Embed Size (px)
Citation preview
193
Acute heart failure (HF) syndrome (AHFS) is a major reason for visits to the emergency department (ED).1,2
Patients with AHFS represent a heterogeneous group defined by new or worsening symptoms of HF that require urgent care.3 Although several potential underlying or precipitating factors are implicated, ischemic heart disease contributes importantly as a pathogenetic factor in AHFS.4 It is estimated that 50% to 70% of patients with AHFS have concomitant coronary artery disease; however, optimal management of ischemic heart dis-ease among patients with HF presenting in the acute hospital setting has not been fully elucidated.5–8
At the current time, the management of AHFS is directed toward symptom improvement because many putative targets for acute therapy have not yielded a mortality benefit.9–11 Recent evidence from a clinical registry suggested that patients with AHFS who underwent coronary angiography in hospital had increased use of evidence-based therapies and revascularization procedures and experienced lower mortality rates than those not undergoing the invasive procedure.12 Furthermore, patients with AFHS who underwent coronary revascularization exhibited mortality risks that did not differ from those without coronary artery disease.13 Although an early invasive investigation and a revascularization strategy similar to that for acute coronary syndromes provide interesting possibilities to improve survival in AHFS, randomized trials have not tested this hypothesis.
Original Article
© 2013 American Heart Association, Inc.
Circ Heart Fail is available at http://circheartfailure.ahajournals.org DOI: 10.1161/CIRCHEARTFAILURE.112.000075
10.1161/CIRCHEARTFAILURE.112.000075
2013
19
March
XXX
2
00
00
© 2013 American Heart Association, Inc.
2013
Received May 9, 2012; accepted January 28, 2013.From the Division of Cardiology, Peter Munk Cardiac Centre, University Health Network, Toronto, Canada (J.R.B., M.E.F., H.J.R., D.S.L.); Institute for
Clinical Evaluative Sciences, Toronto, Canada (J.V.T., P.C.A., A.C., J.J.Y., D.S.L.); Institute of Health Policy, Management, and Evaluation, Toronto, Canada (J.V.T., P.C.A., D.S.L.); Dalla Lana School of Public Health (P.C.A.), Division of Cardiology (J.V.T.), Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Canada; Departments of Medicine, and of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Canada (J.J.Y.); and Heart and Stroke Richard Lewar Centre of Excellence in Cardiovascular Investigation, Toronto, Ontario, Canada (J.V.T., M.E.F., D.S.L.).
The online-only Data Supplement is available at http://circheartfailure.ahajournals.org/lookup/suppl/doi:10.1161/CIRCHEARTFAILURE.112. 000075/-/DC1.
Correspondence to Douglas S. Lee, MD, PhD, Institute for Clinical Evaluative Sciences, University of Toronto, Room G-106, 2075 Bayview Ave, Toronto, ON M4N 3M5, Canada. E-mail [email protected]
Braga et al Troponin Elevation and Acute Heart Failure Outcomes
Background—Cardiac troponins (cTn) may be elevated among patients with acute heart failure syndromes (AHFS). However, the optimal approach to management of AHFS with elevated cTn is unknown.
Methods and Results—We compared the care and outcomes of 13 656 patients with AHFS seeking care in the emergency department stratified by presence (cTn+, n=1845, 13.5%) or absence (cTn−) of elevated troponin. Clinically abstracted data on patients who were admitted or discharged from the emergency department in Ontario, Canada (April 1999 to March 2001 and April 2004 to March 2007) were examined. In an exploratory 2:1 propensity-matched analysis, we examined whether early coronary revascularization (within 14 days of emergency department visit) was associated with survival, stratified by cTn status. For cTn+ AHFS, rates of coronary angiography (21.8 vs 11.4 patients/100 person-years; P<0.001) and coronary revascularization (8.8 vs 3.2 patients/100 person-years; P<0.001) were higher than cTn−. Instantaneous 30-day adjusted hazard ratios for cTn+ versus cTn− patients were 9.17 (95% confidence interval [CI], 8.31–10.12; P<0.001) for death, 5.14 (95% CI, 4.66–5.67; P<0.001) for cardiovascular readmission, and 13.08 (95% CI, 10.95–15.62; P<0.001) for ischemic heart disease hospitalization. In propensity-matched analysis of 143 individuals with cTn+ AHFS, early coronary revascularization was associated with reduced mortality (adjusted hazard ratio, 0.29; 95% CI, 0.09–0.92; P=0.036) compared with those who were not revascularized. Mortality was not significantly reduced among 210 cTn− patients undergoing early coronary revascularization (adjusted hazard ratio, 0.61; 95% CI, 0.36–1.03; P=0.065).
Conclusions—Elevated cTn was associated with increased risk of death and cardiovascular hospitalizations. Highly selected cTn+ patients who underwent early coronary revascularization for obstructive coronary artery disease experienced improved survival. (Circ Heart Fail. 2013;6:193-202.)
Key Words: acute ■ cardiac troponin ■ cardiovascular disease ■ coronary artery disease ■ coronary revascularization ■ heart failure ■ hospitalization ■ ischemic heart disease ■ mortality ■ prognosis ■ readmission
Outcomes and Care of Patients With Acute Heart Failure Syndromes and Cardiac Troponin Elevation
Juarez R. Braga, MD; Jack V. Tu, MD, PhD; Peter C. Austin, PhD; Alice Chong, BSc; John J. You, MD, MSc; Michael E. Farkouh, MD, MSc; Heather J. Ross, MD, MHSc;
Douglas S. Lee, MD, PhD
110
Clinical Perspective on p 202
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

194 Circ Heart Fail March 2013
Furthermore, the risks and costs associated with these interven-tions limit their widespread and nonselective use.14
Elevated cardiac troponins (cTn+) are associated with increased mortality risk in those hospitalized with AHFS.15–19 They have also been shown to be one of the most important factors associated with early death in patients presenting to the ED with HF.20 However, predictors of HF death are not necessarily equally important predictors of readmission.21 Specifically, the importance of cTn as a predictor of future cardiovascular hospitalization has not been determined in a multicenter population-based setting. Furthermore, the clinical characteristics, diagnostic investigations, and therapeutic inter-ventions of patients with cTn+ AHFS have not been described fully and longitudinally over time. Troponin may be an impor-tant biomarker that could identify potential HF patient sub-groups that might benefit from quality improvement efforts. However, before cTn can be systematically regarded in this way, it should be demonstrated that it is associated with a wide range of adverse morbidity and mortality outcomes, investiga-tion and treatment rates are low in those with elevated cTn, and outcomes may be altered by treatment of the higher risk group.
In this study, we compared the presenting features, processes of care, death, and hospitalization outcomes of patients present-ing with cTn+ versus cTn− AHFS. In addition, we examined mortality of patients with or without elevated cTn after early coronary revascularization in a propensity-matched analysis.
MethodsPatientsWe studied patients aged ≥18 years who were residents of Ontario, Canada, who presented to an ED with a primary diagnosis of HF. We examined the clinical data abstracted from 3 complementary data sets. Hospitalized HF patients were identified in the Enhanced Feedback For Effective Cardiac Treatment (EFFECT) Phase 1 (from April 1, 1999, to March 31, 2001) and Phase 2 (from April 1, 2004, to March 31, 2005) studies.22 From the Emergency Heart Failure Mortality Risk Grade (EHMRG) study, we examined both hospi-talized patients and those who were discharged from the ED from April 1, 2004, to March 31, 2007.20 Thus, these 3 similar data sets (EFFECT Phases 1 and 2, and EHMRG) included patients who were either hospitalized or discharged home after the ED visit. All patients included in this study were required to meet the Framingham criteria for HF23 and also have a most responsible diagnosis of HF using the International Classification of Diseases, 9th or 10th revisions (ICD-9-CM code 428 or ICD-10-CA code I50) in the ED or hospital dis-charge abstract.24,25 Ethical approval was obtained from the research ethics board of Sunnybrook Health Sciences Center.
Patients were required to have undergone at least 1 measurement of cTn during the first 24 hours after ED presentation. In case sequential troponins were ordered during this time period, the peak value was chosen to define those who were cTn+ or cTn−. We excluded patients who were hospitalized for an acute coronary syndrome within 14 days before the index ED visit (because troponin values may remain elevated up to 2 weeks after the onset of infarction), those with a serum creatinine concentration >2.0 mg/dL (or 176.8 μmol/L), and those who were palliative or had do-not-resuscitate orders before ED arrival. Unique patients were selected, and thus for those who were included in both the EFFECT and the EHMRG cohorts (eg, had re-peat hospital visits), only the first encounter was chosen.
Data SourcesThe patient data abstracted for the EFFECT and EHMRG cohorts were linked to administrative databases available in the province of Ontario. ED information was obtained from the National Ambulatory
Care Reporting System, which contains records of all ED visits. Mortality was determined using the Registered Persons Database for all deaths. The Canadian Institute for Health Information Discharge Abstract Database was used to identify hospitalizations, procedures, and in-hospital deaths. Dispensation of pharmacological therapies was determined for patients ≥65 years of age using the Ontario Drug Benefit database. We identified fee codes for diagnostic and inter-ventional cardiac procedures using the Ontario Health Insurance Plan physician claims database. All databases have been validated26–28 and were linked using the patients’ unique, encrypted health card number.
