Embed Size (px)
Citation preview

Oral Pathology Exam I Review Slides

Mucocutaneous Disorders

Items covered:• Ectodermal dysplasia• Pachyonychia congenita• White sponge nevus• Hereditary benign intraepithelial dyskeratosis• Dyskeratosis congenita• Xeroderma pigmentosum• Fanconi anemia• Darier Disease• Epidermolysis Bullosa• Lichen Planus
– Classic reticular lichen planus– Atrophic lichen planus– Erosive lichen planus– Plaquelike lichen planus
• Erythema Multiforme• Benign mucous membrane pemphigoid• Pemphigus vulgaris• Paraneoplastic pemphigus• Bullus pemphigoid• Lupus Erythematosus• Scleroderma• CREST syndrome• Graft vs. Host Disease

X-linked recessive disorder which affects the skin and oral adnexal structures, no sweat or sebaceous glands, hypoplastic or no salivary glands (causes xerostomia and URT infections) sparse blonde brittle hair, few teeth which are mostly peg shaped, depressed midface, frontal bossing, protuberant lips, widely spaced eyes
Ectodermal Dysplasia

Autosomal dominant disorder which keratin genes are mutated, resulting in thick abnormal keratin under nails, palmar and plantar hyperkeratosis, diffuse white oral lesions primarily on dorsal and lateral tongue and buccal mucosa, hyperparakeratosis and acanthosis with perinuclear potential, no malignant potential
Panchyonychia Congenita

Autosomal dominant mutation in keratin genes producing thick white plaques throughout the oral mucosa, particuarlly bilaterally on the buccal mucosa, hyperkeratosis and acanthosis, does not affect skin, no malignant potentialHistologic: “Fried egg cells”-clear keratinocytes with pink condensed cytoplasm around nucleus
White Sponge Nevus

Autosomal dominant disorder in triracial (Native Americans, African Americans, Caucasians) isolate from NC, causing thick white lesions like white sponge nevus, conjunctival gelatinous plaques each spring which may cause temporary (occasionally permanent) blindness, but eventually regresses, hyperparakeratosis and acanthosis with dyskeratosis, no malignant potential
Hereditary Benign Intraepithelial Dyskeratosis
(Witkop-Von Sallmann Syndrome)Medium-power photomicrograph exhibiting hyperparakeratosis, acanthosis and dyskeratosis. Inset shows dyskeratotic cells at higher magnification.

X-linked recessive disorder causing impaired telomerase, resulting in cells to live longer than normal. Skin pigment and nail changes, pancytopenia (marrow failure) shortens lifespan to about age 30, widespread red and white oral lesions that transform into SCC at early age.
Dyskeratosis Congenita

Autosomal recessive disorder of chromosomal repair where epithelium cannot repair UV damage, widespread skin atrophy and blotchy pigment/depigmentation, cancer of lips and anterior tongue, multiple sun induced cancers (SCC, BCC, melanoma)
Xeroderma Pigmentosum

Autosomal recessive, disorder of chromosomal repair independent of UV exposure resulting in aplastic anemia (dysfunctional marrow), leukemia, short in stature, small mouth/lips, widespread oral lesions that become SCC at early age, disorders of thumb (missing thumb, may have 2 thumbs, etc.) and radius
Fanconi Anemia
COULDN’TFIND
A PICTURE

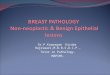
Autosomal dominant disorder which results in defective cohesion of keratinized cells, multiple itchy, smelly red papules all over the trunk, lesions occur on the palate, resembling papillary hyperplasia
Darier Disease (Keratosis
follicularis)Low-power photomicrographshowing a thick keratin plug,intraepithelial clefting, and elongated rete ridges.
The oral mucosa may show multiple white papules.
Erythematous cutaneouspapules on the chest.

Group of 21 genetic disorders characterized by epithelial attachment disorders of keratin, desmosomes or collagen resulting in skin and mucosal bullae, consists of simplex, junctional and recessive dystrophic type (causes bullae after chewing hard foods, mouth scars and becomes susceptible to SCC.

