Embed Size (px)
Citation preview

Older Adults and Alcohol: Visioning a Service Delivery
Network
Elizabeth Dawes & Beth Murphy 2011 BASW HPPAE Fellows
University of Pittsburgh School of Social Work

This manual may be reproduced and used in part or fully provided authorship is credited appropriately, and it is not used for profit-making purposes. In May 2011, a downloadable copy of this guide will be available through the University of Pittsburgh School of Social Work website: http://www.socialwork.pitt.edu/research/hartford.php. To obtain information about the HPPAE project or the authors, please contact:
Elizabeth Mulvaney, HPPAE Coordinator University of Pittsburgh School of Social Work 2117 Cathedral of Learning Pittsburgh, PA 15260 412-624-0036 [email protected]
Publication Date: April 2011

i
Table of Contents Introduction ................................................................................................................................................. 1
Key Terms .................................................................................................................................................... 2
Background .................................................................................................................................................. 4
Population Statistics ............................................................................................................................... 4
National Prevalence Statistics on Alcohol Use .................................................................................. 4
Aging Trends in Allegheny County, Pennsylvania and the United States ...................................... 6
Services Present in Allegheny County ................................................................................................. 7
Medicare and Medicaid Coverage ........................................................................................................ 8
Health Impact of Alcohol ..................................................................................................................... 9
Impact on Caregivers’ Mental and Physical Health ......................................................................... 10
Alcohol and Prescription Drug Use .................................................................................................. 10
Alcoholism and Mental Illness ........................................................................................................... 11
Building an Ideal Service Delivery Network ......................................................................................... 12
System Integration ................................................................................................................................ 12
Prevention and Education Models..................................................................................................... 13
Treatment Principles ............................................................................................................................ 14
Vision for Allegheny and Surrounding Counties ................................................................................. 16
Potential System Integration Ideas..................................................................................................... 16
Potential Utilization of Prevention and Education Ideas ............................................................... 16
Treatment Principles & Ideas ............................................................................................................. 17
Appendix A ................................................................................................................................................ 18
References .................................................................................................................................................. 19
You may click on any of the section headings above to navigate to that part of the document.

ii
Acknowledgements
We owe a great many thanks to our Hartford Partnership Program for Aging Education
(HPPAE) instructors Rafael Engel, Patricia Kolar, and Elizabeth Mulvaney for their help and
guidance. Additionally, we would like to thank our field instructors Jean Kablack and Roxann
Tyger, as well as the Allegheny County Area Agency on Aging (ACAAA) and Ursuline Senior
Services (USS) for their encouragement. Thank you to the faculty of The University of
Pittsburgh’s School of Social Work, especially Keith Caldwell, Gayle Mallinger, Helen Petracchi
and Daniel Rosen, for their assistance and feedback on our project. We would also like to thank
our family and friends for their unconditional love and support.

1
Introduction
Mrs. Jones is 73 year old woman living alone in her home of 45 years. Her husband
died about eighteen months ago. Prior to his death, he had been the primary person driving and
managing the household finances. Her utility company noticed an erratic payment pattern over
the past nine months and contacted a community agency with an energy assistance program
requesting that it check on this senior citizen. A case manger visited her and discovered that she
was struggling in several areas—financially, emotionally, and physically. She had an auto
accident in which no one was injured or ticketed. The car was not repaired and was sitting in
the driveway. She then relied upon others to drive her. She has also had three emergency room
visits in the past nine months—two for falls and a third for confusion. She indicated that she
was diagnosed with depression and started on antidepressants. During a routine screen for
alcohol use, the case manager discovered that Mrs. Jones had a regular use pattern of two drinks
most days while her husband was alive. They drank together in the evening or with friends.
Since his death, she has been drinking at least five drinks of vodka most days. She heard the
MD warn her not to take the antidepressant if she drank. Therefore, she only takes it on the
days she doesn’t drink. It probably has never reached therapeutic levels. When asked, she
stated that medical personnel have not asked about her drinking. She did not tell them. They
all thought her problems were related to her grief and other medical issues.
For an older adult, abusing alcohol may be a major issue that is overlooked leaving the
person with devastating health consequences, not to mention increased health care and living
costs. While in our field placements at Allegheny County Area Agency on Aging (ACAAA) and
Ursuline Senior Services Inc. (USS), we recognized that some in the social service community
lack knowledge about how to recognize the signs of alcoholism and help older adults obtain
resources for recovery. Like Mrs. Jones’ case, professionals confuse the symptoms of alcohol
abuse as belonging to another condition, age biases tend to cause professionals to assume
alcoholism is more of a problem for younger adults, and there is often less impairment in social
and occupational functioning due to other life factors (Rowan and Faul, 2007). This paper
discusses the prevalence of alcohol abuse and how alcohol affects aging adults. It also provides
information on two practice models from around the country and some ideas for potential
implementation locally.
Many addiction treatment programs and some research begin categorizing people as
older adults at the age of 55. For this paper, we will define an older adult as someone age 60
and above. It is at this age that a person can receive county-based aging and senior center
services in Pennsylvania.

2
Key Terms
The following key terms are used throughout this paper.
AAA: Area Agency on Aging
ACAAA: Allegheny County Area Agency on Aging.
Alcoholism: A disease that includes the four symptoms (1) craving, (2) loss of control, (3)
physical dependence, and (4) tolerance (National Institute of Alcohol Abuse and
Alcoholism, 2007).
1. Craving: A strong need, or urge, to drink.
2. Loss of control: Not being able to stop drinking once drinking has begun.
3. Physical dependence: When withdrawal symptoms, such as nausea,
sweating, shakiness, and anxiety occur after stopping drinking.
4. Tolerance: The need to drink greater amounts of alcohol to get "high."
Brief Advice: This method is utilized with people who may be at risk for developing
alcohol problems. It includes educating the person about the effects of increased alcohol
use and is usually provided during regular health exams by a clinician (Substance Abuse and
Mental Health Services Administration [SAMHSA], 2008b).
Brief Intervention: This technique may be used to prevent or treat a problem, regardless of
risk level. The goal of this intervention is to motivate a change of behavior. It usually
involves one or more sessions which may include the following: strategies to motivate
change, education, assessment and direct feedback, contracting and goal setting to change
behavior, behavioral modification techniques, and use of written materials (SAMHSA,
2008b).
Case/Care Management: “A method of providing services whereby a professional social
worker assesses the needs of the client and the client’s family, when appropriate, and
arranges, coordinates, monitors., evaluates, and advocates for a package of multiple services
to meet the specific client’s complex needs (NASW, n.d.).”
DHS: Department of Human Services.
DOH: Department of Health
Formalized Special Treatment: Method used for treatment of alcohol dependence.
Settings for treatment include outpatient services, residential rehabilitation, inpatient
rehabilitation, and inpatient/outpatient detoxification treatment. In these settings cognitive