DefinitionscTn was considered elevated if a test drawn within the first 24 hours of the ED visit exceeded the upper limit of the normal range (includ-ing indeterminate or gray zone values) according to the assay in use at each institution. We examined troponin tests drawn in a 24-hour window to allow greater sensitivity in detecting those with elevated values among those who may have undergone serial testing for po-tentially borderline values. The primary outcome of this study was all-cause mortality. Secondary outcomes included hospitalizations for ischemic heart or cardiovascular disease. Ischemic heart disease hospitalizations were defined as admissions with the most respon-sible diagnosis of angina pectoris, acute myocardial infarction, other acute ischemic heart diseases, and chronic ischemic heart diseases us-ing ICD-9-CM codes 410 to 414 and ICD-10-CA codes I20 to I25.24,25 Hospitalizations for cardiovascular disease included all admissions for ischemic heart disease (ICD-9-CM codes 410–414; ICD-10-CA codes I20 to I25), HF (ICD-9-CM code 428; ICD-10-CA code I50), or other cardiovascular conditions (ICD-9-CM codes 390–398, 401–405, 415–417, 420–427, 429–438, 440–448, 451–453, 458, 780.2, 785.4, 785.5, and 798.1; ICD-10-CA codes I00 to I02, I05 to I13, I15, I26 to I28, I30 to I40, I44 to I49, I51, I52, I60 to I74, I77 to I82, I95, I97, R02, R55, R57, and R96). Elective hospital admissions with length of stay of ≤1 day were not counted as an outcome event in hospitalization analyses.
Statistical AnalysisContinuous variables were expressed as median (25th, 75th percen-tiles) and compared with the Kruskal–Wallis test. Categorical vari-ables were compared using the χ2 statistic. We used Cox proportional hazards models to estimate the effect of troponin on the risk of the occurrence of outcome events, adjusting simultaneously for both clin-ical20 and administratively coded models for mortality and readmis-sion.29,30 The model for mortality was adjusted for age, sex, transport by emergency medical services, systolic blood pressure, heart rate, oxygen saturation, serum creatinine, serum potassium, use of metola-zone, myocardial infarction, previous HF, coronary artery bypass graft surgery (CABG), percutaneous coronary intervention (PCI), diabetes mellitus, hypertension, active and metastatic cancer, unstable angina, stroke, functional disability, cardiopulmonary respiratory failure and shock, pneumonia, chronic pulmonary obstructive disease, protein calorie malnutrition, dementia, trauma, major psychiatric disorders, peripheral vascular disease, chronic liver disease, chronic atheroscle-rotic disease, and valvular disease, as determined by comorbidities coded in the index HF visit and by examining all diagnostic codes in the 3 years before the index ED visit. In addition to the above, hospi-tal readmission models were also adjusted for arrhythmias, decubitus/chronic skin ulcer, other heart diseases, peptic ulcer and other gastro-intestinal diseases, severe hematologic disease, urinary tract disor-ders, end-stage renal disease, and alcohol or drug abuse. All models were also adjusted for the time period: early (1999–2001) versus late (2004–2007). Time to death was determined from the date of initial ED visit, whereas follow-up for readmission began after the date of hospital or ED discharge. The proportional hazards assumption was tested formally using a Kolmogorov–Smirnov supremum-type test on 1000 resamplings of the cumulative sums of martingale residuals.31 If a violation of the assumption of the proportionality of hazards was found, we modeled a time–covariate interaction to model the time-varying hazard ratio (HR) explicitly, and instantaneous time-varying HRs with 95% Wald confidence limits were reported.
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Braga et al Troponin Elevation and Acute Heart Failure Outcomes 195
We conducted 2 separate propensity-score matched analyses in those with cTn+ or cTn− AHFS separately, to estimate the effect of coronary revascularization on survival. We estimated propensity scores for coronary revascularization using the same variables in-cluded in the mortality model, in accordance with previous studies suggesting the need for selection of prognostically important covari-ates.32 Patients were matched in a 1:2 ratio, such that each patient who was revascularized with either PCI or CABG surgery within 14 days was matched to 2 nonrevascularized patients. Propensity-score matching was performed using a greedy nearest-neighbor matching algorithm on the logit of the propensity score with a caliper width of 0.2 of the SD of the logit of the propensity score.33 Patients included in this analysis were required to have survived at least 14 days after ED presentation, and time-to-event analysis began on day 14 after the index ED presentation to avoid survivor-treatment bias. Balances in the baseline covariates were evaluated by calculating standardized differences.34 The effect of revascularization on the risk of an adverse event in the propensity-matched analysis was estimated with a Cox regression model using a robust (sandwich-type) variance estimator to account for matched triplets.35 A 2-sided probability value <0.05 was considered to be statistically significant. All analyses were per-formed using SAS 9.2 (SAS Institute, Inc., Cary, NC).
ResultsStudy CohortAmong a total of 28 101 unique subjects included in the EFFECT and EHMRG cohorts, cTn was measured in 19 601 individuals. The final study cohort was 13 656 patients (Figure 1), of whom 1845 (13.5%) were cTn+ at ED presen-tation. Of the 13 329 patients who were discharged alive and were eligible for readmission, 5563 (41.7%) were readmitted for a cardiovascular cause and 1479 (11.1%) were rehospital-ized for ischemic heart disease within 2 years. There were 4829 (35.4%) deaths during 2-year follow-up from the time of ED presentation, and a total of 44 812 person-years of follow-up were examined for death. Crude median (25th, 75th percentile) troponin value was 0.05 (0.02, 0.21) among all HF patients studied. Among those with peak troponin values that exceeded the upper limit of the normal range, median values were low: 0.30 (0.09–1.40). Median peak troponin values were 0.04 (0.01–0.10) among those with values below the upper limit of normal range. Of the cohort, 10 339 underwent testing with troponin I (75.5%), 3243 were tested with troponin T (23.7%),
and type of troponin was unknown in 74 patients (0.5%). The median (25th, 75th percentile) value of the ratio of the peak cTn/upper limit of normal was 2.80 (1.50, 9.03). Therefore, corresponding raw peak cTn values would be 0.20 (0.11, 0.63) if the upper limit of normal of the troponin assay was 0.07.
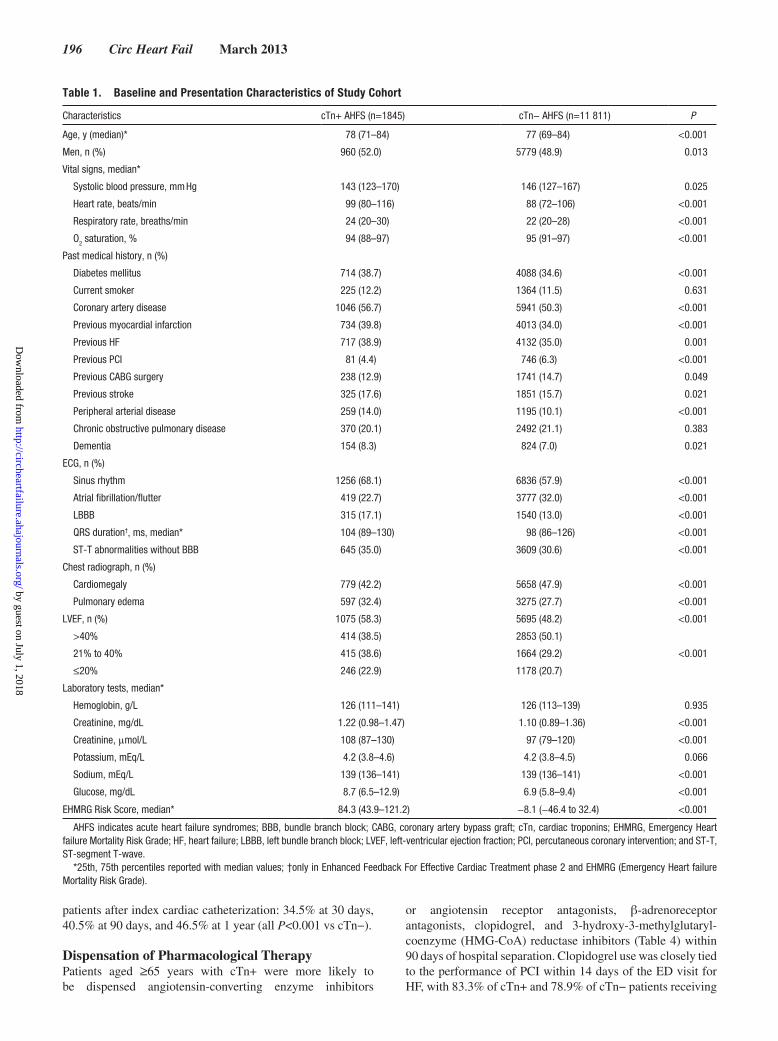
Baseline Characteristics and ED PresentationAs shown in Table 1, cTn+ patients were slightly older, com-prised of more men, and exhibited higher prevalence of coronary disease or previous myocardial infarction. Patients with cTn− AHFS had higher frequency of previous coronary revascular-ization procedures. In the ED, cTn+ patients had more severe presentations, with higher heart rate and respiratory rate, lower oxygen saturation, and chest radiographs consistent with pulmo-nary edema. Atrial fibrillation was more common in cTn− AHFS, whereas ST-segment deviation and T-wave abnormalities sugges-tive of ischemia occurred more frequently among cTn+ patients.
