Embed Size (px)
Citation preview

OUTCOMES OF EARLY REHABILITATION
FOLLOWING LUMBAR MICRODISCECTOMY
by
JENNIFER M. LYNN
May 2009
This thesis is presented in fulfilment of the requirements for the
award of the Master of Medical Science Degree
within the School of Surgery
Faculty of Medicine, Dentistry & Health Science
at
The University of Western Australia
ii
ABSTRACT
BACKGROUND CONTEXT
There have been few studies into the effects of rehabilitation following lumbar
microdiscectomy and consequently little evidence of its effect, if any, on outcome. Most
studies cited fall into one of two categories: research involving a spinal surgery
procedure without rehabilitation, or research involving spinal surgery with a non-
specific generic ‘rehabilitation’ or ‘physical therapy’. In an era of evidence based
medicine the efficacy of specific rehabilitation protocols following defined lumbar
spine surgical procedures needs to be established for surgeons, therapists and patients to
have confidence that the rehabilitation is appropriate and effective.
PURPOSE
The study was proposed to investigate the outcome of a specific and novel rehabilitation
protocol commenced immediately after lumbar microdiscectomy. Data collected from
the research cohort were compared to data collected from a contrast group who under-
went standard rehabilitation at a distant site.
STUDY DESIGN
A retrospective study (Phase One) was carried out with a cohort of post-operative
microdiscectomy patients between February 2000 and December 2002. The outcome of
surgery followed by the rehabilitation protocol was assessed using validated outcome
instruments. A contrast or control group was not included. After reviewing the data
limitations with the design and implementation of the study were identified.
A prospective study (Phase Two) was proposed and changes made in the principal
outcome measure used, in the demographic data to be retrieved, the addition of pain
scales, and in the exclusion of compensable patients. A contrast group was included for
the prospective study.
PATIENT SAMPLE
For Phase Two, the WA study cohort of 47 patients comprised 30 males and 17 females
with an average age of 45 years. The WA cohort was further divided into two groups,
those who under-went microdiscectomy alone and those who required a more extensive
procedure to gain access to the site of the disc herniation, namely: laminectomy, or far
iii
lateral approach to a foraminal prolapse. The contrast group in Queensland was a cohort
of 12 patients, seven males and five females, with an average age of 54 years.
OUTCOME MEASURES
Phase Two employed three outcome measures: the Roland Morris Questionnaire
(RMQ), Visual Analogue Scale (VAS) and a Questionnaire developed to record the
severity of symptoms, generic health status, functional status, work disability and
patient satisfaction. Pain was measured with the VAS. Functional status was measured
using the RMQ, a survey of 24 activities likely to be affected by low back pain.
Other demographic and clinical information, including medication usage and nature of
additional surgical procedures (foraminotomy, laminectomy, etc), were collected for
examination of recovery profiles. The recurrence of herniation requiring further surgery
was monitored through the referring surgeon.
METHOD
Data were collected from 47 consenting consecutive patients referred from a single
neurosurgeon following lumbar disc surgery. A contrast group comprising 12 patients
was recruited from an interstate neurosurgeon. Criteria for inclusion were
microdiscectomy or discectomy with or without laminectomy or foraminotomy, for
lumbar disc prolapse where no other instrumentation was used. The study group
commenced exercise and posture correction the day following surgery. There were
restrictions placed on activity involving bending. The contrast group followed the
advice of the surgeon in Queensland and attended rehabilitation at local physiotherapy
facilities. Both groups were followed for 12 months using outcome instruments.
RESULTS
Strict comparison between WA and QLD cohorts were limited due to sample size,
however trends were observed. Data of the prospective study showed that there was
greater reduction in back pain with the early rehabilitation protocol (P<.0001) compared
to standard rehabilitation (P=.09), while there was no difference between groups in leg
pain. There was a significant improvement in the level of functional disability between
time-points for the WA cohort, and overall change from pre-operative RMQ measures
to 12 months in both groups were statistically significant. The WA group was less
reliant on pain medication and was more satisfied with the results of their surgery.
iv
CONCLUSION
The primary hypothesis of this study that there would be a difference in outcome
following lumbar microdiscectomy in patients who receive early specific rehabilitation
compared to those who receive standard rehabilitation at another centre, was supported
in both primary and secondary outcome data.
The key finding of this study was that commencing the early exercise protocol resulted
in significantly less back pain over the 12 month time period of the study. Other major
findings were that the WA cohort demonstrated significant improvement in function at
all time-points and between all time-points except six to 12 months, took less pain
medication and were more satisfied with the outcome of their surgery than the QLD
cohort.
v
DECLARATION FOR THESES CONTAINING PUBLISHED
WORK AND/OR WORK PREPARED FOR PUBLICATION
The examination of the thesis is an examination of the work of the student. The work
must have been substantially conducted by the student during the enrolment in the
degree.
Where the thesis includes work to which others have contributed, the thesis must
include a statement that makes the student’s contribution clear to the examiners. This
may be in the form of description of the precise contribution of the student to the work
presented for examination and/or a statement of the percentage of the work that was
done by the student.
In addition, in the case of co-authored publications included in the thesis, each author
must give their signed permission for the work to be included. If signatures from all of
the authors cannot be obtained, the statement detailing the student’s contribution to the
work must be signed by the coordinating supervisor.
1. This thesis does not contain work that I have published, nor work under review for
publication.
Signature …………………………….
vi
ACKNOWLEDGEMENT
I wish to thank the many people who have given invaluable professional and personal
support throughout the preparation of this thesis.
Special acknowledgement is extended to Professor Kevin Singer (Principal Supervisor)
for his guidance throughout this project. Thanks also to Mr Quentin Malone
(Supervisor) who has always made himself available to discuss the many challenges of
clinical practice. Gratitude is extended to Dr Richard Kahler for the provision of a
contrast group, an under-taking made more unusual and special given that we have
never met.
Thanks to Ray Smith at Department of Surgery who provided computer expertise,
establishing and monitoring the data returned by e-mail.
Special thanks to Julee Hogan, my secretary, who has ensured the collection of data has
been timely and the input correct. She has been invaluable for proofreading and
collating material.
Professor Harry Lee has been a mentor and friend for many years, providing
challenging discussions and provoking thought processes. I count myself fortunate to
have been one of his students.
My gratitude to the patients who made themselves available to answer questionnaires
throughout the course of the study.
And finally, since the inception of this thesis six years ago many people have been
involved one way or another, but there is only one who has been constant and has made
it possible for me to complete this project, my husband, my partner, my friend, Jim. My
thanks go to Jim for all that he has been and done, not only for these six years, but for
all the years we have been together.
vii
TABLE OF CONTENTS
PAGE
ABSTRACT ii
DECLARATION OF ORIGINALITY v
ACKNOWLEDGEMENT vi
TABLE OF CONTENTS vii
GLOSSARY OF TERMS AND DEFINITIONS xii
LIST OF FIGURES xiii
LIST OF TABLES xvi
LIST OF APPENDICES xvii
CHAPTER 1
THE PROBLEM AND ITS BACKGROUND
1.1 Introduction 1
1.1.1 Acceptance in the medical community 1
1.1.2 Outcome 2
1.1.3 Costs 3
1.2 Statement of the problem 3
1.3 The primary hypothesis 4
1.4 Secondary research questions 4
1.5 Aim 4
1.6 Research approach 4
1.7 Summary 4
CHAPTER 2
REVIEW OF LITERATURE
2.1 Introduction 6
2.2 Anatomy of the lumbar intervertebral disc 6
2.2.1 Overview 6
2.2.2 Anulus fibrosus 7
2.2.3 Nucleus pulposus 9
2.2.4 Vertebral end-plates 11
2.2.5 Intervertebral disc nutrition 12
2.2.6 Longitudinal ligaments 14
viii
2.2.7 Nerve supply 15
2.2.8 Aging of the disc 17
2.2.9 Summary 18
2.3 Mechanics of the intervertebral disc 19
2.3.1 Introduction 19
2.3.2 Role of disc in spinal mechanical 19
2.3.3 Summary 22
2.4 Lumbar musculature 22
2.4.1 Introduction 22
2.4.2 Diaphragm 22
2.4.3 Pelvic diaphragm 23
2.4.4 Anterior abdominal wall 23
2.4.5 Lateral abdominal wall 24
2.4.6 Posterior abdominal wall 24
2.4.7 Function of the lumbar musculature 25
2.4.8 Summary 26
2.5 Historical perspective: surgery 27
2.5.1 Introduction 27
2.5.2 Early development of disc surgery 27
2.5.3 Early twentieth century development 28
2.5.4 Recent developments of disc surgery 29
2.5.5 Summary 29
2.6 Historical perspective: physiotherapy 30
2.7 Current theory 31
2.7.1 Introduction 31
2.7.2 McKenzie approach to treatment of lower back pain 31
2.7.3 Other studies 37
2.7.4 Summary 38
2.8 Development of the Rehabilitation Protocol 38
2.8.1 Introduction 38
2.8.2 Reduction of derangement 38
2.8.3 Maintenance of reduction 39
2.8.4 Recovery of function 39
2.8.5 Prevention of recurrence 42
2.8.6 Summary 43
ix
2.9 Current standard rehabilitation following lumbar microdiscectomy 43
2.9.1 Introduction 43
2.9.2 Standard rehabilitation 44
2.9.3 Summary 44
2.10 Outcome instruments 45
2.10.1 Introduction 45
2.10.2 Oswestry Disability Index 45
2.10.3 Roland-Morris Disability Questionnaire 45
2.10.4 Selection of outcome instrument 46
2.10.5 Visual Analogue Scale 46
2.10.6 Outcome questionnaire prospective study 47
2.10.7 Outcome questionnaire retrospective study 47
2.10.8 Summary 47
2.11 Summary 47
CHAPTER 3
MATERIALS AND METHOD
3.1 Introduction 49
3.2 Study design 49
3.3 Development of Rehabilitation Protocol 50
3.3.1 Introduction 50
3.3.2 Maintenance of the reduction 51
3.3.3 Recovery of function 53
3.3.4 Prevention of recurrence 55
3.3.5 Summary 55
3.4 Clinical Studies 56
3.4.1 Introduction 56
3.4.2 Phase 1: Retrospective study 56
3.4.3 Phase 2: Prospective study 60
3.5 Data management and statistics 64
3.6 Summary 65
CHAPTER 4
RESULTS
4.1 Introduction 66
4.2 Back pain 68
x
4.3 Leg pain 69
4.4 Disability 71
4.5 Repeat surgery due to reherniation of the intervertebral disc 72
4.6 Medication 73
4.7 Satisfaction 73
4.8 Depression 73
4.9 Other results 75
4.10 Microdiscectomy – with and without access 77
4.11 Summary 78
CHAPTER 5
DISCUSSION
5.1 Introduction 80
5.2 Primary outcomes of the study 81
5.2.1 Back pain 81
5.2.2 Leg pain 82
5.2.3 Disability 83
5.2.4 Repeat surgery 84
5.3 Secondary outcomes of the study 85
5.3.1 Medication 85
5.3.2 Satisfaction 85
5.4 Other outcomes 86
5.4.1 Return to work 86
5.4.2 Smoking 87
5.5 Factors effecting outcome of the study 87
5.5.1 Rehabilitation protocol 87
5.5.2 Posture correction 89
5.5.3 Recovery of flexion 90
5.5.4 Effects of flexion on the disc 91
5.5.5 Repeated movement 93
5.6 Limitations 93
5.7 Summary 95
xi
CHAPTER 6
CONCLUSION
6.1 Primary outcome data 97
6.2 Secondary outcome data 98
CHAPTER 7
RECOMMENDATIONS
7.1 Rehabilitation following uncomplicated microdiscectomy (alone) 99
7.2 Education 100
7.3 Clinical practice guidelines 100
7.4 Further research 101
REFERENCES 103
xii
GLOSSARY OF TERMS AND DEFINITIONS
Microdiscectomy Disc surgery with use of an operating microscope
Derangement Internal displacement of articular tissue of whatever origin
will cause pain to remain constant until such time as the
displacement is reduced.
Reduction of derangement The process by which the derangement is progressively
lessened.
Irreducible derangement A derangement in which only loading strategies that
peripheralise, worsen or do not affect symptoms are
found.
Data Plural of datum: facts or figures to be processed;
evidence, records, statistics, etc from which conclusions
can be inferred; information.
xiii
LIST OF FIGURES
PAGE
2.1 A lumbar motion segment. 7
2.2 Axial view of a human lumbar disc (teenaged female). 7
2.3 The concentric layers of the anulus demonstrating the adjacent parallel 8
fibres within each lamella, and alternating layers in opposite direction.
2.4 Incomplete layers of the anulus blending into lamellae. 8
2.5A Scanning electron microscope demonstrating the alternating 9
layers and density of collagen fibrils in the anulus.
2.5B The loose collagen fibril network of the nucleus. 9
2.6 Compression of the disc causes loss of height, increased radial 10
bulging, and a change in alternating fibre angle. The nucleus exhibits a
hydrostatic pressure and creates a tangential hoop stress in the anulus.
2.7 Inner lamellae of the anulus merging into the end-plate. 10
2.8 Vertebral end-plate diagrammatically demonstrating the anulus 12
enclosing the nucleus but not the outer fibres (Sharpey’s fibres) of the
anulus spanning over the rim of the vertebral body to merge into the
anterior longitudinal ligament.
2.9 Transverse section of a lumbar vertebra from a young adult, cut 12
through region of the junction of the vertebral end-plate and the
intervertebral disc. Arteriolar and capillary vessels are seen end-on in
the region. A majority of the vessels are seen to traverse horizontal,
parallel to the vertebral end-plate.
2.10 Changes in disc height over one diurnal loading cycle. The disc 14
fully recovered the height lost during 16 hours of loading by resting
for eight hours.
2.11 Left lateral view of the lumbar vertebrae demonstrating 15
positioning of the anterior and posterior longitudinal ligaments.
2.12 Posterior view of the anterior segments of the lumbar spine 15
demonstrating the saw-tooth nature of the posterior longitudinal
ligament.
xiv
2.13 Lateral view of the lumbar spine demonstrating the anterior 16
longitudinal ligament.
2.14 Axial section of a lumbar disc demonstrating advanced changes. 16
3.1 Sitting with lumbar roll. 52
3.2 Straight leg raise in sitting. 52
3.3 Exercise 1: prone lying. 52
3.4 Exercise 2: prone on elbows. 52
3.5 Exercise 3: extension in lying. 52
3.6 Prone stabilisation. 52
3.7 Rep flexion in lying. 53
3.8 Prone knee bend. 53
3.9 Four point stabilisation. 53
3.10 Three point stabilisation (arm lift). 53
3.11 Three point stabilisation (leg lift). 53
3.12 Two point stabilisation. 53
3.13 Private patients’ self-assessment of outcome of surgery followed by 58
rehabilitation at six monthly time-points.
3.14 Compensable patients’ self-assessment of outcome of surgery followed 59
by rehabilitation at six monthly time-points.
3.15 Comparison of average Oswestry disability index scores of private and 59
compensable patients at six monthly time-points, noting the marked
change for compensable patients between six and 12 months.
3.16 Flowchart showing participant recruitment in WA and QLD cohorts. 62
4.1 Box plot of the 90th to 10th percentile; depicting improvement in back 69
pain data over the 12 month duration of the study, demonstrating
the large decrease in pain at the first time-point after surgery.
4.2 Box plot of the 90th to 10th percentile, depicting improvement in leg pain 70
data over the 12 month duration of the study, recording the sharp
decline in pain immediately following the surgery.
4.3 Box plot of the 90th to 10th percentile, depicting improvement in 72
Roland Morris Questionnaire data over the 12 month duration of
the study.
4.4 Utilisation of pain medication in WA and QLD cohorts demonstrating 74
the rapid decline in pain medication use in both groups at the exit
time-point. In the WA cohort the decline in use continued while in the

xv
QLD is increased slightly at 12 months.
4.5 Utilisation of anti-inflammatory medication (NSAIDs) in WA and QLD 74
cohorts indicating that NSAIDs use reduced following surgery but
increased slightly over time in both groups.
4.6 Satisfaction with outcome of surgery in WA and QLD cohorts 75
demonstrating an increase in dissatisfaction from ‘exit’ to six
months in the QLD cohort whereas the WA cohort maintained the
level established immediately after surgery.
4.7 Responses to depression questions demonstrating a rapid decline after 75
surgery indicating the effect of the surgery itself on mental disposition.
4.8 Graphs of primary outcome data for the WA cohort comparing those 78
who under-went microdiscectomy alone and those who required an
access procedure.

xvi
LIST OF TABLES
PAGE
2.1 Surgical developments from 1964 to 1995 for the treatment of 29
intervertebral disc herniation.
3.1 Demographics of the WA and QLD cohorts. 62
4.1 Primary outcome data over 12 months for WA and QLD cohorts 67
following lumbar microdiscectomy.
4.2 Secondary outcome data over 12 months for WA and QLD cohorts 68
following lumbar microdiscectomy.
4.3 Summary of changes in back pain outcome data (Scheffé) for WA 68
and QLD cohorts comparing pre-operative scores with those at
the other reassessment time-points.
4.4 Comparison of visual analogue scale (VAS) scores for back pain in 69
the WA and QLD cohorts.
4.5 Summary of changes in leg pain outcome data (Scheffé) for WA and 70
QLD cohorts comparing pre-operative scores with those at the
other reassessment time-points.
4.6 Comparison of VAS scores for leg pain in the WA and QLD cohorts. 70
4.7 Summary of changes in RMQ data (Scheffé) for WA and QLD 71
cohorts comparing pre-operative scores with those at the other
reassessment time-points.
4.8 Comparison of Roland-Morris questionnaire scores in the WA and 72
QLD cohorts.
4.9 Demographic data of repeat surgery reporting for re-herniation of 73
intervertebral disc.
4.10 Subsequent procedures primarily for pain relief including nerve sleeve 77
injection, in study cohorts.

xvii
LIST OF APPENDICES
1 Ethics documentation
2 Oswestry disability index (ODI)
3 Outcome questionnaire Phase one (retrospective study)
4 Roland-Morris questionnaire (RMQ)
5 Visual analogue scale (VAS)
6 Outcome questionnaire Phase two (prospective study)
7 Patient Information Sheet provided for subjects eligible to enrol into
Phase two of the study
8 Consent Form for subjects enrolling them into Phase two of the study
9 Aerobic walking schedule provided during rehabilitation
10 Spinal rehabilitation following lumbar surgery; an example of ‘best
practice’ from Queensland
11 Data for planned comparisons (Scheffé) of back and leg pain scores
(VAS) and the RMQ data from the WA and the QLD cohorts.
12 Tables for unpaired ‘t’ tests used to test the null hypothesis of back
and leg pain scores (VAS) and the RMQ data reported from the
WA and QLD surgical cohorts at all time-points.
13 Tables for unpaired t test used to test the null hypothesis of back and
leg pain scores (VAS) and the RMQ data reported from the WA
cohorts comparing subjects with and without access procedure.
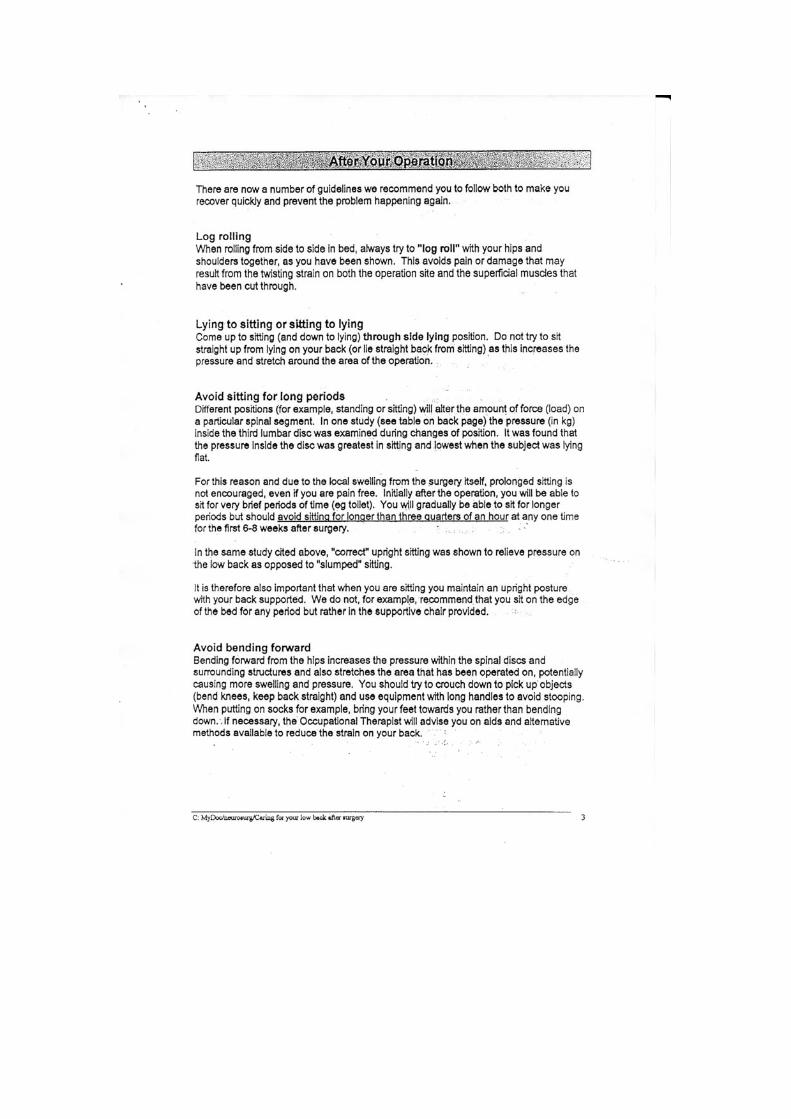
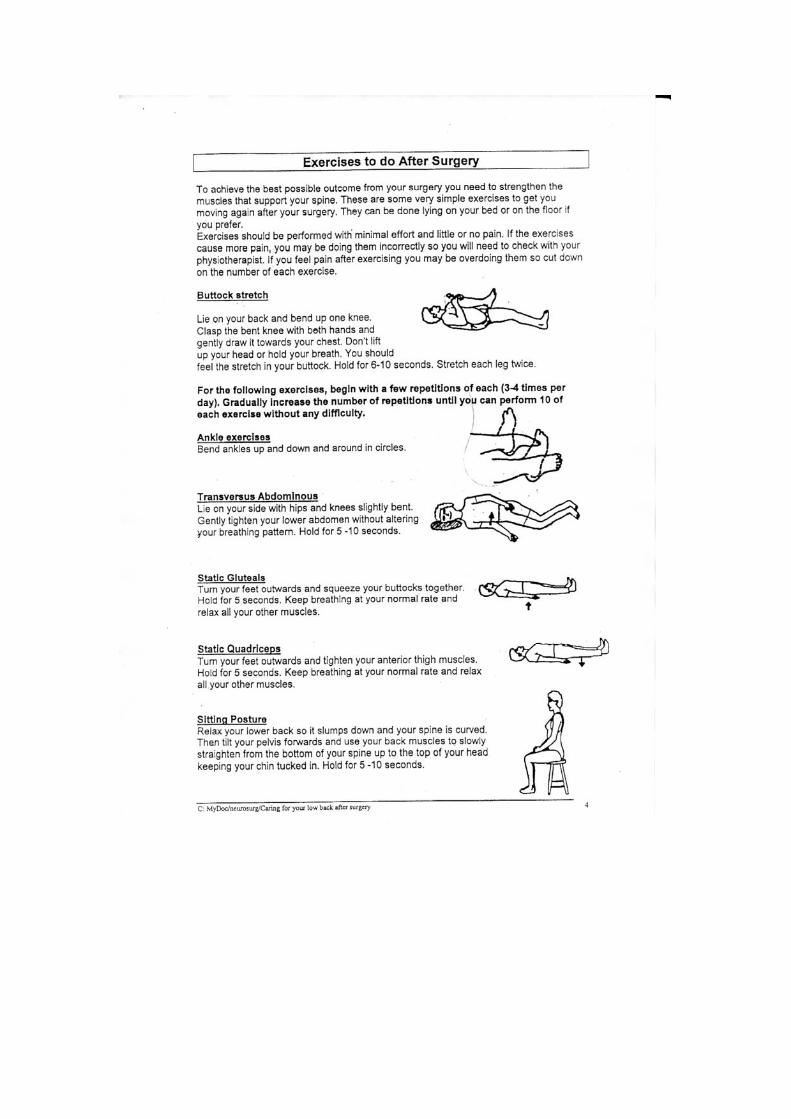
14 Caring for your low back after surgery; an example of standard
rehabilitation from WA provided by a patient. This example has been
used to demonstrate the wide variety of care available following lumbar
microdiscectomy.

1
CHAPTER 1
THE PROBLEM AND ITS BACKGROUND
1.1 INTRODUCTION
There is almost an absence of studies in the literature, prospective or retrospective,
examining the effects of specific rehabilitation protocols following lumbar
microdiscectomy. Most studies cited fall into one of two categories: research involving
a spinal surgery procedure without rehabilitation (Schaller 2004), or research involving
spinal surgery with a non-specific generic ‘rehabilitation’ or ‘physical therapy’ (Fisher,
Noonan, Bishop et al. 2004). There have been few studies into the effects of
rehabilitation following lumbar surgery and consequently little evidence that it alters
outcome (Kjellby-Wendt and Styf 1998; Mayer, McMahon, Gatchel et al. 1998). In an
era of evidence based medicine the efficacy of specific rehabilitation protocols
following defined lumbar spine surgical procedures need to be established for surgeons,
therapists and patients to optimise outcomes.
1.1.1 Acceptance in the medical community
Studies of rehabilitation after surgery, which are cited in the literature, predominantly
involve peripheral joints where specific rehabilitation protocols are followed. Studies of
peripheral joint mobilisation following surgery were prompted early in the twentieth
century by surgeons like Von Riemke. In his presidential address to the Danish Surgical
Society in 1926, he expressed the view that all joint ‘affections’ should be moved soon
after surgery (O'Driscoll and Giori 2000).
Research into his observations lead to the work of Salter whose studies of the effects of
immobilisation on rabbit knee joints resulted in the development of Continuous Passive
Motion (CPM) (Salter and Field 1960). Salter described the damaging effects of
immobilisation on the articular cartilage and termed the condition “obliterative
degeneration of the articular cartilage” (Salter 1982:82).
This fundamental research by Salter and others has resulted in new rehabilitation
protocols being developed simultaneously with the advent of new peripheral joint
surgical procedures. Research involving surveys of the practices and opinions of the
American Orthopaedic Society for Sports Medicine confirms that the issue with
peripheral joint surgery is not ‘if’ but ‘when’ to commence rehabilitation (Delay,
2
Smolinski, Wind et al. 2001). According to the principles laid down by Salter (Salter
and Field 1960; Salter 1982), movement after surgery should begin in a slow and
continuous manner while the patient is still in the recovery room (O'Driscoll and Giori
2000). This very early access to mobilisation does not appear to be recommended for
post-operative spine patients perhaps because of the difficulty of application of these
principles rather than the contra-indication of commencement of movement.
While the need for peripheral joint rehabilitation has long been accepted, there remains
scepticism in the spinal surgery community with regard to the need for post-operative
rehabilitation (Carragee, Helms and O'Sullivan 1996). A debilitated and wasted limb is
easily observed, and weakness readily quantified, but it is only with recent ultrasound,
CT and MRI investigations, highlighting atrophy of the paraspinal muscles following
episodes of back pain or surgery (Rantanen, Hurme and Falck 1993), and developments
in understanding segmental spinal stabilisation, that attention has been brought to the
dysfunction of the spine with, in some cases, years of deconditioning (Richardson, Jull,
Hodges et al. 1999). The research into segmental spinal stabilisation has helped re-
define ‘spinal instability’ from a purely ligamentous insufficiency to one that
incorporates the muscle system and neural control. Segmental spinal stabilisation is
only part of the rehabilitation programme required. The changes in proprioceptive
abilities leading to reduction of postural awareness (O'Sullivan, Twomey and Allison
1997), the loss of small joint mobility resulting in decrease of range and aerobic
conditioning, are all areas which need to be examined and included in the rehabilitation
protocol.
The change in symptoms can be very dramatic following lumbar microdiscectomy
(Maroon 2002). Reduction of pressure on a neural structure, which immediately reduces
or abolishes pain, may mask the true loss of function and muscle strength. While the
crisis of the disc herniation is resolved surgically, the underlying causes of the
herniation often persist and, with the resultant dysfunction, need to be addressed
following surgery.
1.1.2 Outcome
The outcome of the rehabilitation is inextricably linked to the outcome of the surgical
intervention. The measure of outcome must take into account the results as perceived by
three participants: the patient, the surgeon and the therapist. The instruments used must
be reliable and valid measures of outcome.
3
1.1.3 Costs
Following a specific exercise-based protocol may help to control costs of rehabilitation
after spinal surgery by optimising the outcomes. For the most part the progression of
exercise is dependent on repair of disc tissues. Provided inappropriate movement, strain
or infection does not interrupt the normal healing rate, the timing of the progression is
dictated by tissue physiology (Singer and Clark 1999). Without adverse events
occurring during the recovery period most patients will complete their rehabilitation in
four to six weeks (Malone 2003). Understanding the usual response makes those not
recovering in this timeframe more readily identified and enables further medical or
surgical intervention on a timely basis.
1.2 STATEMENT OF PROBLEM
Data available in the United States indicate that lumbar intervertebral discectomy is the
most common neurosurgical procedure with more than 250,000 operations performed
annually (Asch, Lewis, Moreland et al. 2002). No comparable data are available in
Australia as the surgical coding makes it difficult to differentiate particular types of
spine surgery. Following discectomy recurrence of back pain, radiculopathy and
reherniation can occur. Radiculopathy is present in 17% to 33% of patients following
lumbar discectomy, reherniation is reported in 7% to 26% (Carragee, Spinnickie,
Alamin et al. 2006) and Yorimitsu et al (2001) reported 74% of patients complained of
back pain in the ten years after disc surgery. With a microsurgical approach, re-
herniation figures are reported to remain between 7% and 15% (Fritsch, Heisel and
Rupp 1996).
In previous studies of rehabilitation protocols (Manniche, Skall and Braendholt 1993;
Brennan, Schultz, Hood et al. 1994) patients typically began the programme at least
four weeks after surgery, except for a study by Kjellby-Wendt and Styf (1998) which
commenced rehabilitation the day following surgery. Most protocols, including that of
Kjellby-Wendt and Styf, required an extended period of participation. In the case of
Kjellby-Wendt and Styf the more intensive part of their protocol commenced at six
weeks.
The study under review in this thesis involved a rehabilitation protocol, which
commenced the day following surgery and, for most patients, was complete at four
weeks. This approach has been modelled on the McKenzie Method for treatment of
non-specific low back pain (McKenzie 1981; McKenzie and May 2003) and has been
4
developed further to incorporate the post-operative lumbar spine group undergoing
microdiscectomy.
1.3 THE PRIMARY HYPOTHESIS
It was hypothesised that there would be a difference in outcome following lumbar
microdiscectomy between patients who receive early specific rehabilitation compared
with those who receive standard rehabilitation physiotherapy at another centre, as
measured by the incidence of repeat surgery and data derived from a validated self-
report spine specific outcome instrument.
1.4 SECONDARY RESEARCH QUESTIONS
Further, differences in the rate of recovery and outcome between smokers and non-
smokers, as measured by number of visits and time to complete the rehabilitation
protocol would be assessed from the outcome data.
Changes in depression can be gauged by questionnaire during the initial recovery period
demonstrating that commencing early rehabilitation reinforces a feeling of well-being.
There is a difference in the number of days off work in patients who undergo an early
specific rehabilitation protocol compared with those who experience standard
rehabilitation as measured by a standardised questionnaire.
1.5 AIM
To determine if there was a reduction in symptoms or the number of recurrent
herniations when a specific rehabilitation protocol was introduced immediately after
surgery compared with standard rehabilitation at another centre.
1.6 RESEARCH APPROACH
It was proposed to follow prospectively a cohort of consecutive patients referred for
rehabilitation immediately following lumbar microdiscectomy performed by a single
neurosurgeon.
Consecutive patients referred by a second neurosurgeon for standard rehabilitation at a
number of facilities formed a contrast group. The contrast group was located at an inter-
state clinic.
1.7 SUMMARY
Recurrence of herniation or on-going symptoms following lumbar microdiscectomy is
often seen to represent failed primary surgery. Surgeons have sought to address this

