Embed Size (px)
Citation preview
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 1/23
Official reprint from UpToDate
www.uptodate.com ©2017 UpToDate
Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants
Author: Morven S Edwards, MD
Section Editors: Leonard E Weisman, MD, Sheldon L Kaplan, MD
Deputy Editor: Carrie Armsby, MD, MPH
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Apr 2017. | This topic last updated: Apr 11, 2016.
INTRODUCTION — Sepsis is an important cause of morbidity and mortality among newborn infants.
Although the incidence of sepsis in term and late preterm infants is low, the potential for serious adverse
outcomes, including death, is of such great consequence that caregivers should have a low threshold for
evaluation and treatment for possible sepsis in neonates.
The epidemiology, clinical features, diagnosis, and evaluation of sepsis in term and late preterm infants will be
reviewed here. The management and outcome of sepsis in term and late preterm infants, neonatal sepsis in
preterm infants, and evaluation of febrile and illappearing neonates after discharge from the birth
hospitalization are discussed separately:
TERMINOLOGY — The following terms will be used throughout this discussion on neonatal sepsis:
Sepsis is classified according to the infant's age at the onset of symptoms.
Infants with earlyonset sepsis typically present with symptoms during their birth hospitalization. Term infants
with lateonset sepsis generally present to the outpatient setting or emergency department unless comorbid
conditions have prolonged the birth hospitalization. The approach to evaluation of neonates in the outpatient
setting is discussed separately. (See "Approach to the illappearing infant (younger than 90 days of age)" and
®
®
(See "Management and outcome of sepsis in term and late preterm infants".)
(See "Clinical features and diagnosis of bacterial sepsis in the preterm infant (<34 weeks gestation)".)
(See "Treatment and prevention of bacterial sepsis in the preterm infant (<34 weeks gestation)".)
(See "Febrile infant (younger than 90 days of age): Outpatient evaluation".)
(See "Approach to the illappearing infant (younger than 90 days of age)".)
Neonatal sepsis is a clinical syndrome in an infant 28 days of life or younger, manifested by systemic
signs of infection and isolation of a bacterial pathogen from the blood stream [1]. A consensus definition
for neonatal sepsis is lacking [2]. (See 'Diagnosis' below.)
Term infants are those born at a gestational age of 37 weeks or greater.
Late preterm infants (also called nearterm infants) are those born between 34 and 36 completed
weeks of gestation [3]. (See "Late preterm infants".)
Preterm infants are those born at less than 34 weeks of gestation [3].
Earlyonset sepsis is defined as the onset of symptoms before 7 days of age, although some experts
limit the definition to infections occurring within the first 72 hours of life [4].
Lateonset sepsis is generally defined as the onset of symptoms at ≥7 days of age [4]. Similar to early
onset sepsis, there is variability in its definition, ranging from an onset at >72 hours of life to ≥7 days of
age [4,5].
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 2/23
"Febrile infant (younger than 90 days of age): Management", section on 'Neonates (28 days of age andyounger)'.)
PATHOGENESIS — Earlyonset infection is usually due to vertical transmission by ascending contaminatedamniotic fluid or during vaginal delivery from bacteria in the mother's lower genital tract [6]. Maternalchorioamnionitis is a wellrecognized risk factor for earlyonset neonatal sepsis [7,8]. Maternal group Bstreptococcal (GBS) colonization is another important risk factor. (See 'Maternal risk factors' below and"Group B streptococcal infection in neonates and young infants", section on 'Risk factors'.)
Lateonset infections can be acquired by the following mechanisms:
Disruption of the intact skin or mucosa, which can be due to invasive procedures (eg, intravascular catheter),increases the risk of lateonset infection.
Lateonset sepsis is uncommonly associated with maternal obstetrical complications. Use of forceps duringdelivery and electrodes placed for intrauterine monitoring have been implicated in the pathogenesis of earlyonset sepsis because they penetrate the neonatal defensive epithelial barriers [9].
Metabolic factors, including hypoxia, acidosis, hypothermia, and inherited metabolic disorders (eg,galactosemia), are likely to contribute to risk for and severity of neonatal sepsis. These factors are thought todisrupt the neonate's host defenses (ie, immunologic response) [9].
EPIDEMIOLOGY — The overall incidence of neonatal sepsis ranges from one to five cases per 1000 livebirths. Estimated incidence rates vary based on the case definition and the population studied. Infection ratesincrease with decreasing gestational age. The incidence of earlyonset sepsis has decreased primarily due toreduction in group B streptococcal (GBS) infections owing to the use of intrapartum antibiotic prophylaxis [1014].
The estimated incidence of sepsis (both early and lateonset) in term neonates is one to two cases per 1000live births [15,16]. In a prospective national surveillance study (2006 to 2009), the incidence of earlyonsetsepsis (defined as positive blood or cerebrospinal fluid cultures) was 0.98 cases per 1000 live births; the rateamong infants with birth weight >2500 grams was 0.57 per 1000 [17].
The incidence is higher in late preterm than term infants. In an observational cohort study (1996 to 2007), thereported incidences of early and lateonset sepsis (defined as positive blood culture) in late pretermneonates were 4.4 and 6.3 per 1000, respectively [18].
Earlyonset GBS infection rates in the United States reported through the Centers for Disease Control andPrevention's (CDC) Active Bacterial Core Surveillance Report have declined from 0.6 per 1000 live births in2000 to 0.25 per 1000 live births in 2013 [19,20]. Lateonset GBS infection rates have remained relativelystable in the same interval (0.4 per 1000 live births in 2000 and 0.27 per 1000 live births in 2013).
Black race has been identified as an independent risk factor for early and lateonset GBS sepsis. Reasonsfor the disproportionately high disease burden among black populations cannot be fully explained byprematurity, adequacy of prenatal care, or socioeconomic status [10]. (See "Group B streptococcal infection inneonates and young infants", section on 'Epidemiology'.)
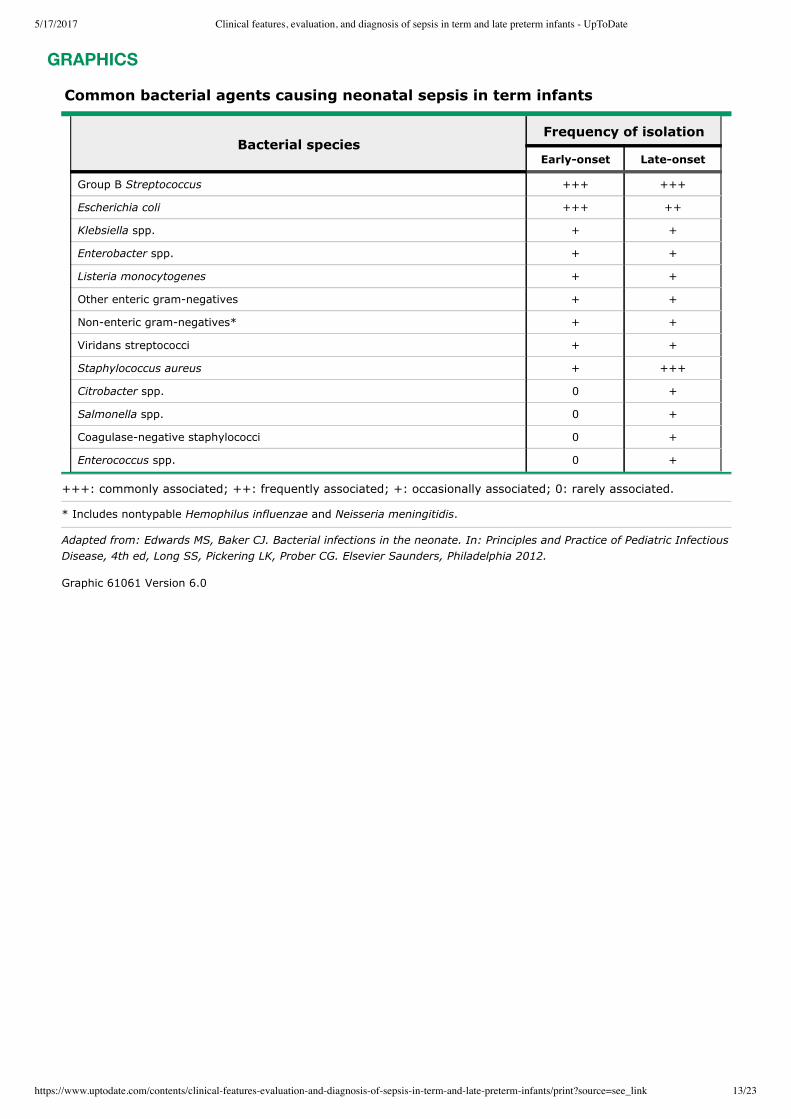
ETIOLOGIC AGENTS — Group B Streptococcus (GBS) and Escherichia coli (E. coli) are the most commoncauses of both early and lateonset sepsis, accounting for approximately twothirds of earlyonset infection[11,21,22].
Other bacterial agents associated with neonatal sepsis include (table 1):
Vertical transmission, resulting in initial neonatal colonization that evolves into later infection
Horizontal transmission from direct contact with care providers or environmental sources
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 3/23
The patterns of pathogens associated with neonatal sepsis have changed over time as reflected bylongitudinal databases from single tertiary centers [11,12]. The incidence of earlyonset GBS has declined by80 percent with the use of intrapartum antibiotic prophylaxis (IAP). IAP appears to also reduce the risk ofearlyonset E. coli infection [27]. (See "Neonatal group B streptococcal disease: Prevention".)
Common nonbacterial agents associated with neonatal sepsis include (see 'Differential diagnosis' below):
MATERNAL RISK FACTORS — The following maternal factors are associated with an increased risk ofsepsis, particularly GBS infection [6,7,28].
Listeria monocytogenes, although a wellrecognized cause of earlyonset sepsis, only accounts for raresporadic cases of neonatal sepsis, and is more commonly seen during an outbreak of listeriosis [23,24].
Staphylococcus aureus (S. aureus), including communityacquired methicillinresistant S. aureus, is anemerging pathogen in neonatal sepsis [25]. Bacteremic staphylococcal infections in term infants oftenoccur in association with skin, bone, or joint sites of involvement.
Enterococcus, a commonly encountered pathogen among preterm infants, is a rare cause of sepsis inotherwise healthy term newborn infants.
Other gramnegative bacteria (including Klebsiella, Enterobacter, and Citrobacter spp.) andPseudomonas aeruginosa are associated with lateonset infection, especially in infants admitted toneonatal intensive care units (NICUs) [26].
Coagulasenegative staphylococci often are a cause of nosocomial infection in ill infants (especiallypremature infants and/or infants who have indwelling intravascular catheters). It may be considered acontaminant in otherwise healthy term infants who have not undergone invasive procedures.
