Embed Size (px)
Citation preview
Nutrición Hospitalaria
ISSN: 0212-1611
info@nutriciónhospitalaria.com
Grupo Aula Médica
España
Ramírez Prada, D.; Delgado, G.; Hidalgo Patiño, C. A.; Pérez-Navero, J.; Gil Campos, M.
Using of WHO guidelines for the management of severe malnutrition to cases of marasmus and
kwashiorkor in a Colombia children's hospital
Nutrición Hospitalaria, vol. 26, núm. 5, septiembre-octubre, 2011, pp. 977-983
Grupo Aula Médica
Madrid, España
Available in: http://www.redalyc.org/articulo.oa?id=309228876009
How to cite
Complete issue
More information about this article
Journal's homepage in redalyc.org
Scientific Information System
Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal
Non-profit academic project, developed under the open access initiative
Nutr Hosp. 2011:26(5):977-983ISSN 0212-1611 • CODEN NUHOEQ
S.V.R.318
Original
Using ofWHO guidelines for the management ofsevere malnutritionto cases ofmarasmus and kwashiorkor in aColombia children's hospitalD. Ramírez Prada', G. Delgado', C. A. Hidalgo Patifío', J. Pérez-Navero- andM. Gil Campos'
'Paediatric Hospital Los Ángeles. Pasto. Colombia. -University ofNariño. Pasto. Colombia. 'Paediatric Research andMetabolims Unit. Reina Sofia University Hospital. Córdoba. Spain.
Abstract
Background: In 2007, the Hospital Infantil Los Ángeles(HILA) in Colombia implemented a slightly-modifiedversion ofthe WHO guidelines for the diagnosis and management ofmalnutrition during childhood.
Objective: To evaluate the efficacy ofthe WHO-HIL;\protocol in children hospitalized w~t~ severe, chron~c
marasmus and kwashiorkor malnutriticn (MS-KWK) m2007 and 2008.
Material and methods: In this descriptive retrospectivestudy the records of 100 children hospitalized with MSKWK were initially evaluated. Of these, 30 fulfilled theinclusion criteria: children of both sexes with a primarydiagnosis of MS- KWK. Patients with any chronic diseaseIiable to cause malnutrition were excluded. Anthropometric parameters, c1inical signs and biochemical indicators of malnutrition were assessed upon admission andagain at discharge following application of the WHOguidelines. Univariate analysis was performed for eachstudy variable; serum hemoglobin and albumin levels onadmission and at discharge were compared, and datawere subjected to bivariate analysis.
Results: Marasmus was diagnosed in 23.3% of children, kwashiorkor in 73.3% and marasmic kwashiorkorin 3.3%. The major c1inical findings were: edema (70%),emaciation (40%), "flag sign" hair (42.86%), low serumalbumin (93%) and anemia (80%). Thirteen children following the WHO-HILA protocol showed a significantnutritional status improvement (p < 0.05), whereas noimprovement was noted in the 17 children not treatedaccording to the protocoI.
Conclusions: Application of the WHO-HILA protocolwas associated with reduced morbimortality in childrenwith marasmus-kwashiorkor malnutrition. Implementationofthis protocol should therefore be considered in all children's hospitals in countries where this disease is prevalent.
(Nutr Hosp. 2011;26:977-983)
DOI:I0.330S/nh.2011.26.S.S1S0Key words: Marasmus. Kwashiorkor. Child malnutrition.
Nutrition disorders.
Correspondence: Mercedes Gil Campos.Paediatric Research and Metabolism Unít.Reina Sofia University Hospital.Avda. Menéndez Pidal, s/n.14004 Córdoba. Spain.E-mail: [email protected]
Recibido: 6-IX-20l0.l." Revisión: 25-XI-20l0.Aceptado: 2-XII-20l0.
APLICACIÓN DEL PROTOCOLO DE LA OMSDE MALNUTRICIÓN MARASMO-KWASHIORKOR
EN UN HOSPITAL DE COLOMBIA
Resumen
Introducción: En 2007, el Hospital Infantil de LosÁngeles (HILA) en Colombia implementó una versión delprotocolo-OMS para el diagnóstico y tratamiento de lamalnutrición en la infancia.
Objetivo: Evaluar la aplicación del protocolo de laOMS-HILA en niños hospitalizados con marasmo y/okwashiorkor (MS-KWK) durante 2007-2008.
Material y métodos: En este estudio retrospectivo, seevaluaron 100 niños hospitalizados con MS-KWK; 30cumplieron los criterios de inclusión: niños de ambossexos con MS-KWK primario. Los pacientes con enfermedades crónicas que pudieran causar desnutrición fueron excluidos. Se evaluaron determinados parámetrosantropométricos, y signos clínicos y bioquímicos de desnutrición según el protocolo de la OMS, al ingreso y alalta. Se realizó un análisis univariante; los niveles dehemoglobina y albúmina séricas fueron comparados alingreso y al alta, y los datos fueron sometidos a análisis dedos variables.
