Embed Size (px)
Citation preview
.•
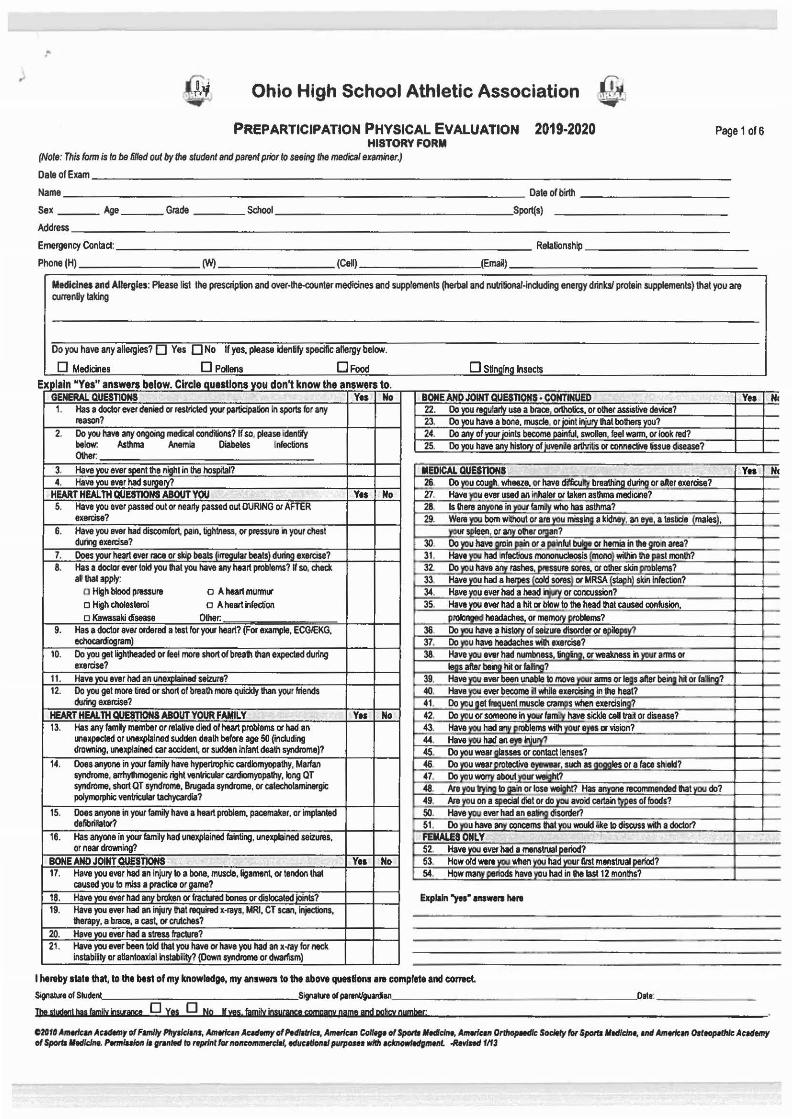
Ohio High School Athletic Association m PREPARTICIPATION PHYSICAL EVALUATION 2019·2020
HISTORY FORM (Note: This fonn is to be 6/led out by the student and parent prior to seeing the medical examiner.}
Page 1 of 6
Oa~ofEum ________________________________________________________________ ..... __ ............... _____ ............... -----
Name ---------------------------------------------- ------------ Date of birth --------------------Sex ___ Age ___ Gtade _____ Schooi _________________ .Sport{s)
Address---------------------------------------------------------------------------------Emergency Contact: _____________________________________________________ Relationship-----------------
Phone (H) (W) (Cell) (Email)
Medicines and Allergies: Please list the prescription and over-the-counter medicines and supplements (herbal and nulrilional·induding energy drinks/ pro~in supplements) that you are currenUy taking
Do you have any allergies? 0 Yes 0 No If yes, please identify specific allergy below.
0 Medicines 0 Pollens 0 Food 0 Stin in Insects
I I y " b Cl I I d I k th Explain 1 es answers elow. rc e auest ons you ont now e answers o. GENERAL QUESnONS Yea No BONE AND JOIHT QUESnONS • CONTINUED Yea
1. Has a cloctw ttver denied or restrfded your participation in sports tor any 22. Do ~u ~u~ use a braoe, OOhotics, or other assistive device? reason? 23. Do you have a bone, muscle or joint Injury that bothe~?
