-
doi: 10.2522/ptj.20090071Originally published online March 25,
2010
2010; 90:663-678.PHYS THER. and Timothy Carl HainJanet Odry
Helminski, David Samuel Zee, Imke JanssenVertigo: A Systematic
Reviewthe Treatment of Benign Paroxysmal Positional Effectiveness
of Particle Repositioning Maneuvers in
http://ptjournal.apta.org/content/90/5/663found online at: The
online version of this article, along with updated information and
services, can be
Collections
Vestibular System Disorders Systematic Reviews/Meta-analyses
Balance Training Balance
in the following collection(s): This article, along with others
on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a
response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
http://ptjournal.apta.org/cgi/eletters/90/5/663be accessed for free
at: 1 e-letter(s) have been posted to this article, which can
E-mail alerts to receive free e-mail alerts hereSign up
at VA Medical CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/cgi/collection/balancehttp://ptjournal.apta.org/cgi/collection/balance_traininghttp://ptjournal.apta.org/cgi/collection/systematic_reviewshttp://ptjournal.apta.org/cgi/collection/vestibular_system_disordershttp://ptjournal.apta.org/letters/submit/ptjournal;90/5/663http://ptjournal.apta.org/subscriptions/etoc.xhtmlhttp://ptjournal.apta.org/
-
Effectiveness of Particle RepositioningManeuvers in the
Treatment ofBenign Paroxysmal Positional Vertigo:A Systematic
ReviewJanet Odry Helminski, David Samuel Zee, Imke Janssen, Timothy
Carl Hain
Background. Benign paroxysmal positional vertigo (BPPV) is the
most commoncause of vertigo.
Purpose. The purpose of this systematic review was to determine
whether pa-tients diagnosed with posterior canal (PC) BPPV, based
on positional testing, andtreated with a particle repositioning
maneuver will show the resolution of benignparoxysmal positional
nystagmus (BPPN) on the Dix-Hallpike Test performed 24hours or more
after treatment.
Data Sources. Data were obtained from an electronic search of
the MEDLINE,EMBASE, and CINAHL databases from 1966 through
September 2009.
Study Selection. The study topics were randomized controlled
trials (RCTs),quasi-RCTs, the diagnosis of PC BPPV, treatment with
the particle repositioningmaneuver, and outcome measured with a
positional test 24 hours or more aftertreatment.
Data Extraction. Data extracted were study descriptors and the
informationused to code for effect size.
Data Synthesis. In 2 double-blind RCTs, the odds in favor of the
resolution ofBPPN were 22 times (95% confidence
interval�3.41–141.73) and 37 times (95%confidence
interval�8.75–159.22) higher in people receiving the canalith
reposition-ing procedure (CRP) than in people receiving a sham
treatment. This finding wassupported by the results reported in 8
nonmasked quasi-RCTs. Studies with limitedmethodological quality
suggested that a liberatory maneuver (LM) was more effectivethan a
control intervention; there was no significant difference in the
effectiveness ofthe LM and the effectiveness of the CRP; the
self-administered CRP was more effectivethan the self-administered
LM; and the CRP administered together with the self-administered
CRP was more effective than the CRP administered alone. The
Brandt-Daroff exercises were the least effective self-administered
treatments.
Limitations. The limitations included the methodological quality
of the studies,the lack of quality-of-life measures, and
confounding factors in reporting vertigo.
Conclusions. Randomized controlled trials provided strong
evidence that theCRP resolves PC BPPN, and quasi-RCTs suggested
that the CRP or the LM performedby a clinician or with proper
instruction at home by the patient resolves PC BPPN.There were no
data on the effects of the maneuvers on outcomes relevant to
patients.
J.O. Helminski, PT, PhD, is Associ-ate Professor, Department
ofPhysical Therapy, MidwesternUniversity, 555 31st St,
DownersGrove, IL 60515 (USA). Address allcorrespondence to Dr
Helminskiat: [email protected].
D.S. Zee, MD, is Professor, Depart-ments of Neurology,
Ophthalmol-ogy, Otolaryngology, and Pathol-ogy, School of Medicine,
TheJohns Hopkins University, Balti-more, Maryland.
I. Janssen, PhD, is Assistant Profes-sor, Department of
PreventiveMedicine, Rush University MedicalCenter, Chicago,
Illinois.
T.C. Hain, MD, is Professor, De-partments of Physical Therapy
andHuman Movement Science, Oto-laryngology, and
Neurology,Northwestern University MedicalSchool, Chicago,
Illinois.
[Helminski JO, Zee DS, Janssen I,Hain TC. Effectiveness of
particlerepositioning maneuvers in thetreatment of benign
paroxysmalpositional vertigo: a systematicreview. Phys Ther.
2010;90:663–678.]
© 2010 American Physical TherapyAssociation
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
May 2010 Volume 90 Number 5 Physical Therapy f 663 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
Benign paroxysmal positionalvertigo (BPPV) is characterizedby
brief periods of vertigo trig-gered by a change in the position ofa
person’s head relative to gravity. Inthe general population, the
lifetimeprevalence of BPPV is 2.4%, and the1-year incidence is
0.6%.1 It is themost common vestibular disorder,accounting for one
third of vestibu-lar diagnoses in the general popula-tion.1 Benign
paroxysmal positionalvertigo can affect the quality of life
ofelderly patients and is associatedwith reduced activities of
daily liv-ing, falls, and depression.2 Patientswith BPPV experience
delays in diag-nosis and treatment, the mean delaybeing 92 weeks,
and they frequentlyare inappropriately treated with ves-tibular
suppressant medications.3
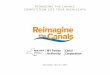
Benign paroxysmal positional ver-tigo is caused by abnormal
mechan-ical stimulation of 1 or more of the 3semicircular canals
within the innerear (Fig. 1). The fluid-filled canalsnormally act
to detect rotation of thehead through the deflection of sen-sory
hair cells embedded within agelatinous membrane, the cupula.The
weighted sensory membrane ofthe maculae normally acts to
detectgravitational forces on the head. InBPPV, calcite particles
(otoconia),which normally weight this mem-brane, become dislodged
and sedi-ment in the canals, changing the dy-namics of the canals.
There are 2primary theories for the mechanismof BPPV. The first is
cupulolithiasis,4
in which the dislodged otoconia di-
rectly attach to the cupula, weight-ing this membrane.
Reorientation ofthe canal relative to gravity deflectsthe cupula,
exciting or inhibiting theampullary organ. The second is
cana-lithiasis,5 in which the otoconiafreely sediment in the
canals. Reori-entation of the canals causes the oto-conia to move
to the lowest part ofthe canals, creating a drag on theendolymph,
resulting in fluid pres-sure on the cupula, and activatingthe
ampullary organ.