Resultados: Se diagnosticaron de marasmo al 23,3 % delos niños, de kwashiorkor al 73,3 % Y de kwashiorkormarásmico al 3,3 %. Los hallazgos clínicos más importantes fueron: edema (70%), emaciación (40%), "signo debandera" (42,86%), albúmina baja (93%) y anemia(80%). Trece niños mostraron mejoría significativa delestado nutricional tras aplicar el protocolo OMS-HILA(p < 0,05), mientras que no ocurrió en 17 niños no tratados según el protocolo.
Conclusiones: La aplicación del protocolo de la OMSHILA se asoció con una reducción de la morbimortalidaden los niños con desnutrición marasmo-kwashiorkor. Laaplicación completa y continuada de este protocolo debeser considerada en los hospitales infantiles de todos lospaíses donde esta enfermedad es prevalente.
(Nutr Hosp. 2011;26:977-983)
DOI:I0.330S/nh.2011.26.S.S1S0Palabras clave: Marasmo. Kwashiorkor. Desnutrición infan
til. Patología nutriciona!.
977

Abbreviations
MS-KWK: Marasmic kwashiorkor.HILA: Hospital Infantil Los Ángeles.
Introduction
Although malnutrition may arise at any stage in life,its occurrence in childr en is particularly noteworthy forits detrimental effect on gro wth and development.Severe chronic malnutrit ion generally occurs duringinfancy and early childhoo d .' In countries at risk formalnutrition, after weaning -which often starts beforethe fourth month- chil dren rece ive little or no dairyfood or other produ cts of animal origin oA low-protein,low-energy diet ocoup led with freguent dige sti ve andrespiratory infections, favours the slow but progressivedevelopment of severe malnutr ition.'
Signs leadin g to the diagnosis of chronic malnutrition inelude low height and weight for age, indicatingstunted growth , whilst the most common biochemicalalterations are low serum hemoglobin and albumin levels: on admission to hospital. patients may also displayhypoglycemia and ion deficiencies.'
Marasmus is a form of chronic malnutrition charac teri zed clinica lly by severe was ting of subcu taneo ustissue, musele and fatowhich gives rise to a wizened,wrinkled appearance. Affec ted childre n tend to bewea k and listl ess, displ aying loss of appe tite anddec reased food tolerance. due to a diet defi cient incalories, macronutri ents and micronut rient s.v'
Kwashiorkor is more freguent in infants with proteindeficiency but adeguate car bohydrate intake' . Seru mprotein and especially albumi n depletion tends to bemore severe in this form of malnutrition, which is associated with a higher risk of infection. Weight is often adeguate for age, and elinical signs inelude the characteristic so-called "moon face", depigmented hair (the "flagsign"), edemas mainl y in the limbs, bloated abdomen.whimpering and irritability. In the mixed formoknow nas marasmi c kwa shiorkor, children display features ofboth types, the most common combination being wasting of subcutaneous tissue, limb edemas. enlarged liverand severe serum protein depletion. "
Accor ding to the National Survey on Nut riti onalStatus in Colombi a (ENSIN). carried out in 2005. thesouth-western department of Nar iño has one of thecountrys wors t reco rds for chro nic malnutrition andretarded growth'. All childre n in thi s area displayingcritical mara smic-kwashiorkor (MS-KWK) malnutrition are referre d to the thi rd-l evel "Hos pital InfantilLos Ángeles" (HIL A). since - due to diffi culty ofaccess and eco nomic co nditions- cases are not diagnosed and treated by local primary healthcare services .
The man agement of pati ent s with sev ere, chroni cMS-KWK malnutrition represe nts something of a challcnge, since thi s co ndition is often associated withcomplications such as hypothermia, hypoglycemia and
infection. which worsen the prognosis. Once patientswith chroni c malnutriti on are hospi talized. the mainaim of treatment is to stabilize hemodynamic function,address pathologies associa ted primaril y with gastrointest inal. ge nitourinary and respi rat ory infec tion, andwork towards the recovery of adeguate nutritional status. Nutritional recovery may take several yea rs,depending on the sever ity of malnutrition." In 2000.the World Health Organiz ation (WHO) set out guidelines for the inpatient management of protein-energymalnutrition (MS-KWK); these have been periodicallyupdated since then. " In 2007. aware of the child malnutrition problem at region al level, the Hospital Infantil Los Ángeles (HILA) impl ement ed a slightlyadap ted version of the WHO guide lin es aimed atimproving the diagnosis and management of childrenwith severe malnutrition . The HILA programme comprised a stabi lization ph ase fo llowed by outpatientcheck-ups intended to achieve full health recovery.
The protocol was established to diagnose and to treatin agree ment with the guidelines of the WHO. and hospital personnel became gualified for it' s use. Nevertheless. the profe ssion als who covered occasional turn sand weekends did not apply it. poss ibly due to lack ofknowledge. In other occasions, when the cause of theadmiss ion was another disease, a suitable nutritionaldiagnosis was obviated. For the childre n who did notfo llow the pr otocol, the modified formul as prop oseF75 and FIOOby the WHO were not provided to them,did not have the suitable isolation or the necessary controls on the admission or at discharge, and seemed thatthe evo lution was not the expec ted one. For this reaso n,the ai m of this study was if demonstrable differen cebetween both groups existed, already defi ned a prioriby the action ofthe profe ssionals, and if the applicationof this protocol was effective to diagn ose and to dealsuitably with the children with this type of undernourishment.