5
perceived failure with changes and improvements in surgical procedures and
techniques.
Comparisons made between groups of patients who received a rehabilitation
programme versus those who did not have shown that, for the most part, no differences
occur. In many of the previous studies the exercise and instruction included in the
rehabilitation programme have not been scrutinised nor the compliance assessed (Fisher
et al. 2004; Schaller 2004).
This study sought to investigate a specific rehabilitation protocol of exercise and
instruction following a standard surgical approach of lumbar microdiscectomy to
examine the rehabilitation outcomes and contrast this result with standard rehabilitation
from a distant clinical site.
6
CHAPTER 2
REVIEW OF LITERATURE
2.1 INTRODUCTION
This thesis examined outcomes following lumbar microdiscectomy. The background
information includes a review of lumbar anatomy and physiology, and then outlines the
history and development of the surgical procedures and rehabilitation protocols.
2.2 ANATOMY OF THE LUMBAR INTERVERTEBRAL DISC
The anatomical component of this review is restricted to the intervertebral disc,
ligaments intimately connected to the disc, anterior and posterior longitudinal
ligaments, and musculature directly involved with both the movement of the
intervertebral segment and stability of the lumbar spine.
2.2.1 Overview
A motion segment of the lumbar spine consists of two vertebrae with the intervertebral
disc between them, the zygapophysial joints and the interconnecting ligaments and joint
structures (Schmorl and Junghanns 1959; Kramer 1990) (Figure 2.1). This arrangement
allows physiological movement to occur, into flexion, extension and rotation, in what
would otherwise be a rigid structure.
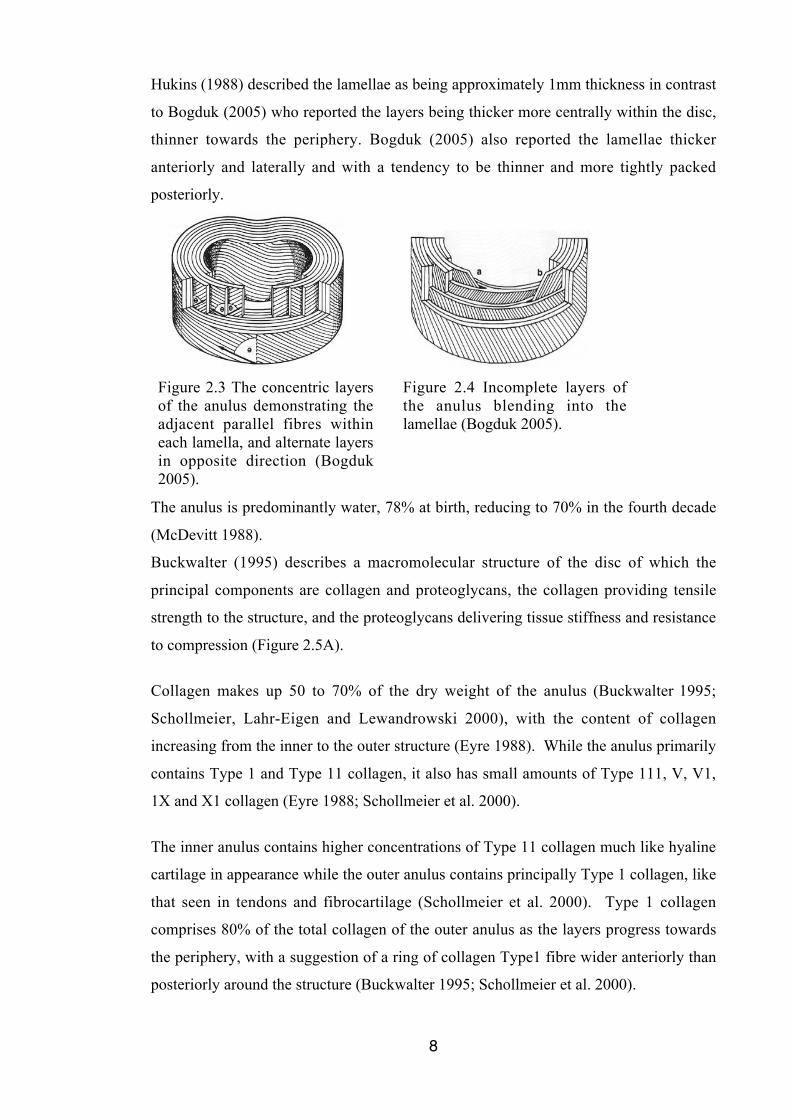
The lumbar discs are almost elliptical in shape across the axial plane, the shape
corresponding to the underlying vertebral body (Figure 2.2). The lumbar discs are 7 to
10 mm thick, and, from anterior to posterior, they are approximately 4cm in diameter
(Urban and Roberts 2003) accounting for 25% of the length of the spine (Krag, Cohen,
Haugh et al. 1990). Sagittal sections demonstrate the wedge shape of the disc with the
anterior height being greater than the posterior height due to the biased anterior
placement of the nucleus. In the newborn the wedge shape of the discs is consistent
throughout the spine with the posterior height greater than anterior, but with
development of secondary curves, cervical and lumbar lordoses, the physiological disc
wedging in those areas reverses (Taylor 1975).
7
Each disc consists of three parts: an outer ring, the anulus fibrosus; an inner core, the
nucleus pulposus; and the transition zone of the disc and the adjacent vertebrae, the end-
plate (Moore 2000; Adams, Bogduk, Burton et al. 2002).
Figure 2.1 A lumbar motion segmentadapted from Gray’s Anatomy for Students(Drake, Vogl and Mitchell 2005).
Figure 2.2 Axial view of a humanlumbar disc (teenaged) female(Hukins 1988).
In young and healthy subjects, the nucleus is distinct at its centre, and the anulus is
distinct at its periphery, with no clear boundary at their junction (Roberts 2002)
(Figure 2.2).
Embrionically the vertebrae, end-plates and anulus fibrosus are mesodermal tissue in
origin, whereas the nucleus pulposus is endodermal tissue, a remnant of the notochord.
(Roberts, Evans, Trivedi et al. 2006).
2.2.2 Anulus Fibrosus
The intervertebral disc has an outer wall, the anulus fibrosus (anulus), of lamellae of
parallel collagen fibres angled at 60 to 70 degrees with respect to the direction of the
spinal axis (Hukins 1988; Bogduk 2005).
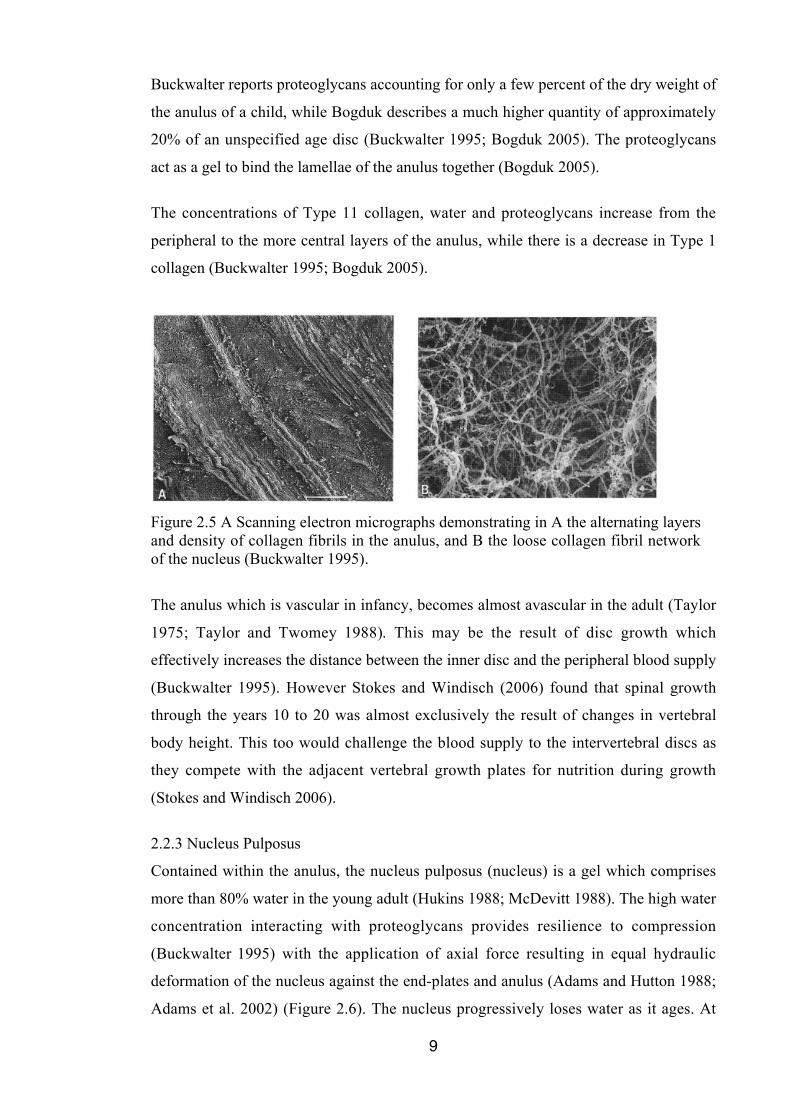
Within each layer the fibres are parallel to one another (Bogduk 2005). The direction of
the angle alternates between adjacent layers of lamellae, each successive layer running
in the opposite direction (Hukins 1988) for the depth of the anulus, from ten to 20 layers
(Bogduk 2005) and, according to Roberts et al, up to 15 to 25 layers (Urban and Roberts
2003; Roberts et al. 2006) (Figure 2.3).
Not all lamellae complete the circumference of the disc, with some layers blending into
others (Figure 2.4). The layers are incomplete in 40% of the anulus and in the posterior
anulus this figure rises to 50% (Bogduk 2005).
8
Hukins (1988) described the lamellae as being approximately 1mm thickness in contrast
to Bogduk (2005) who reported the layers being thicker more centrally within the disc,
thinner towards the periphery. Bogduk (2005) also reported the lamellae thicker
anteriorly and laterally and with a tendency to be thinner and more tightly packed
posteriorly.
Figure 2.3 The concentric layersof the anulus demonstrating theadjacent parallel fibres withineach lamella, and alternate layersin opposite direction (Bogduk2005).
Figure 2.4 Incomplete layers ofthe anulus blending into thelamellae (Bogduk 2005).
The anulus is predominantly water, 78% at birth, reducing to 70% in the fourth decade
(McDevitt 1988).
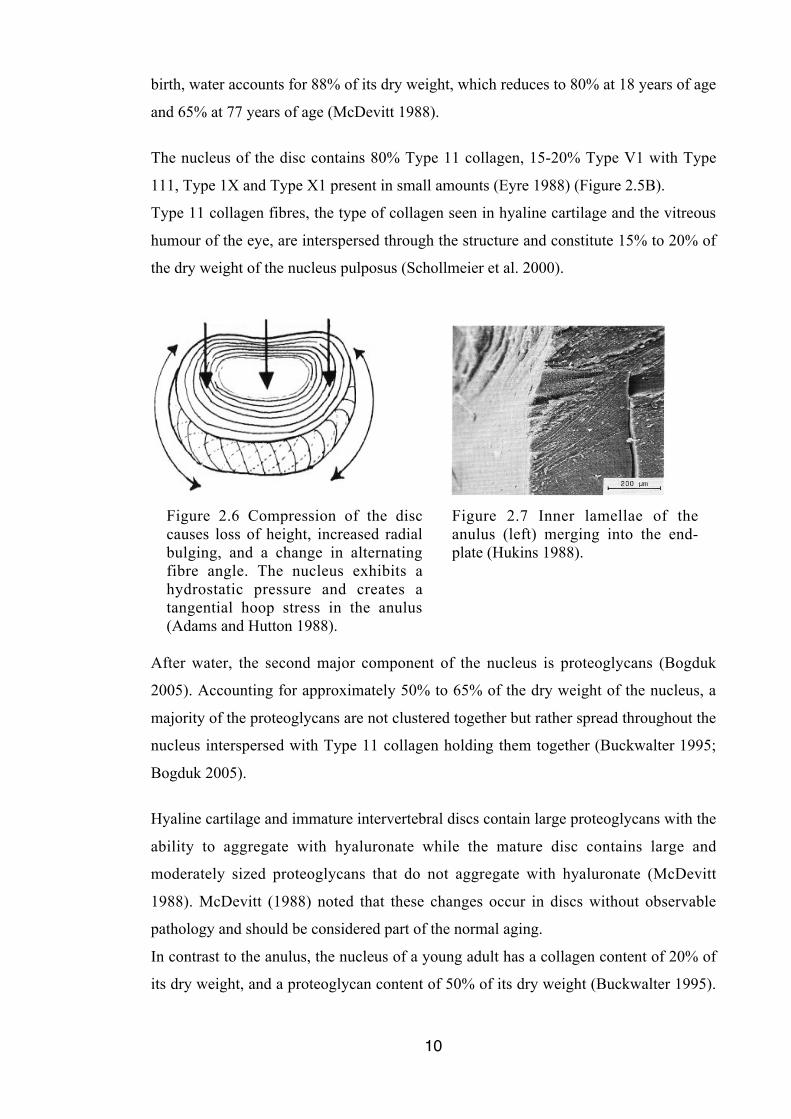
Buckwalter (1995) describes a macromolecular structure of the disc of which the
principal components are collagen and proteoglycans, the collagen providing tensile
strength to the structure, and the proteoglycans delivering tissue stiffness and resistance
to compression (Figure 2.5A).
Collagen makes up 50 to 70% of the dry weight of the anulus (Buckwalter 1995;
Schollmeier, Lahr-Eigen and Lewandrowski 2000), with the content of collagen
increasing from the inner to the outer structure (Eyre 1988). While the anulus primarily
contains Type 1 and Type 11 collagen, it also has small amounts of Type 111, V, V1,
1X and X1 collagen (Eyre 1988; Schollmeier et al. 2000).
The inner anulus contains higher concentrations of Type 11 collagen much like hyaline
cartilage in appearance while the outer anulus contains principally Type 1 collagen, like
that seen in tendons and fibrocartilage (Schollmeier et al. 2000). Type 1 collagen
comprises 80% of the total collagen of the outer anulus as the layers progress towards
the periphery, with a suggestion of a ring of collagen Type1 fibre wider anteriorly than
posteriorly around the structure (Buckwalter 1995; Schollmeier et al. 2000).
9
Buckwalter reports proteoglycans accounting for only a few percent of the dry weight of
the anulus of a child, while Bogduk describes a much higher quantity of approximately
20% of an unspecified age disc (Buckwalter 1995; Bogduk 2005). The proteoglycans
act as a gel to bind the lamellae of the anulus together (Bogduk 2005).
The concentrations of Type 11 collagen, water and proteoglycans increase from the
peripheral to the more central layers of the anulus, while there is a decrease in Type 1
collagen (Buckwalter 1995; Bogduk 2005).
Figure 2.5 A Scanning electron micrographs demonstrating in A the alternating layersand density of collagen fibrils in the anulus, and B the loose collagen fibril networkof the nucleus (Buckwalter 1995).
The anulus which is vascular in infancy, becomes almost avascular in the adult (Taylor
1975; Taylor and Twomey 1988). This may be the result of disc growth which
effectively increases the distance between the inner disc and the peripheral blood supply
(Buckwalter 1995). However Stokes and Windisch (2006) found that spinal growth
through the years 10 to 20 was almost exclusively the result of changes in vertebral
body height. This too would challenge the blood supply to the intervertebral discs as
they compete with the adjacent vertebral growth plates for nutrition during growth
(Stokes and Windisch 2006).
2.2.3 Nucleus Pulposus
Contained within the anulus, the nucleus pulposus (nucleus) is a gel which comprises
more than 80% water in the young adult (Hukins 1988; McDevitt 1988). The high water
concentration interacting with proteoglycans provides resilience to compression
(Buckwalter 1995) with the application of axial force resulting in equal hydraulic
deformation of the nucleus against the end-plates and anulus (Adams and Hutton 1988;
Adams et al. 2002) (Figure 2.6). The nucleus progressively loses water as it ages. At
10
birth, water accounts for 88% of its dry weight, which reduces to 80% at 18 years of age
and 65% at 77 years of age (McDevitt 1988).
The nucleus of the disc contains 80% Type 11 collagen, 15-20% Type V1 with Type
111, Type 1X and Type X1 present in small amounts (Eyre 1988) (Figure 2.5B).
Type 11 collagen fibres, the type of collagen seen in hyaline cartilage and the vitreous
humour of the eye, are interspersed through the structure and constitute 15% to 20% of
the dry weight of the nucleus pulposus (Schollmeier et al. 2000).
Figure 2.6 Compression of the disccauses loss of height, increased radialbulging, and a change in alternatingfibre angle. The nucleus exhibits ahydrostatic pressure and creates atangential hoop stress in the anulus(Adams and Hutton 1988).
Figure 2.7 Inner lamellae of theanulus (left) merging into the end-plate (Hukins 1988).
After water, the second major component of the nucleus is proteoglycans (Bogduk
2005). Accounting for approximately 50% to 65% of the dry weight of the nucleus, a
majority of the proteoglycans are not clustered together but rather spread throughout the
nucleus interspersed with Type 11 collagen holding them together (Buckwalter 1995;
Bogduk 2005).
Hyaline cartilage and immature intervertebral discs contain large proteoglycans with the
ability to aggregate with hyaluronate while the mature disc contains large and
moderately sized proteoglycans that do not aggregate with hyaluronate (McDevitt
1988). McDevitt (1988) noted that these changes occur in discs without observable
pathology and should be considered part of the normal aging.
In contrast to the anulus, the nucleus of a young adult has a collagen content of 20% of
its dry weight, and a proteoglycan content of 50% of its dry weight (Buckwalter 1995).
11
Collectively the proteoglycans and collagen are known as the matrix of the disc
(Maroudas 1988; Bogduk 2005).
2.2.4 Vertebral End-plates
The superior and inferior surfaces of the vertebral / disc junctions are formed by hyaline
cartilage, approximately 0.6mm thick, with calcified cartilage adjoining the bone to
form the vertebral end-plate (Roberts et al. 2006). Edwards et al (2001) and Roberts et
al (1989) described the end-plate thickness as 0.1 to 1.6 mm, with thickness greater in
the lower lumbar vertebrae. Moore (2000) described the end-plate as being variable
across the width of the disc, with the central area being thinnest. These authors reported
no difference between the superior and the inferior end-plates. The end-plate is thinner
than the disc itself, with the disc typically being 1cm thick (Urban and Roberts 2003).
There have been differing opinions as to whether the end-plate is part of the vertebral
structure (Warwick and Williams 1973; Williams 1995; Moore and Dalley 2006) or
included with the disc (Hukins 1988; Taylor and Twomey 1988; Bogduk 2005). Review
of Figure 2.7 demonstrates that end-plates are an intrinsic part of the disc structure.
Hukins (1988) demonstrated that although the anulus and end-plate differ in
composition, sufficient evidence shows that they merge with one another. Taylor and
Twomey described “a lamellar structure in continuity with the anulus fibrosus” (Taylor
and Twomey 1988:66).
Roberts et al (1989) indicate that the end-plates consist of collagen fibres and
proteoglycans. These authors declared that the area of the end-plate covering the anulus
has a higher concentration of collagen, while the inner area of the end-plate covering the
nucleus has higher concentrations of water and proteoglycans as has been seen with the
content on the intervertebral disc. Observations made by Roberts in 2002, show that the
composition of the end-plate, being similar to that of the remainder of the disc, enables
diffusion to occur, with small molecules passing from vessels within the vertebral body
and end-plates to the disc (Roberts 2002).
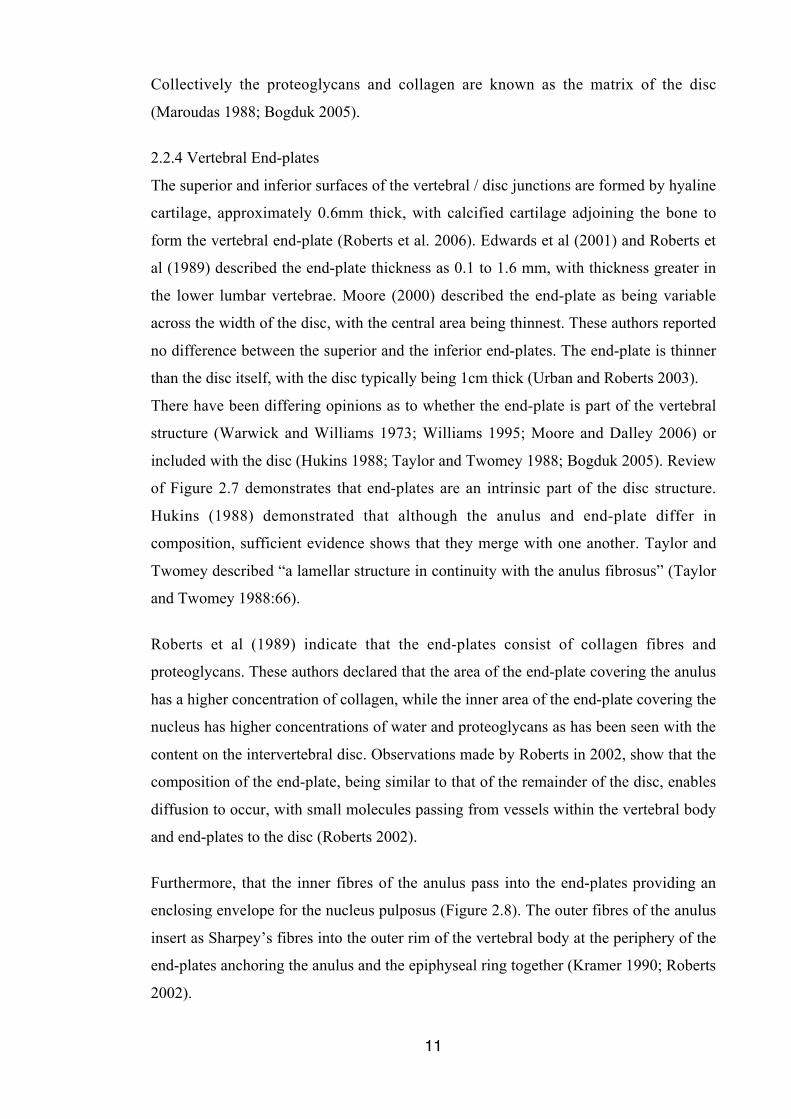
Furthermore, that the inner fibres of the anulus pass into the end-plates providing an
enclosing envelope for the nucleus pulposus (Figure 2.8). The outer fibres of the anulus
insert as Sharpey’s fibres into the outer rim of the vertebral body at the periphery of the
end-plates anchoring the anulus and the epiphyseal ring together (Kramer 1990; Roberts
2002).
12
According to Moore (2000), a variety of collagen types is found in disc tissue, but the
presence of Type X collagen has been of interest as it is thought to be involved in
cartilage calcification. Degeneration of the disc may be the result of abnormal
calcification of the end-plate resulting in reduction of nutrient flow.
Riches et al (2002) described the end-plates as an integral part of the motion segment,
with both the vertebra and the disc attached into them. The end-plates provide the
principal pathway for the transport of fluid into and out of the disc which is assisted by
loading and unloading the intervertebral disc creating a pumping action (Maroudas
1988; Riches et al. 2002), somewhat analogous to the action of a trampoline.
Figure 2.8 Vertebral end-platediagrammatically demonstrating theanulus enclosing the nucleus (Bogduk2005) but not the outer fibres of theanulus (Sharpey’s fibres) spanning overthe rim of the vertebral body to mergeinto the anterior longitudinal ligament .
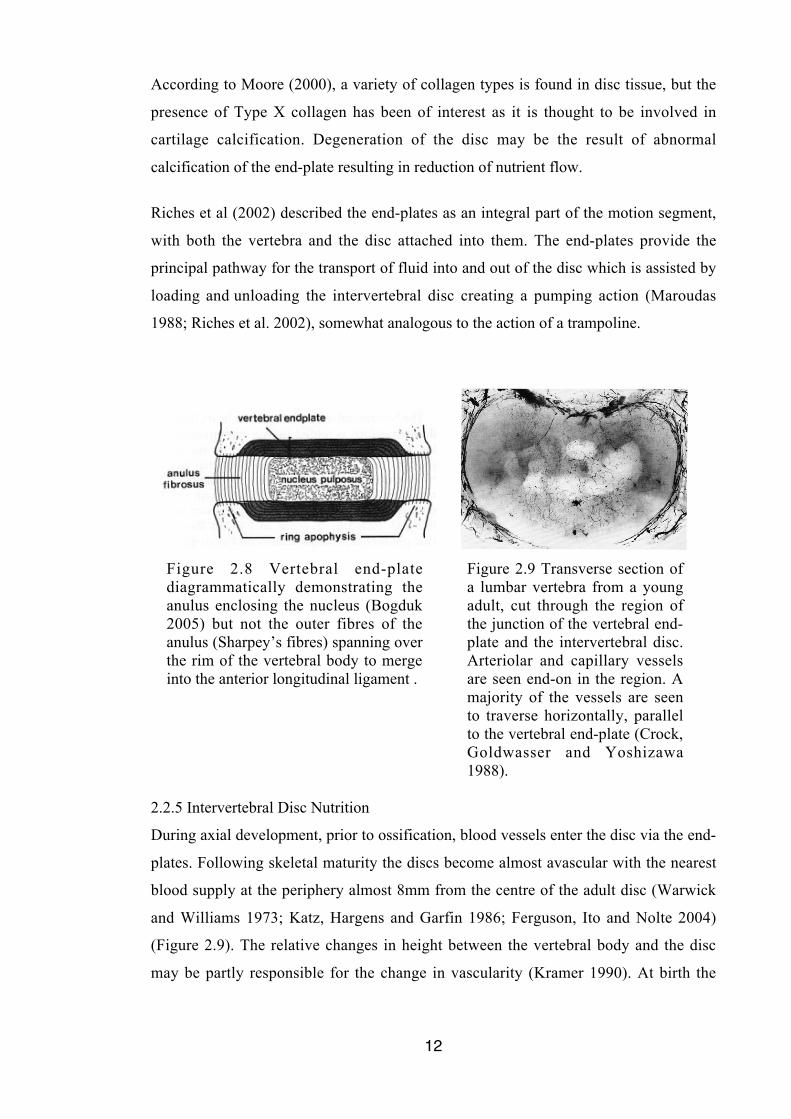
Figure 2.9 Transverse section ofa lumbar vertebra from a youngadult, cut through the region ofthe junction of the vertebral end-plate and the intervertebral disc.Arteriolar and capillary vesselsare seen end-on in the region. Amajority of the vessels are seento traverse horizontally, parallelto the vertebral end-plate (Crock,Goldwasser and Yoshizawa1988).
2.2.5 Intervertebral Disc Nutrition
During axial development, prior to ossification, blood vessels enter the disc via the end-
plates. Following skeletal maturity the discs become almost avascular with the nearest
blood supply at the periphery almost 8mm from the centre of the adult disc (Warwick
and Williams 1973; Katz, Hargens and Garfin 1986; Ferguson, Ito and Nolte 2004)
(Figure 2.9). The relative changes in height between the vertebral body and the disc
may be partly responsible for the change in vascularity (Kramer 1990). At birth the
13
vertebra and disc are of the same height but at maturity the disc is 20% to 33% of the
height of the vertebra (Kramer 1990).
The principal source of nutrition to the disc is derived via the end-plates. Rajasekaran et
al (2004) state that diffusion is the only source to disperse nutrients, such as glucose and
oxygen, into the body of the disc and transfer metabolites (lactic acid and carbon) away
from the disc (Riches et al. 2002; Rajasekaran et al. 2004).
The trabecular spaces of the vertebral body are connected to the thin covering of hyaline
cartilage of the end-plate via marrow connecting channels (MCCs) (Ayotte, Ito and
Tepic 2001; Benneker, Heini, Alini et al. 2005). Capillary buds emerge from the MCCs
providing a pathway enabling the diffusion capability of the disc. As there are more
channels in the central area than the periphery, the nucleus has greater ‘vascular’
contact (Moore 2000; Ayotte et al. 2001).
Nutrition of the disc creates a change in the height of the structure over a 24 hour
period, reported as diurnal disc change (Eklund and Corlett 1984; Tyrell, Reilly and
Troup 1985; Krag, Seroussi, Wilder et al. 1987; Broberg 1993; Hutton, Malko and
Fajman 2003). Two different forces drive the mechanisms of fluid exchange within the
intervertebral disc, mechanical pressure by compression, and osmosis created by the
negatively charged proteoglycans within the disc (Urban and McMullin 1988; Broberg
1993). In an in vitro study applying a compressive weight equal to that of a body across
a disc, Adams and Hutton (1983) concluded that approximately two thirds of the
reduction in height was the result of water loss, and the remainder of the loss due to
other factors.
During the day, considered 16 hours of load bearing, the mechanical force of
compression on the porelastic disc structure creates a fluid flow which leads to
deformation of the disc (Malko, Hutton and Fajman 2002; Ferguson et al. 2004). A
majority of the deformation of the disc occurs in the first four hours of weight bearing,
with 54% loss in the first hour and 83% in three hours and 45 minutes (Tyrell et al.
1985). These figures correspond closely to those of Reilly et al (1984) who found that
height loss during the weight-bearing portion of the day was 54% at one hour and 80%
at three hours. However losses as low as 26% at one hour increasing to 75% at four
hours were found by Krag et al (1990) during an in vivo study involving subjects
examined after eight hours upright and four hours recumbent.
14
The remaining eight hours of the diurnal cycle the body is rested during which time
osmotic pressure drives imbibing of the fluid (Malko et al. 2002). Although the loading
period is twice as long, Ferguson et al (2004) found that the fluid lost through
compression was completely recovered during the rest period with 71% regained during
the first half of the night (Tyrell et al. 1985). In a study where subjects were recumbent
for four hours, Krag et al (1990) found that in the first hour subjects regained 110% of
the height lost during the first four hours of weight bearing and 83% of that lost over
eight hours of weight bearing. But their overall recovery rates are difficult for direct
comparison with Tyrell et al (1985) in that they reported a recovery period of 4.2 hours
recumbency, with 41% recovered in 1.1 hours and 56% at 2.1 hours (Krag et al. 1990).
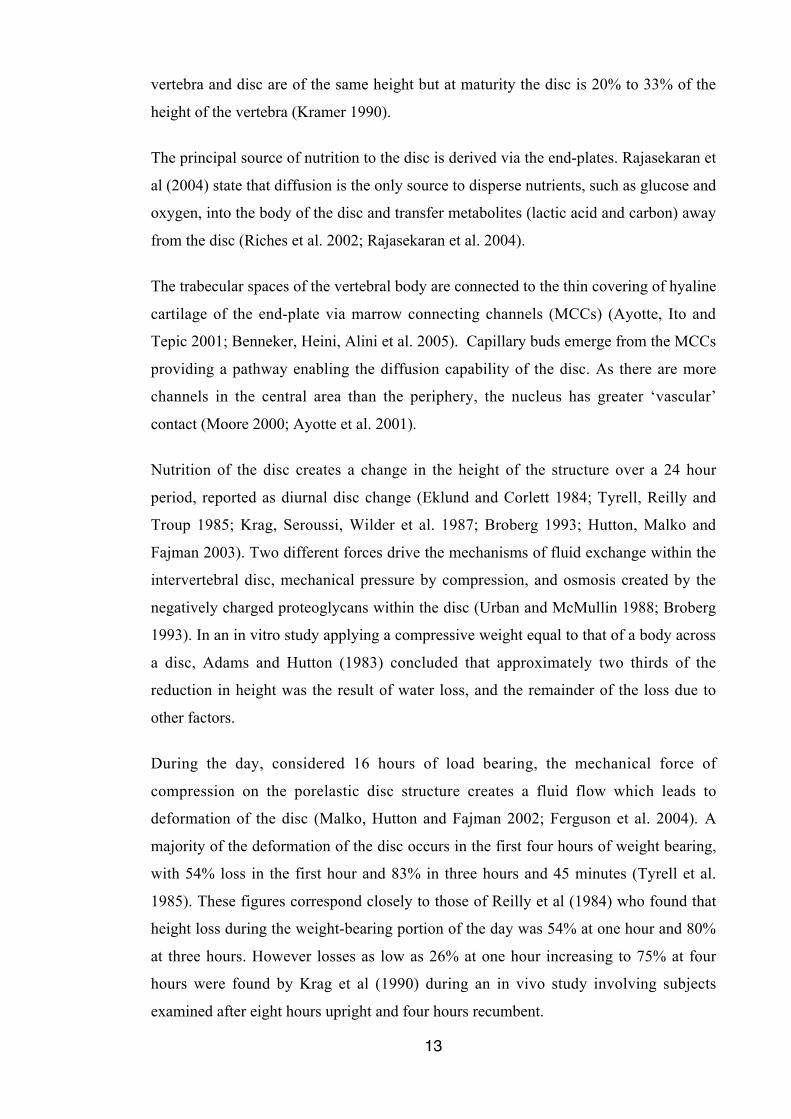
It does seem likely that all the researchers agree that majority of the height loss that
occurs daily is in the first four hours of the day, and that a majority of the height gained
during recumbency is during the first four hours of the night (Tyrell et al. 1985; Krag et
al. 1990; Ferguson et al. 2004) (Figure 2.10).
According to De Puky the average variation from morning to night is a loss of 1%,
0.5% in the elderly and 2% in a child, while Malko et al revealed an increased volume
of 10.6% or 0.9cm3 of fluid as the result of overnight rest (De Puky 1935; Malko et al.
2002; Hutton et al. 2003). Malko et al (2002) described the total fluid exchange during a
single diurnal cycle as being 10% to 20% of the total disc volume.
Figure 2.10 Changes in disc height over one diurnal loading cycle. The disc fullyrecovered the height lost during 16 hours of loading by resting for 8 hours (Fergusonet al. 2004).
2.2.6 Longitudinal Ligaments
Anteriorly and posteriorly ligaments which vary in thickness through the entire spine
interconnect the vertebral bodies as seen in Figure 2.11. The anterior longitudinal
15
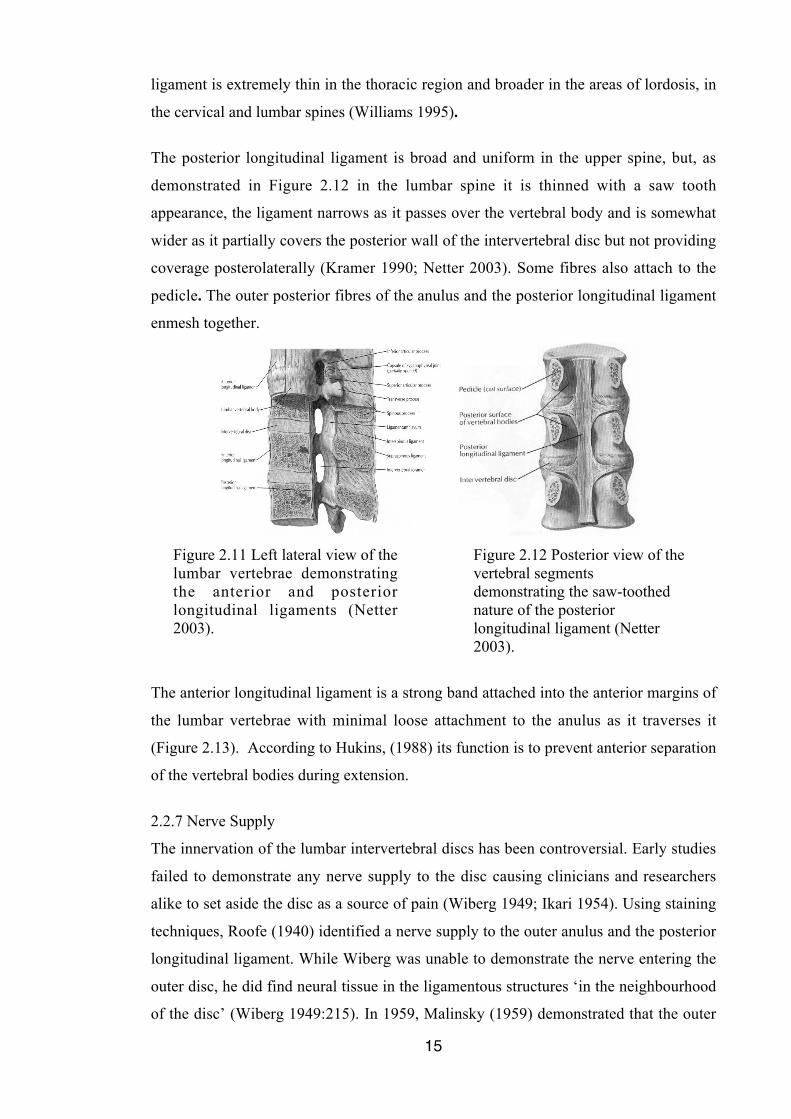
ligament is extremely thin in the thoracic region and broader in the areas of lordosis, in
the cervical and lumbar spines (Williams 1995).
The posterior longitudinal ligament is broad and uniform in the upper spine, but, as
demonstrated in Figure 2.12 in the lumbar spine it is thinned with a saw tooth
appearance, the ligament narrows as it passes over the vertebral body and is somewhat
wider as it partially covers the posterior wall of the intervertebral disc but not providing
coverage posterolaterally (Kramer 1990; Netter 2003). Some fibres also attach to the
pedicle. The outer posterior fibres of the anulus and the posterior longitudinal ligament
enmesh together.
Figure 2.11 Left lateral view of thelumbar vertebrae demonstratingthe anterior and posteriorlongitudinal ligaments (Netter2003).
Figure 2.12 Posterior view of thevertebral segmentsdemonstrating the saw-toothednature of the posteriorlongitudinal ligament (Netter2003).
The anterior longitudinal ligament is a strong band attached into the anterior margins of
the lumbar vertebrae with minimal loose attachment to the anulus as it traverses it
(Figure 2.13). According to Hukins, (1988) its function is to prevent anterior separation
of the vertebral bodies during extension.
2.2.7 Nerve Supply
The innervation of the lumbar intervertebral discs has been controversial. Early studies
failed to demonstrate any nerve supply to the disc causing clinicians and researchers
alike to set aside the disc as a source of pain (Wiberg 1949; Ikari 1954). Using staining
techniques, Roofe (1940) identified a nerve supply to the outer anulus and the posterior
longitudinal ligament. While Wiberg was unable to demonstrate the nerve entering the
outer disc, he did find neural tissue in the ligamentous structures ‘in the neighbourhood
of the disc’ (Wiberg 1949:215). In 1959, Malinsky (1959) demonstrated that the outer
16
third of the anulus contained a variety of nerve endings. Studies, by surgeons, of
intervertebral discs removed during lumbar fusions provided evidence of extensive
innervation of the anterior and posterior longitudinal ligaments and the outer layers of
the anulus fibrosus (Rabischong, Louis, Vignaud et al. 1978; Yoshizawa, O'Brien,
Smith et al. 1980). The elegant studies performed by Stilwell (1956) using primates,
provided a detailed map of spinal innervation which subsequently has been elaborated
in the human by Groen (1990) and others (Taylor and Twomey 1979; Bogduk, Tynan
and Wilson 1981; Coppes, Marani, Thomeer et al. 1997). These studies have typically
used foetal tissues given the enhanced stain within such material.
The nerve plexus innervating the posterior longitudinal ligament and entering at least 3
mm into the outer anulus fibrosus, has been found to include small diameter substance P
(SP)- nerve fibres immunoreactive to neuropeptides calcitonin gene-related peptide
(CGRP)- and vasoactive intestinal peptide (VIP)- (Ashton, Roberts, Jaffray et al. 1994;
Coppes et al. 1997; Palmgren, Gronblad, Virri et al. 1999).
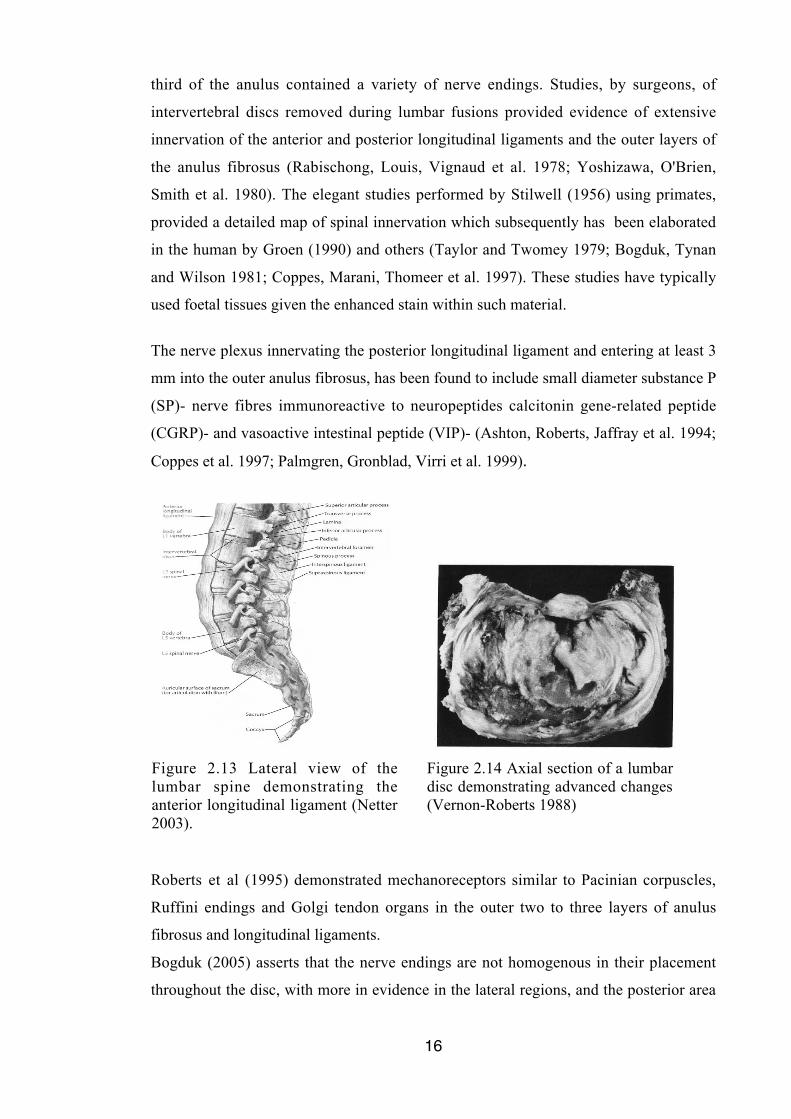
Figure 2.13 Lateral view of thelumbar spine demonstrating theanterior longitudinal ligament (Netter2003).
Figure 2.14 Axial section of a lumbardisc demonstrating advanced changes(Vernon-Roberts 1988)
Roberts et al (1995) demonstrated mechanoreceptors similar to Pacinian corpuscles,
Ruffini endings and Golgi tendon organs in the outer two to three layers of anulus
fibrosus and longitudinal ligaments.
Bogduk (2005) asserts that the nerve endings are not homogenous in their placement
throughout the disc, with more in evidence in the lateral regions, and the posterior area

17
having more than the anterior, but according to Groen et al (1990) an abundant nerve
plexus is present in both the anterior and posterior longitudinal ligaments.
In a prospective study of 193 consecutive patients, Kuslich et al (1991) stimulated a
variety of structures during surgery while the patient was fully awake or only minimally
sedated. In stimulating ligaments, fascia, bony structure, facet joint capsule and
synovium, dura, nerve root, anulus at three sites, nucleus and end-plate, they found that
the outer layer of the anulus and the posterior longitudinal ligament were, by far, the
most common sources of lower back pain. A swollen, stretched or compressed nerve
root was the only source of sciatica. While not providing true anatomical description of
nerve supply, the in vivo study by Kuslich et al (1991) gives clinical appreciation of the
pain sources.
2.2.8 Aging of the Disc
With aging, changes occur in the composition of the nucleus, which according to
Roberts et al (2006), may be attributable to a loss of water. Urban and McMullin (1988)
found that water content reduced from 85% at 14 years of age, to 75% at 91 years.
Reduction of glycosaminoglycan reduces the water attracting ability of the nucleus both
in degeneration and in aging (Roberts et al. 2006) with the loss of water content of the
anulus resulting in a loss of height in the disc. Whether this loss of height is a normal
aging process or a pathological feature remains a matter of conjecture. Twomey and
Taylor (1985) report this phenomena as a pathological process, which is not associated
with normal aging, while Roberts et al (2006) appear to support earlier theories
propounded by Beadle in 1931 (Beadle 1931) that this is indicative of the early
appearance of age changes brought on by “unduly severe functional strain” (Roberts et
al. 2006:13). Degenerative changes in lumbar discs have been observed in young
children aged 11 to 16 (Boos, Weissbach, Rohrbach et al. 2002). While approximately
20% of teenage subjects demonstrate some disc degeneration; by 70 years of age, up to
60% subjects give evidence of severe degeneration (Urban and Roberts 2003) (Figure
2.14).
Coppes et al (1997) and Roberts et al (2006) describe the process of disc aging with the
appearance of larger diameter collagen fibres in the anulus, followed by disorganisation
of the lamellae, and an increase in blood supply and neovascular innervation (ie. nerves
to the smooth muscle of the blood vessels as they grow into the disc through fissures
within the anulus).
18
A cautious approach is recommended by Schollmeier et al (2000) in interpreting age
related changes in collagen content and distribution as the observations may be
conformational changes of the collagen fibrils. Their observations with the use of
immunohistochemistry, including that Type 1 collagen extended further into the nucleus
pulposus in older specimens, and that Type 11 collagen was seen more often in the
outer anulus in specimens over 58 years, must be understood as approximations rather
than exact representation (Schollmeier et al. 2000).
The bifurcation or blending together of the layers of the lamellae was reported by
Urban and Roberts (2003; Roberts et al. 2006) as a sign of degeneration, along with
the disorganisation of the collagen and elastin of the anulus (Roberts et al. 2006).
Adams et al (2002), and Bogduk (2005) have reported this as normal anatomy citing
evidence of discontinuous lamellae in foetal discs.
With aging, changes develop in the calcification of the end-plate which may affect the
transport of proteoglycans to the nucleus resulting in loss of nutrition, essential solutes,
to the disc and reduction in removal of metabolites (Moore 2000). Roberts et al (1996)
and Ayotte et al (2001) observed that the MCCs become occluded, obstructed by
calcification, decreasing the overall permeability of the end-plate. It is likely that
calcification of the MCCs results in this impaired diffusion of fluid into and out of the
intervertebral disc rather than decrease in fluid flow causing calcification of the
channels (Benneker et al. 2005).
In a study which tested the equilibrium hydration of discs in response to stress in
subjects between 14 and 91 years of age, Urban and McMullin (1988) reported that the
35 to 45 year old discs had the highest swelling pressure. Kramer (1990) reported
similar findings, that hydrostatic pressure was responsible for more rapid re-expansion
of discs of adolescents than aged subjects following compression of the disc, but that
subjects aged 30 to 50 demonstrated remarkably high hydrostatic pressure. When this is
considered with changes in the anular wall with aging the highest risk period during life
for a disc disturbance is identified at 35 to 55 years of age
2.2.9 Summary
The structures of the intervertebral disc, intervertebral disc nutrition, nerve supply, and
the effects of aging have been reviewed.
19
2.3 MECHANICS OF THE INTERVERTEBRAL DISC
2.3.1 Introduction
The intervertebral discs allow movement of an otherwise rigid spine. The forces acting
on the spinal column are resisted by different components of the system: the vertebral
bodies resist most of the compressive force acting longitudinally on the spine, with the
intervertebral discs resisting some of the compressive force, the apophyseal joints resist
forces acting perpendicular to their surfaces therefore limiting shear and rotational
forces applied to the disc, and the intervertebral ligaments limit bending (Adams and
Dolan 1995). Rather than acting as a ‘shock absorber’, the principal role of the
intervertebral discs is to transfer forces applied to the spine from vertebra to vertebra via
these structures (Adams and Hutton 1988).
It is likely that damage to the disc does not occur in applying simple loads to the spine,
but with complex loading involving combinations of forces disc disturbance can occur
(Adams and Hutton 1988). In Brinckmann’s investigation of pure axial compression of
the disc without side bending, flexion or extension, even with an instrument induced
fissure and loads of 2kN, the disc wall did not rupture (Brinckmann 1986). Whereas
when a second force vector is included increasing the complexity of loading, the disc
ruptures in a predictable manner (Adams and Hutton 1982; McNally, Adams and
Goodship 1993).
2.3.2 Role of Disc in Spinal Mechanics
During movement of the spine forces are applied to the vertebrae and intervertebral
discs. Compression acts down the long axis of the spine at 90 degrees to the
intervertebral discs causing compaction; shear acts in the midplane of the disc tending
to cause one vertebra to move forward relative to the one below, deforming the disc
without compacting or stretching; tensile force pulls an object apart; and bending allows
the upper body to pivot about the lower one (Adams and Hutton 1988; Adams et al.
2002).
Intervertebral discs are able to resist compression with fracture of the end-plate or
fracture of the vertebral body, as the most likely result of compressive failure of a
motion segment (Adams and Hutton 1988).
20
With compressive load the disc bulges radially. The radial bulge is the response of the
anulus, which is relatively rigid, resisting stresses directly and losing height. After
applying 2.5kN compressive load, Wenger and Schlegel (1997) found that the bulge
was not symmetrical but rather that the disc distorted more in the postero-lateral region,
with the posterior part of the disc somewhat restrained by the posterior longitudinal
ligament.
The response of the nucleus to compression follows the behaviour of a pressurised fluid.
As the external compression raises stress within the nucleus it causes the end-plates to
deflect into the vertebral bodies (Adams and Hutton 1988; Adams and Dolan 1995).
The deformity of the disc seen during compression will resolve, and provided the load is
not sustained the disc will rapidly resume its former shape. However, if the load is
sustained the disc loses height, a state known as creep. McGill and Brown described
creep as “being the progressive deformation of a structure under constant load that is
below the level of load required to complete tissue failure” (McGill and Brown
1992:43). The degree of creep demonstrated by a disc is dependent on the load applied,
the previous loading of the disc and the state of health of the disc (Adams and Dolan
1995). Sustaining load produces a different rate of creep to cyclic loading. McGill and
Brown (1992) demonstrated that 20 minutes of sustained load in flexion producing
creep followed by 20 minutes of rest allowed only a 50% recovery of pre-creep tissue
stiffness (McGill and Brown 1992; Little and Khalsa 2005). Little and Khalsa (2005)
found that while creep occurred with both sustained and repeated flexion, creep
occurred more rapidly with sustained posture. The rate of creep and the recovery period
for complete restoration following unloading is known as hysteresis (Oliver and
Twomey 1995).
Bending includes the movements of flexion, extension and lateral flexion. During
flexion the nucleus tends to move posteriorly while the anterior anulus bulges radially,
and conversely in extension the nucleus tends to move anteriorly and the posterior
anulus bulges radially (Shah, Hampson and Jayson 1978; Krag et al. 1987; Fennell,
Jones and Hukins 1996; Edmondston, Song, Bricknell et al. 2000). Put simply, during
bending movements the nucleus acts like a ball-bearing allowing the upper body to
pivot about the lower one, with the anulus and intervertebral ligaments resisting the
motion (Adams and Hutton 1988). When then the disc is degenerated the behaviour of
21
the nucleus pulposus during flexion and extension is less predictable, especially during
extension (Edmondston et al. 2000).
Adams and Hutton (1988) demonstrated that the motion segment could resist force of
50Nm before sustaining damage, which is approximately double the force applied to the
lumbar spine during toe touching. They concluded that the lumbar spine must receive
considerable support from the back muscles and lumbodorsal fascia (Adams and Hutton
1988). However in the early morning when the fluid content of the discs is greater as a
result of diurnal flow, the back musculature and ligaments are not able to fully
compensate, which increases bending stresses on the spine (Adams and Hutton 1988).
The higher fluid content makes the spine more resistant to forward bending (Adams and
Hutton 1988). Because the back muscles do not fully compensate for this by restricting
range of flexion, bending stresses on the disc, and to a lesser extent on the ligaments,
increase considerably in the morning (Adams and Hutton 1988), the peak bending
moment probably rises by more than 100% (Adams and Dolan 1995).
Lateral bending has not been studied to the same extent as flexion and extension, but it
is likely the disc contents behave in a similar manner, tending to move to the lateral or
postero-lateral disc opposite to the side of bending. Costi et al in a study of maximum
shear strain (MSS) of intervertebral discs found that lateral bending provided more MSS
per degree of rotation than all other tests and that the MSS produced was at the postero-
lateral region opposite the side of bending (Costi, Stokes, Gardner-Morse et al. 2007).
They found that lateral bending and flexion produced the greatest MSS, and that when
the two occurred together there was a greater risk of disc injury (Costi et al. 2007).
Adams and Hutton (1988) have demonstrated in cadaveric studies that lateral flexion
can couple with axial rotation movements. Axial rotation (torsion) is twisting of the
spine about its long axis with the centre of movement placed in the posterior third of the
vertebral bodies and intervertebral discs (Adams et al. 2002). It is not a combination of
forward and lateral bending, but is the rotation seen in a discus throw. Axial rotation is
restricted by the orientation of the zygapophysial joints and the intervertebral disc
(Morgan and King 1957; Farfan, Cossette, Robertson et al. 1970; Krismer, Haid,
Behensky et al. 2000).
Compression has been considered synonymous with spinal loading as measured by
Nachemson who provided the accepted values of pressure transmitted through the disc

