Embed Size (px)
Citation preview

279

O R I G I N A L A R T I C L E
Emerging infectious disease agents and their potential threat totransfusion safety
Susan L. Stramer, F. Blaine Hollinger, Louis M. Katz, Steven Kleinman, Peyton S. Metzel,
Kay R. Gregory, and Roger Y. Dodd
BACKGROUND: Emerging infections have been identi-fied as a continuing threat to human health. Many suchinfections are known to be transmissible by blood trans-fusion, while others have properties indicating thispotential. There has been no comprehensive review ofsuch infectious agents and their threat to transfusionrecipient safety to date.STUDY DESIGN AND METHODS: The members ofAABB’s Transfusion Transmitted Diseases Committeereviewed a large number of information sources inorder to identify infectious agents with actual or poten-tial risk of transfusion transmission now or in the futurein the US or Canada; with few exceptions, these agentsdo not have available interventions to reduce the risk ofsuch transmission. Using a group discussion andwriting process, key characteristics of each agent wereidentified, researched, recorded and documentedin standardized format. A group process was used toprioritize each agent on the basis of scientific/epidemiologic data and a subjective assessment ofpublic perception and/or concern expressed by regula-tory agencies.RESULTS: Sixty-eight infectious agents were identifiedand are described in detail in a single Supplement toTRANSFUSION. Key information will also be providedin web-based form and updated as necessary. Thehighest priorities were assigned to Babesia species,Dengue virus, and vCJD.CONCLUSION: The information is expected to supportthe needs of clinicians and transfusion medicine expertsin the recognition and management of emerging infec-tions among blood donors and blood recipients.
INTRODUCTION
The concept of emerging infectious disease (EID) hasdeveloped over the last 2 decades, as it became apparentthat full control of infectious disease had not beenachieved. From 1997 data, the World Health Organization(WHO) estimated that infectious diseases were respon-sible for about 33% of all deaths worldwide primarily inthe developing world, and these diseases remain one ofthe principal challenges to human survival (WHO TheWorld Health Report 1998: Life in the 21st Century. Avision for all. World Health Organization, Geneva, 1998;http://www.who.int/whr/1998/en/index.html). Emerginginfections are defined as those whose incidence inhumans has increased within the past 2 decades or threat-ens to increase in the near future.1 Emergence may be dueto evolution of an existing organism, to the spread of anew agent, to the recognition of an infection that has beenpresent in the population but has gone undetected, or tothe realization that an established disease has an infec-tious origin. Emergence also may be used to describe thereappearance of a known infection after a decline in inci-dence.1 The first emerging infection to have a major effecton blood safety was human immunodeficiency virus(HIV), the agent responsible for acquired immunodefi-ciency syndrome (AIDS), and the lessons learned from
From the Scientific Support Office, American Red Cross,
Gaithersburg, Maryland; Eugene B. Casey Hepatitis Research
Center, Baylor College of Medicine, Houston, Texas; Mississippi
Valley Regional Blood Center, Davenport, Iowa; UBC School of
Medicine, Victoria, BC, Canada; AABB, Bethesda, Maryland;
Fenwal, Inc., Lake Zurich, Illinois; Regulatory Affairs, AABB,
Bethesda, Maryland; and American Red Cross Holland Labora-
tory, Rockville, Maryland.
Address correspondence to: Susan L. Stramer, PhD, Scien-
tific Support Office, American Red Cross, 9315 Gaither Road,
Gaithersburg, MD 20877; e-mail: [email protected].
doi: 10.1111/j.1537-2995.2009.02279.x
TRANSFUSION 2009;49:1S-29S.
Volume 49, August 2009 Supplement TRANSFUSION 1S280

that epidemic have sensitized us to the need to be alert tothose emerging infections that can impact blood safety inthe future.
Any infection with an asymptomatic blood-bornephase has the potential for transmission by transfusion,whether the infectious phase is prolonged, as is the casefor hepatitis B virus (HBV) or HIV, or short, as in the case ofWest Nile virus (WNV) or dengue virus (DENV). Othercharacteristics that are necessary for transmission bytransfusion are the survival/persistence of the infectiousagent in collected blood or components, and its ability tocause infection by the intravenous route. Transfusiontransmission will be of little relevance unless the agentalso causes identifiable disease in the recipient. The fre-quency with which an infection is transmitted to bloodrecipients depends directly upon the length of the asymp-tomatic blood-borne period, how often blood is donatedduring this period, and the immune status of the recipientpopulation. A number of factors relating both to the infec-tious agent and to the genetic and immunologic makeupof the recipient also will determine the frequency andseverity of the disease resulting from the infection.
Concern about transfusion-transmitted infectionsseems to be driven by two sets of factors. First is the publichealth impact of the infection, characterized by its fre-quency and the severity of the outcomes, and by the risk ofsecondary transmissions that can be determined in moreor less quantitative terms. Second is the public reactionto the disease, which appears to be driven, in someexamples, more by emotional aspects and is not readilyquantitated. The public response may be disproportion-ate to the severity of the infection. However, both aspectsmust be considered when responding to the threat oftransfusion-transmitted infections. Priority setting inresponse to potential and emerging transfusion-transmitted infections must evaluate both the publichealth aspects, driven by scientific data, and the publicresponse to, or perception of, the agents and their risk.
Many mechanisms lead to the emergence of infec-tious diseases.2 Most dramatic is the appearance of a com-pletely new human infection. This most often reflects acircumstance in which a zoonotic infection crosses overinto the human population. A classic example is HIV/AIDS, which is thought to have occurred as a result ofcross-species transmission of simian immunodeficiencyviruses from monkeys to great apes and then to humans inAfrica.3 The original transmission perhaps occurred as aresult of preparation of bushmeat derived from apes forhuman consumption. Such species crossings may beaccompanied, or facilitated, by genetic changes in theinfectious agent.2,4 In the case of HIV, the subsequenttransmission of the virus resulted from a varietyof human behaviors involving sexual and injection druguse networks, travel, and blood-borne transmissions. Asecond example of such a species jump was severe acute
respiratory syndrome (SARS), a disease caused by ananimal coronavirus previously unrecognized in humansand again probably transmitted from exotic mammalsused as a food source.5 Another cause for emergence is theexpansion of existing infections into a larger geographicregion and/or a greater proportion of a susceptible popu-lation, often brought about by ecological and/or behav-ioral changes or by population movement. A strikingexample of this has been the emergence of WNV in theAmericas.6,7 It is unclear how the virus, which is primarilya bird-mosquito pathogen for which humans become anunintentional host, initially entered the United States(US), but its subsequent spread across the continent andinto the Caribbean and Latin America has been extraordi-narily rapid and complete. Other examples of potentiallytransfusion-transmissible agents that are expandinggeographically include DENV and chikungunya viruses(CHIKV), Plasmodium species (malaria), Babesia species,and Trypanosoma cruzi (the agent of Chagas disease).8-12
Another source of apparent emergence is the new recog-nition of existing human agents, often as a result ofpathogen discovery techniques. Examples of this includehuman herpesvirus-8 (HHV-8), the nonpathogenic GBviruses (GBV-C, initially termed hepatitis G virus orHGV),13 and Torque teno viruses (TTV/SEN-V).14 Someinfections emerge (or re-emerge) as a result of the break-down of public health measures for previously controlledinfections including the failure of initially effective vac-cines, antibiotics, or vector control programs; examplesare the re-emergence of malaria in areas of prior controland the geographical spread of DENV and CHIKV. Finally,otherwise benign infections may become serious patho-gens in the face of modern medical treatments, par-ticularly those involving immunosuppression. This groupincludes agents like cytomegalovirus (CMV) and otherherpesviruses, human parvovirus B19 (B19V), and Babesiaspecies.
Several factors that can contribute to the emergenceof an infection frequently work together. Environmentalchange (often as a result of human interventions) is amajor source, but changes in living conditions also mayhave a significant impact. Urbanization, particularly in thedeveloping world, can lead to very crowded conditionswith limited hygiene. Social disruption and conflict alsohave been associated with numerous outbreaks. Of par-ticular relevance to transfusion medicine is travel, whichhas been a major factor in the spread of emerging infec-tion (consider, for example, HIV, Plasmodium species, T.cruzi, DENV, and CHIKV).3 Sometimes the spread of anemerging agent is a result of the importation of an animalhost (for example, the introduction of monkeypox into theUS), a vector such as a mosquito, or even a food. Mobilereservoirs (e.g., birds) can transport pathogens from oneregion to another over long distances (for example, WNVor the highly pathogenic H5N1 influenza A virus). In the
STRAMER ET AL.
2S TRANSFUSION Volume 49, August 2009 Supplement281