However, local adoption of the HILA protocol forthe management of MS-KWK malnutriti on has not yetled to the full achievement of initial objectives, sincethe protocol ha s not been used for all children withdiagnosed malnutrition .
Th is study sought to eva luate the applica tion of theWHO-HILA and the results obtained from the treatment of pedi atric pati ent s with severe. chro nic MSKWK malnutrition admitted in 2007 and 2008.
Material and methods
Thi s descripti ve retrospect ive study evalua ted datadrawn from the elinical records of children admitted tothe "Hospital Infantil Los Ángeles" in Nariño (Colombia) with severe malnutrit ion between Janu ary 2007and December 2008 . Of a total of 100 such patients, 30cases fulfilling inelusion criteria were selected for thestudy. Inelusion criteria were : ch ildren of both sexe s,hospit alized in the period 2007-2 008. with a primary
978 Nutr Hosp, 2011;26(5):977-983 D. Ramírez Prada et al.
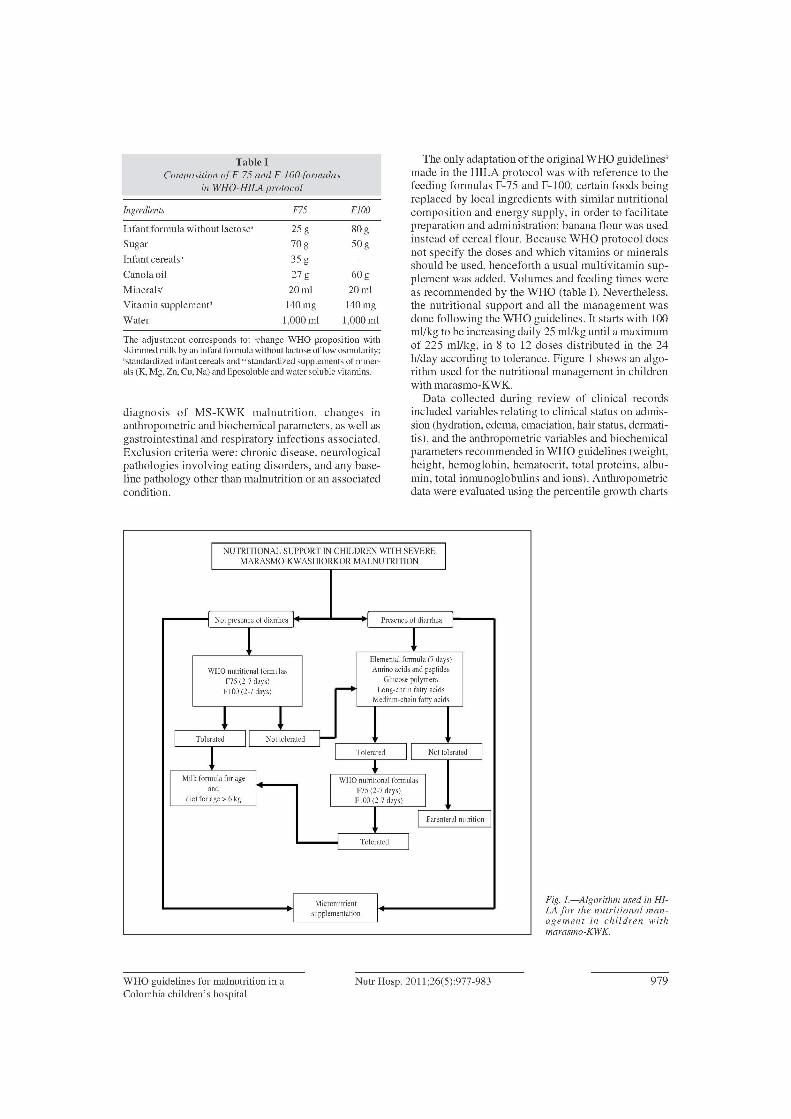
Table 1Comnosition ofF-75 and F-iOO formulas
in WHO-HlLAprotocol
Ingredients F75 FlOO
Infant formula without Iactose- 25 g 80g
Sugar 70g 50g
Infant cereals" 35 g
Canolaoil 27 g 60g
Minerals- 20 mI 20 mI
Vitamin supplement- 140mg 140mg
Water 1,000 mI 1,000 mI
The adjustment corresponds to: -changc WHO proposition withskimmedmilk by an infant formulawithout lactoseof low osmolarity;"standardizedinfant cereals and"standardized supplementsof minerals (K, Mg, Zn, Cu, Na) and liposolubleand water solublevitamins.
diagnosis of MS-KWK malnutrition, changes inanthropometric and biochemical parameters, as well asgastrointestinal and respiratory infections associated.Exclusion criteria were: chronic disease, neurologicalpathologies involving eating disorders, and any baseline pathology other than malnutrition or an associatedcondition.
