Embed Size (px)
Citation preview

Reliance on opioids has resulted in a clinical, societal, and economic burden
• Currently available postsurgical pain management options involve either decades-old technology or synthetic opioids with associated risks1-3
• Opioids have become the mainstay for postsurgical pain with 99% of all surgical patients being prescribed an opioid following surgery4
• Enhanced recovery pathways are complicated by opioid-related adverse events5
• Persistent use of prescription opioids has led to a signifi cant increase in heroin abuse in the US so that now four in fi ve new heroin users fi rst abused prescription painkillers6
With orthopaedic surgeons being the third highest prescribers of opioids,8 they are uniquely situated to be a part of the solution moving forward
There is a growing need to reduce postsurgical opioid use and associated diversion and abuse
• The Centers for Disease Control and Prevention and The Joint Commission (JCAHO) call for a patient-centered multimodal treatment plan, noting that the best approach may be to start with a nonopioid9,10
• Leaders in the industry are already employing opioid minimization strategies to move toward opioid-free facilities, including one of the largest hospital systems in the nation, Trinity Health11
• Many patients are aware of opioid-related risks and prefer nonopioid analgesic options12
Enhanced recovery protocols can be used following orthopaedic procedures*
• Optimize pain management13
• Accelerate mobilization and rehabilitation13
• Improve patient satisfaction13
• Reduce hospital length of stay and readmission13
- May also help to accelerate patient discharge in the outpatient setting
JOINT RECONSTRUCTION • TRAUMA • MITEK SPORTS MEDICINE • SPINE
*EXPAREL® (bupivacaine liposome injectable suspension) has not been clinically proven to reduce length of stay or rate of readmission, accelerate mobilization or rehabilitation
90% 79%Of patients are concerned about side effects, addiction, or dependence12
Of patients prefer a nonopioid pain management option12
Managing Postsurgical Pain with a Nonopioid Approach
0
5,000
10,000
15,000
20,000
´98 ‘00 ’02 ‘04 ‘06 ‘08 ‘10 ’12 ‘14
OVERDOSE DEATHS7
Year
Opioids Heroin
More people are dying from prescription opioids than heroin7
Important Safety Information EXPAREL is contraindicated in obstetrical paracervical block anesthesia. In clinical trials, the most common adverse reactions (incidence ≥10%) following EXPAREL administration were nausea, constipation, and vomiting. Please see additional Important Safety Information on back and accompanying full Prescribing Information for EXPAREL.
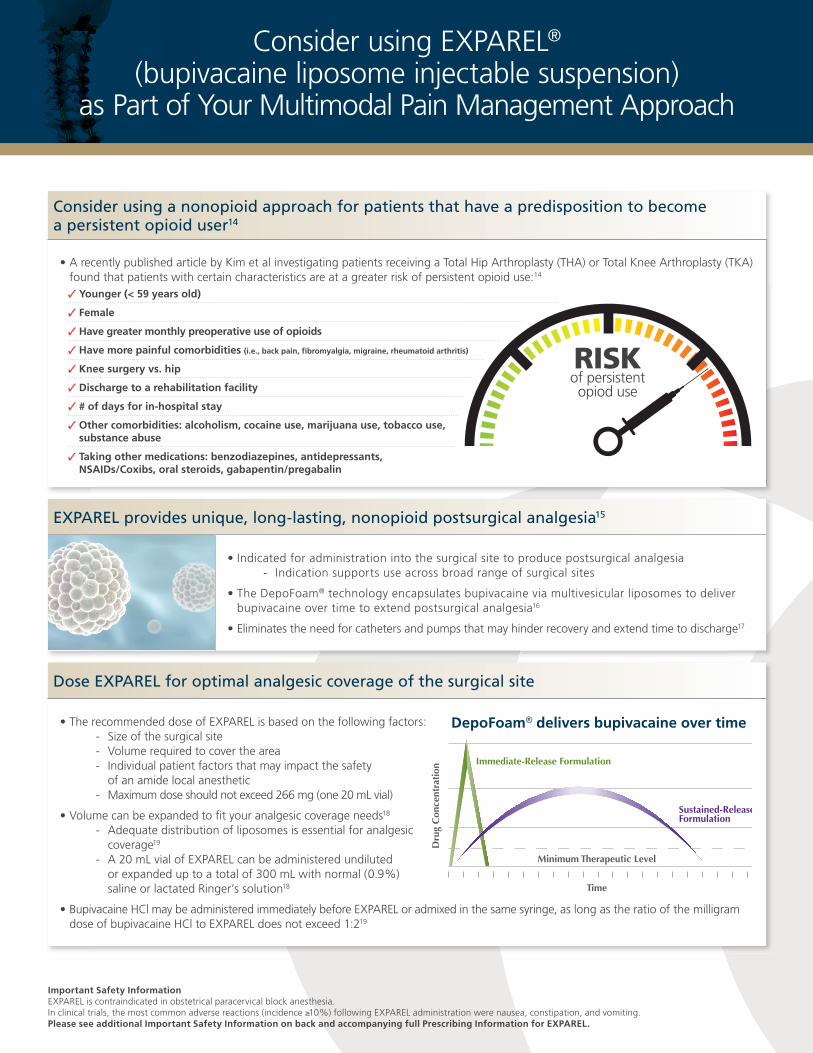
Consider using a nonopioid approach for patients that have a predisposition to become a persistent opioid user14
• A recently published article by Kim et al investigating patients receiving a Total Hip Arthroplasty (THA) or Total Knee Arthroplasty (TKA) found that patients with certain characteristics are at a greater risk of persistent opioid use:14
