Embed Size (px)
Citation preview
Operational Policy
Version FINAL
Issue date April 2019
East Midlands Congenital Heart Operational Policy Page 2
Policy Profile Overview
Key overall purpose of policy Description of clinical operational processes and facility requirement to meet the anticipated new congenital cardiac standards
Principal target audience All Paediatric and Adult Congenital Heart patients.
Application Applies to Paediatric and Adult Congenital patients & staff
Accountable Executive Director
Author(s) Charlotte King / Alison Poole
Approvals and monitoring
Approving body Board or Committee responsible for approving the policy
Date of implementation
Monitoring and audit EMCHC Board
Document Control and History
Version No
Date Approved
Date of Implementation
Next Review Date
Reason for Change e.g. full rewrite, amendment to reflect new legislation, updated flowchart, etc.
Final 05/04/2019 immediate 05/4/2020
East Midlands Congenital Heart Operational Policy Page 3
Document sign off Clinical and Operational sign off for East Midlands Congenital Heart Centre Operational Policy required to meet the 2016 NHS England Congenital Cardiac standards.
Introduction The Operational Policy for the East Midlands Congenital Heart Centre has been developed with clinical and operational leads for each service / department.
The current version of the policy assumes the operational requirements necessary to meet the minimum standards expected in the revised NHS England New Congenital Heart Disease Review (NCHDR) of 500 surgical cases per annum delivered by 4 congenital cardiac surgeons
Sign off I hereby confirm that this Operational Policy represents patient flow, operational working, functionality and required adjacencies (clinical and operational) for my department / service in the East Midlands Congenital Heart Centre.
I confirm that I have shared and discussed these patient flows, operational working, functionality and required adjacencies with my clinical colleagues in the multi-disciplinary team involved in providing the service for which I am responsible.
I acknowledge the information contained within this document will be used as a baseline to inform the design specification and the final design solution required to meet the revised Cardiac review standards.
It is not proposed through this process to ask for sign off of the following:
Activity levels – these will be confirmed and revised to meet the expectation of 500 cases before 2021/22 in line with the NHS England Specialised Commissioning Board decision November 2016
Staffing levels – expected numbers of staff on duty at any one time will be included in the Operational policy to assess impact on space but staffing establishments will not – these will be developed through the workforce planning process for the EMCHC co location project and the associated business case
Budgets – departmental budgets will not be included in the Operational Policy as these will be developed and agreed at a later stage in conjunction with the Business case and through separate work streams
Detailed Equipment Lists – major equipment will be included in the Operational Policy in order to assess impact on space, but the comprehensive equipment lists and detail will be developed and agreed through the separate equipment work stream
East Midlands Congenital Heart Operational Policy Page 4
Signed:
Women’s and Children’s CMG Clinical Lead
Name Date: 07 April 2019
Women’s and Children’s EMCHC Clinical Lead
Name Date: 07 April 2019
Women’s and Children’s CMG Head of Operations
Name Date: 07 April 2019
Women’s and Children’s Head of Nursing
Name Date: 07 April 2019

East Midlands Congenital Heart Operational Policy Page 5
Table of Contents
Policy Profile............................................................................... 2
Document Control and History ................................................... 2
Document sign off ...................................................................... 3
1 Introduction ......................................................................... 9
1.1 Philosophy .................................................................................................... 9
1.2 Principles of Care ......................................................................................... 9
1.3 Objectives ................................................................................................... 10
2 Scope ............................................................................... 10
3 Activity/Workload .............................................................. 11
3.1 Expected population growth ........................................................................ 11
3.2 Expected congenital surgical activity Glenfield Hospital .............................. 11
4 Definitions ......................................................................... 12
5 Roles and responsibilities................................................. 13
5.1 Medical ....................................................................................................... 13
5.1.1 Paediatric Cardiology .................................................................................. 13
5.1.2 Adult Congenital Heart Disease Cardiology ................................................ 14
5.1.3 Interventional Cardiology ............................................................................ 14
5.1.4 Surgery ....................................................................................................... 15
5.1.5 Intensive Care ............................................................................................ 16
5.1.6 Anaesthetics ............................................................................................... 16
5.1.7 Imaging ....................................................................................................... 17
5.2 Associated Health Professionals ................................................................. 17
5.2.1 Perfusion .................................................................................................... 17
5.2.2 Congenital Echocardiography ..................................................................... 18
5.2.3 Physiotherapy ............................................................................................. 18
5.2.4 Occupational Therapy ................................................................................. 18
5.2.5 Psychology ................................................................................................. 19
5.2.6 Therapies / Dietetics ................................................................................... 19
5.3 Nursing ....................................................................................................... 20
5.3.1 Network Lead Nurse ................................................................................... 20
5.3.2 Outpatient Nurses ....................................................................................... 20
5.3.3 Specialist (Cardiac Liaison)......................................................................... 20
5.3.4 Ward Nursing .............................................................................................. 21

East Midlands Congenital Heart Operational Policy Page 6
5.3.5 Play therapists ............................................................................................ 21
5.3.6 PICU/Transport ........................................................................................... 23
5.3.7 ECMO ......................................................................................................... 24
5.4 Management and Administration ................................................................ 24
5.4.1 Management Triumvirate ............................................................................ 24
5.4.2 Data and Outcomes Analyst ....................................................................... 24
5.4.3 Administration ............................................................................................. 24
6 The East Midlands Congenital Heart Network ................. 25
6.1.1 Network Board Membership........................................................................ 25
6.1.2 Governance ................................................................................................ 26
6.1.3 Network Audit and Monitoring ..................................................................... 26
7 Service Description .......................................................... 27
7.1 Department / Patient Flows and facilities .................................................... 27
7.2 Patient pathways and information ............................................................... 28
7.3 Current Accommodation ............................................................................. 28
7.3.1 Ward 30 ...................................................................................................... 28
7.3.2 Parents accommodation (Ward and PICU) ................................................. 29
7.3.3 Outpatients ................................................................................................. 29
7.3.4 ICU ............................................................................................................. 29
7.3.5 Adult wards ................................................................................................. 30
7.3.6 Multi-Disciplinary Team facilities ................................................................. 30
7.3.7 Cardiac Theatres ........................................................................................ 31
7.3.8 Catheter Lab ............................................................................................... 31
7.4 Inter dependencies ..................................................................................... 32
7.5 Non Clinical Support Services ..................................................................... 32
8 EMCHC website ............................................................... 33
9 Co-location of all Children’s services ............................... 34
9.1 Paediatric Cardiac Ward ............................................................................. 35
9.2 Parent Facilities .......................................................................................... 35
9.3 Paediatric EMCHC Outpatient Department ................................................. 35
9.4 Paediatric Intensive Care Unit (PICU) ......................................................... 36
9.5 Multi-Disciplinary Team (MDT) Facilities ..................................................... 36
9.6 Congenital Heart Theatre and Cath Lab Department .................................. 36
9.7 Children’s Hospital Project Phase II ............................................................ 36
10 Patient Feedback Mechanisms ........................................ 37
11 Equality and Diversity ....................................................... 37
East Midlands Congenital Heart Operational Policy Page 7
12 Review .............................................................................. 37
13 Training and Awareness................................................... 38
14 Disaster recovery plan...................................................... 38
15 Appendices ....................................................................... 39
Appendix A – Seven Day Services Clinical Standards Audit ..................................... 39
Appendix B – Summary of current and future budgeted workforce numbers ............ 41
Appendix C – EMCHN Referral and Care guidelines ................................................ 46
1. Introduction ............................................................................................... 53
2. Care closer to home ................................................................................. 53
3. Referral pathways ..................................................................................... 55
4. Antenatal diagnosis – (See Appendix 1, 2 and 3) ................................... 55
5. Acute Paediatric / Neonatal presentation- (See Appendix 4, 5 and 6) ... 56
6. Outpatient based (routine) referrals- (See Appendix 7) ......................... 56
9. Cross sectional imaging - (See Appendix 8) ........................................... 57
10. 24 hour access to Specialist advice - (See Appendix 9) ........................ 57
11. Centre to Centre referrals - See (Appendix 10) ....................................... 58
12. Self-referral- (See Appendix 11) ............................................................... 58
13. Urgent dental assessments- (See Appendix 12) ..................................... 58
14. Transition to Adulthood - (See Appendix 13 and 14) ............................. 59
15. Adult Congenital Cardiac care - (see Appendix 15) ................................ 60
Sub - Appendices ................................................................................................... 68
Appendix 1 Integrated care pathway for prenatal CHD........................................ 69
Appendix 2 - Referral pathway for Fetal Medicine Patients ................................. 70
Appendix 3 –Emergency Balloon Atrial Septostomy and temporary pacing ..... 72
Appendix 4- Management of acutely unwell Cardiac Children ............................ 74
Appendix 5 – Caring for a Neonate with Cardiac query (Clinical Pathway) ........ 75
Appendix 6 – Patient Pathway PDA Ligation in preterm babies ......................... 76
Appendix 7 – Management of a Child with Cardiac query ................................... 90
Appendix 8 - Cross sectional Imaging service at EMCHC ................................... 91
Appendix 9 – 24 hour access to specialist advice ............................................. 100
Appendix 10 - Centre to Centre Referrals, Access to Second Opinions .......... 101
Appendix 11 – Managing patients who self-refer out of hours ......................... 104
Appendix 12 – Urgent dental Assessments........................................................ 106
Appendix 13- Transition of patients from paediatric to adult cardiology services117
Appendix 14 - Minimise loss of patients to follow up (transition & transfer) ... 121
Appendix 15 - Adult Congenital Cardiac Care .................................................... 123
Appendix 16 – Neonatal services and Neonatal Transport ............................... 124
East Midlands Congenital Heart Operational Policy Page 8
Appendix 17- Paediatric Intensive Care Pathway............................................... 140
Appendix 18 – CoMET operational guidance (with special reference to EMCHC)145
Appendix 19 – Network Training Strategy .......................................................... 163
Appendix 20 – EMCHN Terms of Reference ....................................................... 166
Appendix 21 – Abbreviations and definitions .................................................... 175
Appendix D – EMCHC Models of care .................................................................... 179
Appendix E– Patient Pathways ............................................................................... 183
East Midlands Congenital Heart Operational Policy Page 9
1 Introduction In November 2016 the provision of Congenital Heart Disease Services at East Midlands Congenital Heart Centre was confirmed by the NHS England Specialised Commissioning Board. This Operational Policy illustrates the requirements, including working practice, infrastructure, and resource to meet the expected CHD standards. There are two key requirements (1) surrounding the number of Consultant Cardiac Surgeons and their requisite case load with the minimum standard expected being 3 surgeons and a caseload of 375 cases and an expectation that this will rise to 4 surgeons and a total caseload of 500 cases by 2021/22, and (2) that the children’s CHD service is co-located with all other children’s services by December 2020.
It is essential that UHL, its Children’s Hospital and EMCHC, demonstrate a strategy that assumes the delivery of 500 surgical cases by 4 Surgeons per annum – it is acknowledged that the caseload will be phased from the minimum requirement of 3 surgeons and 375 cases to the full complement of 4 surgeons each delivering 125 cases when the caseload dictates.
1.1 Philosophy EMCHC aims to lead the provision of the latest cardiac treatments, which have the best cardiac outcomes for children and adults regionally, and nationally.
1.2 Principles of Care High quality care delivered by a well-trained and educated workforce resourced to meet the projected case mix and workload;
Flexibility of resources, both physical and human, to deal with changing workloads and case mixes;
Care according to clinical guidelines that are compliant with current national and international guidelines where relevant ( stored on UHL Policies and Guidelines Library)
All patients are managed in line with Seven Day Services Clinical Standards Policy (Audit results can be found in Appendix A)
Design for patient safety, privacy & dignity, including age-specific facilities for children, adolescents, adults and adults with additional needs ;
o Minimisation of patient, staff and goods moves;
o Minimisation of steps in processes/hand-offs
o Integration of diagnostic and assessment processes;
o Optimised use of technology, including integrated IT (iCRIS, PACS & EPR);
Requirements to deliver cardiac care must acknowledge effective delivery of paediatric transport services and ECMO
Using the skills and expertise of professional staff flexibly, with joint training in order to transfer skills;
Access to senior clinical opinion from the earliest point in the patient pathway and onwards;
Protocol-led care across the East Midlands Network with standardisation of patient pathways integrating the input of all care practitioners (e.g., fetal medicine, paediatricians with expertise in cardiology, cardiac physiologists, etc.);
East Midlands Congenital Heart Operational Policy Page 10
Improved junior doctor / nursing training and improved skill mix that attracts high quality recruitment and retention
Provision of high quality family centred care with appropriate parent accommodation
1.3 Objectives This policy is designed to:
Assist all healthcare professionals involved in the provision of Fetal, Paediatric, Adolescent and Adult Congenital Cardiac services.
Outline the purpose and function of the clinical services provided in the department and its inter-relationship with supporting services
Ensure that all staff using the facility understand the philosophy of the service and work as a team with a comprehensive understanding of patient flow
Describe the service flow into, through and out of the department.
Describe the services as they will be delivered to meet the CHD standards
Describe the purpose and function of the required accommodation
Identify adjacencies/co-locations required for the service delivery
Outline legislative and mandatory requirements for the delivery of services in line with the current CHD Standards
2 Scope This document is relevant to all clinicians and managers who interface with the East Midlands Congenital Heart Centre and applies to all employees of the Trust. In particular it addresses:
Outpatient services at Glenfield Hospital
Elective and Emergency Cardiac catheterisation
Elective and Emergency Cardiac surgery
Cardiac Paediatric Intensive Care
Acute Cardiology inpatient care
Fetal Cardiology
Appropriate models of care for children, adolescents, adults and adults with additional needs
Dental surgery
Obstetric cardiology
ECMO
Transport NIC/PIC
Training and education
Administrative support space including data management and audit
Research
Plans for the provision of services on the LRI site co located with other Children’s services
East Midlands Congenital Heart Operational Policy Page 11
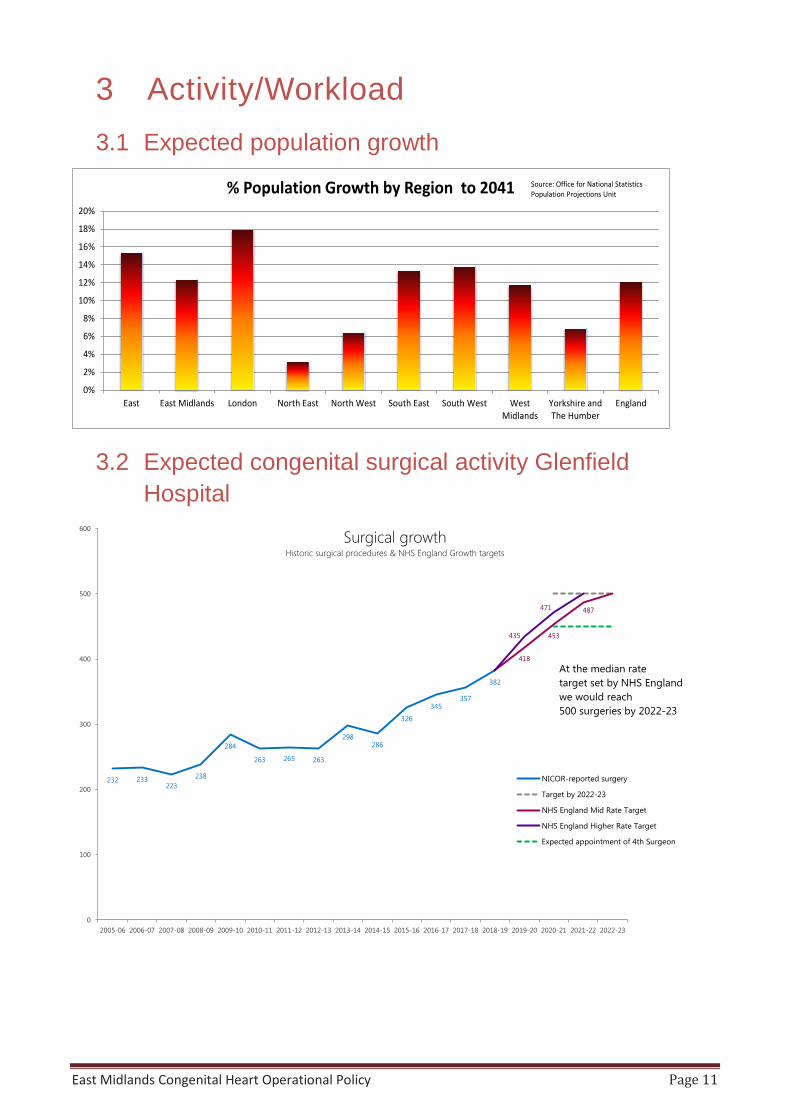
3 Activity/Workload 3.1 Expected population growth
3.2 Expected congenital surgical activity Glenfield Hospital
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
East East Midlands London North East North West South East South West WestMidlands
Yorkshire andThe Humber
England
% Population Growth by Region to 2041 Source: Office for National Statistics Population Projections Unit
232 233223
238
284
263 265 263
298286
326
345357
382
418
453
487
435
471
0
100
200
300
400
500
600
2005-06 2006-07 2007-08 2008-09 2009-10 2010-11 2011-12 2012-13 2013-14 2014-15 2015-16 2016-17 2017-18 2018-19 2019-20 2020-21 2021-22 2022-23
Surgical growthHistoric surgical procedures & NHS England Growth targets
NICOR-reported surgery
Target by 2022-23
NHS England Mid Rate Target
NHS England Higher Rate Target
Expected appointment of 4th Surgeon
At the median rate target set by NHS Englandwe would reach500 surgeries by 2022-23
East Midlands Congenital Heart Operational Policy Page 12
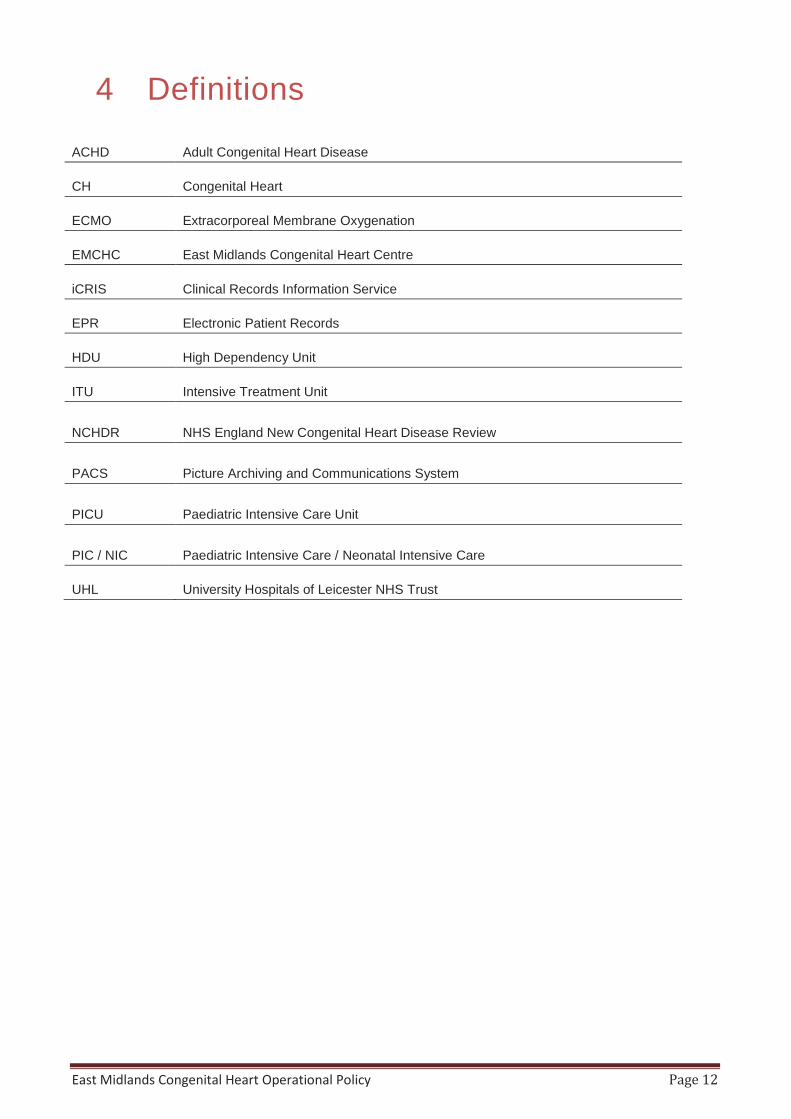
4 Definitions
ACHD Adult Congenital Heart Disease
CH Congenital Heart
ECMO Extracorporeal Membrane Oxygenation
EMCHC East Midlands Congenital Heart Centre
iCRIS Clinical Records Information Service
EPR Electronic Patient Records
HDU High Dependency Unit
ITU Intensive Treatment Unit
NCHDR NHS England New Congenital Heart Disease Review
PACS Picture Archiving and Communications System
PICU Paediatric Intensive Care Unit
PIC / NIC Paediatric Intensive Care / Neonatal Intensive Care
UHL University Hospitals of Leicester NHS Trust
East Midlands Congenital Heart Operational Policy Page 13
5 Roles and responsibilities
Medical 5.1.1 Paediatric Cardiology
The role of the Paediatric Cardiology Consultants within the East Midlands Congenital Heart Centre is to provide specialist care from the time a cardiac problem is diagnosed antenatally, in infancy or through childhood and into adolescence. The majority of our patients need lifelong care and working with our adult congenital consultants is a key part of a successful transition.
EMCHC is currently wholly located at the Glenfield Hospital but works within the Children’s Hospital that spans UHL. There are a network of clinics throughout the East Midlands region including in Nottingham, Mansfield, Derby, Boston, Kettering, Grantham, Peterborough, Nuneaton and Lincoln. We accept referrals from across this network and beyond. Many will be non-urgent referrals from GPs and paediatric colleagues. Urgent referrals for acutely sick children are taken by the on call consultant through a 24 hour on call service often in conjunction with the Paediatric Intensivist.
Guidance documents for all methods of referral including the patient pathways have been approved by the East Midlands Congenital Heart Network Board and are available on the East Midlands Congenital Heart Network website http://www.eastmidlandscongenitalheart.nhs.uk/our-network/ and in Appendix C
Cardiac disease in children takes many forms from simple lesions which can be monitored in peripheral outpatient clinics within our network to children with highly complex and challenging anatomical abnormalities or rhythm problems who need to be inpatients or seen in the outpatient department at Glenfield hospital.
Evaluating the precise nature of a cardiac anomaly is central to the medical and surgical management of the patient. That understanding has to be demonstrated and discussed with the whole multi-disciplinary team in order to deliver the best care for that patient. There are many sub-specialties within paediatric cardiology that are well established but all rapidly expanding. There are a number of sub-specialty interests with in the paediatric cardiology team including fetal cardiology, advanced imaging (echocardiography, CT and MRI), cardiac catheterisation (invasive, minimal access, diagnostic and therapeutic interventions), and electrophysiology and pacing, which deals with disorders of the heart rhythm.
The team itself is an integral part of the Children’s Hospital and consultants provide joined up care with the many other obstetric, neonatal and paediatric specialities. We have 4 national training numbers in paediatric cardiology, one or occasionally two paediatric registrars receiving ‘special interest training in cardiology’, and several clinical fellows at both SHO and SPR level. Teaching other medical trainees and nursing staff is seen as important as is teaching for the undergraduate medical students.
East Midlands Congenital Heart Operational Policy Page 14
5.1.2 Adult Congenital Heart Disease Cardiology The Adult Congenital Cardiology team look after a spectrum of patients, from teenagers transitioned from the paediatric cardiology clinics, to young adults and increasingly, elderly patients with other traditional age related co-morbidities.
The team consists of 3 funded WTE Consultant ACHD consultants, and 2 Interventional Cardiologists whose workload is 50% ACHD patients. The service has a network of outpatient clinics covering Leicester at Glenfield Hospital, and the wider East Midlands with clinics in Derby, Nottingham, Kingsmill, Kettering, Peterborough and Lincoln in a hub and spoke fashion. These clinics also have established links with obstetric colleagues for pregnant women with cardiac disorders and with the specialist pulmonary hypertension services at Papworth and Royal Hallamshire Hospitals. The team also works closely with congenital cardiac surgical colleagues at EMCHC who care for patients across the age ranges. The ‘paediatric’ interventional cardiologists more accurately should be described as paediatric and congenital interventional cardiologists as they are fully trained across the whole life age range and hence are able to deliver the catheterisation programme for adults with congenital heart disease as well. As such, there is a seamless service from fetal to adult congenital cardiology, with doctors and surgeons contributing to patient care across the age range. Communication between the sub-teams is vital for this to work and the whole department comes together twice a week in the formal multi-disciplinary team meeting to ensure that there is full agreement to the major clinical decisions. Ad hoc and emergency MDT discussions are facilitated when necessary with full compliance to an appropriate quorate of clinical specialities.
Also vital are the transition ACHD liaison nurses who provide a link between clinicians and patients, being a less formal point of contact and a ready of source of advice, information and support
EMCHC has strong links with the other teams required to deliver holistic cardiac care including the radiology department, the echocardiography department (a specialist echocardiography team sits within EMCHC), general adult cardiology, the coronary care unit, the intensive care unit, the Clinical Genetics Department and others. The service plans to foster and develop clinical research and build a centre of national and international repute for adult congenital heart disease.
5.1.3 Interventional Cardiology Interventional cardiology provides a non-surgical method for treating significant congenital heart disease. It is a rapidly expanding area, overtaking surgery as therapy in many cases. Catheter based procedures can often be done without the need for admission to ITU and prolonged recovery periods are avoided. Some patients are discharged on the day of their procedure; most are discharged the following morning.
Included within this field is diagnostic catheterisation, which provides the invasive haemodynamic assessment necessary for planning surgery and other management.
UHL have three full time consultant CHD interventionists and have recruited a fourth who is expected to start in Q2 2019/20. In the interim the service is supported by a number of visiting (contracted) consultants whose activity contributes towards the minimum activity requirements for EMCHC and forms part of their individual activity log combined with work carried out in their main centre of employment. Once the new consultant starts employment there will be no requirement for the visiting consultant cover.
East Midlands Congenital Heart Operational Policy Page 15
Paediatric Cardiac Electrophysiology is provided by a Consultant who is jointly employed by UHL and BCH with sufficient PA’s to cover the required caseload. Adult Cardiac Electrophysiology is performed by an Adult Consultant employed at UHL primarily focussing on adult cardiac patients and providing sufficient Adult EP lists to meet demand
Current Interventional catheter activity meets the standards requirements. A fourth Consultant Interventionist will be employed when activity reaches a level where all four Consultants can meet the minimum activity standards which is expected to be in 2020/21
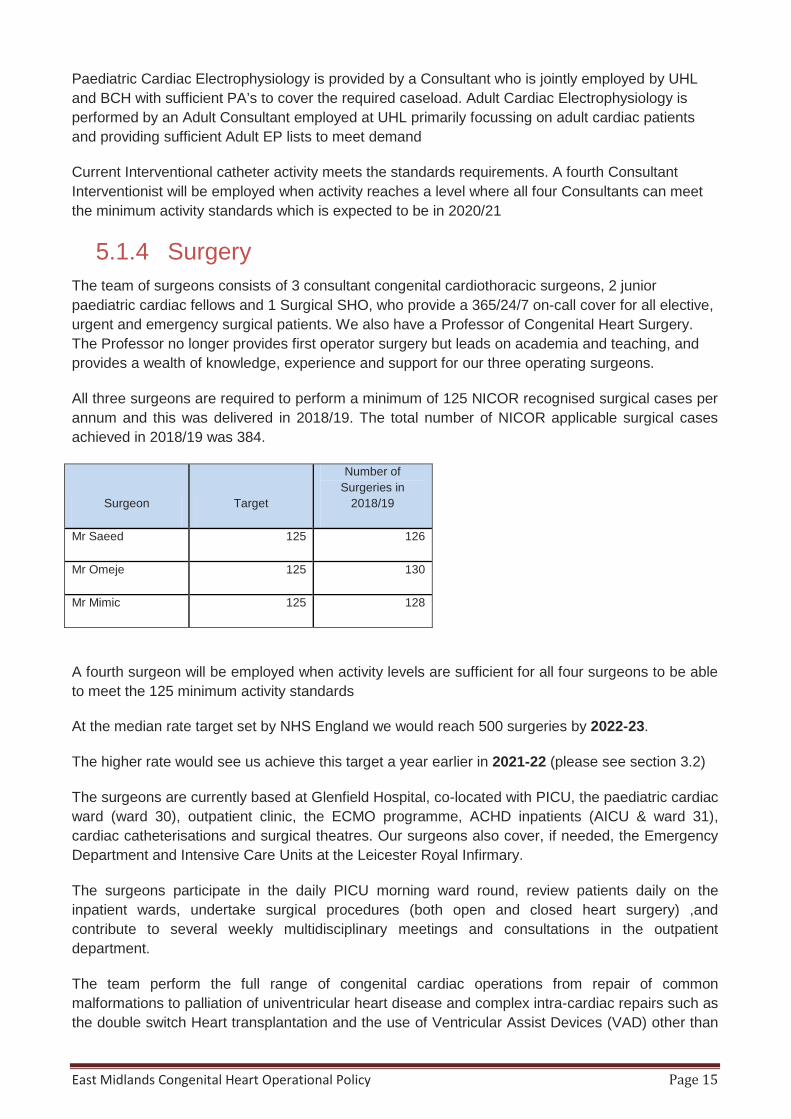
5.1.4 Surgery The team of surgeons consists of 3 consultant congenital cardiothoracic surgeons, 2 junior paediatric cardiac fellows and 1 Surgical SHO, who provide a 365/24/7 on-call cover for all elective, urgent and emergency surgical patients. We also have a Professor of Congenital Heart Surgery. The Professor no longer provides first operator surgery but leads on academia and teaching, and provides a wealth of knowledge, experience and support for our three operating surgeons.
All three surgeons are required to perform a minimum of 125 NICOR recognised surgical cases per annum and this was delivered in 2018/19. The total number of NICOR applicable surgical cases achieved in 2018/19 was 384.
Surgeon Target
Number of Surgeries in
2018/19
Mr Saeed 125 126
Mr Omeje 125 130
Mr Mimic 125 128
A fourth surgeon will be employed when activity levels are sufficient for all four surgeons to be able to meet the 125 minimum activity standards
At the median rate target set by NHS England we would reach 500 surgeries by 2022-23.
The higher rate would see us achieve this target a year earlier in 2021-22 (please see section 3.2)
The surgeons are currently based at Glenfield Hospital, co-located with PICU, the paediatric cardiac ward (ward 30), outpatient clinic, the ECMO programme, ACHD inpatients (AICU & ward 31), cardiac catheterisations and surgical theatres. Our surgeons also cover, if needed, the Emergency Department and Intensive Care Units at the Leicester Royal Infirmary.
The surgeons participate in the daily PICU morning ward round, review patients daily on the inpatient wards, undertake surgical procedures (both open and closed heart surgery) ,and contribute to several weekly multidisciplinary meetings and consultations in the outpatient department.
The team perform the full range of congenital cardiac operations from repair of common malformations to palliation of univentricular heart disease and complex intra-cardiac repairs such as the double switch Heart transplantation and the use of Ventricular Assist Devices (VAD) other than

East Midlands Congenital Heart Operational Policy Page 16
ECMO are not included in the surgical portfolio at Glenfield. Joint working and referral pathways can be found in Appendix C.
The surgical team also deals with airways problems and chest malformations in paediatric patients, frequently in conjunction with the paediatric general and thoracic surgeons based at Leicester Royal Infirmary.
5.1.5 Intensive Care Paediatric Intensive Care in Leicester is currently run as a single unit on two sites, the Paediatric Cardiac and ECMO Intensive Care on the Glenfield Hospital site, part of EMCHC, and the Children’s Intensive Care and High Dependency Unit (CICU and HDU) on the Leicester Royal Infirmary site. This ethos of a single unit on two sites is practically reinforced by close staff links at all levels across town. The medical registrars are part of the paediatric middle grade rota for the East Midlands Deanery and the Paediatric consultant Intensivist provide 24-hour cover for both sites. A rotation for nursing staff through both units is well established.
The ten paediatric Intensivists are responsible for the safe management of patients on the intensive care unit, and for providing support for emergency care to children elsewhere within the EMCHC. This service is consultant delivered, supported by a team of senior trainees in paediatrics and experienced Advanced Nurse Practitioners.
The Unit provides the full range of PIC interventions, including high frequency ventilation, Nitric Oxide therapy, ECMO (in conjunction with the Heartlink ECMO service), renal replacement therapy and others. We submit data to the PICANet national audit database, and the unit has a strong emphasis on multi-disciplinary team-work including organisational structures to optimise patient safety and high quality outcomes.
Adult patients of EMCHC will receive their post-operative recovery on the adult intensive care unit (AICU) at the Glenfield Hospital. Currently there are 22 fully equipped bed spaces on the unit; this is set to increase up to 28 as part of the UHL reconfiguration plans. As well as supporting the emergency admissions at the GH, AICU looks after patients from Cardiac, thoracic, Vascular and Breast surgery. AICU also provide adult ECMO and is the only service that offers mobile ECMO in the country.
5.1.6 Anaesthetics The team of dedicated 3 consultant congenital anaesthetists provide 24 hour anaesthetic support for both paediatric and adult congenital cardiothoracic surgery, diagnostic / interventional cardiology and CT/MRI imaging. A fourth Consultant has been recruited and is due to commence work in May 2019. The service is also in the process of establishing a MTI post for a Consultant from India who will start once all visa applications have been completed
The team also supports general anaesthetic colleagues at other UHL sites for expert assistance with non-cardiac surgery on congenital patients including the 2-3 specialist obstetric deliveries performed at Glenfield Hospital each year. The anaesthetists form a key part of the EMCHC multidisciplinary team. They work particularly closely with surgical colleagues, Cardiologists and Intensivists and their expert contribution can significantly improve outcomes for patients.
The congenital anaesthetic team believe in the importance of maintaining an up to date, cutting edge service, and regularly visit other centres to compare techniques and learn new trends so that they can continue to grow and improve. The team are also members of an international network

East Midlands Congenital Heart Operational Policy Page 17
who can, via an e-mail forum, (CCAN- Cardiac congenital anaesthetic network) seek or deliver help and advice between experts regarding difficult or unusual cases.
The consultant Anaesthetists are supported by a dedicated team of congenital operating theatre practitioners and a dedicated physical measurements technician, as well as excellent office manager support.
The service also offers a Senior Clinical fellow in congenital cardiothoracic anaesthesia post. This is a highly significant post and one of only a few in the UK. This further enhances the service’s reputation and also makes it easier to integrate clinical research into the team’s practice, building specialist training and delivering a service with national and international recognition.
5.1.7 Imaging The Radiology department plays an integral role in diagnostic work up and surveillance of patients with congenital heart disease across the East Midlands. This provides a comprehensive imaging service from fetus to old age. Patients are referred for various specialised imaging modalities, including cardiac magnetic resonance imaging and computed tomography. The service has a Consultant Cardiac Imaging specialist who is responsible for both Cardiac MRI and CT supported by a team of specialised radiologists who are trained in congenital imaging. The cardiac radiographers provide high quality images with the newly acquired scanners, which include the Aera 1.5T Siemens MRI scanner and the Siemens Somatom Definition FLASH CT scanner. The administrative staff and radiographer assistants ensure that the patients are well informed about the entire process.
Regular clinical radiological meetings take place to allow close interaction between radiologists and clinicians as cases are discussed and images reviewed. The team also provide an inpatient cardiac imaging service for acutely unwell patients who require urgent intervention and treatment. The department works in close collaboration with both the paediatric and adult congenital clinical team to provide an efficient, streamlined service.
There is a central electronic echo and radiology imaging server with ability for all service clinicians to access echo and radiology imaging at all times and locations and even from home.
5.2 Associated Health Professionals 5.2.1 Perfusion
Perfusionists are an integral part of the Paediatric Cardiothoracic theatre team. Their main responsibilities revolve around supporting the patient on a Heart Lung machine while they have their corrective Cardiac surgery. We have a team of ten and are trained in both Adult and Paediatric Perfusion techniques. Paediatric Cardiac surgery that needs Bypass cannot go ahead without a Perfusionist. We are integral to the East Midlands Congenital Service.
We also have an input into Infant and Paediatric ECMO support. We are responsible for setting up and priming the ECMO circuit and putting the patient on ECMO helping the ECMO cannulator to achieve this. ECMO is an important part of the East Midlands Congenital Service and offers Respiratory and post Cardiac support to Neonatal and Paediatric patients that need it.

East Midlands Congenital Heart Operational Policy Page 18
5.2.2 Congenital Echocardiography EMCHC have highly specialised physiologists who hold BSE and EAE accreditation in Adult and Paediatric Congenital echocardiography, currently performing and reporting up to 9000 Echo`s a year for both outpatients and inpatients.
We provide support and training in house and for the Network in the following ways:
• Telephone support
• Staff attending our clinics for one to one training
• Attendance to the network clinics to provide support and training for physiologists until no longer required.
• Provide a separate physiology meeting alongside the Network bi annual training meeting to discuss standardisation, guidelines and training.
• Provide supervisors for both medical and technical staff for EAE accreditation.
5.2.3 Physiotherapy The role of Physiotherapy within EMCHC is to provide respiratory assessment and treatment as well as neurological development, rehabilitation, mobility and assisting with discharge planning. The respiratory assessment and treatment is important to diagnose and treat respiratory problems and facilitate the flow of patients from PICU to Ward.30 and then home. This includes aiding secretion clearance and treating decreased lung volumes as well as positioning to support a child’s respiratory and developmental status. The team also provide exercise tolerance education and teaching for patients and their families to ensure they continue to progress once home. This service is provided Monday to Friday 8:30 – 4:30. There is a reduced service at weekends which focuses mainly on improving a child’s respiratory status, and an on-call service overnight for emergency respiratory physiotherapy.
5.2.4 Occupational Therapy The Occupational Therapist works alongside the Physiotherapy Team on PICU and on Ward 30. The Occupational Therapist works with premature/new-borns babies through to teenagers to help them engage in their everyday occupations such as play, exploration, feeding and self-care, in line with their development and age. The Occupational Therapist will provide assessment and treatment to support developmental needs, physical and mental health and well-being. Developmental input begins from birth onwards, assessing the new-borns capacity to interact with their environment, early sensory development and how the child is coping with their environment, through to meeting their development milestones. The Occupational Therapist may provide seating and specialist equipment if clinically indicated, provision of splinting as required and liaison with community services in preparation for discharge. This service is provided Monday to Friday 8 – 4, unfortunately there is no weekend Occupational Therapy service.

East Midlands Congenital Heart Operational Policy Page 19
5.2.5 Psychology The Paediatric Psychology service offers a systematic, high quality specialist clinical psychology services to patients within general acute and community paediatric services, enhancing access to psychological treatment and intervention as an integrated part of their care. The Paediatric Psychology Service manages the psychological aspects of chronic illness in the children in both inpatient and outpatient and community environments with responsibilities including:
• Assessment and intervention with children and families. • Liaison with schools and other community-based professionals working with children. • Staff training for paediatric staff. • Consultation, joint working, support and provision of psychological advice and
treatment. • Supervising and supporting the clinical members of the specialist paediatric team who
provide psychologically based care and treatment as appropriate. • Working within professional guidelines and exercising responsibility for the systematic
supervision of psychological practice within the service. • Utilising research skills for audit, policy and service development and research. • Ensuring the provision of liaison and effective team work with staff from paediatric
services, community health and education as appropriate. If the child has a mental illness as a parallel illness, develops a more severe mental health presentation or has a presentation which is a somatic presentation (i.e. a physical presentation of psychological distress) then a referral will be made to Specialist CAMHS
Adult CHD patients who have not been part of the transition process have access to the LPT clinical psychology. The responsible Adult cardiologist can refer using the pathway available on the trusts in site page. The EMCHN Board are sighted to the requirements for Adult Psychology services in the Network, and this forms part of the 2019/20 work plan for the Network.
5.2.6 Therapies / Dietetics EMCHC has 1x WTE UHL band 7 Senior Specialist Dietitian, dedicated to Cardiology and Paediatric Intensive Care. EMCHC also has an additional 0.2 WTE UHL band 6 Senior Dietitian allocated to Paediatric Cardiology as part of their training rotation.
The dedicated EMCHC Dietitian covers PICU patients, referred patients from the children’s ward, and referred Leicestershire outpatients. The band 6 WTE Senior Dietitian assists with the children’s ward caseload.
As many inpatients are discharged from EMCHC into neighbouring counties, the role involves regular liaison with the Paediatric Dietitians in the neighbouring counties. In addition to this, the EMCHC Dietitian regularly provides peer support and clinical supervision to the Paediatric Dietitians in the neighbouring counties (in East Midlands) when they are managing cardiac patients from their own areas.
The Dietitian also represents EMCHC at Paediatric Cardiology Interest Group (PCDIG) meetings, to contribute to the formation of consensus statements and deliver consistent UK practice across all of the major cardiac centres.
East Midlands Congenital Heart Operational Policy Page 20
5.3 Nursing 5.3.1 Network Lead Nurse
The Lead Nurse for the East Midlands Congenital Heart Network (EMCHN) is responsible for the provision and delivery of a high standard of care to children and adults with congenital heart disease providing professional and clinical leadership to multi-professionals working across the network. They work alongside the Network Manager and Clinical Director to ensure quality of services across the East Midlands ensuring patients and their families have equitable access to services throughout the network.
The lead Nurse is responsible for leading the development and implementation of high quality, evidenced based clinical standards across the EMCHN. They will develop productive working relationships and practices across the network, working in partnership with other relevant agencies and organisations offering advice and provide support to all centres providing CHD care in the EMCHN.
The Lead Nurse will develop dedicated competency based training specific to the Network Centres and ensure a development training programme is in place for CHD nurses and nurses with an interest in CHD across the network as per the Network Training Strategy. (See Appendix C/ sub appendix 19)
This role will contribute specific clinical nursing expertise to the EMCHN team to ensure the implementation of the strategy for CHD care. They will work with the Network Manager to coordinate the set up and running of a Clinical Governance Framework which will assure the EMCHN Board of high quality service provision. The post holder will provide positive communication and sharing of clinical information (guidelines and policies) between Network hospitals and primary care as per the EMCHN Joint Referral and Care Document (See Appendix C / sub appendix 20)
5.3.2 Outpatient Nurses Outpatient nurses undertake baseline observation and take blood tests when required. Assist the consultant in clinic during consultation. Chaperone patients during tests and investigation such as echocardiogram, cardiac echo, stress test etc. Give advice and support to patients and their families as required, ensure that patients are seen in a timely manner and are kept up to date with delays that may impact on the patient and family experience.
Outpatient Nurses ensure follow up appointments are booked when required and ensure that the clinic is run efficiently and effectively with a focus on infection prevention, patient safety and wellbeing at all times.
5.3.3 Specialist (Cardiac Liaison) Cardiac Liaison Nurses support patients and families in their journey through NHS services providing advice, information and support. For some, this can be as brief as a single outpatient review but for others, Liaison Nurse Involvement can start with fetal diagnosis and continue throughout a patient’s lifetime. Liaison Nurses ensure patients and families are given the right information in a way that they can understand in order to help inform their decision making for on-going treatment. They are a point of contact for all patients and families, including offering an email service and helpline support. They ensure continuity of care, information and support, to work as the key worker for patients. They work closely with consultants at the base hospital and also in

East Midlands Congenital Heart Operational Policy Page 21
network clinics to ensure that there is continuity of care for patients and families and that the same standards of care, support, advice and information are available in all settings. They support staff in other hospital to deliver care to patients and families with newly diagnosed or on-going cardiac conditions and treatments.
End of life, palliative care and bereavement support is provided through the Cardiac Liaison team who act as an initial point of contact for the patients/ carers with whom they have established strong relationships. They will signpost and arrange referral to specialist bereavement and palliative care services when required following the UHL protocols and guidance.
They act as a resource for staff at Glenfield in the peripheral hospitals, Allied Healthcare Professionals, Education and Social Care in supporting staff education and communication concerning key issues in a patients diagnose and on-going treatment.
2018/19 staffing provision for Cardiac Liaison Nurses is as follows:
Paediatric – 4.25 WTE (2 WTE vacancy)
Adult - 3.8 WTE (1 WTE vacancy)
Within these numbers there is a designated Fetal Nurse specialist, Transition Nurse Specialist, and Nurse Educator. Recruitment and budget is in place to bring the CLN staffing up to the full requirements dictated by the CHD standards (7WTE Paediatric and 5 WTE Adult) for the financial year 2019/20 with a plan to incorporate support workers and a development post for in house staff.
5.3.4 Ward Nursing Ward 30 specialises in the care of children with a variety of cardiac conditions. Some patients are admitted for scheduled cardiac surgery and there are also children coming in for diagnostic and interventional cardiac procedures. We also have children who may require regular observation for a period of time, for example, if they have changes to medication.
The ward has seventeen beds arranged over two bays and several side rooms. Two of the beds are designated for high dependency patients and two of the side rooms are situated in our adolescent area.
The Nursing team is made up of Registered Children’s Nurses, Associate Nurses and Healthcare Assistants. We also have the support of a designated ward clerk and housekeeper. We facilitate student nurses on placements from University as well as provide in house training for registered nurses.
The ward forms part of Leicester Children’s Hospital which is currently based on 2 sites, Glenfield and Royal Infirmary. Nursing staff keep close links with each other and offer staff rotations as well as helping each other on a shift basis if required. All nursing staff attends cross site training and joint meetings to further promote teamwork. There are plans to relocate Glenfield on to the Infirmary site in a bespoke Children’s hospitable December 2020 after which the ward will benefit from the close proximity of all other children’s services.
5.3.5 Play therapists EMCHC has qualified Play Specialists in our intensive care, ward and outpatient settings who work as part of the multidisciplinary team.