Herpes simplex virus (see "Neonatal herpes simplex virus infection: Clinical features and diagnosis")
Enterovirus and parechovirus (see "Enterovirus and parechovirus infections: Clinical features, laboratorydiagnosis, treatment, and prevention", section on 'Neonates' and "Nosocomial viral infections in theneonatal intensive care unit", section on 'Sepsislike illness and meningitis/encephalitis')
Candida (see "Clinical manifestations and diagnosis of Candida infection in neonates", section on'Systemic infections')
Chorioamnionitis – Chorioamnionitis may reflect intrauterine onset of infection [29]. Consultation withobstetric providers to determine suspicion for chorioamnionitis is an important aspect of neonatalmanagement. (See "Intraamniotic infection (clinical chorioamnionitis or triple I)", section on 'Diagnosis ofintraamniotic infection'.)
Intrapartum maternal temperature ≥38ºC (100.4ºF).
Delivery at <37 weeks gestation.
Maternal GBS colonization and other findings that increase the risk of GBS infection in the neonate,including any of the following:
Positive GBS vaginalrectal screening culture in late gestation during current pregnancy•Previous infant with GBS disease•Documented GBS bacteriuria during the current pregnancy•Intrapartum nucleic acid amplification test positive for GBS•
Membrane rupture ≥18 hours – The risk of proven sepsis increases 10fold to 1 percent whenmembranes are ruptured beyond 18 hours [30].

5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 4/23
GBS screening and maternal intrapartum antibiotic prophylaxis (IAP) reduces the risk of GBS infection butdoes not eliminate it. In a prospective national surveillance study (2006 to 2009), the GBS screening culturewas negative in 81 percent of mothers of term infants with earlyonset GBS [17]. Approximately onehalf ofinfants who developed earlyonset sepsis were born to mothers who received intrapartum antibiotics. (See"Neonatal group B streptococcal disease: Prevention".)
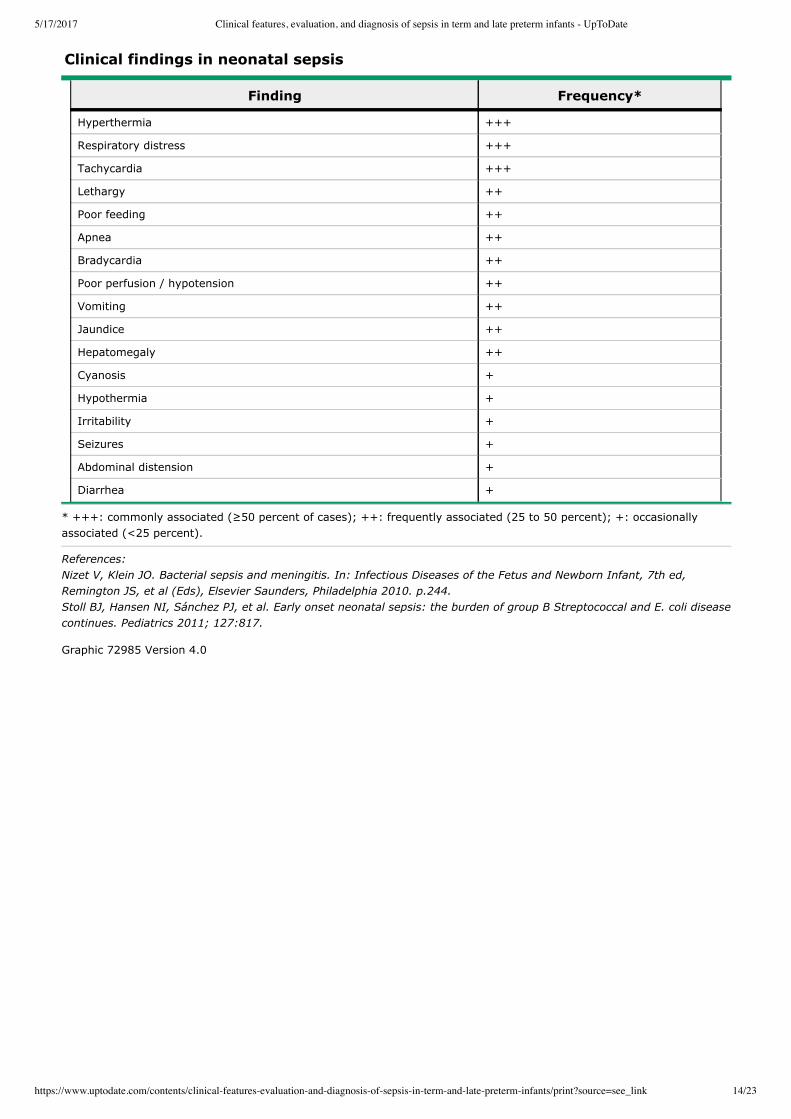
CLINICAL MANIFESTATIONS — Clinical manifestations range from subtle symptoms to profound septicshock. Signs and symptoms of sepsis are nonspecific and include temperature instability (primarily fever),irritability, lethargy, respiratory symptoms (eg, tachypnea, grunting, hypoxia), poor feeding, tachycardia, poorperfusion, and hypotension (table 2) [9].
Because the signs and symptoms of sepsis can be subtle and nonspecific, it is important to identify neonateswith risk factors for sepsis and to have a high index of suspicion for sepsis when an infant deviates from his orher usual pattern of activity or feeding [9].
Signs and symptoms of neonatal sepsis include:
Fetal and delivery room distress – The following signs of fetal and neonatal distress during labor anddelivery may be early indicators of neonatal sepsis:
Intrapartum fetal tachycardia, which may be due to intraamniotic infection. (See "Overview of thegeneral approach to diagnosis and treatment of fetal arrhythmias", section on 'Tachyarrhythmias'.)
•
Meconiumstained amniotic fluid, which is associated with a twofold increased risk of sepsis [7]. (See"Clinical features and diagnosis of meconium aspiration syndrome", section on 'Meconiumpassage'.)
•
Apgar score ≤6, which is associated with a 36fold increased risk of sepsis [31]. (See "Neonatalresuscitation in the delivery room", section on 'Apgar scores'.)
•
Temperature instability – The temperature of an infected infant can be elevated, depressed, or normal.Term infants with sepsis are more likely to be febrile than preterm infants who are more likely to behypothermic [9]. Temperature elevation in fullterm infants is concerning and, if persistent, is highlyindicative of infection [32,33].
Respiratory and cardiocirculatory symptoms – Respiratory and cardiocirculatory symptoms arecommon in infected neonates. Approximately 85 percent of newborns with earlyonset sepsis presentwith respiratory distress (eg, tachypnea, grunting, flaring, use of accessory muscles) [17]. Apnea is lesscommon, occurring in 38 percent of cases, and is more likely in preterm than term infants. Apnea is aclassic presenting symptom in lateonset GBS sepsis. Earlyonset disease can be associated withpersistent pulmonary hypertension of the newborn (PPHN). (See "Persistent pulmonary hypertension ofthe newborn".)
Tachycardia is a common finding in neonatal sepsis but is nonspecific. Bradycardia may also occur. Poorperfusion and hypotension are more sensitive indicators of sepsis but these tend to be late findings. In aprospective national surveillance study, 40 percent of neonates with sepsis required volume expansionand 29 percent required vasopressor support [17].
Neurologic symptoms – Neurologic manifestations of sepsis in the neonate include lethargy, poor tone,poor feeding, irritability, and seizures [9]. Seizures are an uncommon presentation of neonatal sepsis butare associated with a high likelihood of infection. In a prospective study in a single neonatal unit, 38percent of neonates with seizures were found to have sepsis as the etiology [34]. Seizures are apresenting feature in 20 to 50 percent of infants with neonatal meningitis [35]. (See "Bacterial meningitisin the neonate: Clinical features and diagnosis" and "Etiology and prognosis of neonatal seizures".)
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 5/23
EVALUATION AND INITIAL MANAGEMENT — Neonates with signs and symptoms of sepsis require promptevaluation and initiation of antibiotic therapy [6,9]. Because the signs and symptoms of sepsis are subtle andnonspecific, laboratory testing is performed in any infant with identifiable risk factors and/or signs andsymptoms concerning for sepsis. This approach is consistent with guidelines published by the AmericanAcademy of Pediatrics (AAP) and the Center for Disease Control (CDC) [6,36].
Earlyonset sepsis — Evaluation for earlyonset neonatal sepsis should include all of the following:
The extent of the diagnostic evaluation for sepsis is directed by the infant's symptoms and maternal riskfactors.
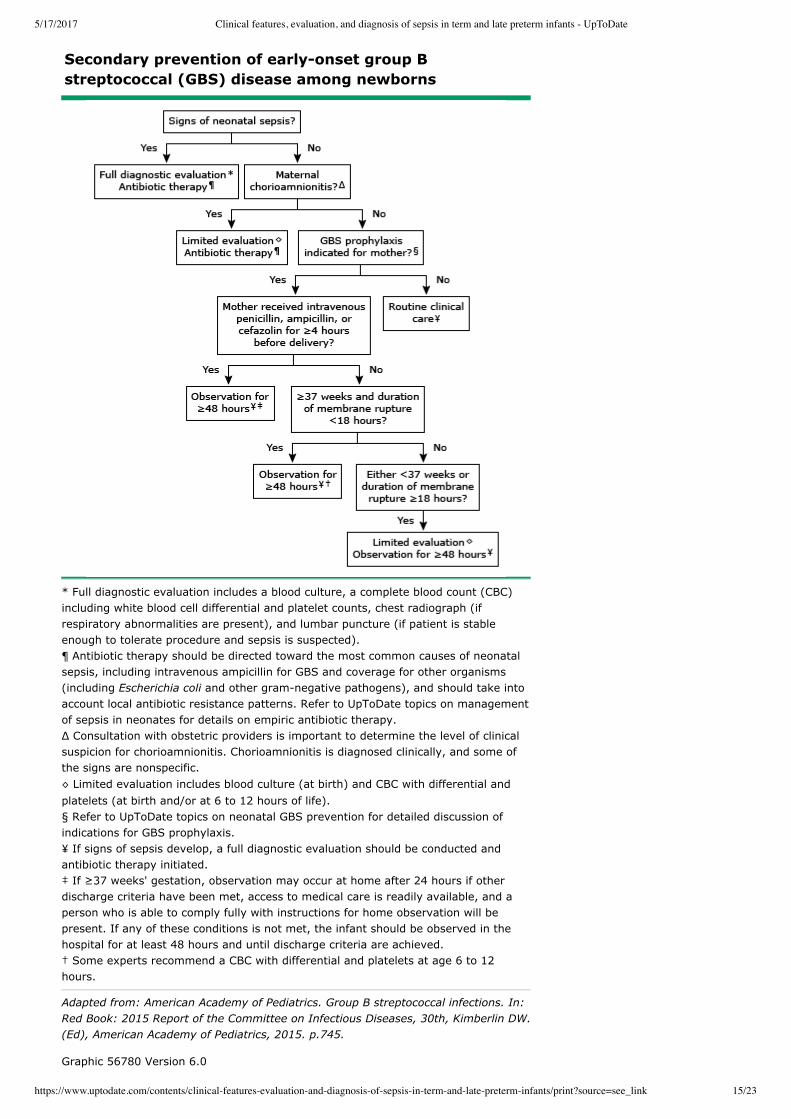
Symptomatic neonates — Infants with signs and symptoms of sepsis should undergo a full diagnosticevaluation and should receive empiric antibiotic treatment (algorithm 1). (See 'Clinical manifestations' aboveand 'Empiric antibiotic therapy' below.)