context of transfusion, while donor travel may not initiateor expand an epidemic, it can result in the transmission ofan exotic, foreign agent to a recipient.
There have been a number of articles and reviews onthe subject of emerging infections and their impact, orpotential impact, on transfusion-associated illnesses,9,10,15
but there does not appear to be any systematic reviewidentifying a wide range of such agents and their key pro-perties. Neither is there any comprehensive guidance totransfusion service and clinical staff on how best to recog-nize and manage emerging transfusion-transmitted infec-tions. In this context, it is important to note that whiledecisions and recommendations about the overall man-agement of blood safety are likely to be made at the insti-tutional level (i.e., regulatory agency, blood system, orprofessional organization), individual practitioners alsohave specific responsibilities. A blood center or transfusionservice physician may need to decide whether to accept ordefer and how to counsel a donor with a history of disease,infection, or exposure, while a caregiver may be faced withthe challenge of diagnosing, recognizing the link to blood,and reporting a suspected posttransfusion infection.
The intent of this Supplement is to provide a set oftools identifying, describing, and prioritizing those EIDagents that have an actual or potential risk of transmis-sion by transfusion and for which there is no currentlyimplemented intervention. Of necessity, this list ofemerging agents is not, and can never be, exhaustive dueto the nature of EID agents, but it does reflect the con-sensus opinion of a group of experts. The major part ofthe Supplement consists of a set of 68 Fact Sheets, eachof which provides referenced, systematic informationabout a single agent. (See Appendix 2.) Included is stan-dard background information about each agent, alongwith an assessment of those characteristics specificallyrelated to transfusion transmission. Although it is notintended that the Fact Sheets should provide specificrecommendations about donor or patient management,consensus opinions about prudent approaches to anumber of issues (such as donor deferral periods) areincluded wherever possible based on facts that are cur-rently inferred or known. Additionally, an attempt hasbeen made to rank the agents according to the consen-sus opinion about their anticipated impact upon bloodsafety. Such a ranking should not be regarded as defini-tive, and another group of experts may come to differentconclusions. However, it may serve to focus attention onagents that merit more immediate attention in the devel-opment of plans for future interventions and might serveto focus the attention of the clinician on possible startingpoints for the diagnosis of an unfamiliar infection poten-tially associated with transfusion. It is critical to re-member, however, that the very essence of emerginginfections is that their evolution and manifestations areinherently unpredictable.
Ideally, there should be systems in place to deal withemerging infections, not only generally, but also specifi-cally in the context of transfusion safety. Primarily, this isthe responsibility of agencies that are charged with themaintenance of public health, the management of theblood supply, and its regulation. As it is unlikely thatthe first occurrence of an emerging infection will be seenin a transfused recipient, it is important that there be asystem of assessing the threat and risk of emerginginfections for their potential impact on blood safety andavailability. This requires a process for evaluating eachemerging infection for its transmissibility by this routeand for estimating the severity and potential extent of thethreat. The risk assessment should help to define the needfor, and urgency of, development and implementation ofinterventions to reduce the risk of transmission of theagent. Such interventions, if implemented, must then beevaluated for efficacy and modified as appropriate.
There is no simple formula for recognizing that atransfusion-transmitted infection has occurred, particu-larly in the case of a rare or unusual disease agent. Nev-ertheless, many such events have been recognized byastute clinicians. Knowledge of the potential for trans-mission of an emerging infection can be valuable andvery likely contributed to the relatively early recognitionof transfusion transmission of WNV.16,17 Unusual post-transfusion events with a suspected infectious originshould be brought to the attention of experts in infec-tious diseases and public health agencies for assistancein identification and follow-up. Investigation of illnessoccurring a few days or more after transfusion can diag-nose infections using serologic or molecular evidence ofinfectious agents in posttransfusion samples. However,such detection is by no means definitive. A pretransfu-sion patient sample is extremely helpful if available, asthis will reveal whether an infection predated the trans-fusion. Clinicians may not realize that type and cross-match samples and diagnostic blood specimens may beavailable for up to 2 weeks following collection beforethey are discarded by the laboratory. Finally, recall andfurther testing of associated donors can tell us whetherone or more of them was the likely source of the infec-tion. Ideally, if the responsible agent can be isolated fromboth donor and recipient, molecular analyses, such asnucleic acid sequencing, can assist in identifying orexcluding the same agent from the two sources. When aconnection is made, testing of co-component recipientscan further confirm transmission from a single donor viamultiple blood components.
There are significant problems in recognizing thatinfections with very long incubation periods may havebeen transmitted by transfusion; this was illustrated byHIV/AIDS, which did not result in well-defined illnessuntil long after the infection occurred. This delayed earlyrecognition of transfusion-transmitted HIV and concealed
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 3S282

the magnitude of the infectious donor and infected reci-pient populations. Proactive approaches to transfusiontransmission of EIDs, especially those with lengthy incu-bation periods, include the serologic or molecular evalu-ation of appropriate donor-recipient sample repositories,or engaging in active surveillance such as that used in theUnited Kingdom (UK) to identify the transmission ofvariant Creutzfeldt-Jakob disease (vCJD) by transfu-sion.18,19 However, donor-recipient repositories require alarge investment to create and maintain and have otherlimitations such as adequacy of sample size to detect rareevents, the timing of collection of the retained samples(which may predate the agent’s emergence), and thegeography of collected samples which may be outside ofthe affected area.20 Hemovigilance programs, whilevaluable for other reasons, are unlikely to contribute sub-stantially to the identification of newly emerging post-transfusion infections since they are generally designed toidentify well-defined acute outcomes.
An important component of preparedness is theestablishment of close relationships between blood estab-lishments, regulatory authorities, public health agencies,the medical community, and industry. This was exempli-fied by the rapid and effective response in the US to theemergence of WNV and the subsequent recognition of itstransfusion transmissibility. Appropriate donor screeningtests were rapidly developed and deployed within lessthan a year of the confirmation of the threat to bloodsafety.7,21,22
Although it is reasonable to consider plans for themanagement of an emerging transfusion-transmittedinfection, it is not clear when, whether, or how a responseto a potential threat should be triggered. Ideally, given theavailability of suitable resources, studies to assess theactual extent and nature of the risk conveyed by high-priority agents would be undertaken. Assessment of theprevalence and incidence of the infection in the donorpopulation and of the nature and dynamics of emergencewould provide valuable information, as would investiga-tion of the infectivity of the agent and of potential inter-ventions. These activities may be time-consuming andinappropriate in the face of an explosive outbreak,although they may offer a foundation for decision makingin the face of a less dramatic emergence, as was donefor T. cruzi antibody blood donation screening in theUS.23,24
The question of when to take specific actions toprevent or mitigate transfusion transmission of an EIDagent is beyond the scope of this Supplement. However,the information provided should contribute materially tothe factual background necessary to make such decisionsand help establish some guiding principles for decisionmaking. Interventions may be based upon questioningprospective donors about their medical risk or exposurehistories (although neither the sensitivity nor the specific-
ity of this approach have proven adequate historically as astandalone strategy, with the exception of the dramaticreduction in HIV transfusion transmission in the early1980s in San Francisco following targeted questioning25)and upon the use of laboratory tests, or a combination ofthese approaches. The availability of a specific donorscreening test, however, should make it possible to elimi-nate or at least refine donor questions.26 Finally, there ishope that pathogen-reduction methods will provide ageneralized, proactive intervention to eliminate or reducethe risk of transmission of emerging infections bytransfusion; however, such methods are not yet availablefor all blood components and their success and safetyhave not undergone extensive validation in the realworld.
Usually interventions are not implemented until itis clear that transfusion transmission has occurred,although in some cases the potential outcome of trans-mission is considered to be so severe that regulatorsrequire action even in the absence of documented trans-mission as was the case for vCJD (a decision that wasbased on, and cited in retrospect to justify, a rather strin-gent form of the precautionary principle27,28). Regulatorshave considered, and some have even implemented, pre-cautions to reduce the risk of transmission of the non-pathogenic simian foamy virus (SFV) out of fear thatinfection occurring in a human might be accompanied bya mutation conferring disease-causing capability to thevirus.29
The precautionary principle is often cited whendecisions about interventions to reduce the risk oftransfusion-transmitted infections are discussed. It is sug-gested that in the absence of any specific informationabout the efficacy of an intervention, implementation isappropriate as long as it does no harm. Commentary onthe precautionary principle suggests that it should notbe invoked without some evaluation to assure that themeasure is not extreme and does not exceed other mea-sures taken in similar circumstances.30 The hope is thatinformation in this Supplement will contribute toinformed decision making and to appropriate and well-reasoned application of “precautionism.”
FRAMEWORK FOR ASSESSMENT
The Supplement is a project undertaken by the AABBTransfusion-Transmitted Diseases (TTD) Committee.The TTD provides consultation on all facets of transfu-sion and transplantation-related diseases and associateddonor management and laboratory testing. It consistsof volunteer members with expertise in various areas ofinfectious disease and blood center operations, andincludes liaisons from the Food and Drug Administration(FDA), Centers for Disease Control and Prevention(CDC), the US Department of Defense (DOD), the
STRAMER ET AL.
4S TRANSFUSION Volume 49, August 2009 Supplement283

