Embed Size (px)
Citation preview
Clinical experiences with a new device for fixed
orthodontic treatment of Angle classes 2 and 3
KEYWORDSSecond Class; Therd Class; Fixed Connecting Device; New device, Herbst; Auxiliary arch.
ABSTRACT
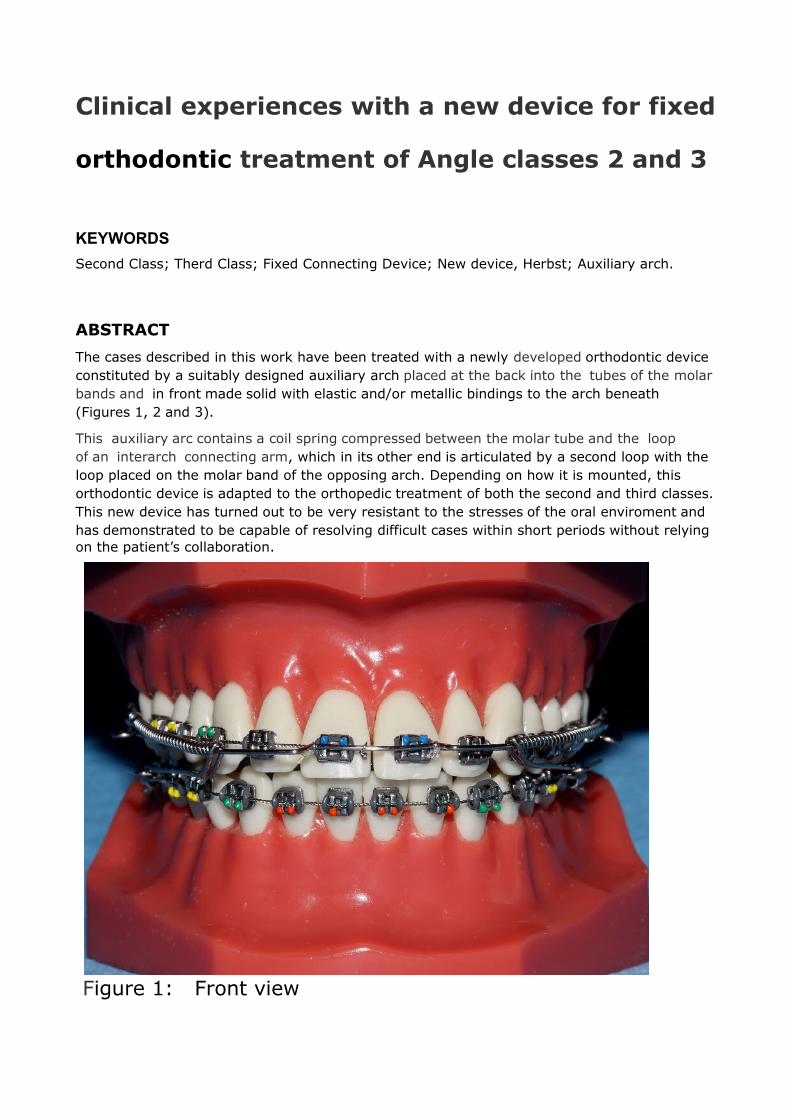
The cases described in this work have been treated with a newly developed orthodontic device constituted by a suitably designed auxiliary arch placed at the back into the tubes of the molar bands and in front made solid with elastic and/or metallic bindings to the arch beneath (Figures 1, 2 and 3).
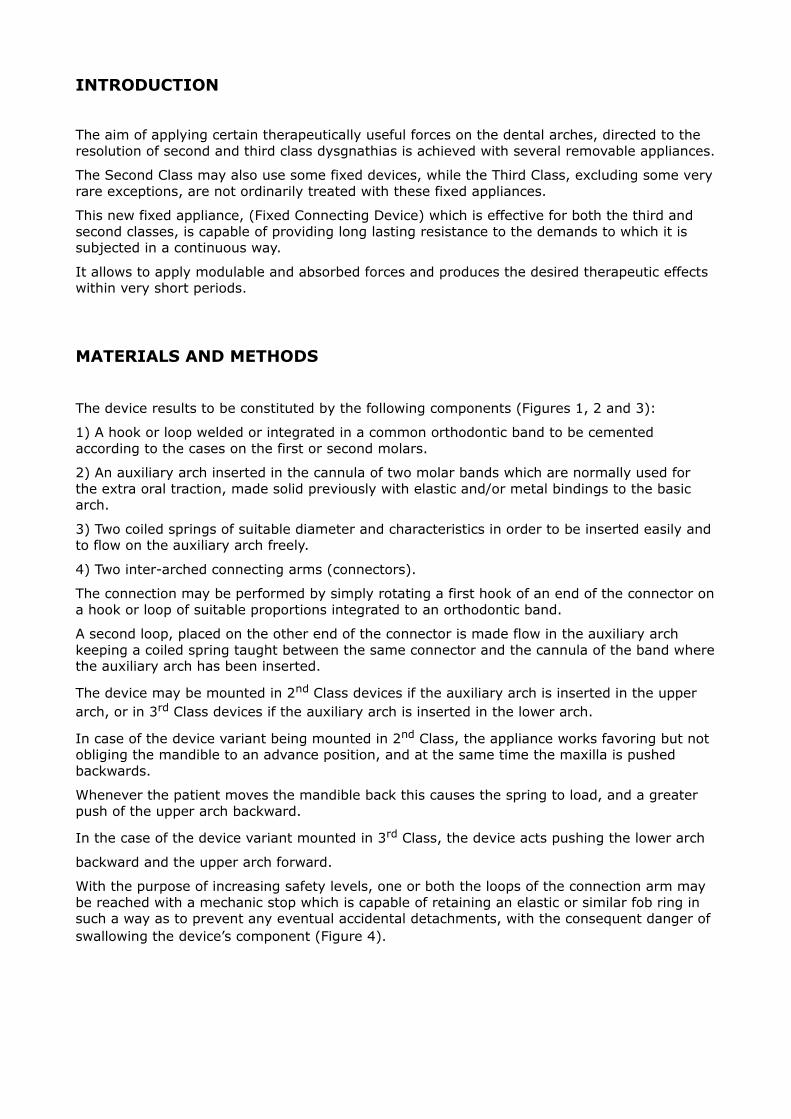
This auxiliary arc contains a coil spring compressed between the molar tube and the loop of an interarch connecting arm, which in its other end is articulated by a second loop with the loop placed on the molar band of the opposing arch. Depending on how it is mounted, this orthodontic device is adapted to the orthopedic treatment of both the second and third classes. This new device has turned out to be very resistant to the stresses of the oral enviroment and has demonstrated to be capable of resolving difficult cases within short periods without relying on the patient’s collaboration.