The only adaptation of the original WHO guidelines"made in the HILA protocol was with reference to thefeeding formulas F-75 and F-lOO, certain foods beingreplaced by local ingredients with similar nutritionalcomposition and energy supply, in order to facilitatepreparation and administration: banana flour was usedinstead of cereal flour. Because WHO protocol doesnot specify the doses and which vitamins or mineralsshould be used, henceforth a usual multivitamin supplement was added. Volumes and feeding times wereas recommended by the WHO (table I). Nevertheless,the nutritional support and all the management wasdone following the WHO guidelines. It starts with 100mlJkg to be increasing daily 25 ml/kg until a maximumof 225 ml/kg, in 8 to 12 doses distributed in the 24h/day according to tolerance. Figure 1 shows an algorithm used for the nutritional management in childrenwith marasmo-KWK.
Data collected during review of clinical recordsincluded variables relating to clinical status on admission (hydration, edema, emaciation, hair status, dermatitis), and the anthropometric variables and biochemicalparameters recommended in WHO guidelines (weight,height, hemoglobin, hematocrit, total proteins, albumin, total inmunoglobulins and ions). Anthropometricdata were evaluated using the percentile growth charts
Fig. I.-AIgorithm used in HiLA Jor the nutritional management in children withmarasmo-KWK.
INUTRITIONAL SUPPORT IN CHILDREN WITHSEVERE
MARASMO-KWASHIORKOR MALNUTRITION
Not presenceof diarrhea Presenceof diarrhea
1 !Elementalformula (7 days)
WHOnutritionalformulas Amina acids and peptides
F75 (2-7 days)~
Glucosepolymers
FIOO (2-7 days) Long-chainfatty acidsMedium-chainfatty acids
1 1 11 Tolerated 11 Not tolerated f-! Tolerated 11 Not tolerated 1
-l
I
Milk formulafor age I WHOnutritionalformulas Iand
IF75 (2-7 days)
diet for age > 6 kg FIOO (2-7 days)
1 I Parenteralnutrition
Tolerated 1
I Micronutrient II supplementation I
WRO guidelines for malnutrition in aColombia children's hospital
Nutr Hosp, 2011;26(5):977-983 979
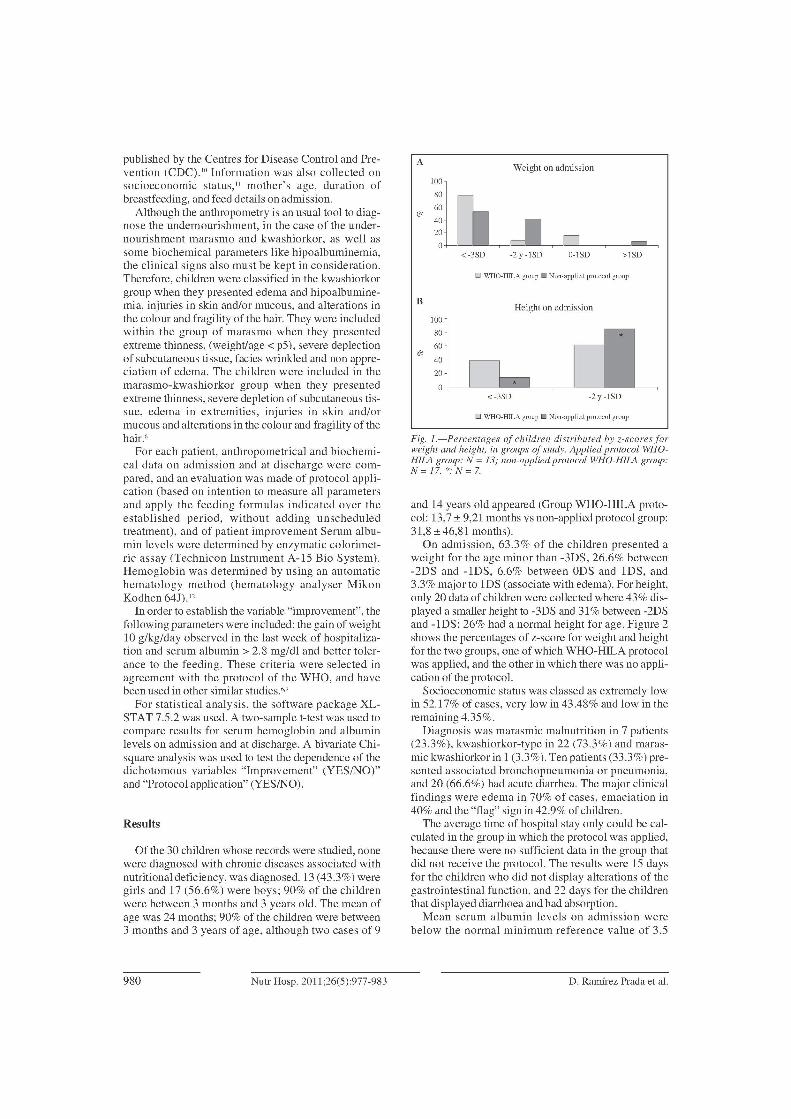
o WHO-HILA group • Non-applied protocol group
o WHO-HILA group • Non-applied protocol group
Fig. 1.-Percentages of children distributed by z-scores forweight and height. in groups of study. Applied protocol WHOHILA group: N = 13; non-applied protocol WHO-HlLA group:N=17. *:N=7.
