Embed Size (px)
Citation preview

Official reprint from UpToDate® www.uptodate.com ©2013 UpToDate®
AuthorsMarco L A Sivilotti, MD, MSc, FRCPC,FACEP, FACMTJames F Winchester, MD
Section EditorsStephen J Traub, MDMichele Burns Ewald, MD
Deputy EditorJonathan Grayzel, MD, FAAEM
Methanol and ethylene glycol poisoning
Disclosures
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Dec 2012. | This topic last updated: Feb 13, 2012.
INTRODUCTION — Methanol and ethylene glycol poisonings cause dozens of fatal intoxications in the UnitedStates (US) annually, and even relatively small ingestions of these alcohols can produce significant toxicity. Rapidrecognition and early treatment, including alcohol dehydrogenase inhibition, are crucial. A summary table tofacilitate emergent management is provided (table 1).
Methanol and ethylene glycol are frequently found in high concentration in automotive antifreeze and de-icingsolutions, windshield wiper fluid, solvents, cleaners, fuels, and other industrial products. Most serious poisoningsoccur following ingestion; inhalation and dermal exposures rarely cause toxicity.
Patients may ingest toxic alcohols as an ethanol substitute, to inflict self-harm, or by accident, sometimes followingtransfer from the original container. Multiple victim methanol poisonings can occur with illicit distillation ("moonshine")or occult substitution for ethanol.
To provide proper management, clinicians must understand the metabolic activation of these alcohols to their toxicacid metabolites, the limitations of available laboratory tests, and the indications for treatment with antidotes, with orwithout hemodialysis.
The diagnosis and management of methanol and ethylene glycol intoxication will be reviewed here. Isopropyl alcoholintoxication and a general approach to the poisoned adult or child are discussed separately. (See "Isopropyl alcoholpoisoning" and "General approach to drug poisoning in adults" and "Approach to the child with occult toxicexposure".)
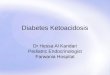
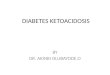
PHARMACOLOGY AND CELLULAR TOXICOLOGY — The "parent alcohols" methanol and ethylene glycol arerelatively nontoxic, and cause mainly central nervous system (CNS) sedation. However, profound toxicity can ensuewhen these parent alcohols are oxidized (primarily by alcohol dehydrogenase and aldehyde dehydrogenase) (figure1 and figure 2).
The methanol metabolite formate and the ethylene glycol metabolites glycolate, glyoxylate, and oxalate accumulatefollowing large ingestions. Above plasma levels of approximately 20 mg/dL (approximately 6 mmol/L of methanol or3 mmol/L of ethylene glycol), these metabolites can cause specific end-organ damage [1-5]:
Formate causes retinal injury with optic disc hyperemia, edema, and eventually permanent blindness, as wellas ischemic or hemorrhagic injury to the basal ganglia [6]. These changes are postulated to result fromdisruption of mitochondrial function.
Ethylene glycol metabolites target the kidney and lead to reversible oliguric or anuric acute kidney injury(acute renal failure), which in turn slows elimination of ethylene glycol [7]. The renal failure is primarily due toglycolate-induced damage to tubules, although tubule obstruction from precipitated oxalate crystals maycontribute [8,9]. Hypocalcemia in ethylene glycol overdose results from calcium oxalate formation.
With ingestions of either parent alcohol, a profound anion gap metabolic acidosis develops, which directly correlateswith the accumulation of toxic acid metabolites [2,4]. Acidemia increases the ability of the toxic metabolites topenetrate cells, further depressing CNS function and causing a rapid downward spiral of hypoxia and acidemia [10].

KINETICS — Like other simple alcohols, methanol and ethylene glycol are rapidly and completely absorbed afteroral ingestion. Peak serum alcohol concentrations are reached within one to two hours. Two-step metabolism viaalcohol dehydrogenase (ADH) and aldehyde dehydrogenase leads to the production of toxic species. Methanolelimination follows zero-order kinetics in the absence of treatment, and has been estimated at 8.5 mg/dL (2.7mmol/L) per hour following overdose [11]. Ethylene glycol elimination appears to follow first-order kinetics in theabsence of treatment, with an estimated serum half-life of between 3 and 9 hours [7,12].
If hepatic oxidation is inhibited ("blocked") by an alcohol dehydrogenase antagonist, such as ethanol or fomepizole,several changes occur. (See 'Alcohol dehydrogenase inhibition' below.)
For methanol, elimination shifts to the pulmonary and renal routes [13,14], becomes first-order, and slowsdramatically (half-life of 48 to 54 hours).
For ethylene glycol, elimination after ADH inhibition becomes almost entirely renal, with a half-life of 17 to 20hours (assuming normal kidney function) [7].
Elimination of formate, the toxic metabolite of methanol, is partially dependent upon tetrahydrofolate, and is thoughtto accelerate following folic acid administration [8]. Pyridoxine and thiamine are involved in minor eliminationpathways of glycolate, an ethylene glycol metabolite, but it is not known if pyridoxine and thiamine supplementationaccelerates metabolism along these minor pathways [15]. (See 'Cofactor therapy' below.)
CLINICAL FEATURES OF OVERDOSE
History — The clinician should make every effort to identify the original source and nature of the exposure. This isideally done by retrieving the original container and consulting product databases, as well as interviewing the patient,relatives, and prehospital workers. Methanol and ethylene glycol are frequently found in high concentration inautomotive antifreeze and de-icing solutions, windshield wiper fluid, solvents, cleaners, fuels, and other industrialproducts. Most serious poisonings occur following ingestion. "Antifreeze" may contain a different alcohol thanoriginally suspected (eg, propylene glycol rather than ethylene glycol). Such information dramatically changes thetreatment strategy, underscoring the need to obtain accurate information.
In the absence of treatment, an ingestion of approximately 1 g/kg of either methanol or ethylene glycol (ie, parentalcohols) is considered lethal, and serious toxicity has been reported following ingestions of as little as one teaspoonof methanol. Inhalation and dermal exposures rarely cause toxicity. Product labels rarely provide the concentrationsof toxic alcohols. As an approximate guide, a 50 percent vol/vol solution contains 0.4 g/mL of methanol or 0.6 g/mLof ethylene glycol.
It is important to clarify when the ingestion occurred and whether ethanol was also ingested. As mentioned above,ethanol competitively inhibits alcohol dehydrogenase, thereby diminishing formation of toxic metabolites of theparent compound.
The intent of the exposure (whether accidental, suicidal, or homicidal) may only become apparent with closerinvestigation (eg, interview of friends and family). The identification of other potential victims may depend uponunderstanding the circumstances of the exposure (eg, occult substitution for ethanol). (See 'Adolescents' below.)
Complaints of visual blurring, central scotomata, and blindness suggest methanol poisoning. Flank pain, hematuria,and oliguria suggest ethylene glycol poisoning.
Physical examination — A brief initial screening examination, including vital signs, mental status, and pupils,should be performed to identify immediate measures required to stabilize the patient. A discussion of thefundamental evaluation of the poisoned patient is found elsewhere. (See "General approach to drug poisoning inadults" and "Approach to the child with occult toxic exposure".)
Patients with large ingestions of methanol or ethylene glycol may present with mild CNS effects, such as inebriationand sedation, similar to ethanol intoxication. Ethanol coingestion may exacerbate such symptoms. Coma, seizures,hyperpnea (Kussmaul-Kien respirations), and hypotension all suggest a substantial portion of the parent alcohol hasbeen metabolized to its toxic byproducts.
An afferent pupillary defect is an ominous sign of advanced methanol poisoning. Eye examination in methanol

