Embed Size (px)
Citation preview

279
Despite significant improvements in the treatment of chronic heart failure (CHF), mortality remains as high as 20% to 30%
after 3 years.1–3 The costs for heart failure (HF) care approach 2% of the total health care expenditure in Western countries, primarily due to hospitalization for decompensation.4 As a result, the past decade has witnessed a surge in finding reliable markers to iden-tify patients at risk of early death and impending decompensation.
Clinical Perspective on p 287
Physical fitness predicts cardiovascular mortality in the population at large.5–7 The collection of multiple parameters
derived during cardiorespiratory exercise testing, in particu-lar the minute ventilation/CO
2 production relationship (the
VE/VCO2 slope) in conjunction with peak O
2 uptake, allows
prognostic stratification in patients with CHF.8 However, repetitive cardiopulmonary exercise testing, which may be required for a dynamic condition such as CHF, is demanding in clinical practice.9
Daily physical activity (PA) has been shown to predict out-come in various chronic diseases.10–12 However, data for the CHF population are scarce and are often based on qualitative subjective patient and physician reports or questionnaires or
Original Article
© 2014 American Heart Association, Inc.
Circ Heart Fail is available at http://circheartfailure.ahajournals.org DOI: 10.1161/CIRCHEARTFAILURE.113.000883
Background—Physical activity (PA) predicts cardiovascular mortality in the population at large. Less is known about its prognostic value in patients with chronic heart failure (HF).
Methods and Results—Data from 836 patients with implantable cardioverter defibrillator without or with cardiac resynchronization therapy enrolled in the Sensitivity of the InSync Sentry OptiVol feature for the prediction of Heart Failure (SENSE-HF)1 study and the Diagnostic Outcome Trial in Heart Failure (DOT-HF) were pooled. The devices continuously measured and stored total daily active time (single-axis accelerometer). Early PA (average daily activity over the earliest 30-day study period) was studied as a predictor of time to death or HF-related hospital admission (primary end point). Data from 781 patients were analyzed (65±10 years; 85% men; left ventricular ejection fraction, 26±7%). Older age, shorter height, ischemic cause, peripheral artery disease, atrial fibrillation, diabetes mellitus, rales, peripheral edema, higher New York Heart Association class, lower diastolic blood pressure, and no angiotensin II receptor blocker/angiotensin-converting enzyme inhibitor use were associated with reduced early PA. The primary end point occurred in 135 patients (15±7 months of follow-up). In multivariable analysis including baseline variables, early PA predicted death or HF hospitalization, with a 4% reduction in risk for each 10 minutes per day additional activity (hazard ratio [HR], 0.96; confidence interval [CI], 0.94–0.98; P=0.0002 compared with a model with the same baseline variables but without PA). PA also predicted death (HR, 0.93; CI, 0.90–0.96; P<0.0001) and HF hospitalization (HR, 0.97; CI, 0.95–0.99; P=0.011).
Conclusions—Early PA, averaged over a 30-day window early after defibrillator implantation or cardiac resynchronization therapy in patients with chronic HF, predicted death or HF hospitalization, as well as mortality and HF hospitalization separately, accounting for baseline HF severity.
Clinical Trial Registration Information—URL: http://www.clinicaltrials.gov. Unique identifiers: NCT00400985, NCT00480077. (Circ Heart Fail. 2014;7:279-287.)
Key Words: heart failure ◼ mortality ◼ physical activity
Received May 6, 2013; accepted January 30, 2014.From the Department of Cardiology, Antwerp University Hospital, Edegem, Belgium (V.V.C.); University of Antwerp, Antwerp, Belgium (V.V.C.);
Department of Research and Education, CIRO+, Center of Expertise for Chronic Organ Failure, Horn, the Netherlands (M.A.S.); REVAL–Rehabilitation Research Center, BIOMED–Biomedical Research Institute, Faculty of Medicine and Life Sciences, Hasselt University, Diepenbeek, Belgium (M.A.S.); Karolinska Institutet, Department of Cardiology, Karolinska University Hospital, Stockholm, Sweden (F.B.); National Heart and Lung Institute, Imperial College, London, United Kingdom (M.R.C.); Maria Cecilia Hospital, GVM Care and Research, E.S. Health Science Foundation, Cotignola, Italy (L.T.); Department of Cardiology, University Hospital Mannheim, Mannheim, Germany (M.B.); Medtronic Inc, Minneapolis, MN (M.R.S.H.); Medtronic Bakken Research Center, Maastricht, the Netherlands (S.J., B.G.); and Department of Cardiology, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands (D.J.v.V).
*Dr Conraads died on December 12, 2013. She is greatly missed.The Data Supplement is available at http://circheartfailure.ahajournals.org/lookup/suppl/doi:10.1161/CIRCHEARTFAILURE.113.000883/-/DC1. Correspondence to Dirk J. van Veldhuisen, MD, Department of Cardiology, University Medical Center Groningen, University of Groningen, PO
Box 30.001, 9700RB Groningen, the Netherlands. E-mail [email protected]
Physical Activity Measured With Implanted Devices Predicts Patient Outcome in Chronic Heart Failure
Viviane M. Conraads, MD*; Martijn A. Spruit, PhD; Frieder Braunschweig, MD; Martin R. Cowie, MD; Luigi Tavazzi, MD; Martin Borggrefe, MD; Michael R.S. Hill, PhD;
Sandra Jacobs, PhD; Bart Gerritse, PhD; Dirk J. van Veldhuisen, MD
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 27, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 27, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
ay 27, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

280 Circ Heart Fail March 2014
short-term measurement with pedometers and accelerometers.13–15 Continuous recording of PA, through accelerometers incorpo-rated in implanted devices, may more accurately address the question whether PA merely reflects disease severity16 or whether it is an independent prognostic marker.
The Sensitivity of the InSync Sentry OptiVol feature for the prediction of Heart Failure (SENSE-HF)1 study and the Diagnostic Outcome Trial in Heart Failure (DOT-HF)17 are recent prospective trials conducted to evaluate the utility of intrathoracic impedance measurement, incorporated as a diag-nostic feature in implantable cardioverter defibrillator without (ICD) or with cardiac resynchronization therapy (CRT-D). These devices also measured and stored total daily active time. We analyzed the pooled patient data from SENSE-HF and DOT-HF to determine whether and to what extent daily PA as measured by implanted devices is related to patient outcome.
MethodsPatient PopulationDetailed descriptions of the design and results of SENSE-HF and DOT-HF have been published previously.18,19 Briefly, SENSE-HF18 enrolled 501 patients <34 days after implantation of an ICD or CRT-D with the OptiVol feature (Medtronic Inc, Minneapolis, MN), which measures intrathoracic impedance. After a waiting period of 34 days to ensure correct measurement of intrathoracic impedance, patients were followed up for 6 months to determine the sensitivity and the positive predictive value of OptiVol intrathoracic fluid monitoring for the detection of HF-related hospitalizations (phase I, blinded). Phase I was followed by maximally 18 months with full access to the device data. PA was recorded and stored during the entire study period, start-ing at day 35 postimplant.
DOT-HF17,19 tested whether physician access to device-based diag-nostic information, including audible patient alerts for decreasing in-trathoracic impedance, would improve outcome in patients with HF. In total, 335 patients were randomized to an access versus a control arm between 35 days and 6 months after implantation with an ICD or CRT-D. Patients were followed up for 15 months, during which PA was continuously measured and stored.
The Table in the Data Supplement describes end points and the major inclusion and exclusion criteria for both studies. Both studies were approved by the local ethics committees, and written informed consent was obtained from all patients. Given the similarities in pa-tient population and treatment, and because all devices in SENSE-HF and DOT-HF recorded and stored PA during daily life on a continuous basis, it was decided to pool and analyze patient data from both trials. The authors had full access to the study data.
