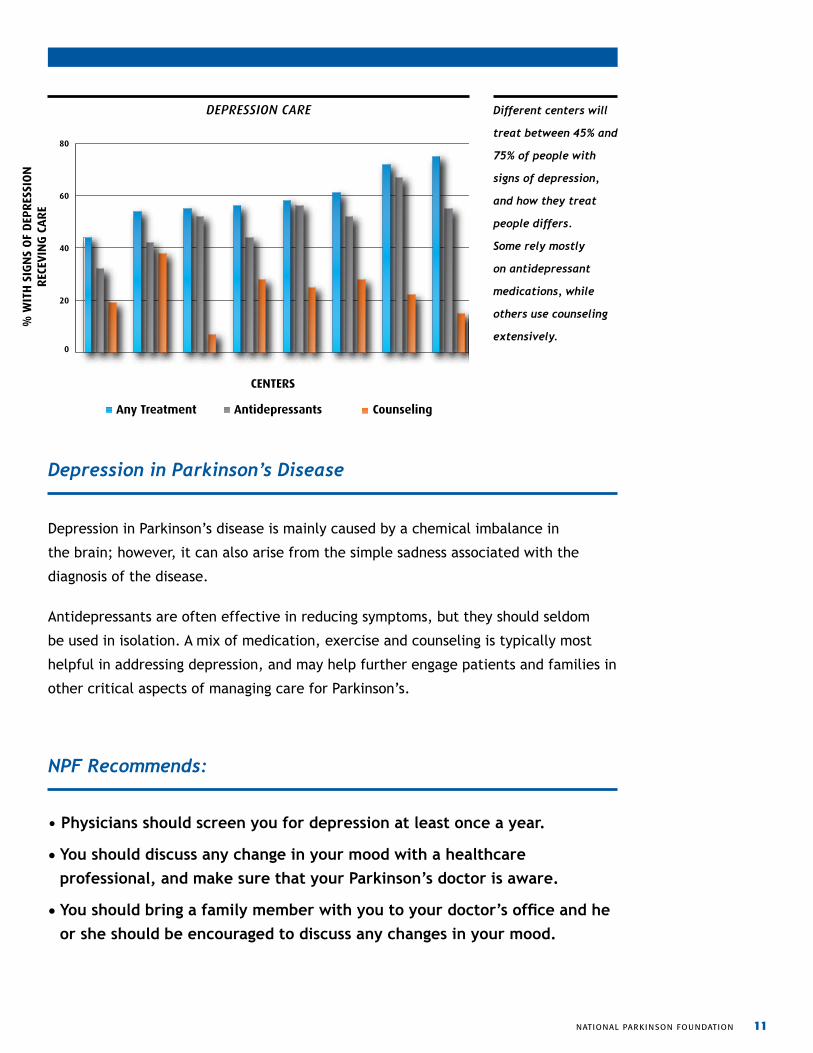
dEpREssioN caRE Different centers will
treat between 45% and
75% of people with
signs of depression,
and how they treat
people differs.
Some rely mostly
on antidepressant
medications, while
others use counseling
extensively.
Depression Care
0
20
40
60
80
% W
ITH
SIG
NS
OF
DEP
RES
SIO
NR
ECEV
ING
CA
RE
CENTERS
Any Treatment Antidepressants Counseling
12 nat ional Parkinson foundation
mobility: Second Most Important Driver
of Health StatusBradykinesia, or slowness of movement, is present in all cases of Parkinson’s. Indeed, impaired mobility in general is considered a defining element of the disease, and it
was the second most influential factor on health status among study participants.
The impact of mobility problems can be serious. They can affect your balance, your
ability to walk, and even everyday tasks such as feeding and bathing. These problems
can result in falls, injury and even death. In addition, difficulty walking can keep you
from doing things that are important to you. Withdrawal from familiar activities can
affect personal relationships, and even how you think others perceive you.
The best way to protect your motor function is to use it regularly. A well-designed
exercise plan can significantly improve almost everything about your health, including
stabilizing your walking, calming tremor, improving mood, and possibly even slowing
progression of the disease. Regular exercise is typically associated with a lower care
burden, as well. Even as motor symptoms progress, many respond well to medical and
surgical treatment. But staying active remains absolutely critical.