A full diagnostic evaluation includes (see 'Laboratory tests' below):
Creactive protein (CRP) levels are not routinely required but may be helpful in determining length of therapyif followed serially. (See 'Other inflammatory markers' below.)
Wellappearing neonates — Wellappearing infants with identified risk factors for neonatal sepsis,particularly GBS, should be observed for a minimum of 48 hours. They may require a limited diagnosticevaluation based on the nature of the risk factor and the use and duration of maternal IAP (algorithm 1). (See"Management of the infant whose mother has received group B streptococcal chemoprophylaxis".)
Lateonset sepsis — Infants presenting with signs and symptoms at ≥7 days of age should undergo promptevaluation and empiric antibiotic treatment. (See "Management and outcome of sepsis in term and latepreterm infants", section on 'Lateonset sepsis'.)
A full diagnostic evaluation should be performed. In addition to the tests described above for earlyonsetsepsis, the following should also be obtained:
Other findings – Other findings associated with neonatal sepsis and their approximate frequencies arelisted below (table 2) [9,17]:
Jaundice: 35 percent•Hepatomegaly: 33 percent•Poor feeding: 28 percent•Vomiting: 25 percent•Abdominal distension: 17 percent•Diarrhea: 11 percent•
Review of the pregnancy, labor, and delivery, including risk factors for sepsis and the use and duration ofmaternal intrapartum antibiotic prophylaxis (IAP) (see 'Maternal risk factors' above)
A comprehensive physical examination (see "Assessment of the newborn infant")
Laboratory testing (see 'Laboratory tests' below)
Blood cultureLumbar puncture (if the infant is clinically stable enough to tolerate the procedure)Complete blood count with differential and platelet countChest radiograph (if respiratory symptoms are present)Cultures from tracheal aspirates if intubated
Urine culture
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 6/23
Infants with lateonset sepsis generally present to the outpatient or emergency department setting unlesscomorbid conditions have prolonged the birth hospitalization. (See "Approach to the illappearing infant(younger than 90 days of age)" and "Febrile infant (younger than 90 days of age): Management", section on'Neonates (28 days of age and younger)'.)
Empiric antibiotic therapy — Indications for empiric antibiotic therapy include:
The empiric antibiotic regimen should include agents active against GBS and other organisms that causeneonatal sepsis (eg, E. coli and other gramnegative pathogens). The combination of ampicillin andgentamicin or ampicillin and cefotaxime are potential regimens that provide empiric coverage for theseorganisms until culture results are available. Ampicillin and gentamicin is generally preferred; however, localantibiotic resistance patterns must be considered. In the era of GBS IAP, approximately 30 percent of earlyonset sepsis is due to ampicillinresistant gramnegative organisms [13]. The addition of a thirdgenerationcephalosporin to the empiric treatment of earlyonset sepsis is warranted among neonates with suspectedmeningitis. (See "Management and outcome of sepsis in term and late preterm infants", section on 'Initialempiric therapy'.)
LABORATORY TESTS — The goals of the diagnostic evaluation are to identify and treat all infants withbacterial sepsis, and minimize the treatment of patients who are not infected. Laboratory assessmentincludes cultures of body fluids that confirm the presence or absence of a bacterial pathogen, and otherstudies that are used to evaluate the likelihood of infection.
Blood culture — A definitive diagnosis of neonatal sepsis is established by a positive blood culture. Thesensitivity of a single blood culture to detect neonatal bacteremia is approximately 90 percent.
Cultures from any other potential foci of infection (eg, tracheal aspirates if intubated, purulent eyedrainage, or pustules)
Illappearance (see "Approach to the illappearing infant (younger than 90 days of age)")
Concerning symptoms, including temperature instability, or respiratory, cardiocirculatory, or neurologicsymptoms (see 'Clinical manifestations' above)
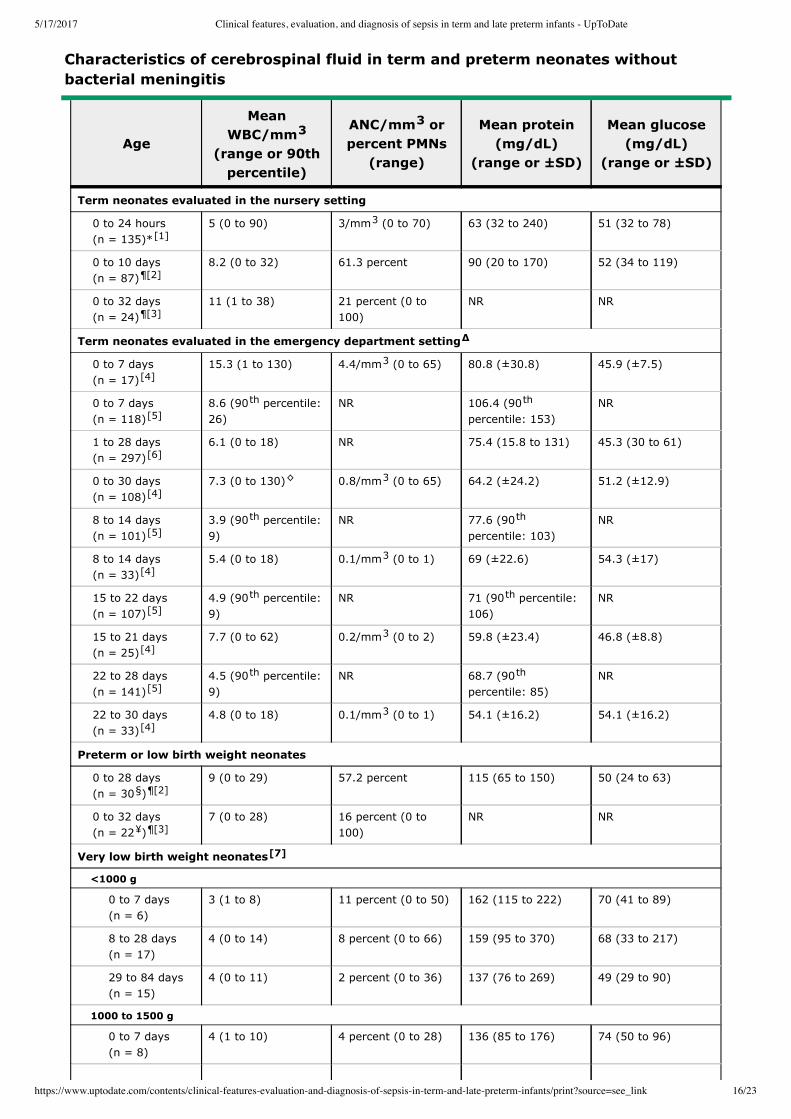
Cerebrospinal fluid (CSF) pleocytosis (white blood cell [WBC] count of >20 to 30 cells/microL) (table 3)(see "Bacterial meningitis in the neonate: Clinical features and diagnosis", section on 'Interpretation ofCSF')
Confirmed or suspected maternal chorioamnionitis (see 'Maternal risk factors' above)
Blood sampling − The following considerations are important when obtaining a blood culture:
Sampling site – Blood cultures can be obtained by venipuncture or arterial puncture, or by samplingfrom a newly inserted umbilical artery or vascular access catheter. Positive culture results of blooddrawn from indwelling umbilical or central venous catheters may indicate contamination or cathetercolonization rather than a true systemic infection [9].
•
Number of cultures – We obtain at least one culture prior to initiating empiric antibiotic therapy inneonates with a high clinical suspicion for sepsis, although other institutions may routinely obtain twoblood cultures. Anaerobic cultures are generally not necessary.
•
Volume of blood – The optimal volume of blood is based on the weight of the infant. A minimum
blood volume of 1 mL is desirable for optimal detection of bacteremia when a single blood culturebottle is used [6]. At the author's institution, the suggested optimal volume is 2 mL for infantsweighing ≤3 kg, and 3 mL for those who weigh >3 to 5 kg. Dividing this volume into two aliquots toinoculate an anaerobic as well as the aerobic culture bottle is discouraged as it is likely to decrease
•
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 7/23
Lumbar puncture — A lumbar puncture (LP) should be performed in neonates undergoing evaluation for
sepsis, because clinical signs suggesting meningitis can be lacking in young infants. When an infant is
critically ill or likely to have cardiovascular or pulmonary compromise from the procedure, the LP can be
deferred until the patient's status has stabilized.
Cerebrospinal fluid (CSF) should be sent for Gram stain, routine culture, cell count with differential, and
protein and glucose concentrations. The interpretation of CSF needs to account for variations due to
gestational age, chronologic age, and birth weight (table 3).
The approach outlined by the 2012 American Academy of Pediatrics (AAP) clinical report recommends that
LP be performed in an infant with any of the following clinical conditions [6]:
Blood culture may be negative in as many as 38 percent of infants with meningitis [6,39]. In a retrospective
study, 8 of the 36 term infants with meningitis had no symptoms referable to the central nervous system, and
had sterile blood cultures [40]. In addition, three infants with both positive CSF and blood cultures were
asymptomatic.
The clinical features and diagnosis of neonatal bacterial meningitis are discussed separately. (See "Bacterial
meningitis in the neonate: Clinical features and diagnosis".)
Urine culture — Urine culture obtained by catheter or bladder tap should be included in the sepsis evaluation
for infants one week of age or older. A urine culture need not be routinely performed in the evaluation of an
infant ≤6 days of age because a positive urine culture in this setting is a reflection of highgrade bacteremia
rather than an isolated urinary tract infection [6,41]. (See "Urinary tract infections in neonates".)
Other cultures — In patients with lateonset infection, cultures should be obtained from any other potential
foci of infection (eg, purulent eye drainage or pustules).
Tracheal aspirates can be of value if obtained immediately after intubation [6]. However, they may reflect
lower respiratory tract colonization rather than indicating a causative pathogen in an infant who has been
intubated for several days.
In infants with earlyonset infection, Gram stains of gastric aspirates are of limited value as are bacterial
cultures of body surface sites (eg, axilla, groin, and external ear canal) [6].