Group of 21 genetic disorders characterized by epithelial attachment disorders of keratin, desmosomes or collagen resulting in skin and mucosal bullae, consists of simplex, junctional and recessive dystrophic type (causes bullae after chewing hard foods, mouth scars and becomes susceptible to SCC.
Epidermolysis Bullosa
Complete separation of the epithelium from the connective tissue is seen in this photomicrographof a tissue section obtained from a patient affected by a junctional form of this disease

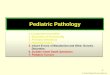
Type IV cytotoxic reaction in which T8+ lymphocytes attack basal cells (become antigenic for unknown reasons) in skin, mouth, genital region, skin lesions consist pruritic, scaly, pink, violaceous or pigmented rhomboid plaques on flexor surfaces of wrists and ankles, Cris-crossed by white Wickham striae, lesions are chronic and appear and disappear, flat shiny papules. Can appear on any oral mucosal surface with mixed manifestations and may be localized or generalized. Frequently infected by candida.Common sites: bilateral buccal mucosa (classic location), lateral tongue, labial mucosa, gingivaClassic features: flexor surfaces of extremities, especially wrists and ankles, scaly papules and flat topped plaques, pink, violaceous or brown in blacks
Lichen Planus
This low-power photomicrograph of an oral lesion shows hyperkeratosis, saw-toothed rete ridges,and a bandlike infiltrate of lymphocytes immediately subjacent to the epithelium.
(Left) High-power photomicrograph of normal epithelium showing an intact basal cell layer and no inflammation. (Right) High-power photomicrograph showing degeneration of the basal epithelial layer and an intense lymphocytic infiltrate in the superficial lamina propria.

Lichen Planus demonstrating classic Wickham striae across buccal mucosa bilaterally, is completely asymptomatic
Classic Reticular Lichen Planus

White striae on a background of red peeling atrophic mucosa, typical on gingiva as a dequamative gingivitis, painful burning sensation, hurts to brush teeth which results in poor oral hygiene which increases pain
Atrophic Lichen Planus
COULDN’TFIND
A PICTURE

Matured atrophic lichen planus, same symptoms as atrophic lichen planus but with peeling or well demarcated serpinginous (slowly spreading, especially healing over one portion while continuing to advance in another) ulcers.
Erosive Lichen Planus

Flat white patches with fissures, mostly seen on dorsal tongue, loss of papillae on dorsal tongue, white, flat plaquelike surfaces with fissures
Plaquelike Lichen Planus
COULDN’TFIND
A PICTURE

Captions for images of lichen planus:
Reticular lesions of the lower lipvermilion.
(Left) Middle-aged woman with mild reticular lichen planus of the left buccal mucosa. (Right) Same patient 2 weeks later. showing exacerbation of the lesions. Such waxing and waning is characteristic of lichen planus.

Captions for images of lichen planus:
With involvement of the dorsal tongue by reticular lichen planus, the characteristic interlacing striae seen in the buccal mucosal lesions are usually not present. Instead, smooth white plaques are typically observed replacing the normal papillary surface of the tongue.
(Left) Middle-aged woman with mild reticular lichen planus of the left buccal mucosa. (Right) Same patient 2 weeks later, showing exacerbation of the lesions. Such waxing and waning is characteristic of lichen planus.

Captions for images of lichen planus:
Ulceration of the buccal mucosa shows peripheral radiating keratotic striae. characteristic of oral erosive lichen planus.
(Left) The dorsal surface of the tongue shows extensive ulceration caused by erosive lichen planus. Note the fine white streaks at the periphery of the ulcerations. (Left) Same patient after systemic corticosteroid therapy. Much of the mucosa has reepithelialized, with only focal ulcerations remaining.

Captions for images of lichen planus:
Erosive lichen planus often appears as a desquamative gingivitis, producing gingival erythema and tenderness.

Captions for images of lichen planus:
(Top)This patient was diagnosed with erosive lichen planus affecting the buccal mucosa and was treated with topical corticosteroids.
(Middle)Same patient 2 weeks later. The creamy-white plaques of pseudomembranous candidiasis have developed as a result of the corticosteroid therapy.
(Bottom) Same patient after antifungal therapy. At this point, he was asymptomatic.

