Embed Size (px)
Citation preview

P»TCHOPHY^1OUX)Y Vol. 28, No .1C"opyn«lil « IWI by The Socmy for P»ychophy«iologic«l Rejarch, Ine Pnnicd in 1) ,S A
P300 in Patients with Unilateral Temporal Lobectomies:The Effects of Reduced Stimulus Quality
MARTEN K. SCHEFFERS, RAY JOHNSON, JR.,
Cognitive Neuro.science Section, Medical Neurology Branch. National Institute of NeuorologicalDisorders and Stroke. The National Institutes of Health. Bethesda. Maryland
AND DANIEL S. Rue HKIN
Department of Physiology. University of Maryland School of Medicine. Baltimore. Maryland
ABSTRACT
The effects of stimulus quality on the amplitude, peak latency, onset latency, and duration of theP300 component of the event-related brain potential were studied In patients with either a left or aright anterior temporal lobectomy and in normal controls. Stimulus quality was reduced by adding"noise" letters to words wbicb signalled eitber a left or a rigbt hand button press. C'onsistent withan interpretation that stimulus quality affects the subject's degree of equivocation, P300 peaklatency, reaction time, and errors were all inversely related to stimulus quality, wbereas I*.3OOamplitude was directly related to stimulus quality. Tbere were no significant differences fn-tweennormal controls and eitber patient group for any of tbe KRF parameters or reaction time. RIgbttemporal lobectomy patients made, bowever, significantly more errors, particularly on tbe catcbtrials, whicb suggests tbat tbey did not process tbe stimuli as tborougbly and accurately as tbesubjects in tbe otber two groups. The absence of significant group differences in eitber the lateralsymmetry or overall P300 amplitude extends the evidence against tbe idea that anterior temporallobe structures make any substantial contribution lo the scalp P30<) in a visual discriminationparadigm. Because of observed delays in tbe onset of P.3fK) in tbe low-quality stimulus condition,procedures were developed to quantify botb P300 onset latency and P.300 duration. Reduced stimulusquality significantly increased P300 onset latency whereas P.30fl duration remained unaffected,indicating tbat stimulus categorization must occur prior to, and not during, P300.
DKS( RIPfOR.S: P300, Neural generators, Iemporal lobectomy patients. Equivocation, P300onset and duration.
The F300 component of the event-related po- 1987), In scalp recordings under similar task con-tential (ERP) has been used as an electrophysio- ditions, however, neither the lateral symmetry norlogical index of the nature and timing of cognitive the overall amplitude of P30() was significantly al-processing(Johnson, 1986, 1988a; Pntchard, 1981). tered after unilateral temporal lobectomy (JohnsonRecently, the location ofthe neural generator(s) of & Fedio, 1986, Johnson, 1988b, 1989a; Stapleton,P300 has been investigated using indwelling intra- Halgren, &. Moreno, 1987), These latter data suggestcranial electrodes in patients with temporal lobe that anterior temporal lobe structures are neitherepilepsy. Using an oddball paradigm, these studies the sole generator nor a major contributor to thehave demonstrated the presence of locally-gener- scalp-recorded P3()0' elicited in the oddball para-ated (mtentials in anterior temporal lobe structures digm.which are functionally similar to the scalp-recordedP3(X) (Halgren, Squires, Rohrbaugh, Babb, & C ran-dall, 1980; Squires, Halgren, Wilson, & C randall, 'The vast majority of P3(K) findings are based on re-1983; Wood et al., 1984; Stapleton & Halgren, cordmgs from the midline, ornear-laleral, electrode sites.
Ciiven the accumulating evidence thai there are a numberD.S. Ruchkin was partially supported by U.S.P.H.S. of distinct neural generators underlying the scalp-recorded
grant NSI1199. P300 (e.g., Johnson 1989a; Ruchkin, Johnson, C anoune.Address requests for reprints to: Ray Johnson, Jr., or Ritter, & Hammer. 1990). it is possible that unilateral
Marten K. Scheffem, The National Institutes of flealth, temporal lobctlomies may affect P.KKI activity at far-lat-Building 10, Room 5C422, Bethesda, MD 20892. eral electrode sites. However, unless such amplitude cf-
274

Mav. 1991 P300, Stimulus Quality, and Temporal Lobectomy 275
Although the oddball paradigm provides a usefulmethod for eliciting P300 activity, it is not clearwhich brain functions and structures are involvedduring its performance. Additional informationabout the nature and/or generators of the P300should be gained by using paradigms that providesome functional information about different brainstructures. For example, functional asymmetrieshave been demonstrated between patients with re-moval of either the left or the right anterior tem-poral lobe (Milner, 1975), Thus, it has been wellestablished that left temporal lobectomy patientshave a verbal memory deficit whereas right tem-poral lobectomy patients suffer from impaired vi-sual perception under conditions that reduce thenormal redundancy of complex stimuli (Kimura,1963; Lansdell, 1968; Meier & French, 1965; Dorf,Mirsky, & Mishkin, 1965; Rosenthal & Fedio,1975).
The present study was an attempt to see whetherthe known differences between left and right tem-poral lobectomy patients would be reflected in theirERP activity. Thus, we manipulated perceptual dif-ficulty by reducing the quality of visually presentedstimuli. Given their visuo-perceptual deficits, righttemporal lobectomy patients were expected to havegreater difficulty in categorizing the stimuli, and
fects extend more medially lo a substantial degree, anysuch findings would appear to bear on generator activityunrelated to those responsible for the extensively studiedP3OOs found over the midline and near-lateral scalp.
thus to have smaller and later P3OOs. than eitherpatients witb a left temporal lobectomy or normalcontrols (cf.. Jobnson & Donchin. 1985). In addi-tion, because peak latency measures do not revealwhether delays in processing occur prior to or dur-,ing a component's appearance, P3(X) onset latencyand duration were quantified along witb peak la-tency.