poisoning may also reveal mydriasis, a retinal sheen due to retinal edema, and hyperemia of the optic disk.
It is important to emphasize that the onset of methanol or ethylene glycol toxicity is delayed when ethanol iscoingested. The possibility of concomitant ethanol and toxic alcohol ingestion must always be considered,particularly in alcoholics, who may ingest alcohol in any form.
Ethylene glycol metabolism can lead to cranial nerve palsies and tetany (thought to result from oxalate-inducedhypocalcemia). Oliguria and hematuria may occur. Cerebral herniation and multisystem organ failure are commonpreterminal events in patients with profound poisoning.
Differential diagnosis — Pending definitive parent alcohol concentrations, the clinician should form a differentialdiagnosis based upon the available clinical information.
Few conditions other than methanol and ethylene glycol intoxication cause a profound high anion gap metabolicacidosis (serum bicarbonate less than 8 meq/L (or 8 mmol/L)), and most of these conditions present in acharacteristic fashion with a high serum lactate (eg, status epilepticus, profound shock, ischemic bowel) or diabeticketoacidosis (table 2). Although some patients with ethylene glycol poisoning present with elevated lactate levels,the rise in lactate is insufficient to account for the degree of acidosis [16]. (See "The Δanion gap/ΔHCO3 ratio inpatients with a high anion gap metabolic acidosis" and "Shock in adults: Types, presentation, and diagnosticapproach".)
A lesser degree of metabolic acidosis in an alcoholic patient may also be caused by alcoholic ketoacidosis, sepsis,alcohol withdrawal seizures, diabetic ketoacidosis, or salicylate intoxication [11]. (See "Alcoholic and fastingketoacidosis" and "Shock in adults: Types, presentation, and diagnostic approach" and "Clinical features anddiagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults" and "Salicylate (aspirin)poisoning in adults".)
An elevated plasma osmolal gap can be seen in patients with methanol or ethylene glycol intoxication, but also inalcoholic or diabetic ketoacidosis, isopropyl alcohol ingestion, large ethanol ingestions, and other serious illnesses(eg, sepsis, ischemic bowel, shock) (table 3). (See 'Plasma osmolal gap' below and "Serum osmolal gap" and"Isopropyl alcohol poisoning".)
Traces of methanol may be detectable in alcoholic patients drinking fermented beverages such as wine.
Laboratory evaluation
Basic testing — Routine laboratory evaluation of any poisoned patient should include the following:
Fingerstick glucose, to rule out hypoglycemia as the cause of any alteration in mental status
Acetaminophen and salicylate levels, to rule out these common coingestions
Electrocardiogram (ECG), to rule out conduction system poisoning by drugs that effect the QRS or QTcintervals; it is important to note that ethylene glycol can prolong the QTc interval via its effects on serumcalcium
Pregnancy test in women of childbearing age
Additional tests with toxic alcohol exposure — All patients suspected of toxic alcohol exposure shouldundergo additional laboratory evaluation including the following:
Basic electrolytes with anion gap determinationSerum calciumBUN and creatinineArterial or venous blood gas analysisSerum ethanol concentrationSerum osmolalitySerum methanol, ethylene glycol, and isopropyl alcohol concentrations
Pitfalls in laboratory testing

Testing for methanol and ethylene glycol — The measurement of serum methanol and ethylene glycolconcentrations is usually performed by gas chromatography, but such testing is not widely available and frequentlymust be performed at a reference laboratory [5,17]. Such "send out" laboratory testing rarely, if ever, returns in timeto assist clinical decision-making.
Some laboratories report a "solvent screen" that does not include ethylene glycol and may falsely reassure clinicians.Thus, if a "solvent screen" is performed, the clinician should clarify exactly which solvents are detected by the test.
Enzymatic methods of ethylene glycol detection are still used in many laboratories, but they can lead to false-positiveresults (eg, from severe acetaminophen toxicity, or interference from propylene glycol, 2, 3-butanediol, or glycolate)[5,13]. We do NOT recommend relying on these tests when evaluating patients with potential ethylene glycol toxicity.
Lactate — Patients with ethylene glycol poisoning can have elevations in their serum lactate concentration [18].In some cases, such elevations (usually minor) can be caused by actual increases in lactate. However, in othercases such elevations may be substantial and are likely to be caused by the misinterpretations of some laboratoryinstruments that cannot differentiate between lactate and glycolate, a metabolite of ethylene glycol that is structurallysimilar to lactate [16,19-22].
A markedly elevated lactate concentration may be the first test result reported in a severely acidotic patient, now thatlactate testing has become readily available, and traditionally suggests alternative diagnoses (eg, tissue hypoxia,metformin poisoning). However, it is important NOT to exclude ethylene glycol as a possible cause of acidosisassociated with an elevated lactate.
Urine testing — Examination of the urine for oxalate crystals and fluorescence is frequently performed inpatients with possible ethylene glycol poisoning, but care should be taken not to over interpret positive or negativeresults. The formation of oxalate crystals in the urine is a late and NONSPECIFIC finding following ethylene glycolingestion [8,14]. Two types of calcium oxalate crystals may be seen: needle-shaped monohydrate crystals, whichmay be misread as hippurate crystals, and envelope-shaped dihydrate crystals (picture 1A-B).
Urine fluorescence is a poor diagnostic test that uses ultraviolet light to detect the fluorescein added to mostantifreeze solutions. Urine fluorescence lacks sensitivity, as not all ethylene glycol preparations contain fluorescein,and fluorescein (when present) appears only transiently in the urine following ingestion. Urine fluorescence alsolacks specificity because normal urine can appear to fluoresce and other substances unrelated to ethylene glycolpoisoning can cause fluorescence [15,23,24].
Plasma osmolal gap — Cryoscopic osmometry is widely used to measure plasma osmolality and to estimate theso-called osmolal gap. While the test must be interpreted cautiously, as described below, an unexplained, largeosmolal gap is presumptive evidence of a recent methanol, ethylene glycol, or isopropyl alcohol exposure in theappropriate clinical setting, as long as a significant ethanol ingestion has been excluded .
The osmolal gap is the difference between the measured osmolality and the calculated plasma osmolality:
Calculated Posm = (2 x plasma [Na]) + [glucose]/18 + [BUN]/2.8
or, with standard units (mmol/L):
Calculated Posm = (2 x plasma [Na]) + [glucose] + [urea]
The serum sodium is multiplied by two to account for accompanying anions (chloride and bicarbonate) and thedivisors 18 and 2.8 in the first formula convert units of mg/dL into mmol/L (standard units).
Details of the plasma osmolal gap and its measurement are discussed separately, but its use in methanol andethylene glycol intoxication will be reviewed here. (See "Serum osmolal gap".) Calculators to determine the osmolalgap are provided (calculator 1 and calculator 2).
The plasma osmolal gap can provide important information in real time, costs little, and is widely available. Cliniciansneed to be able to interpret this test for early treatment decision-making, pending definitive poison identification bygas chromatography [14,25-28].
When interpreting the plasma osmolal gap in the setting of a toxic alcohol ingestion, clinicians should keep in mind