East Midlands Congenital Heart Operational Policy Page 22
The role of a Play Specialist is to organise, initiate and supervise specialised play which is appropriate to a baby or child’s development and medical condition. They will assess individual needs and provide appropriate play activities either at the bedside or in the ward playroom.
They are also experienced in preparation and distraction play techniques which will support children in preparing for, during and following procedures as required.
The role of the Play Specialist on PICU is to provide developmental care and specialised play for patients from birth to 18 years of age. Our aim is to use an individualised approach of positive touch, containment holding, emotional support or guidance, and facilitate play activities to encourage positive interaction and continuation of emotional attachments alongside physical, cognitive, emotional and social development.
This also helps reduce anxiety, agitation and stress levels in patients and parents and increases the patients’ tolerance of different interventions. We use specialised play, preparation and distraction techniques to increase understanding and cooperation as well as building coping techniques for procedures, whilst general play can bring an element of normality and enjoyable experiences to a highly stressful environment

East Midlands Congenital Heart Operational Policy Page 23
5.3.6 PICU/Transport The PICU nursing team consists of a team of band 5, 6 and 7 nurses who provide a nurse to patient ratio of 1:1 for Intensive care nursing and 1:2 for high dependency care as defined by the paediatric intensive care standards. Skill mix ratios are not standardised, however it is referenced that, as a minimum, each shift requires a band 7 Sister / Charge nurse who is experienced and qualified in caring for sick cardiac children requiring intensive care. Each shift requires at least two band 6/7 nurses to undertake shift leadership and retrieval. As the transport team is currently integrated within the PICU team, individuals are allocated for transport duties on a daily basis. The service works on a 24/7 basis retrieving extremely sick babies and children requiring cardiac surgery, cardiology diagnosis/intervention or Extra Corporeal Membrane Oxygenation (ECMO). Retrievals are mainly within the East and West Midlands but can be from anywhere in the UK and sometimes from Europe
EMCHC works closely with the Children’s Medical Emergency Transport (CoMET) Service. Commissioned in 2017, the service provides:
• An acute critical care transport team operating 24/7/52 with capacity to advise on the management of critically ill children who present to an East Midlands Hospital, stabilise them and transport them to an appropriate PCC facility, in line with NHS England Standards and recognised best practice. Using a dedicated call handling service, CoMET Clinicians conference in Cardiologists and Surgeons from EMCHC to provide expert advice where appropriate.
• A repatriation team operating weekdays and during daytime hours only, to safely transport patients to or from PCC facilities, where the level of dependency does not require the full transport service. This will most commonly be ‘back transfers’ to the referring hospital at the end of an episode of critical illness. The purpose of this service is to enable the most efficient use of expensive and pressurised PCC beds, to deliver care to patients in the most appropriate surroundings, and as close to home as possible. This includes the transfer of patient from EMCHC to level 2 units or paediatric wards.
• Outreach advice and training to East Midland’s hospitals in the initial care and stabilisation of acutely ill children, recognising that this improves outcomes and may reduce the need for intensive care admission. This service is provided in line with NHS England Standards and recognised best practice.
The transport team undertake acute transfers, Level 3 repatriations to intensive care facilities nearer the patient’s home where appropriate and support level 2 transfers where necessary. Much transport team time is spent providing advice on resuscitation and stabilisation, managing referral logistics and supporting DGHs with advice around non-PIC transfer cases, as well as in-house and outreach training.
The service also offers mobile ECMO for patients who have deteriorated to a point where standard intensive care transport is no longer an option. COMET does not offer mobile ECMO – This is provided and co-ordinated by the ECMO team using ECMO Specialists and trained PICU Nurses.
In addition to the PICU nursing team, on-going education is essential in an environment that is highly specialised and high tech. Newly qualified nurses require increased depth of understanding of anatomy and physiology, as well as developing core intensive care knowledge and skills. Therefore the service has a fulltime Nurse Educator as an essential addition to the PICU team.
East Midlands Congenital Heart Operational Policy Page 24
5.3.7 ECMO The ECMO service is a national commissioned service for the treatment of babies and children requiring respiratory and cardiac support where conventional means of treatment have failed. The nursing requirements vary from patient to patient. Stable non-complicated ECMO patients require 1:1 care, which is the normal standard within in intensive care. Unstable or complex patients may require two nurses to look after them safely.
Patients require 24/7 care with a focus on continuous observations management of sedation, pain relief, respiratory support, renal support, pain control, systemic support with inotropes and vaso-dilators where required and nutritional requirements. ECMO nursing care will also include support for the family and involving parents in the care of their child where appropriate.
ECMO nurses take part in the ECMO on-call rota and in the coordination of the daily running of the service as well as participating in the mobile ECMO transport service in conjunction with medical and perfusion staff.
5.4 Management and Administration 5.4.1 Management Triumvirate
The General Manager and Head of Operations are directly responsible for the administrative team, and in partnership with the Head of Service / Clinical Lead and Matron, for the day to day running of the service with oversight from the head of nursing. This triumvirate is responsible for the operational performance and strategic development of the service, which includes accountability for delivery of high quality patient care, patient safety, clinical quality and financial performance.
5.4.2 Data and Outcomes Analyst The Data and outcomes analyst is an integral part of the management team and supports the strategic direction of the service by producing robust information and analysis. They are responsible for all information management systems within EMCHC, alongside providing critical reports to support the overall performance management process. He is supported by a data assistant both of whom are responsible for the timely and accurate uploading of data for National Audit purposes.
5.4.3 Administration The administrative team are managed by the Administration Team Leader, and comprise clinic coordinators who arrange appointments and prepare and run the Glenfield outpatient clinics, medical secretaries who support the consultant’s clinical workload and patient administration, and audio typists who provide an in-house transcription service for clinical correspondence.
We have a designated fetal administration team who manage referrals from Maternity services within the Trust and across the Network. This designated team ensure that all fetal anomaly scan referrals are seen by a fetal medicine cardiologist within 2 working days.
A summary of total workforce numbers current and future budgeted can be found in Appendix A
East Midlands Congenital Heart Operational Policy Page 25
6 The East Midlands Congenital Heart Network
The Network is hosted by University Hospitals of Leicester and is governed by a Board which has representatives from across the Level 1 centre and the Level 3 centres across the East Midlands, including clinicians, nurses, associated healthcare professionals, managers, patients and parents and commissioners. An informal Network has been in place for many years, however formal governance and process was established in July 2018 following confirmation of EMCHC being retained as a Level 1 CHD surgical centre. NHS England issued direction for the establishment of the Network which was supported by a CQUIN. The inaugural Board meeting was held on the 3rd October 2018 where the Terms of Reference were agreed. We are still awaiting confirmation regarding whether the Network will be managed as an Operational Delivery Network, if this is agreed the Terms of Reference and current governance structure will be amended. An interim Annual report was produced in December 2018, with a full year report to be published in July 2019.
6.1.1 Network Board Membership At the Board meeting in January 2019 the following roles were elected and ratified by the Board.
Co-Chairs – Chris Pallot, Director of Strategy and Partnerships Northampton General Hospital and Stephanie Smith, Consultant Emergency Paediatric Consultant, Nottingham Children’s Hospital Champion Nottingham University Hospitals
Clinical Director – Aidan Bolger, Head of Service EMCHC
Network Manager – Alison Poole, Senior Manager Special Projects UHL
Network Lead Nurse – vacant – position in recruitment - Interim Anna Duke, Head of Nursing
Network Administrator – Wendy Miller UHL
Network Charity - Keep the Beat
Network Associated Healthcare Profession Leads – Deb Ip – Senior Chief Cardiac Physiologist UHL, Chaitrita Dhagia - Cardiac Physiologist NUH
Up to 2 Named representatives from each Level 3 centre to include Adult Paediatric and Fetal colleagues
In addition to the designated roles membership includes
NHS England Specialised Commissioning, Patient Parent groups and Charities, Maternity and Psychology clinicians
East Midlands Congenital Heart Operational Policy Page 26
6.1.2 Governance The Network is a member of the Children’s Operational Performance, Quality and Safety Board at University Hospitals of Leicester NHS Trust. It will provide regular updates to that Board, including progress updates, risk and issue management. Board members are encouraged to support, check and challenge the Network on any of its activities, and may escalate any issues as deemed necessary through the Women’s and Children’s performance meetings which reports into the Trust’s Senior Leadership Team meeting, chaired by the Chief Executive Officer.
The Network Board meets three times a year with membership drawn from across the network. The Board will form sub-groups or task and finish groups as required for specific pieces of work Membership and the objective of the groups will be agreed by the Main Network Board. The Board will also consider the need for Patient involvement and ensure representation is appropriate.
The Terms of Reference can be found in Appendix C (Sub Appendix 20) All Board papers can be found on http://www.eastmidlandscongenitalheart.nhs.uk/our-network/governance/board-papers/
6.1.3 Network Audit and Monitoring As part of the CHD standards, the Network needs to establish governance and reporting structure. Whilst individual providers are still responsible for reporting and acting upon incidents and risks locally, the Network reporting structure must ensure that learning can be shared across institutions and that the Network can support if multi-provider intervention is required. The structure must also give a clear route of escalation to the Network and then to commissioners should organisations be unable to effectively mitigate risks or address incidents internally.
As a starting point a full review has been completed of the waiting times from referral to Multi-Disciplinary Meetings (MDT) and then surgery and these metrics will be recorded and reported to the Board three times a year. The use of the new Zoom technology for MDT discussions allows Network colleagues to join in our Quality, MDT and M&M meetings where there is discussion and broader learning from incidents and events.
The areas that will be monitored and reviewed are;
o Clinical and patient outcomes o Reviewing national outputs including: o Benchmarking against other services o Results/progress of annual audits o Data outputs such as (SSQDs, VLAD plots) o Reviewing run rates and waiting times o PREM feedback and analysis.
A dashboard with this information will be reviewed as an agenda item at each Board meeting with an appropriate action plan. Development and progression of the audit and monitoring process are within the work plans for the network.
East Midlands Congenital Heart Operational Policy Page 27
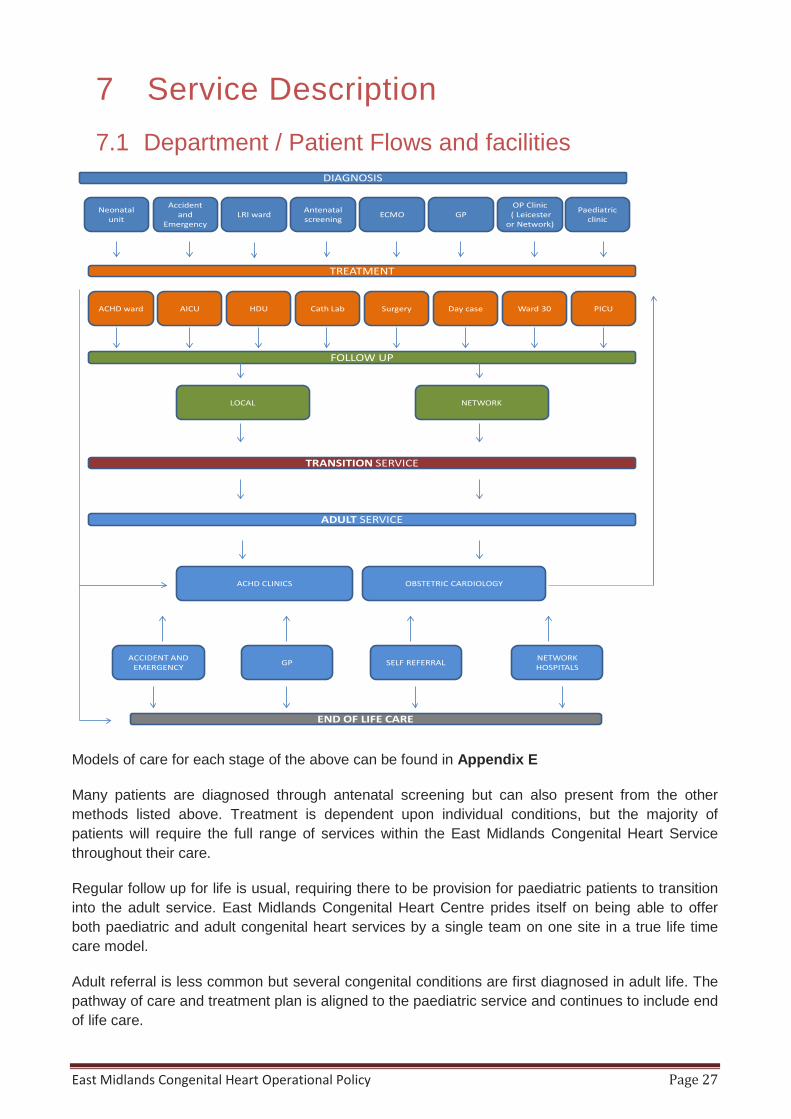
7 Service Description 7.1 Department / Patient Flows and facilities
Models of care for each stage of the above can be found in Appendix E
Many patients are diagnosed through antenatal screening but can also present from the other methods listed above. Treatment is dependent upon individual conditions, but the majority of patients will require the full range of services within the East Midlands Congenital Heart Service throughout their care.
Regular follow up for life is usual, requiring there to be provision for paediatric patients to transition into the adult service. East Midlands Congenital Heart Centre prides itself on being able to offer both paediatric and adult congenital heart services by a single team on one site in a true life time care model.
Adult referral is less common but several congenital conditions are first diagnosed in adult life. The pathway of care and treatment plan is aligned to the paediatric service and continues to include end of life care.
Neonatal unit
Accident and
EmergencyLRI ward Antenatal
screening ECMO GPOP Clinic( Leicester
or Network)
Paediatric clinic
DIAGNOSIS
TREATMENT
ACHD ward AICU HDU Cath Lab Surgery Day case Ward 30 PICU
FOLLOW UP
NETWORKLOCAL
TRANSITION SERVICE
OBSTETRIC CARDIOLOGYACHD CLINICS
ADULT SERVICE
ACCIDENT AND EMERGENCY GP SELF REFERRAL NETWORK
HOSPITALS
END OF LIFE CARE
East Midlands Congenital Heart Operational Policy Page 28
7.2 Patient pathways and information Patient pathways are available to view on the East Midlands Congenital Heart website at http://www.eastmidlandscongenitalheart.nhs.uk/our-centre-of-excellence/patient-pathways/ these pathways signpost patients, parents and carers to what to expect at each stage of the care pathway and where they can receive help and support. There is also a video for patients / parents showing the journey from diagnosis in pregnancy through to adult care and the services available at EMCHC available at; http://www.eastmidlandscongenitalheart.nhs.uk/our-centre-of-excellence/
We have an active task group that includes patient representatives that is focussing on how we improve our patient pathway and support information. The objective of this group is to increase the reach of this information through our social media and online channels.
The full range of patient pathway documents can be found in Appendix
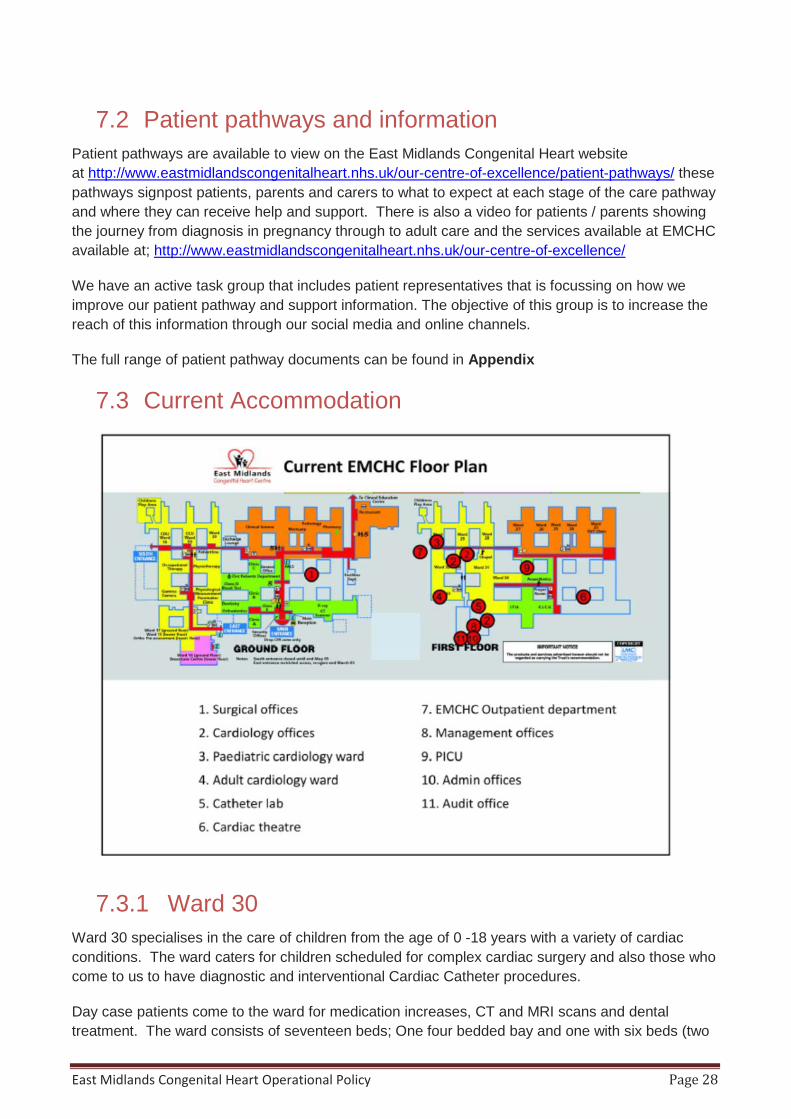
7.3 Current Accommodation
7.3.1 Ward 30 Ward 30 specialises in the care of children from the age of 0 -18 years with a variety of cardiac conditions. The ward caters for children scheduled for complex cardiac surgery and also those who come to us to have diagnostic and interventional Cardiac Catheter procedures.
Day case patients come to the ward for medication increases, CT and MRI scans and dental treatment. The ward consists of seventeen beds; One four bedded bay and one with six beds (two

East Midlands Congenital Heart Operational Policy Page 29
of which are for high dependency patients). We have seven side rooms (one of which is an isolation room) and a designated adolescent area with two side rooms and a range of game consoles, a widescreen television and games and books – ideal for our teenage patients.
There are two play areas for patients and siblings on ward 30 with two dedicated play therapists to support all patients and those with learning difficulties. Age appropriate facilities are available in these areas and mobile sensory equipment is available in treatment rooms and by the bedside.
7.3.2 Parents accommodation (Ward and PICU) There is a parent’s kitchen with fridge, microwaves, kettles and facilities for parents to store and cook fresh food on both ward 30 and our PICU. Both the ward and PICU have a lounge area for parents to relax in as well as a separate quiet room for confidential discussions with staff.
Where possible, when a mother with a baby is admitted to the ward, they will be accommodated in a side room if clinically appropriate to enable mother and baby to be together. There are parent accommodation rooms available to allow parents to be with their child for those not in a side room. Facilities to support breastfeeding and storage of breast milk are accommodated via our children’s ward.
The service has 13 dedicated rooms for parents to stay 24/7 to be close to their child whilst in hospital. These have been kindly funded and equipped by one of our Charity partners – Heart Link who also provided the parents facilities on the ward. Where possible we encourage use of the rooms provided but will also facilitate pull down beds or reclining chairs in the side rooms if preferable to the parents/ carers.
7.3.3 Outpatients The EMCHC outpatient department is situated on the first Floor Glenfield Hospital next to Ward 30. Currently the space is shared between adult and paediatric CHD patients with designated clinics to ensure appropriate age related services. The clinical space within this department includes:
5 Consult/Exam Rooms 3 Echo Rooms 1 Stress Test Room/ Analysis Room 1 ECG Room/ Treatment Room 1 Weights and Measures Room 1 Psychology / Interview Room 1 Audiology/ Hearing Booth
The waiting room has age appropriate facilities, including a play area and adolescent space. There is also access to baby change and breast feeding facilities.
Once the paediatric service collocates with Children’s services Adult CHD outpatients will remain in these facilities with designated clinics appropriate to demand.
7.3.4 ICU Paediatric Intensive Care in Leicester is currently run as a single unit on two sites, the Paediatric Cardiac and ECMO Intensive Care on the Glenfield Hospital site (part of EMCCHN) and the Children’s Intensive Care and High Dependency Unit on the Leicester Royal Infirmary site. This ethos of a single unit on two sites is practically reinforced by close staff links at all levels across town. The Paediatric intensive care consultants provide 24-hour cover for both sites, including
East Midlands Congenital Heart Operational Policy Page 30
resident consultant cover for EMCHC; medical registrars are part of the paediatric middle grade rota for the East Midlands Training Rotation. A rotation for nursing staff through both units is well established. The HeartLink ECMO Centre is also situated at the Glenfield Hospital PICU, one of three supra-regional ECMO centres in England undertaking neonatal, paediatric and adult ECMO. The service also retrieves neonates and children for ECMO from throughout England and Wales, either by road or by helicopter. This is currently separate from CoMET, the regional retrieval service. The Glenfield Hospital benefits from a dedicated helicopter pad.
The scope of the Paediatric Intensive Care Services in Leicester is:
1. Glenfield Hospital Twelve ICU beds for Cardiology/Cardiothoracic Intensive Care and ECMO, currently seven beds staffed and funded.
2. Leicester Royal Infirmary Six intensive care and two high dependency beds in the CICU, currently six beds staffed and funded. There are also flexible HDU (level 2 Critical Care) beds on the adjacent twelve-bedded Respiratory ward.
The two units are three miles apart, and normally there is a consultant paediatric intensivist based at each unit.
There are approximately 900 admissions to the intensive care units a year. Admissions and discharges are agreed by the on-service Paediatric Intensivist and Nurse in charge, in conjunction with other members of the EMCHC team and referring/accepting clinicians
Adult ICU is provided via the AICU at Glenfield. Currently there are 22 fully equipped bed spaces on the unit; this is set to increase up to 33 as part of the UHL reconfiguration plans.
7.3.5 Adult wards Adult CHD in patients are looked after on Ward 31 (Adult Cardiac Surgery, Cardiac Catheterisation), 32, 33, and 28 (Adult Cardiology) at Glenfield Hospital. For patients with learning difficulties facilities are provided for one parent/ carer to stay by the bed in a side room when possible. Accommodation for families for all other adult CHD patients is provided in hospital accommodation on site which has kitchen facilities, or local hotels within 5 minutes’ walk. We provide portable fridge and TV/ DVD facilities for young adults with or without learning difficulties accommodated on an adult ward.
Where possible when a mother with a baby is admitted to the Adult ward, they will be accommodated in a side ward if clinically appropriate to enable mother and baby to be together. Midwifery support is available daily and facilities to support breastfeeding and storage of breast milk are accommodated via our children’s ward.
7.3.6 Multi-Disciplinary Team facilities EMCHC has a dedicated MDT room that provides video conferencing facilities between our Network partners and EMCHC. This practical solution called ‘Zoom’ is a cost effective cloud based video conferencing solution with easy to use interface, is cross platform compatible and has good screen sharing ability. This allows the peripheral teams to participate in one on one video discussions or a group type conference (like our regular MDT, Quality, and Morbidity & Mortality
East Midlands Congenital Heart Operational Policy Page 31
meetings) and remotely view / share echocardiogram images, review cross sectional imagery, view electronic records and communicate to colleagues via audio and video.
Zoom will also work from any device including mobile phone, laptops, desk top, and VC rooms etc. This facility reduces the Information Governance issues associated with file transfer; facilitated consensual screen sharing enables users to view information without actually data transfer.
The facility can be used not only by the clinical teams as above , we have utilised it for ECHO training and will be using it as an integral part of the competency based nurse education programme we are launching as part of our education and training strategy (See Appendix C sub appendix 20 )
Network Board meetings are made available to those unable to attend via this facility.
7.3.7 Cardiac Theatres EMCHC has exclusive access to Theatre 1 at Glenfield for Adult and Paediatric surgical cases. Complex cases are also performed in an additional Cardiac Theatre. Where demand dictates weekend lists are facilitated to ensure the capacity meets the phased expectations of the NHS England Board report November 2017. The additional activity requirements for 2020/21 will be met by the provision of an additional Cardiac Hybrid Theatre once the service relocates to join the rest of Children’s Services at the Leicester Royal Infirmary. Details of this can be found in section 8.
7.3.8 Catheter Lab EMCHC has exclusive access to Cath Lab every Tuesday (2 sessions), Friday (2 sessions) and the 1st & 3rd Wednesday of the month (1 sessions am). A range of diagnostic and interventional procedures are performed by the team with full GA (general anaesthesia) on both days. EMCHC utilise Cath lab B due to the fact the X-ray equipment installed offers bi-plane functionality which is integral to the procedures carried out. The lab spec is detailed below.
• Allura Xper 10/10 Biplane • MacLab (cardiac catheterisation monitoring system) • Ampere RF generator (RF Ablation Generator) • Carto 3 system (Cardiac Electrophysiology Analysis system) • Ensite Velocity (Cardiac Mapping System)
East Midlands Congenital Heart Operational Policy Page 32
7.4 Inter dependencies The new standards dictate the following specialities or services must be located on the same site as the Specialist Children’s Surgical Centre. They must function as part of a Multi-Disciplinary team, and Consultants must be able to provide emergency bedside care from call within 30 minutes
Paediatric cardiology
Paediatric Airway team (capable of complex airway management)
PICU – level 3 paediatric critical care services
HDU- level 2 high dependency beds
Specialise paediatric anaesthesia
Post-operative extra corporeal membrane oxygenation (ECMO). This is distinct from the nationally commissioned ECMO support for respiratory patients
CT MRI scanning
Full range of cardiac physiological investigations to include ECG, Holter monitoring, ECHO
CPEX testing
Isotope imaging
Catheter intervention
Electrophysiological intervention
Pacemaker insertion and extraction
Cardiac surgical intervention
Specialist Adult Congenital Heart Surgery and intervention
Paediatric surgery
Paediatric Nephrology/ Renal replacement Therapy
Vascular surgery
Adult cardiology interventionist
Paediatric Gastroenterology
Paediatric physiotherapy
The current service provision works as a multi-disciplinary team and does meet the 30 min requirement for access to all of the services listed. Plans to co locate with other children’s services are well established. The service will move into the new facilities detailed in Section 8 by December 2020.
7.5 Non Clinical Support Services IT Porter service, catering, linen, domestic service, maintenance, security, fire procedure & waste management are provided by UHL Facilities Management Service and are outside the remit of this operational policy
East Midlands Congenital Heart Operational Policy Page 33
8 EMCHC website The EMCHC website can be found at http://www.eastmidlandscongenitalheart.nhs.uk/. It provides accessible information to patients, families, carers, Health professionals and UHL staff. The site navigation is split into three sections
I. Our services– this section introduces our team and provides information on what we do, resources on CHD conditions and treatments, links to resources to support patients, parents and carers through the service and the third sector. It’s key objective is to be a one stop shop for advice and information to our patients and families
II. Our Network – this section focusses on the Network and the hospitals there in It provides Health care professionals from the network access to guidance documents for referral and care , it provides the governance documents for the Network with our Annual report, work plan , and all board papers being available to down load. It is anticipated that the competency based training plan we are piloting this year with two Network Hospitals will be housed on this section of the website giving Health Care professionals access to all relevant Network information.
III. Our Future – this section focusses on the plans for the service moving forward. It gives details of the project to co locate Children’s services into a single Children’s Hospital and the plans for adult services at Glenfield once the move has happened. It is an essential section of the website for both patient and staff to keep them informed of the exciting times ahead
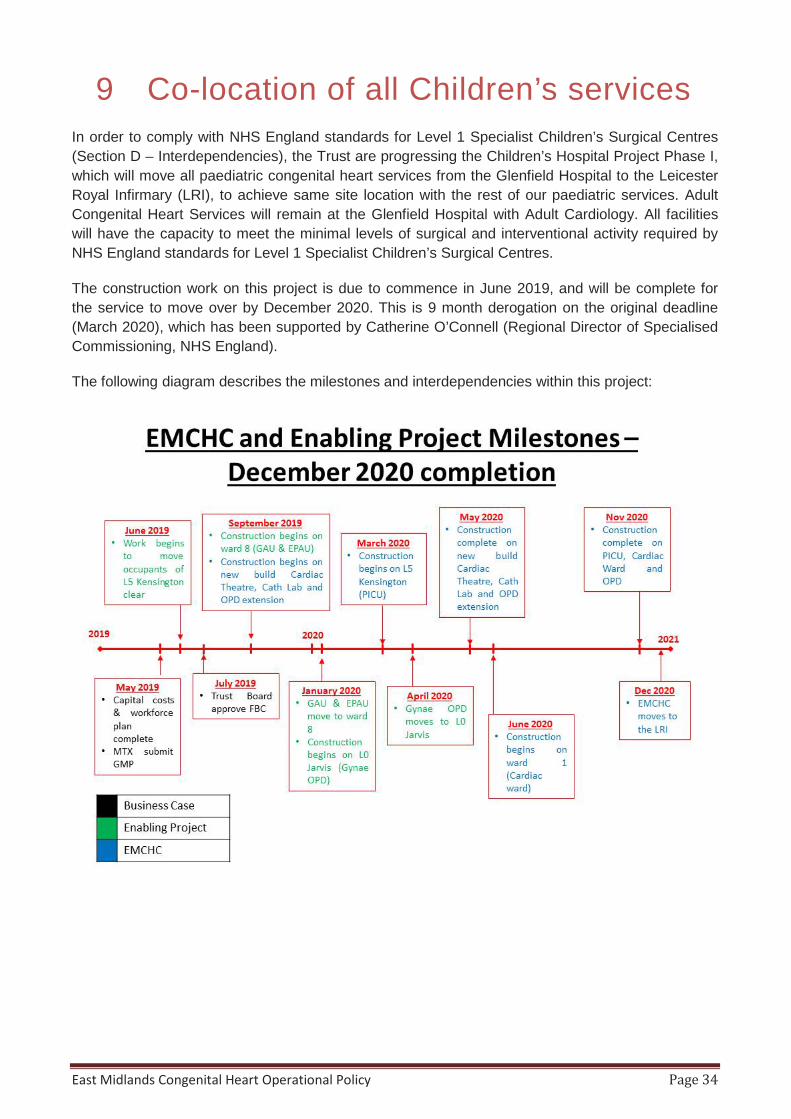
East Midlands Congenital Heart Operational Policy Page 34
9 Co-location of all Children’s services In order to comply with NHS England standards for Level 1 Specialist Children’s Surgical Centres (Section D – Interdependencies), the Trust are progressing the Children’s Hospital Project Phase I, which will move all paediatric congenital heart services from the Glenfield Hospital to the Leicester Royal Infirmary (LRI), to achieve same site location with the rest of our paediatric services. Adult Congenital Heart Services will remain at the Glenfield Hospital with Adult Cardiology. All facilities will have the capacity to meet the minimal levels of surgical and interventional activity required by NHS England standards for Level 1 Specialist Children’s Surgical Centres.
The construction work on this project is due to commence in June 2019, and will be complete for the service to move over by December 2020. This is 9 month derogation on the original deadline (March 2020), which has been supported by Catherine O’Connell (Regional Director of Specialised Commissioning, NHS England).
The following diagram describes the milestones and interdependencies within this project:
East Midlands Congenital Heart Operational Policy Page 35
9.1 Paediatric Cardiac Ward A newly refurbished 17 bed paediatric Cardiac Ward will be situated on Level 1 of the Kensington Building. All paediatric congenital heart patients requiring an inpatient or day case bed will be treated on this ward. Three of the beds will have the medical gases and funded nurses to provide High Dependency (HD) Care, as they step down from the new Paediatric Intensive Care following surgery.
The ward will be designed to provide age appropriate care for congenital heart patients; with an adolescent area for older patients (including a game station, books and magazines, etc.) and a large play area for younger patients. Age appropriate facilities are a fundamental aspect of all space designed for children and young people. The ward will have the environment in order to accommodate all patients up to their 19th birthday, therefore must include age appropriate accommodation for babies and infants (0-4), paediatrics (5-12) and teenagers and young adults (13-18+364 days). Design must ensure that sections of each ward have the appearance and layout aligned to the age of patient – areas which will predominately be used by babies and infants should be designed to maximise observation, whilst areas for teenagers and young adults should be designed with heightened levels of privacy and dignity in mind.
The design of the space will also take into account the particular needs of children and young people with any learning or physical disability.
The Children’s Hospital School will provide support to children of school age who are staying on the ward.
9.2 Parent Facilities Parent/Carer bedrooms will be provided, both on the ward (pull down beds in all side rooms, plus four parent/carers bedrooms) and a short walk away at the Walnut Street accommodation complex.
On both on the ward and the PICU, there will be a parents/carers lounge/kitchen, with facilities to make simple meals and drinks, and a quiet room.
Heartlink will continue to offer support to all parents and carers of congenital heart patients. In order to facilitate this, they will have an office on the Cardiac Ward, and will use the parents/carers lounge to meet with the families of those on the ward and PICU.
9.3 Paediatric EMCHC Outpatient Department The new paediatric EMCHC outpatient department will be situated on the Ground Floor of the Kensington Building. The clinical space within this department will include:
6 Consult/Exam Rooms 4 Echo Rooms 1 Stress Test Room 1 Reporting Room 1 ECG Room 1 Weights and Measures Room 1 Treatment/Venepuncture Room 1 Pacing and Tape Room 1 Interview Room
East Midlands Congenital Heart Operational Policy Page 36
The waiting room will have age appropriate facilities, including a play area and adolescent space. There will also be access to baby change and breast feeding facilities.
9.4 Paediatric Intensive Care Unit (PICU) The 12 bed Paediatric Intensive Care Unit (PICU) will be located on Level 5 of the Kensington Building, and will provide the space for care of pre and post-operative patients requiring Level 3 critical care, as well as those patients on ECMO.
The unit has been designed to include 8 beds in a large bay, 2 side rooms/cubicles (1 with simulation facilities) and two negative pressure isolation rooms.
9.5 Multi-Disciplinary Team (MDT) Facilities The MDT room will be located on the Ground Floor of the Kensington Building, and will be networked to allow multi-site video conferencing MDT meetings. This room will be of adequate size to allow staff from across the service and network to attend the MDT meetings if appropriate.
9.6 Congenital Heart Theatre and Cath Lab Department A New Build Cardiac Theatre and Cath Lab Department will be built immediately adjacent to the Kensington Building at the LRI to facilitate paediatric surgical and interventional procedures.
The Cardiac Theatre will be the primary operating theatre for paediatric surgical cases. The Cath Lab will provide the location for catheter intervention, EP intervention and pacemaker insertion and extraction. In addition to this, it will be fitted with the ventilation, equipment and facilities to allow cardiac surgical intervention (hybrid catheter/surgical treatment) where clinically indicated.
9.7 Children’s Hospital Project Phase II The plans to move the paediatric EMCHC to the Kensington Building form the first phase of the wider Children’s Hospital Project. Phase II (which is a part of the Trust’s wider Reconfiguration Plans) will move all paediatric services from elsewhere on the Leicester Royal Infirmary site into the Kensington Building, to form the only standalone Children’s Hospital in the East Midlands.
East Midlands Congenital Heart Operational Policy Page 37
10 Patient Feedback Mechanisms We continually strive to improve upon the service our patients and their families experience to meet their expectations. Patient feedback is vital for us to achieve this and we currently have three feedback systems in place to enable us to collate this: Message to Matron cards - these are readily available in all of our patient areas to provide a quick and easy way for patients and carers to provide messages, feedback, suggestions for improvement and to identify any staff they wish to acknowledge/thank to our Matrons. These are reviewed and shared at our weekly QUICKA meeting. Patient Experience Survey - this is a Trust wide survey which incorporates the national Friends & Family test. National Congenital Heart Disease Survey - Patient Reported Experience Measures (PREMS) This method of collating patient experience is established in the healthcare arena, but relatively ne for CHD services. There are separate surveys for inpatient and outpatient and for different age groups: - A parent/carers survey aimed primarily at parent/careers of infants and young children - A child patient experience survey - An adult patient experience survey for the older child, young person or adult This is an online survey which can be accessed via www.chdpatientssurvey.co.uk any time after an inpatient stay or outpatient appointment. The information is collated, analysed and reported on by NHS England and provides us with both an overview of patient experiences nationally, how we compare whilst identifying areas/themes for improvement and recognising what you makes a positive experience.
Increasing access to and completion of this survey is important to the EMCHC team, work to find innovative and easily accessible routes to completion are part of the 2019/20 work plan.
11 Equality and Diversity The Trust recognises the diversity of the local community and those in its employ. Our aim is, therefore, to provide a safe environment free from discrimination and a place where all individuals are treated fairly, with dignity and appropriately to their need. The Trust recognises that equality impacts on all aspects of its day-to-day operations and has produced an Equality Policy Statement to reflect this. All policies are assessed in accordance with the Equality initial screening toolkit, the results for which are monitored centrally.
12 Review This policy will be reviewed to meet the requirements of the new EMCHC facilities co located with other children’s services. Earlier review may be required in response to exceptional circumstances, organisational change or relevant changes in legislation of guidance’.

East Midlands Congenital Heart Operational Policy Page 38
13 Training and Awareness The Operational Policy for EMCHC will form part of the mandatory induction process for all new starters.
The revised policy will be disseminated to existing staff by line management and referenced during 121 sessions and annual appraisals to ensure full awareness and understanding of iterations and changes.
Performance management assessments will include the compliance of staff to the Operational Policy
14 Disaster recovery plan EMCHC adheres to the UHL Trust wide Major Incident and Business Continuity Plans in the event of any incident that threatens the provision of the service.
There are currently 3 surgeons – workload is covered in times of leave and illness through sharing of workload internally and close liaison with network colleagues
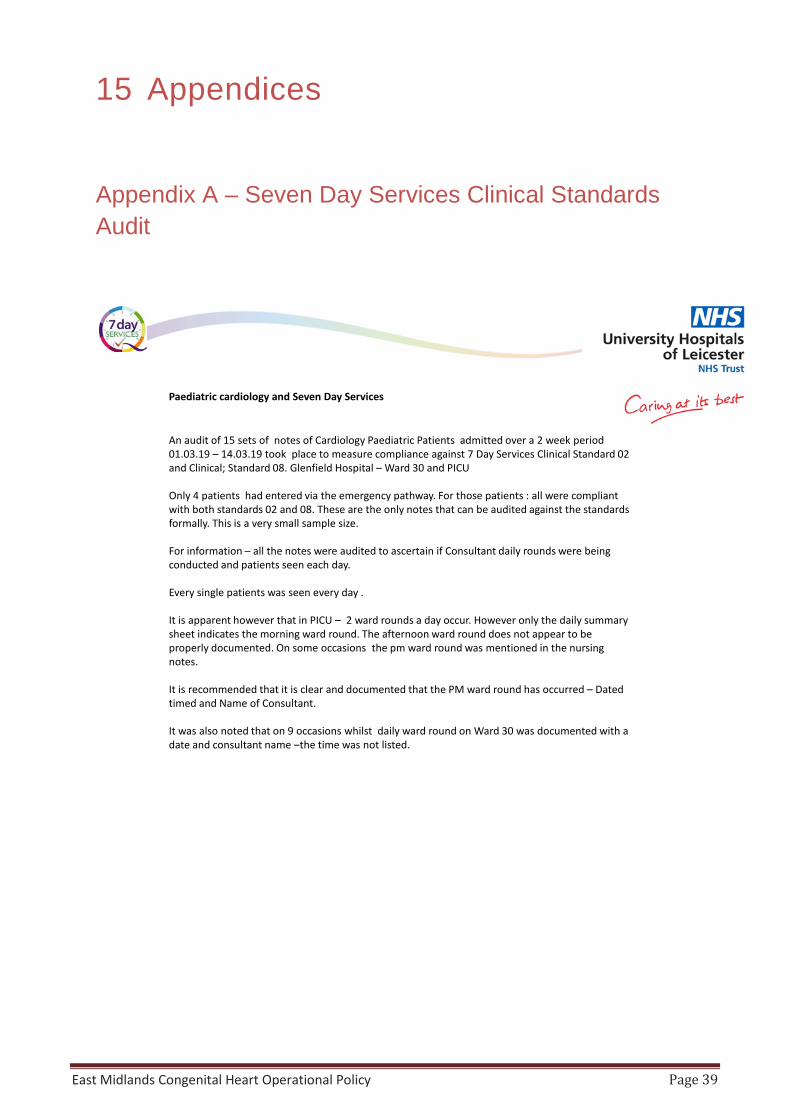
East Midlands Congenital Heart Operational Policy Page 39
15 Appendices
Appendix A – Seven Day Services Clinical Standards Audit
Paediatric cardiology and Seven Day Services
An audit of 15 sets of notes of Cardiology Paediatric Patients admitted over a 2 week period 01.03.19 – 14.03.19 took place to measure compliance against 7 Day Services Clinical Standard 02 and Clinical; Standard 08. Glenfield Hospital – Ward 30 and PICU
Only 4 patients had entered via the emergency pathway. For those patients : all were compliant with both standards 02 and 08. These are the only notes that can be audited against the standards formally. This is a very small sample size.
For information – all the notes were audited to ascertain if Consultant daily rounds were being conducted and patients seen each day.
Every single patients was seen every day .
It is apparent however that in PICU – 2 ward rounds a day occur. However only the daily summary sheet indicates the morning ward round. The afternoon ward round does not appear to be properly documented. On some occasions the pm ward round was mentioned in the nursing notes.
It is recommended that it is clear and documented that the PM ward round has occurred – Dated timed and Name of Consultant.
It was also noted that on 9 occasions whilst daily ward round on Ward 30 was documented with a date and consultant name –the time was not listed.
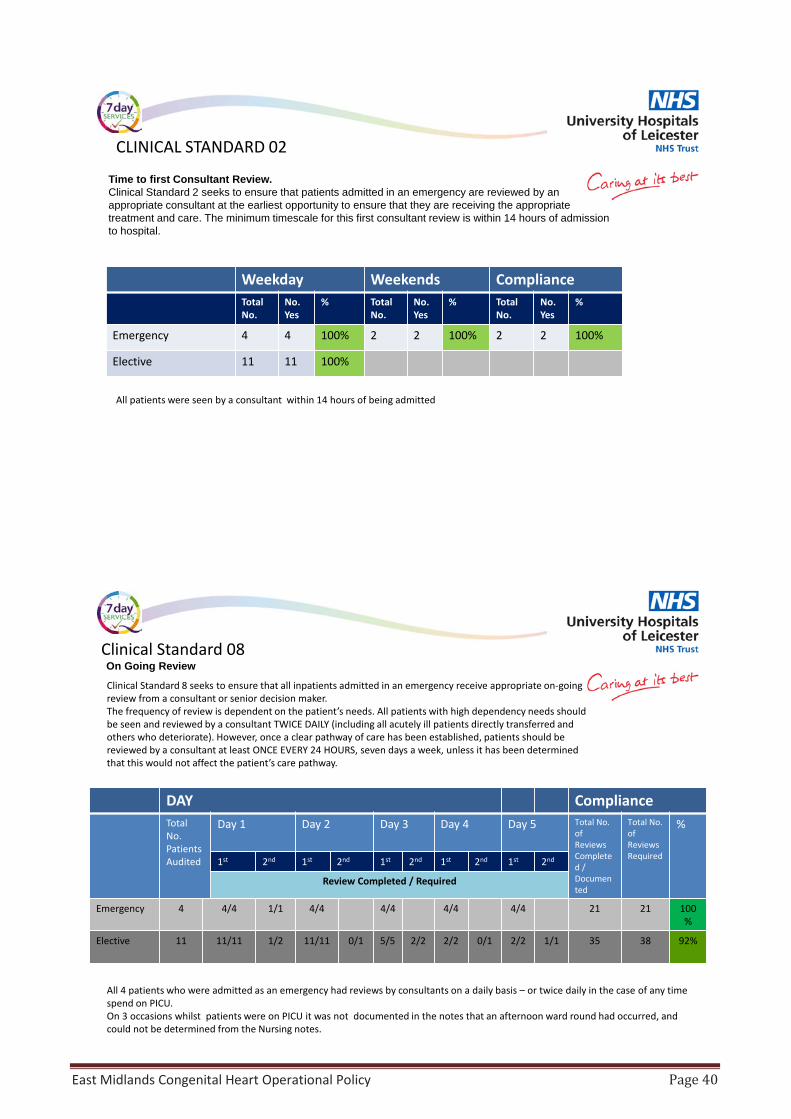
East Midlands Congenital Heart Operational Policy Page 40
Weekday Weekends ComplianceTotal No.
No.Yes
% Total No.
No.Yes
% Total No.
No.Yes
%
Emergency 4 4 100% 2 2 100% 2 2 100%
Elective 11 11 100%
CLINICAL STANDARD 02
Time to first Consultant Review.Clinical Standard 2 seeks to ensure that patients admitted in an emergency are reviewed by an appropriate consultant at the earliest opportunity to ensure that they are receiving the appropriate treatment and care. The minimum timescale for this first consultant review is within 14 hours of admission to hospital.
All patients were seen by a consultant within 14 hours of being admitted
DAY ComplianceTotal No. Patients Audited
Day 1 Day 2 Day 3 Day 4 Day 5 Total No. of Reviews Completed / Documented
Total No. of Reviews Required
%
1st 2nd 1st 2nd 1st 2nd 1st 2nd 1st 2nd
Review Completed / Required
Emergency 4 4/4 1/1 4/4 4/4 4/4 4/4 21 21 100%
Elective 11 11/11 1/2 11/11 0/1 5/5 2/2 2/2 0/1 2/2 1/1 35 38 92%
Clinical Standard 08On Going Review
Clinical Standard 8 seeks to ensure that all inpatients admitted in an emergency receive appropriate on-going review from a consultant or senior decision maker.The frequency of review is dependent on the patient’s needs. All patients with high dependency needs should be seen and reviewed by a consultant TWICE DAILY (including all acutely ill patients directly transferred and others who deteriorate). However, once a clear pathway of care has been established, patients should be reviewed by a consultant at least ONCE EVERY 24 HOURS, seven days a week, unless it has been determined that this would not affect the patient’s care pathway.
All 4 patients who were admitted as an emergency had reviews by consultants on a daily basis – or twice daily in the case of any time spend on PICU.On 3 occasions whilst patients were on PICU it was not documented in the notes that an afternoon ward round had occurred, and could not be determined from the Nursing notes.
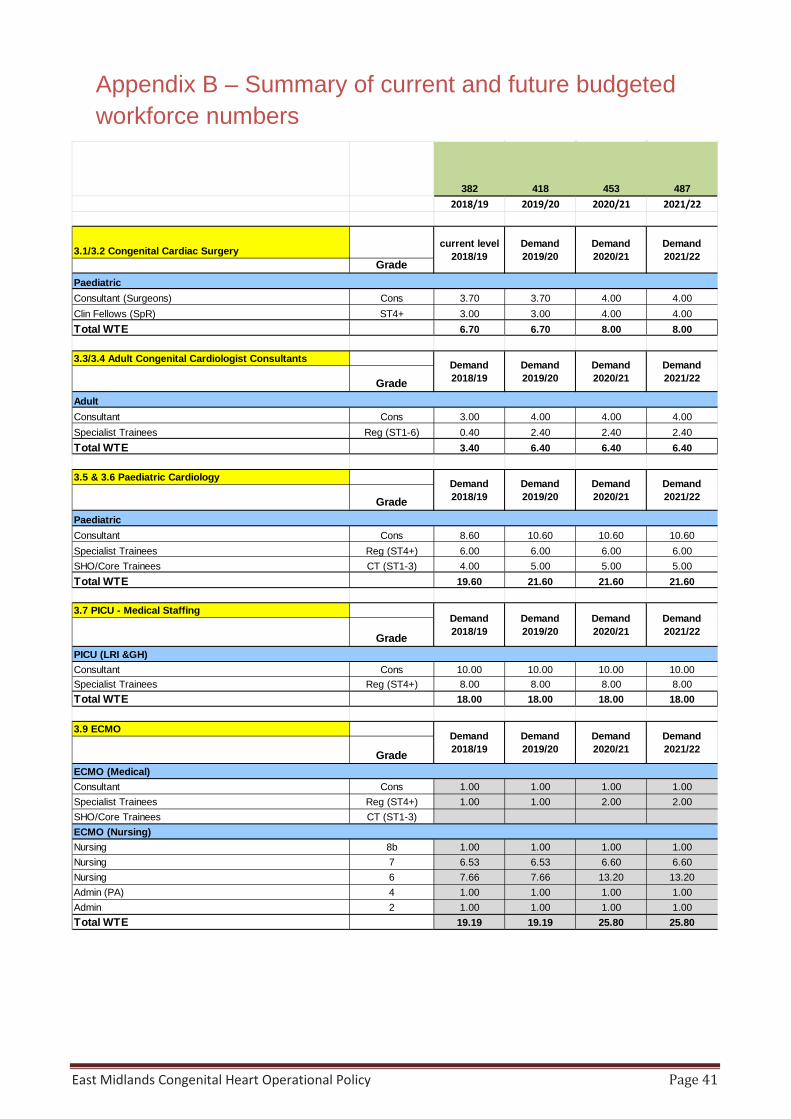
East Midlands Congenital Heart Operational Policy Page 41
Appendix B – Summary of current and future budgeted workforce numbers
382 418 453 4872018/19 2019/20 2020/21 2021/22
3.1/3.2 Congenital Cardiac SurgeryGrade
PaediatricConsultant (Surgeons) Cons 3.70 3.70 4.00 4.00Clin Fellows (SpR) ST4+ 3.00 3.00 4.00 4.00Total WTE 6.70 6.70 8.00 8.00
3.3/3.4 Adult Congenital Cardiologist Consultants
GradeAdultConsultant Cons 3.00 4.00 4.00 4.00Specialist Trainees Reg (ST1-6) 0.40 2.40 2.40 2.40Total WTE 3.40 6.40 6.40 6.40
3.5 & 3.6 Paediatric Cardiology
GradePaediatricConsultant Cons 8.60 10.60 10.60 10.60Specialist Trainees Reg (ST4+) 6.00 6.00 6.00 6.00SHO/Core Trainees CT (ST1-3) 4.00 5.00 5.00 5.00Total WTE 19.60 21.60 21.60 21.60
3.7 PICU - Medical Staffing
GradePICU (LRI &GH)Consultant Cons 10.00 10.00 10.00 10.00Specialist Trainees Reg (ST4+) 8.00 8.00 8.00 8.00Total WTE 18.00 18.00 18.00 18.00
3.9 ECMO
GradeECMO (Medical)Consultant Cons 1.00 1.00 1.00 1.00Specialist Trainees Reg (ST4+) 1.00 1.00 2.00 2.00SHO/Core Trainees CT (ST1-3)ECMO (Nursing)Nursing 8b 1.00 1.00 1.00 1.00Nursing 7 6.53 6.53 6.60 6.60Nursing 6 7.66 7.66 13.20 13.20Admin (PA) 4 1.00 1.00 1.00 1.00Admin 2 1.00 1.00 1.00 1.00Total WTE 19.19 19.19 25.80 25.80
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2019/20
Demand2020/21
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
current level 2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2021/22
Demand2018/19
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
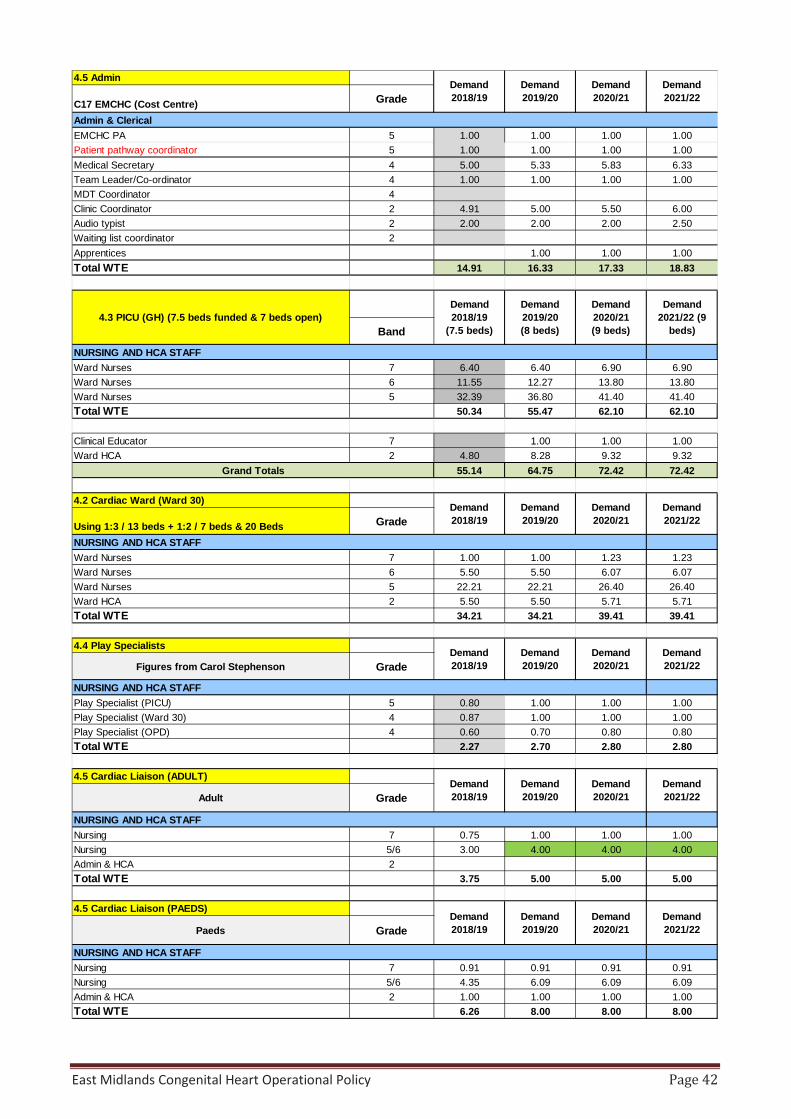
East Midlands Congenital Heart Operational Policy Page 42
4.5 Admin
C17 EMCHC (Cost Centre) Grade
Admin & ClericalEMCHC PA 5 1.00 1.00 1.00 1.00Patient pathway coordinator 5 1.00 1.00 1.00 1.00Medical Secretary 4 5.00 5.33 5.83 6.33Team Leader/Co-ordinator 4 1.00 1.00 1.00 1.00MDT Coordinator 4Clinic Coordinator 2 4.91 5.00 5.50 6.00Audio typist 2 2.00 2.00 2.00 2.50Waiting list coordinator 2Apprentices 1.00 1.00 1.00Total WTE 14.91 16.33 17.33 18.83
Band
NURSING AND HCA STAFFWard Nurses 7 6.40 6.40 6.90 6.90Ward Nurses 6 11.55 12.27 13.80 13.80Ward Nurses 5 32.39 36.80 41.40 41.40Total WTE 50.34 55.47 62.10 62.10
Clinical Educator 7 1.00 1.00 1.00Ward HCA 2 4.80 8.28 9.32 9.32
55.14 64.75 72.42 72.42
4.2 Cardiac Ward (Ward 30)
Using 1:3 / 13 beds + 1:2 / 7 beds & 20 Beds Grade
NURSING AND HCA STAFFWard Nurses 7 1.00 1.00 1.23 1.23Ward Nurses 6 5.50 5.50 6.07 6.07Ward Nurses 5 22.21 22.21 26.40 26.40Ward HCA 2 5.50 5.50 5.71 5.71Total WTE 34.21 34.21 39.41 39.41
4.4 Play Specialists
Figures from Carol Stephenson Grade
NURSING AND HCA STAFFPlay Specialist (PICU) 5 0.80 1.00 1.00 1.00Play Specialist (Ward 30) 4 0.87 1.00 1.00 1.00Play Specialist (OPD) 4 0.60 0.70 0.80 0.80Total WTE 2.27 2.70 2.80 2.80
4.5 Cardiac Liaison (ADULT)
Adult Grade
NURSING AND HCA STAFFNursing 7 0.75 1.00 1.00 1.00Nursing 5/6 3.00 4.00 4.00 4.00Admin & HCA 2Total WTE 3.75 5.00 5.00 5.00
4.5 Cardiac Liaison (PAEDS)
Paeds Grade
NURSING AND HCA STAFFNursing 7 0.91 0.91 0.91 0.91Nursing 5/6 4.35 6.09 6.09 6.09Admin & HCA 2 1.00 1.00 1.00 1.00Total WTE 6.26 8.00 8.00 8.00
Demand2021/22
Demand2021/22 (9
beds)
Demand2021/22
Demand2021/22
Demand2021/22
Demand2021/22
Demand2018/19
Demand2019/20
Demand2020/21
Demand2018/19
Demand2019/20
Demand2020/21
Grand Totals
4.3 PICU (GH) (7.5 beds funded & 7 beds open)Demand2018/19
(7.5 beds)
Demand2019/20(8 beds)
Demand2020/21(9 beds)
Demand2018/19
Demand2019/20
Demand2020/21
Demand2018/19
Demand2019/20
Demand2020/21
Demand2018/19
Demand2019/20
Demand2020/21