Methods
Subjects
Seven normal controls, 7 f)atients with a left tem-poral lobectomy, and 7 patients with a right temporallobectomy were tested. The patient groups included 6left and 6 right temporal lobectomy patients who werereported previously (Johnson, 1988b), The patientshad the anterior pole of their left or right temporallobe surgically removed for the relief of intractableepilepsy. The excision extended an average of 4,5 cm(SD = ,7) from the tip of the temporal pole for lefttemporal lobectomy patients, and 7,1 cm (SD = .9) forright temporal lobectomy patients. The operation con-sisted of complete removal of pes, uneus, amygdala,and partial removal ofthe anterior hippocampal gyms(1,8 cm, SD=.9, and 2.2 cm, SD=,5, for the left andright temporal lobectomy patients respectively). Pa-tients were thoroughly screened to exclude cases withbilateral or extratemporal epileptogenic foci, the pres-ence of any other brain pathology, right hemispherespeech, or any history of psychiatric illness. Patientswere matched with normal controls on age and edu-cation. Additional patient data and neuropsychologi-cal test results are presented in Table I, .\ more ex-tensive description on cognitive functioning of these
Table 1Neurophyschotogical data
Groupi
ComrolsLeft TemporalsRight Temporals
Left Temporal!Right Temporal!
tcf^ Temporal*Right Temporals
Control!
N
777
Yean,
Range
1-144-19
Age
Sex Range
3M,2M,5M,
4F 28-565F 25-402F 29-50
PrtoptratiTe
Age, onad (yean)
Range
6mo-2 l3-20
postop.
Mean (SD)
8 (4,4)10(4.7)
Mean (SD)
6 (7,0)11 (6,8)
Inoatopvrativc
Age, larger)' (years)
Range Mean (SD)
16-36 24(6,7)20-38 27 (5,6)
(ytmn
1
Data
^Data
I )
Mean (SD)
42(10,9)34 ( 6,1)37 ( 7,0)
VIQ
93(11.3)107 (5.8)
No, No.Seizure Medication
Free Free
66
64
Edacalkm (yean)
Range 1
12-1610-169-16
WAIS-Meaa (SD)
PIQ
87(10,2)98 ( 8.5)
Mean (SD)
13.7(1.7)12 (1.7)13 (2.1)
FSIQ
90(9,8)102 (5,4)
WAIS-MeM (SD)
VIQ PIQ
94(12,4) 96 ( 6,2)109 ( 6.0) 102(12.0)
HI ( 9.5) 119(10,2)
FSIQ
94 (8.7)106 (6,7)
115(9,3)

276 SchefFers, Johnson, and Ruchkin Vol. 28. No. 3
patient.s may be found in Fedio, Martin, and Brouwers(1984), Ail subjects were right handed and had normal,or eorrected-to-normal, vision. The patients sufferedfrom small spots of diminished vision in the peripheralvisual field. The procedures were explained thoroughlyin advance and informed consent was obtained fromall subjects. The normal controls were paid for theirparticipation.
Procedure
The subjects had to perform a visual discriminationtask with a choice reaction time response in which theperceptual difficulty of the stimuli varied randomlyfrom trial to trial. Stimulus quality was manipulated toallow comparisons between the processing of "normal,"high-quality stimuli and low-quality stimuli. The high-quality stimuli were the words "LEFT" and "RITE,"whereas the low-quality stimuli were "XLXEXFXTX"and "XRXIXTXEX." All stimuli subtended a lateralvisual angle of less than 3° to ensure that the stimuliwere well inside the peripheral field cuts. The stimuliwere presented on a CRT for 300 ms in a random serieswith an average ISI of 2910 ms. All four possible stimuliwere presented equally often. In each block of 100 trials,there were 10 "catch" trials on which the stimuli weremis,spelled (i,e,, "LFET," "RTIE," "XLXFXEXTX,"and "XRXTXIXEX"), Subjects were instructed tomake fast and accurate button presses with the com-patible thumb and to withhold their response when theydetected the catch stimuli. Maximum acceptable reac-tion time was 2000 ms. Practice trials (15-30) were pre-sented before data collection was started, Tliroughoutthe experimental session, the subjects were seated in acomfortable chair in a darkened room.
Recording
TTie EEG was recorded with chlorided Grass silverdisc electrodes placed on the scalp at F ,̂ Cy, P?, F,,C,, P,, F4, C«, and P«, according to the International10-20 system, all referred to linked mastoid electrodes.The EEG was sampled on-line at 100 Hz for a re-eording epoch of 2150 ms, including a 150-ms pre-stimulus baseline. The data were low-pass filtered at35 Hz (3dB/octave roll-off) and high-pass filtered witha time constant of 10 s prior to digitizing. Eye move-ments (ECXJ) were recorded from electrodes placedbelow and above the nght eye, Tnals with ECXi arti-facts (i,c,, 6 sample points per epoch exceeding 50 MV)were discarded from further analysis. All single-trialEEG and response data, along with accompanyingidentification, were stored in digital format for sub-sequent analysis. Only correct trials were used in theaverages.
Quantification
To assess the effects of experimental variables oncomponent amplitudes, the mean amplitude within aspecified window was computed after subtracting theaverage activity in the 150-ms prestimulus baseline.Mean amplitude was used becau.se it is less susceptible
to the effects of latency variability.^ A symmetricalwindow around the peak latency for each componentwas identified in the individual-subject ERPs at bothlevels of stimulus quality. For P2 and N35O the win-dow was 80 ms wide and positioned around the peaklatency at F/. The P3 window was 160 ms wide andcentered around the peak latency at P̂ ,. Slow Wavewas measured within a window from 750-1450 ms.
Peak latencies for P2, N35O, and P300 were deter-mined with a peak-picking program which calculatedthe peak latencies for each component with a midla-tcncy procedure (Tukey, 1978). In this procedure, themaximum amplitude in a time window at a specifiedelectrode is found and then the component's slopesare searched to find the points at which amplitude was80% of the maximum value. These 80% latencies arethen averaged to yield a measure of the component'speak latency. To minimize interference from adjacentcomponents, the limits on the search windows andelectrode sites used in the peak-picking program were:100-300 ms for P2 (at F )̂, 200-450 ms for N35O (atFz), and 330-1000 ms for P3(X) (at P,), Prior to peakmeasurement, the individual-subject ERPs weresmoothed using a low-pass filter (cutoff—4,8 Hz at3dB),
The amplitude and latency data for each compo-nent were analyzed in separate repeated-measures AN-OVAs. Component amplitudes were first analyzed ina design with the factors Stimulus Quality (high/low),Eleetrode (9), and Group (3), and then in two separatedesigns, one using the data from the lateral electrodes(left hemisphere/right hemisphere) and the other usingthe data from midline electrodes (P/yCjr/Fj.), Ciroupeffects and simple effects of stimulus quality at eaehsingle electrode were also tested. Peak latencies for P2,N35O, and P300 were tested in an ANOVA with re-peated measures on stimulus Quality (high/low), andthe bctween-subjeets factor Group (3). ANOVA resultswere reported when significant at p<.()5. To correctfor the use of the repeated-measures ANOVA design,the degrees of freedom were corrected with the con-servative Greenhouse/Geisser prcKedure (Jennings &Wood, 1976),
Results
The grand-average waveforms for the high- andlow-quality stimuli at all electrode sites for the nor-mal controls are presented in Figure I, These datashow that the earliest deflections, P2 and N350,were particularly visible at the frontal and centralelectrode sites. They were followed by a P3()0, anda small amount of Slow Wave activity, which waspositive at all electrode sites. The grand-averagewaveforms for right and left temporal lobectomypatients (Figure 2) were morphologically quite sim-ilar to those of the normal controls, except for the
^Analyses on haseline-to-peak measurements pro-duced the same pattern of results.