2. Do you have any ongoing medical conditions? If so. please idently 24. Do an_y_ of)'llur joints become ~ful, swollen, feel warm, or look ted? below: Asthma Anemia 00\er.
Diabetes Infections 25. Do you have any history of juvenie arthritis or COMedive tissue disease?
3. Have you ever spent lhe night in lhe hospital? MEDICAL QUESTIONS Yea 4. Have you ever had surgery? 26 Do _}I)U CO.J!lh. wheeze, or have difficu_k bre~ du~ or after exercise?
HEART HEALTH QUESTIONS ABOUT YOU Yes No 27. Have yau ever used an inhaler or taken asthma medlooe? 5. Have you ever passed out or nearly passed out DURING or AFTER 28. Is there anyone in~~~ who has asthma?
exercise? 29. We~ born without or are you missing a kidntv, an 8)'11, a tesbde (males), 6. Have you ever had discomfort. pa1n, tightness, or pressure in your chest ~spleen o~ olher_cMgan?
during exercise? 30 Do ~u haYe ~in~ or ~inld~ or hernia in the groin area? 7. Does your heart ever race or skip beats (irregular beats) during exercise? 31. Hav~ had infectious mononucleosis_(mongl ~the past month? 8. Has a doctor ttver told you that you have any heart problems? If so. check 32. Do you have any rashes~ure sores, or other ski~blems?
al that apply. 33. Have you had a hetpes (cold sores) or t.4RSA [staph) skin Infection? a High blood pressure o A heart munnur 34. Have you ever had a head~ or concussion? o High choles~rol o A heart infection 35. Have you ever had a hit or blow to the head that caused conlusion, o Kawasaki disease Other. prolonged headaches, or me!"OI}' problems?
9. Has a doctor ttver ordered a test for your heart? (For example, ECGIEKG. 36 Do _ll1!!_ have a ~of seizure disorder or epilepql echocardiogram) 37. Do you have headaches wilh exercise?
10. Do you get lightheaded or feel more short of breath than expeded during 38. Have~ever had numbness.~ or weakness in your anns or exercise? ltlgs after beng hit or Ja~q~?
11. Have vou ever had an unelq)lained seizure? 39. Have 'IW •-been unable lo move~ arms or .§s after being hit or f~? 12. Do you get more tired or short of breath more quickly than your friends 40. Have YllU ever become iN while exercisir!g in the heat?
during exerciSe? 41. Do )'I)U ga~uent muscle eta~ when exercising? HEART HEALTH QUESTIONS ABOUT YOUR FAMILY Yt1 No 42. . Do vou 01' someone in your fam!l/ have sicl<Je cell Ira~ or disease? 13. Has any family member or relative died of heart problems or had an 43. Havem had ~roblems with~ or vision?
unexpected or unexplained sudden death before age 50 ~nduding 44. Have YW had an • ir\iUIY'7 drowning, unexplained car accident, or sudden infant death syndrome)? 45. Do you wear glasses or contact lenses? ..
14. Does anyone in your family have hypertrophic cardiomyopathy, Marfan 46. Do yOU wear protective eyewear, such as gogoles 01' e face sh eld? syndrome, armythmogenic right venllicular cardiomyopalhy, long QT 47. Do you wocry aboul~~t? syndrome, short QT syndrome, Brugada syndrome, or cateeholaminergic 48. Are~ 1o ~in or lose weight? Has ~one recommended flat you do? polymorphic ventricular tachycardia? 49. Are you on a special cfl8t ordo}'l!U_avoid certainjyp_es of foods?
15. Does anyone in your family have a heart problem, pacemaker, or implan~ 50. Have 'IW ever h8d an~ disorder? defibrillator? 51. Do you have any conoems that you would like 1o discuss with a doctor?
16. Has anyone in your family had unexplained fainting, unexplained seizures. FEMALES ONLY or near drowning? 52. Have ~ ever had a menstrual period?