Study End PointsThe primary end point of the present analysis was time to death or HF-related hospital admission. Time to death and time to first HF-related hospital admission were analyzed as secondary end points. HF hospi-talizations were adjudicated by study-specific, independent, blinded Adverse Event Advisory Committees.18,19
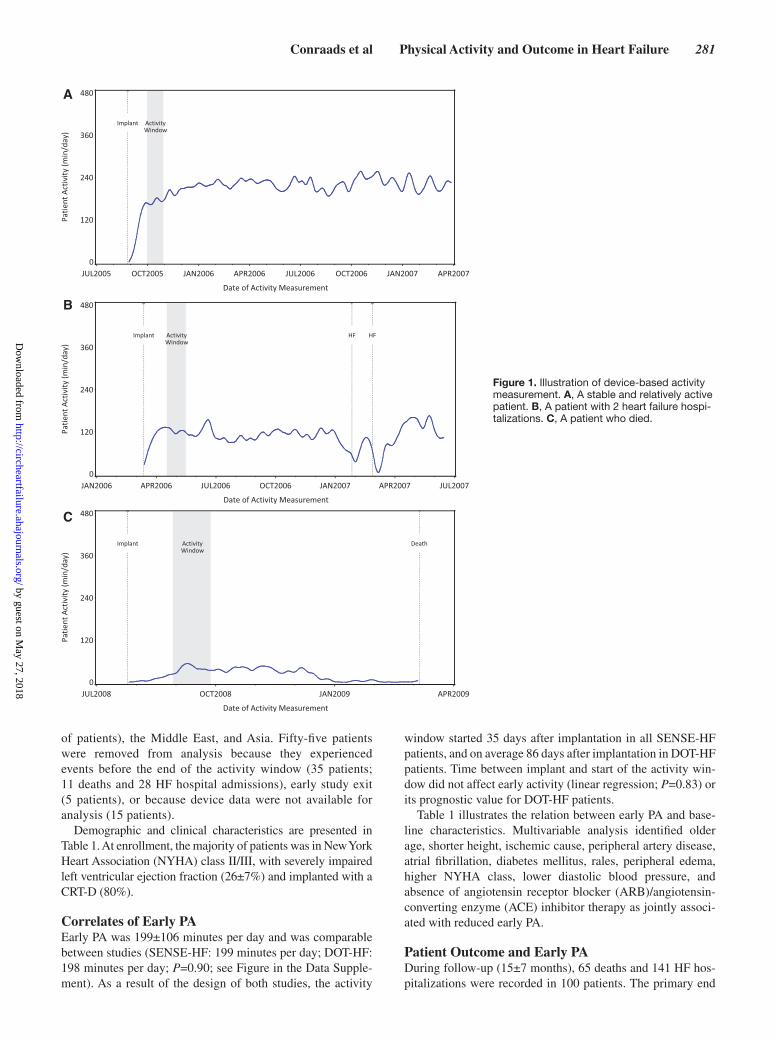
Device Measurement of Daily PAThe activity measurement in the devices is designed to capture nor-mal daily activities in patients with HF, including walking at a slow pace. A single-axis accelerometer is used to capture patient motion as an electric signal. The number of minutes a patient is active per day is counted, where a minute is considered active if a threshold is reached that incorporates both the number and magnitude of deflections in the accelerometer signal. The devices store the number of active minutes for the most recent 425 days (Figure 1), and this information was retrieved from device memory for this analysis. The sensor provides a quantification of patient activity that, due to the specifics of the
algorithm, may numerically differ from measurements obtained from other devices such as pedometers or external accelerometers.
Analyses MethodsWe defined early PA as the average daily activity over the earliest 30-day period in the study (the activity window). For patients in SENSE-HF, this window started 35 days after implant and continued until day 64. For patients in DOT-HF, the activity window started after randomization, which was between day 35 and day 183 post-implant. We averaged 30 daily values to account for within-patient variability. Patients were excluded from analysis if they died or had a HF hospitalization during or before the 30-day activity window, or if there were <7 days with valid activity data in the window.
Because lower activity was expected to be associated with a gener-ally worse condition of patients, we investigated the relation of early activity with baseline characteristics. The relation of early PA and out-come as well as the incremental value of activity as a risk marker when added to known risk factors was assessed in line with the American Heart Association scientific statement on evaluation of novel markers of cardiovascular risk.20 As measures of known risk, we determined the best predictive model based on baseline patient characteristics, and we used The Candesartan in Heart failure Assessment of Reduction in Mortality and morbidity (CHARM) programme risk score, a validated score for risk of all-cause death in patients with HF.21 For both ap-proaches, time-to-event models including and excluding early activity are compared to determine incremental predictive value.
Statistical AnalysesResults are reported with mean and standard deviation for continu-ous, and counts and percentages for categorical variables. The rela-tion between baseline characteristics and early PA was analyzed with t test for dichotomous and linear regression for ordinal and continu-ous characteristics. Reported effect sizes (Table 1) are observed dif-ferences for dichotomous characteristics, and regression coefficients otherwise. Multivariable linear regression with backward variable elimination was used to assess joint association with early activity.
For calculation of the CHARM risk score, coefficients were taken from the study by Pocock et al.21 Multiple imputation was used to ac-count for missing values, using the multivariate normal specification. For categorical variables, the imputed value was rounded to the near-est coded category value. Ten completed data sets were generated. The CHARM risk score was calculated for each completion sepa-rately. Finally, Rubin rule was used to determine a single risk score value per patient.
Cox proportional hazards regression was used to analyze the relation between events and early PA, which was included as a continuous vari-able. Patients were considered at risk starting at the end of the activity window (time zero). Hazard ratio (HR) with associated 95% confidence interval (CI) is reported for 10 minutes per day incremental activity. The incidence of end points is illustrated with Kaplan–Meier graphs with patients divided into 2 or 3 equal-sized groups using medians or tertiles as cut points. Multivariable proportional hazards models using model reduction with backward selection are used to define predictive models based on baseline characteristics. To assess the incremental predictive value of early activity, multivariable models including and excluding early activity are compared using likelihood ratio tests. The predictive ability of models is quantified using the Harrell c-index, which extends the area under the receiver operating characteristic curve to the context of time-to-event data with censoring.22
All analyses were done using SAS (version 9.3; SAS Institute Inc, Cary, NC) or R (version 3.0.1; the R project for statistical computing; www.r-project.org), and P values <0.05 were considered significant. No correction for multiple testing was applied.
ResultsPatientsSENSE-HF and DOT-HF together enrolled 836 patients between 2005 and 2009 in 100 centers across Europe (91%
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
Conraads et al Physical Activity and Outcome in Heart Failure 281
of patients), the Middle East, and Asia. Fifty-five patients were removed from analysis because they experienced events before the end of the activity window (35 patients; 11 deaths and 28 HF hospital admissions), early study exit (5 patients), or because device data were not available for analysis (15 patients).
Demographic and clinical characteristics are presented in Table 1. At enrollment, the majority of patients was in New York Heart Association (NYHA) class II/III, with severely impaired left ventricular ejection fraction (26±7%) and implanted with a CRT-D (80%).
Correlates of Early PAEarly PA was 199±106 minutes per day and was comparable between studies (SENSE-HF: 199 minutes per day; DOT-HF: 198 minutes per day; P=0.90; see Figure in the Data Supple-ment). As a result of the design of both studies, the activity
window started 35 days after implantation in all SENSE-HF patients, and on average 86 days after implantation in DOT-HF patients. Time between implant and start of the activity win-dow did not affect early activity (linear regression; P=0.83) or its prognostic value for DOT-HF patients.
Table 1 illustrates the relation between early PA and base-line characteristics. Multivariable analysis identified older age, shorter height, ischemic cause, peripheral artery disease, atrial fibrillation, diabetes mellitus, rales, peripheral edema, higher NYHA class, lower diastolic blood pressure, and absence of angiotensin receptor blocker (ARB)/angiotensin-converting enzyme (ACE) inhibitor therapy as jointly associ-ated with reduced early PA.
Patient Outcome and Early PADuring follow-up (15±7 months), 65 deaths and 141 HF hos-pitalizations were recorded in 100 patients. The primary end
A
B
C
Figure 1. Illustration of device-based activity measurement. A, A stable and relatively active patient. B, A patient with 2 heart failure hospi-talizations. C, A patient who died.