Figure 1: Front view
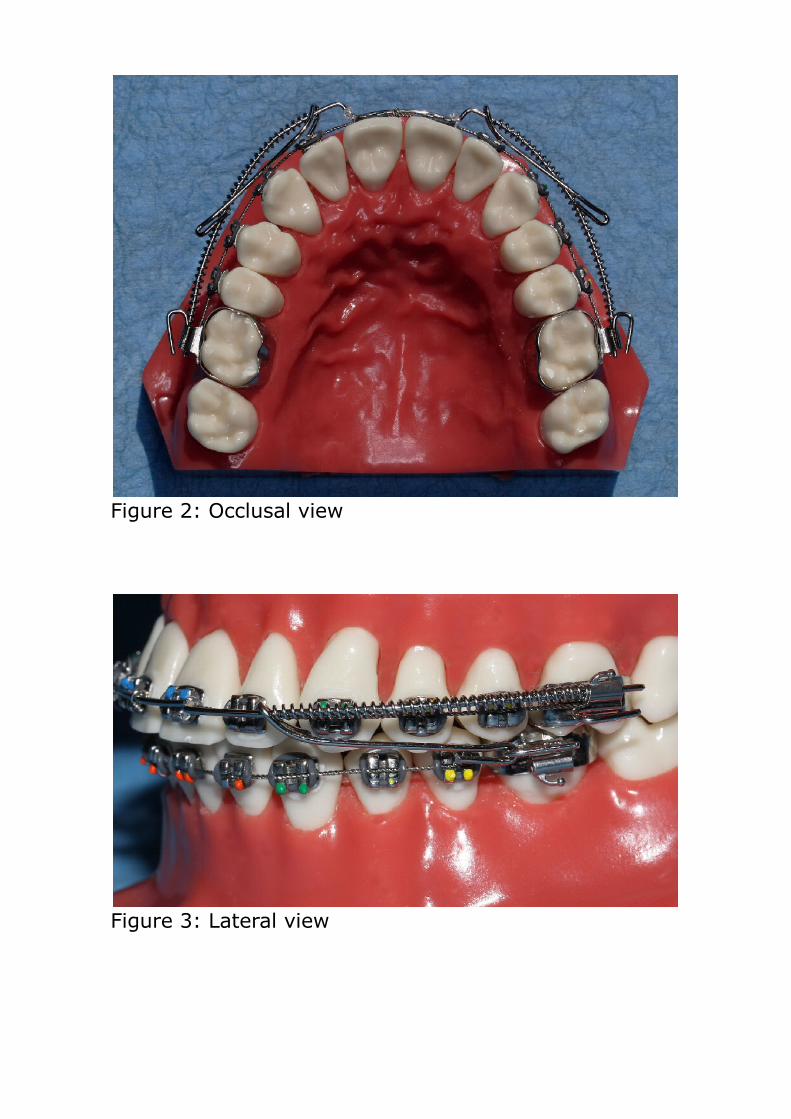
Figure 2: Occlusal view
Figure 3: Lateral view
INTRODUCTION
The aim of applying certain therapeutically useful forces on the dental arches, directed to the resolution of second and third class dysgnathias is achieved with several removable appliances.
The Second Class may also use some fixed devices, while the Third Class, excluding some very rare exceptions, are not ordinarily treated with these fixed appliances.
This new fixed appliance, (Fixed Connecting Device) which is effective for both the third and second classes, is capable of providing long lasting resistance to the demands to which it is subjected in a continuous way.
It allows to apply modulable and absorbed forces and produces the desired therapeutic effects within very short periods.
MATERIALS AND METHODS
The device results to be constituted by the following components (Figures 1, 2 and 3):
1) A hook or loop welded or integrated in a common orthodontic band to be cemented according to the cases on the first or second molars.
2) An auxiliary arch inserted in the cannula of two molar bands which are normally used for the extra oral traction, made solid previously with elastic and/or metal bindings to the basic arch.
3) Two coiled springs of suitable diameter and characteristics in order to be inserted easily and to flow on the auxiliary arch freely.
4) Two inter-arched connecting arms (connectors).
The connection may be performed by simply rotating a first hook of an end of the connector on a hook or loop of suitable proportions integrated to an orthodontic band.
A second loop, placed on the other end of the connector is made flow in the auxiliary arch keeping a coiled spring taught between the same connector and the cannula of the band where the auxiliary arch has been inserted.
The device may be mounted in 2nd Class devices if the auxiliary arch is inserted in the upper arch, or in 3rd Class devices if the auxiliary arch is inserted in the lower arch.
In case of the device variant being mounted in 2nd Class, the appliance works favoring but not obliging the mandible to an advance position, and at the same time the maxilla is pushed backwards.
Whenever the patient moves the mandible back this causes the spring to load, and a greater push of the upper arch backward.
In the case of the device variant mounted in 3rd Class, the device acts pushing the lower arch
backward and the upper arch forward.
With the purpose of increasing safety levels, one or both the loops of the connection arm may be reached with a mechanic stop which is capable of retaining an elastic or similar fob ring in such a way as to prevent any eventual accidental detachments, with the consequent danger of swallowing the device’s component (Figure 4).