->lSD
-2y -lSD
o0-lSD
Height on admission
Weight on admission
<-3SD
A
~ l:~;j ~40
20
o '------~-'----'--~---___,
<-3SD -2y-1SD
B
100
80
60t'2
40
20
and 14 years old appeared (Group WHO-HILA protocol: 13,7 ± 9,21 months vs non-applied protocol group:31,8 ±46,81 months).
On admission, 63.3% of the children presented aweight for the age minor than -3DS, 26.6% between-2DS and -lDS, 6.6% between ODS and lDS, and3.3% major to lDS (associate with edema). For height,only 20 data of children were collected where 43% displayed a smaller height to -3DS and 31% between -2DSand -lDS; 26% had a normal height for age. Figure 2shows the percentages of z-score for weight and heightfor the two groups, one of which WHO-HILA protocolwas applied, and the other in which there was no application of the protocol.
Socioeconomic status was classed as extremely lowin 52.17% of cases, very low in 43.48% and low in theremaining 4.35%.
Diagnosis was marasmic malnutrition in 7 patients(23.3%), kwashiorkor-type in 22 (73.3%) and marasmic kwashiorkor in 1 (3.3%). Ten patients (33.3%) presented associated bronchopneumonia or pneumonia,and 20 (66.6%) had acute diarrhea. The major clinicalfindings were edema in 70% of cases, emaciation in40% and the "flag" sign in 42.9% of children.
The average time of hospital stay only could be calculated in the group in which the protocol was applied,because there were no sufficient data in the group thatdid not receive the protocol. The results were 15 daysfor the children who did not display alterations of thegastrointestinal function, and 22 days for the childrenthat displayed diarrhoea and bad absorption.
Mean serum albumin levels on admission werebelow the normal minimum reference value of 3.5
Of the 30 children whose records were studied, nonewere diagnosed with chronic diseases associated withnutritional deficiency, was diagnosed. 13 (43.3%) weregirls and 17 (56.6%) were boys; 90% of the childrenwere between 3 months and 3 years old. The mean ofage was 24 months; 90% of the children were between3 months and 3 years of age, although two cases of 9
published by the Centres for Disease Control and Prevention (CDC).1O Information was al so collected onsocioeconomic status," mothcr's age, duration ofbreastfeeding, and feed details on admission.
Although the anthropometry is an usual tool to diagnose the undernourishment, in the case of the undernourishment marasmo and kwashiorkor, as well assorne biochemical parameters like hipoalbuminemia,the clinical signs also must be kept in consideration.Therefore, children were classified in the kwashiorkorgroup when they presented edema and hipoalbuminemia, injuries in skin and/or mucous, and alterations inthe colour and fragility of the hair. They were includedwithin the group of marasmo when they presentedextreme thinness, (weight/age < p5), severe deplectionof subcutaneous tissue, facies wrinkled and non appreciation of edema. The children were included in themarasmo-kwashiorkor group when they presentedextreme thinness, severe depletion of subcutaneous tissue, edema in extremities, injuries in skin and/ormucous and alterations in the colour and fragility ofthehair."
For each patient, anthropometrical and biochemical data on admission and at discharge were compared, and an evaluation was made of protocol application (based on intention to measure all parametersand apply the feeding formulas indicated over theestablished period, without adding unscheduledtreatrnent), and of patient improvement Serum albumin levels were determined by enzymatic colorimetric assay (Technicon Instrument A-15 Bio System).Hemoglobin was determined by using an automatichematology method (hematology analyser MikonKodhen 64J)."
In order to establish the variable "improvement", thefollowing parameters were included: the gain of weight10 g/kg/day observed in the last week of hospitalization and serum albumin > 2.8 mg/dl and better tolerance to the feeding. These criteria were selected inagreement with the protocol of the WHO, and ha vebeen used in other similar studies.?"
For statistical analysis, the software package XLSTAT 7.5.2 was used. A two-sample t-test was used tocompare results for serum hemoglobin and albuminlevels on admission and at discharge. A bivariate Chisquare analysis was used to test the dependence of thedichotomous variables "Improvement" (YES/NO)"and "Protocol application" (YES/NO).