The Dix-Hallpike maneuver,6 re-ferred to as the Dix-Hallpike
Test(DHT) in this article, is the standardfrom which the diagnosis
of poste-rior canal (PC) BPPV is made anddifferentiated from other
condi-tions.7,8 The diagnostic criteria forPC BPPV are vertigo
associated withcharacteristic ocular nystagmus thatis torsional
(toward the dependentear) and directed upward, consistentwith the
excitation of the ampullaryorgan of the PC9; a 1- to
40-secondlatency before the onset of vertigoand nystagmus10–12; and
vertigo andnystagmus with a duration of lessthan 60 seconds.13 With
repeated po-sitioning, PC BPPV temporarily be-comes less intense
and disappears.13
For the DHT, the estimated sensitiv-ity and specificity are 79%
(95% con-fidence interval [CI]�65–94) and75% (CI�33–100),
respectively.14
The interrater reliability for inter-preting the direction of
eye move-ment ranges from a mean percentageof agreement of 43%
(fair) to a meanpercentage of agreement of 81%(substantial),
depending on the levelof expertise.15
Treatment of BPPVOnce the involved canal is identified,BPPV
often is treated with particlerepositioning maneuvers. These
ma-neuvers move otoconia out of theaffected canal and back into the
ves-tibule, where it is thought that theparticles
dissolve.16,17
Historically, the first maneuvers usedfor BPPV were the
Brandt-Daroff ex-ercises,10 which were designed tohabituate
symptoms. The patient re-peatedly moved from sitting at theedge of
the bed to lying on the side(side lying) with the head rotated
45degrees toward the ceiling. The pa-tient alternated between left
side ly-ing and right side lying.
The canalith repositioning proce-dure (CRP), developed by
Epley18
(Fig. 2A), was designed to use gravityto treat canalithiasis of
the PC. Theclinician moves the patient througha series of 4
positions. With eachposition, the otoconia settle to thelowest part
of the canal, movearound the arc of the PC, and finallydeposit in
the vestibule. This proce-dure requires a 180-degree turn ofthe
head19–21 and a return to a sittingposition from lying on the
unin-volved side.21 To enable the otoco-nia to settle, each
position is main-tained for at least 30 seconds.20
Vibration applied to the mastoidprocess of the involved side
doesnot affect the outcome of the pro-cedure and is no longer
considerednecessary.22–24
The liberatory maneuver, developedby Semont et al25 (Fig. 2B),
was de-signed to use inertia and gravity totreat cupulolithiasis of
the PC. Toevacuate the particles, the patient israpidly swung from
lying on the in-volved side to lying on the unin-volved side
through a 180-degreecartwheel motion with a duration ofless than
1.3 seconds.19
Both the CRP and the liberatory ma-neuver have been modified to
enablea patient to self-treat. With the self-administered CRP,26,27
the patientmoves through the same positions asin the CRP, except
that the head isextended over the edge of a pillow.With the
self-administered liberatorymaneuver,27 the patient performsthe
maneuver independently, with
Available WithThis Article atptjournal.apta.org
• The Bottom Line
• Audio Abstracts Podcast
This article was published ahead ofprint on March 25, 2010,
atptjournal.apta.org.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
664 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/cgi/content/full/90/5/DC1http://ptjournal.apta.org/cgi/content/full/90/5/DC1http://ptjournal.apta.org/
-
no other modifications. Both exer-cises are stopped when the
patienthas been vertigo free for at least 24hours.26,27
The role of activity restrictions in theoutcome of particle
repositioningmaneuvers remains uncertain. Post-maneuver activity
restrictions didnot improve the efficacy of treat-ment with the
CRP28,29 or the libera-tory maneuver,28 but patients withno
activity restrictions required 1 or2 more treatment sessions to
achievea successful outcome.30
The DHT is critical for determiningthe outcome of particle
reposition-ing maneuvers.7,31 The absence ofthe characteristic
nystagmus indi-cates the resolution of PC BPPV.32
The patient’s report of vertigo ismore variable than the
observationof the characteristic nystagmus onpositional testing.
Patients showing
Figure 1.Mechanisms of benign paroxysmal positional vertigo.
Reprinted with permission from American Dizziness and Balance.
Copyright2007.
The Bottom Line
What do we already know about this topic?
Randomized controlled trials (RCTs) suggest that the canalith
reposition-ing procedure (CRP) is more effective than a sham
treatment in theresolution of posterior canal benign paroxysmal
positional nystagmus (PCBPPN).
What new information does this study offer?
Evidence for the use of other particle repositioning maneuvers
is weakdue to the limited numbers of studies and no RCTs. There is
no significantdifference in the effectiveness of the CRP compared
with the liberatorymaneuver (LM). If properly instructed,
self-administered CRP and LM areeffective. The Brandt-Daroff
habituation exercises are the least effective.The most effective
treatment is a combination of the CRP and the self-administered
CRP.
If you’re a patient, what might these findings mean foryou?
The CRP and LM performed by a clinician or, with proper
instruction, bythe patient at home resolves PC BPPN.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 665 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
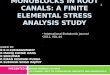
Figure 2.Particle repositioning maneuvers. (A) Canalith
repositioning procedure illustrated for treatment of the right
posterior canal. The clinicianmoves the patient through a series of
4 positions, starting with the placement of the involved canal in
the head-hanging position of theDix-Hallpike Test. To begin, the
patient is positioned in the long sitting position (sitting on the
treatment table with the legs extended).The patient’s head is
rotated 45 degrees toward the right. The patient is then lowered
into the supine position with the neck extended 20degrees over the
edge of the treatment table; this is the head-hanging position. The
head is rotated through 90 degrees of motion, endingin 45 degrees
of neck rotation toward the uninvolved side. This step is followed
by rolling onto the uninvolved side while maintaining
thehead-on-trunk position and, finally, sitting up from lying on
the uninvolved side. Each position is maintained for a minimum of
30 secondsor as long as the nystagmus lasts. The procedure is
repeated 3 times. (B) Liberatory (Semont) maneuver illustrated for
treatment of the rightposterior canal. The patient sits on the edge
of the treatment table. The clinician rapidly moves the patient to
lying on the involved sidewith the head rotated 45 degrees toward
the uninvolved side. While maintaining the head-on-trunk position,
the clinician swings thepatient from lying on the involved side to
lying on the uninvolved side. The head then is gently tapped on the
treatment table. Each positionis maintained for 1.5 minutes. The
procedure is repeated 3 times. Reprinted with permission from
American Dizziness and Balance.Copyright 2007.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
666 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
the resolution of positional nystag-mus on the DHT may report
vertigoif concurrent vestibular deficits ex-ist.33 Patients with
positive findingson the DHT may report no vertigo atthe time of
follow-up if provokingpositions are avoided or if they
haveunrecognized BPPV (imbalance withno vertigo).2 Because of these
con-founding factors, the patient’s reportof vertigo should not be
the onlyoutcome measure.
The time interval between treatmentand outcome assessment is
critical.To separate the effects of activetreatment from a fatigue
response,outcome should be assessed 24hours or more after
treatment.32 Re-peated positioning may cause a fa-tigue response
that can mimic suc-cessful treatment.32 Within 7 days ofPC BPPV
symptom onset, 30% of pa-tients will experience
spontaneousremission.34 To minimize the possi-bility of spontaneous
remission caus-ing a false-negative particle reposi-tioning
maneuver outcome and toavoid a fatigue response, outcomeideally
should be assessed 24 hoursafter treatment.
Patients with BPPV experience a de-crease in health-related
quality of life,which is restored after successful re-mission of
BPPV following treatmentwith a particle repositioning maneu-ver.35
However, health-related quality-of-life measures are not routinely
usedin treatment outcome studies.
