Embed Size (px)
Citation preview

Pediatric PathologyPediatric Pathology
Dr. Krishna Tadepalli, MD, www.mletips.com
1

5. Inborn Errors of Metabolism and Other Genetic Disorders
5. Inborn Errors of Metabolism and Other Genetic Disorders
2
Dr. Krishna Tadepalli, MD, www.mletips.com

• Early diagnosis appropriate dietary regimens prevent clinical illness (PKU and Galactosemia)
• Phenylketonuria (PKU)
• Autosomal recessive
• Mutations of the gene encoding phenylalanine hydroxylase (convert phenylalanine into tyrosine in liver) hyperphenylalaninemia PKU
• PKU variants = benign hyperphenylalaninemia pts, have positive screening tests but not develop PKU (serum phenylalanine levels differentiate)– defects in BH4 (cofactor )recycling
– neurologic disturbances cannot be treated by dietary control of phenylalanine
• Clinical– Musty or mousy odor (due to phenylacetic acid in sweat)
– Brain damage (due to excess phenylalanine or its metabolites
– Normal at birth but in within a few weeks impaired brain growth
– By 6 months severe mental retardation
– Other features decreased pigmentation of hair and skin, and eczema can’t, walk & talk ,Seizures
• Maternal PKU = normal female PKU patients with hyperphenylalaninemia
• Children born to this mothers =mentally retarded and microcephalic (due to teratogenic effects)
3
Dr. Krishna Tadepalli, MD, www.mletips.com

PKUPKU
4
Dr. Krishna Tadepalli, MD, www.mletips.com

• Galactosemia
• Autosomal recessive
• disorder of galactose metabolism
• Lactose of milk split into glucose and galactose in the intestinal microvilli by lactase
• Galactose is converted to glucose
• Two variants – Common variant = total lack of galactose-1-phosphate uridyl transferase (also
known as GALT)
• galactose-1-phosphate accumulates in liver, spleen, lens of the eye, kidneys, heart muscle, cerebral cortex, and erythrocytes
– converts into galactitol &galactonate (toxic)
– Rare variant =deficiency of galactokinase (Milder with mental retardation)
• Clinical – Liver= Hepatomegaly ( due to fatty change) and Cirrhosis (Fibrosis)
– Eye lens= Cataract (Galactitol absorbs more water)
– CNS= non-specific changes (Neuronal loss +gliosis+edema mainly at Dentate and oilvary nuclei)
• Clinical course & Progression5
Dr. Krishna Tadepalli, MD, www.mletips.com

• Galactosemia
• Clinical course & Progression• Immediately after birth = failure to thrive• First few days = vomitings &diarrhea, Hemolysis & Coagulopathy• First few weeks = Jaundice, Hepatomegaly & Cataracts• Months (6-12) = MR, Aminoaciduria and fulminant E. Coli sepsis, • Diagnosis• Urine positive for reducing sugars – gives doubt• Deficiency of enzyme inWBC or RBC = confirmation• Antenatal = GALT in Aminotic fluid or cultured cells• Genetic polymorphisms
– In Non- Hispanics = glutamine to arginine at 188– In Africans = serine to leucine at 135
• Prevention• Avoid galactose in diet for at least for first two years of life
• Can’t avoid speech disorders, Gonadal (ovarian) failure and ataxia (despite dietary restriction)
6
Dr. Krishna Tadepalli, MD, www.mletips.com