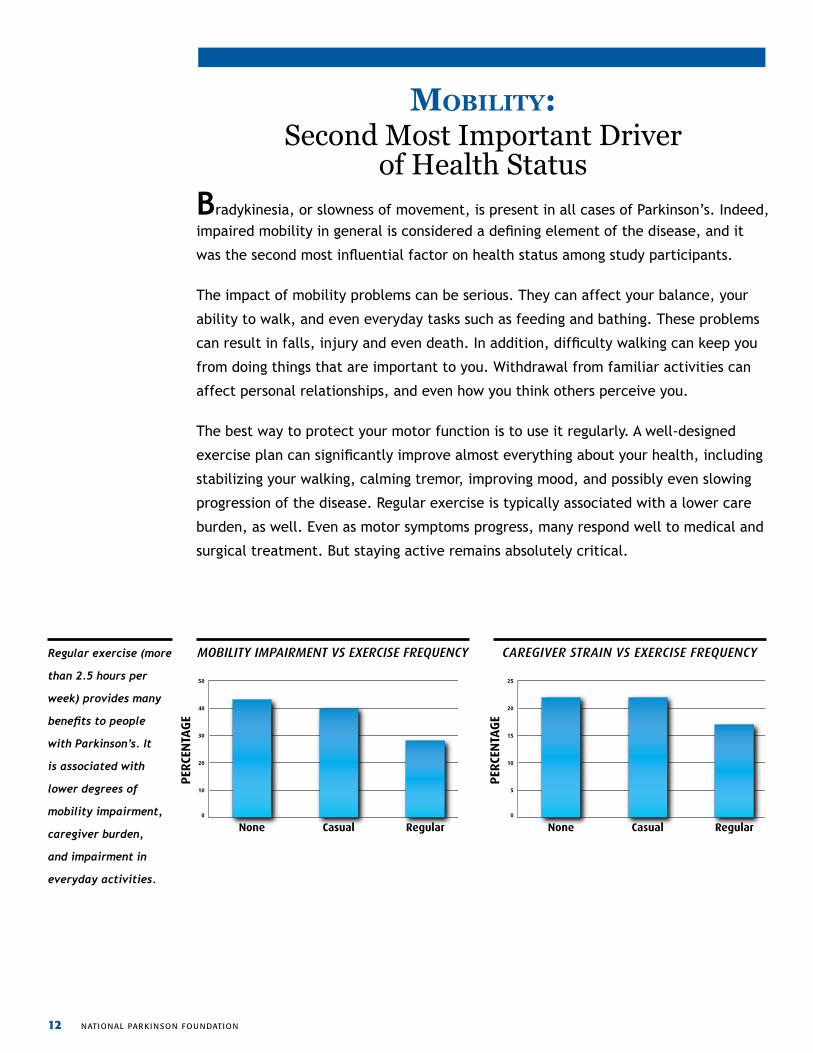
Regular exercise (more
than 2.5 hours per
week) provides many
benefits to people
with Parkinson’s. It
is associated with
lower degrees of
mobility impairment,
caregiver burden,
and impairment in
everyday activities.
0
5
10
15
20
25
RegularCasualNone
Caregiver Strain vs Exercise Frequency
PER
CEN
TAG
E
0
10
20
30
40
50
RegularCasualNone
Mobility Impairment vs Exercise Frequency
PER
CEN
TAG
E
MoBility iMpaiRMENt vs ExERcisE fREqUENcy caREGivER stRaiN vs ExERcisE fREqUENcy
national Parkinson fou ndation 13
NPF Recommends:
• To feel good enough to exercise regularly, take your medications on time.
Keep to your schedule.
• Exercise can help improve all your symptoms. Any exercise you can do safely will help.
• Talk with your doctor about both exercise and physical therapy. On your next visit, discuss the type of program you should pursue.
• If your symptoms become hard to manage, talk to your doctor about your options. There are many ways to try to control difficult symptoms.
• A physical or occupational therapist who understands Parkinson’s can be a great resource between your physician visits.
Although mobility impairment is a central challenge of Parkinson’s, early data from
the QII study suggests the importance of a holistic approach. People who addressed
mood and mobility together, and who used a full complement of elements including
medicine, surgery and exercise, were the most successful in managing the mobility
aspects of their condition.
Your symptoms are connected. Better mobility reduces depression, treating
constipation helps with mobility, and so on. Talk to your doctor about whatever is
bothering you.