3
behavioral approaches, group based approaches, individual counseling, medical/psychiatric
approaches and marital and family therapy may be used as types of treatment.
Inpatient Treatment: Treatment in a residential facility with care 24/7that is also known
as residential treatment.
Outpatient Treatment: Treatment where an individual does not reside at a facility.
Pre-treatment Intervention: This intervention is used when a person is in denial about
his/her alcohol use and involves a planned meeting where loved ones talk about their
concerns for the older person. It is usually moderated by an addictions expert, counselor, or
health or service provider and the goal of the meeting is to help the person recognize the
impact that their alcohol abuse is having on their friends and family.
SAMHSA: Substance Abuse and Mental Health Services Administration.
USS: Ursuline Senior Services, Inc.

4
Background
Population Statistics
The state of Pennsylvania has the third largest percentage of older adults age 65 and
older in the United States, 15.2 %, and the fifth largest number of older adults at 1,885,323
residents (Population Reference Bureau, 2006a, 2006b). These population statistics are
important to consider because as the baby boomers approach age 65, population characteristics
will shift and the aging population countrywide is projected to greatly increase. If the larger
population of older adults experiences health, mental health and addiction problems at the same
rates as the current population, society will need more providers to meet their needs.
States with largest 65+ population by % of state population as of 2006
States with largest 65+ population by # of older adults as of 2006
1) Florida (17.6%) 2) West Virginia (15.3%) 3) Pennsylvania (15.2%) 4) Iowa (14.6%) 5) Maine (14.6%) 6) North Dakota (14.6%) 7) South Dakota (14.2) 8) Hawaii (14.0%) 9) Arkansas (13.9%) 10) Rhode Island (13.9%)
1) California (3,931,514) 2) Florida (3,037,704) 3) New York (2,522,686) 4) Texas (2,334,459) 5) Pennsylvania, (1,885,323) 6) Illinois (1,534,476) 7) Ohio (1,531,994) 8) Michigan (1,260,864) 9) New Jersey (1,127,742) 10) North Carolina (1,076,951)
Source: Population Reference Bureau, 2006a, 2006b
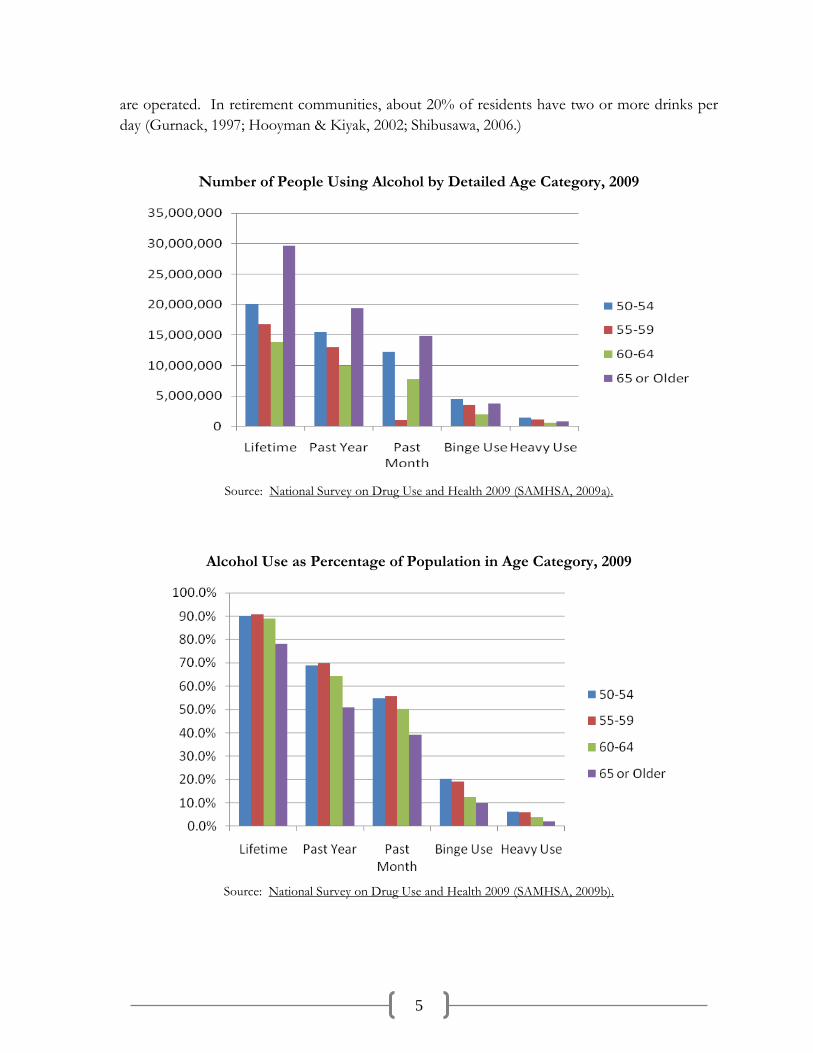
National Prevalence Statistics on Alcohol Use Alcohol use is one concern for older adults. As is outlined later in this paper, its adverse
impact on health and safety can be greater as one ages. The two charts on the next page
demonstrate that there is a higher alcohol consumption rate among people ages 50-54 and 55-59
than among people ages 60-64 and 65 or older. This could indicate a potential rise in drinking
rates among people ages 60-64 and 65 and over as the Baby Boomers enter these age cohorts.
Before the drinking rates potentially increase among older adults, it is important for social
service systems that serve older adults to be prepared to address this need. Even if the rates do
not increase, the sheer numbers will present a challenge to service providers.
There are differences in usage patterns by residence. In 2007, 93% of people 65 and
older lived in independent housing, 4% in long-term care facilities, and 3% in continuing care
retirement communities (U.S. Census Bureau, 2008). Residents of long-term care facilities were
less likely to have access to alcohol than community dwelling seniors due to way such programs
5
are operated. In retirement communities, about 20% of residents have two or more drinks per
day (Gurnack, 1997; Hooyman & Kiyak, 2002; Shibusawa, 2006.)
Number of People Using Alcohol by Detailed Age Category, 2009
Source: National Survey on Drug Use and Health 2009 (SAMHSA, 2009a).
Alcohol Use as Percentage of Population in Age Category, 2009
Source: National Survey on Drug Use and Health 2009 (SAMHSA, 2009b).