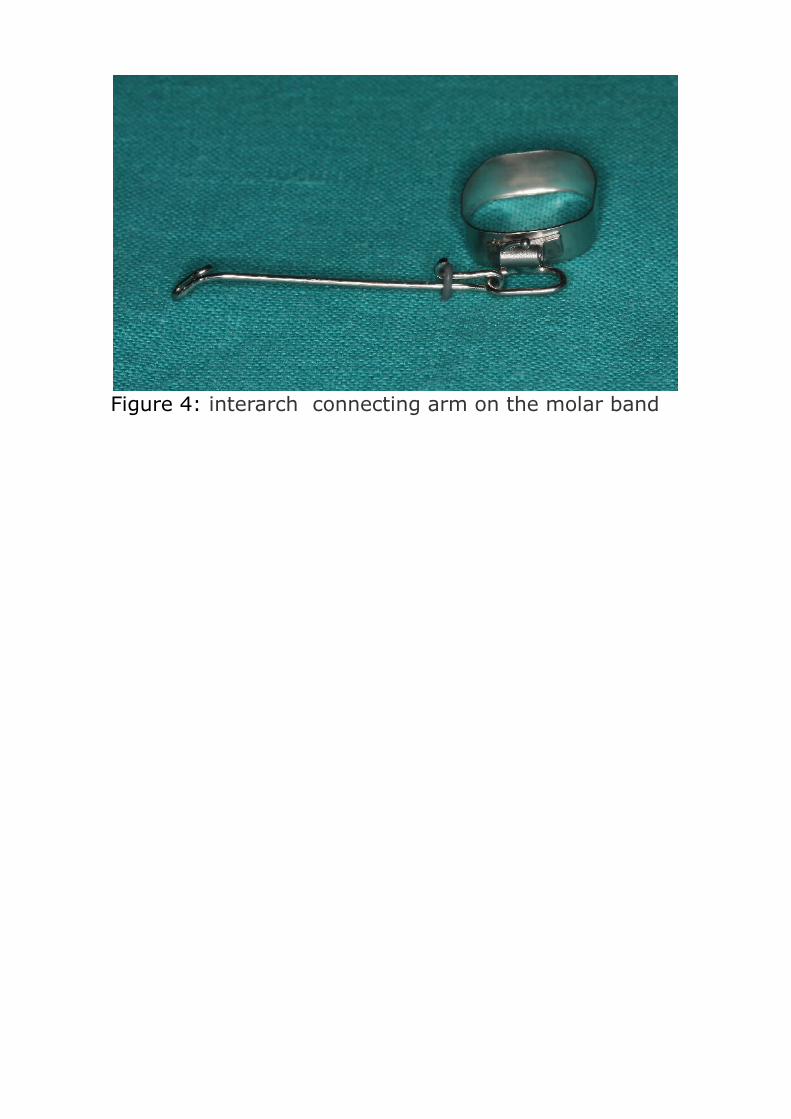
Figure 4: interarch connecting arm on the molar band
CLINICAL CASES
A second class case and a third class case are introduced by way of example.
The pictures show how the situation has evolved gradually, being induced by the new device using in a non continuous way but, depending on the cases, in variable cycles going from one to four weeks.