East Midlands Congenital Heart Operational Policy Page 43
5.1 Cardiac Investigations
Grade
OTHER ALLIED HEALTH PROFESSIONALSSenior Chief Cardiac Physiologist 8a 1.00 1.00 1.00 1.00Chief Cardiac Physiologist ***** 7 4.66 5.66 6.26 6.26Senior Cardiac Physiologist 6 1.00 2.00 2.00 2.00Cardiac physiologist 5 2.00 2.46 2.46 2.46
Technician – Assistant technical Officer/ Cardiographer 2 1.50 2.50 3.50 3.50Total WTE 10.16 13.62 15.22 15.22
5.4 Perfusion
Grade
PERFUSIONPrincipal Perfusionist/Mgr 8b/c 3.00 3.00 3.00 3.00Senior Perfusionist 8a 5.58 6.58 6.58 6.58Staff Grade Perfusionist 7 1.00 2.00 2.00 2.00Trainee Perfusionist 5 1.00 0 0 0Total WTE 10.58 11.58 11.58 11.58
5.7 Theatre Practitioners (excl. Cath Lab)
Grade
Nursing & ODP & HCAClinical Skills Supervisor 6 1.00 1.00 1.00Deputy Team Leader 6 1.00 1.00 1.00Scrub Practitioner (ODP or Nurse) 5 3.28 8.00 9.26 9.26Anaest Practitioner (ODP or Nurse) 5 4.26 8.00 9.26 9.26Ward HCA 2 1.64 2.64 4.38 4.38Total WTE 9.18 20.64 24.90 24.90
5.6 Cardiac Anaesthetics Consultants
Grade
Medical StaffConsultant Cons 2.61 3.00 4.00 4.00Snr Registrar (ST4+) ST4+ 1.00 1.00 2.00 2.00Registrar (ST 1 - 3) ST1-3Foundation/Core Trainee (FY/CT) FY/CTTotal WTE 3.61 4.00 6.00 6.00
6.1 Pharmacy
Grade
OTHER ALLIED HEALTH PROFESSIONALSPharmacist 8b to 8c 0.00 0.00 0.00Pharmacist 8a 2.00 2.50 2.50 2.50Pharmacist 7 1.50 1.50 1.50 1.50Medicines Management Technician 5 0.50 0.50 0.50 0.50Admin 2 0.50 0.50 0.50Total WTE 4.00 5.00 5.00 5.00
6.2 Physio & OT
Grade / PAs
Physiotherapist 7 1.00 1.00 1.00 1.00Physiotherapist 6 1.00 1.00 1.00 1.00Physiotherapist 5 0.50 1.00 1.00 1.00
Occupational Therapist 6 0.50 1.00 1.00 1.00Occupational Therapist 5 1.00 1.00 1.00Total WTE 3.00 5.00 5.00 5.00
Demand2021/22
Demand2021/22
Demand2021/22
OTHER ALLIED HEALTH PROFESSIONALS
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2021/22
WTE Increased in line with activity growth
Demand2018/19
Demand2019/20
Demand2020/21
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2018/19
Demand2019/20
Demand2020/21
Demand2018/19
Demand2019/20
Demand2020/21
Demand2019/20
Demand2020/21
Demand2018/19
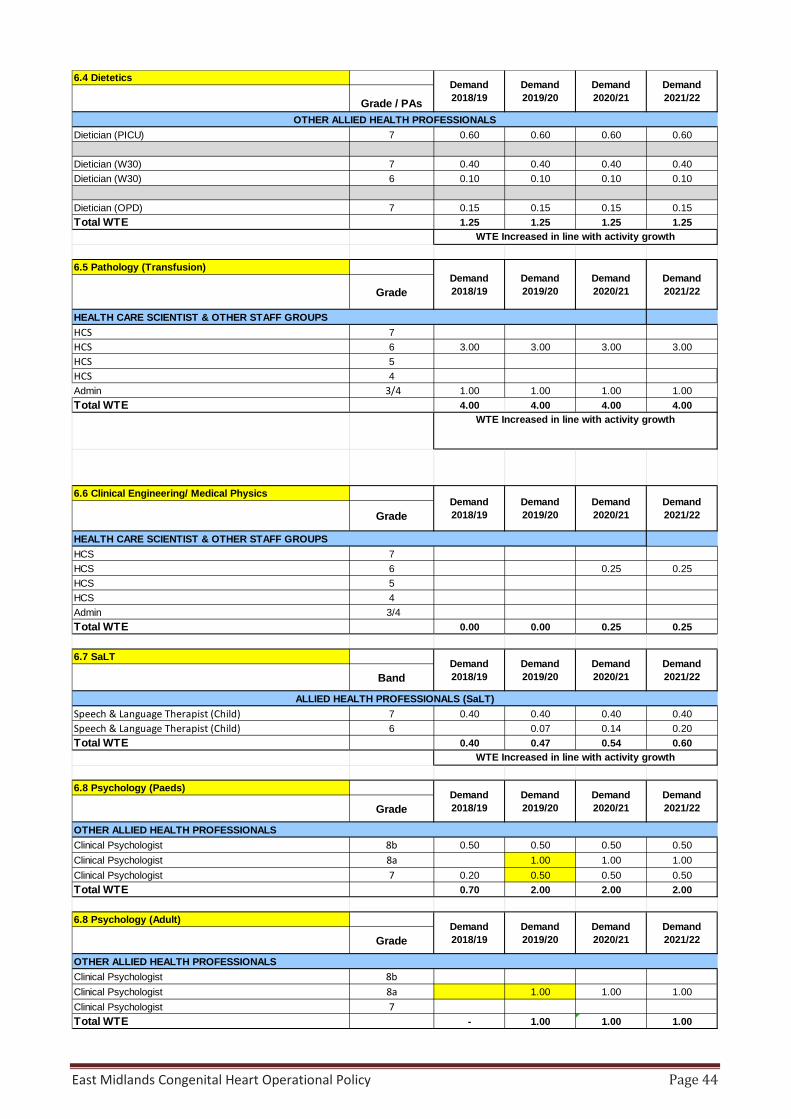
East Midlands Congenital Heart Operational Policy Page 44
6.4 Dietetics
Grade / PAs
Dietician (PICU) 7 0.60 0.60 0.60 0.60
Dietician (W30) 7 0.40 0.40 0.40 0.40Dietician (W30) 6 0.10 0.10 0.10 0.10
Dietician (OPD) 7 0.15 0.15 0.15 0.15Total WTE 1.25 1.25 1.25 1.25
6.5 Pathology (Transfusion)
Grade
HEALTH CARE SCIENTIST & OTHER STAFF GROUPSHCS 7HCS 6 3.00 3.00 3.00 3.00HCS 5HCS 4Admin 3/4 1.00 1.00 1.00 1.00Total WTE 4.00 4.00 4.00 4.00
6.6 Clinical Engineering/ Medical Physics
Grade
HEALTH CARE SCIENTIST & OTHER STAFF GROUPSHCS 7HCS 6 0.25 0.25HCS 5HCS 4Admin 3/4Total WTE 0.00 0.00 0.25 0.25
6.7 SaLT
Band
Speech & Language Therapist (Child) 7 0.40 0.40 0.40 0.40Speech & Language Therapist (Child) 6 0.07 0.14 0.20Total WTE 0.40 0.47 0.54 0.60
6.8 Psychology (Paeds)
Grade
OTHER ALLIED HEALTH PROFESSIONALSClinical Psychologist 8b 0.50 0.50 0.50 0.50Clinical Psychologist 8a 1.00 1.00 1.00Clinical Psychologist 7 0.20 0.50 0.50 0.50Total WTE 0.70 2.00 2.00 2.00
6.8 Psychology (Adult)
Grade
OTHER ALLIED HEALTH PROFESSIONALSClinical Psychologist 8bClinical Psychologist 8a 1.00 1.00 1.00Clinical Psychologist 7Total WTE - 1.00 1.00 1.00
WTE Increased in line with activity growth
WTE Increased in line with activity growth
WTE Increased in line with activity growth
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
ALLIED HEALTH PROFESSIONALS (SaLT)
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
OTHER ALLIED HEALTH PROFESSIONALS
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
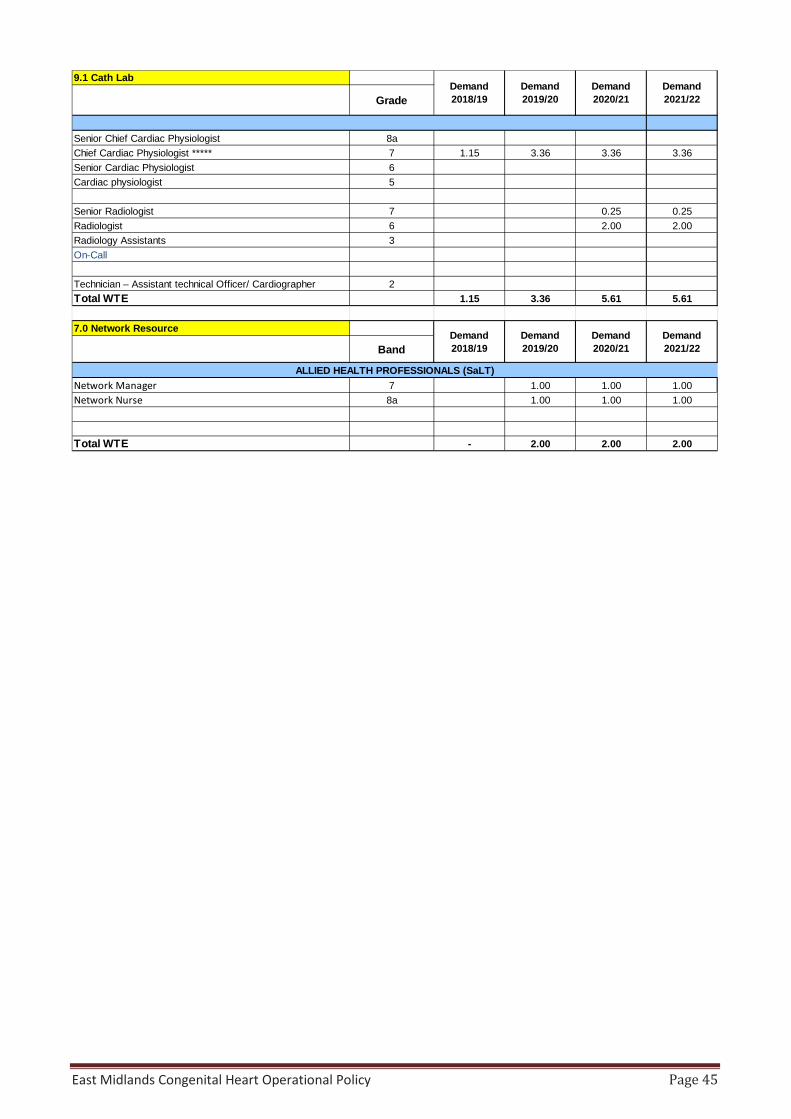
East Midlands Congenital Heart Operational Policy Page 45
9.1 Cath Lab
Grade
Senior Chief Cardiac Physiologist 8aChief Cardiac Physiologist ***** 7 1.15 3.36 3.36 3.36Senior Cardiac Physiologist 6Cardiac physiologist 5
Senior Radiologist 7 0.25 0.25Radiologist 6 2.00 2.00Radiology Assistants 3On-Call
Technician – Assistant technical Officer/ Cardiographer 2Total WTE 1.15 3.36 5.61 5.61
7.0 Network Resource
Band
Network Manager 7 1.00 1.00 1.00Network Nurse 8a 1.00 1.00 1.00
Total WTE - 2.00 2.00 2.00
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
ALLIED HEALTH PROFESSIONALS (SaLT)
Demand2018/19
Demand2019/20
Demand2020/21
Demand2021/22
East Midlands Congenital Heart Operational Policy Page 46
Appendix C – EMCHN Referral and Care guidelines
The East Midlands Congenital Heart Network Joint Referral and Care Guidance documents
East Midlands Congenital Heart Operational Policy Page 47
Approved By: Policy and Guideline Committee (Chair’s urgent approvals process)
Date of Original Approval:
3 April 2019
Trust Reference: E1/2019 Version: 1.0 Supersedes: N/A Trust Lead: Dr Aidan Bolger Board Director Lead: Medical Director – Mr. Andrew Furlong Date of Latest Approval
3 April 2019
Next Review Date: January 2020
East Midlands Congenital Heart Operational Policy Page 48
CONTENTS
Section Page 1 Introduction and Overview 3 2 Policy Scope – Who the Policy applies to and any specific exemptions 3 3 Roles- Who Does What 3 4 Education and Training 3
5 Process for Monitoring Compliance 4 6 Equality Impact Assessment 4 7 Supporting References, Evidence Base and Related Policies 4 8 Process for Version Control, Document Archiving and Review 4
Appendices Page 1 The East Midlands Congenital Heart Network:
Joint Referral and Care Guidance Documents 6
2 The East Midlands Congenital Heart Network Board Terms of Reference 129 3 Definitions and Abbreviations 139
REVIEW DATES AND DETAILS OF CHANGES MADE DURING THE REVIEW This is a new document for approval
KEY WORDS
Congenital Heart Disease, Paediatric Congenital Heart Disease, Adult Congenital Heart Disease, East Midlands Congenital Heart Network
East Midlands Congenital Heart Operational Policy Page 49
1 Introduction and Overview
1.1 This document sets out the University Hospitals of Leicester (UHL) NHS Trust’s Policy and Procedures for Joint referral and care guidelines for Network based clinicians not necessarily employed by UHL NHS Trust, working within the East Midlands Congenital Heart Network
2 Policy Scope –who the policy applies to and any specific exclusions
2.1 The Guidance documents apply to Health Professionals from Network centres across the East Midlands. It also outlines where interaction with UHL staff is required, and the process needed to do this.
2.2 All Health Professionals for whom this policy is intended will require a level of educational and professional standing appropriate to their roles, and that meets the expectations and demands dictated by their employing Network Trust. Where specific training and educational support is needed to help facilitate the referral and care pathway this will be provided by East Midlands Congenital Heart Network via the Training and Educational strategy.
2.3 The guidance document relates to all patients with Congenital Heart Disease from diagnosis in pregnancy through to end of life.
2.4 This policy excludes specific care guidance and policies relating to the individual NHS Trusts within the Network, the responsibility of which lies with those Trusts. Inpatient care at UHL referred to in this document will be governed by the appropriate UHL policy and guideline.
3 Roles – Responsibilities within the organisation (who does what?) An overview of the individual, departmental and committee roles and responsibilities, including levels of responsibility and any education and training requirements :
a) Adult/ Paediatric Congenital Heart Disease Consultant Cardiologists, Consultant Paediatric and Adult Intensivists, Consultant Anaesthetists, Consultant Paediatricians, Consultant Neonatologists, Nursing staff , Clinical Scientists, Clinical Therapists
b) Board Director Lead – Mr Andrew Furlong (Medical Director University Hospitals of Leicester NHS Trust).
c) The policy will be implemented and monitored by The East Midlands Congenital Heart Network (EMCHN) Board. This initial version has been approved by the Clinical Governance Group and will be subject to feedback over the first six months from issue. Feedback will be collated and reviewed by the EMCHN Board. Following this the document will be resubmitted to the policy approval committee for longer term approval.
d) The EMCHN Clinical Governance Group is a delegated sub-group of the EMCHN Board with authority to approve procedures and guidance documents that require review outside of the three times a year Network Board meeting timetable (as part of the EMCHN Terms of Reference), with quorate representation from the East Midlands Network Hospitals and UHL.
East Midlands Congenital Heart Operational Policy Page 50
e) All staff (UHL and Network) needing guidance or clarification on this document should speak to the relevant lead clinician for the area in question, after which they should send any feedback to the EMCHN administrator for review by the Network Clinical Governance Group (CGG). Audit and feedback of the guidance documents is a regular agenda item at EMCHN Board meetings
4 Education and Training Requirements
Please refer to the education and training strategy Appendix 19 of the Associated Document
5 Process for Monitoring Compliance
5.1 These policies will be monitored as per the table below.
6 Equality Impact Assessment 6.1 The Trust recognises the diversity of the local community it serves. Our aim therefore is
to provide a safe environment free from discrimination and treat all individuals fairly with dignity and appropriately according to their needs.
6.2 As part of its development, this policy and its impact on equality have been reviewed and no detriment was identified.
7 Supporting References, Evidence Base and Related Policies
When relevant details of supporting evidence and research will be listed in the document
All guidance and policy complies to the requirements of the Congenital Heart Disease Service Specification https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2016/03/chd-spec-standards-2016.pdf Adult Congenital Heart Disease (ACHD) Service Specification. https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2016/03/achd-spec-2016.pdf
8 Process for Version Control, Document Archiving and Review
Review details are described in the Policy and give details of timescale and who will be responsible for review and updating of the document.
The updated version of the Policy will then be uploaded and available through INsite Documents and the Trust’s externally-accessible Freedom of Information publication scheme. It will be archived through the Trusts PAGL system
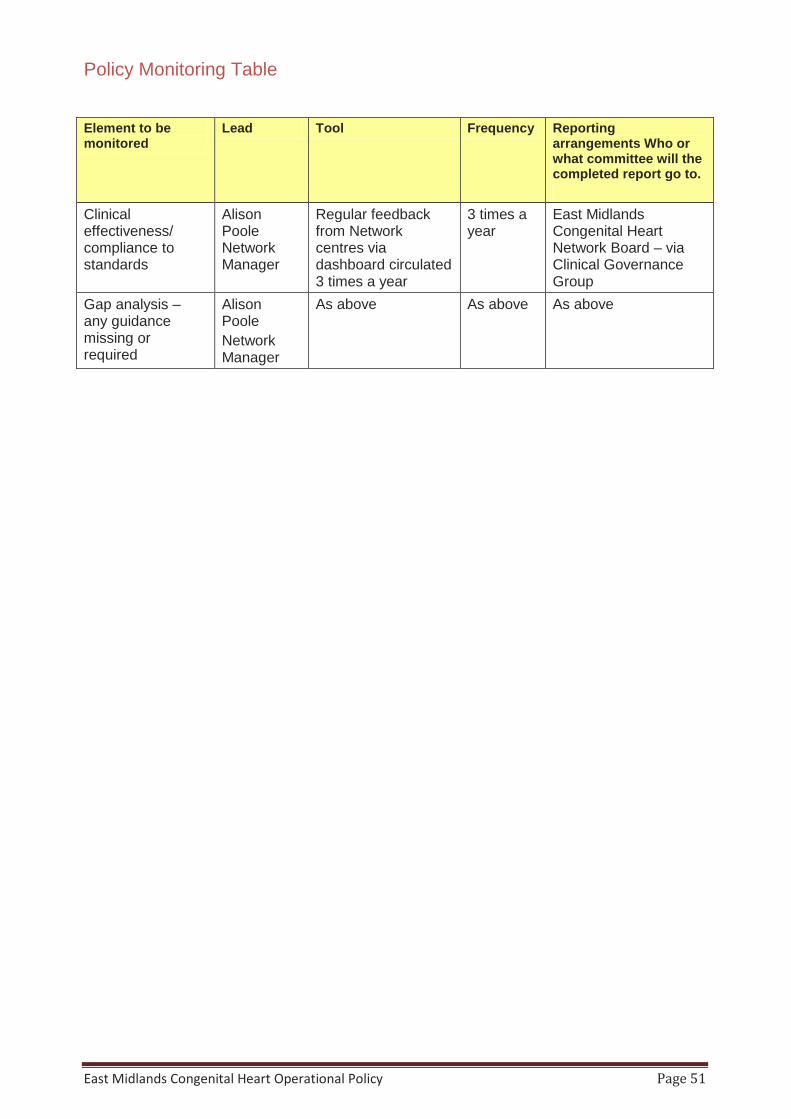
East Midlands Congenital Heart Operational Policy Page 51
Policy Monitoring Table Element to be monitored
Lead Tool Frequency Reporting arrangements Who or what committee will the completed report go to.
Clinical effectiveness/ compliance to standards
Alison Poole Network Manager
Regular feedback from Network centres via dashboard circulated 3 times a year
3 times a year
East Midlands Congenital Heart Network Board – via Clinical Governance Group
Gap analysis – any guidance missing or required
Alison Poole Network Manager
As above As above As above

The East Midlands Congenital Heart
Network: Joint Referral and Care Guidance
Documents
March 2019
UHL telephone number 0300 303 1573
EMCHC Fax 0116 2402422
1. Introduction
This document sets out an agreed model of care for the management of children and adults in the East Midlands with established and suspected congenital and paediatric heart disease, as part of the East Midlands Congenital Heart Network. It aims to document and regularise the existing and well established routes, for referral and communication, for the ‘client population’ currently served by the East Midlands Congenital Heart Centre (EMCHC) at Glenfield Hospital, University Hospitals of Leicester NHS Trust. It should also clarify expectations from the Network which EMCHC aspires to serve more fully.
2. Care closer to home
EMCHC patients live across a wide geographical region, from Leicestershire, Nottinghamshire, Derbyshire, Lincolnshire, Northamptonshire, Warwickshire and Cambridgeshire (Peterborough).
In order to ensure patients have as much of their care as close to home as possible, EMCHC has long standing outreach and referral links with a large number of hospitals across this region.
Patients are largely seen at EMCHC during initial (neonatal) care if required, and around the time of any invasive investigations or treatment including surgery. Otherwise it is the policy of the Network to ensure as many patients as possible are accommodated and managed in their local centres, both as inpatients and as outpatients.
Some hospitals in our region have dual relationships with other cardiac centres; for example Peterborough, the Coventry and Warwickshire Hospitals and Burton-on-Trent. Respect for these relationships is paramount, and EMCHC will continue to support these in whichever ways are possible.
Outreach services have been offered to all centres in the Network. To date, Burton, Coventry and Warwick, and Northampton remain without outreach clinics from our centre. Patients from these areas are generally seen either at EMCHC or in their closest available centre.
In order to ensure that as many East Midlands patients are seen as close to home as possible EMCHC currently provides the following clinics annually;
Paediatric
24 full day and 6 half day clinics at Derby
24 full day clinics at Queens Medical Centre, Nottingham and Kettering
12 full day clinics at Mansfield, Nuneaton, Grantham and Boston
12 half day clinics at Peterborough
Adult
24 clinics at Derby
12 clinics at Nottingham City, Kettering and Lincoln
6 clinics at King’s Mill and Peterborough
We are also supportive of additional clinics within our network as and when required.
EMCHC is equipped to support and provide 24/7 medical advice. We have recently introduced a new cloud based teleconferencing system (Zoom) that allows for Multi-disciplinary team (MDT) discussion and information sharing with all our Network centres and clinicians. EMCHC has a long history of training
Paediatricians with Expertise in Cardiology (PECs) and has a broad network of these now working in the region.
Paediatricians with a specialist expertise in cardiology by clinic are:
Derby - Dr G Joshi, Dr B Etuwewe, Dr B Balasubramanian
Nottingham QMC -Dr P Thakker, Dr S Balmuri
Kettering - Dr P Pandey
Lincoln - Dr R Kollipara
Mansfield (King’s Mill) - Dr D Dave
Nuneaton -Dr A Khan
Peterborough - Dr T Jones
Clinics are also currently provided at Boston and Grantham Hospitals which do not have a PEC.
EMCHC also has a well-established ACHD clinic network supported by the following adult cardiologists with a specialist interest in adult congenital cardiology, in a similar manner to the PEC network.
Nottingham City - Dr W Smith, Dr M Sosin
Derby - Dr D Kelly, Dr A McCance
Lincoln - Dr R Andrews
Kettering- Dr S Hetherington
Peterborough – Dr Rebecca Schofield
Mansfield – pending consultant cardiology appointments in 2019
3. Referral pathways
This document sets out pathways for the following scenarios, involving a fetus, a neonate, a child or an adult with known or suspected cardiac disease.
• Antenatal diagnosis • Acute Paediatric presentation • Out-patient based (routine) referrals • Complex cardiac problems • Transition care to adult services • Adults with CHD • Palliative care • Centre to centre referrals and second opinions • Working with other Networks
The term “children” refers to those from birth to between their 16th and 19th birthdays according to need. Most children will transition towards the ACHD service from 14 years onwards and we would expect the majority to be managed in the ACHD service from their 16th birthday. However, they may remain in the paediatric clinics up to their 19th birthday, especially when there are complex learning or social difficulties.
Patients with heart problems can present with varying manifestations and to a variety of healthcare workers; we have tried to address this by focussing on the clinical need of the child.
4. Antenatal diagnosis – (See Appendix 1, 2 and 3)
Prospective parents will have been seen on a number of occasions, and counselled in conjunction with their local and tertiary obstetric, fetal medicine and neonatal teams and will have had the opportunity to visit EMCHC (and see a surgeon if wished) prior to delivery. Fetal referrals will be facilitated within 2 working days and the pathway and referral forms can be found in (Appendix 2)
A clear plan of care will be agreed and documented prior to delivery with reference to location, timing, and preferred mode of delivery, as well as anticipated immediate postnatal management and transfer plans. All babies with antenatal diagnosed transposition of the great arteries will deliver in Leicester to enable prompt balloon Septostomy if required. Guidance for Emergency Balloon Atrial Septostomy and Temporary Pacing outside a Specialist Surgical Centre can be found in (Appendix 3.)
Babies with other problems will be assessed according to needs, complexity, views of parents and health care professionals, as well as logistics, on an individual basis. The majority of babies are able to deliver in their local unit with ex-utero transfer supported as much as possible. All parents will have contact details for our specialist liaison nurses as well as the fetal cardiac service.

5. Acute Paediatric / Neonatal presentation- (See Appendix 4, 5 and 6)
For any child presenting acutely to a paediatric unit, the priority is, as always, to establish resuscitation and stabilisation based on the national guidelines (APLS) following which contact should be made with the consultant on call, and if necessary the on-call paediatric cardiology team at EMCHC Glenfield. Telemedicine consultations (Zoom) are also available for all our network units and can be enabled for others remotely. Based on the discussion, the child then can be managed locally (e.g. some arrhythmias), and/or transferred to EMCHC depending on the clinical need.
Preterm infants who, in the opinion of the local neonatologists require ligation of the arterial duct (PDA ligation) are referred according to the agreed network SOP (Appendix 6) via the Level 3 neonatal units in the East Midlands (Nottingham and Leicester). The on-call cardiologist, cardiac surgeon and Intensivist at EMCHC will arrange day case (‘away day’) duct ligation in coordination with the Central or East Midlands New-born Network transport Teams. Additional formal cardiological review of all such infants will be undertaken on arrival at EMCHC and prior to transfer to back.
6. Outpatient based (routine) referrals- (See Appendix 7)
Many children are referred for cardiac assessments by GPs, A&E departments and the postnatal wards. Some will be referred from other specialities e.g. clinical genetics. Depending on the centre, these will initially be reviewed / triaged by general paediatricians, neonatologists or the local PEC. These will review the case and make a further referral to the cardiologists if indicated.
Most centres in the East Midlands have now invested in experienced paediatricians with expertise in cardiology (PECs) and there are also some neonatologists with similar expertise, who maintain an on-going presence at and training with EMCHC. The local PECs therefore generally now undertake triaging, initial clinical review and echocardiography as required for these referrals and take responsibility for prioritising and deciding which patients require tertiary cardiological review.
In principle any patient with significant cardiac disease must have their case reviewed by (and usually see) a Cardiologist at least once. In practice this may mean an initial review of their case and investigations between the PEC and the cardiologist to provide advice and formulate a clear follow-up plan in either joint clinics, tertiary cardiac clinics or sometimes in the PECs own review clinics.
In a small number of centres the initial review may be by general paediatricians with access to technician-provided echocardiography, or they may be referred directly to the Network cardiology clinics according to local expertise. Accordingly, the pathway for this group of children would be:
(a) Review and discharge when there is no pathology
(b) Review and management locally without any additional involvement of the cardiologists (non-significant cardiac disease only)
(c) Review and management locally with input from the cardiologists - discussion and review of data (e.g. ECG, Echo, monitors, etc.)
(d) Review and referral to cardiologist
(e) A one off review by the cardiologists with further management by the local team
(f) Follow up with the cardiologists in the Joint Network Cardiology Clinics
(g) Follow up and management at the tertiary (Level 1) cardiac centre
All new patients with a cardiac problem needing follow up should be seen or discussed in detail with a tertiary cardiologist at least once, and a management and follow-up plan agreed.
7. Children with complex cardiac problems
Children with complex heart conditions need careful monitoring of their cardiac condition. In addition, many of these children will need general paediatric input in relation to nutrition, growth and other systemic involvement (e.g. syndromes). In these cases, the principle link should be between the local general paediatrician or the local PEC and the tertiary cardiac service.
When children with a known cardiac problem present to acute paediatric services the initial management (resuscitation and stabilisation) will be the responsibility of the local acute paediatric team and follow the principles of the Resuscitation, Stabilisation and Transfer Pathway which may include the advice and/or transfer to a tertiary cardiac service. These children should in general be seen by the cardiology team from EMCHC for their cardiac issues. Children and adolescents with complex heart disease would come under three major categories as follows:
a) Inter-stage (between operations that are staged) e.g. BT shunts, PA bands b) After completion of palliative surgeries (as opposed to a complete repair) c) After completion of complete repair for those children who need lifelong cardiology reviews and are
at a higher risk for cardiac problems (e.g. Tetralogy of Fallot, Coarctation of aorta, etc.)
8. Inpatient discharge arrangements
Patients that are discharged home from EMCHC are given a handheld copy of their discharge summary. A copy is sent via post to their local PEC/ Link Cardiologist, GP, Health Visitor and any other relevant agencies.
Most patients who have had a procedure will have their initial follow up at EMCHC with ‘repatriation’ to their local hospital outreach clinic as soon as is clinically appropriate.
In patient transfers will only occur by direct communication with the receiving centre Paediatrician/ Cardiologists and will be accompanied by a clear management and follow up plan.
9. Cross sectional imaging - (See Appendix 8)
Cross-sectional imaging services at EMCHC include Cardiac MRI and CT angiography for both children and adults with congenital heart disease. This is an essential part of the service for providing valuable diagnostic information for children and adults with congenital heart disease and sustaining the Congenital Cardiology and Surgical programme with EMCHC
10. 24 hour access to Specialist advice - (See Appendix 9)
EMCHC recognise the need for health care professionals from across the Network and indeed around the country to be able to source specialist advice on our patients at an hour of any day or night. This may be for planned or unplanned admissions, procedures and other investigations. Facilitated by our remote MDT facilities via Zoom technology, our Network colleagues are encouraged to seek advice using the guidance document in (Appendix 9)
11. Centre to Centre referrals - See (Appendix 10)
Centre to Centre referrals and access to second opinion (to include transplant centres and Pulmonary Hypertension Services
As the UK’s leading ECMO (extracorporeal membrane oxygenation centre), EMCHC has a well-developed system for receiving, assessing and prioritising external referrals, involving documented MDT discussion between ECMO, intensive care, surgical and cardiology consultants as appropriate.
For EMCHC patients for whom the MDT opinion is that that a further opinion or opinions are needed to support patient management decisions, this will be agreed and the reasons documented at the MDT. For EMCHC patients for whom the MDT has agreed that their needs would be best served by a procedure in a different centre, it will be determined by the MDT which clinician will make the formal referral in writing (as well usually by telephone or face to face),and ensure that appropriate imaging and physiological information is transferred. Where referral is due to need for individual operator expertise, the EMCHC team will endeavour that a member of the EMCHC team will join the operating team elsewhere in order to continue to build our own institutional and individual expertise.
12. Self-referral- (See Appendix 11)
Parents of children with cardiac problems from around the region can, and do, call EMCHC via Ward 30 at Glenfield, for 24/7 advice. If it is felt that the child requires a hospital review, then parents will almost always be advised to take their child to their local hospital for this. The on-call cardiac team at EMCHC are expected to notify the relevant local acute paediatric service that this has been advised, and provide appropriate information and advice as needed.
Adult patients are all given contact details of their named Cardiac Liaison Nurse for advice in working hours. Out of hours advice is provided through the on call cardiac registrar via the UHL switchboard.
13. Urgent dental assessments- (See Appendix 12)
There is a robust pathway for Congenital Heart Disease Patients presenting with infective endocarditis, dental pain, acute dental pain, acute dental infection or dental trauma. In addition to this all patients require a dental assessment prior to admission and acceptance for surgery. Details of the provision and pathway for Adults with learning difficulties and Children can be found in (Appendix 12)
14. Transition to Adulthood - (See Appendix 13 and 14)
There is a well-established pathway for adolescents and young people with heart problems that aim to provide a seamless transition to adult care.
Whilst many adolescents and young people may have had cardiac concerns that allow appropriate discharge to primary care services, significant numbers will need on-going care and follow up from adult cardiology services.
For this group of teenagers, there are a number of possible outcomes:
a. Discharged (if appropriate) b. GP for on-going follow-up (+/- interval re referral) c. Adult cardiologist with appropriate expertise e.g. Marfan syndrome / heart muscle disease d. Specialist ACHD follow-up or shared care with adult cardiology
Referral to the EMCHC Adult Congenital Cardiology team for Leicester patients can generally occur in a seamless manner due to current the single site nature of the service provided by EMCHC. It is acknowledged that this is soon to change and appropriate adjustments to this process will be made.as part of our relocation operational review and is included in the work plan for 2019/20.
For non-Leicester patients, transition is facilitated by the provision of both paediatric and ACHD outreach clinics at many of our regional centres, often with common notes. However a comprehensive transition referral is required and the patient and family will be involved in that process. Some patients may need or prefer their longer term ACHD follow-up to occur at EMCHC.
There is a Transition Plan / pathway / Guideline which is supported by the EMCHC cardiac liaison team and Transition nurse. Copies can also be found on the website or by contacting [email protected] .and can also be obtained by contacting the liaison team on Tel: 0116 2583338.
It is essential that during the period of Transition patients are monitored and followed up, to reduce the risk of them being lost in the system. The process and guidelines for reducing this risk and monitoring and reporting outcomes can be found in (Appendix 14.)
15. Adult Congenital Cardiac care - (see Appendix 15)
Adult Congenital Cardiac patients may be referred into ACHD clinics either at EMCHC, EMCH Network clinics, or from other services including general adult cardiology, and by GPs. Some will be referred from other specialities e.g. clinical genetics. Depending on the centre, these will initially be reviewed / triaged by the local link Cardiologist or the visiting EMCHC cardiologist themselves.
The local link cardiologist may undertake initial clinical review and echocardiography as required for these referrals and may take responsibility for prioritising and deciding which patients require tertiary cardiological review. In principle any patient with significant cardiac disease must have their case reviewed by (and usually see) a Congenital Cardiology Specialist at least once. In practice this may mean an initial review of their case and investigations between the link cardiologist and the EMCHC ACHD consultant to provide advice and formulate a clear follow-up plan in either joint Network clinics, tertiary cardiac clinics or sometimes in the link cardiologists own review clinics.
In a small number of centres the initial review may be by general cardiologist with access to technician-provided echocardiography, or they may be referred directly to the outreach cardiology clinics according to local expertise. Accordingly, the pathway for this group of patients would be:
(a) Review and discharge as there is no significant pathology
(b) Review and management locally without any additional involvement of the EMCHC cardiologists (minor cardiac disease only)
(c) Review and management locally with an input from the EMCHC ACHD cardiologists - discussion and review of data (e.g. ECG, Echo, MRI / CTetc.)
(d) Review and refer to EMCHC cardiologist
(e) A one off review by the EMCHC cardiologists with further management by the local team
(f) Follow up with EMCHC cardiologists in the Joint Network Cardiology Clinics
(g) Follow up and management at the tertiary cardiac centre
All new patients with a cardiac problem needing follow up should be seen or discussed in detail with a tertiary cardiologist at least once, and a management and follow-up plan agreed.
16. Palliative Care
Children or Adults whose care is moving into end of life services are referred to their local palliative care services as geographically appropriate. Their Cardiac reviews should be made on an as required basis.
17. Communication
For each patient, all correspondence should be simultaneously copied to their:
a. GP
b. (Child’s) named paediatrician
c. PEC / link paediatrician / link cardiologist
d. Parents/primary carer/ patient
e. Any other teams as needed (e.g. other hospital specialists, Health visitor, Community team, social work, etc.)
Since this also constitutes the patients on-going care plan, patients / parents are encouraged to keep copies of this in a file to constitute their hand held records. With time it is anticipated that patients will be offered these electronically. Patients and parents are already encouraged to keep multimedia copies of key investigations such as ECGs, medications etc.
18. Working with other relevant networks
The East Midlands Congenital Heart Network works closely, and is reliant upon a number of other clinical networks to ensure seamless care as close to home as possible.
a. Maternity –
The Complex Pregnancies Network for the East Midlands is newly formed and is the process of developing maternal medicine pathway that in time will include CHD once approved the policy will be added to this document.
b. Neonatal and neonatal transport – (See Appendix 16)
EMCHC is part of the East Midlands Neonatal Operational Delivery Network and conforms to the care pathways designated. The underlying aim of the care pathways is to support the aim of the Network, and East and West Midlands specialised commissioning teams: namely to provide a neonatal service that ensures that mothers and babies are able to access the best and most appropriate level of care at the right place and at the right time, and as close to home as possible. This is underpinned by a focus on clinical discussions, agreement and monitoring.
These pathways detail the clinical thresholds that are expected to be used in order to guide care and to clarify when discussions should take place.
c. Intensive care (See Appendix 17)
Paediatric Intensive Care in Leicester is currently run as a single unit on two sites, the Paediatric Cardiac and ECMO Intensive Care on the Glenfield Hospital site (part of EMCHN) and the Children’s Intensive Care and High Dependency Unit on the Leicester Royal Infirmary site. This ethos of a single unit on two sites is practically reinforced by close staff links at all levels across town. The Paediatric intensive care consultants provide 24-hour cover for both sites, including resident consultant cover for EMCHC; medical registrars are part of the paediatric middle grade rota for the East Midlands Training Rotation. A rotation for nursing staff through both units is well established. The HeartLink ECMO Centre is also situated at the Glenfield Hospital PICU, one of three supra-regional ECMO centres in England undertaking neonatal, paediatric and adult ECMO. The service also retrieves neonates and children for ECMO from throughout England and Wales, either by road or by helicopter. This is currently separate from CoMET, the regional retrieval service. The Glenfield Hospital site has a dedicated helicopter pad.
The scope of the Paediatric Intensive Care Services in Leicester is:
1. Glenfield Hospital
Twelve ICU beds for Cardiology/Cardiothoracic Intensive Care and ECMO, currently seven beds staffed and funded.
2. Leicester Royal Infirmary
Six intensive care and two high dependency beds in the CICU, currently six beds staffed and funded. There are also flexible HDU (level 2 Critical Care) beds on the adjacent twelve-bedded Respiratory ward.
The two units are three miles apart, and normally there is a consultant paediatric Intensivist based at each unit.
There are approximately 900 admissions to the intensive care units a year. Admissions and discharges are agreed by the on-service Paediatric Intensivist and Nurse in charge, in conjunction with other members of the EMCHC team and referring/accepting clinicians (See appendix 17).

For adult ICU admissions, there will be 3 patient groups:
1. Planned post-operative admissions. These should follow the current booking process for adult cardiac surgery. In case of limited availability of ICU beds, a discussion to agree on clinical prioritisation should take place between operating surgeons prior to theatre cases starting.
2. Request for AICU review of inpatients should be by consultant to consultant referral whenever possible, but in emergencies the AICU specialist trainee on call should be contacted.
3. Requests for inter-hospital transfer to AICU should be referred to the duty AICU consultant by the parent speciality consultant.
d. Paediatric Critical Care Transport
EMCHC works closely with the Children’s Medical Emergency Transport (CoMET) Service. Commissioned in 2017, the service provides:
• An acute critical care transport team operating 24/7/52 with capacity to advise on the management of critically ill children who present to an East Midlands Hospital, stabilise them and transport them to an appropriate Paediatric Cardiac Centre (PCC) facility, in line with NHS England Standards and recognised best practice. CoMET Clinicians use Cardiologists and Surgeons from EMCHC to provide expert advice where appropriate through use of conference calls and a dedicated call handling service,
• A repatriation team operating weekdays and during daytime hours only, to safely transport patients to or from PCC facilities, where the level of dependency does not require the full transport service. This will most commonly be ‘back transfers’ to the referring hospital at the end of an episode of critical illness. The purpose of this service is to enable the most efficient use of expensive and pressurised PCC beds, to deliver care to patients in the most appropriate surroundings, and as close to home as possible. This includes the transfer of patient from EMCHC to level 2 units or paediatric wards.
• Outreach advice and training to East Midland’ hospitals in the initial care and stabilisation of acutely ill children; recognising that this improves outcomes and may reduce the need for intensive care admission. This service is provided in line with NHS England Standards and recognised best practice.
The transport team undertake acute transfers, Level 3 repatriations to intensive care facilities nearer the patient’s home where appropriate and support level 2 transfers where necessary. Much transport team time is spent providing advice on resuscitation and stabilisation, managing referral logistics and supporting DGHs with advice around non-PIC transfer cases, as well as in-house and outreach training.
e. Paediatric Community Services
Community paediatric referral pathways are individual to each Network CCG and will vary according to them. Local centres will be expected to adhere to these pathways to ensure all children with complex needs requiring community paediatric support are able to access this appropriately
19. Clinical Governance
Joint Cardiology Clinics
These require:
a. Availability of a PEC (paediatrician with expertise in cardiology) or link paediatrician or Link Adult Cardiologist who:
I. Acts as a focus for correspondence and dissemination of changes in practice / care II. Support links with and request for investigations from the local heart investigation
department III. Supports cardiology services locally
b. Infrastructure –
I. Sufficient nursing support to record and plot height, weight, BP and oxygen saturations for each patient (adult or child) and support the visiting team in the clinic
II. Minimum of ECG and current era cardiac ultrasound facilities available in the clinic, with facilities for electronic image storage and image transfer either on disc, or preferably via PACS or telemedicine.
III. Ability of the local Heart Investigation Unit to support certain cardiac monitoring procedures in adults and children (principally Holter monitoring / event recorders +/- exercise testing.
c. Frequency – this will vary according to population base but needs to accommodate targets for seeing new referrals as well as maintaining acceptable planned follow-up intervals and accommodating repatriation of patients back from tertiary centre after interventions. Additional clinics to the current complement may be added as required.
d. Funding: SLA for attendance and transport costs for Consultant from EMCHC + specialist cardiac liaison nurse.
20. Continuing professional development & validation of existing clinicians
It is vital that for such a service to continue to develop and maintain high quality care, the interests of the clinicians should be considered. Paediatricians who are coordinating the service should feel comfortable with the level of activity that she/he is expected to provide and it would be natural to expect different levels of activities being provided based on the experience, and interest of the clinician. The clinician must be supported by the local paediatric team and also the cardiologists at the tertiary centre.
Special Interest Cardiology Paediatricians are expected to have designated time within their job plans for a sessional commitment to cardiology (ideally a minimum of 2 Direct Clinical Care PAs a week, often more will be needed). This is to facilitate clinics but also MDT attendance (in person or remotely) and to complete related audit and administrative activities. It is suggested that they maintain a log of their activity to ensure a minimal level of activity. Newly appointed consultants will be expected to have achieved the RCPCH SPIN module in Cardiology as part of their CCT. It is also expected that their on-going clinical work is regularly reviewed with their EMCHC cardiologist(s) in keeping with the principles of clinical governance, revalidation and in keeping with guidelines from the GMC and the BCCA outreach guide and role descriptions (currently being updated by the BCCA and PECSiG organisations).
Link ACHD Cardiologists should have designated time within their job plans (ideally a minimum of 2 Direct Clinical Care PAs a week, often more will be needed). This is to facilitate clinics but also MDT attendance (in person or remotely) and to complete related audit and administrative activities. It is suggested that they maintain a log of their activity to ensure a minimal level of activity. Newly appointed consultants will have achieved obligatory curriculum training in ACHD as part of their general cardiology training. EMCHC acknowledges that there is a severe shortage of cardiologists with more extended training in ACHD and that a degree of ‘on the job’ learning may also be required. This will occur as part of the joint clinic process, with regular communication with and support from their outreach EMCHC Cardiologist. It is also expected that their on-going clinical work is regularly reviewed with their EMCHC cardiologist(s) in keeping with the principles of clinical governance, revalidation and in keeping with guidelines from the GMC.

21. Education and Training/CPD – (See Appendix 19)
The EMCHC is committed to a holistic approach to cardiology training, and development of this service for staff and service users by providing on-going CPD, training and clinical governance for all health professionals involved in the provision of paediatric and adult congenital cardiology services. We welcome participation in the weekly paediatric cardiac MDTs and audit / QUICKA meetings at EMCHC along with regular network training days. Our physiologists also provide on-going echo training and support for our network technicians. We also provide local fetal cardiac training and continue to further develop multidisciplinary educational programmes around our referral region. This is additionally facilitated by our new Zoom video conferencing and telemedicine facilities and will be aided by local investment in this as well.
The Network Lead Nurse will lead the education programme for nursing staff across the Network. Where possible a link nurse will be identified in each Network centre and they will be offered competency based training, mentored and supported by one of the Specialist Cardiac Liaison Nursing team. Details of the Network Training strategy can be found in (Appendix 19)
22. East Midlands Congenital Heart Centre Contact details;
For further information see: http://www.eastmidlandscongenitalheart.nhs.uk
Cardiology
Dr Aidan Bolger (ACHD Consultant, Head of Service EMCHC).
Dr Simon MacDonald (ACHD Consultant)
April 2019 (locum Consultant in ACHD)
(Medical Secretary Machaela Pinegar/Angela Hartopp – 0116 2582530)
Prof Frances Bu’Lock (Consultant Congenital Cardiologist)
(Medical secretary Margaret King – 0116 2583904)
Dr Suhair Shebani (Consultant Paediatric Cardiologist)
Dr Thomas Mukasa (Locum Consultant Paediatric Cardiologist)
(Medical Secretary Lorraine Johnson – 0116 2583082)
Dr Daniel Velasco Sanchez (Consultant Paediatric Cardiologist)
Dr Marinos Kantzis (Consultant Paediatric Cardiologist
Dr Rizwan Rehman (Consultant Paediatric Cardiologist) starting May 2019
(Medical secretary Dena Williamson 0116 2582668)
Dr Saravanan Durairaj (Consultant Paediatric Cardiologist)
Dr Gregory Skinner (Consultant Paediatric Cardiologist)
(Medical secretary Jainee Mauree 01162582796)
Dr Katie Linter (Consultant Paediatric Cardiologist)
(Medical Secretary Marina Taylor 0116 2588668)
Sub - Appendices

Appendix 1 Integrated care pathway for prenatal CHD
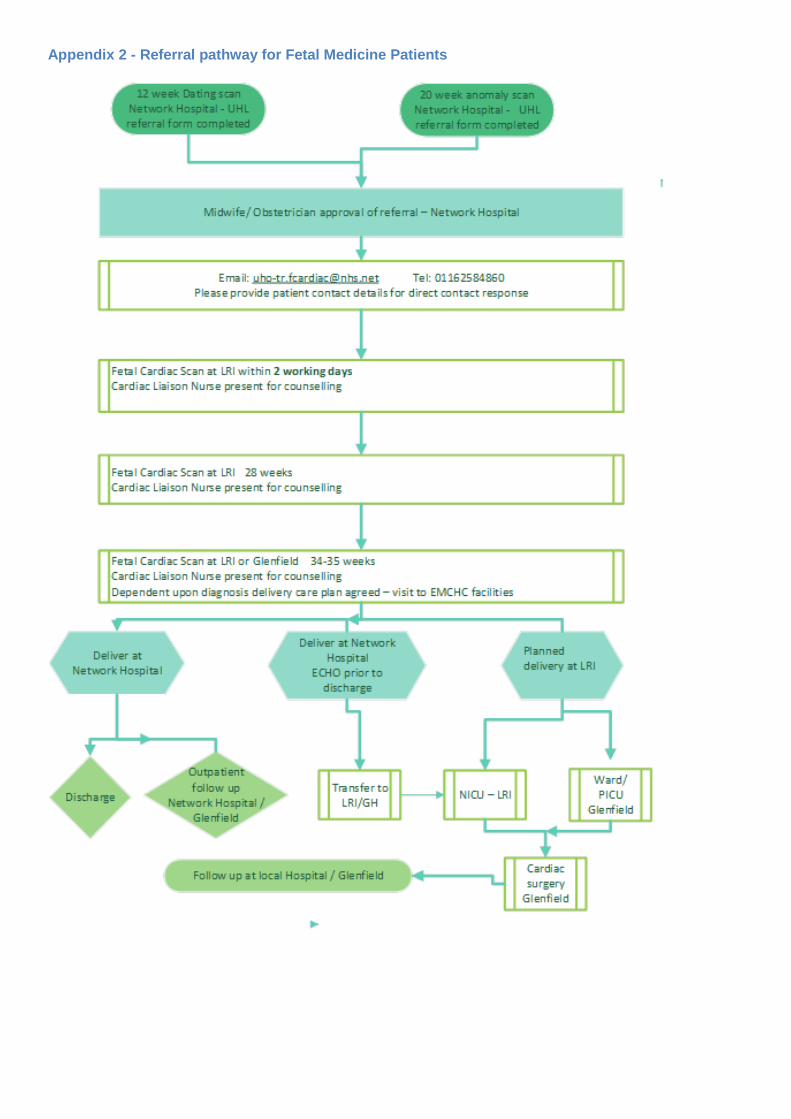
Appendix 2 - Referral pathway for Fetal Medicine Patients
Referral type required. Please enter number from list below 1. Fetal malformation or anomaly identified or suspected. Specify anomalies in the box below.
2. Abnormal 4 or 5 chamber view / suspected structural heart defect on detailed scan. Specify anomalies in the box below.
-For these first two indications, there is evidence of a structural anomaly and a TIMELY diagnostic scan is necessary. A referral form must be sent urgently to our Fetal Cardiac Referrals team, see above for email address. - For information regarding appointments & referrals, or if you would like confirmation that your referral has been received, you may wish to call the Antenatal and Newborn Screening team on 0116 258 4860 Mon - Fri 8:30am and 4pm. - For information / queries about anything else, please contact Dr. Frances Bu’Lock on: 07736 677942.
3. Previous child with structural cardiac defect. Using the box below, indicate diagnosis, date of birth and name of child.
NB: -If previous child has ASD or PDA - subsequent pregnancy does not need antenatal fetal cardiac scan, but should be referred for postnatal cardiac assessment. -History of previous child with a murmur that resolved spontaneously does not require a cardiac referral investigation.
4. Pregnant woman or partner has a history of congenital heart disease. Using the box below, indicate diagnosis, hospital of diagnosis, current status as well as name and DOB of partner if he is the affected individual.
NB: -If pregnant woman or partner has a history of ASD, PDA, an antenatal fetal cardiac scan is not indicated, but the baby should be referred for postnatal cardiac assessment. - History of cardiac murmur that resolved spontaneously in either parent does not require fetal or postnatal cardiac referral.
5. Other Indication: Use box below to specify reason for referral.
In order to provide appropriate information for the fetal cardiac scan, please see below for the type of referral required. Once you know which one is needed, please enter the number into the box below. This information is critical to the planning and performance of the scan. Any additional information is to be added into the ‘Further information’ text box at the bottom of the page.
NHS No: Surname: First Name: DOB: First Line of Address: Postcode: Primary Contact Number: E-mail address:
Name of referrer: Name of Base Hospital: Responsible Consultant: Date of referral: E-mail address of referrer: (For confirmation of receipt) Contact number of referrer:
Parity: Date of detailed scan: EDD: Weight in kg: BMI:
Further Information:
Please provide phone number & e-mail of the patient, as she will be contacted by us directly regarding the appointment.
EAST MIDLANDS CONGENITAL HEART CENTRE FETAL CARDIOLOGY REFERRAL FORM. Email this completed form (along with the detailed scan report) to the ANNB screening team at UHL. E-mail: [email protected] Tel: 0116 258 4860
Alerts / Special Requirements - E.g. allergies, social concerns, other sensitivities:
Please send completed form to: [email protected]
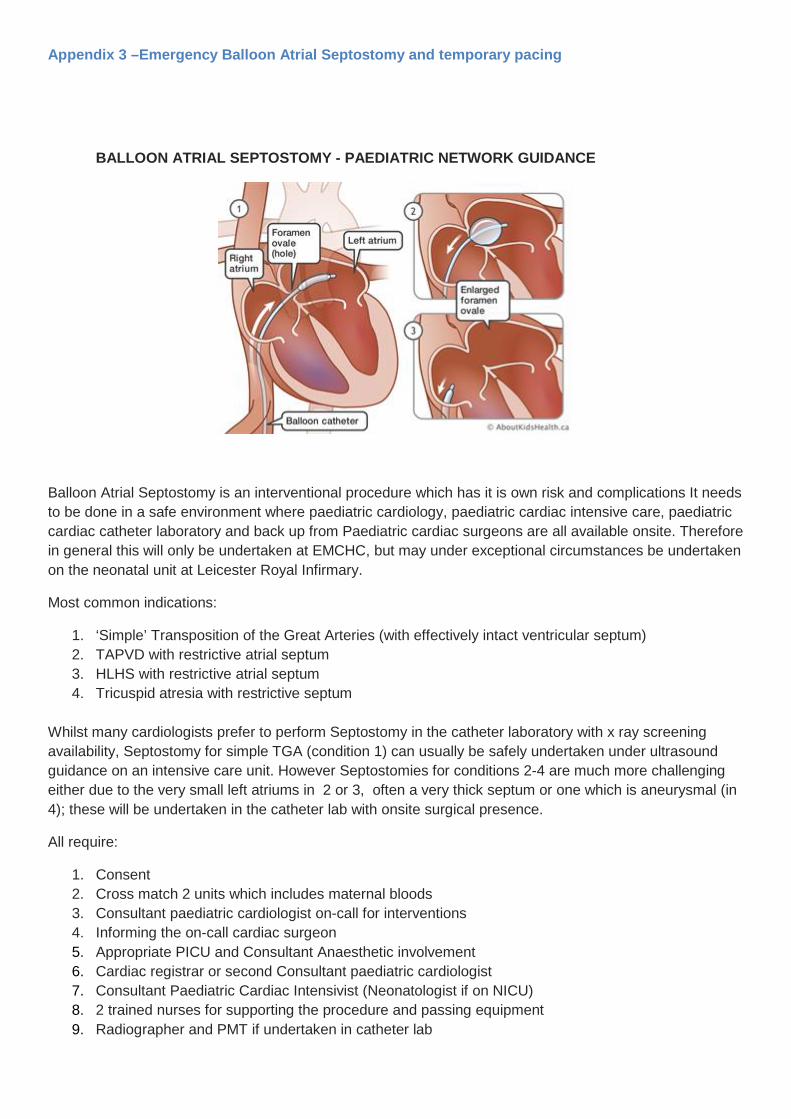
Appendix 3 –Emergency Balloon Atrial Septostomy and temporary pacing
BALLOON ATRIAL SEPTOSTOMY - PAEDIATRIC NETWORK GUIDANCE
Balloon Atrial Septostomy is an interventional procedure which has it is own risk and complications It needs to be done in a safe environment where paediatric cardiology, paediatric cardiac intensive care, paediatric cardiac catheter laboratory and back up from Paediatric cardiac surgeons are all available onsite. Therefore in general this will only be undertaken at EMCHC, but may under exceptional circumstances be undertaken on the neonatal unit at Leicester Royal Infirmary.
Most common indications:
1. ‘Simple’ Transposition of the Great Arteries (with effectively intact ventricular septum) 2. TAPVD with restrictive atrial septum 3. HLHS with restrictive atrial septum 4. Tricuspid atresia with restrictive septum
Whilst many cardiologists prefer to perform Septostomy in the catheter laboratory with x ray screening availability, Septostomy for simple TGA (condition 1) can usually be safely undertaken under ultrasound guidance on an intensive care unit. However Septostomies for conditions 2-4 are much more challenging either due to the very small left atriums in 2 or 3, often a very thick septum or one which is aneurysmal (in 4); these will be undertaken in the catheter lab with onsite surgical presence.
All require:
1. Consent 2. Cross match 2 units which includes maternal bloods 3. Consultant paediatric cardiologist on-call for interventions 4. Informing the on-call cardiac surgeon 5. Appropriate PICU and Consultant Anaesthetic involvement 6. Cardiac registrar or second Consultant paediatric cardiologist 7. Consultant Paediatric Cardiac Intensivist (Neonatologist if on NICU) 8. 2 trained nurses for supporting the procedure and passing equipment 9. Radiographer and PMT if undertaken in catheter lab

