Embed Size (px)
Citation preview

Int. J. Rodiation Oncology Biol. Phys., 1977, Vol. 2, pp. 537-548. Pergamon Press. Printed in tk U.S.A.
??Brief Communication
ONCE A WEEK TREATMENTS
FRANK ELLIS, M.D. and ALFRED L. GOLDSON, M.D. Memorial Sloan Kettering Cancer Center, Department of Radiotherapy, 1275 York
Avenue NY 10021, U.S.A.
In 35 cancer patients who were treated from 1974 through June lW6, once a week treatments (e.g. 7 thnes 615 rad = 4305 rad = 1800 ret) were tolerated as wel1 snd seemed to produce at least as good results as treatments with 4-5 fractions per week. One treatment per week has obvious practical advantages for the non-hospitaiized patient and for a busy department.
Once a week fractionation, Single high dose radiation fractionation, NSD: correlations with single high dose fractionation, Tumor response to non-conventionai fractionation.
INTRODUCTION
Many fractionation schedules have been employed in teletherapy. The early German practice was to give the whole dose at one time. The French school under Regaud’ es- tablished by careful clinical observation, that better results were obtained by fractionating the total dose in many treatments over se- veral weeks. With treatments “never on Sunday ,” this led to 6 treatments per week. With introduction of long weekends, 5 treatments per week became the standard schedule. A 4 treatment per week schedule resulted when Wednesday was kept free; this has become the first choice of some depart- ments for outpatients. Many radiotherapists also have used 3 treatments per week and 2 treatments per week. At the other end of the spectrum, “superfractionation” with 2 and more fractions per day as wel1 as continuous teletherapy radiation also is being tried. By decreasing or increasing the size of each fraction, further modifications are possible.
Recent conferences devoted to the ques- tion of optimal fractionation were held in Kyoto, Japan, 1972 (The Size of Individual
Dose Fractions in Radiobiology and Radio- therapy),” and at the University of Wiscon- sin, 1975 (Time-Dose Relationship in Clini- cal Radiotherapy).’ The detailed conference reports on these meetings vividly demon- strate the uncertainties and the wide diff- erences in clinical practice and in radiobiolo- gical theory.
Despite the great interest in fractionation, one treatment per week has not been tried systematically. One treatment per week is one of the most convenient schedules for most patients who do not have to be hos- pitalized or who live at a distance. A weekly visit to the radiotherapy department usually can be arranged without upsetting his life and work schedule. If the patient needs assistance or transportation, it usually is easy to find a friend, relative or agency, who can bring the patient once a week.
Obviously, 1 treatment per week can be recommended only if it produces ap- proximately the same results as the com- monly used multiple treatments per week. In this paper we report a smal1 series of 35 patients, treated with 1 treatment per week,
Reprint requests to: Dr. Frank Ellis, Cancer Newark, NJ 07107, U.S.A. Institute of New Jersey, 145 Roseville Avenue,
531

