Embed Size (px)
DESCRIPTION
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and offering a wide range of dental certified courses in different formats. Indian dental academy provides dental crown & Bridge,rotary endodontics,fixed orthodontics, Dental implants courses.for details pls visit www.indiandentalacademy.com ,or call 0091-9248678078
Citation preview

INDIAN DENTAL ACADEMY
Leader in continuing dental education www.indiandentalacademy.com
www.indiandentalacademy.comwww.indiandentalacademy.com

Optimum Force Magnitude for Optimum Force Magnitude for Orthodontic Tooth MovementOrthodontic Tooth Movement
- Review of Literature- Review of Literature
Yijin Ren, Jaap C. Maltha.Yijin Ren, Jaap C. Maltha.
The Angle OrthodontistThe Angle Orthodontist
2003; 73, 86-922003; 73, 86-92
www.indiandentalacademy.comwww.indiandentalacademy.com

An optimal force system is important An optimal force system is important for adequate biological response in for adequate biological response in the periodontal ligament and the periodontal ligament and magnitude of this force is related to magnitude of this force is related to the surface area of the root.the surface area of the root.
www.indiandentalacademy.com

Schwarz (1932)Schwarz (1932) proposed the first proposed the first classic concept of the optimal force. classic concept of the optimal force.
He defined optimal continuous force He defined optimal continuous force as ‘‘the force leading to a change in as ‘‘the force leading to a change in tissue pressure that approximated the tissue pressure that approximated the capillary blood pressure, thus capillary blood pressure, thus preventing their occlusion in the preventing their occlusion in the compressed periodontal ligament.’’compressed periodontal ligament.’’
www.indiandentalacademy.com

This pressure in humans is about 15-20 This pressure in humans is about 15-20 mm of Hg; and this comes to be 20 - mm of Hg; and this comes to be 20 - 26 g for 1 sq.cm surface.26 g for 1 sq.cm surface.
Based on this theory, Based on this theory, Jepsen (1963)Jepsen (1963) calculated optimal force for premolar calculated optimal force for premolar with mean root surface area of 2.34 with mean root surface area of 2.34 cmcm2,2, which comes to be 54g. which comes to be 54g.
www.indiandentalacademy.com

According to Schwarz, forces well According to Schwarz, forces well below the optimal level cause no below the optimal level cause no reaction in the periodontal ligament.reaction in the periodontal ligament.
Forces exceeding the optimal level Forces exceeding the optimal level would lead to areas of tissue necrosis, would lead to areas of tissue necrosis, preventing frontal bone resorption. preventing frontal bone resorption.
www.indiandentalacademy.com

Schwarz’s definition was slightly Schwarz’s definition was slightly modified by modified by Oppenheim (1944)Oppenheim (1944) who who advocated the use of the lightest force advocated the use of the lightest force capable of bringing about tooth capable of bringing about tooth movement. movement.
www.indiandentalacademy.com

Reitan (1957)Reitan (1957) based on his based on his histological findings where he histological findings where he demonstrated cell-free compressed demonstrated cell-free compressed areas within the pressure site, strongly areas within the pressure site, strongly advocated use of very light forces to advocated use of very light forces to maintain health of investing tissues.maintain health of investing tissues.
www.indiandentalacademy.com

Storey and smith (1952)Storey and smith (1952) proposed their proposed their theory of “optimal force”.theory of “optimal force”.
Acc to this theory, there is optimal Acc to this theory, there is optimal range of force that produce maximum range of force that produce maximum tooth movement. When force is tooth movement. When force is increased above this range, tooth increased above this range, tooth movement slows down. movement slows down.
www.indiandentalacademy.com

This theory of ‘optimal force’ was critically This theory of ‘optimal force’ was critically reviewed by reviewed by Boester and Johnston (1974).Boester and Johnston (1974).
They found in their study of 10 individuals They found in their study of 10 individuals that space closure after premolar extraction that space closure after premolar extraction was about same after application of 140, was about same after application of 140, 225 or 310g of force during 10 weeks.225 or 310g of force during 10 weeks.
But space closure was significantly less when But space closure was significantly less when
about 55g force was used. about 55g force was used.
www.indiandentalacademy.com

Hixon et al (1969)Hixon et al (1969) reported a more reported a more linear relationship between force linear relationship between force magnitude and tooth movement, at magnitude and tooth movement, at least up to 300g of force.least up to 300g of force.
www.indiandentalacademy.com

The The current concept of optimal forcecurrent concept of optimal force is based is based on the hypothesis that a force of a certain on the hypothesis that a force of a certain magnitude and temporal characteristics magnitude and temporal characteristics (continuous vs intermittent, constant vs (continuous vs intermittent, constant vs declining,etc ) would be capable of declining,etc ) would be capable of producing a maximum rate of tooth producing a maximum rate of tooth movement without tissue damage and with movement without tissue damage and with maximum patient comfort. maximum patient comfort.
The optimal force for tooth movement may The optimal force for tooth movement may differ for each individual.differ for each individual.
www.indiandentalacademy.com