Complete blood count — A complete blood count (CBC) is used to evaluate the likelihood of sepsis in a
neonate with risk factors or signs of infection. Abnormal findings on a CBC cannot be used to establish the
the sensitivity. Anaerobic cultures are generally not necessary and in vitro data suggest that small
sample volumes do not reliably detect low levels of bacteremia [37].
Time to positivity − Automated systems for continuous monitoring of blood cultures are routinely used in
the United States and have shortened the time to identify positive blood cultures. In most cases of
neonatal sepsis, blood cultures become positive within 24 to 36 hours [38].
Distinguishing infection from contamination − A positive blood culture is diagnostic of sepsis when a
known bacterial pathogen is isolated (table 1). Isolation of skin flora (eg, diphtheroids) suggests
contamination rather than infection. Contamination is also suggested when multiple species grow in
culture. Coagulasenegative staphylococci (CoNS) may be pathogenic in patients with indwelling
vascular catheters or other invasive devices, whereas a single blood culture positive for CoNS is likely to
represent a contaminant in fullterm infants without these risk factors [9].
A positive blood culture
Clinical findings that are highly suggestive of sepsis (see 'Clinical manifestations' above)
Laboratory data strongly suggestive of sepsis (see 'Complete blood count' below)
Worsening clinical status while on antibiotic therapy
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 8/23
diagnosis of sepsis.
Earlyonset sepsis — We obtain a CBC in any infant undergoing diagnostic evaluation (either full or
limited) for earlyonset neonatal sepsis. CBC results are used in combination with clinical symptoms and risk
factors to determine the likelihood of sepsis and need for antibiotic treatment.
Abnormal neutrophil indices (including elevated or depressed absolute neutrophil count [ANC] and elevated
ratio of immature to total neutrophil counts [I/T ratio]) are associated with neonatal sepsis. However, these
tests are more useful in identifying neonates who are unlikely to have sepsis than in identifying infants with
sepsis [6].
Two large multicenter studies have evaluated the diagnostic value of CBCs in earlyonset neonatal sepsis
[42,43]. These studies found that low white blood cell count (WBC) (<5000/microL), absolute neutropenia
(ANC <1000 neutrophils/microL), relative neutropenia (ANC <5000 neutrophils/microL), and elevated I/T ratio
were associated with cultureproven sepsis. However, none of the tests were sufficiently sensitive to reliably
predict neonatal sepsis.
CBCs obtained 6 to 12 hours after delivery are more predictive of sepsis than those obtained immediately
after birth because the WBC and ANC normally increase during the first six hours of life [6,42,44].
The following neutrophil indices are used to determine the likelihood of infection:
Lateonset sepsis — CBCs are frequently used to support the diagnosis of lateonset sepsis. In this
setting, CBCs are less variable than in the first days of life. However, WBC indices still perform poorly in
identifying neonates with lateonset sepsis.
I/T ratio − An elevated I/T ratio (≥0.2) has the best sensitivity of the neutrophil indices for predictingneonatal sepsis, and can be helpful as an initial screen when used in combination with risk factors and/or
other tests [7,45,46]. A normal I/T ratio can help rule out sepsis; however, an elevated value is not highly
predictive of sepsis and may be observed in 25 to 50 percent of uninfected infants [6].
In a study of 3154 neonates who underwent evaluation for earlyonset sepsis with blood culture and two
serial WBC measurements, the I/T ratio was ≥0.2 in all 142 neonates with culturepositive or clinical
sepsis as well as in 1473 neonates without infection [47].
The I/T ratio is limited by the wide range of normal values, which reduces its positive predictive value,
especially in asymptomatic patients [48]. Interreader differences in band neutrophil identification with
manual differential counts is another limitation [6]. In addition, exhaustion of the bone marrow reserves,
which may occur during critical illness, will result in low band counts and lead to falsely low ratios. (See
"Evaluating diagnostic tests", section on 'How well does the test perform in specific populations?'.)
Absolute neutrophil count − Although both elevated and low neutrophil counts can be associated withneonatal sepsis, neutropenia has greater specificity, as few conditions other than sepsis and
preeclampsia depress the neutrophil count of neonates [6].
Neutrophil counts vary with gestational age (counts decrease with decreasing gestational age), type of
delivery (counts are lower in infants born by cesarean delivery), site of sampling (counts are lower in
arterial than in venous samples), altitude (counts are higher at elevated altitudes), and timing after
delivery (counts increase during the first six hours of life).
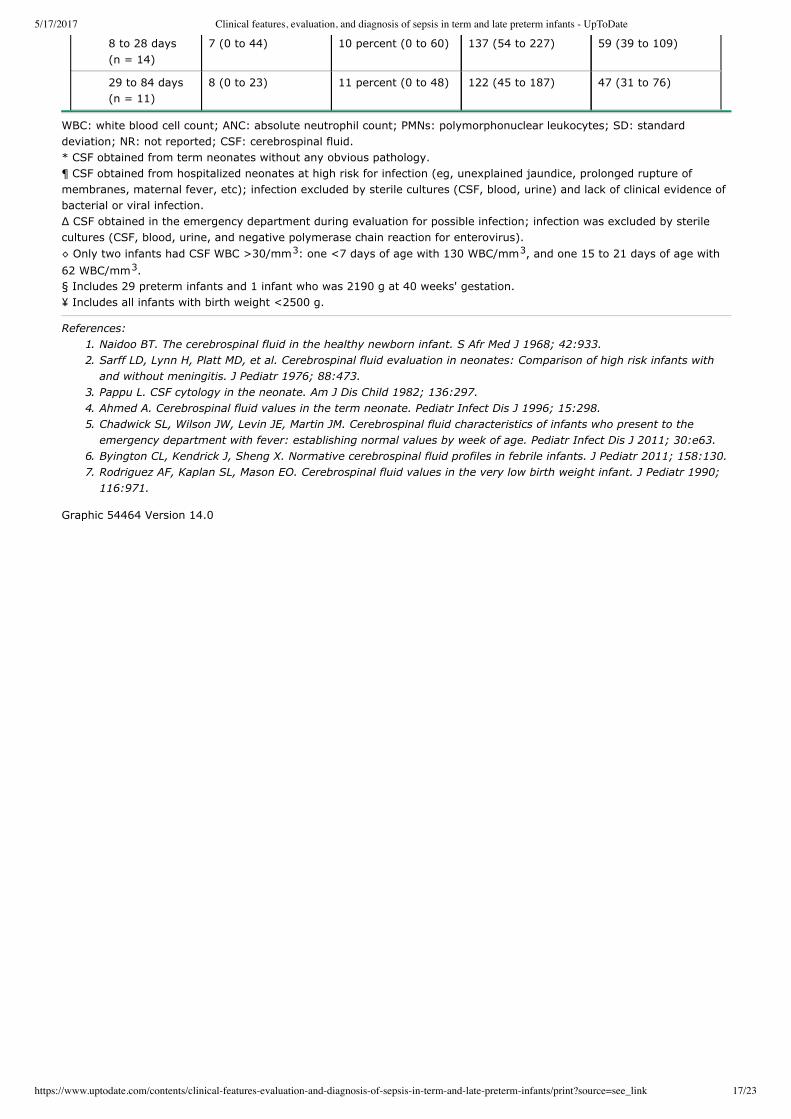
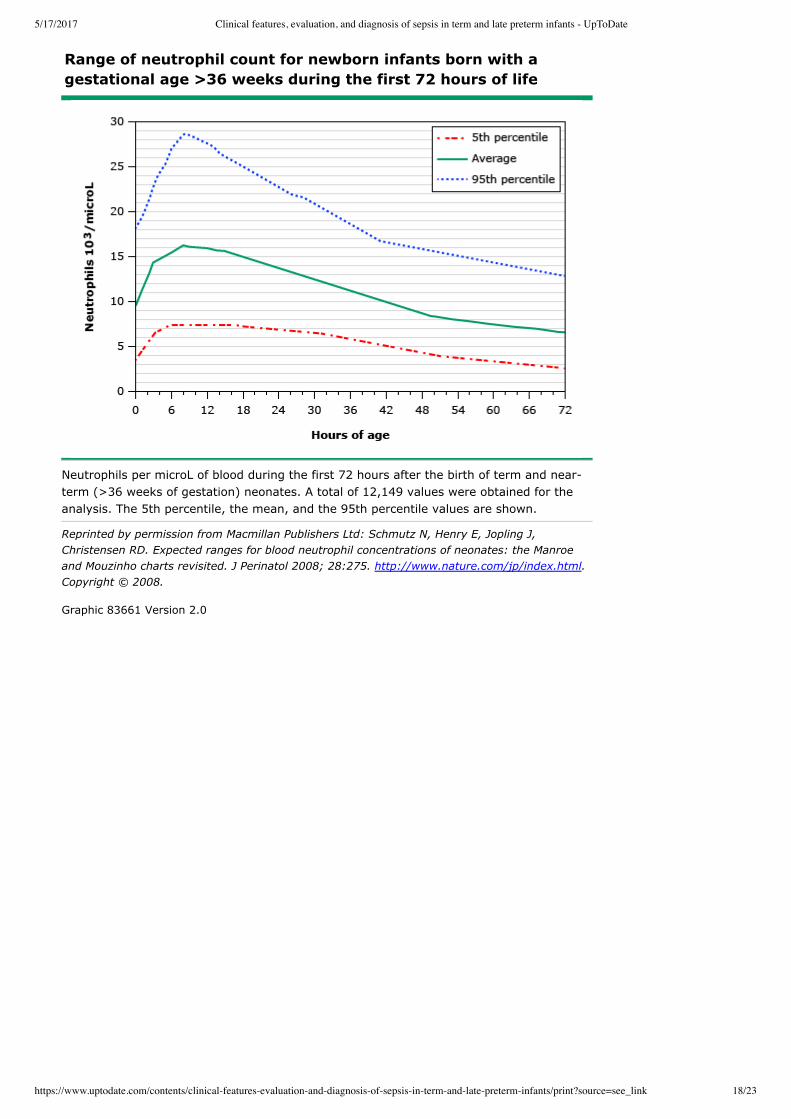
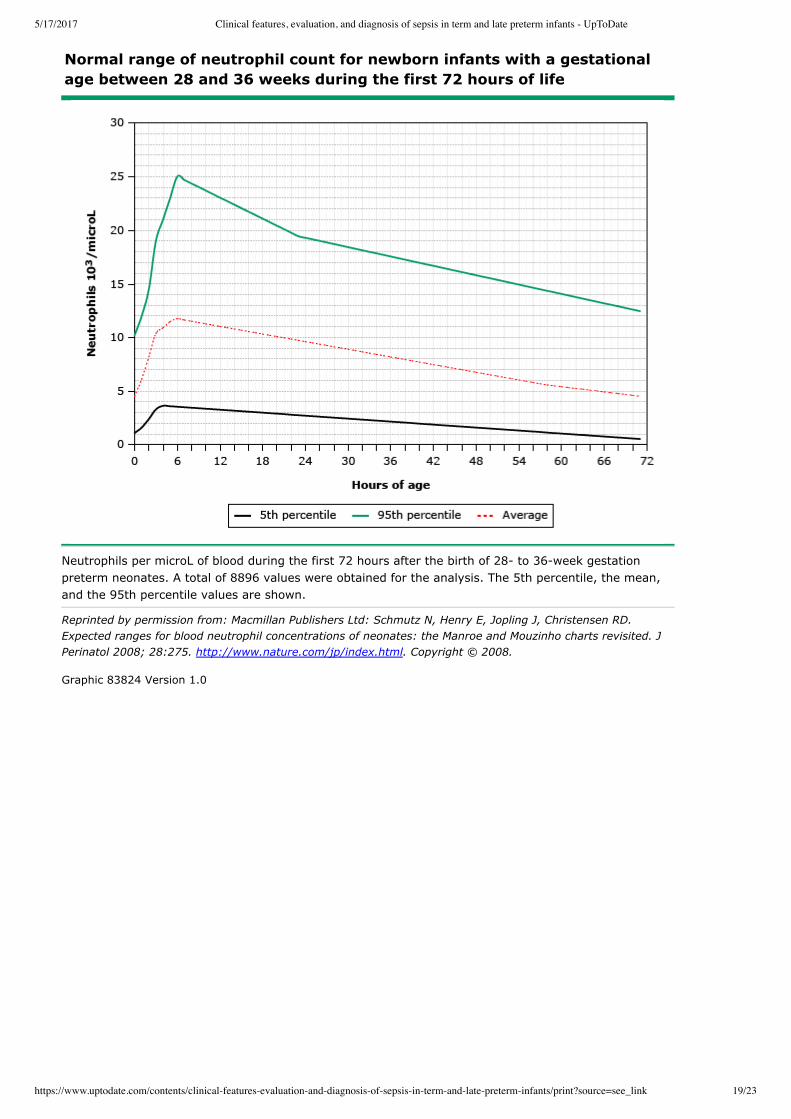
The lower limit of a normal neutrophil count for infants >36 weeks of gestation is 3500/microL at birth and
7500/microL six to eight hours after delivery (figure 1) [49]. For infants born at 28 through 36 weeks of
gestation, the lower limits of normal neutrophil counts at birth and at six to eight hours after birth are
1000/microL and 1500/microL, respectively (figure 2).