EXPAREL provides unique, long-lasting, nonopioid postsurgical analgesia15
• Indicated for administration into the surgical site to produce postsurgical analgesia - Indication supports use across broad range of surgical sites
• The DepoFoam® technology encapsulates bupivacaine via multivesicular liposomes to deliver bupivacaine over time to extend postsurgical analgesia16
• Eliminates the need for catheters and pumps that may hinder recovery and extend time to discharge17
Dose EXPAREL for optimal analgesic coverage of the surgical site
• The recommended dose of EXPAREL is based on the following factors: - Size of the surgical site - Volume required to cover the area - Individual patient factors that may impact the safety
of an amide local anesthetic - Maximum dose should not exceed 266 mg (one 20 mL vial)
• Volume can be expanded to fi t your analgesic coverage needs18
- Adequate distribution of liposomes is essential for analgesic coverage19
- A 20 mL vial of EXPAREL can be administered undiluted or expanded up to a total of 300 mL with normal (0.9%) saline or lactated Ringer’s solution18
• Bupivacaine HCl may be administered immediately before EXPAREL or admixed in the same syringe, as long as the ratio of the milligram dose of bupivacaine HCl to EXPAREL does not exceed 1:219
Consider using EXPAREL® (bupivacaine liposome injectable suspension)
as Part of Your Multimodal Pain Management Approach
� Younger (< 59 years old)
� Female
� Have greater monthly preoperative use of opioids
� Have more painful comorbidities (i.e., back pain, fi bromyalgia, migraine, rheumatoid arthritis)
� Knee surgery vs. hip
� Discharge to a rehabilitation facility
� # of days for in-hospital stay
� Other comorbidities: alcoholism, cocaine use, marijuana use, tobacco use, substance abuse
� Taking other medications: benzodiazepines, antidepressants, NSAIDs/Coxibs, oral steroids, gabapentin/pregabalin
RISKof persistent opiod use
DepoFoam® Technology Optimizes Pharmacokinetics and Pharmacodynamics
Dru
g C
once
ntra
tion
Sustained-Release Formulation
Minimum Therapeutic Level
Time
Immediate-Release Formulation
DepoFoam delivers bupivacaine over time2
Designed to:
• Provide long-lasting postsurgical pain control during the first few days after surgery, when most patients report moderate, severe, or extreme pain3,4
• Eliminate the need for titration with a single dose
• Eliminate the need for external devices to prolong analgesia
• Be different from non-liposomal bupivacaine
— Different formulations of bupivacaine are not bioequivalent even if the milligram dosage is the same
3
Important Safety InformationNon-bupivacaine-based local anesthetics, including lidocaine, may cause an immediate release of bupivacaine from EXPAREL if administered together locally. The administration of EXPAREL may follow the administration of lidocaine after a delay of 20 minutes or more. Formulations of bupivacaine other than EXPAREL should not be administered within 96 hours following administration of EXPAREL.