May, 1991 PSOO, Stimulus Quality, and Temporal Lobectomy 277
NORMAL CONTROLS
FZ F-1
MSK;
too 1000
MSEC
FiRure L Grand-mean ERP waveforms for the normalcontrols at all nine electrode sites in response lo the high-quality (solid lines) and low quality (dashed lines) stimuli.In this and subsequent figures, stimulus onset is denotedby the " S " on the time scale and stimulus duration by thefilled rectangle. Positive voltages are plotted as downwarddeflections.
C3
LEFT TEMPORALS
CZ C4
03
RIGHT TEMPORALS
CZ C*
8 JOO 800 1000 1400MSEC
000 lOOO 1400MStC
S 900 too 1000 1400MSEC
FiRure 2. Grand-mean ERP waveforms for the \cf\. andright temporal lobectomy patients at the central electrodesites in response to high-quality (solid lines) and low-qual-ity (dashed lines) stimuli,
larger P2 component in the left temporal lobectomypatients.
P300
Amplitude. Although there appeared to be somedifferences in P3()0 across groups (Figure 3). theoverall ANOVA revealed no significant group ef-fects (/>'-,88) or Group X Electrode interactions.The former result indicates that there were no sub-stantial differences in overall amplitude whereas thelatter result indieates that the apparent alterations'n the scalp topography of P300 in the patients were
relatively small and not consistent enough to besignificant. The ANOVA on F^. C,. and P^ data alsoindicated that the midline P300 scalp distributionwas not altered due to the surgery (/7 = ,46).
Possible hemispheric differences in P300 be-tween the two patient groups are key to determiningwhether the anterior temporal lobe structures makeany significant contribution to the scalp-recordedP300 in this task. Planned comparisons showed thatP300 activity at the right hemisphere was largerthan at the left hemisphere (/•"( 1/18) = 5,2, p<.Q5).This difference was due to P300 amplitude beinglarger at \^^ and P^ tban at F, and P,. respectively(/•]; 1/18) = 5,2-6,6, ;'<,05), wbereas there were nosignificant differences between C, and C4. The bem-ispheric differences between P300 at the frontal andparietal electrodes were larger in the right temporallobectomy patients, slightly smaller in the left tem-poral lobectomy patients, and absent in normalcontrols (/̂ ((2/18) = 6.1, /7<.O1), These results sup-port the conclusion that when there were topo-graphical differences in P300 activity, it was be-cause the patient groups resembled each other morethan the controls, rather than being due to surgicallyrelated hemispheric asymmetries between the twopatient groups (Figure 3),
The ANOVA on the midline electrodes revealeda pattern of results similar to the overall ANOVA,which confirmed that P300 amplitude was reducedfor low-quality stimuli (/•\1/18)= 16,7, p<.0\). aneffect that was largest at the parietal electrodes andgradually decreased toward the frontal electrodes(/•T1/18)-25,9. p<,01; Figure 3), An analysis of thesimple effects of stimulus quality at each individualelectrode site revealed that these effects reached sig-nificance at parietal (/>s<.001) and central (;>s<.01)electrode sites, but not at frontal (/7s>,06) elec-trodes. Right temporal lobectomy patients did not
> '0
1r
CONTIXXS
A /\'•̂ • • • • . }
itrj
10
•
4
21
./J
•
TTMPOP
A
lALS
^
•
13
10
«
4
1
t
• (MMU.ITVOUMITV
Figure 3. Grand-mean P300 average amplitude at allnine electrode sites in response to high-quality (solid lines)and low-quality (dashed lines) stimuli for the normal con-trols (left panel) and the left (center panel) and nght (rightpanel) temporal lobectomy patients.

278 SchefFers, Johnson, and Ruchkin Vol. 28. No. 3
LEFT TEMPOHALS WGHT TEMPOBALS
QUALITY
Fignre 4. P2 latency (at F,), N35O latency (at F,), P300onset (at P,), P300 peak latency (at P,), and reaction timeas a function of stimulus quality for normal controls (leftpanel) and the left (center panel) and nght (nght panel)temporal lobectomy patients, P3(X) onset latency corre-sponds to the latency at 50% ofthe peak amplitude, P300on.sets were not measured in left temporal lobectomy pa-tients.
have smaller P3OOs, and there were no significantGroup X Stimulus Quality interactions in any ofthe analyses (/?s>,85).
Latency. P3(X) peak latencies (Figure 4) for low-quality stimuli were longer than those for high-qual-ity stimuli, although this difference was only mar-gjnally significant (fTl/l8)=3.6, p = ,074). The in-crease in P300 peak latency in right temporal lo-bectomy patients (16 ms) and left temporal lobec-tomy patients (24 ms) was not significantly smallerthan the 67 ms increase in the controls (/7=.53).
Although easy and convenient to obtain, peaklatencies reveal only the magnitude of overall pro-cessing delays without indicating the source(s) ofdelay. That is, processing delays can occur eitherpnor to a component's appearance, or by increasingthe component's duration. Inspection ofthe grand-average ERPs in Figures 2 and 3 reveals that P3OOselicited by low-quality stimuli not only peaked lat-er, but also appeared to have later on.sets comparedto those elicited by high-quality stimuli. Giventhese data, we analyzed the effects of reduced stim-ulus quality on P300 onset latency and duration.