American Society of Hematology, and the Association ofPublic Health Laboratories.
The TTD committee undertook this project to collate,in a series of Fact Sheets, information concerning EIDagents posing demonstrated or potential risk to the safetyof transfusion or transplant recipients (Appendix 2). Spe-cifically, the task was to review and prioritize the status ofcurrent and EID agents that could be transfusion trans-mitted with potential adverse outcomes for recipients.Creation of such a thorough review document was judgedto be useful for overall policy development and strategicplanning. In this document, most of the emphasis isplaced on transfusion-transmitted disease agents;however, it should be noted that many issues relevant toagents transmitted by transfusion will overlap with agentsthat are transplant transmitted. Due to the potential forblood-borne transmission of agents that are transplanttransmitted, several agents for which organ transmissionhas been documented, even in the absence of transfusiontransmission, have been included (e.g., rabies virus andlymphocytic choriomeningitis virus).31,32
The AABB TTD committee was aware of previousefforts to develop tools for communicating the threat ofEID agents entering the blood supply and was able toobtain current versions of Héma-Québec internal EIDcharts (G. Delage, vice president, Medical Affairs) andinformation from the US DOD; materials being developedby the US Public Health Service were requested but notmade available. Findings of meetings such as the CDCconference on tick-borne diseases33 and FDA conferenceson parvovirus B19, malaria, and donor behavioral riskswere scrutinized:
• www.fda.gov/downloads/BiologicsBloodVaccinesNewsEvents/WorkshopsMeetingsConferences/TranscriptsMinutes/UCM055339.pdf
• www.fda.gov/downloads/BiologicsBloodVaccinesNewsEvents/WorkshopsMeetingsConferences/TranscriptsMinutes/UCM054429.pdf
• www.fda.gov/downloads/BiologicsBloodVaccinesNewsEvents/WorkshopsMeetingsConferences/TranscriptsMinutes/UCM054430.pdf
Although the original intent was to prepare a series ofconsolidated matrices, it was apparent that the amount ofinformation collected exceeded the format of a simplematrix and instead the document evolved into multipageFact Sheets for each specific agent.
In determining which specific EID agents should beincluded in this review, the following factors were consid-ered (agents for which the FDA requires donor testinghave been excluded from this publication):
• The agent must infect or pose a potential risk tohumans.
• With good documentation, the agent must be trans-missible by transfusion or by organ/tissue transplan-tation or such transmission must be biologicallyplausible (i.e., the agent is present in plasma or asso-ciated with blood cells or donor tissue during a timewhen the donor is asymptomatic or has a biologicalbasis to suggest the possibility to replicate in blood,tissue, or organs).
• The agent must have the possibility of being intro-duced into the blood supply during an epidemic, fol-lowing an act of bioterrorism, or inadvertently duringits emergence.
• The agent must lack a current intervention strategythat is widespread and known to be effective.
Many of these agents are considered pandemicthreats or to have epidemic potential outside the US andCanada, but the primary focus for this Supplement wasthe presence, or threat, of the agent emerging in the USand Canada.
Development of the Fact Sheets was an iterativeprocess. First a list of potential agents that met the pro-posed definitions for inclusion was developed and theformat for presenting the information was devised. Bothnaturally occurring agents and agents that could beconsidered bioterrorism threats were included. Thepreliminary draft of each Fact Sheet was prepared by anindividual TTD member. Each Fact Sheet was then sub-jected to broad discussion and underwent several addi-tional review cycles by various groups within the TTD.Articles in conventional and esoteric publications werescrutinized to document blood-borne capability. Thisreview included intensive fact checks and standardizationof format, culminating in a final review by the entire TTDcommittee.
Each Fact Sheet contains data published primarily inpeer-reviewed journals or texts that are relevant to theagent and its potential to be transfusion transmitted, andwhen available also includes data relevant to transplant-transmitted agents. They include general background andepidemiologic information, as well as information specificto blood donation. In lieu of a comprehensive bibliogra-phy, a suggested reading list is provided for each agentthat includes the most relevant citations on the agent’scapacity for transfusion transmission, and the sourcearticles documenting transfusion-transmission events.The list of suggested reading includes one or more recentreview articles or book chapters that will familiarize thereader with the agent’s general biologic and epidemio-logic characteristics.
Pertinent consensus categories that were selected bythe TTD core leadership for the Fact Sheets were designedto provide the necessary background for each agent aswell as other data that were deemed relevant for a discus-sion of their threat to recipient safety. These include:
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 5S284

Disease Agent:Disease Agent Characteristics:Disease Name:Priority Level:
• Scientific/Epidemiologic evidence regardingblood safety:
• Public perception and/or regulatory concernregarding blood safety:
• Public concern regarding disease agent:Background:Common Human Exposure Routes:Likelihood of Secondary Transmission:At-Risk Populations:Vector and Reservoir Involved:Blood Phase:Survival/Persistence in Blood Products:Transmission by Blood Transfusion:Cases/Frequency in Population:Incubation Period:Likelihood of Clinical Disease:Primary Disease Symptoms:Severity of Clinical Disease:Mortality:Chronic Carriage:Treatment Available/Efficacious:Agent-Specific Screening Question(s):Laboratory Test(s) Available:Currently Recommended Donor Deferral Period:Impact on Blood Availability:
• Agent-specific screening question(s):• Laboratory test(s) available:
Impact on Blood Safety:• Agent-specific screening question(s):• Laboratory test(s) available:
Leukoreduction Efficacy:Pathogen Reduction Efficacy for Plasma Derivatives:Other Prevention Measures:Suggested Reading:
Documentation of transfusion transmission and itsclinical outcomes was a key component of this project.When documentation was lacking, agents were evaluatedfor their potential for transfusion transmission. For theformer, the task was relatively straightforward. For thelatter, it was much more difficult because of a paucity ofdata and difficulties in proving the negative propositionthat transfusion is not implicated in transmission. Theoccurrence of an asymptomatic blood phase and its dura-tion (whether a long-term chronic carrier state or shorter-term acute infection) were the critical elements used toestimate this “risk” of transmission. Available evidenceabout the persistence or survival of an infectious agentduring blood component manufacture and storage wasexamined where possible. Treatment availability and itseffectiveness were reviewed.
Many sources were used to judge the plausibility ofblood transmission. Obviously, peer-reviewed publica-tions and textbooks are of great importance and havebeen cited in the suggested reading, but for several of thejudgments, the necessary data have not appeared in thosevenues. Other reputable and easily accessible public datasources such as the ProMed electronic mailing list serverand websites like those of the US CDC and the WHO wereused as appropriate:
• http://www.promedmail.org/pls/otn/f?p=2400:1000• http://www.cdc.gov/• http://www.who.int/en
An estimate of the level of concern about the healththreat from each agent was undertaken to suggest thresh-olds for intervention(s) to reduce or prevent transmissionby transfusion. This was an unavoidably subjective processthat included a review of the biology and epidemiology ofthe agents, an estimate of public and regulatory concernsabout the agents and an assessment of the availability ofsensitive and specific donor screening approaches. Thepriority assessment also was driven by questions such asan agent’s geographic location/presence, projections ofchanges in geographic distribution (where it was going),and where and how frequently prospective donors wouldbe at potential risk of exposure. In addition, the existence ofsurveillance adequate to allow recognition and reportingof putative transfusion transmissions, whether from phy-sicians treating patients or reports to state or local healthdepartments, federal or national public health agencies orblood collection facilities was considered.The deliberationalso took into account the incubation period for each agentand a rough estimation of the period of time that wouldbe required to realize that there is a potential publichealth threat. In so doing, the TTD committee applied theexperience and interventions used for prior emergenttransfusion-transmitted agents to evaluate the selectedEID agents. These included the potential impact of behav-ioral and testing interventions in addition to pathogenreduction strategies. Pathogen reduction strategies thatwere analyzed included the impact of leukoreduction,physicochemical methods used in the manufacture ofclotting factors, and methods used outside the US or indevelopment in the US for cellular components and trans-fusable plasma. Possible interventions were evaluatedrelative to their potential to be effective and their estimatedimpact on the donor base.
If there is a shortcoming to what is known about themany agents for which blood is a plausible vector, it is ourpassive surveillance system for transfusion transmission.For example, how often do clinicians seeing DENV inendemic areas and during epidemics obtain the criticalhistory related to transfusion? Are significant rates oftransfusion-transmitted DENV obscured during an epi-demic of vector-borne infection? The judgments made in
STRAMER ET AL.
6S TRANSFUSION Volume 49, August 2009 Supplement285