6
The information demonstrates that alcohol use generally decreases with age, with people
65 and older being less likely to engage in heavy use or binge use. As explained later, even
moderate use can interact with medications and may not clear the body as quickly. The nearly
40% of older adults who drink monthly could benefit from awareness of the risks associated
with it.
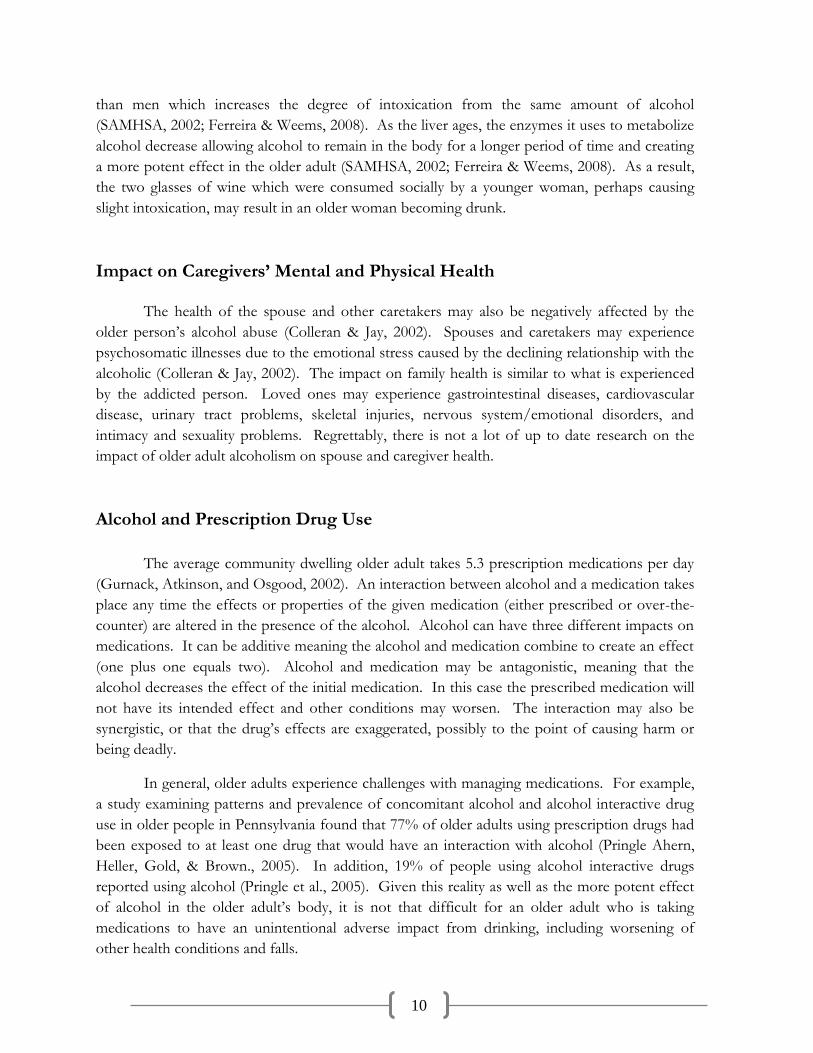
Aging Trends in Allegheny County, Pennsylvania and the United States
Allegheny County has a higher percentage of its residents age 65 and older than the
percentages for Pennsylvania and the United States (U.S. Census Bureau, 2009). When
countrywide alcohol use is high, it can be inferred that there may be a similar or higher
prevalence rate of alcoholism among older adults in Allegheny County based on the proportion
of the population. With baby boomers entering the 65 and older age category and a projected
increase of older adults country-wide, social services must be even more aware of the changing
needs of the aging population, including services for alcoholism.
Source: US Census Bureau 2009a, 2009b, & 2009c

7
Services Present in Allegheny County
To better understand the process of getting help for older adults receiving alcohol
treatment, we reviewed website materials and spoke to the ACAAA, subcontractors of the
ACAAA, alcohol treatment providers, and the Allegheny County Office of Behavioral Health
Services. In February 2011, Allegheny County Department of Human Services’ (DHS) website
stated,
Some programs are specifically designed to treat women; women with children;
pregnant women; pregnant women with children; intravenous drug users, LGBT
individuals; individuals with HIV; and adolescents. Providers serving priority
populations offer immediate assessment and admission to treatment in the
following order: pregnant injection-drug users; pregnant substance abusers;
injection-drug users; and all others. Pregnant women receive preferential
treatment services.
This is frustrating when seeking help for an older adult because many of the resources
listed on the DHS website were only for the listed target groups. After reviewing 20 websites of
treatment programs and centers, we found that only 11 treat older adults. We tried contacting
all 11 providers but only reached 8. Not one of the eight facilities provided age-specific
treatment for older adults in Allegheny County and the surrounding area. Of the eight facilities,
only two accepted Medicare, which is how many older adults pay for medical services.
Additionally, there is no list of specific alcohol services on the DHS website. They are included
in the broader category of substance abuse and mental health services. If you look at Appendix
A in this booklet, there is a chart of some available treatment centers for adults ages 18 and over
in the Allegheny County area. This chart includes information about whether the treatment
center provides inpatient or outpatient treatment and if they accept Medicare.
Most of these formal resources only are useful once a problem has been identified. To
address this issue others will need to recognize its presence. Older adults interact with informal
resources, such as family members and other community members. They also interact with
other formal resources outside the addictions treatment arena such as care managers, people
who work in home delivered meals programs, guardians, community volunteers (such as the cart
to heart program), homemaking and personal care staff, and medical personnel like doctors and
nurses.