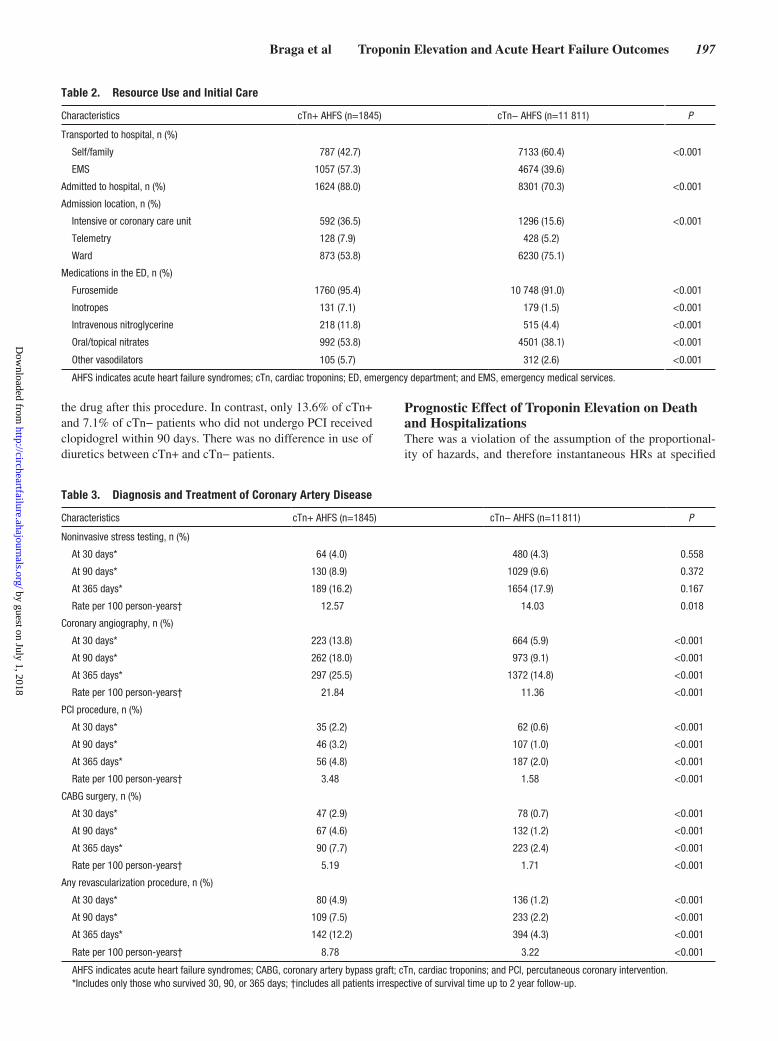
Resource Usage and Initial CareIndividuals with cTn+ AHFS more frequently arrived to the ED using emergency medical transport and were more likely to be admitted from the ED. Although cTn+ patients were more often admitted to a higher intensity care setting, the majority of patients who were admitted to an intensive or coronary care unit did not exhibit cTn elevation (68.6%). Patients with cTn+ were more likely to be initially treated with loop diuretics, inotropes, nitroglycerin, and other vasodilators (Table 2).
Diagnosis and Treatment of Coronary Artery DiseaseHigher rates of noninvasive stress testing were not observed among those with cTn+; however, rates of coronary angiog-raphy were significantly increased among this group (Table 3). Rates of revascularization by PCI or CABG surgery were higher among those with cTn+ AHFS, but the majority of patients did not undergo either type of procedure. Among cTn− patients who underwent cardiac catheterization, coro-nary revascularization procedures were performed in 18.1% at 30 days, 22.0% at 90 days, and 26.9% at 1 year. Coronary revascularization occurred more frequently among cTn+
Figure 1. Patient flow diagram. ACS, acute coronary syndrome; cTn, cardiac troponins; DNR, do not resuscitate; ED, emergency department; EFFECT, Enhanced Feedback For Effective Car-diac Treatment; and EHMRG, Emergency Heart Failure Mortality Risk Grade.
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
196 Circ Heart Fail March 2013
patients after index cardiac catheterization: 34.5% at 30 days, 40.5% at 90 days, and 46.5% at 1 year (all P<0.001 vs cTn−).
Dispensation of Pharmacological TherapyPatients aged ≥65 years with cTn+ were more likely to be dispensed angiotensin-converting enzyme inhibitors
or angiotensin receptor antagonists, β-adrenoreceptor antagonists, clopidogrel, and 3-hydroxy-3-methylglutaryl-coenzyme (HMG-CoA) reductase inhibitors (Table 4) within 90 days of hospital separation. Clopidogrel use was closely tied to the performance of PCI within 14 days of the ED visit for HF, with 83.3% of cTn+ and 78.9% of cTn− patients receiving
Table 1. Baseline and Presentation Characteristics of Study Cohort
Characteristics cTn+ AHFS (n=1845) cTn− AHFS (n=11 811) P
Age, y (median)* 78 (71–84) 77 (69–84) <0.001
Men, n (%) 960 (52.0) 5779 (48.9) 0.013
Vital signs, median*
Systolic blood pressure, mm Hg 143 (123–170) 146 (127–167) 0.025
Heart rate, beats/min 99 (80–116) 88 (72–106) <0.001
Respiratory rate, breaths/min 24 (20–30) 22 (20–28) <0.001
O2 saturation, % 94 (88–97) 95 (91–97) <0.001
Past medical history, n (%)
Diabetes mellitus 714 (38.7) 4088 (34.6) <0.001
Current smoker 225 (12.2) 1364 (11.5) 0.631
Coronary artery disease 1046 (56.7) 5941 (50.3) <0.001
Previous myocardial infarction 734 (39.8) 4013 (34.0) <0.001
Previous HF 717 (38.9) 4132 (35.0) 0.001
Previous PCI 81 (4.4) 746 (6.3) <0.001
Previous CABG surgery 238 (12.9) 1741 (14.7) 0.049
Previous stroke 325 (17.6) 1851 (15.7) 0.021
Peripheral arterial disease 259 (14.0) 1195 (10.1) <0.001
Chronic obstructive pulmonary disease 370 (20.1) 2492 (21.1) 0.383
Dementia 154 (8.3) 824 (7.0) 0.021
ECG, n (%)
Sinus rhythm 1256 (68.1) 6836 (57.9) <0.001
Atrial fibrillation/flutter 419 (22.7) 3777 (32.0) <0.001
LBBB 315 (17.1) 1540 (13.0) <0.001
QRS duration†, ms, median* 104 (89–130) 98 (86–126) <0.001
ST-T abnormalities without BBB 645 (35.0) 3609 (30.6) <0.001
Chest radiograph, n (%)
Cardiomegaly 779 (42.2) 5658 (47.9) <0.001
Pulmonary edema 597 (32.4) 3275 (27.7) <0.001
LVEF, n (%) 1075 (58.3) 5695 (48.2) <0.001
>40% 414 (38.5) 2853 (50.1)
21% to 40% 415 (38.6) 1664 (29.2) <0.001
≤20% 246 (22.9) 1178 (20.7)
Laboratory tests, median*
Hemoglobin, g/L 126 (111–141) 126 (113–139) 0.935
Creatinine, mg/dL 1.22 (0.98–1.47) 1.10 (0.89–1.36) <0.001
Creatinine, μmol/L 108 (87–130) 97 (79–120) <0.001
Potassium, mEq/L 4.2 (3.8–4.6) 4.2 (3.8–4.5) 0.066
Sodium, mEq/L 139 (136–141) 139 (136–141) <0.001
Glucose, mg/dL 8.7 (6.5–12.9) 6.9 (5.8–9.4) <0.001
EHMRG Risk Score, median* 84.3 (43.9–121.2) −8.1 (−46.4 to 32.4) <0.001
AHFS indicates acute heart failure syndromes; BBB, bundle branch block; CABG, coronary artery bypass graft; cTn, cardiac troponins; EHMRG, Emergency Heart failure Mortality Risk Grade; HF, heart failure; LBBB, left bundle branch block; LVEF, left-ventricular ejection fraction; PCI, percutaneous coronary intervention; and ST-T, ST-segment T-wave.
*25th, 75th percentiles reported with median values; †only in Enhanced Feedback For Effective Cardiac Treatment phase 2 and EHMRG (Emergency Heart failure Mortality Risk Grade).
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
Braga et al Troponin Elevation and Acute Heart Failure Outcomes 197
the drug after this procedure. In contrast, only 13.6% of cTn+ and 7.1% of cTn− patients who did not undergo PCI received clopidogrel within 90 days. There was no difference in use of diuretics between cTn+ and cTn− patients.