these Fact Sheets should lead to discussions of where andhow to enhance surveillance by clinicians, the transfusionmedicine community, and public health agencies if wethink the threat from an agent rises to the level of gather-ing more evidence.
A primary use of the Fact Sheets is to present methodsto decrease the risk of a given agent in the event of atransfusion-transmitted threat. However, each Fact Sheetcan also serve as a medical and technical resource toblood providers including medical directors or other cli-nicians and blood center or transfusion service staff in theevent that donors or transfused patients present with ahistory of or evidence for infection with one of theseagents. Importantly, readers must understand that theseFact Sheets do not represent regulatory guidance, butinstead serve as an indicator of what is known, and as suchcan be used as a starting point to develop policy.
The agents included in this Supplement have beenchosen based on what we know now and the current judg-ment of the members of the TTD committee. During thetime it has taken to complete this work, additional FactSheets already have been incorporated into the documentand multiple revisions have been made to the original FactSheets. As new information is accumulated, the TTD willedit the Fact Sheets. Thus, additions and deletions to theSupplement are to be expected and encouraged; a 3-yearcycle is planned. Readers are encouraged to challenge theassessments, provide data, and suggest edits. Much of thevalue of the Supplement will be realized in the future if itsaudience sees it as a living document. Mechanisms toreceive public review/comments will be communicatedthrough AABB publication channels; those commentsmay result in revisions of Fact Sheets prior to regularlyscheduled revisions, depending on the nature of thecomment. The Fact Sheets published in this Supplementwill be posted on the AABB website. Modification of theFact Sheets or new additions to the Supplement will beposted on the AABB website.
PRIORITIZATION OF SPECIFIC AGENTS
The prioritization effort is intended to suggest where intel-lect and resources should be spent in planning for thefuture. This is an especially important message for devel-opers of blood donation screening tests or pathogenreduction methods since the lead time for research anddevelopment and clinical trials to bring products to themarket place is generally many years.
Each agent was assigned a priority risk level underthree different categories: scientific/epidemiologic evi-dence regarding blood safety, public perception and/orregulatory concern regarding blood safety, and publicconcern regarding the disease agent.
Scientific/epidemiologic risk assessment was basedon a review of available data. Factors taken into consider-
ation included proof of transfusion transmission; preva-lence of the agent in an asymptomatic population thatmight donate blood, blood components, or in some casesorgans and tissues; the possibility of an outbreak resultingin increased incidence over a specific time frame; theattack rate and severity of disease caused by the agent;and the availability of effective prevention strategies ortreatment. If there was no published or other credibledocumentation that an agent had been transmitted bytransfusion to humans, it could be assigned a risk of theo-retical or absent. Theoretical was used if transmissionwas biologically plausible because the agent had a bloodphase during asymptomatic infection. Absent was used ifthis possibility was judged to be remote or if the agent wasnot associated with any known human disease.
Classification of the public perception and/or regula-tory concern for each agent’s risk was an inherently moresubjective process. Regulatory concern was judged prima-rily on whether such agents had been discussed in publicforums such as the FDA’s Blood Products Advisory Com-mittee (BPAC) or as part of other regulatory deliberations(e.g., simian foamy virus, monkeypox, and variants of HIV,HBV or HTLV). The category of public concern about anagent was assessed by reviewing whether the agent hadbeen discussed in the popular press in relationship totransfusion and whether queries to the AABB or majorblood providers had occurred.
Each category received an assessment of risk ofhigh, moderate, low, very low, or absent. As previouslydiscussed, the scientific/epidemiologic risk category alsoincluded a classification of theoretical. When risk couldnot be precisely classified, an agent was assigned an inter-mediate categorization or a range (e.g., from low to verylow) depending on where in the US/Canada, or outsidethe US/Canada, concern exists.
The overall prioritization of risk was a synthesis ofthe ratings in each category based on consensus of thegroup with greater emphasis given to ratings in the firsttwo categories: scientific/epidemiologic risk and publicand/or regulatory concern regarding blood safety.Categories of agents deemed to be of high or moderatepriority are indicated by color: red, orange, and yellowas indicated below. The agents that have not been givena priority status at this time were placed in a whitecategory for the purpose of the Tables in this Supple-ment; most of these agents remain on the watch list ofpotential threats, while some have been assessed to havevery little possibility of causing disease in transfusionrecipients.
Red. Agents with low to high scientific/epidemiologicevidence of risk regarding blood safety with the potentialfor severe clinical outcomes. This priority also may beinfluenced by the committee’s estimate of the risk ofemergence of these agents in the US and Canada as well aspublic and/or regulatory concern.
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 7S286

Orange. Agents with sufficient scientific/epide-miologic evidence of risk in regard to blood safety thatmight support their elevation to a higher priority in thefuture.
Yellow. Agents with absent to low scientific/epidemiologic evidence of risk regarding blood safety forwhich there is public and/or regulatory concern.
White. Agents that were evaluated but no higherpriority appears warranted at this time. This categoryrepresents a watch list, subject to modification as circum-stances change.
Appendix 1, Table A1 provides a complete listing of allagents by group (i.e., prions, viruses, rickettsiae, bacteria,protozoa, and nematodes); Tables A2 through A11 providethe priority scores for each agent by group. A completeassignment of the prioritized agents is provided inTables A12 through A14. Those agents associated withdocumented cases of transfusion transmissions are listedin Table A15. Agents that are vector-borne are listed inTable A16. The Fact Sheets are included as Appendix 2.
Agents classified in the red, orange, and yellow cat-egories are as follows:
• Red category agents (highest priority): human variantCreutzfeldt-Jakob disease, dengue viruses, andBabesia species (Table A12).
• Orange category agents: Chikungunya virus, St Louisencephalitis virus, Leishmania species, Plasmodiumspecies, and T. cruzi (Table A13).
• Yellow category agents: chronic wasting diseaseprions, human herpesvirus 8, HIV variants, humanparvovirus B19, influenza A virus subtype H5N1,simian foamy virus, Borrelia burgdorferi, and hepati-tis A virus (Table A14).
Red category agents
Human variant Creutzfeldt-Jakob disease (vCJD)The assignment of the risk of transfusion transmission ofvCJD in the US is based on scientific/epidemiologic evi-dence of transfusion transmissibility and was influencedby several opposing factors. In favor of a higher risk were:1) data from the UK indicating that if a donor is incubatingvCJD, there appears to be a risk of transfusion transmis-sion18 and potentially a risk to hemophiliacs who receivedUK-derived plasma products prior to the implementationof interventions to decrease BSE that were put into effectin 1996 (vCJD abnormal prion protein found in a patientwith hemophilia at postmortem, Health ProtectionAgency, CJD Section, London, UK, http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb_C/1195733818681?p=1225960597236) and 2) the rapid mor-tality associated with clinical disease and the lack ofeffective treatment.34 In favor of a lower risk were: 1) thepresumed very low to absent rate of carriers of the agent in
the general US population and 2) the possibility of an evenlower carrier rate in the US blood donor population due totravel deferrals based on time spent in the UK and Europe.These resulted in a priority rating of low for the scientific/epidemiologic risk category. However, based on highpublic concern about this agent in the UK and other areasof the world that has influenced public perception in theUS about “mad cow disease,” considerable FDA attentionto the issue of vCJD transfusion transmission, and the verydifficult donor counseling issues and potential for largenumbers of donor deferrals attendant on implementationof a test for vCJD, this agent was assigned a high ratingwith regard to public concern about blood safety. With allfactors taken into account, this led to the assignment ofthe red priority category for vCJD.
Dengue viruses (DENV)The assignment of the risk of transfusion transmission ofDENV in the US is based on scientific/epidemiologicevidence of transfusion transmissibility,35,36 and wasinfluenced by several opposing factors. In favor of ahigher risk were: 1) the common occurrence of asymp-tomatic infections and occurrence of viremia during theasymptomatic period; 2) the demonstration of relativelyhigh rates of virus-specific RNA detection in studies ofblood donors from endemic areas;37,38 3) the occurrenceof epidemics that affect a relatively high percentage ofthe population at any one time; 4) the presence of com-petent mosquito vectors in large parts of the US; 5) thedemonstration of high seroprevalence rates in US popu-lations on the Texas-Mexico border;39 and 6) the occur-rence of localized epidemics in Hawaii and Texas andin Puerto Rico from where collected blood may beimported into the continental US. In favor of a lower riskwere: 1) the low incidence of autochthonous transmis-sion in the US and 2) travel deferral for visits to malarialendemic locations that extensively overlap with DENV-endemic areas that should defer returning donors withasymptomatic DENV infection. A consideration of all ofthese factors led the committee to assign a value of lowfor scientific/epidemiologic risk in regard to blood safety.However, in non-US DENV-endemic areas, this assign-ment would be moderate to high based on the preva-lence of the agent. Public concern for blood safety wasjudged to be very low to absent in the US but moderateto high in some dengue-endemic areas. Overall, theseconsiderations led to the classification of DENV as redpriority category agents.
Babesia speciesBased on the large number of transfusion-transmittedcases reported and the perception there is gross under-reporting,40,41 Babesia was assigned a risk rating ofmoderate to high on scientific/epidemiologic groundsregarding blood safety. Pertaining to public concern, the
STRAMER ET AL.
8S TRANSFUSION Volume 49, August 2009 Supplement287