DepoFoam® delivers bupivacaine over time
Important Safety Information EXPAREL is not recommended for the following types or routes of administration: epidural, intrathecal, regional nerve blocks, or intravascular or intra-articular use. Non-bupivacaine-based local anesthetics, including lidocaine, may cause an immediate release of bupivacaine from EXPAREL if administered together locally. Please see additional Important Safety Information on back and accompanying full Prescribing Information for EXPAREL.
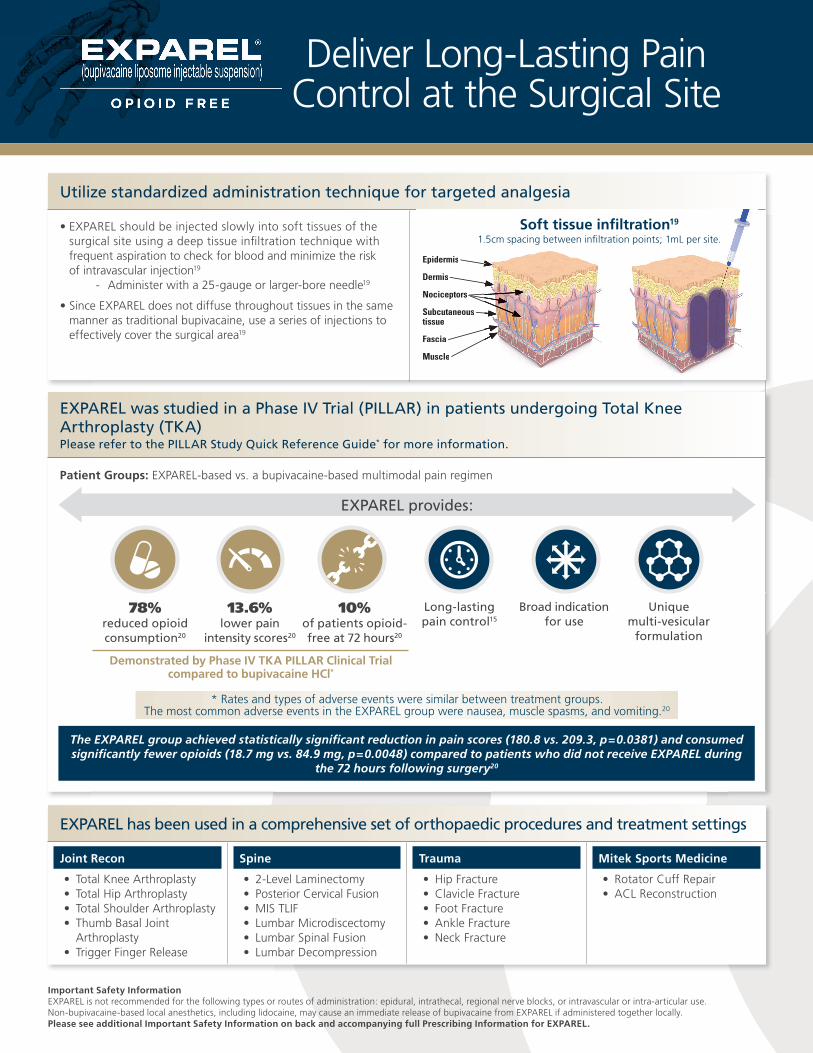
Utilize standardized administration technique for targeted analgesia
• EXPAREL should be injected slowly into soft tissues of the surgical site using a deep tissue infi ltration technique with frequent aspiration to check for blood and minimize the risk of intravascular injection19
- Administer with a 25-gauge or larger-bore needle19
• Since EXPAREL does not diffuse throughout tissues in the same manner as traditional bupivacaine, use a series of injections to effectively cover the surgical area19
EXPAREL was studied in a Phase IV Trial (PILLAR) in patients undergoing Total Knee Arthroplasty (TKA)Please refer to the PILLAR Study Quick Reference Guide* for more information.
Patient Groups: EXPAREL-based vs. a bupivacaine-based multimodal pain regimen
•
Epidermis
Dermis
Nociceptors
Subcutaneoustissue
Fascia
Muscle
Set a smooth recovery in motion with EXPAREL
Administering EXPAREL•
—
•
•
Soft tissue infiltration8
8
Soft tissue infi ltration19
1.5cm spacing between infi ltration points; 1mL per site.