In general, components have been quantified interms of their amplitude and peak latency, althoughthere have been a few instances in which onset la-tencies have been measured (Ritter, Simson,Vaughan, & Macht, 1982; Ritter, Simson, & Vaugh-an, 1983; Renault, Ragot, Lesevre, & Remond,1982). A component's onset is potentially impor-tant as a measure of the beginning of a particularstage of processing. Similarly, a component's du-
ration may index the duration of that processingstage. Ideally, it is desirable to measure onset andoffset latencies at the times at which the componentdeparts from and returns to baseline. However, dueto component overlap, it may not be feasible todetermine these time points either in all subjectswithin an experiment, or in all experiments. In suchcases, onset and offset latencies can still be char-acterized by using suitably defined points on theleading and trailing slopes of a component. For ex-ample, even wben onset/offset latencies are not ob-servable, latencies can be measured at amplitudesthat are a specified fraction of peak amplitude (e,g.,half-amplitude). Although such "fractional" laten-cies do not provide absolute measures of onset/offset latency, they do provide relative measures, inthe sense that "fractional" latencies covary with on-set/offset latencies. In addition, the use of fractionalamplitudes normalizes the data so that the resultingmeasures are independent of any within-subjectamplitude differences due to experimental manip-ulations or scalp distribution or across-subject dif-ferences in absolute amplitude. The particular frac-tional onset/offset latency selected depends uponwhere amplitude measurements can be obtainedfrom a large proportion ofthe subjects.
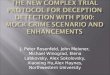
Latencies on the leading and trailing slopes ofthe P3(X) were calculated in 10% steps ofthe peakamplitude in the individual-subject waveforms, asshown schematically in Figure 5, To increase thereliability ofthe measurements, the ERPs were firstlow-pass filtered (3dB at 4,8 Hz) and, to minimizeoverlap with early components, the waveformsfrom P^ were used, A latency search window ex-tending from 330-1000 ms was used to avoid thepeak of N35O, The data from left temporal lobec-tomy patients were excluded from this analysis be-cause their large P2 failed to return to baseline be-fore P300 onset.
As shown in Figures 6a and 6c, this analysisdemonstrated that there was a fairly consistent in-crease in all the P300 onset and offset measures with
Figure 5. ERP waveform for an individual subject elic-ited by the high-quality stimuli, illustrating where the"fractional" latencies on the leading and trailing P3(X)slopes were obtained (filled circles).

May. 1991 P300, Stimulus Quality, and Temporal Lobectomy 279
NORMAL CONTROLS RIGHT TEMPORALSHIOM QU*lirlOW QU*llT
40
60
80
00
C• a• •
* G
• O
• D
• a• D
• O
• a. . . .«
o
• o
D •
O •
a •
300 400 500 800 700 800 900MSEC
B
900 400 soo edMSEC
700 800 900
20 W 80 100 80 60 40 20
P300 PEAK AMPLITUDE % P300 PSAK AMPLITUDE
Fifiure 6. P300 onset and offset times for normal controls (panel .\) andright temporal lobectomy patients (panel C). Onset and offset times on theleading and trailing slofxjs of P300. respectively, were computed at decreasingsteps of 10% of the peak amplitude. The number of normal controls (panelB) and right temporal lobectomy patients (Panel D) for which latency couldbe computed at each amplitude level on the leading and trailing P300 slopeare shown.
reduced stimulus quality, as was evident in thegrand-average waveforms (Figures 1 and 2), It isimportant to note that, due to individual differencesin the ERP waveforms, latency measures could notbe made at all levels of amplitude, and thereforethe size of the database decreased as baseline wasapproached. Figures 6b and 6d illustrate the num-ber of subjects for whom measurements could bemade at all levels on the leading and trailing slopes.Because of this variable number of subjects acrosslevels, separate ANOVAs were done on P300 onsetand duration for the levels between 50% and 90%of tbe peak amplitude. Given multiple tests (i.e., 5)for each type of latency measure, the critical valuewas set at .01. The results showed that P300 onsetwas significantly delayed by low-quality stimuli forboth the right temptiral lobectomy patients and thenormal controls, hut that P.300 duration was unaf-fected (Table 2). Although there was a significantgroup effect and a Group X Stimulus Quality in-teraction for P300 duration at the 50% and 80%levels, these isolated results indicate that the ap-parent shorter P300 duration for the patients wasnot consistent.
P2
Overall, P2 amplitudes in left temporal lobec-tomy patients were signiftcantly larger than thosein either controls or right temporal lobectomy pa-tients (/•T(2/18)-4.3, p<.05). There were no signif-
Table 2P300 onset latency and duration
Source of VaHadoa
90% Peak AmplitudeGroupStimulus Quality idf- \/\2YG X SQ
80% Peak AmplitudeGroupStimulus Quality (iif~\/\2)G X SQ{df-\/\2)
70% Peak AmplitudeGroupStimulus Quality (df- 1/11)G X SQ
60% Peak AmplitudeGroupStimulus Quality (df- I/I 1)G X SQ
50% Peak AmplitudeGroup ((/r-1/9)Stimulus Quality (df-\/\O)G X SQ(i/A-l/9)
FValaet
Onset Latency Dwatfcm
< l 1,312.I** 1,0<1 2.2
< l 2,342,9*^ < 1<1 6.0*
< l 4.729.9*~ 1,8< l 3.5
< l 4,043,3*« 1,7< I 4,0
<1 5.6*27.2**" I.I< l 20.0"
V/°provided only for significant results,•p<OS, ••p<.OOS, • ~ 0 0
icant hemispheric differences for P2 either acrossgroups or levels of stimulus quality in the ANOVAon the lateral electrodes. P2 was significantly largerat F, than at either C, or P^ (fTl/I8)= 10,8, p <,01), Neither P2 amplitude (Figure 7) nor P2 latency(Figure 4) was significantly affected by stimulusquality.

280 SchefFers, Johnson, and Ruchkin 28. No. 3
< A
LEFT TEMPOBALS RIGHT TEMPORALS
,0 P2 N360 ,n n N360
\ V
10
\
V X
ElECTROOe
Fignre 7, Grand-mean P2 and N35O average ampli-tudes at the midlinc electrodes in response to high-quahty(solid lines) and low-quality (dashed lines) stimuli for thenormal controls (left panel) and the left (center panel) andnght (nght panel) temporal lobcctomy patients.