Tabl
e 1.
Res
ults
in
al1
pat
ient
s tre
ated
on
ce
wee
kly
at t
he
Mem
oria
l C
ente
r, N
Y,
1974
-76
Age
, ra
ce
Frac
tions
Ti
me
P at
ient
an
d se
x H
isto
logy
Lo
catio
nlsi
ze
Res
pons
e ra
d/fr
act.
days
R
et
1 Sq
uam
ous
Ca.
Lu
ng,
Med
./lO
4S
+ 7
x 61
5 58
18
00
2 65
WM
Sq
uam
ous
Ca.
C
hest
W
aI1/
18+
+ 5x
355
59
1679
3
71W
F Sq
uam
ous
Ca.
A
nt.
Nec
k/lS
x
10cm
’ +
+ +
+ N
ED*
8x70
0 50
22
00
4 77
WF
Squa
mou
s C
a.
Low
er
Leg/
124
++
+ 7x
600
42
1740
5
83W
F Sq
uam
ous
Ca.
A
nus/
12
x 6
cm*
++
7x61
5 79
18
00
6 68
WM
Sq
uam
ous
Ca.
Lu
ng,
Med
./6
cm4
+++
12x4
00
46
1770
7
82W
M
Squa
mou
s C
a.
Buc
cal
Muc
osal
ó cm
4 ++
+ 1x
850
42
1517
4x
655
8 62
WM
Sq
uam
ous
Ca.
Le
ft m
alar
++
++
regi
on
nose
/2
cm4
NED
6X
600
50
1500
9
83W
F Sq
uam
ous
Ca.
Le
ft an
d R
ight
++
7
x 63
0 45
18
53
ingu
inal
s an
d vu
lva
10
63W
M
Squa
mou
s C
a.
Face
an
d ne
ck
++++
NED
7x
650
57
1900
11
63
WM
Sq
uam
ous
Ca.
Le
ft ne
ck/ll
x
10 cm
* +
10 x
575
52
21
90
12
62W
F B
asal
C
el1
Ca.
Lt
. si
de
face
++
++
8x60
0 51
19
72
15x8
cm2
NED
13
65
WF
Bas
al
Cel
1 C
a.
Nos
e/7
x 6
cm2
++++
NED
7
x 61
5 64
18
00
14
79W
M
Bas
al
Cel
1 C
a.
Rig
ht
nose
/3
cm4
++++
NED
5
x 69
0 29
18
00
15
30W
M
Mel
anom
a Lt
. ne
ck
mas
s/7
cm4
++++
6x
600
59
1746
2x
300
16
62W
M
Mel
anom
a Lt
. an
t. ch
est/5
cm
+ ++
+ 7
x 55
0 40
15
00
17
27W
M
Mel
anom
a Ili
ac
foss
a/8
cm4
+ 9x
500
64
1700
18
55
WF
Mel
anom
a R
t. le
g/75
cm
+
3 x
624
73
780
6X60
0 15
00
then
12
0 ra
d 3x
lday
15
84
x 10
day
s 19
75
WF
Mel
anom
a Sk
in
rt.
neck
/l2cm
+ 0
8x61
5 60
20
57
20
66W
F M
elan
oma
Left
foot
/7
cm+
on
1/4
2 x
650
14
563
com
plet
e
21
54W
M
22
51W
M
Ade
noca
rcin
oma
Rt.
mai
n st
em
colo
n br
onch
us
met
s ++
6X
610
36
1696
fr
om
colo
n 1x
500
Ade
noca
rcin
oma
Pros
tate
++
+ 6
x 57
0 36
15
00

23
59W
F
24
70W
F
25
27W
F 26
59
WF
Ade
noca
rcin
oma
Lt.
supr
acla
vicu
lar
+++
4x61
5 22
12
50
brea
st
1”
Ade
noca
rcin
oma
Lt.
fron
tal
subc
t. pa
rieta
l sk
ull
met
s+
+ +
5 x
680
30
1600
fr
om
brea
st
1”
bone
m
ets
+ A
deno
carc
inom
a Lt
. ne
ck
paro
tid
+ 3
x 56
5 15
67
5 A
deno
carc
inom
a Lt
. an
t. ch
est
brea
st
1”
++
17 x
300
54
15
90
2xlw
k
27
20W
M
28
23W
F 29
44
WF
30
63W
F
Sarc
oma
Sarc
oma
Sarc
oma
Sarc
oma
Lt.
ulna
m
ets
Rt.
knee
po
st
op
Rt.
butto
ck
Rt.
hum
erus
+++
7 x
650
44
1900
++
++N
ED
8x56
5 57
18
00
++++
NED
6
x 62
0 42
15
65
+ 4x
585
22
900
31
20W
F
32
66W
M
33
52B
F
34
50W
M
35
81W
F
Schw
anno
ma
Schw
anno
ma
Schw
anno
ma
Schw
anno
ma
Schw
anno
ma
Lt.
side
of
he
ad/l5
cm
d R
t. he
mi-a
bdom
en/
30 X
17
cm2
Rt.
dosu
m
foot
//6
cm&
R
t &
Lt
neck
/l5
cm4
Lt.
sacr
um
and
hip
+++
7x50
5 43
17
00
+++
7 x
565
82
1450
++++
7
x 58
5 78
16
32
+ 2x
596
51
1470
4x
615
++
6x50
8 50
13
84
1 x
600
tNo
evid
ente
of
dis
ease
. $4
= g
reat
est
diam
eter
of
mea
sura
ble
tum
or.
Nut
e.
Crit
eria
fo
r tu
mor
re
spon
se
are
liste
d in
Tab
le
3.