Prognostic Effect of Troponin Elevation on Death and HospitalizationsThere was a violation of the assumption of the proportional-ity of hazards, and therefore instantaneous HRs at specified
Table 2. Resource Use and Initial Care
Characteristics cTn+ AHFS (n=1845) cTn− AHFS (n=11 811) P
Transported to hospital, n (%)
Self/family 787 (42.7) 7133 (60.4) <0.001
EMS 1057 (57.3) 4674 (39.6)
Admitted to hospital, n (%) 1624 (88.0) 8301 (70.3) <0.001
Admission location, n (%)
Intensive or coronary care unit 592 (36.5) 1296 (15.6) <0.001
Telemetry 128 (7.9) 428 (5.2)
Ward 873 (53.8) 6230 (75.1)
Medications in the ED, n (%)
Furosemide 1760 (95.4) 10 748 (91.0) <0.001
Inotropes 131 (7.1) 179 (1.5) <0.001
Intravenous nitroglycerine 218 (11.8) 515 (4.4) <0.001
Oral/topical nitrates 992 (53.8) 4501 (38.1) <0.001
Other vasodilators 105 (5.7) 312 (2.6) <0.001
AHFS indicates acute heart failure syndromes; cTn, cardiac troponins; ED, emergency department; and EMS, emergency medical services.
Table 3. Diagnosis and Treatment of Coronary Artery Disease
Characteristics cTn+ AHFS (n=1845) cTn− AHFS (n=11 811) P
Noninvasive stress testing, n (%)
At 30 days* 64 (4.0) 480 (4.3) 0.558
At 90 days* 130 (8.9) 1029 (9.6) 0.372
At 365 days* 189 (16.2) 1654 (17.9) 0.167
Rate per 100 person-years† 12.57 14.03 0.018
Coronary angiography, n (%)
At 30 days* 223 (13.8) 664 (5.9) <0.001
At 90 days* 262 (18.0) 973 (9.1) <0.001
At 365 days* 297 (25.5) 1372 (14.8) <0.001
Rate per 100 person-years† 21.84 11.36 <0.001
PCI procedure, n (%)
At 30 days* 35 (2.2) 62 (0.6) <0.001
At 90 days* 46 (3.2) 107 (1.0) <0.001
At 365 days* 56 (4.8) 187 (2.0) <0.001
Rate per 100 person-years† 3.48 1.58 <0.001
CABG surgery, n (%)
At 30 days* 47 (2.9) 78 (0.7) <0.001
At 90 days* 67 (4.6) 132 (1.2) <0.001
At 365 days* 90 (7.7) 223 (2.4) <0.001
Rate per 100 person-years† 5.19 1.71 <0.001
Any revascularization procedure, n (%)
At 30 days* 80 (4.9) 136 (1.2) <0.001
At 90 days* 109 (7.5) 233 (2.2) <0.001
At 365 days* 142 (12.2) 394 (4.3) <0.001
Rate per 100 person-years† 8.78 3.22 <0.001
AHFS indicates acute heart failure syndromes; CABG, coronary artery bypass graft; cTn, cardiac troponins; and PCI, percutaneous coronary intervention.*Includes only those who survived 30, 90, or 365 days; †includes all patients irrespective of survival time up to 2 year follow-up.
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
198 Circ Heart Fail March 2013
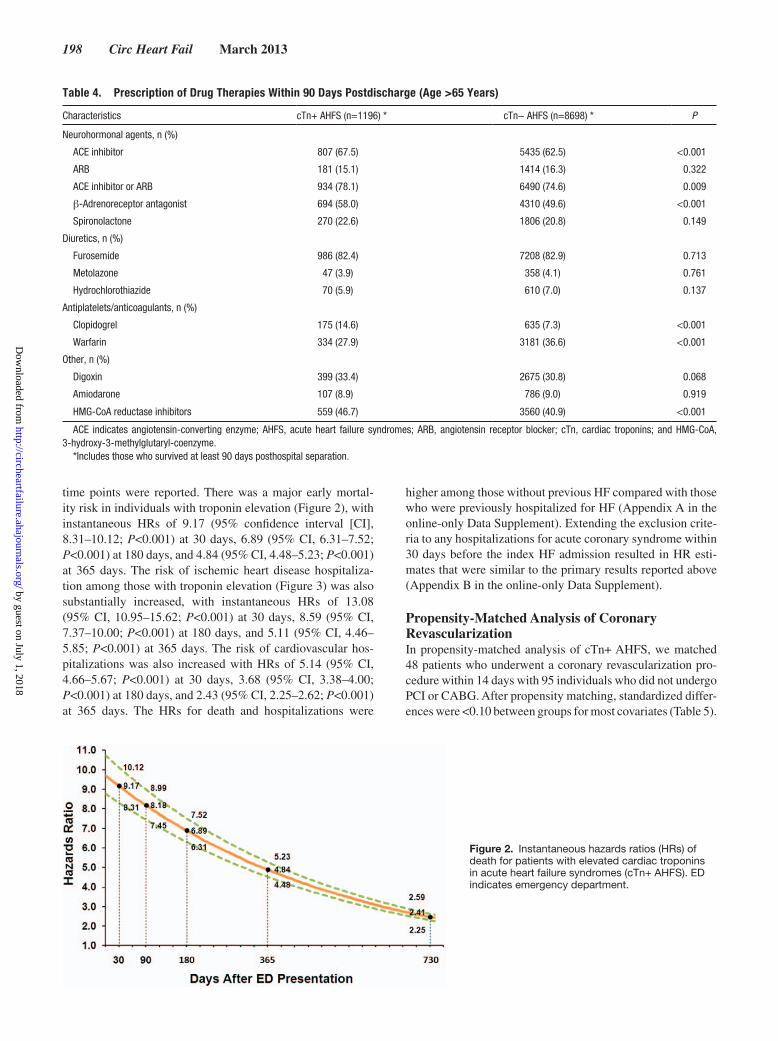
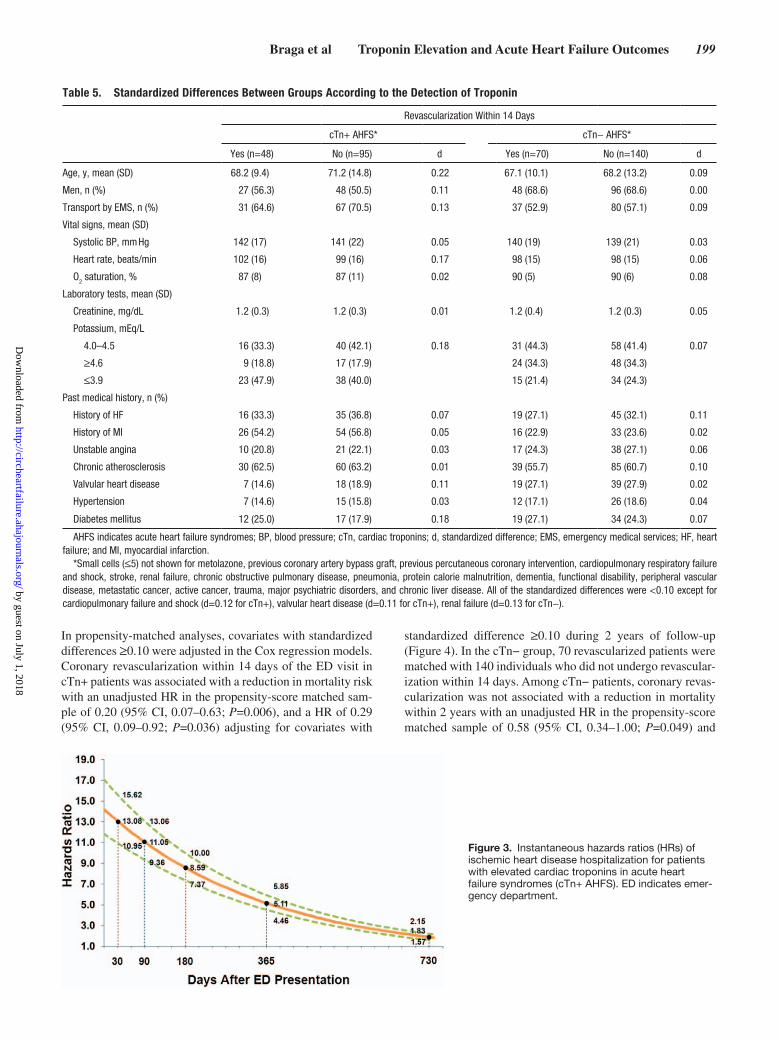
time points were reported. There was a major early mortal-ity risk in individuals with troponin elevation (Figure 2), with instantaneous HRs of 9.17 (95% confidence interval [CI], 8.31–10.12; P<0.001) at 30 days, 6.89 (95% CI, 6.31–7.52; P<0.001) at 180 days, and 4.84 (95% CI, 4.48–5.23; P<0.001) at 365 days. The risk of ischemic heart disease hospitaliza-tion among those with troponin elevation (Figure 3) was also substantially increased, with instantaneous HRs of 13.08 (95% CI, 10.95–15.62; P<0.001) at 30 days, 8.59 (95% CI, 7.37–10.00; P<0.001) at 180 days, and 5.11 (95% CI, 4.46–5.85; P<0.001) at 365 days. The risk of cardiovascular hos-pitalizations was also increased with HRs of 5.14 (95% CI, 4.66–5.67; P<0.001) at 30 days, 3.68 (95% CI, 3.38–4.00; P<0.001) at 180 days, and 2.43 (95% CI, 2.25–2.62; P<0.001) at 365 days. The HRs for death and hospitalizations were
higher among those without previous HF compared with those who were previously hospitalized for HF (Appendix A in the online-only Data Supplement). Extending the exclusion crite-ria to any hospitalizations for acute coronary syndrome within 30 days before the index HF admission resulted in HR esti-mates that were similar to the primary results reported above (Appendix B in the online-only Data Supplement).