Relationship between stress/strain and Relationship between stress/strain and amount of tooth movement amount of tooth movement
Force magnitude is a popular concept Force magnitude is a popular concept in orthodontics. However, it is an in orthodontics. However, it is an incomplete way to describe the forces incomplete way to describe the forces delivered by an orthodontic appliance. delivered by an orthodontic appliance.
www.indiandentalacademy.com

The true mechanical parameter in The true mechanical parameter in tooth movement is not the magnitude tooth movement is not the magnitude of the force per se, but rather the of the force per se, but rather the magnitude of the stress generated by magnitude of the stress generated by the appliance in the surrounding the appliance in the surrounding periodontium. periodontium.
www.indiandentalacademy.com

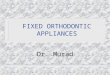
Compressive stress patterns in the periodontal Compressive stress patterns in the periodontal ligament under different force systems. A, Pure force ligament under different force systems. A, Pure force applied at the bracket. B, Force and moment applied applied at the bracket. B, Force and moment applied at the bracketat the bracket
Tipping
Translation
www.indiandentalacademy.com

Clinical interest in characterizing the Clinical interest in characterizing the nature of the relation between the nature of the relation between the magnitudes of applied force (i.e magnitudes of applied force (i.e stress/strain) and the rate of stress/strain) and the rate of orthodontic tooth movement orthodontic tooth movement determining the extent of anchorage determining the extent of anchorage loss began in the 1950s.loss began in the 1950s.
www.indiandentalacademy.com

The assumption was that differential The assumption was that differential movement of teeth, at first proposed movement of teeth, at first proposed by by Begg (1957),Begg (1957), could be generally could be generally achieved with light force without any achieved with light force without any unwanted tooth movement.unwanted tooth movement.
www.indiandentalacademy.com

In the last two decades, one of the In the last two decades, one of the central questions raised about the central questions raised about the exact relationship of stress/strain exact relationship of stress/strain pattern and biologic activity and thus pattern and biologic activity and thus rate of tooth movement, which may rate of tooth movement, which may affect :affect :
- anchorage planning- anchorage planning
- efficiency of appliance in tooth - efficiency of appliance in tooth movementmovement
www.indiandentalacademy.com

This question led to the classic study This question led to the classic study by by Quinn and Yoshikawa (1985)Quinn and Yoshikawa (1985) in in which they proposed four possible which they proposed four possible models for the relation between force models for the relation between force magnitude and the rate of orthodontic magnitude and the rate of orthodontic tooth movement.tooth movement.
www.indiandentalacademy.com

HYPOTHESES OF THE STRESS-HYPOTHESES OF THE STRESS-MOVEMENT RELATIONSHIP MOVEMENT RELATIONSHIP (Robert S. Quinn, and D. Ken (Robert S. Quinn, and D. Ken Yoshikawa, Yoshikawa, jco jco 1985)1985)
The effect of periodontal stress The effect of periodontal stress magnitude on the rate of tooth magnitude on the rate of tooth movement is an important issue in plans movement is an important issue in plans to control the displacement of posterior to control the displacement of posterior teeth. teeth.
www.indiandentalacademy.com

Clinicians base their strategies for Clinicians base their strategies for controlling anchorage on their controlling anchorage on their assumptions about tooth movement. assumptions about tooth movement.
Quinn and Yoshikawa proposed four Quinn and Yoshikawa proposed four possible relationships between stress possible relationships between stress magnitude and rate of movement.magnitude and rate of movement.
www.indiandentalacademy.com

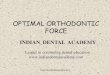
Possible hypotheses of the relationship Possible hypotheses of the relationship between stress magnitude and the rate of between stress magnitude and the rate of
tooth movement tooth movement
www.indiandentalacademy.com

Hypothesis 1Hypothesis 1 shows a constant shows a constant relationship between rate of relationship between rate of movement and stress. movement and stress.
The rate of tooth movement does not The rate of tooth movement does not increase as the stress level is increase as the stress level is increased. increased.
www.indiandentalacademy.com

Acc to this hypothesis, anchorage Acc to this hypothesis, anchorage control does not obey concept of control does not obey concept of ‘differential anchorage’. ‘differential anchorage’.
Hence when elastics are used for Hence when elastics are used for retraction, only one size is necessary. retraction, only one size is necessary.
Loop designs are not critical and can Loop designs are not critical and can be simple and uncomplicated by be simple and uncomplicated by helices. helices.
www.indiandentalacademy.com