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
282 Circ Heart Fail March 2014
point of death or HF hospitalization occurred in 135 patients. Early PA was significantly associated with the primary end point, with 5% relative reduction of risk for each 10 minutes per day additional activity (HR, 0.95; CI, 0.94–0.97; P<0.0001). There were also significant associations with death (HR, 0.92; CI, 0.89–0.95; P<0.0001) and HF hospitalization (HR, 0.97;
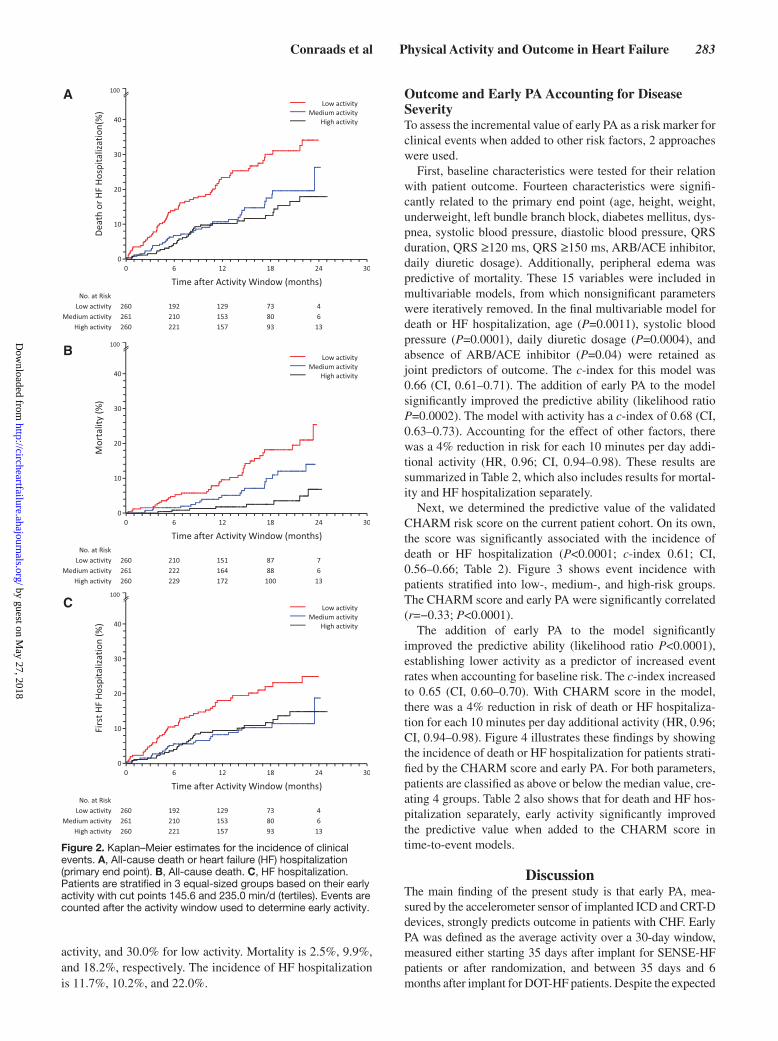
CI, 0.95–0.99; P=0.0011). Figure 2 shows event incidence with patients stratified into 3 equal-sized groups according to early PA. The cut points are 235 minutes per day between high and medium activity and 146 minutes per day between medium and low activity. The incidence of primary end point at 18 months is 12.5% for high activity, 17.5% for medium
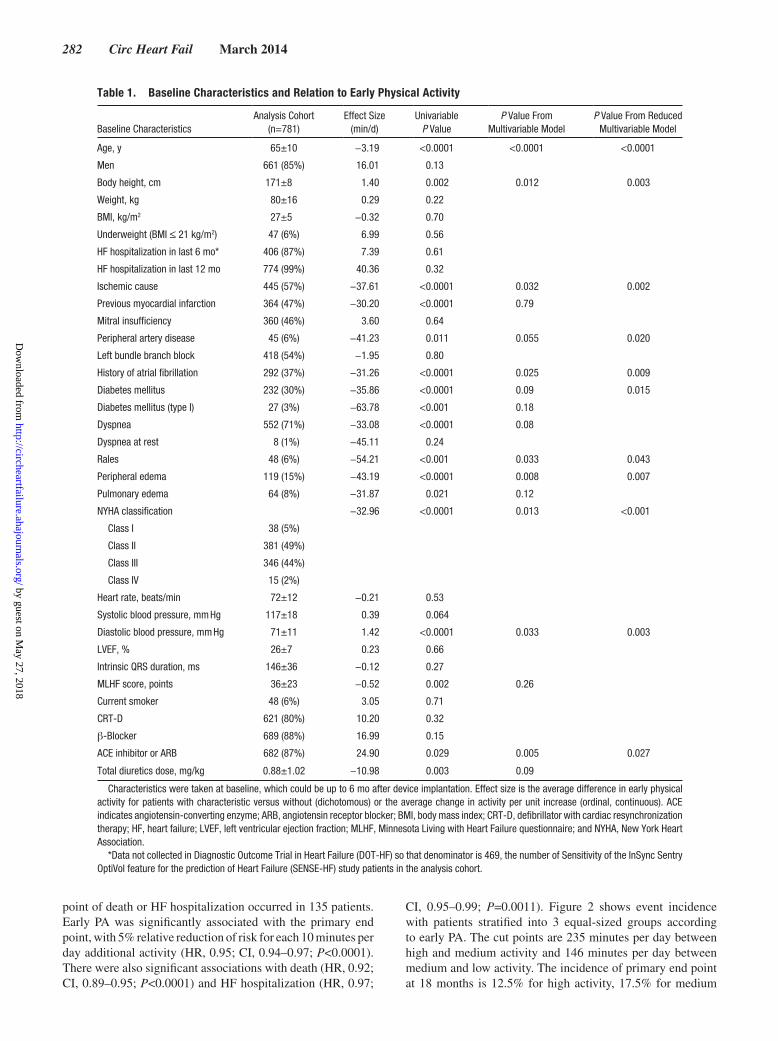
Table 1. Baseline Characteristics and Relation to Early Physical Activity
Baseline CharacteristicsAnalysis Cohort
(n=781)Effect Size
(min/d)Univariable
P ValueP Value From
Multivariable ModelP Value From Reduced
Multivariable Model
Age, y 65±10 −3.19 <0.0001 <0.0001 <0.0001
Men 661 (85%) 16.01 0.13
Body height, cm 171±8 1.40 0.002 0.012 0.003
Weight, kg 80±16 0.29 0.22
BMI, kg/m2 27±5 −0.32 0.70
Underweight (BMI ≤ 21 kg/m2) 47 (6%) 6.99 0.56
HF hospitalization in last 6 mo* 406 (87%) 7.39 0.61
HF hospitalization in last 12 mo 774 (99%) 40.36 0.32
Ischemic cause 445 (57%) −37.61 <0.0001 0.032 0.002
Previous myocardial infarction 364 (47%) −30.20 <0.0001 0.79
Mitral insufficiency 360 (46%) 3.60 0.64
Peripheral artery disease 45 (6%) −41.23 0.011 0.055 0.020
Left bundle branch block 418 (54%) −1.95 0.80
History of atrial fibrillation 292 (37%) −31.26 <0.0001 0.025 0.009
Diabetes mellitus 232 (30%) −35.86 <0.0001 0.09 0.015
Diabetes mellitus (type I) 27 (3%) −63.78 <0.001 0.18
Dyspnea 552 (71%) −33.08 <0.0001 0.08
Dyspnea at rest 8 (1%) −45.11 0.24
Rales 48 (6%) −54.21 <0.001 0.033 0.043
Peripheral edema 119 (15%) −43.19 <0.0001 0.008 0.007
Pulmonary edema 64 (8%) −31.87 0.021 0.12
NYHA classification −32.96 <0.0001 0.013 <0.001
Class I 38 (5%)
Class II 381 (49%)
Class III 346 (44%)
Class IV 15 (2%)
Heart rate, beats/min 72±12 −0.21 0.53
Systolic blood pressure, mm Hg 117±18 0.39 0.064
Diastolic blood pressure, mm Hg 71±11 1.42 <0.0001 0.033 0.003
LVEF, % 26±7 0.23 0.66
Intrinsic QRS duration, ms 146±36 −0.12 0.27
MLHF score, points 36±23 −0.52 0.002 0.26
Current smoker 48 (6%) 3.05 0.71
CRT-D 621 (80%) 10.20 0.32
β-Blocker 689 (88%) 16.99 0.15
ACE inhibitor or ARB 682 (87%) 24.90 0.029 0.005 0.027
Total diuretics dose, mg/kg 0.88±1.02 −10.98 0.003 0.09
Characteristics were taken at baseline, which could be up to 6 mo after device implantation. Effect size is the average difference in early physical activity for patients with characteristic versus without (dichotomous) or the average change in activity per unit increase (ordinal, continuous). ACE indicates angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; CRT-D, defibrillator with cardiac resynchronization therapy; HF, heart failure; LVEF, left ventricular ejection fraction; MLHF, Minnesota Living with Heart Failure questionnaire; and NYHA, New York Heart Association.
*Data not collected in Diagnostic Outcome Trial in Heart Failure (DOT-HF) so that denominator is 469, the number of Sensitivity of the InSync Sentry OptiVol feature for the prediction of Heart Failure (SENSE-HF) study patients in the analysis cohort.
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
Conraads et al Physical Activity and Outcome in Heart Failure 283
activity, and 30.0% for low activity. Mortality is 2.5%, 9.9%, and 18.2%, respectively. The incidence of HF hospitalization is 11.7%, 10.2%, and 22.0%.
Outcome and Early PA Accounting for Disease SeverityTo assess the incremental value of early PA as a risk marker for clinical events when added to other risk factors, 2 approaches were used.