A published overview of the CochraneCollaboration (search dates:
1966–2004)36 and 2 meta-analyses37,38 evalu-ated the effectiveness
of the CRP inthe treatment of BPPV but did not eval-uate other
maneuvers. Two recentlypublished practice guidelines7,8 evalu-ated
the effectiveness of the CRP, theliberatory maneuver, and the
self-administered variants. These publica-tions included
assessments of themethodological quality of the studiesevaluated. A
rigorous qualitative syn-
thesis needs to include an evaluationnot only of the
methodological qualitybut also of the precise performance ofthe
intervention and the validity, reli-ability, and responsiveness of
the testsused in the studies.39
The purpose of this systematic re-view was to determine whether
pa-tients diagnosed with PC BPPV onpositional testing and treated
with aparticle repositioning maneuver willshow the resolution of
benign parox-ysmal positional nystagmus (BPPN)on the DHT performed
24 hours ormore after treatment. A synthesisof methodological
quality was per-formed. The standards of method-ological quality
for this systematicreview were randomization,40 alloca-tion
concealment,41,42 masking,43
and sample size calculation.44 TheCRP, the liberatory maneuver,
andthe self-administered variants wereevaluated. The inclusion and
exclu-sion criteria were based on the find-ings of the proposed
mathematicalmodels of the treatment of BPPV19–21
with the particle repositioning ma-neuvers to take into account
thequality of the performance of the in-tervention and were based
on theperformance of the DHT as an out-come measure to take into
accountthe validity and reliability of theoutcome. The
responsiveness of theDHT has not been reported in
theliterature.
MethodData Sources and SearchesAn electronic literature search
of theMEDLINE, EMBASE, and CINAHL da-tabases for the period from
1966through September 2009 was con-ducted with the medical
subjectheading term “vertigo.” In MEDLINE,to refine the search, the
medical sub-ject heading was combined with an“or” statement
including “benignparoxysmal positional vertigo, BPPV,BPV, benign
paroxysmal positionalnystagmus, BPPN, or BPN.” Thesearch was
restricted to English (pos-
sibly introducing publication bias).In CINAHL, the search was
repli-cated with the same terms. In EM-BASE, because of more
specific index-ing, the search was performed withthe medical
subject heading “ver-tigo” and the subheadings “BPPV”and “therapy.”
A published over-view of the Cochrane Collaboration(search dates:
1966–2004),36 2 meta-analyses37,38 of the treatment of PCBPPV, and
2 practice guidelines7,8
were also reviewed. Bibliographiesof the identified articles
were manu-ally searched for any additional rele-vant articles. The
results of thesearches were compared, and dupli-cates were removed
(Fig. 3).
Study SelectionPublished studies that reported onthe
effectiveness of particle reposi-tioning maneuvers in the
treatmentof PC BPPV were eligible for inclu-sion. The inclusion
criteria (Tab. 1)were as follows:
1. The study design was a random-ized controlled trial (RCT)
orquasi-RCT.
2. Participants had a clinical diagno-sis of unilateral typical
BPPV (PCinvolvement) on the basis of thefindings on the DHT.7,8
3. A manual particle repositioningmaneuver was performed. If
theCRP was used, it included all 4positions described originally
byEpley18 to optimize the removalof loose otoconia from thePC.19–21
For the best outcome,simulated models of the CRP sug-gested from
the initial head-hanging position a full 180-degreeturn of the head
toward the unin-volved side and a return to theupright position
from the unin-volved side.19–21 Acceptable mod-ifications to the
original CRP in-cluded self-administration,26,27,45
performance of the procedure
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 667 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
Table 1.Inclusion and Exclusion Criteriaa
ParameterAngeliet al54
Asawavichiangindaet al55 Blakley56
Califanoet al57
Cavaliereet al58
Changet al59
Cohenand
Kimball60Froehling
et al49 Li61Lynn
et al33
Inclusion criteria
RCT, quasi-RCT � � � � � � � � �
Typical BPPV � � � � � � � � �
Intervention
Manual particlerepositioning maneuver
� � � � � � � � � �
CRP with positionsdescribed by Epley18
� � � � � � �
Administered by:
Clinician � � � � � � �
Self
Activity restrictionsafter treatment
Yes � � � � �
No � � � � �
Outcome
DHT or side-lying testto assess nystagmus
� � � � � � �
Outcome assessed�24 h and �1 mo aftertreatment
� � � � � �
Proportion of participantswho converted frompositive to
negativeDHT results reported
� � � �
Exclusion criteria
Cohort, retrospective,case-control, or casestudy
�
No inclusion criteria �
Atypical BPPV
Bilateral PC BPPV �
Central nervoussystem dysfunction
Intervention: CRP withmodification of positionsdescribed by
Epley18
� �
Outcome: no DHT orside-lying test toassess nystagmus
� � �
a RCT�randomized controlled trial, BPPV�benign paroxysmal
positional vertigo, CRP�canalith repositioning procedure,
DHT�Dix-Hallpike Test,PC�posterior canal.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
668 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
Table 1.Continued
Parameter
Massoudand
Ireland28Munozet al62
Radtkeet al26
Radtkeet al27
Salvinelliet al50
Salvinelliet al51
Serafiniet al63
Shermanand
Massoud52
SotoVarelaet al53
Sridharet al64
Inclusion criteria
RCT, quasi-RCT � � � � � � � � �
Typical BPPV � � � � � � � � � �
Intervention
Manual particlerepositioning maneuver
� � � � � � � � � �
CRP with positionsdescribed by Epley18
� � � � � �
Administered by:
Clinician � � � � � � � �
Self � �
Activity restrictionsafter treatment
Yes � �
No � � � � � � � �
Outcome
DHT or side-lying testto assess nystagmus
� � � � � � � � � �
Outcome assessed�24 h and �1 mo aftertreatment
� � � � � � � � �
Proportion of participantswho converted frompositive to
negativeDHT results reported
� � � � � � � � � �
Exclusion criteria
Cohort, retrospective,case-control, or casestudy
� �
No inclusion criteria
Atypical BPPV
Bilateral PC BPPV �
Central nervoussystem dysfunction
Intervention: CRP withmodification of positionsdescribed by
Epley18
Outcome: no DHT orside-lying test toassess nystagmus
(Continued)
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 669 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
without the use of vibration,22–24
no activity restrictions after theprocedure,28–30 and no
premedi-cation to avoid nausea.
4. The successful outcome of a par-ticle repositioning maneuver
wasdefined as the conversion of apositive DHT result to a
negativeDHT result or side-lying test re-sult33 24 hours or more
after theinitial treatment procedure toavoid the fatiguing
response32 butless than 1 month later to sepa-rate the effects of
active treat-ment from natural history.34
5. The proportion of participantswho showed conversion
fromnystagmus to no nystagmus onthe DHT at the time of follow-upwas
reported.
The exclusion criteria (Tab. 1) wereas follows:
1. The study was a cohort study, aretrospective study, a
case-control study, or a case study.
2. No inclusion criteria weredescribed.
3. Participants had a clinical diagno-sis of atypical BPPV
(lateral canalor anterior canal involvement), bi-lateral PC BPPV
due to confound-ing variables,46 or central vestibu-lar
deficit.
4. The head positions of the CRPoriginally described by
Epley18
were modified. The CRP was per-formed with less than 180
de-grees of head rotation from theinitial head-hanging position
anda return to the upright positionfrom the involved side.19–21
5. The successful outcome of a par-ticle repositioning maneuver
wasdefined only as the resolution ofvertigo.