540 Radiation Oncology 0 Biology 0 Physics May-June 1977, Volume 2, No. 5 and No. 6
who seem to have done surprisingly well. We also wil1 present theoretical considerations, which raise the possibility that some tumors might respond better to once a week treat- ments than to more conventional schedules
METHODS AND MATERIALS Ma terials
Our first patients treated with a once weekly schedule were patients of the senior author while he was at Oxford University in England and at the Milwaukee County Me- dical Complex and the Medical College of Wisconsin, in Milwaukee. These patients had favourable, easily observable skin lesions, and the good long term results without undue damage to normal tissues inspired the present study.
In 1974 we began a study of once a week treatments at the Memorial Center for Cancer in New York City. Until June 1976, when both authors left the Memorial Center, 35 patients were entered. We have tried to ob- serve the tumor response and the normal tissue reactions in these patients as ac- curately and scientifically as possible. We are providing the details of these observations in as much detail as possible, to let other radio- therapists judge for themselves the potential of radiotherapy given in weekly fractions.
covering the affected skin with bolus material if high energy photons (“Co or linear ac- celerators) were used. For deep lesions, the dose distribution was properly planned and whenever possible, checked with ther- moluminescent dosimeters.
The total dose was guided by the data given in Table 2. They are based on the NSD formula D = NSD x T’.” x N”.24, where D is the total dose in rad, NSD the “tolerante dose in ret,” T the overall time of the treat- ment in days and N the number of frac- tions.2-8 The table gives the dose per fraction in rad for once weekly treatments for ?Zo and other supervoltage radiation for 5, 6, 7 and 8 fractions and for ret values of 1800, 1900 and 2000ret. For the commonly used dose of 1800 ret, for instance, 5 treatments of 700 rad = 3500 rad total, or 6 treatments of 680rad = 4800rad total, or 7 treatments of 615rad = 4305, or 8 treatments of 565rad = 4520 rad total would be required. In this series a dose of 1800ret was used in most cases. We realize that 1900ret or even 2000 ret may be desirable so as to approach a higher probability of cure.
Our criteria for response are based on measured regression of the treated lesion (Table 3). We distinguish four degrees of re-
The age, sex, histology and anatomical lo- cation of the tumors of our patients are detailed in Table 1. Many of our 35 patients were failures after surgery and chemotherapy and most had far advanced cancer.
Table 3. Criteria for tumor response
Methods In al1 patients the treatment plan was to
give a uniform dose to the tumor volume. In lesions involving the skin, electron beams were used or build up was achieved by
% of Regression of tumor original diameter
+ 75 ++ 50
+++ 25 ++++ 0
NED NO evidente of disease
Table 2. Rad per fraction for once weekly treatment for 1800, 1900 and 2000ret for “Co and supervoltage radiation
Equivalent Number of fractions dose TDF-ì 5 6 7 8
1800 ret 102 700 rad 680 rad 615 rad 565 rad 1900 ret 108 800 rad 710 rad 640 rad 595 rad 2000 ret 112 81.5 rad 720rad 655 rad 600rad
tTDF = Time, Dose, Fractionation.

Once a week treatments 0 F. ELLIS and A. L. GOLDSON 541
sponse; namely +, ++, +++ and ++++, which denote at least 75%, 50%, 25% and 0% of original tumor diameter. These decreases in diameter correspond to 40%, 12%, 1.5% and 0% of the o’riginal tumor volume. To be scored the regression must have persisted at least 3 months or until death. When the treated tumor had disappeared entirely and no metastases were present at follow up, NED (NO Evidente of Disease) was added to response.
In two cases of extensive skin lesions, supplementary therapy was given by split
skin grafts. Large ulcerated lesions, although they might eventually heal by themselves, are managed more speedily with a skin graft. It should be applied soon after the radiation treatment, while the blood supply is stil1 intact. Chemotherapy was not used during the treatment of these patients.
RJISULTS
As illustrative cases, two patients with basal cel1 carcinoma, one patient with a metastatic malignant melanoma and one pa-
(4 (bl
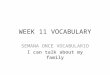
(4 Fig. 1. Response of basal cel1 carcinoma to once weekly treatments. (Patient 1) 8x 600 rad (1600 ret); (a) Before radiation; (b) Post radiation; (c) Skin graft post radiation; (d) 1
year post radiation and graft.