several potential pitfalls:
The plasma osmolal gap cannot distinguish among ethanol, isopropyl alcohol, methanol, or ethylene glycol.
The plasma osmolal gap estimates the molar quantity of uncharged molecules and therefore increases only inthe presence of the parent alcohols. The toxic acid metabolites of methanol (formate) and ethylene glycol(glycolate, glyoxylate, and oxalate) exist primarily in a dissociated (ie, charged) form at physiologic pH; sincethese anions must be accompanied by a cation (mostly sodium), they do not contribute to the calculatedosmolal gap. As a result, the plasma osmolal gap is insensitive in late presentations, since most of the parentalcohol has already been metabolized.
The plasma osmolal gap is not sufficiently sensitive to exclude a small ingestion. The variability of the testmeans that despite a significant ingestion (serum concentrations up to 50 mg/dL (8.1 mmol/L) of ethyleneglycol), the plasma osmolal gap can fall within the upper limits of the normal range (generally less than 10units is considered normal). The plasma osmolal gap has been less than 10 in a small number of seriousexposures [29-31].
Large quantities of ethanol (greater than 100 mg/dL (or 22 mmol/L)) can raise the osmolal gap more thanwould be expected based on its molecular weight. This occurs because serum does not behave as an idealfluid and because mathematical approximations are used in calculating the osmolal gap. We recommend thatthe measured serum ethanol level be increased by 20 to 25 percent when performing plasma osmolal gapcalculations to enable a more accurate interpretation [32,33].
Clinicians should also note that patients who are critically ill may have elevated plasma osmolal gaps, due to so-called idiogenic osmoles. (See "Serum osmolal gap", section on 'Other'.)
In summary, the practice of categorically ruling out methanol or ethylene glycol exposure on the basis of a plasmaosmolal gap less then 10 units is unjustified, as is assuming that a small elevation in the plasma osmolal gap in apatient with a low pretest probability is due to a toxic alcohol.
On the other hand, few substances cause a very high (greater than 25) plasma osmolal gap, and most severelypoisoned methanol and ethylene glycol patients manifest plasma osmolal gaps of this magnitude shortly afteringestion. An unexplained, large osmolal gap is presumptive evidence of a recent methanol, ethylene glycol, orisopropyl alcohol exposure in the appropriate clinical setting [14,27].
MANAGEMENT
Overview of emergent management — Rapid decision-making is critical in the management of the patientpoisoned with methanol or ethylene glycol. The clinician must often make treatment decisions without definitiveserum drug levels, based only upon clinical suspicion and readily available laboratory data. A summary table tofacilitate emergent management is provided (table 1).
The management of methanol and ethylene glycol poisoning involves the following:
Securing the patient's airway, breathing, and circulation, and providing appropriate supportive care
Administering sodium bicarbonate to correct systemic acidosis, which limits the penetration of toxic acids (eg,formic acid) into end-organ tissues such as the retina by converting them to the anion (eg, formate), whichcannot diffuse across cell membrane
Inhibiting the enzyme alcohol dehydrogenase, with either fomepizole (preferred) or ethanol (if fomepizole isunavailable)
Performing hemodialysis for elevated toxic alcohol levels, severe acid-base derangements, or evidence ofend-organ toxicity
Treating with cofactors (folic acid, thiamine, and pyridoxine) to optimize nontoxic metabolic pathways for theelimination of the parent alcohol or its metabolites

We also recommend immediate consultation with a medical toxicologist or poison control center, if methanol orethylene glycol intoxication is suspected. (See 'Additional resources' below.)
Airway, breathing, circulation — The clinician must first assess and secure the patient's airway, breathing, andcirculation. Advanced cardiac life support measures are provided as required. A discussion of fundamentalmanagement of the poisoned patient is found elsewhere. (See "General approach to drug poisoning in adults".)
If endotracheal intubation is required, the patient should be hyperventilated, if a significant metabolic acidosis existsor is suspected. Arterial and/or venous blood gas analysis should be performed frequently to evaluate pH andensure adequate ventilation and oxygenation. Large minute ventilations may be required to prevent profoundacidemia (pH <7.1) in patients with severe intoxication.
Gastrointestinal decontamination — There is little, if any, role for gastrointestinal (GI) decontamination inmethanol or ethylene glycol poisoning, as these simple alcohols are rapidly absorbed. The rare patient known tohave ingested a large amount of methanol or ethylene glycol may benefit from gastric aspiration via flexiblenasogastric tubing if performed within 60 minutes of the ingestion. Activated charcoal (AC), gastric lavage, and syrupof ipecac have no role in the management of toxic alcohol exposures.
Treatment with sodium bicarbonate — Methanol is metabolized to formate, and ethylene glycol to glycolate,glyoxylate, and oxalate. Acidemia leads to protonation of these species to uncharged molecules (eg, formic acid),making them more likely to penetrate end-organ tissues (such as the retina) and more likely to be reabsorbed acrossthe renal epithelium from the urine. Thus, patients with methanol or ethylene glycol poisoning fare worse whensystemic acidemia is present [10]. Treatment with sodium bicarbonate leads to deprotonation of these acid species,making them less likely to penetrate end-organ tissues and more likely to be excreted in the urine.
Despite this clear rationale, no clear evidence exists to determine how bicarbonate should be given. We suggestinitial treatment with 1 to 2 meq/kg of sodium bicarbonate via IV bolus for any patient with a pH below 7.3 [14,27]. Amaintenance infusion is then prepared by mixing approximately 133 meq of sodium bicarbonate in 1 liter of D5W.Infusion rates may range from 150 to 250 mL/hour in adults, or one to two times the maintenance fluid rate inchildren. The appropriate rate depends upon the initial pH, and such parameters as fluid status and serum sodiumconcentration. The goal of treatment is maintenance of an arterial or venous pH above 7.35, at which point theinfusion is discontinued.
Alcohol dehydrogenase inhibition
Approach and initiation — Inhibition of alcohol dehydrogenase (ADH) blocks bioactivation of the parent alcoholto its toxic acid metabolites. Early treatment is crucial since ADH inhibition does not prevent toxicity if completemetabolism to acid species has already occurred.
Fomepizole or ethanol can be used to inhibit ADH (table 4). We recommend treatment with fomepizole. TheAmerican Academy of Clinical Toxicology (AACT) practice guidelines provide some guidance for the initiation of ADHinhibitor therapy [14,27]. (See 'Fomepizole' below.)
The AACT's minimum treatment threshold of 20 mg/dL of either methanol [SI equivalent 6.2 mmol/L] or ethyleneglycol [SI equivalent 3.2 mmol/L] is not evidence-based and is necessarily conservative [34-36]. Parent alcoholconcentrations must be interpreted in clinical context. As an example, a patient with a methanol level of 25 mg/dL (or7.8 mmol/L) and a normal acid base-status may only require one or two doses of fomepizole and observation,whereas a patient with the same level but a significant acidosis and vision deficits may require fomepizole,alkalinization, and hemodialysis.
In the absence of confirmatory drug levels, clinicians must rely upon their clinical judgment and readily availablelaboratory tests when deciding whether to initiate therapy with an ADH inhibitor. Clinicians should be wary ofinitiating such therapy solely on the basis of an anion gap or small osmolal gap without at least circumstantialevidence of toxic alcohol ingestion, especially when ethanol therapy is contemplated. In addition, the clinician shouldnot ascribe metabolic acidosis to a toxic alcohol ingestion if coingested ethanol is present: substantial oxidation ofthe toxic alcohol is highly unlikely in the presence of ethanol.
Once begun, ADH inhibition should be continued until the diagnosis of toxic alcohol ingestion has been ruled out, oruntil blood pH is normal and serum alcohol concentration is less than 20 mg/dL [SI units: methanol 6.2 mmol/L and