Because N35O activity was manifested as a neg-ative deflection that remained on the positive sideof the prestimulus baseline (Figures I and 2), largerN35Os are indicated by smaller mean values (Figure7). Unlike P300, more N35O activity was elicitedwhen stimulus quality was reduced (/•!( 1/18)= 14.2,p<.0\). Activity over the right scalp increased morethan activity over the lefi scalp as a function ofstimulus quality {F(\/\S) = 6.9, p<.05). Across themidline, stimulus quality had its greatest impactover panetal scalp (F(I/I8)= 7.9, p<. 05), whichwas confirmed by tests of the simple effects at P,(;><.OOI), C, (/7= .001), and F, (/7= .02). N35Opeaklatency was not significantly affected by either stim-ulus quality or group (Figure 4),
Slow Wave
The grand-average ERPs in Figures 1 and 2 showthat overall, there was little Slow Wave activitypresent in either experimental condition, as indi-cated by a slightly less steep trailing slope of P300dunng its return to baseline. There were no effectsin any of the ANOVAs on Slow Wave activity thatapproached significance.
Performance Data
The reaction time and error data are presentedin Figure 4 and Table 3 respectively. Reductions instimulus quality resulted in significant increases inthe mean (fl( 1/18)-87.6, p<.001) and standard de-viation (Hl/18)-26.6, p<.OOI) of the responsetimes. There was no group effect or Group X Stim-ulus Quality interaction on reaction time, indicat-ing that there were no group differences in the speed
Table 3Means and standard deviations of error responses
Mean Error* (percent)(SDt in parenthcMi)
Re«pons<ii/Graap*
OmittedControlsLeft TemporalsRight Temporals
IncorrectC'otitrolsLeH TemporalsRight Temporals
CatchControl*tjeft TemporalsRight Temporals
Hlsh Qnallty
0.5 ( 0,7)0.4 ( 0.7)0.8 ( 1.3)
O.I ( 0.3)0.6 ( 1.1)2.2 ( 2.4)
9.t ( 1,8)7.9 ( 9.0)
19.3(14.9)
Low Qnallty
3.0 ( 4.0)0.8 ( L8)1.7 ( 2.6)
1.2 ( 1.0)1.3 ( 1.4)2.6 ( 3.7)
3t ,5( l9 .9)22.7(18.9)49.6 (32.5)
of processing. Omitted (/M( 1/18) = 6.0, p<,05) re-sponses, but not incorrect responses, increased sig-nificantly when stimulus quality was reduced. Thecatch trial data revealed that subjects made moreerroneous responses to misspelled words that werelow-quality than to misspelled words that werehigh-quality (f( 1/18)-= 12,4, /7<.01).» The threegroups differed in the number of errors with righttemporal lobectomy patients making more re-sponses to catch stimuli (/'\ 1/18) = 4.9, /?<.O5) andalso making marginally more incorrect responses(/•1(1/18)''3,4, /?=.O56) than either normal controlsor left temporal lobectomy patients. There were nosignificant group differences for the number ofomitted responses.
Discussion
ERP activity and behavioral performance werestudied in left and right temporal lobectomy pa-tients and normal controls when perceptual diffi-culty was manipulated. Both the ERP measures andthe performance data showed the usual relation tostimulus quality: P3()0 amplitude and response ac-curacy decreased while P300 peak latency and re-action time increased when stimulus quality wasreduced. Although P3(X) onset latency increased asstimulus quality decreased, P3(X) duration did not.Neither P2 amplitude nor P2 latency were affectedby the manipulation of stimulus quality. In accordwith previous data on essentially the same patients,larger P2s were elicited in the left temporal lobec-tomy patients than in either of the other two groups
'The subjects were also run in two blocked conditionsconsisting exclusively of cither high- or low-quality stim-uli. Given that all the results from these conditions wereidentical to the randomised condition, only the data fromthe catch trials arc included here. This exception wasmade in order to increase the reliability of the data fromthis infrequently occurring category of trials.

May, 1991 P300, Stimulus Quality, and Temporal Lobectomy 281
(Johnson, 1989a). Whereas N35O amplitude wasinversely related to stimulus quality, N35O latencywas not significantly altered.
The ERP and behavioral data clearly showedthat we successfully manipulated stimulus quality.Nevertheless, the expected group differences inP3()0 amplitude and latency did not materialize.The reason for the absence of a significant resultmay lie in the behavioral data. The fact that righttemporal lobectomy patients did not respond slow-er than the other two groups while making moreincorrect responses and failing to withhold their re-sponses more often on the catch trials, supports theidea that they used a strategy in which speed wastraded for accuracy. It is reasonable, therefore, tosuggest that these patients processed less of thestimulus (perhaps only one letter) than the subjectsin the other two groups. These behaviors are con-sistent with a visuo-perceptual deficit.
Previous studies have demonstrated the pres-ence of locally-generated potentials in anterior tem-poral lobe structures that are functionally similarto the scalp-recorded P300 in the oddball paradigm(e.g,, Halgren et al,, 1980; Squires et al.. 1983; Woodet al,, 1984; Stapleton & Halgren, 1987; McCarthy,Wood, Williamson, & Spencer, 1989), If these po-tentials were responsible in whole, or in part, forthe scalp-recorded P300, the effects of unilateral re-moval of one of two of these generators would bemanifested at the scalp in one of two ways. If thesebrain areas were the sole neural source for the scalpP300, we would expect to observe the unequivocalpresence of surgically-related hemispheric asym-metries. Altematively, if these areas were respon-sible for generating a sizable fraction of the totalamount of P300 activity that arose from a numberof intracranial sites, then we would expect to ob-serve a decrement in overall amplitude, perhapswith some surgically-related hemispheric asym-ttietry. To date, however, tests of these hypothesesusing patients with unilateral temporal lobectomieshave failed to find any significant alterations in themidline or near-lateral scalp-recorded P300 toeither auditory or visual versions of the oddballparadigm (Johnson & Fedio, 1986; Johnson, 1988b,1989a; Stapleton et al., 1987) or to a feedback par-adigm (Johnson & Fedio, 1987), Even using a mem-ory paradigm. Smith and Halgren (1989) failed tofind either a significant decrement in overall am-plitude or a significant asymmetry in P300 activity.The current findings extend this group of negativeresults to a visual discrimination paradigm.