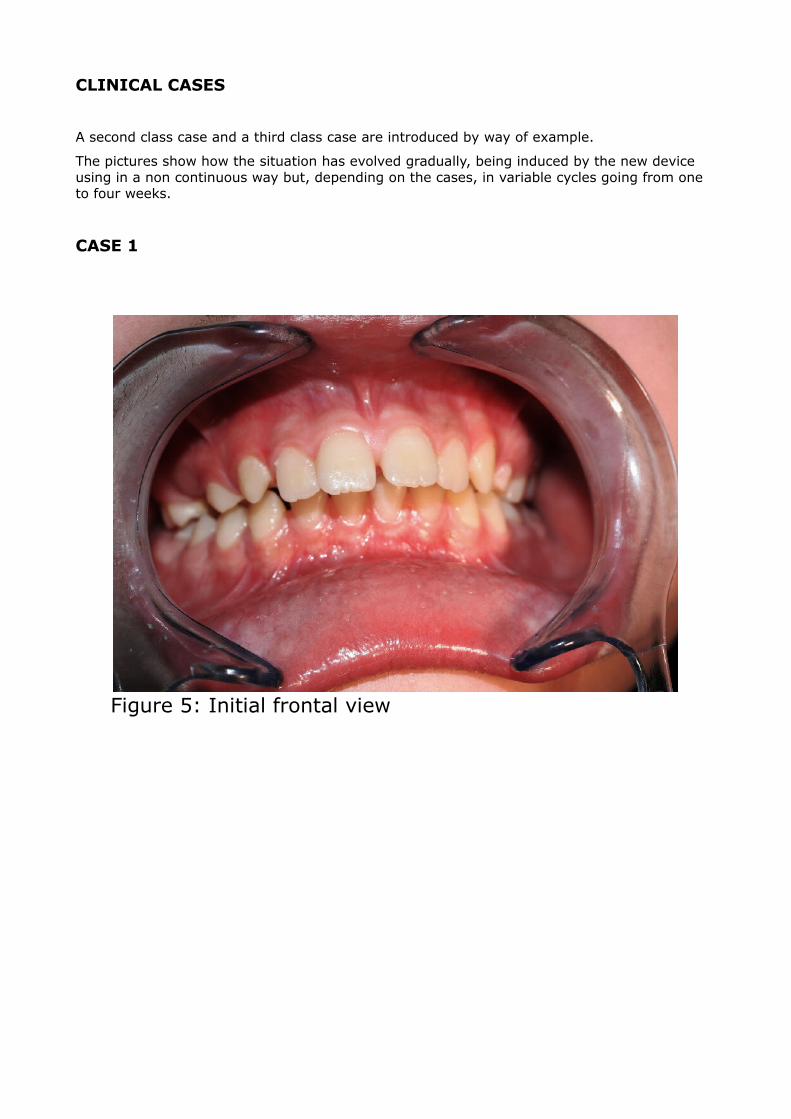
CASE 1
Figure 5: Initial frontal view

Figure 6: Lateral view
Figure 7: The new device mounted in the mouth
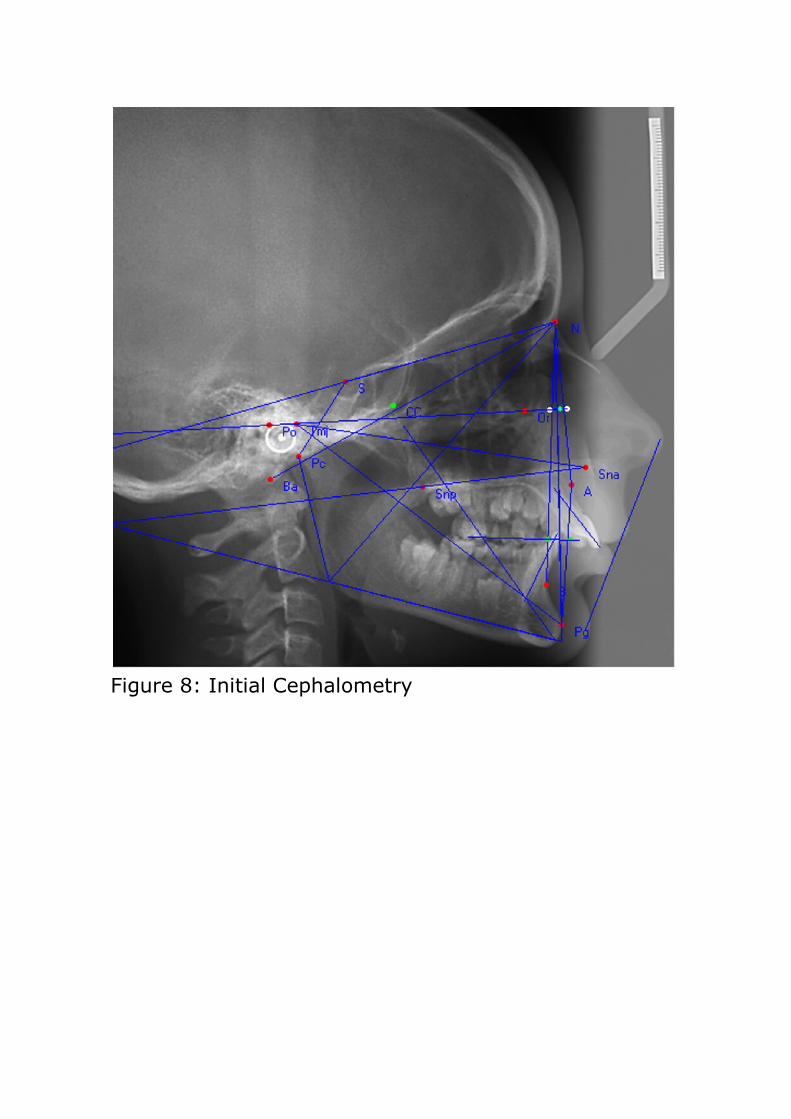
Figure 8: Initial Cephalometry
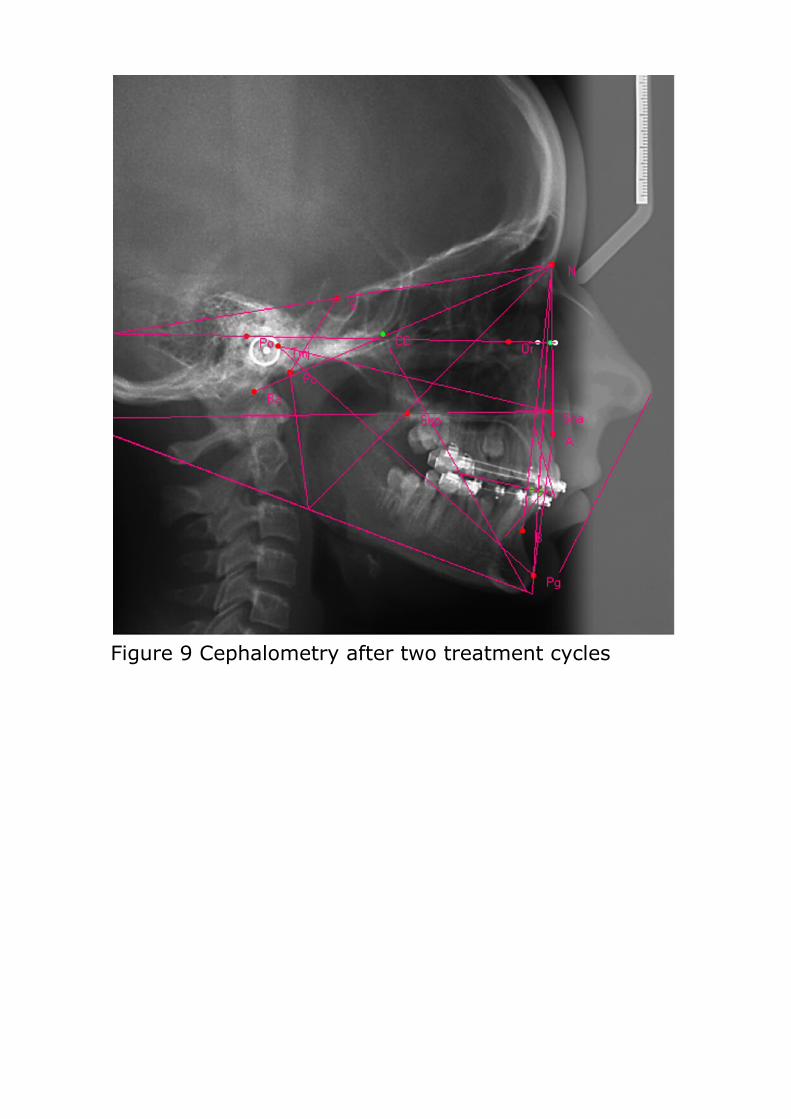
Figure 9 Cephalometry after two treatment cycles
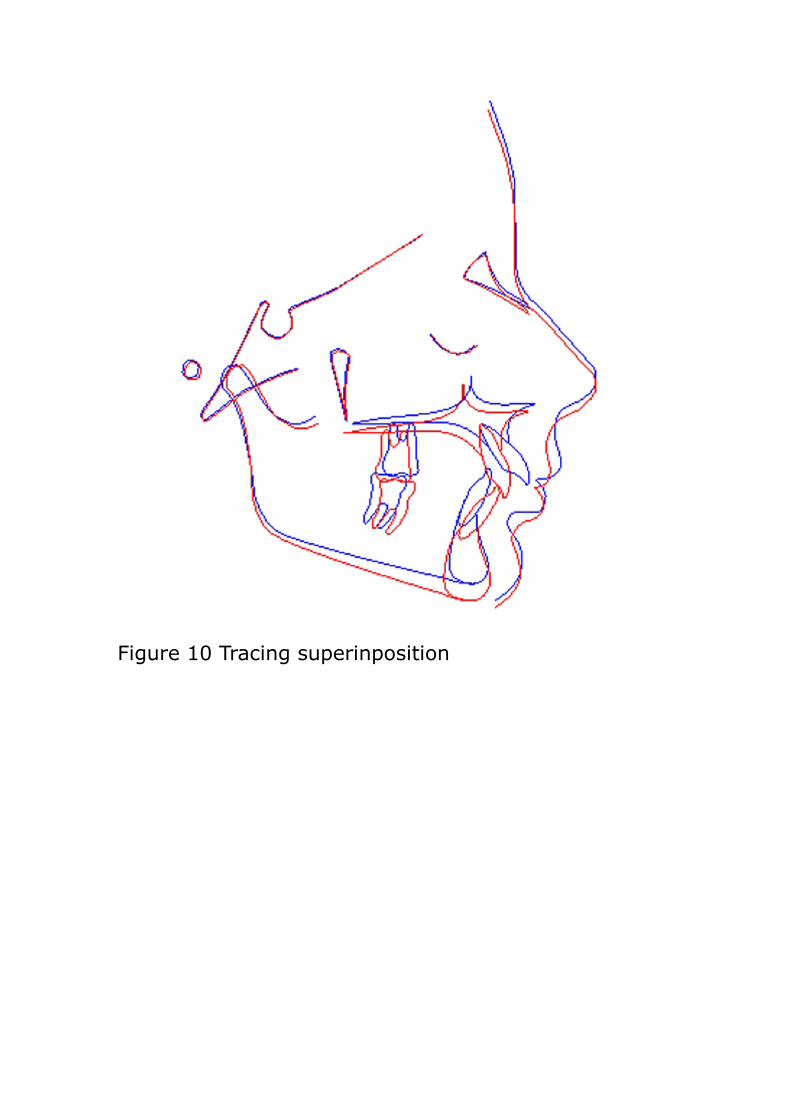