ethylene glycol 3.2 mmol/L] in the presence of retinal or renal injury.
Fomepizole — Fomepizole has been used successfully for years to treat both methanol and ethylene glycolpoisoning [37-39]. There is a virtual consensus among toxicologists that it is a superior antidote to ethanol [12,40-43]. Fomepizole is easy to dose, easy to administer, and side effects are rare [44]. Its main disadvantage is its highcost. However, the cost compares favorably with the total cost of managing patients treated with ethanol, includingethanol titration and possibly hemodialysis and intensive care unit admission [7,42,45].
Fomepizole is loaded at 15 mg/kg intravenously, followed by 10 mg/kg every 12 hours, with adjustments forhemodialysis or after more than two days of therapy. (See 'Hemodialysis' below.)
Ethanol — Historically, ethanol has been used as a competitive inhibitor of ADH, as ADH has greater affinity forethanol than for methanol or ethylene glycol. Although effective, intravenous ethanol treatment creates severalproblems [46]:
Ethanol is difficult to dose, and appropriate levels are difficult to maintain; as a result, frequent testing andinfusion adjustments are often required.
Ethanol requires compounding by the hospital pharmacy, irritates veins when infused, and can complicatefluid balance in oliguric patients.
Most limiting are the sedative and behavioral effects of ethanol, which can cause obtundation, therebyincreasing the risk of aspiration, and other complications [44].
In the rare circumstance in which we use ethanol therapy, we target a serum ethanol concentration of at least one-third of the serum methanol or ethylene glycol concentration expressed as mg/dL. However, most sources cite anabsolute ethanol level of 100 mg/dL (or 22 mmol/L). An intravenous loading dose of 800 mg/kg ethanol in a 10percent vol/vol solution in D5W will raise serum ethanol concentrations by about 100 mg/dL. A maintenance infusionof 80 to 160 mg/kg per hour, or more during hemodialysis, should be titrated according to serial ethanolconcentrations. (See 'Hemodialysis' below.)
There is no benefit to adding ethanol therapy to fomepizole therapy in methanol and ethylene glycol-poisonedpatients.
Hemodialysis — Hemodialysis is the best method to rapidly remove both toxic acid metabolites and parentalcohols, and it plays a fundamental role in treating severely poisoned patients [14,27]. Emergency clinicians shouldinitiate consultation with a nephrologist immediately if they suspect a toxic alcohol ingestion and the patient hasevidence of end-organ dysfunction or acidemia, especially if transfer to a hemodialysis center may be necessary.
In such cases, consultation should not be delayed until confirmatory methanol or ethylene glycol levels are obtained.An arterial or venous blood gas serves as an essential triage tool in this setting. This is particularly true when caringsimultaneously for multiple poisoned patients with limited hemodialysis capability [46,47].
We recommend immediate treatment with hemodialysis in the setting of a known methanol or ethylene glycolingestion if either of the following conditions is present:
High anion gap metabolic acidosis, regardless of drug levelEvidence of end-organ damage (eg, visual changes, renal failure)
In addition, we suggest treatment with hemodialysis in any patient with a suspected toxic alcohol ingestion who hasa severe, otherwise unexplained anion gap metabolic acidosis and significant plasma osmolal gap. It is difficult toprovide precise thresholds for determining when hemodialysis should be performed when the ingestion is uncertain.If a toxic ingestion is strongly suspected, a threshold pH of 7.30 is reasonable; if suspicion is weaker, a pH of 7.10may be more appropriate. (See 'Laboratory evaluation' above.)
For nonacidemic patients, hemodialysis can be used to clear the parent alcohol and abbreviate the course ofantidotal therapy. There is less urgency to treat with hemodialysis if ADH inhibition is adequate. Hemodialysis isoften unnecessary in patients with unmetabolized ethylene glycol provided that [14]:
Fomepizole is given (prolonged ethanol therapy is impractical)