542 Radiation Oncology 0 Biology 0 Physics May-June 1977, Volume 2, No. 5 and No. 6
tient with malignant Schwannoma are dis- cussed.
Patient 1. C.L. This 62 year old female had noticed an increasing ulceration of the left side of her face for more than 10 years. In January, 1975 a biopsy revealed basal cel1 carcinoma. From 2 April 1975 to 22 May 1975 she received once weekly treatment with a total of 4800rad to the left side of her face. Betatron 8 MeV electrons were used in 8 fractions of 600 rad calculated at the 90% isodose leve1 through a lead mask. After radiation she received a skin graft to the left side of her face. In June 1976 there was no evidente of disease (Fig. 1).
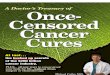
Patient 2. M.M. This 71 year old female presented on 3 May 1975 with a 9 year his- tory of a lesion involving both upper eyelids and both sides of the nose. Biopsy showed basal cel1 carcinoma. From 13 May 1975 to 15 July 1975 she received once weekly treatment with 6 fractions of 615 rad each for a total of 3840 rad. Betatron electrons of 8 MeV were used. On 16 August 1975 an (Ir) 192 re- movable implant was carried out to her forehead and check. On 18 September 1975
she received an additional one time treatment of 615 rad to her anterior right nasolabial fold and to her forehead. On examination on 10 November 1975 and on 5 February 1976 she had slight telangectasis, but no evidente of disease (Fig. 2).
Patient 3. F. W. This 56 year old female had a 7 year history of recurrent malignant melanoma of the left thigh. Initial treatment elsewhere in 1969 was wide surgical excision of the primary with in-continuity left groin dissection with skin graft. In April 1975 she presented with a recurrence in the same re- gion. Biopsy taken from the left thigh, on 10 April 1974 showed malignant melanoma present in dermis and fat. Chest X-ray re- vealed pulmonary metastases; for this she was started on Dacarbazine and Vincristine. She was seen again at Memorial Hospita1 on 16 October 1975 with a large 10 x 8 cm* mobile tumor of the left inner thigh and was started on once a week radiation therapy. From 16 Oc- tober 1975 to 6 January 1976, 4760rad was given in 7 fractions of 680rad by 8 MeV Betatron electrons. A repeat biopsy on 16 February 1976, 2 months post therapy of the
(4 (b) Fig. 2. Response of a basal cel1 carcinoma to once weekly treatments. (Patient 2) 6 x 615 rad plus 19*Ir implant and boost of 1 x 615 (1760 ret); (a) Before radiation; (b) 6 months post
radiation.