In order to carefully evaluate the contributionof medial temporal lobe potentials to scalp ERPactivity, we eliminated all patients whose diseaseinvolved areas outside ofthe anterior temporal lobe
structures, including those with a psychiatric his-tory. Evidence of the stringency of our exclusioncriteria can be seen in the fact that six ofthe sevenpatients in each group have never had a seizurefollowing the surgery, whereas the remaining twocases have had no more than one per year. Thisfact strongly suggests that the extent ofthe diseasedtissue was confined to the medial temporal lobe andthat it was essentially all removed during the sur-gery. It is possible, therefore, that altered scalp po-tentials may be found in post-surgical studies inwhich the epilepsy patients constitute less homo-geneous groups than those described here. Becausethe same could be true in studies of pre-sut^icalepilepsy patients, great care must be taken in in-terpreting the results of studies based on hetero-geneous patient groups.
There are a number of possible reasons why theunilateral temporal lobectomies had little effect onthe scalp-recorded P3(X). First, although the rathergross morphological differences between the medialtemporal lobe P300-Iike potentials and the scalp-recorded P3OOs have been noted (Halgren, Staple-ton, Smith, & Altafullah. 1986), surprisingly littlehas been said about the timing differences betweenthem. In fact, with the exception of the report byStapleton and Halgren (1987), the latencies oftheP3CK) and medial temporal lobe potentials have notbeen reported. These authors found that the intra-cranial potentials/()//oMrJ the scalp P300 by 50 msfor stimuli in both auditory and visual modalities.This result is consistent with measurements madeby visual inspection of the figures in other reportsin which the latency of the medial temporal lobepotentials were delayed relative to the P.̂ OO by upto 100 ms (Halgren etal. 1980; Squires etal.. 1983),These latency data raise the possibility that the me-dial temporal lobe activity is responsible for gen-erating the Slow Wave component that follows theP300 rather than the P300 itself. Both componentsvary in much the same way in the oddball para-digm. Previous reports, however, have also failedto find any significant group differences or hemi-spheric asymmetries in Slow Wave activity, whichsuggests that medial temporal lobe activity is notthe neural source for the scalp-recorded Slow Wave(Johnson, 1988b. 1989a),
A second possible explanation of the minimaleffect ofthe surgeries on P300 amplitude involvesthe propagation of medial temporal lobe activity tothe scalp. Altafullah. Halgren. Stapleton, and Cran-dall (1986) found post-epileptic spike slow waveactivity that propagated to the lateral cortical sur-face from the same general area of the medial tem-poral lobe. They reported that, in comparison tothe attenuation of this slow wave aetivity, the sur-

282 Scheffers, Johnson, and Ruehkin Vol 28. No. 3
face P300 recorded at Fj. was about twice as largeas would be expected if the medial temporal lobewere the sole generator.
Third, because recent studies have shown thatthe scalp distribution is different for auditory, vi-sual, and somatosensory P300s (Barrett, Neshige,& Shibasaki, 1987; Johnson, 1989a, 1989b; Jobn-son, Miltner, & Braun, 1991), the fact that Mc-Carthy et al.'s (1989) medial temporal lobe poten-tials were modality independent would provide ad-ditional evidence against the hypothesis that thescalp-recorded P3(X) activity is related to the medialtemporal lobe activity.
The P3(X) amplitude and latency data, in con-junction with tbe behavioral results, are consistentwith the interpretation that reductions in stimulusquality increase the subject's a posteriori uncertain-ty about having correctly identified the stimulus(i.e., equivocation). Under these conditions, stim-ulus categorization time increases and the amountof information extracted from a stimulus decreases,as reflected by the increased P300 latencies, reactiontimes and response errors, and decreased P300 am-plitudes. These results are in accord with those ob-tained in previous experiments showing that thesubject's degree of equivocation about having cor-rectly identified a stimulus is a powerful determi-nant of P300 amplitude and peak latency (e.g..Johnson & Donchin, 1978, 1985; Kok & Looren deJong, 1980; Ruchkin & Sutton, 1978; Ruchkin, Sut-ton, & Mahaffey, 1987; McCarthy & Donchin,1981).
It has been argued that the P3(X) is elicited aftera stimulus has been categorized and that P300 peaklatency is directly related to stimulus categorizationtime (cf, Kutas, McCarthy, & Donchin, 1977), Theimplicit assumption in this argument is that P300duration does not vary with the difficulty of stim-ulus categorization, and thus that the peak latencyincrease is contingent on the delay in processesprior to P300 rather than being prolonged by in-creased variation within the P300 process itself. Al-though not noted previously, the data presented ina number of reports that manipulated perceptualdifficulty would support the position that P300 on-
set latencies are delayed, along with peak latencies,when stimulus categorization is more difficult (e.g..McCarthy & Donchin, 1981; Magliero, Bashore,Coles, & Donchin, 1984; Fitzgerald & Picton, 1983;Perrault & Picton, 1984),
Our examination of the temporal structure ofP3(X) at P, revealed that, between 50% and 90% ofP3(X) peak amplitude, P300 onset times increasedsignificantly as stimulus quality decreased. At thesame time, we showed that P300 duration remainedvirtually constant across conditions. Together,these data support the assumption that the cogni-tive processes reflected by P300 are delayed, ratherthan being prolonged, when stimuli are difficult tocategorize. Thus, it is reasonable to conclude thatthe P300 is not elicited until after the stimulus hasbeen categorized.
The validity of conclusions based on P300 onsetlatency depend partly on the accuracy of the mea-surement procedure. For example, there could be aquestion as to whether different results would beobtained for different fractional amplitudes. How-ever, our multiple analyses indicate that the onsetand duration effects are robust, in the sense thatthey were consistent over a wide range of mea-surements.
The present study provides additional evidencethat the P.300-like activity generated in the anteriortemporal lobes does not contribute significantly tothe scalp-recorded P300 and thus, that P300 is nota unitary phenomenon (Johnson, 1986, 1988a,1988b, 1989a, 1989b; Johnson et al., 1991; Ruch-kin, Johnson, Canoune, Ritter, & Hammer, 1990;Stapleton et al., 1987; Knight, Scabini, Woods, &Clayworth, 1989). The data do illustrate the valueof information obtained from quantifying the onsetand duration of ERP components. On the basis ofthe onset latency and duration data, we were ableto show that stimulus categorization occurs priorto the onset of, rather than during, the P300, Ap-plying this method of analysis in future studies, anddemonstrating which cognitive processes increaseP300 duration but not P300 onset latency, shouldmake possible the identification of the cognitiveprocesses that underlie P3Q0 activity.