agent was assigned a very low rating nationally buta moderate rating in areas known to be endemic forthe agent (i.e., states in the Northeast and upperMidwest). Regulatory concern is evidenced by sponsor-ship of a workshop on transfusion-associated babesiosisin September 2008 by the FDA (http://www.fda.gov/downloads/BiologicsBloodVaccines/NewsEventsWorkshopsConferences/TranscriptsMinutes/UCM051501.pdf). Overall, the increasing recognition oftransfusion-transmitted cases, the severe outcomes thatcan occur in immunocompromised and asplenic trans-fusion recipients, and the lack of effective interventionsto prevent transfusion transmission led to the classifica-tion of this agent in the red priority category.
Orange category agents
Chikungunya virus (CHIKV)Due to the lack of any proven transfusion-transmittedcases, CHIKV was assigned a scientific/epidemiologic riskrating of theoretical in regard to blood safety. However,several scientific and epidemiologic factors were judged tocontribute to the potential for an increased risk from thisagent in the future. These include the rapid re-emergenceof the infection in the Indian Ocean and parts of Africaand Asia since 2005,42 the geographical spread of the virusby travelers returning from endemic areas to nonendemicregions, the presence of appropriate mosquito vectorsin various geographic locations including the US, theincreased vector efficiency of newly emerged strains,and the presence of asymptomatic viremia in infectedindividuals.43,44
St Louis encephalitis virus (SLEV)Due to the lack of any proven transfusion-transmittedcases, SLEV was assigned a scientific/epidemiologic riskrating of theoretical regarding blood safety. However, dueto its close phylogenetic relationship and similar epide-miology to WNV, and the possibility for large outbreaks ofSt Louis encephalitis in the US, this agent was judged tohave the potential to be a blood safety concern in thefuture.
Leishmania speciesThese agents were assigned a scientific/epidemiologicrisk rating of low in regard to blood safety. This risk ratingwas influenced by several opposing factors. In favor of ahigher risk were: 1) transfusion transmission documentedin at least three cases (and perhaps as many as 10) inwhich the transfused recipients were either infants orimmunocompromised patients;45 2) the propensity forchronic carriage of the agent; and 3) the presence ofasymptomatic parasitemia. In favor of a lower risk were:1) lack of any documented transfusion transmission in
the US or Canada and 2) potentially effective preventionmethods (specific geographical deferral for time spent inIraq or travel to other areas where leishmaniasis andmalaria are both endemic, and the widespread use of leu-koreduction in North America). Public concern regardingblood safety was judged to be low based on discussions atBPAC meetings. Because these agents have been demon-strated to be transmissible by transfusion and becausethey can potentially be introduced into the US by return-ing military personnel (as well as by other travelers), it wasjudged that Leishmania species could be of increasing sig-nificance to blood safety in the future.
Plasmodium speciesMalaria is a major infectious disease associated withtransfusion in many emerging and developing countries.In contrast, this risk is much lower in developed countriesdue to lack of endemicity of the agent. The Plasmodiumspecies were assigned a scientific/epidemiologic riskrating of low in the US and in most nonendemic countriesin regard to blood safety due to their low prevalencecoupled with the effective use of donor deferrals due totravel, residence, or having had malaria. However, the riskmay be moderate to high in some nonendemic countriesbased on the demographics and travel patterns of theirdonor population. Similarly, public concern regardingboth blood safety and transmissibility by other routes islikely to vary between endemic and nonendemic regions.In the US, the level of public concern was judged to bemoderate. Several factors contribute to the possibility thatmalaria may increase as a transfusion risk. These includethe re-emergence of the disease in nonendemic geo-graphic regions due to immigration and travel, an increasein sporadic cases of “airport malaria,” the occurrence ofautochthonous transmission in nonendemic countrieswhen plasmodia are introduced by immigrants (or rarelytravelers), the possibility that global climate change couldresult in an expanded range of vectors, and the lack of ascreening assay to interdict donors for whom risk is notrecognized.
Trypanosoma cruziT. cruzi is included even though an FDA-licensed test forblood donor screening has been available since Decem-ber 2006. The assignment of a blood safety scientific/epidemiologic risk rating for this agent was influenced bythe implementation of blood donor screening in 2007 bythe majority of US blood centers. Based on evidence oftransfusion transmission in Central and South America,documentation of transfusion-transmitted cases in NorthAmerica prior to donor screening, and the risk mitigationachieved by donor screening, this agent was assigned ascientific/epidemiologic risk rating of low regardingblood safety. When assessing public concern for bloodsafety, T. cruzi was assigned a rating of moderate based
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 9S288

on public and regulatory attention given to the introduc-tion of blood donor screening. Although the risk of trans-mission of this agent should be decreasing in the US,uncertainties persist regarding autochthonous transmis-sion and the sensitivity of the donor screening assay.After 2 years of universal donor screening by most bloodcollection facilities in the US, testing strategies will likelybe modified to a selective strategy, based upon at leastone-time testing of every donor. The committee feltthat this agent should be assigned an overall priority oforange, at least for the interval required for data relatingto the efficacy of donor screening and the number of pre-vious transfusion transmissions (as assessed by lookbackinvestigations) to be collected and analyzed.
Yellow category agents
Chronic wasting disease (CWD)This prion agent has never been detected in humans andno transfusion transmission has occurred, leading to ablood safety scientific/epidemiologic risk rating of theo-retical. However, because of public awareness of anotherprion agent, vCJD, which is associated with mad cowdisease and lethal human infection, it was judged thatthere was low to moderate public concern about the pos-sibility that the CWD prion agent also might cross thespecies barrier.46-48 Public concern specific to bloodsafety, however, was judged to be very low. Because ofnew scientific and public focus on this agent and itsassociated disease in deer and elk in the US and Canada,the limited amount of research that has been done todate, the potential for this prion agent to behave in amanner similar to vCJD, and the extensive opportunitiesfor donor exposure attendant to the popularity ofhunting, public health agencies (i.e., CDC) and regula-tory agencies responsible for blood safety have expressedsome concern even in the absence of any substantiatingdata. As a result, this agent was assigned an overall pri-ority rating of yellow.
Human herpesvirus 8 (HHV-8)Although HHV-8 transfusion transmission has beenproven in Africa,49 a material risk of such transmission inthe US has not been convincingly established.50 The USrisk should be considerably lower than that in Africa basedon several factors: the frequency of HHV-8 in the blooddonor population is lower in the US, the storage age ofblood components is longer, and leukoreduction iscommonly, though not universally, employed. Despitetransfusion transmission, clinical disease has not beendocumented to have resulted from such transmission.Taken together, these factors resulted in a scientific/epidemiologic risk rating of low in regard to blood safety.Public concern for blood safety also was judged to be low.
This agent was assigned an overall priority rating of yellowbased on FDA concerns regarding potential transfusiontransmission. These concerns would increase if donordeferral criteria were to be modified for males who havesex with males, due to the relatively high prevalence ofinfection in this population.
HIV variantsDue to the lack of any proven transfusion-transmittedcases, these agents were assigned a scientific/epidemiologic risk rating of theoretical regarding bloodsafety. Although the wild-type agent (HIV-1, Group M) istransfusion transmitted, transmission of HIV variants hasnot been documented. Assuming HIV variants are trans-missible by transfusion, the risk should be minimal in theUS due to low local prevalence, cross-reactivity of HIVscreening tests, and use of questions for malaria exposurethat would temporarily exclude donors who traveled toareas in Africa where HIV variation occurs at a high rate.Since HIV variants may result in AIDS, the public concernin regard to blood safety was judged to be low to moderate.In addition, the FDA has, appropriately, continued to beconcerned about the ability of blood screening tests todetect all HIV variants and the ability of donor historyquestions to screen out all potentially at-risk donors. Forthese reasons, HIV variants have been assigned a priorityrating of yellow.
Human parvovirus B19 (B19V)Transfusion transmission of B19V from blood compo-nents has been proven, with at least four cases docu-mented in the literature. However, the frequency oftransmission has not been determined or estimatedthrough established mathematical models. These factorsresulted in the assignment of a scientific/epidemiologicrisk rating of very low to low regarding blood safety.Public concern regarding blood safety risk was judged tobe very low in the US with the exception of someconcern among specific patient groups (i.e., patientswith hemophilia, those with chronic anemia such assickle cell disease or thalassemia, bone marrow trans-plant recipients, and other immunocompromised indi-viduals). Based on historical transmissions of B19V torecipients of Factor VIII, there has been ongoing scien-tific and regulatory concern about the safety of plasmaderivatives, leading many manufacturers and regulatoryauthorities to require B19V DNA qualification testing ofincoming plasma and release testing of manufacturedlots. When such B19V DNA testing is applied to recoveredplasma, the issue of how to manage associated remain-ing in-date components from B19V DNA-positivedonors has been a subject of much debate. For thesereasons, this agent has been assigned a priority rating ofyellow.
STRAMER ET AL.
10S TRANSFUSION Volume 49, August 2009 Supplement289