Hypothesis 2Hypothesis 2 shows a linear increase in the shows a linear increase in the rate of tooth movement as the stress rate of tooth movement as the stress increases. increases.
In this system, intra-arch anchorage could In this system, intra-arch anchorage could be manipulated by adding teeth (second be manipulated by adding teeth (second molars) to the anchorage unit or moving the molars) to the anchorage unit or moving the extraction site for example, second versus extraction site for example, second versus first premolars. first premolars.
www.indiandentalacademy.com

This would distribute the stress over a This would distribute the stress over a larger root surface, lowering the local larger root surface, lowering the local stresses and slowing the rate of tooth stresses and slowing the rate of tooth movement. movement.
On the other hand, appliance that deliver On the other hand, appliance that deliver
higher stresses would close extraction sites higher stresses would close extraction sites most rapidly. most rapidly.
(since large periodontal stressed will lead to (since large periodontal stressed will lead to faster tooth movement of both anterior and faster tooth movement of both anterior and posterior teeth) posterior teeth)
www.indiandentalacademy.com

Hypothesis 3Hypothesis 3 depicts a relationship in depicts a relationship in which increasing stress causes the which increasing stress causes the rate of movement to increase to a rate of movement to increase to a maximum. maximum.
Once this optimal level is reached, Once this optimal level is reached, additional stress causes the rate of additional stress causes the rate of movement to decline. movement to decline.
www.indiandentalacademy.com

This hypothesis was originally This hypothesis was originally proposed by proposed by Smith and Storey (1952)Smith and Storey (1952) and following clinical strategies have and following clinical strategies have evolved to take advantage of its evolved to take advantage of its implications :implications :
- Use light forces to retract canines - Use light forces to retract canines which will prevent anchorage loss, which will prevent anchorage loss, but but using heavy forces to protract using heavy forces to protract posterior teeth and "anchor" the posterior teeth and "anchor" the canines. (differential anchorage)canines. (differential anchorage)
www.indiandentalacademy.com

Hypothesis 4Hypothesis 4 is a composite of some of the is a composite of some of the foregoing concepts. foregoing concepts.
Here the relationship of rate of movement Here the relationship of rate of movement and stress magnitude is linear up to a point; and stress magnitude is linear up to a point; after this point, an increase in stress causes after this point, an increase in stress causes no appreciable increase or decrease in tooth no appreciable increase or decrease in tooth movement. movement.
Main difference between 3Main difference between 3rdrd and 4 and 4thth hypothesis hypothesis is effect of force beyond optimal range. is effect of force beyond optimal range.
www.indiandentalacademy.com

EVALUATION OF HYPOTHESESEVALUATION OF HYPOTHESES None of the studies in literature support None of the studies in literature support
hypothesis 1hypothesis 1 (constant relationship (constant relationship between stress and rate of movement).between stress and rate of movement).
Hypothesis 2Hypothesis 2 (continuing linear (continuing linear relationship between stress level and relationship between stress level and amount of tooth movement) is also not amount of tooth movement) is also not substantiated well in literature. substantiated well in literature.
www.indiandentalacademy.com

Hypothesis 3Hypothesis 3, the original Smith and , the original Smith and Storey proposal (1952), can no longer Storey proposal (1952), can no longer be considered viable in light of be considered viable in light of subsequent clinical experience. subsequent clinical experience.
www.indiandentalacademy.com

During canine retraction, canine During canine retraction, canine moves more than molar at both the moves more than molar at both the high and low force levels and more high and low force levels and more importantly, there is no evidence for importantly, there is no evidence for the rate of movement to suddenly the rate of movement to suddenly reverse as the stress levels increase reverse as the stress levels increase past a certain "optimum" value.past a certain "optimum" value.
www.indiandentalacademy.com

Evidence for Evidence for 44thth Hypothesis Hypothesis is more is more compellingcompelling
Burstone and Groves, (1961), Hixon et Burstone and Groves, (1961), Hixon et al. (1969) and Boester and Johnston al. (1969) and Boester and Johnston (1974) provide evidence that beyond (1974) provide evidence that beyond a certain stress level, increasing stress a certain stress level, increasing stress no longer alters the rate of tooth no longer alters the rate of tooth movement. (no increase or decrease in movement. (no increase or decrease in rate of movement)rate of movement)
www.indiandentalacademy.com

This study conclude that beyond an This study conclude that beyond an optimal range, there is no effect of optimal range, there is no effect of increased force level on rate of tooth increased force level on rate of tooth movement.movement.
But But “what is the upper limit of this “what is the upper limit of this optimal range”? optimal range”?
www.indiandentalacademy.com

Both type (intermittent or continuous) Both type (intermittent or continuous) and level (magnitude) of force are and level (magnitude) of force are important factors in determining important factors in determining optimal force which will preserve optimal force which will preserve health of tissue. health of tissue.
Any abnormal force will lead to Any abnormal force will lead to adverse tissue reaction in form root adverse tissue reaction in form root resorption.resorption.
www.indiandentalacademy.com