Once a week treatments 0 F. ELLIS and A. L. GOLDSON
Fig. 3. Response of a malignant melanoma to once weekly treatments. (Patient 3) 7 x 680 rad (1980ret); (a) Before radiation; (b) 4.5 months post radiation.
same area showed persistent malignant left neck and tempora1 region in 7 fractions of melanoma in fibrous tissue. However on 20 650rad per week for 1840ret. The patient April 1976,4.5 months post irradiation, biopsy died on 10 January 1975 at another hospita1 showed only fibrous connective tissue with with intracranial extension. The treated tu- abundant melanotic pigment but no melanoma mor had regressed significantly before death, cells. (Figs. 3, 4). as can be seen from the photographs. (Fig. 5.)
Patient 4. M.P. This 20 year old female had neurofibromatosis since childhood. She was admitted to the Memorial Center on 17 July 1974, with a rapidly enlarging 8 x 10 x 6 cm3 firm left neck mass and pain, which on biopsy proved to be a malignant Schwannoma. Ex- cision of the vascular lesion from the left side of the neck and elective tracheostomy were performed on 31 July 1974. From August 1974 to September 1974, she received che- motherapy. Then she was referred for emer- gency treatment to the radiotherapy depart- ment, because the tumor was growing rapidly. Significant regression of the tumor occurred after the first treatment. As of 11 October 1974, she had received a total dose of 4550 rad by wedge fields with wax bolus to
The majority of patients (97%) showed at least a 25% regression to once a week treat- ments. Only 1 melanoma patient showed no response. In 11 of 35 patients (31%) complete regression of the treated lesions occurred. The difficulties to compare these results to his- torical controls are, of course, too wel1 known to merit discussion here, and ob- viously one cannot draw far reaching con- clusions from this relatively smal1 number of patients. However, we would like to record that the response of this group of tumors to once weekly treatments seemed to be dis- tinctly better than we had anticipated on the basis of our experience with radiotherapy with multiple fractions per week. This sub- jective clinical judgement must be substan-

544 Radiation Oncology 0 Biology 0 Physics May-June 1977, Volume 2, No. 5 and No. 6
Fig. 4(a).

Once a week treatments 0 F. ELLIS and A. L. GOLDSON 545
Fig. 4(b).

546 Radiation Oncology 0 Biology 0 Physics May-June 1977, Volume 2, No. 5 and No. 6
Fig. 3);( pers
Fig. 4(c).
4. Histological response of a malignant melanoma to once weekly treatments. (Patient a) Original biopsy: melanoma present in dermis and fat; (b) Two months post radiation; ;istent melanoma in dense fibrous tissue; (c) 4.5 months post radiation: abundant fibrous
connective tissue with melanotic pigment but no malignant cells.

Once a week treatments 0 F. ELLIS and A. L. GOLDSON 547
(al (bl Fig. 5. Response of a malignant Schwannoma to once weekly treatments. (Patient 4)
7 X 650 rad (1840 ret); (a) Before radiation; (b) Two months post radition.
tiated in the future by large numbers of patients, by a greater variety of tumors and if possible by prospective clinical trial.
In the 35 patients treated at Memorial by this fractiohation schedule, the ret dose ran- ged from a low of 563 to 2190ret. Careful follow up of these 35 patients revealed mild and transient symptomatology, such as ery- thema, tanning, diarrhea and telangiectasia in approximately 50% of cases, but no severe morbidity or mortality attributable to radia- tion with 1800 ret was encountered. We admit that our follow up period is short, with maximum follow up period approaching only 2 years.
DISCUSSION Radiotherapy once a week clearly is a most
attractive time schedule, if it can be shown that the results are as good as those with multiple fractions per week. It permits the cancer patient who does not have to be hospitalized and who lives within commuting distance to go on without interrupting his life and work schedule and at the same time to get the medical care and supervision he needs for proper cancer management. Few cancer patients who are undergoing radiation therapy need a medical examination including blood counts more than once a week.
The advantages of once a week treatments
are so obvious in some situations, that this schedule has been used on occasion by a number of radiotherapists. For instance at Ohio State University Hospita1 Henschke treated 30 patients in the years 1952-55 with 500 rad per week for a total dose of 5000 rad. (Personal Communication oral, October 1976.) These were patients from outlying farms in Ohio, who could not come or could not be brought for radiotherapy more often. The response seemed to be essentially the same as with conventional fractionation. Aris- tizabal’ reported from Columbia, South America that with only one cobalt machine for 3 million people, treatments of 500 rad given once a week made it possible to treat many patients, who otherwise would have gone untreated. He also stated, that at the Puerto Rico Nuclear Center, 38 cases of ad- vanced carcinoma of the breast have been treated with once a week doses of 500 rad for a total of 5000 rad with satisfactory res- ponse.’
The most facinating implication of our data is the possibility, that at least for some tumors, once a week treatment may be better than multiple fractions per week. This pos- sibility rarely has been considered, but it is by no means a radiobiological impossibility. It has been suggested previously by Ellis that for cells with higher extrapolation num-