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 9/23
In a study of 37,826 neonates (mostly infants continuously hospitalized from birth) who underwent evaluationfor lateonset (defined as 4 to 120 days) sepsis with blood culture and CBC, abnormal WBC (<1000 or>50,000/microL), high absolute neutrophil count (>17,670/microL), elevated I/T ratio (≥0.2), and low plateletcount (<50,000/microL) were associated with culture positivity [50]. However, sensitivity was inadequate toreliably predict lateonset sepsis.
Screening protocols used to identify serious bacterial infections (SBI) in febrile infants two to three months ofage are inadequate in neonates, as they fail to accurately identify neonates with SBI [40]. (See "Febrile infant(younger than 90 days of age): Outpatient evaluation", section on 'Traditional approaches'.)
Other inflammatory markers — A number of acute phase reactants have been used to identify infectednewborns. Many of these tests have a high sensitivity; however, they lack specificity, resulting in a poorpredictive value [51].
Further research aimed at better understanding the neonatal inflammatory response to sepsis may result inthe identification of sensitive and specific markers of inflammation or the development of pathogenspecificrapid diagnostic tests for early detection of neonatal sepsis [56]. With a sensitive and specific marker forsystemic bacterial infection, the management of neonatal sepsis would be significantly altered so thatantimicrobial therapy could be safely withheld in infants for whom sepsis is unlikely.
Creactive protein (CRP) – CRP is increased in inflammatory conditions, including sepsis. A variety ofnoninfectious inflammatory conditions can also cause elevated CRP, including maternal fever, fetaldistress, stressful delivery, perinatal asphyxia, meconium aspiration, and intraventricular hemorrhage[52].
A single measurement of CRP soon after birth is not a useful marker in the diagnosis of neonatal sepsis.However, sequential assessment of CRP values may help support a diagnosis of sepsis. If the CRP levelremains persistently normal (<1 mg/dL [10 mg/L]), neonatal bacterial sepsis is unlikely [6].
CRP levels can be helpful in guiding the duration of antibiotic therapy in suspected neonatal bacterialinfection. Infants with elevated CRP levels that decrease to <1 mg/dL (10 mg/L) 24 to 48 hours afterinitiation of antibiotic therapy typically are not infected and generally do not require further antibiotictreatment if cultures are negative. However, routine use of serial CRP measurements can be associatedwith longer length of hospital stay [53].
An elevated CRP level alone does not justify continuation of empiric antibiotics for more than 48 hours inwellappearing infants with negative culture results [54]. Additional evaluation may be warranted toinvestigate alternative explanations for persistently elevated CRP values.
Procalcitonin – Procalcitonin is the peptide precursor of calcitonin. It is released by parenchymal cells inresponse to bacterial toxins, leading to elevated serum levels in patients with bacterial infections. Severalobservational studies have suggested that procalcitonin may be a useful marker to detect seriousbacterial infections in young febrile infants [55]. Limited data in preterm infants suggest that elevatedprocalcitonin (greater than 0.5 ng/mL [0.5 mcg/L]) is equivalent or better than CRP in detecting bacterialinfection [56]. In a metaanalysis of 16 studies, the pooled sensitivity of procalcitonin for detection ofneonatal sepsis was 81 percent and the specificity was 79 percent [57]. Thus, although procalcitonin is apromising marker, it does not appear to be reliable as the sole or main diagnostic indicator for neonatalsepsis.
Cytokines – Both proinflammatory (interleukin2 [IL2], IL6, IL8, interferon gamma, and tumor necrosisfactor alpha) and antiinflammatory cytokines (IL4 and IL10) are increased in infected infants comparedwith those without infections [56,5860]. However, these cytokines are not routinely measured because ofthe cost of testing and because no single biomarker or panel of tests is sufficiently sensitive to reliablydetect neonatal sepsis [56].

5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 10/23
DIAGNOSIS — The diagnosis of neonatal sepsis can be established only by a positive blood culture. Otherthan blood culture, no specific finding or test reliably identifies infected infants [61].
Ongoing research is focused on developing validated risk stratification strategies based on maternal riskfactors and neonatal presentation that will improve the predictive ability to detect neonatal sepsis [62].
Cultureproven sepsis — The isolation of pathogenic bacteria from a blood culture is the gold standard toconfirm the diagnosis of neonatal sepsis. A positive blood culture is diagnostic of sepsis when a bacterialpathogen is isolated (table 1). Isolation of skin flora (eg, diphtheroids, and coagulasenegative staphylococci)in culture suggests contamination rather than infection, although coagulasenegative staphylococci can bepathogenic in patients with indwelling vascular catheters or other devices [9]. (See 'Blood culture' above and"Management and outcome of sepsis in term and late preterm infants", section on 'Cultureproven sepsis'.)
Probable sepsis — In some cases, a pathogen may not be isolated in culture, yet the neonate has a clinicalcourse that is concerning for sepsis (eg, ongoing temperature instability; ongoing respiratory,cardiocirculatory, or neurologic symptoms not explained by other conditions; or ongoing laboratoryabnormalities suggestive of sepsis [ie, cerebrospinal fluid pleocytosis, elevated ratio of immature to totalneutrophil counts, or elevated Creactive protein]).
A composite of observational assessment and serial laboratory testing is typically used to make a diagnosisof probable sepsis [45]. The criteria used are usually broad, in an attempt to ensure that all infected infantsare identified, but at the cost of testing and treating a number of uninfected infants. There is no consensusdefinition for the diagnosis of probable sepsis in neonates [2].
Alternative diagnoses (table 4) should also be entertained when an infant with suspected sepsis has negativecultures. (See "Management and outcome of sepsis in term and late preterm infants", section on 'Probablebut unproven sepsis' and 'Differential diagnosis' below.)
Infection unlikely — Infants with mild and/or transient symptoms (ie, fever alone or other symptoms thatquickly resolve) who remain wellappearing with normal laboratory values and negative cultures at 48 hoursare unlikely to have sepsis. Empiric antibiotic therapy should be discontinued after 48 hours in theseneonates [6,63].
In a retrospective study of 2785 newborns who underwent evaluation for sepsis based on clinical symptoms(54 percent) or risk factors (46 percent), 22 infants (0.8 percent) were found to have cultureproven sepsisand 40 (1.4 percent) had probable sepsis (ie, culturenegative clinical sepsis) [7].