Effect of force level Effect of force level (magnitude) on rate of tooth (magnitude) on rate of tooth movement and root resorptionmovement and root resorption
Many studies have been performed to Many studies have been performed to investigate the relationship between investigate the relationship between magnitude of applied force and amount magnitude of applied force and amount of tooth movement and root resorption.of tooth movement and root resorption.
(Storey and Smith, 1952;Reitan, 1960; Burstone and (Storey and Smith, 1952;Reitan, 1960; Burstone and Groves, 1961; Andreasen and Johnson, 1967; Hixon Groves, 1961; Andreasen and Johnson, 1967; Hixon et et aI., aI., 1969, 1970; Boester and Johnston, 1974; 1969, 1970; Boester and Johnston, 1974; Andreasen and Zwanziger, 1980; Maltha Andreasen and Zwanziger, 1980; Maltha et al., et al., 1993)1993)
www.indiandentalacademy.com

A clinical inter-individual study was A clinical inter-individual study was recently carried out to investigate tooth recently carried out to investigate tooth movements and adverse reactions of movements and adverse reactions of the tooth-supporting tissues when the the tooth-supporting tissues when the applied continuous force was doubled applied continuous force was doubled from 50g to 100g for tipping movement from 50g to 100g for tipping movement of premolar tooth of premolar tooth (Owman-Moll (Owman-Moll et al., et al., 1995).1995).
Note – force of 50-55g is optimal for premolar tipping (acc. to Note – force of 50-55g is optimal for premolar tipping (acc. to
SchwarzSchwarz))www.indiandentalacademy.com

The results demonstrated that the The results demonstrated that the rate rate of tooth movement increased but of tooth movement increased but severity of root resorption severity of root resorption (surface (surface extension and depth of root extension and depth of root resorption)resorption) showed no significant showed no significant differencedifference when force of 100g was when force of 100g was applied and compared with 50g. applied and compared with 50g.
www.indiandentalacademy.com

An additional investigation was An additional investigation was undertaken by same authors to undertaken by same authors to determine whether a further determine whether a further substantial increase of force substantial increase of force magnitude would result in faster magnitude would result in faster movement of the teeth without movement of the teeth without deleterious side effects. deleterious side effects.
www.indiandentalacademy.com

The effects of a four-fold increased The effects of a four-fold increased orthodontic force magnitude on orthodontic force magnitude on tooth movement and root tooth movement and root resorption.resorption.
- intra-individual study in - intra-individual study in adolescentsadolescents
Owman-Moll, Juri Kurol and Dan LundgrenOwman-Moll, Juri Kurol and Dan Lundgren
EJO 1996;18, 287-294EJO 1996;18, 287-294www.indiandentalacademy.com

This clinical and histological study was This clinical and histological study was designed as an intra-individual study designed as an intra-individual study to investigate the effect of continuous to investigate the effect of continuous force of 50g and 200g :force of 50g and 200g :
- on tooth movements and - on tooth movements and
- adverse tissue reactions - adverse tissue reactions
(root resorption)(root resorption)
www.indiandentalacademy.com

Subjects and methodsSubjects and methods
Experimental design and orthodontic Experimental design and orthodontic appliance appliance
The maxillary first premolars bilaterally The maxillary first premolars bilaterally in eight individuals, six boys and two in eight individuals, six boys and two girls aged 12.1-13.6 years (mean age girls aged 12.1-13.6 years (mean age 13.0 years), formed test teeth. 13.0 years), formed test teeth.
www.indiandentalacademy.com

A fixed orthodontic appliance was A fixed orthodontic appliance was inserted the day the experimental inserted the day the experimental period started and consisted of molar period started and consisted of molar bands on the first maxillary molars bands on the first maxillary molars joined with a half round transpalatal joined with a half round transpalatal bar for reinforcement of the bar for reinforcement of the anchorage. anchorage.
www.indiandentalacademy.com

A lingual arch with A lingual arch with an anterior acrylic an anterior acrylic bite block was bite block was soldered to the soldered to the molar bands to molar bands to reduce the occlusal reduce the occlusal forces on the test forces on the test teeth.teeth.
www.indiandentalacademy.com

The buccally directed tooth movement The buccally directed tooth movement was performed with a sectional arch was performed with a sectional arch (Sentalloy 0.018” when 50g force was (Sentalloy 0.018” when 50g force was applied and Australian wire 0.018” applied and Australian wire 0.018” when 200g force was applied). when 200g force was applied).
These wires were attached to the These wires were attached to the molar band and ligated to a bonded molar band and ligated to a bonded 0.018” bracket on the test teeth. 0.018” bracket on the test teeth.
www.indiandentalacademy.com