8
Medicare and Medicaid Coverage
Since services for older adults are not always adequately covered by Medicare, Medicaid
and/or Medigap insurance, paying for treatment can present a challenge. Medicare Part A
covers inpatient hospital services, including mental health services, whether the hospitalization is
for a physical health problem or an addiction. The one difference is that inpatient mental health
care in a psychiatric hospital or addictions treatment center is limited to a total of 190 days in a
lifetime. (U.S. Department of Health and Human Services, 2011).
Medicare Part B covers Substance Abuse Outpatient Care if the treatment provider
accepts Medicare. Medicare covers outpatient mental health services provided by a doctor,
clinical social worker, clinical psychologist, clinical nurse specialist or a physician assistant in
settings such as a hospital outpatient department, an office, or a clinic (U.S. Department of
Health and Human Services, 2009). Under Part B an older adult may pay up to 45% of the
Medicare-approved amount and may also pay separate co-payments for services provided by the
facility (U.S. Department of Health and Human Services, 2009). This is important to consider
because Medicare recipients are normally required to pay only 20% of most doctor’s services in
inpatient facilities or for outpatient treatment and therapies for physical illnesses or limitations
(U.S. Department of Health and Human Services, 2011). This discrepancy in payment
percentages may hinder an older adult’s ability to pursue treatment. Additional medical
insurance coverage may be provided by private pay insurance companies and through the
purchase of elective Medigap insurance policies. This coverage varies by policy.
Medicaid coverage may help an older adult offset these costs. In Pennsylvania, Medicaid
health insurance provides coverage for low-income individuals. This coverage may include long-
term care assistance to individuals over the age of 65 and individuals with disabilities. This
insurance covers gaps in the Medicare program and may fund institutions that serve a
disproportionate number of low-income patients with special needs. In regard to covering gaps
in the Medicare program, Medicaid must pay Medicare premiums and/or cost sharing for
Medicare beneficiaries who meet the income and asset requirements for coverage (Pennsylvania
Medicaid Policy Center, 2011). Given these facts about insurance payments, some older adults
who are living on a fixed income will be disadvantaged in paying for treatment services for an
alcoholism problem.
Nationally, 17.7% of treatment facilities provided specialized programming to treat older
adults with alcohol abuse (Schultz et al., 2003). Rothrauff and colleagues (2011) found that 18%
of private substance abuse treatment centers offered specialized services for older adults. A
higher proportion of Medicare patients served by the facility predicted increased availability of
specialized services at these private treatment centers (Rothrauff et al., 2011).

9
Health Impact of Alcohol
When misuse or prolonged use of alcohol occurs, there are many negative health
consequences. The following table is based upon the work of Colleran and Jay (2002) in which
they explain how alcohol misuse or prolonged use may impact physical health of older adults.
System / Condition
Potential Health Impact on Older Adults
Brain Impaired judgment, reasoning, learning, coordination, memory, and speech. A sedative effect can occur which may result in death. Prolonged heavy drinking can cause brain damage. Some professionals refer to dementia caused by alcoholism as Wernicke-Korsakoff Syndrome.
Bladder Resistance to infections decreases, increase in incontinence, frequency of urination, and may develop cystitis or prostatitis.
Bones and Blood Osteoporosis, loss of calcium, lowers the resistance to disease, decreases red and white blood cell production, causes anemia, and increases chances of bruising.
Cancers Leukemia, lymphoma, cancer of the larynx and esophagus, lung, urinary tract, liver, pancreatic, gastric, colorectal, breast and brain cancer.
Digestive tract Gastritis, bleeding, ulcers, swelling, perforations, and colitis. Nutrient absorption is also diminished by use, especially vitamin B, zinc, calcium, and magnesium.
Heart Hypertension, increased cholesterol and fatty acids, arrhythmias or abnormal heart rhythms, myocarditis, and an increased risk factor for coronary artery disease.
Kidneys Nephritis, which can lead to permanent kidney damage. Edema can also develop.
Liver Hepatitis, jaundice, cirrhosis, low or high blood sugar, fatty liver, gout, cell fluid may be lost which decrease the ability to fight infection, and poor blood clotting
Pancreas Pancreatitis may develop which can lead to death.
For people, even using alcohol in smaller, socially appropriate amounts may be a
problem. For example, if they already have compromised body systems, alcohol may further
complicate their health in those areas. For example, someone with an Alzheimer’s type
dementia who even drinks a single beer with dinner may further impair his or her ability to
function. Someone who has gastritis or ulcerative bleeding could stimulate acute pain or
bleeding by drinking.
Another concern is that the body composition of older adults changes as aging occurs
and alters its ability to respond to and metabolize alcohol. During aging, the amount of water in
the body decreases. As alcohol is water soluble, less water in the body results in a higher level of
intoxication (SAMHSA, 2002). Additionally, women at most ages have less water in their bodies
10
than men which increases the degree of intoxication from the same amount of alcohol
(SAMHSA, 2002; Ferreira & Weems, 2008). As the liver ages, the enzymes it uses to metabolize
alcohol decrease allowing alcohol to remain in the body for a longer period of time and creating
a more potent effect in the older adult (SAMHSA, 2002; Ferreira & Weems, 2008). As a result,
the two glasses of wine which were consumed socially by a younger woman, perhaps causing
slight intoxication, may result in an older woman becoming drunk.
Impact on Caregivers’ Mental and Physical Health
The health of the spouse and other caretakers may also be negatively affected by the
older person’s alcohol abuse (Colleran & Jay, 2002). Spouses and caretakers may experience
psychosomatic illnesses due to the emotional stress caused by the declining relationship with the
alcoholic (Colleran & Jay, 2002). The impact on family health is similar to what is experienced
by the addicted person. Loved ones may experience gastrointestinal diseases, cardiovascular
disease, urinary tract problems, skeletal injuries, nervous system/emotional disorders, and
intimacy and sexuality problems. Regrettably, there is not a lot of up to date research on the
impact of older adult alcoholism on spouse and caregiver health.
Alcohol and Prescription Drug Use
The average community dwelling older adult takes 5.3 prescription medications per day
(Gurnack, Atkinson, and Osgood, 2002). An interaction between alcohol and a medication takes
place any time the effects or properties of the given medication (either prescribed or over-the-
counter) are altered in the presence of the alcohol. Alcohol can have three different impacts on
medications. It can be additive meaning the alcohol and medication combine to create an effect
(one plus one equals two). Alcohol and medication may be antagonistic, meaning that the
alcohol decreases the effect of the initial medication. In this case the prescribed medication will
not have its intended effect and other conditions may worsen. The interaction may also be
synergistic, or that the drug’s effects are exaggerated, possibly to the point of causing harm or
being deadly.
In general, older adults experience challenges with managing medications. For example,
a study examining patterns and prevalence of concomitant alcohol and alcohol interactive drug
use in older people in Pennsylvania found that 77% of older adults using prescription drugs had
been exposed to at least one drug that would have an interaction with alcohol (Pringle Ahern,
Heller, Gold, & Brown., 2005). In addition, 19% of people using alcohol interactive drugs
reported using alcohol (Pringle et al., 2005). Given this reality as well as the more potent effect
of alcohol in the older adult’s body, it is not that difficult for an older adult who is taking
medications to have an unintentional adverse impact from drinking, including worsening of
other health conditions and falls.