Deliver Long-Lasting Pain Control at the Surgical Site
EXPAREL has been used in a comprehensive set of orthopaedic procedures and treatment settings
Joint Recon
• Total Knee Arthroplasty• Total Hip Arthroplasty• Total Shoulder Arthroplasty• Thumb Basal Joint
Arthroplasty• Trigger Finger Release
Spine
• 2-Level Laminectomy• Posterior Cervical Fusion• MIS TLIF• Lumbar Microdiscectomy• Lumbar Spinal Fusion• Lumbar Decompression
Trauma
• Hip Fracture• Clavicle Fracture• Foot Fracture• Ankle Fracture• Neck Fracture
Mitek Sports Medicine
• Rotator Cuff Repair• ACL Reconstruction
The EXPAREL group achieved statistically signifi cant reduction in pain scores (180.8 vs. 209.3, p=0.0381) and consumed signifi cantly fewer opioids (18.7 mg vs. 84.9 mg, p=0.0048) compared to patients who did not receive EXPAREL during
the 72 hours following surgery20
EXPAREL provides:
78% reduced opioid consumption20
13.6% lower pain
intensity scores20
10% of patients opioid-free at 72 hours20
Long-lasting pain control15
Broad indication for use
Unique multi-vesicular
formulation
Demonstrated by Phase IV TKA PILLAR Clinical Trial compared to bupivacaine HCl*
* Rates and types of adverse events were similar between treatment groups. The most common adverse events in the EXPAREL group were nausea, muscle spasms, and vomiting.20

The clinical benefi t of the decrease in opioid consumption was not demonstrated in the pivotal trials. EXPAREL is indicated for administration into the surgical site to produce postsurgical analgesia.
For more information on EXPAREL, please visit www.EXPAREL.com or call 1-855-RX-EXPAREL (793-9727).
IMPORTANT SAFETY INFORMATION• EXPAREL is contraindicated in obstetrical paracervical block anesthesia • In clinical trials, the most common adverse reactions (incidence ≥10%) following EXPAREL administration were nausea, constipation, and vomiting• EXPAREL is not recommended to be used in the following patient population: patients <18 years old and/or pregnant patients• Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients
with hepatic disease. Patients with severe hepatic disease, because of their inability to metabolize local anesthetics normally, are at a greater risk of developing toxic plasma concentrations
WARNINGS AND PRECAUTIONS SPECIFIC TO EXPAREL• EXPAREL is not recommended for the following types or routes of administration: epidural, intrathecal, regional nerve blocks, or
intravascular or intra-articular use• Non-bupivacaine-based local anesthetics, including lidocaine, may cause an immediate release of bupivacaine from EXPAREL if administered
together locally. The administration of EXPAREL may follow the administration of lidocaine after a delay of 20 minutes or more. Formulations of bupivacaine other than EXPAREL should not be administered within 96 hours following administration of EXPAREL
WARNINGS AND PRECAUTIONS FOR BUPIVACAINE-CONTAINING PRODUCTS• Central Nervous System (CNS) Reactions: There have been reports of adverse neurologic reactions with the use of local anesthetics.
These include persistent anesthesia and paresthesias. CNS reactions are characterized by excitation and/or depression• Cardiovascular System Reactions: Toxic blood concentrations depress cardiac conductivity and excitability which may lead to dysrhythmias
sometimes leading to death• Allergic Reactions: Allergic-type reactions (eg, anaphylaxis and angioedema) are rare and may occur as a result of hypersensitivity to the
local anesthetic or to other formulation ingredients• Chondrolysis: There have been reports of chondrolysis (mostly in the shoulder joint) following intra-articular infusion of local anesthetics,
which is an unapproved use
PLEASE SEE ACCOMPANYING FULL PRESCRIBING INFORMATION FOR EXPAREL