22
by inserting pressure sensitive needles into the L3/4 disc of volunteers (Nachemson
1960). This study was repeated by Wilke et al (1999) and by Sato et al (1999) with the
L4/5 disc pressures measured with very similar results verifying Nachemson’s earlier
work. However these measurements of pressures are with combined forces, not axial
compression alone.
2.3.3 Summary
The intervertebral discs allow movement of an otherwise rigid spine, with various
components of the motion segment resisting specific forces acting on the spinal column.
Complex loading of the intervertebral disc is more likely to result in damage to the
structure than the application of simple loads.
2.4 LUMBAR MUSCULATURE.
2.4.1 Introduction
The lumbar spine may be conceptualised as an articulated rod, at times flexible to allow
movement, and at other times rigid to maintain position or to transfer forces through the
vertebral column. Richardson et al (1999) discuss the trunk muscles in two categories,
namely; the local and the global stabilising systems. The local system comprises
muscles attached to the lumbar spine to influence spinal segmental stiffness and posture
and a global system by muscles of the trunk, which are primarily involved in
movement, and transfer of loads between the pelvis and the thorax.
2.4.2 The Diaphragm
The diaphragm is a large domed muscle positioned with a convex surface directed into
the thorax, serving as a functional septum between the heart and lungs above and the
contents of the abdomen below. Arising from costal and sternal attachments, the
diaphragm sits higher anteriorly and slopes downwards as it passes back to form the
medial and lateral arcuate ligaments, and the attachment to the anterior vertebral bodies
via the crura, which cross the abdominal aorta (Williams 1995). The medial and lateral
arcuate ligaments give attachment to the transverse processes of the upper lumbar spine
(Williams 1995). The crura are continuous with the anterior longitudinal ligament and
possibly form a majority of this structure in the lumbar spine (Williams 1995; Bogduk
2005).
Although primarily a muscle of respiration, it is likely that the diaphragm provides a
lumbar stabilising mechanism but is not involved in lumbar movement (Richardson et
al. 1999; Hodges, Heijnen and Gandevia 2001).
23
2.4.3 The Pelvic Diaphragm
The inferior boundary of the abdomen, the pelvic diaphragm, is comprised of the deep
muscle layer of levator ani and coccygeus (Williams 1995).
Levator ani is comprised of pubococcygeus, iliococcygeus and ischiococcygeus, arising
respectively from the pubis, from the tendinous arch between the pubis and the ischial
spine, and from the ischium (Williams 1995).
The pubococcygeus is the strongest of these muscles, with the muscle from one side
meeting midline with its opposite number, forming the central tendon of the perineum,
attaching into the anterior sacrococcygeal ligament, and surrounding the internal and
external sphincters of the anus. In effect, the pubococcygeus acts like a muscle sling
from the pubis anteriorly to the sacrum posteriorly (Williams 1995).
The coccygeus arises from the ischial spine and passes as a flat triangular muscle to fuse
with the sacrospinous ligament. It is in the same plane as levator ani, placed more
posteriorly (Williams 1995).
Pelvic diaphragm muscles contract with transversus abdominis probably assisting in
controlling intra-abdominal pressure (Richardson et al. 1999). Contraction of
pubococcygeus occurs with transversus abdominis to stabilise the lumbar spine during
movement of a limb (Richardson et al. 1999) and conversely, it has been noticed that
transversus abdominis co-contracts with the pelvic floor during retraining of bladder
function for urinary stress incontinence (Sapsford, Hodges, Richardson et al. 2001).
2.4.4 Anterior Abdominal Wall
The rectus abdominis bilaterally arranged vertically from superficial to deep, the
external and internal oblique, and the transversus abdominis form the flat muscular
sheet of the anterior abdominal wall. The oblique abdominal muscles together with
bilaterally arranged transversus form a bilaminar aponeurosis which envelops the
midline rectus anteriorly and posteriorly. Each aponeurosis crosses the midline blending
to form a thickening, the linea alba (Williams 1995).
With the pelvis fixed, the recti act as prime movers, and the external and internal
oblique muscles in a secondary role, to flex the lumbar spine. Unilateral contraction
may produce side bending, and rotation occurs with the contraction of the external
oblique of the opposite side and the internal oblique of the same side.
24
Traditional descriptions of muscle action do not portray transversus as having direct
action on the lumbar spine (Williams 1995), but Richardson et al (1999) describe
bilateral transversus abdominis as part of a local stabilising system acting via the
thoracolumbar fascia. The transversus has a higher proportion of slow twitch fibres than
fast twitch, histologically more like the lumbar paravertebral muscles than the other
abdominal muscles, supporting the view of this muscle as important in maintenance of
posture (Jorgensen, Mag, Nicholaisen et al. 1993).
2.4.5 Lateral Abdominal Wall
Antero-laterally, two large muscles, psoas major and quadratus lumborum, have their
origins in the lumbar spine but their ability to act on the spine has been contentious
(Bogduk, Pearcy and Hadfield 1992; McGill, Juker and Kropf 1996; Richardson et al.
1999; Penning 2000).
Psoas major is a hip flexor and external rotator but as it gains attachment from the
lateral aspects of the vertebrae, discs and transverse processes from T12 to L5, thus it
has the potential to act on the lumbar spine. Despite these attachments, Richardson et al
(1999) consider psoas major to be a hip flexor and an exception to the local stabilising
system. Biomechanical analysis has demonstrated that psoas has the ability to extend
the upper and flex the lower lumbar segments (Bogduk 2005:102) leading Penning
(2000) to further comment on its contribution as movement neutral with the potential to
stabilise the lumbar spine in upright stance.
Quadratus lumborum can be considered in two separate functional units. The medial
fibres which attach to the transverse processes of the lumbar vertebrae have been
confirmed with EMG as local stabilisers (McGill et al. 1996), while the lateral fibres are
without vertebral attachment and are considered to be global stabilisers (Richardson et
al. 1999).
2.4.6 Posterior Abdominal Wall
Posteriorly there is a deep layer of small intersegmental muscles with two more
superficial muscle groups, the polysegmental group which attach to the lumbar spine,
multifidus and erector spinae, and the longer muscles of the back, the thoracic
components of longissimus and iliocostalis lumborum which cross the lumbar spine not
necessarily attaching to it (Anderson 1976).
25
The intersegmental muscles directly connecting adjacent vertebrae, intertransversarii
laterales dorsales, intertransversarii laterales ventrales, intertransversarii mediales,
rotatores and interspinales, are small muscles unlikely to play a role in spinal movement
as they are positioned at a mechanical disadvantage outside the axis of movement.
The polysegmental group of muscles act in a synergy to provide movement and posture
of the lumbar spine (Jorgensen et al. 1993).
Multifidus is a fleshy muscle, each fasciculus arising from the lamina and inferior edge
of the spinous process, it passes caudad two to five levels with fibres attaching to the
mamillary processes of the subjacent vertebrae (Macintosh, Valencia, Bogduk et al.
1986; Jemmett, MacDonald and Agur 2004; Bogduk 2005).
Lying lateral and superficial to multifidus in the lumbar spine, the erector spinae
comprises longissimus thoracis, iliocostalis lumborum and spinalis thoracis.
Spinalis thoracis arises by three or four tendons from the eleventh thoracic to the second
lumbar vertebral spines. It passes cephalad and medial to longissimus thoracis, inserting
to the spines of the upper four to eight thoracic vertebrae.
Longissimus thoracis arises from the posterior surfaces of the transverse process and
accessory process of each of the lumbar vertebrae. The muscle digits from L1 to L4
form tendons at their caudal ends and attach to the ilium lateral to the insertion of L5.
This, in effect, is a common tendon of insertion.
Iliocostalis lumborum arises from the tip of the transverse process of the vertebrae from
L1 to L4, where it blends with longissimus, and inserts into the iliac crest lateral to the
posterior superior iliac spine. The fascicle from L5 is described as the iliolumbar
ligament.
2.4.7 Function of the Lumbar Musculature
Multifidus has been described as producing extension with spinales, lateral flexion with
intertransversarii, and rotation with rotatores (Williams 1995), but it is likely that these
small muscles, with abundant muscle spindles, provide proprioception for the lumbar
spine (Adams et al. 2002) and that multifidus, with its arrangement of muscle fibre
pulling downwards on each spinous process, is an extensor with the ability to increase
lumbar lordosis (Quint, Wilke, Shiraz-Adl et al. 1998; Bogduk 2005).
The placement of the muscle fibres of longissimus thoracis provides it with the ability
to act both vertically and horizontally. Each digit of the muscle can act segmentally, and
26
either unilaterally or bilaterally. Acting unilaterally results in lateral flexion, and
bilaterally produces extension.
Like the longissimus thoracis, the iliocostalis lumborum can act both vertically and
horizontally. With the origin of the muscle attaching to the tip of the transverse process,
unilateral contraction will result in strong lateral flexion of the trunk. Bilateral
contraction may be observed to produce extension. The orientation of fibres indicates
that iliocostalis lumborum should be able to produce axial rotation when acting
unilaterally, but primarily the oblique abdominal muscles carry out this action.
Iliocostalis lumborum works with multifidus to resist flexion which occurs
simultaneously with abdominal oblique muscle contraction to produce rotation
(Richardson et al. 1999).
According to Richardson et al (1999) multifidus, longissimus and iliocostalis are part of
the local stabilising system, with histochemical analysis revealing four to five
capillaries in contact with each muscle cell putatively supplying these muscles with a
high concentration of oxidative enzymes and therefore endurance capacity (Jorgensen et
al. 1993). This analysis together with Type 1 muscle fibres found in these paravertebral
muscles is strongly indicative of muscle used in maintenance of position (Jorgensen et
al. 1993).
The thoracic components of longissimus and iliocostalis lumborum are to be considered
part of the global stabilising system, crossing the lumbar spine without attachment
(Richardson et al. 1999). Fascicles of these muscles connect the thoracic vertebrae and
ribs to the sacrum and ilium. Bilateral contraction will result in extension and unilateral
contraction will laterally flex the lumbar spine (Bogduk 2005).
2.4.8 Summary
Whether each of the muscles is involved in larger trunk movement or in segmental
stabilisation, the stability of the muscle system of the trunk as a whole is dependent on
the integrity of each of its components. The muscles of the trunk inter-relate with one
another so that while trunk movement is occurring the spine remains segmentally stable.
27
2.5 HISTORICAL PERSPECTIVE
SPINAL SURGERY
2.5.1 Introduction
The evolution of the intervertebral disc as a cause of pain, loss of muscle power, and
loss of sensation in the back and upper and lower limbs, took 170 years to progress from
the point, in 1764, when Domenico Cotugno (1764) described ‘sciatica’ as a clinical
phenomenon to acceptance by the medical community of Mixter and Barr’s classic
description of intervertebral disc prolapse causing the clinical signs and symptoms
observed (Mixter and Barr 1934). The changes, which occurred over time, were to the
surgical procedures in isolation; at no point were changes directed at rehabilitation. The
surgeon’s anticipation has been that the surgery corrects the derangement and the
patient will spontaneously recover. As recently as 1951, O’Connell (1951) reported
patients being bed-bound for eight days after surgery and hospitalised for three weeks.
That was the extent of the ‘rehabilitation’. Success of surgery was measured against
such complications as: major neurological deficit; loss of bladder or bowel function;
and in the extreme, death (O'Connell 1951).
2.5.2 Early Development of Disc Surgery
During the late 19th century, there was great progress towards resolution of the
symptoms of spinal cord and neural compression seen regularly by physicians. In the
1880’s, William Macewen and Sir Victor Horsley of Kensington, England were
successful in removing ‘connective tissue tumors’ by means of laminectomy (Macewen
1884; 1885; Gowers and Horsley 1888; Scarff 1955).
Towards the end of the 19th century, Rudolf Virchow and Theodor Kocher disclosed
disc extrusion at autopsy (Kocher 1896; Le Vay 1990), and in 1911 Middleton &
Teacher, and Goldthwait observed herniations (Le Vay 1990). Despite these
observations, herniations of the nucleus pulposus were diagnosed and treated as
extradural chondromas (Dandy 1926; Elsberg 1928).
In 1925 a pathologist, Georg Schmorl, together with a radiologist, Herbert Junghanns,
began routine post-mortem examination of the spine. While his peers were convinced
that ‘chondromas’ of one type or another caused the signs they observed, Schmorl had
found herniations into the superior and inferior end plates of vertebrae, and anteriorly
and posteriorly protruding from the intervertebral disc. These he named ‘Schmorl’s
Nodes” (Schmorl and Junghanns 1959).
28
2.5.3 Early twentieth century developments
Walter Dandy further developed the understanding of the clinical signs and symptoms
of disc herniation enabling appropriate surgical treatment for patients (Dandy 1926;
1929). With an accurate history and examination, Dandy was able to piece together
much of what we currently know about disc related back pain (Dandy 1926; 1929;
1942). He found that the initial onset was often insignificant back pain, with signs and
symptoms increasing with recurrence. A loss of normal anterior lumbar curve (lumbar
lordosis) and a scoliosis (lateral shift) were often observed. He noted spasm of the
erector spine and tenderness on palpation of the spinous processes (Dandy 1929). On
peripheral neurological examination changes in reflexes were present. Patients often
reported loss of bladder and bowel control. He recognised radicular symptoms could
alter with changes in discal pressure as in sneezing (Schultze 1903; Cassirer 1923;
Dandy 1926; 1929).
He recognised that standard X-rays did not always disclose information pertaining to
herniation of the intervertebral disc (Dandy 1929). A loss of height might be observed
but its cause was not necessarily intervertebral disc herniation. Dandy (1929)
recognised that the clinical presentation included a history of recurrent episodes
occurring with varying intervals from months to years. The final episode prior to
surgery often involved trauma or heavy lifting (Dandy 1929).
On occasion there was spontaneous resolution as evidenced by the disappearance of
signs and symptoms (Dandy 1942). Dandy (1929) noted that most patients recovered
fully after surgery and did not experience recurrence. However, of paramount
importance at that time, was surviving the surgery and the immediate post-operative
period, and secondly recovering bladder and bowel function, sensation and muscle
power (Dandy 1929).
Mixter and Barr (1934) caused great controversy with the publication of their now
classic article published in the New England Journal of Medicine in August 1934.
Together they had documented 19 cases by Mixter, 17 of which under-went a surgical
procedure to decompress the spinal cord or nerve roots. The timing of the onset of
symptoms caused Barr to think beyond the accepted diagnosis of ‘enchondroma’.
Pathology of the tissue proved them correct; it was normal disc tissue.
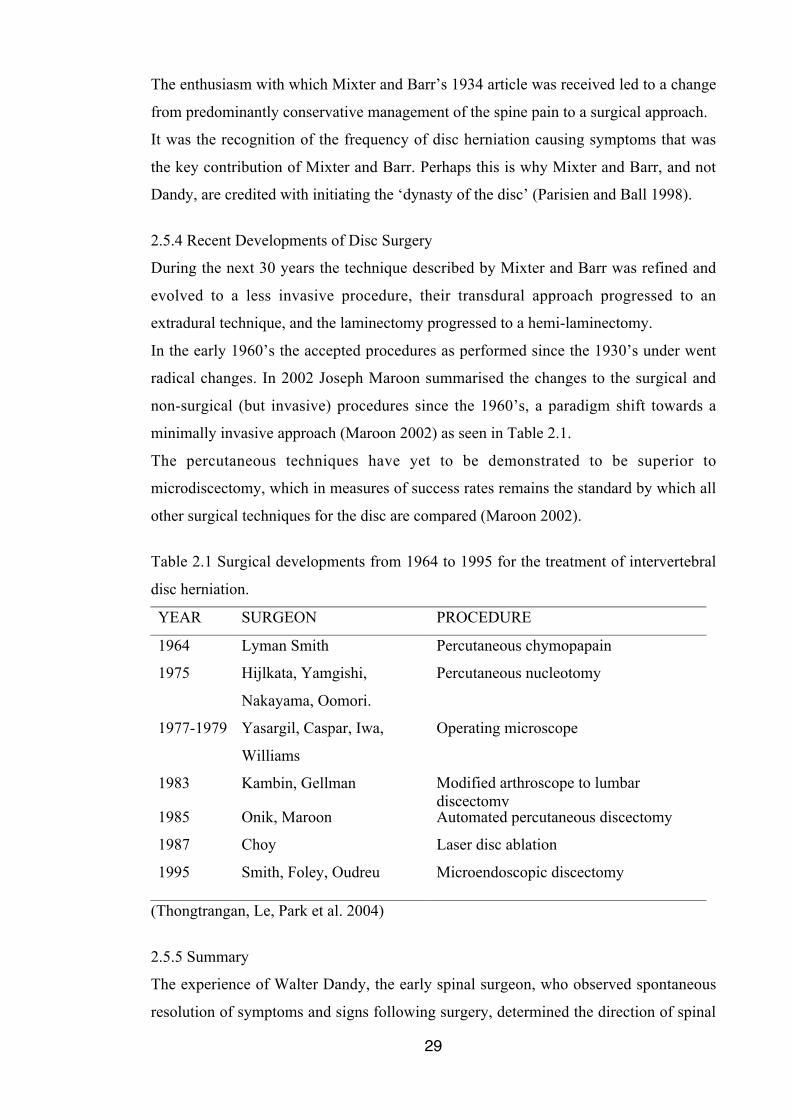
29
The enthusiasm with which Mixter and Barr’s 1934 article was received led to a change
from predominantly conservative management of the spine pain to a surgical approach.
It was the recognition of the frequency of disc herniation causing symptoms that was
the key contribution of Mixter and Barr. Perhaps this is why Mixter and Barr, and not
Dandy, are credited with initiating the ‘dynasty of the disc’ (Parisien and Ball 1998).
2.5.4 Recent Developments of Disc Surgery
During the next 30 years the technique described by Mixter and Barr was refined and
evolved to a less invasive procedure, their transdural approach progressed to an
extradural technique, and the laminectomy progressed to a hemi-laminectomy.
In the early 1960’s the accepted procedures as performed since the 1930’s under went
radical changes. In 2002 Joseph Maroon summarised the changes to the surgical and
non-surgical (but invasive) procedures since the 1960’s, a paradigm shift towards a
minimally invasive approach (Maroon 2002) as seen in Table 2.1.
The percutaneous techniques have yet to be demonstrated to be superior to
microdiscectomy, which in measures of success rates remains the standard by which all
other surgical techniques for the disc are compared (Maroon 2002).
Table 2.1 Surgical developments from 1964 to 1995 for the treatment of intervertebral
disc herniation.
YEAR SURGEON PROCEDURE
1964 Lyman Smith Percutaneous chymopapain
1975 Hijlkata, Yamgishi,
Nakayama, Oomori.
Percutaneous nucleotomy
1977-1979 Yasargil, Caspar, Iwa,
Williams
Operating microscope
1983 Kambin, Gellman Modified arthroscope to lumbardiscectomy
1985 Onik, Maroon Automated percutaneous discectomy
1987 Choy Laser disc ablation
1995 Smith, Foley, Oudreu Microendoscopic discectomy
(Thongtrangan, Le, Park et al. 2004)
2.5.5 Summary
The experience of Walter Dandy, the early spinal surgeon, who observed spontaneous
resolution of symptoms and signs following surgery, determined the direction of spinal

30
surgery, and probably post-surgical rehabilitation, for the next 50 years. As surgeons
have become more aware of ‘outcomes’ following surgery they have recognised that
there is often not the spontaneous resolution of symptoms that was readily accepted 80
years ago. They have sought improvement in the surgical techniques to achieve better
results (Maroon 2002). It is likely that their interest in rehabilitation post-surgically has
been restricted by the belief that the surgery would provide spontaneous resolution of
symptoms and signs as described by Dandy.
2.6 HISTORICAL PERSPECTIVE
PHYSIOTHERAPY
Historically physiotherapy has been directed towards the management of non-surgical
spine conditions. In the 1950s and early 1960s when acute spine care came to the
attention of physiotherapists, physiotherapy was by referral only, for the most part on
prescription (Maitland 1964). A revolution was required to move from application of
treatment modalities on prescription to assessment and treatment of complex spine
problems. In Australia, Geoffrey Maitland who established the principles of
examination and treatment, and then encouraged the influencing of medical
practitioners, guided physiotherapists through this period. The general medical
practitioners were eager to have help with management of the acute and chronic spine
patients in their practice (Maitland 1968). Consequently physiotherapy for non-surgical
spine patients developed and attracted therapists interested in research and development
of the specialty.
However the spinal surgeons who saw rapid changes with surgical decompression of
neural tissue, relieving pain and restoring function immediately in many cases, were
less interested in seeking physiotherapy assistance for the rehabilitation of their patients.
When patients failed to recover fully or experienced recurrence of symptoms, a solution
was sought with drugs or further surgery. There has been little research published that
encouraged surgeons to seek physiotherapy management to further optimise outcomes
after spinal surgery.
There has been little or no research into the effects of specific physiotherapy modalities
or techniques post-operatively. The care of the post-operative patient has been ad hoc,
with many approaches having no scientific basis and the results have been unpredictable
(McFarland 1994; McFarland and Burkhart 1999). Even those who have advocated a
31
more scientific approach (McFarland 1994; McFarland and Burkhart 1999) have failed
to use evidence to base the interventions after surgery.
While the rehabilitation of post-operative spine patients is a small portion of the total
caseload of physiotherapists, there is very little literature available to educate the
therapist interested in this area.
2.7 CURRENT THEORY
2.7.1 Introduction
The Cochrane collaboration reviewed the available studies of rehabilitation following
first time lumbar disc surgery and found13 studies worthy of review, six of which were
considered high quality (Ostelo, de Vet, Waddell et al. 2002). There was a wide variety
of exercise and time frames for initiating the protocols. Other studies have been
commenced after the Cochrane review, some of which have published preliminary data,
again looking at introducing exercise after surgery (Donaldson, Shipton, Inglis et al.
2006). None of the studies in the current literature appears to have the same starting
point as this research project which reports adapting the McKenzie approach to the
treatment of low back pain. The primary problem for the patient, which precipitates
surgery, is herniation of a lumbar disc. All other developments are sequelae to this, for
example loss of mobility, neural dysfunction, muscle weakness and loss of aerobic
conditioning. Following surgery the recovery of the disc must be the primary concern.
By introducing the treatment usually reserved for treatment of non-operable disc
disturbances it is postulated that the recovery would be improved.
2.7.2 McKenzie Approach to Treatment of Lower Back Pain
2.7.2.1 Introduction
Robin McKenzie, a physiotherapist from New Zealand, developed the McKenzie
Method of treatment for non-specific mechanical back pain using pain behaviour and its
relationship to movements and positions to determine appropriate physical treatment.
Clinical assessment permits classification of the non-specific spectrum of low back pain
into syndromes which facilitates clinical decision-making (McKenzie and May 2003).
McKenzie’s approach to the examination and treatment of non-specific low back pain
encompasses the entire category of patients, which is described in detail in the recent
publication; The Lumbar Spine Mechanical Diagnosis and Treatment (McKenzie and
May 2003). The treatment approach to one of the syndromes, defined as ’derangement’,
32
has been further developed to make it applicable to the post-operative rehabilitation
following lumbar microdiscectomy.
2.7.2.2 Centralisation
During development of his approach to treatment of low back pain, McKenzie became
aware of the phenomenon he termed ‘centralisation’ which he defines as “in response to
therapeutic loading strategies, pain is progressively abolished in distal-to-proximal
direction with each progressive abolition being retained over time until all symptoms
are abolished” (McKenzie and May 2003:167). The opposite of centralisation is
‘peripheralisation’ where the response to loading strategies progressively refers the
symptoms from more proximal to distal (McKenzie and May 2003).
McKenzie hypothesised that a ‘dynamic disc model’ was the underlying anatomical
mechanism for centralisation (McKenzie 1981; McKenzie and May 2003). In this
model and as a result of the disc’s fluid matrix, nuclear deformation could occur in
response to trunk movements or loading as long as the anular hydrostatic mechanism is
maintained.
Movements or positions which centralise symptoms are described as demonstrating
directional preference (McKenzie and May 2003; Wetzel and Donelson 2003).
2.7.2.3 Lateral Shift
In 1972 McKenzie (1972) proposed an alternative explanation and treatment for sciatic
scoliosis, a condition he called lateral shift. Data gathered over two years documenting
the treatment of 500 patients with lateral shift was presented. Of this cohort 479
deviated away from the painful side, and 473 exhibited a loss of lordosis while 27
exhibited an increased lordosis. He proposed that postero-lateral accumulation of the
nucleus pulposus in a herniating but contained intervertebral disc was the cause of the
deformity, and that prior to discal herniation there was a time when the internal
derangement of the disc was reversible.
Prior to McKenzie’s description there was a widely held belief that the ‘scoliosis’ was
secondary to pain and caused by muscle spasm (Falconer, McGeorge and Begg 1948;
Lorio, Bernstein and Simmons 1995). McKenzie’s correction of the scoliosis with
centralisation of symptoms supported his hypothesis that it was a primary deformity and
a direct result of the internal derangement (McKenzie 1972). A lateral shift is
33
characteristically gravity induced, present in weight bearing and abolished in lying
down (Porter and Miller 1986; Gillan, Ross, McLean et al. 1998). In order to
differentiate the acute sciatic scoliosis from structural scoliosis McKenzie created the
term lateral shift (McKenzie 1979).
The Scoliosis Research Society defines lateral shift as a non-structural scoliosis caused
by nerve root irritation from disc herniation or tumour (Lorio et al. 1995; McKenzie and
May 2003). However Gillan et al (1998) in a study involving subjects with lateral shift,
found that only ten of 25 had limited straight leg raise, and three reported pain below
the knee. This would seem to indicate that the neural structure is not necessarily
involved in the presence of a lateral shift, confirming the findings of Falconer et al
(1948) that neural compromise is not a requisite feature of sciatic scoliosis.
2.7.2.4 Derangement Syndrome
The most common of McKenzie’s three syndromes, ‘derangement’ is related to pain
caused by internal articular displacement resulting in mechanical deformation of pain
sensitive tissues (McKenzie and May 2003).
Disc disturbance has been described as a continuum, commencing with minor trauma to
the anular wall with initially circumferential fissures and, with continued strain, radial
fissures (Vanharanta, Sachs and Spivey 1987; McKenzie and May 2003). Minor disc
disturbances may produce little or no symptom or apparent loss of function, but with
recurrent episodes the severity of the disc damage increases, as do the symptoms and
limitations (Moneta, Videman, Kaivanto et al. 1994; McKenzie and May 2003).
Derangement symptoms demonstrate directional preference, that is they worsen in
response to movements or positions which increase loading or distortion of pain
sensitive structures, and improve with opposite loading strategies (McKenzie and May
2003).
The patient with derangement often exhibits acute spinal deformity, a reduced, kyphotic
or accentuated lumbar lordosis, or a lateral shift.
On examination of movement, patients within this category always demonstrate loss of
movement and function. Certain movements produce, increase or peripheralise the
symptoms and repetition of these movements will worsen the condition. Other
movements may decrease, abolish or centralise symptoms and repeating the movements
34
may improve the condition. In the Derangement Syndrome sustaining certain positions
will exacerbate, while other sustained positions may decrease or abolish symptoms.
Lumbar derangements may occur at any age from teens to old age but are most
frequently seen in the 20 to 55 age group.
During the 1960’s and 1970’s as McKenzie was developing his system of examination
and treatment there was limited understanding of the behaviour of the intervertebral
disc. Clinically he observed the effects of repeated and sustained positions, and
determined that the disc played a great role as the cause of back pain (McKenzie 1981;
McKenzie and May 2003). He cited the work of Nachemson (1960), Matthews (1976)
and Vernon-Roberts (1976) to explain the phenomena he had observed clinically. He
speculated that as long as the hydrostatic mechanism of the intervertebral disc was
intact movement of the spinal column could be utilised to reverse internal derangement.
Hyodo et al (2005) in a study in which patients with non-specific low back pain under-
went intradiscal injection to the disc with an obvious enhanced region on MRI,
concluded the disc was indeed able to be responsible for non-specific low back pain.
Since the mid 1980’s research has supported the theory that movement of the spinal
column influences position of the nucleus pulposus (Krag et al. 1987; Fennell et al.
1996; Edmondston et al. 2000; Fazey, Song, Monsas et al. 2006). Posterior deformation
of the nuclear content in response to anterior disc loading with flexion has been
demonstrated (Shah et al. 1978; Krag et al. 1987; Fennell et al. 1996; Edmondston et al.
2000) as has anterior deformation in response to extension (Wetzel and Donelson 2003).
From the embryonic stage of disc disturbance to disc herniation, the derangement can
be followed through the patient’s signs and symptoms. Once recognised as a continuum,
appropriate intervention can restrict the progression.
2.7.2.5 Treatment of Derangement
The treatment of derangement has four stages:
1. Reduction of derangement
2. Maintenance of reduction
3. Recovery of function
4. Prevention of recurrence
35
2.7.2.5(1) Reduction of the Derangement
Reduction of the derangement will be determined by directional preference which is
established by examination, either flexion, extension or lateral. On a regular basis, the
patient must perform self-management exercise until the symptoms are abolished and
function is restored (McKenzie 1981; McKenzie and May 2003).
2.7.2.5(2) Maintenance of the Reduction
Once the derangement is reduced, the patient must avoid aggravating postures and
positions which may cause recurrence of symptoms.
In the case of a posterior derangement where the posterior or postero-lateral anular wall
has been disturbed, flexion, especially when it is sustained or repeated, is an
aggravating factor. Sitting is considered a sustained flexion posture. In order to maintain
lumbar lordosis and avoid flexed sitting postures a lumbar roll support and correct
seating is advised. Prevention of postural stresses and posterior creep is essential to
maintain the reduction of the posterior derangement. Adams and Dolan (1996) found
that sitting resulted in marked lumbar flexion which was greatly affected by the chair
shape.
Andersson et al (1979) found in their study of backrest inclination, that the lumbar
lordosis reduced into flexion when a subject sat from a standing position. Changes in
the backrest inclination had some effect, but a lumbar support provided significant
influence. In a previous study, Andersson et al (1975) found that placement of the
lumbar support in the lordosis reduced disc pressure more than at other locations in the
lumbar spine and reduced lumbar disc pressure more than either supported sitting
without specific lumbar support or unsupported sitting.
It is recommended that sitting is frequently interrupted and that repeated flexion is
avoided. Adams and Dolan, (1996) reported other sustained flexion postures, notably
gardening, result in creep leaving the intervertebral disc vulnerable to herniation.
The exercise, which reduced the derangement, should be continued on a regular basis
(McKenzie 1981; McKenzie and May 2003).
In the case of an anterior derangement where the anterior anular wall has been
disturbed, extension is an aggravating factor. Postures and positions which sustain or
repeat extension should be avoided, as in standing or walking (McKenzie and May
2003).
36
2.7.2.5(3) Recovery of Function
While maintaining the reduction of the derangement the patient has avoided certain
positions and movements which must be recovered to prevent adaptive shortening
occurring. All movements, including lateral glide, must be recovered fully, leaving the
patient confident to move and perform all usual activities (McKenzie and May 2003).
Following a posterior derangement, flexion must be restored once the derangement is
stable. Repeating flexion should not affect the ability to extend (McKenzie and May
2003). Following an anterior derangement there is rarely demonstrable loss of function
(McKenzie and May 2003).
2.7.2.5(4) Prevention of Recurrence
During the treatment period the patient is educated as to postural habit, awareness of
sustained postures, and exercise for reduction of derangement should there be
recurrence (McKenzie and May 2003).
McKenzie recommends the lifetime use of a lumbar roll (McKenzie and May 2003). In
a study involving subjects with chronic low back pain, O’Sullivan et al found that there
was a lack of proprioception resulting in the inability to sit in the neutral lordotic
posture (O'Sullivan, Burnett, Floyd et al. 2003; Dankaerts, O'Sullivan, Burnett et al.
2006). The continuum of development of derangement could result in this cohort
lacking in proprioception thereby requiring a lumbar roll to enable sitting in neutral on a
permanent basis.
In order to recover full mobility and confidence with usual activities McKenzie
recommends continuing with the exercise programme for six weeks, and in order to
prevent recurrence of posterior derangement regular performance of extension in lying
is encouraged (McKenzie and May 2003). Larsen et al (2002) in a prospective
randomised controlled study using passive extension in lying performed on a regular
basis to prevent onset of low back pain, concluded that in fact it did reduce the
prevalence rate of back problems. Lonn et al (1999) found that education and specific
exercise reduced frequency and severity of recurrence.
Vulnerability of the posterior disc wall occurs in sustained flexion postures (Adams and
Dolan 1996). McKenzie does not recommend avoidance of these postures but rather an
awareness of their effect with a recommendation to interrupt these positions frequently
(McKenzie 1979; McKenzie 1981; McKenzie and May 2003).
37
2.7.2.6 Summary
Robin McKenzie developed an approach to examination and treatment of non-specific
low back pain. He described the development of disturbance within the disc as a
continuum commencing with minor disruption which caused minor symptoms to major
disc derangement which could result in severe symptoms.
2.7.3 Other Studies
In the 13 studies reviewed by the Cochrane collaboration there were no studies of good
quality which included rehabilitation commencing immediately post-operatively (Ostelo
et al. 2002). In most studies the rehabilitation protocol began at least four weeks after
surgery (Manniche et al. 1993; Brennan et al. 1994; Kjellby-Wendt and Styf 1998;
Kjellby-Wendt and Styf 2002). Most protocols demanded an extended period of
involvement. In 1998 Kjelby-Wendt and Styf’s prospective, randomised and controlled
study, the group receiving an early active training (EAT) programme commenced
posture correction and were instructed in the maintenance of the lumbar lordosis with a
lumbar support the day following surgery. The second more intensive part of training
commenced six weeks after surgery and continued for 12 weeks. While some of the
instructions used in the Kjellby-Wendt and Styf’s EAT programme are similar to those
used in this early rehabilitation protocol, it did not have its basis in the McKenzie
approach to the treatment of derangement, rather it appears to have used selected
material from the approach (Kjellby-Wendt and Styf 1998; Kjellby-Wendt and Styf
2002).
A study by Filiz at el (2005) compared two different exercise programmes and a control
group following single level lumbar microdiscectomy. While the intensive exercise
programmes proved more effective than the control group, cost effectiveness was
questioned. Filiz et al commenced their study one month after surgery and involved
education and intensive exercise over eight weeks, with one group in continuous contact
with a physician.
One of the criteria shown by the Cochrane review to improve functional outcome post-
operatively was an intensive exercise programme (Ostelo et al. 2002). Donaldson et al
(2006) evaluated the effect of a formal gym-based exercise programme compared with
the usual rehabilitative advice given by a spinal surgeon, and planned a three-year
follow-up. After one year there was no statistical advantage gained by the exercise
cohort.
38
According to the Cochrane collaboration there was no evidence to recommend
commencing rehabilitation immediately following lumbar disc surgery because of the
lack of good quality studies.
2.7.4 Summary
The theory, which has lead to the development of the study protocol, has been reviewed.
Also discussed are the other protocols which have recently been applied to address
rehabilitation after lumbar disc surgery.
2.8 DEVELOPMENT OF THE REHABILITATION PROTOCOL
2.8.1 Introduction
The protocol under review was developed using the principles of the McKenzie Method
for treatment of derangement with or without referral of symptoms, and applying them
to the rehabilitation of patients following lumbar microdiscectomy.
The principles of effective management of derangement involve a mixture of education
and mechanical therapy.
Recovery of function has been expanded from McKenzie’s classic approach to
derangement to include core trunk stabilisation, neural mobilisation and aerobic
conditioning.
2.8.2 Reduction of Derangement
Once the hydrostatic mechanism of the intervertebral disc is no longer intact, the
derangement becomes irreducible with movement or position of the lumbar spine i.e. no
position or movement will abolish, reduce or centralise symptoms and maintain the
reduction of the derangement (McKenzie and May 2003).
While it is possible to have either an irreducible anterior or posterior derangement, it is
the irreducible posterior derangement which may proceed to surgery. The irreducible
anterior derangement would not meet the criteria for surgery, as it is incapable of
producing the signs and symptoms required. Lumbar disc surgery is performed at the
discretion of the surgeon following evaluation which may include CT or MRI. The
decision to operate is based on the patient’s presenting signs and symptoms and failure
to respond to conservative management. Criteria for surgery are unremitting radicular
pain with or without back pain, neurological deficit correlating to findings on CT or
MRI, cauda equina symptoms, and failure to respond to conservative management
(Asch et al. 2002).

39
The rehabilitation process after lumbar microdiscectomy is able to be tissue specific, as
the cause of the patient’s previous symptoms is known. Directional preference, that is
extension principle, is established by the surgical intervention with the disc herniation
occurring posterior or postero-lateral.
2.8.3 Maintenance of Reduction
Following the principles of McKenzie (McKenzie and May 2003) for the treatment of a
posterior derangement, the patient was encouraged to maintain lumbar lordosis at all
times using a lumbar roll in sitting, and all flexion activities were discouraged.
The lordotic posture of the lumbar spine allows transfer of forces through the
zygapophyseal joints and intervertebral discs (Twomey, Taylor and Oliver 1988).
Allowing the lumbar spine to flex during sitting permits the weight of the upper body to
bring about creep, according to Twomey et al, “ a progressive deformation of a structure
under constant load” (Twomey et al. 1988:130). In a healthy structure creep is not
considered to generate force sufficient to cause structural damage, but when the load is
on a structure under repair, as post-operatively, the creep force may be responsible for
further damage, failure to repair or poor quality healing (Twomey et al. 1988). After
sustained loading in vivo, recovery of lumbar lordosis is slow, with one hour of
sustained loading requiring many hours at rest to recover (Twomey et al. 1988).
Flexion has been acknowledged as the single greatest cause of disc disturbance and
without flexion, no amount of compression or torsion can damage the lumbar discs
before the vertebrae (Adams et al. 2002). In vivo, hyperflexion injuries are the exclusive
cause of disc extrusions and in vitro studies have shown bending and lifting constitute
the highest known risk factor for acute disc prolapse (Brinckmann 1986). In the healthy
spine flexion is not dangerous, but discal injury is more likely to occur as the result of
flexion than other single physiological movement. Not only was flexion discouraged to
maintain the surgical reduction of the disc herniation but also passive extension exercise
was instituted to reduce posterior disc loading.
2.8.4 Recovery of Function
Recovery of function includes restoration of neural mobility, core trunk stabilisation,
recovery of postural awareness, aerobic conditioning and recovery of flexion and
normal spine activities including bending and lifting.
40
2.8.4.1 Neural Mobilisation
One of the clinical signs which leads to the decision to operate is loss of neural mobility
as indicated by a reduction in (or a positive) Straight Leg Raise (SLR) or Prone Knee
Bend (PKB). This loss of mobility may result in scarring or adhesion even before
surgery. At the time of surgery the nerve root(s) may need to be elevated or mobilised,
which may result in neural irritation. The surgery site involves fibrotic tissue healing the
wound through to the level of the disc, with peridural scar replacing the normal epidural
fat (Ross, Robertson, Frederickson et al. 1996). As scar tissue is not selective it will
adhere to any structure in its pathway, including the nerve roots and the spinal cord or
theca.
As discussed previously (2.2.7), Kuslich et al (1991) provided the results of surgery on
minimally sedated patients. They found that there was fibrosis around the neural
structure in all patients who had previously under-gone laminectomy. While the scar
tissue itself was not painful, the nerve root was frequently symptomatic. The presence
of the scar tissue immobilised the nerve root increasing the likelihood of compression or
tension (Kuslich et al. 1991).
Epidural fibrosis is considered to be a major cause of recurrence of symptoms following
microdiscectomy (Ross et al. 1996; Skaf, Bouclaous C., Alaraj A. et al. 2005). Skaf, in a
prospective study of 50 patients under-going repeat lumbar surgery for recurrent
symptoms, found that fibrosis or adhesion in the region of the nerve root was
responsible for symptoms in 34% of the cohort (Skaf et al. 2005).
Mobilisation of the nerve roots from the day after surgery should limit adhesion forming
between the scar and the nerve roots, reducing the risk of tethering or compression of
the neural structure (Butler 1991). The appropriate duration of the neural mobilisation
remains questionable. Ross et al (1996) considered that scar would not be visible on
MRI at one month and they repeated studies at six months to examine the state of
peridiscal scarring. They indicated that fibrosis would have stabilised by that time-point
with no change seen later (12 months).
The causes of Failed Back Surgery Syndrome identified by Burton et al (1981) were
primarily lateral or central spinal stenosis, adhesive arachnoiditis (epidural fibrosis), or
recurrent disc herniation.
41
2.8.4.2 Stabilisation
“A fundamental tenet is that lost mechanical integrity in any load bearing tissue will
result in stiffness losses and an increased risk of unstable behaviour” (McGill, Grenier,
Kavcic et al. 2003:353).
Skaf et al discussed lumbar instability as a cause of recurrent symptoms. 28% of their
cohort of 50 patients undergoing repeat surgery for recurrent symptoms demonstrated
listhesis or abnormal movement on flexion/extension films (Skaf et al. 2005). Rates of
instability increased with an increase in the number of repeat surgeries, from 12% in the
first revision to 50% in the fourth revision.
A retrospective study by Kotilainen (1998) of a cohort of 190 disclosed 39 subjects with
spinal instability which had developed following lumbar microdiscectomy. The
investigator concluded there was a direct correlation between clinical instability and a
poor post-operative recovery. He drew comparisons between the success rates in
microdiscectomy in general in completely resolving pain, 36% to 54% in different
studies, and in those with instability, 10% after five years. However there was no
specified post-operative rehabilitation in this cohort, and the only conservative
treatment options given to those who were symptomatic were analgesics and wearing of
lumbo-sacral corsets.
2.8.4.3 Postural Awareness (Proprioception)
Proprioception, the ability to sense joint position and movement, originates from the
muscle spindles, Golgi tendon organs, joint receptors and cutaneous receptors
(Leinonen, Kankaanpaa, Luukkonen et al. 2003). Multifidus muscle has been shown to
atrophy and become denervated in the presence of lumbar disc herniation (Rantanen et
al. 1993) which may affect muscle receptors and spinal proprioception.
Proprioception is impaired in the presence of joint disease (Swinkels and Dolan 1998).
Gill and Callaghan (1998) found that there were differences in proprioceptive ability in
cohorts with and without back pain, findings which were confirmed by Brugmagne
(2000). Leinonen et al (2003) found that there were similar differences present in a
cohort after lumbar disc surgery. They found that with a short course of rehabilitation
after surgery that lumbar proprioception and paraspinal reflexes recovered but postural
control did not and further that those with poor outcome demonstrated greater loss of
postural control (Leinonen et al. 2003). The use of a lumbar roll support may assist in
re-educating the postural control.
42
2.8.4.4 Aerobic Conditioning
Due to limitations in the ability to exercise following disc herniation and sciatica, it is
anticipated the subject will experience reduction in aerobic conditioning (Brennan,
Shultz, Hood et al. 1994; Hides, Richardson and Jull 1996; McGregor, Burton and Sell
2007). Loss of fitness may also effect the perception of symptoms with a decrease in
pain tolerance and an increase in depression (Anshel and Russell 1994). There is a
positive relationship between low back pain and physical fitness, with fit people
experiencing less low back pain (Casazza, Young and Herring 1998).
Commencing an aerobic walking programme three weeks after surgery is considered an
appropriate inclusion in the rehabilitation process (Casazza et al. 1998).
2.8.4.5 Recovery of Flexion
Following a period of avoiding flexion as the posterior disc wall recovers from the
surgical intervention, restoration of flexion provides load to the scar tissue establishing
lines of force to strengthen (Jarvinen, Jarvinen, Kaariainen et al. 2007); it provides
stretch to soft tissue to prevent adaptive shortening (McKenzie and May 2003); and
limits fear avoidance behaviour (Waddell, Newton, Somerville et al. 1993; Main and
Spanswick 2000; McKenzie and May 2003; Cleland, Fritz and G. 2008).
In a study involving a cohort of low back pain sufferers recovering without medical
intervention, Thomas and France (2008) found that lumbar flexion was inversely related
to fear. Individuals who perceived potential pain in flexion, failed to recover flexion. It
was determined that fear avoidance behaviour was a strong predictor of future disability
and chronic symptoms (Thomas and France 2008).
Disc nutrition creates changes in height and volume of the structure over a 24 hour
period, reported as diurnal disc change (Eklund and Corlett 1984; Tyrell et al. 1985;
Krag et al. 1987; Broberg 1993; Hutton et al. 2003). A majority of the height loss that
occurs daily is in the first four hours of the day (Tyrell et al. 1985) while an increase in
volume of 10.6% or 0.9cm3 occurs during the overnight rest period (Malko et al. 2002)
(Figure 2.10). There is greater pressure within the disc on rising in the morning and
flexion exercise is best avoided during the first four hours of the day in the recovery
period (McKenzie and May 2003).
Without recovery of flexion after microdiscectomy, the patient may develop shortening
of soft tissues pre-disposing them to future recurrence of symptoms (McKenzie and
May 2003).
43
2.8.5 Prevention of Recurrence
Following lumbar microdiscectomy the prevention of recurrence was as McKenzie
described for prevention of recurrence of derangement where the patient was educated
as to postural habit, awareness of sustained postures, and exercise for reduction of
derangement should there be recurrence (McKenzie and May 2003). The education
process was continuous, occurring during the rehabilitation process reinforcing the steps
undertaken during surgery and rehabilitation: reduction of derangement, maintenance of
reduction, recovery of function and prevention of recurrence.
Patients were encouraged to recover full mobility and confidence with usual activities.
It was recommended that the exercise protocol was continued for at least six weeks, and
in order to prevent recurrence of posterior derangement regular performance of
extension in lying was encouraged for the long term (McKenzie and May 2003).
Interruption of sustained postures was encouraged to reduce vulnerability of the
posterior disc wall which occurred in sustained flexion postures, as in sitting (Adams
and Dolan 1996; McKenzie and May 2003).
Patients were encouraged to persist with the use of a lumbar roll to maintain support of
the lumbar lordosis. In the post-operative group, the ability to maintain a neutral lumbar
lordosis may be compromised with loss of proprioception and an inability to sit in the
neutral lordotic posture (O'Sullivan et al. 2003; Dankaerts et al. 2006).
2.8.6 Summary
Using the principles of the McKenzie Method for treatment of derangement a protocol
was developed and applied to the rehabilitation of patients following lumbar
microdiscectomy. The post-operative protocol incorporated core trunk stabilisation,
neural mobilisation and aerobic conditioning together with McKenzie’s classic
approach to the treatment of derangement using education and mechanical therapy.
2.9 CURRENT STANDARD REHABILITATION FOLLOWING LUMBAR
MICRODISCECTOMY
2.9.1 Introduction
Ostelo et al (2002) reviewed published trials on all active rehabilitation programs after
first time lumbar disc surgery. The protocols they reviewed were investigations of a
variety of approaches to post-operative rehabilitation and not necessarily the treatment
44
seen in current management of the post-operative patient. In practice, the surgeon often
dictates rehabilitation after lumbar spine surgery, but those providing the service must
develop a protocol which is appropriate and able to achieve the desired goals with
contingencies for complications. Surgery and rehabilitation co-exist but the two should
be looked on as complementary, not exclusive, with the surgeon and therapist
contributing appropriately.
2.9.2 Standard Rehabilitation
A review of protocols used for both inpatient and outpatient management of patients
after lumbar disc surgery revealed a wide variety of clinical practice (Williamson,
White and Rushton 2007). Post-operatively patients were provided exercise for general
mobility including stair walking, spinal range of movement, stability exercise, neural
mobility exercise and advice and education. Williamson et al (2007) reported a wide
range of exercise including knee/hip flexion, pelvic tilting, muscle stabilisation (mostly
for transversus abdominis), sit-ups and gluteal exercise. There did not appear to be
consensus on the type of exercise nor the timing for addition of each activity.
Similarly McGregor et al found that “post-operative management after lumbar surgery
is inconsistent leading to uncertainty amongst surgeons and patients about post-
operative restrictions, reactivation, and return to work” (McGregor et al. 2007:339).
Examples of post-operative care provide often very detailed exercise and changes for
almost every aspect of the patient’s daily activities (Maxey and Magnusson 2007).
Maxey and Magnusson (2007) discuss the importance of maintenance of lumbar
lordosis in prevention of recurrence of herniation but the exercises provided in their
guidelines do not always support this notion, for example pelvic tilting, lying prone with
a pillow under the stomach which places the lumbar spine in flexion and partial sit-ups.
Guidelines reviewed in assessing standard rehabilitation provide not only a variety of
exercise but also recommendations for therapist techniques for mobilisation of thoracic
spine and hip joints, and modalities (ice, heat, electrical stimulation) (McFarland 1994;
McFarland and Burkhart 1999; Maxey and Magnusson 2007; Spencer 2007).
2.9.3 Summary
Current standard rehabilitation following lumbar microdiscectomy includes a wide
range of advice, exercise, technique and modalities.
45
2.10 OUTCOME INSTRUMENTS
2.10.1 Introduction
During the course of the research involved in this study, two different sets of outcome
instruments were used. The first phase utilised two outcome measures: the Oswestry
Disability Index [Appendix 2] and an Outcome Questionnaire [Appendix 3], while the
second phase included three outcome measures: the Roland Morris Questionnaire
[Appendix 4], Visual Analogue Scale [Appendix 5] and a Questionnaire [Appendix 6].
Their validity, reliability and responsiveness are reviewed.
2.10.2 Oswestry Disability Index (ODI)
Developed in 1976 to help determine the interruption which low back pain caused to
activities of daily living, the ODI concentrated on scoring ten aspects of the patients’
activities and perceived pain. Each category comprised a score from 0 to 5, the higher
the score the greater the disability.
The ODI has been accepted as a valid indicator of disability with excellent test-retest
reliability (Fairbank, Couper, Davies et al. 1980; Fairbank and Pynsent 2000; Roland
and Fairbank 2000). It has been accepted as a sensitive measure to clinical change over
time in patients complaining of low back pain (Beurskens, de Vet, K'ke et al. 1995). It
has also been found to have a high test-retest correlation comparing a hard copy to a
computer version (Fairbank and Pynsent 2000).
Following surgery the scores have been found to vary but the percentage change is a
reliable marker of outcome (Little and MacDonald 1994).
For patients under-going spinal fusion, the U.S. Food and Drug Administration has
recommended a minimum reduction of 15 points between the pre-surgical and follow-
up data collection as measure of successful outcome (Fairbank and Pynsent 2000).
2.10.3 Roland Morris Questionnaire (RMQ)
From the 136-item Sickness Impact Profile (SIP), the authors of the RMQ selected 24
activities likely to be affected by low back pain (Roland and Fairbank 2000). Statements
were identified that provide information on a wide range of daily activities (Roland and
Morris 1983). A score of one point is given to every statement checked on the
questionnaire, with a possible low score of zero (no disability) and a high score of 24
(maximum disability) (Roland and Morris 1983). Roland and Morris (1983) concluded
that a score of 14 or more four weeks after presentation constituted a ‘poor outcome’.