11
Alcoholism and Mental Illness
Findings from SAMHSA (2009c, 2009d) show that mental health problems and
alcoholism can be co-occurring conditions. The table below illustrates that nationally 959,000
people who misuse alcohol at age 50 or older have some form of mental illness. If these
percentages are extrapolated to Allegheny County’s population, about 3,478 people age 50 and
over may both misuse alcohol and be mentally ill. According to Blow and colleagues (2004),
“Drinking among elders elevates suicide risk through interactions with other factors that are
more prevalent in this age group, such as depressive symptoms, medical illness, negatively
perceived health status and low social support (pg. 48s).” It is important to address the issue of
alcoholism and mental illness as being co-occurring disorders because often when an older adult
is treated for alcoholism, it must also be kept in mind they may need additional resources to help
treat mental illness.
Alcohol Misuse in the 2009 in the United States among People 50 or Older Considering
Mental Illness and Gender (Number and Percentages of Population of That Age)
Source: Substance Abuse and Mental Health Services Administration (2009c, 2009d)
Gender / Age
Total Population Misusing Alcohol (# / %)
Population Misusing
Alcohol with Any Mental
Illness (# / %)
Population Misusing Alcohol
without Mental Illness (# / %)
Total: 50 or Older 3,338,000
3.5% 959,000 28.7%
2,379,000 71.39%
Males: 50 or Older 2,276,000
5.2% 539,000 23.7%
1,737,000 76.3%
Females: 50 or Older 1,062,000
2.1% 420,000 39.5%
642,000 60.5%

12
Building an Ideal Service Delivery Network
By studying the available information on this topic, we have learned that effective social
service delivery networks for alcohol abuse and treatment should have three areas of focus to
obtain a high quality service provision. These three areas of focus are:
1. Collaborative system integration,
2. Utilization of well-rounded prevention and education models, and
3. The understanding of applicable treatment principles.
If each area of focus is put into place effectively, a successful system for addressing the needs of
older adults and alcohol use would be in place.
System Integration
Intensive research has been conducted in Maine to address the subject of older adults
and alcohol abuse. The University of Maine’s Center on Aging partnered with the Healthy
Hancock Collaborative and the AdCare Educational Institute to conduct research on this
population in the state. The “Hancock County and Statewide Needs, Resources, and Readiness
Assessment on Older Adult Alcohol Abuse” research project examines the resources of
Hancock county and the county’s ability to meet the needs of alcohol abusing older adults. This
project utilized focus groups, surveys, and interviews with key informants to better understand
the issue. Older adults, professionals, and caregivers were included in the research (University of
Maine Center on Aging, 2006a).
This is considered a best practice model of system integration because if social services
workers keep the following guidelines in mind when working with older adults, then older adults
will have more outlets to obtain information and resources about alcohol abuse and to receive
help. Based on data gathered during the project, recommendations were made for
implementation on a broader state and national level to best meet the needs of this population
(University of Maine Center on Aging, 2006b).
Healthcare providers and administrators should connect healthcare and substance abuse
providers through streamlined referrals.
Professionals who work with older adults (doctors, nurses, social workers, home health
workers, direct care workers, and others) should be aware of the problem so they may
have discussions about alcohol use and abuse with older adults with whom they have
contact. Additionally, routine medical visits have been identified as an appropriate time
for this engagement with older adults and their caregivers, especially when problems are
suspected.