First, baseline characteristics were tested for their relation with patient outcome. Fourteen characteristics were signifi-cantly related to the primary end point (age, height, weight, underweight, left bundle branch block, diabetes mellitus, dys-pnea, systolic blood pressure, diastolic blood pressure, QRS duration, QRS ≥120 ms, QRS ≥150 ms, ARB/ACE inhibitor, daily diuretic dosage). Additionally, peripheral edema was predictive of mortality. These 15 variables were included in multivariable models, from which nonsignificant parameters were iteratively removed. In the final multivariable model for death or HF hospitalization, age (P=0.0011), systolic blood pressure (P=0.0001), daily diuretic dosage (P=0.0004), and absence of ARB/ACE inhibitor (P=0.04) were retained as joint predictors of outcome. The c-index for this model was 0.66 (CI, 0.61–0.71). The addition of early PA to the model significantly improved the predictive ability (likelihood ratio P=0.0002). The model with activity has a c-index of 0.68 (CI, 0.63–0.73). Accounting for the effect of other factors, there was a 4% reduction in risk for each 10 minutes per day addi-tional activity (HR, 0.96; CI, 0.94–0.98). These results are summarized in Table 2, which also includes results for mortal-ity and HF hospitalization separately.
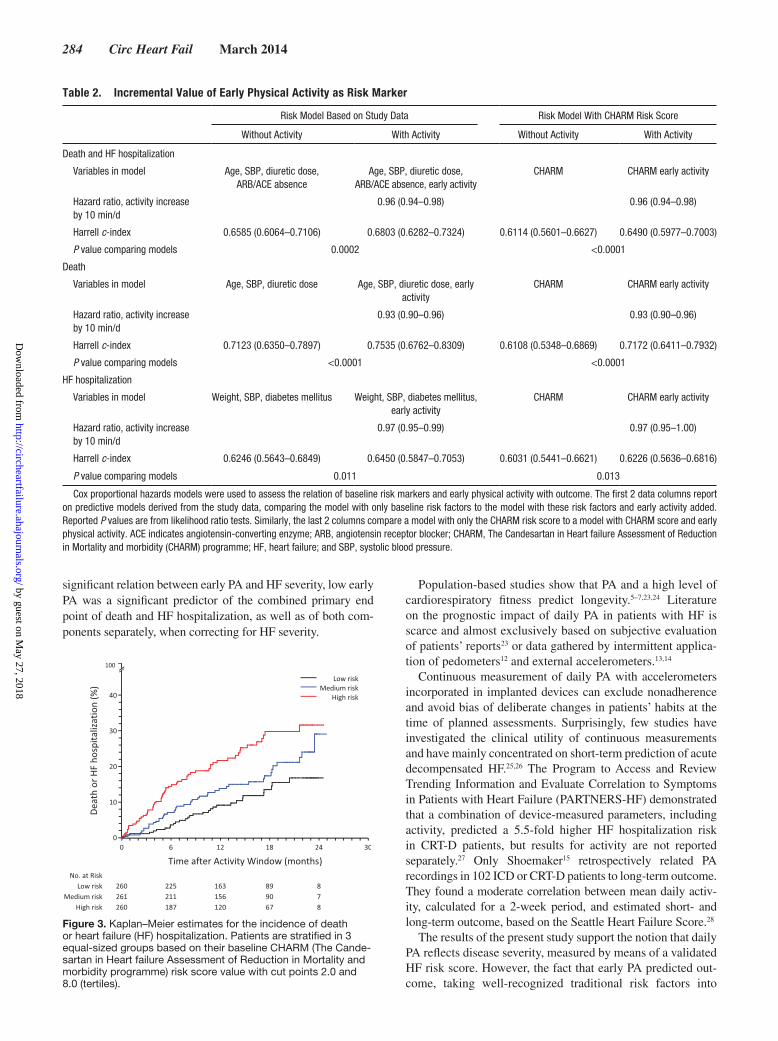
Next, we determined the predictive value of the validated CHARM risk score on the current patient cohort. On its own, the score was significantly associated with the incidence of death or HF hospitalization (P<0.0001; c-index 0.61; CI, 0.56–0.66; Table 2). Figure 3 shows event incidence with patients stratified into low-, medium-, and high-risk groups. The CHARM score and early PA were significantly correlated (r=−0.33; P<0.0001).
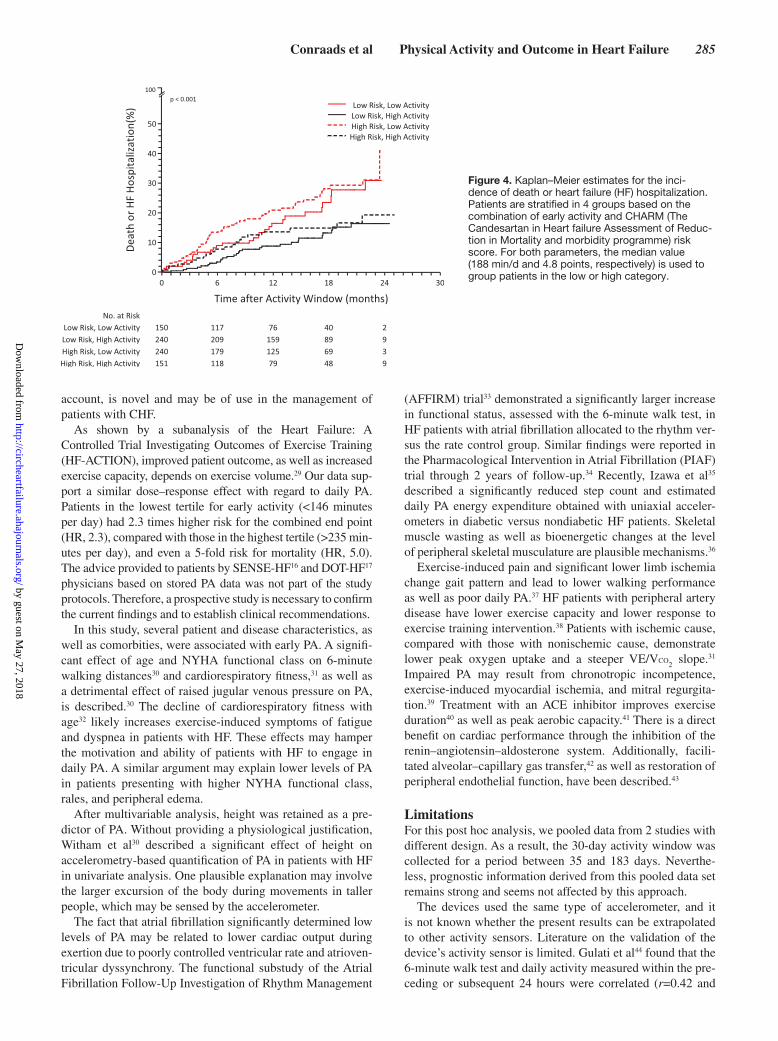
The addition of early PA to the model significantly improved the predictive ability (likelihood ratio P<0.0001), establishing lower activity as a predictor of increased event rates when accounting for baseline risk. The c-index increased to 0.65 (CI, 0.60–0.70). With CHARM score in the model, there was a 4% reduction in risk of death or HF hospitaliza-tion for each 10 minutes per day additional activity (HR, 0.96; CI, 0.94–0.98). Figure 4 illustrates these findings by showing the incidence of death or HF hospitalization for patients strati-fied by the CHARM score and early PA. For both parameters, patients are classified as above or below the median value, cre-ating 4 groups. Table 2 also shows that for death and HF hos-pitalization separately, early activity significantly improved the predictive value when added to the CHARM score in time-to-event models.
DiscussionThe main finding of the present study is that early PA, mea-sured by the accelerometer sensor of implanted ICD and CRT-D devices, strongly predicts outcome in patients with CHF. Early PA was defined as the average activity over a 30-day window, measured either starting 35 days after implant for SENSE-HF patients or after randomization, and between 35 days and 6 months after implant for DOT-HF patients. Despite the expected
A
B
C
Figure 2. Kaplan–Meier estimates for the incidence of clinical events. A, All-cause death or heart failure (HF) hospitalization (primary end point). B, All-cause death. C, HF hospitalization. Patients are stratified in 3 equal-sized groups based on their early activity with cut points 145.6 and 235.0 min/d (tertiles). Events are counted after the activity window used to determine early activity.
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
284 Circ Heart Fail March 2014
significant relation between early PA and HF severity, low early PA was a significant predictor of the combined primary end point of death and HF hospitalization, as well as of both com-ponents separately, when correcting for HF severity.