The serum pH is normal or near normal (ie, little glycolate is present)The serum creatinine remains normal
Patients with ethylene glycol concentrations greater than 300 mg/dL [48 mmol/L] have been successfully treated withfomepizole alone when therapy was initiated before the appearance of acidosis. Treatment with hemodialysis is stillrecommended for large methanol ingestions because serum methanol elimination becomes extremely slow whenADH is inhibited [27,48,49].
The hemodialysis prescription should include a large surface area dialyzer (>1.5 m2), a blood flow rate in excess of300 mL/min, and a bicarbonate bath. Hemodialysis should continue until the serum pH is normal and parent alcoholconcentrations are less than approximately 25 mg/dL or 5 mmol/L. The duration of hemodialysis in hours can beestimated using the formula (-V ln (5/A)/0.06 k), where V is total body water in liters, A is the initial alcoholconcentration in mmol/L, and k is 80 percent of the dialyzer urea clearance in mL/min at the observed blood flow rate[50-52]. Serum alcohol concentrations should be verified near the end of hemodialysis and again two hours post-hemodialysis to ascertain the adequacy of treatment. (See "Acute hemodialysis prescription".)
More than one round of hemodialysis may be necessary in massive overdoses and for ethylene glycol-poisonedpatients with renal failure. Renal function often recovers over a period of days to months in survivors of ethyleneglycol poisoning.
Fomepizole is dialyzable, and the frequency of its dosing should be increased to every four hours duringhemodialysis. An additional dose should be given at the beginning of hemodialysis if six or more hours have elapsedsince the prior dose.
If ethanol is used for alcohol dehydrogenase (ADH) inhibition, adjustments in the dose must be made duringhemodialysis. A fall in ethanol levels can be avoided or ameliorated by increasing the rate of ethanol infusion andpossibly by adding ethanol directly to the dialysate [53,54]. In one such case, a dialysate ethanol concentration of100 mg/dL was prepared by administering a 95 percent ethanol solution into the dialysate inlet tubing at a rate of 40mL/h via an infusion pump. The dialysate flow rate was maintained at 500 mL/min, and the dialyzer blood flowaveraged 280 mL/min. An average plasma ethanol level of 90 mg/dL was obtained during the six-hour hemodialysissession.
Peritoneal dialysis and other forms of continuous renal replacement therapy are inefficient at clearing toxic alcoholsand their metabolites and are not recommended.
Cofactor therapy — All methanol patients treated with ADH inhibition should also receive cofactor therapy: eitherfolinic acid (leucovorin) 50 mg IV or folic acid 50 mg IV every six hours [27,55,56]. It is not known whethersupplemental thiamine (100 mg IV) or pyridoxine (50 mg IV) benefits patients poisoned with ethylene glycol, but weroutinely administer both, particularly if the patient's nutritional status is suspect.
Preterminal care — Severely poisoned patients who present in coma may not survive despite maximum intensivetherapy. Consideration should be given to organ harvesting prior to withdrawal of support for such patients,especially after severe methanol poisoning. Formate is a highly specific neurotoxin, and case series support theviability of other organs harvested from such patients [57,58].
ADDITIONAL RESOURCES — To obtain emergent consultation with a medical toxicologist, call the United StatesPoison Control Network at 1-800-222-1222, or access the World Health Organization's list of international poisoncenters (www.who.int/gho/phe/chemical_safety/poisons_centres/en/index.html).
PEDIATRIC CONSIDERATIONS
Younger children — A common clinical presentation involves the child who may have swallowed one or twomouthfuls of a concentrated methanol or ethylene glycol solution. These children should not be managed at home[59].
Most victims of unintentional exposure present for evaluation shortly after ingestion and do not manifest significantmetabolic acidosis or any evidence of end-organ dysfunction. The ideal approach is to measure the serumconcentration of the specific alcohol in order to quantify the absorbed dose and predict the clinical course.Unfortunately, such concentrations are rarely available within a few hours of the ingestion, creating a diagnostic and

therapeutic dilemma.
One approach to this problem (described below) can be used if all of the following criteria are met:
The ingestion was unintentional and of small volumeThe product is accurately identifiedThe patient is asymptomaticThe patient has a normal pH and normal anion gapThere is no coingestion or treatment with ethanol or fomepizole
If all conditions are met, the clinician can observe the patient and monitor venous blood gases and electrolytes everyone to two hours to exclude the development of a metabolic acidosis or an increasing anion gap. If acidosis does notdevelop within eight hours of the ingestion, a toxic alcohol poisoning can be excluded. Alcohol dehydrogenase(ADH) inhibition with fomepizole or ethanol should NOT be initiated during this observation period, as such treatmentwill prevent the development of acidosis even in patients with massive ingestions. Treatment with fomepizole orethanol invalidates the above protocol.
Parents should be counseled about safe storage of household products and pharmaceuticals prior to discharge.
Occasionally, infants with inherited metabolic disorders such as methylmalonic acidemia present with features thatresemble ethylene glycol poisoning, and vice versa [60,61]. The clinician should obtain organic acid testing in allinfants presenting with unexplained metabolic acidosis. (See "Organic acidemias".)
Adolescents — Groups of adolescents trying to become inebriated may consume toxic alcohols knowingly oraccidentally in contaminated beverages. When treating an adolescent for a possible toxic alcohol ingestion,clinicians should always consider the possibility of other as-yet unidentified victims.
SUMMARY AND RECOMMENDATIONS — Methanol and ethylene glycol poisonings cause dozens of fatalintoxications in the United States annually. Rapid recognition and early treatment are crucial. A summary table tofacilitate emergent management is provided (table 1).
Assessment
The "parent alcohols" methanol and ethylene glycol are themselves relatively nontoxic, causing mainly centralnervous system sedation. The methanol metabolite formate can cause retinal and basal ganglia injury, andthe ethylene glycol metabolites can cause renal failure following large ingestions. (See 'Pharmacology andcellular toxicology' above.)
Methanol and ethylene glycol are rapidly and completely absorbed after oral ingestion. Peak serum alcoholconcentrations are reached within one to two hours.
The clinician should make every effort to identify the source and nature of the exposure. This is ideally doneby retrieving the original container and consulting product databases. It is important to clarify when theingestion occurred, whether ethanol was also ingested, and the intent of the exposure (whether accidental,suicidal, or homicidal). (See 'History' above.)
Ingestion of approximately 1 g/kg of either methanol or ethylene glycol is considered lethal, and serioustoxicity has been reported following ingestions of as little as 8 g of methanol.
Complaints of visual blurring, central scotomata, and blindness suggest methanol poisoning. Flank pain andhematuria suggest ethylene glycol poisoning. Coma, seizures, hyperpnea, and hypotension all suggest asubstantial portion of the parent alcohols has been metabolized to toxic acids. (See 'History' above.)
Few conditions other than methanol and ethylene glycol intoxication present with a profound metabolicacidosis (serum bicarbonate less than 8 meq/L), and most of these conditions present in a characteristicfashion (eg, status epilepticus, profound shock, ischemic bowel) (table 2). (See 'Differential diagnosis' above.)
Direct testing of toxic alcohols is the preferred diagnostic test when available. If a "solvent screen" isperformed, the clinician should clarify exactly which solvents are detected by the test. (See 'Laboratory