Propensity-Matched Analysis of Coronary RevascularizationIn propensity-matched analysis of cTn+ AHFS, we matched 48 patients who underwent a coronary revascularization pro-cedure within 14 days with 95 individuals who did not undergo PCI or CABG. After propensity matching, standardized differ-ences were <0.10 between groups for most covariates (Table 5).
Table 4. Prescription of Drug Therapies Within 90 Days Postdischarge (Age >65 Years)
Characteristics cTn+ AHFS (n=1196) * cTn− AHFS (n=8698) * P
Neurohormonal agents, n (%)
ACE inhibitor 807 (67.5) 5435 (62.5) <0.001
ARB 181 (15.1) 1414 (16.3) 0.322
ACE inhibitor or ARB 934 (78.1) 6490 (74.6) 0.009
β-Adrenoreceptor antagonist 694 (58.0) 4310 (49.6) <0.001
Spironolactone 270 (22.6) 1806 (20.8) 0.149
Diuretics, n (%)
Furosemide 986 (82.4) 7208 (82.9) 0.713
Metolazone 47 (3.9) 358 (4.1) 0.761
Hydrochlorothiazide 70 (5.9) 610 (7.0) 0.137
Antiplatelets/anticoagulants, n (%)
Clopidogrel 175 (14.6) 635 (7.3) <0.001
Warfarin 334 (27.9) 3181 (36.6) <0.001
Other, n (%)
Digoxin 399 (33.4) 2675 (30.8) 0.068
Amiodarone 107 (8.9) 786 (9.0) 0.919
HMG-CoA reductase inhibitors 559 (46.7) 3560 (40.9) <0.001
ACE indicates angiotensin-converting enzyme; AHFS, acute heart failure syndromes; ARB, angiotensin receptor blocker; cTn, cardiac troponins; and HMG-CoA, 3-hydroxy-3-methylglutaryl-coenzyme.
*Includes those who survived at least 90 days posthospital separation.
Figure 2. Instantaneous hazards ratios (HRs) of death for patients with elevated cardiac troponins in acute heart failure syndromes (cTn+ AHFS). ED indicates emergency department.
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
Braga et al Troponin Elevation and Acute Heart Failure Outcomes 199
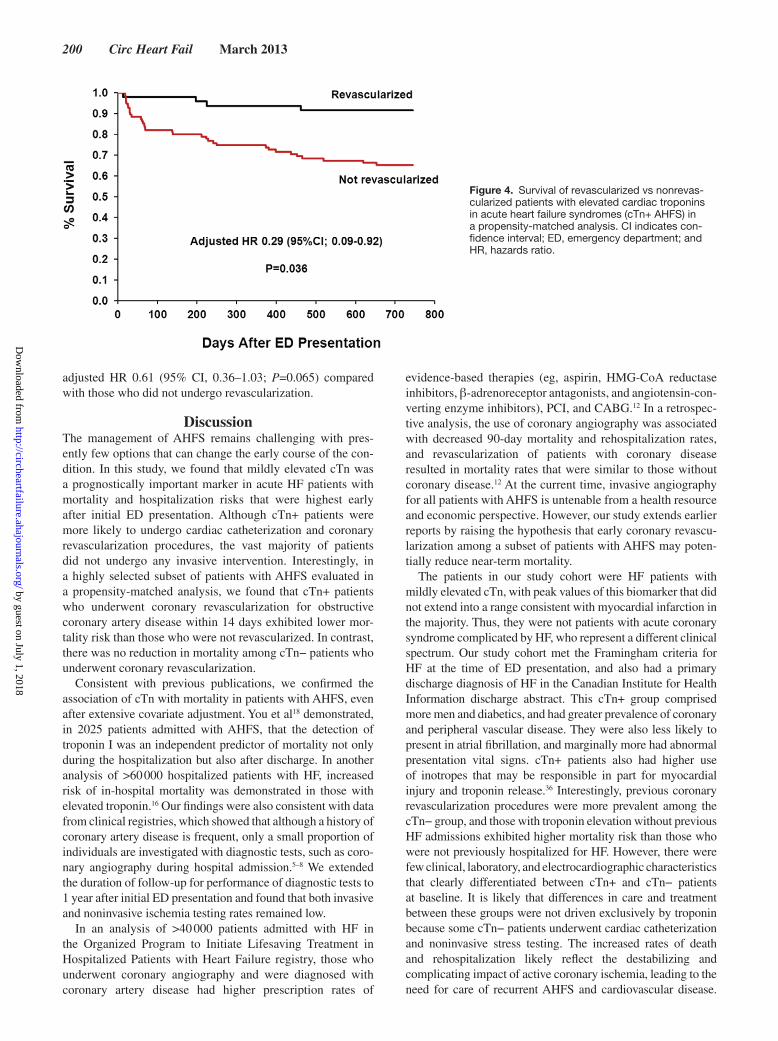
In propensity-matched analyses, covariates with standardized differences ≥0.10 were adjusted in the Cox regression models. Coronary revascularization within 14 days of the ED visit in cTn+ patients was associated with a reduction in mortality risk with an unadjusted HR in the propensity-score matched sam-ple of 0.20 (95% CI, 0.07–0.63; P=0.006), and a HR of 0.29 (95% CI, 0.09–0.92; P=0.036) adjusting for covariates with
standardized difference ≥0.10 during 2 years of follow-up (Figure 4). In the cTn− group, 70 revascularized patients were matched with 140 individuals who did not undergo revascular-ization within 14 days. Among cTn− patients, coronary revas-cularization was not associated with a reduction in mortality within 2 years with an unadjusted HR in the propensity-score matched sample of 0.58 (95% CI, 0.34–1.00; P=0.049) and
Figure 3. Instantaneous hazards ratios (HRs) of ischemic heart disease hospitalization for patients with elevated cardiac troponins in acute heart failure syndromes (cTn+ AHFS). ED indicates emer-gency department.
Table 5. Standardized Differences Between Groups According to the Detection of Troponin
Revascularization Within 14 Days
cTn+ AHFS* cTn− AHFS*
Yes (n=48) No (n=95) d Yes (n=70) No (n=140) d
Age, y, mean (SD) 68.2 (9.4) 71.2 (14.8) 0.22 67.1 (10.1) 68.2 (13.2) 0.09
Men, n (%) 27 (56.3) 48 (50.5) 0.11 48 (68.6) 96 (68.6) 0.00
Transport by EMS, n (%) 31 (64.6) 67 (70.5) 0.13 37 (52.9) 80 (57.1) 0.09
Vital signs, mean (SD)
Systolic BP, mm Hg 142 (17) 141 (22) 0.05 140 (19) 139 (21) 0.03
Heart rate, beats/min 102 (16) 99 (16) 0.17 98 (15) 98 (15) 0.06
O2 saturation, % 87 (8) 87 (11) 0.02 90 (5) 90 (6) 0.08
Laboratory tests, mean (SD)
Creatinine, mg/dL 1.2 (0.3) 1.2 (0.3) 0.01 1.2 (0.4) 1.2 (0.3) 0.05
Potassium, mEq/L
4.0–4.5 16 (33.3) 40 (42.1) 0.18 31 (44.3) 58 (41.4) 0.07
≥4.6 9 (18.8) 17 (17.9) 24 (34.3) 48 (34.3)
≤3.9 23 (47.9) 38 (40.0) 15 (21.4) 34 (24.3)
Past medical history, n (%)
History of HF 16 (33.3) 35 (36.8) 0.07 19 (27.1) 45 (32.1) 0.11
History of MI 26 (54.2) 54 (56.8) 0.05 16 (22.9) 33 (23.6) 0.02
Unstable angina 10 (20.8) 21 (22.1) 0.03 17 (24.3) 38 (27.1) 0.06
Chronic atherosclerosis 30 (62.5) 60 (63.2) 0.01 39 (55.7) 85 (60.7) 0.10
Valvular heart disease 7 (14.6) 18 (18.9) 0.11 19 (27.1) 39 (27.9) 0.02
Hypertension 7 (14.6) 15 (15.8) 0.03 12 (17.1) 26 (18.6) 0.04
Diabetes mellitus 12 (25.0) 17 (17.9) 0.18 19 (27.1) 34 (24.3) 0.07
AHFS indicates acute heart failure syndromes; BP, blood pressure; cTn, cardiac troponins; d, standardized difference; EMS, emergency medical services; HF, heart failure; and MI, myocardial infarction.
*Small cells (≤5) not shown for metolazone, previous coronary artery bypass graft, previous percutaneous coronary intervention, cardiopulmonary respiratory failure and shock, stroke, renal failure, chronic obstructive pulmonary disease, pneumonia, protein calorie malnutrition, dementia, functional disability, peripheral vascular disease, metastatic cancer, active cancer, trauma, major psychiatric disorders, and chronic liver disease. All of the standardized differences were <0.10 except for cardiopulmonary failure and shock (d=0.12 for cTn+), valvular heart disease (d=0.11 for cTn+), renal failure (d=0.13 for cTn−).