Table 1.Continued
ParameterTanimoto
et al45
vonBrevernet al32
Wolfet al65
Yimtaeet al66
Inclusion criteria
RCT, quasi-RCT � � � �
Typical BPPV � � � �
Intervention
Manual particlerepositioning maneuver
� � � �
CRP with positionsdescribed by Epley18
� � �
Administered by:
Clinician � � � �
Self �
Activity restrictionsafter treatment
Yes �
No � � �
Outcome
DHT or side-lying testto assess nystagmus
� � � �
Outcome assessed�24 h and �1 mo aftertreatment
� � � �
Proportion of participantswho converted frompositive to
negativeDHT results reported
� � � �
Exclusion criteria
Cohort, retrospective,case-control, or casestudy
No inclusion criteria
Atypical BPPV
Bilateral PC BPPV �
Central nervoussystem dysfunction
Intervention: CRP withmodification of positionsdescribed by
Epley18
�
Outcome: no DHT orside-lying test toassess nystagmus
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
670 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
6. A successful outcome was assessedless than 24 hours after
treatment.
7. The proportion of participantswho showed successful
conver-sion from nystagmus to no nystag-mus on the DHT at the time
offollow-up was not documented.
Data Extraction and QualityAssessmentAbstracts were screened. If
the studywas an RCT or a quasi-RCT and thestudy population was
diagnosedwith PC BPPV, then the article wasobtained and reviewed by
2 review-ers (J.O.H. and D.S.Z.). When dis-crepancies occurred, the
reasonswere identified, and a final decisionwas made on the basis
of the unani-mous agreement of the authors
(J.O.H., D.S.Z., and T.C.H.). Thestudies were stratified
according tothe particle repositioning maneuver.
The methodological quality stan-dards for this systematic review
wererandomization,40 allocation conceal-ment,41,42 masking,43 and
samplesize calculation.44 Lack of randomiza-tion, allocation
concealment, ormasking could change the treatmenteffects, resulting
in study selectionand confounding biases. Lack of cal-culation of
the sample size could re-sult in a greater risk of a type
IIerror.44
Data were extracted, and a data formwas completed to evaluate
the meth-odological quality and quality of theinterventions, tests,
and outcomes of
each study. The data collection formconsisted of items compiled
from acombination of instruments.39,47,48
Information was obtained on the set-ting, study design, patient
selectionprocess, masking, intervention, out-comes, and statistics
to evaluate thecomponents of internal validity (se-lection bias,
performance bias, de-tection bias, and attrition bias) andexternal
validity (patients, interven-tion, setting, and outcomes) for
po-tential bias. In addition, we compiledthe following variables:
patient re-port and quantitative outcomes onpositional testing at
short-termfollow-up (first follow-up session)and long-term
follow-up (if multiplefollow-up sessions, last
session),complications, and postprocedureinstructions. When studies
used re-
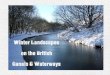
Figure 3.Preferred Reporting Items for Systematic Reviews and
Meta-Analyses (PRISMA) statement flow diagram of the literature
search.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 671 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
peated follow-up periods, the short-est time between 1 and 30
days tofollow-up was used to allow for thestrongest association
between treat-ment and outcome. Studies that metthe inclusion
criteria were stratifiedaccording to the study design
andintervention.
Data Synthesis and AnalysisTo assess the outcome of each
study,the effect size was calculated. Thesuccessful outcome of a
particle re-positioning maneuver was defined asthe conversion of a
positive posi-tional test to a negative positionaltest (no BPPN).
The patient’s reportof vertigo was not qualitatively ana-lyzed.
Two-by-two contingency ta-bles were used to organize the out-come
data. The odds ratio (OR) andthe 95% CI were calculated to
deter-mine the odds of a successful out-come or a negative
positional test.The OR measures the association be-tween treatment
and outcome. Forquasi-RCTs comparing active treat-ments, the OR was
calculated withthe standard treatment (control) asthe CRP. The CRP
was selected asthe standard of treatment becausethe 2 RCTs
supported its effective-ness.32,33 Only trials in which ran-domized
treatment assignments anda clearly defined control group wereused
were considered for inclusionin a meta-analysis. Because only 2such
trials existed, a meta-analysiswas not performed. We
includedquasi-RCTs and nonmasked trials inthe systematic review. We
acknowl-edge that these studies may be bi-ased and may overestimate
treat-ment efficacy.
Statistical analysis of the data wasperformed with SAS/STAT
(version9.1).* All tests of significance wereperformed at an �
level of .05.
ResultsInitially, 868 records were identifiedthrough an
electronic database search(Fig. 3). From these records, 24
full-text articles were assessed for eligibil-ity on the basis of
their titles and ab-stracts. After complete articles wereread, only
10 articles met the inclusioncriteria,27,28,32,33,45,49–53 and 14
met theexclusion criteria.26,54–66 The mainreasons for exclusion
were study de-sign, inclusion criteria (no inclusioncriteria
discussed or bilateral PC BPPVincluded), modifications to the
headposition used in the CRP, outcome notmeasured with a positional
test, out-come assessed less than 24 hours ormore than 1 month
after treatment,and inadequate statistics (Tab. 1).
Of the 10 articles included in thequalitative synthesis, 2
studies usedsealed envelopes with a computer-generated
randomization code32 or ablock randomization scheme (num-bered,
sealed envelopes containingtreatment group assignments, pre-pared
before the start of the study)33
to randomly allocate their partici-pants to groups. Two studies
quasi-randomly allocated their partici-pants to groups on the basis
of thedate of their first visit.51,52 Six studiesstated that
participants were ran-domly allocated to groups but didnot describe
the method of ran-domization.27,28,45,49,50,53 Maskingof
participants and outcome oc-curred in 3 studies.32,33,49 None ofthe
studies reported calculation ofthe sample size.27,28,32,33,45,49
–53 At-trition was described but was notincluded in statistical
calculationsin 8 studies (intention-to-treat
anal-ysis)27,28,32,33,45,49,52,53 and was notaddressed in the
remaining 2 arti-cles.50,51 A summary of the itemsincluded to
assess the methodolog-ical quality of the studies is pro-vided in
Table 2.
Two RCTs32,33 and 2 quasi-RCTs49,52
compared the effectiveness of the CRPwithout vibration and the
effective-
ness of a sham treatment.32,33,49,52 Atshort-term follow-up, the
success ratesfor patients treated with the CRP were67% to
95%,32,33,49,52 those obtainedwith the sham treatment were 10%
to38%,32,33,49,52 and that obtained withthe control was 60%.52 The
magnitudeof the effect of the CRP comparedwith that of the sham
treatment wassignificant in all 4 studies.32,33,49,52 Be-cause of
the small sample sizes andthe wide confidence intervals,
ho-mogeneity could not be determined.The odds in favor of symptom
reso-lution in the RCTs were 22 to 37times higher in people
receivingthe CRP32,33 and were more variablein the quasi-RCTs (3–25
timeshigher).49,52
Two quasi-RCTs compared the lib-eratory maneuver and no
treatment(control).50,51 At short-term follow-up, the success rates
for patientstreated with the liberatory maneuverwere 80% to 85%,
whereas sponta-neous resolution in the controlgroup was 35% to 38%.
The odds infavor of symptom resolution were 7to 10 times higher in
patients receiv-ing the liberatory maneuver than inthe control
group (Tab. 3). Theremay have been overlap of partici-pants in
these 2 studies becausethe data were collected over thesame time
periods by the sameauthors.50,51
Two quasi-RCTs compared the CRPand the liberatory maneuver.28,53
Atshort-term follow-up, the successrates were 71% to 93% for the
CRPand 74% to 92% for the liberatorymaneuver. To calculate the OR,
theCRP was selected as the standard oftreatment. The odds in favor
ofsymptom resolution were 0.80 and1.16 higher in participants using
theCRP, and the 95% CIs included 1,suggesting no significant
differencein effectiveness between the libera-tory maneuver and the
CRP.