evaluation' above and 'Pitfalls in laboratory testing' above.)
Few substances cause a very high (greater than 25 mOsm) osmolal gap, and most severely poisonedmethanol and ethylene glycol patients manifest osmolal gaps of this magnitude shortly after ingestion. Anunexplained, large osmolal gap is presumptive evidence of a recent methanol, ethylene glycol, or isopropylalcohol exposure in the appropriate clinical setting. (See 'Plasma osmolal gap' above.)
Treatment
First assess and secure the patient's airway, breathing, and circulation. If mechanical ventilation is required,large minute ventilations may be needed to prevent profound acidemia (pH <7.1) in patients with severeintoxication. (See 'Airway, breathing, circulation' above.)
Patients with methanol or ethylene glycol poisoning fare worse when systemic acidemia is present. Forpatients with a serum pH below 7.3, we recommend treatment with sodium bicarbonate (Grade 1C). Begintreatment with 1 to 2 meq/kg of sodium bicarbonate via IV bolus infusion. (See 'Treatment with sodiumbicarbonate' above.)
We recommend that alcohol dehydrogenase (ADH) inhibition therapy with fomepizole be initiated in anypatient in whom the clinician has strong suspicion of poisoning with either methanol or ethylene glycolcoupled with an elevated plasma osmolal gap, or acidemia, or a measured methanol or ethylene glycolconcentration over 20 mg/dL methanol [SI equivalent: methanol 6.2 mmol/L; ethylene glycol 3.2 mmol/L](Grade 1B). Fomepizole is loaded at 15 mg/kg intravenously, followed by 10 mg/kg every 12 hours, withadjustments for hemodialysis or after more than two days of therapy. If fomepizole is unavailable, werecommend treatment with ethanol in these same circumstances (Grade 1B). We provide cofactor therapy toall patients receiving ADH inhibition. (See 'Alcohol dehydrogenase inhibition' above and 'Cofactortherapy' above.)
We recommend immediate hemodialysis be performed in the setting of a known methanol or ethylene glycolingestion when the following conditions are present (Grade 1B):
Metabolic acidosis, regardless of drug level
Elevated serum levels of methanol or ethylene glycol (more than 50 mg/dL [SI equivalent: methanol 15.6mmol/L; ethylene glycol 8.1 mmol/L]), unless arterial pH is above 7.3
Evidence of end-organ damage (eg, visual changes, renal failure)
We recommend treatment with hemodialysis if the clinician suspects a toxic alcohol ingestion in a patientwith a severe, unexplained anion gap metabolic acidosis and significant osmolal gap (Grade 1B). Wegenerally refrain from using hemodialysis to treat patients with elevated ethylene glycol concentrations,provided their serum pH is near normal, their renal function is normal, and fomepizole is given. (See'Hemodialysis' above.)
Consultation with a medical toxicologist at a regional poison center is strongly recommended for all suspectedexposures and for cases in which fomepizole, ethanol, or hemodialysis therapy may be used. Consultationwith nephrology and emergent hemodialysis should be immediately obtained for severely acidotic patients inwhom the diagnosis appears likely, especially if accompanied by visual or renal impairment.
Activated charcoal (AC), gastric lavage, and syrup of ipecac have no role in the management of toxic alcoholexposures.
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. d'Alessandro A, Osterloh JD, Chuwers P, et al. Formate in serum and urine after controlled methanol exposure

at the threshold limit value. Environ Health Perspect 1994; 102:178.2. Kerns W 2nd, Tomaszewski C, McMartin K, et al. Formate kinetics in methanol poisoning. J Toxicol Clin
Toxicol 2002; 40:137.3. Liesivuori J, Savolainen H. Methanol and formic acid toxicity: biochemical mechanisms. Pharmacol Toxicol
1991; 69:157.4. Moreau CL, Kerns W 2nd, Tomaszewski CA, et al. Glycolate kinetics and hemodialysis clearance in ethylene
glycol poisoning. META Study Group. J Toxicol Clin Toxicol 1998; 36:659.5. Fraser AD. Clinical toxicologic implications of ethylene glycol and glycolic acid poisoning. Ther Drug Monit
2002; 24:232.6. Sivilotti ML, Burns MJ, Aaron CK, et al. Reversal of severe methanol-induced visual impairment: no evidence
of retinal toxicity due to fomepizole. J Toxicol Clin Toxicol 2001; 39:627.7. Sivilotti ML, Burns MJ, McMartin KE, Brent J. Toxicokinetics of ethylene glycol during fomepizole therapy:
implications for management. For the Methylpyrazole for Toxic Alcohols Study Group. Ann Emerg Med 2000;36:114.
8. Jacobsen D, Hewlett TP, Webb R, et al. Ethylene glycol intoxication: evaluation of kinetics and crystalluria. AmJ Med 1988; 84:145.
9. Bove KE. Ethylene glycol toxicity. Am J Clin Pathol 1966; 45:46.10. Jacobsen D, McMartin KE. Methanol and ethylene glycol poisonings. Mechanism of toxicity, clinical course,
diagnosis and treatment. Med Toxicol 1986; 1:309.11. Höjer J. Severe metabolic acidosis in the alcoholic: differential diagnosis and management. Hum Exp Toxicol
1996; 15:482.12. Jacobsen D, McMartin KE. Antidotes for methanol and ethylene glycol poisoning. J Toxicol Clin Toxicol 1997;
35:127.13. Malandain H, Cano Y. Interferences of glycerol, propylene glycol, and other diols in the enzymatic assay of
ethylene glycol. Eur J Clin Chem Clin Biochem 1996; 34:651.14. Barceloux DG, Krenzelok EP, Olson K, Watson W. American Academy of Clinical Toxicology Practice
Guidelines on the Treatment of Ethylene Glycol Poisoning. Ad Hoc Committee. J Toxicol Clin Toxicol 1999;37:537.
15. Casavant MJ, Shah MN, Battels R. Does fluorescent urine indicate antifreeze ingestion by children? Pediatrics2001; 107:113.
16. Shirey T, Sivilotti M. Reaction of lactate electrodes to glycolate. Crit Care Med 1999; 27:2305.17. Church AS, Witting MD. Laboratory testing in ethanol, methanol, ethylene glycol, and isopropanol toxicities. J
Emerg Med 1997; 15:687.18. Gabow PA, Clay K, Sullivan JB, Lepoff R. Organic acids in ethylene glycol intoxication. Ann Intern Med 1986;
105:16.19. Eder AF, Dowdy YG, Gardiner JA, et al. Serum lactate and lactate dehydrogenase in high concentrations
interfere in enzymatic assay of ethylene glycol. Clin Chem 1996; 42:1489.20. Morgan TJ, Clark C, Clague A. Artifactual elevation of measured plasma L-lactate concentration in the
presence of glycolate. Crit Care Med 1999; 27:2177.21. Porter WH, Crellin M, Rutter PW, Oeltgen P. Interference by glycolic acid in the Beckman synchron method for
lactate: a useful clue for unsuspected ethylene glycol intoxication. Clin Chem 2000; 46:874.22. Brindley PG, Butler MS, Cembrowski G, Brindley DN. Falsely elevated point-of-care lactate measurement after
ingestion of ethylene glycol. CMAJ 2007; 176:1097.23. Wallace KL, Suchard JR, Curry SC, Reagan C. Diagnostic use of physicians' detection of urine fluorescence in
a simulated ingestion of sodium fluorescein-containing antifreeze. Ann Emerg Med 2001; 38:49.24. Sharma AN, O'Shaughnessy PM, Hoffman RS. Urine fluorescence: is it a good test for ethylene glycol
ingestion? Pediatrics 2002; 109:345.25. Koga Y, Purssell RA, Lynd LD. The irrationality of the present use of the osmole gap: applicable physical
chemistry principles and recommendations to improve the validity of current practices. Toxicol Rev 2004;23:203.
26. Hoffman RS, Smilkstein MJ, Howland MA, Goldfrank LR. Osmol gaps revisited: normal values and limitations.J Toxicol Clin Toxicol 1993; 31:81.
27. Barceloux DG, Bond GR, Krenzelok EP, et al. American Academy of Clinical Toxicology practice guidelines onthe treatment of methanol poisoning. J Toxicol Clin Toxicol 2002; 40:415.