This continuous orthodontic force was This continuous orthodontic force was applied for 7 weeks (total duration of applied for 7 weeks (total duration of study). study).
The force magnitude was controlled The force magnitude was controlled weekly and reactivated to 50g and weekly and reactivated to 50g and 200g, and was measured to the 200g, and was measured to the nearest 1g with a strain gauge nearest 1g with a strain gauge (Haldex'E Halmstad, Sweden).(Haldex'E Halmstad, Sweden).
www.indiandentalacademy.com

The orthodontic force magnitude The orthodontic force magnitude declined on average from 50g to 41g declined on average from 50g to 41g (18 per cent) and on average from 200 (18 per cent) and on average from 200 to 145g (28 per cent) during each to 145g (28 per cent) during each week of appliance reactivation.week of appliance reactivation.
www.indiandentalacademy.com

Tooth movement registrationTooth movement registration
Alginate impressions were taken just Alginate impressions were taken just before start and at the end of the before start and at the end of the experiment. experiment.
With a sharp pencil, a point on each of With a sharp pencil, a point on each of the buccal and palatal cusps of the the buccal and palatal cusps of the test and control teeth was marked on test and control teeth was marked on the cast. the cast.
www.indiandentalacademy.com

The horizontal (buccal) tooth The horizontal (buccal) tooth movement was measured with a movement was measured with a coordinate measuring machine coordinate measuring machine (Validator lOO@, TESA SA, Renens, (Validator lOO@, TESA SA, Renens, Switzerland) to the Switzerland) to the nearest 0.01 nearest 0.01 mm.mm.
www.indiandentalacademy.com

Radiographic registrationsRadiographic registrations
Periapical radiographs using a long Periapical radiographs using a long cone parallel technique were taken cone parallel technique were taken within a week before the start of the within a week before the start of the tooth movement and immediately tooth movement and immediately before extraction of the teeth. before extraction of the teeth.
www.indiandentalacademy.com

Histological proceduresHistological procedures
At the end of the experiment, the teeth At the end of the experiment, the teeth were extracted.were extracted.
With the microtome set to 4 With the microtome set to 4 µµm, m, the the teeth were serially sectioned parallel to teeth were serially sectioned parallel to the long axis in a bucco- palatal the long axis in a bucco- palatal direction from the mesial surface to the direction from the mesial surface to the middle of the root (with total 3 middle of the root (with total 3 levels). levels).
www.indiandentalacademy.com

The sections were stained with The sections were stained with haematoxylin and eosin. haematoxylin and eosin.
A light microscope with a micrometer A light microscope with a micrometer fitted into the eye-piece was used to fitted into the eye-piece was used to measure surface extension and depth measure surface extension and depth of root resorption.of root resorption.
www.indiandentalacademy.com

The surface The surface extension of extension of resorption was resorption was measured parallel measured parallel to the root surface. to the root surface.
www.indiandentalacademy.com

The depth of each The depth of each resorption lacuna was resorption lacuna was measured at the measured at the deepest point by deepest point by using the distance using the distance from the bottom of from the bottom of the cavity the cavity perpendicular to the perpendicular to the tangent passing tangent passing through the borders of through the borders of the resorption lacuna the resorption lacuna on the root surface. on the root surface.
www.indiandentalacademy.com

The mean value of root contour and root The mean value of root contour and root area were calculated in order to describe area were calculated in order to describe the:the:
1 1 Resorbed root contour Resorbed root contour (%). (%).
The sum of the extension of the resorption The sum of the extension of the resorption along the root surface in the three along the root surface in the three longitudinal and bucco palatally directed longitudinal and bucco palatally directed histological sections of each tooth was histological sections of each tooth was registered and a mean was calculated and registered and a mean was calculated and related to a registered mean root contour.related to a registered mean root contour.
www.indiandentalacademy.com

2 2 Resorbed root area Resorbed root area (%). (%).
The sum of the resorbed root area The sum of the resorbed root area (extension x depth of the resorption (extension x depth of the resorption lacuna) in the three longitudinal and lacuna) in the three longitudinal and bucco-palatally directed histological bucco-palatally directed histological sections of each tooth was registered sections of each tooth was registered and a mean was calculated and and a mean was calculated and related to a registered mean root area.related to a registered mean root area.
www.indiandentalacademy.com

ResultsResults
Amount of tooth movementAmount of tooth movement
After application of a continuous force After application of a continuous force of 50g for 7 weeks, the tooth of 50g for 7 weeks, the tooth displacements varied between 1.5 and displacements varied between 1.5 and 5.9 mm (5.9 mm (mean 3.5mean 3.5 +/- 1.2 mm). +/- 1.2 mm).
When a continuous force of 200g was When a continuous force of 200g was applied, the movements varied applied, the movements varied between 1.9 and 7.9 mm (between 1.9 and 7.9 mm (mean 5.1mean 5.1 +/- 1.9 mm). +/- 1.9 mm).
www.indiandentalacademy.com