GalactosemiaGalactosemia
7
Dr. Krishna Tadepalli, MD, www.mletips.com

GalactosemiaGalactosemia
8
Dr. Krishna Tadepalli, MD, www.mletips.com

• Cystic Fibrosis (MUCOVISCIDOSIS)
• Autosomal recessive
• MC lethal genetic disease that affects Caucasian populations (1 in 2500 live births with carrier frequency 1 in 20 among Caucasians )
• Disorder of ion transport in epithelial cells
• Secretion in exocrine glands and epithelial lining of the respiratory, gastrointestinal, and reproductive tracts
• Abnormally viscous secretions obstruct organ passages
• Even heterozygote carriers have respiratory and pancreatic diseases
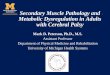
• The Cystic Fibrosis-Associated Gene: Normal Structure and Function • CFTR gene on chromosome 7q31.2
• Normal CFTR decreases ENaC activity (in cystic fibrosis, ENaC activity increases with exception of sweat ducts to this rule )
• CFTR can regulate multiple ion channels and cellular processes
• interaction of CFTR with the ENaC most pathophysiologic relevance
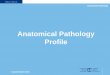
• CFTR functions are tissue-specific & impact of CFTR mutation also tissue-specific (sweat hypertonic, respiratory and intestinal secretions low volume but isotonic)
• CFTR mediates transport of bicarbonate ions (some CFTR mutant variants Cl ¯ transport is normal but HCo3 ¯ transport is abnormal epithelia secrete acidic fluids ↑ mucin precipitation and plugging of ducts, ↑ bacterial binding to mucin plugs
9
Dr. Krishna Tadepalli, MD, www.mletips.com

• Cystic Fibrosis (MUCOVISCIDOSIS) contd…
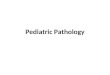
• Classic cystic fibrosis phenotype Severe mutations (pancreatic insufficiency, sinopulmonary infections, and gastrointestinal symptoms)
• less severe phenotype "mild“ mutations
• Genotype -phenotype correlation is most consistent for pancreatic disease but less consistent in pulmonary disease
• Non-classic or atypical cystic fibrosis have CFTR mutations but do not other features of cystic fibrosis (examples =idiopathic chronic pancreatitis, late-onset chronic pulmonary disease, idiopathic bronchiectasis, and obstructive azoospermia )
• Genetic and Environmental Modifiers = decide the phenotypic features ( mainly pulmonary )
10
Dr. Krishna Tadepalli, MD, www.mletips.com

• Cystic Fibrosis (MUCOVISCIDOSIS) contd…• Morphology
• Pancreatic abnormalities (seen in 85% to 90% of patients )
• Varies from only accumulations of mucus and duct dilation to severe duct obstruction (by mucus plugs)atrophy and progressive fibrosis of exocrine pancreas
• Liver = Bile canaliculi obstruction ductular proliferation and portal inflammation and later steatosis & biliary cirrhosis
• salivary glands = similar to pancreas
• Pulmonary changes =most serious complications
– chronic bronchitis and bronchiectasis
– Staphylococcus aureus, Hemophilus influenzae, and Pseudomonas aeruginosa are most common organisms
– Burkholderia cenocepacia (group of pseudomonads) =most common of all
• Azoospermia and infertility =in 95% of the males associated with congenital bilateral absence of the vas deferens
• Diagnosis
• Most cases =persistently elevated sweat electrolyte
• "gold standard" =Sequencing the CFTR gene
• Management = potent antimicrobial therapies +pancreatic enzyme replacement +bilateral lung transplantation
• Gene therapy =undergoing early-phase clinical trials
11
Dr. Krishna Tadepalli, MD, www.mletips.com

Normal CFTRNormal CFTR
12
Dr. Krishna Tadepalli, MD, www.mletips.com

Cystic FibrosisCystic Fibrosis
13
Dr. Krishna Tadepalli, MD, www.mletips.com

Cystic Fibrosis – Disease SpectrumCystic Fibrosis – Disease Spectrum
14
Dr. Krishna Tadepalli, MD, www.mletips.com

Cystic Fibrosis – PancreasCystic Fibrosis – Pancreas
15
Dr. Krishna Tadepalli, MD, www.mletips.com

Cystic Fibrosis – LungsCystic Fibrosis – Lungs
16
Dr. Krishna Tadepalli, MD, www.mletips.com

17