Results
980 Nutr Hosp, 2011;26(5):977-983 D. Ramírez Prada el al.
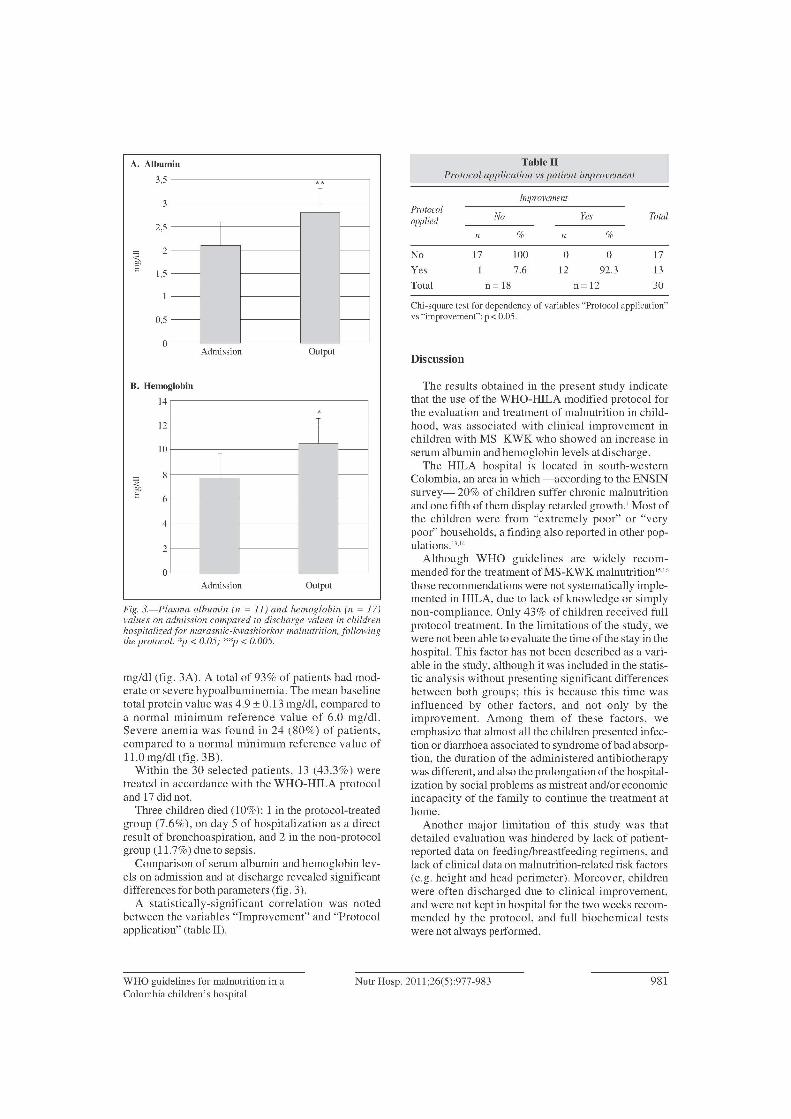
Table 11Protocol application vs paticnt improvement
ImprovemeniProtocol
No fes Totalapplied
n % n %
No 17 100 O O 17
Yes 1 7.6 12 92.3 13
Total n= 18 n= 12 30
Discussion
Chi-square test for dependency of variables "Protocol application"vs "improvcmcnt":p < 0.05.
OutputAdmissian
**T
T r---I
r--- r---
r--- r---
r--- r---
r--- r---
o
1,5
0,5
2
2,5
3
A. Albumin
3,5
Fig. 3.-Plasma albumin (n = 11) and hemoglobin (n = 17)values on admission compared to discharge values in childrenhospitalized for marasmic-kwashiorkor malnutrition, followingthe protocol. *1' < 0.05; **1'< 0.005.
mg/dl (fig. 3A). A total of 93% of patients had moderate or severe hypoalbuminemia. The mean baselinetotal protein value was 4.9 ± 0.13 mg/dl, compared toa normal minimum reference value of 6.0 mg/dl.Severe anemia was found in 24 (80%) of patients,compared to a normal minimum reference value ofll.O mg/dl (fig. 3B).
Within the 30 selected patients, 13 (43.3%) weretreated in accordance with the WHO-HILA protocoland 17 did not.
Three children died (10%): 1 in the protocol-treatedgroup (7.6%), on day 5 ofhospitalization as a directresult of bronchoaspiration, and 2 in the non-protocolgroup (11.7%) due to sepsis.
Comparison of serum albumin and hemoglobin levels on admission and at discharge revealed significantdifferences for both parameters (fig. 3).
A statistically-significant correlation was notedbetween the variables "Improvement" and "Protocolapplication" (table II).
The results obtained in the present study indicatethat the use of the WHO-HILA modified protocol forthe evaluation and treatment of malnutrition in childhood, was associated with clinical improvement inchildren with MS-KWK who showed an increase inserum albumin and hemoglobin levels at discharge.
The HILA hospital is located in south-westernColombia, an area in which -according to the ENSINsurvey- 20% of children suffer chronic malnutritionand one fifth of them display retarded growth. 1 Most ofthe children were from "extremely poor" or "verypoor" households, a finding also reported in other populations.'>"
Although WHO guidelines are widely recommended for the treatment ofMS-KWK malnutrition"-"those recommendations were not systematically implemented in HILA, due to lack ofknowledge or simplynon-compliance. Only 43% of children received fullprotocol treatment. In the limitations of the study, wewere not been able to evaluate the time of the stay in thehospital. This factor has not been described as a variable in the study, although it was included in the statistic analysis without presenting significant differencesbetween both groups; this is because this time wasinfluenced by other factors, and not only by theimprovement. Among them of these factors, weemphasize that almost all the children presented infection or diarrhoea associated to syndrome ofbad absorption, the duration of the administered antibiotherapywas different, and also the prolongation of the hospitalization by social problems as mistreat and/or economicincapacity of the family to continue the treatment athome.