46
A score change between four to five is required between two points of time to be
confident that meaningful change has occurred (Stratford, Binkley and Solomon 1994).
Stratford et al (1994) found fewer incomplete responses with the RMQ than with the
ODI. It is recommended in populations where the outcome is anticipated to be in the
lower level of disability (Bombardier 2000) and it has been suggested that the RMQ is
the preferred measure for post lumbar surgery patients (Ostelo, de Vet, Knol et al.
2004).
Beurskens et al (1995) reported that the RMQ was sensitive to clinical change over time
for low back pain patients.
2.10.4 Selection of Outcome Instrument
Outcome measures should be reliable, valid, responsive, applicable, practical and
comprehensive (Bouter, van Tulder and Koes 1998). Both the ODI and the RMQ meet
these criteria. Both have been found to measure the functional status, both have similar
test-retest reliability and are useful in the primary care setting, but where the anticipated
level of disability is low, the RMQ may prove superior (Deyo, Battie, Beurskens et al.
1998). In a review of the RMQ and the ODI by Roland and Fairbank (2000) it was
perceived that the RMQ may discriminate when the ODI scores were low, making it
more useful when rapid recovery is anticipated.
The ODI tends to score higher than the RMQ making it more useful in evaluation of
seriously disabled patients (Fairbank and Pynsent 2000).
Asch et al (2002) trialled questionnaires one day post-operatively and deleted them
from the data when, after 140 patients, they found the score was consistently near zero.
They found the ten-day review gave a realistic indication of the patient’s status.
2.10.5 Visual Analogue Scale
The Visual Analogue Scale is a linear measurement of perceived pain which uses a 10
cm long line, with ends labelled at the extremes of pain (eg. ‘no pain’ to ‘pain as severe
as possible’). The VAS is considered a highly responsive measure of pain (Von Korff,
Jensen and Karoly 2000). The minimal clinically important difference for the VAS of
back pain is between 12% and 20% (Kelly 2001; Hagg, Fritzell and Nordwall 2003;
Haefeli and Elfering 2006; Copay, Glassman, Subach et al. 2008) and the minimal
clinically important difference for the VAS of leg pain is reported as 1.6 on a 10 point
scale (Copay et al. 2008).
47
2.10.6 Outcome Questionnaire Prospective Study (Phase Two)
According to recommendations from Deyo et al (1998) a core set of measures to assess
outcome includes: back specific function, generic health status, pain, work disability
and patient satisfaction.
Generic health status, work disability and patient satisfaction were assessed with a
specific questionnaire using questions validated elsewhere (Deyo et al. 1998). Items
included in this questionnaire have been validated previously in the Sickness Impact
File (SIF), SF-36 and Modified Core Network Low Back Pain Medical Screening
Questionnaire (CORE) (Deyo et al. 1998). The patient questionnaire was developed for
the thesis study and considered the severity of symptoms, the functional status and
satisfaction with care.
The functional status was reflected in the time taken to return to the work place or to
usual duties (as the case might be).
Satisfaction with care, while not a health issue, was of concern in being aware of the
patient’s perception of the level and quality of care.
2.10.7 Outcome Questionnaire Retrospective Study (Phase One)
The outcome questionnaire for the retrospective study was developed using questions
validated elsewhere (Deyo et al. 1998). It did not include the core set of measures as
recommended by Deyo (1998) and therefore did not provide a complete assessment of
the patient’s status. Questions regarding medication use, work ability and psychological
impairment were omitted.
2.10.8 Summary
The outcome instruments used in the research into outcomes of early rehabilitation
following lumbar microdiscectomy have been reviewed.
2.11 SUMMARY
This thesis examines outcomes following lumbar microdiscectomy. The background
information has included a review of lumbar anatomy including the intervertebral disc,
ligaments intimately connected to the disc and musculature directly involved with both
the movement of the intervertebral segment and stability of the lumbar spine. The
importance of normal physiology including blood supply and nutrition of the
48
intervertebral disc: and mechanics of the intervertebral disc and its role in providing
mobility to an otherwise rigid lumbar spine is emphasised.
The outcome instruments used in this area of clinical research have been reviewed.
The histories of lumbar disc surgery and rehabilitation protocols were reviewed with
developments traced to the late twentieth century, with specific emphasis on the
development of the protocol under examination in this study.
It is clear that a careful examination of clinical outcomes after lumbar intervertebral disc
surgery is warranted to consider the merit of instituting an early exercise regime. A
contrast with standard rehabilitation physiotherapy would provide an opportunity to
consider different approaches used by the physiotherapy community in this post-
operative patient group.
49
CHAPTER 3
MATERIAL AND METHOD
3.1 INTRODUCTION
An original Rehabilitation Protocol for patients after lumbar microdiscectomy was
developed using the McKenzie Approach for the treatment of lower back pain as its
basis (McKenzie and May 2003). In order to assess the effectiveness of this protocol, a
retrospective study (Phase One), was carried out with a cohort of post-operative patients
between February 2000 and December 2002. The outcome of the surgery followed by
the rehabilitation protocol was assessed using validated outcome measures. A contrast
or control group was not included.
After reviewing the data collected, there were limitations with the design and
implementation of the study. A prospective study (Phase Two) was proposed to address
these issues. Changes were made in the principal outcome measure used, in the
demographic data to be retrieved via the questionnaires, in the addition of pain scores,
and in the exclusion of compensable patients. A contrast group was included for the
prospective study.
The purpose of the prospective study was to assess the outcomes of the rehabilitation
model in lumbar microdiscectomy patients, determining if there was any difference in
those who followed a specific post-surgical protocol and those who followed standard
rehabilitation at another location. This research was approved by the Research Ethics
Committee at the University of Western Australia. [Appendix 1.]
The retrospective study was reviewed to critically evaluate the data retrieved and to
inform the prospective study.
3.2 STUDY DESIGN
Consecutive patients were referred from two neurosurgeons, one to rehabilitation using
the study protocol, the other, operating at a distant site, to their local physiotherapy
providers.
In participating practices the surgeon identified appropriate patients who, if interested,
were enrolled into the study by practice staff.
50
Patients were provided with the Patient Information Sheet [Appendix 7], Patient
Consent [Appendix 8] and questionnaires [Appendices 4, 5 and 6], with the request for
forms to be completed before surgery (Entry questionnaires).
Patients within the study group (WA) commenced rehabilitation the day following
surgery, while the control group (QLD) were referred to local physiotherapists once
they had left the hospital according to protocols in use at that centre.
The WA cohort completed outcome questionnaires at their first office visit ten days post
surgery (Post-op), at completion of the rehabilitation protocol approximately four weeks
post-surgery (Exit), and at six and 12 months. The QLD cohort completed outcome
questionnaires at six weeks post-surgery on their review with the neurosurgeon (Exit)
and at six and 12 months.
3.3 DEVELOPMENT OF REHABILITATION PROTOCOL
3.3.1 Introduction
The rehabilitation protocol was developed with the understanding that with the
reduction of a posterior derangement pressure on the posterior anular wall is lessened
(McKenzie and May 2003). When a disc herniation becomes accomplished, that is fully
protruded, no movement or position will reduce symptoms or signs. Very often spinal
extension becomes difficult and painful. Surgical removal of the protrusion or fragment
of disc at microdiscectomy enables movement into extension to be recovered. It was
theorised that primary intention healing could occur more readily with the posterior disc
wall in neutral to extension, reducing the risk of reherniation and poor outcome
associated with on-going symptoms, the result of secondary intention healing.
In the McKenzie Approach, the principles of effective management of derangement
involve a mixture of education and mechanical therapy. This methodology is described
in detail elsewhere (McKenzie and May 2003).
The treatment of derangement has four stages: reduction of the derangement;
maintenance of the reduction; recovery of function; and prevention of recurrence.
As the derangement has been surgically reduced, the post surgical rehabilitation process
has been decreased to three stages: maintenance of the reduction; recovery of function;
and prevention of recurrence.
51
3.3.2 Maintenance of the Reduction
Treatment commenced the day following surgery. The patient was introduced to the
concept of maintenance of the lumbar lordosis and prevention of flexion. Detailed
instruction was given in correction of posture in lying, sitting and standing; and the use
of a lumbar roll to maintain lumbar lordosis in sitting (Figure 3.1). The use of a backrest
has been shown to reduce flexion in sitting and a lumbar support has even greater effect
on maintenance of lumbar lordosis (Andersson et al. 1975).
The patient commenced prone lying (Figure 3.3), prone on elbows (Figure 3.4) and
extension in lying (Figure 3.5) with this cycle of exercise to be completed two hourly,
during waking hours, for the next ten days. As exercises were tailored to each patient,
the number of repetitions was at the discretion of the treating therapist.
Prior to lying prone two hourly the patient was encouraged to walk for ten minutes at a
steady pace over level terrain.
Neural mobility exercise (Figures 3.2, 3.8) was introduced with exercise to be
completed four times daily.
The patient was discharged from hospital following the therapist’s visit with instruction
to comply with the exercise and posture as instructed, to avoid bending, lifting or
twisting, to continue with prescribed medication and to arrange an office visit in ten
days.
On day ten the patient was reviewed with subjective examination, peripheral
neurological examination and review of exercise as it had been performed during the
interim period. Completion of outcome questionnaires provided an insight into
compliance: limitations of function indicated by RMQ score, VAS scores, medication
use and ability to perform exercise regularly should demonstrate a relationship to one
another. Further questioning might be necessary to establish if particular difficulties had
been encountered. Familiarity with exercise and ease of movement indicated
understanding of principles and compliance with the protocol. Compliance was not
measured other than in questioning the patient. Once assessment commenced patients
readily reveal details of ability to follow all instructions.
Posture correction in sitting and correct use of the lumbar roll was observed.
Peripheral neurological examination included manual muscle testing of myotome
strength, neural mobility with either straight leg raise or prone knee bend, response of
relevant reflexes, and sensory testing.
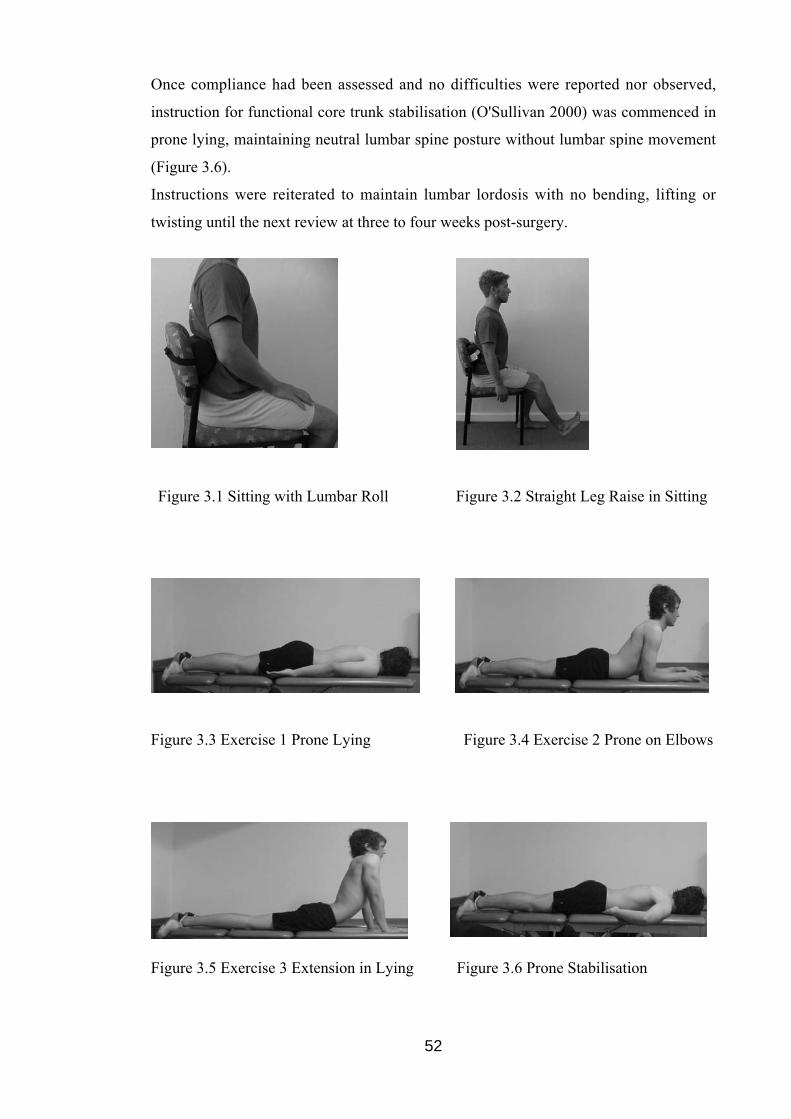
52
Once compliance had been assessed and no difficulties were reported nor observed,
instruction for functional core trunk stabilisation (O'Sullivan 2000) was commenced in
prone lying, maintaining neutral lumbar spine posture without lumbar spine movement
(Figure 3.6).
Instructions were reiterated to maintain lumbar lordosis with no bending, lifting or
twisting until the next review at three to four weeks post-surgery.
Figure 3.1 Sitting with Lumbar Roll Figure 3.2 Straight Leg Raise in Sitting
Figure 3.3 Exercise 1 Prone Lying Figure 3.4 Exercise 2 Prone on Elbows
Figure 3.5 Exercise 3 Extension in Lying Figure 3.6 Prone Stabilisation
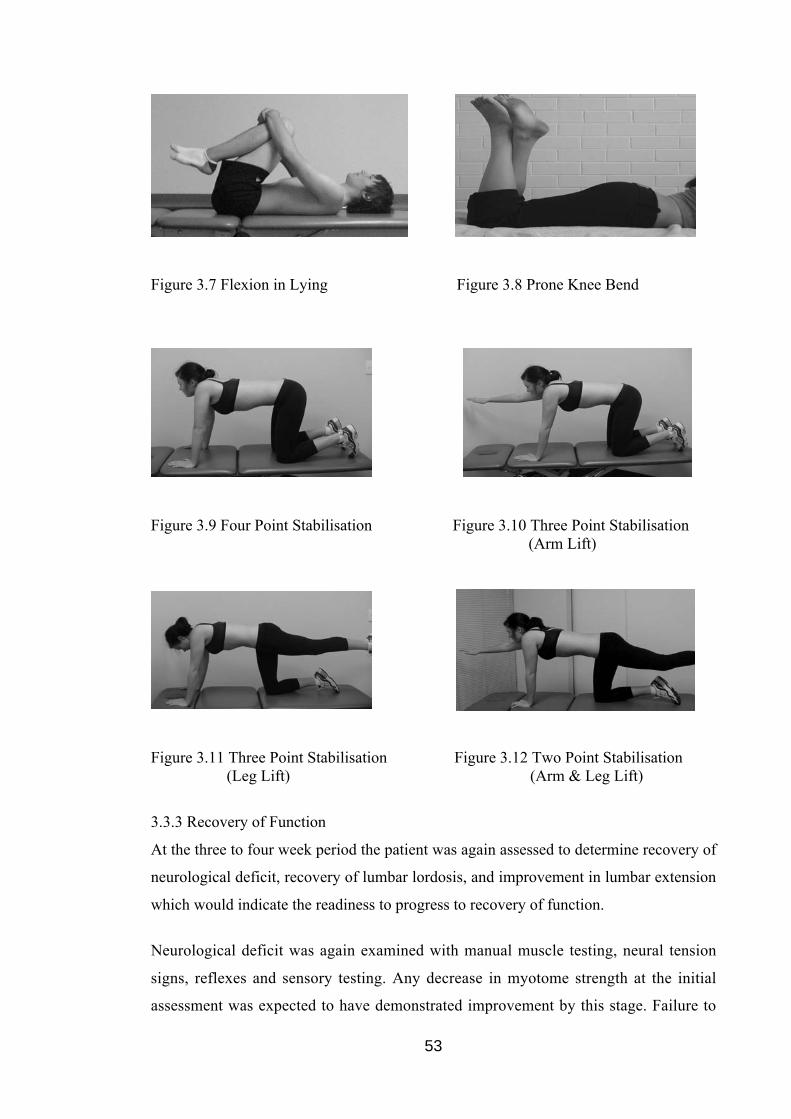
53
Figure 3.7 Flexion in Lying Figure 3.8 Prone Knee Bend
Figure 3.9 Four Point Stabilisation Figure 3.10 Three Point Stabilisation (Arm Lift)
Figure 3.11 Three Point Stabilisation (Leg Lift)
Figure 3.12 Two Point Stabilisation (Arm & Leg Lift)
3.3.3 Recovery of Function
At the three to four week period the patient was again assessed to determine recovery of
neurological deficit, recovery of lumbar lordosis, and improvement in lumbar extension
which would indicate the readiness to progress to recovery of function.
Neurological deficit was again examined with manual muscle testing, neural tension
signs, reflexes and sensory testing. Any decrease in myotome strength at the initial
assessment was expected to have demonstrated improvement by this stage. Failure to
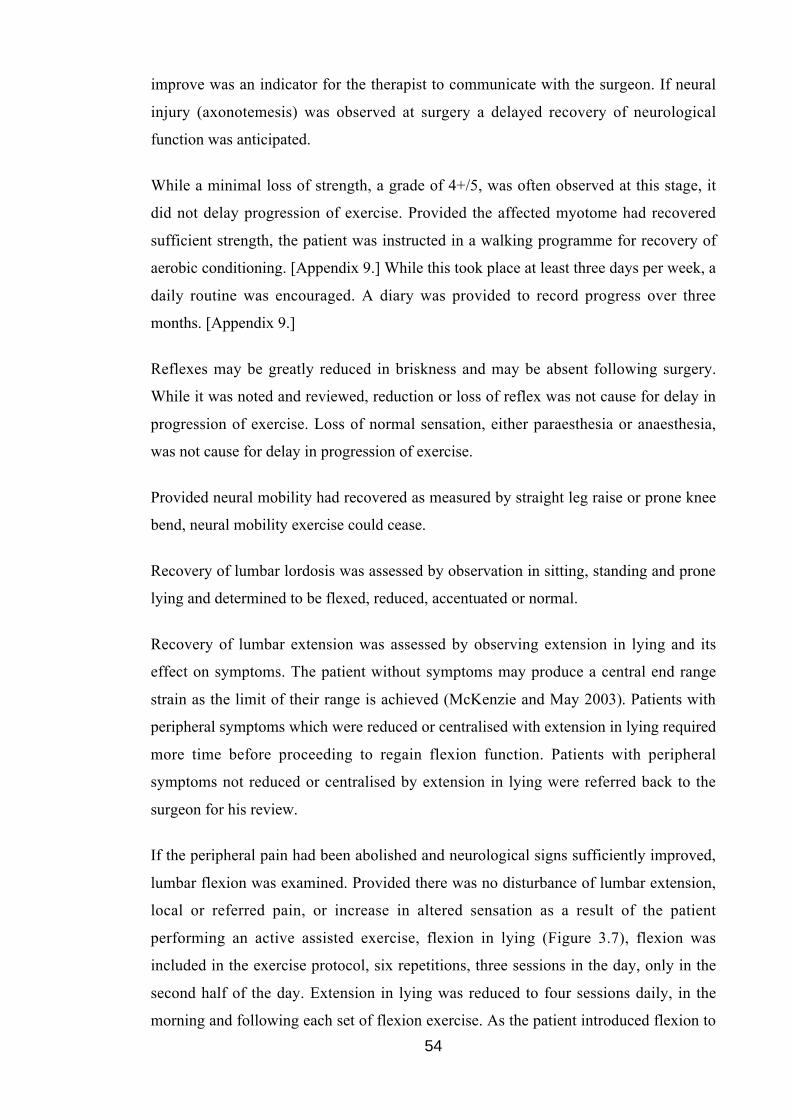
54
improve was an indicator for the therapist to communicate with the surgeon. If neural
injury (axonotemesis) was observed at surgery a delayed recovery of neurological
function was anticipated.
While a minimal loss of strength, a grade of 4+/5, was often observed at this stage, it
did not delay progression of exercise. Provided the affected myotome had recovered
sufficient strength, the patient was instructed in a walking programme for recovery of
aerobic conditioning. [Appendix 9.] While this took place at least three days per week, a
daily routine was encouraged. A diary was provided to record progress over three
months. [Appendix 9.]
Reflexes may be greatly reduced in briskness and may be absent following surgery.
While it was noted and reviewed, reduction or loss of reflex was not cause for delay in
progression of exercise. Loss of normal sensation, either paraesthesia or anaesthesia,
was not cause for delay in progression of exercise.
Provided neural mobility had recovered as measured by straight leg raise or prone knee
bend, neural mobility exercise could cease.
Recovery of lumbar lordosis was assessed by observation in sitting, standing and prone
lying and determined to be flexed, reduced, accentuated or normal.
Recovery of lumbar extension was assessed by observing extension in lying and its
effect on symptoms. The patient without symptoms may produce a central end range
strain as the limit of their range is achieved (McKenzie and May 2003). Patients with
peripheral symptoms which were reduced or centralised with extension in lying required
more time before proceeding to regain flexion function. Patients with peripheral
symptoms not reduced or centralised by extension in lying were referred back to the
surgeon for his review.
If the peripheral pain had been abolished and neurological signs sufficiently improved,
lumbar flexion was examined. Provided there was no disturbance of lumbar extension,
local or referred pain, or increase in altered sensation as a result of the patient
performing an active assisted exercise, flexion in lying (Figure 3.7), flexion was
included in the exercise protocol, six repetitions, three sessions in the day, only in the
second half of the day. Extension in lying was reduced to four sessions daily, in the
morning and following each set of flexion exercise. As the patient introduced flexion to
55
their exercise protocol normal daily activities were encouraged, including resumption of
household and work duties.
If the worker was required to do heavy manual work, or work in sustained flexion
postures, such as plumbing, carpentry and some office work requiring long periods of
uninterrupted sitting, return to work could be delayed until after the neurosurgeon’s
review six weeks after surgery.
Functional core trunk stabilisation was progressed to four point kneeling exercise with
progressions through three point and two point kneeling as tolerated (Figures 3.9, 3.10,
3.11, 3.12). Functional core trunk stability exercise (O'Sullivan 2000) was encouraged
to progress through different positions of stability ceasing only when they were
confident of their ability.
If for any reason the protocol could not be completed at this time further follow-up was
arranged. However if there were no difficulties, the patient was instructed to continue
with the exercise as discussed for one week. At that time flexion could be discontinued
while extension in lying was to be used for the long term at least twice daily, and more
frequently where the patient was required to repeat or sustain flexion.
3.3.4 Prevention of Recurrence
Advice given to the patient during ‘maintenance of reduction’ and ‘recovery of
function’ is the basis for preventing recurrence of symptoms arising from: reherniation,
neural adhesion or irritation of the posterior anulus. Education regarding prophylaxis is
included as the patient advances through the exercise and posture correction protocol
(McKenzie and May 2003). For the post-surgical low back patient, awareness of
appropriate exercise and sustained postural loading is most important in prevention of
recurrence.
3.3.5 Summary
Based upon a retrospective study the McKenzie Approach for treatment of lumbar spine
derangements has been further developed in a novel approach to treat patients after
lumbar microdiscectomy. The principles of effective management of derangement
involving a mixture of education and mechanical therapy have been used to maintain
the reduction of the herniation; recover function; and prevent recurrence.
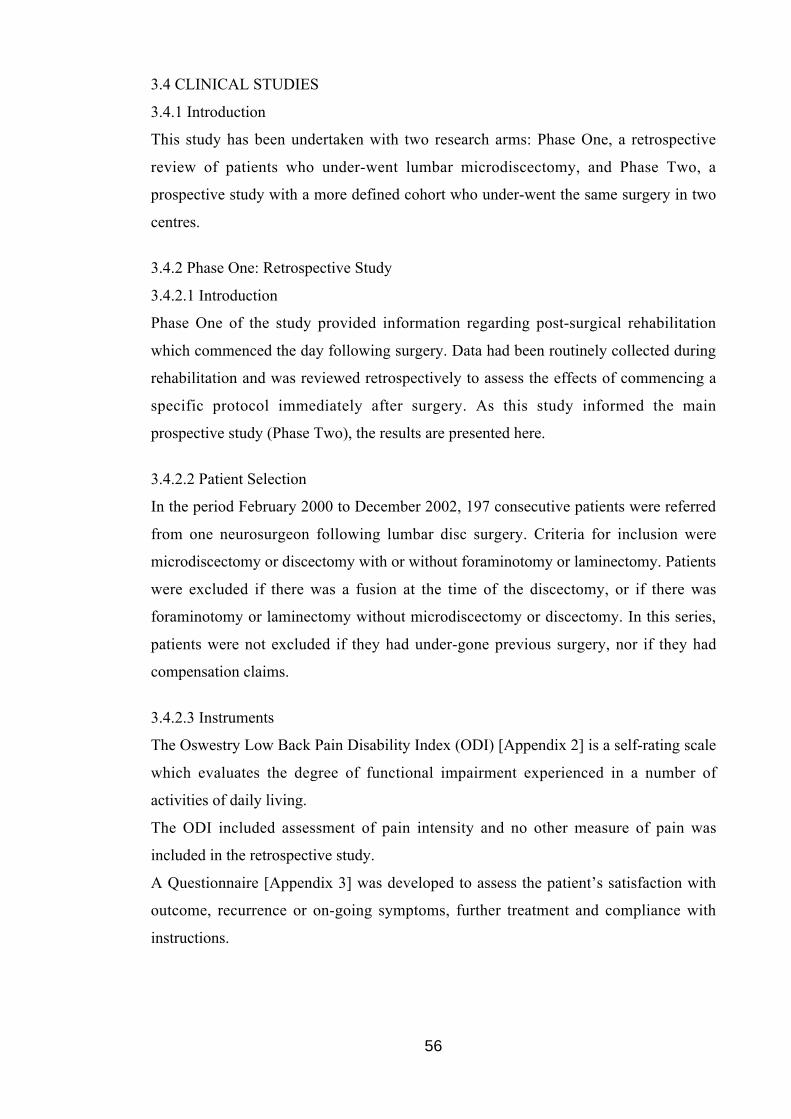
56
3.4 CLINICAL STUDIES
3.4.1 Introduction
This study has been undertaken with two research arms: Phase One, a retrospective
review of patients who under-went lumbar microdiscectomy, and Phase Two, a
prospective study with a more defined cohort who under-went the same surgery in two
centres.
3.4.2 Phase One: Retrospective Study
3.4.2.1 Introduction
Phase One of the study provided information regarding post-surgical rehabilitation
which commenced the day following surgery. Data had been routinely collected during
rehabilitation and was reviewed retrospectively to assess the effects of commencing a
specific protocol immediately after surgery. As this study informed the main
prospective study (Phase Two), the results are presented here.
3.4.2.2 Patient Selection
In the period February 2000 to December 2002, 197 consecutive patients were referred
from one neurosurgeon following lumbar disc surgery. Criteria for inclusion were
microdiscectomy or discectomy with or without foraminotomy or laminectomy. Patients
were excluded if there was a fusion at the time of the discectomy, or if there was
foraminotomy or laminectomy without microdiscectomy or discectomy. In this series,
patients were not excluded if they had under-gone previous surgery, nor if they had
compensation claims.
3.4.2.3 Instruments
The Oswestry Low Back Pain Disability Index (ODI) [Appendix 2] is a self-rating scale
which evaluates the degree of functional impairment experienced in a number of
activities of daily living.
The ODI included assessment of pain intensity and no other measure of pain was
included in the retrospective study.
A Questionnaire [Appendix 3] was developed to assess the patient’s satisfaction with
outcome, recurrence or on-going symptoms, further treatment and compliance with
instructions.
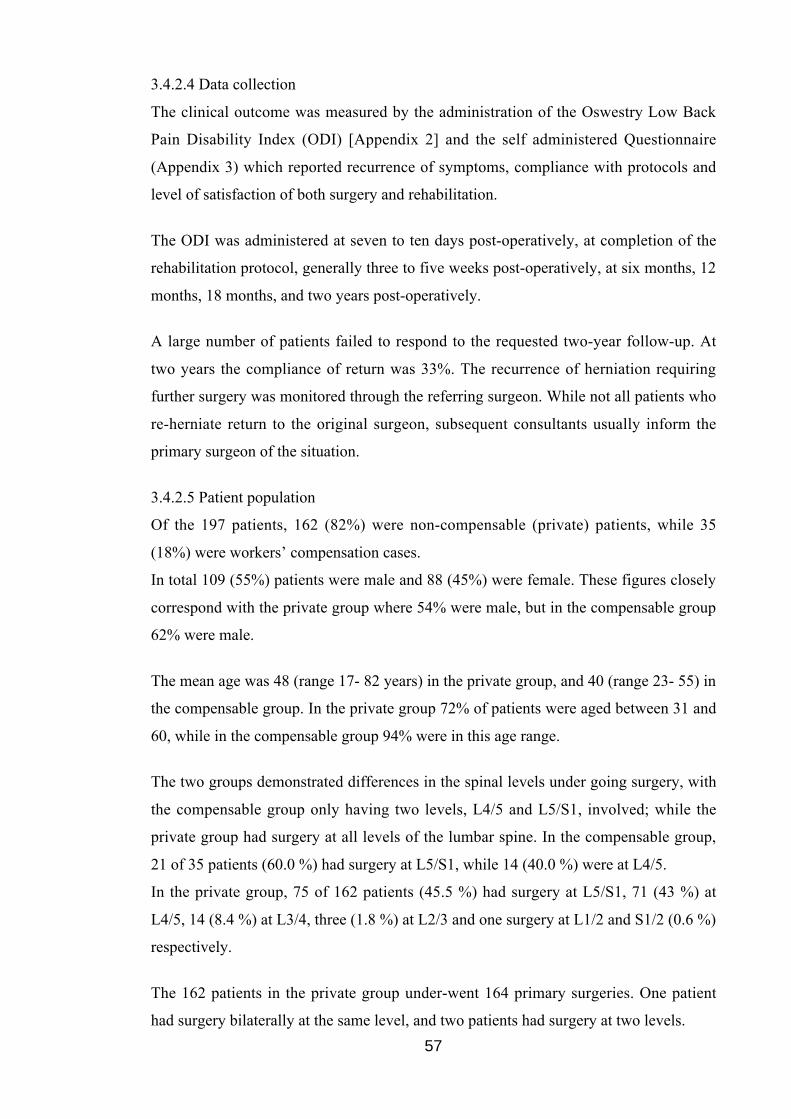
57
3.4.2.4 Data collection
The clinical outcome was measured by the administration of the Oswestry Low Back
Pain Disability Index (ODI) [Appendix 2] and the self administered Questionnaire
(Appendix 3) which reported recurrence of symptoms, compliance with protocols and
level of satisfaction of both surgery and rehabilitation.
The ODI was administered at seven to ten days post-operatively, at completion of the
rehabilitation protocol, generally three to five weeks post-operatively, at six months, 12
months, 18 months, and two years post-operatively.
A large number of patients failed to respond to the requested two-year follow-up. At
two years the compliance of return was 33%. The recurrence of herniation requiring
further surgery was monitored through the referring surgeon. While not all patients who
re-herniate return to the original surgeon, subsequent consultants usually inform the
primary surgeon of the situation.
3.4.2.5 Patient population
Of the 197 patients, 162 (82%) were non-compensable (private) patients, while 35
(18%) were workers’ compensation cases.
In total 109 (55%) patients were male and 88 (45%) were female. These figures closely
correspond with the private group where 54% were male, but in the compensable group
62% were male.
The mean age was 48 (range 17- 82 years) in the private group, and 40 (range 23- 55) in
the compensable group. In the private group 72% of patients were aged between 31 and
60, while in the compensable group 94% were in this age range.
The two groups demonstrated differences in the spinal levels under going surgery, with
the compensable group only having two levels, L4/5 and L5/S1, involved; while the
private group had surgery at all levels of the lumbar spine. In the compensable group,
21 of 35 patients (60.0 %) had surgery at L5/S1, while 14 (40.0 %) were at L4/5.
In the private group, 75 of 162 patients (45.5 %) had surgery at L5/S1, 71 (43 %) at
L4/5, 14 (8.4 %) at L3/4, three (1.8 %) at L2/3 and one surgery at L1/2 and S1/2 (0.6 %)
respectively.
The 162 patients in the private group under-went 164 primary surgeries. One patient
had surgery bilaterally at the same level, and two patients had surgery at two levels.
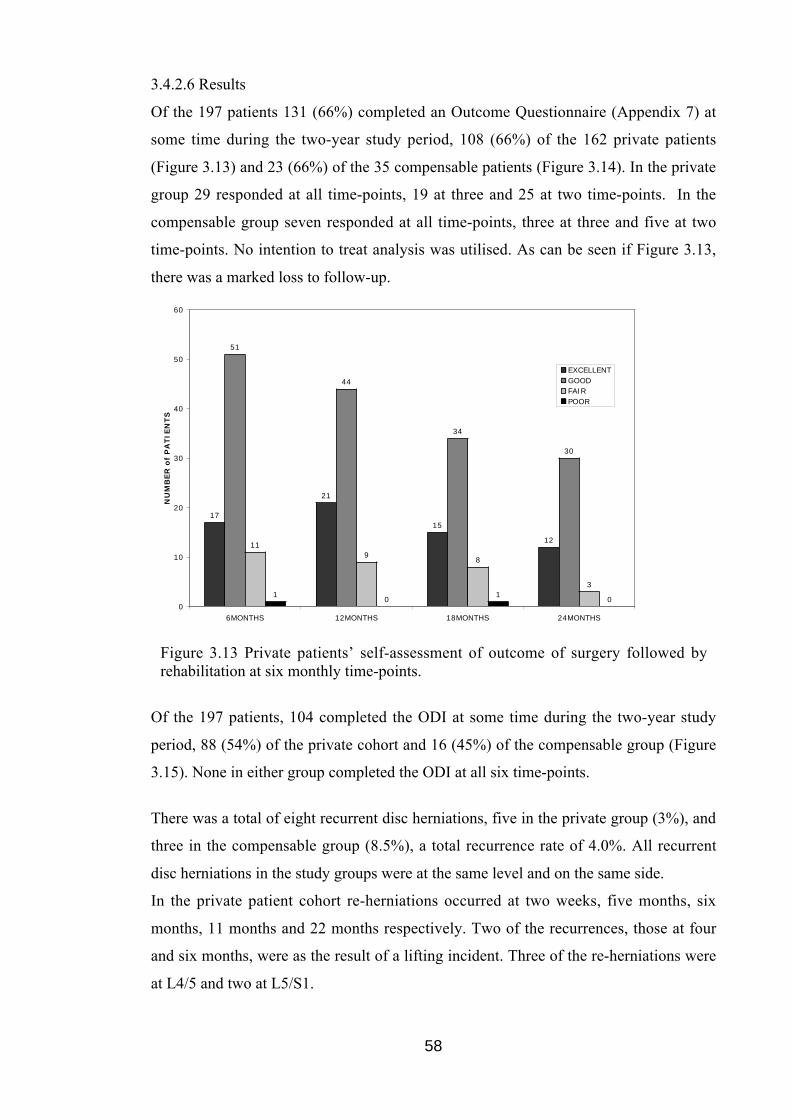
58
3.4.2.6 Results
Of the 197 patients 131 (66%) completed an Outcome Questionnaire (Appendix 7) at
some time during the two-year study period, 108 (66%) of the 162 private patients
(Figure 3.13) and 23 (66%) of the 35 compensable patients (Figure 3.14). In the private
group 29 responded at all time-points, 19 at three and 25 at two time-points. In the
compensable group seven responded at all time-points, three at three and five at two
time-points. No intention to treat analysis was utilised. As can be seen if Figure 3.13,
there was a marked loss to follow-up.
17
21
15
12
51
44
34
30
119
8
31
01
00
10
20
30
40
50
60
6MONTHS 12MONTHS 18MONTHS 24MONTHS
NU
MB
ER
of
PA
TIE
NTS
EXCELLENTGOODFAIRPOOR
Figure 3.13 Private patients’ self-assessment of outcome of surgery followed byrehabilitation at six monthly time-points.
Of the 197 patients, 104 completed the ODI at some time during the two-year study
period, 88 (54%) of the private cohort and 16 (45%) of the compensable group (Figure
3.15). None in either group completed the ODI at all six time-points.
There was a total of eight recurrent disc herniations, five in the private group (3%), and
three in the compensable group (8.5%), a total recurrence rate of 4.0%. All recurrent
disc herniations in the study groups were at the same level and on the same side.
In the private patient cohort re-herniations occurred at two weeks, five months, six
months, 11 months and 22 months respectively. Two of the recurrences, those at four
and six months, were as the result of a lifting incident. Three of the re-herniations were
at L4/5 and two at L5/S1.
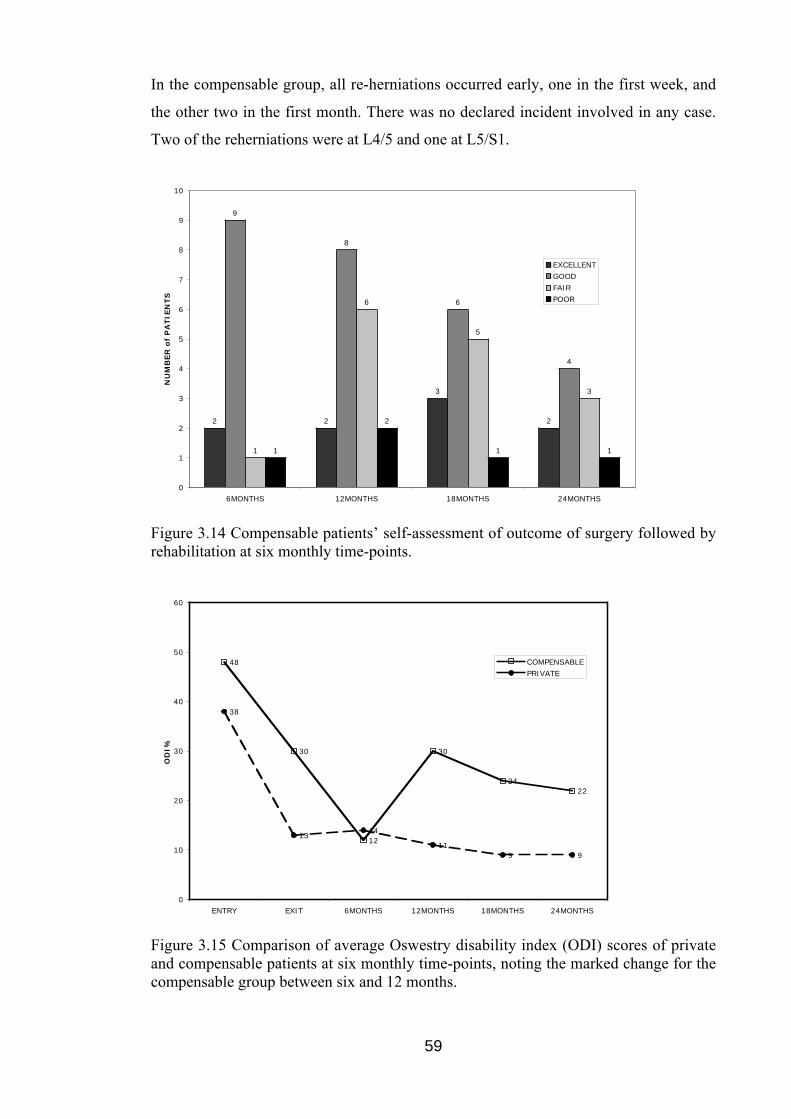
59
In the compensable group, all re-herniations occurred early, one in the first week, and
the other two in the first month. There was no declared incident involved in any case.
Two of the reherniations were at L4/5 and one at L5/S1.
2 2
3
2
9
8
6
4
1
6
5
3
1
2
1 1
0
1
2
3
4
5
6
7
8
9
10
6MONTHS 12MONTHS 18MONTHS 24MONTHS
NU
MB
ER
of
PA
TIE
NTS
EXCELLENT
GOOD
FAIR
POOR
Figure 3.14 Compensable patients’ self-assessment of outcome of surgery followed byrehabilitation at six monthly time-points.
48
30
12
30
2422
38
1314
119 9
0
10
20
30
40
50
60
ENTRY EXIT 6MONTHS 12MONTHS 18MONTHS 24MONTHS
OD
I%
COMPENSABLE
PRIVATE
Figure 3.15 Comparison of average Oswestry disability index (ODI) scores of privateand compensable patients at six monthly time-points, noting the marked change for thecompensable group between six and 12 months.
60
The low number of re-herniations gave very little direction of trends. No further
outcome information could be gleaned from the surveys returned due to the very poor
response rate. Although two of the eight re-herniations in the private cohort and all three
of the re-herniations in the compensable group occurred early, the recurrent herniation
should not be linked to the implementation of the exercise protocol. Moving into
extension has been shown to unload the posterior wall of the disc (Shah et al. 1978;
Krag et al. 1987; Fennell et al. 1996; Edmondston et al. 2000; Wetzel and Donelson
2003) while bending and lifting are the greatest risk factors for acute disc prolapse
(Adams et al. 2002). Brinckmann (1986) found in his in vivo studies that disc extrusions
were produced exclusively by flexion injuries.
The retrospective study confirmed the need for more detailed patient information and a
greater compliance in completion of follow-up questionnaires. This experience helped
inform the prospective study in that the eligibility criteria were narrowed with
compensable patients excluded and outcome questionnaires modified.
The compensable group provided a small subset of data. The expectation of outcome
following surgery in this group is different as is indicated in the Retrospective Study
reviewed. The outcome of compensable patients incorporates several complex issues
including clinical, fiscal and functional outcome.
Consequently the prospective study (Phase Two) did not include compensable patients.
3.4.2.7 Summary
The retrospective study confirmed the need for more detailed patient information, the
inclusion of another form of rehabilitation for comparison and a greater compliance in
completion of follow-up questionnaires to examine outcomes of exercise and
rehabilitation. The eligibility criteria were narrowed with compensable patients
excluded and outcome questionnaires changed.
3.4.3 Phase Two: Prospective Study
3.4.3.1 Introduction
With the information gained from Phase One of the study, the prospective study was
designed to address limitations of the study design. The cohort was refined to reduce
confounding information, data were collected prior to surgery as well as during the
rehabilitation process, the instruments used for outcome assessment were changed, and
intention to treat analysis was adopted.
61
3.4.3.2 Patient Selection
For this prospective study data were collected from 47 consenting consecutive patients
referred from a single neurosurgeon following lumbar disc surgery.
A contrast group comprising 12 patients was recruited from an interstate neurosurgeon.
Criteria for inclusion were microdiscectomy or discectomy with or without
foraminotomy or laminectomy, for disc prolapse where no other device (eg interspinous
prosthesis) was utilised. Subjects were 18 years or older. All aspects of this study were
approved by the Human Research Ethics Committee at the University of Western
Australia. [Appendix 1.]
Patients were excluded if there was a fusion or arthroplasty at the time of discectomy, if
they had previous lumbar spine surgery, or a worker’s compensation claim. Patients
with surgical complications preventing commencement of the protocol the day
following surgery were excluded.
The inclusion and exclusion criteria for each group, the study group and the contrast
group, were the same. The contrast group received standard rehabilitation provided
through referral by the neurosurgeon to local physiotherapists in Queensland.
The candidate administered the rehabilitation protocol in Western Australia, and
collated and analysed the data. These processes were not performed in a blinded
manner.
3.4.3.3 Patient Population
The WA cohort of 47 patients comprised 30 males and 17 females. The average age at
surgery was 45 years.
The side of surgery was equally distributed with 24 left sided surgeries, 22 right sided
and one surgery which was to both left and right (bilateral).
The spinal level of surgery was also equally distributed between L5/S1 and L4/5, with
L4/5 responsible for 23 surgeries, L5/S1 with 22 surgeries and L3/4 with only two
surgeries. The bilateral surgery occurred at L4/5.
The WA cohort was further divided into two groups, those who under-went
microdiscectomy alone (14) and those who required surgery to gain access to the site of
the disc herniation (33), namely: laminectomy, or far lateral approach to a foraminal
prolapse.
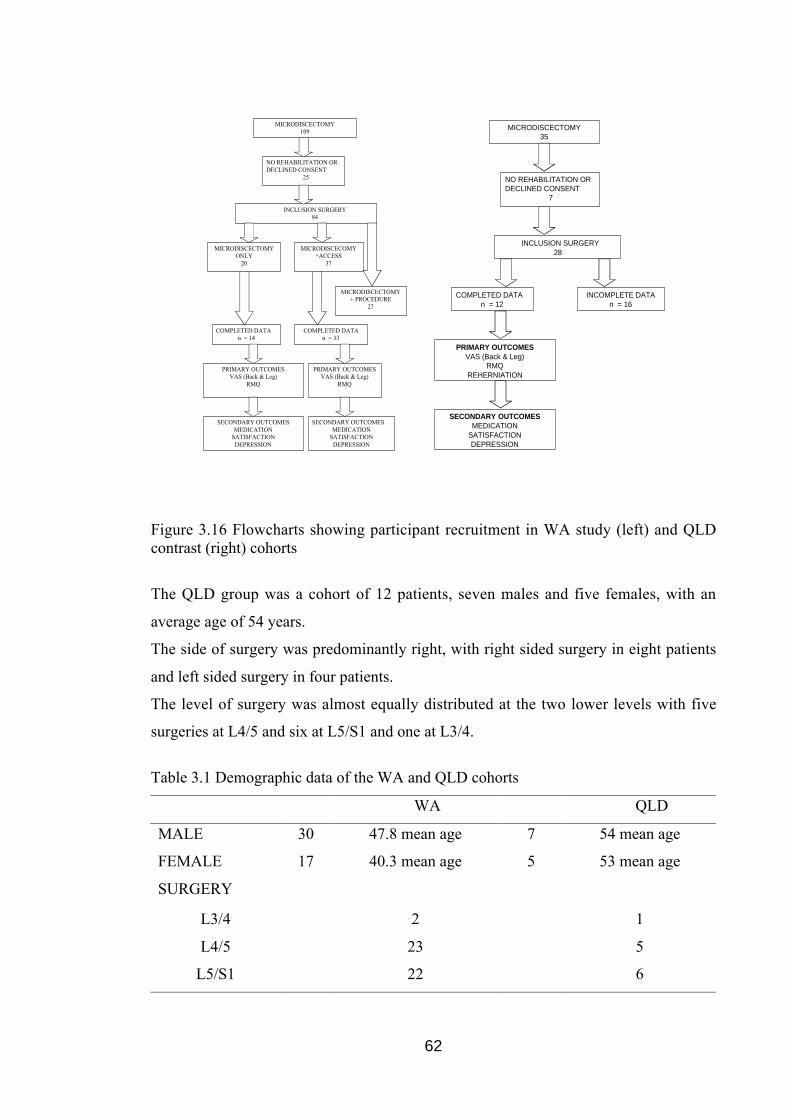
62
MICRODISCECTOMY109
NO REHABILITATION ORDECLINED CONSENT
25
INCLUSION SURGERY84
MICRODISCECTOMYONLY
20
MICRODISCECOMY+ACCESS
37
MICRODISCECTOMY+ PROCEDURE
27
COMPLETED DATAn = 14
COMPLETED DATAn = 33
PRIMARY OUTCOMESVAS (Back & Leg)
RMQ
PRIMARY OUTCOMESVAS (Back & Leg)
RMQ
SECONDARY OUTCOMESMEDICATION
SATISFACTIONDEPRESSION
SECONDARY OUTCOMESMEDICATION
SATISFACTIONDEPRESSION
MICRODISCECTOMY35
NO REHABILITATION ORDECLINED CONSENT
7
INCLUSION SURGERY 28
COMPLETED DATAn = 12
INCOMPLETE DATAn = 16
PRIMARY OUTCOMESVAS (Back & Leg)
RMQREHERNIATION
SECONDARY OUTCOMESMEDICATION
SATISFACTIONDEPRESSION
Figure 3.16 Flowcharts showing participant recruitment in WA study (left) and QLDcontrast (right) cohorts
The QLD group was a cohort of 12 patients, seven males and five females, with an
average age of 54 years.
The side of surgery was predominantly right, with right sided surgery in eight patients
and left sided surgery in four patients.
The level of surgery was almost equally distributed at the two lower levels with five
surgeries at L4/5 and six at L5/S1 and one at L3/4.
Table 3.1 Demographic data of the WA and QLD cohorts
WA QLD
MALE 30 47.8 mean age 7 54 mean age
FEMALE 17 40.3 mean age 5 53 mean age
SURGERY
L3/4 2 1
L4/5 23 5
L5/S1 22 6