10. USS machine for guided femoral access if umbilical access fails 11. Echocardiography machine to guide the Septostomy Under exceptional circumstances, when a baby on the LRI neonatal unit is extremely unstable and transport cannot be sourced in a timely manner, a consultant interventionist will attend LRI NNU to undertake a Septostomy. However, even in this situation, a transport team should still actively be being sourced as there is still a risk that the septum may be difficult to open.
Septostomy Kit (kept in PICU in 2 boxes, checked weekly to ensure in date, or after use)
3 x 4ml 5fr 4ml Miller Atrioseptostomy Balloons 3 x 4ml 5fr 1.8ml Miller Atrioseptostomy Balloons 2 x 5fr Paediatric sheath 2 x 7fr Paediatric/adult short sheath 4 x 22g percutaneous entry Thinwall Needle 4 x 21g percutaneous entry thin wall needle 4 x 20g needles 4 x 24g Yellow Abbocath 4 x 22g Blue Abbocath 4 x 20g Pink Abbocaths 4 x 21g winged Butterfly Needles 4 x 0.021’’ Short guide wire 4 x 0.015’’ Short guide Wire 4 x 3f Arterial Leadercath 2 x of each size of Sterile Gloves 6 - 8.5 4 x 2/0 Mersilk suture with cured needles 4 x Ethicon nylon tapes 4 x Tegaderm film 4 x Packs of sterile swabs 4 x Clear Fenestrated Drapes 4 x Steristrips 4 x Chloraprep 2 x Suture instrument Packs 4 x Blade size 11 with handle 2 x Central line Packs 4 x 2ml LL syringes 4 x 3ml LL syringes 4 x 5ml LL syringes 4 x 10m LL syringes Ultra sound Probe Cover x 2
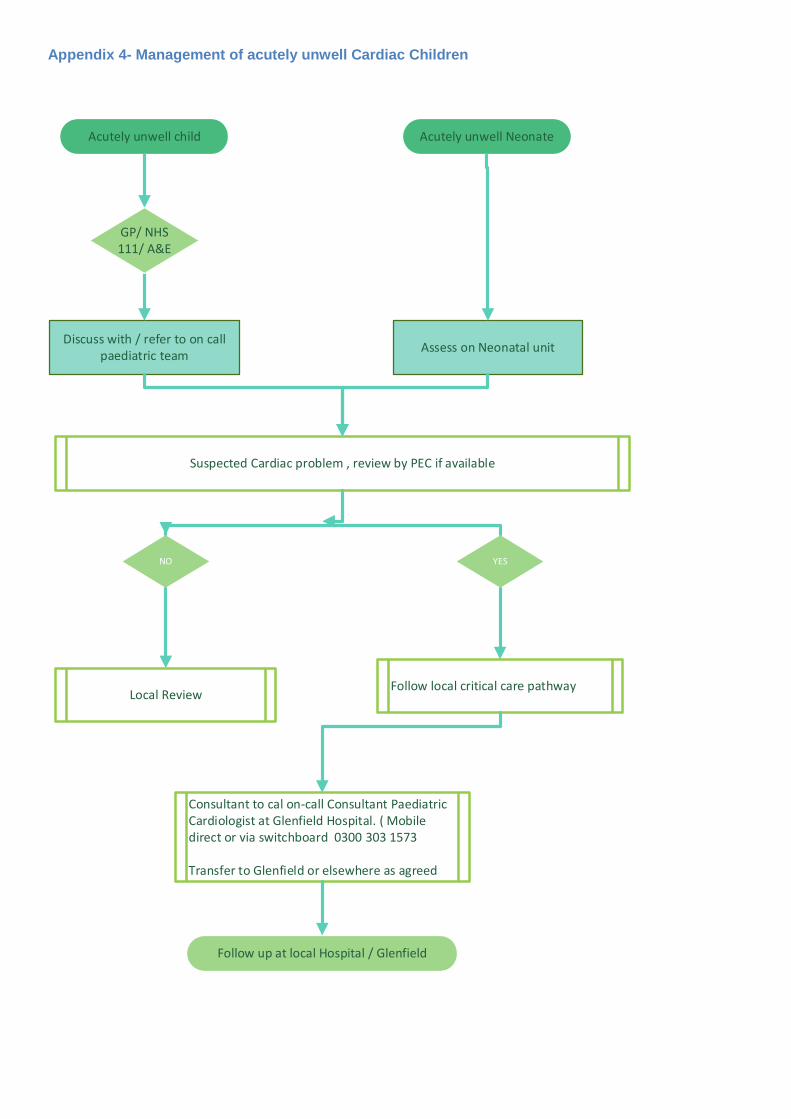
Appendix 4- Management of acutely unwell Cardiac Children
Acutely unwell child Acutely unwell Neonate
Discuss with / refer to on call paediatric team
Suspected Cardiac problem , review by PEC if available
Local Review
Consultant to cal on-call Consultant Paediatric Cardiologist at Glenfield Hospital. ( Mobile direct or via switchboard 0300 303 1573
Transfer to Glenfield or elsewhere as agreed
Follow up at local Hospital / Glenfield
Assess on Neonatal unit
GP/ NHS 111/ A&E
NO YES
Follow local critical care pathway
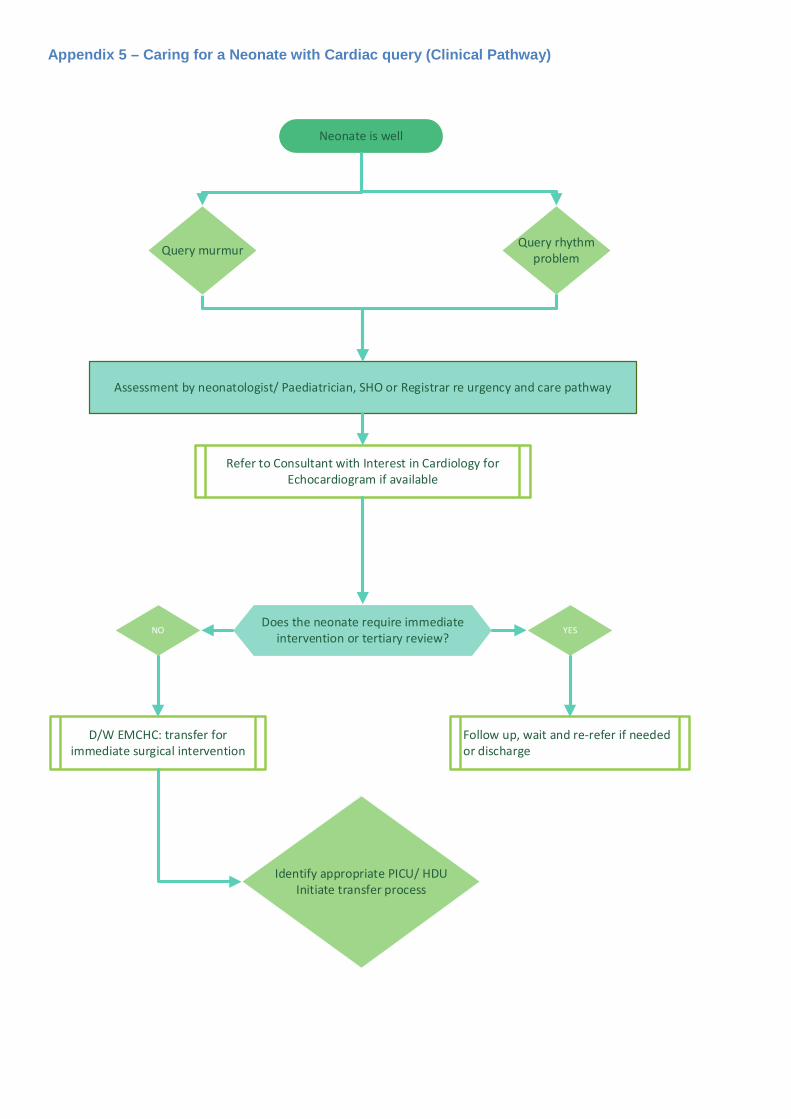
Appendix 5 – Caring for a Neonate with Cardiac query (Clinical Pathway)
Neonate is well
Assessment by neonatologist/ Paediatrician, SHO or Registrar re urgency and care pathway
Refer to Consultant with Interest in Cardiology for Echocardiogram if available
D/W EMCHC: transfer for immediate surgical intervention
Query murmur
NO YES
Follow up, wait and re-refer if needed or discharge
Query rhythmproblem
Does the neonate require immediate intervention or tertiary review?
Identify appropriate PICU/ HDU Initiate transfer process
Appendix 6 – Patient Pathway PDA Ligation in preterm babies
University Hospitals of Leicester NHS Trust
Version 12th November 2018
Directorate Women’s and Children
Department EMCHC and CenTre
Clinical Medical Lead Katie Linter
Document Reference: PDA: V5 12 11 18
Document Name: Standard operating procedure: Patient Pathway PDA Ligation in preterm babies
Authors Dr Linter, Mr Saeed, Andrew Leslie, Dr.B Schoonaker
Publication date 12 September 2018
Target Audience: Referring Neonatal Units, CenTre, EMCHC, Blood Bank
Additional Circulation: CMG Women and Children, regional NNU
Description. This document will provide the overview for the patient pathway from the point of recognition that a premature infant has a PDA which is haemodynamically significant and requires surgical ligation to permit reduction of ventilator support to successful recovery to surgery and stabilising infant at receiving unit post-surgery. It aims to ensure that within the East Midlands Neonatal Operational Delivery Network (EMNODN) the NICUs, surgical NICU,Transport team and EMCHC will provide surgical ligation of PDA when indicated, whilst minimising time of referral to time of surgery and time infant is outside of Neonatal Intensive Care Unit environment.
Actions required. Circulate to appropriate stakeholders for review and comment
1. Purpose
1.1. To work as a coordinated team for the best interest of the pre- term neonate
1.2. To undertake surgery within 48 hrs. of referral, 7 days a week
1.3. To provide case by case debrief for quality assurance purposes
1.4. Meet national recommendations and standards
2. Scope
2.1. This Standard Operating Procedure (SOP) includes a description of the premature neonate pathway from referral for Patent Ductus Arteriosus (PDA) ligation by the referring Neonatal Intensive Care Unit (NICU), to admission for surgery at the East Midlands Congenital Heart Centre (EMCHC) and return to Accepting NICU post-surgery
2.2. This SOP covers roles, responsibilities and routine tasks of the pathway within the normal working practice of the referring NICU, Accepting NICU, EMCHC and CenTre transport team
2.3. This SOP does not cover
• Indication for referral
• Transport arrangements between referring NICU and Accepting NICU
3. Definitions
3.1. NICU is the Tertiary Neonatal Intensive Care Unit at NUH or UHL referring the neonate
3.2. EMCHC is the organisation which will accept the patient referral and undertake surgery
3.3. CenTre is the specialist neonatal transport team which will manage transfer of neonate from the accepting NICU to Glenfield Hospital, management of stay at Glenfield hospital and transfer back to Base Hospital
3.4. PICU is the Paediatric Intensive Care Unit; Glenfield Hospital who will provide the space for observation and monitoring in preparation for to surgery and postoperative recovery prior to discharge from unit
3.5. HeartSuite is the data management system that is used to record details of all NICOR related surgeries and is accessible to external clinical teams on prior arrangement
3.6. East Midlands Neonatal Operational Delivery Network (EMNODN) is the support network for Stakeholders within Acute Trusts and lease with Specialist Commissioners
3.7. The Principles for the PDA patient pathway
4.1 Provision of surgical care must follow the principles directed by UHL NHS Trust to include;
• High quality care of the neonate at all points in patient pathway
• High quality care and communication between and within working teams
• Well informed, timely, multidisciplinary team working
• Accurate documentation and communication of decision making process
• Minimal delays in process
• Clear information to Referring NICU/ Accepting NICU of what is required for referral, necessary investigations to complete before transfer
• The provision of 1 unit cross matched, irradiated CMV negative blood to be available at time of surgery- in theatre fridge at time of surgery.
• Accurate information provided to parents with regard to procedure, timescale and what to expect at EMCHC
• Effective delivery of service to minimise time neonate spends in transport and outside NICU
• Minimal steps in hand over
• Best use of CenTre service
• Paediatric Intensive Care Medical and Nursing staff should not be expected to provide care unless in exceptional circumstances
• Identification of key staff and contacts
• Flexibility to optimise use of theatre space
• Explicit instructions for postoperative care after discharge
4. The expected model of care
4.1. Referral is treated with highest priority to provide high quality care of the neonate identified to require surgical PDA
4.2. Time points are optimised to
• Minimise time between referral and acceptance of patient for surgical ligation
• Minimise time waiting for surgery / procedure
• Minimise time patient out of neonatal intensive care unit (NICU)–during transfer and operating process
• Safety is embedded throughout the process
4.3. Decision to refer is made according to referring hospital clinical guidelines for management of patients with a clinically significant PDA
4.4. Referrals for PDA ligations will only be accepted from the tertiary neonatologist in Nottingham or Leicester
4.5. Patients in Other EMNODN units requiring duct ligation
4.6. When there is consideration that a duct ligation will be required for a baby receiving care in a local neonatal unit or SCBU a discussion is required with the lead tertiary centre for the appropriate hub (NCH or QMC north – for Lincoln, Boston, Kingsmill, & Derby, Leicester Neonatal Service for Northampton, Kettering and Burton). All babies will be reviewed as inpatients in one of the tertiary NICUs prior to definitive decisions being made regarding the need for duct ligation. Referral for duct ligation will then follow the processes as outlined in this pathway.
4.7. The referring neonatologist at the Tertiary Centre (NUH or UHL) and local neonatal unit must be identified and contact details made available a copy of the EMCHC discharge summary should be copied to all clinicians involved.
4.8. The referral should be made in writing to the On-call Cardiology SpR (who will inform the Cardiology Consultant) or the On-call Cardiology Consultant
4.9. When the referral is made by email this should always be copied and filed in patients notes
4.10. The Referral should include patient’s details including parents’ name and contact number, clinical status, MRSA status, echocardiogram and CXR
4.11. IT systems should be in place for transfer of images between NHS Trusts.
4.12. The Cardiology SpR will confirm data has been received, identify and request missing data and set up MDT.
4.13. The patient pathway manager (PPM) will register the patient and enter details on to Heart Suite and generate notes. (In exceptional circumstances out of hours/during leave this will be provided by the duty manager/medical secretary). From UHL the patient notes will transfer with the patient. From NUH photocopies of the patient record are required.
4.14. The quorum for an appropriate MDT is EMCHC Surgeon and Cardiologist. The MDT will review the data and accept the referral for closure. Should the referral not be accepted, the referring Neonatologist will be informed by the Cardiologist or Surgeon, with the rationale for declining at this moment in time. This will be followed up in writing. The Cardiology SpR will inform the PPM immediately and complete outcome for HeartSuite.
5. Once the referral is accepted:
5.1. Decision will be sent to Patient Pathway Manager to list for surgery. The decision is relayed to Local NNU and Tertiary NICU Hospital (It is expected that this will be during/immediately after MDT. This is the responsibility of Cardiology SpR)
5.2. Tertiary NICU Hospital will refer to CenTre team, and coordinate transfer if required
• CenTre will advise on availability of transport for the proposed surgical slot. Same-day referrals will not usually be possible unless clinically indicated. CenTre will be unable to undertake more than one PDA transfer at a time. CenTre will advise on any unusual contingencies which might limit transport availability for the proposed surgical slot
• The responsible Neonatology Consultant, Cardiology Consultant, responsible Cardiothoracic Surgeon, and Patient Pathway Manager will be identified and be available to communicate effectively
• Prior to transfer, full blood count, biochemistry and clotting parameters must have been checked and be in normal range appropriate to gestational age of neonate according to local neonatal guidelines these will also be reviewed at Glenfield by the transport team prior to the patient going into theatre.
5.3. Blood transfusion provision - For surgery to proceed on time and minimise waiting communication with Blood transfusion is vital
5.4. 1 unit cross matched (XM), CMV negative, irradiated blood must be available in theatre blood fridge when patient goes to theatre

6. For Inpatients on the NICU, Leicester Royal Infirmary
• Patient and maternal samples should be sent to LRI laboratory immediately. Request form should state ‘Neonate for PDA ligation at the Glenfield Hospital. Please test sample at LRI immediately’
<4mo age: LRI Blood Transfusion laboratory require neonatal sample for grouping and a maternal sample for Anti body testing
>4mo age: group and antibody testing on same neonatal sample
• The LRI lab will perform testing and identify any potential issues that may arise with testing
• When date of PDA ligation is confirmed the Glenfield Hospital team should send a separate request form to Glenfield Hospital Blood Bank stating date of procedure and requesting 1 unit to be cross matched, CMV negative and irradiated. Stating samples tested at LRI, Blood required at Glenfield.
7. For Nottingham patients
• A maternal sample (This should include the mothers first name, surname, date of birth and NHS number) and neonatal sample must be made available for UHL to test before blood can be cross matched for procedure – the sample will be brought by the transport team. Samples can be sent to Glenfield Blood Bank)
• The PDA Ligation Proforma ( Appendix 1) should be used to communicate effectively what actions are expected by the team at QMC/NCH or LRI prior to transfer for duct ligation by the CenTre transport team as follows:
• Up to date summary letter/Badger summary
• Photocopy of relevant medical notes or agreement for CenTre to take the medical notes
• 2 correct name bands on infant
• 2 working cannulas
• All blood, and blood gas results from previous 12 hours to be available
• PDA ligation leaflet to be given to patients (Appendix 2)
• The PDA Ligation Proforma must be retained with patient notes and passed to the CenTre transport team as part of the handover during their arrival at the referring unit.
7.1. On day of surgery the patient will be discussed at 08.30 PICU huddle. Patient should not be included as a patient bed-space,
7.2. CenTre to contact PICU, when patient leaves Tertiary NICU
Should a referral be terminated PPM/CenTre will be informed immediately
8. On arrival at EMCHC PICU
8.1. Expected time of surgery to be confirmed by Congenital Cardiothoracic Team when referral accepted and listed: Confirmation between PPM, PICU, CenTre and NICU.
8.2. Patient should only leave NICU when theatre time is confirmed on day.
8.3. The expectation is that the baby goes to theatre without avoidable delay from admission to unit

8.4. On arrival, receiving staff (PICU nurse in charge) will inform Identified Surgeon, On Call Cardiology SpR/Consultant and Anaesthetist. Liaison Nurse (in hours)
8.5. CenTre team will continue to monitor neonate and provide medical and nursing care to neonate – CenTre to confirm checklist
8.6. Echocardiogram to be performed to ensure exclude duct dependent circulation, check ductal size, patency and significance, cardiac function and estimated Right heart pressures
8.7. Standard pre -op procedures, consent to be performed by the Cardiothoracic SpR with appropriate competency/delegated authority or Cardiothoracic Surgeon. This will be taken face to face or via telephone (and documented on in house standard consent form as ‘ken by phone’) if parents unable to accompany baby.
8.8. Theatre team to be kept informed and it is expected that an emergency team is made available to prevent any booked second case from being cancelled in line with Chief Executive’s escalation procedure for CHD surgical cases
8.9. If the first case over-runs then this will mean there will be a delay in the patient leaving PICU. Team relief by the night team may be required to transport the patient back to NNU.
9. Patient returns to PICU
9.1. The following actions will be performed:
• Echo
• CXR
• CenTre assessment
• Cardiothoracic Notes and anaesthetic notes photocopied for referring unit.
• Provide accepting NNU with update and expected time of arrival at accepting NICU.
• Speak to parents either face to face or by telephone if not accompanied patient to Glenfield Hospital.
9.2. Pre departure details will be completed according to PDA ligation Proforma
9.3. Specific Post-operative care plan provided to include drain removal and wound care. The post-op plan should be clearly documented onto the proforma. A copy of the proforma is required for EMCHD audit purposes
9.4. Transport Unit to contact Patient Pathway manager when transfer to Accepting Hospital is complete
9.5. Copy of PDA ligation proforma is returned to Patient Pathway Manager for collection of data for quality Assurance and Audit process

10. Roles and responsibilities
Cardiology SpR
Receive referral, inform Cardiology Consultant on-call, checks all data is available for MDT, completes entry of cardiac MDT conference summary onto Heart Suite , informs referring team of outcome of MDT, performs pre and post-operative ECHO Providing timely assessment pre and post theatre
Cardiothoracic Surgical SpR
May be responsible (when appropriately trained) for delegated consent. Provides accepting NICU with post-surgical plan, liaises with blood bank re XM unit, may assist or perform surgical procedure
Cardiology Consultant of week/On Call
Identified as the Named Consultant for patient, attends MDT, informs referring
Will be responsible Named Cardiologist for patient when referral accepted
Nominates Doctor to document outcome of MDT on Heart Suite.
Will inform referring neonatologist if decision is not to accept.
Cardiothoracic Surgeon/On Call
Attends MDT, liaises directly with PPM, Takes or delegates taking of consent, performs surgery or supervises SpR, provide post-operative assessment and care plan.
Nominates Doctor to document outcome of MDT on Heart Suite.
Anaesthetist
Pre surgical assessment, handover to CenTre team
Members of CenTre team
Liaise with Surgical NICU and EMCHC, oversee and complete PDA Ligation Proforma, send copy of Proforma to PPM. Responsible and accountable for provision of safe transport. Keeping parents and other members of team informed
PICU nurse in charge
Liaise with CenTre, inform EMCHC team expected time of arrival of patient
PICU ward clerk
Copy surgical anaesthetic notes give copy to CenTre team
Ensure consent forms are on PICU.
PICU consultant
Pre and post operatively the baby is residing on PICU and the consultant is responsible for providing immediate hands-on support if needed by the transport team in the event of an emergency, for example cardiac arrest
Patient Pathway Manager/ Duty Manager
List patient for surgery, add to HeartSuite data base, and ensure all details are on Heart Suite,
responsible and accountable for keeping Ormis updated
Blood Transfusion Laboratory - provide efficient process for sample analysis, update referring unit if further samples are required, to have available 1 unit of XM, CMV negative, irradiated blood for procedure in Glenfield Theatres for day of surgery.
EMCHC team are responsible and accountable for provision of safe and effective surgical care, and consent. Keeping parents and other members of team informed of process, progress, issues and on-going care. Responsible and accountable for publication of ligation proforma, details of referral process, and parent information to be distributed to all referring centres.
Referring and Surgical NICU
Responsible and accountable for correct referral details and readiness for transfer out and for readmission of neonate post procedure. Completion of first section of PDA Ligation proforma. Keeping parents and other members of team informed. Identification of factors which should defer surgery referral i.e. signs of sepsis, Necrotising Enterocolitis (NEC), or reverse decision to refer i.e. clinical improvement. Provide samples for Blood Bank as per protocol
All teams
Responsible for Problem-solving and Problem-spotting, Escalate and proactively manage actual or predicted problems that might affect patient pathway and delay time to theatre, lengthen pathway.
11. Patient Information
11.1. The required Information booklet (appendix 2) will have been provided by the Referral Hospital to parents including a copy of the consent form, along with information to aid familiarisation with environment, and where food and drink is available
11.2. Information provided must include understanding of why referral and transfer decision has been made to facilitate timely consent and risks associated with surgery
11.3. Information must include the possibility that transfer does not guarantee procedure will take place as circumstances may change even during transfer and the EMCHC team must make the final decision after assessment on arrival
11.4. Parents to be kept informed of anticipated operating date and expected times by Referring NICU, and any management changes necessary as they occur by the appropriate medical or nursing staff according to time point along pathway
12. Contact Numbers
UHL Main Switchboard 0300 303 1573
Cardiology Registrar on call - Bleep 2528
Surgical Registrar on call 07538 077590
CenTre 0300 300 0038
PICU Glenfield Hospital 0116 258 3288
Patient Pathway Manager 0116 256 3963
Theatre Control 0116
Nottingham City Neonatal Unit
Queens Medical Centre Neonatal Unit
Leicester Royal Infirmary Neonatal Unit 0116 2585832/0116 2586464
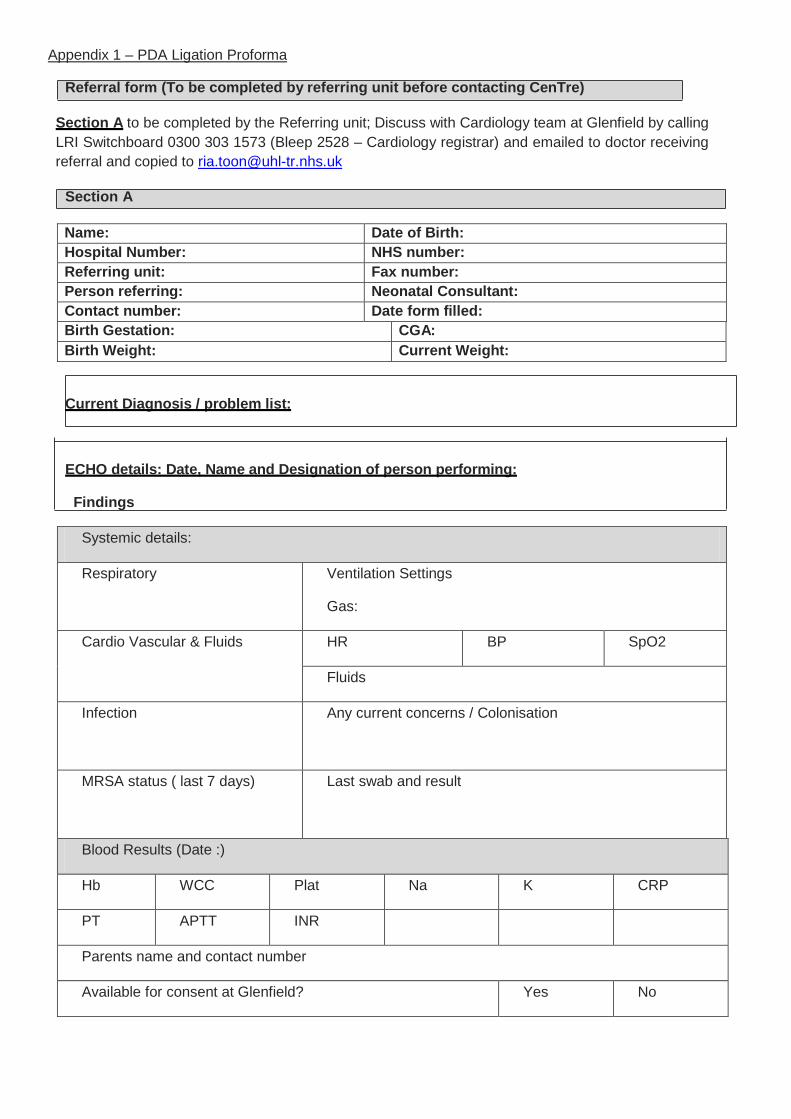
Appendix 1 – PDA Ligation Proforma
Referral form (To be completed by referring unit before contacting CenTre)
Section A to be completed by the Referring unit; Discuss with Cardiology team at Glenfield by calling LRI Switchboard 0300 303 1573 (Bleep 2528 – Cardiology registrar) and emailed to doctor receiving referral and copied to [email protected]
Section A
Name: Date of Birth: Hospital Number: NHS number: Referring unit: Fax number: Person referring: Neonatal Consultant: Contact number: Date form filled: Birth Gestation: CGA: Birth Weight: Current Weight:
Current Diagnosis / problem list:
ECHO details: Date, Name and Designation of person performing:
Findings
Systemic details:
Respiratory Ventilation Settings
Gas:
Cardio Vascular & Fluids HR BP SpO2
Fluids
Infection
Any current concerns / Colonisation
MRSA status ( last 7 days) Last swab and result
Blood Results (Date :)
Hb WCC Plat Na K CRP
PT APTT INR
Parents name and contact number
Available for consent at Glenfield? Yes No
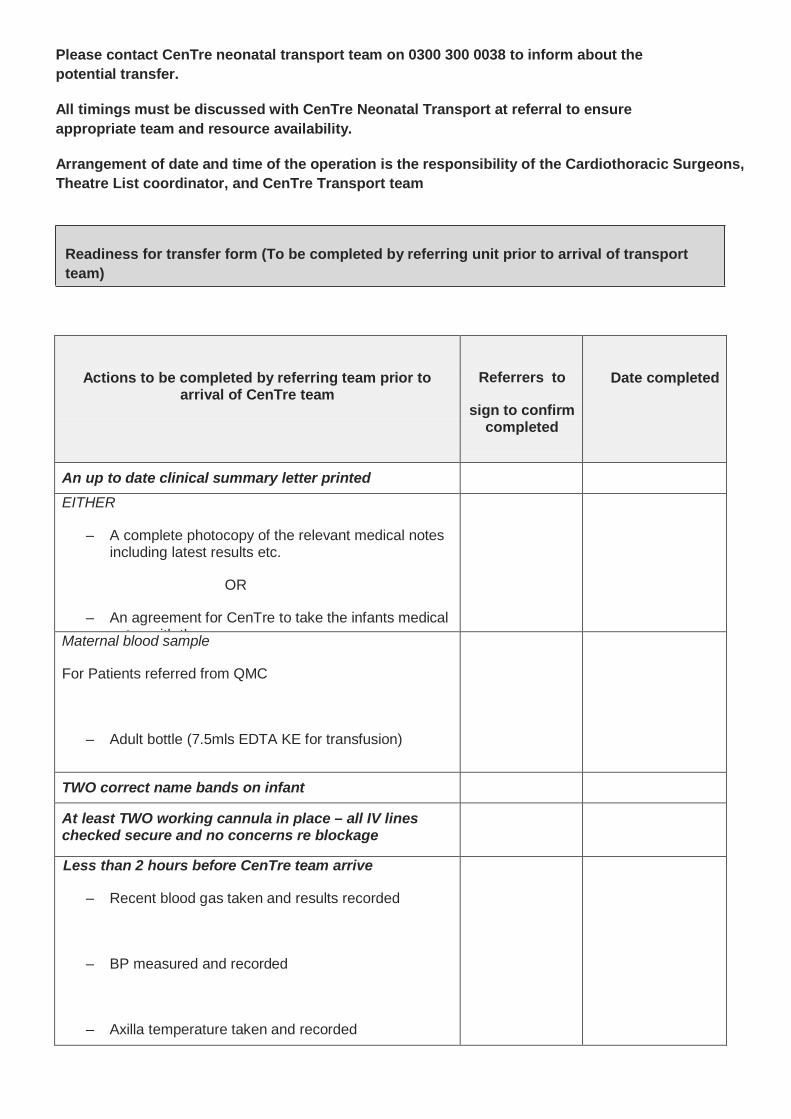
Please contact CenTre neonatal transport team on 0300 300 0038 to inform about the potential transfer.
All timings must be discussed with CenTre Neonatal Transport at referral to ensure appropriate team and resource availability.
Arrangement of date and time of the operation is the responsibility of the Cardiothoracic Surgeons, Theatre List coordinator, and CenTre Transport team
Readiness for transfer form (To be completed by referring unit prior to arrival of transport team)
Actions to be completed by referring team prior to arrival of CenTre team
Referrers to
sign to confirm completed
Date completed
An up to date clinical summary letter printed
EITHER
– A complete photocopy of the relevant medical notes including latest results etc.
OR
– An agreement for CenTre to take the infants medical notes ith them
Maternal blood sample
For Patients referred from QMC
– Adult bottle (7.5mls EDTA KE for transfusion)
TWO correct name bands on infant
At least TWO working cannula in place – all IV lines checked secure and no concerns re blockage
Less than 2 hours before CenTre team arrive
– Recent blood gas taken and results recorded
– BP measured and recorded
– Axilla temperature taken and recorded
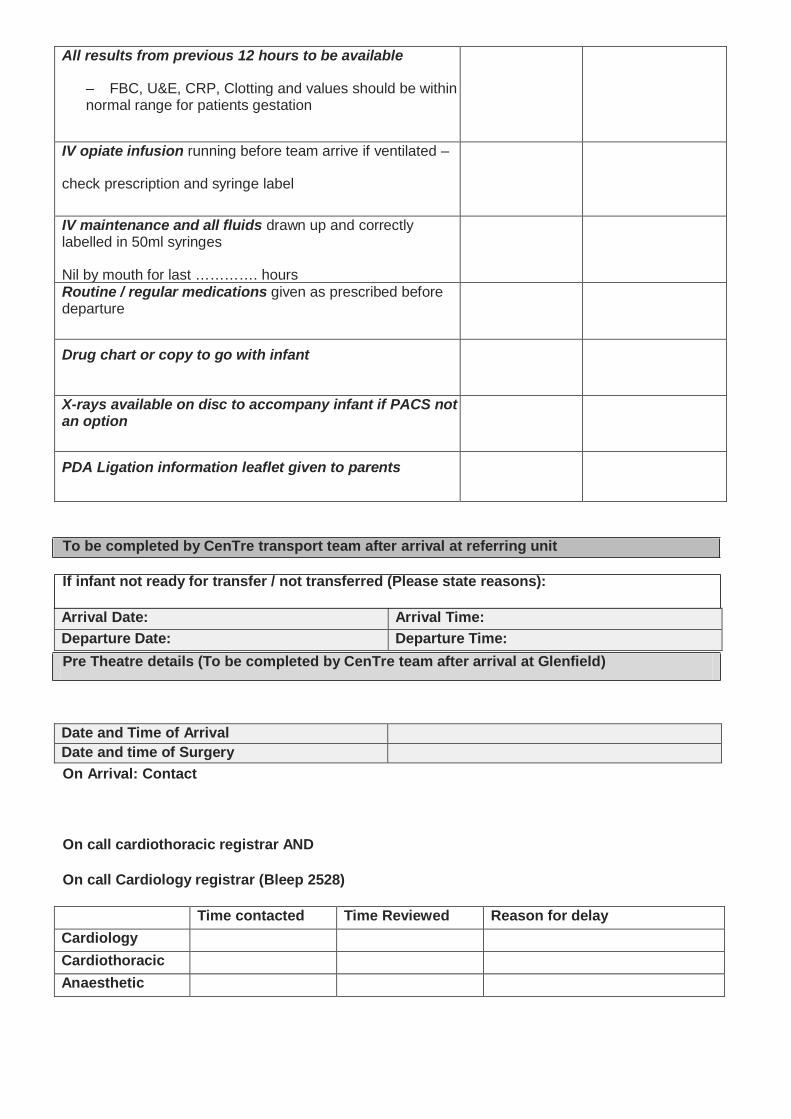
All results from previous 12 hours to be available
– FBC, U&E, CRP, Clotting and values should be within normal range for patients gestation
IV opiate infusion running before team arrive if ventilated –
check prescription and syringe label
IV maintenance and all fluids drawn up and correctly labelled in 50ml syringes
Nil by mouth for last …………. hours
Routine / regular medications given as prescribed before departure
Drug chart or copy to go with infant
X-rays available on disc to accompany infant if PACS not an option
PDA Ligation information leaflet given to parents
To be completed by CenTre transport team after arrival at referring unit
If infant not ready for transfer / not transferred (Please state reasons):
Arrival Date: Arrival Time: Departure Date: Departure Time: Pre Theatre details (To be completed by CenTre team after arrival at Glenfield)
Date and Time of Arrival Date and time of Surgery On Arrival: Contact
On call cardiothoracic registrar AND
On call Cardiology registrar (Bleep 2528)
Time contacted Time Reviewed Reason for delay Cardiology Cardiothoracic Anaesthetic
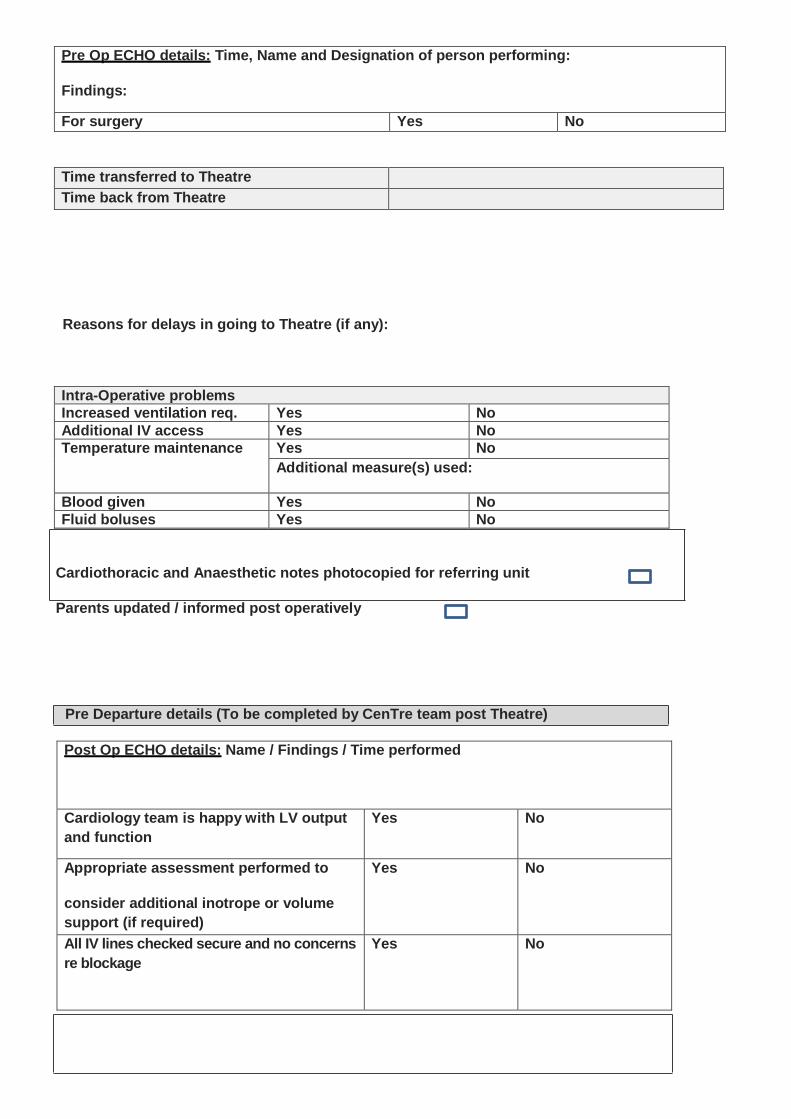
Pre Op ECHO details: Time, Name and Designation of person performing:
Findings:
For surgery Yes No
Time transferred to Theatre Time back from Theatre
Reasons for delays in going to Theatre (if any):
Intra-Operative problems Increased ventilation req. Yes No Additional IV access Yes No Temperature maintenance Yes No
Additional measure(s) used:
Blood given Yes No Fluid boluses Yes No
Cardiothoracic and Anaesthetic notes photocopied for referring unit
Parents updated / informed post operatively
Pre Departure details (To be completed by CenTre team post Theatre)
Post Op ECHO details: Name / Findings / Time performed
Cardiology team is happy with LV output and function
Yes No
Appropriate assessment performed to
consider additional inotrope or volume support (if required)
Yes No
All IV lines checked secure and no concerns re blockage
Yes No

Post Op Chest X-ray: Findings / Time performed
Specific Post-Operative care plan:
Pre departure checks Sign to confirm
Ventilation adjusted, consider reducing pressures
Cardiovascular function assessed & stable observations
Cardiology team happy for transfer
Temperature stable (in normal range)
Inform Cardiology / Cardiothoracic / PICU re departure
Parents informed and updated
Receiving unit informed
Transport consultant informed
All documents and equipment checked
Time of Departure:
Time of Arrival at receiving unit:
Time of Arrival at base:
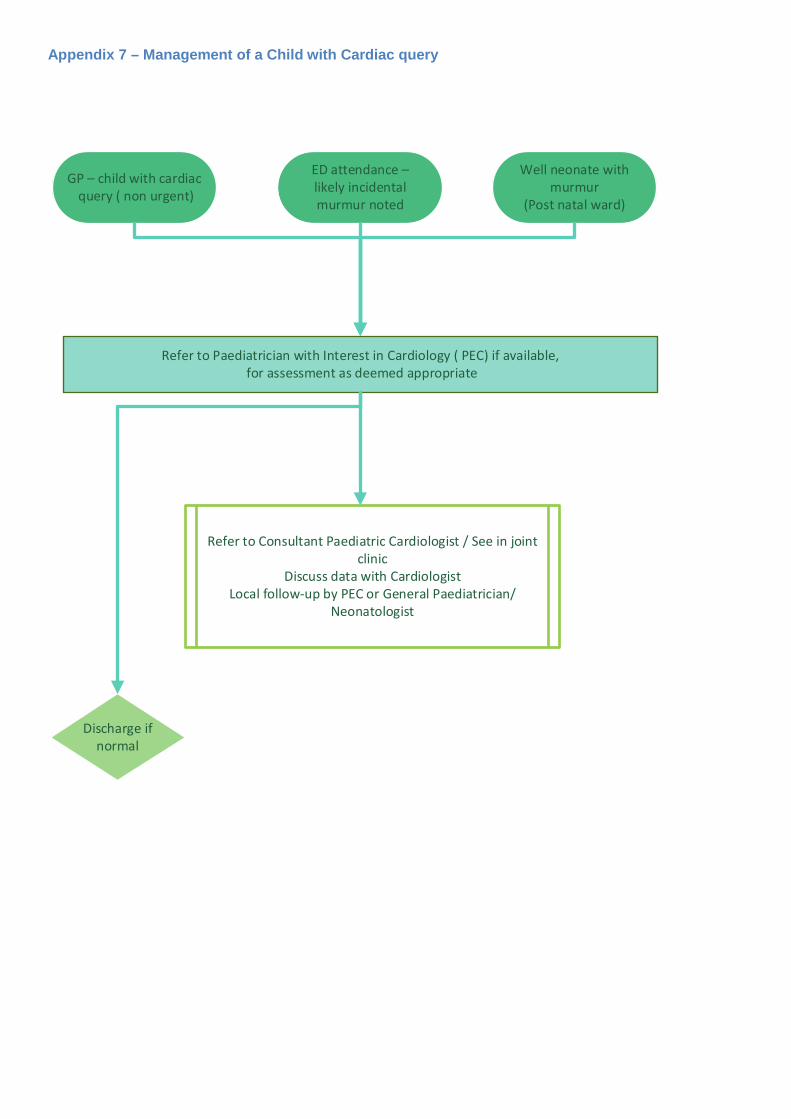
Appendix 7 – Management of a Child with Cardiac query
GP – child with cardiac query ( non urgent)
Refer to Paediatrician with Interest in Cardiology ( PEC) if available, for assessment as deemed appropriate
Refer to Consultant Paediatric Cardiologist / See in joint clinic
Discuss data with CardiologistLocal follow-up by PEC or General Paediatrician/
Neonatologist
Discharge if normal
Well neonate with murmur
(Post natal ward)
ED attendance – likely incidental murmur noted
Appendix 8 - Cross sectional Imaging service at EMCHC
Cross sectional imaging service at EMCHC includes cardiac MRI and cardiac CT angiogram for children. This is an essential part of the service for sustaining and providing valuable diagnostic information for children and adults with congenital heart disease and sustaining the Paediatric Cardiology and Cardiothoracic Programme within EMCHC.
Cardiac MRI service at EMCHC:
The service offers both GA (general Anaesthesia) and Non GA cardiac MRI scans for children and adults with congenital heart disease. The GA service is primarily for children <7-8 yrs. of age and adults with learning difficulties/special needs but not for perfusion studies. The service was reinstated at Glenfield Hospital cardiac MRI suite (F24) from 17th August 2016.
The service is lead between EMCHC (Dr Aidan Bolger/Dr S Durairaj) and UHL Radiology Departments (Dr Andy Ricketts/Dr Aparna Deshpande).
The Team:
Consultants: Dr Aparna Deshpande (adults and children >16 yrs.) / Dr Saravanan Durairaj (All children < 16 yrs. and adult who require general anaesthesia)
Radiographer lead: Bentom Ouma
MR Superintendent: Dean Mawby
Anaesthetic team: Dr Jaswant Sumal and Dr Anand Gore
ODP team: Karan Marlow/ITAPS
Recovery nurse’s team coordinator: Carolyn
Play specialist: Ward 30
CMR coordinator: Grishma
Monitoring equipment support: Ian Benton, Wardray
MR physicist: based at LRI
MRI safety:
All staff involved should complete MRI safety training and questionnaire
Radiographer/Radiologist/Anaesthetic team should have evacuation training
In events of emergency, the scanning will stop (note scanner is always on) and the patients will be transferred to resuscitation room where the resuscitation team will wait to receive the patient
MR radiographer will gate keep during these events to avoid untoward events
Patients or carers/parents should fill MR safety questionnaire for each episode of scanning
MR conditional devices in patients should be highlighted and might need to be checked against MR safety list (www.mrisafety.com)
In events of doubts, this will be discussed with MR Superintendent and MR physicist before bring the patient into scanner.
CMR timetable:
The scanning sessions will take place every week
Monday session: 9am – 1 pm for non-GA cases (4 Non GA ACHD cases)
Wednesday session: 1pm - 6 pm for GA and non-GA cases (we will aim to do 1 GA cases and 2 non GAs)
Equipment availability:
Siemens Aera 1.5T MR scanner
Tesla 3 MR compatible monitoring system with remote module
Referral pathway:
CMR request should be done on a normal radiology form, which will be sent to radiology reception or on ICE for inpatients. The forms will be uploaded on CRIS. CMR consultant on CRIS system will vet the request with a provisional time scale for scanning and any specific MR conditional implants will be highlighted.
Any referral, which is not relevant for CMR, will be discussed with referrer to consider alternate investigation.
The listing will be guided by CMR consultant based on clinical need and information on the form. Appointments will be sent with instruction regarding admission plan and starvation if appropriate.
The list will be circulated to ward and clinicians (ideally one list).
Useful information on the request form:
• Clinical question to be answered • Any MR safety concerns • Child >8 years, please mention any condition, which preclude non-GA • Any previous MRI • Any renal concerns • Any contrast related side effects
Referring from Peripheral clinics:
We suggest filling a radiology request form by visiting cardiologist who then brings it back to EMCHC for it to be processed in the usual way. Network consultant can also refer directly once discussed with the visiting cardiologist regarding indication.
Pre scanning:
Children undergoing GA for CMR will be admitted either the day before or on Wednesday morning in day-case unit/ward 30 for assessment.
SHO or Registrar in ward 30 will see/clerk children for GA cases and admission paper work will be completed.
Current weight and height is Mandatory.
Initial procedure/investigation should include: IV access, Blood for renal function and CXR (if last CXR was >3 month old or had any intervention in the interim). Kindly request up-to-date ECHO if not done in last 6 months.
Cyanotic children will be admitted the day before to receive IV hydration during fasting. Anaesthetic team will instruct fasting times and premedication.
CMR consultant will do consent form for GA cases.
Non GA cases will also have IV access, Blood for renal function and CXR (if last CXR was >3 month old or had any intervention in the interim). Consent form for CMR not required.
For needle phobic non-GA cases, we would consider non contrast MRI provided the clinical question could be answered.
GA cases will be transferred to CMR suite after premedication and anaesthetic team will take over in CMR preparation room. The standard Safer Surgery/Stop the Line WHO checklist is used and patients are anaesthetized on the CMR safe trolley. They are monitored using MR-safe monitoring equipment. IV access is also checked again.
All MR unsafe equipment/s should be removed and MR conditional will be checked counterchecked. If in doubt this will be discussed with CMR consultant and MR radiographer/Superintendent.
MR safety check will be done for all cases by radiographer before going into the scanner and parents will be asked to fill the safety question for the child.
For Non-GA cases, children will see play specialist and go through the process in the ward or CMR suite. Parents will be requested to fill safety questionnaire for the child/adolescent.
Parents are allowed to go into the scanner with children for an ‘awake’ scan’ but will have to dress appropriately and need to fill safety questionnaire for themselves.
Encourage non GA cases to empty bladder before coming into scanner.
Sedated CT will also be treated as GA cases but no CXR needed. Consider IV fluids for cyanotic children and for neonates/infants with prolonged starvation > 4hrs. Regarding sedation dose please refer sedation guidelines for painless procedure. In events for sedation failure and urgent scans please consider discussing with PICU team for use of ketamine or with anaesthetist for GA.
Post Scanning:
After scanning the patient will be extubated in the anaesthetic room and will be handed over to ward 30 recovery nursing team for on-going care. Children will return to ward 30 after GA.
Non GA cases can go home from CMR suite once scans are completed and cannula taken out if inserted.
**Radiographer will fill CMR audit form for every case.
Imaging plan: Priority is to answer clinical question.
1 Axial Haste
2 Localisers
3 4 Chamber and 2 chamber view
4 MR angiogram as appropriate
5 3D navigator Volume imaging
6 Short axis stack
Tru Fisp cine. Slices placed parallel to the plane of the mitral valve (perpendicular to the septum) on 4 CH and checked for position on the 2 CH. Slice thickness will be 8 mm (at least 12 slices)
7 Cines of relevant structures: Tru Fisp cine, preferably breath holding
8 Flows using phase contrast imaging
9 Scar imaging if relevant (2CH, 3CH, 4CH, SA)
Cines -Use 5mm slices with a 100 gap. True Fisp cine retrospective if possible. Small FOV ~320. If necessary put segments as high as possible in physio card, keeping TR<50, in order to reduce scan time. If patient has arrhythmia use prospective gating. Set the acquisition window to 10% below RR interval in physio card. Need to increase no. of slices to 2 to set the gap then put back to 1. May need to reduce TR from 700, reduce by as little as possible.
Flow Quant
Through plane and in-plane if needed retro gated. Set the venc in the angio card appropriately. Increase as high as 600 for a tight stenosis and low for venous flows.
Late enhancement
8 mins after CE run the TI Scout to determine the optimal TI to best null myocardium. Copy the 4CH position
At 10 mins begin imaging (4CH, 2CH, LVOT). Use the phase sensitive 6 slice sequence to cover the short axis in two blocks. Aim to finish by 20 mins. Post CA.
Set the TI according to the Scout and increase by 10 every 3rd sequence.
Post processing and JCC:
After the scanning session, report will be done by CMR consultant and where appropriate will be discussed with network partners before releasing it.
The report will be available in 2 weeks for non-urgent cases and all reports will be sent to relevant Consultants. The cases will be reviewed in JCC if appropriate. Urgent cases will be reported within 24 hrs.
Volume and flow quantification will be done in Siemen’s based software- Argus. Rest of the reporting will be done in Osirix MD.
The report will be on CRIS/ICE system. The report will also be available on Heart suite for CMR.
Key documents:
MR policy
Cardiac CT service at EMCHC:

The service offers sedated and non-sedated CTA scans for children and adults with congenital heart disease. The GA service is primarily for children who fail sedation and for adults with learning difficulties/special needs.
The service is lead between EMCHC (Dr Aidan Bolger/Dr S Durairaj) and UHL Radiology Departments (Dr Andy Ricketts/Dr Aparna Deshpande).
The Team:
Consultants:
Adults: Dr Aparna Deshpande (adults and children >16 yrs.) /
Paediatric: Dr Rachael Holmes, Dr Saravanan Durairaj and Dr Gregory Skinner
Radiographer lead: Bentom Ouma
MR Superintendent: Dean Mawby
Anaesthetic team: Dr Jaswant Sumal and Dr Anand Gore
ODP team: Karan Marlow/ITAPS
Recovery nurse’s team coordinator: Carolyn
Play specialist: Ward 30
CT coordinator: Tracey Rawsthrone
Monitoring equipment support: Ian Benton, Wardray
CT safety lead: Mrs Helen Diggle
CT safety:
All staff involved should complete CT safety questionnaire
Radiographer/Radiologist/Anaesthetic team should have evacuation training
In events of emergency, the scanning will stop (note scanner is always on) and the patients will be transferred to resuscitation room where the resuscitation team will wait to receive the patient
MR radiographer will gate keep during these events to avoid untoward events
Patients or carers/parents should CT safety questionnaire for each episode of scanning if they wish to be with the child
CMR timetable:
The scanning sessions will take place every week
Monday afternoon session: 2am – 4 pm for non-GA cases
Friday mid-day session: 11:30pm - 1 pm for one sedated and normal
Equipment availability:
Siemens Definition Flash scanner
Tesla 3 MR compatible monitoring system with remote module
Referral pathway:
CT request should be done on a normal radiology form, which will be sent to radiology reception or on ICE for inpatients. The forms will be uploaded on CRIS. CT consultant on CRIS system will vet the request with a provisional time scale for scanning and any specific MR conditional implants will be highlighted.
Any referral, which is not relevant for CT, will be discussed with referrer to consider alternate investigation.
The listing will be guided by CT consultant based on clinical need and information on the form. Appointments will be sent with instruction regarding admission plan and starvation if appropriate.
The list will be circulated to ward and clinicians (ideally one list).
Useful information on the request form:
• Clinical question to be answered
• Any safety concerns
• Child >5 years, please mention any condition, which preclude non-GA
• Any renal concerns
• Any contrast related side effects
Referring from Peripheral clinics:
We suggest filling a radiology request form by visiting cardiologist who then brings it back to EMCHC for it to be processed in the usual way. Network consultant can also refer directly once discussed with the visiting cardiologist regarding indication.
Written by S Durairaj
27/07/16 amended 20/12/2018
CMR sticker:
PAEDIATRIC CMR
Date of CMR:
Contrast administered: Yes/No
Any Complication:
Comments:
ADMISSION DOCUMENT
PAEDIATRIC CARDIAC MAGNETIC RESONANCE IMAGING/CT ANGIOGRAM
Date:
Name:
Consultant:
DOB:
Weight (kg):
S number:
Height (cms):
IV Access site:
Cannula gauge:
Sedation or GA required: yes/no
U&E date:
Na: K: Ur: Cr: GFR:
CXR date:
Diagnosis/Procedure:
Indication:
Devices in situ: for MRI only: (please enter the manufacture of the device and implant date)
History (relevant for this admission):
Name: S Number:
MR audit form:
Safety questionnaire complete
Yes/No
MR safety breach Yes/No
Mode of scanning GA/Non GA
Duration of scan (in min)
Complication: Yes/No
Contrast given: Yes/No
Contrast extravasation: Yes/No
Cancellation: Yes/No
CT Audit form:
Safety questionnaire complete
Yes/No
CT safety breach Yes/No
Sedation Yes/no
Radiation dose
Complication: Yes/No
Contrast extravasation: Yes/No
Cancellation: Yes/No
Comments:
Observation:
HR: Sat: BP:
Examination:
Additional Notes:
Name: Sign:
Appendix 9 – 24 hour access to specialist advice
EMCHC recognise the need for health care professionals from across the Network and indeed around the country to be able to source specialist advice on our patients at an hour of any day or night. This may be for planned or indeed unplanned admissions, procedures and other investigations.
Planned procedures
All patients / families should know the names of and have contact details for their responsible EMCHC and Network Consultant, the relevant secretary, and the liaison nurse team. All patients are copied into their clinic letters and given a copy of any discharge summaries which also carry this information.
Thus all patients /parents should be able to direct external clinicians to an access route for elective advice from their responsible specialist. This may be sought be telephone, by email or on paper, and the advice given should also be recorded.
Where there are specific concerns about anaesthesia, the external clinicians will be put in contact with our specialist consultant cardiac anaesthetists, who will also respond to request for advice by phone, email or letter.
Out of hours / emergencies
There is 24/7 cover for emergencies at EMCHC, provided by the On-Service (Consultant of the Week) Paediatric and Adult Congenital Cardiologists and SpRs during daytime hours, and by the On Call Paediatric (and Congenital) Cardiology Consultants and SpRs out of hours. UHL Switchboard (0300 303 1573) has a copy of these rotas and contact details for the responsible doctors.
The Cardiology Consultants and SpRs are able to answer the majority of queries but will also discuss with or pass on directly to the relevant other on call specialists (e.g. On-Call Consultant Anaesthetist) as necessary.
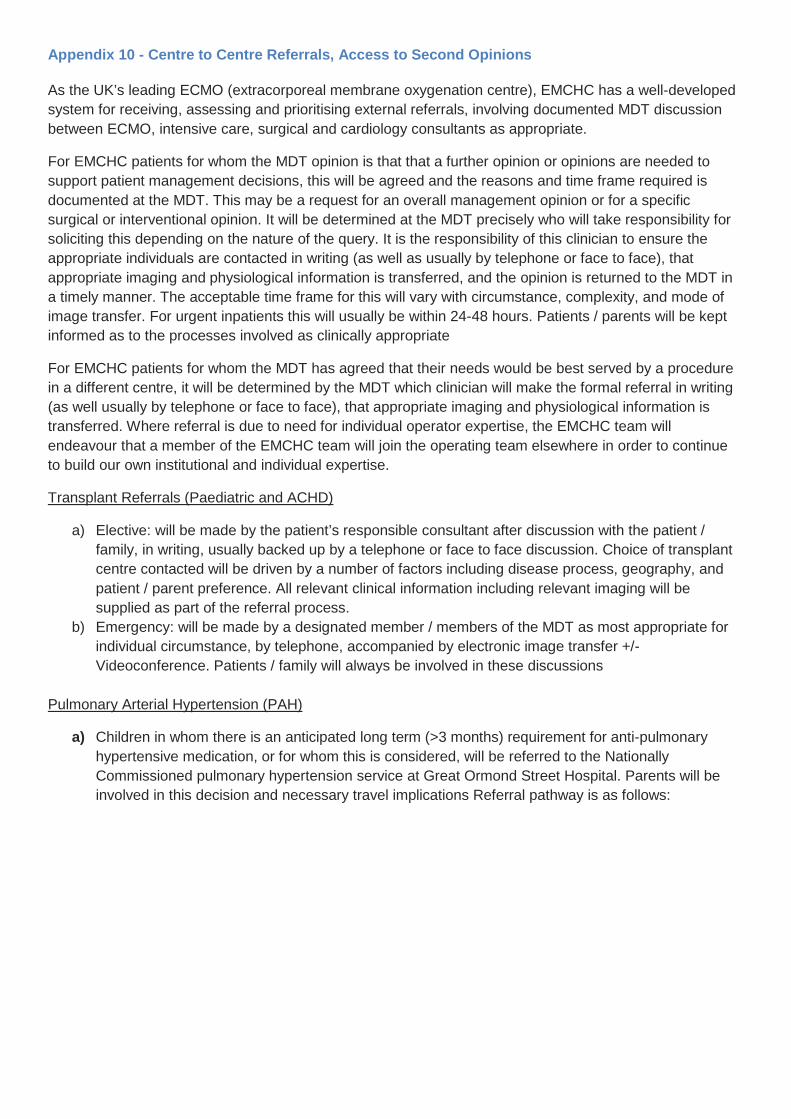
Appendix 10 - Centre to Centre Referrals, Access to Second Opinions
As the UK’s leading ECMO (extracorporeal membrane oxygenation centre), EMCHC has a well-developed system for receiving, assessing and prioritising external referrals, involving documented MDT discussion between ECMO, intensive care, surgical and cardiology consultants as appropriate.
For EMCHC patients for whom the MDT opinion is that that a further opinion or opinions are needed to support patient management decisions, this will be agreed and the reasons and time frame required is documented at the MDT. This may be a request for an overall management opinion or for a specific surgical or interventional opinion. It will be determined at the MDT precisely who will take responsibility for soliciting this depending on the nature of the query. It is the responsibility of this clinician to ensure the appropriate individuals are contacted in writing (as well as usually by telephone or face to face), that appropriate imaging and physiological information is transferred, and the opinion is returned to the MDT in a timely manner. The acceptable time frame for this will vary with circumstance, complexity, and mode of image transfer. For urgent inpatients this will usually be within 24-48 hours. Patients / parents will be kept informed as to the processes involved as clinically appropriate
For EMCHC patients for whom the MDT has agreed that their needs would be best served by a procedure in a different centre, it will be determined by the MDT which clinician will make the formal referral in writing (as well usually by telephone or face to face), that appropriate imaging and physiological information is transferred. Where referral is due to need for individual operator expertise, the EMCHC team will endeavour that a member of the EMCHC team will join the operating team elsewhere in order to continue to build our own institutional and individual expertise.
Transplant Referrals (Paediatric and ACHD)
a) Elective: will be made by the patient’s responsible consultant after discussion with the patient / family, in writing, usually backed up by a telephone or face to face discussion. Choice of transplant centre contacted will be driven by a number of factors including disease process, geography, and patient / parent preference. All relevant clinical information including relevant imaging will be supplied as part of the referral process.
b) Emergency: will be made by a designated member / members of the MDT as most appropriate for individual circumstance, by telephone, accompanied by electronic image transfer +/- Videoconference. Patients / family will always be involved in these discussions
Pulmonary Arterial Hypertension (PAH)
a) Children in whom there is an anticipated long term (>3 months) requirement for anti-pulmonary hypertensive medication, or for whom this is considered, will be referred to the Nationally Commissioned pulmonary hypertension service at Great Ormond Street Hospital. Parents will be involved in this decision and necessary travel implications Referral pathway is as follows:
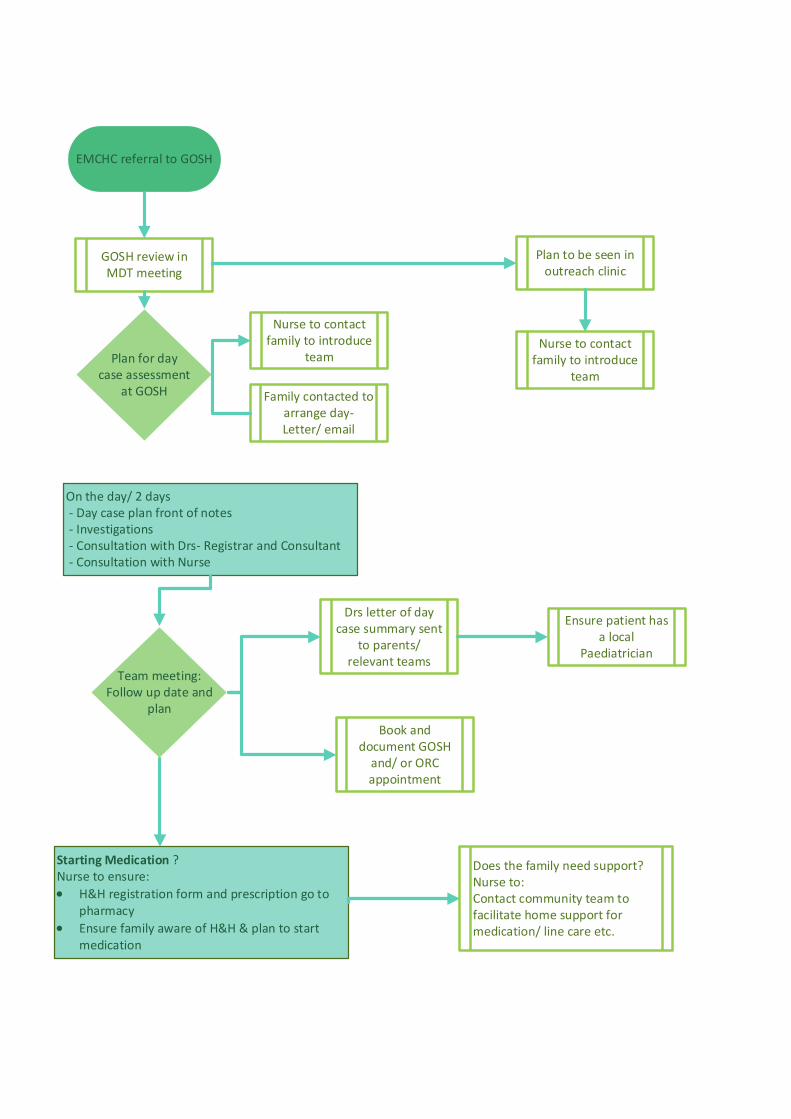
EMCHC referral to GOSH
On the day/ 2 days - Day case plan front of notes - Investigations - Consultation with Drs- Registrar and Consultant - Consultation with Nurse
GOSH review in MDT meeting
Plan to be seen in outreach clinic
Plan for day case assessment
at GOSH
Nurse to contact family to introduce
team
Family contacted to arrange day- Letter/ email
Nurse to contact family to introduce
team
Drs letter of day case summary sent
to parents/ relevant teams
Book and document GOSH
and/ or ORC appointment
Ensure patient has a local
Paediatrician
Team meeting:Follow up date and
plan
Starting Medication ?Nurse to ensure:• H&H registration form and prescription go to
pharmacy• Ensure family aware of H&H & plan to start
medication
Does the family need support?Nurse to:Contact community team to facilitate home support for medication/ line care etc.
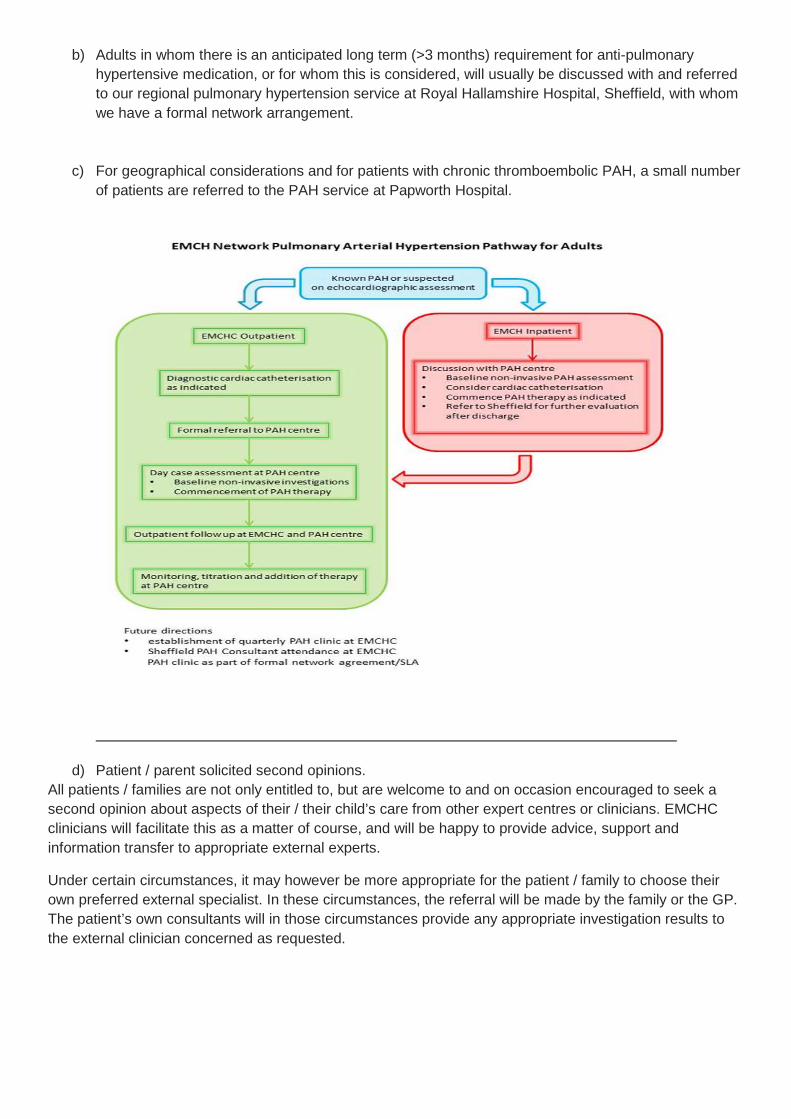
b) Adults in whom there is an anticipated long term (>3 months) requirement for anti-pulmonary hypertensive medication, or for whom this is considered, will usually be discussed with and referred to our regional pulmonary hypertension service at Royal Hallamshire Hospital, Sheffield, with whom we have a formal network arrangement.
c) For geographical considerations and for patients with chronic thromboembolic PAH, a small number of patients are referred to the PAH service at Papworth Hospital.
d) Patient / parent solicited second opinions. All patients / families are not only entitled to, but are welcome to and on occasion encouraged to seek a second opinion about aspects of their / their child’s care from other expert centres or clinicians. EMCHC clinicians will facilitate this as a matter of course, and will be happy to provide advice, support and information transfer to appropriate external experts.
Under certain circumstances, it may however be more appropriate for the patient / family to choose their own preferred external specialist. In these circumstances, the referral will be made by the family or the GP. The patient’s own consultants will in those circumstances provide any appropriate investigation results to the external clinician concerned as requested.
Appendix 11 – Managing patients who self-refer out of hours
EMCHC recognises the need for patients / parents to be able to self-refer or indeed seek expert advice from their Tertiary Cardiac expert at any time. Out of hours enquiries are usually patients / parents seeking expert advice / assistance. There are many routes through which this may be sought at EMCHC and these are described below.
Children
1. All of our patients have a known liaison nurse and are given individual contact details (mobile number, email address and office number) when we see them in our network clinics, surgical or catheter preadmission or fetal cardiac clinics.
2. All EMCHC clinic letters have the contact details for our secretaries and liaison nurses on them.
3. Team names and contact details are given out in clinics with our contact cards.
4. The office answer machine (0116 235 3338) message states that messages are listened to throughout the day but not in the evenings, weekends or bank holidays. It also states that ‘if you are concerned about your child you can contact the children’s ward on 0116 256 3961’. It also informs callers that out of hours, the hospital switchboard can be asked to contact the on-call ‘paediatric cardiac registrar’ for advice.
5. At discharge, those children who have been admitted to or been seen on our paediatric ward (Ward 30), are given the ward telephone number and advised that they can telephone the ward for advice at any time of the day and night. They are also told that if they have any acute concerns about their child they must take them to their nearest Emergency Department or call 999, rather than come to Ward 30 unannounced.
6. If a parent or patient phones Ward 30 (or the Paediatric Cardiac Registrar on call), they will be offered advice (escalated to the On-Call consultant if appropriate) and if physical review is appropriate, will either be seen on Ward 30 or arrangements will be made for review at their local Network Centre. The On Call Cardiology team will also communicate this to the on-call team in the relevant Network Centre and ask for feedback on the patient once seen.
7. Parents / patients are asked to inform us if they are admitted to other centres so that we don’t rely solely on that centre contacting us to inform us of an admission.
Adults
1. All of our patients have a known liaison nurse and are given individual contact details (mobile number, email address and office number) if we see them in our network, surgical, catheter preadmission or maternal medicine clinics.
2. Team names and contact details are given out in ACHD clinics with our contact cards.
3. The office answer-machine message states that messages are listened to throughout the day but not in the evenings, weekends or bank holidays. It also informs callers that out of hours, the hospital switchboard can be asked to contact the on-call ‘paediatric cardiac registrar’ (who also all covers Adult Congenital Heart disease out of hours) for advice.
4. If a parent or patient phones Ward 30 or the Paediatric Cardiac Registrar on call), they will be offered advice (escalated to the On-Call consultant if appropriate) and if physical review is appropriate, will either be seen at EMCHC or arrangements will be made for review at their local Network Centre. The On Call Cardiology team will also communicate this to the on-call team in the relevant Network Centre and ask for feedback on the patient once seen.
5. If we receive queries within hours and offer advice, we also encourage patients to visit walk-in centres, GP’s for non-acute issues, and A&E for advice if they consider it cannot wait to be dealt with.
6. We ask our patients to let us know if they are admitted to other centres or CDU /A&E in Leicester so that we don’t rely solely on that centre contacting us to inform us of an admission.
Patients not previously known to EMCHC may also ‘self-refer’. This most frequently happens either by individual email (or via our website contact portal). These contacts are dealt with on a case by case basis and the team will always involve the patient’s GP and seek additional information from other known health care providers to ensure continuity of care. Others may happen as part of an emergency admission or review and will be escalated by the admitting team to the service as needed. Again, additional information will always be sought.

Appendix 12 – Urgent dental Assessments
Standard operating procedure: Paediatric congenital heart patient pathway – Dental services
University Hospitals of Leicester NHS Trust
Version 12th September 2018
Directorate Women’s and Children
Department EMCHC
Clinical Medical Lead Jancy Pope
Document Reference:
Document Name: Standard operating procedure: Patient Pathway for East Midlands congenital heart centre patients requiring Dental input
Authors Charlotte King and Jancy Pope
Publication date 12 September 2018
Target Audience: Referring clinicians
Additional Circulation: CMG Women’s and Children, regional Dental Team
Description. This document will provide the overview for the patient pathway from the point of.
Actions required. Circulate to appropriate stakeholders for review and comment
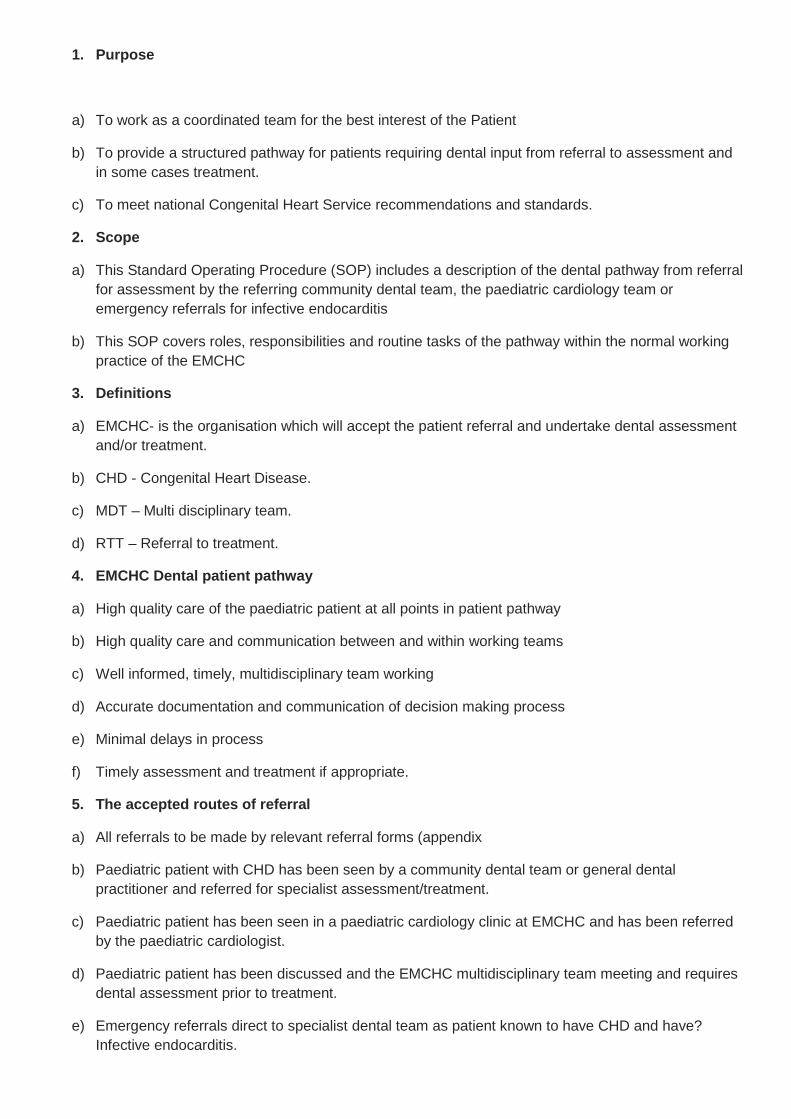
1. Purpose
a) To work as a coordinated team for the best interest of the Patient
b) To provide a structured pathway for patients requiring dental input from referral to assessment and in some cases treatment.
c) To meet national Congenital Heart Service recommendations and standards.
2. Scope
a) This Standard Operating Procedure (SOP) includes a description of the dental pathway from referral for assessment by the referring community dental team, the paediatric cardiology team or emergency referrals for infective endocarditis
b) This SOP covers roles, responsibilities and routine tasks of the pathway within the normal working practice of the EMCHC
3. Definitions
a) EMCHC- is the organisation which will accept the patient referral and undertake dental assessment and/or treatment.
b) CHD - Congenital Heart Disease.
c) MDT – Multi disciplinary team.
d) RTT – Referral to treatment.
4. EMCHC Dental patient pathway
a) High quality care of the paediatric patient at all points in patient pathway
b) High quality care and communication between and within working teams
c) Well informed, timely, multidisciplinary team working
d) Accurate documentation and communication of decision making process
e) Minimal delays in process
f) Timely assessment and treatment if appropriate.
5. The accepted routes of referral
a) All referrals to be made by relevant referral forms (appendix
b) Paediatric patient with CHD has been seen by a community dental team or general dental practitioner and referred for specialist assessment/treatment.
c) Paediatric patient has been seen in a paediatric cardiology clinic at EMCHC and has been referred by the paediatric cardiologist.
d) Paediatric patient has been discussed and the EMCHC multidisciplinary team meeting and requires dental assessment prior to treatment.
e) Emergency referrals direct to specialist dental team as patient known to have CHD and have? Infective endocarditis.
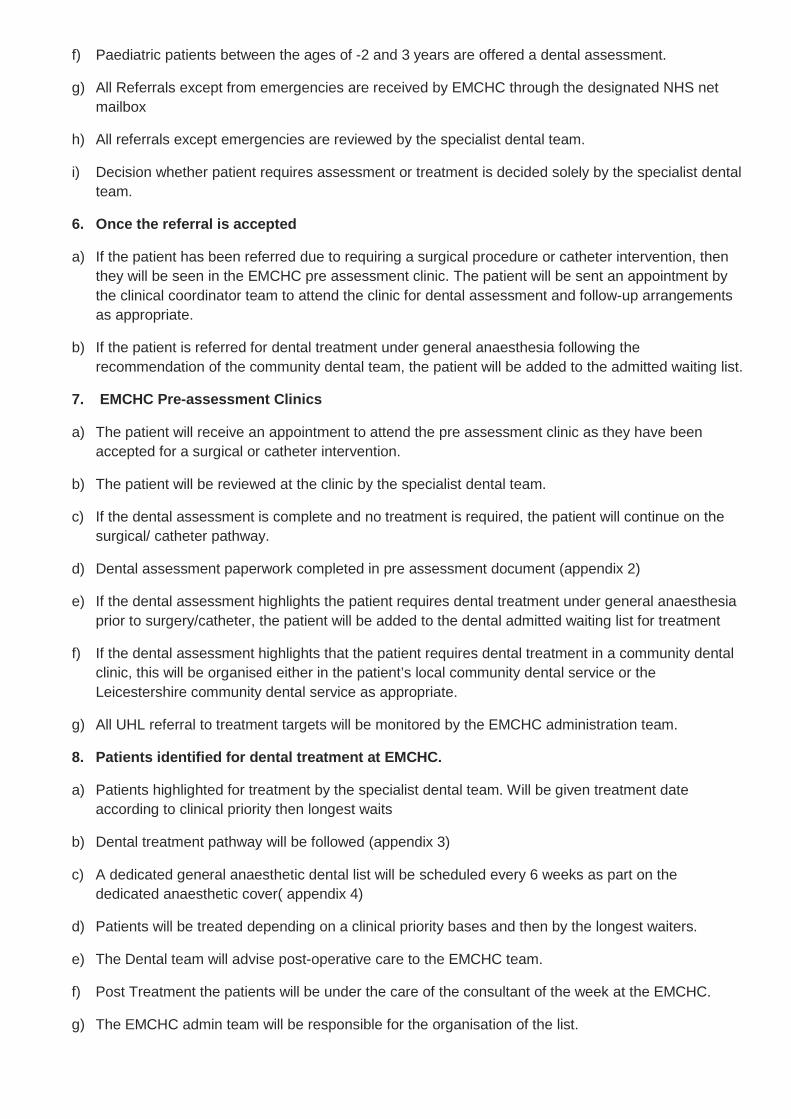
f) Paediatric patients between the ages of -2 and 3 years are offered a dental assessment.
g) All Referrals except from emergencies are received by EMCHC through the designated NHS net mailbox
h) All referrals except emergencies are reviewed by the specialist dental team.
i) Decision whether patient requires assessment or treatment is decided solely by the specialist dental team.
6. Once the referral is accepted
a) If the patient has been referred due to requiring a surgical procedure or catheter intervention, then they will be seen in the EMCHC pre assessment clinic. The patient will be sent an appointment by the clinical coordinator team to attend the clinic for dental assessment and follow-up arrangements as appropriate.
b) If the patient is referred for dental treatment under general anaesthesia following the recommendation of the community dental team, the patient will be added to the admitted waiting list.
7. EMCHC Pre-assessment Clinics
a) The patient will receive an appointment to attend the pre assessment clinic as they have been accepted for a surgical or catheter intervention.
b) The patient will be reviewed at the clinic by the specialist dental team.
c) If the dental assessment is complete and no treatment is required, the patient will continue on the surgical/ catheter pathway.
d) Dental assessment paperwork completed in pre assessment document (appendix 2)
e) If the dental assessment highlights the patient requires dental treatment under general anaesthesia prior to surgery/catheter, the patient will be added to the dental admitted waiting list for treatment
f) If the dental assessment highlights that the patient requires dental treatment in a community dental clinic, this will be organised either in the patient’s local community dental service or the Leicestershire community dental service as appropriate.
g) All UHL referral to treatment targets will be monitored by the EMCHC administration team.
8. Patients identified for dental treatment at EMCHC.
a) Patients highlighted for treatment by the specialist dental team. Will be given treatment date according to clinical priority then longest waits
b) Dental treatment pathway will be followed (appendix 3)
c) A dedicated general anaesthetic dental list will be scheduled every 6 weeks as part on the dedicated anaesthetic cover( appendix 4)
d) Patients will be treated depending on a clinical priority bases and then by the longest waiters.
e) The Dental team will advise post-operative care to the EMCHC team.
f) Post Treatment the patients will be under the care of the consultant of the week at the EMCHC.
g) The EMCHC admin team will be responsible for the organisation of the list.

h) The waiting times of patients will be monitored weekly through EMCHC RTT reports.
9. Patient Information
a) The required Dental Information leaflets (appendix 12.5) will be provided to the paediatric patient’s next of Kin or legal guardian.
b) Information provided must include understanding of why referral and treatment decision has been made
c) Information leaflet regarding care of patient following treatment will be given on discharge with contact numbers including ward 30 phone number.
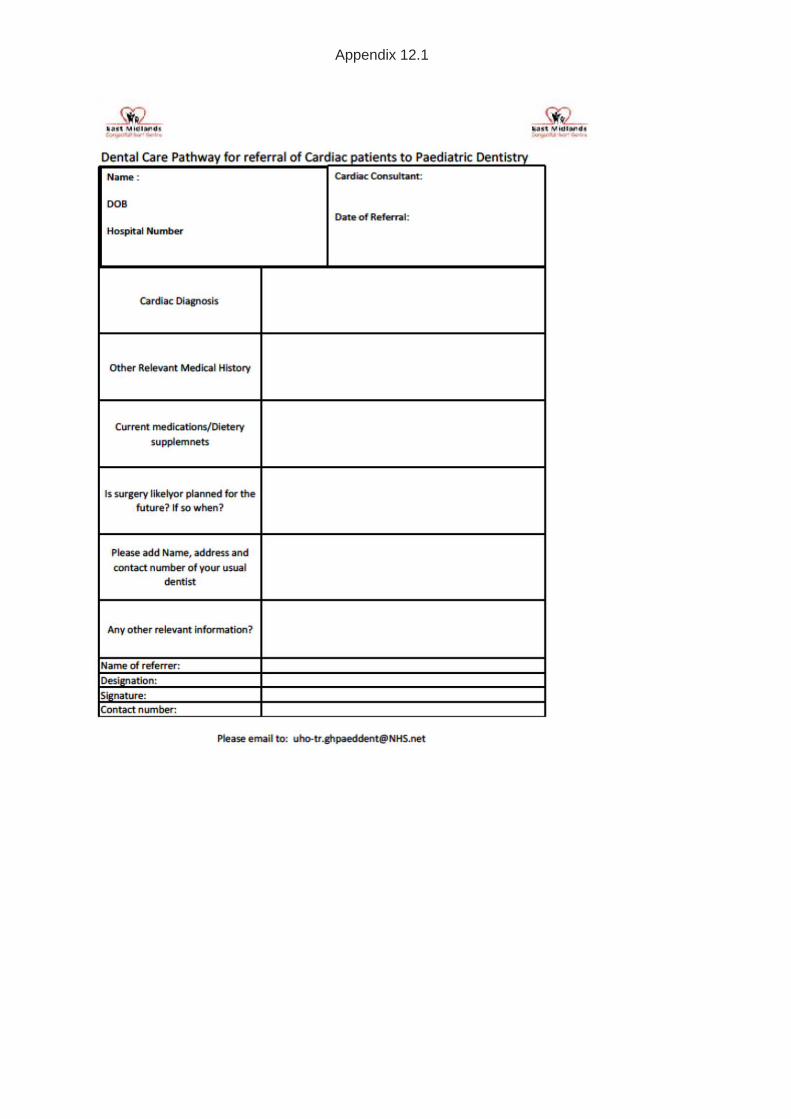
Appendix 12.1
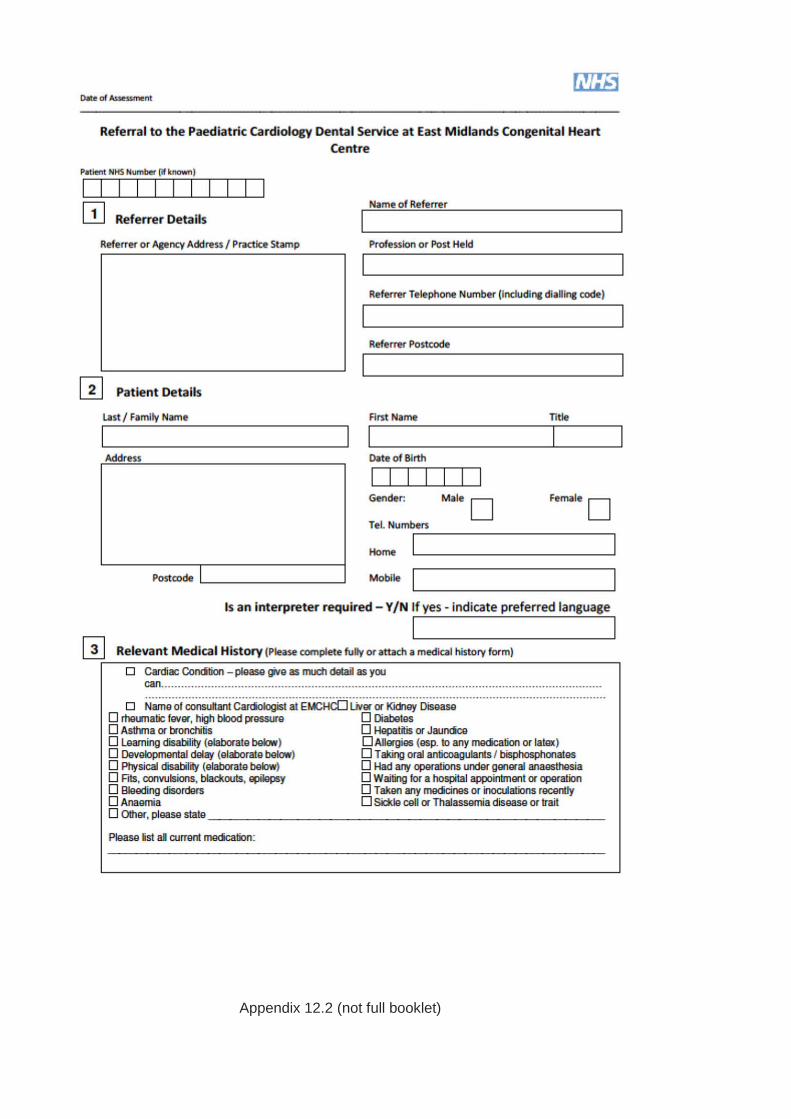
Appendix 12.2 (not full booklet)
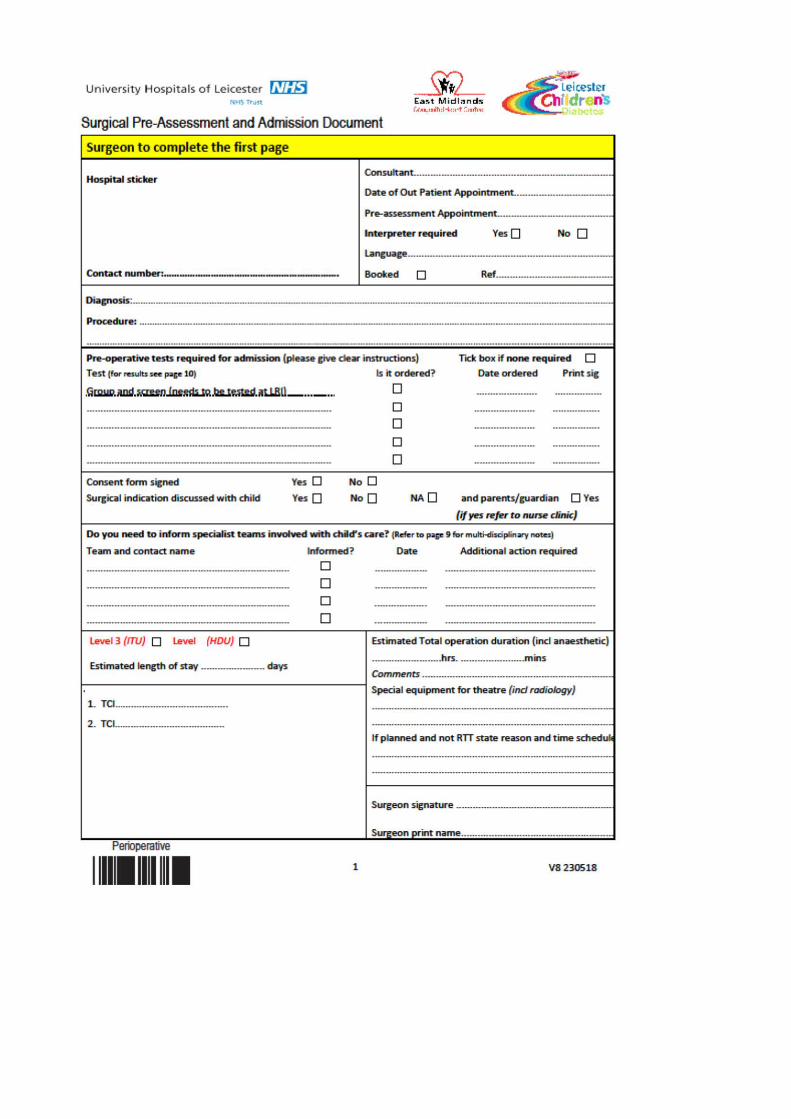

Appendix 12.3
Community Dental Team
Clinic Coordinator to add patient to either non admitted waiting list for assessment, or Admitted waiting list for treatment. EMCHC dental team to confirm which
Electronic referral sent to:[email protected] mailbox
Inform by phone EMCHC dental
team for emergency assessment
Patient seen at Outpatient appointment +/- treatment by
specialist dental team
EMCHC Outpatient Clinic
EMCHC MDT as patient requires intervention or cardiac surgery
Urgent assessment for ? Infective endocarditis
Patient referred by:
Patient added to Admitted waiting list for treatment
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 114
Appendix 12.4
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 115

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 116
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 117
Appendix 13- Transition of patients from paediatric to adult cardiology services
Without structured transfer of care from paediatric to adult cardiology services patients may suffer delayed or inappropriate care, undue emotional stress, and may even be lost to follow up. Robust systems must be in place to ensure that this does not occur and that instead a seamless transition is made between disciplines. This document details the East Midlands Congenital Heart Centre (EMCHC) policy on high quality transition arrangements.
Aims
The transition program should provide uninterrupted health care that is patient centred, age and developmentally appropriate, flexible, and comprehensive. It should include age-appropriate education about medical conditions and promote skills in communication, decision making, self-care, and self-advocacy. It should foster greater personal and medical independence and a greater sense of control over health, healthcare decisions, and psychosocial environment. The ultimate goal of a transition program is to optimize the quality of life, life expectancy, and future productivity of young patients.
Timing of transition
The transition process should start at 12 years of age and be sensitive to the patient’s medical and developmental status as well their wishes. For the majority transition should be complete by 16 years and no later than 18 years.
Setting
Transition should begin in the paediatric cardiology clinic and be completed in the adult clinic. Outpatient booking systems at Glenfield Hospital and in the peripheral clinics should allow for long-term follow up appointments at appropriate intervals (from a few weeks to five years). Inpatients should be managed in age appropriate areas so that on completion of the transition process patients expect to be accommodated within adult cardiology practice and feel comfortable in this setting. In the case of patients with special needs, provision should be made, when necessary, for parents and carers to stay overnight in the hospital.
Process
It is the responsibility of the patient’s named consultant that the EMCHC policy on transition is adhered to. Each patient should have a named liaison nurse as a point of contact and the EMCHC should have a named lead liaison nurse for local and regional services with appropriate training in the transition process.
Transfer of care will occur in the following settings
• from Glenfield paediatric cardiology clinics to Glenfield adult congenital cardiology clinics • from peripheral paediatric cardiology clinics in the region to the equivalent peripheral adult
congenital cardiology clinics where they exist within the same trust or locality • from peripheral paediatric cardiology clinics to Glenfield adult congenital cardiology clinics
where local adult cardiology clinics do not exist • from Glenfield paediatric cardiology to peripheral adult congenital clinic
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 118
The transition plan should be carefully explained to patients and their families both in clinic and a written plan provided to them and their general practitioner. A formal transition document should be produced (a detailed clinic letter will suffice) that outlines the on-going medical and social issues and this should be sent to a named adult congenital cardiologist, the patient and the patient’s GP. A Transition Checklist (copy attached) will be filed in each patients notes and completion will act as an ‘aid memoir’ to the transition process.
If outpatient transition is planned from peripheral to peripheral clinic or from Glenfield to peripheral clinic all efforts should be made to provide a comparable set of notes. These must include, where possible, operation and catheter intervention reports, discharge summaries and clinic letters. Clear instruction should be given to administration staff to ensure that relevant paper work is copied.
Since Congenital Heart Disease is a lifelong condition, EMCHC should have in place a clear policy and system to ensure that notes of congenital heart disease patients at EMCHC should be kept until at least 5 years after the patient’s death.
Content of transition
For patients and parents
Preparation for Transition should really begin at the time of diagnosis of any lifelong condition. Thus the discussion should start early, to prompt parents to ‘envision a future’ for their child, to consider expectations for their child’s education, and their prospects for employment and ultimately for independent living. As patients are prepared to take increased responsibility for their health care, their parents will also need education and support to gradually share and then hand over this responsibility to their child.
Right from initial diagnosis, discussion with parents should therefore include reference to transitional topics (at least couched in terms of current understanding of the situation), to help parents prepare for this shift in responsibility. There should also be acknowledgement that this situation may change over the years as our understanding and management, especially of very complex conditions, evolves.
Preparing the patient for self-care will should begin in early childhood and continue into adulthood to allow the development of the necessary self-care skills. The process will be individually tailored to the developmental stages of adolescence and must acknowledge impact of chronic illness. During childhood, each patient should become increasingly involved in direct discussions about his or her diagnosis, medications, and exercise limitations. In the teenage years, discussions about heart-healthy behaviours and the risks of smoking, alcohol, and drugs will be introduced and reviewed regularly. Self-care education will not terminate on transfer to adult care but will remain an on-going educational process to address life changes. Even patients who remain under the care of the same congenital cardiologist need to undergo a process of transition.
Vocational and employment advice will continue into early adulthood, with facilitated access to National Services such as ‘Connexions ‘as appropriate. Discussions about sex, contraception, risks of pregnancy and inheritance risk (both sexes) will be introduced in an age specific manner and may need to be reemphasised frequently.
Clear communication with the patient’s primary care practitioner during this process is essential as they are often the only ‘constant’ during a period of significant life changes.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 119
Summary of Health Supervision Issues for Primary Care and Hospital Follow-Up Needs
For Patients
1. The timing of transition should be guided by emotional maturity and developmental level (as opposed to chronological age) for transition planning (Class I; Level of Evidence C).
2. The adolescent should be engaged in transition planning (Class I; Level of Evidence C).
3. The adolescent should be asked about their understanding of their disease in relation to their current health status, restrictions on activities, and future goals (Class I; Level of evidence C).
4. The adolescent should be encouraged to share concerns about QOL issues (physical restrictions, school, peers, and social relationships) (Class I; Level of Evidence C).
5. The adolescent’s fears and concerns should be acknowledged in an empathetic, non-judgmental manner (Class I; Level of Evidence C).
6. The paediatric cardiology provider should initiate and work together with the adolescent on a written transition plan (Class I; Level of Evidence C).
7. Providers should begin to direct health discussions more toward the adolescent than the parent (Class I; Level of Evidence C).
8. QOL issues should be discussed privately with the adolescent (Class I; Level of Evidence C).
9. Be flexible (Class I; Level of Evidence C).
For Parents
1. The paediatric cardiology provider should initiate discussions on transition planning in partnership with parents (Class I; Level of Evidence C).
2. The paediatric cardiology provider should solicit information about parental perceptions of their child’s QOL (Class I; Level of Evidence C).
3. The paediatric cardiology provider should encourage discussion of parental understanding of their child’s disease and concerns in relation to future goals (illness management, education, and career) (Class I; Level of Evidence C).
4. The paediatric cardiology provider should be non-judgmental and empathetic when acknowledging fears70 (Class I; Level of Evidence C).
The adult congenital cardiology providers will respect the therapeutic plan that was established by their paediatric cardiology colleagues and represent this in their communications with young patients and their families. However it must also be clear that the care of congenital heart patients evolves, and is a process of continual re-evaluation. Clear and tactful communication of this to patients is essential to maintain trust and sustain healthy life-long therapeutic relationships.
References
Adult Congenital Heart Disease: A commissioning guide for services for young people and Grown Ups with Congenital Heart Disease (GUCH). Department of Health
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 120
2006. http://www.dh.gov.uk/dr_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4134696.pdf
Sable C, Foster E, Uzark K, et al. Best practices in managing transition to adulthood for adolescents with congenital heart disease: the transition process and medical and psychosocial issues: a scientific statement from the American Heart Association. Circulation 2011 Apr 5; 123(13):1454-85. http://circ.ahajournals.org/content/123/13/1454.full.pdf
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 121
Appendix 14 - Minimise loss of patients to follow up (transition & transfer)
EMCHC has a robust approach to minimising loss to follow-up in recognition of the complex nature of many of our patient’s conditions, and their associated vulnerability. Therefore we have an SOP involving both our liaison nurse team and Safeguarding Services (attached) in order to minimise loss to follow-up. In house, we have Did Not Attend (DNA) labels which must be attached to the case record indicating the DNA or ‘Was Not Brought’ (WNB), and actions taken.
The process is similar for our outreach clinics and all our liaison nurses can access the NHS Spine to ensure as far as possible that correct addresses are being used. Where on-going follow-up is deemed important for children and vulnerable adults, the full range of approaches to ensure attendance will be applied, including identifying individual cases to the MDT forum, followed by recourse to social services when appropriate.
Competent adult patients cannot be forced to attend clinics and persistent non-attenders (whether through transition or older) therefore will be returned to the care of their GP once all appropriate avenues to encourage attendance have been explored.
Discharges are tracked by our audit team and those associated with serial non-attendance (as opposed to planned discharge or referral elsewhere) are identified by age group and new / follow-up, which will also capture our patients transitioning from paediatric to ACHD services. Along with all our dashboard data, these will be reviewed on a regular basis in our QUICKA meetings (our weekly quality improvement meetings) which are also open to Network members. They will also be shared across the Network via the Network Board.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 122
DNA - Standard Operating Procedure.
DNA/WNB label for notes
Inform Consultant
Inform if Previous DNA/WNB
1st WNB • Phone Parents and rebook appointment
• Letter to be sent to parents of new ap-pointment details
• WNB sticker put in patient notes.
Paediatric WNB
Did Not Attend/ Was Not Brought Standard Operating Procedure For EMCHC patients.
Adult DNA
1st DNA • Phone Patient
• Rebook appointment and send out letter
• DNA sticker placed in notes.
2nd DNA • Inform Consultant.
• DNA sticker placed in notes
• Letter sent to GP and Patient discharging them from the service as per trust policy.
Existing Patients with complex cardiac conditions.
• Inform Consultant / MDT discussion
• Referral to Adult/Paediactric safeguarding team. if patient is deemed to lack mental capacity or has learning disabilities.
• If appropriate, complete A form
New Patient Referrals • Inform Consultant / MDT discussion
• Referral Made to child safe guarding team as per trust policy.
• Letter sent to GP and parent informing them of Discharge from service and referral to safeguarding team.
2nd WNB
DNA/WNB Pt details Correct Yes No
Date Last seen :
No of Previous DNA/WNB
Consultant Decision:
Rebook appointment D/C back to GP
Ref to safeguarding team CLN Aware

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 123
Appendix 15 - Adult Congenital Cardiac Care
ACHD Care Pathways
Transition frompaediatric cardiology• Network clinic• EMCHC
GPAdult cardiology• Network hospital• EMCHC
ClinicalGenetics
Other Network• Patient relocation• Patient preference
Outpatient clinics• Network• EMCHC Cardiology consultation Liaison nurse ECG, echo, tapes
Care plan
Surgery or intervention
EMCHC MDT• incorporating ZOOM
Waiting list
Admit to EMCHC
Networkhospital A&E
InpatientNetwork hospital
Treatment• catheter intervention• surgery
1st follow up at EMCHC• Intervention clinic• Surgical clinic• “ward review”
Self-referral
Outpatientfollow up
Furtherinvestigation
Surgical or intervention clinic• Consultant• liaison nurse• Pre-admission
Glenfield CDU
LRI A&E
Referral pathway
Elective pathway
Acute pathway
Treatment pathway
Follow up pathway
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 124
Appendix 16 – Neonatal services and Neonatal Transport
CenTre Neonatal Transport Service
Operational Guidance
V1 Aug 2015