548 Radiation Oncology 0 Biology 0 Physics May-June lW7, Volume 2, No. 5 and No. 6
bers a smal1 number of large fractions may, for the same NSD, leave fewer survivors than wil1 the conventional 30 doses of 200rad. Moreover, it appeared that for cells with extrapolation numbers of 2, such as connective tissue a smal1 number of large fractions might have a smaller effect than the conventional30 x 200 rad. As has been shown by Ellis and Sorenson,2.3 the graphs of cel1 survival and ret are almost coincident if numbers of fractions are plotted against dose per fractions for D,, = 160 n = 2 or Do = 150 n = 2.2. In other words, a smal1 number of large dose fractions have in the NSD concept the same cell-killing effect on the normal connective tissue as conventional fractionation, but a greater cell-killing effect on cells with high extrapolation numbers, such as seem to be characteristic of resistant tumors. Conceptually it seems reasonable (if malignant cells are dividing slowly and die only as a result of radiation in subsequent mitoses), to allow time between fractions for proliferation of normal cells. Their growth may be aided by homoeostatic recovery processes and by improved oxygenation, which leave gaps in the tumor because of
gradual autolysis of the destroyed malignant cells.
In this connection, it also is interesting that recent skin erythema studies on patients by Turesson and Natter” showed that the radiation reactions of the normal skin were identical after 5 treatments per week with 235 rad each for a total of 3760rad in 16 treatments in 22 days (1400 ret) and after irradiation once a week with 675 rad for a total of 2700 rad in 4 treatments in 22 days (1400 ret).
Finally, we would like to reflect, that widely different time and dose schedules have shown in clinical practice only such smal1 differences in tumor control and normal tissue damage, that no schedule has emerged, which clearly is superior. If different sche- dules give essentially the same results, one should pick the one which is more convenient for the patient and which permits to take care of more patients in the areas of the world, which lack radiation therapists and supervol- tage machines. Once a week treatments thus could become a significant contribution to practica1 cancer management.
REFERENCES 1. Aristizabal, S.: Discussion remarks. In Proc. radiotherapy. Front. Rad. Ther., Vol. 3, ed. by
Conf. on the Time-dose Relationship in Clini- Vaeth, J.M. Karger, Basel, 1968, pp. 131-140. cal Radiotherapy, ed. by Caldwell W.L., Tol- 7. Ellis, F.: Fractionation in radiotherapy. In bert D.D. Middleton, Wisconsin, Madison Modem Trends in Radiotherapy, ed. by Printing & Publishing, 1975, p. 189. Seeley, T.J., Wood, C.A. London, Butter-
2. Ellis, F., Sorensen, A.: A method of estimating worths, 1967, Chap. 2, pp. 34-51. biological effect of combined intracavitary low 8. Ellis, F.: Tolerante dosage in radiotherapy dose rate radiation with external in carcinoma of with 200KV X-rays. Br. J. Radiol. 15: 348, the cervix uteri. Radiology 110-681, 1974. 1942.
3. Ellis, F.: Letter: The NSD concept and 9. Regaud, C.: Influence de la duree d’irradiation radioresistant tumors. Br. J. Radiol. 47 sur les effects determines dans le testicule par (564) p. 909, 1974. le radium. Compt. Rend Sec. de Biol. 86: 787-
4. Ellis, F.: Nomina1 standard dose and the ret. 790, 1922. Br. J. Radiol. 44: 101-108, 1971. 10. Sugahara, T., Revesz, L., Scott, 0. (eds):
5. Ellis, F.: The relationship of biological effect Fraction Size in Radiobiology, Tokyo, Igaku to dose-time fractionation factors in radio- Shoin, 1973, pp. 180-187. therapy. Current Topics in Radiation ll. Turesson I., Notter, G.: Control of dose ad- Research, Vol. 4, ed. by Ebert, M., Howard, J. ministered once a week and three times a day H. Amsterdam, North-Holland, 1968, Chap. 7, according to schedules calculated by the CRE pp. 359-397. formula, using skin reaction as a biological
6. Ellis, F.: Time, fractionation and dose rate in parameter. Radiology 120: 339404, 1976.