BONEANDJ~QUESTIONS Y11 No 53. How old we~ whe~ had~ur first menstrua~liod? 17. Have you aver had an injury to a bone. muscle,ligament or tendon that 54. How many Pl!lods have you had in the last 12 months?
caused you to miss a practice or game? 18. Have you ttver had any broken or ftactured bones or dislocated joints? Explain "yea" answers hers 19. Have you ever had an injury that required x·rays, MRI, CT scan, injections,
therapy, a brace, a cast 01' crutches? 20. Have you ever had a stress fracture? 21. Have you ever been told that you have or have you had an x -tay for neck
instabirtty or aUantoaxial nstability? (Down syndrome or dwarfism)
I hereby 1tatelhlt, to the btsl of my knowledge, my 1nswersto the above questions are c:ompleteand conct SignaveofStude Slgnallreofpatenllguanlian, _______________ ___ _ _ oate: --------
Jbe s!!!dtat bas familY ;nv;m 0 Yes 0 No K ves. familY !nsucanct amganv name and oohcy oymbar;
~2G111 Allltlk111 A~..,_,, of Fllrllly Plry.SdiDI, Amllfcln A~tmy ofPid/111/A, Amttle~~t Collfge of Spotfr II..Jda., AmwiAn Orlhopadk Sodtly for Spotts lied/cine, IM AmtrleM! Olltoplthk A~ademy of $porta lied/doe. Pttmluloll/s rr-nled ID rtptfnl fw noncommwcl•l, adu~lllonll purp0111 wfltl aeknowfedimtnt .lfewfftd 1113
He
Nc
('
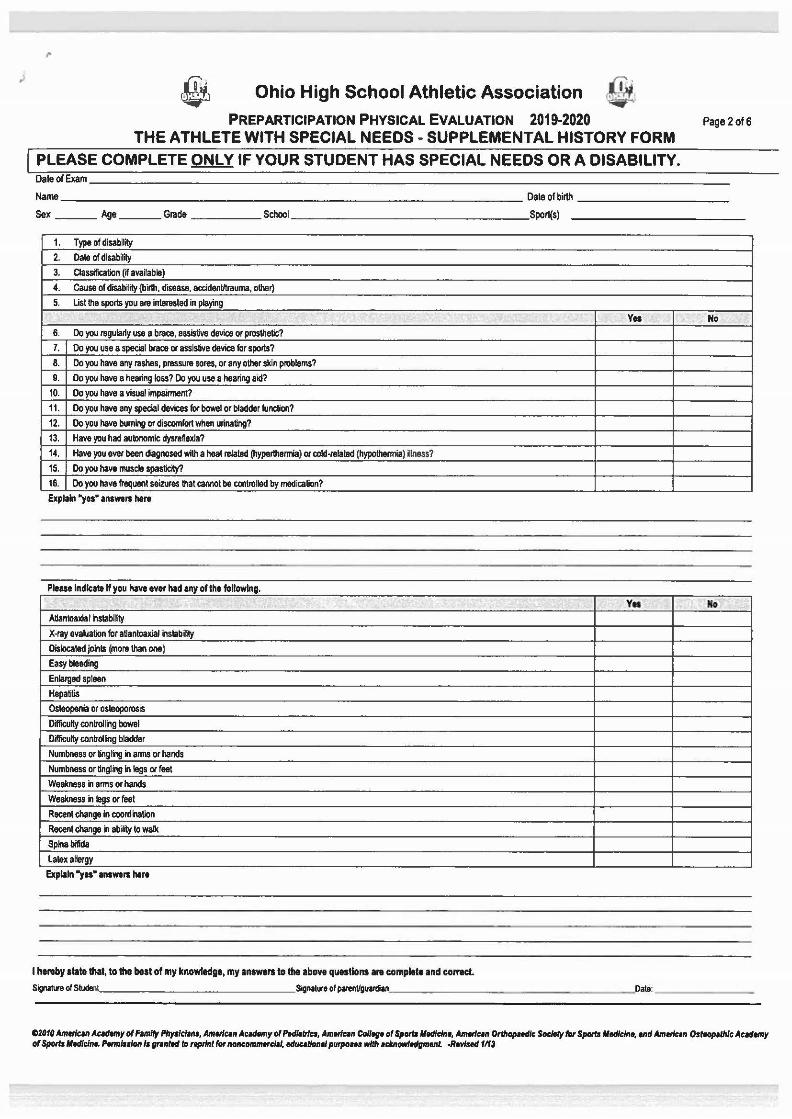
Ohio High School Athletic Association PREPARTICIPATION PHYSICAL EVALUATION 2019-2020 Page 2 of6
THE ATHLETE WITH SPECIAL NEEDS - SUPPLEMENTAL HISTORY FORM
PLEASE COMPLETE ONLY IF YOUR STUDENT HAS SPECIAL NEEDS OR A DISABILITY. Daleo! Exam ___________________________________________ _
Name ________________________________ Oateolbirth ----------
Sex ___ Age ___ Grade _____ Schooi ________________ Sport(s)
1. Type of disability
2. Date of disability
3 . Classification r.r available)
•• Cause of disability (birth, disease, accidenlltrauma, other)