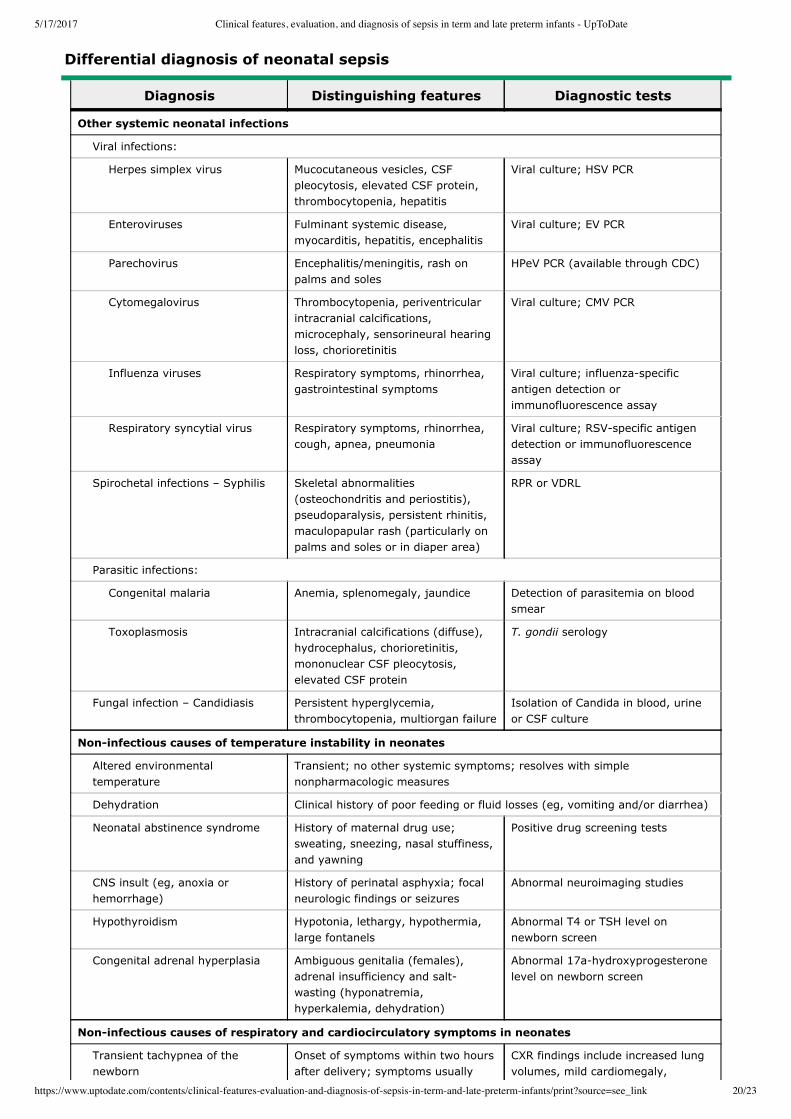
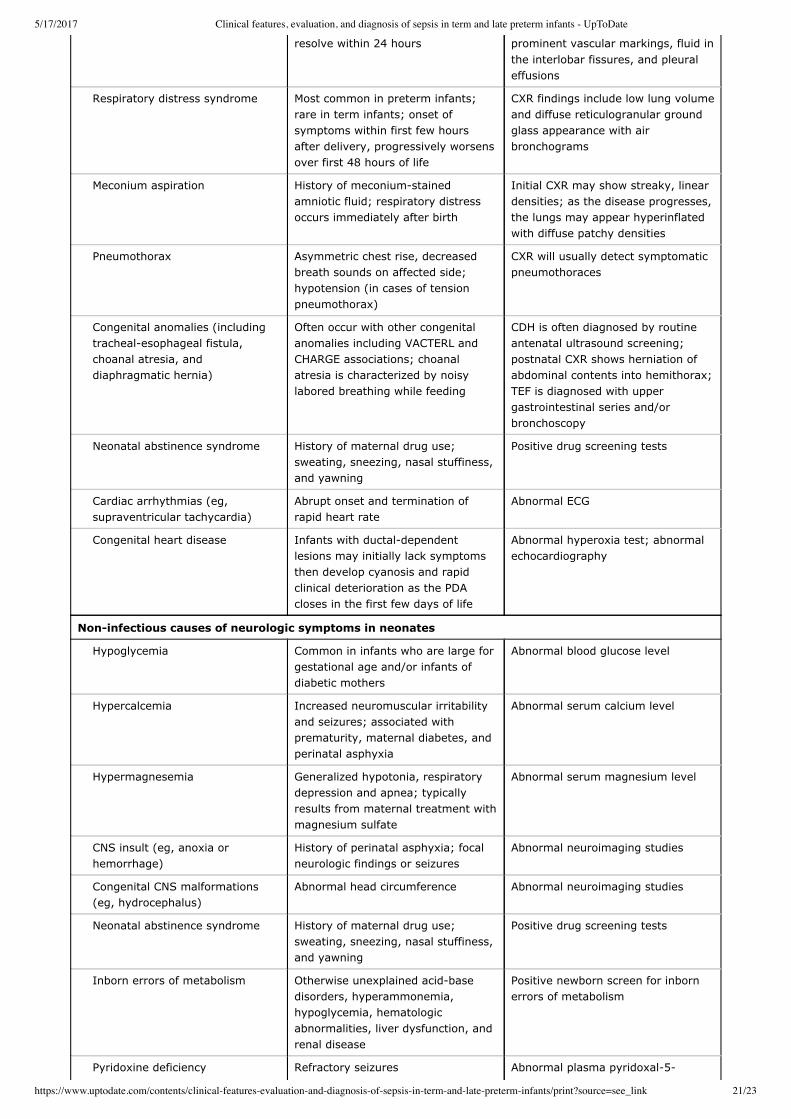
DIFFERENTIAL DIAGNOSIS — The differential diagnosis of neonatal sepsis includes systemic viral, fungal,and parasitic infections and noninfectious causes of temperature instability, and respiratory, cardiocirculatory,and neurologic symptoms (table 4). Appropriate microbiologic testing distinguishes neonatal bacterial sepsisfrom nonbacterial systemic infections. The clinical history, disease course, chest radiograph,electrocardiogram (ECG), hyperoxia testing, drug screening, neuroimaging, blood glucose, serumelectrolytes, and newborn screening may assist in distinguishing noninfectious disorders from neonatalsepsis.
It is often difficult to differentiate neonatal sepsis from other conditions. However, given the morbidity andmortality of neonatal sepsis, empiric antibiotic therapy should be provided (after cultures are obtained) toinfants with suspected sepsis pending definitive culturebased diagnosis.
SOCIETY GUIDELINE LINKS — Links to society and governmentsponsored guidelines from selectedcountries and regions around the world are provided separately. (See "Society guideline links: Sepsis inneonates".)
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics"and "Beyond the Basics." The Basics patient education pieces are written in plain language, at the 5 to 6grade reading level, and they answer the four or five key questions a patient might have about a given
th th
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 11/23
condition. These articles are best for patients who want a general overview and who prefer short, easyto
read materials. Beyond the Basics patient education pieces are longer, more sophisticated, and more
detailed. These articles are written at the 10 to 12 grade reading level and are best for patients who want
indepth information and are comfortable with some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or email
these topics to your patients. (You can also locate patient education articles on a variety of subjects by
searching on "patient info" and the keyword(s) of interest.)
SUMMARY AND RECOMMENDATIONS
th th
Basics topics (see "Patient education: Sepsis in newborn babies (The Basics)")
Although the incidence of sepsis in term and late preterm infants is low (approximately one to six cases
per 1000 births), the potential for serious adverse outcomes, including death, is of such great
consequence that caregivers should have a low threshold for evaluation and treatment for possible
sepsis. (See 'Epidemiology' above.)
Group B Streptococcus (GBS) and Escherichia coli are the most common bacteria causing neonatalsepsis (table 1). (See 'Etiologic agents' above.)
Maternal risk factors for neonatal sepsis in term and late preterm infants include chorioamnionitis,
intrapartum maternal temperature ≥38°C (100.4°F), delivery at <37 weeks gestation, maternal GBS
colonization, and prolonged rupture of membranes (≥18 hours). (See 'Maternal risk factors' above.)
Clinical manifestations are nonspecific and include fetal distress; low apgar score; temperature instability
(usually fever); respiratory and cardiocirculatory symptoms (most commonly respiratory distress and
tachycardia); neurologic symptoms (irritability, lethargy, poor tone, and seizures); and gastrointestinal
abnormalities (poor feeding, vomiting, and abdominal distension) (table 2). (See 'Clinical manifestations'
above.)
Evaluation and initial management of neonates with suspected sepsis should include a review of the
pregnancy, labor, and delivery; complete physical examination; laboratory evaluation; and prompt
initiation of empiric antibiotics. (See 'Evaluation and initial management' above and "Management and
outcome of sepsis in term and late preterm infants", section on 'Initial empiric therapy'.)
Neonates with signs or symptoms of earlyonset sepsis (onset of symptoms before seven days of age)
should undergo a full diagnostic evaluation including blood culture, complete blood count (CBC) with
differential, lumbar puncture, and chest radiograph (if respiratory symptoms are present). Empiric
antibiotics should be provided to these neonates pending blood culture results. (See 'Symptomatic
neonates' above and "Management and outcome of sepsis in term and late preterm infants", section on
'Earlyonset sepsis'.)
Wellappearing newborns born to mothers colonized with GBS require observation for a minimum of 48
hours. The need for a limited diagnostic evaluation (which consists of a blood culture and CBC) in these
asymptomatic infants is determined by the nature of the risk factor(s) and whether or not the mother
received adequate intrapartum antibiotic prophylaxis (IAP) (algorithm 1). Infants born to mothers with
proven or suspected chorioamnionitis should receive empiric antibiotic treatment while awaiting culture
results. (See 'Wellappearing neonates' above and "Management and outcome of sepsis in term and late
preterm infants", section on 'Earlyonset sepsis' and "Management of the infant whose mother has
received group B streptococcal chemoprophylaxis".)
Neonates presenting with signs and symptoms of lateonset sepsis (onset of symptoms from 7 to 28
days of life) should undergo a full diagnostic evaluation (similar to that described above for earlyonset
sepsis, but also including a urine culture and cultures from potential foci of infection [eg, tracheal
aspirates if intubated, purulent eye drainage, or pustules]). Empiric antibiotic treatment should be initiated
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 12/23
Use of UpToDate is subject to the Subscription and License Agreement.
Topic 5043 Version 40.0
in these infants pending blood culture results. (See 'Lateonset sepsis' above and "Management andoutcome of sepsis in term and late preterm infants", section on 'Lateonset sepsis' and "Febrile infant(younger than 90 days of age): Management", section on 'Neonates (28 days of age and younger)'.)
Isolation of a pathogen from a blood culture confirms the diagnosis of neonatal sepsis. (See 'Diagnosis'above and "Management and outcome of sepsis in term and late preterm infants", section on 'Initialempiric therapy'.)
The differential diagnosis of neonatal sepsis includes other systemic infections and noninfectiousconditions including respiratory diseases (eg, transient tachypnea of the newborn and respiratory distresssyndrome); cardiac diseases (eg, congenital heart disease and supraventricular tachycardia); neurologicinjury (eg, from anoxia or hemorrhage); inborn errors of metabolism; and neonatal abstinence syndrome(table 4). (See 'Differential diagnosis' above.)
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 13/23
GRAPHICS
Common bacterial agents causing neonatal sepsis in term infants
Bacterial speciesFrequency of isolation
Earlyonset Lateonset
Group B Streptococcus +++ +++
Escherichia coli +++ ++
Klebsiella spp. + +
Enterobacter spp. + +
Listeria monocytogenes + +
Other enteric gramnegatives + +
Nonenteric gramnegatives* + +
Viridans streptococci + +
Staphylococcus aureus + +++
Citrobacter spp. 0 +
Salmonella spp. 0 +
Coagulasenegative staphylococci 0 +
Enterococcus spp. 0 +
+++: commonly associated; ++: frequently associated; +: occasionally associated; 0: rarely associated.
* Includes nontypable Hemophilus influenzae and Neisseria meningitidis.
Adapted from: Edwards MS, Baker CJ. Bacterial infections in the neonate. In: Principles and Practice of Pediatric Infectious
Disease, 4th ed, Long SS, Pickering LK, Prober CG. Elsevier Saunders, Philadelphia 2012.