Influenza A virus, subtype H5N1Due to the lack of any proven transfusion-transmittedcases, this highly pathogenic avian influenza agent wasassigned a blood safety scientific/epidemiologic riskrating of theoretical. Furthermore, based on the biology ofknown influenza viruses and of H5N1, it was concludedthat transfusion transmission was unlikely to occur.51
However, because H5N1 has been discussed as an agentthat could lead to a worldwide influenza pandemic, publicconcern about community transmission of this agent wasjudged to be high, whereas concern related specifically toblood safety was judged to be very low. The high profile ofthis agent in the public health sector, especially withregard to pandemic planning, led to assigning a priorityrating of yellow.
Simian foamy virus (SFV)Although SFV transfusion transmission has been docu-mented in experiments in nonhuman primates, trans-mission by transfusion has not been demonstrated inhumans. In addition, this agent has not been shown tocause any human disease. For these reasons, this agentwas assigned a scientific/epidemiologic risk rating oftheoretical with regard to blood safety. Public concernabout this agent was judged to be absent. In contrast,some level of concern has been demonstrated by regula-tory agencies. This concern relates to the theoreticalpossibility that clinical disease does occur but has notyet been recognized and/or that mutated strains of thisagent may eventually show increased pathogenicity inhumans.2,4 In the US, SFV has been discussed at meetingsof the BPAC without concern expressed by stakeholdergroups or other members of the public (http://www.fda.gov/ohrms/dockets/ac/04/transcripts/2004-4074t1.htm). In contrast, Health Canada, the Regulatory agencyin Canada (http://www.hc-sc.gc.ca/dhp-mps/brgtherap/activit/fs-fi/fact_simian_foamy_virus_spumeux_simien_feuillet-eng.php), requires a permanent deferral forpotential blood donors whose employment involvescontact with monkeys or their body fluids.29 For thesereasons, this agent has been assigned a priority rating ofyellow.
Borrelia burgdorferiDue to the lack of any proven transfusion-transmittedcases, this agent was assigned a scientific/epidemiologicrisk rating of theoretical regarding blood safety. Iftransfusion-transmission does occur, it is likely to be rare.Conversely, given that this agent has been recognized andstudied for many years, public concern about the generaltransmissibility of this agent and its resulting diseasemanifestations (i.e., Lyme disease) was judged to be mod-erate, whereas public concern regarding blood safety wasjudged to be very low. Based primarily on the public
apprehension of Lyme disease in areas of the country witha higher prevalence of this disease, the agent has beenassigned a priority rating of yellow.
Hepatitis A virus (HAV)HAV transmission through blood is uncommon, but welldocumented, and can lead to secondary cases especiallywhen transmission occurs among infants in neonatalintensive care units. Viremia often precedes the develop-ment of symptoms by 7-14 days. The presumed rarity oftransfusion-associated cases is due to several factors thatinclude a short viremic phase, low concentration of virusin the blood, absence of a carrier state, neutralization ofthe virus by specific antibody in other components con-currently administered, routine immunization in popula-tions with high HAV incidence, and increasing prevalenceof immunity in recipients with age. HAV remains in theyellow category based on the fact that the scientific/epidemiologic evidence regarding blood safety is low butpublic concern is low to moderate, especially during acommunity outbreak of the disease. In the US, risk oftransmission during a common source epidemic is miti-gated by the addition of a specific question to the donorquestionnaire regarding exposure that leads to a 120-daydeferral postexposure.
Selected specific white category agentsIn addition to the previously categorized agents, severalagents on the watch list (i.e., white category agents) meritfurther discussion, either because of recently changinginformation (e.g., hepatitis E virus [HEV] and Anaplasmaphagocytophilum) or because of concerns about thepotential use of the agent in a bioterrorist attack. Some ofthese latter agents are discussed in more detail in thesection on bioterrorism.
Hepatitis E virus (HEV)A small number of cases of HEV transmission by bloodtransfusion has been documented52 both in areas classi-cally viewed as endemic for human infection as well as indeveloped, industrialized countries.53 The sporadic(nontransfusion) cases in humans observed in the UShave been mostly imported from endemic areas.53
This has led to assignment of a scientific/epidemiologicrisk rating of very low for this agent. The impact ofthis disease currently remains very low in the US andpublic concern is absent for blood safety and clinicaldisease. Nevertheless, the potential for human infection inthe US remains a possibility given that an HEV reservoirexists in pigs. The existence of this reservoir, combinedwith several cases of transfusion transmission in otherdeveloped countries, indicates that HEV may increase inpriority.
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 11S290

Anaplasma phagocytophilumThere have been two published case reports oftransfusion-transmitted infection in the US (one as anabstract54 and one by the CDC in Morbidity and MortalityWeekly Report55). Due to this low number ofreported transfusion-transmitted cases, the scientific/epidemiologic risk assigned was very low. However, it islikely that more cases have occurred and have not beenrecognized or reported. Given the high seroprevalencerates in donors in some geographic locations, the demon-strated survival of the organism in refrigerated red cells,documented transfusion transmission in animal models,and an unknown period of asymptomatic bacteremia, itis possible that an increasing number of transfusion-transmitted cases will be recognized if surveillance isadequate.
CATEGORIZATION INTERSECTION:SCIENCE VERSUS THE PUBLIC’S
PERCEPTION
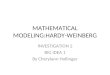
As noted, categorization of agents on the scientific/epidemiologic scale was based on data that appeared inthe scientific literature. In contrast, the public perceptioncategorizations were developed by a more subjectiveprocess. Agents may have low scientific priorities butmay be high on the public’s “radar” screen if the agentsare perceived as being those that might lead to signifi-cant human disease. As a means of showing the variousconflicts or agreements in priorities,agents having red, orange, or yellowpriority levels were plotted by factor-analytic representation56 (Fig. 1) wherethe x-axis is the scientific/epidemiologic scale that ranges from atheoretical transfusion-transmissionrisk to higher levels of proof of trans-mission and/or disease severity andincidence. In contrast, the y-axis ispublic concern (i.e., perception of risk)ranging from absent to high that occurswhen there is the perceived potentialfor dread, catastrophic or fatal conse-quences often accompanied by socialstigma (e.g., HIV/AIDS) with lack ofcontrol over the outcome. Risk com-munication and risk managementscience have shown that the higher theperceived risk, the more people want tosee the risk reduced, and the more theywant to see strict regulation employedto achieve the desired reduction in risk.Risk management efforts are destinedto fail unless they are structured usingsuch a two-way process (expert data
synthesis, opinion, and public perception).56 The lessonthat we have learned since HIV emerged as atransfusion-transmitted agent is that what we do toprotect the safety of the blood supply is dependent onboth science and the expectations of the communitiesthat we serve.
CATEGORY A AGENTS OF BIOTERRORISM:BLOOD SAFETY IMPLICATIONS AND
ACTIONS IN THE EVENT OF AN ATTACK
Blood establishments need to be appropriately preparedin the event of a bioterrorist event. Key concerns are themanagement of the existing and future blood supply oncean attack has been identified. This requires knowledge ofthe potential impact of agents of bioterrorism on bloodsafety and availability. Different actions may need to betaken depending upon the magnitude of the attack andthe agent(s) involved.
The CDC has classified several agents that might beused for bioterrorism. Those considered to be of thegravest concern are classified as Category A (http://www.bt.cdc.gov/agent/agentlist-category.asp#a), andinclude the agents of anthrax, botulism, plague, small-pox, tularemia, and viral hemorrhagic fevers. Theseagents, exclusive of botulism, are listed in Appendix 1,Table A17. The characteristics and potential actions rela-tive to these agents are summarized in Appendix 1,
Plasmodia
B19 virus
absent
very low
low
moderate
high
theoretical very low low moderate high
Science/Epidemiology
Range reflects subjectivity/uncertainty geographic variability
CW
D
Ch
iku
ng
un
ya v
iru
s
SL
E v
iru
s
HIV
var
ian
ts
Infl
uen
za v
iru
s su
bty
pe
H5N
1
Pu
blic
Per
cep
tio
n
HH
V-8
HA
V
SFV
Den
gu
e vi
ruse
s
vCJD
Bab
es
iaLe
ish
man
ia
T.
cru
zi
B. b
urg
do
rferi
Fig. 1. EID agent priority matrix, where the y-axis represents the priority based on
public perception ranging from absent to high and the x-axis represents the
priority based on science and epidemiology ranging from theoretical to high
(see text).
STRAMER ET AL.
12S TRANSFUSION Volume 49, August 2009 Supplement291

Table A18. These high-priority agents include organismsthat pose a risk to national security because they:
• Can be easily disseminated.• Can be transmitted from person to person.• Result in high morbidity or mortality rates and have
the potential for major public health impact.• Might cause public panic and social disruption.• Require special action for public health preparedness.
The items that require specific consideration forblood organizations in relation to a bioterrorist attack are:
• The risk of infectivity of blood components if anexposed individual gives blood prior to the appear-ance of symptoms.
• The risk of contamination of collected blood as aresult of direct or indirect deposition of the agent onblood containers (also putting staff at risk).
• The impact of a bioterrorist attack on the availabilityof donors and facility personnel.
• The impact of the attack upon the need for bloodcomponents.
• The impact of regulatory actions taken in response toan attack.
A major attack may compromise the safety of theblood supply to such an extent that blood collectionoperations would have to be shut down in the areaimpacted by the attack. In addition, it may be necessaryto quarantine in-date products, at least until the nature,extent, and likely date of the attack is known. However,an attack of lesser magnitude (for example, the anthraxattacks in 2001) will probably require management ofeach donor and product according to individualcircumstances.
The CDC bioterrorism page (http://www.bt.cdc.gov/agent/agentlist.asp) is a useful resource providing descrip-tive information on all agents and ways to managesuspected attacks or exposures. There are also links toother sites covering issues including reporting and clean-up. A series of articles in the Journal of American MedicalAssociation provides very useful information and thespecific reference is noted in each subtitle below. Thekey characteristics of the agents listed in Table A18 areoutlined.
Anthrax57
Anthrax is caused by the gram-positive, spore-formingbacterium, Bacillus anthracis. Three forms of disease arerecognized: inhalation anthrax resulting from respiratoryexposure (most likely to occur in the event of a deliberateattack); gastrointestinal anthrax resulting from the con-sumption of contaminated food; and cutaneous anthraxmanifesting as skin lesions, most often on the hand. It has
also become apparent that individuals may be colonizedbut exhibit no symptoms. Inhalation and gastrointestinalanthrax have incubation periods of 1-7 days, and ifuntreated, fatality rates of 97% and 25-60%, respectively.Cutaneous anthrax has an incubation period of 1-12 daysand an untreated fatality rate of 20%. Anthrax is nottransmitted from person to person. While B. anthracis isfrequently present in the blood of ill patients, the FDAreports that bacteremia is thought to be extremelyunlikely in asymptomatic individuals. Consequently,anthrax transmission by blood transfusion is not believedto occur provided blood is collected only from healthydonors with normal temperatures.
A bioterrorism attack would most likely occurthrough distribution of anthrax spores by the aerosolroute and/or distribution of the spores in powdered form.Spores are resistant to sterilization by chemicals or heatand restoring a contaminated area to a safe condition isdifficult and time-consuming. In the event of known con-tamination of a blood establishment, it would be neces-sary to evacuate staff and donors and to close theestablishment pending remediation.
In 2001, following the anthrax attacks, the FDAissued Guidance for Industry entitled: “Recommen-dations for assessment of donor suitability and bloodand blood product safety in cases of possible ex-posure to anthrax” (http://www.fda.gov/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Blood/ucm076711.htm). In this document,the FDA did not recommend any changes to standarddonor screening and blood collection practices to iden-tify or otherwise query donors who may have beenexposed to anthrax. (Note that the document was pre-pared after a rather limited exposure and that regulatoryadvice might change in the face of a massive attack.) TheFDA did recommend deferral for donors with diagnosedanthrax, suspected skin lesions, or known colonizationuntil they have completed a full course of antibiotictreatment and have been shown to be free of the bacte-ria. Donors with skin lesions suspected to be anthraxshould be deferred until the lesion is later shown not tobe anthrax or until the lesion is shown to be anthrax andthe individual completes a full course of treatment andthe infection is considered to be resolved.
In the event that a donor reports postdonation infor-mation of anthrax, in-date blood components from priordonations should be quarantined and retrieved promptly;this should date back to the time of exposure or 60 daysprior to onset of illness, whichever is shortest. The FDAalso recommends recipient notification and that medicaldirectors should determine an appropriate course ofaction in the event of postdonation illness among donorssuspected of having been exposed. Should direct contami-nation of components with anthrax spores occur, bloodproducts would have to be destroyed.
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 13S292