Mobility and Motor Control: Findings of the Quality Improvement Initiative
14 nat ional Parkinson foundation
the future of Parkinson’s: The Evidence We Need to Personalize Care
No two people face Parkinson’s in quite the same way. People vary substantially in
their combination of symptoms, rate of progression, and reaction to treatment.
It may be that no two doctors approach Parkinson’s in quite the same way, either;
unlike many other diseases, there are no clearly established standards for treating a
person with Parkinson’s in a particular circumstance. As a result, two neurologists who
might prescribe identical therapies for similar patients with Alzheimer’s disease would
likely recommend different strategies for similar patients with Parkinson’s.
The reason is that, despite many prior studies on specific elements of the disease,
none has successfully evaluated the full range of factors that bear on the experience
of the disease. The Parkinson’s Outcomes Project is beginning to change that.
By embracing the diversity of people with Parkinson’s, we are gathering the most
complete data set ever assembled. By involving the world’s best neurologists at
NPF Centers of Excellence, we are developing the best insights into individual
care. And by working together, we will define standards of care for people with
Parkinson’s everywhere.
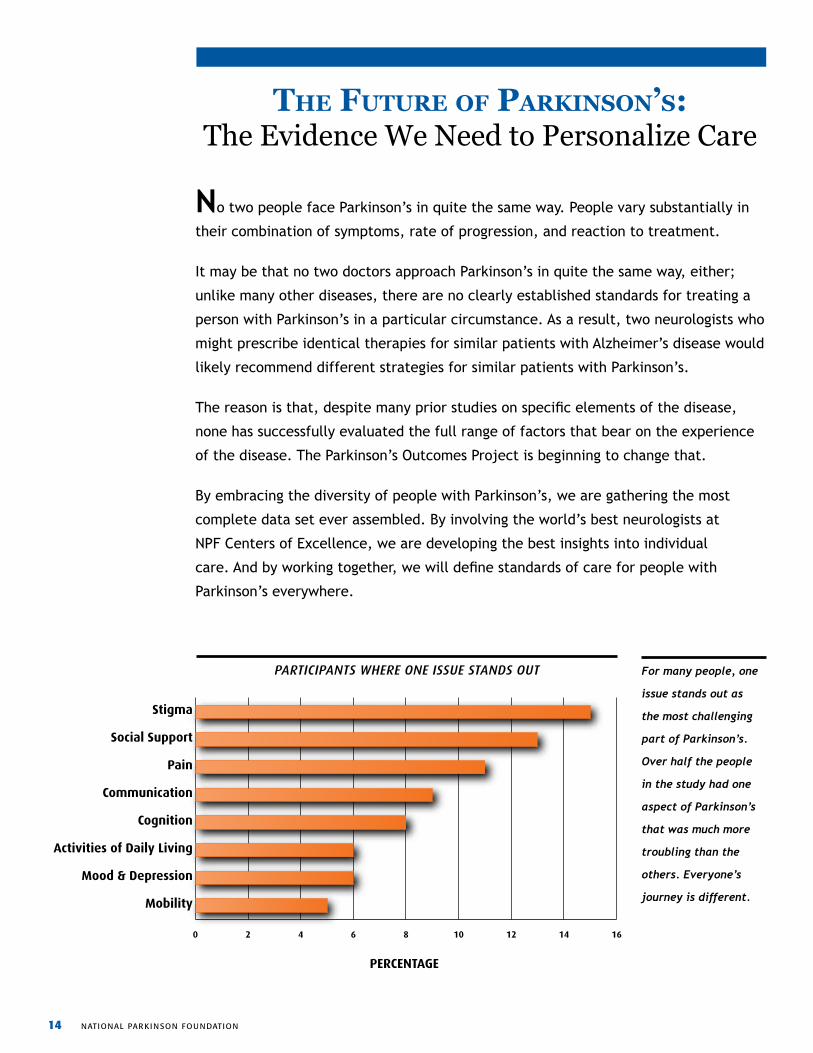
For many people, one
issue stands out as
the most challenging
part of Parkinson’s.
Over half the people
in the study had one
aspect of Parkinson’s
that was much more
troubling than the
others. Everyone’s
journey is different.