5. List the sports you a~e intemted in playing
Y11 No
6. Do you ~egula~y use a brace, assistive device or prosthetic?
7. Oo you use a speeial brace or assistive device for sports?
8. Do you have any rashes, prassu~e sam, or any other skin problems?
9. Do you have a hearing loss? Do you use a hearing aid?
10. Oo you have a visual impairment?
11. Oo you have any special devices lor bowel or bladder function?
12. Do you have burning or discomfort when urinating?
13. Have you had au1onomic dysraftexia7
14. Have you ever been diagnosed with a heal ~elated (hyperlhermia) or alld-related (hypothermia) illness?
15. Do you have muscle spasticity?
16. Oo you have frequent seizures that cannot be controlled by medication?
Explain "yes• answers here
Please Indicate If you have ever hid any of the following.
'· .; " v .. ... AUantoaxial instability
X-ray evaklation for aUantoaxial ilstabilily
Dislocated jolnls (mora than one)
Easy bleeding
Enlarged spleen
Hepatitis
Osteopenia or osleoporos IS
Difficulty conlrolling bowel
Difficulty controllng bladder
Numbness or tinglilg in arms or hands
Numbness or tingling in legs or feet
Weakness in arms or hands
Weakness in legs or feet
RIICent change in coordilation
Recent change in ab~ to walk
Spinabifida
latex allergy
Explain "yu" answers here
I hereby state that, to the best of my knowledge, my answers to tile above questions are complete and comet. Si,annofSIIl,-~ ________ _____ Sillflalureofparenllgullldian'---- - --------- -----'Oate: ______ _
C201a Amwlcrn Ac..temy Dl Fllfll/y l'llyslclrns, Amlrlcen Ac.nmy Dl Pedleltlc., Amerlc.n Col/tgt ol SpOttllltdlcltlt, Alllttlr:.n Orthopaedic Sodtlyfw Spomlledlclnt, end Amlrlcen Osteopefhlc Acedemy or $porta lledlr:lne. l'tnnluiOIIII gt~nled ID nptlnl for noncOIIUIItl'del, eduullonel pUfJIOHI with tcknowltdgmtnt -RIWiftd 11f3
,I
J"
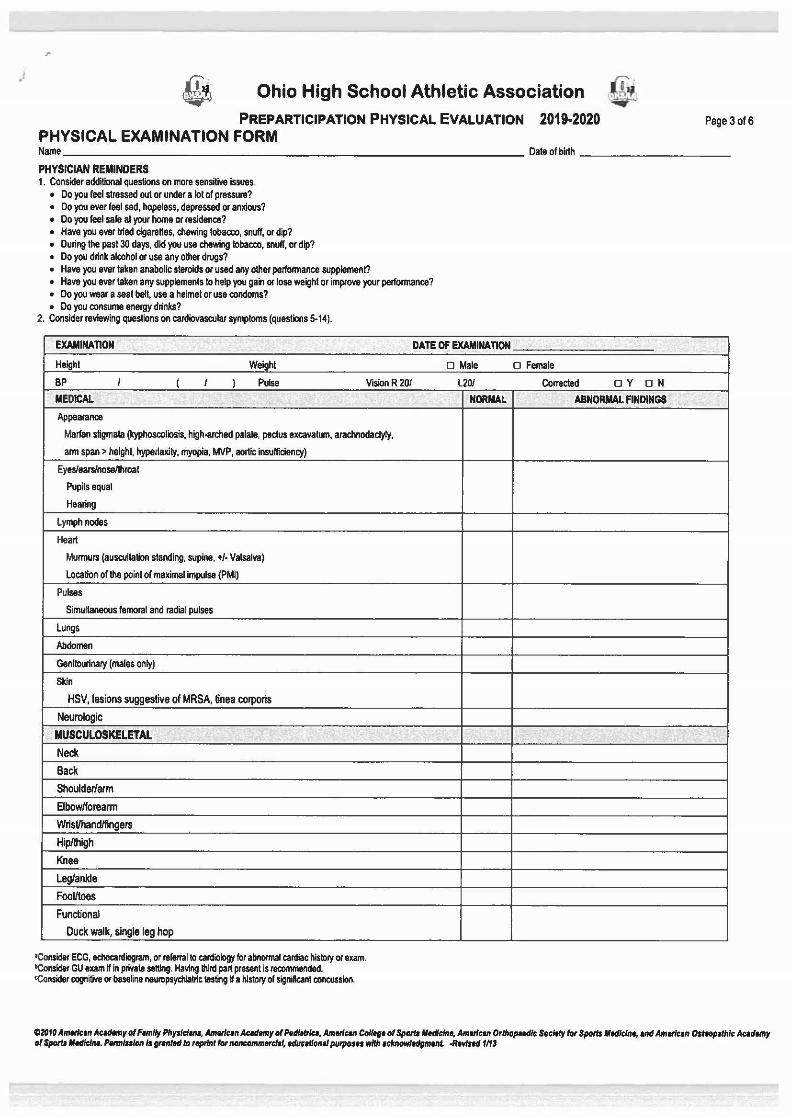
Ohio High School Athletic Association
PREPARTICIPATION PHYSICAL EVALUATION 2019·2020 PHYSICAL EXAMINATION FORM
Page 3 of6
Name _________________________________ Oateofbirth -----------