Figure 10 Tracing superinposition
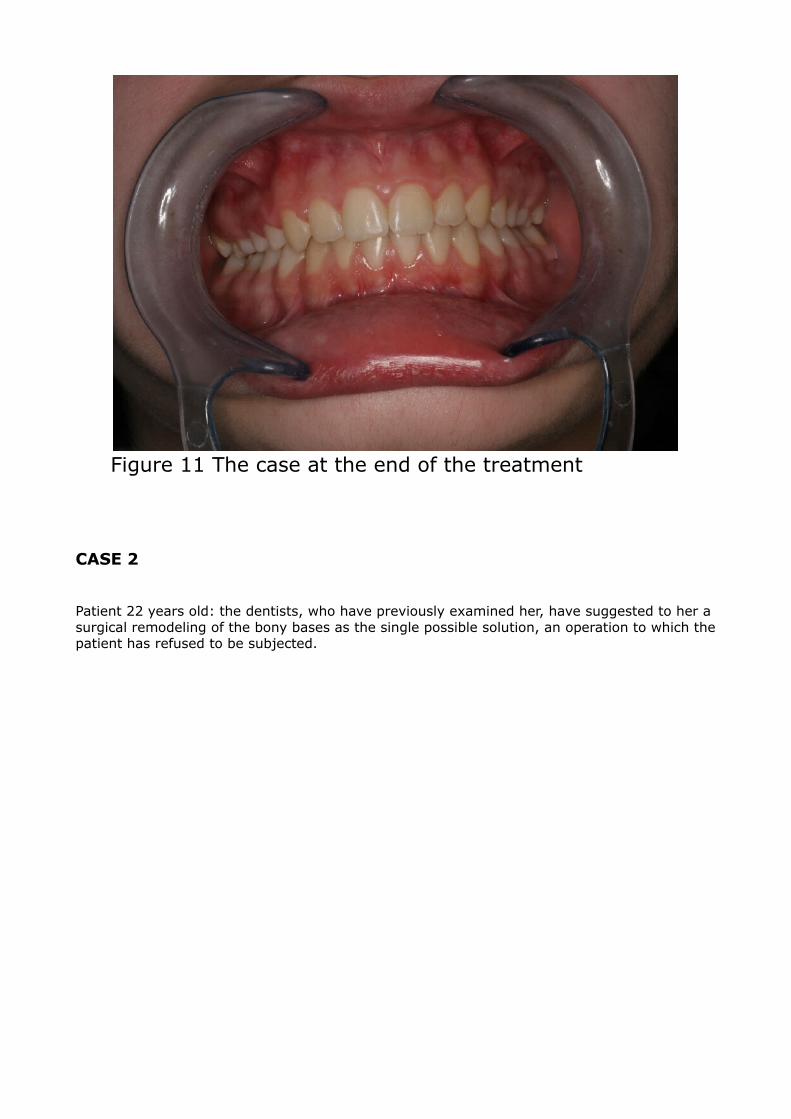
Figure 11 The case at the end of the treatment
CASE 2
Patient 22 years old: the dentists, who have previously examined her, have suggested to her a surgical remodeling of the bony bases as the single possible solution, an operation to which the patient has refused to be subjected.