63
3.4.3.4 Outcome Measures
According to recommendations from Deyo et al (1998) a core set of measures to assess
outcome includes: back specific function, generic health status, pain, work disability
and patient satisfaction.
Generic health status, work disability and patient satisfaction were assessed with a
specific questionnaire using items validated elsewhere (Deyo et al. 1998). [Appendix 6.]
The patient questionnaire was developed to include the severity of symptoms, the
functional status and satisfaction with care. The functional status was reflected in the
time taken to return to the workplace or to usual duties (as the case might be).
Satisfaction with care, while not a health issue, was of concern in being aware of the
patient’s perception of the level and quality of care.
Other demographic and clinical information, including medication usage and nature of
additional surgical procedures (foraminotomy, laminectomy, etc), were collected for
examination of recovery profiles.
Pain was measured with the Visual Analogue Scale, i.e. the linear VAS, a 10cm long
line, with ends labelled as the extremes of pain (eg. ‘no pain’ to ‘pain as severe as
possible’). [Appendix 5.]
Disability was measured with the 24 item RMQ (Roland and Fairbank 2000).
(Appendix 4.) A score of one point is given to every statement checked on the
questionnaire, with a possible low score of zero (no disability) and a high score of 24
(maximum disability) (Roland and Morris 1983).
The recurrence of herniation requiring further surgery, typically few in number, was
monitored through the referring surgeon. All data were analysed to examine those cases
of re-herniations requiring further surgery, according to: gender, age, side of surgery,
spinal level of surgery, return to usual duties, pain and limitations.
3.4.3.5 Data Collection
Prior to surgery each patient in the WA cohort received Patient Information sheet
[Appendix 7], and the Consent Form [Appendix 8] and a package that included three
outcome measurement instruments: an outcome instrument, the Roland-Morris
Disability Questionnaire (RMQ) [Appendix 4], a linear Visual Analogue Scale (VAS)

64
[Appendix 5] to determine the intensity of back pain and referred leg pain, and a
Questionnaire [Appendix 6]. The outcome instruments were completed before surgery.
Each outcome measurement instrument was completed: before surgery, ten days after
surgery, at the completion of the rehabilitation protocol and at six months and 12
months post-surgery. The first three data collections were undertaken in person while
the latter two were by post or online via web-based forms. The candidate undertook
phone contact with all patients to optimise completion of all questionnaires.
The patients in the QLD cohort received the same package of Patient Information Sheet,
Consent Form and the three outcome measurement instruments which were completed
prior to surgery. Instruments were repeated at the follow-up with the surgeon and at six
and 12 months following their surgery. Periodically these questionnaires were mailed to
the investigator in WA for collating into the database for each cohort.
3.4.3.6 Summary
Forty-seven patients were enrolled into the study from a total of 226 lumbar surgeries
(Figure 3.16). Patients were excluded if they under-went arthrodesis, arthroplasty,
insertion of posterior stabilising devices, had previous surgery or were less than 18
years of age. After completing pre-operative questionnaires the subjects completed a
protocol which commenced the day after surgery and completed further outcome
instruments at time-points over the next 12 months.
3.5 DATA MANAGEMENT AND STATISTICS
Data were presented according to the demographic characteristics of the cohort, and
sub-group analysis was undertaken to consider the potential for different recovery
patterns according to the type of surgery. Repeated measures analysis of variance were
employed to analyse the primary outcome measure scores at the respective time-points
of: pre-surgery, immediate post-operative assessment, at completion of rehabilitation,
after six months and 12 months. An intention to treat design was proposed, with
statistical significance set at a probability of P<0.05. Where data have been incomplete
at exit from rehabilitation or at six months an intention to treat was applied with data
from the previous time-point carried forward. Subjects who under-went repeat surgery
had their data carried forward to the final time-point. A Scheffé test was used for the
planned comparisons to determine whether statistically significant differences occurred

65
between time-points. Sub-group analysis was examined for differences related to factors
which may predict the rate of recovery.
3.6 SUMMARY
Using the McKenzie Approach for the treatment of low back pain, a rehabilitation
protocol was developed to examine outcomes following lumbar microdiscectomy. A
two phase study, with retrospective and prospective arms, was carried out to examine
the effectiveness of the rehabilitation protocol. The second phase of the study included a
contrast cohort at a distant site. The data collected were examined to determine if
there was a difference in outcome following lumbar microdiscectomy between patients
who receive early specific rehabilitation compared with those who receive standard
rehabilitation at another centre, as measured by the incidence of repeat surgery and data
derived from a validated self-report spine specific outcome instrument.
66
CHAPTER 4
RESULTS
4.1 INTRODUCTION
The hypothesis of this study proposed that there would be a difference in outcome
following lumbar microdiscectomy in patients who received early specific rehabilitation
compared with those who received standard rehabilitation at another centre, as
measured by self-reported outcomes and the incidence of repeat surgery.
The primary aim of this study was to determine if there was a reduction in symptoms or
the number of recurrent herniations when a specific rehabilitation protocol, introduced
immediately after surgery, compared with standard rehabilitation at another centre.
[Appendix 10.] Secondary research questions were to determine if there were
differences in the use of pain and anti-inflammatory medications, differences in
depression perception, differences in the perception of satisfaction with surgery and
outcome between those patients who under-went an early specific rehabilitation
protocol and those who experienced standard rehabilitation, as measured by a
standardised questionnaire.
A prospective study of early rehabilitation following lumbar microdiscectomy involving
a study group in Western Australia (WA) and a contrast group in Queensland (QLD)
was commenced in July 2005 with patients followed for one year. The protocol applied
to the WA cohort involved application of the McKenzie Approach to lower back pain
modified for the post-operative patient. For the QLD cohort, standard rehabilitation as
determined by the usual standard of care of Queensland physiotherapy practices, was
implemented. [Appendix 9.]
Primary outcome data included Roland Morris Questionnaire, VAS scores for both back
and leg pain and repeat surgery. Secondary outcome data included medication use,
satisfaction with surgery and responses to questions regarding depression. The WA
group had data collected pre-operatively, post-operatively (at 10 days), at exit from
rehabilitation, at six months and 12 months. This cohort was further divided into two
groups, those who under-went microdiscectomy alone and those who required greater
intervention to access the site of disc herniation, eg. laminectomy or far lateral approach
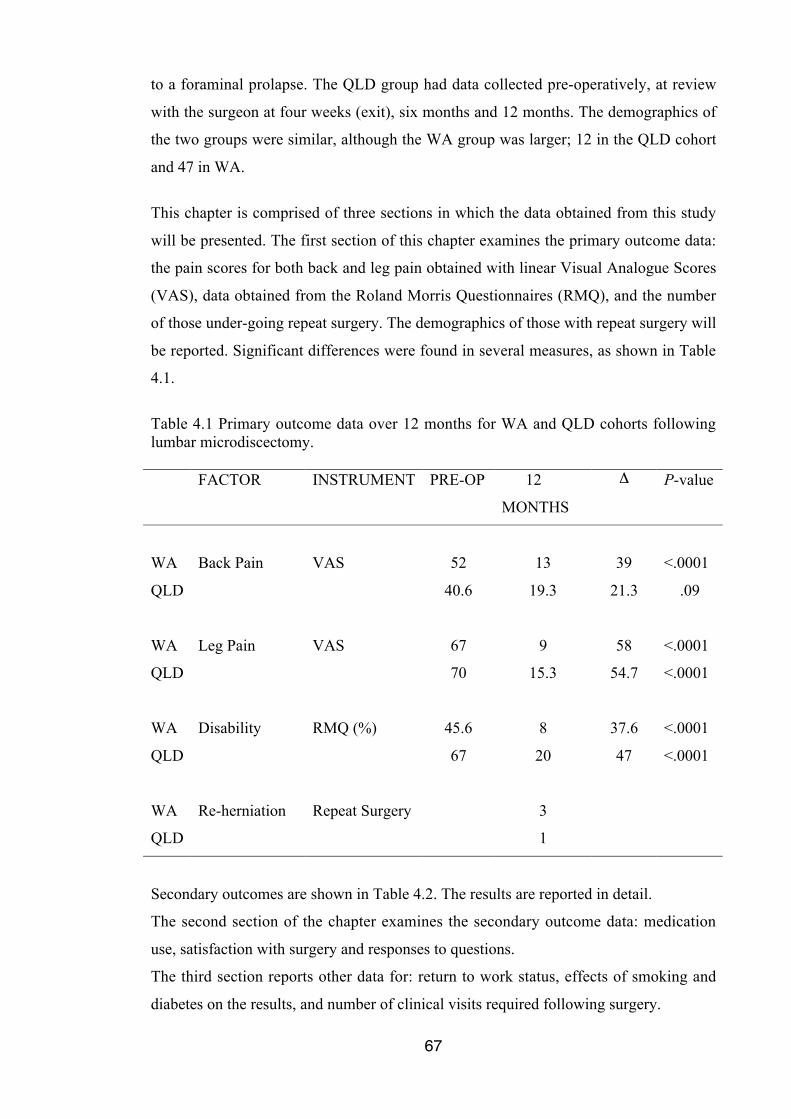
67
to a foraminal prolapse. The QLD group had data collected pre-operatively, at review
with the surgeon at four weeks (exit), six months and 12 months. The demographics of
the two groups were similar, although the WA group was larger; 12 in the QLD cohort
and 47 in WA.
This chapter is comprised of three sections in which the data obtained from this study
will be presented. The first section of this chapter examines the primary outcome data:
the pain scores for both back and leg pain obtained with linear Visual Analogue Scores
(VAS), data obtained from the Roland Morris Questionnaires (RMQ), and the number
of those under-going repeat surgery. The demographics of those with repeat surgery will
be reported. Significant differences were found in several measures, as shown in Table
4.1.
Table 4.1 Primary outcome data over 12 months for WA and QLD cohorts followinglumbar microdiscectomy.
FACTOR INSTRUMENT PRE-OP 12
MONTHS
Δ P-value
WA Back Pain VAS 52 13 39 <.0001
QLD 40.6 19.3 21.3 .09
WA Leg Pain VAS 67 9 58 <.0001
QLD 70 15.3 54.7 <.0001
WA Disability RMQ (%) 45.6 8 37.6 <.0001
QLD 67 20 47 <.0001
WA Re-herniation Repeat Surgery 3
QLD 1
Secondary outcomes are shown in Table 4.2. The results are reported in detail.
The second section of the chapter examines the secondary outcome data: medication
use, satisfaction with surgery and responses to questions.
The third section reports other data for: return to work status, effects of smoking and
diabetes on the results, and number of clinical visits required following surgery.
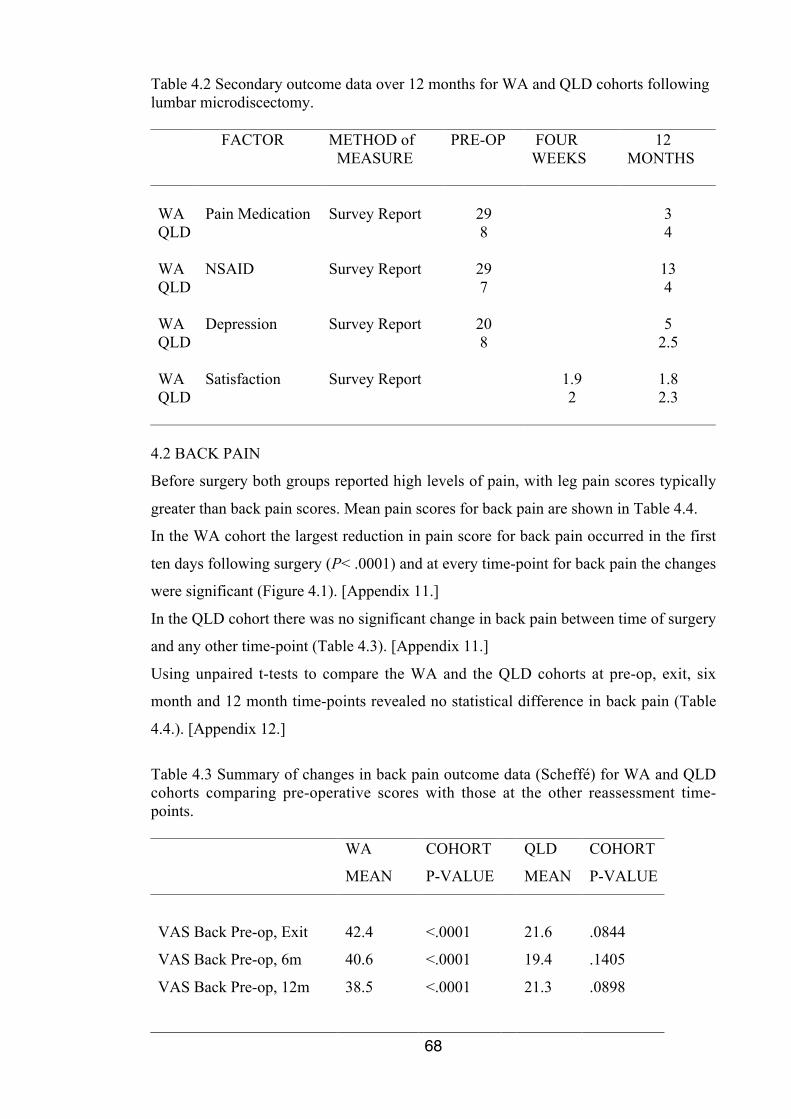
68
Table 4.2 Secondary outcome data over 12 months for WA and QLD cohorts followinglumbar microdiscectomy.
FACTOR METHOD of MEASURE
PRE-OP FOURWEEKS
12MONTHS
WA Pain Medication Survey Report 29 3QLD 8 4
WA NSAID Survey Report 29 13QLD 7 4
WA Depression Survey Report 20 5QLD 8 2.5
WA Satisfaction Survey Report 1.9 1.8QLD 2 2.3
4.2 BACK PAIN
Before surgery both groups reported high levels of pain, with leg pain scores typically
greater than back pain scores. Mean pain scores for back pain are shown in Table 4.4.
In the WA cohort the largest reduction in pain score for back pain occurred in the first
ten days following surgery (P< .0001) and at every time-point for back pain the changes
were significant (Figure 4.1). [Appendix 11.]
In the QLD cohort there was no significant change in back pain between time of surgery
and any other time-point (Table 4.3). [Appendix 11.]
Using unpaired t-tests to compare the WA and the QLD cohorts at pre-op, exit, six
month and 12 month time-points revealed no statistical difference in back pain (Table
4.4.). [Appendix 12.]
Table 4.3 Summary of changes in back pain outcome data (Scheffé) for WA and QLDcohorts comparing pre-operative scores with those at the other reassessment time-points.
WA COHORT QLD COHORT
MEAN P-VALUE MEAN P-VALUE
VAS Back Pre-op, Exit 42.4 <.0001 21.6 .0844
VAS Back Pre-op, 6m 40.6 <.0001 19.4 .1405
VAS Back Pre-op, 12m 38.5 <.0001 21.3 .0898
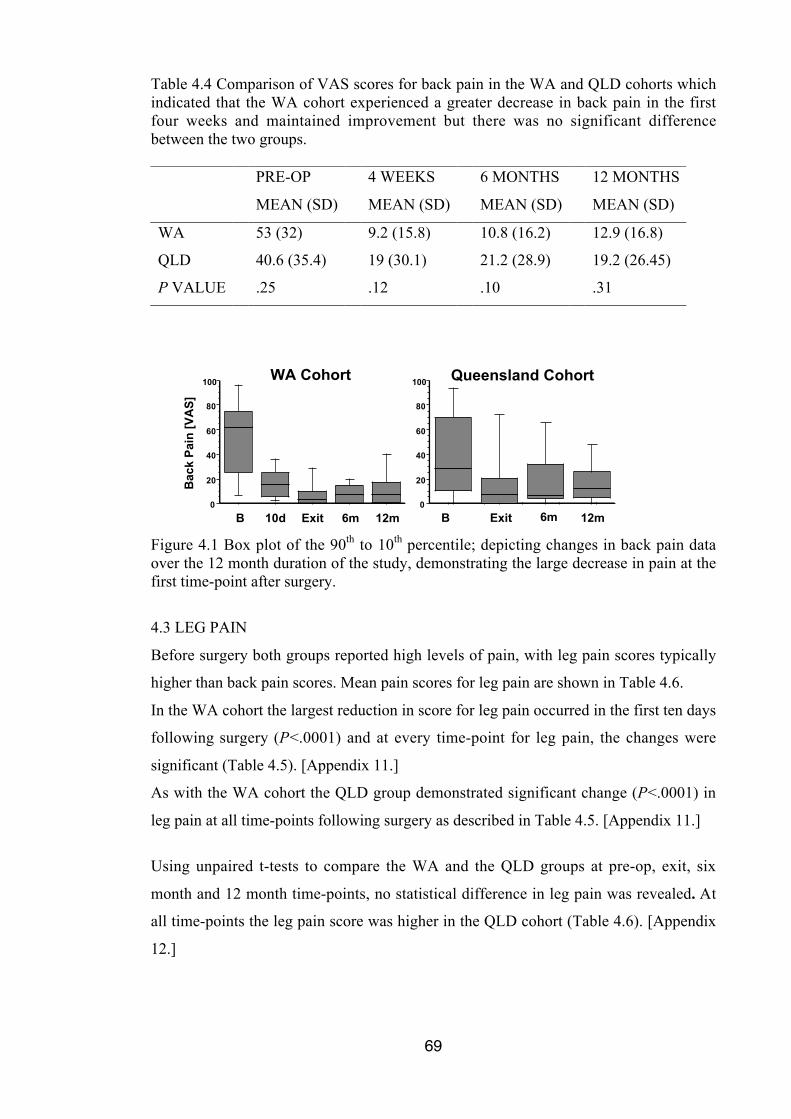
69
Table 4.4 Comparison of VAS scores for back pain in the WA and QLD cohorts whichindicated that the WA cohort experienced a greater decrease in back pain in the firstfour weeks and maintained improvement but there was no significant differencebetween the two groups.
PRE-OP
MEAN (SD)
4 WEEKS
MEAN (SD)
6 MONTHS
MEAN (SD)
12 MONTHS
MEAN (SD)
WA 53 (32) 9.2 (15.8) 10.8 (16.2) 12.9 (16.8)
QLD 40.6 (35.4) 19 (30.1) 21.2 (28.9) 19.2 (26.45)
P VALUE .25 .12 .10 .31
10dB Exit 6m 12m B Exit 6m 12m
Bac
k P
ain
[V
AS
]
0
20
40
60
80
100WA Cohort
0
20
40
60
80
100 Queensland Cohort
Figure 4.1 Box plot of the 90th to 10th percentile; depicting changes in back pain dataover the 12 month duration of the study, demonstrating the large decrease in pain at thefirst time-point after surgery.
4.3 LEG PAIN
Before surgery both groups reported high levels of pain, with leg pain scores typically
higher than back pain scores. Mean pain scores for leg pain are shown in Table 4.6.
In the WA cohort the largest reduction in score for leg pain occurred in the first ten days
following surgery (P<.0001) and at every time-point for leg pain, the changes were
significant (Table 4.5). [Appendix 11.]
As with the WA cohort the QLD group demonstrated significant change (P<.0001) in
leg pain at all time-points following surgery as described in Table 4.5. [Appendix 11.]
Using unpaired t-tests to compare the WA and the QLD groups at pre-op, exit, six
month and 12 month time-points, no statistical difference in leg pain was revealed. At
all time-points the leg pain score was higher in the QLD cohort (Table 4.6). [Appendix
12.]

70
Table 4.5 Summary of changes in leg pain outcome data (Scheffé) for WA and QLDcohorts comparing pre-operative scores with those at the other reassessment time-points.
WA COHORT QLD COHORT
MEAN P-VALUE MEAN P-VALUE
VAS Leg Pre-op, Exit 57.3 <.0001 50.4 <.0001
VAS Leg Pre-op, 6m 57.4 <.0001 51.7 <.0001
VAS Leg Pre-op, 12m 56.2 <.0001 54.5 <.0001
Table 4.6 Comparison of VAS scores for leg pain in the WA and QLD cohorts whichindicated that both groups under-went marked reduction of leg pain immediatelyfollowing the surgery. The improvement was maintained for the course of the study.There was no significant difference between the two groups.
PRE-OP
MEAN (SD)
4 WEEKS
MEAN (SD)
6 MONTHS
MEAN (SD)
12 MONTHS
MEAN (SD)
WA 66.4 (29.6) 8 (16.1) 7.9 (15.9) 9.04 (18.5)
QLD 69.7 (19.2) 19 (27.8) 18.1 (29.2) 15.25 (30.08)
P VALUE .71 .07 .11 .37
10dB Exit 6m 12m B Exit 6m 12m
WA Cohort Queensland Cohort
Leg
Pai
n [
VA
S]
0
20
40
60
80
100
0
20
40
60
80
100
Figure 4.2 Box plot of the 90th to 10th percentile, depicting changes in leg pain data overthe 12 month duration of the study, recording the sharp decline in pain immediatelyfollowing the surgery. In the WA cohort there is an evident decline between ten daysand the exit at four weeks which is maintained throughout the 12 months.
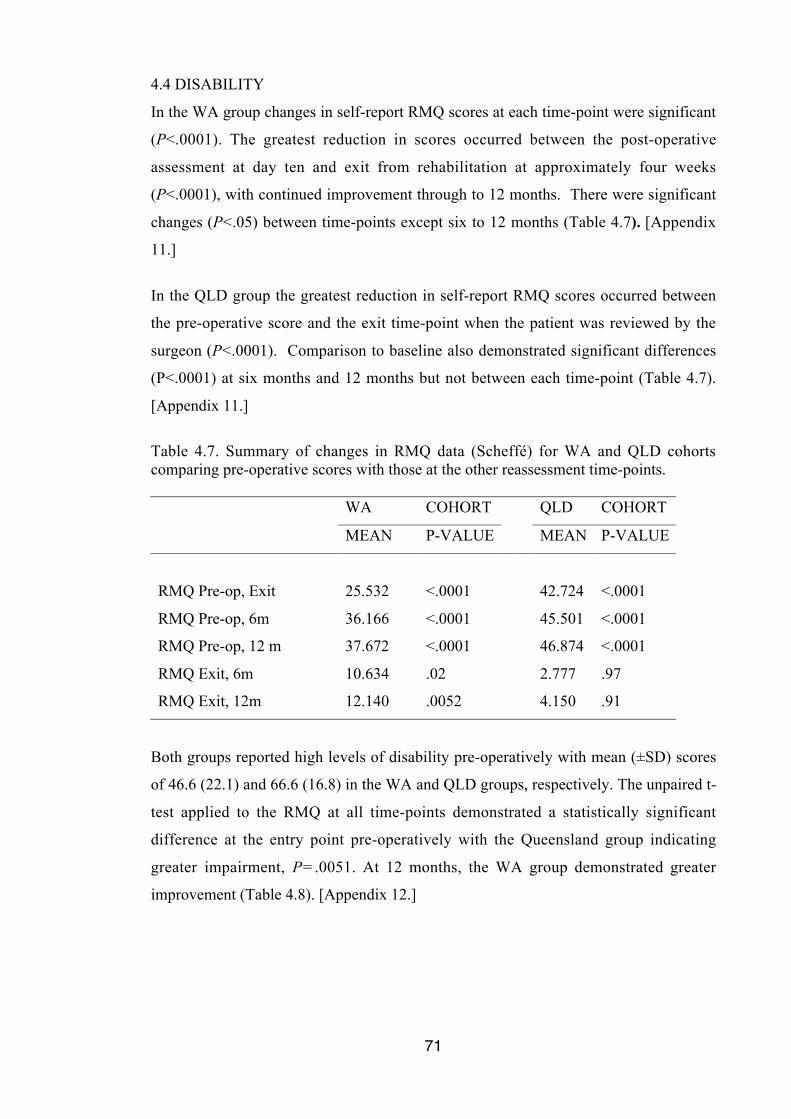
71
4.4 DISABILITY
In the WA group changes in self-report RMQ scores at each time-point were significant
(P<.0001). The greatest reduction in scores occurred between the post-operative
assessment at day ten and exit from rehabilitation at approximately four weeks
(P<.0001), with continued improvement through to 12 months. There were significant
changes (P<.05) between time-points except six to 12 months (Table 4.7). [Appendix
11.]
In the QLD group the greatest reduction in self-report RMQ scores occurred between
the pre-operative score and the exit time-point when the patient was reviewed by the
surgeon (P<.0001). Comparison to baseline also demonstrated significant differences
(P<.0001) at six months and 12 months but not between each time-point (Table 4.7).
[Appendix 11.]
Table 4.7. Summary of changes in RMQ data (Scheffé) for WA and QLD cohortscomparing pre-operative scores with those at the other reassessment time-points.
WA COHORT QLD COHORT
MEAN P-VALUE MEAN P-VALUE
RMQ Pre-op, Exit 25.532 <.0001 42.724 <.0001
RMQ Pre-op, 6m 36.166 <.0001 45.501 <.0001
RMQ Pre-op, 12 m 37.672 <.0001 46.874 <.0001
RMQ Exit, 6m 10.634 .02 2.777 .97
RMQ Exit, 12m 12.140 .0052 4.150 .91
Both groups reported high levels of disability pre-operatively with mean (±SD) scores
of 46.6 (22.1) and 66.6 (16.8) in the WA and QLD groups, respectively. The unpaired t-
test applied to the RMQ at all time-points demonstrated a statistically significant
difference at the entry point pre-operatively with the Queensland group indicating
greater impairment, P=.0051. At 12 months, the WA group demonstrated greater
improvement (Table 4.8). [Appendix 12.]
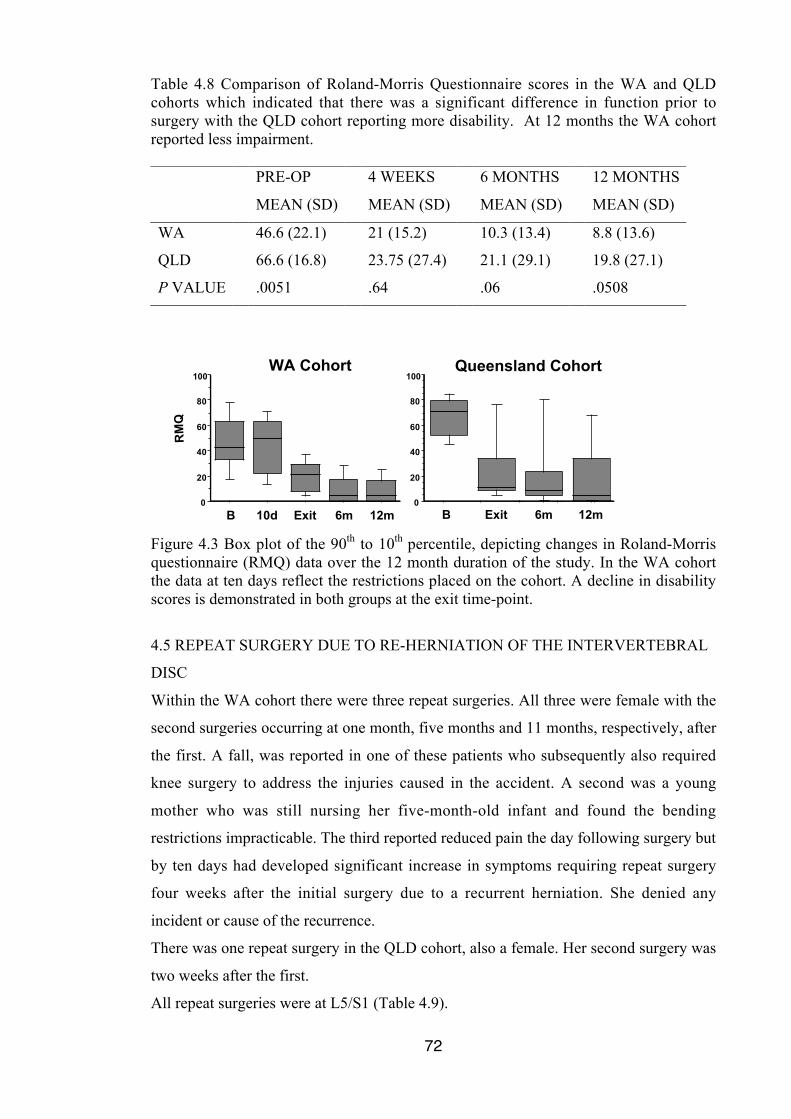
72
Table 4.8 Comparison of Roland-Morris Questionnaire scores in the WA and QLDcohorts which indicated that there was a significant difference in function prior tosurgery with the QLD cohort reporting more disability. At 12 months the WA cohortreported less impairment.
PRE-OP
MEAN (SD)
4 WEEKS
MEAN (SD)
6 MONTHS
MEAN (SD)
12 MONTHS
MEAN (SD)
WA 46.6 (22.1) 21 (15.2) 10.3 (13.4) 8.8 (13.6)
QLD 66.6 (16.8) 23.75 (27.4) 21.1 (29.1) 19.8 (27.1)
P VALUE .0051 .64 .06 .0508
WA Cohort Queensland Cohort
RM
Q
0
20
40
60
80
100
10dB Exit 6m 12m0
20
40
60
80
100
B Exit 6m 12m
Figure 4.3 Box plot of the 90th to 10th percentile, depicting changes in Roland-Morrisquestionnaire (RMQ) data over the 12 month duration of the study. In the WA cohortthe data at ten days reflect the restrictions placed on the cohort. A decline in disabilityscores is demonstrated in both groups at the exit time-point.
4.5 REPEAT SURGERY DUE TO RE-HERNIATION OF THE INTERVERTEBRAL
DISC
Within the WA cohort there were three repeat surgeries. All three were female with the
second surgeries occurring at one month, five months and 11 months, respectively, after
the first. A fall, was reported in one of these patients who subsequently also required
knee surgery to address the injuries caused in the accident. A second was a young
mother who was still nursing her five-month-old infant and found the bending
restrictions impracticable. The third reported reduced pain the day following surgery but
by ten days had developed significant increase in symptoms requiring repeat surgery
four weeks after the initial surgery due to a recurrent herniation. She denied any
incident or cause of the recurrence.
There was one repeat surgery in the QLD cohort, also a female. Her second surgery was
two weeks after the first.
All repeat surgeries were at L5/S1 (Table 4.9).
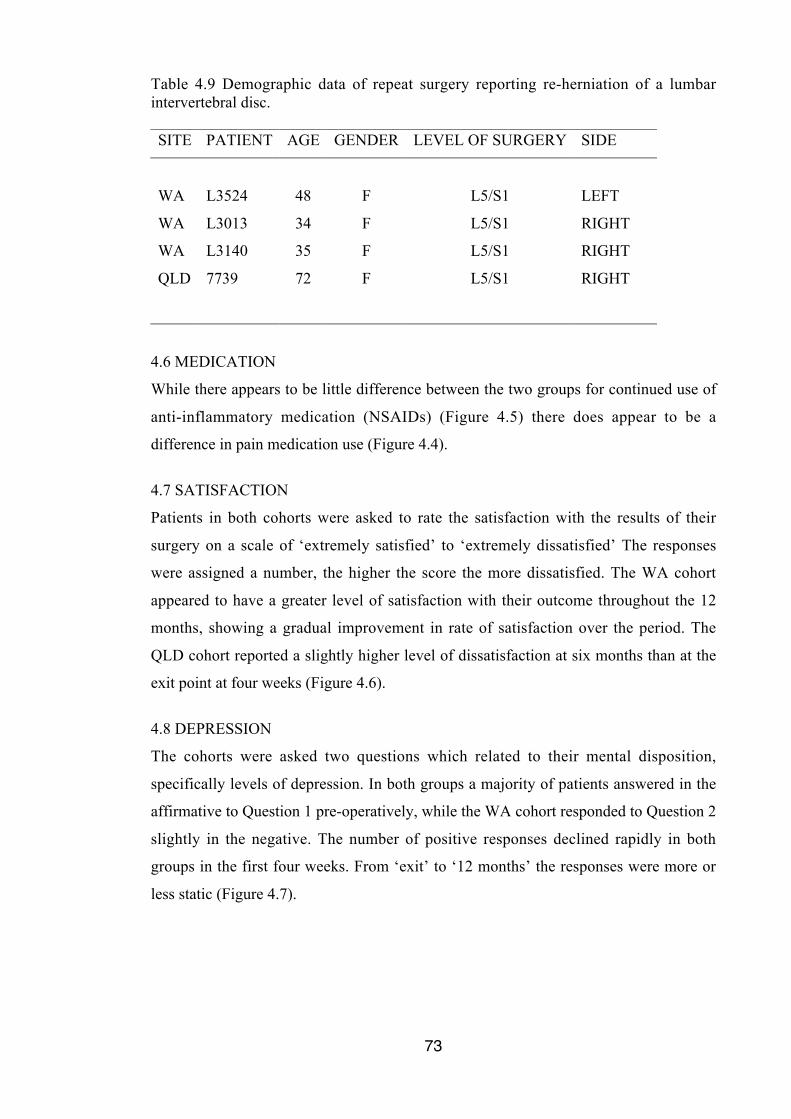
73
Table 4.9 Demographic data of repeat surgery reporting re-herniation of a lumbarintervertebral disc.
SITE PATIENT AGE GENDER LEVEL OF SURGERY SIDE
WA L3524 48 F L5/S1 LEFT
WA L3013 34 F L5/S1 RIGHT
WA L3140 35 F L5/S1 RIGHT
QLD 7739 72 F L5/S1 RIGHT
4.6 MEDICATION
While there appears to be little difference between the two groups for continued use of
anti-inflammatory medication (NSAIDs) (Figure 4.5) there does appear to be a
difference in pain medication use (Figure 4.4).
4.7 SATISFACTION
Patients in both cohorts were asked to rate the satisfaction with the results of their
surgery on a scale of ‘extremely satisfied’ to ‘extremely dissatisfied’ The responses
were assigned a number, the higher the score the more dissatisfied. The WA cohort
appeared to have a greater level of satisfaction with their outcome throughout the 12
months, showing a gradual improvement in rate of satisfaction over the period. The
QLD cohort reported a slightly higher level of dissatisfaction at six months than at the
exit point at four weeks (Figure 4.6).
4.8 DEPRESSION
The cohorts were asked two questions which related to their mental disposition,
specifically levels of depression. In both groups a majority of patients answered in the
affirmative to Question 1 pre-operatively, while the WA cohort responded to Question 2
slightly in the negative. The number of positive responses declined rapidly in both
groups in the first four weeks. From ‘exit’ to ‘12 months’ the responses were more or
less static (Figure 4.7).
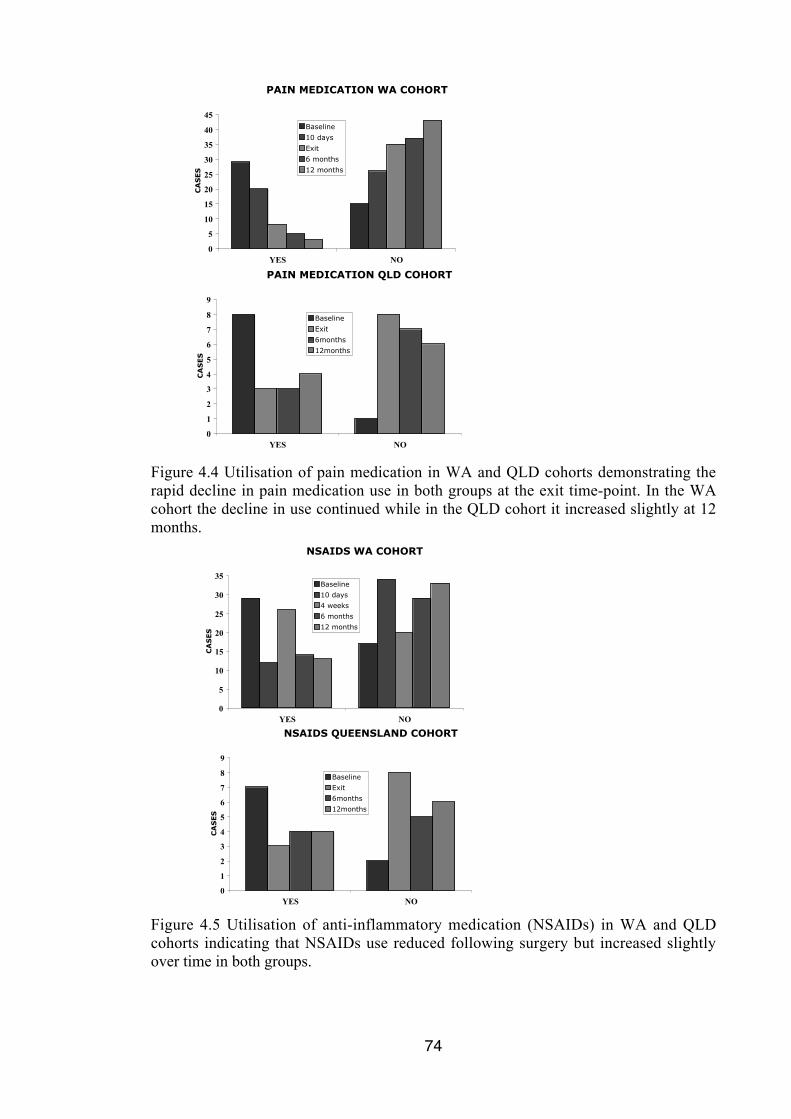
74
YES NO
PAIN MEDICATION WA COHORT
0
5
10
15
20
25
30
35
40
45
YES NO
CA
SE
S
Baseline
10 days
Exit
6 months
12 months
PAIN MEDICATION QLD COHORT
0
1
2
3
4
5
6
7
8
9
CA
SE
S
Baseline
Exit
6months
12months
Figure 4.4 Utilisation of pain medication in WA and QLD cohorts demonstrating therapid decline in pain medication use in both groups at the exit time-point. In the WAcohort the decline in use continued while in the QLD cohort it increased slightly at 12months.
YES NO
NSAIDS WA COHORT
0
5
10
15
20
25
30
35
YES NO
CA
SE
S
Baseline
10 days
4 weeks
6 months
12 months
NSAIDS QUEENSLAND COHORT
0
1
2
3
4
5
6
7
8
9
CA
SE
S
Baseline
Exit
6months
12months
Figure 4.5 Utilisation of anti-inflammatory medication (NSAIDs) in WA and QLDcohorts indicating that NSAIDs use reduced following surgery but increased slightlyover time in both groups.
75
SATISFACTION
0
0.5
1
1.5
2
2.5
3
10 days 4 weeks 6 months 12 months
STUDY GROUP
CONTRAST
Figure 4.6 Satisfaction with outcome of surgery in WA and QLD cohorts demonstratingan increase in dissatisfaction from ‘exit’ to six months in the QLD cohort whereas theWA cohort maintained the level established immediately after surgery.
DEPRESSION WA COHORT
0
5
10
15
20
25
30
35
40
45
YES YES NO NO
CA
SE
S
Baseline
10 days
Exit
6 months
12 months
DEPRESSION QUEENSLAND COHORT
01
23
45
67
89
10
YES YES NO NO
Q1 Q2 Q1 Q2
CA
SE
S
Baseline
Exit
6months
12months
Figure 4.7 Responses to depression questions. In both questions the positive responsesrapidly declined after surgery which indicated that the surgery itself had a great effecton the patients’ mental disposition.
4.9 OTHER RESULTS
Data was collected regarding the effects of the early rehabilitation following lumbar
microdiscectomy on the timing of return to work and the ability to perform usual duties.
76
Patients were asked to describe their work function as: same job, full-time, full-duties;
same work, full-time, modified duties; same work, part-time; different work because of
back pain; and unable to work because of back pain.
In the WA cohort four were retired and in the QLD group three were retired. However
in the former group one of the retirees returned to the work force full-time, modified
duties at 12 months.
In the WA cohort pre-operatively 27 thought they would return to the same job, full-
time, full duties and all accomplished this goal. Six planned to work the same job, full-
time, modified duties. At six months one was able to return to full duties. Five planned
to work in the same work, part-time following surgery but at 12 months one of these
had to find different employment because of back pain. One reported not being able to
work following surgery.
In the QLD cohort five planned to return to the same job, full-time, full duties. At 12
months, two of these had modified activities. Two patients returned to the same job,
full-time, modified duties, and one who returned to same work, part-time increased to
same job, full-time at 12 months.
There were six patients in the WA cohort who declared they were smokers (2-35 per
day), and one in the QLD group (15 per day). Due to the few data no statistical
comparison was performed however on average the VAS scores for back pain in
smokers were equal to the cohort average at the pre-op time-point and were –6.8 at 12
months. The VAS scores for leg pain were +11 pre-operatively and -7 at 12 months for
the smokers compared to the average of the WA cohort. The RMQ was +5 at the pre-
operative time-point and –0.7 at 12 months with the smoking cohort indicating a very
slightly better level of function. At the pre-operative time-point and –0.7 at 12 months
with the smoking cohort indicating a very slightly better level of function.
The one smoker in the QLD cohort reported a pre-op VAS of 70 for back pain, and at
12 months a score of 26 compared to the cohort average of 41 at the earlier time-point
and 19 at the latter. The VAS for leg pain was the same in both groups pre-operatively,
and at 12 months the smoker’s VAS was –6.3. The RMQ was the same at the earliest
time-point but at 12 months it was +17.5 for the smoker.
There were two diabetics in the WA cohort and none in the QLD cohort. Due to the few
data no statistical comparison was performed.
77
The WA cohort had an average of 4.4 visits (range 3-13) for rehabilitation including one
visit in the hospital the day following surgery. These data were not collected in the QLD
cohort as they were not enrolled in a specific exercise protocol but rather attended their
local physiotherapist for standard rehabilitation. The Queensland practice often
involved in rehabilitation for the QLD surgeon provided one to three in-patient visits
and an average of four outpatient visits. Some patients chose to continue with on-going
exercise within the rehabilitation environment.
Other procedures following microdiscectomy, including nerve root sleeve injection,
were prescribed by the surgeon for either back or leg pain relief. Relative to sample
size, no marked differences were noted between the two groups.
Table 4.10 Subsequent procedures primarily for pain relief including nerve sleeveinjection in study cohorts.
WA COHORT QLD COHORT
EXIT 4 2
6 MONTHS 5 2
12 MONTHS 0 0
4.10 MICRODISCECTOMY – WITH AND WITHOUT ACCESS
A sub-group analysis of the WA cohort was examined to ascertain if there were
differences in outcome attributable to the more extensive surgical intervention required
with some derangement presentations. 33 of the 47 patients in the cohort required a
laminectomy, foraminotomy or far lateral approach to enable removal of the herniated
disc material. There were no significant differences in any outcome measures as
demonstrated graphically in Figure 4.8 and a subgroup analysis, using unpaired ‘t’ tests,
showed no significant differences for these three dependent variables. [Appendix 13.]
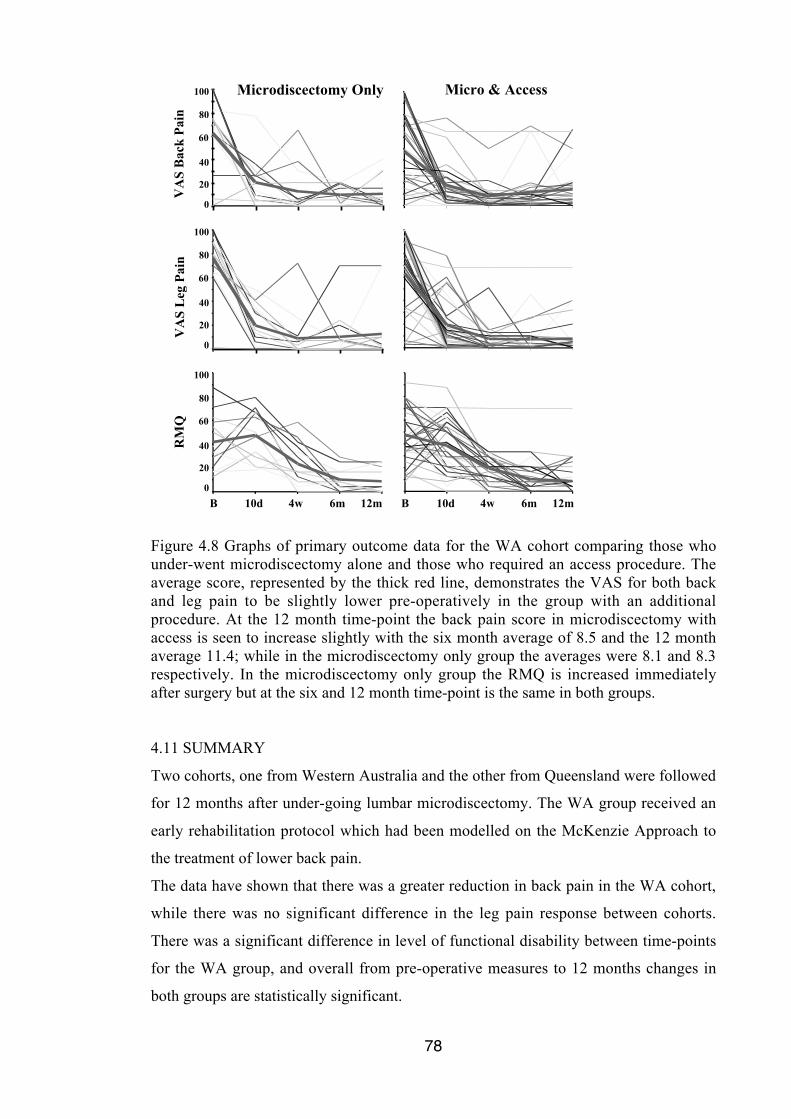
78
100
80
20
60
40
0
100
80
20
60
40
0
100
80
20
60
40
0
Microdiscectomy Only
VA
S B
ack
Pai
nV
AS
Leg
Pai
nR
MQ
10dB 4w 6m 12m 10dB 4w 6m 12m
Micro & Access
Figure 4.8 Graphs of primary outcome data for the WA cohort comparing those whounder-went microdiscectomy alone and those who required an access procedure. Theaverage score, represented by the thick red line, demonstrates the VAS for both backand leg pain to be slightly lower pre-operatively in the group with an additionalprocedure. At the 12 month time-point the back pain score in microdiscectomy withaccess is seen to increase slightly with the six month average of 8.5 and the 12 monthaverage 11.4; while in the microdiscectomy only group the averages were 8.1 and 8.3respectively. In the microdiscectomy only group the RMQ is increased immediatelyafter surgery but at the six and 12 month time-point is the same in both groups.
4.11 SUMMARY
Two cohorts, one from Western Australia and the other from Queensland were followed
for 12 months after under-going lumbar microdiscectomy. The WA group received an
early rehabilitation protocol which had been modelled on the McKenzie Approach to
the treatment of lower back pain.
The data have shown that there was a greater reduction in back pain in the WA cohort,
while there was no significant difference in the leg pain response between cohorts.
There was a significant difference in level of functional disability between time-points
for the WA group, and overall from pre-operative measures to 12 months changes in
both groups are statistically significant.