This difference in horizontal tooth This difference in horizontal tooth movement was significant movement was significant (P=0.02) (P=0.02) with a 95 per cent confidence interval.with a 95 per cent confidence interval.
www.indiandentalacademy.com

Root resorptionRoot resorption
Root resorption was registered in all Root resorption was registered in all test teeth and there were no test teeth and there were no significant difference in number (n) or significant difference in number (n) or severity of root resorption (i.e. severity of root resorption (i.e. resorbed root contour (%) and resorbed root contour (%) and resorbed root area (%)) after resorbed root area (%)) after application of a 50g compared with a application of a 50g compared with a 200g force.200g force.
www.indiandentalacademy.com

www.indiandentalacademy.com

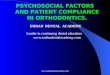
Frequency and severity of root resorption Frequency and severity of root resorption showed great individual variation, whether showed great individual variation, whether 50g or 200g force was used. 50g or 200g force was used.
50g force200g force
www.indiandentalacademy.com

DiscussionDiscussion A force of 50g has often been used and A force of 50g has often been used and
recommended when buccal tipping of recommended when buccal tipping of premolars is desired.premolars is desired.
The results of this study showed that The results of this study showed that when applied continuous force when applied continuous force increased four fold, (200g) tooth increased four fold, (200g) tooth movement increased 50 % without any movement increased 50 % without any significant increase in root resorption.significant increase in root resorption.
www.indiandentalacademy.com

One of the main findings in this One of the main findings in this investigation was that the individual investigation was that the individual variations in tooth movement as well variations in tooth movement as well as in frequency and severity of root as in frequency and severity of root resorption were large, irrespective of resorption were large, irrespective of amount of force. amount of force.
www.indiandentalacademy.com

This finding indicate that the major This finding indicate that the major source of variation is probably not the source of variation is probably not the magnitude of force, but variation in magnitude of force, but variation in metabolic response.metabolic response.
It is well known that prostaglandins It is well known that prostaglandins play a major role in resorption play a major role in resorption processes. processes.
(Klein and Raisz, 1970; Somjen (Klein and Raisz, 1970; Somjen et a/., et a/., 1980; Ngan 1980; Ngan et al., et al., 1988; 1988; Brudvik and Rygh, 1991). Brudvik and Rygh, 1991).
www.indiandentalacademy.com

In yet another hypothesis, it may be In yet another hypothesis, it may be speculated that a force magnitude of speculated that a force magnitude of 200g may be too large to express 200g may be too large to express cellular reactions close to the root cellular reactions close to the root surface and that tooth movement may surface and that tooth movement may take place mainly by undermining take place mainly by undermining resorption of the alveolar bone. (as resorption of the alveolar bone. (as proposed by proposed by Reitan, 1985Reitan, 1985). ).
www.indiandentalacademy.com

Where adverse tissue reactions are Where adverse tissue reactions are concerned, heavy force application may concerned, heavy force application may primarily prevent cellular reactions on the primarily prevent cellular reactions on the root surface. root surface.
But still, in a longer perspective, when the But still, in a longer perspective, when the force is reduced due to tooth movement, force is reduced due to tooth movement, extensive root resorption may take place. extensive root resorption may take place.
(as in this study also, higher forces have (as in this study also, higher forces have influenced the root surface)influenced the root surface)
www.indiandentalacademy.com

But this short term study of early tissue But this short term study of early tissue reactions in adolescents can not answer reactions in adolescents can not answer this assumption.this assumption.
The experimental model used in this The experimental model used in this study does not allow long term study does not allow long term investigations due to the limited bucco investigations due to the limited bucco lingual extension of the alveolar lingual extension of the alveolar process. process.
www.indiandentalacademy.com

It is therefore, necessary to utilize It is therefore, necessary to utilize another type of model, permitting another type of model, permitting tooth movement along the alveolar tooth movement along the alveolar ridge, if long-term results are to be ridge, if long-term results are to be studied.studied.
www.indiandentalacademy.com

Effect of type of force on rate Effect of type of force on rate of tooth movement and root of tooth movement and root resorptionresorption
ReitanReitan (1957, 1970, 1985) (1957, 1970, 1985) advocated use of intermittent forces advocated use of intermittent forces to prevent the development of root to prevent the development of root resorption by enabling reparative resorption by enabling reparative processes to occur during periods processes to occur during periods with little or no force.with little or no force.
www.indiandentalacademy.com

Maltha and DijkmanMaltha and Dijkman (1996)(1996) reported more reported more resorption in dogs when using continuous resorption in dogs when using continuous rather than intermittent forces. rather than intermittent forces.
Faltin et al. (2001) confirmed that a reduction of continuous force magnitude should be considered to preserve the integrity of the tissues.
www.indiandentalacademy.com