PHYSICIAN REMINDERS 1. Consider additional questions on more sensitive issues..
• Do you reet stressed out or under a lot of pressure? • Do you ever feel sad, hopeless, depressed or anxious? • Do you feet safe at your home or residence? • Have you ever tried cigarettes, chewing tobacco, snuff, or dip? • During the pasl30 days, did you use chewing tobacco, snull, or dip? • Do you drink alcohol or use any other drugs? • Have you ever taken anabolic steroids or used any other performance supplement? • Have you ever taken any supplements to help you gain or lose weight or improve your performance? • Do you wear a seat belt, use a helmet or use condoms? • Do you consume energy drinks?
2. Consider reviewing questions on cardiovascular symptoms (questions 5-14).
EXAMINAnON
Height Weight
BP ' ( ' ) Pulse Vision R20f
MEDICAl
Appearance
Marfan stigmata (kyphoscoliosis, high-arched palate, pectus excavatum, arachnodactyly,
arm span> height. hyperlaxity, myopia, MVP, aortic insufficiency)
Eyeslearsfnoseflhroat
Pupils equal
Hearing
Lymph nodes
Heart
Murmurs (auscultation standing, supine, +f- Valsalva)
Location of the point of maximal impulse (PMI)
Pulses
Simultaneous femoral and radial pulses
Lungs
Abdomen Genitourinary (males only)
Skin
HSV, lesions suggestive of MRSA, tinea corporis
Neurologic
MUSCULOSKELETAL
Neck
Back
Shoulder/arm
Elbowlforeann
WrisUhandlfingers
Hip/lhigh
Knee Leg/ankle
FooUtoes
Functional
Duck walk, single leg hop
'Consider ECG, echocardiogram, or referral to cardiology for abnormal cardiac history or exam. bConsider GU exam Win private setting. Having lhird part present is recommended. <Consider cognitive or baseline neuropsydlialric tasting W a history of significant concussion.
_.
DATE OF EXAMINAnON
D Male
l20f
NORMAL
o Female
CO!l'ected D Y O N
ABNORMAL FINDINGS
02010 Ametlc:111 Acldemy of Family Phy•lclllls, Amfllc.n Ac.demy ofPtd~trlu, AmetiCIII College of Span. Medicine, Am.nc111 Orthopaedic Soc:llfy for Sport. Medlclrlfl, VIII Ametfcen Omopelb/c Acedtmy of Sport. Mllllclnt. Penn/ulon 11 gnnled ID teprfnl for noncom~1l, edue~tlonll PUIJIOSII with 1clmowledgment -Relllstd 1113
,.