* SAS Institute Inc, 100 SAS Campus Dr, Cary,NC 27513-2414.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
672 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
Table 2.Summary of Methodological Qualitya
ParameterFroehling
et al49Lynn
et al33
Massoudand
Ireland28Radtkeet al27
Salvinelliet al50
Salvinelliet al51
Shermanand
Massoud52
SotoVarelaet al53
Tanimotoet al45
vonBrevernet al32
Setting Urgentcare/IM
Oto OP Oto/Neuro Oto Oto BD Oto Oto Oto/Neuro
Study design Quasi-RCT RCT Quasi-RCT Quasi-RCT Quasi-RCT
Quasi-RCT Quasi-RCT Quasi-RCT Quasi-RCT RCT
Participant selection
Inclusion andexclusioncriteria
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Method ofrandomization
No Yes No No No No No No No Yes
Method of quasi-randomization
Yes Yes Yes Yes Yes Yes Yes Yes
Method ofrandomizationconcealed
No Yes No No No No No No No Yes
Baselinecomparability
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Masking
Masking ofparticipants
Yes Yes No No No No No No No Yes
Masking ofoutcome
Yes Yes No No No No No No No Yes
Intervention
Treatmentprotocoladequatelydescribed
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Control orplaceboadequate
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Testing ofparticipantadherence totreatmentprotocol
No Yes No Yes No No No No Yes No
Description ofwithdrawaland dropouts
NA Yes NA Yes No No Yes Yes Yes Yes
Participantfollow-updetailsreported
Yes Yes Yes Yes No No Yes Yes Yes Yes
Follow-up periodadequate
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Outcomes
Outcomemeasuredescribed
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Relevantoutcomes used
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
(Continued)
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 673 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
Three quasi-RCTs reported the resultsof self-administered
maneuvers27,45,53
(Tab. 3). All of these studies compared2 or more maneuvers. At 1
week, thesuccess rates were 90% to 95% for theself-administered CRP
or the CRP ad-ministered together with the self-administered
CRP,27,45 58% for theself-administered liberatory maneu-ver,27 and
24% for the Brandt-Daroffexercises.53 The low success rate forthe
Brandt-Daroff exercises in thosestudies was contrary to the high
suc-cess rate (98%) originally describedin a 2-week, nonrandomized
trialwith longer treatment durations.10
To calculate the OR, the CRP wasselected as the standard of
treat-ment. If CRP was not performed,then the self-administered CRP
wasselected. The odds in favor of symp-tom resolution were only
0.13 timeshigher in participants using theBrandt-Daroff exercises
(OR�0.13,95% CI�0.04–0.38) and 0.08 timeshigher in participants
using theself-administered liberatory maneu-
ver (OR�0.08, 95% CI�0.02–0.38)(Tab. 3). The odds in favor of
symp-tom resolution were 3.54 timeshigher (95% CI�1.02–12.30)
withthe CRP plus the self-administeredCRP than with the CRP
alone(Tab. 3), suggesting better outcomeswith the performance of a
combina-tion of the CRP plus the self-administered CRP.
Two RCTs32,33 comparing the effec-tiveness of the CRP without
vibra-tion and the effectiveness of a shamtreatment were eligible
for quantita-tive synthesis. Because of the limitednumber of
studies, a meta-analysiswas not performed.
DiscussionThis systematic review evaluated theeffectiveness of
several particle repo-sitioning maneuvers, namely, theCRP, the
liberatory maneuver, andthe self-administered variants, in
thetreatment of PC BPPV. The presentsystematic review is a
qualitative syn-
thesis of methodological quality. Ourinclusion and exclusion
criteria tookinto account the quality of the per-formance of the
intervention and theappropriateness of the tests and mea-sures
used.
Our inclusion and exclusion criteriawere based on the findings
of theproposed mathematical models forthe treatment of BPPV19–21
with theparticle repositioning maneuvers.We excluded studies that
includedparticipants with bilateral BPPV toavoid confounding
variables.56,64,65
We did not rate the methodologicalquality of the articles but
provided adescription of the quality becausenot all of the
qualitative scales ad-dressed the quality of the physicaltherapy
interventions and the valid-ity, reliability, and responsiveness
ofthe outcomes used.39
Our results agree with those of ear-lier reviews7,8,36–38—that
the CRP ismore effective than a control in the
Table 2.Continued
ParameterFroehling
et al49Lynn
et al33
Massoudand
Ireland28Radtkeet al27
Salvinelliet al50
Salvinelliet al51
Shermanand
Massoud52
SotoVarelaet al53
Tanimotoet al45
vonBrevernet al32
Use ofquantitativeoutcomemeasure
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Statistics
Descriptivemeasuresidentified andreported forprimaryoutcome
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Appropriatestatistics used
Yes Yes Yes Yes No Yes Yes Yes Yes Yes
Sample sizecalculationperformed
No No No No No No No No No No
Adequate samplesize
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
Intention-to-treatanalysis used
NA No NA No No No No No No No
a IM�internal medicine, Oto�otolaryngology, OP�outpatient,
Neuro�neurology, BD�balance and dizziness, RCT�randomized
controlled trial, NA�notavailable.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
674 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
treatment of PC BPPV. On the basisof our inclusion and
exclusioncriteria, only 2 studies32,33 met thecriteria for
quantitative synthesis;therefore, a meta-analysis was notperformed.
The greater variability inthe quasi-RCTs may have been due to
the clinical expertise of the studypersonnel49 or to a
difference in thepatient populations. Professionalswere trained to
evaluate ocular nys-tagmus during positional testing.49
The interrater reliability for inter-preting the direction of
eye move-
ment varied depending on the levelof expertise.15 The low OR may
re-flect the lack of experience of thetrained professionals in
evaluatingeye movements and may support theneed for experienced
professionalsto treat BPPV to minimize delays in
Table 3.Information Used to Code for Effect Size
Study Group
Outcome Outcome Measures
No. ofParticipants/
Group
No. ofParticipants
WithNegative
Dix-HallpikeTest Result
% ofParticipants
Cured
ReportedLevel of
Significance(P) Groups
Odds Ratio(95% Confidence
Interval)
Lynn et al33 CRP 18 16 89 �.001 CRP vs sham 22.0
(3.41–141.73)
Sham 15 4 27
Massoud andIreland28,a
CRP 46 43 93 �.2b LM vs CRP 0.80 (0.17–3.79)
LM 50 46 92
Froehling et al49 CRP 24 16 67 .046 CRP vs sham 3.20
(1.00–10.20)
Sham 26 10 38
Sherman andMassoud52
CRP 33 27 82 .06 CRP vs sham 24.75 (4.31–142.02)
Sham 13 2 15
Control 25 15 60
Soto Varela et al53,a Brandt-Daroffexercises
29 7 24 �.00001 Brandt-Daroffexercises vsCRP
0.13 (0.04–0.38)
LM 35 26 74 .15315b LM vs CRP 1.16 (0.42–3.18)
CRP 42 30 71
Salvinelli et al50 LM 40 32 80 �.01 LM vs control 6.67
(2.44–18.21)
Control 40 15 38
Radtke et al27,c Self-administeredCRP
37 35 95 �.001 Self-administeredLM vs self-administeredCRP
0.08 (0.02–0.38)
Self-administeredLM
33 19 58
Salvinelli et al51 LM 52 44 85 �.001 LM vs control 10.39
(4.04–26.74)
Flunarizine 52 30 58
Control 52 18 35
Tanimoto et al45,a CRP only 39 28 72 .048 Self-administeredCRP
vs CRP
3.54 (1.02–12.30)
CRP and self-administeredCRP
40 36 90
von Brevern et al32 CRP 35 28 80 �.001 CRP vs sham 37.33
(8.75–159.22)
Sham 31 3 10
a Quasi-randomized controlled trial; standard treatment:
canalith repositioning procedure (CRP).b No significance of
comparison of liberatory maneuver (LM) and CRP.c Quasi-randomized
controlled trial; standard treatment: self-administered CRP.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 675 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
treatment and reduce health carecosts.