28. Lynd LD, Richardson KJ, Purssell RA, et al. An evaluation of the osmole gap as a screening test for toxicalcohol poisoning. BMC Emerg Med 2008; 8:5.
29. Steinhart B. Case report: severe ethylene glycol intoxication with normal osmolal gap--"a chilling thought". JEmerg Med 1990; 8:583.
30. Ammar KA, Heckerling PS. Ethylene glycol poisoning with a normal anion gap caused by concurrent ethanolingestion: importance of the osmolal gap. Am J Kidney Dis 1996; 27:130.
31. Purssell RA, Lynd LD, Koga Y. The use of the osmole gap as a screening test for the presence of exogenoussubstances. Toxicol Rev 2004; 23:189.
32. Purssell RA, Pudek M, Brubacher J, Abu-Laban RB. Derivation and validation of a formula to calculate thecontribution of ethanol to the osmolal gap. Ann Emerg Med 2001; 38:653.
33. Sivilotti ML. Methanol intoxication. Ann Emerg Med 2000; 35:313.34. Kostic MA, Dart RC. Rethinking the toxic methanol level. J Toxicol Clin Toxicol 2003; 41:793.35. Porter WH, Rutter PW, Bush BA, et al. Ethylene glycol toxicity: the role of serum glycolic acid in hemodialysis.
J Toxicol Clin Toxicol 2001; 39:607.36. De Leacy EA, Moxon LN, Ellis VM, et al. A report of accidental ethylene glycol ingestion in 2 siblings.
Pathology 1995; 27:273.37. Baud FJ, Galliot M, Astier A, et al. Treatment of ethylene glycol poisoning with intravenous 4-methylpyrazole.
N Engl J Med 1988; 319:97.38. Brent J, McMartin K, Phillips S, et al. Fomepizole for the treatment of ethylene glycol poisoning.
Methylpyrazole for Toxic Alcohols Study Group. N Engl J Med 1999; 340:832.39. Brent J, McMartin K, Phillips S, et al. Fomepizole for the treatment of methanol poisoning. N Engl J Med 2001;
344:424.40. Shannon M. Toxicology reviews: fomepizole--a new antidote. Pediatr Emerg Care 1998; 14:170.41. Battistella M. Fomepizole as an antidote for ethylene glycol poisoning. Ann Pharmacother 2002; 36:1085.42. Sivilotti ML. Ethanol: tastes great! Fomepizole: less filling! Ann Emerg Med 2009; 53:451.43. Dart RC, Borron SW, Caravati EM, et al. Expert consensus guidelines for stocking of antidotes in hospitals that
provide emergency care. Ann Emerg Med 2009; 54:386.44. Lepik KJ, Levy AR, Sobolev BG, et al. Adverse drug events associated with the antidotes for methanol and
ethylene glycol poisoning: a comparison of ethanol and fomepizole. Ann Emerg Med 2009; 53:439.45. Boyer EW, Mejia M, Woolf A, Shannon M. Severe ethylene glycol ingestion treated without hemodialysis.
Pediatrics 2001; 107:172.46. Paasma R, Hovda KE, Tikkerberi A, Jacobsen D. Methanol mass poisoning in Estonia: outbreak in 154
patients. Clin Toxicol (Phila) 2007; 45:152.47. Naraqi S, Dethlefs RF, Slobodniuk RA, Sairere JS. An outbreak of acute methyl alcohol intoxication. Aust N Z
J Med 1979; 9:65.48. Burns MJ, Graudins A, Aaron CK, et al. Treatment of methanol poisoning with intravenous 4-methylpyrazole.
Ann Emerg Med 1997; 30:829.49. Bekka R, Borron SW, Astier A, et al. Treatment of methanol and isopropanol poisoning with intravenous
fomepizole. J Toxicol Clin Toxicol 2001; 39:59.50. Youssef GM, Hirsch DJ. Validation of a method to predict required dialysis time for cases of methanol and
ethylene glycol poisoning. Am J Kidney Dis 2005; 46:509.51. McMurray M, Carty D, Toffelmire EB. Predicting methanol clearance during hemodialysis when direct
measurement is not available. CANNT J 2002; 12:29.52. Burns AB, Bailie GR, Eisele G, et al. Use of pharmacokinetics to determine the duration of dialysis in
management of methanol poisoning. Am J Emerg Med 1998; 16:538.53. Chow MT, Di Silvestro VA, Yung CY, et al. Treatment of acute methanol intoxication with hemodialysis using
an ethanol-enriched, bicarbonate-based dialysate. Am J Kidney Dis 1997; 30:568.54. Dorval M, Pichette V, Cardinal J, et al. The use of an ethanol- and phosphate-enriched dialysate to maintain
stable serum ethanol levels during haemodialysis for methanol intoxication. Nephrol Dial Transplant 1999;14:1774.
55. Ghosh A, Boyd R. Leucovorin (calcium folinate) in "antifreeze" poisoning. Emerg Med J 2003; 20:466.56. McMartin KE, Martin-Amat G, Makar AB, Tephly TR. Methanol poisoning. V. Role of formate metabolism in the
monkey. J Pharmacol Exp Ther 1977; 201:564.