13
Three Levels of Education and
Prevention
1. Brief Advice
2. Brief Intervention
3. Pretreatment Intervention
SAMHSA, 2008b
Advocate for change on a macro level to increase prevention and treatment
programming as well as reimbursement for the programs.
Create funding for community-based and formal prevention and treatment
programming.
Be sure to represent older adults on community boards and committees. Create local
senior councils to ensure opportunity for participation.
Awareness campaigns should be implemented in communities and should be focused on
alleviating stigma.
Educational materials should be located in accessible and anonymous places for older
adults and their caregivers.
Prevention and Education Models
According to SAMHSA (2008b), there are three levels of education and prevention: (1)
brief advice, (2) brief intervention, and (3) pretreatment intervention. They are explained below.
Brief advice is a best practice to use for older
adults who are at risk for developing problems.
People in this category include those who have
experienced recent losses including the death of a
loved one, loss of social support, loss of status or
self-esteem due to retirement, declining health,
and loss of mobility/independence. Brief advice
includes educating the person about the effects of
increased alcohol use and is easily provided
during regular health exams or regular visits by
various professionals.
Brief Intervention may be used with an older adult who uses alcohol as a prevention
measure. It includes utilizing written materials, education, assessment, feedback, and
goal setting for behavior change. It may also include behavioral modification techniques
when appropriate.
Pretreatment Intervention should be used when an older adult is in denial of substance
abuse. This involves a planned meeting with loved ones, and typically a professional as
a moderator, to talk about their concerns for the older person. The goal of the meeting is
to help the person recognize the impact of their alcohol abuse and agree to seek
treatment.
Formalized, special treatment should be pursued when alcohol dependence is evident.
Forms of treatment include outpatient services, inpatient rehabilitation, residential rehabilitation,
and inpatient/outpatient detoxification treatment (SAMSHA, 2008b). Actual types of treatment

14
include cognitive behavioral approaches, group-based approaches, individual counseling,
medical/psychiatric approaches that utilize medication with counseling, and family/marital
therapy that may enhance treatment and rebuild an older person’s social support network. The
risk and protective factors to identify older adults who are abusing or potentially could abuse
alcohol are listed on the next page.
Treatment Principles
Florida, a state with a larger aging population than Pennsylvania, is the location of an
interesting program to serve older adults with alcohol problems. The Hanley Center’s Center
for Older Adult Recovery in West Palm Beach, Florida seeks to meet the unique needs of older
adults. According to its website,
The Center for Older Adult Recovery is the first 12-Step based drug and alcohol
rehabilitation center designed specifically for adults 55 and over. Our residential
Risk Factors for Developing Problems with Alcohol
death of a spouse, friends and other family members
loss of a job and related income, social status, and, sometimes, self-esteem-as a result of retirement
loss of mobility (trouble using public transportation, inability to drive, problems walking)
impaired vision and hearing, insomnia, and memory problems
declining health because of chronic illnesses
separation from children and loss of home as a result of relocation
loss of social support and interesting activities
(SAMHSA, 2008a)
Protective Factors for Avoiding Problems with Alcohol
access to resources, such as housing and health care
availability of support networks and social bonds
involvement in community activities
supportive family relationships
education (e.g. wise use of medications) and skills
sense of purpose and identity
ability to live independently
(SAMHSA, 2008a)

15
Unique Factors in Treating
Older Adults with Alcohol
Addiction
Loneliness & isolation
Lack of purpose
Medical concerns
Life transitions
Depression
Pain management
Grief and losses
The Hanley Center, 2011a
treatment center provides a safe and supportive environment that encourages
older adults to begin the recovery journey with peers of their own age (The
Hanley Center, 2011 a).
The Hanley Center’s Center for Older Adult Recovery
recognizes that Older Adults need different treatment
and recovery programs than other population groups.
The website states (2011 a) that there are many unique
factors and issues in treating older adults (see inset box).
Additionally, the professionals there advocate for (1) “an
extended detoxification and medical stabilization
process,” (2) a “need for slower transitions between
levels of care,” (3) recognizing that they may experience,
“complications due to cognitive function level, speech or
hearing impairment, and (4) providing “longer rest and
relaxation periods,” during treatment (The Hanley
Center, 2011a).
This center represents a Best Practice Model in the
area of age-specific treatment principles because while it serves people of all ages with
addictions, it divides the groups by age so that participants can relate better to their peers and
receive age-specific treatment that accommodates the individuals’ unique needs for recovery.
This age specific method is known nationally as “The Hanley Model.”
The center works in collaboration with other agencies in the area, such as The University
of Miami’s Comprehensive Drug Research Center and The Palm Beach County Health
Department, to conduct research projects that identify best practices in the field of age-specific
alcohol treatment. One research project that is currently underway is “The Five Year Plan.”
Over the next five years, it will assess numerous factors such as the effectiveness of the
treatments at Hanley and if the success rates of recovery are different among men, women and
older adults. Thus far, only one year of the study has been completed and the age-specific
results have not yet been published (The Hanley Center, 2011b). This is an important study as
other literature and research, including that from Maine, suggests that age-specific treatment
represents a best practice. This research seeks to confirm or deny that.

16
Vision for Allegheny and Surrounding Counties
While Allegheny County has many alcohol rehabilitation facilities, if the focus areas of
collaborative system integration, utilization of well-rounded prevention and education models
and the understanding of applicable treatment principles were applied to the facilities and to
social service workers in Allegheny County, older adult alcohol treatment would be strengthened
in the future. While there are resources available in Allegheny County, the following is a
suggestion for what Allegheny County (AAA and Office of Behavioral Health Services along
with subcontractors) can implement in the future to improve alcohol treatment services for
older adults.
Potential System Integration Ideas
Since the above recommendations for implementation were made to apply to a broader
state and national level, these ideas can easily be applied for Allegheny County. Below are a few
potential system integration ideas specific to Allegheny County.
Case managers and social service workers in Allegheny County should utilize the chart of
rehabilitation centers included in this booklet and the Allegheny County Department of
Human Services’ Where to Call Directory available on the DHS website to find available
rehabilitation services for older adults.
If a social service worker suspects alcohol abuse, he or she should (within the allowable
limits of confidentiality and privacy practices) contact a family member or the client’s
primary medical doctor and follow up to remain informed about the client’s status.
Educational materials should be located in senior centers and social services agencies
throughout Allegheny County, as well as in retirement homes, nursing facilities, senior
high-rise buildings, medical offices, and other accessible and anonymous places for older
adults and their caregivers.
Potential Utilization of Prevention and Education Ideas
A prevention model that can be used in Allegheny County is a brief intervention model.
Social service workers and medical employees can use the risk factors in the chart on page 14 to
recognize when an older adult may be at risk for abusing alcohol. Based upon this screening, the
worker should distribute available written materials, educate the client on the topic, help the
client set goals, and obtain help if necessary. If the individual is already abusing alcohol and
denying that they have a problem, the worker should use pretreatment intervention, an