Another major limitation of this study was thatdetailed evaluation was hindered by lack of patientreported data on feeding/breastfeeding regimcns, andlack of clinical data on malnutrition-related risk factors(e.g. height and head perimeter). Moreover, childrenwere often discharged due to clinical improvement,and were not kept in hospital for the two weeks recommended by the protocol, and full biochemical testswere not always performed.
OutputAdmissian
*T
~
Ir---
r---
f---- f----
f---- r---
f---- f----2
o
4
6
10
12
B. Hemaglabin
14
WRO guidelines for malnutrition in aColombia children's hospital
Nutr Hosp, 2011;26(5):977-983 981

As in other countries, kwashiorkor was found to bemore common than marasmus among children withchronic malnutrition."-" Children were often referrednot for malnutrition but for associated conditions,including respiratory infections, hemodynamic instability, persistent diarrhea or even malabsorption syndrome. Sepsis was the main cause of death amongstthese patients.":"
The effects of severe malnutrition are usually multisystemic. Initialloss of muscle mass is followed in themost severe cases by marked depletion of subcutaneous fat.> Edema is a characteristic sign of decliningserum albumin levels, and is associated with greatermorbimortality." Skin diseases develop due to chronicvitarnin and micronutrient deficiencies."-" Children inthis study displayed edema, severe muscular emaciation and depigmented hair ("flag" sign), all of whichare clinical signs of severe malnutrition. In the presentstudy, the depletion of subcutaneous fat stores wasreversed, and tissue/mucosa lesions improved, in thesecond week of treatment using nutritional recoveryformulas.
Low albumin levels and deficiency anemias werecornmon on adrnission -as in most reported patients-i-"but a notable recovery was recorded by the end of protocol-based treatment. Most children displayed moderate or severe hypoalbuminemia and severe primaryiron-deficiency or vitamin A-deficiency; these constitute a major public health problem in Colombia'.Increased albumin and hemoglobin levels by discharge(fig. 1) suggested a satisfactory response among children treated in accordance with the WHO-HILA protocol. In the six non-protocol children displayingincreased hemoglobin levels, the increase was attributed to transfusions on adrnission. There is no consensus in the literature on the advisability of transfusionsand serum albumin replacement therapy.v A study carried out in Ethiopia suggested that these proceduresshould be lirnited to cases of severe anemia (hemoglobin 4 mg/dl and hematocrit 12%) and critical albumindeficiency (no specific values adduced).'4 Indeed,Bachou et al. (2008)," reporting on the application theWHO guidelines in malnourished children in Africa,recorded greater mortality among those receivingblood transfusions or intravenous fluids on admission(73% of total deaths), concluding that application ofthe WHO protocol could reduce the need for transfusions, and lower the mortality rate.
In the present study, the overall mortality rate was10%, a percentage similar to that reported elsewhere inColombia and Latin America. '4,26 None of the childrenin the non-protocol group displayed any improvement,whilst 92.3% of children in the protocol-treated groupshowed sorne improvement (table II). Among the factors associated with mortality in these patients are thedifficulty in ensuring strict isolation, and the exposureof patients to nosocomial infections. Moreover, giventhe patients' poor clinical condition, symptoms ofinfection -such as fever- may not always appear, so
that appropriate antibiotic therapy may not be implemented.'? Given the persistently high incidence of disease and death among children with MS-KWK malnutrition, these patients require exhaustive evaluation andconstant monitoring. In conclusion, using the WHOHILA protocol was associated with an improvement innutritional and overall health status of severely malnourished children. Implementation of the protocolshould therefore be considered in all children's hospital s in developing countries where this pathology isprevalent. In general, prospective studies should becarried out in patients with protein-energy malnutrition, in order to monitor the systematic application ofthe WHO guidelines and ensure their beneficial effectson child health.
References
1. Instituto Colombiano de Bienestar Familiar. Encuesta nacionalde la situación nutricional en Colombia, ENSIN 2005; 30 p.
2. Vega-Franco L. Hitos conceptuales en la desnutrición proteicaenergética. Salud Pública Mex 1999; 41: 328-333.
3. Jahoor F, Badaloo A, Reid M, Forrester T. Protein metabolismin severe childhood malnutrition. Ann Trop Paediatr 2008; 28:87-101.
4. Müller O, Krawinkel M. Malnutrition and health in developingcountries. CMAJ2005; 173: 279-86.
5. SimporeJ, KaboreF,ZongoF , DansouD , BereA ,Pignatelli Set al. Nutrition rehabilitation of undernourished children utilizing Spiruline and Misola. Nutr J2006; 5: 3.
6. Maitland K, Berkley JA, Shebbe M, Peshu N, English M, Newton CR. Children with Severe Malnutrition: Can Those at Highest Risk ofDeath Be Identified with the WHO Protocol? PLoSMedicine 2003; 326: 146-51.
7. Bhan MK, Bhandari N, Bahl R. Management of the severelymalnourished child: perspective from developing countries.BMJ2003;326: 146-51.