The liberatory maneuver was effec-tive in the treatment of PC
BPPV, andthe quasi-RCTs found that the libera-tory maneuver was as
effective as theCRP. However, RCTs need to be per-formed to
determine whether theliberatory maneuver is more effec-tive for PC
BPPV than a sham treat-ment and whether there is a correla-tion
between the speed at which themaneuver is performed and the
suc-cess of the maneuver.19
The self-administered CRP was moreeffective than the
self-administeredliberatory maneuver in the treatmentof PC BPPV.
More patients per-formed the self-administered libera-tory maneuver
incorrectly than per-formed the self-administered CRPincorrectly.
The Brandt-Daroff exer-cises had little or no effect on symp-tom
resolution.53 Although this con-clusion is based on a
singlerandomized study, the low successrate of the Brandt-Daroff
exerciseswas consistent with the findings ofan earlier
nonrandomized trial.26
Therefore, the self-administered CRPhas the highest reported
treatmentefficacy, whereas the Brandt-Daroffexercises have the
lowest reportedefficacy. For this reason, the Brandt-Daroff
exercises are not recom-mended as an initial treatment ma-neuver.
Patients should be physicallyand mentally screened to
determinewhether they are good candidatesfor instruction in and
correct perfor-mance of self-administered maneu-vers. To optimize
outcomes, all pa-tients should receive illustratedinstructions with
specific exercisesfor the affected ear, perform the ex-ercises
under the supervision of anexperienced clinician, and be askedto
perform the maneuver at the timeof follow-up to assess the accuracy
ofperformance.27
Although these data demonstratethat the CRP, the liberatory
maneu-ver, and the self-administered variantof the CRP are
effective treatmentsfor PC BPPV,27,28,32,33,45,49–53,57 clini-cians
must recognize that with bothof these maneuvers, there is achance
(2.5%–6%) of causing a tran-sient worsening of the patient’s
con-dition through a “canal conversion”from the PC to the lateral
canal.45,67
Because of this possibility, cliniciansusing these maneuvers
should beable to recognize and treat lateralcanal BPPV, although in
most casesthe complication resolves on itsown. Patients performing
self-administered treatments should beeducated about the
possibility of acanal conversion. Unfortunately,RCTs regarding the
treatment of lat-eral canal BPPV are not available.
Limitations of Study/Further InvestigationOnly 2 RCTs32,33
compared the effec-tiveness of the CRP and the effective-ness of a
control in the treatment ofPC BPPV. The limited number ofstudies
prevented us from includingthe articles in a quantitative
synthe-sis or meta-analysis. The method-ological quality was low
and theprobability of bias was high in stud-ies investigating the
effectiveness ofthe liberatory maneuver and self-administered
variants. Therefore, in-terpretation of the data should belimited.
Randomized controlled tri-als investigating the effectivenessof the
liberatory maneuver and self-administered variants need to
beconducted.
The CRP was designed to use theforces associated with gravity
totreat canalithiasis of the PC,18 andthe liberatory maneuver was
de-signed to use both inertia and gravityto treat cupulolithiasis
of the PC.25
The mechanism of BPPV may bedetermined on the basis of the
char-acteristic nystagmus parameters oflatency to onset, duration,
and am-
plitude. The nystagmus parameterswere not reported for the
particlerepositioning maneuvers; therefore,correlations between the
mecha-nism of BPPV and the outcome of themaneuvers could not be
determined.Further research on this topic isneeded.
Two studies reported by the sameauthors attempted to
evaluatequality-of-life measures before and af-ter the treatment of
PC BPPV withthe liberatory maneuver.50,51 Infor-mation was
insufficient to draw anyconclusions. Further studies assess-ing the
quality of life before and afterthe successful treatment of PC
BPPVwith particle repositioning maneu-vers are needed.
We did not qualitatively assess theoutcome of the patient’s
report ofvertigo. The patient’s report of ver-tigo may be assessed
during the DHTor with the patient’s daily routine (1week before the
follow-up appoint-ment). The scales vary in that theyuse the
frequency of reports of ver-tigo, the intensity of vertigo on
ananalog scale of 1 to 10, and catego-rization of the resolution of
BPPV onthe basis of a combination of subjec-tive symptoms and
findings on theDHT. There was considerable vari-ability in the
collection of the reportsof vertigo. The resolution of vertigowas
reported at follow-up during po-sitional testing,32,49 within 1
week offollow-up during daily activities,33 atfollow-up with the
completion of aquestionnaire (Vestibular DisordersActivities of
Daily Living Scale68),50,51
through categorization of the resolu-tion of both symptoms and
nystag-mus45,53 as first described by Epley,18
or no mention of symptoms.27,28,52
The development of a means for as-sessing the patient’s report
of vertigois indicated.
ConclusionRandomized controlled trials sug-gested that the CRP
was more effec-
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
676 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
tive than a control in the resolutionof BPPN in patients with PC
BPPV.The evidence for the use of otherparticle repositioning
maneuvers inthe treatment of PC BPPV was weak.There were limited
numbers of stud-ies and no RCTs. Individual resultssuggested that
the liberatory maneu-ver was more effective than a con-trol; there
was no significant differ-ence in the effectiveness of
theliberatory maneuver and the effective-ness of the CRP; the
self-administeredCRP was more effective than the self-administered
liberatory maneuver; andthe CRP administered together withthe
self-administered CRP wasmore effective than the CRP admin-istered
alone. The Brandt-Daroff ex-ercises were the least effective
self-administered treatments. There wereno data on the effects of
the particlerepositioning maneuvers on out-comes relevant to
patients.
Dr Helminski, Dr Zee, and Dr Hain providedconcept/idea/research
design and writing.Dr Helminski provided data collection andproject
management. Dr Helminski and DrJanssen provided data analysis. Dr
Hain pro-vided consultation (including review ofmanuscript before
submission). The authorsacknowledge the assistance of
MidwesternUniversity’s librarian, Rebecca Caton, MLIS,who assisted
with the electronic literaturesearch, and Sandra Levi, PT, PhD, for
herguidance in writing this systematic review.
A poster presentation of data from this studywas given at the
Combined Sections Meet-ing of the American Physical Therapy
Asso-ciation; February 9–12, 2009; Las Vegas,Nevada.
This article was submitted March 10, 2009,and was accepted
December 21, 2009.
DOI: 10.2522/ptj.20090071
References1 von Brevern M, Radtke A, Lezius F, et al.
Epidemiology of benign paroxysmal posi-tional vertigo: a
population based study.J Neurol Neurosurg Psychiatry.
2007;78:710–715.