Acute type IV hypersensitivity whereby T8+ lymphocytes attack epithelium. Triggered by various stimuli including herpes outbreak, URTI (particularly mycoplasma infection), and medications (particularly antibiotics), target (bulls-eye) lesions with a central focus, palmar and plantar target lesions, blood crusted lips, conjunctival lesions (redness of conjunctiva, pus), confluent oral slough, gingiva is the only tissue that is spared

Acute type IV hypersensitivity whereby T8+ lymphocytes attack epithelium. Triggered by various stimuli including herpes outbreak, URTI (particularly mycoplasma infection), and medications (particularly antibiotics), target (bulls-eye) lesions with a central focus, palmar and plantar target lesions, blood crusted lips, conjunctival lesions (redness of conjunctiva, pus), confluent oral slough, gingiva is the only tissue that is spared
Erythema Multiforme
This medium powerphotomicrograph shows inflammation and intraepithelial vesicleformation in the basilar portion of the epithelium. Numerousnecrotic eosinophilic keratlnocytes are present in the blister area.
This medium powerphotomicrograph shows perivascular inflammatory infiltrate.

Additional info on Erythema Multiforme:
With erythema multiforme major (Stevens-Johnson syndrome), other mucosal surfaces may show involvement, such as the severe conjunctivitisdepicted in this photograph.
Toxic epidermal necrolysis (Lyell disease). This severe form of erythema multiforme exhibits diffuse bullous skin lesions.

Autoimmune disease of mucosa/skin in which immunoglobulins are made against the basement membrane, causing subbasilar separation and resulting in tense bullae and sloughing erosions. Affects women over age 50, blisters form between epithelium and CT, lack of inflammatory cells. Will have a positive Nikolsky sign (rub a region next to blister and epithelium peels off), lacks white striaeHistologic: clean sub-epithelial separation between the basal layer and connective tissue, in immunofluoroescence, linear band of IgG and C3 (apple green solid line) along the basement membrane zone
Benign Mucous Membrane Pemphigoid (Cicatricial or Scarring Pemphigoid)
Medium-power photomicrographof perilesional tissue shows characteristic subepithelial clefting.
Direct immunofluorescencestudies show a deposition of immunoreactants at the basement membrane zone of the epithelium.

Type 2 autoimmune disease whereby antibody is produced to intercellular bridges (Desmoglen 1 in stratum spinosum, Desmoglen 3 in basilar layer), making epithelial cells detach and fall apart. Positive Nikolsky sign and Tzanck test (blister fluid from lesion would show all detached epithelial cells floating around) Begins in the oral cavity in 50% of cases, fatal due to electrolyte loss.
Histologic: Suprabasilar vesicle with acantholytic cells, basal cells remain attached to connective tissue, acantholytic cells floating in fluid of blister, no lymphocytic infiltrates, immunostain shows IgG surrounding each epithelial cell, stratum

Type 2 autoimmune disease whereby antibody is produced to intercellular bridges (Desmoglen 1 in stratum spinosum, Desmoglen 3 in basilar layer), making epithelial cells detach and fall apart. Positive Nikolsky sign and Tzanck test (blister fluid from lesion would show all detached epithelial cells floating around) Begins in the oral cavity in 50% of cases, fatal due to electrolyte loss.
Histologic: Suprabasilar vesicle with acantholytic cells, basal cells remain attached to connective tissue, acantholytic cells floating in fluid of blister, no lymphocytic infiltrates, immunostain shows IgG surrounding each epithelial cell, stratum
Pemphigus Vulgaris
High-power photomicrographshowing rounded. acantholytic epithelial cells sitting within the intraepithelial cleft .
Note the intraepithelial cleft located just above the basal cell layer.

Severe form of acute onset pemphigus resembling Stevens-Johnson syndrome, due to an internal malignancy, most often lymphoma or leukemia, histology and immunofluorescence not specific or diagnostic in separating from pemphigus vulgaris, blood must be drawn to establish the diagnosis

Severe form of acute onset pemphigus resembling Stevens-Johnson syndrome, due to an internal malignancy, most often lymphoma or leukemia, histology and immunofluorescence not specific or diagnostic in separating from pemphigus vulgaris, blood must be drawn to establish the diagnosis
Paraneoplastic Pemphigus
This medium-power photomicrograph shows both intraepithelial and subepithelial cleftlng.