Graphic 61061 Version 6.0
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 14/23
Clinical findings in neonatal sepsis
Finding Frequency*
Hyperthermia +++
Respiratory distress +++
Tachycardia +++
Lethargy ++
Poor feeding ++
Apnea ++
Bradycardia ++
Poor perfusion / hypotension ++
Vomiting ++
Jaundice ++
Hepatomegaly ++
Cyanosis +
Hypothermia +
Irritability +
Seizures +
Abdominal distension +
Diarrhea +
* +++: commonly associated (≥50 percent of cases); ++: frequently associated (25 to 50 percent); +: occasionally
associated (<25 percent).
References: Nizet V, Klein JO. Bacterial sepsis and meningitis. In: Infectious Diseases of the Fetus and Newborn Infant, 7th ed,Remington JS, et al (Eds), Elsevier Saunders, Philadelphia 2010. p.244. Stoll BJ, Hansen NI, Sánchez PJ, et al. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli diseasecontinues. Pediatrics 2011; 127:817.
Graphic 72985 Version 4.0
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 15/23
Secondary prevention of earlyonset group Bstreptococcal (GBS) disease among newborns
* Full diagnostic evaluation includes a blood culture, a complete blood count (CBC)including white blood cell differential and platelet counts, chest radiograph (ifrespiratory abnormalities are present), and lumbar puncture (if patient is stableenough to tolerate procedure and sepsis is suspected). ¶ Antibiotic therapy should be directed toward the most common causes of neonatalsepsis, including intravenous ampicillin for GBS and coverage for other organisms(including Escherichia coli and other gramnegative pathogens), and should take intoaccount local antibiotic resistance patterns. Refer to UpToDate topics on managementof sepsis in neonates for details on empiric antibiotic therapy. Δ Consultation with obstetric providers is important to determine the level of clinicalsuspicion for chorioamnionitis. Chorioamnionitis is diagnosed clinically, and some ofthe signs are nonspecific. ◊ Limited evaluation includes blood culture (at birth) and CBC with differential andplatelets (at birth and/or at 6 to 12 hours of life). § Refer to UpToDate topics on neonatal GBS prevention for detailed discussion ofindications for GBS prophylaxis. ¥ If signs of sepsis develop, a full diagnostic evaluation should be conducted andantibiotic therapy initiated. ‡ If ≥37 weeks' gestation, observation may occur at home after 24 hours if otherdischarge criteria have been met, access to medical care is readily available, and aperson who is able to comply fully with instructions for home observation will bepresent. If any of these conditions is not met, the infant should be observed in thehospital for at least 48 hours and until discharge criteria are achieved. † Some experts recommend a CBC with differential and platelets at age 6 to 12hours.
Adapted from: American Academy of Pediatrics. Group B streptococcal infections. In:Red Book: 2015 Report of the Committee on Infectious Diseases, 30th, Kimberlin DW.(Ed), American Academy of Pediatrics, 2015. p.745.
Graphic 56780 Version 6.0
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 16/23
Characteristics of cerebrospinal fluid in term and preterm neonates withoutbacterial meningitis
Age
MeanWBC/mm
(range or 90thpercentile)
ANC/mm orpercent PMNs (range)
Mean protein(mg/dL)
(range or ±SD)
Mean glucose(mg/dL)
(range or ±SD)
Term neonates evaluated in the nursery setting
0 to 24 hours (n = 135)*
5 (0 to 90) 3/mm (0 to 70) 63 (32 to 240) 51 (32 to 78)
0 to 10 days (n = 87)
8.2 (0 to 32) 61.3 percent 90 (20 to 170) 52 (34 to 119)
0 to 32 days (n = 24)
11 (1 to 38) 21 percent (0 to100)
NR NR
Term neonates evaluated in the emergency department setting
0 to 7 days (n = 17)
15.3 (1 to 130) 4.4/mm (0 to 65) 80.8 (±30.8) 45.9 (±7.5)
0 to 7 days (n = 118)
8.6 (90 percentile:26)
NR 106.4 (90percentile: 153)
NR
1 to 28 days (n = 297)
6.1 (0 to 18) NR 75.4 (15.8 to 131) 45.3 (30 to 61)
0 to 30 days (n = 108)
7.3 (0 to 130) 0.8/mm (0 to 65) 64.2 (±24.2) 51.2 (±12.9)
8 to 14 days (n = 101)
3.9 (90 percentile:9)
NR 77.6 (90percentile: 103)
NR
8 to 14 days (n = 33)
5.4 (0 to 18) 0.1/mm (0 to 1) 69 (±22.6) 54.3 (±17)
15 to 22 days (n = 107)
4.9 (90 percentile:9)
NR 71 (90 percentile:106)
NR
15 to 21 days (n = 25)
7.7 (0 to 62) 0.2/mm (0 to 2) 59.8 (±23.4) 46.8 (±8.8)
22 to 28 days (n = 141)
4.5 (90 percentile:9)
NR 68.7 (90percentile: 85)
NR
22 to 30 days (n = 33)
4.8 (0 to 18) 0.1/mm (0 to 1) 54.1 (±16.2) 54.1 (±16.2)
Preterm or low birth weight neonates
0 to 28 days (n = 30 )
9 (0 to 29) 57.2 percent 115 (65 to 150) 50 (24 to 63)
0 to 32 days (n = 22 )
7 (0 to 28) 16 percent (0 to100)
NR NR
Very low birth weight neonates
<1000 g
0 to 7 days (n = 6)
3 (1 to 8) 11 percent (0 to 50) 162 (115 to 222) 70 (41 to 89)
8 to 28 days (n = 17)
4 (0 to 14) 8 percent (0 to 66) 159 (95 to 370) 68 (33 to 217)
29 to 84 days (n = 15)
4 (0 to 11) 2 percent (0 to 36) 137 (76 to 269) 49 (29 to 90)
1000 to 1500 g
0 to 7 days (n = 8)
4 (1 to 10) 4 percent (0 to 28) 136 (85 to 176) 74 (50 to 96)
33
[1]3
¶[2]
¶[3]
Δ
[4]3
[5]th th
[6]
[4]◊ 3
[5]th th
[4]3
[5]th th
[4]3
[5]th th
[4]3
§ ¶[2]
¥ ¶[3]
[7]
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 17/23
8 to 28 days
(n = 14)
7 (0 to 44) 10 percent (0 to 60) 137 (54 to 227) 59 (39 to 109)
29 to 84 days
(n = 11)
8 (0 to 23) 11 percent (0 to 48) 122 (45 to 187) 47 (31 to 76)
WBC: white blood cell count; ANC: absolute neutrophil count; PMNs: polymorphonuclear leukocytes; SD: standard
deviation; NR: not reported; CSF: cerebrospinal fluid.
* CSF obtained from term neonates without any obvious pathology.
¶ CSF obtained from hospitalized neonates at high risk for infection (eg, unexplained jaundice, prolonged rupture of
membranes, maternal fever, etc); infection excluded by sterile cultures (CSF, blood, urine) and lack of clinical evidence of
bacterial or viral infection.
Δ CSF obtained in the emergency department during evaluation for possible infection; infection was excluded by sterile
cultures (CSF, blood, urine, and negative polymerase chain reaction for enterovirus).
◊ Only two infants had CSF WBC >30/mm : one <7 days of age with 130 WBC/mm , and one 15 to 21 days of age with
62 WBC/mm .
§ Includes 29 preterm infants and 1 infant who was 2190 g at 40 weeks' gestation.
¥ Includes all infants with birth weight <2500 g.
References: 1. Naidoo BT. The cerebrospinal fluid in the healthy newborn infant. S Afr Med J 1968; 42:933.2. Sarff LD, Lynn H, Platt MD, et al. Cerebrospinal fluid evaluation in neonates: Comparison of high risk infants withand without meningitis. J Pediatr 1976; 88:473.
3. Pappu L. CSF cytology in the neonate. Am J Dis Child 1982; 136:297.4. Ahmed A. Cerebrospinal fluid values in the term neonate. Pediatr Infect Dis J 1996; 15:298.5. Chadwick SL, Wilson JW, Levin JE, Martin JM. Cerebrospinal fluid characteristics of infants who present to theemergency department with fever: establishing normal values by week of age. Pediatr Infect Dis J 2011; 30:e63.
6. Byington CL, Kendrick J, Sheng X. Normative cerebrospinal fluid profiles in febrile infants. J Pediatr 2011; 158:130.7. Rodriguez AF, Kaplan SL, Mason EO. Cerebrospinal fluid values in the very low birth weight infant. J Pediatr 1990;116:971.
Graphic 54464 Version 14.0
3 3
3
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 18/23
Range of neutrophil count for newborn infants born with agestational age >36 weeks during the first 72 hours of life
Neutrophils per microL of blood during the first 72 hours after the birth of term and nearterm (>36 weeks of gestation) neonates. A total of 12,149 values were obtained for theanalysis. The 5th percentile, the mean, and the 95th percentile values are shown.
Reprinted by permission from Macmillan Publishers Ltd: Schmutz N, Henry E, Jopling J,
Christensen RD. Expected ranges for blood neutrophil concentrations of neonates: the Manroe
and Mouzinho charts revisited. J Perinatol 2008; 28:275. http://www.nature.com/jp/index.html.
Copyright © 2008.
Graphic 83661 Version 2.0
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 19/23
Normal range of neutrophil count for newborn infants with a gestationalage between 28 and 36 weeks during the first 72 hours of life
Neutrophils per microL of blood during the first 72 hours after the birth of 28 to 36week gestationpreterm neonates. A total of 8896 values were obtained for the analysis. The 5th percentile, the mean,and the 95th percentile values are shown.
Reprinted by permission from: Macmillan Publishers Ltd: Schmutz N, Henry E, Jopling J, Christensen RD.
Expected ranges for blood neutrophil concentrations of neonates: the Manroe and Mouzinho charts revisited. J
Perinatol 2008; 28:275. http://www.nature.com/jp/index.html. Copyright © 2008.