79
It appears that the WA group was less reliant on pain medication and was more satisfied
with the results of their surgery.
80
CHAPTER 5
DISCUSSION
5.1 INTRODUCTION
The primary aim of this study was to test the hypothesis that there would be a difference
in outcome following lumbar microdiscectomy in patients who received early specific
rehabilitation compared with those who receive contemporary standard rehabilitation
physiotherapy.
Outcome data were collected to determine if there was a reduction in symptoms, the
number of recurrent herniations, differences in the use of pain and anti-inflammatory
medications, depression perception and in the perception of satisfaction with surgery.
The study involved two cohorts, one commencing a novel rehabilitation protocol the
day after lumbar microdiscectomy and the other following standard after surgery
physiotherapy. Pre-operatively data were collected using identical validated outcome
instruments. The questionnaires were repeated ten days after surgery, at exit from care
approximately four weeks post-operatively, then at six and 12 months. Forty-seven
patients from Western Australia (WA) were recruited into the study cohort and 12 from
Queensland (QLD) in to the contrast group.
In summary it was found that the WA cohort reported significantly less back pain at all
time-points, had significantly better function not only at all time-points but also between
each time-point except six to 12 months, took less pain medication and appeared to be
more satisfied with their outcome than the QLD cohort. Both cohorts demonstrated
significant reduction in leg pain. The recurrence rate for herniation was similar in both
groups (3/47 and 1/12), but statistical analysis could not be applied consistently because
of the small numbers in the QLD cohort.
These findings suggest that early introduction of a specific exercise protocol following
lumbar microdiscectomy may reduce back pain and reliance on pain medication.
This discussion focuses on the results which are most pertinent to the hypothesis
concerning difference in outcome in the WA and QLD cohorts. Discussion will be in
the context of the literature review.
81
The first section of this chapter discusses whether the results of the study support the
hypothesis. Differences in primary and secondary outcome data are shown on Tables
4.1 and 4.2.
The second section of this chapter discusses factors which possibly affect the outcome
of surgery and rehabilitation after lumbar microdiscectomy.
The limitations associated with this study are also described.
5.2 PRIMARY OUTCOMES OF THE STUDY
The outcome of the rehabilitation is inextricably linked to the outcome of the surgical
intervention. The measure of outcome must take into account the results as perceived by
three participants: the patient, the surgeon and the therapist. The instruments used must
be reliable and valid measures of outcome.
Prior to surgery, most patients under-going lumbar microdiscectomy have considerable
back and leg pain with significant loss of function. Their expectation is that symptoms
will be relieved, function return to normal, and no further interventions will be required.
However it has been noted that a considerable number experience persistent back and
leg pain and experience on-going disability following lumbar disc surgery (McGregor et
al. 2007).
5.2.1 Back Pain
Following discectomy recurrence of back pain, radiculopathy and herniation can occur.
Radiculopathy is present in 17% to 33% of patients following lumbar discectomy, re-
herniation is reported in 7% to 26% (Carragee et al. 2006), and Yorimitsu et al (2001)
reported 74% of patients complained of back pain in the ten years after disc surgery.
Recurrence or unresolved back pain is not an unexpected result for most surgeons as the
purpose of the surgery was to address the leg symptoms not the back pain (Awad and
Moskovich 2006). Low back pain is the second most common reason for physician
consultation in the United States and back pain after lumbar disc surgery is a large
contributor to this persistent problem (Awad and Moskovich 2006; Hazard 2006).
Along with many researchers Awad and Moskovich (2006) suggest the rate of recurrent
symptoms may vary depending on the technique and experience of the surgeon,
concurrently stating that independent studies performed more than a decade apart
showed no difference in results (Tullberg, Isacson and Weidenhielm 1993; Toyone,
Tanaka, Kato et al. 2004; Awad and Moskovich 2006). In none of these studies was
rehabilitation discussed.
82
Persistent lower back pain after lumbar surgery is seen as a primary cause for a decrease
in satisfaction over time (Awad and Moskovich 2006) while also being a major
contributor to the diagnosis of Failed Back Surgery Syndrome (FBSS) often leading to
surgical fusion (Hazard 2006). Back pain after lumbar surgery is a major problem
(Awad and Moskovich 2006).
While the rehabilitation intervention may be responsible for the statistical differences
seen in back pain in the two cohorts (Table 4.3), there are clear caveats in interpretation
of these results. The cohorts demonstrate random effects of sample size and age
difference, difference of surgeon and perhaps surgical technique, and difference in the
rehabilitation providers, as well the rehabilitation itself.
Patient satisfaction, an important aspect of outcome, is difficult to measure (Bombardier
2000; Hudak and Wright 2000). The design of the questions in the Outcome
Questionnaire [Appendix 6] precluded statistical analysis of the data, but the trends
demonstrated an increasing dissatisfaction with outcome in the QLD cohort, perhaps
related to the back pain, as noted by Awad and Moskovich (2006) (Figure 4.6).
Recent literature has described a difference between a statistically significant score
change and clinical importance (Hagg et al. 2003). Jaeschke et al defined minimal
clinically important difference (MCID) as “the smallest difference in score in the
domain of interest which patients perceive as beneficial” (Jaeschke, Singer and Guyatt
1989:408); MCID is interpreted as the minimum score a clinician believes to be
clinically significant.
The MCID of the VAS for back pain was estimated to be as high as 20% and as low as
12% with the lower measure dominating especially in acute pain (Kelly 2001; Hagg et
al. 2003; Haefeli and Elfering 2006; Copay et al. 2008). Using an unpaired t-test to
compare the two cohorts, the pre-operative score for back pain demonstrated clinical
significance with the WA cohort reporting higher pain scores. [Appendix 12.] With
mean differences of 9.8 and 10.3 at exit and six months, respectively, clinical change
for the WA cohort did not achieve MCID.
5.2.2 Leg Pain
One of the primary reasons for under-taking a lumbar microdiscectomy is to relieve leg
pain. All patients anticipate significant change in leg pain immediately following
surgery and the such a change was reflected in the data collected with the greatest
83
change occurring between the pre-op and the first post-operative measure: in the WA
cohort at ten days and in the QLD cohort at the exit point. This change was maintained
through the length of the study. It is probable that the immediate change in leg pain is
the result of the surgical intervention.
There was no access to the operation notes of the QLD cohort to distinguish those who
under-went microdiscectomy alone and those who required a more extensive surgical
access, but in the WA cohort there was no trend for difference between those two
groups (Results 4.10).
At all time-points the change in leg pain was statistically significant in both cohorts
however the difference in leg pain between the two cohorts was not statistically
significant (Table 4.5). The minimal clinically important difference (MCID) at six and
12 months was examined. Studies of MCID for VAS scores have concentrated on back
pain, with little research into MCID of leg pain. Copay et al (2008) reported 1.6 points
(on a ten point scale) as the MCID for leg pain. Given that the mean difference between
the two cohorts for leg pain at six months and 12 months was 11.4 and 10.2 respectively
(on a 100 point scale), and that Copay et al exhort the clinician that this is a minimal
change and not a yardstick for measuring treatment success, the two cohorts did not
experience a clinically significant difference in leg pain.
Recurrence of leg pain is often cited as a problem after lumbar microdiscectomy
(McGregor et al. 2007). The causes of exacerbation are likely to be the result of
reherniation, nerve root irritation, or neural adhesion. The WA cohort was examined in
two groups, those who under-went additional surgical intervention in order to remove
the herniated material, and those who did not. It was anticipated that the group with
more intervention may report more pain especially leg pain but no difference was found
between the groups, within the period studied. [Appendix 13.] However, it should be
noted that the study was not powered to answer this question.
5.2.3 Disability
The WA cohort had an additional review at ten days. At this time-point the level of
disability was unchanged from the pre-operative score, as demonstrated in the box plot
depicting changes in RMQ data over the length of the study (Figure 4.3). This is not an
unexpected finding as the patients had been given very specific instructions as to
activity and limitations the day following surgery. At achieving the exit point the
84
disability scores had altered significantly (Table 4.7). At all time-points the changes in
the level of function as measured by RMQ were statistically significant in both cohorts,
with the WA group also reporting significant changes between all time-points except
between six and 12 months.
Using the unpaired t-test to compare both cohorts, pre-operatively the QLD cohort was
more functionally impaired (p=0.0051) but at other time-points there was not a
statistically significant difference (Table 4.8). [Appendix 12.]
The MCID for RMQ lies between 2.5 (10.4%) and 5 (21%) points (Roland and
Fairbank 2000). Stratford et al suggest that for patients with little disability 1 to 2 points
(4 to 8%) is the minimum clinically important change, 7 to 8 points (29 to 33.3%) for
patients reporting high levels of disability, and 5 (21%) points for unselected patients
(Stratford et al. 1994; Hagg et al. 2003). In the unpaired t-tests at six and 12 months the
mean difference between the two cohorts was 10.7% and 11% respectively, with the
WA cohort achieving the lower score (Table 4.8). [Appendix 12.] Although not
statistically significant the RMQ suggests a clinically meaningful difference at these
two time-points.
Therapist contact was similar during the post-operative period, the WA cohort being
seen once in the hospital and three to four outpatient visits (average 4.4 overall), and
one to three inpatient visits and four outpatient visits for the standard rehabilitation in
Queensland. The WA cohort was followed in one physiotherapy practice for
rehabilitation with care provided by one of two therapists, whereas the QLD cohort
could have attended any one of a number of providers. Consequently, there may have
been a professional/patient effect in the WA cohort which may have influenced the
results.
5.2.4 Repeat Surgery
There were four repeat surgeries in the study, three in WA and one in QLD. None of the
three in WA demonstrated neural adhesion, all three had re-herniated the same lumbar
disc. The operation notes for the one in QLD were not available but as the surgery was
within one month of the primary surgery it is unlikely neural adhesion was the cause of
recurrence of symptoms.
85
With the low numbers in the QLD cohort direct comparison of repeat surgery for disc
herniation was not possible. Three repeat surgeries in the WA cohort of 47, a recurrence
rate of 6.4%, was in the lower end of the figures quoted in the literature (Carragee et al.
2006), but this cohort was relatively small and had only been followed for 12 months.
5.3 SECONDARY OUTCOMES OF THE STUDY
5.3.1 Medication
The use of anti-inflammatory drugs after surgery was possibly skewed by comorbities.
While the data demonstrate a reduction in use from the pre-operative measure to all
other time-points in both groups it was a relatively large proportion of the cohort who
remained on medication (Figure 4.5).
Data of pain medication use demonstrate a sharp reduction in their use at the exit time-
point in both cohorts indicating the effect of the surgical intervention (Figure 4.4). In
the WA cohort the data indicated a continuing reduction in pain medication use during
the 12 months of the follow-up whereas the QLD cohort increased use between six and
12 months. The QLD cohort was small and comparison of medication use should be
cautious, but there does appear to be a trend towards less pain medication use in the WA
group.
Although detail of type and quantity of medication was asked in the Questionnaire, a
majority of patients did not complete that detail therefore further inspection of these
trends is not possible.
5.3.2 Satisfaction
Satisfaction is a multi-faceted subject with different meanings to different people in a
variety of circumstances (Bombardier 2000). Without being specific in questioning,
approaching the questionnaire from a global direction, will give a more ambiguous
result. In rating ‘satisfaction’ the patient may think about a particular treatment outcome
or overall medical care. Multidimensional measures including one or two questions, as
in the questionnaire [Appendix 6], provided the patient with the opportunity to respond
directly about a particular aspect of their treatment (Hudak and Wright 2000). Questions
may be direct, as in the question: “All things considered, how satisfied are you with the
results of your recent surgery?” Or questions may be indirect as in: “Would you
recommend this treatment to a friend with a similar problem?”
86
Not only is the meaning of satisfaction ambiguous, patients who are dissatisfied are
more likely to withdraw from a study meaning their numbers are often unrepresentative
(Hudak and Wright 2000). Often in studies, the difficulty in interpreting the data
retrieved in questioning satisfaction is that the results are clustered at the very satisfied
end of the scale, resulting in difficulty in detecting change. In this study it appears that
there is an increase in the score for the QLD cohort at six and 12 months indicating a
greater level of dissatisfaction but there is no suitable method of determining if this is
clinically significant (Figure 4.6).
5.4 OTHER OUTCOMES
5.4.1 Return to Work
In order to assess the ability to return to work, Bombardier (2000) recommends that in
the least, work status should be measured at the first and last visit and there should be a
measurement of work time lost (Bombardier 2000). Work status was evaluated at each
time-point through the study but there was no measurement of work time lost (See 4.9
Other Results). Days lost due to recovery after surgery may have been a more objective
measure than the ability to return to full time or part time work, but the two pieces of
information together may have given a better measure of any difference between the
two cohorts.
Carragee et al (1996, 1999) investigated the effects of removing post-operative
restrictions after lumbar discectomy. His primary outcome measures were return to
work and re-herniation. Some of his cohort returned to work earlier than in this
investigation where restrictions on activities were imposed and patients did not return to
work for at least two weeks. The days lost due to recovery would have provided a better
comparison between this study which imposed restrictions and Carraggee’s
investigation which did not. He reported back and leg scores as being low at follow-up,
but did not provide the data (Carragee et al. 1996; 1999).
There is evidence that work capacity following lumbar disc surgery is related to pain
avoidance, such as fear of movement (den Boer, Oostendorp, Beems et al. 2006). In the
WA cohort movement commenced with specific exercise, avoiding bending, the day
following surgery, and at three to four weeks flexion was commenced. Even when
flexion did not demonstrate restriction of range, exercise in this direction was still
encouraged to limit the development of fear of bending.
87
Puolakka et al (2008) in a study of reduced work capacity following lumbar disc
surgery found that 53% reported back pain related sick leave or early retirement in the
five years after surgery. While the Puolakka followed the cohort over a considerably
longer period than the 12 months of this study, the data at 12 months in both cohorts of
this study do not appear to indicate loss of work capacity to the same magnitude.
The cohort of 12 in QLD included three retirees, while there were four in WA. The
proportion of retirees in the QLD community was not taken in to account in developing
the Questionnaire which did not allow for non-workers in the community. Other
questions relating to participating in activities may have provided more information
regarding this group.
5.4.2 Smoking
Grunhagen et al (2006) describe how factors which influence blood supply to the disc
can alter cell activity and viability. With skeletal maturity the discs become almost
avascular, the nearest blood supply at the periphery in the end-plates almost 8mm from
the centre of the adult disc (Warwick and Williams 1973; Katz et al. 1986; Ferguson et
al. 2004). It has been suggested that smoking can reduce the blood supply to the disc
and cause degeneration and delayed healing (Battie, Videman, Gill et al. 1991;
Andersen, Christensen, Laursen et al. 2001). In a study of an active military cohort
under going lumbar microdiscectomy, Dewing et al (2008) found that smokers had a
significantly lower return to full duties than non-smokers, while Kara et al (2005) found
that lack of exercise was a greater predictor of repeat disc surgery than smoking. In the
current study there were few smokers, one in the QLD cohort and six in the WA cohort.
The scores for back and leg pain and disability were no worse in smokers than non-
smokers. One of the total of four re-herniations was in a smoker.
The study by Dewing (2008) provides an insight into a specific cohort of US military
personnel where 22 percent were smokers.
5.5 FACTORS AFFECTING THE OUTCOME OF THE STUDY
5.5.1 Rehabilitation Protocol
There is almost an absence of studies in the literature, prospective or retrospective,
examining the effects of specific rehabilitation protocols following lumbar
microdiscectomy. However there is evidence to support rehabilitation following lumbar
microdiscectomy (Ostelo et al. 2002). The Cochrane Report found that there was strong
88
evidence for an active rehabilitation with early intensive exercise programmes
commencing at four to six weeks (Ostelo et al. 2002). Importantly, they reported that
none of the investigated treatments seemed harmful. Despite strong evidence in favour
of active rehabilitation and the lack of evidence of harm resulting from early exercise,
there remains infrequent referral for rehabilitation and inconsistency in advice and
rehabilitation following surgery (McGregor et al. 2007). For the patient who is under-
going surgery the lack of direction with appropriate clear and concise information,
about both the surgery and the recovery plan, is likely to increase anxiety and perhaps
delay recovery (McGregor et al. 2007).
In the physiotherapy community, those providing rehabilitation after lumbar spine
surgery offer a wide variety of advice and exercise, not all of which appears to be
evidence based (McFarland 1994; McFarland and Burkhart 1999; Maxey and
Magnusson 2007; McGregor et al. 2007; Williamson et al. 2007). This does not dismiss
clinical empiricism, or practice based evidence, as clinical experience is, as Sackett
declares, a very important part of the management approach (Sackett, Rosenberg, Gray
et al. 1996).
While it is not possible to generalise on all rehabilitation providers who offered services
to the QLD cohort, a physiotherapist who on occasion provided rehabilitation for the
neurosurgeon involved in the QLD cohort of the study provided an example of standard
rehabilitation following lumbar microdiscectomy. [Appendix 10.] In-patient care was
directed at mobilising the patient out of bed to allow discharge from the hospital and
achieving very basic contraction of gluteal and lower abdominal wall muscles.
Directions for limitations of activity, for example sitting, were time rather than
symptom based. In the outpatient setting, exercise was primarily directed towards
recovery of lumbar stabilisation. Whereas another example of standard rehabilitation
provided by Sir Charles Gairdner Hospital, Perth [Appendix 14], included minimal
exercise directed at lumbar stabilisation. These two facilities offered different advice
and exercise which is indicative of the problem within rehabilitation after lumbar
microdiscectomy: there is no specific standard of care. It is apparent from the literature
that the problem of conflicting advice and variability of exercise is widespread
(McFarland 1994; McFarland and Burkhart 1999; Maxey and Magnusson 2007;
McGregor et al. 2007; Williamson et al. 2007).
89
In developing the rehabilitation protocol the importance of lumbar stabilisation has been
recognised, however following the direction of McGill, as previously quoted, in that “a
fundamental tenet is that lost mechanical integrity in any load bearing tissue will result
in stiffness losses and an increased risk of unstable behaviour” (McGill et al. 2003:353),
the restoration of normal lumbar spine function is of primary importance.
The standard rehabilitation from Queensland and the WA protocol had in common
exercise for lumbar stabilisation and neural mobility with differing degrees of emphasis.
The WA protocol strongly emphasised the recovery of the disc structure following the
principles of treatment of derangement (McKenzie and May 2003). The results
demonstrated a significant difference in back pain and functional status between the two
groups.
5.5.2 Posture Correction
One of the differences between the WA protocol and the standard rehabilitation
supplied by a physiotherapy practice in Queensland [Appendix 9] was the emphasis
placed on posture correction, especially sitting posture. With the WA cohort instruction
was very specific with supply of a lumbar roll for support and specific instruction as to
type of chair and sitting posture. Sitting was restricted to the time possible to sit
comfortably without exacerbation of back or leg symptoms. Other post-operative
programmes reviewed may have mentioned sitting correctly but without the supply of
lumbar support, written detail of correction, and time rather than symptoms as the
limitation. [Appendices 10 and 14.]
According to the principles of the treatment of derangement as described by McKenzie
and May (2003), following reduction of the derangement, recurrence of symptoms may
be caused by aggravating postures and positions. In the post-surgical application of this
principle it is known that the derangement was posterior or postero-lateral, with flexion
and sitting as aggravating factors.
Toyone et al (2004) found that excision of the herniated disc gave relief of both sciatica
and back pain raising the question as to whether a lumbar disc herniation could be
responsible for low back pain. The emphasis on correction of sitting posture in the WA
group may result in unloading the posterior wall of the disc and may contribute to less
back pain in this cohort as demonstrated in the results (Tables 4.3, 4.4 and Figure 4.1).
90
5.5.3 Recovery of Flexion
Two considerations in the recovery of flexion following surgery are the healing process
of the disc and the effects of flexion on the disc.
Most investigations of the healing process of the disc are in animal models. Ahlgren et
al (2000) investigated direct repair of disc incisions in a sheep model, and found that it
provided no improvement in healing with all anular incisions, repaired or not,
demonstrating significant improvement in pressure-volume test data between two and
four weeks. The incised discs were considerably less able to withstand pressure increase
than the control uninjured discs, 2127 kPa compared to 929 kPa. It is unknown if this
data would alter in the human subject who had the ability to follow instruction and
avoid painful postures.
During the healing process of injured soft tissues, animal studies have shown that stress
reduction through immobilisation impairs healing of fibrous connective tissues
(Provenzano, Martinez, Grindeland et al. 2003) but before remodelling commences with
application of stress, there must be time for the scar to establish with connective tissue
matrix deposition (Diegelmann and Evans 2004). Delay in remodelling can result in an
over abundance of collagen affecting the structure function, and if not enough collagen
is laid down the structure will be weak and may dehisce (Diegelmann and Evans 2004).
Primary intention healing is the formation of a new extracellular matrix with the wound
edges held in close approximation. In wounds that do not approximate the margins heal
with secondary intention, an excess of connective tissue (Diegelmann and Evans 2004).
The final tensile strength of the wound depends on time, vascularity, innervation, and
the contraction of the connective tissue matrix which decreases the wound size and
approximates the wound margins (Mutsaers, Bishop, McGrouther et al. 1997).
In the immediate post-operative period, primary intention healing of the disc and wound
tract may be encouraged by reduction of stress on the posterior elements of the disc and
soft tissues of the back.
During remodelling of the collagen, application of stress is thought to align collagen
fibres parallel to the direction of force influencing the healing process (Mutsaers et al.
1997; Culav, Clark and Merrilees 1999).
91
In the course of examining flexion after lumbar disc surgery, it has been found that
repeating flexion in lying, up to six repetitions, produces lower back pain and, on
occasion, lower limb pain, when applied too early, less than 21 days (unpublished
clinical observation). This clinical information may relate to the initial formation of
new collagen and the matrix, the scar formation, followed by scar remodelling.
While flexion was introduced very cautiously after at least three weeks post-operatively
in the WA cohort, standard rehabilitation introduces flexion earlier with a number of
exercises in the hospital and through the first two weeks (knee rocking, transversus
abdominus exercises in supine, neural mobilisation, single leg and double leg knees to
chest and lumbar slide against a wall). The introduction of flexion early in some
exercise programmes was noted by Williamson (2007).
5.5.4 Effects of Flexion on the Disc
There are several aspects to the effect of flexion on the disc: time of day, change of
structure in response to movement, repetition of movement and sustaining of flexion.
It has been demonstrated that flexion and flexion related postures, such as sitting,
increase intradiscal pressures (Nachemson 1960) and that the direction of nuclear
deformation tends to be directed posteriorly (Shah et al. 1978; Krag et al. 1987; Fennell
et al. 1996; Edmondston et al. 2000; Fazey et al. 2006). Flexion in the immediate post-
operative period may be a factor in poor quality healing of the anular wall and perhaps
on-going back pain and re-herniation.
The timing of the addition of flexion into the rehabilitation protocol is important given
the understanding that during recumbency overnight, nutrition of the disc results in an
increased volume of 10.6% or 0.9cm3 of fluid (De Puky 1935; Malko et al. 2002;
Hutton et al. 2003). Bending stresses on the disc, and to a lesser extent on the ligaments,
increase considerably in the morning (Adams and Hutton 1988), the peak bending
moment probably rises by more than 100% (Adams and Dolan 1995).
Following lumbar microdiscectomy, it is known that damage has previously occurred to
the posterior disc wall and that it is in a state of repair. The factors which are known to
cause anulus failure, axial compression load, bending and twisting, and disc saturation
should be considered in recovery of movement, as when one of these factors is lacking,
failure is more difficult (Lu, Hutton and Gharpuray 1996). Conversely when all of these
factors are present, failure of the disc is more likely. Recovery of flexion was with
92
caution in the WA cohort, following elimination of as many as possible of the known
factors which lead to increase in posterior disc pressure. To assess the readiness of the
patient to commence forward bending after surgery, flexion was tested in lying to
reduce the effects of axial compression load, and after the first four hours of the
patient’s day to allow for a decrease in disc hydration. Once it was established that
flexion could commence they were asked to move in this direction only after noon.
The protocol developed for rehabilitation in the WA cohort was based on the principles
of treatment of derangement as described by McKenzie (McKenzie and May 2003). In
reducing the derangement and maintaining reduction, McKenzie considers correction of
sitting posture essential and advocates the lifetime use of a lumbar support (McKenzie
and May 2003). In the rehabilitation of patients after microdiscectomy, the reduction
had occurred surgically, and in maintaining that reduction, posture correction is
considered equally important as in the non-surgical patient to allow for loss of
proprioception and enable sitting in a neutral lordotic posture. (O'Sullivan et al. 2003;
Dankaerts et al. 2006).
Sitting is considered to be sustained flexion, the degree of flexion depending on the
chair, the amount of support for the lumbar lordosis and the habit of the patient. A
flexed or slouched sitting posture places the lumbar spine into kyphosis displacing the
nucleus posteriorly towards the posterior disc (Shah et al. 1978; Krag et al. 1987;
Fennell et al. 1996; Edmondston et al. 2000) and without support the disc pressure is
40% greater than standing (Nachemson 1976). In the WA cohort, correction of sitting
posture and use of a lumbar support to maintain the lordosis was considered essential,
the lumbar support reducing the load on the intervertebral discs and disc pressure
(Andersson et al. 1975).
In the current study detailed instruction in posture correction in sitting and provision of
an appropriate lumbar support was commenced the day following surgery.
Interruption of sitting on a frequent basis is considered to be important to disc nutrition
(Pynt, Higgs and Mackey 2001) perhaps reducing the effects of creep, described
previously as the “progressive deformation of a structure under constant load that is
below the level of load required to complete tissue failure” (McGill and Brown
1992:43). As creep is dependent on the load applied, the previous loading of the disc
and the state of health of the disc (Adams and Dolan 1995), following lumbar
93
microdiscectomy, when the posterior anular wall is under repair, it would be likely that
the creep required to cause tissue failure must be reduced. Maintaining the lumbar
lordosis and interrupting sitting frequently interrupts the slow deformation of the disc
that is creep (McMillan, Garbutt and Adams 1996).
5.5.5 Repeated Movement
Following the treatment of derangement as described by McKenzie has resulted in the
inclusion of repeated end range extension from the immediate post-operative period
(McKenzie and May 2003). McKenzie describes a directional preference in
determining which direction is used in the treatment, that direction being determined
by examination (McKenzie and May 2003). In the case of the post-surgical patient
that direction was determined by the known posterior derangement, a posterior or
postero-lateral herniation.
In the non-surgical derangement examined into extension there is often a difference in
movement applied singly compared to repeated movement. Having established
directional preference, the effect of repeated end range movement is to reduce and
centralise symptoms regardless of the symptom response to a single movement
(Donelson 2007). Using the experience of treating the non-surgical patient, and the
knowledge that in a normal intervertebral disc positioned into extension the nucleus
tends to deform anteriorly, unloading the damaged posterior anulus (Shah et al. 1978;
Krag et al. 1987; Fennell et al. 1996; Edmondston et al. 2000) the principles of repeated
extension were extrapolated to the patient after lumbar microdiscectomy.
5.6 LIMITATIONS
There are a number of limitations within the current study, which require
acknowledgement.
The design of the study incorporating a contrast group provided difficulties. The
primary neurosurgeon assisted in securing the support of a neurosurgical colleague in
QLD to provide a contrast cohort. The site of the contrast cohort was thousands of
kilometres distant, and without funding visiting the site was not possible.
Communication between the two locations was inconsistent. Identification of potential
research subjects may have been neglected without regular contact from the researcher
reminding the staff of enrolments.
94
Data collection was made more accessible with provision of a website. Of the WA
cohort 25 participants used the website for completing their outcome instruments on at
least one occasion. In the QLD cohort, there was no use of the website. Whether this
access was not explained to the subjects is not known. Ease of data input and collection
may have affected the number of participants who completed the 12 month follow-up.
The QLD cohort was smaller with 12 subjects who completed entry and follow-up
outcome instruments, compared to 47 in the WA cohort.
The contrast cohort was, on average, an older group. The average age of the QLD
cohort was 54, while the average age of the WA cohort was 45. The QLD cohort
included a greater proportion of retired persons. It is unknown if this group were more
or less active than those who participated in the work force. It may have been that
without the pressure to return to work that the retired group were more able to be
compliant with instruction.
Similarly a variety of occupations may have affected the outcome. Given the small
numbers such covariant analysis was not contemplated.
Within the study there were two neurosurgeons, who while equally trained, may have
contributed to differences to the outcome. Such influences as theatre time, recovery
time, pain medication usage during surgery etc was not investigated but are potential
influences on the surgical outcome.
The WA cohort received rehabilitation from a single physiotherapy practice; all in-
patient care provided by one physiotherapist, and outpatient care with one of two
physiotherapists, equally trained and long term collaborators.
The QLD cohort received rehabilitation at an unknown number of providers under the
care of an unknown number of therapists. One practice, at a location close to the
surgeon and often involved in the rehabilitation of his patients, provided a printed
example of standard rehabilitation for the purpose of this study. [Appendix 9.] It is
unknown how widely this protocol was used, nor how closely this was adhered to
within the single practice. Other clinical information may have been included and some
advice may have been omitted with individual patients.
During rehabilitation of the WA cohort, support was provided for the subjects between
office visits in that the therapist was available to answer questions that arose. While not
95
used frequently this support may affect the retention rate of participants. It is unknown
if similar support was offered to the QLD cohort. Such interactions in a research setting
are termed a ‘Hawthorne’ effect, and may have contributed positively to the outcomes
of the WA cohort.
Symptom management can affect retention in a study. If the participant believes that
the rehabilitation is adequate they may be more inclined to complete the study
instruments. This may affect the outcome in that the less satisfied subjects drop out of
the trial.
Coincidentally at the time of the commencement of the study, the neurosurgical practice
in WA implemented insertion of a posterior stabilising device (DIAM, Medtronic USA)
used in conjunction with microdiscectomy. Such patients were excluded from this thesis
cohort. A majority of patients under-going the dual procedure were having second or
subsequent lumbar spine surgery and were ineligible for the study. At the discretion of
the surgeon, some patients with a primary microdiscectomy under-went placement of
the prosthesis. These patients were likely to have suffered a substantial loss of height of
the disc with resultant foraminal stenosis. Without the intervention of the interspinous
prosthesis it is unknown what effect this group would have had on the study outcome.
This trial was not set up as a formal RCT but rather to explore relative outcomes from
two models of rehabilitation following lumbar microdiscectomy. To the extent
reasonable the ‘CONSORT Guidelines’ were observed (Vaarbakken, Ljunggren and
Hendriks 2008).
5.7 SUMMARY
This prospective study involving cohorts in WA and QLD aimed at assessing the
difference in outcome following lumbar microdiscectomy according to specific
rehabilitation protocols. The study intervention involved commencing a novel
rehabilitation protocol the day after lumbar microdiscectomy and a contrast group in
QLD who received standard rehabilitation.
The findings of the study must be viewed with caution as there was no formal control
group and the intervention of surgery is individual in nature and effect. Additionally
two surgeons at different locations performed the surgery.
96
The WA cohort which commenced the exercise protocol the day after surgery reported
significantly less back pain over the 12 month time period of the study. Other major
findings were that the WA cohort demonstrated significant improvement in function at
all time-points and between all time-points except six to 12 months, took less pain
medication and were relatively more satisfied with the outcome of their surgery than the
QLD group.
In regard to the stated limitations of the study, the primary hypothesis of the study was
supported in that there was a difference in outcome following lumbar microdiscectomy
between patients who received early specific rehabilitation compared with those who
received standard practice physiotherapy at another centre, as measured by the
incidence of repeat surgery and data derived from validated self-report spine specific
outcome instruments.
97
CHAPTER 6
CONCLUSION
The primary purpose of this study was to examine for differences in outcome following
lumbar microdiscectomy in patients who receive early specific rehabilitation compared
to those who receive standard rehabilitation at another centre.
The key finding of this study was that commencing the early exercise protocol resulted
in significantly less back pain over the 12 month time period of the study. Other major
findings were that the WA cohort demonstrated significant changes in function at all
time-points and between all time-points except six to 12 months, took less pain
medication and were more satisfied with the outcome of their surgery than the QLD
cohort.
The key conclusions that may be drawn from the current investigation are presented in
terms of primary and secondary outcomes.
6.1 PRIMARY OUTCOME DATA
a) In the WA cohort the largest reduction in pain score for back pain occurred in the
first ten days following surgery (P<.0001) and at all subsequent time-points to 12
months.
b) In the QLD cohort there was no significant change in back pain between time of
surgery and any other time-point.
c) There was significant improvement (P<.0001) in leg pain at all time-points following
surgery in both the WA and QLD cohorts.
d) Data related to functional disability (Roland Morris Questionnaire) demonstrated
significant changes (P <.0001) at each time-point in the WA group.
e) In the QLD group comparison to baseline demonstrated significant differences in
functional disability (P<.0001) at the six and 12 month time-points but not between
each time-point.
98
f) The Queensland group indicated greater impairment of functional disability as
measured by the RMQ at entry, P.0051, while the WA cohort demonstrated greater
improvement in functional disability at 12 months.
6.2 SECONDARY OUTCOME DATA
a) Use of pain medication in WA and QLD cohorts demonstrated a rapid decline in use
at the exit time-point. In the WA group the decline in use continued while in the QLD
group it increased slightly at 12 months.
b) The WA cohort appeared to have a greater level of satisfaction with their outcome
throughout the 12 months, showing a gradual improvement in rate of satisfaction over
the period. The QLD cohort reported a slightly higher level of dissatisfaction at six
months than at the exit point at four weeks.