2 Oghalai JS, Manolidis S, Barth JL, et al. Un-recognized benign
paroxysmal positionalvertigo in elderly patients. OtolaryngolHead
Neck Surg. 2000;122:630–634.
3 Fife D, FitzGerald JE. Do patients with be-nign paroxysmal
positional vertigo receiveprompt treatment? Analysis of
waitingtimes and human and financial costs asso-ciated with current
practice. Int J Audiol.2005;44:50–57.
4 Schuknecht HF. Cupulolithiasis. Arch Oto-laryngol.
1969;90:765–778.
5 Hall SF, Ruby RR, McClure JA. The me-chanics of benign
paroxysmal vertigo. JOtolaryngol. 1979;8:151–158.
6 Dix MR, Hallpike CS. The pathology,symptomatology, and
diagnosis of certaincommon disorders of the vestibular sys-tem.
Proc R Soc Med. 1952;45:341–354.
7 Bhattacharyya N, Baugh RF, Orvidas L,et al. Clinical practice
guideline: benignparoxysmal positional vertigo. Otolaryn-gol Head
Neck Surg. 2008;139(5 suppl 4):S47–S81.
8 Fife TD, Iverson DJ, Lempert T, et al. Prac-tice parameter:
therapies for benign par-oxysmal positional vertigo (an
evidence-based review): report of the QualityStandards Subcommittee
of the AmericanAcademy of Neurology. Neurology.
2008;70:2067–2074.
9 Aw ST, Todd MJ, Aw GE, et al. Benignpositional nystagmus: a
study of its three-dimensional spatio-temporal characteris-tics.
Neurology. 2005;64:1897–1905.
10 Brandt T, Daroff RB. Physical therapy forbenign paroxysmal
positional vertigo.Arch Otolaryngol. 1980;106:484–485.
11 Epley JM. New dimensions of benign par-oxysmal positional
vertigo. OtolaryngolHead Neck Surg. 1980;88:599–605.
12 Herdman SJ. Treatment of benign parox-ysmal positional
vertigo. Phys Ther. 1990;70:381–388.
13 Baloh RW, Jacobson K, Honrubia V. Hori-zontal semicircular
canal variant of benignpositional vertigo. Neurology.
1993;43:2542–2549.
14 Halker RB, Barrs DM, Wellik KE, et al. Es-tablishing a
diagnosis of benign paroxys-mal positional vertigo through the
Dix-Hallpike and side-lying maneuvers: acritically appraised topic.
Neurologist.2008;14:201–204.
15 Blau P, Shoup A. Reliability of a ratingscale used to
distinguish direction of eyemovement using infrared/video ENG
re-cordings during repositioning maneuvers.Int J Audiol.
2007;46:427–432.
16 Harada Y. Metabolic disorder, absorptionarea and formation
area of the statoconia.J Clin Electron Microsc. 1982;18:1–18.
17 Lim DJ. Formation and fate of the otoco-nia: scanning and
transmission electronmicroscopy. Ann Otol Rhinol
Laryngol.1973;82:23–35.
18 Epley JM. The canalith repositioning pro-cedure: for
treatment of benign paroxys-mal positional vertigo. Otolaryngol
HeadNeck Surg. 1992;107:399–404.
19 Faldon ME, Bronstein AM. Head accelera-tions during particle
repositioning ma-noeuvres. Audiol Neurootol. 2008;13:345–356.
20 Hain TC, Squires TM, Stone HA. Clinicalimplications of a
mathematical model ofbenign paroxysmal positional vertigo.Ann N Y
Acad Sci. 2005;1039:384–394.
21 Rajguru SM, Ifediba MA, Rabbitt RD.Three-dimensional
biomechanical modelof benign paroxysmal positional vertigo.Ann
Biomed Eng. 2004;32:831–846.
22 Hain TC, Helminski JO, Reis IL, Uddin MK.Vibration does not
improve results of thecanalith repositioning procedure.
ArchOtolaryngol Head Neck Surg. 2000;126:617–622.
23 Macias JD, Ellensohn A, Massingale S, Ger-kin R. Vibration
with the canalith reposi-tioning maneuver: a prospective
random-ized study to determine efficacy.Laryngoscope.
2004;114:1011–1014.
24 Motamed M, Osinubi O, Cook JA. Effect ofmastoid oscillation
on the outcome of thecanalith repositioning procedure.
Laryn-goscope. 2004;114:1296–1298.
25 Semont A, Freyss G, Vitte E. Benign par-oxysmal positional
vertigo and provoca-tive maneuvers [in French]. Ann Otolar-yngol
Chir Cervicofac. 1989;106:473–476.
26 Radtke A, Neuhauser H, von Brevern M,Lempert T. A modified
Epley’s procedurefor self-treatment of benign paroxysmalpositional
vertigo. Neurology. 1999;53:1358–1360.
27 Radtke A, von Brevern M, Tiel-Wilck K,et al. Self-treatment
of benign paroxysmalpositional vertigo: Semont maneuver vsEpley
procedure. Neurology. 2004;63:150–152.
28 Massoud EA, Ireland DJ. Post-treatment in-structions in the
nonsurgical managementof benign paroxysmal positional vertigo.
JOtolaryngol. 1996;25:121–125.
29 Roberts RA, Gans RE, DeBoodt JL, Lister JJ.Treatment of
benign paroxysmal posi-tional vertigo: necessity of
postmaneuverpatient restrictions. J Am Acad
Audiol.2005;16:357–366.
30 Cakir BO, Ercan I, Cakir ZA, Turgut S. Ef-ficacy of postural
restriction in treating be-nign paroxysmal positional vertigo.
ArchOtolaryngol Head Neck Surg. 2006;132:501–505.
31 Baarsma EA. Vestibular testing in Mé-nière’s syndrome [in
Dutch]. Acta Otorhi-nolaryngol Belg. 1979;33:254–263.
32 von Brevern M, Seelig T, Radtke A, et al.Short-term efficacy
of Epley’s manoeuvre:a double-blind randomised trial. J
NeurolNeurosurg Psychiatry. 2006;77:980–982.
33 Lynn S, Pool A, Rose D, et al. Randomizedtrial of the
canalith repositioning proce-dure. Otolaryngol Head Neck Surg.
1995;113:712–720.
34 Imai T, Ito M, Takeda N, et al. Naturalcourse of the
remission of vertigo in pa-tients with benign paroxysmal
positionalvertigo. Neurology. 2005;64:920–921.
35 Lopez-Escamez JA, Gamiz MJ, Fernandez-Perez A, Gomez-Finana
M. Long-termoutcome and health-related quality of lifein benign
paroxysmal positional vertigo.Eur Arch Otorhinolaryngol.
2005;262:507–511.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
May 2010 Volume 90 Number 5 Physical Therapy f 677 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
36 Hilton M, Pinder D. The Epley (canalithrepositioning)
manoeuvre for benign par-oxysmal positional vertigo. Cochrane
Da-tabase Syst Rev. 2004;2:CD003162.
37 Teixeira LJ, Machado JN. Maneuvers forthe treatment of benign
positional parox-ysmal vertigo: a systematic review. Braz
JOtorhinolaryngol. 2006;72:130–139.
38 Woodworth BA, Gillespie MB, LambertPR. The canalith
repositioning procedurefor benign positional vertigo: a
meta-anal-ysis. Laryngoscope. 2004;114:1143–1146.
39 Olivo SA, Macedo LG, Gadotti IC, et al.Scales to assess the
quality of randomizedcontrolled trials: a systematic review.