Population-based studies show that PA and a high level of cardiorespiratory fitness predict longevity.5–7,23,24 Literature on the prognostic impact of daily PA in patients with HF is scarce and almost exclusively based on subjective evaluation of patients’ reports23 or data gathered by intermittent applica-tion of pedometers12 and external accelerometers.13,14
Continuous measurement of daily PA with accelerometers incorporated in implanted devices can exclude nonadherence and avoid bias of deliberate changes in patients’ habits at the time of planned assessments. Surprisingly, few studies have investigated the clinical utility of continuous measurements and have mainly concentrated on short-term prediction of acute decompensated HF.25,26 The Program to Access and Review Trending Information and Evaluate Correlation to Symptoms in Patients with Heart Failure (PARTNERS-HF) demonstrated that a combination of device-measured parameters, including activity, predicted a 5.5-fold higher HF hospitalization risk in CRT-D patients, but results for activity are not reported separately.27 Only Shoemaker15 retrospectively related PA recordings in 102 ICD or CRT-D patients to long-term outcome. They found a moderate correlation between mean daily activ-ity, calculated for a 2-week period, and estimated short- and long-term outcome, based on the Seattle Heart Failure Score.28
The results of the present study support the notion that daily PA reflects disease severity, measured by means of a validated HF risk score. However, the fact that early PA predicted out-come, taking well-recognized traditional risk factors into
Figure 3. Kaplan–Meier estimates for the incidence of death or heart failure (HF) hospitalization. Patients are stratified in 3 equal-sized groups based on their baseline CHARM (The Cande-sartan in Heart failure Assessment of Reduction in Mortality and morbidity programme) risk score value with cut points 2.0 and 8.0 (tertiles).
Table 2. Incremental Value of Early Physical Activity as Risk Marker
Risk Model Based on Study Data Risk Model With CHARM Risk Score
Without Activity With Activity Without Activity With Activity
Death and HF hospitalization
Variables in model Age, SBP, diuretic dose, ARB/ACE absence
Age, SBP, diuretic dose, ARB/ACE absence, early activity
CHARM CHARM early activity
Hazard ratio, activity increase by 10 min/d
0.96 (0.94–0.98) 0.96 (0.94–0.98)
Harrell c-index 0.6585 (0.6064–0.7106) 0.6803 (0.6282–0.7324) 0.6114 (0.5601–0.6627) 0.6490 (0.5977–0.7003)
P value comparing models 0.0002 <0.0001
Death
Variables in model Age, SBP, diuretic dose Age, SBP, diuretic dose, early activity
CHARM CHARM early activity
Hazard ratio, activity increase by 10 min/d
0.93 (0.90–0.96) 0.93 (0.90–0.96)
Harrell c-index 0.7123 (0.6350–0.7897) 0.7535 (0.6762–0.8309) 0.6108 (0.5348–0.6869) 0.7172 (0.6411–0.7932)
P value comparing models <0.0001 <0.0001
HF hospitalization
Variables in model Weight, SBP, diabetes mellitus Weight, SBP, diabetes mellitus, early activity
CHARM CHARM early activity
Hazard ratio, activity increase by 10 min/d
0.97 (0.95–0.99) 0.97 (0.95–1.00)
Harrell c-index 0.6246 (0.5643–0.6849) 0.6450 (0.5847–0.7053) 0.6031 (0.5441–0.6621) 0.6226 (0.5636–0.6816)
P value comparing models 0.011 0.013
Cox proportional hazards models were used to assess the relation of baseline risk markers and early physical activity with outcome. The first 2 data columns report on predictive models derived from the study data, comparing the model with only baseline risk factors to the model with these risk factors and early activity added. Reported P values are from likelihood ratio tests. Similarly, the last 2 columns compare a model with only the CHARM risk score to a model with CHARM score and early physical activity. ACE indicates angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CHARM, The Candesartan in Heart failure Assessment of Reduction in Mortality and morbidity (CHARM) programme; HF, heart failure; and SBP, systolic blood pressure.
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
Conraads et al Physical Activity and Outcome in Heart Failure 285
account, is novel and may be of use in the management of patients with CHF.
As shown by a subanalysis of the Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training (HF-ACTION), improved patient outcome, as well as increased exercise capacity, depends on exercise volume.29 Our data sup-port a similar dose–response effect with regard to daily PA. Patients in the lowest tertile for early activity (<146 minutes per day) had 2.3 times higher risk for the combined end point (HR, 2.3), compared with those in the highest tertile (>235 min-utes per day), and even a 5-fold risk for mortality (HR, 5.0). The advice provided to patients by SENSE-HF16 and DOT-HF17 physicians based on stored PA data was not part of the study protocols. Therefore, a prospective study is necessary to confirm the current findings and to establish clinical recommendations.
In this study, several patient and disease characteristics, as well as comorbities, were associated with early PA. A signifi-cant effect of age and NYHA functional class on 6-minute walking distances30 and cardiorespiratory fitness,31 as well as a detrimental effect of raised jugular venous pressure on PA, is described.30 The decline of cardiorespiratory fitness with age32 likely increases exercise-induced symptoms of fatigue and dyspnea in patients with HF. These effects may hamper the motivation and ability of patients with HF to engage in daily PA. A similar argument may explain lower levels of PA in patients presenting with higher NYHA functional class, rales, and peripheral edema.
After multivariable analysis, height was retained as a pre-dictor of PA. Without providing a physiological justification, Witham et al30 described a significant effect of height on accelerometry-based quantification of PA in patients with HF in univariate analysis. One plausible explanation may involve the larger excursion of the body during movements in taller people, which may be sensed by the accelerometer.
The fact that atrial fibrillation significantly determined low levels of PA may be related to lower cardiac output during exertion due to poorly controlled ventricular rate and atrioven-tricular dyssynchrony. The functional substudy of the Atrial Fibrillation Follow-Up Investigation of Rhythm Management
(AFFIRM) trial33 demonstrated a significantly larger increase in functional status, assessed with the 6-minute walk test, in HF patients with atrial fibrillation allocated to the rhythm ver-sus the rate control group. Similar findings were reported in the Pharmacological Intervention in Atrial Fibrillation (PIAF) trial through 2 years of follow-up.34 Recently, Izawa et al35 described a significantly reduced step count and estimated daily PA energy expenditure obtained with uniaxial acceler-ometers in diabetic versus nondiabetic HF patients. Skeletal muscle wasting as well as bioenergetic changes at the level of peripheral skeletal musculature are plausible mechanisms.36
Exercise-induced pain and significant lower limb ischemia change gait pattern and lead to lower walking performance as well as poor daily PA.37 HF patients with peripheral artery disease have lower exercise capacity and lower response to exercise training intervention.38 Patients with ischemic cause, compared with those with nonischemic cause, demonstrate lower peak oxygen uptake and a steeper VE/VCO
2 slope.31
Impaired PA may result from chronotropic incompetence, exercise-induced myocardial ischemia, and mitral regurgita-tion.39 Treatment with an ACE inhibitor improves exercise duration40 as well as peak aerobic capacity.41 There is a direct benefit on cardiac performance through the inhibition of the renin–angiotensin–aldosterone system. Additionally, facili-tated alveolar–capillary gas transfer,42 as well as restoration of peripheral endothelial function, have been described.43
LimitationsFor this post hoc analysis, we pooled data from 2 studies with different design. As a result, the 30-day activity window was collected for a period between 35 and 183 days. Neverthe-less, prognostic information derived from this pooled data set remains strong and seems not affected by this approach.
The devices used the same type of accelerometer, and it is not known whether the present results can be extrapolated to other activity sensors. Literature on the validation of the device’s activity sensor is limited. Gulati et al44 found that the 6-minute walk test and daily activity measured within the pre-ceding or subsequent 24 hours were correlated (r=0.42 and
Figure 4. Kaplan–Meier estimates for the inci-dence of death or heart failure (HF) hospitalization. Patients are stratified in 4 groups based on the combination of early activity and CHARM (The Candesartan in Heart failure Assessment of Reduc-tion in Mortality and morbidity programme) risk score. For both parameters, the median value (188 min/d and 4.8 points, respectively) is used to group patients in the low or high category.
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

286 Circ Heart Fail March 2014
0.49, respectively). A similar relation was found in a subset of 83 patients enrolled in SENSE-HF in whom the 6-minute walk test was conducted (r=0.43; P<0.0001). Braunschweig et al45 calculated weekly means of PA in a group of 56 patients after the novo device implant using the same accelerometer. There was a steady increase in weekly PA, which was clearly related to NYHA functional class with absolute values after 4 weeks that were well within the range of current observations (283±97, 206±132, and 186±53 minutes per day for NYHA II, III, and IV, respectively).
The CHARM risk score was developed from a large num-ber of nondevice patients across a broad spectrum of HF.21 Nevertheless, the risk score strongly predicted outcome for the currently analyzed cohort of patients, characterized by broad QRS complexes, impaired systolic left ventricular func-tion, and implanted with either an ICD or a CRT-D.
The studies analyzed here did not enroll patients in the United States. Therefore, clinical recommendations for daily PA derived from the present analyses may not be applicable to the American HF population. Finally, >30 tests were performed to assess the relation between activity and baseline character-istics so that some of the significant findings may be spurious.
ConclusionsEarly PA, averaged over a 30-day window early after ICD or CRT-D implant in patients with CHF, predicted death or HF hospitalization, as well as mortality and HF hospitalization separately, also corrected for disease severity. These findings underscore the validity of spontaneous PA as a clinical status marker. Whether regular follow-up of PA, provided by accel-erometers in implanted devices, will aid physicians in modify-ing patients’ lifestyle and whether this will improve outcome may need to be prospectively studied.