Graphic 83824 Version 1.0
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 20/23
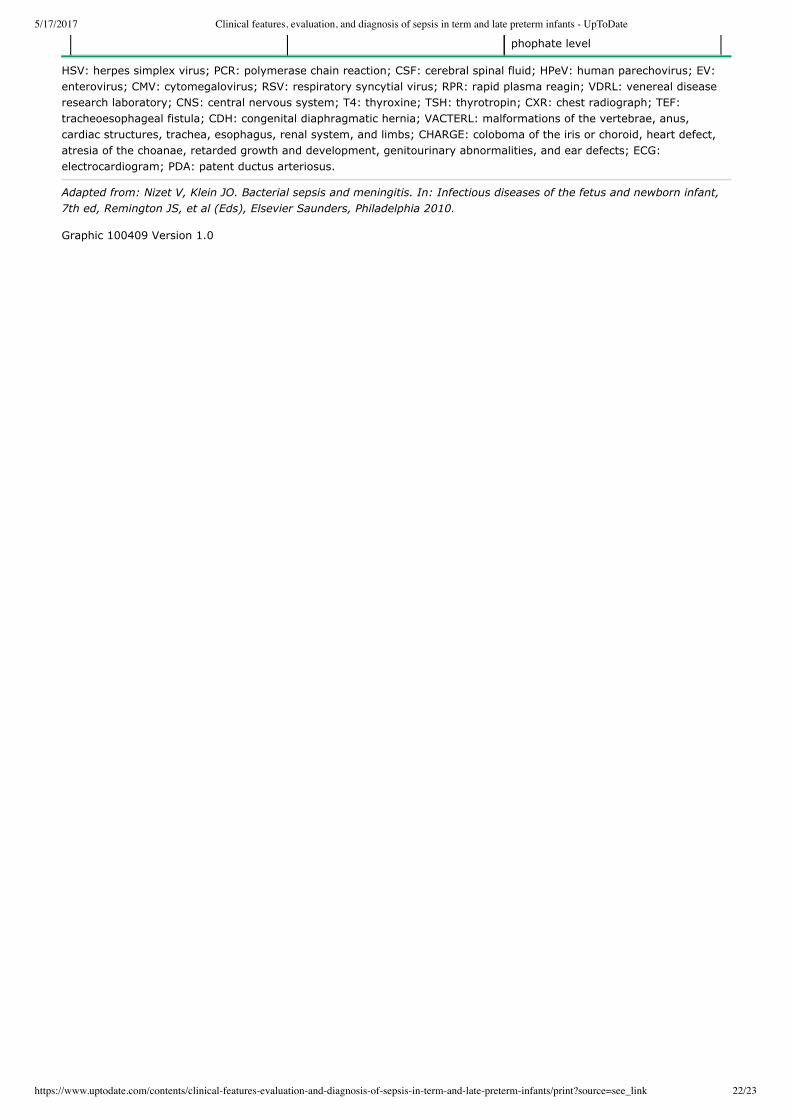
Differential diagnosis of neonatal sepsis
Diagnosis Distinguishing features Diagnostic tests
Other systemic neonatal infections
Viral infections:
Herpes simplex virus Mucocutaneous vesicles, CSFpleocytosis, elevated CSF protein,thrombocytopenia, hepatitis
Viral culture; HSV PCR
Enteroviruses Fulminant systemic disease,myocarditis, hepatitis, encephalitis
Viral culture; EV PCR
Parechovirus Encephalitis/meningitis, rash onpalms and soles
HPeV PCR (available through CDC)
Cytomegalovirus Thrombocytopenia, periventricularintracranial calcifications,microcephaly, sensorineural hearingloss, chorioretinitis
Viral culture; CMV PCR
Influenza viruses Respiratory symptoms, rhinorrhea,gastrointestinal symptoms
Viral culture; influenzaspecificantigen detection orimmunofluorescence assay
Respiratory syncytial virus Respiratory symptoms, rhinorrhea,cough, apnea, pneumonia
Viral culture; RSVspecific antigendetection or immunofluorescenceassay
Spirochetal infections – Syphilis Skeletal abnormalities(osteochondritis and periostitis),pseudoparalysis, persistent rhinitis,maculopapular rash (particularly onpalms and soles or in diaper area)
RPR or VDRL
Parasitic infections:
Congenital malaria Anemia, splenomegaly, jaundice Detection of parasitemia on bloodsmear
Toxoplasmosis Intracranial calcifications (diffuse),hydrocephalus, chorioretinitis,mononuclear CSF pleocytosis,elevated CSF protein
T. gondii serology
Fungal infection – Candidiasis Persistent hyperglycemia,thrombocytopenia, multiorgan failure
Isolation of Candida in blood, urineor CSF culture
Noninfectious causes of temperature instability in neonates
Altered environmentaltemperature
Transient; no other systemic symptoms; resolves with simplenonpharmacologic measures
Dehydration Clinical history of poor feeding or fluid losses (eg, vomiting and/or diarrhea)
Neonatal abstinence syndrome History of maternal drug use;sweating, sneezing, nasal stuffiness,and yawning
Positive drug screening tests
CNS insult (eg, anoxia orhemorrhage)
History of perinatal asphyxia; focalneurologic findings or seizures
Abnormal neuroimaging studies
Hypothyroidism Hypotonia, lethargy, hypothermia,large fontanels
Abnormal T4 or TSH level onnewborn screen
Congenital adrenal hyperplasia Ambiguous genitalia (females),adrenal insufficiency and saltwasting (hyponatremia,hyperkalemia, dehydration)
Abnormal 17ahydroxyprogesteronelevel on newborn screen
Noninfectious causes of respiratory and cardiocirculatory symptoms in neonates
Transient tachypnea of thenewborn
Onset of symptoms within two hoursafter delivery; symptoms usually
CXR findings include increased lungvolumes, mild cardiomegaly,
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 21/23
resolve within 24 hours prominent vascular markings, fluid inthe interlobar fissures, and pleuraleffusions
Respiratory distress syndrome Most common in preterm infants;rare in term infants; onset ofsymptoms within first few hoursafter delivery, progressively worsensover first 48 hours of life
CXR findings include low lung volumeand diffuse reticulogranular groundglass appearance with airbronchograms
Meconium aspiration History of meconiumstainedamniotic fluid; respiratory distressoccurs immediately after birth
Initial CXR may show streaky, lineardensities; as the disease progresses,the lungs may appear hyperinflatedwith diffuse patchy densities
Pneumothorax Asymmetric chest rise, decreasedbreath sounds on affected side;hypotension (in cases of tensionpneumothorax)
CXR will usually detect symptomaticpneumothoraces
Congenital anomalies (includingtrachealesophageal fistula,choanal atresia, anddiaphragmatic hernia)
Often occur with other congenitalanomalies including VACTERL andCHARGE associations; choanalatresia is characterized by noisylabored breathing while feeding
CDH is often diagnosed by routineantenatal ultrasound screening;postnatal CXR shows herniation ofabdominal contents into hemithorax;TEF is diagnosed with uppergastrointestinal series and/orbronchoscopy
Neonatal abstinence syndrome History of maternal drug use;sweating, sneezing, nasal stuffiness,and yawning
Positive drug screening tests
Cardiac arrhythmias (eg,supraventricular tachycardia)
Abrupt onset and termination ofrapid heart rate
Abnormal ECG
Congenital heart disease Infants with ductaldependentlesions may initially lack symptomsthen develop cyanosis and rapidclinical deterioration as the PDAcloses in the first few days of life
Abnormal hyperoxia test; abnormalechocardiography
Noninfectious causes of neurologic symptoms in neonates
Hypoglycemia Common in infants who are large forgestational age and/or infants ofdiabetic mothers
Abnormal blood glucose level
Hypercalcemia Increased neuromuscular irritabilityand seizures; associated withprematurity, maternal diabetes, andperinatal asphyxia
Abnormal serum calcium level
Hypermagnesemia Generalized hypotonia, respiratorydepression and apnea; typicallyresults from maternal treatment withmagnesium sulfate
Abnormal serum magnesium level
CNS insult (eg, anoxia orhemorrhage)
History of perinatal asphyxia; focalneurologic findings or seizures
Abnormal neuroimaging studies
Congenital CNS malformations(eg, hydrocephalus)
Abnormal head circumference Abnormal neuroimaging studies
Neonatal abstinence syndrome History of maternal drug use;sweating, sneezing, nasal stuffiness,and yawning
Positive drug screening tests
Inborn errors of metabolism Otherwise unexplained acidbasedisorders, hyperammonemia,hypoglycemia, hematologicabnormalities, liver dysfunction, andrenal disease
Positive newborn screen for inbornerrors of metabolism
Pyridoxine deficiency Refractory seizures Abnormal plasma pyridoxal5
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 22/23
phophate level
HSV: herpes simplex virus; PCR: polymerase chain reaction; CSF: cerebral spinal fluid; HPeV: human parechovirus; EV:
enterovirus; CMV: cytomegalovirus; RSV: respiratory syncytial virus; RPR: rapid plasma reagin; VDRL: venereal disease
research laboratory; CNS: central nervous system; T4: thyroxine; TSH: thyrotropin; CXR: chest radiograph; TEF:
tracheoesophageal fistula; CDH: congenital diaphragmatic hernia; VACTERL: malformations of the vertebrae, anus,
cardiac structures, trachea, esophagus, renal system, and limbs; CHARGE: coloboma of the iris or choroid, heart defect,
atresia of the choanae, retarded growth and development, genitourinary abnormalities, and ear defects; ECG:
electrocardiogram; PDA: patent ductus arteriosus.
Adapted from: Nizet V, Klein JO. Bacterial sepsis and meningitis. In: Infectious diseases of the fetus and newborn infant,
7th ed, Remington JS, et al (Eds), Elsevier Saunders, Philadelphia 2010.
Graphic 100409 Version 1.0
5/17/2017 Clinical features, evaluation, and diagnosis of sepsis in term and late preterm infants - UpToDate
https://www.uptodate.com/contents/clinical-features-evaluation-and-diagnosis-of-sepsis-in-term-and-late-preterm-infants/print?source=see_link 23/23
Contributor DisclosuresMorven S Edwards, MD Grant/Research/Clinical Trial Support: Pfizer Inc. [Group B
Streptococcus]. Leonard E Weisman, MD Grant/Research/Clinical Trial Support: Vax-Immune [Ureaplasmadiagnosis, vaccines, antibodies, other medical diagnostics and pre-analytical devices]. Consultant/AdvisoryBoards: Glaxo-Smith Kline [Malaria vaccine]; NIAID [Staphylococcus aureus (Mupirocin)]. Patent Holder:Baylor College of Medicine [Ureaplasma diagnosis, vaccines, antibodies, process for preparing biologicalsamples]. Equity Ownership/Stock Options: Vax-Immune [Ureaplasma diagnosis, vaccines, antibodies, othermedical diagnostics and pre-analytical devices]. Equity Ownership/Stock Options (Spouse): Vax-Immune[Ureaplasma diagnosis, vaccines, antibodies, other medical diagnostics and pre-analyticaldevices]. Sheldon L Kaplan, MD Grant/Research/Clinical Trial Support: Pfizer [S. pneumoniae (PCV13,Linezolid)]; Cubist [S. aureus (Tedizolid)]; Forest Lab [Osteomyelitis (Ceftaroline)]. Consultant/AdvisoryBoards: Pfizer [S. pneumoniae (PCV13, Linezolid); S. aureus (vaccine development)]; Theravance [S. aureus(Telavancin)]. Carrie Armsby, MD, MPH Nothing to disclose
Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these areaddressed by vetting through a multi-level review process, and through requirements for references to beprovided to support the content. Appropriately referenced content is required of all authors and mustconform to UpToDate standards of evidence.
Conflict of interest policy