Participants where one issue stands out
0 2 4 6 8 10 12 14 16
Mobility
Mood & Depression
Activities of Daily Living
Cognition
Communication
Pain
Social Support
Stigma
PERCENTAGE
paRticipaNts whERE oNE issUE staNds oUt
national Parkinson fou ndation 15
Baylor College of Medicine Houston, TX
Joseph Jankovic, MD
Center PrinCiPal investigator
Christine Hunter, RN, CCRC
Center Coordinator
Beth Israel Deaconess Medical Center Boston MA
Daniel Tarsy, MD
Center PrinCiPal investigator
Althea Silver, MPH, BSN, RN
Center Coordinator
Georgia Health and Science University Augusta, GA
John Morgan, MD, PhD
Center PrinCiPal investigator
Lisa Bush
Zachary Martin
Center Coordinators
Georgetown UniversityWashington, DC
Fernando Pagan, MDCenter PrinCiPal investigator
Helen Howard, MA, RNCenter Coordinator
Johns Hopkins University Baltimore, MD
Zoltan Mari, MD
Center PrinCiPal investigator
Rebecca Dunlop, RN, BSN
Arita McCoy, RN
Center Coordinators
Centre for Movement Disorders Toronto, Canada
Mark Guttman, MD
Center PrinCiPal investigator
Alanna Sheinberg
Kevin Sorokin
Center Coordinators
Mount Sinai Medical Center New York, NY
Barbara Changizi, MD
Center PrinCiPal investigator
Joan Bratton
Amber Servi
Center Coordinators
Muhammad Ali Parkinson Center of Barrow Neurological Institute Phoenix, AZ
Anthony Santiago, MD
Center PrinCiPal investigator
Margaret Anne Coles, BSR, MQI, OTR/L
Patty Hatton, CTRS
Center Coordinators
Northwestern University Chicago, IL
Tanya Simuni, MD
Center PrinCiPal investigator
Elaina Ziehm
Center Coordinator
Parkinson’s outcomes Project: Participating Centers of Excellence
The QII, part of the Parkinson’s Outcome Project, is overseen by a steering committee of the lead
investigators at each participating NPF Center of Excellence and a group of leaders in care quality from
the broader community.
At the 20 participating centers, 153 physicians, supported by 96 research assistants, have participated in
delivering care to the more than 5,500 people with Parkinson’s in the study. Each of these individuals is
engaged daily in delivering the best care they can to people with Parkinson’s, and each joins us in our
goal of changing the course of Parkinson’s.
16 nat ional Parkinson foundation
Oregon Health and Science University Portland, OR
John Nutt, MD
Center PrinCiPal investigator
Anna Lovelace
Center Coordinator
Parkinson’s Institute and Clinical Center Sunnyvale, CA
Melanie Brandabur, MD
Center PrinCiPal investigator
Lizza Reys
Center Coordinator
Struthers Parkinson’s Center Golden Valley, MN
Sotirios Parashos, MD, PhD
Center PrinCiPal investigator
Joan Gardner, RN
Catherine Wielinski, MPH
Center Coordinators
University of Florida Gainesville, FL
Michael Okun, MD
study advisor
Irene Malaty, MD
Center PrinCiPal investigator
Amanda Eilers
Center Coordinator
University of Kansas Medical Center Kansas City, KS
Kelly Lyons, PhD
Center PrinCiPal investigator
Jessica Cooper, BS, BGS
Center Coordinator
University of South Florida Tampa, FL
Robert Hauser, MD, MBA
Center PrinCiPal investigator
Claudia Rocha
Holly Delgado, RN
Center Coordinators
Vanderbilt University Nashville, TN
Thomas Davis, MD
Center PrinCiPal investigator
Kelly Arney, MSSW
Center Coordinator
University of Pennsylvania Philadelphia, PA
Nabila Dahodwala, MD
Center PrinCiPal investigator
James Minger
Center Coordinator
Radboud University Nijmegen Medical Center Nijmegen, The Netherlands
Bastiaan Bloem, MD
Center PrinCiPal investigator
Bart Post, MD
Center Coordinator
Tel-Aviv Sourasky Medical Center Tel-Aviv, Israel
Nir Giladi, MD study advisor
Tanya Gurevich, MD
Center PrinCiPal investigator
Naama Cohen
Dana Yekutieli Tzur, BSc
Center Coordinators
Toronto Western Hospital Toronto, Canada
Janis Miyasaki, MD, FRCPC
Center PrinCiPal investigator
Julie Racioppa
Center Coordinator
Other Study Advisors
Eric Cheng, MD
University of California San Francisco,
San Francisco, CA
Laura Marsh, MD Michael E. DeBakey VA Medical Center,
Houston, TX
national Parkinson fou ndation 17
The main findings reported in this document are derived from the QII study and presentations and
publications based on its information. These publications include:
A. Hassan, S.S. Wu, P. Schmidt, I. Malaty, Y.F. Dai, J.M. Miyasaki, M.S. Okun. What are the issues facing
Parkinson’s disease patients at ten years of disease and beyond? Data from the NPF-QII study. Parkinsonism
and Related Disorders. 2012. 18(8):925-30.