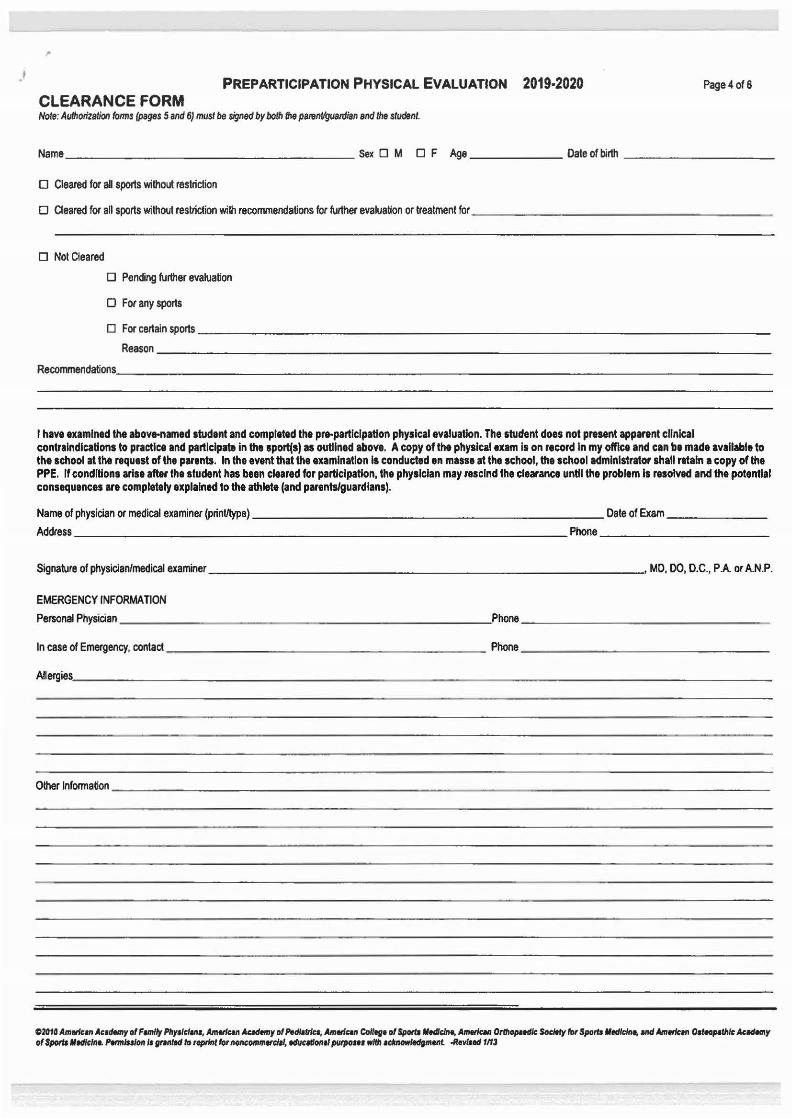
PREPARTICIPATION PHYSICAL EVALUATION 2019·2020 Page4of6
CLEARANCE FORM Note: Authorization forms (pages 5 and 6) must be signed by both the panml/g(Jardian and the student.
Name ___________________ sex 0 M 0 F Age ______ Dateofbirth ----------
0 Cleared for all sports without restriction
0 Cleared for all sports without restriction with recommendations for further evaluation or treatment for ____________________ _
0 Not Cleared
0 Pending further evaluation
0 For any sports
0 Forcettainsports ______________________________________ _ Reason ____________________________________________ _
Re~datioos. _________________________________________________________ __
I have examined the abov•named student and completed the pre-participation physical evaluation. The student does not present apparent clinical contraindication• to practice and participate in the aport(s) as outlined above. A copy of the physical exam Is on record In my office and can be made available to the school at the request of the parents. In the evant that the examination Ia conducted en masse at the school, the school administrator shall retain a copy of the PPE. If conditions arise after the student has been cleared for participation, the physician may rescind the clearance until the problem Is resolved and the potential consequences are completely explained to the athlete (and parents/guardians).
Name of physician or medical examiner {print/type) -------------------------Date of Exam-------
Address - ------------------ - ---------------Phone----------------
Signature ofphysiclan/medical examiner ___________________________ _. MD. 00, D.C., PA Of A.N.P.