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
200 Circ Heart Fail March 2013
adjusted HR 0.61 (95% CI, 0.36–1.03; P=0.065) compared with those who did not undergo revascularization.
DiscussionThe management of AHFS remains challenging with pres-ently few options that can change the early course of the con-dition. In this study, we found that mildly elevated cTn was a prognostically important marker in acute HF patients with mortality and hospitalization risks that were highest early after initial ED presentation. Although cTn+ patients were more likely to undergo cardiac catheterization and coronary revascularization procedures, the vast majority of patients did not undergo any invasive intervention. Interestingly, in a highly selected subset of patients with AHFS evaluated in a propensity-matched analysis, we found that cTn+ patients who underwent coronary revascularization for obstructive coronary artery disease within 14 days exhibited lower mor-tality risk than those who were not revascularized. In contrast, there was no reduction in mortality among cTn− patients who underwent coronary revascularization.
Consistent with previous publications, we confirmed the association of cTn with mortality in patients with AHFS, even after extensive covariate adjustment. You et al18 demonstrated, in 2025 patients admitted with AHFS, that the detection of troponin I was an independent predictor of mortality not only during the hospitalization but also after discharge. In another analysis of >60 000 hospitalized patients with HF, increased risk of in-hospital mortality was demonstrated in those with elevated troponin.16 Our findings were also consistent with data from clinical registries, which showed that although a history of coronary artery disease is frequent, only a small proportion of individuals are investigated with diagnostic tests, such as coro-nary angiography during hospital admission.5–8 We extended the duration of follow-up for performance of diagnostic tests to 1 year after initial ED presentation and found that both invasive and noninvasive ischemia testing rates remained low.
In an analysis of >40 000 patients admitted with HF in the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure registry, those who underwent coronary angiography and were diagnosed with coronary artery disease had higher prescription rates of
evidence-based therapies (eg, aspirin, HMG-CoA reductase inhibitors, β-adrenoreceptor antagonists, and angiotensin-con-verting enzyme inhibitors), PCI, and CABG.12 In a retrospec-tive analysis, the use of coronary angiography was associated with decreased 90-day mortality and rehospitalization rates, and revascularization of patients with coronary disease resulted in mortality rates that were similar to those without coronary disease.12 At the current time, invasive angiography for all patients with AHFS is untenable from a health resource and economic perspective. However, our study extends earlier reports by raising the hypothesis that early coronary revascu-larization among a subset of patients with AHFS may poten-tially reduce near-term mortality.
The patients in our study cohort were HF patients with mildly elevated cTn, with peak values of this biomarker that did not extend into a range consistent with myocardial infarction in the majority. Thus, they were not patients with acute coronary syndrome complicated by HF, who represent a different clinical spectrum. Our study cohort met the Framingham criteria for HF at the time of ED presentation, and also had a primary discharge diagnosis of HF in the Canadian Institute for Health Information discharge abstract. This cTn+ group comprised more men and diabetics, and had greater prevalence of coronary and peripheral vascular disease. They were also less likely to present in atrial fibrillation, and marginally more had abnormal presentation vital signs. cTn+ patients also had higher use of inotropes that may be responsible in part for myocardial injury and troponin release.36 Interestingly, previous coronary revascularization procedures were more prevalent among the cTn− group, and those with troponin elevation without previous HF admissions exhibited higher mortality risk than those who were not previously hospitalized for HF. However, there were few clinical, laboratory, and electrocardiographic characteristics that clearly differentiated between cTn+ and cTn− patients at baseline. It is likely that differences in care and treatment between these groups were not driven exclusively by troponin because some cTn− patients underwent cardiac catheterization and noninvasive stress testing. The increased rates of death and rehospitalization likely reflect the destabilizing and complicating impact of active coronary ischemia, leading to the need for care of recurrent AHFS and cardiovascular disease.
Figure 4. Survival of revascularized vs nonrevas-cularized patients with elevated cardiac troponins in acute heart failure syndromes (cTn+ AHFS) in a propensity-matched analysis. CI indicates con-fidence interval; ED, emergency department; and HR, hazards ratio.
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Braga et al Troponin Elevation and Acute Heart Failure Outcomes 201
Although several mechanisms for troponin release are probably active in an individual patient with HF,14 myocardial ischemia as the main reason for detectable troponin is supported by increased prevalence of previous revascularization procedures among cTn− patients at presentation, higher rates of coronary revascularization procedures after cardiac catheterization among cTn+ than cTn− patients, and improved survival in a small cTn+ subcohort undergoing early coronary revascularization in propensity-matched analysis.
The implications of this study are underscored by the pau-city of treatment options that can improve the course of AHFS. Our study suggests that in AHFS, troponin is not simply a bystander that correlates with the degree of patient sickness. Instead, elevation of this biomarker in the acute setting may indicate the active contribution of ischemia to HF prognosis as demonstrated by the increased risk of rehospitalization and death. Patients with elevation of this biomarker should be con-sidered for further investigation with noninvasive testing or coronary angiography irrespective of left-ventricular function, and optimization of medical therapy should be performed. Furthermore, our study promotes the hypothesis that it may be reasonable to consider coronary revascularization in selected patients with cTn+ AHFS if coronary ischemia and evidence of anatomic disease are present.
There are some notable limitations of this study. Troponin measurement was not standard of care during the time hori-zon of this study; therefore, a sizeable proportion of patients without such testing were excluded. Although high-sensitivity troponin assays were not available during the time frame of the EFFECT and EHMRG studies, the findings of the cur-rent study may directly extend to the use of this biomarker in HF. The propensity risk analysis allows only for adjustment based on measured variables while important factors, such as the extent and severity of ischemia or coronary artery disease, and how the decision was made to refer individuals to angi-ography were not evaluated. However, these factors may have been directly associated with the probability of coronary angi-ography and revascularization. Although it is conceivable that individuals with cTn+ had more ischemia or severe coronary disease on angiography, we were unable to determine whether such an association was present. Finally, the intriguing results from the propensity-matched analysis of early revasculariza-tion were also limited by the low rates of procedures conducted in an acute time frame of 14 days after ED presentation.
ConclusionsIn conclusion, patients with cTn+ AHFS demonstrated higher risk of rehospitalization and death in long-term follow-up. Although cTn+ patients received higher rates of prescription of evidence-based therapies and use of invasive procedures for the diagnosis and treatment of ischemic heart disease, the overall rates were low compared with the adverse outcomes experienced by this group. Our study generates the hypothesis that presence of elevated troponin may help identify patients with AHFS who may benefit from further investigation for coronary artery disease and early coronary revascularization. Further studies are needed to determine the best strategies for identifying patients who would benefit from referral to coro-nary angiography and possible revascularization procedure.
Sources of FundingThe Institute for Clinical Evaluative Sciences is supported in part by a grant from the Ontario Ministry of Health and Long Term Care. The opinions, results, and conclusions are those of the authors, and no en-dorsement by the Ontario Ministry of Health and Long Term Care or by the Institute for Clinical Evaluative Sciences is intended or should be inferred. This research was supported by an operating grant from the Canadian Institutes of Health Research (CIHR MOP 114937), a CIHR clinician-scientist award (D.S.L.), a Career Investigator Award from the Heart and Stroke Foundation of Ontario (P.C.A. and J.V.T.), a Canada Research Chair in Health Services Research (J.V.T.), and a Hamilton Health Sciences Research Early Career Award (J.J.Y.).
DisclosuresNone.
References 1. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among
patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428.
2. Lee DS, Schull MJ, Alter DA, Austin PC, Laupacis A, Chong A, Tu JV, Stukel TA. Early deaths in patients with heart failure discharged from the emergency department: a population-based analysis. Circ Heart Fail. 2010;3:228–235.
3. Gheorghiade M, Pang PS. Acute heart failure syndromes. J Am Coll Car-diol. 2009;53:557–573.
4. Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framing-ham heart study of the national heart, lung, and blood institute. Circula-tion. 2009;119:3070–3077.
5. Fox KF, Cowie MR, Wood DA, Coats AJ, Gibbs JS, Underwood SR, Turner RM, Poole-Wilson PA, Davies SW, Sutton GC. Coronary artery disease as the cause of incident heart failure in the population. Eur Heart J. 2001;22:228–236.
6. O’Connor CM, Stough WG, Gallup DS, Hasselblad V, Gheorghiade M. Demographics, clinical characteristics, and outcomes of patients hospi-talized for decompensated heart failure: observations from the IMPACT-HF registry. J Card Fail. 2005;11:200–205.
7. Fonarow GC, Heywood JT, Heidenreich PA, Lopatin M, Yancy CW; ADHERE Scientific Advisory Committee and Investigators. Temporal trends in clinical characteristics, treatments, and outcomes for heart failure hospitalizations, 2002 to 2004: findings from Acute Decom-pensated Heart Failure National Registry (ADHERE). Am Heart J. 2007;153:1021–1028.
8. Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, Hochadel M, Komajda M, Lassus J, Lopez-Sendon JL, Ponikowski P, Tavazzi L; EuroHeart Survey Investigators; Heart Failure Association, European Society of Cardiology. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of popu-lation. Eur Heart J. 2006;27:2725–2736.
9. Konstam MA, Gheorghiade M, Burnett JC Jr, Grinfeld L, Maggioni AP, Swedberg K, Udelson JE, Zannad F, Cook T, Ouyang J, Zimmer C, Or-landi C; Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Effects of oral tolvap-tan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. JAMA. 2007;297:1319–1331.
10. Mebazaa A, Nieminen MS, Packer M, Cohen-Solal A, Kleber FX, Pocock SJ, Thakkar R, Padley RJ, Põder P, Kivikko M; SURVIVE In-vestigators. Levosimendan vs dobutamine for patients with acute de-compensated heart failure: the SURVIVE Randomized Trial. JAMA. 2007;297:1883–1891.
11. O’Connor CM, Starling RC, Hernandez AF, Armstrong PW, Dickstein K, Hasselblad V, Heizer GM, Komajda M, Massie BM, McMurray JJ, Nieminen MS, Reist CJ, Rouleau JL, Swedberg K, Adams KF Jr, Anker SD, Atar D, Battler A, Botero R, Bohidar NR, Butler J, Clausell N, Cor-balán R, Costanzo MR, Dahlstrom U, Deckelbaum LI, Diaz R, Dunlap ME, Ezekowitz JA, Feldman D, Felker GM, Fonarow GC, Gennevois D, Gottlieb SS, Hill JA, Hollander JE, Howlett JG, Hudson MP, Kociol RD, Krum H, Laucevicius A, Levy WC, Méndez GF, Metra M, Mittal S, Oh BH, Pereira NL, Ponikowski P, Tang WH, Wilson WH, Tanomsup S, Teerlink JR, Triposkiadis F, Troughton RW, Voors AA, Whellan DJ,
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
202 Circ Heart Fail March 2013
Zannad F, Califf RM. Effect of nesiritide in patients with acute decom-pensated heart failure. N Engl J Med. 2011;365:32–43.
12. Flaherty JD, Rossi JS, Fonarow GC, Nunez E, Stough WG, Abraham WT, Albert NM, Greenberg BH, O’Connor CM, Yancy CW, Young JB, Davidson CJ, Gheorghiade M. Influence of coronary angiography on the utilization of therapies in patients with acute heart failure syndromes: findings from Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am Heart J. 2009;157:1018–1025.
13. Rossi JS, Flaherty JD, Fonarow GC, Nunez E, Gattis Stough W, Abra-ham WT, Albert NM, Greenberg BH, O’Connor CM, Yancy CW, Young JB, Davidson CJ, Gheorghiade M. Influence of coronary artery disease and coronary revascularization status on outcomes in patients with acute heart failure syndromes: a report from OPTIMIZE-HF (Organized Pro-gram to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure). Eur J Heart Fail. 2008;10:1215–1223.
14. Kociol RD, Pang PS, Gheorghiade M, Fonarow GC, O’Connor CM, Felker GM. Troponin elevation in heart failure prevalence, mechanisms, and clinical implications. J Am Coll Cardiol. 2010;56:1071–1078.
15. Metra M, Nodari S, Parrinello G, Specchia C, Brentana L, Rocca P, Fra-cassi F, Bordonali T, Milani P, Danesi R, Verzura G, Chiari E, Dei Cas L. The role of plasma biomarkers in acute heart failure. Serial changes and independent prognostic value of NT-proBNP and cardiac troponin-T. Eur J Heart Fail. 2007;9:776–786.
16. Peacock WF 4th, De Marco T, Fonarow GC, Diercks D, Wynne J, Apple FS, Wu AH; ADHERE Investigators. Cardiac troponin and outcome in acute heart failure. N Engl J Med. 2008;358:2117–2126.
17. Perna ER, Macín SM, Cimbaro Canella JP, Alvarenga PM, Ríos NG, Pantich R, Augier N, Farías EF, Jantus E, Brizuela M, Medina F. Minor myocardial damage detected by troponin T is a powerful predictor of long-term prognosis in patients with acute decompensated heart failure. Int J Cardiol. 2005;99:253–261.
18. You JJ, Austin PC, Alter DA, Ko DT, Tu JV. Relation between cardiac troponin I and mortality in acute decompensated heart failure. Am Heart J. 2007;153:462–470.
19. Zairis MN, Tsiaousis GZ, Georgilas AT, Makrygiannis SS, Adamo-poulou EN, Handanis SM, Batika PC, Prekates AA, Velissaris D, Kouris NT, Mytas DZ, Babalis DK, Karidis KS, Foussas SG. Mul-timarker strategy for the prediction of 31 days cardiac death in pa-tients with acutely decompensated chronic heart failure. Int J Cardiol. 2010;141:284–290.
20. Lee DS, Stitt A, Austin PC, Stukel TA, Schull MJ, Chong A, Newton GE, Lee JS, Tu JV. Prediction of heart failure mortality in emergent care: a cohort study. Ann Intern Med. 2012;156:767–75, W.
21. Ross JS, Mulvey GK, Stauffer B, Patlolla V, Bernheim SM, Keenan PS, Krumholz HM. Statistical models and patient predictors of re-admission for heart failure: a systematic review. Arch Intern Med. 2008;168:1371–1386.
22. Tu JV, Donovan LR, Lee DS, Wang JT, Austin PC, Alter DA, Ko DT. Ef-fectiveness of public report cards for improving the quality of cardiac care: the EFFECT study: a randomized trial. JAMA. 2009;302:2330–2337.
23. Lee DS, Pencina MJ, Benjamin EJ, Wang TJ, Levy D, O’Donnell CJ, Nam BH, Larson MG, D’Agostino RB, Vasan RS. Association of pa-rental heart failure with risk of heart failure in offspring. N Engl J Med. 2006;355:138–147.
24. US Department of Health and Human Services. International Classifica-tion of Diseases, Ninth Revision, Clinical Modification. Washington, DC: Public Health Service, US Department of Health and Human Services; 1988.
25. World Health Organization. International Statistical Classification of Diseases and Related Health Problems, Tenth Revision. Geneva, Swit-zerland: World Health Organization; 1992.
26. Juurlink D, Preyra C, Croxford R, Chong A, Austin P, Tu J, Laupacis A. Canadian Institute for Health Information Discharge Abstract Data-base: A Validation Study. Toronto, Canada: Institute for Clinical Evalua-tive Sciences; 2006.
27. Tu JV, Naylor CD, Austin P. Temporal changes in the outcomes of acute myocardial infarction in Ontario, 1992-1996. CMAJ. 1999;161:1257–1261.
28. Lee DS, Donovan L, Austin PC, Gong Y, Liu PP, Rouleau JL, Tu JV. Com-parison of coding of heart failure and comorbidities in administrative and clinical data for use in outcomes research. Med Care. 2005;43:182–188.
29. Krumholz HM, Wang Y, Mattera JA, Wang Y, Han LF, Ingber MJ, Roman S, Normand SL. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with heart failure. Circulation. 2006;113:1693–1701.
30. Keenan PS, Normand SL, Lin Z, Drye EE, Bhat KR, Ross JS, Schuur JD, Stauffer BD, Bernheim SM, Epstein AJ, Wang Y, Herrin J, Chen J, Fe-derer JJ, Mattera JA, Wang Y, Krumholz HM. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1:29–3C7.
31. Lin DY, Wei LJ, Ying Z. Checking the Cox model with cumulative sums of martingale-based residuals. Biometrika. 1993; 80:557–72.
32. Austin PC, Grootendorst P, Anderson GM. A comparison of the abil-ity of different propensity score models to balance measured variables between treated and untreated subjects: a Monte Carlo study. Stat Med. 2007;26:734–753.
33. Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in obser-vational studies. Pharm Stat. 2011;10:150–161.
34. Austin PC. The performance of different propensity-score methods for estimating differences in proportions (risk differences or absolute risk reductions) in observational studies. Stat Med. 2010;29:2137–2148.
35. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46:399–424.
36. Felker GM, Benza RL, Chandler AB, Leimberger JD, Cuffe MS, Cal-iff RM, Gheorghiade M, O’Connor CM; OPTIME-CHF Investigators. Heart failure etiology and response to milrinone in decompensated heart failure: results from the OPTIME-CHF study. J Am Coll Cardiol. 2003;41:997–1003.
CLINICAL PERSPECTIVETroponin may be mildly elevated above the upper limit of the normal range in patients with acute heart failure syndromes; however, the prognostic implications and optimal approach to treatment are unknown. In this study of 13 656 patients present-ing to the emergency department with acute heart failure, troponin was mildly elevated above the upper limit of the normal range in 13.5%. The mortality impact of mildly elevated troponin was time dependent with a 9-fold risk of death at 30 days after emergency department presentation. The risk of ischemic heart disease hospitalization was 13-fold higher for those with mildly elevated troponin at 30 days after hospital separation. Patients with elevated troponin exhibited higher risk clinical features at emergency department presentation, with higher heart rate and respiratory rate, lower oxygen saturation, and pul-monary edema on chest radiography. Despite the higher risks of adverse outcomes among those with elevated troponin, rates of coronary angiography were low, albeit higher than those without troponin elevation (21.8 vs 11.4 patients per 100 person-years). Among patients with at least mild troponin elevation, early coronary revascularization performed within 14 days of ini-tial presentation was associated with reduced risk of death (adjusted hazard ratio, 0.29; [95% confidence interval, 0.09–0.92]). However, there was no significant reduction in mortality when early coronary revascularization was performed in those with-out troponin elevation. Although larger, confirmatory studies are required, our findings suggest that highly selected acute heart failure patients with troponin elevation who undergo early coronary revascularization may exhibit improved survival.