Sources of FundingThis study was funded by the Medtronic Bakken Research Center. M.R.C. receives salary support from the National Institute for Health Research Cardiovascular Biomedical Research Unit at the Royal Brompton Hospital. D.J.v.V. is an established investigator of the Netherlands Heart Foundation (grant No. D97.017). V.M.C. was sup-ported by Fonds Wetenschappelijk Onderzoek-Flanders as a clinical postdoctoral fellow.
DisclosuresDrs Borggrefe, Braunschweig, Conraads, Cowie, van Veldhuisen, and Tavazzi received consultancy fees or research grants from Medtronic and from other device companies. Drs Conraads, Cowie, and Tavazzi served on the Steering Committee of the SENSE-HF study. Drs Borggrefe, Braunschweig, Conraads, Cowie, and van Veldhuisen served on the Steering Committee for DOT-HF. Drs Hill, Jacobs, and Gerritse are employees of Medtronic. Dr Gerritse reports having eq-uity in Medtronic. Dr Spruit has no conflicts to report.
References 1. Böhm M, Swedberg K, Komajda M, Borer JS, Ford I, Dubost-Brama
A, Lerebours G, Tavazzi L; SHIFT Investigators. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet. 2010;376:886–894.
2. Meta-analysis Global Group in Chronic Heart F. The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: an individual patient data meta-analysis. Eur Heart J. 2012;33:1750–1757.
3. Braunschweig F, Cowie MR, Auricchio A. What are the costs of heart failure? Europace. 2011;13(suppl 2):ii13–ii17.
4. Paffenbarger RS Jr, Hyde RT, Wing AL, Lee IM, Jung DL, Kampert JB. The association of changes in physical-activity level and other lifestyle charac-teristics with mortality among men. N Engl J Med. 1993;328:538–545.
5. Blair SN, Kohl HW III, Barlow CE, Paffenbarger RS Jr, Gibbons LW, Macera CA. Changes in physical fitness and all-cause mortality. A prospec-tive study of healthy and unhealthy men. JAMA. 1995;273:1093–1098.
6. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346:793–801.
7. Guazzi M, Adams V, Conraads V, Halle M, Mezzani A, Vanhees L, Arena R, Fletcher GF, Forman DE, Kitzman DW, Lavie CJ, Myers J; European Association for Cardiovascular Prevention and Rehabilitation; American Heart Association. EACPR/AHA Scientific Statement. Clinical recom-mendations for cardiopulmonary exercise testing data assessment in spe-cific patient populations. Circulation. 2012;126:2261–2274.
8. Arena R, Myers J, Abella J, Pinkstaff S, Brubaker P, Kitzman D, Peberdy MA, Bensimhon D, Chase P, Forman DE, Guazzi M. Defining the opti-mal prognostic window for cardiopulmonary exercise testing in patients with heart failure. Circ Heart Fail. 2010;3:405–411.
9. Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61:772–778.
10. Johansen KL, Kaysen GA, Dalrymple LS, Grimes BA, Glidden DV, Anand S, Chertow GM. Association of physical activity with survival among ambulatory patients on dialysis: the Comprehensive Dialysis Study. Clin J Am Soc Nephrol. 2013;8:248–253.
11. Waschki B, Kirsten A, Holz O, Müller KC, Meyer T, Watz H, Magnussen H. Physical activity is the strongest predictor of all-cause mortality in pa-tients with COPD: a prospective cohort study. Chest. 2011;140:331–342.
12. Walsh JT, Charlesworth A, Andrews R, Hawkins M, Cowley AJ. Relation of daily activity levels in patients with chronic heart failure to long-term prognosis. Am J Cardiol. 1997;79:1364–1369.
13. Jehn M, Schmidt-Trucksäss A, Schuster T, Weis M, Hanssen H, Halle M, Koehler F. Daily walking performance as an independent predictor of advanced heart failure: prediction of exercise capacity in chronic heart failure. Am Heart J. 2009;157:292–298.
14. Howell J, Strong BM, Weisenberg J, Kakade A, Gao Q, Cuddihy P, Delisle S, Kachnowski S, Maurer MS. Maximum daily 6 minutes of activity: an index of functional capacity derived from actigraphy and its application to older adults with heart failure. J Am Geriatr Soc. 2010;58:931–936.
15. Shoemaker MJ, Curtis A, Vangsnes E, Dickinson M, Paul R. Analysis of daily activity data from implanted cardiac defibrillators: the minimum clinically important difference and relationship to mortality/life expec-tancy. World J Cardiovasc Dis. 2012;2:129–135.
16. Conraads VM, Tavazzi L, Santini M, Oliva F, Gerritse B, Yu CM, Cowie MR. Sensitivity and positive predictive value of implantable intrathorac-ic impedance monitoring as a predictor of heart failure hospitalizations: the SENSE-HF trial. Eur Heart J. 2011;32:2266–2273.
17. van Veldhuisen DJ, Braunschweig F, Conraads V, Ford I, Cowie MR, Jondeau G, Kautzner J, Aguilera RM, Lunati M, Yu CM, Gerritse B, Borggrefe M; DOT-HF Investigators. Intrathoracic impedance monitor-ing, audible patient alerts, and outcome in patients with heart failure. Circulation. 2011;124:1719–1726.
18. Cowie MR, Conraads V, Tavazzi L, Yu CM; SENSE-HF Investigators. Rationale and design of a prospective trial to assess the sensitivity and positive predictive value of implantable intrathoracic impedance moni-toring in the prediction of heart failure hospitalizations: the SENSE-HF study. J Card Fail. 2009;15:394–400.
19. Braunschweig F, Ford I, Conraads V, Cowie MR, Jondeau G, Kautzner J, Lunati M, Munoz Aguilera R, Man Yu C, Marijianowski M, Borggrefe M, van Veldhuisen DJ; DOT-HF Steering Committee and Investigators. Can monitoring of intrathoracic impedance reduce morbidity and mor-tality in patients with chronic heart failure? Rationale and design of the Diagnostic Outcome Trial in Heart Failure (DOT-HF). Eur J Heart Fail. 2008;10:907–916.
20. Hlatky MA, Greenland P, Arnett DK, Ballantyne CM, Criqui MH, Elkind MS, Go AS, Harrell FE Jr, Hong Y, Howard BV, Howard VJ, Hsue PY, Kramer CM, McConnell JP, Normand SL, O’Donnell CJ, Smith SC Jr, Wilson PW; American Heart Association Expert Panel on Subclinical Atherosclerotic Diseases and Emerging Risk Factors and the Stroke Council. Criteria for evaluation of novel markers of cardiovascular risk:
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Conraads et al Physical Activity and Outcome in Heart Failure 287
a scientific statement from the American Heart Association. Circulation. 2009;119:2408–2416.
21. Pocock SJ, Wang D, Pfeffer MA, Yusuf S, McMurray JJ, Swedberg KB, Ostergren J, Michelson EL, Pieper KS, Granger CB. Predictors of mor-tality and morbidity in patients with chronic heart failure. Eur Heart J. 2006;27:65–75.
22. Harrell FE Jr. Regression Modeling Strategies. Springer: New York; 2001.
23. Aspenes ST, Nilsen TI, Skaug EA, Bertheussen GF, Ellingsen Ø, Vatten L, Wisløff U. Peak oxygen uptake and cardiovascular risk factors in 4631 healthy women and men. Med Sci Sports Exerc. 2011;43:1465–1473.
24. Myers J, Kaykha A, George S, Abella J, Zaheer N, Lear S, Yamazaki T, Froelicher V. Fitness versus physical activity patterns in predicting mortality in men. Am J Med. 2004;117:912–918.
25. Adamson PB, Smith AL, Abraham WT, Kleckner KJ, Stadler RW, Shih A, Rhodes MM; InSync III Model 8042 and Attain OTW Lead Model 4193 Clinical Trial Investigators. Continuous autonomic assessment in patients with symptomatic heart failure: prognostic value of heart rate variability measured by an implanted cardiac resynchronization device. Circulation. 2004;110:2389–2394.
26. Small RS, Wickemeyer W, Germany R, Hoppe B, Andrulli J, Brady PA, Labeau M, Koehler J, Sarkar S, Hettrick DA, Tang WH. Changes in in-trathoracic impedance are associated with subsequent risk of hospitaliza-tions for acute decompensated heart failure: clinical utility of implanted device monitoring without a patient alert. J Card Fail. 2009;15:475–481.