Constant versus dissipating forces in Constant versus dissipating forces in orthodontics: the effect on initial tooth orthodontics: the effect on initial tooth movement and root resorption.movement and root resorption.
F. WeilandF. Weiland
EJO 2003; 25, 335-342EJO 2003; 25, 335-342
www.indiandentalacademy.com

The aim of this clinical and laser The aim of this clinical and laser scanning microscopic study was to scanning microscopic study was to compare the effects of two frequently compare the effects of two frequently used arch wires on tooth movement used arch wires on tooth movement and root resorption. and root resorption.
www.indiandentalacademy.com

In a inter-individual comparison study In a inter-individual comparison study design, a total of 90 premolars in 27 design, a total of 90 premolars in 27 individuals (10 boys, 17 girls, with a individuals (10 boys, 17 girls, with a mean age of 12.5 years) were used in mean age of 12.5 years) were used in study.study.
Out of these 90 teeth, 6 teeth served Out of these 90 teeth, 6 teeth served as control.as control.
www.indiandentalacademy.com

Therefore, 84 teeth (maxilla/mandible) Therefore, 84 teeth (maxilla/mandible) were moved buccally with an were moved buccally with an experimental fixed orthodontic experimental fixed orthodontic appliance. appliance.
Impressions using alginate were taken Impressions using alginate were taken immediately before insertion of the immediately before insertion of the experimental appliance.experimental appliance.
www.indiandentalacademy.com

Appliance design Appliance design
A fixed orthodontic appliance was A fixed orthodontic appliance was cemented at the start of the cemented at the start of the experiment. experiment.
Appliance consisted of an acrylic splint Appliance consisted of an acrylic splint covering all but the experimental covering all but the experimental teeth.teeth.
www.indiandentalacademy.com

A fixed orthodontic appliance was cemented at the startA fixed orthodontic appliance was cemented at the startof the experiment. of the experiment. It consisted of an acrylic splintIt consisted of an acrylic splintcovering all but the experimental teeth in one archcovering all but the experimental teeth in one arch..
www.indiandentalacademy.com

Brackets (0.018 inch slot) were Brackets (0.018 inch slot) were bonded to the experimental teeth. bonded to the experimental teeth.
The brackets were incorporated in the The brackets were incorporated in the splints in such a way that a normal splints in such a way that a normal inter-bracket distance (5mm) existed inter-bracket distance (5mm) existed between the brackets on the splint and between the brackets on the splint and the bracket on the experimental tooththe bracket on the experimental tooth
www.indiandentalacademy.com

Base of the slot of the ‘splint brackets’ Base of the slot of the ‘splint brackets’ was 4.5 mm more buccally positioned was 4.5 mm more buccally positioned than that of the bracket on the than that of the bracket on the experimental tooth in the middle.experimental tooth in the middle.
The premolar on one side was activated The premolar on one side was activated with a stainless steel wire (0.016 inch) with a stainless steel wire (0.016 inch) with a buccal offset of 1 mm, which was with a buccal offset of 1 mm, which was reactivated every four weeks. reactivated every four weeks.
www.indiandentalacademy.com

The contra lateral premolar was moved The contra lateral premolar was moved with a super elastic wire (0.016 inch) with a super elastic wire (0.016 inch) with a force plateau of 0.8–1 N. with a force plateau of 0.8–1 N.
(This wire had an initial activation of (This wire had an initial activation of 4.5 mm and was not reactivated 4.5 mm and was not reactivated during the 12 week experimental during the 12 week experimental period).period).
www.indiandentalacademy.com

www.indiandentalacademy.com

At the end of the experimental period, At the end of the experimental period, tooth displacement was studied three-tooth displacement was studied three-dimensionally on dental casts with a co-dimensionally on dental casts with a co-ordinate measuring machine. ordinate measuring machine.
Teeth were then extracted. Six Teeth were then extracted. Six premolars were used as control teeth premolars were used as control teeth and were extracted before the and were extracted before the experiment started.experiment started.
www.indiandentalacademy.com

The depth, area, and volume of the The depth, area, and volume of the resorption lacunae were measured resorption lacunae were measured using three-dimensional digital images using three-dimensional digital images made with a confocal laser scanning made with a confocal laser scanning microscope (CLSM).microscope (CLSM).
www.indiandentalacademy.com

ResultResult
Tooth movementTooth movement
Teeth with the superelastic wire moved Teeth with the superelastic wire moved significantly more (3.50 versus 2.30 significantly more (3.50 versus 2.30 mm) and tipped buccally to a larger mm) and tipped buccally to a larger degree (9.26° versus 7.81°) during degree (9.26° versus 7.81°) during the 12-week experimental period than the 12-week experimental period than those moved with the stainless steel those moved with the stainless steel wire. wire.
www.indiandentalacademy.com