PhysTher. 2008;88:156–175.
40 Chalmers TC, Celano P, Sacks HS, Smith HJr. Bias in treatment
assignment in con-trolled clinical trials. N Engl J Med.
1983;309:1358–1361.
41 Moher D, Cook DJ, Eastwood S, et al. Im-proving the quality
of reports of meta-analyses of randomised controlled trials:the
QUOROM statement. Quality of Re-porting of Meta-analyses. Lancet.
1999;354:1896–1900.
42 Moher D, Cook DJ, Jadad AR, et al. Assess-ing the quality of
reports of randomisedtrials: implications for the conduct
ofmeta-analyses. Health Technol Assess.1999;3:i–iv, 1–98.
43 Schulz KF, Chalmers I, Hayes RJ, AltmanDG. Empirical evidence
of bias: dimen-sions of methodological quality associatedwith
estimates of treatment effects in con-trolled trials. JAMA.
1995;273:408–412.
44 Moher D, Dulberg CS, Wells GA. Statisticalpower, sample size,
and their reporting inrandomized controlled trials. JAMA.
1994;272:122–124.
45 Tanimoto H, Doi K, Katata K, Nibu KI.Self-treatment for
benign paroxysmal po-sitional vertigo of the posterior
semicircu-lar canal. Neurology. 2005;65:1299–1300.
46 Longridge NS, Barber HO. Bilateral parox-ysmal positioning
nystagmus. J Otolaryn-gol. 1978;7:395–400.
47 Portney LG, Watkins MP. Foundations ofClinical Research:
Applications to Prac-tice. 3rd ed. Upper Saddle River, NJ: Pear-son
Prentice Hall; 2009.
48 Sherrington C, Herbert RD, Maher CG,Moseley AM. PEDro: a
database of random-ized trials and systematic reviews in
phys-iotherapy. Man Ther. 2000;5:223–226.
49 Froehling DA, Bowen JM, Mohr DN, et al.The canalith
repositioning procedure forthe treatment of benign paroxysmal
posi-tional vertigo: a randomized controlled tri-al. Mayo Clin
Proc. 2000;75:695–700.
50 Salvinelli F, Casale M, Trivelli M, et al. Be-nign paroxysmal
positional vertigo: a com-parative prospective study on the
efficacyof Semont’s maneuver and no treatmentstrategy. Clin Ter.
2003;154:7–11.
51 Salvinelli F, Trivelli M, Casale M, et al.Treatment of benign
positional vertigo inthe elderly: a randomized trial.
Laryngo-scope. 2004;114:827–831.
52 Sherman D, Massoud EA. Treatment out-comes of benign
paroxysmal positionalvertigo. J Otolaryngol. 2001;30:295–299.
53 Soto Varela A, Bartual Magro J, SantosPérez S, et al. Benign
paroxysmal vertigo: acomparative prospective study of the effi-cacy
of Brandt and Daroff exercises, Se-mont and Epley maneuver. Rev
LaryngolOtol Rhinol (Bord). 2001;122:179–183.
54 Angeli SI, Hawley R, Gomez O. Systematicapproach to benign
paroxysmal positionalvertigo in the elderly. Otolaryngol HeadNeck
Surg. 2003;128:719–725.
55 Asawavichianginda S, Isipradit P, Snid-vongs K, Supiyaphun P.
Canalith reposi-tioning for benign paroxysmal positionalvertigo: a
randomized, controlled trial.Ear Nose Throat J. 2000;79:732–734,736
–737.
56 Blakley BW. A randomized, controlled as-sessment of the
canalith repositioning ma-neuver. Otolaryngol Head Neck
Surg.1994;110:391–396.
57 Califano L, Capparuccia PG, Di Maria D,et al. Treatment of
benign paroxysmal po-sitional vertigo of posterior
semicircularcanal by “Quick Liberatory Rotation Ma-noeuvre.” Acta
Otorhinolaryngol Ital.2003;23:161–167.
58 Cavaliere M, Mottola G, Iemma M. Benignparoxysmal positional
vertigo: a study oftwo manoeuvres with and without beta-histine.
Acta Otorhinolaryngol Ital. 2005;25:107–112.
59 Chang AK, Schoeman G, Hill M. A random-ized clinical trial to
assess the efficacy ofthe Epley maneuver in the treatment ofacute
benign positional vertigo. AcadEmerg Med. 2004;11:918–924.
60 Cohen HS, Kimball KT. Effectiveness oftreatments for benign
paroxysmal posi-tional vertigo of the posterior canal.
OtolNeurotol. 2005;26:1034–1040.
61 Li JC. Mastoid oscillation: a critical factorfor success in
canalith repositioning pro-cedure. Otolaryngol Head Neck
Surg.1995;112:670–675.
62 Munoz JE, Miklea JT, Howard M, et al.Canalith repositioning
maneuver for be-nign paroxysmal positional vertigo: ran-domized
controlled trial in family practice.Can Fam Physician.
2007;53:1049–1053,1048.
63 Serafini G, Palmieri AM, Simoncelli C. Be-nign paroxysmal
positional vertigo of pos-terior semicircular canal: results in
160cases treated with Semont’s maneuver.Ann Otol Rhinol Laryngol.
1996;105:770–775.
64 Sridhar S, Panda N, Raghunathan M. Effi-cacy of particle
repositioning maneuver inBPPV: a prospective study. Am J
Otolar-yngol. 2003;24:355–360.
65 Wolf M, Hertanu T, Novikov I, Kronen-berg J. Epley’s
manoeuvre for benign par-oxysmal positional vertigo: a
prospectivestudy. Clin Otolaryngol Allied Sci. 1999;24:43–46.
66 Yimtae K, Srirompotong S, SrirompotongS, Sae-Seaw P. A
randomized trial of thecanalith repositioning procedure.
Laryn-goscope. 2003;113:828–832.
67 Herdman SJ, Tusa RJ. Complications of thecanalith
repositioning procedure. ArchOtolaryngol Head Neck Surg.
1996;122:281–286.
68 Cohen HS, Kimball KT. Development ofthe Vestibular Disorders
Activities of DailyLiving Scale. Arch Otolaryngol Head NeckSurg.
2000;126:881–887.
Particle Repositioning Maneuvers in the Treatment of Benign
Paroxysmal Positional Vertigo
678 f Physical Therapy Volume 90 Number 5 May 2010 at VA Medical
CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/
-
doi: 10.2522/ptj.20090071Originally published online March 25,
2010
2010; 90:663-678.PHYS THER. and Timothy Carl HainJanet Odry
Helminski, David Samuel Zee, Imke JanssenVertigo: A Systematic
Reviewthe Treatment of Benign Paroxysmal Positional Effectiveness
of Particle Repositioning Maneuvers in
References
http://ptjournal.apta.org/content/90/5/663#BIBLfor free at: This
article cites 67 articles, 14 of which you can access
Cited by
http://ptjournal.apta.org/content/90/5/663#otherarticles
This article has been cited by 8 HighWire-hosted articles:
Information Subscription
http://ptjournal.apta.org/subscriptions/
Permissions and Reprints
http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors
http://ptjournal.apta.org/site/misc/ifora.xhtml
at VA Medical CenterRoom 1100 on March 28,
2013http://ptjournal.apta.org/Downloaded from
http://ptjournal.apta.org/content/90/5/663#BIBLhttp://ptjournal.apta.org/content/90/5/663#otherarticleshttp://ptjournal.apta.org/