27. Whellan DJ, Ousdigian KT, Al-Khatib SM, Pu W, Sarkar S, Porter CB, Pavri BB, O’Connor CM. Combined heart failure device diagnostics identify patients at higher risk of subsequent heart failure hospitaliza-tions: results from partners hf (program to access and review trending information and evaluate correlation to symptoms in patients with heart failure) study. J Am Coll Cardiol. 2010;55:1803–1810.
28. Levy WC, Mozaffarian D, Linker DT, Sutradhar SC, Anker SD, Cropp AB, Anand I, Maggioni A, Burton P, Sullivan MD, Pitt B, Poole-Wilson PA, Mann DL, Packer M. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113:1424–1433.
29. Keteyian SJ, Leifer ES, Houston-Miller N, Kraus WE, Brawner CA, O’Connor CM, Whellan DJ, Cooper LS, Fleg JL, Kitzman DW, Cohen-Solal A, Blumenthal JA, Rendall DS, Piña IL; HF-ACTION Investigators. Relation between volume of exercise and clinical outcomes in patients with heart failure. J Am Coll Cardiol. 2012;60:1899–1905.
30. Witham MD, Argo IS, Johnston DW, Struthers AD, McMurdo ME. Predictors of exercise capacity and everyday activity in older heart fail-ure patients. Eur J Heart Fail. 2006;8:203–207.
31. De Feo S, Franceschini L, Brighetti G, Cicoira M, Zanolla L, Rossi A, Golia G, Zardini P. Ischemic etiology of heart failure identifies patients with more severely impaired exercise capacity. Int J Cardiol. 2005;104:292–297.
32. Forman DE, Clare R, Kitzman DW, Ellis SJ, Fleg JL, Chiara T, Fletcher G, Kraus WE; HF-ACTION Investigators. Relationship of age and exer-cise performance in patients with heart failure: the HF-ACTION study. Am Heart J. 2009;158(4 suppl):S6–S15.
33. Chung MK, Shemanski L, Sherman DG, Greene HL, Hogan DB, Kellen JC, Kim SG, Martin LW, Rosenberg Y, Wyse DG; AFFIRM Investigators.
Functional status in rate-versus rhythm-control strategies for atrial fi-brillation: results of the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) Functional Status Substudy. J Am Coll Cardiol. 2005;46:1891–1899.
34. Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation–Pharmacological Intervention in Atrial Fibrillation (PIAF): a randomised trial. Lancet. 2000;356:1789–1794.
35. Izawa KP, Watanabe S, Oka K, Osada N, Omiya K, Brubaker PH, Shimizu H. Diabetes mellitus may lower daily physical activity in heart failure patients. Int J Cardiol. 2013;168:4882–4883.
36. Scheuermann-Freestone M, Madsen PL, Manners D, Blamire AM, Buckingham RE, Styles P, Radda GK, Neubauer S, Clarke K. Abnormal cardiac and skeletal muscle energy metabolism in patients with type 2 diabetes. Circulation. 2003;107:3040–3046.
37. Crowther RG, Spinks WL, Leicht AS, Quigley F, Golledge J. Relationship between temporal-spatial gait parameters, gait kinematics, walking per-formance, exercise capacity, and physical activity level in peripheral ar-terial disease. J Vasc Surg. 2007;45:1172–1178.
38. Jones WS, Clare R, Ellis SJ, Mills JS, Fischman DL, Kraus WE, Whellan DJ, O’Connor CM, Patel MR. Effect of peripheral arterial disease on functional and clinical outcomes in patients with heart failure (from HF-ACTION). Am J Cardiol. 2011;108:380–384.
39. Lapu-Bula R, Robert A, Van Craeynest D, D’Hondt AM, Gerber BL, Pasquet A, Melin JA, De Kock M, Vanoverschelde JL. Contribution of exercise-induced mitral regurgitation to exercise stroke volume and exercise capacity in patients with left ventricular systolic dysfunction. Circulation. 2002;106:1342–1348.
40. Abdulla J, Abildstrom SZ, Christensen E, Kober L, Torp-Pedersen C. A meta-analysis of the effect of angiotensin-converting enzyme inhibi-tors on functional capacity in patients with symptomatic left ventricular systolic dysfunction. Eur J Heart Fail. 2004;6:927–935.
41. Guazzi M, Arena R. The impact of pharmacotherapy on the cardiopul-monary exercise test response in patients with heart failure: a mini re-view. Curr Vasc Pharmacol. 2009;7:557–569.
42. Guazzi M, Melzi G, Marenzi GC, Agostoni P. Angiotensin-converting enzyme inhibition facilitates alveolar-capillary gas transfer and improves ventilation-perfusion coupling in patients with left ventricular dysfunc-tion. Clin Pharmacol Ther. 1999;65:319–327.
43. Poelzl G, Frick M, Lackner B, Huegel H, Alber HF, Mair J, Herold M, Schwarzacher SP, Pachinger O, Weidinger F. Short-term improve-ment in submaximal exercise capacity by optimized therapy with ACE inhibitors and beta blockers in heart failure patients is associ-ated with restoration of peripheral endothelial function. Int J Cardiol. 2006;108:48–54.
44. Gulati SK, McKenzie J, Crossley G, Papp MA, Sims J, Andriulli J. Device measured physical activity: is it the new 6-minute hall walk? J Cardiac Failure. 2009;15:S119–S120.
45. Braunschweig F, Mortensen PT, Gras D, Reiser W, Lawo T, Mansour H, Sogaard P, Stegemann B, Bruns HJ, Linde C; InSync III Study Investigators. Monitoring of physical activity and heart rate variability in patients with chronic heart failure using cardiac resynchronization de-vices. Am J Cardiol. 2005;95:1104–1107.
CLInICAL PERSPECTIvEThis study shows that patient activity measured by implanted devices predicts death and hospitalization for worsening heart failure. It included 781 heart failure patients with implanted defibrillators (most with resynchronization therapy). The patient activity measured by device accelerometers was averaged over a 30-day period shortly after device implantation. The resulting early physical activity (PA) level was strongly predictive of later clinical events. Each 10 minutes per day of incre-mental activity was associated with 8% reduction of the risk of death (P<0.0001), 3% reduction of the risk of heart failure hospitalization (P=0.001), and 5% reduction of the risk of the composite event (P<0.0001). Similar results were observed after correction for known heart failure risk factors. Risk stratification based on device-measured early PA may contribute to efficient patient management. However, further research is needed to assess if device-measured activity can be used to monitor patient status, or whether and to what extent increasing activity levels by exercise programs or patient counseling will result in better outcomes.
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
VeldhuisenTavazzi, Martin Borggrefe, Michael R.S. Hill, Sandra Jacobs, Bart Gerritse and Dirk J. van
Viviane M. Conraads, Martijn A. Spruit, Frieder Braunschweig, Martin R. Cowie, LuigiHeart Failure
Physical Activity Measured With Implanted Devices Predicts Patient Outcome in Chronic
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2014 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation: Heart Failure
doi: 10.1161/CIRCHEARTFAILURE.113.0008832014;7:279-287; originally published online February 11, 2014;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/7/2/279World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2014/02/11/CIRCHEARTFAILURE.113.000883.DC1Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information isthe Editorial Office. Once the online version of the published article for which permission is being requested
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculation: Heart Failurein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 27, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
SUPPLEMENTAL MATERIAL
Physical activity, measured with implanted devices,
predicts patient outcome in Chronic Heart Failure.
Viviane M Conraads, MD1, Martijn A Spruit, PhD2,3, Frieder Braunschweig, MD4, Martin R
Cowie, MD5, Luigi Tavazzi, MD6, Martin Borggrefe, MD7, Michael RS Hill, PhD8, Sandra Jacobs,
PhD9, Bart Gerritse, PhD9, Dirk J van Veldhuisen, MD10
1Department of Cardiology, Antwerp University Hospital, Edegem, Belgium
University of Antwerp, Antwerp, Belgium
2Department of Research & Education, CIRO+, center of expertise for chronic organ failure,
Horn, The Netherlands
3 REVAL - Rehabilitation Research Center, BIOMED - Biomedical Research Institute, Faculty of
Medicine and Life Sciences, Hasselt University, Diepenbeek, Belgium
4Karolinska Institutet, Dept of Cardiology, Karolinska University Hospital, Stockholm, Sweden
5National Heart & Lung Institute, Imperial College, London, UK
6Maria Cecilia Hospital, GVM Care and Research, E.S. Health Science Foundation, Cotignola,
Italy
7Department of Cardiology, University Hospital Mannheim, Mannheim, Germany
8Medtronic Inc., Minneapolis, MN, USA
9Medtronic Bakken Research Center, Maastricht, The Netherlands
10Department of Cardiology, University Medical Center Groningen, University of Groningen,
Groningen, The Netherlands
Methods
The table below (eTable 1) provides additional details of the designs of SENSE-HF and DOT-
HF. Investigators may have influenced patient behavior based on physical activity records,
which were accessible after Phase I for SENSE-HF (unblinding after Phase I) and for patients in
the access arm of DOT-HF. We therefore investigated the interaction effect between access to
device diagnostic data and early physical activity. Both studies were approved by the local
ethics committees, and written informed consent was obtained from all patients. The authors
had full access to study data
To evaluate the possible confounding effect of a positive response to CRT, in terms of exercise
tolerance, as well as outcome, we compared patients implanted with an ICD only to those with
an implanted CRT-D device.