Most common autoimmune blistering disease, histologically similar to BMMP, occasionally find lesions in the oral cavity
Bullous Pemphigoid
Cutaneous vesiculobullouslesions of the heel. The bullae eventually rupture, leaving hemorrhagiccrusted areas.
These oral lesions appearAs large, shallow ulcerations involving the soft palate.

Autoimmune disease of type III hypersensitivity (immune complexes trigger tissue destruction), affects primarily women, affects skin, oral mucosa, blood vessels, kidneys, heart (DLE affects skin and mucosa only), butterfly rash is classic sign, oral lesions are lichenoid (chronic red and white atrophic ulcerating painful lesions usually on palate, vermilion and buccal mucosa, and may have striae), skin lesions usually present, oral lesions have a tendency to transform to SCC
Histologic: resembles lichen planus but with lymphocyte perivasculitis and salivary gland infiltrates, immunofluorescence shows granular bands of immunoglobulins or C3 at the basement membrane (lupus band test), basal cells are damaged (liquefaction necrosis), hyperkeratosis, edema

Autoimmune disease of type III hypersensitivity (immune complexes trigger tissue destruction), affects primarily women, affects skin, oral mucosa, blood vessels, kidneys, heart (DLE affects skin and mucosa only), butterfly rash is classic sign, oral lesions are lichenoid (chronic red and white atrophic ulcerating painful lesions usually on palate, vermilion and buccal mucosa, and may have striae), skin lesions usually present, oral lesions have a tendency to transform to SCC
Histologic: resembles lichen planus but with lymphocyte perivasculitis and salivary gland infiltrates, immunofluorescence shows granular bands of immunoglobulins or C3 at the basement membrane (lupus band test), basal cells are damaged (liquefaction necrosis), hyperkeratosis, edema
Lupus Erythematosus
Low-power photomicrographshowing hyperparakeratosis with interface mucositisand perivascular inflammation.
High-power photomicrographof the interface mucositis.

Autoimmune disease in which there is a deposition of collagen throughout the body, affects adult women, skin, esophagus, vessels, heart, lungs and kidneys most affected with fibrosis, mask (mouse) like face, sclerodactyly (claw hands), small lips/mouth, difficulty opening, no wrinkles on face, Raynaud phenomenon, vasculitis, stricture and dysphagia of esophagus, gingival recession Radiographic: widening of PDL around ALL teeth, resorption of posterior ramus, condyle and coronoid process are a classic sign

Autoimmune disease in which there is a deposition of collagen throughout the body, affects adult women, skin, esophagus, vessels, heart, lungs and kidneys most affected with fibrosis, mask (mouse) like face, sclerodactyly (claw hands), small lips/mouth, difficulty opening, no wrinkles on face, Raynaud phenomenon, vasculitis, stricture and dysphagia of esophagus, gingival recession Radiographic: widening of PDL around ALL teeth, resorption of posterior ramus, condyle and coronoid process are a classic sign
Diffuse widening of the periodontalligament space is often identified on evaluation of periapical radiographs.
Panoramic radiographic evaluation may show a characteristicresorption of the ramus, coronoid process, or condyle.

Autoimmune disease in which there is a deposition of collagen throughout the body, affects adult women, skin, esophagus, vessels, heart, lungs and kidneys most affected with fibrosis, mask (mouse) like face, sclerodactyly (claw hands), small lips/mouth, difficulty opening, no wrinkles on face, Raynaud phenomenon, vasculitis, stricture and dysphagia of esophagus, gingival recession Radiographic: widening of PDL around ALL teeth, resorption of posterior ramus, condyle and coronoid process are a classic sign
Scleroderma Medium-power photomicrograph of an oral biopsy specimen. Diffuse deposition of collagen is apparent throughout the lamina propria.

Calcinosis cutis (can feel calcifications in skin), Raynaud phenomenon, Esophageal dysfunction, Sclerodactyly, Telectangic mats, doesn’t involve systemic organs
CREST syndrome

Graft T-cells react against host HLA antigens in bone marrow transplants, causing skin and oral lesions that resemble lichen planus, lupus or scleroderma, salivary involvement causes xerostomia, histologically resembles lichen planus, differential diagnosis is made by asking the patient if they recently had a bone marrow transplant
Graft vs. host disease