A. Hassan, S.S. Wu, P. Schmidt, I. Malaty, M.S. Okun, Risk Factors for ER and Hospitalization in Parkinson’s
disease: Results from the NPF Quality Improvement Initiative (NPF-QII). Movement Disorders Society 16th
International Congress. Dublin, Ireland. 2012.
J.D. Jones, I. Malaty, C.C. Price, M.S. Okun, D. Bowers. Health comorbidities and cognition in 1948 patients
with idiopathic Parkinson’s disease. Data from the NPF-QII study. Parkinsonism and Related Disorders. 2012.
In press.
M. Kwasny, O. Oguh, B. Stell, T. Simuni, on behalf of the NPF-QII investigators. Speech therapy utilization in
Parkinson’s disease. Movement Disorders Society 16th International Congress. Dublin, Ireland. 2012.
J.G. Nutt, A.D. Siderowf, M. Guttman, E.C. Nelson, P. Schmidt, J. Zamudio, S.S. Wu, M.S. Okun, on behalf
of the NPF-QII investigators. Correlates of health-related quality of life (HRQL) in Parkinson’s disease.
Movement Disorders Society 16th International Congress. Dublin, Ireland. 2012.
O. Oguh, M. Kwasny, J. Carter, T. Simuni, on behalf of the NPF-QII investigators. Predictors of caregiver
burden in Parkinson’s disease. Movement Disorders Society 16th International Congress. Dublin, Ireland.
2012.
O. Oguh, M. Kwasny, T. Simuni C., Zadikoff on behalf of the NPF-QII investigators. Racial disparities in access
to deep brain stimulation. Movement Disorders Society 16th International Congress. Dublin, Ireland. 2012.
O. Oguh, M. Kwasny, B. Stell, T. Simuni, on behalf of the NPF-QII investigators. Predictors of caregiver
burden in Parkinson’s disease. American Academy of Neurology 64th Annual Meeting. New Orleans, Louisiana.
2012.
References
18 nat ional Parkinson foundation
O. Oguh, M. Kwasny, B. Stell, T. Simuni, on behalf of the NPF-QII investigators. Predictors of exercise habits
in Parkinson’s disease. Movement Disorders Society 16th International Congress. Dublin, Ireland. 2012.
M.S. Okun, A. Siderowf, J.G. Nutt, G.T. O’Conner, B.R. Bloem, E.M. Olmstead, M. Guttman, T. Simuni,
E. Cheng, E.V. Cohen, S. Parashos, L. Marsh, I. Malaty, N. Giladi, P. Schmidt, J. Oberdorf,. Piloting the NPF
data-driven quality improvement initiative. Data from the QII study. Parkinsonism and Related Disorders.
2010. 16(8):517-21.
S.A. Parashos, C.L. Wielinski, on behalf of the NPF QII investigators. National Parkinson Foundation Quality
Improvement Initiative: Risk Factors for Falls in Parkinson Disease. Movement Disorders Society 16th
International Congress. Dublin, Ireland. 2012.
P. Schmidt, M.S. Okun, A.D. Siderowf, J.G. Nutt, G.T. O’Conner, B.R. Bloem, E.M. Olmstead, M. Guttman,
T. Simuni, E. Cheng, S.A. Parashos, L. Marsh, I.A. Malaty, N. Giladi, S.S. Wu, J. Oberdorf. Are results from PD
trials generalizable? The NPF database reveals a mismatch between typical clinic populations and subjects in
PD trials. World Parkinson’s Congress 2nd International Congress. Glasgow, Scotland. 2010.
P. Schmidt, A.D. Siderowf, M. Guttman, E. Nelson, J. Zamudio, M.S. Okun, J.G. Nutt, on behalf of the NPF-
QII investigators. How should pushing off or the use of assistive devices be incorporated in the timed up and
go (TUG)? Movement Disorders Society 16th International Congress. Dublin, Ireland. 2012.