Influences of access to diagnostics and CRT were assessed from interaction terms.
Results:
The average early physical activity is 199 minutes per day, with a standard deviation of 106
min/day. Further descriptive statistics are: range: 3-579 min/day; and quartiles 120 and 259
min/day. eFigure 1 provides the frequency distribution.
Access to device diagnostic data for patients enrolled in DOT-HF did not influence the relation
between early activity and the primary endpoint (HR=0.96 in patients with, and HR=0.95 in
patients without access, interaction p=0.58). Patients with ICD and CRT-D were comparable
with respect to early activity (p=0.32) and incidence of primary endpoints (p=0.17). The
association between early activity and primary endpoints did also not differ significantly
(HR=0.92 in ICD patients and HR=0.96 in CRT-D patients, interaction p=0.15).
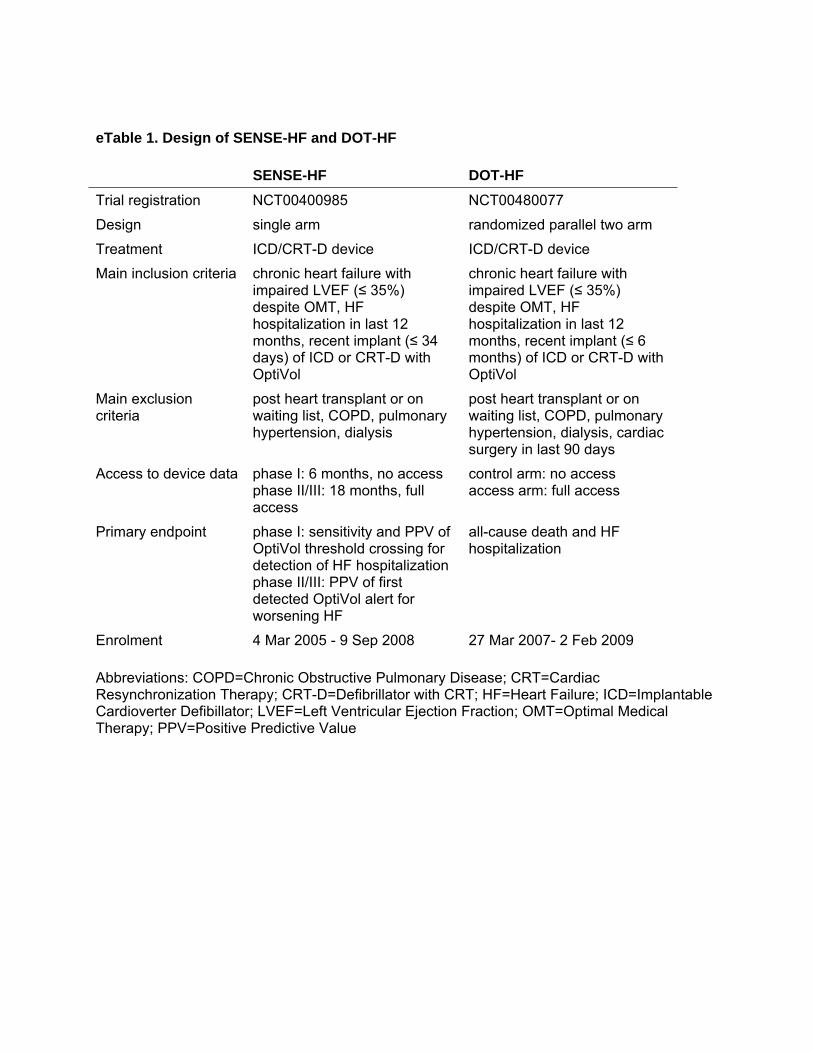
eTable 1. Design of SENSE-HF and DOT-HF
SENSE-HF DOT-HF
Trial registration NCT00400985 NCT00480077
Design single arm randomized parallel two arm
Treatment ICD/CRT-D device ICD/CRT-D device
Main inclusion criteria chronic heart failure with impaired LVEF (≤ 35%) despite OMT, HF hospitalization in last 12 months, recent implant (≤ 34 days) of ICD or CRT-D with OptiVol
chronic heart failure with impaired LVEF (≤ 35%) despite OMT, HF hospitalization in last 12 months, recent implant (≤ 6 months) of ICD or CRT-D with OptiVol
Main exclusion criteria
post heart transplant or on waiting list, COPD, pulmonary hypertension, dialysis
post heart transplant or on waiting list, COPD, pulmonary hypertension, dialysis, cardiac surgery in last 90 days
Access to device data phase I: 6 months, no access phase II/III: 18 months, full access
control arm: no access access arm: full access
Primary endpoint phase I: sensitivity and PPV of OptiVol threshold crossing for detection of HF hospitalization phase II/III: PPV of first detected OptiVol alert for worsening HF
all-cause death and HF hospitalization
Enrolment 4 Mar 2005 - 9 Sep 2008 27 Mar 2007- 2 Feb 2009
Abbreviations: COPD=Chronic Obstructive Pulmonary Disease; CRT=Cardiac Resynchronization Therapy; CRT-D=Defibrillator with CRT; HF=Heart Failure; ICD=Implantable Cardioverter Defibillator; LVEF=Left Ventricular Ejection Fraction; OMT=Optimal Medical Therapy; PPV=Positive Predictive Value
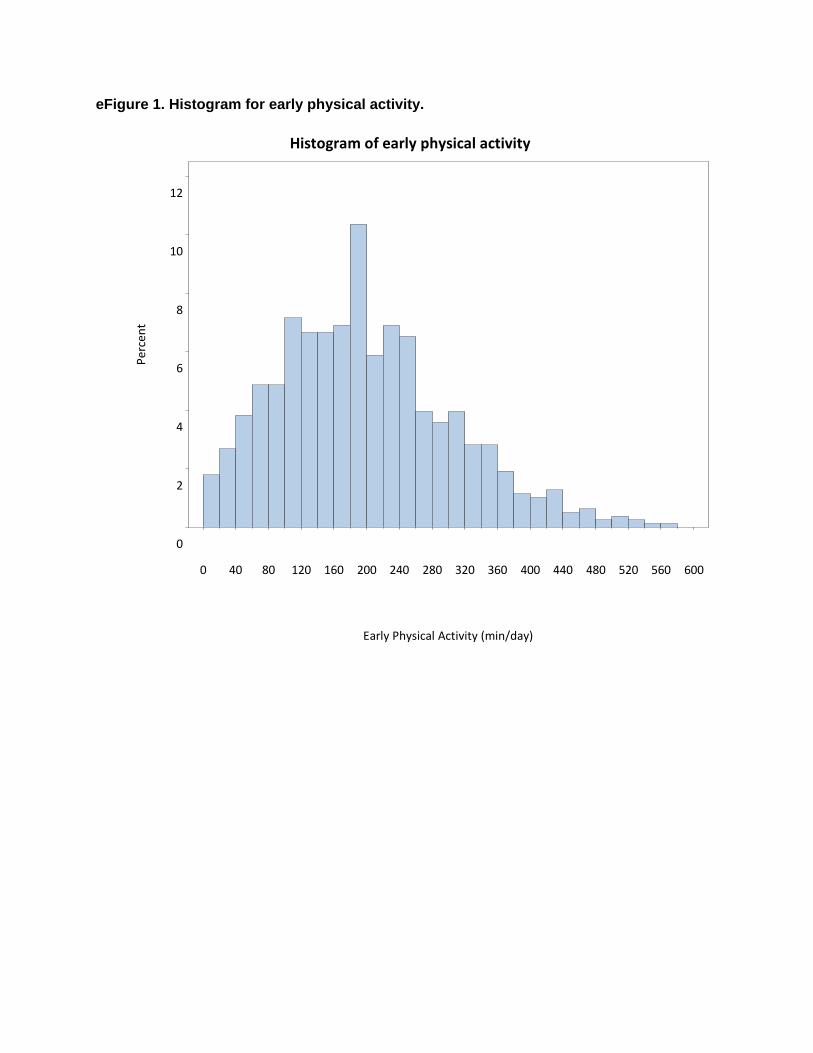
eFigure 1. Histogram for early physical activity.
Histogram of early physical activity
0 40 80 120 160 200 240 280 320 360 400 440 480 520 560 600
0
2
4
6
8
10
12
Percent
Early Physical Activity (min/day)





