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 125
Section Title Page
1 Introduction 3
2 The scope of the service 3
3 The referral process 4
4 Team activation 6
5 Operational hours 7
6 Advice calls 8
7 Documentation 9
8 In transit 10
9 Equipment 10
10 Responsibility for patients 11
11 CenTre team 13
12 Parents 14
13 Triage 14
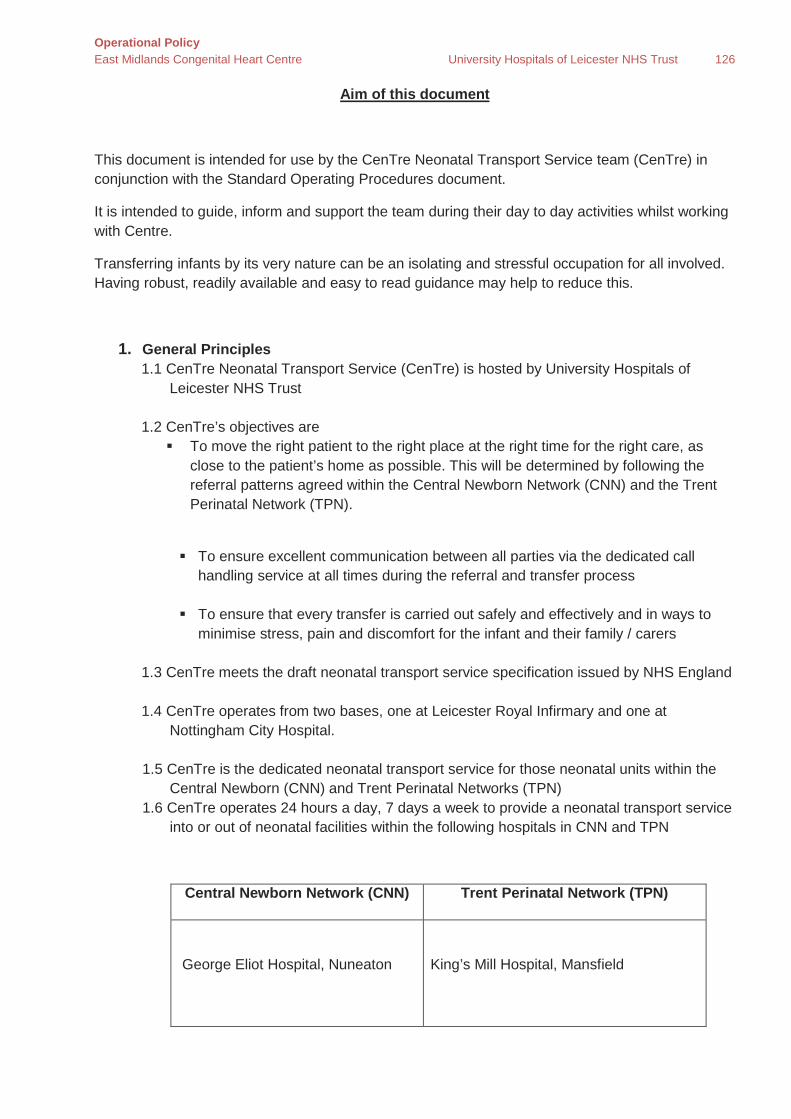
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 126
Aim of this document
This document is intended for use by the CenTre Neonatal Transport Service team (CenTre) in conjunction with the Standard Operating Procedures document.
It is intended to guide, inform and support the team during their day to day activities whilst working with Centre.
Transferring infants by its very nature can be an isolating and stressful occupation for all involved. Having robust, readily available and easy to read guidance may help to reduce this.
1. General Principles 1.1 CenTre Neonatal Transport Service (CenTre) is hosted by University Hospitals of
Leicester NHS Trust 1.2 CenTre’s objectives are To move the right patient to the right place at the right time for the right care, as
close to the patient’s home as possible. This will be determined by following the referral patterns agreed within the Central Newborn Network (CNN) and the Trent Perinatal Network (TPN).
To ensure excellent communication between all parties via the dedicated call
handling service at all times during the referral and transfer process
To ensure that every transfer is carried out safely and effectively and in ways to minimise stress, pain and discomfort for the infant and their family / carers
1.3 CenTre meets the draft neonatal transport service specification issued by NHS England 1.4 CenTre operates from two bases, one at Leicester Royal Infirmary and one at
Nottingham City Hospital. 1.5 CenTre is the dedicated neonatal transport service for those neonatal units within the
Central Newborn (CNN) and Trent Perinatal Networks (TPN) 1.6 CenTre operates 24 hours a day, 7 days a week to provide a neonatal transport service
into or out of neonatal facilities within the following hospitals in CNN and TPN
Central Newborn Network (CNN) Trent Perinatal Network (TPN)
George Eliot Hospital, Nuneaton
King’s Mill Hospital, Mansfield
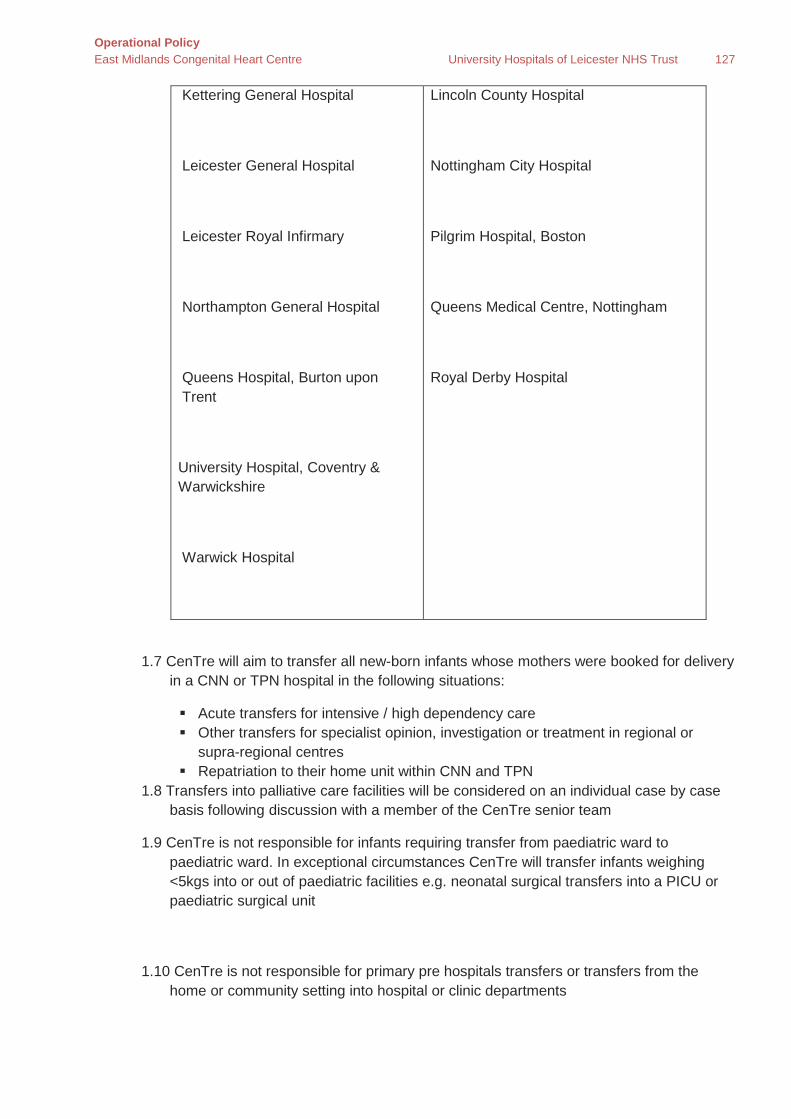
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 127
Kettering General Hospital
Leicester General Hospital
Leicester Royal Infirmary
Northampton General Hospital
Queens Hospital, Burton upon Trent
University Hospital, Coventry & Warwickshire
Warwick Hospital
Lincoln County Hospital
Nottingham City Hospital
Pilgrim Hospital, Boston
Queens Medical Centre, Nottingham
Royal Derby Hospital
1.7 CenTre will aim to transfer all new-born infants whose mothers were booked for delivery in a CNN or TPN hospital in the following situations:
Acute transfers for intensive / high dependency care Other transfers for specialist opinion, investigation or treatment in regional or
supra-regional centres Repatriation to their home unit within CNN and TPN
1.8 Transfers into palliative care facilities will be considered on an individual case by case basis following discussion with a member of the CenTre senior team
1.9 CenTre is not responsible for infants requiring transfer from paediatric ward to paediatric ward. In exceptional circumstances CenTre will transfer infants weighing <5kgs into or out of paediatric facilities e.g. neonatal surgical transfers into a PICU or paediatric surgical unit
1.10 CenTre is not responsible for primary pre hospitals transfers or transfers from the home or community setting into hospital or clinic departments
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 128
1.11 CenTre does not undertake airborne transfers, although it may agree to provide the ground transportation to / from the aircraft where the air transfer is undertaken by another service
2. The referral process
2.1 To activate the transfer process the referring unit team should contact CenTre via the dedicated call handling service on 0300 300 0038
2.2 All calls will be recorded for training and governance purposes, all participants of calls must be made aware of this
2.3 The call centre will accept calls from:
Obstetric services in order to locate a maternal bed and neonatal cot in order to activate an in-utero transfer. These transfers are not undertaken by CenTre. It is the responsibility of the referring obstetric team to organise appropriate staff and ambulance in order to carry out the transfer safely
Staff from one of the neonatal units within CNN or TPN who require a transfer Staff from other neonatal units in hospitals outside of CNN and TPN who require
transport into or out of a neonatal unit in a CNN or TPN hospital Staff from other neonatal / paediatric transport services who may request the
support of CenTre teams during times of high demand on their resources. Such requests are at the discretion of the Transport Consultant
2.4 Emergency referrals are those which could not necessarily have been planned for. They may be referred to as Uplift or Capacity transfers
The referring unit should contact CenTre via the dedicated call handling service The call handler will utilise agreed algorithms to identify which CenTre team
personnel to direct the call to
Initial demographic and clinical background details will be recorded on the CenTre documentation
The Transport Nurse and Registrar / ANNP will be included in this initial referral
call as standard practice The Transport Consultant’s inclusion in the referral can be requested by anyone at
any point during the referral process if further expertise or decision support is required. It is expected that the Transport Consultant will be involved in the referral process for the following transfers (although this list is not exclusive):
o An infant being transferred into or out of PICU o All surgical referrals o All cooling referrals o Anticipated need for inhaled nitric oxide in transit o All palliative care

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 129
o Any request for transfer where the condition of the infant at referral is felt to be unstable
A call conference involving all parties can be initiated by anyone involved in the call at any time. The call centre team will facilitate this.
For emergency referrals CenTre will locate the closest appropriate cot. 2.5 Time Critical referrals are identified by certain criteria set down by the National
Transport Group. This list is not exclusive and there may be locally agreed additions.
o An infant with a gastroschisis o A ventilated infant with a tracheo-oesophageal fistula +/- atresia o An infant with an intestinal perforation o An infant with a duct dependent lesion that is not responding to an
infusion of Prostin o Any unstable infant with either respiratory or cardiovascular
instability not responding to appropriate management 2.6 CenTre will aim to dispatch an appropriate team within 60 minutes of receiving the
initial call for all time critical referrals. 2. 7 Where demand exceeds team availability the Transport Consultant will make priority
decisions based on clinical condition of the infants referred. 2.8 Planned referrals are usually anticipated and include transfers back to local units
(repatriations); infants referred for elective surgery (including PDA ligations) and out patients investigations.
CenTre does not locate a cot for planned transfers – the initial referral and securing
an appropriate cot should take place between the referrer and the receiving unit prior to contacting CenTre.
At least 24 hours’ notice is recommended for planned transfers although if
workload allows same day transfers may be considered. Where the proposed transfer may be anticipated to require the prolonged
attendance of a CenTre team, e.g. for a PDA ligation or long distance transfer, then 48 hours’ notice is preferable.
The referring unit contact CenTre via the dedicated call handling service. The call handler will utilise agreed algorithms to identify which CenTre team
personnel to direct the call to.
Initial demographic and clinical background details will be recorded on the CenTre documentation.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 130
4. Team activation
4.1 The decision to activate a team is based on clinical information received from the referring unit.
4.2 All decisions will be documented on the CenTre transport paperwork.
4.3 All calls via the dedicated call handling service are recorded and stored.
4.4 One person transfers are usually undertaken by a trained transport nurse.
4.5 The decision to dispatch a single person team will be made following a comprehensive referral of the infant’s condition and after discussion with senior team members on duty.
4.6 Examples of infants suitable for single person team transfers may include, but are not limited to:
o A stable infant requiring back transfer or transfer for on-going special care
o A stable infant requiring transfer for an outpatient appointment / special investigation not requiring sedation
o A stable baby requiring transfer for specific investigation, intervention or surgical procedure / review
o A stable infant requiring transfer due to cot capacity issues o A stable infant receiving low flow oxygen therapy
For the purposes of single-person transfers a stable infant is defined as:
o Not requiring respiratory support in the form of mechanical ventilation, high flow oxygen therapy or CPAP.
o Not on inotropes or Prostin. o No central or umbilical lines in situ
The ultimate decision to dispatch a single person team to undertake transport lies with the transport consultant.
4.7 Two person transfers will usually be undertaken by a CenTre trained transport nurse and a doctor. An ANNP may take the place of either team member
4.8 Final team composition will be decided by the Transport Consultant based on the
knowledge and skills of staff available and the clinical condition of the infant requiring transfer
4.9 Examples of infants requiring two person team transfers may include, but are not
limited to:
o All infants requiring respiratory support such as endotracheal intubation and ventilation or CPAP
o Any infant with a newly formed tracheostomy o Any infant having regular desaturations and / or bradycardias as they
may require intubation or CPAP for the transfer

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 131
o Any infant on high flow oxygen, as such infants will require CPAP for the transfer
o Any infant requiring regular suction e.g. tracheosophageal fistula with a Replogle tube in situ
o Any infant requiring cardiovascular support e.g. an infusion of Prostin /inotropes or fluid boluses
o Any baby with a UAC or peripheral arterial line in situ
o Any baby with a chest drain in situ
o Any baby transferred for palliative care o Any baby who is having or has recently had convulsions
o Any unstable baby requiring surgery, intervention or investigation
o Any baby weighing less than 750g. Between 750g and 1000g a doctor / ANNP will usually attend the transfer but if the infant is otherwise well and at
the discretion of the transport nurse this requirement may be waived. 5. Operational hours
5.1 CenTre operates 24 hours a day, 7 days a week 5.2 There are 3 day time teams comprising of:
o One single person team with 2 crew from East Midlands Ambulance Service (EMAS)
o Two 2 person teams each with one EMAS crew member each 5.3 There is one night time team comprising of a 2 person CenTre team with 2 EMAS
crew members
5.4 The daytime teams will commence work from 07:45hrs and finish at 20:15hrs
5.5 The night time team will commence work at 19:45hrs and end at 08:15hrs 5.6 Teams will not usually be expected to depart their base office for transfers that will
predictability make them over 1 hour late finishing their shift. 5.7 Exceptions to this may include but are not limited to:
o Where the Transport Consultant deems that the life of the infant is in danger if delivery of transport expertise is delayed
5.8 Team Relief: - If a team are still out on a transfer at the start of the next shift the
Transport Consultant will be contacted and told that a relief team is being sent out. In the majority of circumstances the relief team will be from the same base as the late running team. They will begin to travel towards the late running team as soon as all team members / EMAS crew are available.
o If the late running team are able to leave the referring unit before the relief team arrive and are transferring the infant to their base hospital they should be allowed to continue with the transfer. In such circumstances the relief team will return to base.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 132
o If the late running team are able to leave the referring unit but are transferring the infant to another unit they should agree on a safe location to handover the infant to the relief team. In such circumstance the teams will swap vehicles i.e. the late running team will use the new vehicle to return to base and the relief team will take the original vehicle and infant on to the receiving unit.
5.9 Planned transfers will usually take place during the normal day shift working hour.
5.10 Planned transfer will not usually be undertaken during the night shift as this could lead to a delay should an emergency referral be received.
5.11 The consultant covering CenTre may authorise a planned transfer by the night team if:
o The transfer cannot reasonably be deferred to the following day o The transfer is not long distance, where it would occupy the team for
the whole night o The team can be diverted at short notice should a clinically more
important referral be received, this may mean the medic accompanying the nurse
5.12 Emergency transfers may be undertaken at any time 5.13 Dispatch of the night team for an emergency transfer should be done after
consideration of the need for the infant to be transferred during the night. The result of dispatching the night team means there is no other neonatal facility available in CNN and TPN until that transfer is completed
5.14 An emergency transfer may be deferred until the morning if:
o It is deemed clinically appropriate by the Transport Consultant and the referring and receiving teams
o There is no clinical urgency to deliver the infant to a site of definitive care
6. Advice Calls
6.1 Advice calls may form part of the transport process or be independent of any request for transfer.
Advice should only be given by a member of the CenTre team when it falls into their area of expertise. This area will vary according to the team member’s background and experience
6.2 Any request for advice should be made via the dedicated call handling service to ensure all calls are recorded
6.3 CenTre will operate as the facilitator for the advice calls but not necessarily the provider of the advice.
6.4 Advice may come from 4 sources:
o The CenTre Neonatal Transport team o The receiving / accepting team
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 133
o A 3rd party consultant (in a tertiary centre) who would not normally have responsibility for the infant
o A member of a specialist team e.g. neurosurgery or cardiology
6.5 The clinician giving advice is responsible for their advice, accepting that it is based on the information provided to them and they are unable to insist that such advice is acted upon
6.6 Where advice is sought in relation to a potential transfer of an infant it is acceptable
for the CenTre team including the Transport Consultant covering to offer advice 6.7 Where advice is sought but does not relate to a potential transfer of an infant it is
acceptable for the CenTre call handling service to facilitate a conference call between the referrer and senior medical staff in their network lead unit
7. Documentation
7.1 Patient identification o All calls concerning individual infants will have basic details
recorded by the centre call handling team. o A unique identification number will be allocated by the centre call
handling team. o Where possible the infants NHS number should be recorded. o The infant’s first name, family name and date of birth will be
recorded on the top of every page of the CenTre transport documentation.
o All infants will have 2 name-bands in situ. These will be checked with the staff in the referring unit and receiving unit and will be clearly recorded as doing so in the transport documentation.
7.2 All calls will be documented using the Centre initial referral form and then the
appropriate transport form.
7.3 Completed transport documentation will form part of the infants clinical records – a copy will be left with or posted on to the receiving team.
7.4 Each member of the CenTre transport team that accompanies the infant will be
expected to write in the transport notes. Each entry must be dated and signed.
7.5 All relevant sections of the CenTre transport documentation must be completed 7.6 Any documentation that is faxed must be sent with a fax covering form and
confirmation of its arrival must be obtained 7.7 As part of the CenTre patient records the relevant parts of the documentation will
be completed for any advice given and for all transfers undertaken. This will include:
o Details of the CenTre team.
o Operational data.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 134
o Additional history and notes.
o Initial assessment.
o Summary of interventions.
o Mandatory observations (at ‘first look’, prior to departure and on arrival at the receiving hospital).
o A record of any safeguarding issues.
o Documentation of discussion with parents.
o Transport Interest Group dataset items.
o Regular observations from the time of ‘first look’ until handover at the receiving hospital. These will be completed at a minimum of every 30 minutes and will include a record of any acute interventions.
o Pre-departure checklist.
o Handover details at the receiving hospital.
o Transfer outcome.
o Safeguarding information (child protection/vulnerable adults).
o A record of any adverse events (in addition to Trust incident reporting procedure).
o Any other information relevant to the retrieval.
7.8 All untoward incidents and adverse events will be recorded in the infant’s transfer notes. In addition the relevant untoward incident form will be completed and forwarded to the appropriate Risk Management Department. The appropriate members of the CenTre senior team should be made aware of any untoward incidents.
7.9 Copies of the CenTre notes, as completed to that point, will be left at the receiving unit to form part of their clinical notes. The final part will be returned to CenTre to complete the records for that episode. All notes should be stored in accordance with the UHL Documentation Policy for Patients’ Case Notes.
8. In transit
8.1 The infant will be securely restrained in the transport incubator using the appropriate harness
8.2 The transport system will be securely locked into place in the ambulance before
beginning the transfer 8.3 All personnel in the ambulance will wear the supplied restraining seat belts at all
times the vehicle is in motion 8.4 All equipment bags, milk cool bags, parents’ / or infants luggage etc. must be
securely restrained before the transfer begins
8.5 CenTre will only transfer small amounts of frozen expressed breast milk
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 135
8.6 Regular observations will be recorded on the Centre transport documentation
during the transfer. The frequency of observations is dependent upon whether it is a one or two person transfer.
8.7 On a one person transfer if the clinical condition allows it is acceptable for
observations to be recorded every 30 minutes
8.8 On a two person transfer it is recommended that observation be recorded every 15 minutes
8.9 CenTre transport team personnel and any passengers travelling with the team will
not distract the driver of the ambulance whilst it is in motion unless there is an emergency that they need notifying about
9. Equipment
9.1 CenTre transport systems are configured to allow for single infant transfer only 9.2 The transport incubator will allow for the transfer of infants up to approximately 5kg
in weight.
9.3 All CenTre transport systems are fitted with infusion pumps, a multi parameter monitor, a ventilator, a suction unit and an oxygen analyser
9.4 All systems have the facility to securely add a Nitric Oxide delivery system to them
9.5 All equipment is maintained by Medical Physics departments at the University
Hospitals of Leicester NHS Trust (UHL) and Nottingham University Hospitals NHS Trust (NUH)
9.6 All equipment is cleaned in conjunction with the guidance from the Infection
Prevention teams at UHL and NUH
9.7 All faults relating to equipment must be reported to the appropriate Medical Physics department.
9.8 All CenTre transport nurses will be trained and assessed as competent at using the
CenTre transport systems.
9.9 CenTre medical staff will receive training on how to safely use the transport systems on commencing work either with CenTre or on the neonatal units at UHL and NUH.
9.10 All CenTre transport systems will be checked at the start of every shift. Kit checks
will be recorded and kept for reference.
10. Responsibility for patients 10.1 The transfer of infants by CenTre necessitates that care is handed over from the
referring hospital to the transport team and thereafter at the receiving hospital to
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 136
the receiving hospital team. With this handover of care is also a handover of responsibility for the patient.
10.2 Central to any consideration of responsibility is the understanding that a patient’s best interests remain paramount throughout the transport process.
From referral to handover to transport team
10.3 The infant remains the sole responsibility of the referring hospital team (and
consultant) until an adequate handover to the CenTre team has been completed. This can only take place once the CenTre team has arrived in the referring hospital.
10.4 The referring team is responsible for the stabilisation and on-going care of the patient and should continue to provide the highest available levels of care until the CenTre transport team has arrived and the patient has been handed over to them.
10.5 During this time the referring hospital team may be given advice from the transport service or a third party (such as the receiving unit/other specialist clinician) but is responsible for providing adequate information upon which that advice is obtained and for deciding whether or not to act in accordance with that advice.
From handover in the referring hospital to handover in the receiving hospital.
10.6 The infant becomes the primary responsibility of the CenTre team at completion of the handover by the referring hospital. The Transport Consultant assumes ultimate responsibility for the patient at this time.
10.7 This does not mean that the Referring consultant(s) and team relinquish all responsibility for the infant to the CenTre team at handover but rather that the consultant(s), as the senior clinician(s) present and other responsible staff within the referring hospital, should render to the CenTre team any assistance necessary to enable the safe preparation of the infant for transfer.
10.8 The infant remains the CenTre team’s primary responsibility until an adequate
handover to the receiving team has been completed. Responsibility for the infant passes completely over to the receiving team once they have been transferred from the transport equipment and, where required, stabilised on the receiving team’s life support equipment.
10.9 It is expected that upon arrival at the receiving hospital, the receiving team would,
if necessary, render to the CenTre team any immediate assistance necessary for the welfare of the infant. This may take place even before the handover process has been completed.
10.10 On rare occasions additional support of the CenTre team may be required (e.g. to facilitate a scan on arrival). This should be agreed with the team at the earliest opportunity. Under these circumstances the primary responsibility for the infant rests with the receiving team. The CenTre team will act solely as technicians for the safe transfer of the infant using CenTre team equipment.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 137
During transfer
10.11 During the transfer of an infant from the place of care in the referring hospital until arrival at the place of care in the receiving hospital, the CenTre team is solely responsible for the infant’s welfare.
10.12 The Transport Consultant is ultimately responsible for the infant during the transfer. This line of responsibility is maintained despite a lack of physical proximity.
10.13 During this time the CenTre team may act upon advice from a third party (e.g. from the receiving unit / other specialist clinician) but is responsible for providing adequate information upon which that advice is obtained and for deciding whether or not to act in accordance with the advice.
10.14 Due to the two-base structure of CenTre it may be appropriate for the nominated Transport Consultant to formally pass the Transport Consultant responsibility for an individual transport over to the Consultant who will be receiving the patient at the other base. This may be appropriate for example where the Transport Consultant has multiple complex transport demands. For this to happen there must be a direct conversation between the two Consultants involved. The CenTre team attending the transfer must also be directly informed
Nurse, ANNP or trainee medical staff delivered transfers.
10.15 The responsibility and accountability arrangements continue to apply when transfers are delivered by transport nurses, advanced nurse practitioners or trainee medical staff acting independently.
Before accepting responsibility for an infant the transport nurse should independently assess that infant and decide whether or not the transfer is within his/her experience and competence. Should he/she decide that this is not the case, responsibility remains with the referring team until such times as alternative arrangements can be made.
11. CenTre Team 11.1 The CenTre team consists of:
o Nurse Consultant o Consultant Neonatologists o Paediatric trainee doctors o Advanced neonatal nurse practitioners o Nurses specifically trained in neonatal intensive care o Dedicated ambulance service personnel, technicians and emergency
care assistants who drive our dedicated ambulances o Dedicated call handling team o Dedicated clerical support
11.2 All staff receives a site specific orientation and induction
11.3 In order to be a competent CenTre transport nurse every nurse must complete a
comprehensive competency document. This is both self, peer and transport educator assessed.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 138
11.4 Upon completion of their induction new transport nurses are accompanied on
transfers by colleagues and the transport educator in order to achieve the required level of competency before being signed off
11.5 Progress of trainee transport nurses is monitored at regular intervals by the
transport educator and plans are put in place to ensure the required level of competency is reached
11.5 Records of completed competency records are kept by the transport educator
11.6 Medical staff working for CenTre receives an induction and basic training on the
equipment to ensure they are a safe competent practitioner before being rostered to undertake independent transports.
12. Parents
12.1 The CenTre transport team will keep parents fully informed of all aspects of their infants care.
12.2 All discussions / communications with parents will be recorded in the transport
documentation
12.3 Discussions will include: o The nature of the condition affecting their infant o The reason for the transfer o A detailed explanation of the transfer process
12.4 CenTre will not take consent for a 3rd party procedure e.g. laparotomy
12.5 CenTre will not take formal written consent for the transfer
12.6 Where possible and appropriate, parent(s) may be invited to travel with their infant.
In doing so they will be asked to abide by the safety precautions as identified by the CenTre transport team
12.7 Parents must be medically fit in order to travel with their infant
12.8 The CenTre team cannot take responsibility for the health of a parent accompanying
their infant
12.9 Mothers who have recently given birth and wish to travel with their infant must have been discharged from obstetric care and must be 72 hours post delivery
12.10 Should a parent become unwell whilst travelling with the CenTre transport team,
immediate assistance should be offered but will only be equivalent to that of an ordinary member of the public?
12.11 Parents will be offered an information leaflet informing them about CenTre Neonatal
Transport Service and any questions will be answered as clearly as possible by the transport team
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 139
13. Triage
13.1 At times the demands made on CenTre will exceed the resources available. At these times workload will be prioritised on a clinical need basis
13.2 The highest priority will be given to infants who:
o Have a time critical diagnosis requiring transfer to a specialist hospital where delay may result in worsening prognosis, or
o Unstable infants where the referring team are struggling to achieve physiological control
13.3 Triage will be performed by the Transport Consultant following discussions via the
dedicated call handling service with all of the clinical teams involved
13.4 It may be possible to raise additional transport resources by:
o Requesting transport nurses be released from NICU work o Consultant undertaking transfers o Seeking assistance from adjacent transport services
13.5 The availability of additional resources may be used flexibly to ensure that the
clinical needs of the infants are given appropriate priority
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 140
Appendix 17- Paediatric Intensive Care Pathway
Paediatric Admission & Discharge Criteria to CICU & PICU
1. Introduction & Scope
The following document provides a framework for all admissions and discharges to the Children’s Intensive Care Unit (CICU) and the Paediatric Intensive Care Unit (PICU). This document only applies to patients admitted or discharged from CICU or PICU. The document should also apply to inter-unit transfers except where these are covered by the relevant CoMET guidance.
2. Admission Criteria:
• All admissions to CICU/PICU must be approved by the duty PICU Consul t ant. • All admissions must have an admitting parent specialty Consul t ant • Referrals to PICU / CICU should be Consultant to Consultant when at all possible
2. Discharge Criteria
• All discharges from CICU/ PICU must be approved by the duty PICU consult ant • The parent specialty team/Consul t ant should be informed of the discharge • All patients should be accompanied by a discharge summary, which should be verified by
the Consultant within 24 hours • The potential discharges should be identified at each ward round. • Children will be identified by the PICU team as approaching “ready for discharge” status.
(08:30h, 16:00h, and 20:30 h). • Patients in the CICU/PICU should be evaluated and considered for discharge based on the
reversal of the disease process or resolution of the unstable physiologic condition that prompted admission to the unit. Suitable area for transfer (HDU/ Single room/ Ward) will be identified as per their clinical requirement.
Suitability for transfer/discharge will be based on the following:
1. Stable haemodynamic parameters.
2. Stable respiratory status (patient extubated with stable blood gases) and airway patency.
3. Minimal oxygen requirements that do not exceed ward or HDU guidelines
4. Intravenous inotropic support, vasodilators, and antiarrhythmic drugs are no longer required or, when applicable, low doses of these medications can be administered
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 141
safely in otherwise stable patients in a ward or HDU.
5. Cardiac dysrhythmias are controlled.
6. Neurologic stability with control of seizures.
7. Chronically mechanically ventilated patients whose critical illness has been reversed or resolved and who are otherwise stable may be discharged to a ward or to HDU if they continue to need the same level of respiratory support as before while they were at home.
8. Routine peritoneal or haemodialysis with resolution of critical illness not exceeding ward guidelines.
9. The health care team and the patient’s family, after careful assessment, determine that there is no benefit in keeping the child in the CICU / PICU or that the course of treatment is medically futile.
3. Categories of Discharge
• Category 1 Routine. Critical Care has a least one available bed. Patients will be discharged within 4 hours.
• Category 2 Urgent. Critical care areas have no available space i.e. reached capacity. Patients will be discharged within 2 hours
• Category 3 Time Critical*. Critical Care has no available space and a critically ill patient requires immediate admission. Patient will be discharged as quickly as possible.
*This situation is not desirable and may result in a compromise to patient safety.
4. Further considerations:
ALL discharge summaries should be reviewed and signed by the Duty Consultant prior to discharge. If this is not possible they should be presented to the Duty Consultant within 25 hrs.
Discharge Summaries should be started by the night shift person and then completed after the Consultant Ward round.
Discharges should ensure the management plan is communicated clearly and child protection procedures or concerns must be specifically detailed.
It is a rare occurrence for a child to be discharged home straight from CICU/PICU and should only be done with the specific approval of the duty PIC Consultant and Parent Specialty team.
The final decision to discharge should be confirmed by the CICU/PIC Duty Consultant and Parent Specialty team.
5. Discharge Procedure:
Timing of patient discharge from critical care impacts on the outcome of the patient. Poor planning may result in disruption of care, delayed recovery and high readmission rates. It has been shown that discharge at night increases patient mortality. It has been recommended that transfer from critical care areas to the general ward between 20:00 and 07:00 should be avoided and documented as an adverse event if it occurs.
5.1 When discharging to another Ward:
• Inform the Bed Co-ordinator of the discharge
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 142
• Inform Parent Specialty team of imminent discharge
• Complete the Discharge Summary
• Print Discharge Summary letter to accompany patient ensure signed by Consultant. Copy to the GP and referring hospital.
• Perform clinical review & early warning score immediately prior to discharge to confirm suitability
• PICU Nurse to handover to Ward Nurse
5.2 When Discharging to another Hospital
• Discuss with PIC Consultant and Parent Specialty team
• Inform PIC Nurse in Charge of anticipated need for transfer arrangements
• Inform accepting hospital Consultant
• Inform GP when transfer is to a hospice
• Inform accepting Ward Nurse in Charge
• Complete the Discharge Summary and ensure plans are clearly documented especially drain/central line removal
• Print Discharge Summary letter to accompany patient, ensure signed off by Consultant. Copy to the GP and referring hospital.
• Perform clinical review & early warning score immediately prior to discharge to confirm suitability
• Appropriate transfer team/nurse to accompany patient
The discharge of any patient from critical care involves planning however it is especially important to plan the discharge of long term or complex patients. Defining this group is difficult but should include all patients who have required Critical Care for greater than 2 weeks. Patients, their relatives and ward staff all need time to prepare for the discharge. Specific needs must be identified as soon as practical. Specialist services will need time to co-ordinate all aspects required for continuing care. This may take several days but the process should start before they are ready for discharge to ensure that a timely discharge from Critical Care.
6. Access to Regional Specialist Services
If a Specialist Service is commissioned in the Critical Care unit, it may be necessary to discharge patients to another critical care unit if they are not able to transition from critical care if the Specialist Service is no longer required. It is essential that regional specialist services are protected by avoiding any undue delay in discharge.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 143
The possibility of discharge to another critical care facility needs not only agreement between the PICU Consultant but also agreement of the referring team in the tertiary centre and in the non-specialist unit. The patient’s requirements are paramount to any change of facility.
7. Roles & Responsibilities
7.1 Medical Staff
The final decision that a patient is fit for discharge/step down from critical care remains with the Critical Care Consultant. It is essential that the parent team (or their representative out of hours) is aware of all discharges.
7.2 Nursing Staff
It is the nursing staff’s responsibility to ensure a safe and timely discharge of a patient from critical care areas once a bed has been identified. Unless there is an immediate threat to capacity on the critical care unit, discharges must not occur within the hours of 20:00 and 07:00. They must also ensure all documentation is complete to accompany the patient. For patients with complex needs and those classed as long-term patients, the Nurse in Charge of the receiving area must ensure that a face to face handover has been obtained whilst in the critical care unit.
7.3 Bed Co-ordinator
It is the responsibility of the bed co-ordinator to ensure identification of an appropriate bed in conjunction with key stakeholders and within the timescale appropriate for the capacity of the critical care area. Patients should be cared for in the most appropriate setting and maximise availability of critical care capacity.
8. Handover of Care
The discharging team and the receiving team both have a responsibility to ensure the appropriate care of the patient being discharged. They should ensure:
• There is continuity of care facilitated by a formal structured handover of care from critical care area staff to ward staff (including both medical and nursing staff), supported by a written plan.
• That the receiving ward, with support from critical care if required, can deliver the agreed plan.
When patients are transferred to the general ward from a critical care area, they and their parents/carers should be offered information about their condition and encouraged to actively participate in decisions that relate to their recovery. The information should be tailored to individual circumstances.
8.1 A Structured Handover Must Include:
• A summary of the critical care stay, including diagnosis and treatment and a full history of any long term and complex needs the child may have.
• A monitoring and investigation plan
• An escalation plan should deterioration of the child occur
• A plan for on-going treatment, including drugs and therapies, nutrition plan, infection status and any agreed limitations of treatment.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 144
• Physical and rehabilitation needs
It is essential to give a detailed review of medication. Treatment to be reviewed or stopped must be clearly identified, as must the timing. Long term medications must be also considered. If these have been changed or not yet restarted this must be documented.
If there are any variations or changes to any part of the discharge plan, this should be clearly documented in the medical notes
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 145
Appendix 18 – CoMET operational guidance (with special reference to EMCHC)
Children’s Medical Emergency Transport Service
This document outlines the operational policies of CoMET, the East Midlands Children’s Medical Emergency Transport Service, and in particular the relationship between CoMET and the East Midlands Children’s Congenital Heart Network (EMCCHN). The document is extracted from the CoMET Operational Guidance version 5, published in March 2018, and in the case of any discrepancy, that Operational Guidance will take precedence.
Section:
1 Introduction
2 Scope of Care
3 Referral Call
4 Activation of a transport team
5 Advice calls
6 Responsibility for patients
7 Mobilisation of transport team
8 Arrival of transport team at patient bedside
9 Departure from referring hospital and journey to destination
10 Care of family
11 Arrival back to base and management and checking of equipment
12 Documentation and database management
Section 1: Introduction
1.1 The operational guidance provides a frame work within which the Children’s Medical Emergency Transport Service (CoMET) will operate.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 146
1.2 CoMET is hosted by the University Hospitals of Leicester NHS trust working in partnership with the Nottingham University Hospitals NHS Trust.
1.3 It is expected that all individuals who work within CoMET are aware of and work within the clinical governance structure of UHL and CoMET
1.4 The Service meets the standards set by the UK Paediatric Intensive Care Society NHS England specifications for the provision of specialist transport services.
1.5 Mission Statement
CoMET aims to provide the highest quality care for infants, children and young people and their families from the first point of contact to arrival at their destination. CoMET’s mission is to:
• Move the patient to the right place at the right time for the right care, as close to the patients home as possible. This will be determined by following the agreed referral pattern within the EMCHN region.
• To maintain appropriate communication between all parties to ensure effective continuity of patient care.
• To ensure that every transfer is carried out safely and effectively and in ways that minimise the pain, discomfort or distress felt by the patient and parents/carers.
• Transfer critically ill children between hospitals in a timely and safe manner, by providing a well-equipped and appropriately trained team
• To meet the service specification as issued by NHS England (E07: Standard contract for Paediatric Intensive Care Transport).
1.6 The CoMET Team consists of: • CoMET Lead Consultants • CoMET Team Leader • CoMET Educator • CoMET Paediatric Consultants • Paediatric trainee doctors • CoMET Nursing team • Advanced Clinical Practitioners (ACP) • Dedicated call handling team • Dedicated clerical support
1.6.1 Medical Team: The service is consultant-led and often consultant delivered. Specialist
Registrars, Advanced Clinical Practitioners and Clinical Fellows are trained with the aim that they can lead retrievals independently, but always with close consultant supervision. They receive specialist training to gain airway management skills, competence in the use of retrieval equipment and undertake supervised retrievals as means of assessing overall performance. Trainees complete the Paediatric Transport Passport whilst gaining experience within the critical care environment. ‘Medical staff’ (including ACPs) will have completed APLS training before retrieving unsupervised.
1.6.2 The ACP is not a substitute doctor but an advanced role working alongside medical and nursing staff. The objectives of the ACP role are:
• To work within the boundaries of the ACP role acknowledging areas of competency
• To work within local and national guidelines and within the code of the NMC or other appropriate regulatory body
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 147
• Follow UHL Policy for ‘Non-medical prescribing’
1.6.3 Nursing Team: Each nurse who is a member of CoMET will have completed a critical care accredited course and will also have a current APLS/EPLS certificate.
1.7 CoMET Orientation: All staff will receive a site-specific orientation and induction. In order to be considered competent and perform unsupervised acute transports, each nurse must complete the comprehensive Paediatric Transport Passport. This is both self, peer and transport educator assessed. Each Transport Nurse will also be expected to complete the CoMET Transport Equipment Competency Booklet, and will be responsible in ensuring continual competence is assessed triennially.
1.7.1 New Transport Nurses will attend a 12-week induction period with the transport team. They will be allocated a mentor, and it is expected that during the first 8 weeks they remain supernumerary and work alongside their mentor or educator for a minimum of 30% of their shifts. An induction booklet will be provided and guidance given for regular review meetings throughout this period. During the 12 weeks, it is expected that the trainee nurse will achieve all outcomes within the Transport Passport, and provide evidence of 3 successfully assessed acute transports, performed by a recognised assessor. They will also be expected to have completed the equipment competencies, and any other training identified within their PDP (Professional Development Plan) before being considered competent.
1.7.2 Records of completed competency records are kept by the transport educator.
1.7.3 Medical staff working for CoMET will receive an induction and training on the equipment to ensure they are safe competent practitioners before being rostered to undertake independent transfers. Equipment training will be provided by the lead educator, lead nurse, or others as appropriate. The CoMET Lead Consultants will be responsible for ensuring that their level of competence is achieved prior to undertaking lone transfers.
1.8 Insurance
Insurance will be covered by the Trust for transport activities. Additional personal cover is provided by membership of the PIC society and this is recommended for CoMET staff members. Parents travelling in the ambulance are covered by the ambulance provider insurance.
Section 2: Scope of care
2.1 CoMET is a specialised service commissioned to support the children’s services delivered by the hospitals in the East Midlands and other associated hospitals within the EMCHC footprint, as well as supporting hospitals in other regions close to the East Midlands.
2.1.1 CoMET serves approximately 0.7 million children within the East Midlands. It is a dedicated transport service operating from two bases, one at Leicester Royal Infirmary (LRI) and one at Nottingham University Hospital (NUH).
2.2 Hours of service
2.2.1 CoMET will provide a 24 hour, seven day a week service for acute transport, and a 12 hour, seven day service for repatriations from EMCHC to hospitals nearer home, or to other appropriate facilities.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 148
2.2.2 All calls regardless of whether CoMET is on service will be via Call CenTre Handling on 0300 300 0023. The call handler has details of which service is operating when, and will direct the call to the correct CoMET Team.
2.2.3 Planned repatriation transfers will be undertaken during daytime hours (07:30am to 20:00pm). Planned transfers will not normally be undertaken by the night-time team as this would result in no cover for acute (unplanned) transfers. The transport consultant may authorise night-time team to undertake a planned transport, but this should only be authorised where the transfer:
• Cannot reasonably be deferred to the next morning • Is required to create patient flow in PCC • Is not long-distance, where it would occupy the team for most of the night • Can be diverted at short-notice should a more urgent unplanned referral be received.
2.3 Accepting Criteria
Calls will be accepted from
2.3.1 Paediatric services at EMCHC network hospitals requiring the transfer of a critically ill child who also meets one of the criteria set out in 2.3.2-5
2.3.2 Planned critical care transfer for specialist opinion, investigation or treatment in EMCHC.
2.3.3 Repatriation of these children from level 2 or level 3 critical care to their home units.
2.3.4 In exceptional circumstances, and at the discretion of the receiving Trusts unit, children and young people over the age of 16 years, presenting to EMCHC who due to their specialist needs require critical care in a tertiary paediatric setting.
2.3.5 Transfers into palliative care facilities (considered on an individual case by case basis following discussion with a member of CoMET senior team and EMCHC Clinicians).
2.3.6 Outside of normal pathways above, for example where an adjacent paediatric transport service is experiencing high demands.
2.4 Exclusions
CoMET will not normally be responsible for the transfer of the following patient groups:
2.4.1 Children and young adults over the age of 16 except in circumstances described in 2.3.54
2.4.2 Primary transfers, for example from home or from community hospital/clinic settings
2.4.3 Patients who require urgent neurosurgery deemed to be time critical. These should be transferred by the referring hospital - please refer to the Time Critical Transfer Guideline.
2.4.4 Other time critical transfers for immediate lifesaving treatment e.g. atrial Septostomy, where it is deemed that the referring hospital will be able to transfer more quickly and that this non-specialist transfer will result in significant clinical benefit.
2.4.5 Children requiring transfer from a paediatric ward to a paediatric ward, unless this helps to facilitate critical care flow.
2.4.6 Patients who have been exposed to hazardous materials
2.4.7 Patients who weigh over 140Kg will not routinely be transported using standard CoMET equipment.
2.5 Patient Criteria 2.5.1 Patients who require paediatric critical care will normally be accepted for transfer providing
they meet one or more of the following criteria:
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 149
• They require (or may require) advanced respiratory support such as endotracheal intubation and ventilation, CPAP or high flow nasal cannula oxygen therapy
• Any child with a chest drain in situ • They require (or may require) intensive care-dependent procedures • Have symptoms or evidence of shock, severe respiratory distress ore respiratory
depression • Have the potential to develop airway compromise • Have an unexplained deteriorating level of consciousness • Have required resuscitation or are requiring some form of continuing resuscitation • Have received significant injury requiring airway and/or circulatory support • Have had prolonged surgery or any surgical procedure that is of medium or high risk or
of a specialist nature • Have potential or actual severe metabolic derangement, fluid or electrolyte imbalance • Have an acute organ (or organ system) failure • Have established chronic disease or organ-system failure) and experience a severe
acute clinical deterioration or secondary failure in another organ-system • Require one to one nursing because of complexity of an acute or acute on chronic
illness • Require further care at a tertiary level centre e.g. cardiac/burns • Arterial access in situ
2.5.2 Patients may be referred to the repatriation service provided they are:
• Within a level 2 or level 3 critical care facility and their home postcode falls within the area of the EMCHC Network.
• The transfer is required to create patient flow in EMCHC.
Section 3: Referral call
3.1 To activate the transfer process the referring unit will contact the CenTre call handling service on 0300 300 0023. All calls are recorded for training and governance purposes, all participants of calls must be made aware of this
3.2 Acute referrals for paediatric critical care will be dealt with by the following procedure:
3.2.1 Referring units contact the CenTre Call Handling Service via the direct dial dedicated line.
3.2.2 The Call handler answers the call and asks the caller if they are referring a neonatal, paediatric or ECMO patient.
3.2.3 If the caller is referring a paediatric patient they will take basic patient details and referrer contact details (Name of caller, location of patient, phone number of caller, NHS number of patient) on a dedicated database.
3.2.4 The Call handler will then use the designated call centre algorithms to direct the call appropriately.
3.2.5 The Call handler asks whether they are calling for an acute or repatriation transfer.
3.2.6 Acute transfer The Call handler connects the call to the on-call consultant and the registrar on for transport (although the connection of the two medical staff should not delay answering the referral)
3.2.6.1 Clinical details presented by the referring clinician and recorded by CoMET consultant/ registrar on the CoMET data base. If this is not available a hard copy of ‘CoMET referral form’ is completed and uploaded as soon as possible.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 150
3.2.6.2 Immediate clinical advice is provided by the CoMET consultant as required and a decision made as to whether the patient is to be accepted for transport.
3.2.6.3 Additional clinical specialists from EMCHC and elsewhere can be added to the call conference as required.
3.2.6.4 Plan agreed for clinical stabilisation and transfer of patient if required.
3.2.6.5 Activation of the CoMET transport team can occur at any point in the process under the direction of the CoMET consultant.
3.2.6.6 Location of appropriate and available critical care beds to be identified by CoMET personnel.
3.2.6.7 For acute transfers the team will depart the transport base within 30 minutes from the time the referral is accepted for retrieval. Mobilisation times are reported quarterly to the PICU Dashboard.
3.2.6.8 A consultant who is covering the transport service will make priority decisions where demand for transport exceeds supply.
3.2.6.9 The decision to mobilise is made by the consultant on for CoMET.
3.2.7 Repatriation: The Call handler will connect the call to the repatriation nurse on duty if available.
3.2.7.1 The nurse on duty will take clinical details and establish from the caller if a bed has been located for the patient. If a bed has been located then the nurse will proceed to book transport and liaise with referring and receiving hospital.
3.2.7.2 CoMET does not undertake to locate beds for repatriation transfers- the initial referral and securing of the bed should be undertaken directly between the referring and receiving unit clinician.
Section 4: Activation of a transport team
4.1 The decision to activate the CoMET Transport team is based upon the clinical information provided by the referring unit by direct telephone referral.
4.1.1 The decision to transfer will take into account the workload for CoMET and the CoMET Transfer Priority List along with the criteria set out in 2.5.1 for acceptance of acute transfers.
4.2 All decisions will be clearly documented as part of CoMET clinical records. Conference calls will be digitally recorded and stored.
4.3 The CoMET Consultant will decide upon the composition of the team based upon the clinical information available and his/her knowledge of the competencies of CoMET staff on duty. The acute transfers will be normally be undertaken by a doctor or advanced practitioner and a nurse although other team compositions may be appropriate at the CoMET consultant’s discretion.
4.4 The decision to activate a ‘Nurse delivered transfer’ will be made by the consultant on duty for CoMET following initial referral and assessment of the clinical condition of the patient.
4.5 One-person repatriations are usually undertaken by a nurse and the decision to transfer by a one-person team will be made by the senior clinical staff on-duty for CoMET in consultation with the consultant covering the service. A comprehensive referral should identify if a child is deemed stable enough for a single practitioner transfer.
4.6 If a CoMET consultant is not available to provide triage (e.g. due to giving direct care to a critically ill patient) the following set of criteria applies before a transport is accepted.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 151
4.6.1 The regional PIC consultant must participate in the call conference (irrespective of PICU bed availability)
4.6.2 The non-consultant doctor/ACP should decide if they have sufficient competence and experience to undertake the transport based on the clinical information provided. If they feel they DO NOT have the appropriate level of experience this should be clearly stated to the regional PIC consultant.
4.6.3 The regional consultant must agree to support the non-consultant doctor/ACP during transfer via phone. This responsibility will be transferred to the accepting consultant as soon as a bed is located and confirmed.
4.6.4 Arrangements for the transport must be confirmed with the on-call CoMET consultant at the earliest opportunity.
4.7 Team unable to mobilise 4.7.1 CoMET is funded for 1 acute transport team functioning 24 hours a day 7 days a week. As
a result, it is recognised that there may be occasions when an acute transfer is required when another patient episode is already in progress. When this happens, patients will be prioritised by the CoMET consultant.
4.7.2 The highest priority will be given to children who:
• Have a diagnosis requiring transport to a site of definitive care where delay may result in worsening prognosis.
• Unstable children where the referring team are struggling to achieve physiological control.
• Patients referred from hospitals within EMCHC usual catchment area will normally be prioritised. If the patient is referred from out of region, they will be asked to refer to the appropriate local service if available.
4.7.3 Triage will be performed by the CoMET consultant following discussion with clinical teams at the referring hospital
4.7.4 The length of wait until a team becomes available will be assessed.
4.7.5 Discussion will take place between the on-call CoMET consultant and/or nurse co-ordinator, and a consultant at the referring hospital and receiving hospital and a clinical decision will be made either to
• Wait • Consider if the repatriation nurse from the opposite base can be appropriately paired
with a medic • Ask the referring hospital to transfer • Ask another transport service to transfer
4.8 Time of day and shift-changeover times
4.8.1 Teams will not usually be expected to depart base for a transfer that will predictably make them over one hour late finishing their shift. The exceptions to this will be:
• Where the consultant deems that the life of the patient is in danger if delivery of transport expertise is delayed, or
• Where the team are content to undertake the proposed transfer and a plan is in place to recompense their extra work
• Consideration should also be given to asking the subsequent shift if it is possible for them to attend to their shift earlier than planned.
4.8.2 When the incoming new transport shift learns that the previous shift team is still out on a transfer, they should enquire as to the need for the new shift to be deployed to relieve the previous shift. This decision should be approved by the CoMET consultant in the light of knowledge of other transport activity.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 152
4.8.3 The relief team will begin to travel towards the late running team as soon as all team members/ ambulance crew are available.
• If the late running team can leave the referring hospital before the relief team arrive and are transferring the child to their base hospital they should be allowed to continue with their transfer. In such circumstances the relief team will return to base.
• If the late running team can leave the referring unit but are transferring the child to another unit (not their base), they should agree on a safe location to handover the child to the relief team. In such circumstances the teams will swap vehicles i.e. The late running team will use the new vehicle to return to base and the relief team will take the original vehicle and child on to the receiving unit.
4.8.4 If any staff member has been out for a long period of time they must consider whether they are in a fit condition to drive home. A taxi can be provided if this is required.
Section 5: Advice calls
5.1 Advice calls may form part of the transport process or be independent of any request for transfer. Advice is provided by the CoMET consultant to the referring team regarding resuscitation and stabilisation and any tests that maybe useful. A copy of all advice calls and outcome will be recorded via the CoMET database.
5.2 Advice will only be given by a member of the CoMET when it falls into their level of expertise. This area will vary according to the team member’s background and experience. The CoMET is thereby the facilitator for obtaining the advice but not necessarily the provider of that advice.
5.3 Advice may come from four sources. The (usually senior) clinicians giving this advice are responsible for their advice, accepting that it is based upon the information provided to them and that they are unable to insist that such advice is acted upon.
The four sources are:
• CoMET • The receiving team • A third party consultant (e.g. consultant from a tertiary centre) who would otherwise have
no responsibility to the patient. • A member of a specialist team (e.g. neurosurgery or cardiology)
5.4 Record keeping
Advice calls involving CoMET personnel engaging in CoMET business should be made via the Call Handling Service so that the advice is recorded. A written record should be completed on the CoMET Database
5.5 Pre-transfer stabilisation advice is provided by the CoMET consultant to the referring team via telephone conference.
Section 6: Responsibility for patients
6.1 The transfer of patients by CoMET necessitates that the care of patients is handed over from the referring hospital to the transport team and thereafter at the receiving hospital to the receiving hospital team. With this handover of care is also a handover of responsibility for the patients.
6.1.1 Central to any consideration of responsibility is the understanding that a patient’s best interests remain paramount throughout the transport process, and that there is not a
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 153
sudden change in responsibility for the patients care. Responsibility shifts and is dynamic during stabilisation and preparation for transfer.
6.2 From referral to handover 6.2.1 The patient remains the primary responsibility of the referring hospital team until an
adequate handover of the patient to the transport team has been completed. This can only take place once the CoMET has arrived in the referring hospital.
6.2.2 The referring team is responsible for the on-going care of the patient and should continue to provide the highest available levels of care until CoMET has arrived and the patient has been handed over to them.
6.2.3 During this time the referring hospital team may be given advice from the transport service or a third party (such as receiving unit/other specialist clinician) but is responsible for providing adequate information upon which that advice is obtained and for deciding whether or not to act in accordance with that advice.
6.3 From handover in the referring hospital to handover in the receiving hospital 6.3.1 The patient becomes the primary responsibility of the CoMET at completion of the handover
by the referring hospital. The CoMET consultant resumes ultimate responsibility for the patient at this time.
6.3.2 This does not mean that the referring hospital consultant and team relinquish all responsibility for the patient to the transport team at handover but rather the consultant(s), as the senior clinician(s) present and other responsible staff within the referring hospital, should render to the transport team any assistance necessary to enable the safe preparation of the patient for transfer.
6.3.3 The patient remains the transport team’s primary responsibility until adequate handover for the patient to the receiving team has been completed. Responsibility for the patient passes completely over to the receiving team once the patient has been transferred from the transport equipment and, where required, stabilised on the receiving team’s life support equipment.
6.3.4 It is expected that upon arrival at the receiving hospital, the receiving team would, if necessary, render to the CoMET any immediate assistance necessary for the welfare of the patient. This may take place even before the handover process has been completed.
6.3.5 On rare occasions additional support of the CoMET may be required (e.g. to facilitate a scan on arrival). This should be agreed with the team at the earliest opportunity. Under these circumstances the primary responsibility for the patient’s rests with the receiving team. The retrieval team will act to ensure the safe transfer of the patient using the transport service equipment.
6.4 During transfer
6.4.1 During the transfer of a patient from the place of care in the referring hospital until arrival at the place of care in the receiving hospital, CoMET is responsible for the patient’s welfare.
6.4.2 The CoMET consultant is ultimately responsible for the patient during the transfer. This line of responsibility is maintained despite a lack of physical proximity.
6.4.3 During this time the team may act upon advice from a third party (e.g. from the receiving unit / other specialist clinician) but is responsible for providing adequate information upon which that advice is obtained and for deciding whether or not to act in accordance with the advice.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 154
6.4.4 Because of the two-base structure of CoMET it may be appropriate for the nominated Transport Consultant to formally pass the Transport Consultant responsibility for an individual transport over to the Consultant who will be receiving the patient at the other base. This may be appropriate for example where the Transport Consultant has multiple complex transport demands. For this to happen there must be a direct conversation between the two Consultants involved. The transport personnel attending the transfer must also be directly informed.
6.5 Nurse delivered transfers 6.5.1 The responsibility and accountability arrangements continue to apply when transfers are
delivered by nurses acting independently.
6.5.2 Before accepting responsibility for a patient the nurse should independently assess that patient and decide whether or not the transfer of the patient is within his/her experience and competence. Should he/she decide that this is not the case, responsibility remains with the referring team until such times as alternative arrangements can be made.
6.6 Transfers delivered by trainee medical staff or advanced practitioners
6.6.1 The responsibility and accountability arrangements continue to apply when transfers are delivered by trainee medical staff or Advanced Practitioners acting independently.
6.6.2 Before accepting responsibility for a patient, the medical trainee or advanced practitioner should independently assess the patient and decide whether or not the transfer of the patient is within his/her experience and competence. Should he/she decide that this is not the case, responsibility remains with the referring team until such time as alternative arrangements can be made.
Section 7: Mobilisation of transport team
7.1 CoMET aims to mobilise within 30 minutes of the decision to accept referral for a PICU bed in line with the PICU national dashboard.
7.1.1 Mobilisation time is defined as the time between being instructed to launch the team (decision to accept referral for PCC bed) and when the ambulance actually begins the journey to the patient (departure time).
7.1.2 This mobilisation time will be audited both locally and nationally as part of the National PICU dashboard.
7.1.3 Failing to manage the mobilisation period could result in the team departing without the necessary resources or unnecessary prolonging of arriving at the child’s bedside.
7.2 Preparation and readiness for mobilisation
7.2.1 The CoMET Team (Doctor/ACP, Nurse) are expected to be prepared for mobilisation throughout their shift, to ensure delay is minimised. The equipment, ambulance and resources should be prepared at the beginning of every shift according to the CoMET Shift checks.
7.3 Pre-departure checks
7.3.1 Pre-departure checks (as highlighted on CoMET documentation) should be performed by nurse and doctor/ACP prior to leaving the unit and final ambulance checks should be undertaken jointly by the Doctor/ACP and nurse prior to departure.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 155
7.3.2 CoMET trolley should be secured into the universal clamps and the equipment bags restrained appropriately. Staff must sit with seatbelts applied. The ambulance crew are responsible for confirming this before departure.
7.3.3 Doctor/ACP will request the ‘journey category’ required (see appendix 10: Clinical Triage Categories) at the time of requesting departure, as per ‘clinical triage for CoMET categories’
7.4 Monitoring of Mobilisation
7.4.1 The length of each mobilisation will be recorded on the CoMET database. Any mobilisations greater than 30 minutes when the team is at base will be reviewed daily by CoMET governance process to determine what factors caused the delay. Any incidents of teams departing without needed resources should be recorded upon a Datix form.
Section 8: Arrival of transport team at patient bedside
8.1 Arrival at the referring hospital begins with safe disembarking from the ambulance with the trolley and equipment, and a timely transfer to the patient’s bedside by the most direct route.
8.2 Once handover has been completed, CoMET will assume joint responsibility for the management of the patient with the referring clinician (as per section 6). The principle aim of the team is preparation of the child for transport. This may occasionally take some time. It is vital that the child not be transferred until they have been stabilised as far as possible and vascular access and monitoring have been achieved. In extreme cases where the child cannot be stabilised, transfer may not be possible.
8.3 On Arrival at the child’s bedside;
• Joint introductions of CoMET Team and referring hospital, identifying names and roles; • All team members to wash hands and observe appropriate local infection control
practices; • Full handover taken from local team with simultaneous completion of CoMET retrieval
documentation, and first charting of vital signs, infusion rates, ventilator settings and the family situation.
8.4 CoMET Team Assessment and Treatment of Patient
a. CoMET team examination/assessment of patients’ clinical condition in accordance with Advanced Paediatric Life Support (APLS) guidelines. This includes therapies in progress, radiological and other laboratory investigations. CoMET Doctor/ACP acts as team leader.
b. Communication and close-working with local team must continue to ensure assistance available, access to DGH resources and for ensuring smooth coordinated care throughout the stabilisation period. Request that identified local doctor if possible and nurse remain with CoMET Team throughout stabilisation period.
c. Full physiological monitoring including ECG, blood pressure, respiratory rate, core/peripheral temperature, pulse oximetry (and capnography for intubated patients) should be measured on arrival as a baseline set of observations and recorded on the CoMET Transport Chart. Observations should be recorded in the referring hospital as appropriate thereafter. Continuous reassessment and re-evaluation of the patient’s clinical condition and therapy delivery should be in progress.
d. CoMET Team to telephone CoMET Consultant to discuss condition and agree treatment plan.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 156
e. Necessary clinical procedures performed in line with CoMET Policies, Procedures and recognised best practice.
f. Where patient intubated: Fixation of endotracheal tube (ET) reviewed and fixation replaced if necessary. Melbourne strapping fixation method utilised by CoMET team; size and length of ET tube to be documented on transport chart;
g. Bi-lateral chest inflation confirmed visually and through auscultation; h. Chest X-ray post endotracheal intubation checked and documented; i. Minimum of 2 working intravenous cannulas or a multi-lumen CVL present, flushed
working and secured; j. DGH intravenous infusion labelling reviewed, clarification from local team where
required. Pump rates checked to ensure the correct drug dosages are being delivered - document;
k. NPSA compliant nasogastric or orogastric (orogastric for suspected or confirmed basal skull fracture) tube inserted, on free drainage, checked and length documented;
l. Temperature management instituted appropriate to pathology and clinical condition; m. Appropriate fluid management instituted with maintenance running at prescribed rate. n. Sedation, analgesia and muscle relaxant infusions delivered to optimise patient comfort,
safety and mechanical ventilation delivery; o. Radiological images transmitted to destination unit by referrer on PACS system, or
computer disc (or plains films) transferred by CoMET team; p. CoMET team telephone consultation with CoMET consultant to discuss progress and
consider further actions; q. Parents updated throughout by CoMET team; where possible 1 parent will be offered
the opportunity to travel in ambulance. Parents will be provided with appropriate written information.
Section 9: Departure from referring hospital and journey to destination
9.1 Departure from referring hospital encompasses ensuring the clinical patient preparation, documentation, investigation results, the staff and equipment resources can proceed safely to the ambulance and onward to the destination
9.2 CoMET Consultant Authorisation to Depart: When the CoMET Team at the bedside are satisfied that the patient is ready for transport and have obtained the clinical information and investigation results necessary the Transport Doctor/ACP should telephone the CoMET Consultant to discuss the patient and confirm authorisation for departure, unless previously agreed with the consultant that this is not necessary.
9.3 Pre-Departure Checklist: Transport Doctor/ACP and Nurse perform ‘pre-departure checklist’ on the documentation. The infant/ child must be securely restrained in either the babypod or the trolley using the appropriate harness (Vacuum mattress/ ACR).
9.4 Discontinuation of Referring Hospital Power and Oxygen/Air Supply
9.4.1 CoMET Trolley is disconnected from referring hospital mains power; team to check that all electronic instrumentation continues to function.
9.4.2 Oxygen/Air supply will be transferred from referring hospital source to CoMET Trolley Cylinders under direct observation of CoMET Doctor/ANP or Nurse who will monitor patient, vital signs and ventilator pressure gauge. Following transfer CoMET Doctor/ACP or Nurse to confirm that bi-lateral chest inflation, end tidal capnography and ventilator pressure readings are satisfactory.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 157
9.5 Transfer of Patient, Team and Equipment to Ambulance: CoMET Team to proceed to ambulance in timely, controlled manner ensuring that all staff and resources remain together. CoMET Doctor/ACP or Nurse to observe patient, monitor and equipment at all times.
9.6 Transfer of CoMET Trolley into Ambulance: Patient trolley transferred into ambulance and secured into Universal Clamps; under direct supervision of ambulance technician. No staff are to ride on the tail lift (if on use on the vehicle), which may only be operated by the Ambulance Technician. Ambulance Technician to check trolley is secure and safely loaded into the clamps.
9.7 Medical Gas and Electricity Supply Changeover in Ambulance
9.7.1 Medical Gas supply will be transferred from trolley source to Ambulance supply under direct observation of CoMET Doctor/ACP or Nurse who will monitor patient, vital signs and ventilator pressure gauge. Following transfer CoMET Doctor/ACP or Nurse to confirm that bi-lateral chest inflation, end tidal capnography and ventilator pressure readings are satisfactory.
9.7.2 It must be ascertained prior to departure that the oxygen supply is sufficient for the needs of the journey.
9.7.3 CoMET Ambulance Inverter to be activated, CoMET transport Trolley to be plugged into 3 Pin electrical socket or Anderson connector, with confirmation of electricity delivery to pumps and monitor (check AC light illuminated).
9.8 Securing of Staff, Parents, Equipment Bags and Other Items in Ambulance
9.8.1 Equipment bag to be secured into designated storage with provided straps; any other equipment secured within lockers. No loose equipment is permitted in the cabin.
9.8.2 Parent/s are to receive safety briefing from CoMET team if they are accompanying the child in the ambulance. Ambulance technician does final check that all staff/parents seated correctly wearing seatbelts, that Trolley is securely in the Universal Clamps and that there is no loose equipment.
9.8.3 Ambulance technician confirms with CoMET team that departure can commence and destination confirmed
9.8.4 CoMET Doctor/ACP confirms journey category (1, 2 or 3) to Ambulance Technician – see Clinical triage for CoMET categories (appendix 10).
9.8.5 All personnel in the ambulance will wear the supplied restraining seat belts at all times the vehicle is in motion. If any patient interventions are required, the ambulance should be requested to stop. Discretion may need to be used when there is an indication for urgent life or limb saving medical procedures, which can only be provided at the destination hospital. A Datix form should be completed once back at base (Appendix 12).
9.8.6 If the child arrests and requires cardiopulmonary resuscitation and/or defibrillation the ambulance must be stopped. If defibrillation is required, this should be done in accordance with APLS guidelines. Oxygen must be turned off at the flow meter during defibrillation due to the risk of ignition from defibrillation in an enclosed space.
9.8.7 CoMET personnel and any passengers travelling with the team will not distract the driver of the ambulance whilst it is in motion unless there is an emergency that they need to be notified of.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 158
• Patient Monitoring during Journey to Destination
• Patient colour, chest inflation, equipment functionality, restraint and comfort to be monitored continually throughout journey.
• Patient vital signs, ventilator observations and infusion delivery rates/dosages recorded upon Transport Chart every 15 minutes or more frequently if clinically indicated.
• CO2 monitoring and waveform must be displayed on all intubated patients.
• Communications during Journey to Destination
9.10.1 CoMET Consultant should be contacted to discuss any significant clinical changes to condition or therapy delivery, this will be at the discretion of the CoMET Team.
9.10.2 CoMET Team will inform the Nurse in Charge of the destination unit of the expected time of arrival (ETA) and to reaffirm the child’s condition and current treatment delivery.
9.9 On arrival at patient destination. CoMET will hand over the patient to the receiving unit (please refer to section 7- responsibility of patient) completing accountability checklist on documentation.
9.10 Documentation will be photocopied and left with the destination unit. The original transport log must be brought back to base.
Section 10: Care of families
10.1 CoMET aims to provide high quality, effective, safe intensive care to critically ill children from the point of referral, throughout the transport pathway. CoMET will work respectfully with referring staff and listen to the feedback given by these centres. The families will receive high quality information and be cared for throughout the transport pathway. Parents will be kept fully informed of all aspects of their child’s care. These discussions will be recorded in the patient’s transfer records.
10.1.1 Discussions with parents to include:
• The nature of the condition affecting their child • The reason for transfer • A detailed explanation of the transfer process • At present no formal written consent for transfer will be taken, rather the assumption of
implied consent will be sought.
10.2 Parents travelling in the ambulance
10.2.1 Standards for the care of Critically Ill Children (Paediatric Intensive Care Society 2015) state that wherever possible and appropriate parents should be given the option to accompany their child during transfer. However this may not always be possible and the decision remains at the discretion of the team.
10.2.2 CoMET does not have a blanket policy regarding family travelling in the ambulance. This will be discussed on a case by case basis and may be dependent on the vehicle available to the team. Considerations for parents travelling in the ambulance include:
• The stability of the child: assess the need for potential interventions
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 159
• Transport safety: all ambulance occupants must be in a forward or rearward facing seat with a 3 point harness. Potential use of lights and sirens must be considered.
• Child related issues: anxiety cause by separation from parent • Parent: signs of aggressive or difficult behaviour need to be emotionally supported.
CoMET cannot be responsible for the health of the parent accompanying their child. Travel in the ambulance should only be offered if the parent is medically fit to travel. Mum must have been discharged from postnatal care and be cleared for travel by the discharging team. Should a parent become unwell whilst travelling, immediate assistance will be offered but will only be equivalent to that of an ordinary member of the public.
10.2.3 The ambulance crew are responsible for ensuring that the parent is safely assisted in and out of the ambulance, and for ensuring that seatbelts are worn. Before the journey commences; the ambulance technician or another team member will read a ‘safety briefing’ to the parent advising them to remain seated with the seatbelt fastened throughout the journey, and informs them that they must follow the instructions of the CoMET staff in the event of a clinical incident or vehicle emergency. CoMET records the names of parents who travel on the transport database at the start of each journey. In case the vehicle is involved in an accident and this information is required by police. Parents must not travel in front with the driver because it causes anxiety for the parent and may distract the driver.
10.3 Blood samples: A sample of maternal blood should be obtained for all babies and infants less than 6 months of age for whom there is a reasonable expectation of an early blood transfusion, This must be a cross-match sample, collected and labelled in accordance to transfusion guidelines.
10.4 Parental care when not travelling in the ambulance
10.4.1 Parents/carers not travelling in the ambulance are recommended to either wait 10-15 minutes after the transfer team has departed before following on at a safe pace or go home to make arrangements for a stay on PICU (see other children, get fresh clothes, toiletries etc.). Preferably a friend or relative should drive. It is imperative that:
• Parents do not leave for the destination hospital before the transfer team in case of a sudden deterioration in the condition of their child.
• Parents do not follow or ‘chase’ the ambulance • Contact numbers are obtained from all parents.
10.4.2 CoMET carries a range of information, maps and the offer of the loan of a ‘sat-nav’ which can be provided to parents who plan to drive in their own car to the destination unit. Parental booklets and information for most centres that provide paediatric intensive care in the UK will be provided.
10.4.3 Where parents do not wish to travel in the ambulance, and do not have their own transport, the CoMET will liaise with the referring hospital team about arranging a taxi or other form of transport.
Section 11: Arrival back to base and management and checking of equipment
11.1 On arrival back to base it is the responsibility of the team to ensure that all equipment is cleaned in conjunction with guidance from the infection prevention teams at UHL and NUH respectively.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 160
11.1.1 The trolley must be plugged back in and staff ensures that all equipment is charging appropriately
11.1.2 Any faults relating to equipment on transport must be reported to the appropriate MESU department, and the MESU Equipment log (appendix 11) completed to that any common themes or issues across the two sites can be highlighted and shared.
11.1.3 All fridge drugs and CD drugs must be accounted for, signed back in or disposed of.
11.1.4 All bags and pouches must be resealed and documented on the equipment checklists.
11.1.5 All documentation must be completed in full and this needs inputting into CoMET database in a timely fashion.
11.1.6 Any critical incidents must be filled in on BOTH the transport paperwork and a Datix form must be completed.
11.2 CoMET equipment
• CoMET transport systems are configured to allow for single child transfers only.
• The babypod will allow for the transfer of infants from approximately 2-8kg
• The paraid trolley will allow for the transport of persons up to the weight of 140 kg
• All systems are fitted with infusion pumps, monitor, ventilator, and a suction unit.
11.3 Management of CoMET Equipment: All equipment is maintained by Medical Physics departments at the University Hospitals of Leicester NHS Trust (UHL) and Nottingham University Hospitals NHS Trust (NUH)
11.4 Training and use of equipment: All CoMET staff will be trained and assessed as competent at using the CoMET transport systems and have a record of the corresponding competency documents.
11.5 Monthly equipment management: Monthly equipment checks (appendix 13) must be completed and signed for and are as follows:
• Complete kit bag check including all expiry dates (appendix 14) - any kit due to expire within the next 6 months to be rotated with stock from the unit.
• Complete drug box/CD Box and fridge bag check including expiry dates- this will need documenting on specific checklist (see appendix 15). Any drugs that are due to expire in the next 6 months are to be rotated with stock from the unit, thereby minimising any waste.
• Any missing kit needs to be reported: o If when the kit is checked you are unable to replace something report this so that it
can be ordered and a replacement can be sourced as soon as possible. Document this on the paperwork and ensure that it is handed over to the next shift and that it is an item for the morning meeting agenda.
o Ensure a datix form is done if when out on retrieval there is something missing from sealed kit bag.
• External WEQAS testing for iSTAT (where carried) - these samples will be delivered by PCOT and need to be completed within 5 days- ideally testing should be completed on arrival of samples.
• Monthly stock check of equipment levels. Any stock which needs ordering needs highlighting to corresponding unit and recording (see Appendix 16: record of consumables).
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 161
11.6 Daily equipment checking: The clinical team (Doctor/ACP and nurse) is responsible for completing a full check of the CoMET equipment which will be used for transporting patients. The daily transport equipment checklist (Appendix 5) must be completed and signed for by both the nurse and doctor/ACP. Any equipment found to be faulty, or failing routine calibrations will be removed from service and sent to the Medical Engineering Department, the corresponding MESU Equipment Log will also need completing (Appendix 10).
11.7 Compliance: Compliance with monthly and daily kit checking will be the responsibility of the lead nurse and clinical educator. Monthly compliance with the daily checking will be displayed upon the ‘Transport’ Notice board at either site.
Section 12: Documentation and data management
12.1 Patient identification
12.1.1 All calls concerning individual patients will have basic details recorded by call centre staff and a unique identification number attached.
12.1.2 Wherever possible the NHS number should be recorded.
12.1.3 Patient identification (surname, given name, date of birth and NHS number where available) will be recorded on all transport forms.
12.2 Referral calls
12.2.1 All calls will be documented on the appropriate CoMET forms or directly into the CoMET database. This information will form part of the clinical records of the patient and will be signed and dated by the individual completing them.
12.3 Patient Transfer documentation
12.3.1 As part of CoMET patient records the relevant parts of the documentation will be completed for any advice given and for all transfers undertaken. This will include:
• Details of the CoMET team • Operational data • Additional history and notes • Initial assessment • Summary of interventions • Mandatory observations (at first look, prior to departure and on arrival at the receiving
hospital) • A record of any safeguarding issues • Documentation of discussion with parents • Dataset on audit form for PICANet • Regular observations from the time of ‘first look’ until handover at the receiving hospital,
These will be completed at an appropriate frequency at the referring hospital and every 15 minutes during transfer (or more often if appropriate) and will include a record of any acute interventions
• Pre-departure checklist • Handover details at the receiving hospital • Transfer outcome • A record of any adverse event (in addition to Trust incident reporting procedure) • Any other information relevant to the retrieval
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 162
12.4 Reporting untoward incidents and adverse events: All untoward incidents and adverse events will be recorded in the patients transfer notes. In addition a Datix form will be completed on-line for investigation. The appropriate members of the CoMET senior team should be made aware of any untoward incidents.
12.5 Patient notes: Copies of the CoMET notes, as completed to that point, will be left at the receiving unit to form part of their clinical notes. The original will be returned to CoMET to complete the records for that episode. All notes should be stored in accordance with the UHL Documentation Policy for Patients’ case Notes.
12.6 All notes will be stored on an electronic database.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 163
Appendix 19 – Network Training Strategy
Training and Education Strategy
Objective
To ensure that all healthcare professionals involved in the care of patients with CHD have access to standardised training and competency based education programmes across the Congenital Heart Network including linked neonatal units.
Approach
Nursing
Over the next two years we aim to expand the scope of local expertise by first establishing a virtual network of Link Cardiac Nurses who are willing to commit to (and are supported to do so by their employers) becoming local experts and a point of liaison for dissemination and feedback of information relating to both patient care and professional nursing practice in congenital cardiology.
The training will be open to all Network centers’ that have inpatient CHD facilities, Specialist Cardiac Liaison support will be provided for those centers’ without inpatient facilities.
The training will consist of a competency based Programme (based upon the RCN competences: Children and Young people’s cardiac nursing) and will be supported by the following;
• Educational support from the EMCHN lead Nurse • Named mentor from the EMCHC specialised Cardiac Liaison nursing team • A competency based , time related preceptorship to include required periods of face to face
training, online modules, consultant led outpatients sessions, individual mentor training sessions, and bi- annual training days for CPD
• Web based access to training modules will enable both the Link Nurse , her mentor and the EMCHN Lead Nurse to monitor progress and track completion of the required competencies in appropriate time periods
The Link Nurse on completion of the training will be able to demonstrate the following skills and knowledge
• Full understanding of normal cardiac anatomy and physiology • Good understanding of the key areas of Congenital Heart Disease and the implications
of these on the anatomy and physiology of the patient • Ability to explain the conditions in simple terms to patients and parents/ carers • Good understanding of the expected patient pathways for each condition
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 164
• Good understanding of the support available for the patient from the EMCHC Network and third sector organisations
• The ability to signpost the patient to a Named Specialist Cardiac Liaison Nurse at EMCHC who will lead the future support in conjunction with the local Link Nurse
Next steps
EMCHC current training programme to be reviewed against the competencies required in the Network Training and viability for Network colleagues to participate. Nurse leadership to ensure competency training is cascaded down to all ward staff.
Lead Nurse (once recruited) to establish education needs across the Network and review viability of offering a training day in each Network centre per annum.
A pilot scheme will be implemented with two Network centres – Derby Hospitals NHS Trust, and North West Anglia NHS Trust both of whom have identified paediatric nursing staff to embark on the proposed training.
The service delivery group established as a sub group from the Network Board will work on the detail of the training plan, and the implementation/ monitoring of the pilot scheme.
The service delivery group will also investigate the most appropriate method of online access and modules for nurses of all experience levels throughout the Network as a method of personal CPD.
Timescales
Q1/2 2019/20 – Confirm structure of training plan, agree competency matrix and monitoring mechanism – gain approval through Network Board
Q3 – commence pilot in two Network centres
Q1 2020/21 – analyse results and recruit in other network centres – Ensure Network communications are robust so every network centre is aware of the education and training plan on offer.
Associated Health Professionals
EMCHC have highly specialised physiologists who hold BSE and EAE accreditation in Congenital echocardiography, currently performing and reporting up to 9000 Echo`s a year for both outpatients and inpatients.
We provide support and training for the network in the following ways:
Telephone support
• Network staff attending our clinics for one to one training, currently Nottingham. (Other centres attended Derby and Peterborough)
• Attendance to the network clinics to provide support and training for physiologists until no longer required.
• Provide a separate physiology meeting alongside the Network bi annual training meeting to discuss standardisation, guidelines and training.
• Provide supervisors for both medical and technical staff for EAE accreditation. The aim for the rest of 2018/19 and moving into 2019/20 is to investigate the opportunities for wider Echo training across the Network utilising the Zoom technology.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 165
Educational Meetings for the East Midlands Congenital Heart Network
Key Goals:
• To encourage Network collaboration and share knowledge • To support clinicians particularly PEC/ACHD interest cardiologists to help them maintain
their competency in Congenital Cardiology • To provide SPIN model training for trainees in region with interest in Paediatric Cardiology
to achieve certification and offer career advice Regional study days:
EMCHC have organised and delivered half a day educational meetings, twice a year since 2016. Feedback from these sessions has been very good. We endeavour to focus on topics which are useful for those attending from across the EMCHN.
With the formal establishment of the EMCHN it is proposed to continue with these meetings. The meeting will be a regular event on last Friday of January every year and will be held at Leicester. The second meeting will be on last Friday of June, every year. This will be at any one of the regional EMCHC Network centres.
We will invite all PEC, ACHD cardiologist, neonatologist, trainees, general paediatricians, intensive care team, echo cardiographers, paediatric nurses, community nurses and relevant other professional to this meeting. The meeting will also be available to participate via videoconferencing link. It is intended that this meeting will also offer a choice of educational presentations in the afternoon session, to allow nursing/ associated health professional colleagues the opportunity to tailor their learning.
All presentations will be made available on request.
We constantly strive to improve the quality of these training days hence feedback forms will be distributed during these meeting and reviewed through the Network Board
Local study days:
It is not always possible for local clinicians to attend the study days organised for the Network so offering something in the local centre will enable a broader reach across the Network. The local study days will be organised by the PEC after discussion with the visiting cardiologist. This will depend on the availability of visiting cardiologist and expression of interest by local team and will be available to all disciplines.
Local educational meetings:
EMCHC will video conference all departmental educational meeting i.e., MDTs and Journals clubs across the network to improve opportunity of peripheral team to participate and learn. All Network centres will be provided access to ‘Zoom’ technology to enable easy access to these training sessions. Advance notification of the dates and times will be made available through circulation lists and on the EMCHN website
Other support:
We also welcome clinicians from the Network to attend various specialist clinics and in-house activities at Glenfield Hospital to facilitate learning and CPD activities. Honorary contracts are provided for clinicians on request.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 166
Appendix 20 – EMCHN Terms of Reference
CONGENITAL HEART NETWORK BOARD
FOR THE EAST MIDLANDS AND EAST OF ENGLAND
TERMS OF REFERENCE
1. Overview
The key aim of the Congenital Heart Network is to support the provision of high quality care for Congenital Heart Disease patients across the East Midlands and East of England.
Its vision is to be a Network whereby:
• Patients have equitable access to services regardless of geography • Care is provided seamlessly across the Network and its various stages of transition (between ages,
locations, services and where there are co-morbidities) • High quality care is delivered and participating centres meet national standards of CHD care • The provision of high quality information for patients, families, staff and commissioners is
supported • There is a strong and collective voice for Network stakeholders • There is a strong culture of collaboration and action to continually improve services • All work will be clinically led and informed by patients and their carers; • Patient care will be kept, or developed, closer to home where possible;
The Network’s key objectives are:
1. To provide strategic direction for CHD care across the East Midlands and East of England 2. To monitor and drive improvements in quality of care 3. To support the delivery of equitable, timely access for patients 4. To support improvements in patient and family experience 5. To support the education, training and development of the workforce within the Network 6. To be a central point of information and communication for Network stakeholders 7. To ensure it can demonstrate the value of the Network and its activities
2. Responsibilities
University Hospitals of Leicester NHS Trust is the host organisation for the Network. Responsibility for the performance management of the Network is overseen by the Network Board with the primary responsibility retained by the constituent organisation.
This Network Board will be responsible for ensuring the effective functioning of the Network working in conjunction with commissioners from England and Wales. The Network Board will be responsible for the delivery of following areas of work:
2.1 Strategic Direction and Planning
• Offering professional and clinical leadership across the CHD Network
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 167
• Developing an annual work programme for the Network to deliver national strategy and outcomes • Producing an annual report • Ensuring transparent and active management of Network risks • Ensuring effective links with national programmes of care • Ensuring effective links with local, regional and national commissioners • Engaging with Clinical Reference Groups, Academic Health Science Networks, other relevant
Networks and Senates
2.2 Improved Quality and Standards of Care
• Assessing and monitoring participating Centres against national standards of care for CHD centres • Developing and implementing network best practice, policies and guidance for CHD care • Delivering effective clinical governance of the Network, including:
o Network Mortality and Morbidity reviews o Risk analysis and risk management o Incident reporting with follow up action plans/shared learning o Delivery of an annual audit programme agreed with members, and reporting outcomes o Undertaking benchmarking activities as required o Peer review programme
• Driving ongoing service improvements, ensuring best practice models are embedded and contribute to improved quality performance
• Developing and monitoring any Network information systems (e.g. dashboard) • Signposting to training and Continued Professional Development opportunities to support learning
across the Network •
2.3 Equitable, Timely Access for Patients
• Understanding and monitoring waiting times for access to care across the network • Supporting improvement plans whereby waiting times or access to services (e.g. nursing,
psychology) fall below expected standards • Ensure equity of access across the Network • To ensure consistency of pathways and care across the Network
2.4 Improved Patient and Family Experience
• To ensure the provision of high quality information for patients and families across the Network • To create and implement a Network Communication and Engagement strategy • To ensure the voice of patients and families is heard throughout Network activities • To ensure the Network seeks, listens to and acts upon patient and family feedback • To embrace the use of technology to support improve patient and family experience • To engage with and support third sector partners including patient/family support groups and
charities
2.5 Education, Training and Workforce
• To develop an Education and Training strategy for the Network, building on existing clinical network programmes of training and education
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 168
• To signpost/coordinate/deliver (as appropriate) opportunities for education, training and CPD for different professional groups within the Network
• To understand any trends in workforce issues and support collective solutions where possible • To support programmes of research across the Network • Linking into local Education and Training Boards (LETBs)
2.6 Information and Communication
• To be a central point of information for Network stakeholders • To provide access and training to Heart Suite data information system • To ensure the provision of high quality information for stakeholders • To embrace different communication channels in order to communicate effectively with
stakeholders • To ensure regular and two way communication between stakeholders
2.7 Demonstrate Value Adding
• To ensure Network activities are planned and delivered in line with the views of stakeholders • To ensure good use of existing resources • To deliver on required outputs in a timely fashion • To be a collective voice for Network stakeholders on local, regional and national matters • To create a culture of collaboration, action and partnership working
3. Accountability
The Network Board is held to account by the host Chief Executive Officer and by commissioners in England and Wales through arrangements to be defined in the first year of operation.
3.1 Structures within University Hospitals of Leicester NHS Trust
The Network will be a member of the Children’s Operational Performance, Quality and Safety Board at University Hospitals of Leicester NHS Trust. It will provide regular updates to that Board, including progress updates, risk and issue management. Board members are encouraged to support, check and challenge the Network on any of its activities, and may escalate any issues as deemed necessary through the Women’s and Children’s performance meetings which reports into the Trust’s Senior Leadership Team meeting, chaired by the Chief Executive Officer.
3.2 Structures within commissioning bodies
NHS England
The Network provides assurance to the NHS England hub team who reports into the Executive Management Team and the Regional Senior Manager, who will review the Terms of Reference, Annual Work Plans, Non clinical Policies or guidelines, Network Patient & Public Involvement Strategy and Network Communications & Engagement Strategy. The Network will provide a quarterly Assurance Report and Annual Report.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 169
3.3 Diagram outlining accountabilities and reporting lines
Accountable to; Providing Assurance to;
4. Board Membership
4.1 The following groups should be represented on the Network Board:
Member/Representative Notes
Co -Chairs
Voting Member (One Vote each )
The Co- Chairs will be elected by a majority vote of Network Board members at a Network Board meeting. If a majority decision cannot be reached by the network board the Chief Executive of the Host Organisation will have the deciding vote.
Nominations for the Chair of the Network Board will be requested from Board Members to be submitted 14 days before a meeting where a vote is taken.
The Chair may be from any centre within the Network (see section 4.2 for a list of centres). Either the Chair or Deputy Chair must be from the Host Organisation.
The Co- Chair will be either a senior clinician with management
Clinical Guidance
Group
UHL Children’s Operational Quality and
Performance Board
UHL Women’s & Children’s performance
meetings
UHL Senior Leadership Team
NHS England Specialised Commissioning (Midlands and
East)
NHS England East Executive Management Team and Regional
Senior Management Team
CHD Network Board
Task and Finish Group
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 170
responsibilities or a director level manager.
It is the responsibility of the Co- Chair to confirm that the actual membership of the Board is consistent with the peer review requirements for representation of fetal, paediatric, and adult age groups from all professions across the network.
Term of Office Two years, may be re-elected for up to two terms
Network Clinical Director
Voting member (One Vote)
The Network Clinical Director will be elected by a majority vote of Network Board members at a Network Board meeting.
Nominations for the Network Clinical Director will be requested from Board Members to be submitted 14 days before a meeting where a vote is taken.
The Network Clinical Director must be from the lead Level 1 centre.
The Network Clinical Director will be a senior consultant medic with management responsibilities.
Term of Office: Two years, may be re-elected for up to two terms.
Network Lead Nurse Voting member (One Vote)
The Network Lead Nurse will be a Senior Nurse with management responsibilities from the lead Level 1 centre.
This will be a permanent position
Nurse representation from other Network centres will be encouraged where possible and will form part of the Network centre’s nominated members
Associated Health Professional
Voting member
(One Vote)
The Network Associated Health Professional will be elected by a majority vote of Network Board members at a Network Board meeting.
Nominations for the Network Associated Health Professional will be requested from Board Members to be submitted 14 days before a meeting where a vote is taken.
The Network Associated Health Professional may be from any centre within the Network (see section 4.2 for a list of centres).
The Network Associated Health Professional will be a senior physiologist, dietician or play specialist with management responsibilities.
Term of Office: Two years, may be re-elected for up to two terms.
Network Centre Representatives
(One Vote per Centre)
All Network centres within the East Midlands Congenital Heart Network will be invited to nominate a minimum of two representatives to the Board.
Representatives will be requested through the centre’s medical director. Representatives must be able to represent the centre and the views of Fetal, Neonatal, Paediatric, and Adult services where appropriate.
Representatives may be from any of the following groups: senior medics;
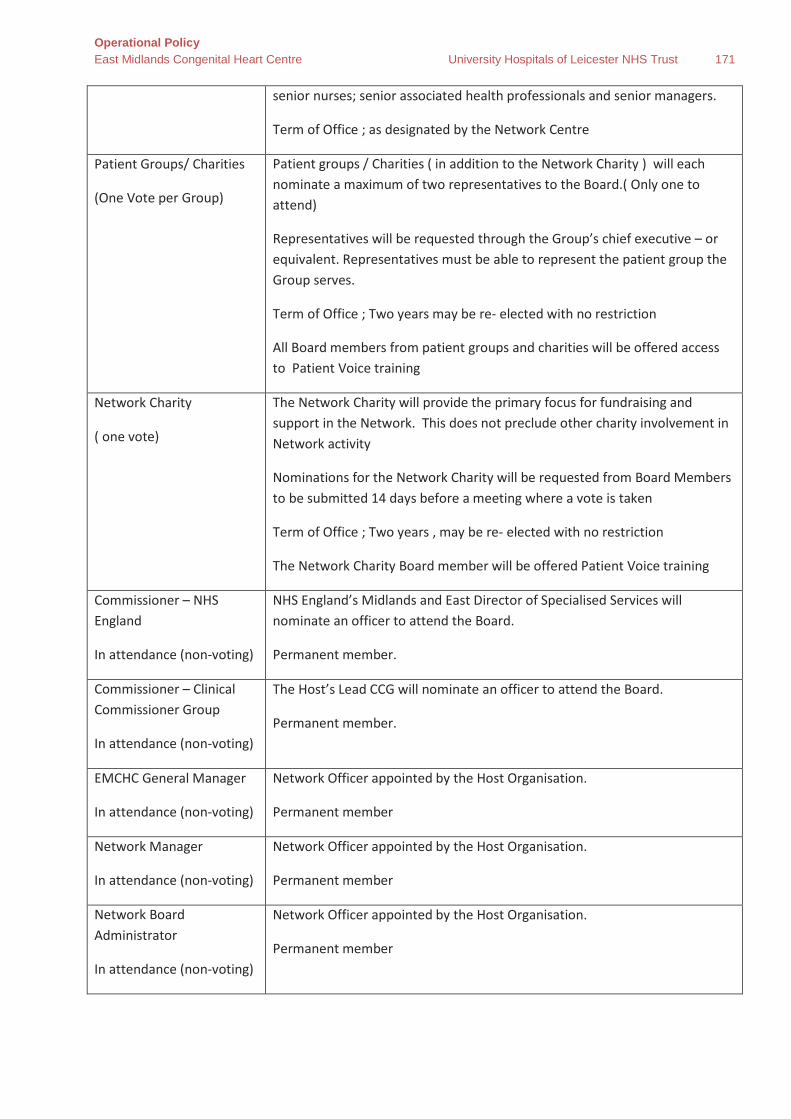
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 171
senior nurses; senior associated health professionals and senior managers.
Term of Office ; as designated by the Network Centre
Patient Groups/ Charities
(One Vote per Group)
Patient groups / Charities ( in addition to the Network Charity ) will each nominate a maximum of two representatives to the Board.( Only one to attend)
Representatives will be requested through the Group’s chief executive – or equivalent. Representatives must be able to represent the patient group the Group serves.
Term of Office ; Two years may be re- elected with no restriction
All Board members from patient groups and charities will be offered access to Patient Voice training
Network Charity
( one vote)
The Network Charity will provide the primary focus for fundraising and support in the Network. This does not preclude other charity involvement in Network activity
Nominations for the Network Charity will be requested from Board Members to be submitted 14 days before a meeting where a vote is taken
Term of Office ; Two years , may be re- elected with no restriction
The Network Charity Board member will be offered Patient Voice training
Commissioner – NHS England
In attendance (non-voting)
NHS England’s Midlands and East Director of Specialised Services will nominate an officer to attend the Board.
Permanent member.
Commissioner – Clinical Commissioner Group
In attendance (non-voting)
The Host’s Lead CCG will nominate an officer to attend the Board.
Permanent member.
EMCHC General Manager
In attendance (non-voting)
Network Officer appointed by the Host Organisation.
Permanent member
Network Manager
In attendance (non-voting)
Network Officer appointed by the Host Organisation.
Permanent member
Network Board Administrator
In attendance (non-voting)
Network Officer appointed by the Host Organisation.
Permanent member