Figure 12 Initial situation front view
Figure 13 Initial situation lateral view
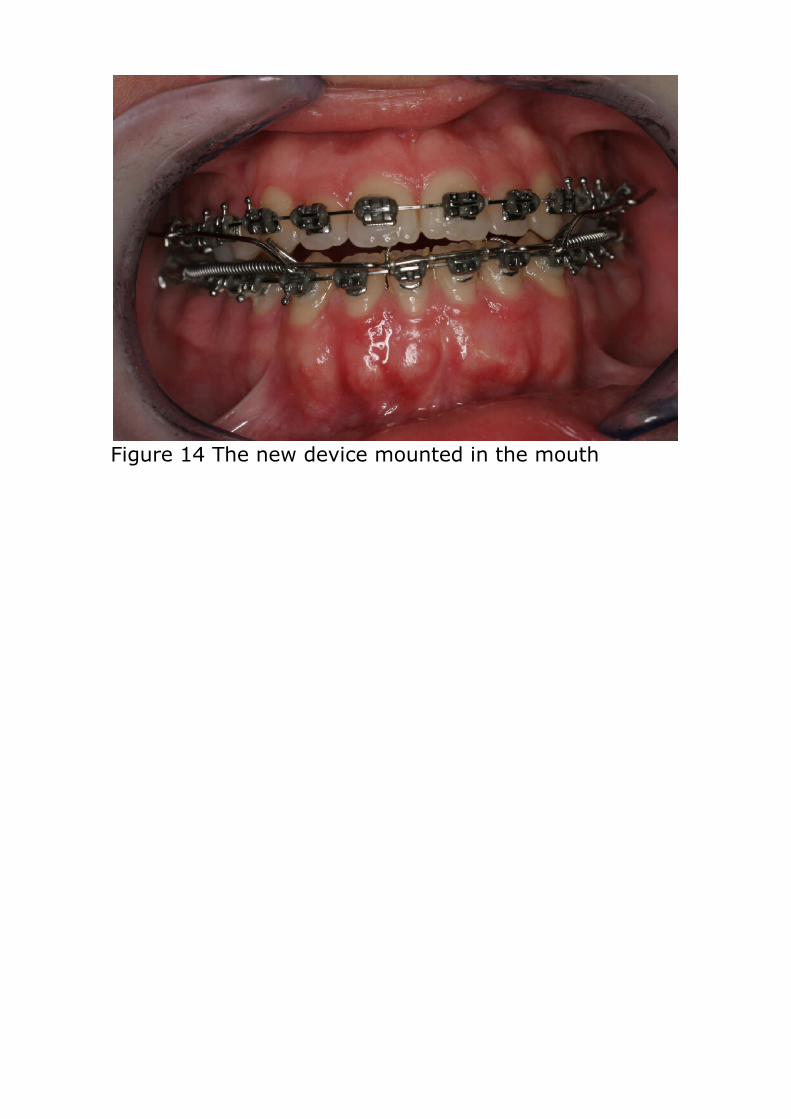
Figure 14 The new device mounted in the mouth
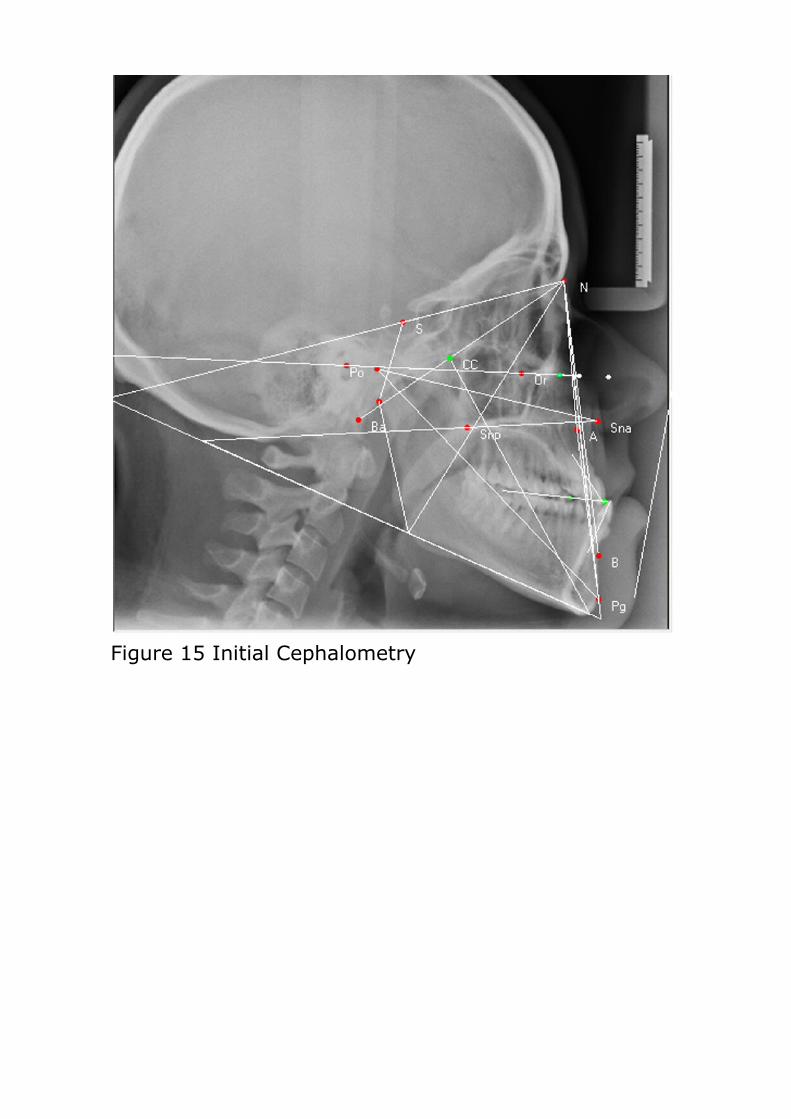
Figure 15 Initial Cephalometry
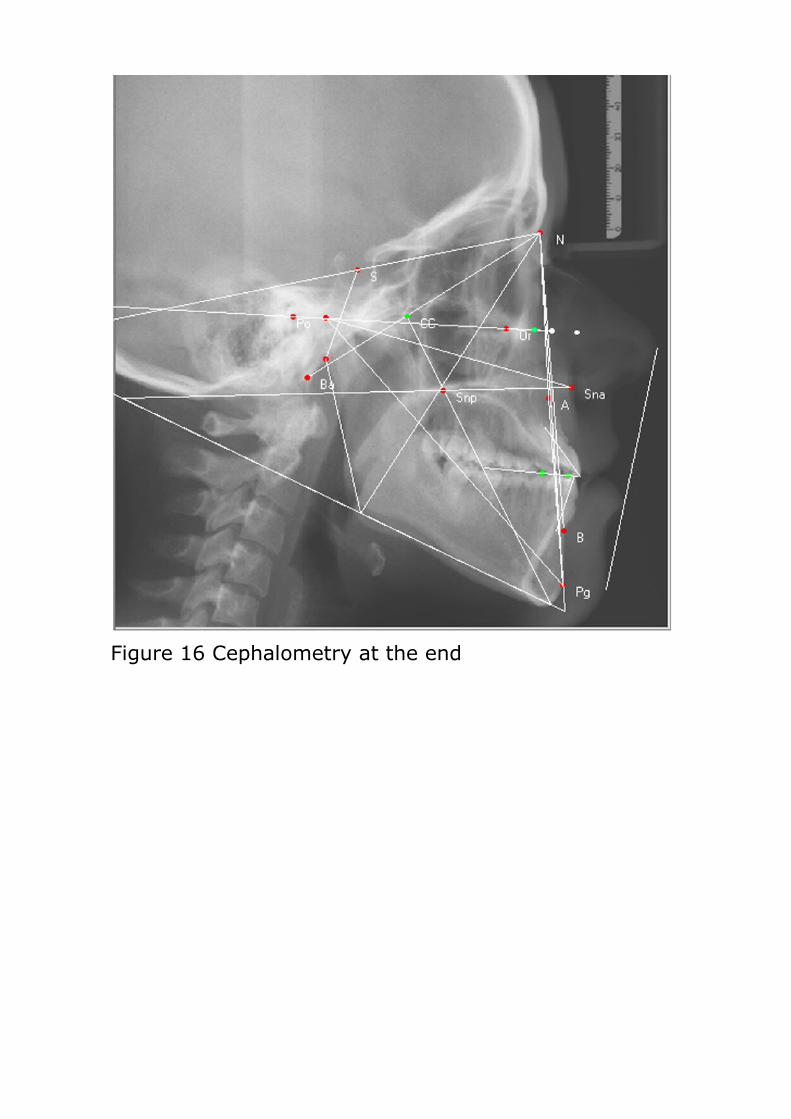
Figure 16 Cephalometry at the end
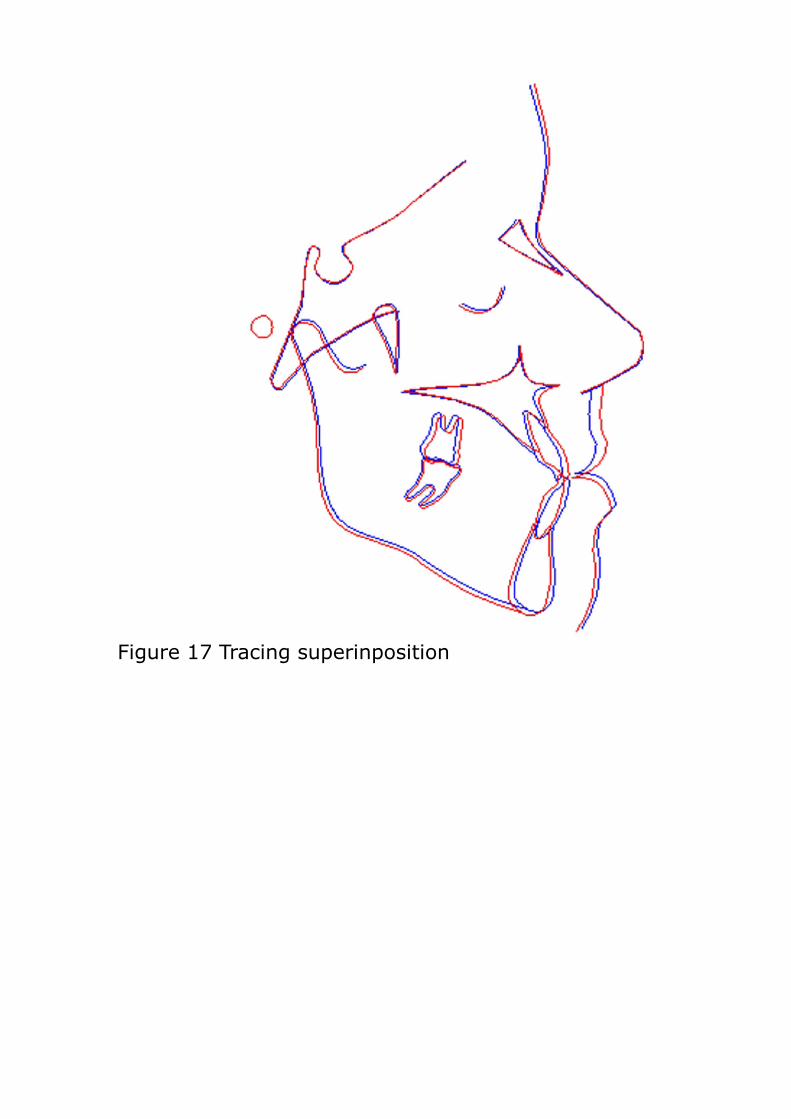
Figure 17 Tracing superinposition
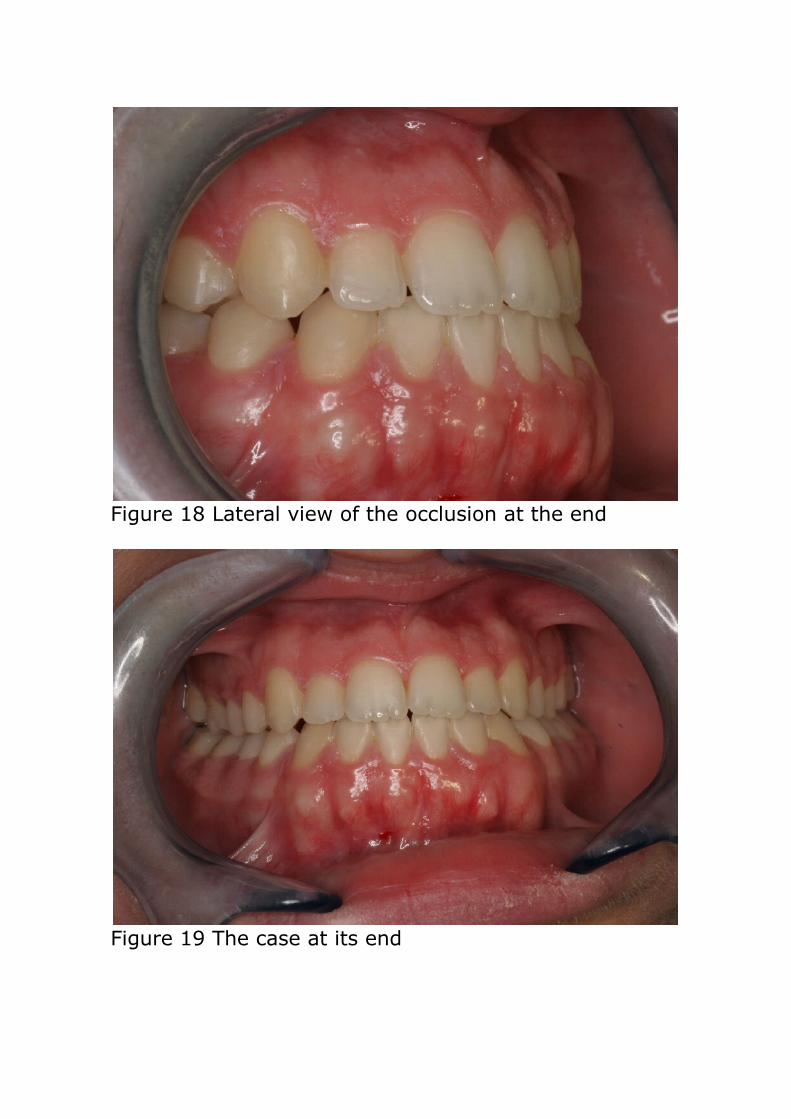
Figure 18 Lateral view of the occlusion at the end
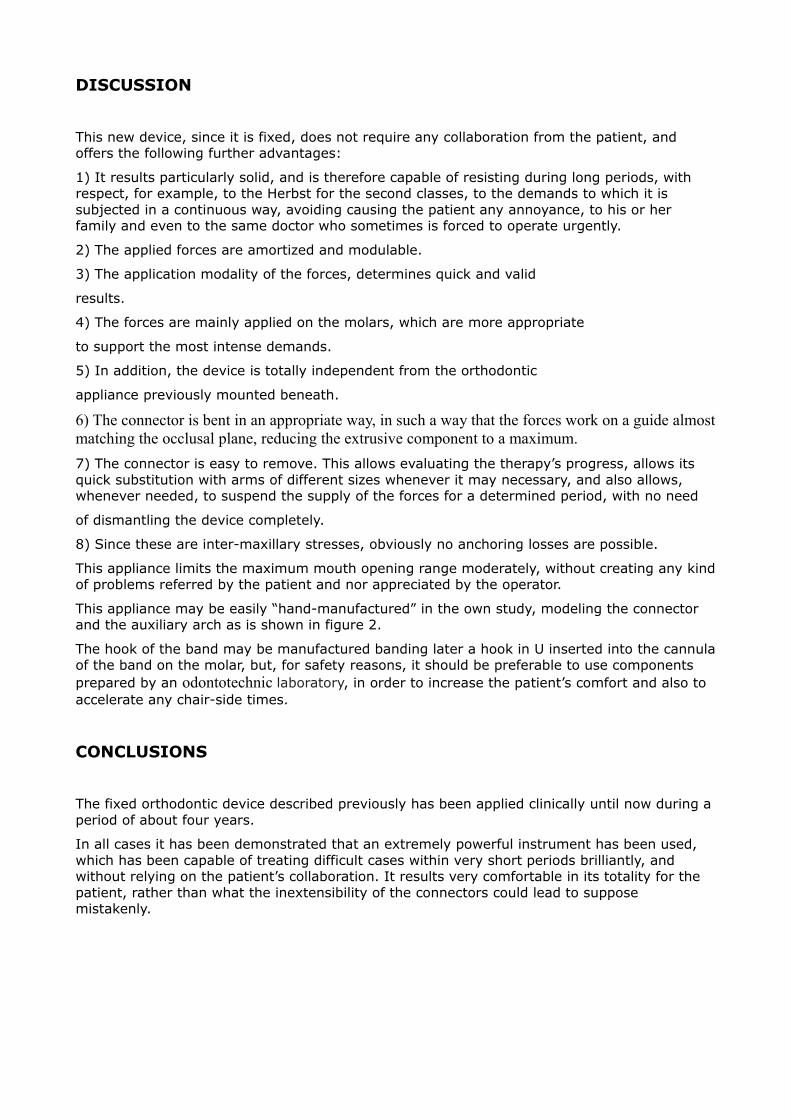
Figure 19 The case at its end
DISCUSSION
This new device, since it is fixed, does not require any collaboration from the patient, and offers the following further advantages:
1) It results particularly solid, and is therefore capable of resisting during long periods, with respect, for example, to the Herbst for the second classes, to the demands to which it is subjected in a continuous way, avoiding causing the patient any annoyance, to his or her family and even to the same doctor who sometimes is forced to operate urgently.