Botulism58
Botulism results from exposure to a toxin produced by thebacterium Clostridium botulinum. The toxin is extraordi-narily potent and a lethal human dose is thought to be0.09-0.15 mg intravenously, 0.70-0.90 mg by inhalation and70 mg orally. Natural forms of botulism are foodborne,wound, and intestinal, but all have similar clinical out-comes, namely an acute, afebrile descending flaccidparalysis that may lead to death from paralysis of themuscles of respiration. The incubation period depends onthe quantity of preformed toxin to which an individual isexposed and, in the case of foodborne exposure, maybe from 2 hours to 10 days, but is usually 18-36 hours.A bioterrorist attack is likely to occur as a result ofdistribution of the toxin by the aerosol route or perhaps bydeliberate contamination of food. An attack via the watersupply is technically not feasible.
There is no possibility of person-to-person transmis-sion of C. botulinum. It would seem very unlikely, if notimpossible, that a lethal dose could be transmitted byblood transfusion, as such transmission would requirethat the donor would have to have a lethal dose of pre-formed toxin in the blood. Thus, no Fact Sheet was devel-oped for C. botulinum. Donor deferral and quarantine andretrieval of components will not be needed unless anattack targeted a blood establishment for contaminationof products.
Plague59
Plague is caused by the gram-negative bacterium, Yersiniapestis. There are two major forms of disease: bubonic,usually acquired by the bites of fleas that have fed onbacteremic rodents; and pneumonic, resulting fromaerosol (respiratory) exposure. Primary or secondary sep-ticemic plague also may occur. Pneumonic plague is theform most likely to occur as a result of a bioterrorist attack,although intentional transmission using infected fleas hasoccurred. The overall mortality of bubonic plague is about15%, but 50-60% of cases may die in the absence of treat-ment. Untreated pneumonic disease is usually fatal. Pneu-monic disease may be transmitted from person to personthrough respiratory droplets. The incubation period is 1-7days or 1-4 days for primary pneumonic plague. A bioter-rorist attack would manifest itself as an outbreak ofrapidly fatal respiratory illness 1-6 days after the attack;secondary cases would occur. Affected individuals mayhave been bacteremic briefly at some time prior to theappearance of illness; therefore, their donated blood mustbe presumed to be infectious. Quarantine and retrieval ofblood collected up to 10 days prior to the recognition ofthe outbreak would probably be prudent in the event of alarge outbreak. Presenting donors exposed to known casesshould be deferred (probably for 2 weeks or until com-pletion of a prophylactic course of antibiotics). Staff or
donors with respiratory symptoms should be referred formedical evaluation and treatment. In the event of a majorregional outbreak, it may be necessary to suspend bloodcollection in that region until the outbreak is terminated.Significant residual contamination of facilities is unlikely,as the bacterium is very sensitive to environmentalinactivation.
Smallpox60
Smallpox is caused by a large DNA virus known as thevariola virus. Unlike other potential bioweapons, smallpoxhas been eradicated in nature. The disease spreads rapidlyfrom person to person by droplet and aerosol routes andby direct contact: contaminated surfaces such as beddingand clothing also may spread the infection. Individuals aremost infectious from the time that the rash appears until7-10 days thereafter. The usual incubation period is 12-14days (with a 7-17 day range), and there is asymptomaticviremia starting about 3-4 days after exposure. The mor-tality is up to 30% and there is no known effective treat-ment. A biological attack would likely involve aerosolrelease that would be recognized as a cluster of cases. Eachcase may infect 10-20 others and isolation of cases wouldbe required. Although there is no reported case of trans-mission of smallpox by transfusion, this remains a possi-bility. Therefore, robust interventions would be requiredfor blood establishments, including deferral of cases andcase-contacts and quarantine and recovery of blood com-ponents collected up to 21 days prior to the first case.Second wave cases would complicate the situation. Therealso would be obvious concern about staff exposure and itmay be necessary to cease all operations until the extent ofthe outbreak is determined. Environmental contamina-tion from the attack itself will not be a serious issue as thevirus is not expected to persist in the environment formore than 2 days. It is likely that an attack would result inthe implementation of widespread vaccination programs.The FDA has provided guidance on donor managementin the context of a smallpox vaccine program (http://www.fda.gov/BiologicsBloodVaccines/GuidanceComplianceRegulatoryInformation/Guidances/Blood/ucm075115.htm). It should be noted that this guidance requiresdonor deferral and such a deferral may have a significantimpact upon product availability (particularly for plate-lets). An attack with smallpox is likely to be extremely chal-lenging to the blood system.
Tularemia61
Tularemia is caused by a small, gram-negative bacterium,Francisella tularensis. This organism infects a number ofwild animals naturally and may be found as an environ-mental contaminant. Humans may be infected via theaerosol or droplet route, accidental inoculation, the bite of
STRAMER ET AL.
14S TRANSFUSION Volume 49, August 2009 Supplement293

fleas or other arthropods, or even via food or water. Theagent is highly infectious, with as few as 10 organismscausing disease. However, person-to-person transmissiondoes not occur. It is likely that a bioterrorism attack wouldbe accomplished via an aerosol release. This would resultin an outbreak of acute, febrile illness with respiratorysymptoms. The incubation period is 3-5 days, with a rangeof 1-14 days. Although subjects may be incapacitated in amatter of days, the untreated disease may be prolongedand can last weeks to months. Untreated inhalation tula-remia may have a mortality rate of 30-60%. Bacteremiadoes occur and deferral of cases and individuals thought tobe at risk of primary exposure would be necessary, pendingsuccessful completion of therapy or of antibiotic prophy-laxis. Additionally, quarantine and recovery of productscollected from the time of the presumed attack until itsrecognition would be advisable. Although the organism isrelatively hardy, simple surface decontamination with 10%bleach would be adequate and residual contaminationfrom the attack is not anticipated to be a problem.
Viral hemorrhagic fevers62
This is a complex area as about eight different virusesbelonging to four different groups are thought to bepotential threats for a bioterrorist attack. However, thereare some general shared characteristics. All are envelopedRNA viruses and all tend to cause a similar illness. Person-to-person spread by direct contact with infected bloodand body fluids is a primary route of transmission, espe-cially among those providing direct care for infectedpersons. Viruses that might be used in this context includeEbola, Marburg, Lassa, New World arenaviruses, Rift Valleyfever, yellow fever, Omsk hemorrhagic fever, Crimean-Congo hemorrhagic fever, and Kyasanur Forest diseaseviruses. A deliberate attack would most likely involve anaerosol release of virus. The result would be an outbreak ofundifferentiated febrile illness 2-21 days later. Clinicalmanifestations could include rash, hemorrhagic manifes-tations, and shock. Case fatality rates would depend uponthe agent used, but vary from a low of 0.5% (Omsk hem-orrhagic fever) to a high of 90% (Ebola). Diagnosis wouldnot be easy and it might take time before the cause of theoutbreak was established. Depending on the agent used,considerable caution may have to be used in patient care.Some, but not all, of the viruses are somewhat responsiveto selected antiviral drugs. These viruses are present in theblood, but little is known about viremia in the presymp-tomatic phases. Quarantine and recovery of productsfrom infected, and possibly exposed, donors collectedduring the incubation period would have to be under-taken. If the involved virus were not identified, the pre-sumed maximum incubation period would have to beused; this could be 4 weeks or more. Secondary caseswould be most likely to occur among caregivers with
direct contact with symptomatic cases; consequently, itmay be necessary to defer such individuals from donation.The viruses are not expected to survive very long in theenvironment, so there should be no significant facilityclean-up issues for blood establishments. Finally, itshould be noted that the clinical effects of these agentsmay result in a need for blood components, and especiallyplatelets, to correct the bleeding.
PATHOGEN REDUCTION AS A SAFETYSTRATEGY FOR EID
IntroductionThis Supplement presents detailed information onselected EID agents, including their biology, potentialthreat to recipient safety, and existing interventions. His-torically, the transfusion medicine community’s responseto EID agents has been to add new donor deferral criteriaand/or new screening tests. EIDs will continue to appear,and continuous addition of deferrals and screening testsmay not be sustainable. Furthermore, this approachinvolves waiting for disease emergence, identification ofthe agent, understanding of epidemiological risk factors ofinfection to craft donor deferrals, and then developmentand implementation of an assay. During this intervalbefore introduction of the assay, morbidity and mortalitymay accumulate. This reactive strategy of donor qualifica-tion via questions and tests will continue unless morebroad-reaching interventions are developed and imple-mented. Pathogen reduction (PR) offers a proactivestrategy to address these threats; if a PR technology offersa broad spectrum of inactivation, there is a high likelihoodthat it will inactivate the new agent, thereby preventinginfections and perhaps obviating the need for the intro-duction of new donor deferral criteria and new screeningtests. PR should also be of benefit in those situationswhere an assay fails to detect an infectious agent due to alow level of antigen/antibody/nucleic acid in the testsample during the “window period” when the analyte hasnot reached its detection threshold. Finally, PR mayinterdict agents with very long incubation periods orunrecognized pathogenicity for which the associationwith transfusion may be obscure.
The intent of the following section is to provide anoverview of what is known regarding PR systems thathave progressed to clinical trials or have been imple-mented in other countries. It provides a brief review ofeach PR method by blood component including: thecompany name and the name of the technology, thecompany’s website (as a source of additional unpub-lished data), a description of how the process would beused, the agent’s mechanism of action, a composite tableof published inactivation results, and a brief summary ofthe clinical performance and regulatory status. There isalso brief commentary on limitations of PR, including
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 15S294