REFERENCES
Alufullah, I,, Halgren, E,, Supleton, J.M., & Crandall,PH. (1986). Interictal spike-wave complexes in the hu-man medial temporal lobe: Typical topography andcompansons with cognitive potentials. Electroenceph-alography A Clinical Neurophysiology. 63, 503-516.
Barrett, G., Neshige, R,, & Shibasaki. H. (1987). Humanauditory and somatosensory event-related potentials.
Electroencephalography A Clinical Neurophysiology,66, 409-419.
Dorf, J.E., Mirsky, A.F., & Mishkin, M. (1965). Effects ofunilateral temporal lobe removals in man on tachis-toscopic recognition in the lef\ and right visual fields.Neuropsychologia, 3. 39-51.
Fedio, P., Martin, A., & Brouwers, P. (1984). The effects

May, 1991 F300, Stimulus Quality, and Temporal Lobectomy 283
of focal cortical lesions on cognitive functions. In R.J.Porter (Ed.). Advances in epileptology: XVth epilepsyinternational symposium (pp, 489-496), New York:Raven Press,
Fil/gcrald, PG., & Picton, T.W. (1983). Event-related po-tentials recorded during the discrimination of im-probable stimuli. Biological Psychology, 17. 241-276.
Halgren, E., Squires, N.K., Rohrbaugh, J.W., Babb, T.L,.& Crandall, PH. (1980). Endogenous potentials gen-erated in the human hipp<Kampal formation andamygdala by infrequent events. .Science, 210, 803-805,
Halgren, E,, Stapleton, J.S., Smith, M., & Altafullah, 1,(1986). Generators ofthe human scalp P3(s), In R.Y,Cracco & I. Bodis-Wollner (Eds.), Evoked potentials(pp. 269-284). New York: Alan R. Liss.
Jennings, JR., & Wood, C.C. (1976). The epsilon adjustedprocedure for repeated measures analyses of variance,P.sychophy.siology, 17, 111-119..
Johnson, R,, Jr, (1986). A triarchic model of P300 am-plitude. Psychophysiology. 23. 367-384.
Johnson, R., Jr, (1988a). The amplitude of the P.̂ 00 com-ponent ofthe event-related potential: Review and syn-thesis. In P.K. Ackles, JR. Jennings, & M.G.H, Coles(Eds,), Advances in psychophysiology (\o\. 3, pp. 69-138). Connecticut: JAI Press,
Johnson, R., Jr. (1988b). Scalp-recorded P300 activity inpatients following unilateral temporal lobectomy.Brain. III. 1517-1529.
Johnson, R., Jr. (1989a). Auditory and visual P.1OOs intemporal lobectomy patients: Evidence for modality-dependent generators. Psychophysiology. 26. 6.^3-650,
Johnson, R., Jr. (1989b). Developmental evidence for mo-dality-dependent P.300 generators: A normative study,Psvchophystology, 26. 651-667,
Johnson, R.. Jr,, & Donchin, E, (1978), On how P300amplitude varies with the utility ofthe eliciting stim-uli, Electroencephalography A Clinical Neurophysiot-ogy, 44, 424-437,
Johnson, R,, Jr,, & Donchin, E, (1985), Second thoughts:Multiple P300s elicited by a single stimulus. Psycho-physiology. 22. 182-194,
Johnson, R,, Jr,, & Fedio, P, (1986). P30() activity in pa-tients following unilateral temporal lobectomy. InW,C . McC allum, R. Zapoli, & F. Denoth (Eds.), Cer-ebral psvchophysiology: .Studies in event-related poten-tials. Electroencephalography A Clinical Neurophysi-ology, .Suppl. 39 (pp. 552-554). Amsterdam: ElsevierScience Publishers.
Johnson. R., Jr., & Fedio, P (1987), Task-related changesin P.MX) scalp distribution in temporal lobectomy pa-tients. In R. Johnson, Jr., J.W. Rohrbaugh, & R. Par-asuraman (Eds.), Current research tn event-relatedbrain potential research. Electroencephalography AClinical Neurophysiology, Suppl. 40, (pp. 699-704).Amsterdam: Elsevier Science Publishers.
Johnson, R,, Jr,, Miltner, W,, & Braun, C (1991), Audi-tory and somalosensory eveni-related potentials: 1. Ef-fects of attention. Journal of Psychophvstology. 5, 11-25,
Kimura, D, (1963), Right lemporal-lobc damage. Archivesof Neurology, 8. 264-271,
Knight, RT,, Scabini, D,, Woods, D,L,, & Clayworth, C.C.(1989), Contributions of temporal-parietal junction tothe human auditory P3, Brain Research. 502. 109-116,
Kok, A,, & Looren de Jong, H, (1980), Components ofthe event-related potentials following degraded andundcgraded visual stimuli. Biological Psychology, tl.117-133.
Kutas, M., McCarthy, G., & Donchin, E. (1977), Aug-menting mental chronometry: The P300 as a measureof stimulus evaluation time. Science. 197. 792-795.
Lansdell, H, (1968). Effect of extent of temporal lobe abla-tions on two lateralized deficits. Physiology and Be-havior. 3. 271-273,
Magliero. A,, Bashore. T,R,, Coles, M,G,H,, & Donchin.E, (1984), On the dependence of P300 latency on stim-ulus evaluation processes, Psyvhophysiology. 21. 171-186.
McCarthy, G,, & Donchin, E. (1981), A metnc for thought:A comparison of P300 latency and reaction time. Sci-ence. 211. 77-79.
McCarthy, G., Wood, C.C, Williamson, P.D,, & Spencer,D,D, (1989), Task-dependent field potentials in humanhippocampal formation. The Journal of Neuro.science.9. 4253-4268,
Meier, M,J,, & French, L,A, (1965), Lateralized deficits incomplex visual discrimination and bilateral transfer ofreminiscence following unilateral temporal lobectomy,Neuropsychologia. 3. 261-272,
Milner, B, (1975), Psychological aspects of focal epilepsyand its neurosurgical management. In D,P, Purpura,J,K., Penry, & R,D, Walter (Eds,), Advances in neu-rology (\o\. 8, pp, 299-321), New York: Raven Press.