P. Schmidt, J. Zamudio, M. Guttman, J. Nutt, A. Siderowf, E. Nelson, on behalf of the NPF-QII investigators.
Variation of patient-reported outcomes (PDQ-39) in a cross-sectional analysis of the NPF-QII research
registry. American Academy of Neurology 64th Annual Meeting. New Orleans, Louisiana. 2012.
P. Schmidt. Current and future impact on clinical practice. Movement Disorders Society 16th International
Congress. Dublin, Ireland. 2012.
B. Stell , O. Oguh, M. Kwasny, T. Simuni, on behalf of the NPF-QII investigators. Utilization of antidepressants
and mental health services in a large cohort of patients with Parkinson’s disease. Movement Disorders
Society 16th International Congress. Dublin, Ireland. 2012.
national Parkinson fou ndation 19
In addition to the QII study, important points and recommendations concerning Parkinson’s are drawn
from a range of publications, including:
J.M. Miyasaki, K. Shannon, V. Voon, B. Ravina, G. Kleiner-Fisman, K. Anderson, L.M. Shulman, G. Gronseth,
W.J. Weiner; Quality Standards Subcommittee of the American academy of neurology. Practice Parameter:
evaluation and treatment of depression, psychosis, and dementia in Parkinson disease (an evidence-based
review): report of the QualityStandards Subcommittee of the American Academy of Neurology. Neurology.
2006. 66(7):996-1002.
S.K. Van Den Eeden, C.M. Tanner, A.L. Bernstein, R.D. Fross, A. Leimpeter, D.A. Bloch, L.M. Nelson. Incidence
of Parkinson’s disease: variation by age, gender, and race/ethnicity. American Journal of Epidemiology. 2003.
157(11):1015-22.
J.M. Pavon, H.E. Whitson, M.S. Okun. Parkinson’s disease in women: a call for improved clinical studies and
for comparative effectiveness research. Maturitas. 2010. 65(4) 352-8.
C. Goetz, W. Poewe, O. Rascol, C. Sampiro, G.T. Stebbins, C. Counsell, N. Giladi, R.G. Holloway, C.G. Moore,
G.K. Wenning, M.D. Yahr, L. Seid; Movement Disorder Society Task Force on Rating Scales for Parkinson’s
Disease. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and
recommendations. Movement Disorders. 2004. 19(9):1020-8.
L.O. Ramig, S. Sapir, S. Countryman, A.A. Pawlas, C. O’Brien, M. Hoehn, L.L. Thompson. Intensive
voice treatment (LSVT) for patients with Parkinson’s disease: a 2 year follow up. Journal of Neurology,
Neurosurgery, and Psychiatry. 2001. 71(4):493-8.
20 nat ional Parkinson foundation
Over the past two years, the National Parkinson Foundation has invested more than $2 million in this study.
This important research initiative is made possible by the support of thousands of people like you who
made a donation to support the National Parkinson Foundation, and generous support from the following
foundations and corporations:
Abbott
Braman Family Foundation, Inc.
Major League Baseball Players Trust
Parkinson Association of Minnesota
Parkinson’s Unity Walk
South Palm Beach County, Chapter of the National Parkinson Foundation
St. Jude Medical
Teva Neuroscience, Inc.
The Greenberg-May Foundation, Inc.
The Kinetics Foundation
The Leir Charitable Foundation
The Thompkins-Broll Family Foundation
QII Study Support
About the National Parkinson Foundation
Unique among the Parkinson’s organizations, the National Parkinson
Foundation (NPF) has a singular focus: our mission is to improve
the quality of care through research, education and outreach.
We have created a global network serving the needs of the
Parkinson’s community including:
• 41 Centers of Excellence at top medical centers around the world,
including 26 in the U.S. and 15 internationally
• An extensive network of chapters and support groups across
the U.S., serving more than 100,000 people with Parkinson’s
and their families
• Website and educational materials that reach more than
1 million people each year.

Find Answers. Change Lives. Beat Parkinson’s.
1501 NW 9th AvenueBob Hope RoadMiami, FL 33138
Parkinson.org web305.243.6666 office305.243.6073 fax800.4PD.INFO helpline





