17
Top Recommendations for Region
System Integration:
Increase awareness of older adult alcohol misuse and abuse for all professionals in the aging services network.
Prevention and Education
Place Education material in numerous locations
During routine visits, perform screenings
Treatment
Increase number of Medicare Certified treatment centers
Develop age-specific treatment in the region
interaction method where the goal is to help the person recognize the impact that their alcohol
abuse is having on their friends and family and to receive treatment if necessary. If the client
recognizes their addiction, the next step would be to receive formalized special treatment in
Allegheny County. As employees of social services agencies, workers must be careful not to
overstep professional boundaries to help a client. A way to do this is to involve the family,
friends and health professionals of the client in the entire process.
Treatment Principles & Ideas
Although it is stated above that none of the eight contacted rehabilitation programs in
Allegheny County has age-specific treatment programs for older adults, these programs still play
an essential part in the recovery of older adults. If rehabilitation programs keep the following
key concepts from the Hanley Model in mind while treating older adults, maybe older adults will
be more encouraged to seek help and will have successful treatment outcomes.
Even if a facility does not offer age-specific treatment, it should be kept in mind that the
recovery needs of each patient is different and by offering individualized treatment plans,
patients may recover more quickly and permanently.
Older adults usually need more time in rehabilitation programs because of the
complexity of medical and cognitive conditions.
While receiving treatment, older patients need more resting periods.
If an older adult is receiving outpatient treatment, their transportation situation to and
from the facility should be kept in mind.
Employees of rehabilitation centers should be extremely careful not to stigmatize older
adults because of their age and patients because of their rehabilitation status.
If a facility provides individualized care plans and its’ employees are understanding and
accommodating not only towards older adults, but also towards all patients, this
supportive environment will hopefully foster the patients’ recovery.
.

18
Appendix A
Treatment Centers Serving Allegheny County
Agency Information
Inp
ati
en
t
Ou
tpati
en
t
Accepts Medicare Notes
First Step Recovery Homes, Inc
412-672-7681
Yes No Funded through DHS, do not need
insurance or payment
Males only, ages 18-80.
Gateway Rehabilitation Center
412-604-8900 http://www.gatewayrehab.org
Yes Yes No, if Medicare is primary payment must self-pay for
treatment
No age-specific treatment options. Age and gender requirements vary by location, most 18 and over.
Greenbriar Treatment Center
724-225-9700
http://www.greenbriar.net/index.php
Yes* Yes* Yes For males and females 18 and over. Has dual diagnosis treatments.
Mercy Behavioral Health
1-877.637.2924 (Open 24/7)
http://www.mercybehavioral.org
Yes Yes Yes No age-specific treatment options. For males and females 18 and over.
Mon Yough Community Services, Inc.
412-675-8300
http://www.mycs.org
No Yes No No age-specific treatment options. For males and females 18 and over.
Pyramid Health Care, Inc.
888-694-9996
Yes Yes No, but takes other state insurance
No age-specific treatment options. For males and females 18 and over.
Salvation Army Harbor Light Center **
412-231-0500 and http://www.use.salvationarmy.org/use/www_use_westPenn.nsf/vw-search/529BD63DA2B06B3C802573060061C026?opendocument
Tadiso, Inc.
(412) 322-8415 or (412) 362-8510
http://www.tadiso.org
No Yes No No age-specific treatment options. For males 18 and over only.
Turtle Creek Alternatives **
412-381-2100 x 8851 and http://www.tcv.net/
Western Psychiatric Institute and Clinic **
412-624-1000 then press 5 and http://www.upmc.com/HospitalsFacilities/Hospitals/wpic/Pages/contact-us.aspx
White Deer Run, Inc
877.907.6237 http://www.whitedeerrun.com
Yes Yes No No age-specific treatment options. For males and females 18 and over.
* Depends upon the location within the agency. ** Unable to get needed information by time of printing.