2) The applied forces are amortized and modulable.
3) The application modality of the forces, determines quick and valid
results.
4) The forces are mainly applied on the molars, which are more appropriate
to support the most intense demands.
5) In addition, the device is totally independent from the orthodontic
appliance previously mounted beneath.
6) The connector is bent in an appropriate way, in such a way that the forces work on a guide almost matching the occlusal plane, reducing the extrusive component to a maximum.7) The connector is easy to remove. This allows evaluating the therapy’s progress, allows its quick substitution with arms of different sizes whenever it may necessary, and also allows, whenever needed, to suspend the supply of the forces for a determined period, with no need
of dismantling the device completely.
8) Since these are inter-maxillary stresses, obviously no anchoring losses are possible.
This appliance limits the maximum mouth opening range moderately, without creating any kind of problems referred by the patient and nor appreciated by the operator.
This appliance may be easily “hand-manufactured” in the own study, modeling the connector and the auxiliary arch as is shown in figure 2.
The hook of the band may be manufactured banding later a hook in U inserted into the cannula of the band on the molar, but, for safety reasons, it should be preferable to use components prepared by an odontotechnic laboratory, in order to increase the patient’s comfort and also to accelerate any chair-side times.
CONCLUSIONS
The fixed orthodontic device described previously has been applied clinically until now during a period of about four years.
In all cases it has been demonstrated that an extremely powerful instrument has been used, which has been capable of treating difficult cases within very short periods brilliantly, and without relying on the patient’s collaboration. It results very comfortable in its totality for the patient, rather than what the inextensibility of the connectors could lead to suppose mistakenly.