the long and complex regulatory cycle (especially in theUS and Canada), reductions in product efficacy or toxi-cology associated with PR technologies, and lastly, agentsthat might be resistant either inherently or due to highconcentrations of the agent in the product. This reviewdoes not address costs associated with the use of thesetechnologies.
PLATELET PATHOGEN REDUCTIONSYSTEMS
There are three technologies for PR in platelets, none ofwhich is licensed for clinical use in the US or Canada:
• Cerus Corporation INTERCEPT Blood System™(http://www.cerus.com) Concord, CA, USA;
• CaridianBCT Biotechnologies Mirasol® PRT (http://www.caridianbct.com/) Lakewood, CO, USA; and
• MacoPharma’s Theraflex© UV. (http://www.macopharma.com/) Tourcoing, France.
Cerus Corporation INTERCEPT Blood System forplateletsPlatelets suspended in approximately 65% additive solu-tion (InterSol, Fenwal, Inc., Lake Zurich, IL) and 35%plasma are treated by adding amotosalen, a psoralen com-pound, to the platelets and delivering 3 Joules (J)/cm2
ultraviolet A light (320-400 nm) in approximately 5minutes. This results in irreversible cross-linking ofnucleic acids. Unreacted amotosalen and photoproductsare adsorbed during incubation of illuminated platelets ina separate container containing theCompound Adsorption Device (CAD)for at least 4 hours and up to 16 hours;the platelets are transferred to a finalcontainer for storage and transfusion.63
The process is shown in Fig. 2.
CaridianBCT BiotechnologiesMirasol for plateletsPlatelets suspended in 100% plasma aretreated by adding riboflavin (the normalnutrient, vitamin B2) to the platelets,then delivering 6.2 J/cm2 ultraviolet(UV) light (265-370 nm) in approxi-mately 10 minutes. This results in irre-versible photo-oxidative damage tonucleic acid. After illumination, theproduct is ready for transfusion withoutfurther processing.64,66 The process isshown in Fig. 3A. Alternatively, Caridi-anBCT Biotechnologies is developing aprocess in which a hyperconcentrated
platelet with low plasma content can be collected andphotochemically treated; after treatment, platelet additivesolution (PAS) is then added to yield a platelet stored in65% PAS and 35% plasma (Fig. 3B) (Raymond Goodrich,pers. comm., 2009).
MacoPharma Theraflex UV for plateletsPlatelets suspended in approximately 65% Storage Solu-tion for Platelets (SSP, including magnesium and potas-sium, MacoPharma, Tourcoing, France) and 35% plasmaare loosely placed on a quartz plate in bags to produce athin platelet layer (approximately 4-5 mm), then treated
Fig. 2. Cerus Corporation INTERCEPT Blood System for
platelets.
Fig. 3. CaridianBCT Biotechnologies Mirasol for platelets. (A) Platelets stored in
100% plasma. (B) Platelets stored in PAS.
STRAMER ET AL.
16S TRANSFUSION Volume 49, August 2009 Supplement295

by exposure to 0.3 J/cm2 monochro-matic wavelength UV light (254 nm)with intense agitation (approximately100 cycles/min) for about 1 minute.65
No photoactive compound is required;nucleic acid damage presumably occursdue to cyclobutyl ring formation. Afterillumination, the platelets are trans-ferred into a storage container and areready for transfusion with no furtherprocessing. The process is shown inFig. 4.
Pathogen reduction in plateletsData that have been published in peer-reviewed journals are provided inTables 1 through 4. Data from abstractsor unpublished data available fromstudies conducted by the manufacturersare included as personal communica-tions from the companies’ represen-tatives. Cerus (INTERCEPT) hasdemonstrated >6.4 log activity forCHIKV in platelets (Lily Lin, pers.comm., 2009). CaridianBCT Biotech-nologies (Mirasol) has demonstratedinactivation of the following agents:Viruses: Sindbis virus (3.2 logs); influ-enza A virus (>5.3 logs); infectiousbovine rhinotracheitis virus (2.1 logs);HAV (2 logs); HBV (>4 logs by PCR);bovine enterovirus (3.0 logs); pseudora-bies virus (2.5 logs); encepha-lomyocarditis virus (3.2 logs); CHIKV(2-3 logs); Bacteria/Yeast: Acinetobacterbaumannii (1.8 logs); Klebsiella oxytoca(1 log); K. pneumoniae (2.8 logs); Strep-tococcus mitis (3.7 logs); S. pyogenes (2.3logs); Yersinia enterocolitica (3.3 logs);Candida albicans (1.8 logs); andProtozoa: Plasmodium falciparum(>3.0 logs); and Babesia microti(>5.0 logs) (Raymond Goodrich, pers.comm., 2009). MacoPharma TheraflexUV process for platelets using only UVCand agitation has been presented atmeetings held by the AABB, ISBT, andGerman Society for Transfusion Medi-cine and Immunohaematology and has shown inactiva-tion against the following viruses: WNV (>5 logs); Sindbisvirus (5.6 logs); encephalomyocarditis virus and porcineparvovirus (5-6 logs); vesicular stomatitis virus (VSV) (>6logs); Suid herpesvirus 1 (3.7 logs); HIV-1 (1.4 logs) (FrankTolksdorf and Stefan Reichenberg, pers. comm., 2009).
PLASMA PATHOGEN REDUCTIONSYSTEMS
The same three companies have processes for PR inplasma. Cerus and CaridianBCT Biotechnologies use thesame photoactive substance and process as employed in
Fig. 4. MacoPharma Theraflex UV for platelets.
TABLE 1. Log10 reduction of known transfusion-transmitted virusesin platelets
Virus INTERCEPT63 Mirasol64,66
EnvelopedHIV-1• Cell-free >6.2 5.9 (includes cell-associated)• Cell-associated >6.1 See above• Proviral To limit of detection 4.5
HBV >5.5 CID50*HCV >4.5 CID50
HTLV-I, cell-associated 4.7HTLV-II, cell-associated 5.1CMV, cell-associated >5.9WNV >6.067 5.2
NonenvelopedB19V 4-5.568
HAV 0†
* Chimp Infectious Dose where 50% of the animals become infected.† No reduction was observed (Lily Lin, pers comm., 2009).
TABLE 2. Log10 reduction of model viruses in plateletsVirus Model for INTERCEPT63 Mirasol64,66
EnvelopedVesicular stomatitis Enveloped viruses >5.8 >6.3Influenza A (H5N1) Influenza viruses �5.969
Duck HBV HBV >6.2 ID50*Bovine viral diarrhea HCV >6.0SARS >6.270
Vaccinia >5.2Nonenveloped
Bluetongue Nonenveloped viruses 6.1-6.4Calicivirus Nonenveloped viruses 1.7-2.4Simian adenovirus 15 Nonenveloped viruses 0.7-2.3Human adenovirus 5 Nonenveloped viruses >5.7Porcine parvovirus Nonenveloped viruses 0† �5.0
* Infectious dose where 50% of the ducks are infected.† No reduction was observed.
EID AND TRANSFUSION SAFETY
Volume 49, August 2009 Supplement TRANSFUSION 17S296














![User Equipage Costs (Hollinger).ppt [Read-Only]](https://img.pdfslide.us/doc/110x75/623c024ed8ef4029da21a607/user-equipage-costs-hollingerppt-read-only.jpg)