Resorption Resorption
The number of resorptions on the roots The number of resorptions on the roots of the teeth moved with a super elastic of the teeth moved with a super elastic wire was significantly greater than wire was significantly greater than those moved with a stainless steel those moved with a stainless steel wire (22 versus 16, wire (22 versus 16, P P < 0.001).< 0.001).
www.indiandentalacademy.com

www.indiandentalacademy.com

The amount of The amount of resorptive damageresorptive damage, , defined as the largest depth, defined as the largest depth, perimeter, area, and volume were perimeter, area, and volume were compared between these two groups.compared between these two groups.
The teeth moved with the super elastic The teeth moved with the super elastic wire showed significantly more wire showed significantly more resorptive damage regarding all these resorptive damage regarding all these parameters.parameters.
www.indiandentalacademy.com

www.indiandentalacademy.com

ConclusionConclusion
This study confirms earlier studies This study confirms earlier studies regarding potential damage to tissues regarding potential damage to tissues with use of continuous force.with use of continuous force.
(Gibson (Gibson et al.et al. 1992; Owman-Moll 1992; Owman-Moll et al.et al. 1995; 1995;
Daskalogiannakis and McLachlan. 1996; Daskalogiannakis and McLachlan. 1996; Darendeliler Darendeliler et et
alal., 1997 and Faltin ., 1997 and Faltin et al. et al. 2001)2001)
www.indiandentalacademy.com

It could not be confirmed that It could not be confirmed that maxillary teeth are at higher maxillary teeth are at higher resorptive risk than mandibular teeth, resorptive risk than mandibular teeth, as has been stated in the literature as has been stated in the literature
(Ketcham, 1927, 1929;Massler and Malone, 1954; Massler and (Ketcham, 1927, 1929;Massler and Malone, 1954; Massler and Perreault, 1954;Phillips, 1955; McFadden Perreault, 1954;Phillips, 1955; McFadden et alet al., 1989). ., 1989).
www.indiandentalacademy.com

The differing sensitivity is mostly The differing sensitivity is mostly explained by the differing mechanical explained by the differing mechanical load of the upper and lower teeth load of the upper and lower teeth during treatment or differing amounts during treatment or differing amounts of tooth movement during orthodontic of tooth movement during orthodontic therapy. therapy.
In this investigation, the force system In this investigation, the force system used in the maxilla and mandible was used in the maxilla and mandible was the same.the same.
www.indiandentalacademy.com

The amount of tooth movement and the The amount of tooth movement and the amount of resorptive activity were amount of resorptive activity were correlated. However, this correlation was correlated. However, this correlation was weak, the correlation coefficient (weak, the correlation coefficient (rr) being ) being 0.35 0.35
This confirms data from the literature (Stuteville, 1937, 1938; This confirms data from the literature (Stuteville, 1937, 1938; Morse, 1971; Von der Ahe, 1973; Hollender Morse, 1971; Von der Ahe, 1973; Hollender et alet al., 1980; ., 1980; Sharpe Sharpe et alet al., 1987; Kelley ., 1987; Kelley et alet al., 1993; Beck and Harris, 1994; ., 1993; Beck and Harris, 1994; Baumrind Baumrind et alet al., 1996; Costopoulos and Nanda, 1996).., 1996; Costopoulos and Nanda, 1996).
www.indiandentalacademy.com

Individual variations have been Individual variations have been reported to be an important factor for reported to be an important factor for both tooth movement in both force both tooth movement in both force systems. systems.
(Hixon (Hixon et alet al., 1970; Maltha ., 1970; Maltha et alet al., 1993; Lundgren ., 1993; Lundgren et alet al., 1996) ., 1996) and root resorption (Henry and Weinman, 1951; Massler and and root resorption (Henry and Weinman, 1951; Massler and Malone, 1954; Kvam, 1972; Reitan, 1974; Zachrisson, 1976; Malone, 1954; Kvam, 1972; Reitan, 1974; Zachrisson, 1976; Linge and Linge, 1983). This clinical study confirms these Linge and Linge, 1983). This clinical study confirms these findings.findings.
www.indiandentalacademy.com

Rygh and Brudvik (1993)Rygh and Brudvik (1993) stated : stated :
‘ ‘New wire qualities pose challenges for New wire qualities pose challenges for the orthodontist who must try to avoid the orthodontist who must try to avoid continuous forces that are heavy continuous forces that are heavy enough to lead to necrosis of the enough to lead to necrosis of the periodontal ligament, and last long periodontal ligament, and last long enough to prevent the root from enough to prevent the root from recovering from damage inflicted on recovering from damage inflicted on its surface’.its surface’.
www.indiandentalacademy.com

Thank youThank you
For more details please visit For more details please visit
www.indiandentalacademy.comwww.indiandentalacademy.com
www.indiandentalacademy.com