8. Scherbaum V, Fürst P. New concepts on nutritional management of severe malnutrition: the role of protein. Curr Opin ClinNutr Metab Care 2000; 3: 31-8.
9. World Health Organization. Management of severe malnutrition. A manual for physicians and other senior health workers.Geneva: World Health Organization, 1999.
10. Kuczmarski RI, Ogden CL, Grummer-Strawn LM, Flegal KM,Guo SS, Wei R et al. CDC Growth Charts: United States.Advance data frorn vital and health statistics; no 314.Hyattsville, Maryland: National Center for Health Statistics.2000. www.cdc.gov/growthcharts.
11. Departamento Administrativo Nacional de Estadística, DANE.Estratificación socio económica, versión Mayo 2004. http://www.redbogota.com/home/archivos_extension/20062/
12. Doumas BT, Watson WA, Biggs HG. Albumin standards andthe measurement of serum albumin with bromocresol green.Clin ChimActa 1971: 31: 87-96.
13. Acevedo E, Sanabria MC, Castillo Durán C. Kwashiorkor ymarasmo-kwashiorkor en niños hospitalizados. Pediatr (Asunción) 2004; 1: 31.
14. Weisstaub G, Soria R, Araya M. SevereMalnutrition in a Pediatrics Hospital. Rev Soc Bol Ped 2006; 45: 90-4.
15. Deen J, FunkM, Guevara V, Saloojee H, Doe J, Palmer A, et al.Implementation of WHO guidelines on management of severemalnutrition in hospitals in Africa, World Health Organization.Bulletin ofthe WorldHealth Organization. Geneva: 2003; 81: 237.
16. Ashworth A, Chopra M, McCoy D, Sanders D, Jackson D,Karaolis N et al. WHO guidelines for management of severemalnutrition in rural South African hospitals: effect on casefatality and the influence of operational factors. Lancet 2004;363: 1110-15.
982 Nutr Hosp, 2011;26(5):977-983 D. Ramírez Prada el al.

17. Cartmell E. Natalal H. Francois l. Ferreira MH. Grahnquist L.Nutritional and clinical status of children admitted to the malnutrition ward, Maputo central hospital: a comparison of datafrom 2001 and 1983. J Trop Pediatr 2005; 51: 102-5.
18. Brewster DR. Critical appraisal of the management of severemalnutrition: 3. Complications. J Paediatr Child Health 2006;42: 583-93.
19. Saccardo Sarni RO. Suano de Souza FI. Catherino p. Kochi C.Ceragioli Oliveira FL. de Nobrega FJ. Treatment of severelymalnourished children with WHO protocolo experience of areferral center in Sao Paulo, Brazil. Arch Latinoam Nutr 2005;55: 336-44.
20. Heath ML. Sidbury R. Cutaneous manifestations of nutritionaldcficicncy. Curr Opin Pediatr 2006; 18: 417-22.
21. Velasquez Rodriguez CM. Parra Sosa B. Morales Mira G.Agudelo G. Cardona O. Bernal C. et al. M. "Free" iron, transíerrin and ferritin levels in serum and their relation with severemalnutrition. An Pediatr IBarc¡ 2007; 66: 17-23.
22. Weisstaub G. Medina M. Pizarro F. Araya M. Copper, iron, and
zinc status in children with moderate and severe acute malnutrition recovered tollowing WHO protocols. Biol Trace Elem Res2008; 124: 1-11.
23. Jahoor F. Badaloo A. Reid M. Forrester T. Protein kinetic diIíerences between children with edematous and nonedematoussevere childhood undernutrition in the fed and postabsorptivestates. Am J cu« Nutr 2005; 82: 792-800.
24. GoldenM. GrelletyY. Protocol for the managementof severeacutemalnutrition. Federal Ministry ofHealth. Etiophya: 2007. Available al: http://titun.etharc.orglresources/guidelinesresources/adultandadolescentguidelines/samguidelinetinalmarch2007.pdI
25. Bachou H. Tumwine JK. Mwadime RK. Ahmed T. Tylleskar T.Reduction oIunnecessary transfusion and intravenous fluids inseverely malnourished children is not enough to reduce mortality. Ann Trop Paediatr 2008; 28: 23-33.
26. Bernal C. Velasquez C. Alcaraz G. Botero J. Treatment ofsevere malnutrition in children: experience in implementing theWorld Health Organization guidelines in Turbo. Colombia.J Pediatr Gastroenterol Nutr 2008; 46: 322-8.
WRO guidelines for malnutrition in aColombia children's hospital
Nutr Hosp, 2011;26(5):977-983 983
![Diet and kwashiorkor: a prospective study from rural DR Congo filethose with kwashiorkor [2, 3] Kwashiorkor and marasmus are characterised by different metabolic response to severe](https://img.pdfslide.us/doc/110x75/5e0e221d94d92e23bf1821df/diet-and-kwashiorkor-a-prospective-study-from-rural-dr-congo-with-kwashiorkor-2.jpg)




