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
Heather J. Ross and Douglas S. LeeJuarez R. Braga, Jack V. Tu, Peter C. Austin, Alice Chong, John J. You, Michael E. Farkouh,
Troponin ElevationOutcomes and Care of Patients With Acute Heart Failure Syndromes and Cardiac
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2013 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation: Heart Failure
doi: 10.1161/CIRCHEARTFAILURE.112.0000752013;6:193-202; originally published online February 6, 2013;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/6/2/193World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2013/02/06/CIRCHEARTFAILURE.112.000075.DC1Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information isthe Editorial Office. Once the online version of the published article for which permission is being requested
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculation: Heart Failurein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 1, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
SUPPLEMENTAL MATERIAL
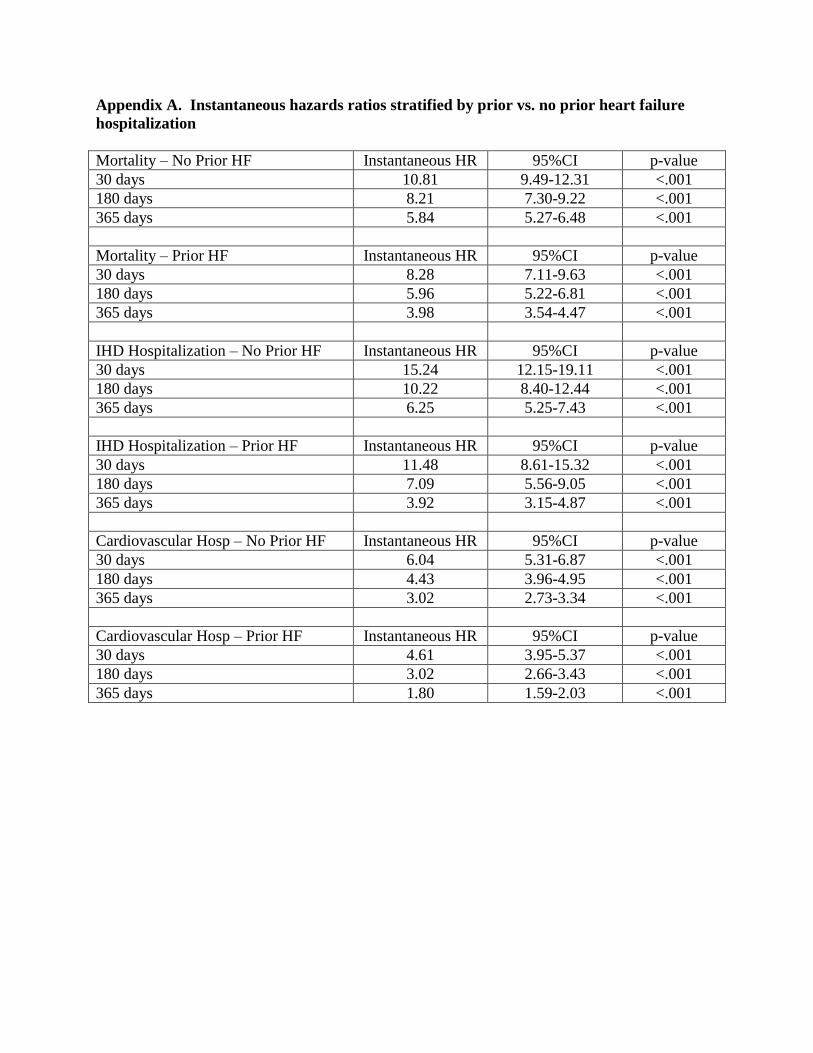
Appendix A. Instantaneous hazards ratios stratified by prior vs. no prior heart failure
hospitalization
Mortality – No Prior HF Instantaneous HR 95%CI p-value
30 days 10.81 9.49-12.31 <.001
180 days 8.21 7.30-9.22 <.001
365 days 5.84 5.27-6.48 <.001
Mortality – Prior HF Instantaneous HR 95%CI p-value
30 days 8.28 7.11-9.63 <.001
180 days 5.96 5.22-6.81 <.001
365 days 3.98 3.54-4.47 <.001
IHD Hospitalization – No Prior HF Instantaneous HR 95%CI p-value
30 days 15.24 12.15-19.11 <.001
180 days 10.22 8.40-12.44 <.001
365 days 6.25 5.25-7.43 <.001
IHD Hospitalization – Prior HF Instantaneous HR 95%CI p-value
30 days 11.48 8.61-15.32 <.001
180 days 7.09 5.56-9.05 <.001
365 days 3.92 3.15-4.87 <.001
Cardiovascular Hosp – No Prior HF Instantaneous HR 95%CI p-value
30 days 6.04 5.31-6.87 <.001
180 days 4.43 3.96-4.95 <.001
365 days 3.02 2.73-3.34 <.001
Cardiovascular Hosp – Prior HF Instantaneous HR 95%CI p-value
30 days 4.61 3.95-5.37 <.001
180 days 3.02 2.66-3.43 <.001
365 days 1.80 1.59-2.03 <.001
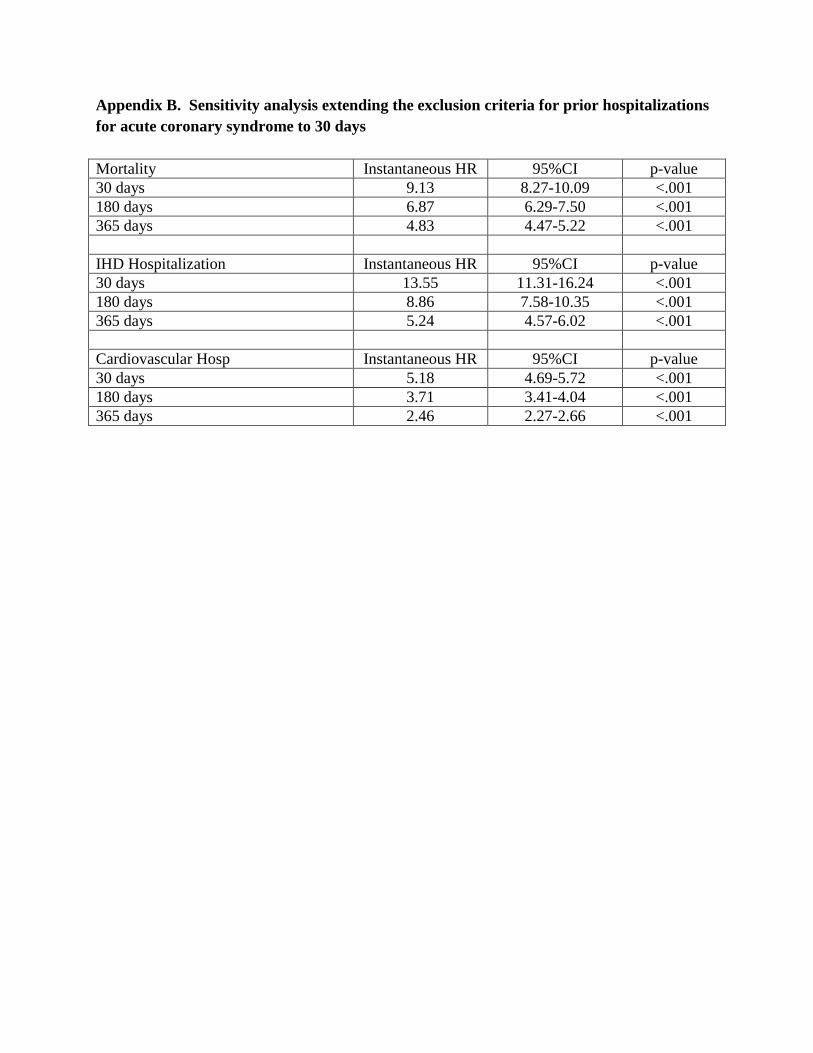
Appendix B. Sensitivity analysis extending the exclusion criteria for prior hospitalizations
for acute coronary syndrome to 30 days
Mortality Instantaneous HR 95%CI p-value
30 days 9.13 8.27-10.09 <.001
180 days 6.87 6.29-7.50 <.001
365 days 4.83 4.47-5.22 <.001
IHD Hospitalization Instantaneous HR 95%CI p-value
30 days 13.55 11.31-16.24 <.001
180 days 8.86 7.58-10.35 <.001
365 days 5.24 4.57-6.02 <.001
Cardiovascular Hosp Instantaneous HR 95%CI p-value
30 days 5.18 4.69-5.72 <.001
180 days 3.71 3.41-4.04 <.001
365 days 2.46 2.27-2.66 <.001