99
CHAPTER 7
RECOMMENDATIONS
The recommendations emerging from the study reported here relate to rehabilitation
following lumbar microdiscectomy, with considerations for further research.
7.1 REHABILITATION FOLLOWING UNCOMPLICATED LUMBAR
MICRODISCECTOMY (ALONE)
Studies may be undertaken to compare the WA early rehabilitation protocol with a
cohort without post-operative restriction or rehabilitation (Carragee et al. 1996; 1999).
Such studies could employ randomised control studies (RCT) or case control studies
adhering to the ‘CONSORT Guidelines’ (Vaarbakken et al. 2008). The RCT would
require randomisation of the cohort into a group receiving the rehabilitation protocol
while a matched cohort received no post-operative rehabilitation or were not restricted
in activity after surgery.
A case control study would require random allocation after surgery into subjects
receiving the early rehabilitation protocol, or those which did not receive the
rehabilitation protocol.
In either case, RCT or case control, the demographics of the cohort should be defined to
a specific patient population (age, occupation eg 35-50 year old office workers) for
whom a single procedure was performed (microdiscectomy without other intervention).
However a more generally applicable result may be attained by not placing restrictions
on age and occupation.
Studies may be undertaken to compare the effects of restricted and unrestricted activity
after lumbar microdiscectomy. Ahlgren et al (2000) have demonstrated anular repair of
the intervertebral disc in a sheep model, reporting that repair after a box, cruciate or slit
incision did not significantly alter the healing strength, but the box incision did not
demonstrate the significant increase in strength of the cruciate or slit incision after two
weeks. Using an unrepaired slit or cruciate incision in an animal model which behaves
in a more human manner may provide a more realistic example of healing of the disc
after microdiscectomy. The macaque is a primate which has been used in direct
comparison with human spine pathologies and may be suitable for this study (Kramer,
100
Newell-Morris and Simkin 2002; Nuckley, Kramer, Del Rosario et al. 2008). It is
proposed that following surgery one cohort return to all activity in an unrestricted
manner while a second cohort be braced to prevent flexion but allow extension. A third
cohort would not undergo surgery and would serve as a control. In order to assess the
state of healing which has occurred in the WA cohort as they commenced flexion,
histological evidence of quality of repair of the disc in each cohort would be examined
with sequential sacrifice at two weeks, four weeks, six weeks, three months and six
months. Evidence of healing may provide insight into the ideal time to commence
loading the disc with flexion, the mechanical strength assessed with pressure-volume
testing (Panjabi, Brown and Lindahl 1988; Ahlgren et al. 2000).
The quality of the scar tissue may be able to be determined in a human population with
examination of the disc site in cases presenting for surgery following re-herniation.
However this would be a qualitative evaluation with poor validity given the re-
herniation of the anulus.
7.2 EDUCATION
A standard of care could be established for patients after uncomplicated lumbar
microdiscectomy and taught as under-graduate or post-graduate coursework for both
medical students and physiotherapists. Physiotherapy after spinal surgery is a small area
of the total clinical practice available to therapists but it is important if patient outcomes
are to be optimised for this special group. It is equally important that medical
practitioners are familiar with the potential to optimise rehabilitation outcomes of
proven theories.
7.3 CLINICAL PRACTICE GUIDELINES
Research of the literature has revealed a lack of consensus for provision of evidence
based clinical guidelines for rehabilitation of patients after lumbar microdiscectomy
(McGregor et al. 2007; Williamson et al. 2007). It is recommended that a group of
interested rehabilitation specialists be assembled to develop guidelines for rehabilitation
after lumbar microdiscectomy preferably following the completion of a clinical trial
incorporating a control group. This would necessitate locating a surgeon who did not
routinely use any form of post-operative rehabilitation to provide a control group. While
the surgeons in the study may be equally trained, an individual’s operating technique
may contribute to difference in outcome. Other influences including a particular
surgeon’s approach to pain management and patient selection may affect outcome.
101
Therefore covariance analysis would be required to control for inter-surgeon differences
in any planned statistical comparisons. To achieve such statistical controls, full
disclosure regarding duration and severity of symptoms, surgical procedures, operative
time or complications, post-operative management, pain control, surgeon expectations,
and patient instructions, would need to be examined along with other factors deemed
critical in any outcome assessment. Beyond the time of the acute management, life
experiences will influence subsequent outcomes if a long-term follow-up was planned.
Finally, a formal clinical study must ensure blinding of evaluators to minimise
expectations by investigators for bias. The ‘CONSORT Guidelines’ provide all guiding
principles for this type of research (Vaarbakken et al. 2008).
7.4 FURTHER RESEARCH
With regard to further research on rehabilitation following lumbar microdiscectomy it is
recommended that:
Future studies should include more specific questioning regarding return to work which
should include pre-operative plans for days off work after surgery, actual days off post-
operatively because of symptoms, and specific questions for retired and those not in
paid employment: for example questions relating to return to usual household duties,
return to sporting activities (bowls, golf, tennis), and resumption of hobbies
(woodworking, pottery, painting).
Future studies should collect data for assessment of longer term outcomes, two years as
a minimum extending to five years.
Future studies should include more specific questioning regarding use of pain and anti-
inflammatory medication including strength and quantity, period of use and reason for
use of medication. In a study designed to provide prognostic indicators of outcome,
Ostelo et al (2005) perceived recovery and functional status at three and 12 months after
surgery was poorer in the group taking pain medication at baseline (six weeks after
surgery) than in those that did not.
Further research regarding costs associated with the period following surgery including
length of stay in hospital, number of visits for rehabilitation, and number of
consultations with the surgeon for aftercare. Other considerations in the total cost of
care for this cohort include cost of pharmacy, utilisation of other services associated
102
with lumbar problems such as radiology for MRI, CT, x-rays, and procedures such as
facet joint blocks and nerve sleeve injections. Consideration must also be given to the
costs associated with alternative health care and provision of supports and corsets.
Daffner et al (2008) investigated the costs in the 90 days prior to lumbar discectomy
using online data base of insurance records identifying patients by American Medical
Association (AMA) Current Procedural Terminology (CPT) codes. The collection of
this data post-operatively would provide information relating to QALY (Quality
Adjusted Life Year) which is a quality of life assessment. Such study assumes access of
data from insurance, state and federal agencies.
103
REFERENCES
Adams M and Hutton W. Prolapsed intervertebral disc: a hyperflexion injury.Spine 1982; 7: 184-191.
Adams M and Hutton W. The effect of posture on the fluid content of lumbarintervertebral discs. Spine 1983; 8: 665-671.
Adams M and Hutton W. Mechanics of the intervertebral disc. The biology ofthe intervertebral disc. 1988; Ghosh P [ed]. Boca Raton, Florida, CRCPress.2.
Adams M and Dolan P. Recent advances in lumbar spinal mechanics and theirclinical significance. Clinical Biomechanics 1995; 10: 3-19.
Adams M and Dolan P. Time-dependent changes in the lumbar spine'sresistance to bending. Clinical Biomechanics 1996; 11: 194-200.
Adams M, Bogduk N, Burton K, et al. The biomechanics of back pain.2002.Edinburgh, Churchill Livingstone.
Ahlgren B, Lui W, Herkowitz H, et al. Effect of anular repair on healing strengthof the intervertebral disc. A sheep model. Spine 2000; 25: 2165-2170.
Andersen T, Christensen F, Laursen M, et al. Smoking as a predictor ofnegative outcome in lumbar spinal fusion. Spine 2001; 26: 2623-2628.
Anderson J, [Ed]. Grant's atlas of anatomy.1976. Baltimore, Williams &Wilkins.
Andersson B, Ortengren R, Nachemson A, et al. The sitting posture: Anelectromyographic and discometric study. Orthopedic Clinics of NorthAmerica 1975; 6: 105-120.
Andersson B, Murphy R, Ortengren R., et al. The influence of backrestinclination and lumbar support on lumbar lordosis. Spine 1979; 4: 52-58.
Anshel M and Russell K. Effect of aerobic and strength training on paintolerance, pain appraisal and mood of unfit males as a function of painlocation. Journal of Sports Science 1994; 12: 535-547.
Asch H, Lewis P, Moreland D, et al. Prospective multiple outcomes study ofoutpatient lumbar microdiscectomy: should 75 to 80% success rates bethe norm? Journal of Neurosurgery 2002; 96: 34-44.
Ashton I, Roberts S, Jaffray D, et al. Neuropeptides in the human intervertebraldisc. Journal of Orthopaedic Research 1994; 12: 186-192.
Awad J and Moskovich R. Lumbar disc herniations: Surgical versus nonsurgicaltreatment. Clinical Orthopaedics and Related Research 2006; 443:183-197.
Ayotte D, Ito K and Tepic S. Direction dependent resistance to flow in the end-plate of the intervertebral disc: an ex vivo study. Journal of OrthopaedicResearch 2001; 19: 1073-1077.
Battie M, Videman T, Gill K, et al. Smoking and lumbar intervertebral discdegeneration: An MRI study of identical twins. Spine 1991; 16: 1015-1021.
Beadle O. The intervertebral disc: observations on their normal andmorbid anatomy in relation to certain spinal deformities. London,Publisher.1931.
Benneker L, Heini P, Alini M, et al. Vertebral endplate marrow contact channelocclusions and intervertebral disc degeneration. Spine 2005; 30: 167-173.
104
Beurskens A, de Vet H, K'ke A, et al. Measuring the functional status of patientswith low back pain: Assessment of the quality of four disease specificquestionnaires. Spine 1995; 20: 1017-28.
Bogduk N, Tynan W and Wilson A. The nerve supply to the human lumbarintervertebral discs. Journal of Anatomy 1981; 132: 39-56.
Bogduk N, Pearcy M and Hadfield G. Anatomy and biomechanics of psoasmajor. Clinical Biomechanics 1992; 7: 109-119.
Bogduk N. Clinical anatomy of the lumbar spine and sacrum 4thedition.2005. Edinburgh, Elsevier Churchill Livingstone.
Bombardier C. Outcome assessments in the evaluation of treatment of spinaldisorders: Summary and general recommendations. Spine 2000; 25:3100-3103.
Boos N, Weissbach S, Rohrbach H, et al. Classification of age-related changesin lumbar intervertebral discs. Spine 2002; 27: 2631-2644.
Bouter L, van Tulder M and Koes B. Methodologic issues in low back painresearch in primary care. Spine 1998; 23: 2014-2020.
Brennan G, Schultz B, Hood R, et al. The effects of aerobic exercises afterlumbar microdiscectomy. Spine 1994; 19: 735-739.
Brennan G, Shultz B, Hood R, et al. The effects of aerobic exercise after lumbarmicrodiscectomy. Spine 1994; 19: 735-739.
Brinckmann P. Injury of the annulus fibrosus and disc protrusions. An in vitroinvestigation on human lumbar discs. Spine 1986; 11: 149-153.
Broberg K. Slow deformation of intervertebral discs. Journal of Biomechanics1993; 26: 501-512.
Brumagne S, Cordo P, Lysens R, et al. The role of paraspinal muscle spindlesin lumbosacral position sense in individuals with and without low backpain. Spine 2000; 25: 989-994.
Buckwalter J. Aging and degeneration of the human intervertebral disc. Spine1995; 20: 1307-1314.
Burton C, Kirkaldy-Willis W, Yong-Hing K, et al. Causes of failure of surgery onthe lumbar spine. Clinical Orthopedics and Related Research 1981;157: 191-199.
Butler D. Mobilisation of the nervous system.1991. Melbourne, ChurchillLivingstone.
Carragee E, Helms E and O'Sullivan G. Are postoperative activity restrictionsnecessary after posterior lumbar discectomy? A prospective study ofoutcomes in 50 consecutive cases. Spine 1996; 21: 1893-1897.
Carragee E, Han M, Yang B, et al. Activity restrictions after posterior lumbardiscectomy: a prospective study of outcomes in 152 cases with nopostoperative restrictions. Spine 1999; 24: 2346-2351.
Carragee E, Spinnickie A, Alamin T, et al. A prospective controlled study oflimited versus subtotal posterior discectomy: short-term outcomes inpatients with herniated lumbar intervertebral discs and large posterioranular defect. Spine 2006; 31: 653-657.
Casazza B, Young J and Herring S. The role of exercise in the prevention andmanagement of acute low back pain. Occupational Medicine 1998; 13:47-60.
Cassirer. Die tumoren des ruckenmarks. Oppenheims Lehrbuch derNervenkrankheiten 1923; 1: 521.
105
Cleland J, Fritz J and G. B. Predictive validity of initial fear avoidance beliefs inpatients with low back pain receiving physical therapy: is the FABQ auseful screening tool for identifying patients at risk for a poor recovery?European Spine Journal 2008; 17: 70-79.
Copay A, Glassman S, Subach B, et al. The minimum clinically importantdifference in lumbar spine surgery patients: a choice of methods usingthe Oswestry Disability Index, Medical Outcomes Study questionnaireShort Form 36, and Pain Scales. Spine Journal 2008; on-line January.
Coppes M, Marani E, Thomeer R, et al. Innervation of "painful" lumbar discs.Spine 1997; 22: 2342-2349.
Costi J, Stokes I, Gardner-Morse M, et al. Direct measurement of intervertebraldisc maximum shear strain in six degrees of freedom: Motions that placedisc tissue at risk of injury. Journal of Biomechanics 2007; Article inPress, July 2007.
Cotugno D. De ischiade nervosa commentarius: fratres simonios. 1764.Crock H, Goldwasser M and Yoshizawa H. Vascular anatomy related to the
intervertebral disc. The biology of the intervertebral disc. 1988; GhoshP [ed]. Boca Raton, Florida, CRC Press.1.
Culav E, Clark C and Merrilees M. Connective tissues: Matrix composition andits relevance to physical therapy. Physical Therapy 1999; 79: 308-319.
Daffner S, Hymanson H and Wang J. Cost and utilization of conservativemanagement of lumbar disc herniation in patients undergoing surgicaldiscectomy. NASS 23rd Annual Meeting.2008.
Dandy W. A sign and symptom of spinal cord tumors. Archives of Surgery1926; 16: 435-441.
Dandy W. Loose cartilage from intervertebral disk simulating tumor of the spinalcord. Archives of Surgery 1929; 19: 660-672.
Dandy W. Serious complications of ruptured intervertebral discs. Journal of theAmerican Medical Association. 1942; 119: 474-477.
Dankaerts W, O'Sullivan P, Burnett A, et al. Differences in sitting postures areassociated with nonspecific chronic low back pain disorders whenpatients are subclassified. Spine 2006; 31: 698-704.
De Puky P. The physiological oscillation of the length of the body. Acta OrthopScand 1935; 6: 338-347.
Delay B, Smolinski R, Wind W, et al. Current practices and opinions in ACLreconstruction and rehabilitation: results of a survey of the AmericanOrthopaedic Society for Sports Medicine. American Journal of KneeSurgery 2001; Spring 14: 85-91.
den Boer J, Oostendorp R, Beems T, et al. Reduced work capacity after lumbardisc surgery: The role of cognitive-behavioural and work-related riskfactors. Pain 2006; 126: 72-78.
Dewing C, Provencher M, Riffenburgh R, et al. The outcomes of lumbarmicrodiscectomy in a young, active population: correlation by herniationtype and level. Spine 2008; 33: 33-38.
Deyo R, Battie M, Beurskens A, et al. Outcome measures for low back painresearch. A proposal for standardized use. Spine 1998; 23: 2003-2013.
Diegelmann R and Evans M. Wound healing. Frontiers in Bioscience 2004; 9:283-289.
Donaldson B, Shipton E, Inglis G, et al. Comparison of usual surgical adviceversus a nonaggravating six-month gym-based exercise rehabilitation
106
program post-lumbar discectomy: results at one-year follow-up. SpineJournal 2006; 6: 357-363.
Donelson R. Rapidly reversible low back pain.2007. Hanover, NewHampshire, SelfCare First, LLC.
Drake R, Vogl W and Mitchell A, Eds. Gray's anatomy for students.2005.Philadelphia, Elsevier Churchill Livingstone.
Edmondston S, Song S, Bricknell R, et al. MRI evaluation of lumbar spineflexion and extension in asymptomatic individuals. Manual Therapy2000; 5: 158-164.
Edwards W, Zheng Y, Ferrara LA., et al. Structural features and thickness of thevertebral cortex in the thoracolumbar spine. Spine 2001; 26: 218-225.
Eklund J and Corlett N. Shrinkage as a measure of the effect of load on thespine. Spine 1984; 9: 189-194.
Elsberg C. Extradural spinal tumors- primary, secondary, metastatic. Surgery,Gynecology and Obstetrics 1928; 46: 1.
Eyre D. Collagens of the disc. The biology of the intervertebral disc. 1988;Ghosh P [ed]. Boca Raton, CRC Press.1.
Fairbank J, Couper J, Davies J, et al. The Oswestry Low Back Pain DisabilityQuestionnaire. Physiotherapy 1980; 65: 271-73.
Fairbank J and Pynsent P. The Oswestry Disability Index (Literature review).Spine 2000; 25: 2940-2953.
Falconer M, McGeorge M and Begg A. Observations on the cause andmechanism of symptom-production in sciatica and low-back pain.Journal of Neurology, Neurosurgery and Psychiatry. 1948; 11: 13-26.
Farfan H, Cossette J, Robertson G, et al. The effects of torsion on the lumbarintervertebral joints: The role of torsion in the production of discdegeneration. Journal of Bone and Joint Surgery 1970; 52(A): 468-497.
Fazey P, Song S, Monsas A, et al. An MRI investigation of intervertebral discformation in response to torsion. Clinical Biomechanics 2006; 21: 538-542.
Fennell A, Jones A and Hukins D. Migration of the nucleus pulposus within theintervertebral disc during flexion and extension of the spine. Spine 1996;21: 2753-2757.
Ferguson S, Ito K and Nolte L. Fluid flow and convective transport of soluteswithin the intervertebral disc. Journal of Biomechanics 2004; 37: 213-221.
Filiz M, Cakmak A and Ozcan E. The effectiveness of exercise programmesafter lumbar disc surgery: a randomised controlled study. ClinicalRehabilitation. 2005; 19: 4-11.
Fisher C, Noonan V, Bishop P, et al. Outcome evaluation of the operativemanagement of lumbar disc herniation causing sciatica. Neurosurgery(Spine) 2004; 100: 317-324.
Fritsch E, Heisel J and Rupp S. The failed back surgery syndrome: reasons,intra operative findings, and long term results: a report of 182 operativetreatments. Spine 1996; 21: 626-633.
Gill K and Callaghan M. The measurement of lumbar proprioception inindividuals with and without low back pain. Spine 1998; 23: 371-377.
107
Gillan M, Ross J, McLean I, et al. The natural history of trunk list, its associateddisability and the influence of McKenzie management. European SpineJournal 1998; 7: 480-483.
Gowers W and Horsley V. A case of tumour of the spinal cord; removal;recovery. Medico-chirurgical Transactions 1888; 2nd s: 377-428.
Groen G, Baljet B and Drukker J. Nerves and nerve plexuses of the humanvertebral column. American Journal of Anatomy 1990; 188: 282-296.
Grunhagen T, Wilde G, Soukane D, et al. Nutrient supply and intervertebral discmetabolism. Journal of Bone and Joint Surgery 2006; 88(A): 30-35.
Haefeli M and Elfering A. Pain assessment. European Spine Journal 2006;15: S17-S24.
Hagg O, Fritzell P and Nordwall A. The clinical importance of changes inoutcome scores after treatment for chronic low back pain. EuropeanSpine Journal 2003; 12: 12-20.
Hazard R. Failed back surgery syndrome: Surgical and nonsurgicalapproaches. Clinical Orthopaedics and Related Research 2006; 443:228-232.
Hides J, Richardson C and Jull G. Multifidus muscle recovery is not automaticafter resolution of acute first episode low back pain. Spine 1996; 21:2763-2769.
Hodges P, Heijnen I and Gandevia S. Postural activity of the diaphragm isreduced in humans when respiratory demand increases. The Journal ofPhysiology 2001; 537: 999-1008.
Hudak P and Wright J. The characteristics of patient satisfaction measures.Spine 2000; 25: 3167-3177.
Hukins D. Disc structure and function. The biology of the intervertebral disc.1988; Ghosh P [ed]. Boca Raton Florida, CRC Press.1.
Hutton W, Malko J and Fajman W. Lumbar disc volume measured by MRI:effects of bed rest, horizontal exercise and vertical loading. AviationSpace and Environmental Medicine 2003; 74: 73-78.
Hyodo H, Sato T, Sasaki H, et al. Discogenic pain in acute nonspecific low-backpain. European Spine Journal 2005; 14: 573-577.
Ikari C. A study of the mechanism of low-back pain. The neurohistologicalexamination of the disease. Journal of Bone and Joint Surgery (A)1954; 36: 195.
Jaeschke R, Singer J and Guyatt G. Measurement of health status.Ascertaining the minimal clinically important difference. Control ClinTrials 1989; 10: 407-415.
Jarvinen T, Jarvinen T, Kaariainen M, et al. Muscle injuries: optimising recovery.Best Pract Res Clin Rheumatol 2007; 21: 317-331.
Jemmett R, MacDonald D and Agur A. Anatomical relationships betweenselected segmental muscles of the lumbar spine in the context of multi-planar segmental motion: a preliminary investigation. Manual Therapy2004; 9: 203-210.
Jorgensen K, Mag C, Nicholaisen T, et al. Muscle fibre distribution, capillarydensity and enzymatic activities in the lumbar paravertebral muscles ofyoung men. Significance for isometric endurance. Spine 1993; 18: 1439-1450.

108
Kara B, Tulum Z and Acar U. Functional results and the risk factors ofreoperations after lumbar disc surgery. European Spine Journal 2005;14: 43-48.
Katz M, Hargens A and Garfin S. Intervertebral disc nutrition diffusion versusconvection. Clinical Orthopedics and Related Research 1986; 210:243-245.
Kelly A-M. The minimum clinically significant difference in visual analogue scalepain score does not differ with severity of pain. Emergency MedicineJournal 2001; 18: 205-207.
Kjellby-Wendt G and Styf J. Early active training after lumbar discectomy. Aprospective, randomised and controlled study. Spine 1998; 23: 2345-2351.
Kjellby-Wendt G and Styf J. Results of early active rehabilitation 5-7 years aftersurgical treatment for lumbar disc herniation. Journal of SpinalDisorders and Techniques 2002; 15: 404-409.
Kocher T. Die verletzun der wirbelsaule zugleich als beitrag zur physiologie demenschlichen. Ruckenmarke. Mitt. a. d. Grenzgeb. d. Med. u. Chir.1896; 1: 415.
Kotilainen E. Long-term outcome of patients suffering from clinical instabilityafter microsurgical treatment of lumbar disc herniation. ActaNeurochirurgia 1998; 140: 120-125.
Krag M, Seroussi R, Wilder D, et al. Internal displacement distribution from 'invitro' loading of the human thoracic and lumbar spinal motion segments:experimental result and theoretical predictions. Spine 1987; 12: 1001-1007.
Krag M, Cohen M, Haugh L, et al. Body height change during upright andrecumbent posture. Spine 1990; 15: 202-207.
Kramer J. Intervertebral disk diseases. Causes, diagnosis, treatment andprophylaxis.1990. New York, Thieme Medical Publishers, Inc.
Kramer P, Newell-Morris L and Simkin P. Spinal degenerative disk disease(DDD) in female macaque monkeys: epidemiology and comparison withwomen. Journal of Orthopaedic Research 2002; 20: 399-408.
Krismer M, Haid C, Behensky H, et al. Motion in lumbar functional spine unitsduring side bending and axial rotation moments depending on the degreeof degeneration. Spine 2000; 25: 2020-2027.
Kuslich S, Ulstrom C and Michael C. The tissue origin of low back pain andsciatica: A report of pain response to tissue stimulation during operationson the lumbar spine using local anaesthesia. Orthopedic Clinics ofNorth America 1991; 22: 181-187.
Larsen K, Flemming W and Leboeuf-Yde C. Can passive prone extensions ofthe back prevent back problems? A randomised, controlled interventiontrial of 314 military conscripts. Spine 2002; 27: 2747-2752.
Le Vay D. The history of orthopaedics.1990. Carforth, U.K., Parthenon.Leinonen V, Kankaanpaa M, Luukkonen M, et al. Lumbar paraspinal muscle
function, perception of lumbar position, and postural control in discherniation related back pain. Spine 2003; 28: 842-848.
Little D and MacDonald D. The use of the percentage change in oswestrydisability index score as an outcome measure in lumbar spine surgery.Spine 1994; 19: 2139-43.
109
Little J and Khalsa P. Human lumbar spine creep during cyclic and staticflexion: Creep rate, biomechanics, and facet joint capsule strain. Annulsof Biomedical Engineering 2005; 33: 391-401.
Lonn J, Glomsrod B, Soukup M, et al. Active back school: Prophylacticmanagement for low back pain: A randomized, controlled, 1-year follow-up study. Spine 1999; 24: 864- 871.
Lorio M, Bernstein A and Simmons E. Sciatic spinal deformity- lumbosacral list:An "unusual" presentation with review of the literature. Journal of SpinalDisorders 1995; 8: 201-205.
Lu Y, Hutton W and Gharpuray V. Do bending, twisting, and diurnal fluidchanges in the disc affect the propensity to prolapse? A viscoelastic finiteelement model. Spine 1996; 21: 2570-2579.
Macewen W. Trephining of the spine for paraplegia. Glasgow Medical Journal1884; 4s: 55-58.
Macewen W. Two cases in which excision of the laminae of portions of thespinal vertebrae had been performed in order to relieve pressure on thespinal cord causing paraplegia. Glasgow Medical Journal. 1885; 4s:210-212.
Macintosh J, Valencia F, Bogduk N, et al. The morphology of the human lumbarmultifidus. Clinical Biomechanics 1986; 1: 196-204.
Main C and Spanswick C. Pain management; an interdisciplinaryapproach.2000, Churchill Livingstone.
Maitland G. Vertebral Manipulation.1964. London, Butterworths.Maitland G. Vertebral Manipulation.1968. London, Butterworths.Malinsky J. The ontogenetic development of nerve terminations in the
intervertebral discs of man. Acta Anat 1959; 38: 96-113.Malko J, Hutton W and Fajman W. An in vivo MRI study of the vertebral
changes in volume (and fluid content) of the lumbar intervertebral discafter overnight bed rest and during an 8-hour walking protocol. Journalof Spinal Disorders and Techniques 2002; 15: 157-163.
Malone Q. 2003; Consultant neurosurgeon. Centre for Neurological Surgery.West Perth. Western Australia. Personal communication.
Manniche C, Skall H and Braendholt L, et al. Clinical trial of postoperativedynamic back exercises after first lumbar discectomy. Spine 1993; 18:92-97.
Maroon J. Current concepts in minimally invasive discectomy. Journal ofNeurosurgery 2002; 51: S2-137-S2-145.
Maroudas A. Nutrition and metabolism of the intervertebral disc. The biology ofthe intervertebral disc. 1988; Ghosh P [ed]. Boca Raton, Florida, CRCPress, Inc.Volume 2.
Mathews J. Epidurography-A technique for diagnosis and research.1976.Edinburgh, Churchill Livingstone.
Maxey L and Magnusson J, Eds. Rehabilitation for the post-surgicalorthopedic patient.2007. St Louis, Elsevier.
Mayer T, McMahon M, Gatchel R, et al. Socioeconomic outcomes of combinedspine surgery and functional restoration in workers' compensation spinaldisorders with matched controls. Spine 1998; 23: 598-605.
McDevitt C. Proteoglycans of the intervertebral disc. The biology of theintervertebral disc. 1988; Ghosh P [ed]. Boca Raton, CRC Press.1.
110
McFarland C. Considerations for physical therapy management of thepostoperative spine patient. Orthopaedic Practice 1994; 6: 8-11.
McFarland C and Burkhart D. Rehabilitation protocols for surgical andnonsurgical procedures.1999. Berkeley, California, North AtlanticBooks.
McGill S and Brown S. Creep response of the lumbar spine to prolonged fullflexion. Clinical Biomechanics 1992; 7: 43-46.
McGill S, Juker D and Kropf P. Quantitative intramuscular myoelectric activity ofquadratus lumborum during a wide variety of tasks. ClinicalBiomechanics 1996; 11: 170-172.
McGill S, Grenier S, Kavcic N, et al. Coordination of muscle activity to assurestability of the lumbar spine. Journal of Electromyography andKinesiology 2003; 13: 353-359.
McGregor AH, Burton AK and Sell P. The development of an evidence-basedpatient booklet for undergoing lumbar discectomy and un-instrumenteddecompression. European Spine Journal 2007; 16: 339-346.
McKenzie R. Manual correction of sciatic scoliosis. New Zealand MedicalJournal 1972; 76: 194-199.
McKenzie R. Prophylaxis in recurrent low back pain. New Zealand MedicalJournal 1979; 89: 22-23.
McKenzie R. The Lumbar Spine. Mechanical Diagnosis and Therapy.1981,Spinal Publications.
McKenzie R and May S. The Lumbar Spine Mechanical Diagnosis andTreatment.2003, Spinal Publications New Zealand Ltd.
McMillan D, Garbutt G and Adams M. Effect of sustained loading on the watercontent of intervertebral discs: implications for disc metabolism. AnnRheum Dis 1996; 55: 880-887.
McNally D, Adams M and Goodship A. Can intervertebral disc prolapse bepredicted by disc mechanics? Spine 1993; 18: 1525-1530.
Mixter W and Barr J. Rupture of the intervertebral disc with involvement of thespinal canal. New England Journal of Medicine 1934; 211: 210-214.
Moneta G, Videman T, Kaivanto K, et al. Reported pain during lumbardiscography as a function of anular ruptures and disc degeneration.Spine 1994; 19: 1968-1974.
Moore K and Dalley A. Clinically oriented anatomy.2006, Lippincott Williams& Wilkins.
Moore R. The vertebral end-plate: what do we know? European Spine Journal2000; 9: 92-96.
Morgan F and King T. Primary instability of lumbar vertebrae as a commoncause of low back pain. Journal of Bone and Joint Surgery 1957;39(B): 6-22.
Mutsaers S, Bishop J, McGrouther G, et al. Mechanisms of tissue repair: fromwound healing to fibrosis. The International Journal of Biochemistry &Cell Biology 1997; 29: 5-17.
Nachemson A. Lumbar intradiscal pressure. Acta Orth. Scand 1960; Suppl 43.Nachemson A. The lumbar spine: an orthopaedic challenge. Spine 1976; 1: 59-
69.Netter F. Atlas of human anatomy.2003. Teterboro, New Jersey, Icon
Learning Systems.
111
Nuckley D, Kramer P, Del Rosario A, et al. Intervertebral disc degeneration in anaturally occurring primate model: radiographic and biomechanicalevidence. Journal of Orthopaedic Research 2008; 26: 1283-1288.
O'Connell J. Protrusions of the lumbar intervertebral discs. A clinical reviewbased on five hundred cases treated by excision of the protrusion.Journal of Bone and Joint Surgery 1951; 33 (B): 8-30.
O'Driscoll S and Giori N. Continuous passive motion (CPM): theory andprinciples of clinical application. Journal of Rehabilitation Researchand Development 2000; 37: 179-188.
O'Sullivan P, Twomey L and Allison G. Dysfunction of the neuromuscularsystem in the presence of low back pain- implications for physicaltherapy management. Journal of Manual and Manipulative Therapy1997; 5: 20-26.
O'Sullivan P. Lumbar segmental 'instability': clinical presentation and specificstabilizing exercise management. Manual Therapy 2000; 5: 2-12.
O'Sullivan P, Burnett A, Floyd A, et al. Lumbar repositioning deficit in a specificlow back pain population. Spine 2003; 28: 1074-1079.
Oliver M and Twomey L. Extension creep in the lumbar spine. ClinicalBiomechanics 1995; 10: 363-368.
Ostelo R, de Vet H, Waddell G, et al. Rehabilitation after lumbar disc surgery.Cochrane Database Syst Rev 2 2002.
Ostelo R, de Vet H, Knol D, et al. 24- item Roland-Morris DisabilityQuestionnaire was preferred out of six functional status questionnairesfor post-lumbar disc surgery. Journal of Clinical Epidemiology 2004;57: 268-276.
Ostelo R, Vlaeyen J, van den Brandt P, et al. Residual complaints followinglumbar disc surgery: prognostic indicators of outcome
. Pain 2005; 114: 177-185.Palmgren T, Gronblad M, Virri J, et al. An immunohistochemical study of nerve
structures in the anulus fibrosus of human normal lumbar intervertebraldiscs. Spine 1999; 24: 2075-2081.
Panjabi M, Brown M and Lindahl S. Intrinsic disc pressure as a measure ofintegrity of the lumbar spine. Spine 1988; 13: 913-917.
Parisien R and Ball P. Historical perspective William Jason Mixter (1880-1958):Ushering in the "dynasty of the disc". (Historical perspective). Spine1998; 23: 2363-2366.
Penning L. Psoas muscle and lumbar spine stability: a concept uniting existingcontroversies. Critical review and hypothesis. European Spine Journal2000; 9: 577-585.
Porter R and Miller C. Back pain and trunk list. Spine 1986; 11: 596-600.Provenzano P, Martinez D, Grindeland R, et al. Hindlimb unloading alters
ligament healing. Journal of Applied Physiology 2003; 94: 314-324.Puolakka K, Ylinen J, Neva M, et al. Risk factors for back pain-related loss of
work time after surgery for lumbar disc herniation: a 5-year follow-upstudy. European Spine Journal 2008; 17: 386-392.
Pynt J, Higgs J and Mackey M. Seeking the optimal posture of the seatedlumbar spine. Physiotherapy Theory and Practice 2001; 17: 5-21.
Quint U, Wilke H, Shiraz-Adl A, et al. Importance of the intersegmental trunkmuscles for the stability of the lumbar spine: a biomechanical study invitro. Spine 1998; 23: 1937-1945.
112
Rabischong P, Louis R, Vignaud J, et al. The intervertebral disc. Anat Clin1978; 1: 55-54.
Rajasekaran S, Babu J, Arun R, et al. A study of diffusion in human lumbardiscs: A serial magnetic resonance imaging study documenting theinfluence of the endplate on diffusion in normal and degenerate discs.Spine 2004; 29: 2654-2667.
Rantanen J, Hurme M and Falck B. The lumbar multifidus muscle five yearsafter surgery for a lumbar intervertebral disc herniation. Spine 1993; 18:568-574.
Reilly T, Tyrell A and Troup J. Circadian variation in human stature. ChronobiolInt 1984; 1: 121-126.
Richardson C, Jull G, Hodges P, et al. Therapeutic Exercise for SpinalSegmental Stabilisation in Low Back Pain.1999, Churchill Livingstone.
Riches P, Dhillon N, Lotz J, et al. The internal mechanics of the intervertebraldisc under cyclic loading. Journal of Biomechanics 2002; 35: 1263-1271.
Roberts S, Menage J and Urban J. Biochemical and structural properties of thecartilage end-plate and its relation to the intervertebral disc. Spine 1989;14: 166-174.
Roberts S, Eisenstein S, Menage J, et al. Mechanoreceptors in intervertebraldiscs. Morphology, distribution, and neuropeptides. Spine 1995; 20:2645-2651.
Roberts S, Urban J, Evans H, et al. Transport properties of the human cartilageendplate in relation to its composition and calcification. Spine 1996; 21:415-420.
Roberts S. Disc morphology in health and disease. Biochemical SocietyTransactions 2002; 30: 864-869.
Roberts S, Evans H, Trivedi J, et al. Histology and pathology of the humanintervertebral disc. Journal of Bone and Joint Surgery (A) 2006; 88:10-14.
Roland M and Morris R. A study of the natural history of back pain. Part 1:Development of a reliable and sensitive measure of disability in low backpain. Spine 1983; 8: 141-144.
Roland M and Fairbank J. The Roland-Morris Disability Questionnaire and theOswestry Disability Questionnaire. Spine 2000; 25: 3115-3124.
Roofe P. Innervation of the annulus fibrosus and posterior longitudinal ligament.Archives of Neurological Psychiatry 1940; 44: 100.
Ross J, Robertson J, Frederickson R, et al. Association between peridural scarand recurrent radicular pain after lumbar discectomy: magneticresonance evaluation. Journal of Neurosurgery 1996; 38: 855-863.
Sackett D, Rosenberg W, Gray J, et al. Evidence based medicine: what it is andwhat it isn't: It's
about integrating individual clinical expertise and the best external evidence.British Medical Journal 1996; 312: 71-72.
Salter R and Field P. The effects of continuous compression on living cartilage.An experimental investigation. Journal of Bone and Joint Surgery (A)1960; 42: 31-49.
Salter R. Motion vs Rest. Why immobilise joints? Journal of Bone and JointSurgery (B) 1982; 64: 251-254.
113
Sapsford R, Hodges P, Richardson C, et al. Co-activation of the abdominal andpelvic floor muscles during voluntary exercise. Neurourology andUrodynamics 2001; 20: 31-42.
Sato K, Kikuchi S and Yonezawa T. In vivo intradiscal pressure measurement inhealthy individuals and in patients with on-going back problems. Spine1999; 24: 2468-2474.
Scarff J. Fifty years of neurosurgery. Int. Abstr. Surgery 1955; 101: 417-513.Schaller B. Failed back surgery syndrome: the role of symptomatic segmental
single level instability after lumbar microdiscectomy. European SpineJournal 2004; 13: 193-198.
Schmorl G and Junghanns H. The human spine in health and disease.1959.New York and London, Grune and Stratton.
Schollmeier G, Lahr-Eigen R and Lewandrowski K-U. Observations on fiber-forming collagens in the anulus fibrosus. Spine 2000; 25: 2736-2741.
Schultze. Zur diagnostik und behandlung der ruckenmarkshautgeschwulste.Mitt. Grenzgeb. Med. Chir. 1903; 12.
Shah J, Hampson W and Jayson M. The distribution of surface strain in thecadaveric lumbar spine. Journal of Bone and Joint Surgery (B) 1978;60: 246-251.
Singer A and Clark A. Cutaneous Wound Healing. New England Journal ofMedicine 1999; 341: 738-746.
Skaf G, Bouclaous C., Alaraj A., et al. Clinical outcome of surgical treatment offailed back surgery syndrome. Surgical Neurology 2005; 64: 483-489.
Spencer T. 2007; Physiotherapist. Spencer & Associates. Brisbane.Queensland. Personal communication.
Stilwell D. The nerve supply of the vertebral column and associated structuresin the monkey. Anatomical Record 1956; 125: 139-169.
Stokes I and Windisch L. Vertebral height growth predominates overintervertebral disc growth in adolescents with scoliosis. Spine 2006; 31:1600-1604.
Stratford P, Binkley J and Solomon P, et al. Assessing change over time inpatients with low back pain. Physical Therapy 1994; 74: 528-533.
Swinkels A and Dolan P. Regional assessment of joint position sense in thespine. Spine 1998; 23: 590-597.
Taylor J. Growth of human intervertebral discs and vertebral bodies. Journal ofAnatomy 1975; 120: 49-68.
Taylor J and Twomey L. Innervation of lumbar intervertebral discs. MedicalJournal of Australia 1979; 2: 701-702.
Taylor J and Twomey L. The development of the human intervertebral disc. The biology of the intervertebral disc. 1988; Ghosh P [ed], CRC Press.1.Taylor J and Twomey L. The development of the human intervertebral disc. The
biology of the intervertebral disc. 1988; Ghosh P [ed], CRC Press.1.Thomas J and France C. The relationship between pain related fear and lumbar
flexion during natural recovery from low back pain. European SpineJournal 2008; 17: 97-103.
Thongtrangan I, Le H, Park J, et al. Minimally invasive spinal surgery: ahistorical perspective. Neurosurgical Focus 2004; 16: 1-10.
Toyone T, Tanaka T, Kato D, et al. Low back pain following surgery for lumbardisc herniation. Journal of Bone and Joint Surgery 2004; 86 (A): 893-896.
114
Tullberg T, Isacson J and Weidenhielm L. Does microscopic removal of lumbardisc herniation lead to better results than the standard procedure? Resultof a one-year randomized study. Spine 1993; 18: 24-27.
Twomey L and Taylor J. Age changes in lumbar intervertebral discs. Acta Orth.Scand 1985; 56: 496-499.
Twomey L, Taylor J and Oliver M. Sustained flexion loading, rapid extensionloading of the lumbar spine, and the physical therapy of related injuries.Physiotherapy Practice 1988; 4: 129-138.
Tyrell A, Reilly T and Troup J. Circadian variation in stature and the effects ofspinal loading. Spine 1985; 10: 161-164.
Urban J and McMullin J. Swelling pressure of the lumbar intervertebral discs:Influence of age, spinal level and degeneration. Spine 1988; 13: 179-187.
Urban J and Roberts S. Degeneration of the intervertebral disc. ArthritisResearch and Therapy 2003; 5: 120-130.
Vaarbakken K, Ljunggren A and Hendriks E. The importance of the newCONSORT Statement for clinicians. Australian Journal ofPhysiotherapy 2008; 54: 155-156.
Vanharanta H, Sachs B and Spivey M. The relationship of pain provocation tolumbar disc deterioration as seen by CT/discography. Spine 1987; 12:295-298.
Vernon-Roberts B. Pathology of degenerative spondylosis.1976. Edinburgh,Churchill Livingstone.
Vernon-Roberts B. Disc pathology and disease states. The biology of theintervertebral disc. 1988; Ghosh P [ed]. Boca Raton, Florida., CRCPress.2.
Von Korff M, Jensen M and Karoly P. Assessing global pain by self-report inclinical and health services research. Spine 2000; 25: 3140-3151.
Waddell G, Newton M, Somerville D, et al. A fear avoidance beliefsquestionnaire (FABQ) and the role of fear avoidance beliefs in chroniclow back pain and disability. Pain 1993; 52: 157-168.
Warwick R and Williams P, Eds. Gray's Anatomy.1973. Philadelphia,W.B.Saunders.
Wenger K and Schlegel J. Annular bulge contours from an axialphotogrammetric method. Clinical Biomechanics 1997; 12: 438-444.
Wetzel F and Donelson R. The role of repeated end-range/pain responseassessment in the management of symptomatic lumbar discs. The SpineJournal 2003; 3: 146-154.
Wiberg G. Back pain in relation to the nerve supply of the intervertebral disc.Acta Orth Scand 1949; 19: 211-221.
Wilke H-J, Neef P, Caimi M, et al. New in vivo measurements of pressures inthe intervertebral disc in daily life. Spine 1999; 24: 755-762.
Williams P, [Ed]. Gray's Anatomy.1995. New York, Churchill Livingstone.Williamson E, White L and Rushton A. A survey of post-operative management
for patients following first time lumbar discectomy. European SpineJournal 2007; 16: 795-802.
Yorimitsu E, Chiba K, Toyama Y, et al. Long-term outcomes of standarddiscectomy for lumbar disc herniation: a follow -up study of more than 10years. Spine 2001; 26: 652-7.
115
Yoshizawa H, O'Brien J, Smith W, et al. The neuropathology of intervertebraldiscs removed for low back pain. Journal of Pathology 1980; 132: 95-104.
116
APPENDIX 1
Approval from the Human Research Ethics Committee for study of outcomes of earlyrehabilitation following lumbar microdiscectomy.