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 172
4.2 The Centres who fall within the network catchment area are:
Level 1 Centre • University Hospitals of Leicester NHS Trust (East Midlands Congenital Heart Centre)
Level 3 Centres: • United Hospitals Lincolnshire NHS Trust • Nottingham University Hospitals NHS Trust • Derby Teaching Hospitals NHS Foundation Trust • Sherwood Forest NHS Foundation Trust • Northampton General Hospital NHS Trust • Kettering General Hospital NHS Foundation Trust • The George Eliot Hospital NHS Trust • North West Anglia Foundation Trust • University Hospital Coventry and Warwick • Burton NHS Foundation Trust • Chesterfield Royal NHS Foundation Trust • Doncaster and Bassetlaw NHS Trust • Royal Stoke University Hospitals • Milton Keynes University Hospital • Bedford Hospital NHS Trust • Queen Elizabeth Hospital , Kings Lynn
4.3 Sub – Groups from the Main Network Board
The Network Board will form sub-groups or task and finish groups as required for specific pieces of work with membership drawn from across the network. Membership and the objective of the groups will be agreed by the Main Network Board. The Board will also consider the need for Patient involvement and ensure representation is appropriate.
1. Clinical Guidance Group - this group will review pathways and guidelines for the Network the group will feedback to the main board with recommendations for final approval
2. Task and Finish groups - these groups will work on specific tasks that are identified by the Board that require a particular focus or wider involvement. They will make recommendations to the main board for approval and sign off
4.4 Frequency of Meetings
The Network Board will meet 3 times per annum in January, May and September. The meetings will be held at the Level 1 centre (Glenfield Hospital). The Board will consider the possibility of the meeting being held via video conference, or at a Network Hospital as appropriate.
The Clinical guidance group - will meet as required in person or via video/ tele conference, but a minimum of 3 times per annum to inform the Main Network Board meeting.
Task and finish group - meets as required to work on key actions identified by the Board
Membership of the two sub groups will include representatives from the Network hospitals and stakeholders who do not necessarily (but may also) sit on the network Board – but are able to represent the views of their Organisation.
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 173
4.2 Quorum
The quorum of the group will be:
• Network Chair or Deputy;
• The Network Manager, Clinical Director and Lead Nurse;
• A representative from at least 4 of the 16 Centres, including at least 2 of the Level 3 centres and a minimum of one adult and one paediatric representative;
• A commissioning, non-NHS organisation or patient/family representative.
4.3 Responsibility of Board Members
A requirement for board membership is that all members attend a minimum of at least 1 meeting a year, although where possible all board meetings should be prioritised. The ability to commit to board meetings should form part of member’s decision making process when nominating themselves to the board. Network Board meeting dates will be published well in advance with a minimum of 8 weeks’ notice.
It is the responsibility of Board members that they are fully prepared, and have reviewed the papers for each meeting to ensure that recommendations are made in the best interests of the Network as a whole and are not influenced by locality bias.
All papers will be issued one week in advance of meetings.
The Chair must ensure that the Board’s decisions on all matters brought before it are taken in an open, balanced, objective and unbiased manner. In turn individual group members must demonstrate through their actions, that their contribution to the group’s decision making is based upon the best interest of the Network rather than of the individual Trusts by which they are employed. The Network must feel that the Board exists to represent a collective view and that the nature of its membership therein must not be felt to disadvantage any unit or trust from across the East Midlands and East of England.
Decisions will be made through a majority voting process from Board members who are in attendance, unless prior arrangements have been made for voting preferences to be made in advance. Each Board member has an equal vote with the Chair carrying the casting vote.
4.4 Reporting
The Network Board will;
• Report to the UHL Children’s Operational Quality and Performance Board • Report formally to the NHS England Specialist Commissioning Team’s on the Board’s activities. This
includes updates on activity, the submission of minutes, written reports and an annual report. • Submit formal work plan and annual report to the UHL Trust Board and NHS Commissioners (as
required). • Provide details of any significant matters under consideration by Board to the relevant
Commissioners. • Ensure appropriate escalation arrangements are in place to alert both the Commissioners and
Trusts of any urgent or critical matters that may compromise patient care and/or affect the operation or reputation of commissioning or CHD care services across the Network.

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 174
4.5 Sub-groups
The Board will oversee any sub-groups that form part of the Network and are responsible for their progress and outputs.
5. Review
The constitution, membership and terms of reference of the Network Board will be formally reviewed soon after the first 12 months of operation and when required thereafter.
Document Control
Author:
Name: Position: Date:
Alison Poole Network Manager 16.04.18
Amendments:
Name: Details: Date:
Jon Currington Comments 16 04 18
Alison Poole Revised as per comments 21 05018
Alison Poole Clean version issued 19 06 18
Alison Poole Revised as per comments from Board meeting on the 3rd October 2018
11/10/18
Approved By:
Name: Position: Date:
Board Vote Network Board meeting 23/01/19

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 175
Appendix 21 – Abbreviations and definitions
Abbreviation Definition
A&E Accident and Emergency
ACHD Adult Congenital Heart Disease
ACP Advanced Clinical Practioners
ACR Urine albumin to creatinine ratio
AICU Adult Intensive Care Unit
ANNB Antenatal and Newborn Screening
ANNP Advance Neonatal Nurse Practitioner
APLS Advanced Paediatric Life Support
APTT Activated Partial Thromboplastin Clotting Time
BCCA British Congenital Cardiac Association
BP Blood Pressure
BSE Bovine spongiform encephalopathy
BT shunts Blalock-Thomas-Tausig shunt
CCT Certificate of Completion of Training
CD Controlled Drugs
CenTre CenTre Neonatal Transport Service
CHD Congenital Heart Disease
CICU Children's Intensive Care Unit
CMG Clinical Management Group
CMV Cytomegalovirus
CNN Central Newborn Network
CoMET Children's Medical Emergency Transport Service
CPAP Continuous positive airway pressure
CPD Continual Professional Development
CRP C-reactive protein
CT Computerised Tomography
CVL Central Venous Line
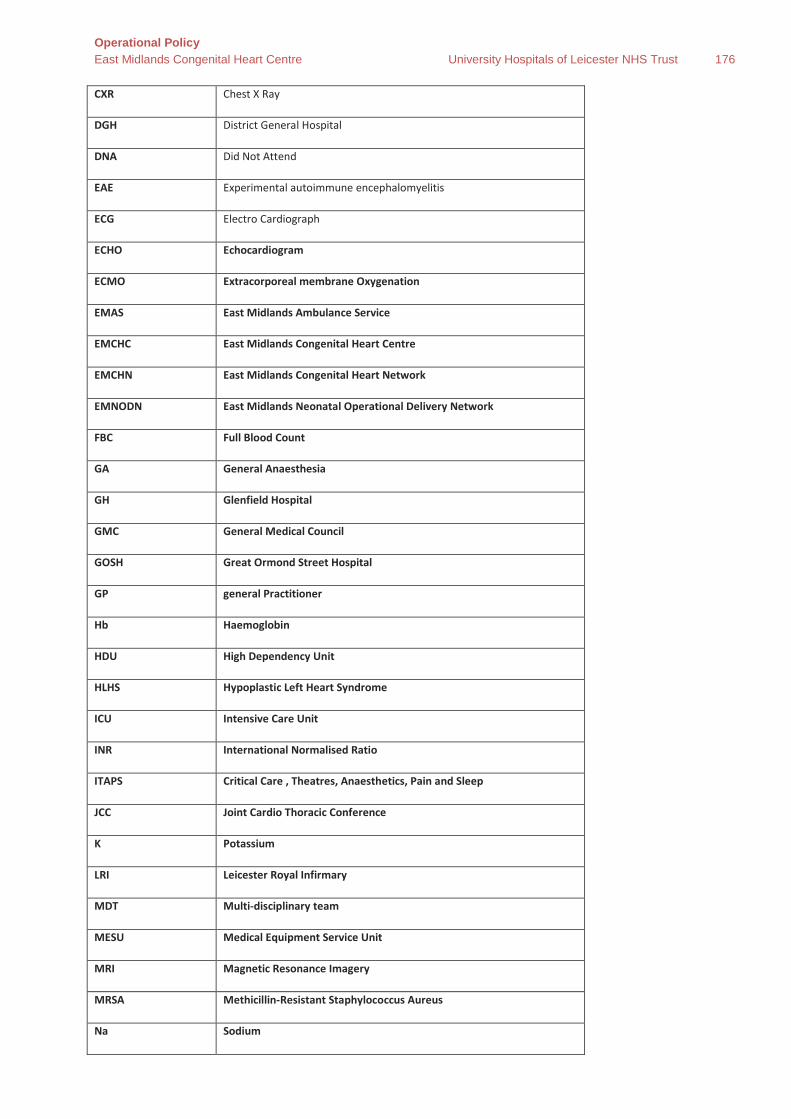
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 176
CXR Chest X Ray
DGH District General Hospital
DNA Did Not Attend
EAE Experimental autoimmune encephalomyelitis
ECG Electro Cardiograph
ECHO Echocardiogram
ECMO Extracorporeal membrane Oxygenation
EMAS East Midlands Ambulance Service
EMCHC East Midlands Congenital Heart Centre
EMCHN East Midlands Congenital Heart Network
EMNODN East Midlands Neonatal Operational Delivery Network
FBC Full Blood Count
GA General Anaesthesia
GH Glenfield Hospital
GMC General Medical Council
GOSH Great Ormond Street Hospital
GP general Practitioner
Hb Haemoglobin
HDU High Dependency Unit
HLHS Hypoplastic Left Heart Syndrome
ICU Intensive Care Unit
INR International Normalised Ratio
ITAPS Critical Care , Theatres, Anaesthetics, Pain and Sleep
JCC Joint Cardio Thoracic Conference
K Potassium
LRI Leicester Royal Infirmary
MDT Multi-disciplinary team
MESU Medical Equipment Service Unit
MRI Magnetic Resonance Imagery
MRSA Methicillin-Resistant Staphylococcus Aureus
Na Sodium
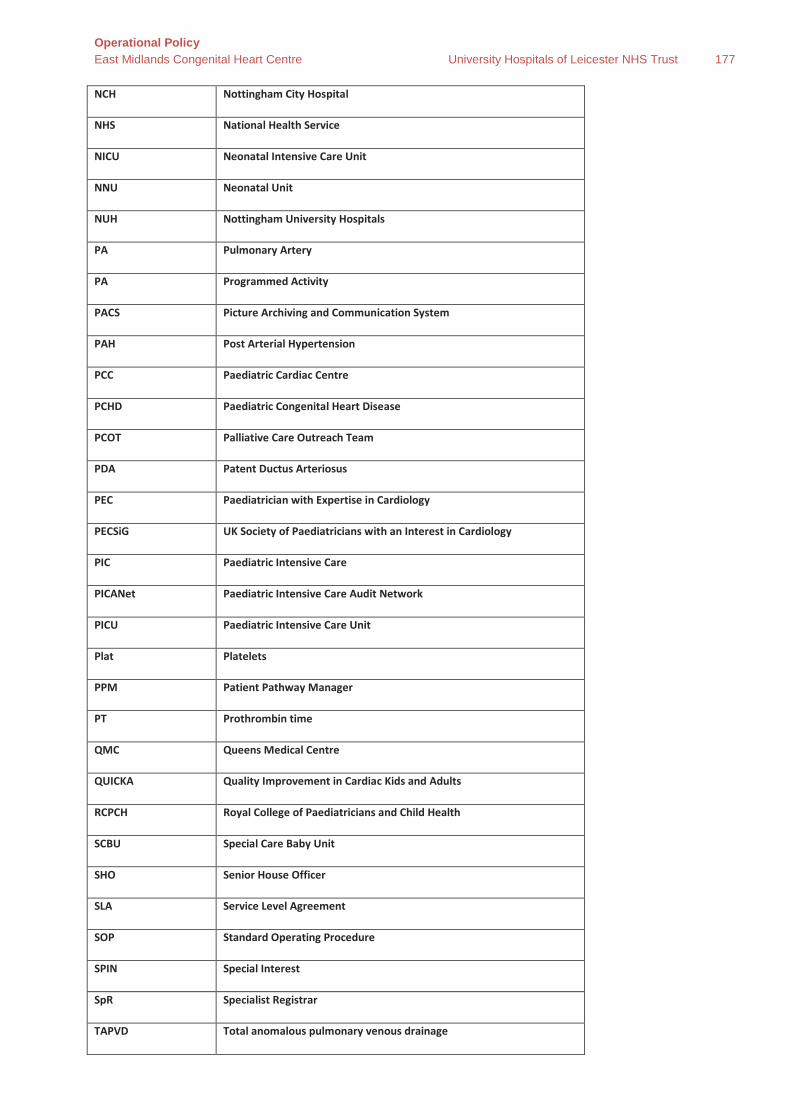
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 177
NCH Nottingham City Hospital
NHS National Health Service
NICU Neonatal Intensive Care Unit
NNU Neonatal Unit
NUH Nottingham University Hospitals
PA Pulmonary Artery
PA Programmed Activity
PACS Picture Archiving and Communication System
PAH Post Arterial Hypertension
PCC Paediatric Cardiac Centre
PCHD Paediatric Congenital Heart Disease
PCOT Palliative Care Outreach Team
PDA Patent Ductus Arteriosus
PEC Paediatrician with Expertise in Cardiology
PECSiG UK Society of Paediatricians with an Interest in Cardiology
PIC Paediatric Intensive Care
PICANet Paediatric Intensive Care Audit Network
PICU Paediatric Intensive Care Unit
Plat Platelets
PPM Patient Pathway Manager
PT Prothrombin time
QMC Queens Medical Centre
QUICKA Quality Improvement in Cardiac Kids and Adults
RCPCH Royal College of Paediatricians and Child Health
SCBU Special Care Baby Unit
SHO Senior House Officer
SLA Service Level Agreement
SOP Standard Operating Procedure
SPIN Special Interest
SpR Specialist Registrar
TAPVD Total anomalous pulmonary venous drainage
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 178
TPN Trent Perinatal Network
U&E Urea and Electrolytes
UHL University Hospitals of Leicester
WCC White Cell Count
WEQAS Wales External Quality Assessment
WNB Was Not Brought
XM Cross Match
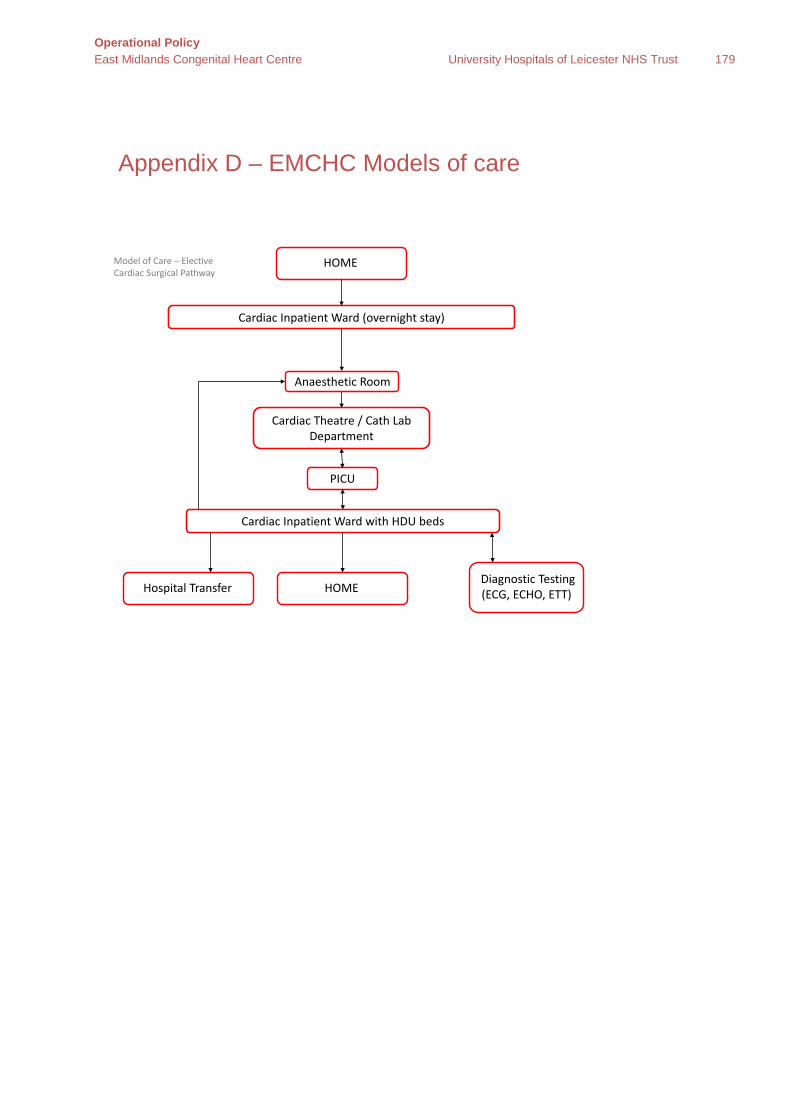
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 179
Appendix D – EMCHC Models of care
PICU
HOMEModel of Care – ElectiveCardiac Surgical Pathway
Cardiac Inpatient Ward (overnight stay)
Cardiac Theatre / Cath Lab Department
Anaesthetic Room
Cardiac Inpatient Ward with HDU beds
HOMEDiagnostic Testing (ECG, ECHO, ETT) Hospital Transfer
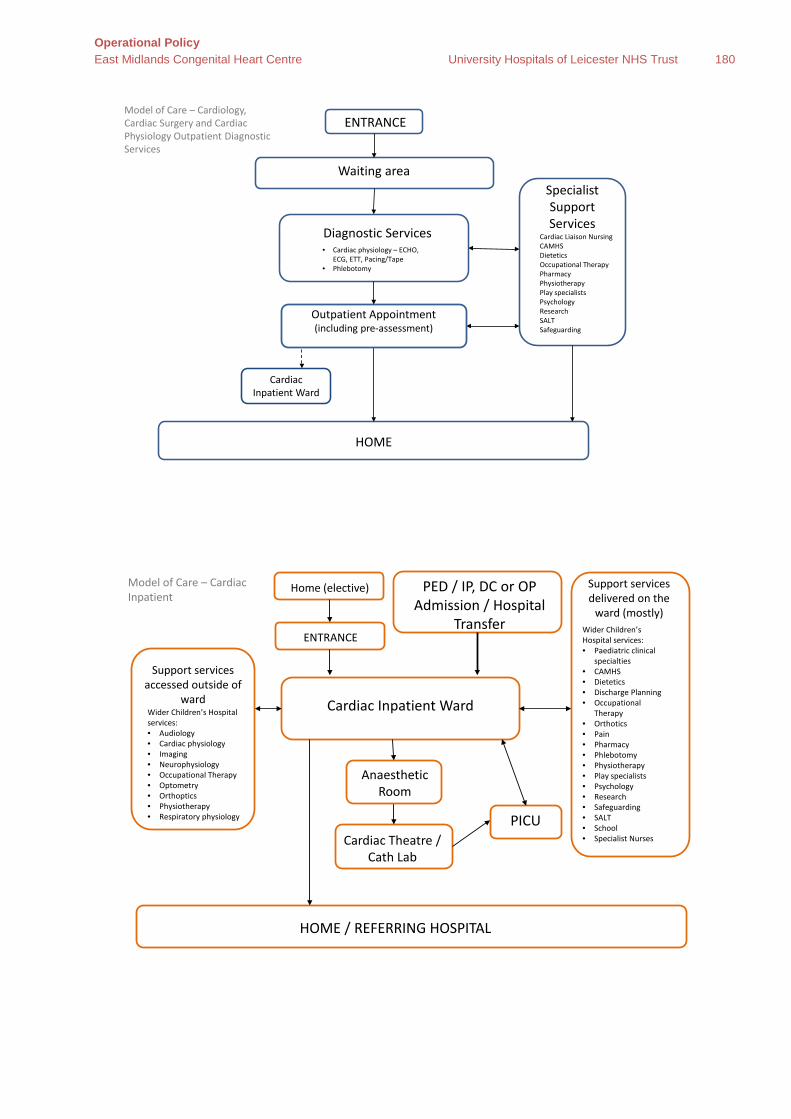
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 180
ENTRANCE
Waiting area
Diagnostic Services
Specialist Support Services
HOME
Model of Care – Cardiology, Cardiac Surgery and Cardiac Physiology Outpatient Diagnostic Services
• Cardiac physiology – ECHO, ECG, ETT, Pacing/Tape
• Phlebotomy
Cardiac Liaison Nursing CAMHSDieteticsOccupational TherapyPharmacyPhysiotherapyPlay specialists PsychologyResearch SALTSafeguarding
Outpatient Appointment(including pre-assessment)
Cardiac Inpatient Ward
Model of Care – Cardiac Inpatient
ENTRANCE
Cardiac Inpatient Ward
Support services accessed outside of
ward Wider Children’s Hospital services: • Audiology• Cardiac physiology• Imaging• Neurophysiology• Occupational Therapy• Optometry• Orthoptics• Physiotherapy• Respiratory physiology
Support services delivered on the
ward (mostly)Wider Children’s Hospital services: • Paediatric clinical
specialties• CAMHS• Dietetics• Discharge Planning• Occupational
Therapy• Orthotics• Pain• Pharmacy• Phlebotomy• Physiotherapy• Play specialists • Psychology• Research • Safeguarding• SALT• School• Specialist NursesCardiac Theatre /
Cath Lab
HOME / REFERRING HOSPITAL
PICU
PED / IP, DC or OP Admission / Hospital
Transfer
Home (elective)
Anaesthetic Room
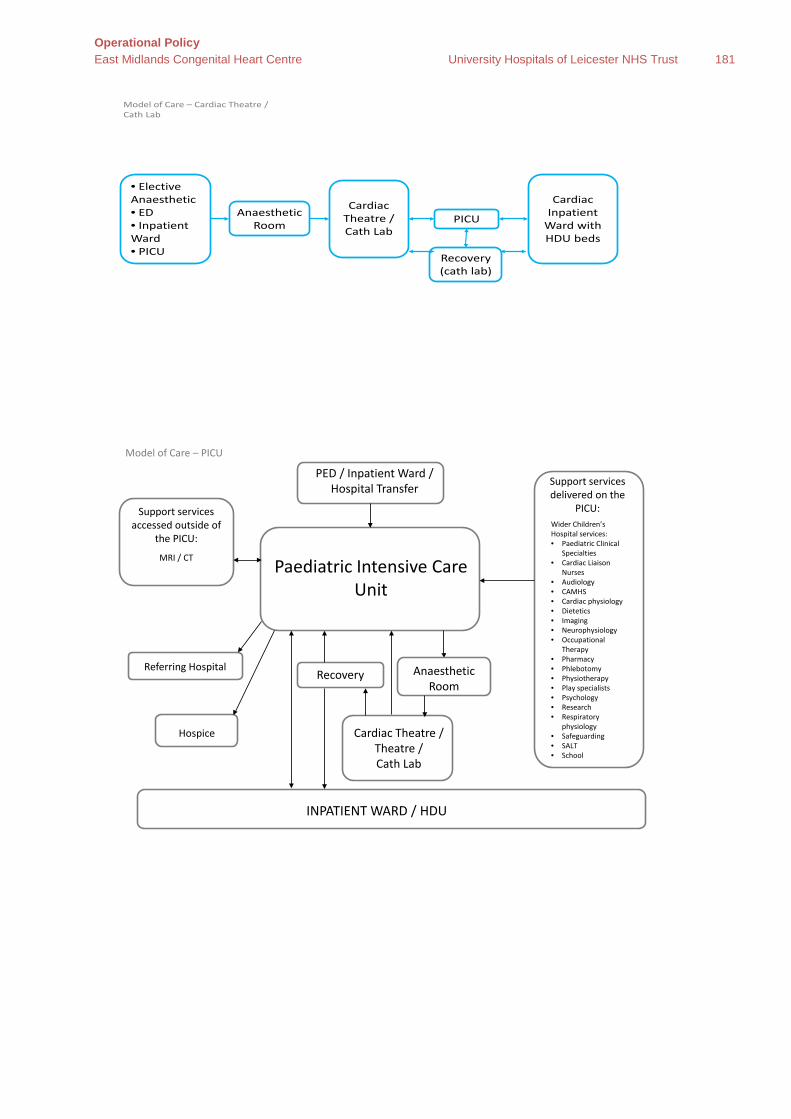
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 181
Model of Care – Cardiac Theatre / Cath Lab
Cardiac Theatre / Cath Lab
• Elective Anaesthetic • ED• Inpatient Ward• PICU
Anaesthetic Room PICU
Cardiac Inpatient
Ward with HDU beds
Recovery (cath lab)
Model of Care – PICU
Paediatric Intensive Care Unit
Support services accessed outside of
the PICU:
MRI / CT
Support services delivered on the
PICU:Wider Children’s Hospital services: • Paediatric Clinical
Specialties• Cardiac Liaison
Nurses• Audiology• CAMHS• Cardiac physiology• Dietetics• Imaging• Neurophysiology• Occupational
Therapy• Pharmacy• Phlebotomy• Physiotherapy• Play specialists • Psychology• Research • Respiratory
physiology• Safeguarding• SALT• School
Cardiac Theatre / Theatre / Cath Lab
INPATIENT WARD / HDU
Recovery
PED / Inpatient Ward / Hospital Transfer
Referring Hospital
Hospice
Anaesthetic Room