EMERGENCY INFORMATION P~~Ph~an _____________________________________ ,p~-------------------------
In case of Emergency, contact------------------ --- Phone-----------------
~e~~s~-----------------------------------------------------
Other lnfonnation -------------------------------------------------------
~1010 Amlrlcan Ac•dMry of Family Pttyslcl111s, Amldcan Academy of f'ldlalrlca, AmldCIII Col/lflt of Spw lltdldnt, AlfllriCIII Ortllopatdlc Socltly rot Spora lledlclne, llld Am""'" Osttopalhlc Academy of $periJ lltdlclne. l'wmluiOII Is gtlllltdla ttptlnt rot IIOIICOIIIIfllfcla/, tdu"IIOIIII putpoHI wltll lcAA~IIIIIIt -Revlsad 11f3
PREPARTICIPATION PHYSICAL EVALUATION 2019-2020 THE STUDENT SHALL NOT BE CLEARED TO PARTICIPATE IN INTERSCHOLASTIC ATHLETICS
UNTIL THIS FORM HAS BEEN SIGNED AND RETURNED TO THE SCHOOL
OHSAA AUTHORIZAnON FORM 2019·2020
I hereby authorize the release and disclosure of the personal health information of ("Student"), as described below, to ___________ {"School").
PageS of6
The information described below may be released to the School principal or assistant principal, athle~c director, coach, athletic trainer, physical education teacher, school nurse or other member of lhe School's administrative staff as necessary to evaluate the Studenrs eligibility to participate in school sponsored activities, including but not limited to interscholastic sports programs, physical education classes or other classroom activities.
Personal health information of the Student which may be released and disclosed includes records of physical examinations performed to determine the Student's eligibility to participate in school sponsored activities, including but not timited to the Pre-participation Evaluation form or other similar document required by the School prior to determining eligibMity of lhe Student to participate in classroom or other School sponsored activities; records of the evaluation, diagnosis and treatment of ~uries which the Student incurred while engaging in school sponsored activities, induding but not limited to practice sessions, training and competition; and other records as necessary to determine the SIUdenrs physical fitness to participate in school sponsored activities.
The personal health information described above may be released or disclosed to the School by the Studenfs personal physician or physicians; a physician or other health care professional retained by the School to perform physical examinations to determine the Studenrs eiglbiRty to participate in certain school sponsored activities or to provide treatment to students Injured while participating in such activities, whether or not such physicians or other health care professionals are paid for their services or volunteer their time to the School; or any other EMT, hospital, physician or other health care professional who evaluates, diagnoses or treats an injury or other condition incurred by the student while participating in school sponsored adivities.
I understand that the School has requested this authorization to release or disclose the personal health information described above to make certain decisions about the Student's health and ability to participate in certain school sponsored and classroom activities, and that lhe School is a not a health care provider or health plan covered by federal HIPAA privacy regulations, and the information described below may be red1sclosed and may not continue to be protected by the federal HIPAA privacy regulations. I also understand lhat the School is covered under the federal regulations lhat govem the privacy of educational records, and that the personal health information disclosed under this authorization may be protected by those regulations.
I also understand that health care proVIders and health plans may not condillon the provis;on of treatment or payment on the signing of this authorization; however, the Student's participation in certain school sponsored activities may be conditioned on the signing of this authorization.
I understand !hall may revoke this authorization in writing at any time, except to the extent that action has been taken by a health care provider in re~ance on this authorization, by sending a written revocation to the school principal (or designee) whose name and address appears be'ow.
Name of Principal:
Schoo Address:
This authorization wll expire when the student is no longer enrolled as a student at the school,
NOTE: IF THE STUDENT IS UNDER 18 YEARS OF AGE, THIS AUTHORIZATION MUST BE SIGNED BY A PARENT OR LEGAL GUARDIAN TO BE VALID. IF THE STUDENT IS 18 YEARS OF AGE OR OVER, THE STUDENT MUST SIGN THIS AUTHORIZATION PERSONALLY.
Studenrs Signature Birth date of Student, induding year
Name of SIUdenrs personal representative, if applicable
I am tie Studenfs (check one): __ Parent __ Legal Guardian (documentation must be provided)
Signature of Student's personal representative, if applicable Dale
A copy of thlsslaned form has bl!n p(Oylded to the student or his/her personal "presentative
020111 Amwfc111 Actdemy of F1mlty Pllyald""- Amlrle~n Ae~demy or PH/Mrlu, Amwfwr Co/Mflt or Sports lltdlclnt, Amwfwr OrtltopHdk Soc:ltty tor SpoiU lltdldn .. Md Am-*'n Osttopalhlc Acldemy of Spotts lltdldnt. Pwmlsslon Is f'lllttd to rtpdnt for noncommetdll, tduclllonll pii'JIO$N wltll edmowltdfllltnt -lfllflud 1113