Perrault, N,, & Picton, T,W, (1984), Event-related poten-tials recorded from the scalp and nasopharynx. II. N2,P3 and slow wave. Electroencephalography A Clinical.\europhysiology. 59, 261-278,
Pritchard, W,S. (1981), Psychophysiology of P300. Psy-chological Bulletin. 89. 506-540,
Renault. B,, Ragot. R., Lesevre. N., & Remond, A. (1982).Onset and offset of brain events as indices of mentalchronometry. Science. 215. 1413-1415,
Ritter. W,, Simson, R,. Vaughan. H,G,. Jr,, & Macht, M.(1982), Manipulations of event-related potential man-ifestations of information processing stages. Science..'/.S, 909-911.
Riltcr, W., Simson, R., & Vaughan, H.G., Jr. (1983).Event-related potential correlates of two stages of in-formation processing in physical and semantic dis-crimination tasks, P.sychophysiology, 20. 168-179,
Rosenthal, L,S,, & Fedio, P, (1975), Recognition thresh-olds in the central and lateral visual fields followingtemporal lobectomy, Corte.x, II, 217-229,
Ruchkin, D,S,, Johnson, R,, Jr,, Canoune, H,L,, Ritter,W., & Hammer, M, (1990). Multiple sources of P3bassociated with different types of information. Psy-chophy.siology. 27. 157-176,
Ruchkin, D,S,, & Sutton, S, (1978), Equivocation andP.̂ 00 amplitude. In D. Otto (Ed.), Multidisctplinaryperspectives tn ewnt-related potential research (pp.175-177). Washington, DC: U.S. Government Print-ing Office/EPA,

284 Scheffers, Johnson, and Ruchkin kb/. 28. No. 3
Ruchkin, D.S., Sutton. S,, & Mahaffey. D. (1987), Func- ponentsand task correlates. Eleetroencephalography &tional differences between members of the P300 com- Clinical Neurophysiology. 67, 44-52,plex: P3e and P3b. Psychophysiology. 24. 87-103. Stapleton, J.M., Halgren, E., & Moreno, K.A. (1987). En-
Smith, M.e,. & Halgren, E, (1989), Association of rec- dogenous potentials after anterior temporal lobecto-ognition memory components following temporal lobe "̂ y- Neuropsychologia. 3. 549-557,lesions. Journal of Experimental Psychology: Learn- Tukey, J,W, (1978), Measurement of event-related poten-ing. Memory and Cognition. 15. 50-60, ''«'*• Commentary: A data analyst's comments on a
Squires, N,K,, Halgren. E., Wilson, C, & Crandall, P vanety of points and issues. In E.CaMoway, P Tuetmg,,.',, ,, . . . . . , „ & S.H. Kos\ov/{Eds.). Event-related brain potentials(1983). Human endogenous hmb.c potentials: Cross ,„ ^^^ 139-151), New York: Academic Press,modality and depth/surface companions in epileptic ^ ^ <. (-. McCarthy, G,, Squires, N,K,, Vaughan, H,G,,subjects. In A.W.K. Gaillard & W. Ritter (Eds,), Tu- vVoods, D,L, & McCallum, W,C. (1984). Anatomicaltorials in event-related potentials: Endogenous com- jp^ physiological substrates of event-related poten-ponenti (pp. 217-232). Amsterdam: North Holland tials: Two case studies. In R, Karrer, J. Cohen, & PPublishing Company. Tueting (Eds.), Brain and information: Event-related
Supleton, J.M., & Halgren, E, (1987). Endogenous po- potentials. Annals of the New York Aeademy of Sci-tentiaU evoked in simple cognitive tasks: Depth com- ences. 425. 722-742.
(Manuscript received February 16, 1990; accepted for publication June 14, 1990)
Announcements
Postdoctoral Research Position inEvent-Related Potentials and Alzheimer's Disease
The Cognitive Electrophysiology Laboratory of the Division of Developmental and BehavioralStudies at New York State Psychiatric Institute, New York City, New York, has a position availableat the postdoctoral level. The position is supported by a grant from NIA dealing with memory andAlzheimer's disease using event-related potentials concurrently recorded during tasks presumed totap implicit memory performance. The candidate should have experience in the recording and analysisof psychophysiological data with emphasis on event-related potentials, and be comfortable workingwith patients. Knowledge of computerized data collection and analysis on mini-, micro-, and main-frame computers is essential. Competency with the DOS operating system is critical, and programmingskills are highly desirable. The appointment can begin as early as September. 1991, Salary range isbased on NIH guidelines with excellent fringe benefits.
Please send (I) a letter of application describing interests and experience, (2) curriculum vitae andrepresentative repnnts, and (3) the names and addresses of three references, to: Dr, David Friedman,Department of Medical Genetics, A3O8, Box 58, New York Sute Psychiatric Institute, 722 West 168thStreet, New York City, New York 10032,
Third International Conference on Alzheimer's DiseaseFrom July 12th through 17th, 1992, the Third International Conference on Alzheimer's Disease
and Related Disorders will be held at the Palazzo del Turismo, Montegrette Terme, Padova, Italy,The convenors ofthe conference are: Drs, M, Nicolini, K, Iqbal, B, Winblad, and H.M, Wisniewski,For further information and abstract forms, contact: Conference Organizer, Dr, P, Zatta, CNR-UNIT,Dipartimento di Biologia, via Trieste 75, 35131 Padova. Italy (telephone (49) 8286361, fax (49)8286359).
Cognitive PsychophysiologistThe Cognitive Neuroscience Unit in the National Institute of Neurological Disorders and Stroke
has an opening for a cognitive psychophysiologist, starting December 1991, who is familiar withevent-related potentials (ERPs). to study patients with a variety of neurological deficits. We are seekinga mature individual, with less than three years of postdoctoral experience, who is capable of inde-pendent rewarch within an interdiviciplinary team. Skills in recording and analyzing ERPs and pro-gramming In FORTRAN are essential. Salary ranges from $25,(XK)-$31,OCX) depending upon quali-fications. Plea»e send C V, statement of research interests, explicit description of skills and workexperience, the name« and telephone numbers of three professionals you have worked with, andrepnnts/prepnntsof your work to: Ray Johnson, Jr,, National Institutes of Health, NINDS/CognitiveNeuroscience Unit, MNB, Building 10, Room 4C422, Bethesda, MD 20892. The NIH is an equalOpportunity employer.