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 182
Model of Care – MRI / CT
MRI / CT Scan
Anaesthetic Room
PED / Inpatient & Daycase Ward /
Outpatient Areas / PICU
Home
Small waiting area
Recovery
Home Inpatient Ward / Daycase Areas / PICU

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 183
Appendix E– Patient Pathways Paediatric
Your Congenital Heart Journey – Children
Initi
al re
ferr
al
Dia
gnos
is
Care
pat
hway
s
Your antenatal / postnatal team
GP or paediatrician who may refer you to an outpatient clinic near you
Your Catheter Pathway
If your medical team at your local centre are concerned that your baby or your child has a heart condition , then they will need to refer you to one of the East Midlands Congenital Heart team for further investigations and you may follow one or more of the pathways below
At this stage you will also be introduced to a Cardiac Liaison Nurse who will be there for you along the way , and will ensure you have all the support and information you need
Accident and Emergency
Your Surgical Pathway
Your Inpatient pathway
Your Outpatient Pathway
Your Transition pathway
Patient Information
Your Fetal Pathway
Car
e o
pti
ons
D
iag
nosi
s C
are
pat
hway
s
You will be invited to a fetal cardiac clinic to have a detailed scan of your baby’s heart by a
specialist in fetal heart problems.
You will be introduced at this stage to a specialist Cardiac Liaison Nurse who will spend more time explaining what is happening and provide you with information to take away and her contact
details. You may also see a fetal medicine consultant, midwife and may be referred to other
doctors such as a geneticist as well
If the scan shows that your baby has a heart
condition your cardiologist will talk to you about the condition, what it means and options for you and your treatment and care
This pathway tells you more about what happens when you are referred to an antenatal cardiac clinic. Your local antenatal team will explain to you that they wish you to have further investigations to clarify if your baby has a cardiac condition or not. They will then refer you to the East Midlands Congenital
Heart team who will offer to see you within 2 working days.
Your Surgical Pathway
Your Inpatient pathway Your Outpatient Pathway
If your scan shows your baby has a normal heart structure
then you will be looked after by your local antenatal team
Your baby may not initially need specialist care but will be monitored by the cardiac team
for potential treatment later
You may be able to have your baby locally and come to the
East Midlands Congenital Heart Centre for treatment when
needed
Your team may recommend that you deliver your baby at
Leicester Hospitals where specialist treatment is available
If the team feel your baby needs treatment or monitoring they will follow one or more of the pathways below
Your Catheter Pathway
Patient Information
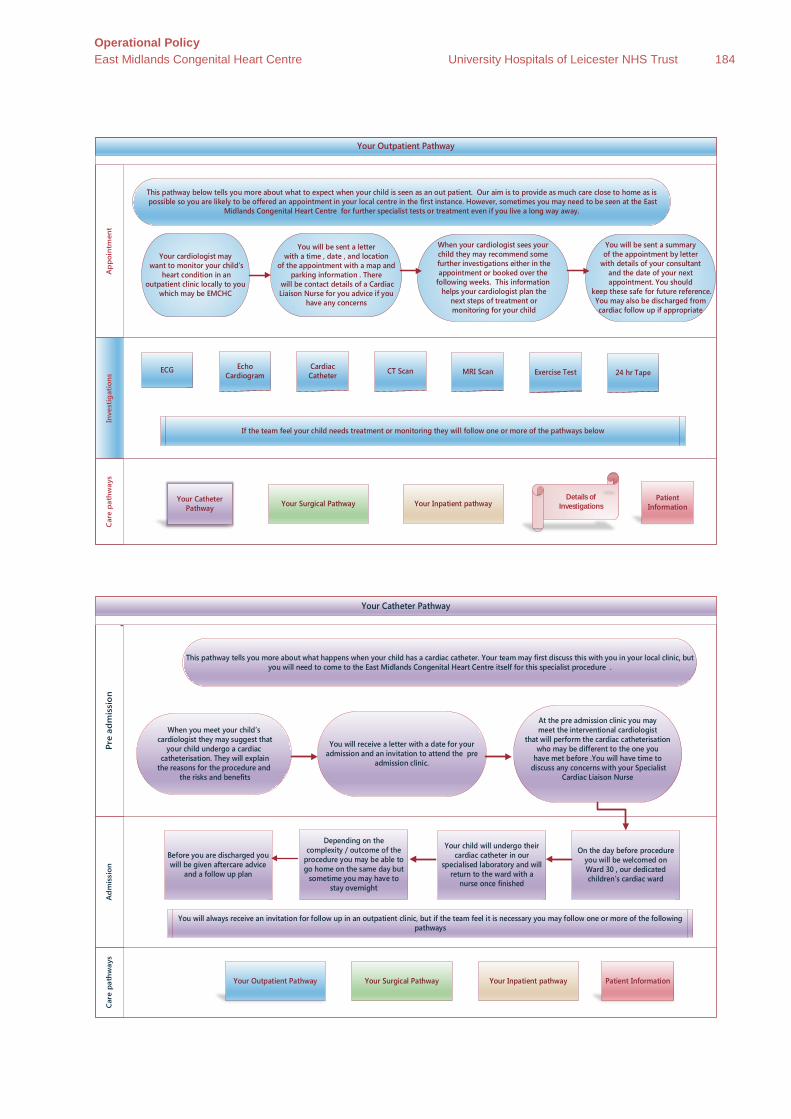
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 184
Your Outpatient Pathway
Inve
stig
atio
ns
A
ppo
intm
ent
C
are
path
way
s
Your cardiologist may want to monitor your child’s
heart condition in an outpatient clinic locally to you
which may be EMCHC
When your cardiologist sees your child they may recommend some
further investigations either in the appointment or booked over the
following weeks. This information helps your cardiologist plan the
next steps of treatment or monitoring for your child
You will be sent a letter with a time , date , and location
of the appointment with a map and parking information . There
will be contact details of a Cardiac Liaison Nurse for you advice if you
have any concerns
This pathway below tells you more about what to expect when your child is seen as an out patient. Our aim is to provide as much care close to home as is possible so you are likely to be offered an appointment in your local centre in the first instance. However, sometimes you may need to be seen at the East
Midlands Congenital Heart Centre for further specialist tests or treatment even if you live a long way away.
Your Surgical Pathway Your Inpatient pathway
ECG Echo Cardiogram
Cardiac Catheter CT Scan
If the team feel your child needs treatment or monitoring they will follow one or more of the pathways below
Your Catheter Pathway
You will be sent a summary of the appointment by letter
with details of your consultant and the date of your next appointment. You should
keep these safe for future reference. You may also be discharged from cardiac follow up if appropriate
MRI Scan
Details of Investigations
Patient Information
Exercise Test 24 hr Tape
Your Catheter Pathway
Ad
mis
sion
Pr
e ad
mis
sio
n
Car
e pa
thw
ays
When you meet your child’s cardiologist they may suggest that
your child undergo a cardiac catheterisation. They will explain the reasons for the procedure and
the risks and benefits
At the pre admission clinic you may meet the interventional cardiologist
that will perform the cardiac catheterisation who may be different to the one you
have met before .You will have time to discuss any concerns with your Specialist
Cardiac Liaison Nurse
You will receive a letter with a date for your admission and an invitation to attend the pre
admission clinic.
This pathway tells you more about what happens when your child has a cardiac catheter. Your team may first discuss this with you in your local clinic, but you will need to come to the East Midlands Congenital Heart Centre itself for this specialist procedure .
Your Surgical Pathway Your Inpatient pathway Your Outpatient Pathway
Before you are discharged you will be given aftercare advice
and a follow up plan
Depending on the complexity / outcome of the
procedure you may be able to go home on the same day but
sometime you may have to stay overnight
Your child will undergo their cardiac catheter in our
specialised laboratory and will return to the ward with a
nurse once finished
On the day before procedure you will be welcomed on Ward 30 , our dedicated children’s cardiac ward
You will always receive an invitation for follow up in an outpatient clinic, but if the team feel it is necessary you may follow one or more of the following pathways
Patient Information
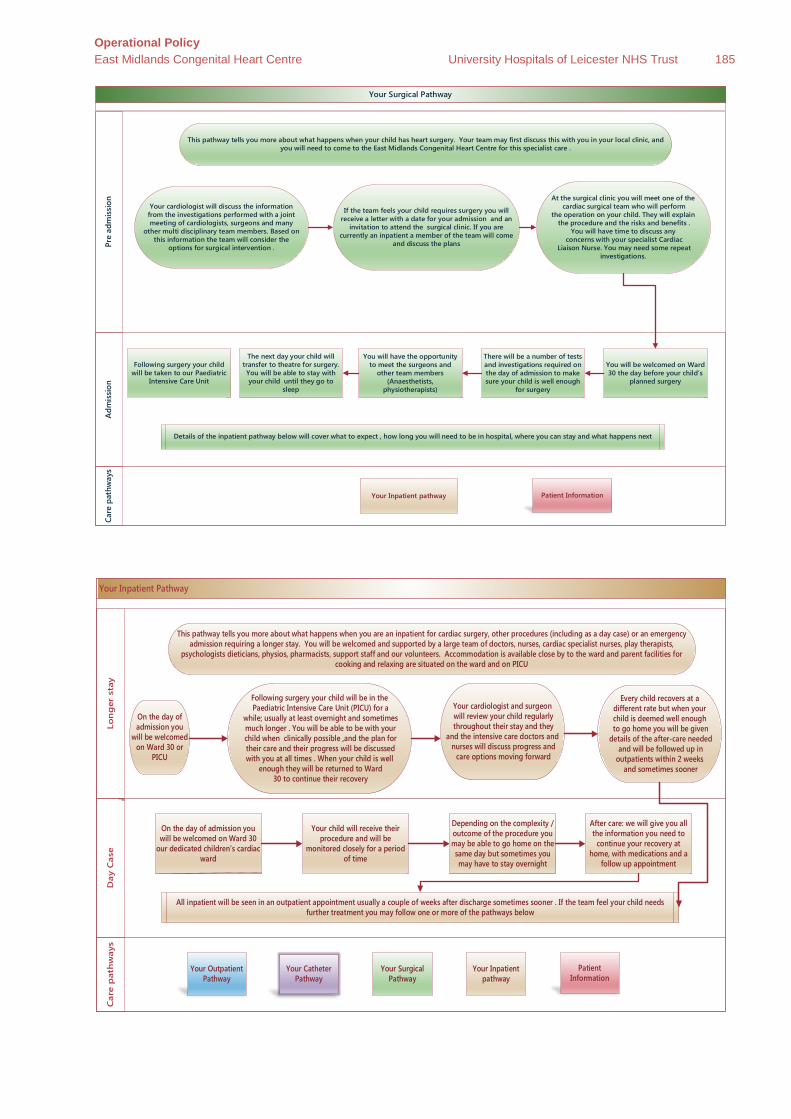
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 185
Your Surgical Pathway A
dmis
sion
Pr
e ad
mis
sion
Ca
re p
athw
ays
Your cardiologist will discuss the information from the investigations performed with a joint meeting of cardiologists, surgeons and many
other multi disciplinary team members. Based on this information the team will consider the
options for surgical intervention .
At the surgical clinic you will meet one of the cardiac surgical team who will perform
the operation on your child. They will explain the procedure and the risks and benefits .
You will have time to discuss any concerns with your specialist Cardiac
Liaison Nurse. You may need some repeat investigations.
If the team feels your child requires surgery you will receive a letter with a date for your admission and an
invitation to attend the surgical clinic. If you are currently an inpatient a member of the team will come
and discuss the plans
This pathway tells you more about what happens when your child has heart surgery. Your team may first discuss this with you in your local clinic, and you will need to come to the East Midlands Congenital Heart Centre for this specialist care .
Your Inpatient pathway
Following surgery your child will be taken to our Paediatric
Intensive Care Unit
The next day your child will transfer to theatre for surgery. You will be able to stay with your child until they go to
sleep
There will be a number of tests and investigations required on the day of admission to make sure your child is well enough
for surgery
You will be welcomed on Ward 30 the day before your child’s
planned surgery
Details of the inpatient pathway below will cover what to expect , how long you will need to be in hospital, where you can stay and what happens next
Patient Information
You will have the opportunity to meet the surgeons and
other team members (Anaesthetists,
physiotherapists)
Your Inpatient Pathway
Day
Cas
e Lo
ng
er s
tay
Car
e p
ath
way
s
Every child recovers at a different rate but when your child is deemed well enough
to go home you will be given details of the after-care needed
and will be followed up in outpatients within 2 weeks
and sometimes sooner
Following surgery your child will be in the Paediatric Intensive Care Unit (PICU) for a
while; usually at least overnight and sometimes much longer . You will be able to be with your child when clinically possible ,and the plan for their care and their progress will be discussed with you at all times . When your child is well
enough they will be returned to Ward 30 to continue their recovery
Your cardiologist and surgeon will review your child regularly throughout their stay and they
and the intensive care doctors and nurses will discuss progress and
care options moving forward
This pathway tells you more about what happens when you are an inpatient for cardiac surgery, other procedures (including as a day case) or an emergency admission requiring a longer stay. You will be welcomed and supported by a large team of doctors, nurses, cardiac specialist nurses, play therapists,
psychologists dieticians, physios, pharmacists, support staff and our volunteers. Accommodation is available close by to the ward and parent facilities for cooking and relaxing are situated on the ward and on PICU
Your Surgical Pathway
Your Inpatient pathway
Your Outpatient Pathway
After care: we will give you all the information you need to
continue your recovery at home, with medications and a
follow up appointment
Depending on the complexity / outcome of the procedure you may be able to go home on the same day but sometimes you may have to stay overnight
Your child will receive their procedure and will be
monitored closely for a period of time
On the day of admission you will be welcomed on Ward 30
our dedicated children’s cardiac ward
All inpatient will be seen in an outpatient appointment usually a couple of weeks after discharge sometimes sooner . If the team feel your child needs further treatment you may follow one or more of the pathways below
Your Catheter Pathway
Patient Information
On the day of admission you
will be welcomed on Ward 30 or
PICU
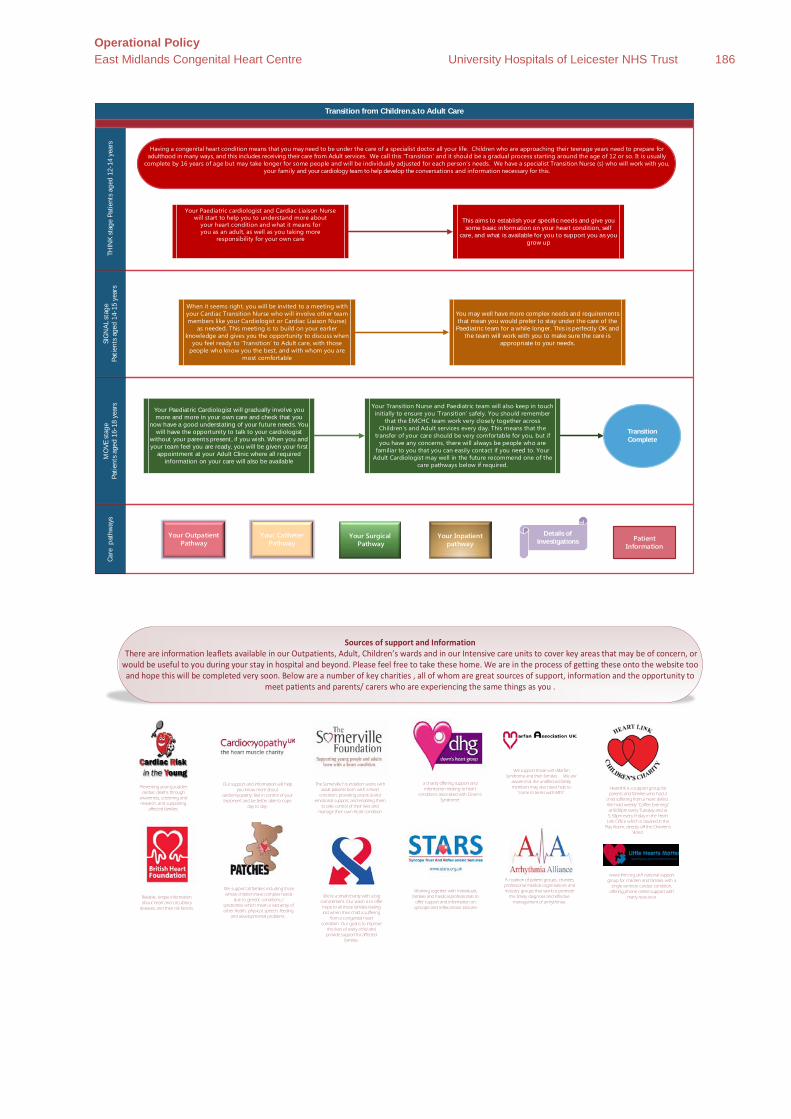
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 186
Transition from Children…s to Adult Care SI
GN
AL s
tage
Patie
nts
aged
14-
15 y
ears
THIN
K st
age
Patie
nts
aged
12-
14 y
ears
MO
VE s
tage
Patie
nts
aged
16-
18 y
ears
Care
pat
hway
s
Having a congenital heart condition means that you may need to be under the care of a specialist doctor all your li Children who are approaching their teenage years need to prepare for adulthood in many ways, and this includes receiving their care from Adult services. We call this ‘Transition’ and it should be a gradual process starting around the age of 12 or so. It is usually
complete by 16 years of age but may take longer for some people and will be individually adjusted for each person’s needs. We have a specialist Transition Nurse (s) who ill work with you, your family and your cardiology team to help develop the conversations and information necessary for this.
Your Paediatric cardiologist and Cardiac Liaison Nurse will start to help you to understand more about
your heart condition and what it means for you as an adult, as well as you taking more
responsibility for your own care
This aims to establish your specific needs and give you some basic information on your heart condition, self
care, and what is available for you to support you as you grow up
When it seems right, you will be invited to a meeting with your Cardiac Transition Nurse who will involve other team members like your Cardiologist or Cardiac Liaison Nurse)
as needed. This meeting is to build on your earlier knowledge and gives you the opportunity to discuss when
you feel ready to ‘Transition’ to Adult care, with those people who know you the best, and with whom you are
most comfortable
You may well have more complex needs and requirements that mean you would prefer to stay under the care of the
Paediatric team for a while longer. This is perfectly OK and the team will work with you to make sure the care is
appropriate to your needs.
Your Paediat ric Cardiologist will gradually involve you more and more in your own care and check that you
now have a good understating of your future needs. You will have the opportunity to talk to your cardiologist
without your parents present, if you wish. When you and your team feel you are ready, you will be given your first
appointment at your Adult Clinic where all required information on your care will also be available
Your Transition Nurse and Paediatric team will also keep in touch initially to ensure you ‘Transition’ safely. You should remember
that the EMCHC team work very closely together across Children’s and Adult services every day. This means that the
transfer of your care should be very comfortable for you, but if you have any concerns, there will always be people who are
familiar to you that you can easily contact if you need to. Your Adult Cardiologist may well in the future recommend one of the
care pathways below if required.
Your Surgical Pathway
Your Inpatient pathway
Your Outpatient Pathway
Your Catheter Pathway
Patient Information
Details of Investigations
Transition Complete
Sources of support and Information There are information leaflets available in our Outpatients, Adult, Children’s wards and in our Intensive care units to cover key areas that may be of concern, or would be useful to you during your stay in hospital and beyond. Please feel free to take these home. We are in the process of getting these onto the website too and hope this will be completed very soon. Below are a number of key charities , all of whom are great sources of support, information and the opportunity to
meet patients and parents/ carers who are experiencing the same things as you .
Our support and information will help you know more about
cardiomyopathy, feel in control of your treatment and be better able to cope
day to day.
Reliable, simple information about heart and circulatory
diseases, and their risk factors.
a charity offering support and information relating to heart
conditions associated with Down's Syndrome.
We support those with Marfan Syndrome and their families…….We are
aware that the unaffected family members may also need help to
“come to terms with MFS”.Preventing young sudden
cardiac deaths through awareness, screening and research, and supporting
affected families.
We support all families including those whose children have complex needs
due to genetic conditions / syndromes which mean a vast array of other health, physical, speech, feeding
and developmental problems .
A coalition of patient groups, charities, professional medical organisations and industry groups that work to promote
the timely diagnosis and effective management of arrhythmias.
The Somerville Foundation works with adult patients born with a heart
condition, providing practical and emotional support, and enabling them
to take control of their lives and manage their own heart condition
Working together with individuals, families and medical professionals to
offer support and information on syncope and reflex anoxic seizures
www.lhm.org.ukA national support group for children and families with a
single ventricle cardiac condition, offering phone online support with
many resources
Heartlink is a support group for parents and families who had a
child suffering from a heart defect.. We hold weekly "Coffee Evenings" at 8.00pm every Tuesday and at 5.30pm every Friday in the Heart Link Office which is situated in the
Play Room, directly off the Children's Ward.
We’re a small charity with a big commitment. Our vision is to offer hope to all those families feeling lost when their child is suffering
from a congenital heart condition. Our goal is to improve
the lives of every child and provide support for affected
families.
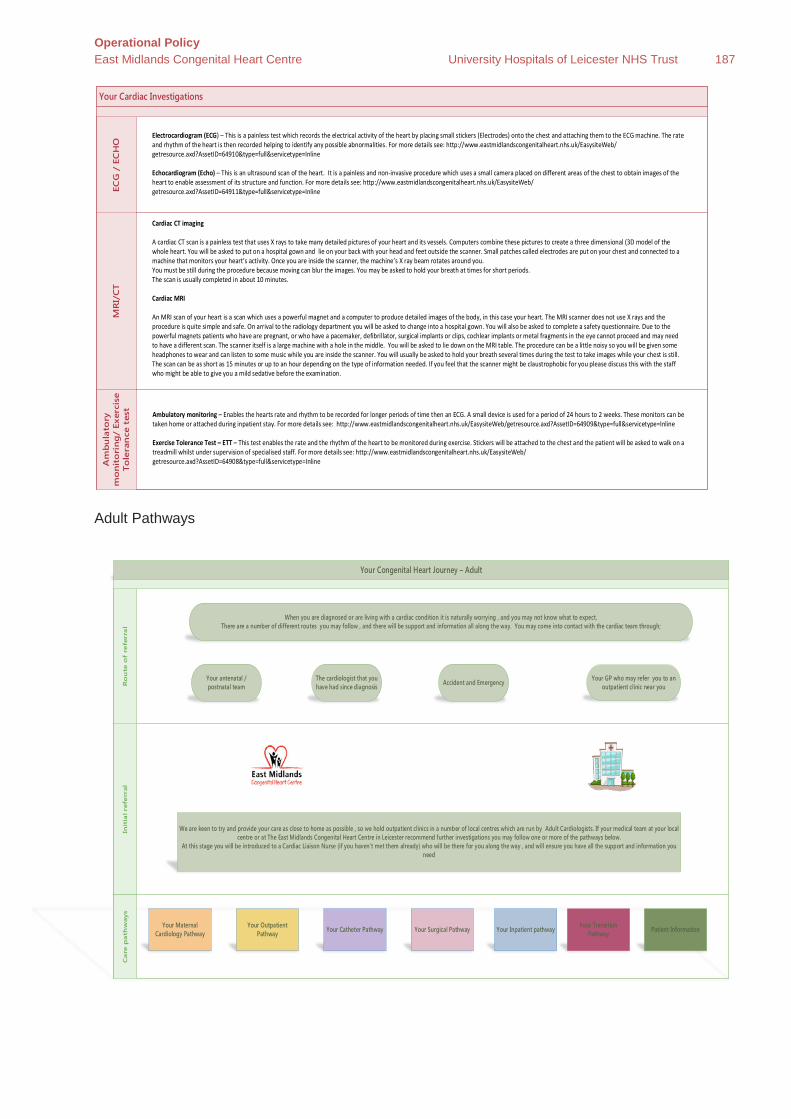
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 187
Adult Pathways
Your Cardiac Investigations
MR
I/C
TEC
G /
EC
HO
Am
bu
lato
ry
mo
nit
ori
ng
/ Ex
erci
se
Tole
ran
ce t
est
Electrocardiogram (ECG) – This is a painless test which records the electrical activity of the heart by placing small stickers (Electrodes) onto the chest and attaching them to the ECG machine. The rate and rhythm of the heart is then recorded helping to identify any possible abnormalities. For more details see: http://www.eastmidlandscongenitalheart.nhs.uk/EasysiteWeb/getresource.axd?AssetID=64910&type=full&servicetype=Inline
Echocardiogram (Echo) – This is an ultrasound scan of the heart. It is a painless and non-invasive procedure which uses a small camera placed on different areas of the chest to obtain images of the heart to enable assessment of its structure and function. For more details see: http://www.eastmidlandscongenitalheart.nhs.uk/EasysiteWeb/getresource.axd?AssetID=64911&type=full&servicetype=Inline
Ambulatory monitoring – Enables the hearts rate and rhythm to be recorded for longer periods of time then an ECG. A small device is used for a period of 24 hours to 2 weeks. These monitors can be taken home or attached during inpatient stay. For more details see: http://www.eastmidlandscongenitalheart.nhs.uk/EasysiteWeb/getresource.axd?AssetID=64909&type=full&servicetype=Inline
Exercise Tolerance Test – ETT – This test enables the rate and the rhythm of the heart to be monitored during exercise. Stickers will be attached to the chest and the patient will be asked to walk on a treadmill whilst under supervision of specialised staff. For more details see: http://www.eastmidlandscongenitalheart.nhs.uk/EasysiteWeb/getresource.axd?AssetID=64908&type=full&servicetype=Inline
Cardiac CT imaging
A cardiac CT scan is a painless test that uses X rays to take many detailed pictures of your heart and its vessels. Computers combine these pictures to create a three dimensional (3D model of the whole heart. You will be asked to put on a hospital gown and lie on your back with your head and feet outside the scanner. Small patches called electrodes are put on your chest and connected to a machine that monitors your heart’s activity. Once you are inside the scanner, the machine’s X ray beam rotates around you.You must be still during the procedure because moving can blur the images. You may be asked to hold your breath at times for short periods.The scan is usually completed in about 10 minutes.
Cardiac MRI
An MRI scan of your heart is a scan which uses a powerful magnet and a computer to produce detailed images of the body, in this case your heart. The MRI scanner does not use X rays and the procedure is quite simple and safe. On arrival to the radiology department you will be asked to change into a hospital gown. You will also be asked to complete a safety questionnaire. Due to the powerful magnets patients who have are pregnant, or who have a pacemaker, defibrillator, surgical implants or clips, cochlear implants or metal fragments in the eye cannot proceed and may need to have a different scan. The scanner itself is a large machine with a hole in the middle. You will be asked to lie down on the MRI table. The procedure can be a little noisy so you will be given some headphones to wear and can listen to some music while you are inside the scanner. You will usually be asked to hold your breath several times during the test to take images while your chest is still. The scan can be as short as 15 minutes or up to an hour depending on the type of information needed. If you feel that the scanner might be claustrophobic for you please discuss this with the staff who might be able to give you a mild sedative before the examination.
Your Congenital Heart Journey – Adult
Init
ial re
ferr
al
Ro
ute
of
refe
rral
Care
path
ways
Your antenatal / postnatal team
Your GP who may refer you to an outpatient clinic near you
Your Catheter Pathway
We are keen to try and provide your care as close to home as possible , so we hold outpatient clinics in a number of local centres which are run by Adult Cardiologists. If your medical team at your local centre or at The East Midlands Congenital Heart Centre in Leicester recommend further investigations you may follow one or more of the pathways below.
At this stage you will be introduced to a Cardiac Liaison Nurse (if you haven't met them already) who will be there for you along the way , and will ensure you have all the support and information you need
Accident and Emergency
When you are diagnosed or are living with a cardiac condition it is naturally worrying , and you may not know what to expect. There are a number of different routes you may follow , and there will be support and information all along the way. You may come into contact with the cardiac team through;
Your Surgical Pathway Your Inpatient pathway Your Outpatient Pathway
Your Maternal Cardiology Pathway
The cardiologist that you have had since diagnosis
Patient Information Your Transition Pathway
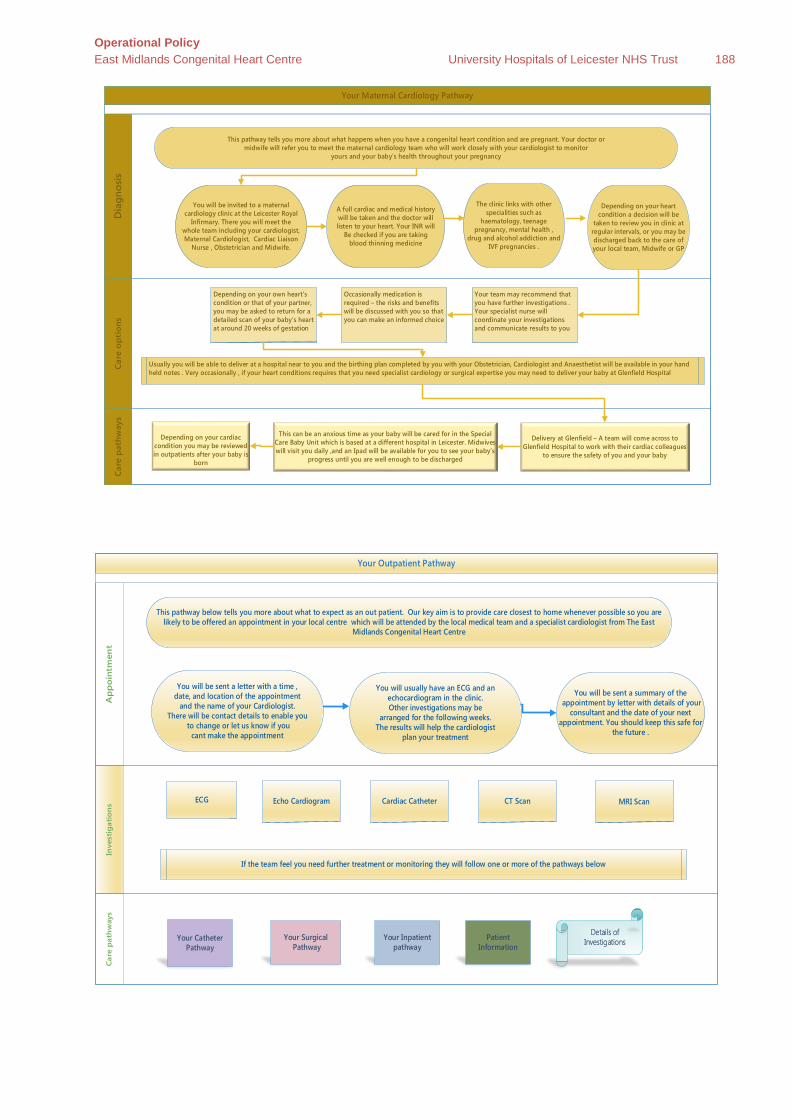
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 188
Your Maternal Cardiology Pathway
Car
e o
pti
ons
D
iagn
osis
C
are
pat
hway
s
You will be invited to a maternal cardiology clinic at the Leicester Royal
Infirmary. There you will meet the whole team including your cardiologist, Maternal Cardiologist, Cardiac Liaison
Nurse , Obstetrician and Midwife.
The clinic links with other specialities such as
haematology, teenage pregnancy, mental health ,
drug and alcohol addiction and IVF pregnancies .
A full cardiac and medical history will be taken and the doctor will listen to your heart. Your INR will
Be checked if you are taking blood thinning medicine
This pathway tells you more about what happens when you have a congenital heart condition and are pregnant. Your doctor or midwife will refer you to meet the maternal cardiology team who will work closely with your cardiologist to monitor
yours and your baby’s health throughout your pregnancy
Delivery at Glenfield – A team will come across to Glenfield Hospital to work with their cardiac colleagues
to ensure the safety of you and your baby
Depending on your cardiac
condition you may be reviewed in outpatients after your baby is
born
Depending on your own heart’s condition or that of your partner, you may be asked to return for a detailed scan of your baby’s heart at around 20 weeks of gestation
Occasionally medication is required – the risks and benefits will be discussed with you so that you can make an informed choice
Your team may recommend that you have further investigations . Your specialist nurse will coordinate your investigations and communicate results to you
Usually you will be able to deliver at a hospital near to you and the birthing plan completed by you with your Obstetrician, Cardiologist and Anaesthetist will be available in your hand held notes . Very occasionally , if your heart conditions requires that you need specialist cardiology or surgical expertise you may need to deliver your baby at Glenfield Hospital
Depending on your heart condition a decision will be
taken to review you in clinic at regular intervals, or you may be discharged back to the care of your local team, Midwife or GP
This can be an anxious time as your baby will be cared for in the Special Care Baby Unit which is based at a different hospital in Leicester. Midwives will visit you daily ,and an Ipad will be available for you to see your baby’s
progress until you are well enough to be discharged
Your Outpatient Pathway
Inve
stig
atio
ns
A
pp
oin
tmen
t
Car
e p
ath
way
s
You will usually have an ECG and an echocardiogram in the clinic. Other investigations may be
arranged for the following weeks. The results will help the cardiologist
plan your treatment
You will be sent a letter with a time , date, and location of the appointment
and the name of your Cardiologist. There will be contact details to enable you
to change or let us know if you cant make the appointment
This pathway below tells you more about what to expect as an out patient. Our key aim is to provide care closest to home whenever possible so you are likely to be offered an appointment in your local centre which will be attended by the local medical team and a specialist cardiologist from The East
Midlands Congenital Heart Centre
Your Surgical Pathway
Your Inpatient pathway
ECG Echo Cardiogram Cardiac Catheter CT Scan
If the team feel you need further treatment or monitoring they will follow one or more of the pathways below
Your Catheter Pathway
You will be sent a summary of the appointment by letter with details of your
consultant and the date of your next appointment. You should keep this safe for
the future .
MRI Scan
Details of Investigations Patient
Information

Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 189
Your Catheter Pathway A
dm
issi
on
Pre
ad
mis
sio
n
Car
e p
athw
ays
When you meet your Cardiologist they may suggest that
you undergo a cardiac catheterisation . They will explain the reasons for the procedure and
the risks and benefits
At the pre admission clinic appointment you will have bloods taken and swabs for MRSA , receive
any necessary medication and information
You will receive a letter with a date for your admission and an invitation to attend the pre
admission clinic.
This pathway tells you more about what happens when you have a cardiac catheter. Your team may first discuss this with you in your local clinic, and then refer you to the East Midlands Congenital Heart Centre for specialist care .
Your Surgical Pathway Your Inpatient pathway Your Outpatient Pathway
Before you are discharged you will be given aftercare advice and a follow up plan
Depending on the complexity / outcome of the procedure you may be able to go home on the same day but sometime you may have to stay overnight
You will receive your cardiac catheter in our specialised laboratory and will return to your admission ward with a nurse once finished
On the day of admission you will be welcomed on Ward 32 ,
You will always receive an invitation for follow up in an outpatient clinic, but if the team feel it is necessary you may follow one or more of the following pathways
Patient Information
Your Surgical Pathway
Ad
mis
sio
n P
re a
dm
issi
on
C
are
pat
hway
s
Your Cardiologist will discuss the information from the investigations performed with a joint meeting of Cardiologists, Surgeons and many
other multi-disciplinary team members. Based on this information the team will consider the
options for surgical intervention .
At the surgical clinic you will meet one of the cardiac team that will perform your
operation .They will explain the procedure and the risks and benefits .You will meet Cardiac Liaison Nurse and receive details
on how to contact them by email or telephone
If the team feels you require surgery you will receive a letter with a date for your admission and an invitation
to attend the surgical clinic . It is essential that you have an up to date dental check prior to admission to make
sure it is safe for you to have surgery.
This pathway tells you more about what happens when you have cardiac surgery. Your team may first discuss this with you in your local clinic, and then refer you to the East Midlands Congenital Heart Centre for specialist care .
Your Inpatient pathway
You will be seen by your Surgeon and Anaesthetist on the morning of your
surgery, who will be able to answer any questions you may have and obtain
consent
You will be admitted to our cardiac wards ( 31,33, 34, or 28) for longer stays or ward 32 for
day case
You will receive a letter inviting you to a pre admission clinic . At this appointment you will have bloods taken
and swabs for MRSA , receive any necessary medication and information
Details of the inpatient pathway below will cover what to expect , how long you will need to be in hospital, where you can stay and what happens next
Patient Information
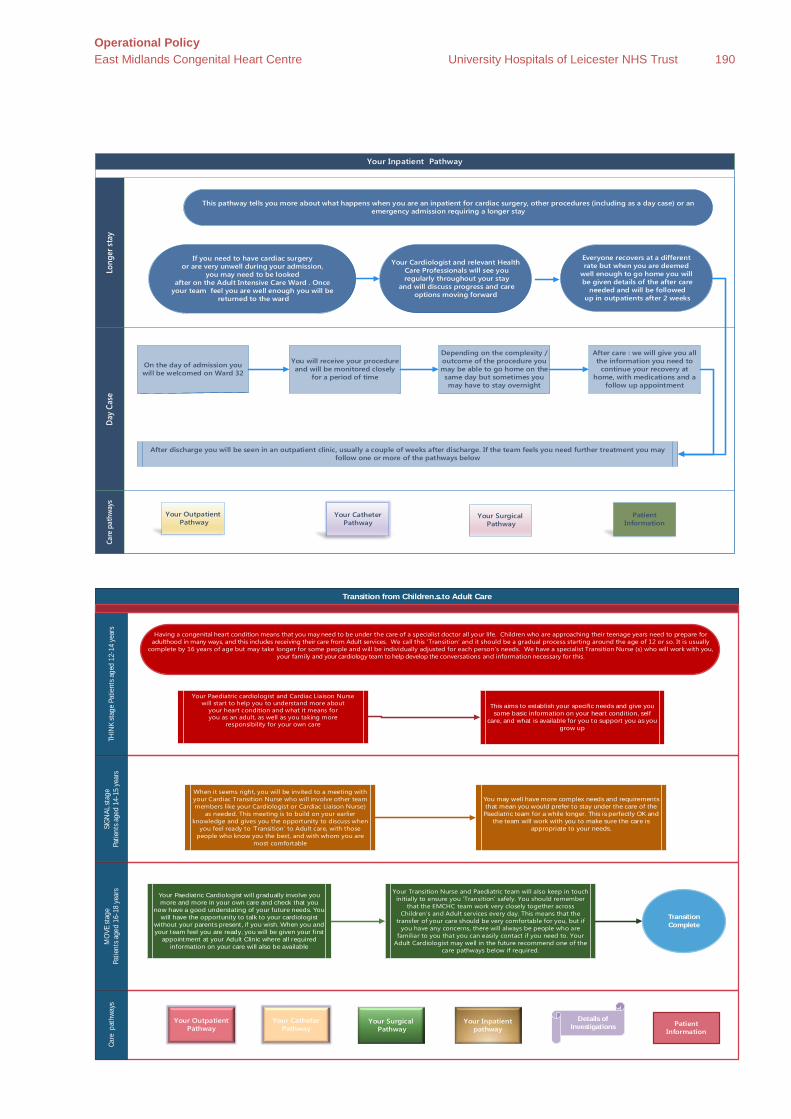
Operational Policy East Midlands Congenital Heart Centre University Hospitals of Leicester NHS Trust 190
Your Inpatient Pathway
Day
Cas
e Lo
nger
sta
y Ca
re p
athw
ays
Everyone recovers at a different rate but when you are deemed
well enough to go home you will be given details of the after care
needed and will be followed up in outpatients after 2 weeks
If you need to have cardiac surgery or are very unwell during your admission,
you may need to be looked after on the Adult Intensive Care Ward . Once
your team feel you are well enough you will be returned to the ward
Your Cardiologist and relevant Health Care Professionals will see you regularly throughout your stay
and will discuss progress and care options moving forward
This pathway tells you more about what happens when you are an inpatient for cardiac surgery, other procedures (including as a day case) or an emergency admission requiring a longer stay
Your Surgical Pathway
Your Outpatient Pathway
After care : we will give you all the information you need to
continue your recovery at home, with medications and a
follow up appointment
Depending on the complexity / outcome of the procedure you may be able to go home on the same day but sometimes you may have to stay overnight
You will receive your procedure and will be monitored closely
for a period of time
On the day of admission you will be welcomed on Ward 32
After discharge you will be seen in an outpatient clinic, usually a couple of weeks after discharge. If the team feels you need further treatment you may follow one or more of the pathways below
Your Catheter Pathway
Patient Information
Transition from Children…s to Adult Care
SIGN
AL st
age
Patie
nts a
ged
14-1
5 ye
ars
THIN
K st
age
Patie
nts a
ged
12-1
4 ye
ars
MO
VE st
age
Patie
nts a
ged
16-1
8 ye
ars
Care
pat
hway
s
Having a congenital heart condition means that you may need to be under the care of a specialist doctor all your li Children who are approaching their teenage years need to prepare for adulthood in many ways, and this includes receiving their care from Adult services. We call this ‘Transition’ and it should be a gradual process starting around the age of 12 or so. It is usually
complete by 16 years of age but may take longer for some people and will be individually adjusted for each person’s needs. We have a specialist Transition Nurse (s) who ill work with you, your family and your cardiology team to help develop the conversations and information necessary for this.
Your Paediatric cardiologist and Cardiac Liaison Nurse will start to help you to understand more about
your heart condition and what it means for you as an adult, as well as you taking more
responsibility for your own care
This aims to establish your specific needs and give you some basic information on your heart condition, self
care, and what is available for you to support you as you grow up
When it seems right, you will be invited to a meeting with your Cardiac Transition Nurse who will involve other team members like your Cardiologist or Cardiac Liaison Nurse)
as needed. This meeting is to build on your earlier knowledge and gives you the opportunity to discuss when
you feel ready to ‘Transition’ to Adult care, with those people who know you the best, and with whom you are
most comfortable
You may well have more complex needs and requirements that mean you would prefer to stay under the care of the
Paediatric team for a while longer. This is perfectly OK and the team will work with you to make sure the care is
appropriate to your needs.
Your Paediat ric Cardiologist will gradually involve you more and more in your own care and check that you
now have a good understating of your future needs. You will have the opportunity to talk to your cardiologist
without your parents present, if you wish. When you and your team feel you are ready, you will be given your first
appointment at your Adult Clinic where all required information on your care will also be available
Your Transition Nurse and Paediatric team will also keep in touch initially to ensure you ‘Transition’ safely. You should remember
that the EMCHC team work very closely together across Children’s and Adult services every day. This means that the
transfer of your care should be very comfortable for you, but if you have any concerns, there will always be people who are
familiar to you that you can easily contact if you need to. Your Adult Cardiologist may well in the future recommend one of the
care pathways below if required.
Your Surgical Pathway
Your Inpatient pathway
Your Outpatient Pathway
Your Catheter Pathway
Patient Information
Details of Investigations
Transition Complete