19
References
Allegheny County Department of Human Services (2011, February). Substance abuse management. Retrieved from http://www.alleghenycounty.us/dhs/substanceabuse.aspx
Blow, F. C., Brockmann, L.M., & Barry, K. L. (2004). Role of Alcohol in Late-Life Suicide. Alcoholism: Clinical and Experimental Research, 28(5), 48S-56S. doi:10.1097/01.ALC.0000127414.15000.83?
Colleran, C., & Jay, D. (2002). Aging and addiction: helping older adults overcome alcohol or medication dependence. Center City, Minnesota: Hazelden.
Ferreira, M.P. & Weems, S. (2008). Alcohol consumption by aging adults in the United States: health benefits and detriments. Journal of the American Dietetic Association, 108, 1668-1676. doi:10.1016/j.jada.2008.07.011
Gurnack, A.M. (1997). Older adults’ misuse of alcohol, medicines, and other drugs. New York: Springer.
Gurnack, A.M., Atkinson, R., & Osgood, N. (Eds.). (2002). Treating alcohol and drug abuse in the elderly. New York: Springer.
Hooyman, N.R, & Kiyak, H.A. (2002). Social gerontology: A multidisciplinary perspective. Boston: Allyn & Bacon
National Association of Social Workers (n.d). Information booklet with application and reference forms for certified Social Work case Manager and Certified Advanced Social Work Case Manager. Retrieved March 28, 2011 from http://www.socialworkers.org/credentials/applications/c-aswcm.pdf.
National Institute on Alcohol Abuse and Alcoholism (2007). What is alcoholism? Frequently Asked Questions for the General Public. Retrieved from http://www.niaaa.nih.gov/FAQs/General-English/Pages/default.aspx#whatis
Pennsylvania Medicaid Policy Center. (2011). Frequently asked questions. Retrieved fromhttp://www.pamedicaid.pitt.edu/faqs.html#a9
Population Reference Bureau. (2006a). Data comparisons by topic bar: population ages 65 and
older, 2006 #. [Data file]. Retrieved from http://www.prb.org/Datafinder/Topic/Bar.aspx?sort=v&order=d&variable=395
Population Reference Bureau. (2006b). Data comparisons by topic bar: population ages 65 and older, 2006 %. [Data file]. Retrieved from
http://www.prb.org/Datafinder/Topic/Bar.aspx?sort=v&order=d&variable=396
Pringle, K.E., Ahern, F.M, Heller, D.A., Gold, C.H., & Brown, T.V. (2005). Potential for Alcohol and prescription drug interactions in older people. Journal of the American Geriatrics Society, 53, 1930-1936. doi:10.1111/j.1532-5415.2005.00474.x
Rothrauff, T.C., Abraham, A.J., Bride, B.E., & Roman, P.M. (2011). Substance abuse treatment for older adults in private centers. Substance Abuse: Official Publication of the Association for Medical Education and Research in Substance Abuse, 32(1), 7-15.
Rowan, N. L., & Faul, A.C. (2007). Substance Abuse. In J.A. Blackburn &, C.N. Dulmus (Eds.), Handbook of Gerontology: Evidenced-Based Approaches to Theory, Practice, and Policy (pp. 309-332). Hoboken, NJ: John Wiley & Sons, Inc.
Schultz, S.K., Arndt, S. & Liesveld, J. (2003). Locations of facilities with special programs for older substance abuse clients in the U.S. International Journal of Geriatric Psychiatry, 18, 839-843.
Shibusawa, T. (2006). Older adults with substance/alcohol abuse problems. In B. Berkman (Ed.), Handbook of social work in health and aging (pp. 141-148). New York: Oxford University Press.
Substance Abuse and Mental Health Services Administration. (2002, July 3). At any age, it does matter: substance abuse and older adults (for professionals). Retrieved on March 16, 2011 from http://pathwayscourses.samhsa.gov/aaap/aaap_3_pg6.htm.
Substance Abuse and Mental Health Services Administration. (2008a). Fact sheet #4 An invisible problem: alcohol and older adults.

20
Get Connected! Linking Older Adults with Medication, Alcohol, and Mental Health Resources. Washington, D.C.: Government Printing Office
Substance Abuse and Mental Health Services Administration. (2008b). Fact sheet #5 Prevention, intervention, and treatment of alcohol problems among older adults. Get Connected! Linking Older Adults with Medication, Alcohol, and Mental Health Resources. Washington, D.C.: Government Printing Office
Substance Abuse and Mental Health Services Administration. (2009a). Alcohol use in lifetime, past year, and past month, by detailed age category: numbers in thousands, 2008 and 2009. [Data file]. Retrieved from http://oas.samhsa.gov/NSDUH/2k9NSDUH/tabs/Sect2peTabs1to42.htm#Tab2.15A
Substance Abuse and Mental Health Services Administration. (2009b). Alcohol use in lifetime, past year, and past month, by detailed age category: percentages, 2008 and 2009. [Data file]. Retrieved from http://oas.samhsa.gov/NSDUH/2k9NSDUH/tabs/Sect2peTabs1to42.htm#Tab2.15B
Substance Abuse and Mental Health Services Administration (2009c). Alcohol dependence or abuse in the past year among persons aged 18 or older, by past year level of mental illness, gender, and age group: numbers in thousands, 2008 and 2009. [Data file]. Retrieved from http://oas.samhsa.gov/NSDUH/2k9NSDUH/MH/tabs/Sect1peMHtabs.htm#Tab1.12A
Substance Abuse and Mental Health Services Administration (2009d). Alcohol dependence or abuse in the past year among persons aged 18 or older, by past year level of mental illness, gender, and age group: percentages, 2008 and 2009. [Data file]. Retrieved from http://oas.samhsa.gov/NSDUH/2k9NSDUH/MH/tabs/Sect1peMHtabs.htm#Tab1.12B
The Hanley Center (2011a). Center for Older Adult Recovery. Retrieved from http://www.hanleycenter.org/programs/adults-recovery/
The Hanley Center (2011b). Research Collaborative. Retrieved from
http://www.hanleycenter.org/research/research-collaborative/
U.S. Census Bureau. (2008). American housing survey for the US: 2007. Current Housing Reports. Series H150-70. Washington, D.C.: U.S. Government Printing office.
U.S. Census Bureau. (2009a). State and county quick facts: Allegheny County, PA [Data file]. Retrieved from http://quickfacts.census.gov/qfd/states/42/42003.html
U.S. Census Bureau. (2009b). State and county quick facts: Pennsylvania [Data file]. Retrieved from http://quickfacts.census.gov/qfd/states/42000.html
U.S. Census Bureau. (2009c). State and county Quick facts: USA [Data file]. Retrieved from http://quickfacts.census.gov/qfd/states/00000.html
U.S. Department of Health and Human Services. (2011). Centers for Medicare & Medicaid Services: Medicare and You 2011. Retrieved from http://www.medicare.gov/publications/pubs/pdf/10050.pdf
U. S. Department of Health and Human Services (2009). Substance abuse care (outpatient). your Medicare coverage: Pennsylvania [Data file]. Retrieved from http://www.medicare.gov/Coverage/Search/Results.asp?State=PA%7CPennsylvania&Coverage=78%7CSubstance+Abuse+Care+%28Outpatient%29&submitState=View+Results+%3E
University of Maine Center on Aging. (2006a). Hancock County and Statewide Needs, Resources, and Readiness Assessment on Older Adult Alcohol Abuse. Retrieved from <http://www.umaine.edu/mainecenteronaging/documents/CoAHancockCountyneeds_000.pdf>
University of Maine Center on Aging. (2006b). Key Project Recommendations: How You Can Help. Hancock County Needs, Resources, and Readiness Assessment on Older Adult Alcohol Abuse. Retrieved from http://www.umaine.edu/mainecenteronaging/documents/OSAneedskeyrecs.pdf