1. Dvorsky, G. A brief history of painkillers (and why they work). Gizmodo Daily Explainer website. http://io9.gizmodo.com/how-drugs-work-to-help-you-ease-the-pain-1452216695. Updated Oct 2013. Accessed Mar 2017. 2. About us: Our story. Tylenol website. https://www.tylenol.com/news/about-us. Accessed Mar 2017. 3. Buer JK. Origins and impact of the term “NSAID.” Infl ammopharmacology. 2014;22(5):263-267. doi: 10.1007/s10787-014-0211-2. 4. Kessler ER, Shah M, Gruschkus S, Raju A. Cost and quality implications of opioid-based postsurgical pain control using administrative claims data from a large health system: Opioid-related adverse events and their impact on clinical and economic outcomes. Pharmacotherapy. 2013;33(4):383-391.5. Barrington JW, Halaszynski TM, Sinatra RS. Expert working group on anesthesia and orthopaedics critical issues in hip and knee replacement arthroplasty. Perioperative pain management in hip and knee replacement surgery. Am J Orthop (Belle Mead NJ). 2014;43(4 Suppl):S1-S16. 6. American Society of Addiction Medicine. Opioid Addiction 2016 Facts & Figures. http://www.asam.org/docs/default-source/advocacy/opioid-addiction-disease-facts-fi gures.pdf. Accessed Mar 2017. 7. Nolan, D., Amico, C. How Bad is the Opioid Epidemic? Published Feb 2016. http://www.pbs.org/wgbh/frontline/article/how-bad-is-the-opioid-epidemic/. Accessed Mar 2017. 8. Volkow N, McLellan T, Cotto J. Research letter. JAMA. 2011;305(13):1299-1301. doi:10.1111/bjd.13910. 9. The Joint Commission. Safe use of opioids in hospitals. Sentinel Event Alert. 2012;8(49): 1-5. 10. CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016 Morbidity and Mortality Weekly Report. MMWR Recomm Reports. 2016;65(1):1-52. http://www.cdc.gov/mmwr/cme/conted.html. Accessed July 26, 2017. 11. Trinity Health and Pacira Pharmaceuticals announce collaboration to decrease opioid use nationwide. Pacira Pharmaceuticals Inc website. http://investor.pacira.com/phoenix.zhtml?c=220759&p=irol-newsArticle&ID=2254388. Updated Mar 2017. Accessed Jun 2017. 12. Pacira Pharmaceuticals, Inc. News Release. New research: opioid addiction and dependence after surgery is signifi cantly higher than previously known. http://investor.pacira.com/phoenix.zhtml?c=220759&p=irolnewsArticle_pf&ID=2191316. Published Aug 2016. Accessed Mar 2017. 13. Crosson J. Multimodal analgesia (MMA) as the cornerstone of the enhanced recovery after surgery (ERAS) protocol. Becker’s Hospital Review. Published Jan 2017. Accessed Jun 2017. 14. Kim SC, Choudry N, Franklin JM, et al. Patterns and predictors of persistent opioid use following hip or knee arthroplasty. Osteoarthr Cartil. 2017; 1-8. doi:10.1016/j.joca.2017.04.002. 15. Gorfi ne SR, Onel E, Patou G, Krivokapic ZV. Bupivacaine extended-release liposome injection for prolonged postsurgical analgesia in patients undergoing hemorrhoidectomy: a multicenter, randomized, double-blind, placebo-controlled trial. Dis Colon Rectum. 2011;54(12):1552-1559. doi:10.1097/DCR.0b013e18232d4c1. 16. Lambert WJ, Los K. In: Rathbone MJ, et al, eds. Modifi ed-Release Drug Delivery Technology. Volume 2. 2nd ed. New York: Informa Healthcare; 2008:207-214. 17. Grissinger M. Improved safety needed in handling elastomeric reservoir balls used for pain relief. P&T. 2013;38(5):243-245. 18. Dosing EXPAREL®. Pacira Pharmaceuticals Inc website. http://www.exparel.com/hcp/how-to-use/dosing.shtml. Accessed Jul 2017. 19. EXPAREL® administration. Pacira Pharmaceuticals Inc website. http://www.exparel.com/hcp/how-to-use/EXPAREL-administration.shtml. Accessed Jul 2017. 20. Mont MA, Beaver WB, Dysart SH, Barrington JW, Del Gaizo DJ. Local infi ltration analgesia with liposomal bupivacaine improves pain scores and reduces opioid use after total knee arthroplasty: results of a randomized controlled trial. J Arthroplasty. 2017:1-7. doi:10.1016/j.arth.2017.07.024.
PLEASE CONTACT YOUR DEPUY SYNTHES SALES CONSULTANT FOR MORE INFORMATION
FOR MORE INFORMATION ON THE PILLAR CLINICAL TRIAL, VISIT WWW.EXPAREL.COM/PILLAR.
©Pacira Pharmaceuticals, Inc. © DePuy Synthes 2017. All rights reserved.
The third-party trademarks used herein are the trademarks of their respective owners.
PP-EX-US-2818 DSUS/MOC/0717/0799(1)
www.EXPAREL.com/pillar