118
APPENDIX 2
Outcome measure of functional disability for phase one of the study, Oswestry
Disability Index.
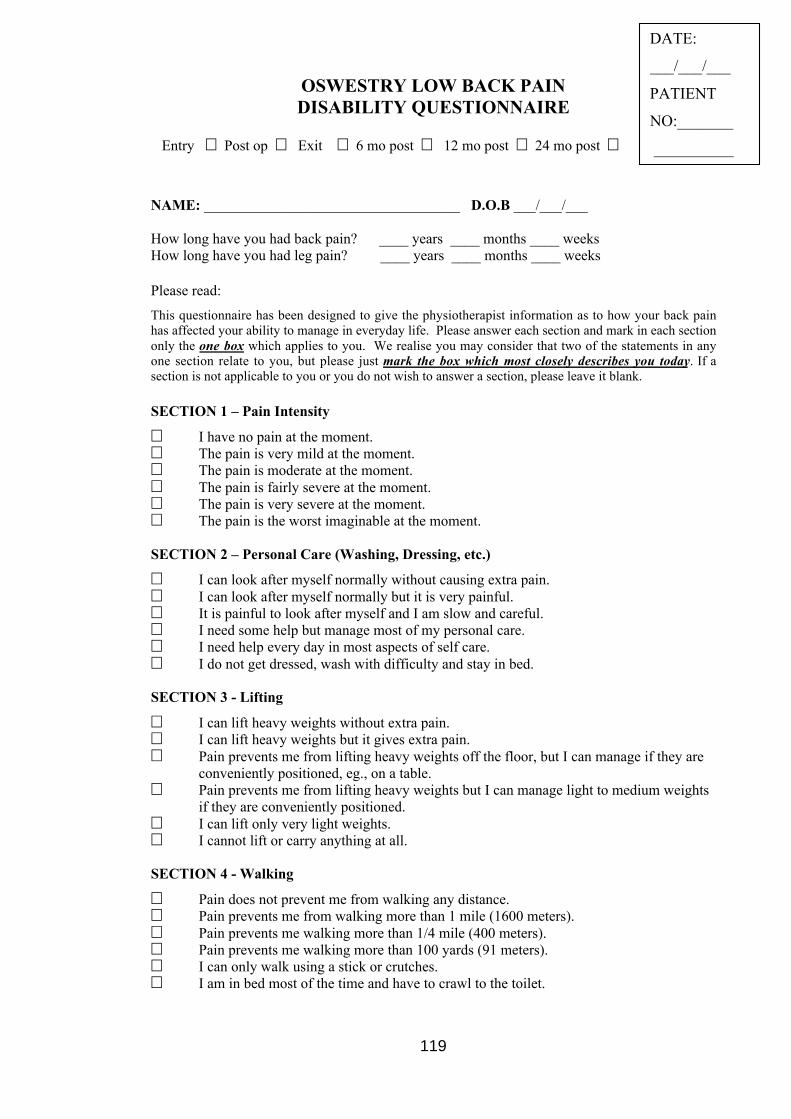
119
OSWESTRY LOW BACK PAINDISABILITY QUESTIONNAIRE
Entry � Post op � Exit � 6 mo post � 12 mo post � 24 mo post �
NAME: ___________________________________ D.O.B ___/___/___
How long have you had back pain? ____ years ____ months ____ weeksHow long have you had leg pain? ____ years ____ months ____ weeks
Please read:
This questionnaire has been designed to give the physiotherapist information as to how your back painhas affected your ability to manage in everyday life. Please answer each section and mark in each sectiononly the one box which applies to you. We realise you may consider that two of the statements in anyone section relate to you, but please just mark the box which most closely describes you today. If asection is not applicable to you or you do not wish to answer a section, please leave it blank.
SECTION 1 – Pain Intensity
� I have no pain at the moment.� The pain is very mild at the moment.� The pain is moderate at the moment.� The pain is fairly severe at the moment.� The pain is very severe at the moment.� The pain is the worst imaginable at the moment.
SECTION 2 – Personal Care (Washing, Dressing, etc.)
� I can look after myself normally without causing extra pain.� I can look after myself normally but it is very painful.� It is painful to look after myself and I am slow and careful.� I need some help but manage most of my personal care.� I need help every day in most aspects of self care.� I do not get dressed, wash with difficulty and stay in bed.
SECTION 3 - Lifting
� I can lift heavy weights without extra pain.� I can lift heavy weights but it gives extra pain.� Pain prevents me from lifting heavy weights off the floor, but I can manage if they are
conveniently positioned, eg., on a table.� Pain prevents me from lifting heavy weights but I can manage light to medium weights
if they are conveniently positioned.� I can lift only very light weights.� I cannot lift or carry anything at all.
SECTION 4 - Walking
� Pain does not prevent me from walking any distance.� Pain prevents me from walking more than 1 mile (1600 meters).� Pain prevents me walking more than 1/4 mile (400 meters).� Pain prevents me walking more than 100 yards (91 meters).� I can only walk using a stick or crutches.� I am in bed most of the time and have to crawl to the toilet.
DATE:
___/___/___
PATIENT
NO:_______
__________
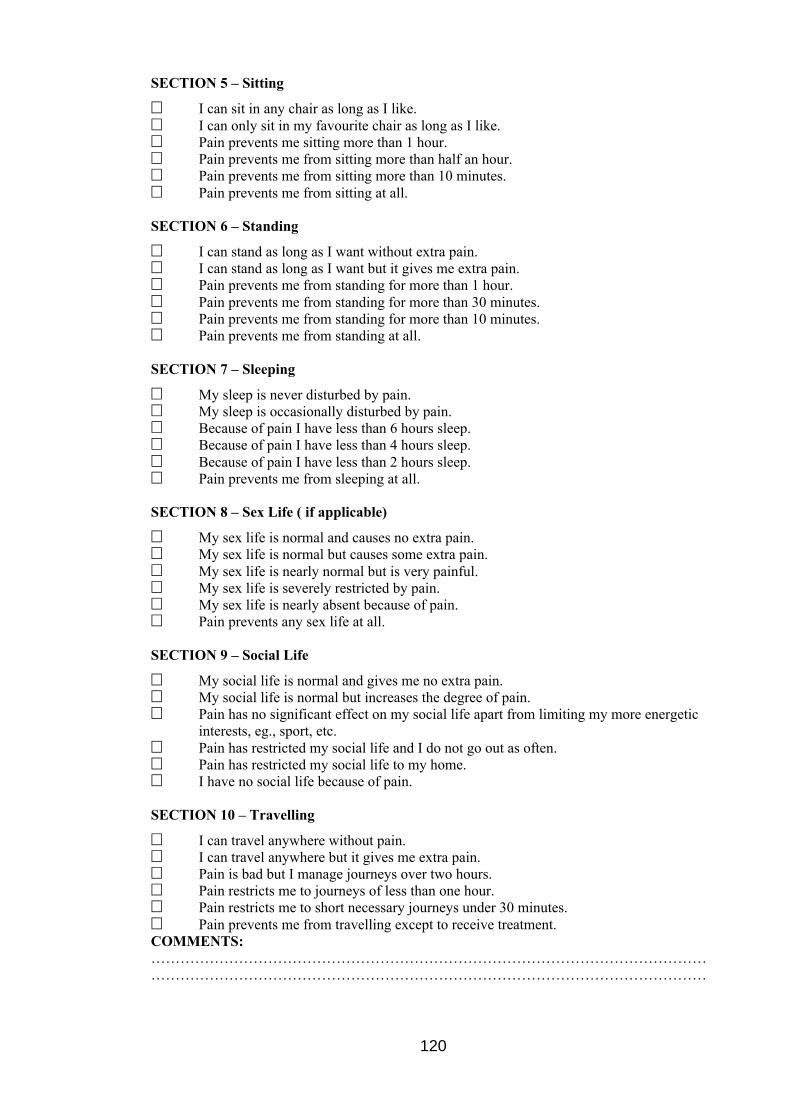
120
SECTION 5 – Sitting
� I can sit in any chair as long as I like.� I can only sit in my favourite chair as long as I like.� Pain prevents me sitting more than 1 hour.� Pain prevents me from sitting more than half an hour.� Pain prevents me from sitting more than 10 minutes.� Pain prevents me from sitting at all.
SECTION 6 – Standing
� I can stand as long as I want without extra pain.� I can stand as long as I want but it gives me extra pain.� Pain prevents me from standing for more than 1 hour.� Pain prevents me from standing for more than 30 minutes.� Pain prevents me from standing for more than 10 minutes.� Pain prevents me from standing at all.
SECTION 7 – Sleeping
� My sleep is never disturbed by pain.� My sleep is occasionally disturbed by pain.� Because of pain I have less than 6 hours sleep.� Because of pain I have less than 4 hours sleep.� Because of pain I have less than 2 hours sleep.� Pain prevents me from sleeping at all.
SECTION 8 – Sex Life ( if applicable)
� My sex life is normal and causes no extra pain.� My sex life is normal but causes some extra pain.� My sex life is nearly normal but is very painful.� My sex life is severely restricted by pain.� My sex life is nearly absent because of pain.� Pain prevents any sex life at all.
SECTION 9 – Social Life
� My social life is normal and gives me no extra pain.� My social life is normal but increases the degree of pain.� Pain has no significant effect on my social life apart from limiting my more energetic
interests, eg., sport, etc.� Pain has restricted my social life and I do not go out as often.� Pain has restricted my social life to my home.� I have no social life because of pain.
SECTION 10 – Travelling
� I can travel anywhere without pain.� I can travel anywhere but it gives me extra pain.� Pain is bad but I manage journeys over two hours.� Pain restricts me to journeys of less than one hour.� Pain restricts me to short necessary journeys under 30 minutes.� Pain prevents me from travelling except to receive treatment.COMMENTS:…………………………………………………………………………………………………………………………………………………………………………………………………………
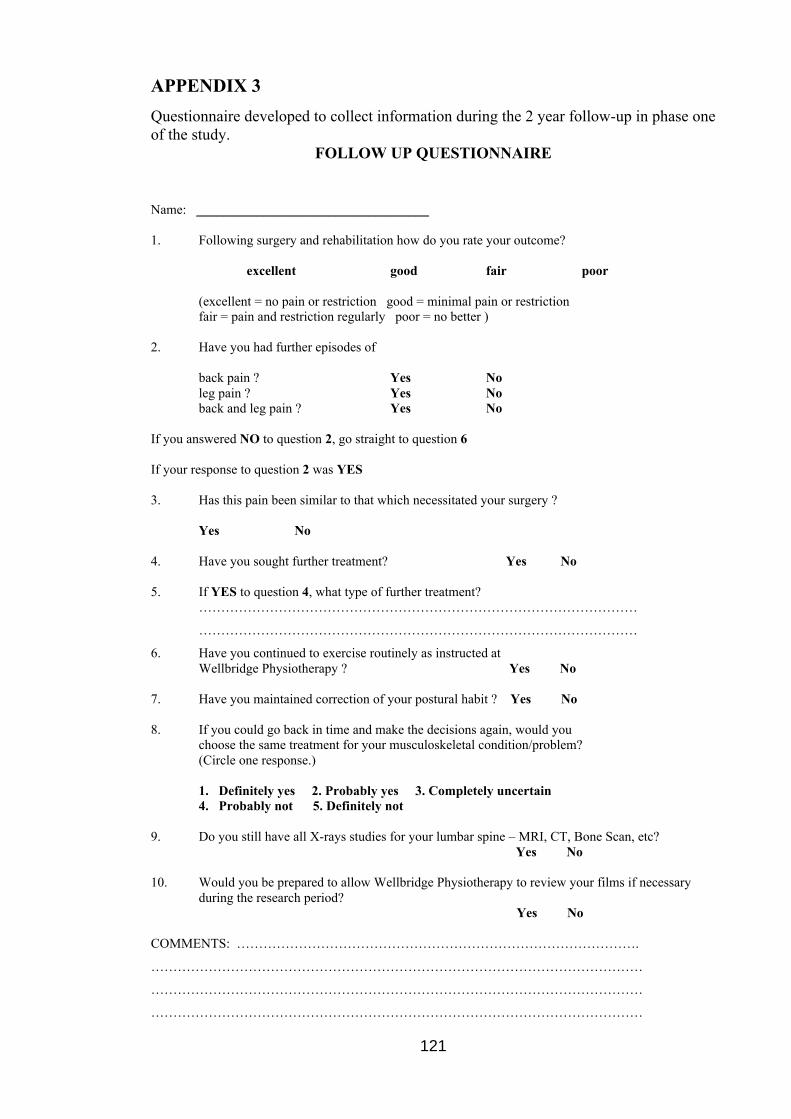
121
APPENDIX 3
Questionnaire developed to collect information during the 2 year follow-up in phase oneof the study.
FOLLOW UP QUESTIONNAIRE
Name: ___________________________________
1. Following surgery and rehabilitation how do you rate your outcome?
excellent good fair poor
(excellent = no pain or restriction good = minimal pain or restrictionfair = pain and restriction regularly poor = no better )
2. Have you had further episodes of
back pain ? Yes Noleg pain ? Yes Noback and leg pain ? Yes No
If you answered NO to question 2, go straight to question 6
If your response to question 2 was YES
3. Has this pain been similar to that which necessitated your surgery ?
Yes No
4. Have you sought further treatment? Yes No
5. If YES to question 4, what type of further treatment?………………………………………………………………………………………
………………………………………………………………………………………
6. Have you continued to exercise routinely as instructed atWellbridge Physiotherapy ? Yes No
7. Have you maintained correction of your postural habit ? Yes No
8. If you could go back in time and make the decisions again, would youchoose the same treatment for your musculoskeletal condition/problem?(Circle one response.)
1. Definitely yes 2. Probably yes 3. Completely uncertain4. Probably not 5. Definitely not
9. Do you still have all X-rays studies for your lumbar spine – MRI, CT, Bone Scan, etc? Yes No
10. Would you be prepared to allow Wellbridge Physiotherapy to review your films if necessaryduring the research period?
Yes No
COMMENTS: ……………………………………………………………………………….
…………………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………
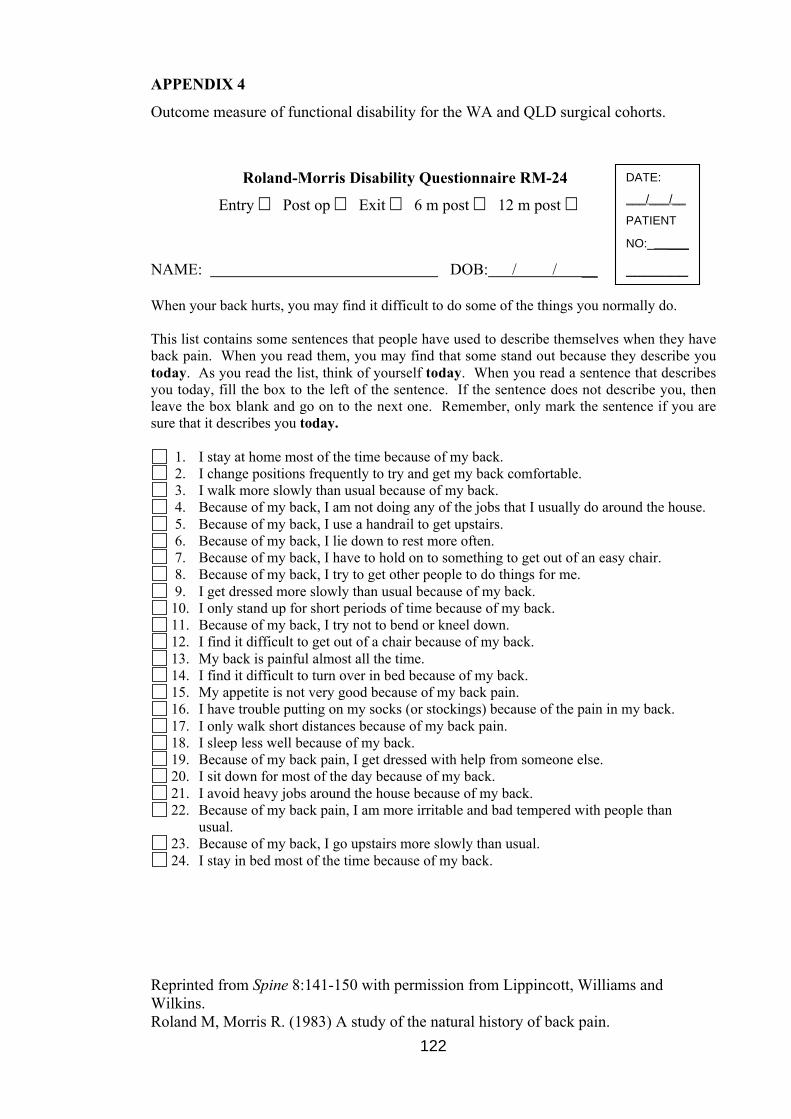
122
APPENDIX 4
Outcome measure of functional disability for the WA and QLD surgical cohorts.
Roland-Morris Disability Questionnaire RM-24
Entry � Post op � Exit � 6 m post � 12 m post �
NAME: DOB: / / __
When your back hurts, you may find it difficult to do some of the things you normally do.
This list contains some sentences that people have used to describe themselves when they haveback pain. When you read them, you may find that some stand out because they describe youtoday. As you read the list, think of yourself today. When you read a sentence that describesyou today, fill the box to the left of the sentence. If the sentence does not describe you, thenleave the box blank and go on to the next one. Remember, only mark the sentence if you aresure that it describes you today.
1. I stay at home most of the time because of my back. 2. I change positions frequently to try and get my back comfortable. 3. I walk more slowly than usual because of my back. 4. Because of my back, I am not doing any of the jobs that I usually do around the house. 5. Because of my back, I use a handrail to get upstairs. 6. Because of my back, I lie down to rest more often. 7. Because of my back, I have to hold on to something to get out of an easy chair. 8. Because of my back, I try to get other people to do things for me. 9. I get dressed more slowly than usual because of my back. 10. I only stand up for short periods of time because of my back. 11. Because of my back, I try not to bend or kneel down. 12. I find it difficult to get out of a chair because of my back. 13. My back is painful almost all the time. 14. I find it difficult to turn over in bed because of my back. 15. My appetite is not very good because of my back pain. 16. I have trouble putting on my socks (or stockings) because of the pain in my back. 17. I only walk short distances because of my back pain. 18. I sleep less well because of my back. 19. Because of my back pain, I get dressed with help from someone else. 20. I sit down for most of the day because of my back. 21. I avoid heavy jobs around the house because of my back. 22. Because of my back pain, I am more irritable and bad tempered with people than
usual. 23. Because of my back, I go upstairs more slowly than usual. 24. I stay in bed most of the time because of my back.
Reprinted from Spine 8:141-150 with permission from Lippincott, Williams andWilkins.Roland M, Morris R. (1983) A study of the natural history of back pain.
DATE:___/___/__PATIENT
NO:______
_______
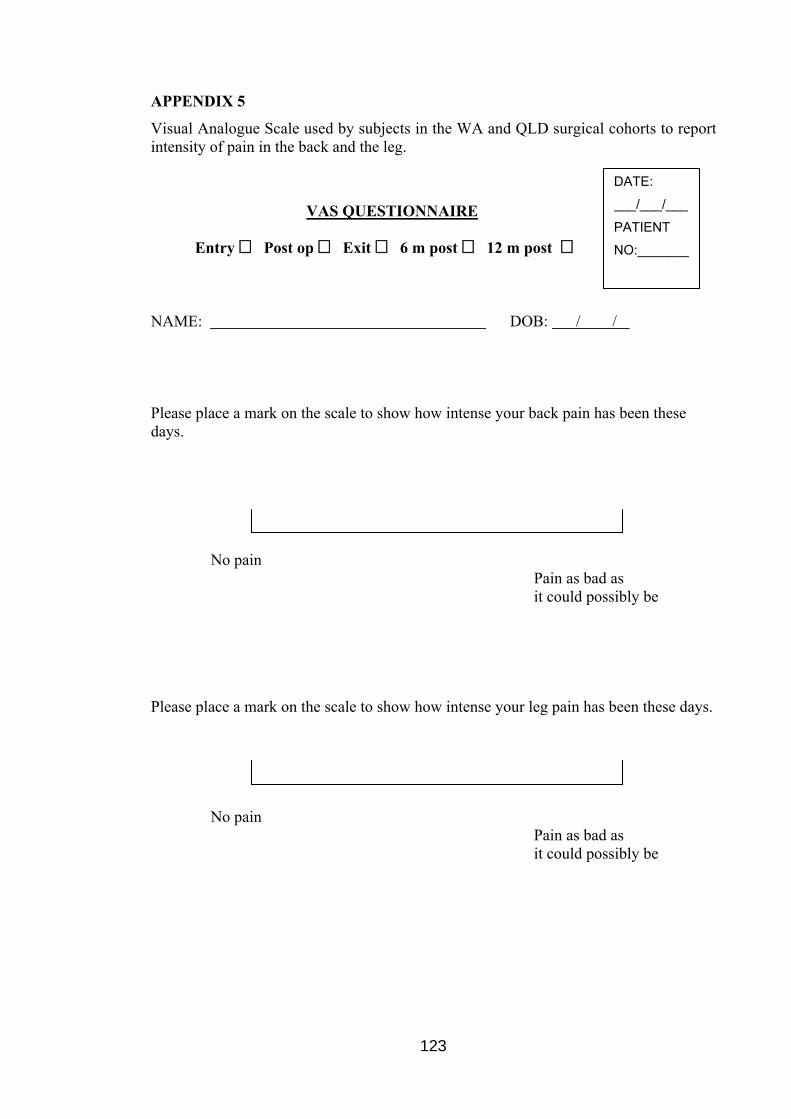
123
APPENDIX 5
Visual Analogue Scale used by subjects in the WA and QLD surgical cohorts to reportintensity of pain in the back and the leg.
VAS QUESTIONNAIRE
Entry � Post op � Exit � 6 m post � 12 m post �
NAME: DOB: / /
Please place a mark on the scale to show how intense your back pain has been thesedays.
No pain Pain as bad as
it could possibly be
Please place a mark on the scale to show how intense your leg pain has been these days.
No painPain as bad as
it could possibly be
DATE:
___/___/___
PATIENT
NO:_______
_________
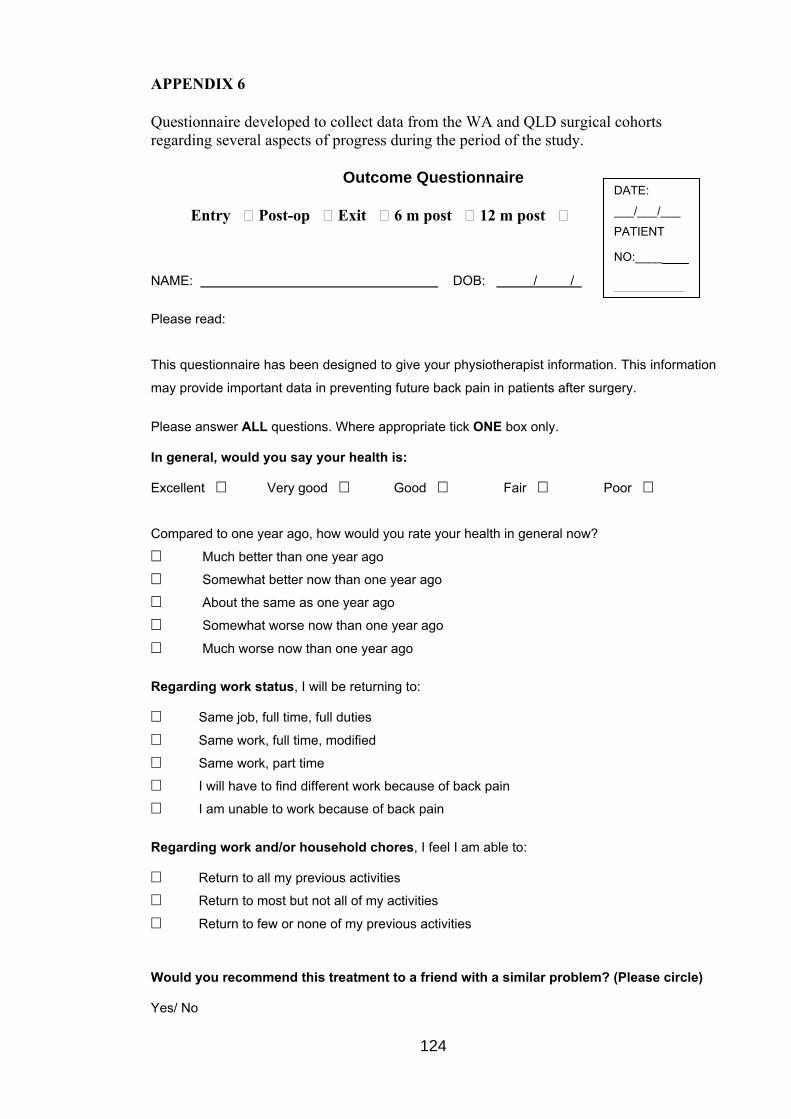
124
APPENDIX 6
Questionnaire developed to collect data from the WA and QLD surgical cohortsregarding several aspects of progress during the period of the study.
Outcome Questionnaire
Entry � Post-op � Exit � 6 m post � 12 m post �
NAME: DOB: / /
Please read:
This questionnaire has been designed to give your physiotherapist information. This information
may provide important data in preventing future back pain in patients after surgery.
Please answer ALL questions. Where appropriate tick ONE box only.
In general, would you say your health is:
Excellent � Very good � Good � Fair � Poor �
Compared to one year ago, how would you rate your health in general now?
� Much better than one year ago
� Somewhat better now than one year ago
� About the same as one year ago
� Somewhat worse now than one year ago
� Much worse now than one year ago
Regarding work status, I will be returning to:
� Same job, full time, full duties
� Same work, full time, modified
� Same work, part time
� I will have to find different work because of back pain
� I am unable to work because of back pain
Regarding work and/or household chores, I feel I am able to:
� Return to all my previous activities
� Return to most but not all of my activities
� Return to few or none of my previous activities
Would you recommend this treatment to a friend with a similar problem? (Please circle)
Yes/ No
DATE:
___/___/___
PATIENT
NO:_______________-
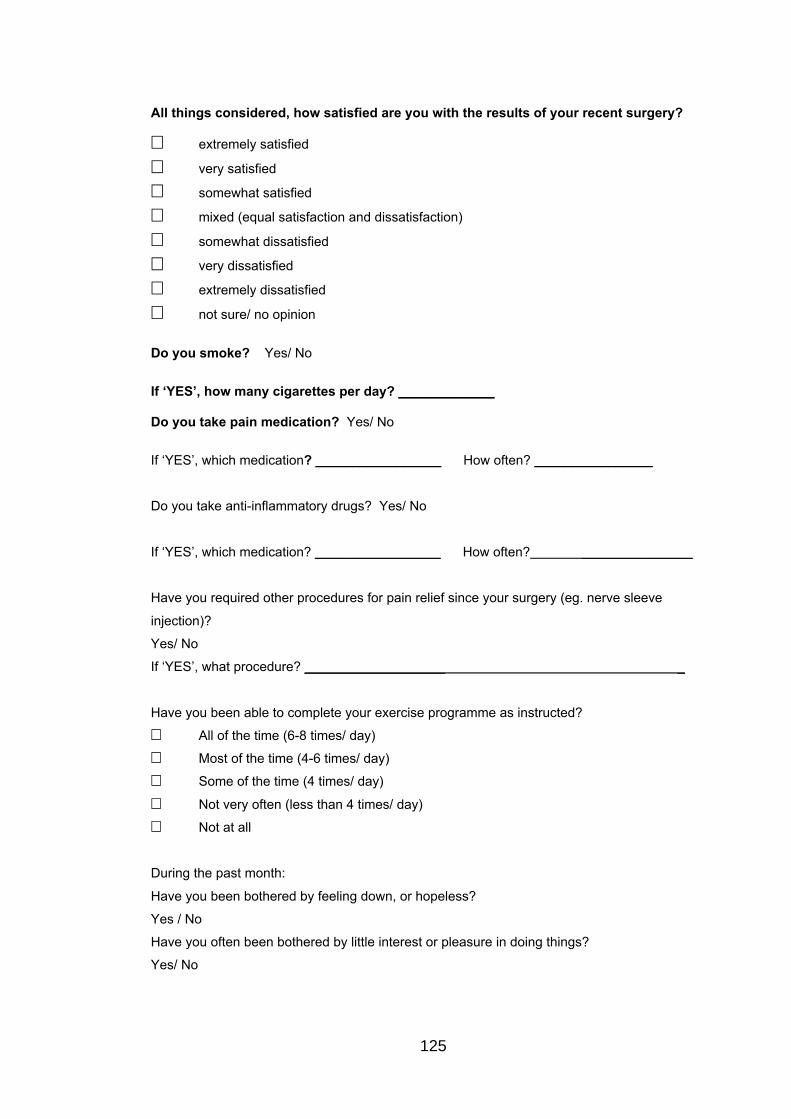
125
All things considered, how satisfied are you with the results of your recent surgery?
� extremely satisfied
� very satisfied
� somewhat satisfied
� mixed (equal satisfaction and dissatisfaction)
� somewhat dissatisfied
� very dissatisfied
� extremely dissatisfied
� not sure/ no opinion
Do you smoke? Yes/ No
If ‘YES’, how many cigarettes per day? _____________
Do you take pain medication? Yes/ No
If ‘YES’, which medication? _________________ How often? ________________
Do you take anti-inflammatory drugs? Yes/ No
If ‘YES’, which medication? _________________ How often? _______________
Have you required other procedures for pain relief since your surgery (eg. nerve sleeve
injection)?
Yes/ No
If ‘YES’, what procedure? ___________________ _
Have you been able to complete your exercise programme as instructed?
� All of the time (6-8 times/ day)
� Most of the time (4-6 times/ day)
� Some of the time (4 times/ day)
� Not very often (less than 4 times/ day)
� Not at all
During the past month:
Have you been bothered by feeling down, or hopeless?
Yes / No
Have you often been bothered by little interest or pleasure in doing things?
Yes/ No

126
APPENDIX 7
Patient information sheet provided to the subjects in WA and QLD enrolling into phasetwo of the study.
Dr Kevin Singer, Chief InvestigatorJennifer Lynn, Masters Degree Candidate
Centre for Musculoskeletal Studies, School of Surgery & Pathology,University of Western Australia.
Patient Information Form
Outcomes of Early Rehabilitation Following Lumbar Microdiscectomy
Professor Kevin Singer is the chief investigator of this research project. He is supervisingJennifer Lynn in her study as part of a Masters Degree by Research. Should you wish tocontact Dr Singer with questions regarding this study you may do so on 9224 0200.
This research aims to study the effects of introducing early rehabilitation following your lumbarmicrodiscectomy. This project will involve you in reporting your pain and back function byquestionnaire over a period of one year following surgery. Your data will be kept confidentialand will be used only for the purpose of this research. Once the research is complete all datawill be assessed. The results may be published however will not identify you by name.
The research includes instruction in exercises to be commenced in the hospital immediatelyfollowing your surgery. Your surgeon will request that you attend Wellbridge Physiotherapy at402A Scarborough Beach Road, Osborne Park, for treatment (usually 2 to 4 visits over 3 to 4weeks). This is a routine practice for all of your surgeon’s post-operative patients.
You will be requested to complete questionnaires before the surgery, at your firstphysiotherapy office visit, and your last physiotherapy office visit. Questionnaires will beposted to you for completion 6 and 12 months after your surgery. If you prefer, thequestionnaires may be completed over the internet. On each occasion the questionnairesrequire approximately 10 minutes to complete.
The exercise protocol used in this research is the same as you will receive should you decidenot to participate in the research. The only difference is the requested data collection. Thereshould be no pain associated with exercises used in this rehabilitation programme. However,there may be discomfort associated with the commencement of new exercise and theadoption of new postures.
Your participation in this study does not prejudice any right to compensation, which you mayhave under statute or common law.
The benefit from participation in this formal study of early rehabilitation following lumbarmicrodiscectomy may be a better appreciation of the outcomes of this type of surgery, and theeffectiveness of early specific exercises designed to improve spinal support and mobility, andto reduce further back pain following lumbar microdiscectomy.
For the participant: If there is any complaint regarding the manner, in which this researchproject is conducted, this concern may be discussed with the Chief Investigator, Dr Singer(2224 0200), the Researcher (9201 9658) or, alternatively to the Secretary, Human ResearchEthics Committee, Registrar’s Office, University of Western Australia, 35 Stirling Highway,Crawley, WA 6009 (6488 3703). All study participants will be provided with a copy of theInformation Sheet and Consent Form for their personal records.

128
APPENDIX 8
Patient consent form provided to the subjects in WA and QLD enrolling into phase twoof the study.
Dr Kevin Singer, Chief InvestigatorJennifer Lynn, Masters Degree Candidate
Centre for Musculoskeletal Studies, School of Surgery & Pathology,University of Western Australia.
Patient Consent Form
Outcomes of Early Rehabilitation Following Lumbar Microdiscectomy
A study concerned with the outcomes of early rehabilitation exercises after surgery.
I, , freely and voluntarily consent toparticipate in a research project to be conducted by Jennifer M. Lynn, a MastersDegree candidate at the University of Western Australia. I understand that theproject is being undertaken in order to test the effectiveness of a treatmentapproach/ a method of assessing patients and is part of the candidate’s MastersDegree research project.
I have read the information provided and any questions I have asked have beenanswered to my satisfaction. I agree to participate in this activity, realizing that I maywithdraw at any time without reason and without prejudice. (Or where applicable –without prejudice to my future medical treatment). In such a case, my record is to bedestroyed, unless otherwise agree by me.
I understand that all information provided is treated as strictly confidential and willnot be released by the investigator unless required to by law. I have been advised asto what data is being collected, what the purpose is, and what will be done with thedata upon completion of the research.
I agree that research data gathered for the study may be published provided myname or other identifying information is not used.
Signature Date
E-mail Address __________________________
For the participant: If there is any complaint regarding the manner, in which thisresearch project is conducted, it may be given to the Principal investigator Dr KevinSinger [ph: 9224 0200], researcher [ph: 9201 9658] or, alternatively to the Secretary,Human Research Ethics Committee, Registrar’s Office, University of WesternAustralia, 35 Stirling Highway, Crawley, WA 6009 (telephone number 6488 3703).All study participants will be provided with a copy of the Information Sheet andConsent Form for their personal records.
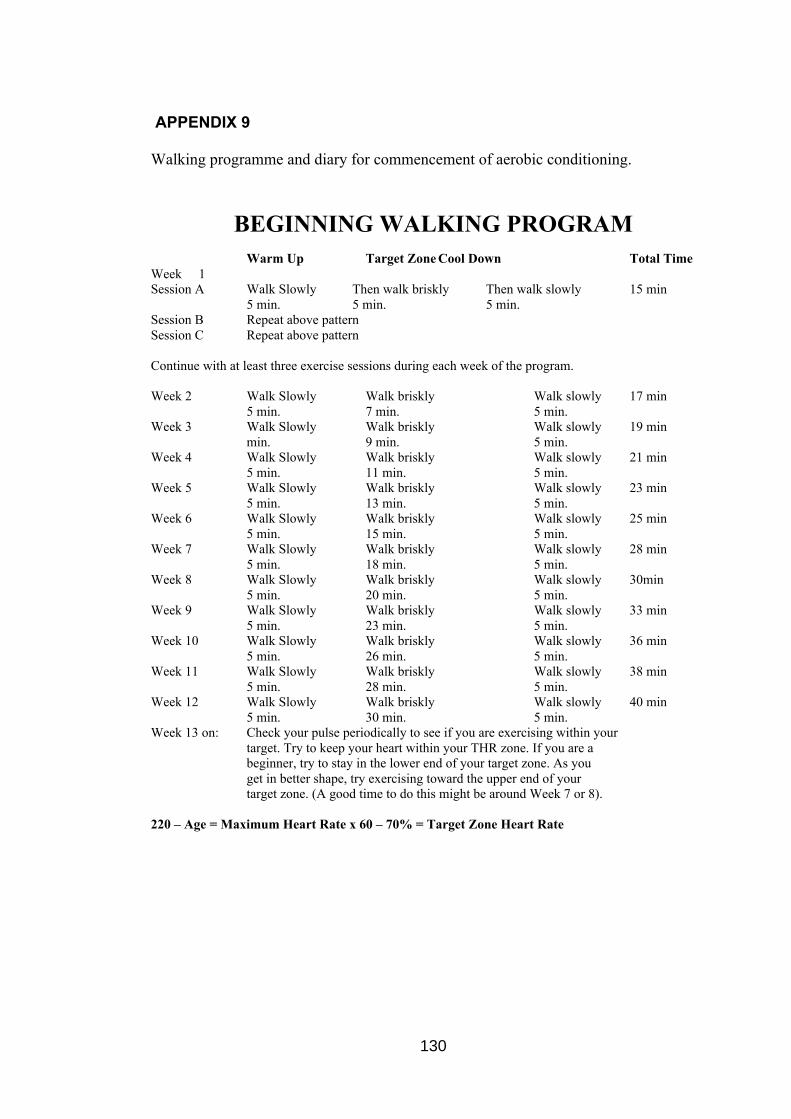
130
APPENDIX 9
Walking programme and diary for commencement of aerobic conditioning.
BEGINNING WALKING PROGRAMWarm Up Target Zone Cool Down Total Time
Week 1Session A Walk Slowly Then walk briskly Then walk slowly 15 min
5 min. 5 min. 5 min.Session B Repeat above patternSession C Repeat above pattern
Continue with at least three exercise sessions during each week of the program.
Week 2 Walk Slowly Walk briskly Walk slowly 17 min5 min. 7 min. 5 min.
Week 3 Walk Slowly Walk briskly Walk slowly 19 minmin. 9 min. 5 min.
Week 4 Walk Slowly Walk briskly Walk slowly 21 min5 min. 11 min. 5 min.
Week 5 Walk Slowly Walk briskly Walk slowly 23 min5 min. 13 min. 5 min.
Week 6 Walk Slowly Walk briskly Walk slowly 25 min5 min. 15 min. 5 min.
Week 7 Walk Slowly Walk briskly Walk slowly 28 min5 min. 18 min. 5 min.
Week 8 Walk Slowly Walk briskly Walk slowly 30min5 min. 20 min. 5 min.
Week 9 Walk Slowly Walk briskly Walk slowly 33 min5 min. 23 min. 5 min.
Week 10 Walk Slowly Walk briskly Walk slowly 36 min5 min. 26 min. 5 min.
Week 11 Walk Slowly Walk briskly Walk slowly 38 min5 min. 28 min. 5 min.
Week 12 Walk Slowly Walk briskly Walk slowly 40 min5 min. 30 min. 5 min.
Week 13 on: Check your pulse periodically to see if you are exercising within yourtarget. Try to keep your heart within your THR zone. If you are abeginner, try to stay in the lower end of your target zone. As youget in better shape, try exercising toward the upper end of yourtarget zone. (A good time to do this might be around Week 7 or 8).
220 – Age = Maximum Heart Rate x 60 – 70% = Target Zone Heart Rate

131
APPENDIX 10
An example of standard rehabilitation physiotherapy documentation from Queenslanddescribing typical elements of the rehabilitation programme after lumbar disc surgery.This but one illustration of the physiotherapy rehabilitation programmes which mayhave been used.
132
SPINAL REHAB
Dear
Re:
This patient has recently under-gone lumbar spine surgery by Dr and been seenby me as an inpatient at the Hospital. They may ring you for an appointment postop.
Surgery performed:
Mobility:
At discharge the patient had been given transverse abdominus in lying, static gluteusmaximus, gluteus medius (level1), very gentle sciatic mobility on pillows or with hip at90º, lumbar rotations, taught to log roll, has 20min limit of sitting for 2 weeks whichcan be increased to 40 min from 2-4 weeks. Walking was encouraged graduallyincreasing as tolerated, aiming to walk up to 1 hour by 4 weeks. General back care.Walking in water is also encouraged, freestyle and backstroke may be started at 3-4weeks if their stroke is fair. They have been advised they are unable to drive for 4weeks.
I have asked him/her to see you to start gentle ROM exercise. At 2 weeks post–op hipflex (single leg-progressing to double leg) in supine, lumbar side glide against a wall,gentle lumbar extension perhaps in form of anterior pelvic tilt initially, progression ofleg work esp gluts, whilst maintaining lumbar control. Bridging is often too much forthem until 4-6 weeks. Please progress neural mobility (not stretching) and stability infunctional positions eg. sitting & standing. We don’t start multifidus till week 4.
The normal protocol is for fortnightly follow ups, weekly if worried, encouraging thepatient to be responsible for their own management as much as possible. Treatmentfocus is on functional control and muscle imbalances – rather than passivemobilisations/electrotherapy. Due to the connective tissue healing, instability and neuralsensitivity please do not attempt any passive articular work, eg SIJ adjustments orPPIVMS/PAIVMS, strong muscle stretches or deep connective tissue work in theseearly stages. Noting that connective tissue maturity occurs from 6-12 weeks.
If the patient is having difficulty with TA or multifidus and its progression I’d be happyto review ultrasonically at Performance Rehab - . if you have any concerns pleasedon’t hesitate to contact me.
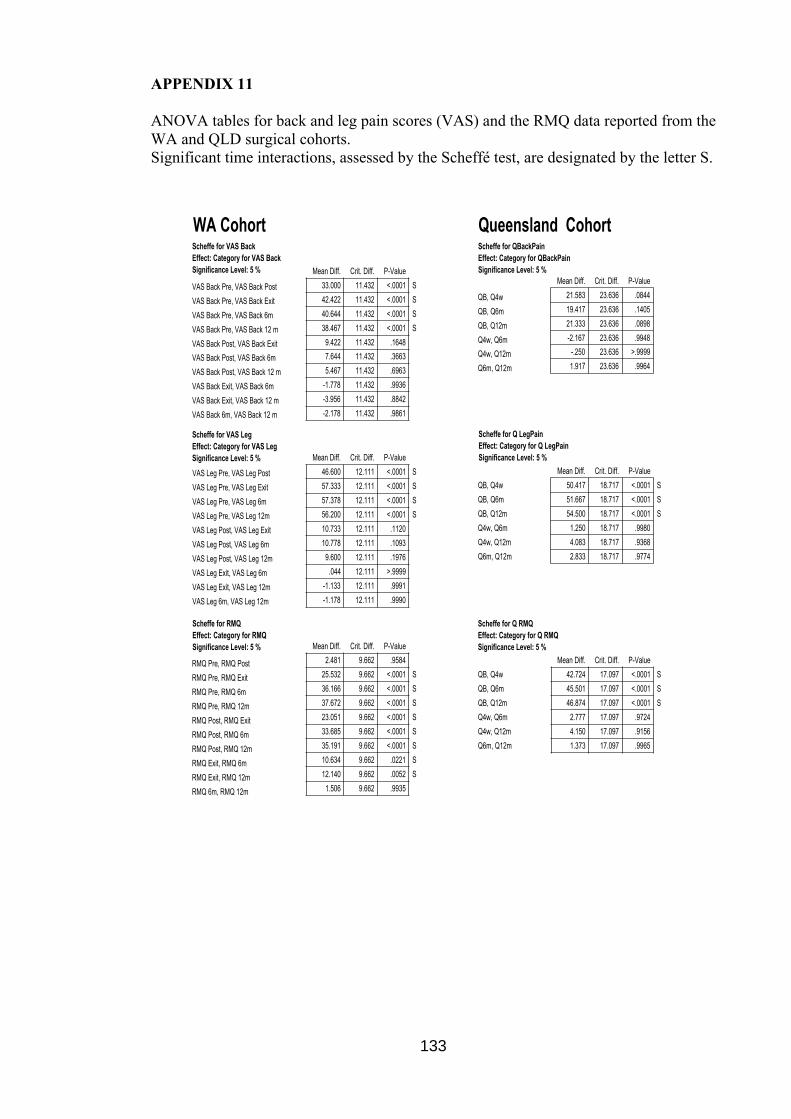
133
APPENDIX 11
ANOVA tables for back and leg pain scores (VAS) and the RMQ data reported from theWA and QLD surgical cohorts.Significant time interactions, assessed by the Scheffé test, are designated by the letter S.
VAS Back Pre, VAS Back Post
VAS Back Pre, VAS Back Exit
VAS Back Pre, VAS Back 6m
VAS Back Pre, VAS Back 12 m
VAS Back Post, VAS Back Exit
VAS Back Post, VAS Back 6m
VAS Back Post, VAS Back 12 m
VAS Back Exit, VAS Back 6m
VAS Back Exit, VAS Back 12 m
VAS Back 6m, VAS Back 12 m
33.000 11.432 <.0001 S
42.422 11.432 <.0001 S
40.644 11.432 <.0001 S
38.467 11.432 <.0001 S
9.422 11.432 .1648
7.644 11.432 .3663
5.467 11.432 .6963
-1.778 11.432 .9936
-3.956 11.432 .8842
-2.178 11.432 .9861
Mean Diff. Crit. Diff. P-Value
Scheffe for VAS BackEffect: Category for VAS BackSignificance Level: 5 %
VAS Leg Pre, VAS Leg Post
VAS Leg Pre, VAS Leg Exit
VAS Leg Pre, VAS Leg 6m
VAS Leg Pre, VAS Leg 12m
VAS Leg Post, VAS Leg Exit
VAS Leg Post, VAS Leg 6m
VAS Leg Post, VAS Leg 12m
VAS Leg Exit, VAS Leg 6m
VAS Leg Exit, VAS Leg 12m
VAS Leg 6m, VAS Leg 12m
46.600 12.111 <.0001 S
57.333 12.111 <.0001 S
57.378 12.111 <.0001 S
56.200 12.111 <.0001 S
10.733 12.111 .1120
10.778 12.111 .1093
9.600 12.111 .1976
.044 12.111 >.9999
-1.133 12.111 .9991
-1.178 12.111 .9990
Mean Diff. Crit. Diff. P-Value
Scheffe for VAS LegEffect: Category for VAS LegSignificance Level: 5 %
RMQ Pre, RMQ Post
RMQ Pre, RMQ Exit
RMQ Pre, RMQ 6m
RMQ Pre, RMQ 12m
RMQ Post, RMQ Exit
RMQ Post, RMQ 6m
RMQ Post, RMQ 12m
RMQ Exit, RMQ 6m
RMQ Exit, RMQ 12m
RMQ 6m, RMQ 12m
2.481 9.662 .9584
25.532 9.662 <.0001 S
36.166 9.662 <.0001 S
37.672 9.662 <.0001 S
23.051 9.662 <.0001 S
33.685 9.662 <.0001 S
35.191 9.662 <.0001 S
10.634 9.662 .0221 S
12.140 9.662 .0052 S
1.506 9.662 .9935
Mean Diff. Crit. Diff. P-Value
Scheffe for RMQEffect: Category for RMQSignificance Level: 5 %
WA Cohort
QB, Q4w
QB, Q6m
QB, Q12m
Q4w, Q6m
Q4w, Q12m
Q6m, Q12m
21.583 23.636 .0844
19.417 23.636 .1405
21.333 23.636 .0898
-2.167 23.636 .9948
-.250 23.636 >.9999
1.917 23.636 .9964
Mean Diff. Crit. Diff. P-Value
Scheffe for QBackPainEffect: Category for QBackPainSignificance Level: 5 %
QB, Q4w
QB, Q6m
QB, Q12m
Q4w, Q6m
Q4w, Q12m
Q6m, Q12m
50.417 18.717 <.0001 S
51.667 18.717 <.0001 S
54.500 18.717 <.0001 S
1.250 18.717 .9980
4.083 18.717 .9368
2.833 18.717 .9774
Mean Diff. Crit. Diff. P-Value
Scheffe for Q LegPainEffect: Category for Q LegPainSignificance Level: 5 %
QB, Q4w
QB, Q6m
QB, Q12m
Q4w, Q6m
Q4w, Q12m
Q6m, Q12m
42.724 17.097 <.0001 S
45.501 17.097 <.0001 S
46.874 17.097 <.0001 S
2.777 17.097 .9724
4.150 17.097 .9156
1.373 17.097 .9965
Mean Diff. Crit. Diff. P-Value
Scheffe for Q RMQEffect: Category for Q RMQSignificance Level: 5 %
Queensland Cohort
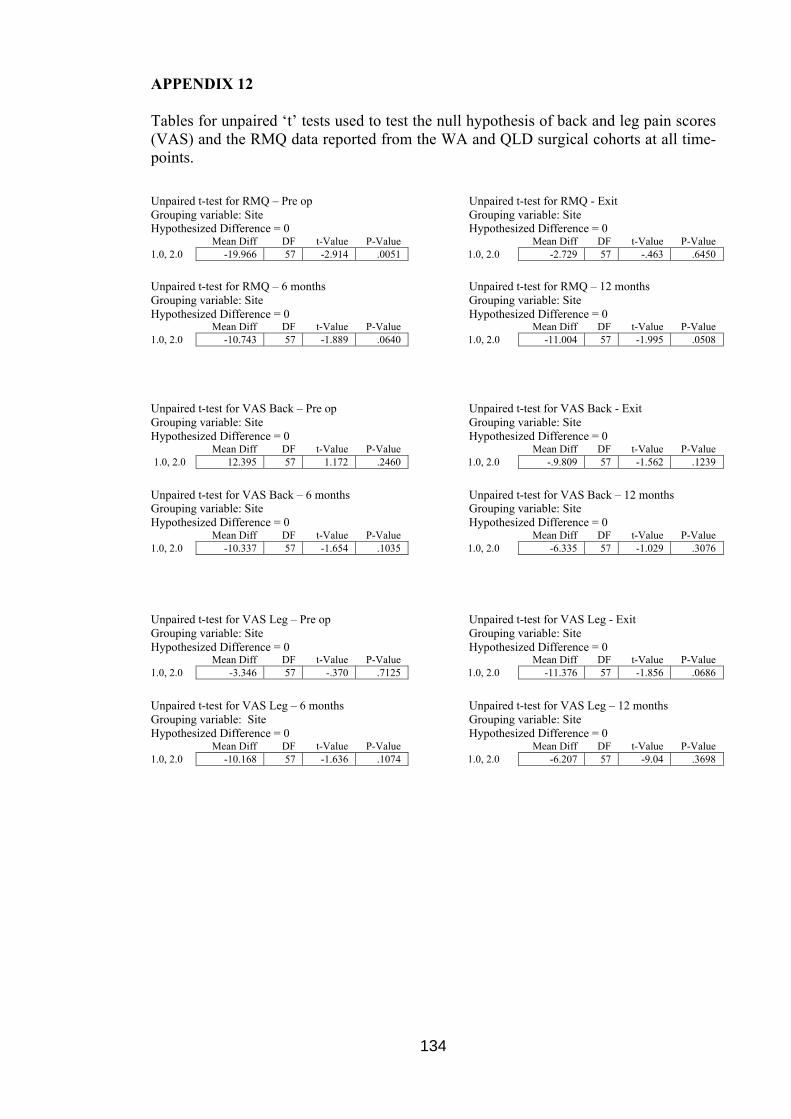
134
APPENDIX 12
Tables for unpaired ‘t’ tests used to test the null hypothesis of back and leg pain scores(VAS) and the RMQ data reported from the WA and QLD surgical cohorts at all time-points.
Unpaired t-test for RMQ – Pre opGrouping variable: SiteHypothesized Difference = 0
Unpaired t-test for RMQ - ExitGrouping variable: SiteHypothesized Difference = 0
Mean Diff DF t-Value P-Value Mean Diff DF t-Value P-Value1.0, 2.0 -19.966 57 -2.914 .0051 1.0, 2.0 -2.729 57 -.463 .6450
Unpaired t-test for RMQ – 6 monthsGrouping variable: SiteHypothesized Difference = 0
Unpaired t-test for RMQ – 12 monthsGrouping variable: SiteHypothesized Difference = 0
Mean Diff DF t-Value P-Value Mean Diff DF t-Value P-Value1.0, 2.0 -10.743 57 -1.889 .0640 1.0, 2.0 -11.004 57 -1.995 .0508
Unpaired t-test for VAS Back – Pre opGrouping variable: SiteHypothesized Difference = 0
Unpaired t-test for VAS Back - ExitGrouping variable: SiteHypothesized Difference = 0
Mean Diff DF t-Value P-Value Mean Diff DF t-Value P-Value1.0, 2.0 12.395 57 1.172 .2460 1.0, 2.0 -.9.809 57 -1.562 .1239
Unpaired t-test for VAS Back – 6 monthsGrouping variable: SiteHypothesized Difference = 0
Unpaired t-test for VAS Back – 12 monthsGrouping variable: SiteHypothesized Difference = 0
Mean Diff DF t-Value P-Value Mean Diff DF t-Value P-Value1.0, 2.0 -10.337 57 -1.654 .1035 1.0, 2.0 -6.335 57 -1.029 .3076
Unpaired t-test for VAS Leg – Pre opGrouping variable: SiteHypothesized Difference = 0
Unpaired t-test for VAS Leg - ExitGrouping variable: SiteHypothesized Difference = 0
Mean Diff DF t-Value P-Value Mean Diff DF t-Value P-Value1.0, 2.0 -3.346 57 -.370 .7125 1.0, 2.0 -11.376 57 -1.856 .0686
Unpaired t-test for VAS Leg – 6 monthsGrouping variable: SiteHypothesized Difference = 0
Unpaired t-test for VAS Leg – 12 monthsGrouping variable: SiteHypothesized Difference = 0
Mean Diff DF t-Value P-Value Mean Diff DF t-Value P-Value1.0, 2.0 -10.168 57 -1.636 .1074 1.0, 2.0 -6.207 57 -9.04 .3698
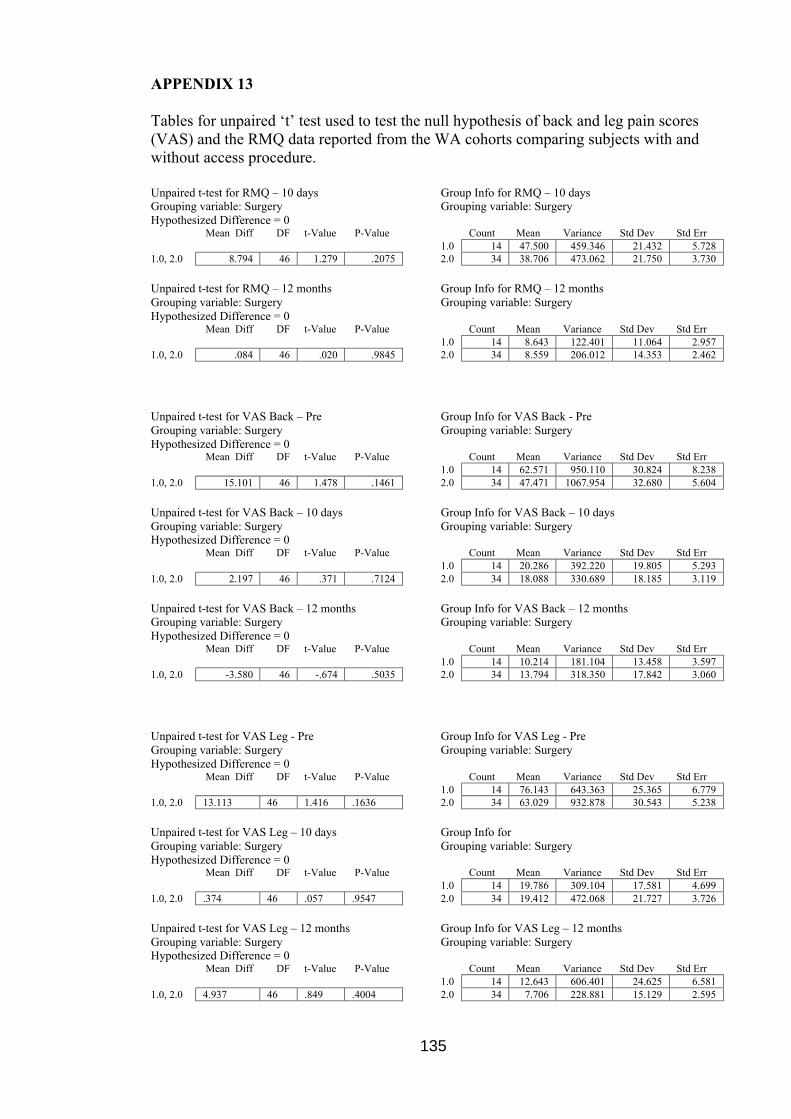
135
APPENDIX 13
Tables for unpaired ‘t’ test used to test the null hypothesis of back and leg pain scores(VAS) and the RMQ data reported from the WA cohorts comparing subjects with andwithout access procedure.
Unpaired t-test for RMQ – 10 daysGrouping variable: SurgeryHypothesized Difference = 0
Group Info for RMQ – 10 daysGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 47.500 459.346 21.432 5.728
1.0, 2.0 8.794 46 1.279 .2075 2.0 34 38.706 473.062 21.750 3.730
Unpaired t-test for RMQ – 12 monthsGrouping variable: SurgeryHypothesized Difference = 0
Group Info for RMQ – 12 monthsGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 8.643 122.401 11.064 2.957
1.0, 2.0 .084 46 .020 .9845 2.0 34 8.559 206.012 14.353 2.462
Unpaired t-test for VAS Back – PreGrouping variable: SurgeryHypothesized Difference = 0
Group Info for VAS Back - PreGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 62.571 950.110 30.824 8.238
1.0, 2.0 15.101 46 1.478 .1461 2.0 34 47.471 1067.954 32.680 5.604
Unpaired t-test for VAS Back – 10 daysGrouping variable: SurgeryHypothesized Difference = 0
Group Info for VAS Back – 10 daysGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 20.286 392.220 19.805 5.293
1.0, 2.0 2.197 46 .371 .7124 2.0 34 18.088 330.689 18.185 3.119
Unpaired t-test for VAS Back – 12 monthsGrouping variable: SurgeryHypothesized Difference = 0
Group Info for VAS Back – 12 monthsGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 10.214 181.104 13.458 3.597
1.0, 2.0 -3.580 46 -.674 .5035 2.0 34 13.794 318.350 17.842 3.060
Unpaired t-test for VAS Leg - PreGrouping variable: SurgeryHypothesized Difference = 0
Group Info for VAS Leg - PreGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 76.143 643.363 25.365 6.779
1.0, 2.0 13.113 46 1.416 .1636 2.0 34 63.029 932.878 30.543 5.238
Unpaired t-test for VAS Leg – 10 daysGrouping variable: SurgeryHypothesized Difference = 0
Group Info forGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 19.786 309.104 17.581 4.699
1.0, 2.0 .374 46 .057 .9547 2.0 34 19.412 472.068 21.727 3.726
Unpaired t-test for VAS Leg – 12 monthsGrouping variable: SurgeryHypothesized Difference = 0
Group Info for VAS Leg – 12 monthsGrouping variable: Surgery
Mean Diff DF t-Value P-Value Count Mean Variance Std Dev Std Err1.0 14 12.643 606.401 24.625 6.581
1.0, 2.0 4.937 46 .849 .4004 2.0 34 7.706 228.881 15.129 2.595

136
APPENDIX 14
An example of standard rehabilitation physiotherapy after lumbar disc surgery fromWestern Australia.