57. Hantson P, Vanormelingen P, Lecomte C, et al. Fatal methanol poisoning and organ donation: experience withseven cases in a single center. Transplant Proc 2000; 32:491.
58. López-Navidad A, Caballero F, González-Segura C, et al. Short- and long-term success of organstransplanted from acute methanol poisoned donors. Clin Transplant 2002; 16:151.
59. Caravati EM, Erdman AR, Christianson G, et al. Ethylene glycol exposure: an evidence-based consensusguideline for out-of-hospital management. Clin Toxicol (Phila) 2005; 43:327.
60. Woolf AD, Wynshaw-Boris A, Rinaldo P, Levy HL. Intentional infantile ethylene glycol poisoning presenting asan inherited metabolic disorder. J Pediatr 1992; 120:421.
61. Shoemaker JD, Lynch RE, Hoffmann JW, Sly WS. Misidentification of propionic acid as ethylene glycol in apatient with methylmalonic acidemia. J Pediatr 1992; 120:417.
Topic 336 Version 8.0

GRAPHICS
Rapid overview of methanol and ethylene glycol intoxication
To obtain emergent consultation with a medical toxicologist, call the United States Poison ControlNetwork at 1-800-222-1222, or access the World Health Organization's list of internationalpoison centers (www.who.int/gho/phe/chemical_safety/poisons_centres/en/index.html).
Clinical featuresEarly toxicity: CNS sedation and inebriation similar to ethanol intoxication
Late toxicity: metabolic acidosis with elevated anion gap; compensatory tachypnea/hyperpnea;coma in severe cases, accompanied by ocular toxicity (methanol) or renal failure (ethyleneglycol)
Diagnostic testingArterial or venous blood gas (to determine extent of acidosis)
Basic chemistry (to determine anion gap and renal function)
Serum osmolality (to help determine diagnosis)
Serum ethanol concentration (to help determine osmolal gap)
Serum calcium concentration (to rule out ethylene-glycol associated hypocalcemia)
Serum methanol, ethylene glycol, and isopropanol concentrations (to establish diagnosis)
Urinalysis (for oxalate crystals)
TreatmentSecure airway as necessary in severely intoxicated patients
Treat hypotension with intravenous crystalloid, followed by standard vasopressors as necessary
Block alchohol dehydrogenase with fomepizole, 15 mg/kg IV loading dose, followed by 10mg/kg q 12 h x 4 doses. If patient requires further treatment after this regimen, increase dose to15mg/kg every 12 hours
If fomepizole is unavailable or patient has a known allergy, block alcohol dehydrogenase withethanol, 10 mL/kg of a 10 percent ethanol solution, followed by 1 mL/kg of 10 percent ethanolsolution infused per hour. Titrate to serum ethanol concentration of 100 mg/dL.
Administer sodium bicarbonate, 1 to 2 meq/kg bolus followed by infusion of 132 meq NaHCO3in 1 L D5W to run at 200 to 250 mL/hour for patients with pH below 7.3
For patients with known or suspected methanol poisoning, administer folic acid, 50 mg IV everysix hours
For patients with known or suspected ethylene glycol poisoning, administer thiamine, 100 mgIV, and administer pyridoxine, 50 mg IV
If the diagnosis is uncertain but clinical suspicion is high, the clinician should initiate antidotaltreatment with alcohol dehydrogenase blockade and consultation for hemodialysis
Hemodialysis is indicated in severe toxicity, which we define as follows:Metabolic acidosis, regardless of drug level
Elevated serum methanol or ethylene glycol levels (more than 50 mg/dL; or methanol 15.6mmol/L, ethylene glycol 8.1 mmol/L), unless arterial pH is above 7.3
Evidence of end-organ damage (eg, visual changes, renal failure)

Methanol metabolism
* Blocked by ethanol and fomepizole.

Ethylene glycol metabolism
* Blocked by ethanol and fomepizole.

Major causes of metabolic acidosis according to mechanism and aniongap
Mechanism of acidosis Increased AG Normal AG
Increased acid production Lactic acidosis
Ketoacidosis
Diabetes mellitus
Starvation
Alcohol-associated
Ingestions
Methanol
Ethylene glycol
Aspirin
Toluene (if early) Toluene ingestion (if late due to urinaryexcretion of hippurate)
Diethylene glycol
Propylene glycol
D-lactic acidosis
Pyroglutamic acid (5-oxoproline)
Loss of bicarbonate orbicarbonate precursors
Diarrhea or other intestinal losses (eg,tube drainage)
Type 2 (proximal) renal tubularacidosis (RTA)
Posttreatment of ketoacidosis
Carbonic anhydrase inhibitors
Ureteral diversion (eg, ileal loop)
Decreased renal acid excretion Chronic kidneydisease
Some cases of chronic kidney disease
Type 1 (distal) RTA
Type 4 RTA (hypoaldosteronism)

Differential diagnosis of an elevated plasma osmolal gap
With anion gap metabolic acidosisEthylene glycol ingestion
Methanol ingestion
End-stage chronic kidney disease (GFR <10 mL/min) without regular dialysis
Diabetic ketoacidosis
Alcoholic ketoacidosis
Lactic acidosis
Formaldehyde ingestion
Paraldehyde ingestion
Without metabolic acidosisEthanol or isopropyl alcohol ingestion
Diethyl ether ingestion
Infusion of nonconductive glycine, sorbitol, or mannitol solutions
Severe hyperproteinemia
Severe hyperlipidemia

Urinary calcium oxalate monohydrate crystals underpolarized light
Urine sediment viewed under polarized light showing coarse,needle-shaped calcium oxalate monohydrate crystals. Thesecrystals have a similar appearance to hippurate crystals.Courtesy of W Merrill Hicks, MD.

Calcium oxalate crystals in the urine
Urine sediment showing both dumbbell-shaped calcium oxalatemonohydrate (long arrow) and envelope-shaped calcium oxalatedihydrate (short arrows) crystals. Although not shown, themonohydrate crystals may also have a needle-shapedappearance. The formation of calcium oxalate crystals isindependent of the urine pH.Courtesy of Frances Andrus, BA, Victoria Hospital, London, Ontario.

Indications for antidotal therapy with fomepizole or ethanol
Documented serum methanol or ethylene glycol concentration >20 mg/dL (methanol SIequivalent 6.2 mmol/L; ethylene glycol SI equivalent 3.2 mmol/L)
OR
Documented recent history of ingesting toxic amounts of methanol or ethylene glycol and serumosmol gap >10
OR
Strong clinical suspicion of methanol or ethylene glycol poisoning and at least two of thefollowing:
a) Arterial pH <7.3
b) Serum bicarbonate <20 meq/L (mmol/L)
c) Osmol gap >10
d) Urinary oxalate crystals present

© 2013 UpToDate, Inc. All rights reserved. | Subscription and License Agreement | Release: 20.12 - C21.4 Licensed to: UpToDate Individual Web - Anna Katharina Parsch, MD | Support Tag: [ecapp0604p.utd.com-115.70.110.227-5133E1C2B3-6.18.14-34375246]